
OBJECTIVES - Georgetown University
15
5/11/2017 1 DELVING DEEPER: DISPARITIES IN DEVELOPMENTAL DISABILITIES SERVICES AND SUPPORTS Tawara D. Goode & Vivian Jackson May 11, 2017 OBJECTIVES Participants will: 1. Examine concepts and definitions of disparity, equity, and inequity from the extant literature and their implications for systems serving individuals with developmental and other disabilities and their families. 2. Apply a framework to analyze disparities experienced by individuals with developmental and other disabilities that uses the lens of availability, accessibility, acceptability, quality, and utilization of services and supports. 3. List at least five contributing factors to disparities experienced by individuals with developmental and other disabilities from underserved and unserved groups and explore the applicability to their respective state, territory, or jurisdiction. 4. Describe seven approaches to address disparities that affect individuals with developmental and other disabilities. 5. Reflect on the role of leadership in addressing disparities impacting individuals with developmental and other disabilities and their families. Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
Transcript of OBJECTIVES - Georgetown University

5/11/2017
1
DELVING DEEPER:DISPARITIES IN DEVELOPMENTAL DISABILITIES SERVICES AND SUPPORTS
Tawara D. Goode & Vivian Jackson
May 11, 2017
OBJECTIVESParticipants will:
1. Examine concepts and definitions of disparity, equity, and inequity from the extant literature and their implications for systems serving individuals with developmental and other disabilities and their families.
2. Apply a framework to analyze disparities experienced by individuals with developmental and other disabilities that uses the lens of availability, accessibility, acceptability, quality, and utilization of services and supports.
3. List at least five contributing factors to disparities experienced by individuals with developmental and other disabilities from underserved and unserved groups and explore the applicability to their respective state, territory, or jurisdiction.
4. Describe seven approaches to address disparities that affect individuals with developmental and other disabilities.
5. Reflect on the role of leadership in addressing disparities impacting individuals with developmental and other disabilities and their families.
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence

5/11/2017
2
Health Related Activities
Transportation
Education & Early
Intervention
Employment Related
Activities
Recreation Related
Activities
Child Care
Housing
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
Mandates from the DD ACTfor
UCEDDsP&As
DD Councils
Advocacy
Capacity Building
Systems Change
Developing a Targeted Disparity Goal or Objective
The starting point for developing a targeted disparity goal or objective is with the analysis of the barriers to full participation of unserved and underserved groups of individuals with developmental disabilities and their families (Section III of the Comprehensive Review and Analysis (Part (C) (ii)). Based on the findings of the analysis, the DD Council should develop the goal or objective and include the identified subpopulation; the identified disparity the DD Council is trying to decrease, and; identify the strategy the DD Council will use to reduce the disparity.
GUIDANCE FOR DD COUNCILS FIVE-YEAR STATE PLAN

5/11/2017
3
UNSERVED AND UNDERSERVEDThe term “unserved and underserved” includes populations such as individuals from racial and ethnic minority backgrounds, disadvantaged individuals, individuals with limited English proficiency, individuals from underserved geographic areas (rural or urban), and specific groups of individuals within the population of individuals with developmental disabilities, including individuals who require assistive technology in order to participate in and contribute to community life.
Data source: retrieved on 5/9/17 from https://acl.gov/Programs/AIDD/DDA_BOR_ACT_2000/p2_tI_subtitleA.aspx
The Developmental Disabilities Assistance and Bill of Rights Act of 2000
Public Law 106–402 106th Congress
Slide Source:© 2017 Georgetown University National Center for Cultural Competence
What is a disparity?

5/11/2017
4
Difference Not equal Lack of similarity
Disparities in and of themselves can be neutral, neither good nor bad, just a descriptive difference.
Disparity in height
Slide Source:© 2017 Georgetown University National Center for Cultural Competence
DEFINING DISPARITY
Slide Source:© 2017 Georgetown University National Center for Cultural Competence
Concepts and
Definitions from
the Health Care
Literature

5/11/2017
5
HEALTH DISPARITIES ARE THE PRODUCT OF HEALTH INEQUITY
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
A health disparity is defined as a particular type of health difference that is closely linked with social or economic disadvantage – that is people who have experienced obstacles based on their:
race or ethnicity religion gender sexual orientation or
gender identity geographic location or
“place”
mental health socioeconomic status cognitive, sensory or
physical disability other characteristics
linked to discrimination or exclusion
Carter-Pokras O, Baquet C. What is a "health disparity"? Public Health Rep. September-October 2002;117(5):426-434.
U.S. Department of Health and Human Services. The Secretary’s Advisory Committee on National Health Promotion and Disease Prevention Objectives for 2020. Phase I report: Recommendations for the framework and format of Healthy People 2020. Section IV. Advisory Committee findings and recommendations. Available at: http://www.healthypeople.gov/hp2020/advisory/PhaseI/sec4.htm#_Toc211942917. Accessed 3/22/17.
Disparities in health care are differences in the quality of treatment, care, and services given to one group, when compared to another group, even though there are no differences between these group in:
insurance access to care needs and preferences
These difference in care cannot be explained by the disease, illness, or health status of the patient.
Smedley BD, Stith AY, Nelson, AR, eds. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care .Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care, Board on Health Sciences Policy, Institute of Medicine. Washington, DC: National Academies Press; 2003:19.
Balsa A, McGuire TG. Prejudice, clinical uncertainty and stereotyping as sources of health disparities. J Health Econ.2003;22:89-116.
US Department of Health and Human Services. The Secretary’s Advisory Committee on National Health Promotion and Disease Prevention. Objectives for 2020. phase I report: recommendations for the framework and format of Healthy People 2020. section IV. Advisory Committee findings and recommendations. Available at: http://www.healthypeople.gov/hp2020/advisory/PhaseI/sec4.htm#_Toc211942917. Accessed February 21, 2014
Slide Source:© 2017 Georgetown University National Center for Cultural Competence
DEFINING DISPARITIES IN HEALTH CARE

5/11/2017
6
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
INEQUITIES IN HEALTH DEFINED
Inequities in health systematically put
groups of people who are already
socially disadvantaged (for example, by
virtue of being poor, female, and/or
members of a disenfranchised racial,
ethnic, or religious group) at further
disadvantage with respect to their
health.
Source: Braveman, P. & Gruskin. Defining equity in health. J Epidemiol Community Health 2003;57:254-258. retrieved on
9/7/16 from http://jech.bmj.com/content/57/4/254.full.pdf+html
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
EQUITY IN HEALTH DEFINED
“Equity in health can be defined as the absence of
systematic disparities in health (or in the major social
determinants of health) between social groups who
have different levels of underlying social
advantage/disadvantage—that is, different positions in
a social hierarchy.”
“Health is essential to well-being and to overcoming
other effects of social disadvantage.”
Source: Braveman, P. & Gruskin. Defining equity in health. J Epidemiol Community Health 2003;57:254-258. retrieved on
9/7/16 from http://jech.bmj.com/content/57/4/254.full.pdf+html

5/11/2017
7
Disparities experienced by individuals
Actions to mitigate disparities and achieve equity
Total System Transformation!
Image source: https://ehhsdean.com/tag/equity/
How do these definitions and frameworks apply to disparities
experienced by underserved and unserved groups in your
State or Territory?
Slide Source:© 2017 Georgetown University National Center for Cultural Competence
5/11/2017
8
Slide Source:© 2017 Georgetown University National Center for Cultural Competence
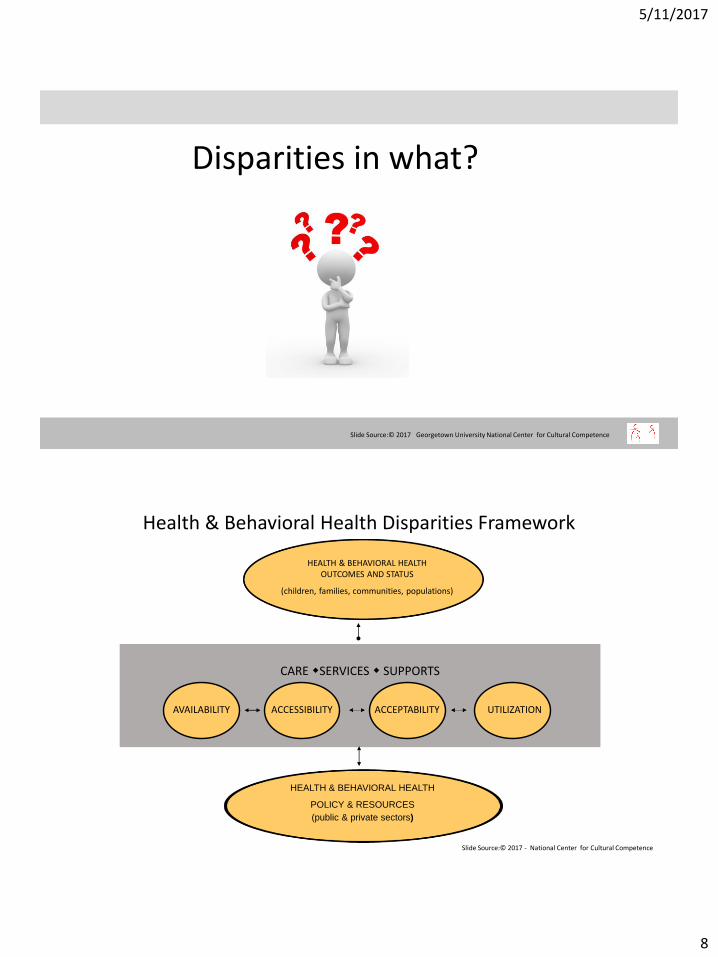
Disparities in what?
HEALTH & BEHAVIORAL HEALTH OUTCOMES AND STATUS
(children, families, communities, populations)
CARE SERVICES SUPPORTS
AVAILABILITY ACCESSIBILITY ACCEPTABILITY UTILIZATION
HEALTH & BEHAVIORAL HEALTH
POLICY & RESOURCES
(public & private sectors)
Slide Source:© 2011 - National Center for Cultural Competence
Health & Behavioral Health Disparities Framework
Slide Source:© 2017 - National Center for Cultural Competence

5/11/2017
9
Health Care Disparities: Health Care Policy, Resources, Accessibility, and Health Outcomes
THE TRAGIC CONSEQUENCES FOR DEMONTE DRIVER
Demonte’s mother could not find a dentist that would accept Medicaid insurance. In the time she was seeking care, Demonte’s abscess spread to his brain.
Heroic efforts were made to save Demonte, including two operations
and 8 weeks of additional care and
therapy totaling about $250,000.
But it was all too late. Demonte died on February 25, 2007 -- when his life could have been saved by a routine dental visit and an $80 tooth extraction.
SERVICES & SUPPORTS
AVAILABILITY ACCESSIBILITY ACCEPTABILITY UTILIZATION
Slide Source:© 2011 - National Center for Cultural Competence
A Developmental Disabilities Disparities Framework
Slide Source:© 2017 - National Center for Cultural Competence
QUALITY
FULL PARTICIPATION OF INDIVIDUALS WITH DEVELOPMENTAL AND OTHER DISABILITIESin all facets of community life

5/11/2017
10
Health □ yes □ no □ don’t know Transportation □ yes □ no □ don’t know Education & Early Intervention □ yes □ no □ don’t know Employment □ yes □ no □ don’t know Recreation □ yes □ no □ don’t know Child care □ yes □ no □ don’t know Housing □ yes □ no □ don’t know
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
Polling Question
Do you know the disparities experienced by underserved and underserved groups in your state/territory in the following areas mandated by the DD Act?
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
Why do we have disparities in our DD systems of services
and supports for individuals with
developmental and other disabilities?

5/11/2017
11
The “ISMs” is an umbrella term used to refer to a range of attitudes and behaviors that involve perceived superiority, oppression, prejudice, and discrimination based on such factors as race, national origin, ethnicity, language, class, disability, sexual orientation, and gender identity and expression.
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
Selected CONTRIBUTING FACTORS
Individual and family factors Culturally-defined beliefs and practices about
developmental disabilities Lack of knowledge about services and supports
… do we have disparities in our
systems of services and supports for
individuals with developmental
and other disabilities?
System-related factors ISMs Public Policy and Resources Social determinants

5/11/2017
12
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
Discussion
What do you see as the role of three AIDD-funded programs in addressing the disparities in your State/Territory?
Advocacy
Capacity Building
Systems Change
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
Things to Consider in Addressing Disparities
Sharing ownership
Actively engaging underserved and underserved populations in solutions
Confronting the ISMs at individual and systemic levels
Collecting & analyzing data
Employing culturally and linguistically competent polices and practices
Advocating for changes in policy and resource allocation
Nurturing and supporting leadership

5/11/2017
13
Organizational Change Theories Applied to the Role of Cultural & Linguistic Competence in Addressing Disparities
Resistance is a characteristic of any major organizational change effort and a major reason why organizational change efforts fail. (Prochaska, Prochaska and Levesque, 2001).
Resistance should be expected in different stages of multicultural organizational change because the topics of prejudice, discrimination and oppression are controversial and emotionally charged. (Brantley, Frost and Razak, 1996).
The Transtheoretical Model of Change suggests that it is counterproductive to forge ahead with action without addressing issues such as resistance, that stand in the way of individual and organizational readiness for change.
Data Source:Mayeno, L. Multicultural Organizational Development: A Resource for Health Equity, in Cultural Competence in Health Care Series, The California Endowment and Compasspoint Nonprofit Services, April 2007.
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
Cultural competence and linguistic competence are neither the panacea nor
cure for disparities in developmental disabilities services and supports –they are only part of the solution.
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
Thoughts about the Role of Cultural and Linguistic Competence

5/11/2017
14
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
Reflecting on the Role of Leaders
Leaders use power in alignment with the values & principles of cultural and linguistic competence. A leader is cognizant of the power and influence he/she possesses, exercises that power
wisely and respectfully, and uses it to achieve organizational goals for cultural and linguistic competence.
Leaders are champions. A leader must be vocal, visible, energetic proponent of the changes that need to be made.
Leaders are advocates. A leader must be an advocate on behalf of and in partnership with excluded or underserved groups.
Leaders facilitate conflict resolution. A leader recognizes and effectively addresses inherent conflicts between and among diverse cultural groups.
Goode, T., & Jackson, V. H. unpublished manuscript
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
Reflecting on the Role of Leaders
Leaders persevere. A leader can “stand in the fire of resistance” that is ever present when challenging the “isms”
at the individual, institutional, and community levels.
Leaders facilitate learning. A leader assures processes to: (1) learn about conceptual frameworks of cultural and linguistic competence and their value for the organization, and (2) acquire cultural knowledge of the children, youth and families receiving services and the communities in which they live.
Leaders serve as role model, coach & mentor. A leader “walks the talk” and supports others to do the same in an authentic and compelling
manner.
Leaders plan for leadership succession. A leader accepts that the work to advance and sustain cultural and linguistic competence is a continuous process, therefore prepares others for leadership roles.
Goode, T., & Jackson, V. H. unpublished manuscript

5/11/2017
15
*Adapted from: Brown C. & Mazza, G. (2005). Leading Diverse Communities: A How-To Guide for Moving from Healing into Action. National Coalition Building Institute. Jossey-Bass: San Francisco, CA.
Effective leadership for cultural and
linguistic competence requires having the
integrity to take principled stands.*
Leadership for addressing disparities requires (re)claiming courage.*
CLOSING THOUGHTS
Slide Source:© 2017 - Georgetown University National Center for Cultural Competence
CONTACT US
National Center for Cultural Competencehttp://nccc.georgetown.edu
The content of and this PowerPoint presentation are copyrighted and are protected by Georgetown University's copyright policies.
Permission is granted to use this PowerPoint presentation in its entirety and/or individual slides for non-commercial purposes if:
the material is not to be altered and
• proper credit is given to the author(s) and to the National Center for Cultural Competence.
Permission is required if the material is to be:
• modified in any way
• used in broad distribution.
To request permission and for more information, contact [email protected].


















