Objectives Choosing the Right Vehicle
10
tolerance, which ultimately affects patient compliance. There are many types of dermatological vehi- cles, and choosing the right one is both an art and a science. This arti- cle will explore how vehicles work, how and when to choose the ap- propriate vehicle, and how both es- tablished and new formulations af- Continued on page 210 Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Contin- uing Medical Education by the Council on Podiatric Medical Education. You may enroll: 1) on a per issue basis (at $20.00 per topic) or 2) per year, for the special introductory rate of $139 (you save $61). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the near future, you may be able to submit via the Internet. If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned cred- its. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test at no additional cost. A list of states currently honoring CPME approved credits is listed on pg. 216. Other than those entities currently accepting CPME-approved credit, Podiatry Management cannot guarantee that these CME credits will be accept- able by any state licensing agency, hospital, managed care organization or other entity. PM will, however, use its best efforts to ensure the widest acceptance of this program possible. This instructional CME program is designed to supplement, NOT replace, existing CME seminars. The goal of this program is to advance the knowledge of practicing podiatrists. We will endeavor to publish high quality manuscripts by noted authors and researchers. If you have any questions or comments about this program, you can write or call us at: Podiatry Management, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us at [email protected]. Following this article, an answer sheet and full set of instructions are provided (p. 217).—Editor JUNE/JULY 2008 • PODIATRY MANAGEMENT www.podiatrym.com 209 Continuing Medical Education Objectives 1) To discuss the inherent properties of dermatologi- cal vehicles as well as the various types. 2) To demonstrate how to choose the appropriate vehicle based on anatomy and skin condition treated. 3) To discuss the latest vehicle technology and how it relates to current prescribing practices. dermatological vehicle houses and supports the active ingredient. 1 The vehicle also has properties of its own; namely, it must direct or “drive” the active medication either past the stratum corneum or into the dermis to take therapeutic ef- fect. Not only does the vehicle drive the active ingredient into the skin, but it also enhances patient Choosing the Right Vehicle Tracey C. Vlahovic, DPM Introduction Topical dermatological products allow direct treatment of a skin condition with fewer side effects than those associated with systemic agents. These products have a key component, the vehicle, in addi- tion to the active ingredient. The Topical preparations involve more than just their active ingredients. Choosing the Right Vehicle PODIATRIC DERMATOLOGY PODIATRIC DERMATOLOGY
Transcript of Objectives Choosing the Right Vehicle

tolerance, which ultimately affectspatient compliance. There aremany types of dermatological vehi-cles, and choosing the right one isboth an art and a science. This arti-cle will explore how vehicles work,how and when to choose the ap-propriate vehicle, and how both es-tablished and new formulations af-
Continued on page 210
Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Contin-uing Medical Education by the Council on Podiatric Medical Education.
You may enroll: 1) on a per issue basis (at $20.00 per topic) or 2) per year, for the special introductory rate of $139 (yousave $61). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the nearfuture, you may be able to submit via the Internet.
If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned cred-its. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test atno additional cost. A list of states currently honoring CPME approved credits is listed on pg. 216. Other than those entitiescurrently accepting CPME-approved credit, Podiatry Management cannot guarantee that these CME credits will be accept-able by any state licensing agency, hospital, managed care organization or other entity. PM will, however, use its best effortsto ensure the widest acceptance of this program possible.
This instructional CME program is designed to supplement, NOT replace, existing CME seminars.The goal of this program is to advance the knowledge of practicing podiatrists. We will endeavor to publish high qualitymanuscripts by noted authors and researchers. If you have any questions or comments about this program, you can write orcall us at: Podiatry Management, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us [email protected].
Following this article, an answer sheet and full set of instructions are provided (p. 217).—Editor
JUNE/JULY 2008 • PODIATRY MANAGEMENTwww.podiatrym.com 209
Continuing
Medical Education
Objectives
1) To discuss the inherentproperties of dermatologi-cal vehicles as well as thevarious types.
2) To demonstrate howto choose the appropriatevehicle based on anatomyand skin condition treated.
3) To discuss the latestvehicle technology andhow it relates to currentprescribing practices.
dermatological vehicle houses andsupports the active ingredient.1 Thevehicle also has properties of itsown; namely, it must direct or“drive” the active medication eitherpast the stratum corneum or intothe dermis to take therapeutic ef-fect. Not only does the vehicledrive the active ingredient into theskin, but it also enhances patient
Choosing the Right Vehicle
Tracey C. Vlahovic, DPM
IntroductionTopical dermatological products
allow direct treatment of a skincondition with fewer side effectsthan those associated with systemicagents. These products have a keycomponent, the vehicle, in addi-tion to the active ingredient. The
Topical preparations involvemore than just their activeingredients.
Choosing the Right Vehicle
P O D I A T R I C D E R M A T O L O G YP O D I A T R I C D E R M A T O L O G Y
fuses through the deep skin layersand reaches the bloodstream. Thespeed at which this process occursis determined by the rate at whichthe active ingredient passesthrough the uppermost layer of epi-dermis, the stratum corneum.2
How do Vehicles Affect theSpeed of Absorption?
There are various mechanismsby which a vehicle “drives” thisprocess. First, the solubility of theactive medication in the vehiclewill determine how effectively themedication will leave the vehicleand penetrate the skin. Second, theingredients of the vehicle itself caneither interfere with or enhance theactive ingredient’s journey into thestratum corneum. Also, the amountof occlusion the vehicle providescan affect the active ingredient.
For example, an ointment, suchas a corticosteroid ointment, pro-vides significant occlusion and willprevent rapid evaporation, enhanc-ing penetration of active ingredient
into the skin both in intertriginousareas and places where the skin isnot intact.2
Additionally, a vehicle thatcauses occlusion may help to repairthe skin barrier, enhancing the effi-cacy of the active drug, such as indiaper rash preparations. 3 If anointment were applied to openskin, the active drug would crossthe compromised skin much fasterthan intact skin. These are all fac-tors to consider when choosing avehicle.
When topical medications areprescribed for dermatological con-ditions, systemic absorption is notthe desired goal. It is more impor-tant to note how long the activeingredient remains in the epider-mis. For instance, with a topicalantifungal, it is preferable to pre-scribe a medication that remains inthe stratum corneum or epidermisbeyond 24 hours since many pa-tients may be inconsistent with ap-plication.
Continued on page 211
210 www.podiatrym.comPODIATRY MANAGEMENT • JUNE/JULY 2008
Right Vehicle...
fect the podiatric physician’sprescribing habits.
How Vehicles WorkOver the last few years, older ac-
tive ingredients (such as some topi-cal corticosteroids) with reformulat-ed vehicles have flooded the mar-ket. In order to know which one toprescribe, it is important to knowhow vehicles work. Realizing thatthe majority of the topical medica-tion is the vehicle, it is importantto delve into the world of percuta-neous absorption. A topical medica-tion is absorbed through the stra-tum corneum and ultimately theentire skin unit via the followingsteps, all of which are vehicle driv-en. First, the skin must have a rea-son to absorb the topical. This is ac-complished through a concentra-tion gradient once the topical is ap-plied. Then, the active ingredientmust leave the vehicle and enterthe skin. Lastly, the medication dif-
Contin
uing
Medica
l Edu
catio
n
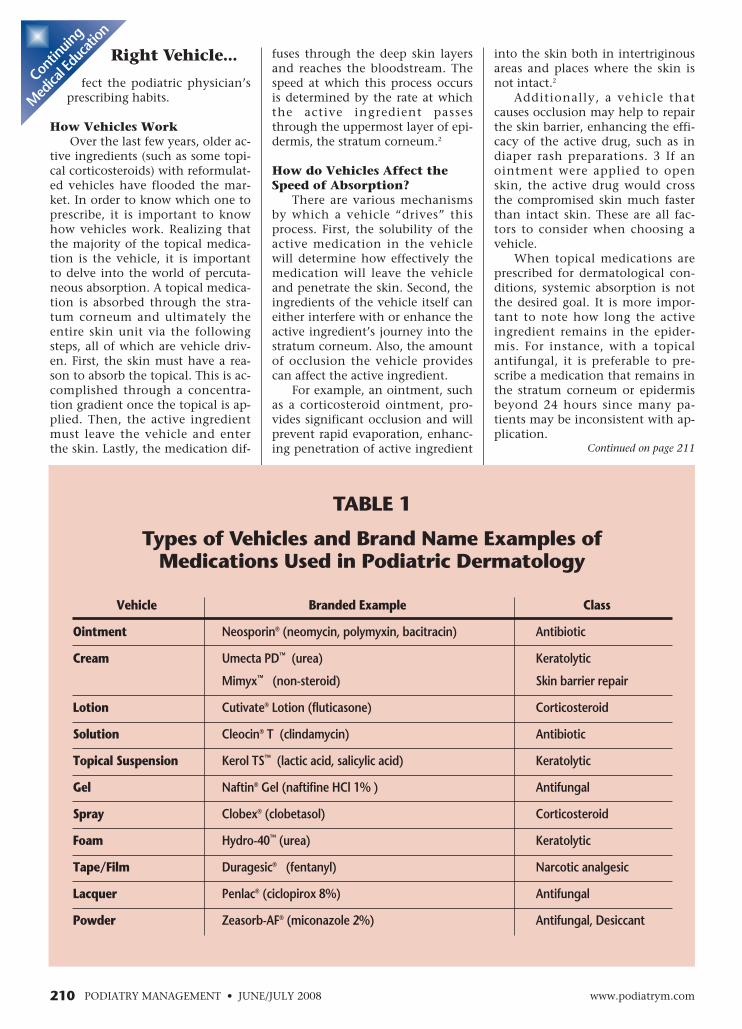
TABLE 1
Types of Vehicles and Brand Name Examples ofMedications Used in Podiatric Dermatology
Vehicle Branded Example Class
Ointment Neosporin® (neomycin, polymyxin, bacitracin) Antibiotic
Cream Umecta PD™ (urea) Keratolytic
Mimyx™ (non-steroid) Skin barrier repair
Lotion Cutivate® Lotion (fluticasone) Corticosteroid
Solution Cleocin® T (clindamycin) Antibiotic
Topical Suspension Kerol TS™ (lactic acid, salicylic acid) Keratolytic
Gel Naftin® Gel (naftifine HCl 1% ) Antifungal
Spray Clobex® (clobetasol) Corticosteroid
Foam Hydro-40™ (urea) Keratolytic
Tape/Film Duragesic® (fentanyl) Narcotic analgesic
Lacquer Penlac® (ciclopirox 8%) Antifungal
Powder Zeasorb-AF® (miconazole 2%) Antifungal, Desiccant

JUNE/JULY 2008 • PODIATRY MANAGEMENTwww.podiatrym.com 211
to release the active ingredient in atime-controlled manner.
Lacquers are organic materialswith an evaporable solvent thatleaves a film on the skin or nail.
Powders are solids that areground up or pulverized ingredientsthat generally have a drying effect.
How and When to Choose theRight Vehicle
An ideal vehicle is odorless,non-greasy, easy to apply, inexpen-sive, non-irritating, stable, and itleaves little-to-no residue. Does theperfect vehicle exist? Not yet; how-ever, choosing the right vehicle forthe appropriate anatomy and skincondition is imperative for thepracticing physician.
“Wet” Skin ConditionsAs classically stated by most
dermatologists, “if it is wet, dry it;if it is dry, wet it.” Most of thatstatement still applies today, butthe options to desiccate the area aremuch more extensive. For macerat-ed skin in interdigital spaces, a gel-based medication is the standardbecause of its drying effect, but insome instances, a medicated pow-der, topical suspension, or spraymay be considered. Using an oint-ment or more occlusive vehicle insuch an area would not be advis-able, as it could lead to skin macer-ation and possible skin breakdown.
For dermatitis with wet, weepy,erythematous areas, a spray or foamwould be preferred over an oint-ment or cream, which may be tooocclusive or cause enhanced pene-tration due to the lack of skin barri-er. The occlusive nature of an oint-ment would not allow the moistskin to dry. The patient should beadvised, though, that the use of analcohol-based spray or foam mightcause a stinging pain upon applica-tion to that type of area. If the paincannot be tolerated, a cream wouldbe the next best choice.
Clinical PearlIf a gel is the most appropriate
vehicle but stinging is a concern,offer the patient cream samples touse for the first few days but writethe prescription for gel.
“Dry” Skin ConditionsLikewise, for patients with severe
Types of VehiclesArmed with knowledge of vehic-
ular chemistry, it is the physician’sjob to choose the appropriate vehicleas well as the active drug. There arenumerous types of vehicles on themarket (Table 1), but each has itsown unique properties4:
Ointments are either petrola-tum- or propylene glycol–based.Petrolatum-based ointments are oc-clusive and retard evaporation, thuscreating an oily residue on the skin.This greasy residue may be a deter-rent for some patients to use consis-tently, but it allows greater absorp-tion of the active drug into the skinby increasing the hydration of thestratum corneum. Ointments arewell-suited to glabrous areas of skin.
Creams are emulsions. Theycan either be oil-in-water or water-in-oil formulations that leave aslight oily residue on the skin.Creams are easily washed off andgenerally more cosmetically elegantthan ointments. Cosmetic elegancerefers to the ability of a topicalmedication to leave little-to-noresidue on the skin as well as dryquickly, giving the illusion that nomedication has been used.
Lotions are one liquid (oil) sur-rounded by another liquid (water)which creates an emulsion or topicalsuspension. Lotions are typically lessmoisturizing than creams. These areeasy to spread (i.e., cover the entireleg) and cool the skin as the water inthe preparation evaporates.
Gels are either alcohol-based orwater-based. Alcohol-based gelstend to sting more than the water-based gels, but both are used fortheir rapid drying and excellentpenetration properties. Gels are alsoexcellent for hair-bearing areas andwork well in intertriginous areasand areas that tend to stay moist(i.e., interdigital spaces).
Sprays are metered (premea-sured) pumps of emulsions that dryquickly and can be spread easilyover large surface areas.
Foams are a dispersion of gas insmall amounts of liquid. Foams arecosmetically elegant and easy to use.
Tapes are strips of an occlusiveadhesive with the active ingredientimpregnated and often formulated
Right Vehicle... xerosis, a chronic dry der-matitis with fissures, ortinea pedis, an ointment,cream, or lotion could be used inorder to add moisture to the area.The goal with these medications is todecrease transepidermal water loss;however, some of the newer foamscould be used for their penetrationpower as well as their moisturizingproperties (see section below on Pro-derm Technology™).
Anatomical ConsiderationsTraditional treatment of scalp
psoriasis illustrates the importanceof matching the appropriate vehicleto the anatomic part. Traditionaloptions to treat scalp flakiness, red-ness, and pruritus included oils,ointments, and an agent (an-thralin) that stings, burns, andstains clothing. Both physiciansand patients requested a more cos-metically elegant preparation for amore discreet method of treatmentwhich would enhance compliance.Steroid-impregnated foams (i.e.,Olux®, Verdeso™, Luxiq®) were thenintroduced into the market andallow for scalp psoriasis treatmentwithout a messy, oily regimen.
Similar cosmetic considerationscan be applied to lower extremities.How easily products can be spreadand how quickly they dry are twoimportant factors when choosing atopical for a large, hair-bearing sur-face area like the lower leg. Hair-bearing areas require special consid-eration, and gels tend to penetratethe hair follicle better than creamsor ointments. In addition, non-greasy formulations like gels maybe preferable in areas covered byclothing to enhance patient com-pliance.
Likewise, efficient penetrationof the active ingredient into thickplantar skin is an important consid-eration. In Feldman’s research oncutaneous absorption of a topicalcorticosteroid, the flexor aspect ofthe forearm was used as a frame ofreference.5 Compared with the fore-arm, the plantar foot had 0.14 orten times less absorption; whereas,the axilla (an example of an intert-riginous area) had three times moreabsorption of the product. Theankle area had 0.42 or slightly lessabsorption than the forearm. With
Continued on page 212
Continuing
Medical Education

symptom relief may not be as imme-diate as with an ointment.
In contrast, small areas that aremacerated, such as interdigitalspaces, respond well to vehicles suchas gels. For further information onmatching the vehicle to the anatom-ical area for common podiatric der-matological conditions, see Table 2.
Patient ConsiderationsA prescription for a topical
medication is only useful if the pa-tient is compliant. Vehicles trulydrive compliance. Tolerability,spreadability, durability, ease ofuse, cosmetic elegance, patient sat-isfaction, and need for special stor-age are just some of the many fac-tors affecting patient compliance.In a Cutis study that aimed to de-velop a quantitative measure of ve-hicle preference in psoriasis pa-tients, twenty subjects sampled andassessed the properties of numeroustopicals.6 Each patient applied a
cream, solution, gel, ointment,foam, and emollient on the skin ofhis or her forearm.
Each topical was assessed forquality-of-life factors such as timeneeded for application, smell, feelon the skin, look of body hairwhen product is applied, stains onclothes, messiness, and method ofapplication. Overall, the preferredvehicles were solutions and foamsover the cream, gel, and ointmentpreparations.
Inspired by the Cutis article, theauthor performed a pilot study as-sessing Naftin® (naftifine hy-drochloride 1%) cream and gelpreference in patients at TempleUniversity Foot and Ankle Institute.Twenty patients were asked to char-acterize properties such as stinging,feel on skin, spreadability, time todry, and messiness when the prod-ucts were applied to the forearm.All patients preferred the gel, de-
Continued on page 213
212 www.podiatrym.comPODIATRY MANAGEMENT • JUNE/JULY 2008
Right Vehicle...
this in mind, lotions, topicalsuspensions, foams, and sprays
allow for application to the lowerleg that is fast, efficient, and nicelypenetrating, which is important toa patient who wants to don socksimmediately after application.
Unfortunately, due to the thick-ness of the epidermis, the ideal topi-cal for the plantar surface of the footis a vehicle with superior penetra-tion: an ointment. Ointments tendto be messy and greasy, makingthem the patients’ least favorite ve-hicle to use. Using an ointment onplantar skin is more important incases of acute inflammatory skinconditions such as eczema and psori-asis where immediate relief is need-ed. In reality, a patient who does notwant the greasy residue of an oint-ment in a sock or shoe can opt for acream, emulsion, or topical suspen-sion but should be advised that
Contin
uing
Medica
l Edu
catio
n
TABLE 2
Various Skin Conditions and Possible Vehicles toUse Based on Anatomical Location
Condition Anatomical Location Brand Name/vehicle
Moccasin Tinea Pedis Plantar surface Naftin® Cream, Loprox® Topical Suspension (TS)
Interdigital Tinea Pedis Interdigital spaces Naftin® Gel, Loprox® Gel
Allergic Contact Plantar surface Utravate® Ointment, Temovate Emollient CreamDermatitis
Dorsal foot Topicort® Cream, DesOwen® Lotion
Leg Cutivate® Lotion, Clobex® Spray
Xerosis Plantar surface Lactinol-E® Cream, Umecta PD™ Emulsion
Dorsal foot Kerol TS,™ Salex™ Lotion
Leg Hydro-40™ Foam, AmLactin® Lotion
Psoriasis Plantar surface Taclonex® Ointment, Olux® Foam
Dorsal foot Lidex® Cream, Elocon® Cream
Leg Cutivate® Lotion, Clobex® Spray
Fissures Foot/Leg Bionect® Gel, Amerigel® Wound Dressing
Hyperhidrosis Plantar Foot B-Drier® Solution, Zeasorb® Powder

JUNE/JULY 2008 • PODIATRY MANAGEMENTwww.podiatrym.com 213
ing than topical creams. Thisthought may be explained by theclinical doctrine that suggests thatgel formulations are more dryingand thus may be more irritating.However, a study comparingmetronidazole gel and cream con-cluded that there was no significantdifference in the cumulative irritan-cy potential of cream and gel andthat topical formulations should beconsidered on a case-by-case basis.3
The clinician should also be awareof the inactive ingredients in topi-cal medications that containknown sensitizing agents such asantimicrobial preservatives for ex-tended shelf-life. The issues sur-rounding inactive ingredients arealso very important when patientschoose to use non-prescription orover-the-counter medications.
scribing it as “fast drying, cooling,and not stinging.” The cream wasdescribed as messy, but the vehiclethey would prefer if they had tospread it on the plantar foot.
Besides quality-of-life factors, itis also important to consider prefer-ences between male and female pa-tients. When treating tinea pedis,men often prefer a gel to a creambecause it dries more quickly. Forthe same reason, men prefer foamsto emollients for treatment of xero-sis. In contrast, women often prefermedications that are moisturizingfor both conditions. Besides genderpreference, younger patients mayprefer newer vehicles such as gels,foams, and sprays because they per-ceive them to be better than older,more traditional topicals.
Vehicular Adverse EventsAdverse events are typically
discussed in relation to the mar-keted product. However, if you ex-amine the actual clinical trial re-sults for topical medications youwill often find that the adverseevents are similar in both the vehi-cle (placebo) and active groups. So,it is important to note that if a pa-tient has a reaction to a topicalmedication, it may be either thevehicle or the active ingredientcausing the problem. Typical ad-verse events include erythema,burning, stinging, local irritationand pruritus. It is important to ob-tain good baseline informationabout the patient’s symptoms priorto the use of a new topical medica-tion because it may be difficult todetermine whether adverse eventsare the result of a reaction to themedication or simply symptoms ofthe condition being treated. Cer-tain vehicles may be more likely tocause irritation than others. For in-stance, propylene glycol is a fairlycommon vehicle ingredient that isknown to cause both allergic andirritant contact dermatitis. Propy-lene glycol is primarily foundmainly in topical corticosteroidpreparations.
The irritation potential of cer-tain vehicles may vary betweensimilar products and manufactur-ers. Physicians often think that top-ical gels are inherently more irritat-
Right Vehicle... New VehicleTechnology inPodiatric DermatologicalPreparations
Recently, two new advances inthe world of vehicles have beenintroduced to the market: Phar-maDur™ and Proderm™.
PharmaDur™ is a polymer that isboth hydrophobic and hydrophilic.It was synthesized to create a con-trolled-release film on the skin.Shah, et al. painted the modifiedpolymer onto skin and, using a UVlight, showed that it created a filmthat lasted 24 hours.7 In a similarstudy, patients applied a moisturizerincorporated with PharmaDur™ andwere subjected to a variety of analy-ses.7 The study showed that a smallamount of PharmaDur™ added tothe moisturizer increased skin mois-ture by 75% over a six-hour period.Overall, the incorporation of Phar-maDur™ into topical medicationscreates an invisible, long-lastinglayer that enhances the effect of theactive medication to which it isadded. This advancement in vehicletechnology is seen in the UmectaPD™ emulsion and topical suspen-sion products (JSJ Pharmaceuticals).
Clinical ExampleA patient presented to the emer-
gency department with painful fis-sures on both plantar heels. The EDgave the patient crutches and nar-cotic pain medication, but no topi-cal moisturizer. Upon examinationof the patient in the clinic, it was
decided to prescribe both UmectaPD™ (urea 40%) emulsion for the se-vere xerosis and Bionect (hyaluronicacid) Gel for the painful fissures. Inthree weeks, the patient no longercomplained of pain and fissures weresignificantly healed (Figures 1 and 2).
Proderm™ is a water-lipid–basedfoam vehicle made of physiologicallipids, dimethicone, and glycerine. Dr.Rudy Ghadially demonstrated themovement of lipids in Proderm™ intothe epidermis in murine skin.8 Labeledfatty acid was incorporated into Pro-derm™ and applied to skin. After twohours, a sample of skin was collectedand reviewed under a fluorescent mi-croscope to determine the extent ofpenetration. Labeled Proderm™ was eas-ily visible in the stratum corneum aswell as the rest of the epidermis. In
Continued on page 214
Continuing
Medical Education
Figure 1: Patient with painful heel fissures andscale at first visit
Figure 2: Patient three weeks later after using anemulsion and gel to treat the area

demonstrated decreased activitycompared to that of both dilutions.9
Even with this information show-ing the inferiority of generic topicals,there is no assay to determinewhether a generic is truly equivalentto its brand name counterpart. It trulybecomes a “buyer beware” situationfor both physician and patient.
ConclusionThe world of dermatological vehi-
cles is fascinating and ever changingwith new technologies and innova-
tions. With the knowledge of bothvehicle mechanism of action and ap-propriate anatomical placement, theprudent podiatric physician may pre-scribe topical medications that willenhance patient compliance and pro-vide positive changes in dermatologi-cal conditions of the lower extremity.
References:1 Lipsker D., et al. “Other Topical
Medications” in Bolognia J ed, Derma-tology. Mosby, pp 2056-2058, 2003.
2 Piacquadio D., and Kligman A.“The critical role of the vehicle to thera-peutic efficacy and patient compliance,”JAAD 39: S67-73, 1998.
3 Bikowski J. “Vehicular Compli-ance: Driving Drugs into the Skin,” Prac-tical Dermatology, 32-37, January 2007.
4 Wolverton S. “Basic PharmacologicalPrinciples,” in Wolverton S. ed, Compre-hensive Dermatologic Drug Therapy. WBSaunders, Philadelphia, pp 11-14, 2001.
5 Feldman R.J., and Maibach H.I.“Regional variation in percutaneouspenetration of 14C cortisol in man,” JInvest Dermatol 48:181-3, 1967.
6 Housman T.S., Mellen B.G., Rapp S.R.,Fleisher A.B., and Feldman S.R. “Patientswith psoriasis prefer solution and foam ve-hicles: a quantitative assessment of vehiclepreference,” Cutis 70(6): 327-32, 2002.
7 Shah K.R. “PharmaDur Bioadhe-sive Delivery System,” in John J. Willeed, Skin Delivery Systems. BlackwellPublishing, Iowa, pp 211-222, 2006.
8 Ghadially R., “Penetration Studyusing Proderm Technology Foam,” ab-stract presented at 7th AnnualCaribbean Dermatology Symposium, StThomas, US Virgin Islands, 2008.
9 Guin J.D., Wallis M.D., Walls R., etal. “Quantitative vasoconstrictor assayfor topical corticosteroids: the puzzlingcase of fluocinolone acetonide,” J AmAcad Dermatol 29: 197-202, 1993.
214 www.podiatrym.comPODIATRY MANAGEMENT • JUNE/JULY 2008
Right Vehicle...
contrast, the control of petrola-tum with dimethicone showed
strong fluorescence in the stratumcorneum, but no penetration into theepidermis. Overall, the Proderm™ tech-nology added to medications providesa strong barrier for the stratumcorneum while driving the active medi-cation into the epidermis. This ad-vanced technology is found in Hydro-40™ Foam (Quinnova Pharmaceuticals).
Clinical ExampleA patient presented with severe
plantar psoriasis. The patient had re-ceived only strong topical steroids untilthis point, but had not received any top-ical medication to treat the scale. Thepatient was prescribed Taclonex® Oint-ment, a combination of calcipotrieneand betamethasone dipropionate usedonce daily. The patient was also pre-scribed Hydro-40™ Foam to be used onceto twice daily on all scaly areas. Afterthree months, the patient had no visibleplantar scale and was continuing to usebarrier repair creams to further improveskin health (Figures 3 and 4).
Generic Medications andVehicle Efficacy
As seen in the new technologiesdescribed previously, research of avehicle delivery system is just as im-portant as the active medication’smechanism of action in the finisheddermatological product. Unfortu-nately, most physicians, pharma-cists, and patients believe in theequality of generic and brand namemedications.2 In reality, generic andbrand name dermatological prepara-tions can be very different. Ofcourse, generic medications are re-quired to meet quality standards, butthey may differ in vehicular ingredi-ents and preservatives as well as inthe overall manufacturing process.
Changes in the vehicle can affectthe performance and overall actionof the active medication, which maylead to patient frustration (if theyhave used the brand name drug pre-viously). For example, generic fluoci-nolone acetonide ointment dilutedin petrolatum was studied to showhow variations in the vehicle impactperformance on the skin. The generictopical steroid was pitted against a1:1 and 1:3 dilution of the product inpetrolatum. The non-diluted generic
Contin
uing
Medica
l Edu
catio
n
Dr. Vlahovic isan associate pro-fessor at theTemple Univer-sity School ofPodiatric Medi-cine where sheteaches the Fun-damentals ofDermato logycourse. She wasthe first podiatric physician in the U.S.to complete both a Fellowship in Podia-tric Dermatology at St Luke’s Hospital,Allentown, PA and the MedicalMarigold Training Certification fromthe Royal London Homeopathic Hospi-tal, London, UK. She is a Fellow of theAmerican Professional Wound Care As-sociation.
Figure 3: Patient with plantar psoriasison initial presentation
Figure 4: After three months of patientusing a combination ointment andfoam keratolytic.
JUNE/JULY 2008 • PODIATRY MANAGEMENTwww.podiatrym.com 215
6) Quality-of-life factors involvedin choosing one vehicle over an-other are:
A) smellB) feel on skinC) ease of useD all of the above
7) The main goal of a topicalmedication when treating a dryskin condition is:
A) increase trans-epidermal water lossB) decrease trans-epidermal water lossC) increase spreadabilityD) decrease tolerability
8) Generic topical medicationsdiffer from Brand name withwhich ingredient and/or quality?
A) active ingredientb) preservativesC) colorD) odor
9) The most appropriate vehicleto use for a dermatosis on theentire lower leg is:
A) sprayB) tapeC) lacquerD) powder
10) The most appropriate vehicleto use for interdigital macerationis:
A) ointmentB) creamC) taped) gel
1) A perfect, all-purpose vehiclewould include all of the follow-ing except:
A) odorlessB) inexpensiveC) stableD) oily
2) Vehicles may drive the activemedication into the skin by:
A) drying the skinB) hydrating the skinC) irritating the skinD) warming the skin
3) The rate at which the activemedication penetrates the skinis how fast it passes throughthe:
A) stratum basaleB) stratum germinativumC) stratum lucidumD) stratum corneum
4) Gels are often:A) alcohol-basedB) glycerine-basedC) oilyD) not used on hair-bearing
skin
5) If the skin is macerated andweeping, it is best to use all ofthe following except:
A) ointmentB) sprayC) gelD) foam
11) An example of a cosmeti-cally elegant preparation is:
A) ointmentB) powderC) foamD) tape
12) In contrast to most malepatients, most female patientsprefer:
A) vehicles that are mois-turizingB) vehicles that are dryingC) vehicles that are oilyD) vehicles that are mal-odorous
13) Which of the followingwould be appropriate fortreating plantar moccasintinea pedis
A) ointmentB) tapeC) powderD) cream
14) Which would be the bestchoice to treat plantar hyper-hidrosis?
A) ointmentB) creamC) powderDd) lotion
15) A lacquer leaves _____ onthe skin or nail:
A) an oily residueB) a filmC) a stainD) an indestructible residue
Continuing
Medical Education
E X A M I N A T I O N
See answer sheet on page 217.
Continued on page 216

216 PODIATRY MANAGEMENT
16) An ointment allows for greater absorptionof the skin due to which property?
A) occlusivenessB) spreadabiltyC) dryingD) film-leaving
17) Which part of the body is the least likely toabsorb medication effectively when comparedto the axilla?
A) palmB) forearmC) ankleD) plantar foot
18) Under fluorescent microscopy, labeled Pro-derm™ was seen where?
A) epidermisB) dermisC) subcutaneous layerD) muscle
19) PharmaDur™ lasted on the skin for ____hours)
A) 12B) 24C) 48D) 72
20) Choosing the proper dermatological topicalmay be based on:
A) anatomic locationB) quality generic substituteC) pleasantness of odorD) shelf life
E X A M I N A T I O N
(cont’d)
See answer sheet on page 217.
Contin
uing
Medica
l Edu
catio
n
PM’sCPME Program
Welcome to the innovative Continuing EducationProgram brought to you by Podiatry ManagementMagazine. Our journal has been approved as asponsor of Continuing Medical Education by theCouncil on Podiatric Medical Education.
Now it’s even easier and more convenientto enroll in PM’s CE program!
You can now enroll at any time during the yearand submit eligible exams at any time during yourenrollment period.
PM enrollees are entitled to submit ten examspublished during their consecutive, twelve–monthenrollment period. Your enrollment period beginswith the month payment is received. For example,if your payment is received on September 1, 2006,your enrollment is valid through August 31, 2007.
If you’re not enrolled, you may also submit anyexam(s) published in PM magazine within the pasttwelve months. CME articles and examinationquestions from past issues of Podiatry Man-agement can be found on the Internet athttp://www.podiatrym.com/cme. Each lessonis approved for 1.5 hours continuing education con-tact hours. Please read the testing, grading and pay-ment instructions to decide which method of partici-pation is best for you.
Please call (631) 563-1604 if you have any ques-tions. A personal operator will be happy to assist you.
Each of the 10 lessons will count as 1.5 credits;thus a maximum of 15 CME credits may beearned during any 12-month period. You may se-lect any 10 in a 24-month period.
The Podiatry Management Magazine CMEprogram is approved by the Council on PodiatricEducation in all states where credits in instruction-al media are accepted. This article is approved for1.5 Continuing Education Contact Hours (or 0.15CEU’s) for each examination successfully completed.
www.podiatrym.com
Home Study CME credits nowaccepted in Pennsylvania

Over, please
Please print clearly...Certificate will be issued from information below.
Name _______________________________________________________________________Soc. Sec. #______________________________Please Print: FIRST MI LAST
Address_____________________________________________________________________________________________________________
City__________________________________________________State_______________________Zip________________________________
Charge to: _____Visa _____ MasterCard _____ American Express
Card #________________________________________________Exp. Date____________________
Note: Credit card is the only method of payment. Checks are no longer accepted.
Signature__________________________________Soc. Sec.#______________________Daytime Phone_____________________________
State License(s)___________________________Is this a new address? Yes________ No________
Check one: ______ I am currently enrolled. (If faxing or phoning in your answer form please note that $2.50 will be charged to your credit card.)
______ I am not enrolled. Enclosed is my credit card information. Please charge my credit card $20.00 for each exam submitted. (plus $2.50 for each exam if submitting by fax or phone).
______ I am not enrolled and I wish to enroll for 10 courses at $139.00 (thus saving me $61 over the cost of 10 individual exam fees). I understand there will be an additional fee of $2.50 for any exam I wish to submit via fax or phone.
Note: If you are mailing your answer sheet, you must completeall info. on the front and back of this page and mail with yourcredit card information to: Podiatry Management, P.O. Box490, East Islip, NY 11730.
TESTING, GRADING AND PAYMENT INSTRUCTIONS(1) Each participant achieving a passing grade of 70% or
higher on any examination will receive an official computer formstating the number of CE credits earned. This form should be safe-guarded and may be used as documentation of credits earned.
(2) Participants receiving a failing grade on any exam will benotified and permitted to take one re-examination at no extra cost.
(3) All answers should be recorded on the answer formbelow. For each question, decide which choice is the best an-swer, and circle the letter representing your choice.
(4) Complete all other information on the front and back ofthis page.
(5) Choose one out of the 3 options for testgrading: mail-in,fax, or phone. To select the type of service that best suits yourneeds, please read the following section, “Test Grading Options”.
TEST GRADING OPTIONSMail-In GradingTo receive your CME certificate, complete all information
and mail with your credit card information to:Podiatry Management
P.O. Box 490, East Islip, NY 11730There is no charge for the mail-in service if you have already
enrolled in the annual exam CPME program, and we receive this
E N R O L L M E N T F O R M & A N S W E R S H E E T
✄
217
Continuing
Medical Education
exam during your current enrollment period. If you are not en-rolled, please send $20.00 per exam, or $139 to cover all 10 exams(thus saving $61* over the cost of 10 individual exam fees).
Facsimile GradingTo receive your CPME certificate, complete all information and
fax 24 hours a day to 1-631-563-1907. Your CPME certificate willbe dated and mailed within 48 hours. This service is available for$2.50 per exam if you are currently enrolled in the annual 10-examCPME program (and this exam falls within your enrollment period),and can be charged to your Visa, MasterCard, or American Express.
If you are not enrolled in the annual 10-exam CPME pro-gram, the fee is $20 per exam.
Phone-In GradingYou may also complete your exam by using the toll-free ser-
vice. Call 1-800-232-4422 from 10 a.m. to 5 p.m. EST, Mondaythrough Friday. Your CPME certificate will be dated the same dayyou call and mailed within 48 hours. There is a $2.50 charge forthis service if you are currently enrolled in the annual 10-examCPME program (and this exam falls within your enrollment peri-od), and this fee can be charged to your Visa, Mastercard, Ameri-can Express, or Discover. If you are not currently enrolled, the feeis $20 per exam. When you call, please have ready:
1. Program number (Month and Year)2. The answers to the test3. Your social security number4. Credit card information
In the event you require additional CPME information,please contact PMS, Inc., at 1-631-563-1604.
Enrollment/Testing Informationand Answer Sheet
✄
218 www.podiatrym.comPODIATRY MANAGEMENT • JUNE/JULY 2008
E N R O L L M E N T F O R M & A N S W E R S H E E T (cont’d)Con
tinuin
g
Medica
l Edu
catio
n
LESSON EVALUATION
Please indicate the date you completed this exam
_____________________________
How much time did it take you to complete the lesson?
______ hours ______minutes
How well did this lesson achieve its educational objectives?
_______Very well _________Well
________Somewhat __________Not at all
What overall grade would you assign this lesson?
A B C D
Degree____________________________
Additional comments and suggestions for future exams:
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
Circle:
EXAM #5/08Choosing theRight Vehicle
(Vlahovic)