
Oblique Facial Clefts: Pathology, Etiology, and...
14
Oblique Facial Clefts: Pathology, Etiology, and Reconstruction J. C. H. van der Meulen, M.D. Rotterdam, The Netherlands Reprinted from PLASTIC AND RECONSTRUCTIVE SuRGERY Copyrighted by The American Society of Plastic and Reconstructive Surgeons August 1985
Transcript of Oblique Facial Clefts: Pathology, Etiology, and...
Oblique Facial Clefts: Pathology, Etiology, and Reconstruction J. C. H. van der Meulen, M.D.
Rotterdam, The Netherlands
Reprinted from PLASTIC AND RECONSTRUCTIVE SuRGERY
Copyrighted by The American Society of Plastic and Reconstructive Surgeons
August 1985

Oblique Facial Clefts: Pathology, Etiology, and Reconstruction J. C. H. van der Meulen, M.D. Rullerdam, The Netherlands
Modern views on embryology have increased our undel·standing of the nature of oblique facial clefts. The anomalies that have their origin at the junction of facial processes, such as the nasomaxillary dysplasias, may be named primary clefts or transformation. The maxillary clefts that arc due to a developmental arrest of the skeleton are in fact secondary defects of differentiation defects. The teratology of these malformations is discussed, and attention is drawn to the amniotic rupture syndrome as a possible cause.
All these clefts are rare, their incidence ranging from 0.75 to 5.4 per 1000 common clefts. This author has been involved in the treatment of nine of these patients. Four harl their malformation reconstructed with one of the conventional procedures described in the literature, but the results, although initially acceptable, soon deteriorated. A more aggressive approach was therefore chosen. Rotation and advancement of the cheek proved to be extremely effective and is now advocated as the procedure of choice. The transposition of a median forehead flap is considered an excellent alteruative. Use of these procedures in five patients is reported. There were no complications.
Oblique clefts, excepting only the mildest forms, are a catastrophic facial anomaly. Usually multiple operations are required for reconstruction and the results in n1ost cases are Eu fron1 ideal. 1
Although oblique facial clefts had been reported before,' in 18 2 3 Laroche" was the first to differentiate between ordinary cleft lip or harelip and clefts of the cheek. Further distinction was made in 1864 by Pelvet,' who separated oblique clefts involving the nose from the other cheek clefts. Drawing on Ahlfeld's work,' in 1887 Morian6 collected 29 cases from the literature, contributing 7 cases of his own. Morian recognized three different groups of oblique facial
clefts. Since then, excellent reviews have been written by Griinberg7 in 1913, Boo-Chai' in 1970, and Millard9 in 1977.
This paper is devoted to the morphology and morphogenesis of oblique facial clefts, to their etiology, and to the principles used in correcting some of these malformations.
MORPHOLOGY AND MORPHOGENESIS
Oblique facial clefts have been classified according to the following:
I. The direction they take, which may be oronaso-ocular (oculonasal) or oro-ocular (oculofacial). The latter type is being subdivided 10 into oromedial canthal and orolateral canthal, depending on the relationship of the defect to the infraorbital foramen.
2. The period in which the development was disturbed, e.g., primary or secondary clefting.7
3. The position of one cleft in relation to the other (Morian6 I, II, III; Tessier 11 3, 4, 5).
4. The areas in which the malformations have their origin: nasomaxillary 12
-14 and maxil
lary (medial and lateral) dysplasia13· 14
Other craniofacial malformations, such as encephaloceles,6 hydrocephaly, 15 widow's peak or cow's lick, 12
• 16 hypertelorism, 17
• 18 choanal atre
sia/6· 19 anophthalmia and microphthalmia, 12· 16
colobomata of the iris, 1' or choroid20 and epibulbar dermoids, 17' 21 ·22 have also been reported, and associated deformities, such as constric-
From lhe Department of Plastic and Recon.~truclive Surgery at the Academy Hospital Rotterdarn-Dijkzigt. Received for publication September 10, 1984; revised .January 28, 1985.
Pre~enled at the Intemalional Congress of Plastic and Reconstructive Surgery, in June of 1983, in Montreal, Canada.
212
Vol. 76, No. 2 j OBLIQUE FACIAL CLEFTS
tion rings of the limbs, 1·8
·12
· 10
· 19 aplasia cutis con
genita, 19 club feet, 12 and ectopia vesicae, 12 have been described.
Nasomaxillary Dysplasia
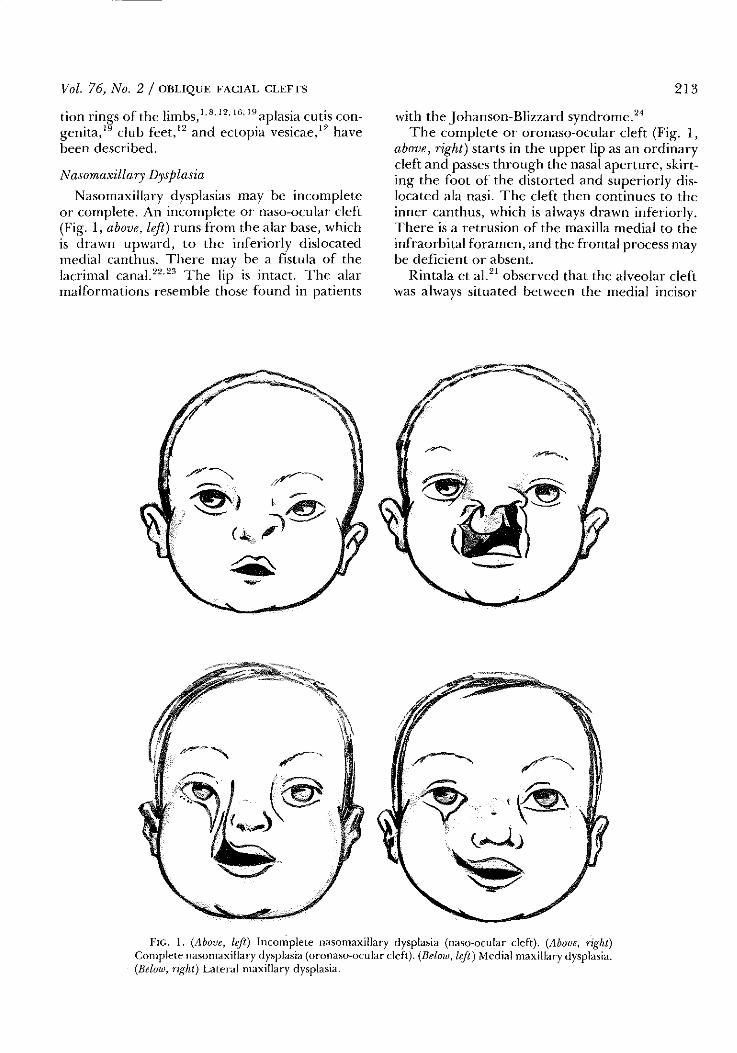
Nasomaxillary dysplasias may be incomplete or complete. An incomplete or naso-ocular cleft (Fig. I, above, left) runs from the alar base, which is drawn upward, to the inferiorly dislocated medial canthus. There may be a fistula of the lacrimal canal. 22
'23 The lip is intact. The alar
malformations resemble those found in patients
213
with the Johanson-Blizzard syndrome.21
The complete or oronaso-ocular cleft (Fig. I, above, right) starts in the upper lip as an ordinary cleft and passes through the nasal aperture, skirting the foot of the distorted and superiorly dislocated ala nasi. The cleft then continues to the inner canthus, which is always drawn inferiorly. There is a retrusion of the maxilla medial to the infraorbital foramen, and the frontal process may be deficient or absent.
Rintala et al. 21 observed that the alveolar cleft was always situated between the medial incisor
FIG. I. (Above, left) Incomplete nasomaxillary dysplasia (naso-ocular cleft). (Above, right) Complete nasomaxillary dysplasia (oronaso-ocular cleft). (Below, lefl) Medial maxillary dysplasia. (Below, right) Lateral maxillary dysplasia.

214 PLASTIC AND RECONSTRUCTIVE SURGERY, August 1985
and the canine tooth, while the lateral incisor was frequently missing. The complete cleft is frequently associated with a palatal cleft.6
· 16 The
nasolacrimal apparatus is deficient in the majority of cases.
The morphology of these clefts can be simply explained 13 on the basis of early embryonic development of the face up to and including the 17-mm C.RL stage and that of the secondary palate from the 27-mm C.RL stage on. An incomplete or naso-ocular cleft will result when the disturbance in fusion is restricted to the lateranasal and maxillary processes. In these patients, the lip will develop normally. A complete or oronaso-ocular cleft will occur when fusion between the medial nasal and maxillary processes is also disturbed. A cleft between the medial and lateral incisors, if present,6 may be explained by one of the dental anomalies so common in cleft palate patients, such as agenesis or a supernumerary element.
The appearance of the incomplete as well as of the complete cleft will depend on the period in which the arrest occurred. If the arrest occurs before the different processes have merged at the 17-mm C.RL stage, the lacrimal canal will fail to form and a so-called primary or transfonnation 13 defect will be formed. If the disturbance takes place after closure of the ectodenn of the face has been completed and a canal has been produced, a secondary or differentiation defect13 will result.
Maxillary Dysplasia (Medial)
In this deformity, the cleft (Fig. I, below, left) extends from the lip midway between the philtrum and the oral commissure, proceeding laterally from the intact but superiorly dislocated nasal aperture to a lower lid coloboma. The maxilla, medial t.o the infraorbital foramen, is always hypoplastic, causing a severe retrusion of the rim of the piriform aperture and a funnelshaped concavity (infundibulum) in the medial or anterior part of the orbital floor. There may be a cleft in the alveolus between the lateral incisor and the canine tooth or, rarely, between two incisors, as Morian6 reported. In his case, however, the incisor lateral to the cleft proved to be supernumerary. Not surprisingly, clefting of the palate, whether complete or partial, has also been reported, and malformations of the nasolacrin1al apparatus have been observed in the majority of patients. The morphogenesis of this cleft can now be explained on the basis of known embryologic theories. The presence of a
normal nasal aperture is proof that fusion of the facial processes has been normal and, consequently, the development arrest has occurred after the 17-mm C.RL stage, when the ectoderm of the face has closed. 13 The resulting secondary or differentiation defects 13 may produce an hourglass deformity 14 with the developmental arrest in the middle and a coloboma at both ends. The many defects of the nasolacrimal apparatus that are found in some of these patients have been extensively described by Ask and van der Hoeven.25 Their morphogenesis has recently been explained by Vermeij-Keers et al. 26
Maxillary Dysplasia (Lateral)
This cleft (Fig. I, below, right) starts in the lip, in or near the oral commissure, and arches upward to a coloboma in the lateral part of the lower eyelid. There are skeletal defects lateral to the infraorbital nerve. One frequently finds a cleft in the alveolus between the canine and the first molar. 8 ·
11•27 Both unilateral and bilateral
deformities have been described, but they are rare, 6
·8
·11
·19
•21
·27
-33 and some are poorly docu
mented. However, the malformation may in fact not be so unique considering the striking superficial resemblance11
• 34 with maxillozygomatic
dysplasia, Tessier's no. 6 cleft. In maxillozygomatic dysplasia the defect is found between the maxilla and the zygoma. The cleft extends into the inferior fissure and the alveolar process is not involved. In Chavane's case, 27 lateral maxillary dysplasia was observed on one side and maxillozygomatic dysplasia on the other. The symptoms observed in this malformation can be explained on the basis of a developmental arrest in the lateroposterior part of the maxillary ossification center(s). 13
'14
INCIDENCE
In their excellent reviews35 ·% of rare facial clefts, Kawamoto et a!. came to the conclusion that the occurrence rate of these malformations would range from 1.43 to 4.85 per I 00,000 births and from 9.5 to 34.0 per 1000 common clefts. The best indication as to the frequency of oblique facial clefts can indeed be deduced from the figures produced by centers where large numbers of clefts are seen. These data show (Table I) that the incidence varies between 0.75 and 5.4 percent.
ETIOLOGY
... infants become crippled in the following way: where in the womb there is a narrowness at the part where in fact

Vol. 76, No. 2 /OBLIQUE FACIAL CLEFTS
TABLF. I
Incidence of Oblique Clefts
Oblique Facial Author Clefts Clefts
Giinther 1 ~ 4 900 Rintala ct al. 21 II 3600 Wilson et al. 1
Pitanguy and Franco32 726 Davis37 5 944 Fogh-AnderscJJ38 3 3988 Kubacek and Penkava39 5 2880
Pern·1H
4.4 3.0 2.5 1.4 5.4 0.75 1.7
the crippling is produced, it is inevitable that the body moving in a narrow place shall be crippled in that part.
Hippocrates40
The foundations of the science of teratology were laid by Meckel41 and by father and son Geoffroy St. Hilaire42
·'13 Meckel believed that
oblique clefts were caused by a developmental arrest, while Geoffroy St. Hilaire (1832) felt that amniotic bands were responsible. Since then, the debate has never stopped.
Proponents of the first theory believe that focal fetal dysplasia is the primary defect. 44 They have suggested a variety of mechanisn1s, such as linear necrosis along the watershed between developing vascular areas,1
·"' the occurrence of a diminished arterial supply in a crucial period of development,'6 ·
47 a disturbance in the migration of neural crest cells,48 or a failure of mesodermal penetration and coalescence between facial processes.<" In theory, these mechanisms may be caused by genetic as well as nongenetic factors. Genetic factors do not seem to play a role, since familiarity has not been reported in the literature. Nongenetic factors have never been identified with certainty, but hemon·age and fetal necrosis have been produced in experiments with a linoleic acid-deficient diet, 50 maternal injection51 with epinephrine and vasopressin, and uterine ischemia"' caused by clamping of its vasculature.
Proponents of the second theory, who believe that clefts are caused by bands, 53 are now in the minority, since, logically, the origin of these clefts cannot be band-related. First, the pattern of facial clefts, although subject to slight variation, is always consistent and reflects a crania-oral direction. It is furthermore inconceivable that perfectly symmetrical clefts can be caused by haphazardly produced bands. Second, several malformations that may be associated with an oblique cleft cannot be explained by amniotic
215
bands, such as encephaloceles, widow's peak, microphthalmia, choana] atresia, and cleft palate. Third, amniotic bands consist of embryonic tissue that is not known to possess contractile qualities. Finally, the existence of bands between different parts of the face54
-59 cannot be attrib
uted to an amniotic process. The origin of these bands may, however, be readily explained by the healing of fetal defects with adhesion formation.
Is it perhaps possible to reconcile these different schools of thought? Proponents of a third theory believe that craniofacial clefts and amniotic bands may be part of the amnion rupture syndrome together with visceral and extremity defects. The incidence of this syndrome has been reported to vary from 1:5000 to 1:15,000. 53
· 61
Familial incidence has not been reported, and the fact that facial clefts have been observed in one of two monozygotic twins62 clearly dernonstrates that nongenetic factors rnay be involved in their production. Drug ingestion has been implicated in some patients,63
·fi·l as well as in animal tnodels,65 but an amniogenic mechanism seen1s to be the predominant cause.
Torpin53 has stressed the role of maternal trauma and premature amnion rupture in the production of the syndrome, and his observations are consistent with those made in experiments. Amnion rupture or amniocentesis66
-72 is
known to produce compression-related malformations of the craniofacial complex (encephaloceles, hydrocephalus, palatal clefts), of the vertebrae (spina bifida), and of the limb (constriction ring anomalies, acrosyndactyly, etc.). Similar effects have been obtained by injection of amnion with glucose.73
The spectrum of abnormalties produced by these experiments only rarely includes oblique facial clefts, but despite this, the possibility should be considered that oblique facial clefts and other anomalies have their origin in compressionrelated focal fetal dysplasia. 74
• 75 Oblique facial
clefts and constriction ring defects of the extremities are frequently observed 1
·8
• 12
•16
' 19 in the am
nion rupture syndrome. Differences in nature and incidence of the several defects can be explained by a variation in susceptibility of the developing area and by the timing and severity of the causative insult.
TREATMENT
An attempted correction of a facial cleft may easily result in a surgical catastrophe, for the deficiencies of skin and skeleton are frequently underestimated. Scar tissue does not keep pace

216 PLASTIC AND RECONSTRUCTIVE SURGERY, August 1985
with growth of normal tissues. Secondary bone deformities may be produced by the contraction of skin and n1ucosa, and what initially appears to be an excellent result may gradually turn into a monstrous disfigureJnent.
In the past 20 years, I have been involved in the treatment of nine patients with oblique facial clefts, three caused by nasomaxillary dysplasia and six by medial maxillary dysplasia. Four of my patients with oblique clefts were either lost to follow-up or their history is of little interest to the reader.
CASE REPORTS
Case 1
This patient (Fig. 2) was born on May 9, 1968, with the following severe craJJiofacial malformations: plagiocephaly, hypertelorism, unilateral microorbitism, complete bilateral nasomaxillary dysplasia, and palatoschisis. Constriction ring anomalies of the extremities were also observed. The clefts were closed in a series of successive stages by transposition and interdigitation of glabel!ar nasal flaps and by a lip adhesion procedure. The palate was closed at a later stage. Since the boy had been deserted by his unmarried mother, he was adopted by foster parents and later raised in an institute for backward children. Further corrections, although urgently needed, were refused on several grounds. I lowever, despite his handicap, the boy has developed surprisingly well and now has himself asked for further correc-
tion. The increased interorbital distance has now been reduced and his nasal deformities have been corrected by rotation and advancement of both cheeks and by transposition of a median forehead flap.
Case 2
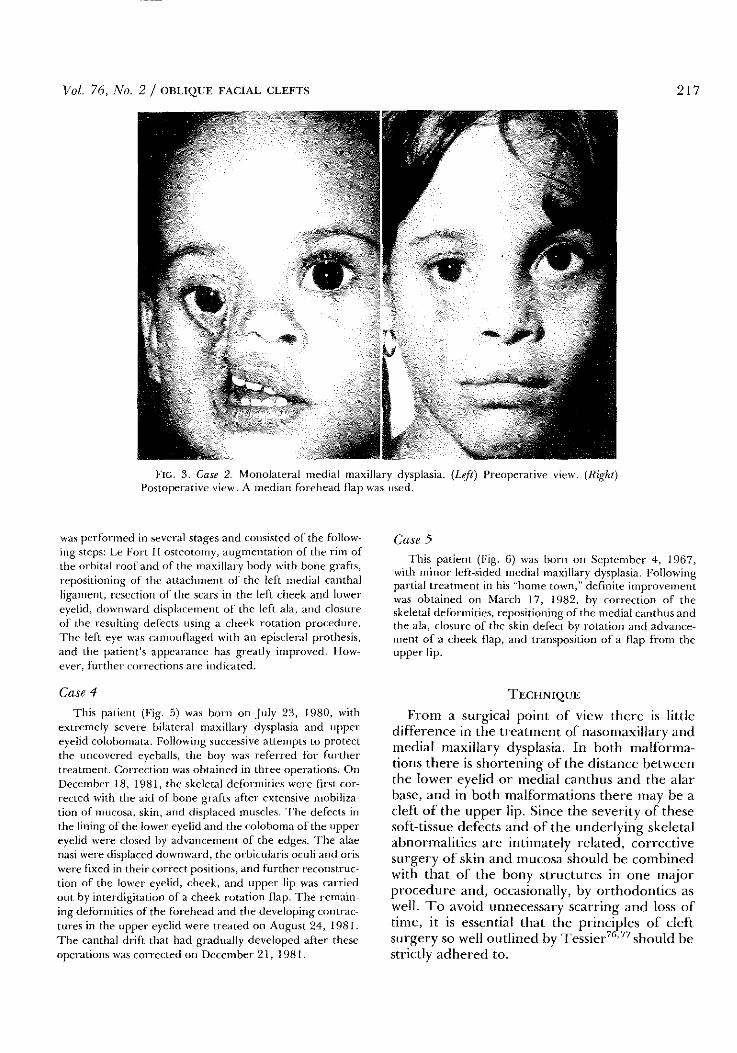
This patient (Fig. 3) was born on November 22, 1969, with a right-sided medial maxillary dysplasia. Exploration after primary closure elsewhere revealed severe hypoplasia of the body of the maxilla. No deft was found in the bone, and the alveolar process was normal. On September 20, 1976, the following corrections were carried out: repositioning of the ala nasi and the medial canthus, reconstruction of the lacrimal canal with a flap from the nasal mucosa, augment.'ltion of the skeleton with an iliac graft, and supplementation of the skin shortage in the lower eyelid and medial canthal regions with a median forehead flap. The result was satisfactory, except for the difference in color match between the skin of the forehead flap and that of the cheek. Further augmentation of the maxilla will be needed in the future.
Case 3
This patient (Fig. 4) was born on May 27, 1963, and was seen in 1980 with severe deformities following the closure of a left-sided medial maxillary dysplasia and right-sided cleft lip. Exarnination revealed clefting of the left eyebrow with underlying skeletal retrusion, lagophthalmos due to scarring of the upper and lower eyelids, ophthalmic dysplasia, canthal dystopia, upward displacement of the left ala, massive scarring of the cheek and upper lip, retrusion of the hypoplastic maxilla, and dental abnormalities. Treatment
FIG. 2. Case 1. Extreme bilateral complete nasomaxillary dysplasia. (Left) Preoperative view. (Right) Postoperative view. Correction was mainly obtained by rotation and advancement of both cheeks and by transposition of a forehead flap to lengthen the nose in two stages.
Vol. 76, No. 2 / ORI.IQUE FACIAL CLEFTS 217
FIG. 3. Case 2. Monolateral medial maxillary dysplasia. (Left) Preoperative view. (Right) Postopermive view. A median forehead flap was used.
was performed in several stages and consisted of the following steps: LeFort II osteotomy, augmentation of the rim of the orbital roof and of the maxillary body with bone grafts, repositioning of the attachment of the left medial canthal ligament, resection of the scars in the left cheek and lower eyelid, downward displacement of the left ala, and closure of the resulting defects using a cheek rotation procedure. The left eye ",:as camouflaged with an episcleral prothesis, and the patient's appearance has greatly improved. However, further corrections arc indicated.
Case 4
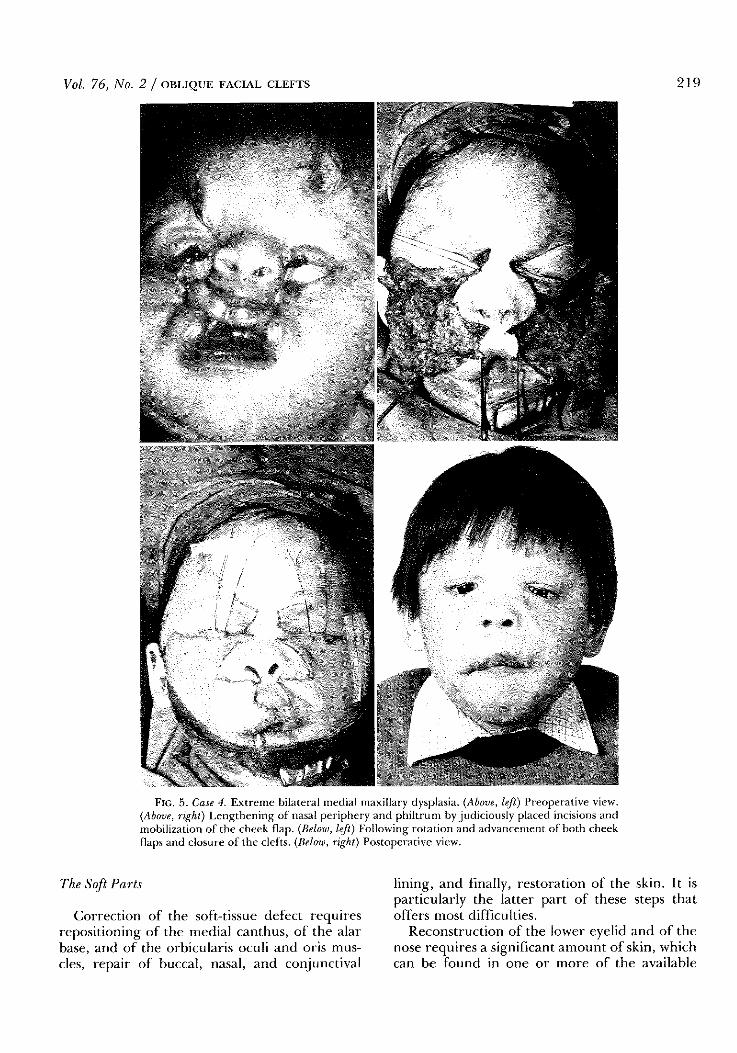
This patient (Fig. 5) was born on July 23, 1980, with extremely severe bilateral maxillary dysplasia and upper eyelid colobomata. Following successive attempts to protect the uncovered eyeballs, the boy was referred for further treatment. Correction was obtained in three operations. On December 18, 1981, the skeletal deformities were first corrected with the aid of bone grafts after extensive mobilization of mucosa, skin, and displaced muscles. The defects in the lining of the lower eyelid and the coloboma of the upper eyelid were closed by advancement of the edges. The alae nasi were displaced downward, the orbicularis oculi and oris were fixed in their correct positions, and further reconstruction of the lower eyelid, cheek, and upper lip was carried out by interdigitation of a cheek rotation flap. The remaining deformities of the fOrehead and the developing contractures in the upper eyelid were treated on August 24, 1981. The canthal drift that had gradually developed after these operations was corrected on December 21, 1981.
Case 5
This patient (Fig. 6) was born on September 4, 1967, with minor left-sided medial maxillary dysplasia. Following partial treatment in his "home town," definite improvement was obtained on March 17, 1982, by correction of the skeletal defOrmities, repositioning of the medial canthus and the ala, closure of the skin defect by rotation and advancement of a cheek flap, and transposition of a flap from the upper lip.
TECHNIQUE
From a surgical point of view there is little difference in the treatment of nasomaxillary and medial maxillary dysplasia. In both malformations there is shortening of the distance between the lower eyelid or medial canthus and the alar base, and in both malformations there may be a cleft of the upper lip. Since the severity of these soft-tissue defects and of the underlying skeletal abnormalities are intimately related, corrective surgery of skin and mucosa should be combined with that of the bony structures in one major procedure and, occasionally, by orthodontics as well. To avoid unnecessary scarring and loss of time, it is essential that the principles of cleft surgery so well outlined by Tessier76
• 77 should be
strictly adhered to.

218 PLASTIC AND RECONSTRUCTIVE SURGERY, August 1985
FIG. 4. Case 3. Monolateral medial maxillary dysplasia. (Above, left) Result of correction in early childhood. (Above, right) Malformation of orbital floor. (Below, left) Rotation and advancement of the cheek. (Below, right) Postoperative view.
The Skeleton
Dissection and mobilization of the edges of the cleft are followed by inspection of the maxilla. Here, anomalies are characterized by caudalization of the anterior part of the orbital floor, by lateralization of the medial wall of the maxillary
sinus, and by retrusion of the anterior wall of this structure. Correction is obtained by apposition of hone grafts on the orbital floor and on the anterior surface of the sinus. The cleft should be left open in order not to prevent repositioning of the central structures by the forces that will be generated by closure of the soft-tissue defects.
Vol. 76, No. 2 /OBLIQUE FACIAL CLEFTS 219
FIG. 5. Case 4. Extreme bilateral medial maxillary dysplasia. (Above, left) Preoperative view. (Above, right) Lengthening of nasal periphery and philtrum by judiciously placed incisions and mobilization of the cheek flap. (Below, left) Following rotation and advancement of both cheek flaps and closure of the clefts. (Below, right) Postoperative view.
The Soft Parts
Correction of the soft-tissue defect requires repositioning of the medial canthus, of the alar base, and of the orbicularis oculi and oris muscles, repair of buccal, nasal, and conjunctival
lining, and finally, restoration of the skin. It is particularly the latter part of these steps that offers most difficulties.
Reconstruction of the lower eyelid and of the nose requires a significant amount of skin, which can be found in one or more of the available

220 PLASTIC AND RECONSTRUCTIVE SURGERY, August 1985
FIG. 6. Case 5. Moderate medial maxillary dysplasia. (Left) Preoperative view. (Right) Postoperative view following rotation and advancement of cheek flap.

Vol. 76, No. 2 /OBLIQUE FACIAL CLEFTS 221
FIG. 7. The use of a median forehead flap to lengthen the nose. (Above, left) Marking the incisions. (Above, right) Mobilization of the flaps on both sides of one cleft. (Below, left) Transposition of the forehead flap and interdigitation of the raised flaps in the cheek and nose to correct one-half the malformation. (Below, right) Final result with symmetrical scars after mobilization and interdigitation of the flaps in the contralateral half of the face using the pedicle of the forehead flap.
donor areas: the upper eyelid, the forehead, and the cheek. Skin of the upper eyelid may be used for reconstruction of the lower eyelid, but with the restriction that only small flaps can be transposed. Skin of the forehead is available in sufficient quantity, and although its texture and color
leave somewhat to be desired, it may be used for reconstruction of the lower eyelid and the medial canthal region. The surplus of tissue provided by a forehead flap78 may be of particular value in bilateral cases if reconstruction of the medial canthus and alar bone are not sufficient to pro-

222 PLASTIC AND RECONSTRUCTIVE SURGERY, August 1985
'i
FIG. 8. The use of cheek flaps for the correction of oblique facial clefts. (Left) Marking of the incisions. (Center) Rotation, advancement, and interdigitation of the cheek flaps. (Right) Final result with symmetrical scars.
duce adequate lengthening of the nasal dorsum (Fig. 7). In these cases, the distal half of the flap may serve to close the defect on one side of the face in the first stage, while the contralateral defect and the defect created by the transection of the nasal dorsum may be resurfaced with the pedicle of this flap in a second stage.
Skin of the cheek may be used in a variety of ways, and its texture and color are perfect, The only question is how to take the best advantage of these qualities, Interdigitation of the cutaneous edges of the cleft has been reported by many authors, but the shortage of skin may be so extreme that the result obtained is far from optimaL Rotation and advancement of the cheek79 (Fig. 8) has to our knowledge not been recorded, but the results obtained with this technique in our patients indicate that it permits maximal correction at the expense of minimal scarring and should therefore be advocated as the procedure of choice in the majority of cases. I C. H. van der Meulen, M.D. Acad. Hospital Rotterdam-Dijkzigt Department of Plastic and Reconstructive Surgery Dr. Molewaterplein 40 3015 CD Rotterdam The Netherlands
REFERENCES
l. Wilson, L. F., Musgrave, R. H., Garret, W., and Conklin,J. E. Reconstruction of oblique facial clefts. Cleft Palate]. 9: 109, 1972.
2. Von Kulmus, Vide R. Marian. 3. Laroche Essai d'anatomie pathologique sur les
monstres ou vices de conform, primitive de Ia face. These de Paris, 1823.
4. Pelvet, M. Memoire sur les fissures congenitales des joues. Gaz. Med. Paris 19: 417, 1864.
5. Ahlfeld, P. Die missbildungen des Menschen. Leipzig, 1882.
6. Morian, R. Uber die schrage Gesichtsspalte. Arch. Klin. Chir. 35: 245, 1887.
7. GrUnberg, K. Die Gesichtsspalten und die zu ihnen in genetischer Beziehung stehenden anderweitigen Missbildungen der Gesichtes. In E. Schwalbe (Ed.), Die Morphologie der Missbildungen des Menschen und der Tiere, Vol. 3.Jena: Fischer Verlag, 1909.
8. Boo-Chai, K. The oblique facial cleft: A report of 2 cases and a review of 41 cases. Br. I Plast. Surg. 23: 352, 1970.
9. Millard, D. R. Cleft Craft. Boston: Little, Brown, 1977. 10. Harkins, C. S., Berlin, A., Harding, R. L., Longacre,].
J., and Snodgrasse, R. M. A classification of cleft lip and cleft palate. Plast. Reconstr. Surg. 29: 31, 1962.
11. Tessier, P. Anatomical classification of facial, craniofacial and laterofacial clefts. J. Maxillofac. Surg. 4: 69, 1976.
12. GUnther, G. S. Nasomaxillary clefts. Plast. Reconstr. Surg. 32:637, 1963.
13. Vermeij-Keers, C., Mazzola, R. F., van der Meulen, J. C., and Stricker, M. Cerebra-craniofacial and craniofacial malformations: An embryological analysis. Cleft Palate J. 20: 128, 1983.
14. van der Meulen, J. C., Mazzola, R. F., Vermeij-Keers, C., Stricker, M., and Raphael, B. A. Morphogenetic classification of craniofacial malformations. Plast. Reconstr. Surg. 71: 560, 1983.
15. Sakurai, E. H., Mitchel, D. F., and Holmes, L. A. Bilateral oblique facial clefts and amniotic bands: A report of two cases. Cleft Palate I 3: 181, 1966.

Vol. 76, No. 2 /OBLIQUE FACIAL CLEFTS
16. Dey, D. L. Oblique facial clefts. Plast. Reconstr. Surg. 52: 258, 1973.
17. Onizuka, T., Kato, I., Ichinose, M., eta!. Naso-ocular clefts. Three case reports. Plasl. Reconstr. Surg. 61: 118,1978.
18. Bartels, R . .J., O'Malley,J. E., Baker,]. L., and Douglas, W. M. Naso-ocular clefts. Plast. Reconstr. Surg. 47: 351, 1971.
19. Mayou, B. J., and Fenton, 0. M. Oblique facial clefts caused by amniotic bands. Plast. Reconstr. Surg. 68: 675, 1981.
20. Tower, P. Coloboma of lower lid and choroid, with facial defects and deformity of hand and forearm. Arch. Ophthalmol. 50: 333, 1953.
21. R;ntala, A., I.e;s,;, L., L;esmaa, M., and Ranta, R. Oblique facial clefts. Scand . .f. Plast. Surg. 14: 291, 1980.
22. Francois, J., and Bacskulin, J. External congenital fistulae of the lacrimal sac. Ophthalmologica 159: 249, 1969.
23. Pichler, A. Triinennasengang und schrage Gesichtsspalte. Arch. Augenheil. Band 68: 172, 1911.
24 . .Johanson, A., and Blizzard, R. A syndrome of congenital aplasia of the alae nasi, deafness, hypothyroidism, dwarfism, absent permanent teeth and malabsorption. J. Pediatr. 79: 982, 1971.
25. Ask, F., and van der Hoeven,J. Beitriige zur Kenntnis der Entwicklung der TriinenrOhrchen unter normalen unci ahnormalen Verhiiltnissen, letzteres an Fiillen von offener schr;lger Gesichtsspalte. Albrecht v. Graefes Arch. Ophtal. lOS: 1157, 1921.
26. Venneij-Keers, C., Koppenberg, J., and Maat, G. J. R. The oro-ocular clefts: An embryological subdivision. Orbit 2: 111, I 983.
27. Chavane M. Malformation b.ciale (section par bride amniotic). Bull. Soc. A nat. Paris 65: 137, 1890.
28. Remacly De fissura genae congenita. Dissertation, Bonn, 1864.
29. Fergusson, W. 1l System of Practical Surgery, 4th ed. London:]. Churchill, 1857.
30. Hyner Vide Walker. 31. Cowell Vide Walker. 32. Pitanguy, 1., and Franco, T. Nonoperated facial fis
sures in adults. Plast. Reconstr. Surg. 39: 569, 1967. 33. Pfeifer, G. Systematik und Morphologic der kranio
fazialen Anomalien. Fortschr. Kiefer Gesichtschir. 18: 1' 1974.
34. Ilovey, J. Vide Millard. 35. Kawamoto, H. K. The kaleidoscopic world of rare
craniofacial clefts: Order- out of chaos (Tessier classification). Clin. Plast. Surg. 3: 529, 1976.
36. Kawamoto, H. K., Jr., Wang, M. K. H., and Brandon Macomber, W. Rare Craniofacial Clefts. In J. M. Converse (Ed.), Reconst1·uctive Plastic Surgery, 2d Ed. Philadelphia: Saunders, 1977. Chap. 46.
3 7. Davis, W. B. Congenital deformities of the face. Types found in a series of one thousand cases. Surg. Gynecol. Obstet. 61: 201, 1935.
38. Fogh-Andersen, P. Rare clefts of the face. Acta Chir. Scand. 129: 275, 1965.
39. Kubacek, V., and Penkava, J. Oblique clefts of the face. Acta Chir. Plast. 16: 152, 1974.
40. Hippocrates Vide Ballantyne. 41. Meckel, J. l\.1eckel's Archiv., 1828. 42. St. Hilair~. G. Philosophie anatomique des monstruositis
223
humaines. Paris, 1822. 43. St. Hilaire, G. Traiti de tiratologie. Paris, 1832. 44. Streeter, G. L. Focal deficiencies in fetal tissues and
their relation to intrauterine amputation. Contrib. Embryol. 22:41, 1930.
45. Keith, A. Concerning the origin and nature of certain malformations of the face, head and foot. Br. J. Surg. 28: 173, 1940.
46. McKenzie,]. The first arch syndrome. Arch. Dis. Child. 33:477, 1958.
47. Sanvenero Rosselli, G. Developmental Pathology of the Face and the Dysraphic Syndrome: An Essay of Interpretation Based on Experimentally Produced Congenital Defects. Presented at the 21st Annual Meeting of the American Society of Plastic and Reconstructive Surgeons, New York, 1952.
48. Johnston, M. C. A radioautographic study of the migration and fate of cranial neural crest cells in the chick embryo. Anat. Rec. 156: 143, 1966.
49. Stark, R. B. The pathogenesis of harelip and cleft palate. Plast. Reconstr. Surg. 13: 20, 1954.
50. Martinet, M. Hemorragies embryonnaires par deficience en acide linoleique. Ann. Med. Intern. 53: 286, 1958.
51. Jost, A. Sur le rOle de la vasopressine et de Ia corticostimuline (ACTH) dans Ia production experimentale de lesions des extremites foetales (hemorragies, necroses, amputations congenitales). Comp. Rendu Siances Soc. Bioi. 4: 23, 1961.
52. Franklin,J. B., and Brent, R. L. The effect of uterine vascular clamping on the development of rat embryos three to fourteen days old. J. Morpho!. 115: 273, 1964.
53. Torpin, R. Fetal Malformations Caused by Amnion Rupture during Gestation. Springfield, Ill.: Thomas, 1968.
S4. von Bruns, V. Handbuch der praktischen Chirurgie I. Tubingen: H. Laupp, 1859.
55. Martz, W. Fall von Missbildung am Auge (coloboma palpebrae congenitum). Albrecht von Graefe's Archiv. Ophthalmol. 24: 145, 1878.
56. Polaillon, M. Vice de conformation des yeux. Gaz. Hopitaux 31: 245, 1874.
57. Nuei,J. P. Un cas de coloboma de Ia paupiere superieure et. des sourcils. Arch. Ophtalmol. 7: 437, 1881 (Ju;llct).
58. van Duyse Bride dennoide oculo-palpebral ct colobome partie! de Ia paupiere. Ann. Oculist. 88: 101, 1882.
59. Jones, K. L., Sm;th, D. W., Hall, B. D., Hall, J. G., Ebbin, A. ]., Massoud, H., and Golbus, M. S. A pattern of craniofacial and limb defects secondary to aberrant tissue bands. J. Pediatr. 84: 90, I 97 4.
60. Ossipoff, V ., and Hall, B. B. Etiologic factors in the amniotic band syndrome: A study of24 patients. Birth Defects 13: 117, 1977.
61. Baker, C. J., and Rudolph, A.]. Congenital ring constrictions and intrauterine amputations. Am. J. Dis. Child 121:393, 1971.
62. Garcia Velasco, D. M. Tratamiento de las hendiduras faciales tipo III, IVy V. III congreso ibero LatinaAmericana de Cirugia plastica y reconstructiva y V congreso nacional, Valencia, June 1980.
63. Berman, P. Congenital abnormalities associated with maternal clomiphene ingestion. Lancet 2: 878, 1975.
64. Carakushansky, G., Neu, R. L., and Gardner, L
224 PLASTIC AND RECONSTRUCTIVE SURGERY, August 1985
I. Lysergide and cannabis as possible teratogens in man. Lancet!: 150, 1969.
65. Abramovici, A. The Teratogenic Effect of Cosmetic Constituents on the Chick Embryo. In M. A. Klingberg, A. Abramovici, and .J. Chemke (Eds.), Drugs and Fetal Development. New York: Plenum, 1972.
66. Trasler, D. G., Walker, B. E., and Fraser, F. C. Congenital malformations produced by amniotic-sac puncture. Science 124:439, 1956.
67. Poswillo, D. Observations of fetal posture and causal mechanism of congenital deformity of palate, mandible and limbs. J. Dent. Res. 45: 584, 1966.
68. Kendrick, F. J, and Field, L E. Congenital anomalies induced in normal and adrenalectomized rats by amniocentesis. A nat. Rec. 159: 353, 1967.
69. DeMyer, W., and Baird, I. Mortality and skeletal malformations from amniocentesis and oligohydramnios in rats: Cleft palate, club foot, microstomia and adactyly. Teratology 2: 33, 1969.
70. Singh, S., Mathur, M. M., and Singh, G. Congenital anomalies in rat fetuses induced by amniocentesis. lndianf. Ivied. Res. 62:394, 1974.
71. Kino, Y. Clinical and experimental studies of the congenital constriction band syndrome, with an emphasis on its etiology . .f. Bone Joint Surg. 57 a: 636, 1975.
72. Kennedy, L. A., and Persaud, T. V. N. Pathogenesis of developmental defects induced in the rat by amniotic sac puncture. Acta Anal. 97: 23, 1977.
73. Clavert, J. M., Clavert, A., Berlizon, A., and Buck, P. La maladie amniotique, nouvelle approche de sa pathogenieMed. Infant. 87: 197, 1980.
74. Miller, M. E., Graham,J. M., Higginbottom, M. C., and Smith, D. W. Compression-related defects from early amnion rupture: Evidence for mechanical teratogenesis.]. Pediatr. 98: 292, 1981.
75. Graham,]. G., Miller, M. E., Stephan, M.J., and Smith, D. W. Limb reduction anomalies and early in utero limb compression.]. Pediatr. 96: 1052, 1980.
76. Tessier, P. Colobomas: Vertical and oblique complete facial clefts. Panminerva Med. 11: 95, 1969.
77. Tessier, P. Fentes orbito-faciales verticales et obliques (colobomas), completes et frustes. Ann. Chir. Plast. 14: 301, 1969.
78. Delpech, J. M. Chirurgie Clinique de Montpellier ou Observations et Reflexion tirees des Travaux de Chirurgie Clinique de cette Ecole. Paris: Chez Gabon, Libraire, 1828.
79. Esser,.J. S. F. Die Rotation der Wange und Allgemeine Bemerkungen bei chirurgischer Gesichtsplastik. Leipzig: F. C. W. Vogel Verlag, 1918.


















