
OASIS-D... · Objectives 1. Learn the specific OASIS-D items and guidance that are new. 2. Get...
575
1 OASIS-D 50 Shades of Gray Presented by: Arlynn Hansell, PT, HCS-D, HCS-H, HCS-O, COS-C Owner, Therapy and More, LLC Presented to the , 2019
Transcript of OASIS-D... · Objectives 1. Learn the specific OASIS-D items and guidance that are new. 2. Get...
1
OASIS-D50 Shades of Gray
Presented by: Arlynn Hansell, PT, HCS-D, HCS-H, HCS-O, COS-C
Owner, Therapy and More, LLC
Presented to the
, 2019
Objectives1. Learn the specific OASIS-D items and guidance that are new.
2. Get details on items that were removed moving from OASIS-C2 to OASIS-D. Learn how to capture these conditions now that they are no longer on the assessment form.
3. Avoid CMS surveyor scrutiny with best practices for answering the OASIS SOC/ROC in a timely fashion.
4. Correctly apply OASIS conventions to item-specific scenarios, while also learning how to apply OASIS-specific definitions for terms such as active treatment, care episode, same day, minimal assistance, and more.
5. Master the complicated wound items, including how to report pressure ulcers, stasis ulcers, surgical wounds and trauma wounds.
6. Ensure accuracy in the reporting of neuro/emotional/behavioral items.
7. Work through the ADL/GG items to ensure you're accurately reporting the patient's functional status.
8. Walk away with best practices to ensure your documentation matches the OASIS, which matches the plan of care.
2
3
Keys to Content
Guidance is based on the latest revisions to the OASIS-D Guidance Manual, CMS Q&As, WOCN guidance, and the Medicare Conditions of Participation (CoPs).
= Process measure
$$$ = Data item that contributes to the episode payment (Home Health Resource Group)
P
Outcome and Assessment
Information Set
OASIS-D Guidance Manual
Effective January 1, 2019
Centers for Medicare & Medicaid Services
M0090
4
Says Who?
• Official final version of OASIS-D Guidance Manual, dated January 1, 2019
• OASIS-D Guidance Manual errata, dated August 6, 2018, released again January 25, 2019
• CMS Quarterly Q&As, 4th quarter released January 15, 2019
• Future dates: April 17, July 17, October 16
• Consolidated CMS OASIS Q&As Static Version dated 10-01-2018, Categories 1 through 4
• Material in this presentation is current as of March 22, 2019
OASIS-D Core Reference Documents
OASIS-D Guidance Manual
• Chapter 1 – Conventions
• Chapter 3 – Item Guidance
CMS OASIS-D Q&As
WOCN OASIS-D Integumentary Items: Best Practice for Clinicians (2019)
OASIS Considerations for Medicare PPS Patients (01/10)
6
7
Do you know?
“OASIS” is an acronym for:
Outcome and ASsessment Information Set
• It is a group of data elements that:• Represent core items of a comprehensive assessment for an
adult, non-maternity home care patient;• Form the basis for measuring patient outcomes for the
purpose of outcome-based quality monitoring (OBQM), outcome-based quality improvement (OBQI), and the reporting initiative;
• Provide the foundation data on which provider reimbursement for Medicare PPS patients is calculated; and
• Are used in the enhanced survey process to promote a standardized approach to agency compliance surveys.
8
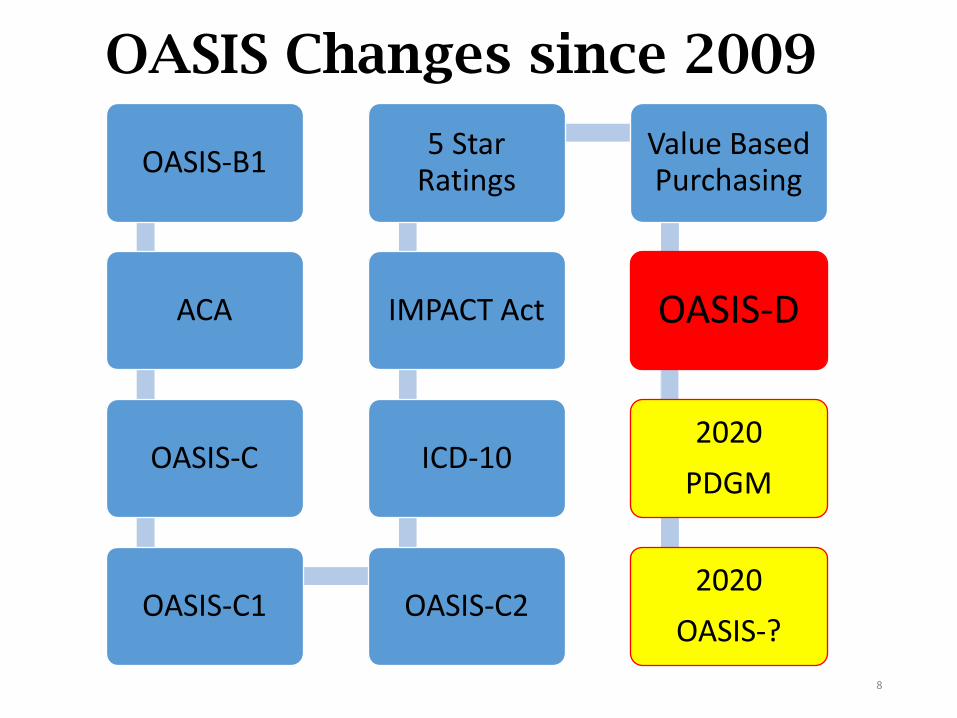
OASIS Changes since 2009
OASIS-B1
ACA
OASIS-C
OASIS-C1 OASIS-C2
ICD-10
IMPACT Act
5 Star Ratings
Value Based Purchasing
OASIS-D
2020
PDGM
2020
OASIS-?
9
History of OASIS
• To provide services reimbursed by Medicare and
Medicaid, home health agencies must demonstrate
compliance with Medicare Conditions of Participation
(CoPs).
• The Centers for Medicare and Medicaid Services (CMS)
is required to monitor the quality of home health care
with a “standardized, reproducible assessment
instrument.”
• The Outcome and Assessment Information Set
(OASIS) was the instrument selected to improve
quality of care and to comply with the law.
10
Why is OASIS so challenging?
• Multiple uses of the tool:• Data collection
• Quality measurement
• Reimbursement
• Identification of patterns of fraud and abuse
• Guidance not always clear…is sometimes confusing
• Requires significant depth of knowledge
• Pressure to “get it right” for:• Staying compliant with rules and regulations
• Best possible reimbursement for care provided
Background for OASIS-D
• OASIS-D was implemented January 1, 2019. Used for episodes with M0090 date on or after January 1, 2019.
• Changes proposed due to1:• Include changes per the IMPACT Act
• Accommodate data element removals (to reduce burden)
• Items not used for payment, quality measurement, or survey purpose removed
• Improve formatting
11
1. Supporting Statement A: CMS-10545/OMB control number: 0938-1279
Why Continued Changes to the OASIS?
• Section 1899B(b)(3) of the IMPACT Act requires that PAC settings standardize patient assessment datasets to meet these conditions:
• Data element uniformity in the tool used
• Comparison of quality and data across settings (cross-setting alignment)
• Alignment in content of items that support cross-setting measures
• Drug Regimen Review (DRR)
• Pressure Ulcers
• Active Diagnoses
• Height & Weight
• Improved discharge planning, exchangeability of data, and coordinated care between settings
12
OASIS-D Changes for Measurement Usage
• New standardized items to support measurement domains per IMPACT Act
• GG0130 Self-Care
• GG0170 Mobility a–b, d–s (we previously had “c” in OASIS-C2)
• J1800 Any Falls since SOC/ROC
• J1900 Number of Falls since SOC/ROC
• Despite their presence on the OASIS, these items do not have any impact on outcomes measures or process measures YET
• But …data that we began collecting in January 2019 will eventually be reportable in 2021 under the measure of Application of % of Patients with an Admission and Discharge Functional Assessment and a Care Plan that Addresses Function
• We want to avoid gathering “sloppy” data now, only to suddenly, in 2021, start answering accurately due to the publicly reportable measure
13
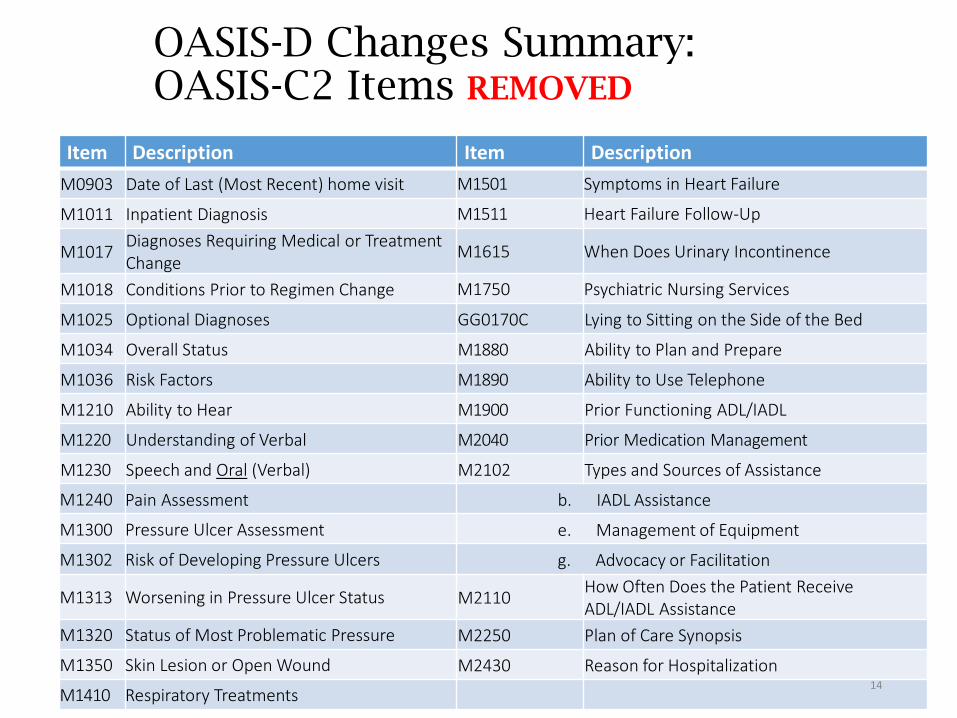
OASIS-D Changes Summary: OASIS-C2 Items REMOVED
Item Description Item Description
M0903 Date of Last (Most Recent) home visit M1501 Symptoms in Heart Failure
M1011 Inpatient Diagnosis M1511 Heart Failure Follow-Up
M1017Diagnoses Requiring Medical or Treatment Change
M1615 When Does Urinary Incontinence
M1018 Conditions Prior to Regimen Change M1750 Psychiatric Nursing Services
M1025 Optional Diagnoses GG0170C Lying to Sitting on the Side of the Bed
M1034 Overall Status M1880 Ability to Plan and Prepare
M1036 Risk Factors M1890 Ability to Use Telephone
M1210 Ability to Hear M1900 Prior Functioning ADL/IADL
M1220 Understanding of Verbal M2040 Prior Medication Management
M1230 Speech and Oral (Verbal) M2102 Types and Sources of Assistance
M1240 Pain Assessment b. IADL Assistance
M1300 Pressure Ulcer Assessment e. Management of Equipment
M1302 Risk of Developing Pressure Ulcers g. Advocacy or Facilitation
M1313 Worsening in Pressure Ulcer Status M2110How Often Does the Patient Receive ADL/IADL Assistance
M1320 Status of Most Problematic Pressure M2250 Plan of Care Synopsis
M1350 Skin Lesion or Open Wound M2430 Reason for Hospitalization
M1410 Respiratory Treatments14
Removed Items
Why were they removed?
• They did not support:
-- HH QRP measures
− HH Prospective Payment System (PPS)
− Survey process for Medicare certification
− HH Value-Based Purchasing (VBP) demonstration measures
− Critical risk-adjustment factors
− Conditions of Participation
15
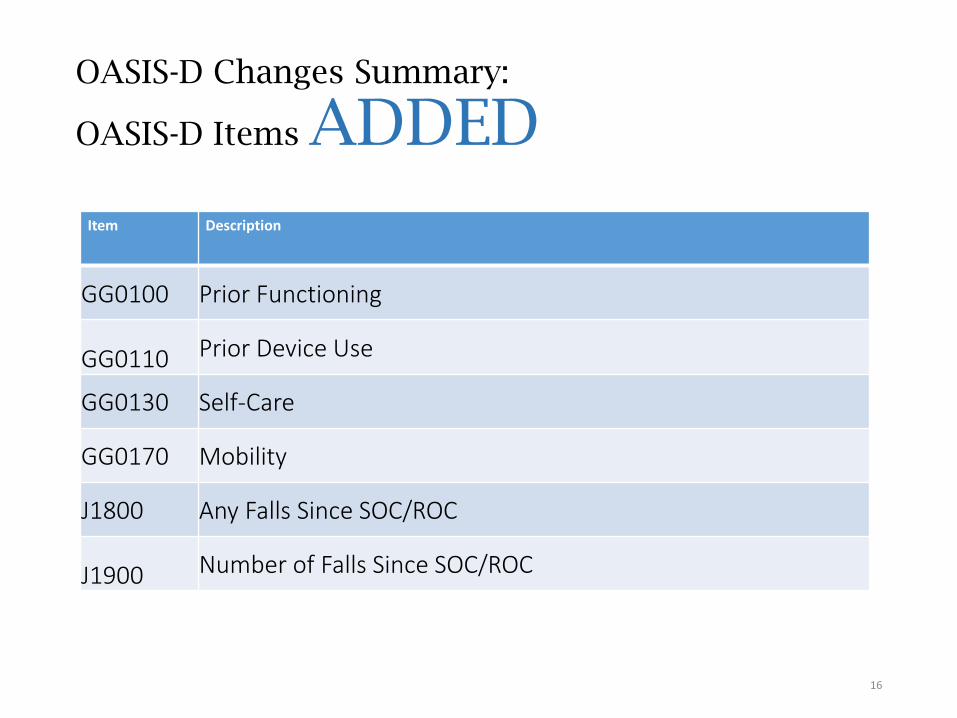
OASIS-D Changes Summary:
OASIS-D Items ADDED
Item Description
GG0100 Prior Functioning
GG0110 Prior Device Use
GG0130 Self-Care
GG0170 Mobility
J1800 Any Falls Since SOC/ROC
J1900 Number of Falls Since SOC/ROC
16
PDGM is coming…..
Key to Accurate Payment is Accurate Data
• Interdisciplinary collaboration key under OASIS-D and for best practice care planning under PDGM.
• Have a consensus discussion among all who saw the patient
• Consider a comprehensive ADL (OASIS) Assessment education program developed by therapists (PT & OT) for RNs with return demonstration
• Discipline-neutral (RN, PT, ST, OT) competence in OASIS assessment process is critical to gain and sustain accuracy
• Review OASIS prior to data being transmitted
17
OASIS is All About the Data
• Multiple uses of the OASIS tool:• Conditions of Participation (CoPs)
• Measurement of quality of care and care processes
• Episode payment / reimbursement
• Measurement of resource utilization
• Identification of patterns of fraud and abuse
• Value Based Purchasing (VBP) Model in 2016
• Ongoing pressure to “get it right”:• Best possible outcomes and reimbursement for care
provided
• Compliance with ever-changing rules and regulations
• Requires significant depth of knowledge.• Guidance not always clear, language can be confusing
18
19
How is OASIS data used?
• Outcome-Based Quality Improvement (OBQI)• Gauges how well an entity provides care to its patients
based on scientific evidence
• Outcome-Based Quality Management (OBQM)• Potential avoidable events – markers for potential
problems in care, which are adjusted for variations in patient characteristics
• Process-Based Quality Improvement (PBQI)• Use of specific best care processes recommended for
providing effective care to promote outcome improvement
• Home Health Compare Reports and Star Ratings
• Home Health Value-Based Purchasing
Home Health Quality Reporting Program
• The HHQRP was implemented in 2007.
• Accurate (and useful) reporting of home health quality information is based on the submission of a minimum of two OASIS assessments per patient.
• A SOC/ROC assessment
• A matching End of Care assessment (Transfer, Death, or Discharge)
• The matching assessments are defined as a “quality episode of care”.
20
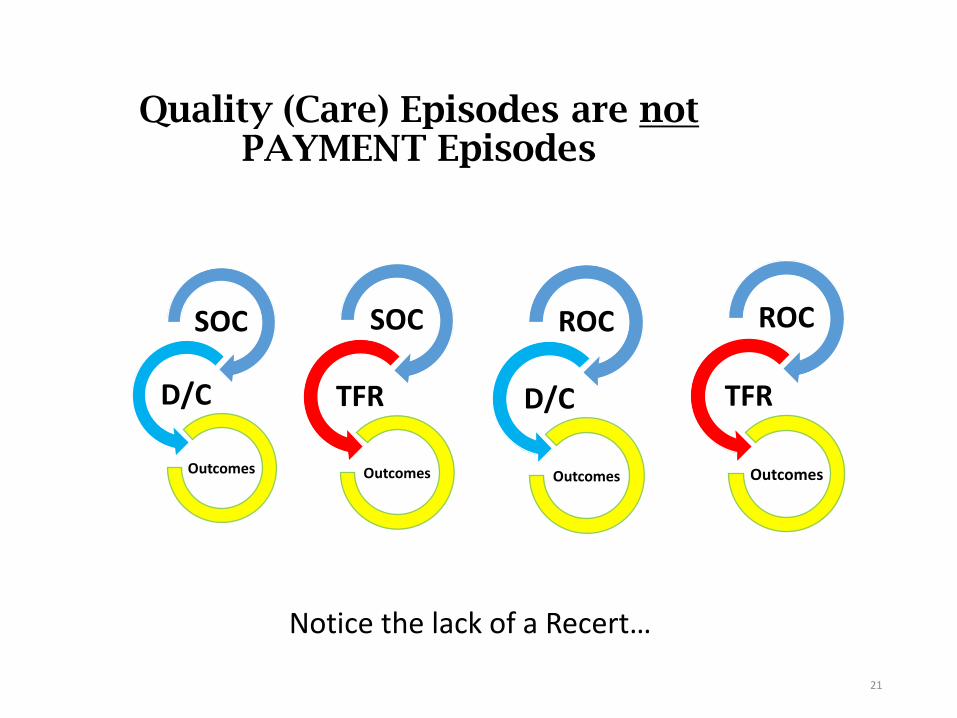
Quality (Care) Episodes are notPAYMENT Episodes
SOC
D/C
Outcomes
21
SOC
TFR
Outcomes
ROC
D/C
Outcomes
ROC
TFR
Outcomes
Notice the lack of a Recert…
22
IMPACT Act of 2014
• Requires standardized patient assessment data across post-acute care (PAC) that will enable:
Quality care and improved outcomes
Data element uniformity
Comparison of quality and data across PAC settings
Improved, person-centered, goals-driven discharge planning
Exchangeability of data
Coordinated care
23
2 key Elements
Data element uniformity
Comparison of quality and data across PAC settings
• Provider access to longitudinal information to facilitate coordinated care
• Enable comparable data and quality across PAC settings, as there is currently a lack of interoperability across PAC settings
24
• Process Measures
• Show how often HHA’s gave recommended care or treatments that research shows get the best results for most patients
• Outcome Measures
• Show the results of care given by the HHA
• M item based (OASIS)
2 Types of Measures
25
Why implement process measures?
• They provide data addressing the “why” for some patient outcomes.
• They address:• Health care services provided;
• Adherence to recommendations based on evidence or consensus; and
• Care that may require improvement.
• They were developed from evidence-based practice that HHAs can use to:
• Help prevent exacerbations;
• Improve patient care; and
• Avoid adverse events.
26
Agencies are Encouragedto Aim High, but…
• CMS acknowledges that the process measures do notpertain to every patient.
• 100% is not expected for any agency for any measure.
• When a process of care has no application for a particular patient, no related assessment or intervention is needed.
• Clinicians should document in the patient record the rationale for clinical decisions and actions.
• e.g., why a process was not appropriate or possible
27
Measures are NOT Mandated
• OASIS care processes are NOT mandated under the Conditions of Participation.
• Home health agencies may elect not to practice OASIS process measures.
but…• Home Health Compare and Quality of Patient Care Star
Rating scores will be poor for those who do not adopt publically reported care processes.
28
Outcome versus Process Measures
Outcome Measures
• Assess the results of health care experienced by patients between two time points – from SOC or ROC to discharge or transfer to an inpatient facilityStabilization;
Improvement; or
Decline
• Measure specific care quality related to process measures
• Are risk-adjusted
Process Measures
• Evaluate the rate of HHA use of specific evidence-based processes of care
• Deemed to be under the control of HHAs
• Focus on high-risk, high-volume, problem-prone areas
• Facilitate good patient outcomes
• Are not risk-adjusted
29
QUIZ
True or False?
If the nurse marks that the patient is able to take injectable meds:
Independently (M2030 = 0) at SOC, and
With assistance (M2030 = 1) at Recert
T/F: This outcome measure will show a decline.
30
Answer
True or False?
If the nurse marks that the patient is able to take injectable meds: Independently (M2030 = 0) at SOC, and With assistance (M2030 = 1) at Recert
T/F: This outcome measure will show a decline.
False: Outcome measures are not calculated at Recertification – only from SOC or ROC to discharge ortransfer to an inpatient facility.
31
OASIS data also used for…
• Determining the Home Health Resource Group (HHRG) and Non-Routine Supply (NRS) resources needed
• Calculation of the Home Health Prospective Payment System (HHPPS) episode rate is based on a 60-day episode of care (“payment episode”).
• Reimbursement for a 60-day episode of care is determined by the amount of resources needed to care for the patient.
32
OASIS and Reimbursement
• Patient resource use is based on characteristics determined by information collected using the OASIS data set, and payment is calculated by certain OASIS responses in three dimensions:
• Clinical Severity (C1-C3)
• Functional Status (F1-F3)
• Service utilization {based on therapy visits} (S1-S5)
• Scores in these three dimensions classify patients into case-mix groups or home health resource groups (HHRGs).
• 45 HHRGs; 153 case-mix weights – C1F1S1 to C3F3S5
• Each case-mix weight = a different payment
Certain diagnoses and OASIS items also contribute to payment for non-routine supplies, which is in addition to the episode payment.
33
Where Does the Money Come From?• Certain M items within the OASIS contribute to the Clinical ‘C’
score (see next slide)
• Certain diagnosis codes contribute case mix points as well toward the C score
• ADL items within the OASIS contribute toward the Functional ‘F’ score, as well as potentially help toward combining with diagnosis codes to assist with C score points
• Therapy visits solely contribute toward the Service Utilization ‘S’ score
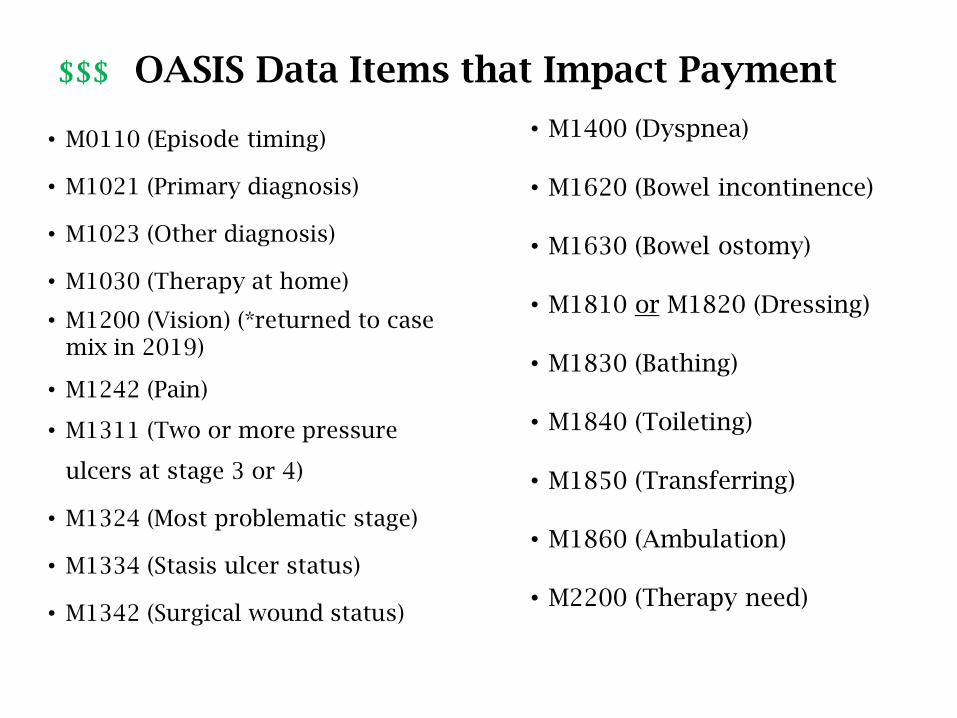
$$$ OASIS Data Items that Impact Payment
• M0110 (Episode timing)
• M1021 (Primary diagnosis)
• M1023 (Other diagnosis)
• M1030 (Therapy at home)
• M1200 (Vision) (*returned to case mix in 2019)
• M1242 (Pain)
• M1311 (Two or more pressure
ulcers at stage 3 or 4)
• M1324 (Most problematic stage)
• M1334 (Stasis ulcer status)
• M1342 (Surgical wound status)
• M1400 (Dyspnea)
• M1620 (Bowel incontinence)
• M1630 (Bowel ostomy)
• M1810 or M1820 (Dressing)
• M1830 (Bathing)
• M1840 (Toileting)
• M1850 (Transferring)
• M1860 (Ambulation)
• M2200 (Therapy need)
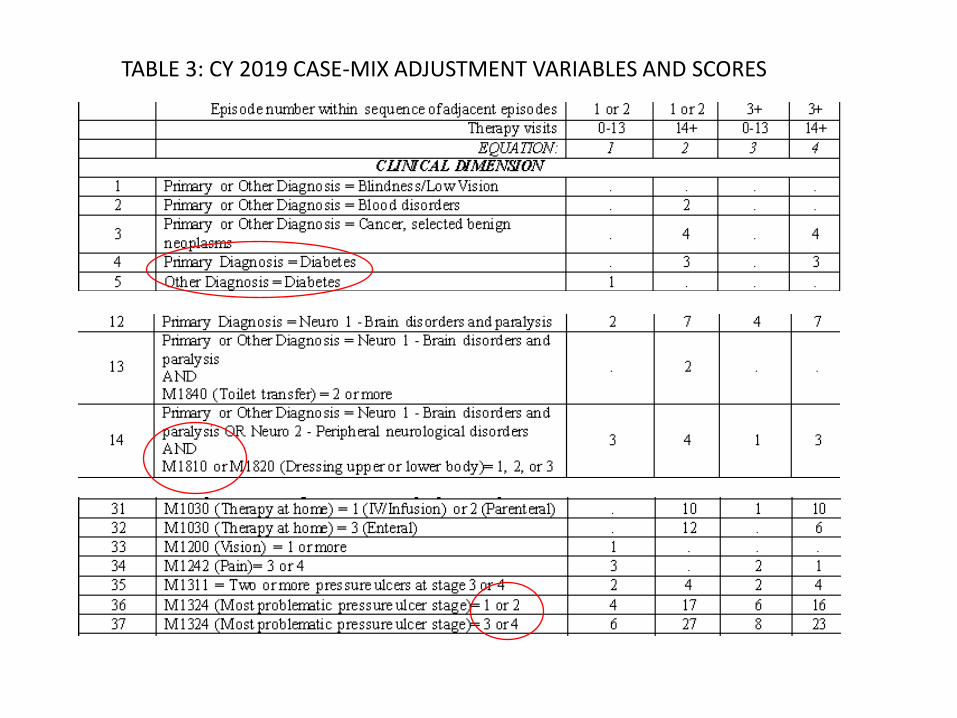
TABLE 3: CY 2019 CASE-MIX ADJUSTMENT VARIABLES AND SCORES

36
Clinical and Functional ThresholdsFinal Rule 2019
Dimension 1st & 2nd Episodes
EARLY
3rd + Episodes
LATER
All Episodes
0-13
Therapy
Visits
14-19
Therapy
Visits
0-13
Therapy
Visits
14-19
Therapy
Visits
20 +
Therapy
Visits
Equation 1 2 3 4 (2 & 4)
Clinical
(sum of
points)
C1 0 - 1 0 – 1 0 – 1 0 – 1 0 – 3
C2 2 - 3 2 - 7 2 2 – 9 4 – 16
C3 4+ 8+ 3+ 10+ 17+
Functional
(sum of points)
F1 0 – 12 0 –7 0 – 6 0 - 2 0 – 2
F2 13 8 – 12 7 – 10 3 – 7 3 – 6
F3 14+ 13+ 11+ 8+ 7+
Service
Utilization
(number of
therapy
visits)
S1 0 - 5 14 - 15 0 - 5 14 - 15 20+
S2 6 16 - 17 6 16 - 17
S3 7 - 9 18 - 19 7 - 9 18 - 19
S4 10 10
S5 11 - 13 11 - 13
37
UnderstandingOASIS-D
Ignorance ≠ Innocence

The Rules
38

One-Clinician Rule Reminder (Highlights)CMS Quarterly OASIS Q&As – April 2018, Question 1
• Effective January 1, 2018, as the assessing clinician, you may elicit input from the patient, caregivers, and other healthcare personnel, including the physician, the pharmacist, and/or other agency staff, to assist you in your completion of any or all OASIS items integrated within the comprehensive assessment document.
• When collaboration is utilized, the assessing clinician is responsible for considering available input from these other sources and selecting the appropriate OASIS item response(s) within the appropriate time frame and consistent with data collection guidance.
39
One-Clinician Rule Reminder (Highlights)CMS Quarterly OASIS Q&As – April 2018, Question 1
• For OASIS items requiring a patient assessment, the collaborating healthcare providers (e.g., other agency clinical staff: LPN/LVN, PTA, COTA, MSW, HHA) should have had direct in-person contact with the patient …
• M0090 (Date Assessment Completed) will indicate the last day the assessing clinician gathered or received any input used to complete the comprehensive assessment document, which includes the OASIS items. Reminder: for SOC the window is 5 days; for ROC/discharge the window is 2 days. 40
41
Painting the Picture
Every answer to an OASIS question is a brush stroke painting the picture of your patient!
42
CMS expectations
Select and assign OASIS diagnoses:• Based on comprehensive assessment of each patient’s overall medical condition and care needs;
• Verified by the physician;
• Following diagnosis coding rules; and
• According to clinical correctness, NOT to case-mix status.
43
CMS also expects HHAs to…
• Report any indication of fraudulent coding directly to the HHA administrator.
• Follow CMS OASIS correction policy, keeping OASIS corrections transparent.
• Stay current with guidance & updates.• When guidance from two CMS sources vary, follow the most
recent.
• Updates in Q&As supersede other guidance.
44
First things first…Qualifying Criteria
These criteria must be met in order to qualify for home care services under the Medicare benefit:
MUST have a physician to provide orders
MUST be homebound
Physician MUST participate, as required:
Complete a Face-to-Face encounter.
Establish a Plan of Care (collaborate with HHA) and review/update, as needed and at ROC, FollowUp, Recert, and DC.
MUST have a problem covered by the regulations
See Medicare Benefit Policy Manual – Chapter 7
45
Certifying Physician Must…
• Be a doctor of medicine, osteopathy, or podiatry
• Have no financial relationship with the HHA
• Have the patient under his/her care
• Establish, review, and update the home health POC
• Provide and sign orders
• Certify a face-to-face encounter was:• Done 90 days before or within 30 days after SOC • Related to the primary reason for home care • Performed by a physician or allowed NPP
46
Plan of Care
The “physician-ordered plan of care,” means that “the patient condition has been discussed and there is agreement as to the plan of care between the home health agency staff and the physician.”
Medicare CoP - §484.60 Standard: Plan of Care: “If a physician refers a patient under a plan of care that cannot be completed until after an evaluation visit, the physician is consulted to approve additions or modifications to the original plan.”
47
Face-to-Face Documentation
•Must include:• Certifying physician’s signature and date and
• Date of encounter
•Physician’s narrative is not required.
• The Medicare Administrative Contractor (MAC) will seek supporting documentation from certifying physician or inpatient facility.
Best practice: Agency should obtain this documentation from physician or facility for the patient record.
48
Homebound Requirement(Updated 11/19/13)
30.1.1 - Patient Confined to the Home
•For purposes of the statute, an individual shall be considered “confined to the home” (homebound) if the following two criteria are met:
49
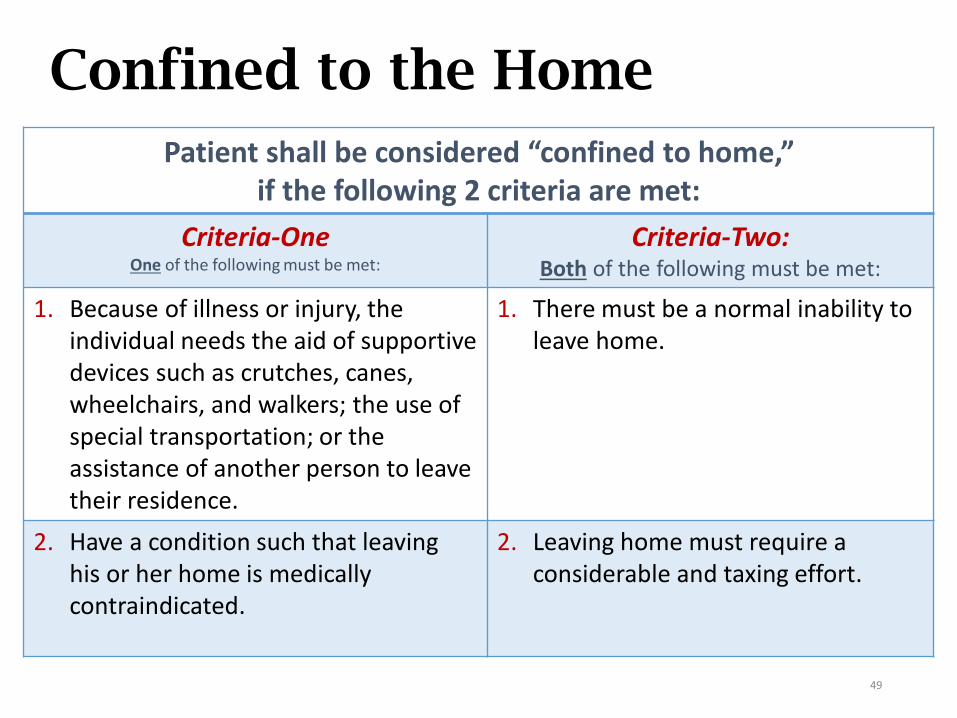
Confined to the Home
Patient shall be considered “confined to home,” if the following 2 criteria are met:
Criteria-OneOne of the following must be met:
Criteria-Two:Both of the following must be met:
1. Because of illness or injury, the individual needs the aid of supportive devices such as crutches, canes, wheelchairs, and walkers; the use of special transportation; or the assistance of another person to leave their residence.
1. There must be a normal inability to leave home.
2. Have a condition such that leaving his or her home is medically contraindicated.
2. Leaving home must require a considerable and taxing effort.
50
Skilled Need
Patient must have a Medicare-covered skilled service need
SN intermittent, skilled need, or
PT or SLP qualifying service, or
Continued OT need after SOC.
51
Assessments:Initial and Comprehensive
52
Initial Assessment
• Determines eligibility, immediate care needs, and homebound status
• Must be conducted either:• Within 48 hours of referral
• Within 48 hours of return home from inpatient admission (or upon notification of discharge) (this is in the CoPs as well)
• On the physician-ordered SOC date
Process measure – Timeliness of CareP
53
Who can conduct the assessment?
• Referral indicates nursing and therapy needs:• Case is NOT therapy-only.
• An RN must do both the initial assessment, to establish eligibility for home care, and the comprehensive assessment.
• If the order for nursing is not known at SOC and originates from a verbal order after SOC, the case is therapy-only at SOC, and a qualified therapist may perform the SOC assessment.
• LPN’s, PTA’s, COTA’s, MSW are not permitted to perform a comprehensive assessment, including the OASIS
54
Who can conduct the assessment?
• If therapy-only:• Appropriate therapist – PT or SLP/ST – may perform the
initial assessment.
• OT may only complete this assessment if the need for OT establishes program eligibility.Note: OT alone does not establish eligibility for the Medicare
home health benefit at SOC. However, it may under other programs, such as Medicaid, some Medicare Advantage plans, or private insurers. The payer must be queried regarding coverage guidelines.
• Agency policy to have RN perform OASIS SOC: • The RN can conduct the comprehensive assessment within the
first five days of the episode, but it must be done:• on the same date as the therapist’s SOC date
• or after the therapist SOC date (within 5 calendar days).
• The nursing visit for the therapy admit is not billable.
55
Comprehensive Assessment
• OASIS Assessment
• Must be completed in a timely manner• Consistent with patient’s immediate needs
• No later than 5 days after SOC (SOC date is day 0)
• Within 2 days of discharge from an inpatient facility or notification of discharge (ROC)
• On physician-ordered ROC date
• The comprehensive assessment must:• Identify the patient’s continuing need for home care, including
medical, nursing, rehabilitation, social, and discharge planning needs; and
• Include a drug regimen review.
• May perform initial assessment and comprehensive assessment on same visit or on different visits
• Must deliver a skilled service to be a reimbursable visit
56
Who can perform the updates?
• The discipline is not mandated after SOC.
• RN, PT, ST/SLP or OT may perform the updates; basically, any qualified discipline that is still active with the patient.
• RN is not required to perform the follow-up (recertification), resumption, and discharge OASIS, just because the nurse did the admission.
57
OASIS Requirements
58
Is OASIS required or not?
• OASIS is required for Medicare and Medicaid patients:• 18 years of age or older
• Receiving skilled non-maternity services
• OASIS is not required for patients:• Under 18 years of age
• Receiving skilled pre- and post-natal services
• Receiving personal care, housekeeping, or chore services only
• With single visit quality episodes
59
OASIS Data Collection Time PointsRFA 1: Start of Care (SOC)
RFA 3: Resumption of Care (ROC) following inpatient facility stay
RFA 4: Follow-Up (Recertification) within last 5 days of each 60-day episode
RFA 5: Other Follow-Up during the HH episode of care
RFA 6: Transfer to inpatient facility, not discharged from the agency
RFA 7: Transfer to inpatient facility, discharged from the agency
RFA 8: Death at Home
RFA 9: Discharge, not to a facility
• All time points, except transfer to an inpatient facility and death at home, require a comprehensive assessment.
Only SOC and Follow-Up assessments are used for determining payment based on a HHRG.
60
OASIS Management of Single Visit (SOC)
OASIS is not required by regulation if:• Only one visit planned and provided
• More visits planned but not provided after SOC
• One visit made, then patient admitted for qualifying inpatient stay before 2nd visit
• One visit made, but patient died before 2nd visit
• One visit made, but patient not taken under care
• A ROC visit made and patient refuses further visits
• If SOC OASIS is not required, a discharge OASIS is notrequired.
• A discharge summary is required, if the patient was admitted.
61
What if OASIS done and no further visits?
What if the OASIS has already been completed, encoded, and/or transmitted, and then no further visits are made?
• Conduct no further assessments.
• Document that no further visits occurred and why.
• Patient’s name will appear in the data system for 6 months.
• If patient is re-admitted, a warning will show the OASIS as out of sequence, but will not prevent transmission of further OASIS assessments.
62
If OASIS is Not Required by Payer
• HHAs must provide each patient, regardless of payment source, with a patient-specific comprehensive assessment that accurately reflects the patient’s current health status.
• Only exception is housekeeping and chore services
• The comprehensive assessment must:• Identify the patient’s continuing need for home care, including
medical, nursing, rehabilitation, social, and discharge planning needs; and
• Include a drug regimen review.
• HHAs may collect OASIS data on their non-Medicare and non-Medicaid patients for their own use.
63
OASIS Conventions
64
OASIS Conventions
• Conventions are general rules that should be observed when completing the OASIS.
• Chapter 1, OASIS Guidance Manual • 14 general Conventions
• 6 ADL/IADL-specific Conventions
• Updated through the Q&As• https://www.qtso.com/hhatrain.html
• Anyone may submit questions on how to complete OASIS items, if a patient’s situation has not been addressed by CMS-published or accepted resources.
General Conventions
• Follow rules included in the Item Specific Guidance.
• Stay current with evolving CMS OASIS guidance updates.
• The Dash (-): Some items allow a dash response. A dash (–) value indicates that no information is available, and/or an item could not be assessed. Most often occurs when patient is unexpectedly transferred, discharged or dies before assessment of the item could be completed. CMS expects dash use to be a rare occurrence.
65
General Conventions
• Direct observation: the preferred strategy when assessing physiologic or functional health status.
• Definition of Assistance: means assistance from another person unless otherwise specified within the item.
• Includes verbal cues, supervision, and stand-by assist.
• One Clinician Rule: Only one clinician takes responsibility for accurately completing a comprehensive assessment. (More on this later).
• Complete OASIS items accurately and comprehensively, and adhere to skip patterns.
• Minimize the use of “NA” and “Unknown” responses.
• Understand the definitions of words used in OASIS.
66
General Convention: Day of Assessment
• Day of Assessment: Understand the time period under consideration for each item. Report what is true on the day of assessment unless a different time period has been indicated in the item or related guidance. “Day of assessment” is defined as the 24 hours immediately preceding the home visit and the time spent by the clinician in the home.
• Examples of other time periods in OASIS:• Last 14 days
• Same day
• Recent pertinent past
• Prior to the current illness, exacerbation, or injury
• At or since the time of the last SOC/ROC
67
General Convention: Care Episode
• Care Episode: A care episode (also referred to as a quality episode) must have a beginning (that is, a SOC or ROC assessment) and a conclusion (that is, a Transfer or Discharge assessment) to be considered a complete care episode. Note: Care episodes are the basis for quality measurements
• Scenario: The patient was admitted to home health on 7/1 and transferred to the hospital on 7/15. ROC was performed by the agency on 7/23. The patient was discharged from the agency on 8/20.
• How many complete “care episode(s)” did the patient have?
• What were the start and end point(s) for the care episode(s)?
• How many payment episodes did patient have?
68
General Convention: Care Episode
• Scenario: The patient was admitted to home health
on 7/1 and transferred to the hospital on 7/15. ROC
was performed by the agency on 7/23. The patient
was discharged from the agency on 8/20.
• How many complete “care episode(s)” did the patient have?
• Answer: Two
• What were the start and end point(s) for the care episode(s)?
• Answer: 7/1 – 7/15; 7/23 – 8/20
• How many payment episodes did patient have?
• Answer: One: 7/1 to 8/20
69
General Convention: Usual Status
• Majority Rules: If the patient’s ability or status varies on the day of the assessment, report the patient’s “usual status” or what is true greater than 50% of the assessment time frame, unless the item specifies differently.
• M2020 Management of Oral Medications and M2030 Management of Injectable Medications: instead of “usual status” or “greater than 50% of the time,” consider the medication or equipment for which the most assistance is needed.
• M1860 Ambulation/Locomotion: Usual status convention does not apply because of the structure of the response options. (CMS Q&A #154.1)
70
71
“Look Back”
• Several process items require documentation of prior care, at the time or since the time of the most recent SOC or ROC OASIS assessment.
• Review the record, and
• Consult with other disciplines.
• These instructions are included in item guidance for the relevant OASIS questions.
Look-Back Period example
• Even though this is no longer new guidance, many still struggle with this.
• (M2401) Intervention Synopsis: (Check only one box in each row.) At the time of or at any time since the most recent SOC/ROC assessment, were the following interventions BOTH included in the physician-ordered plan of care AND implemented?
Mrs. Simple is seen Oct. 1, 2018 for new onset of diabetes. Her initial POC consists of orders for diabetic teaching, med monitoring and education, which were completed during the first episode.
72
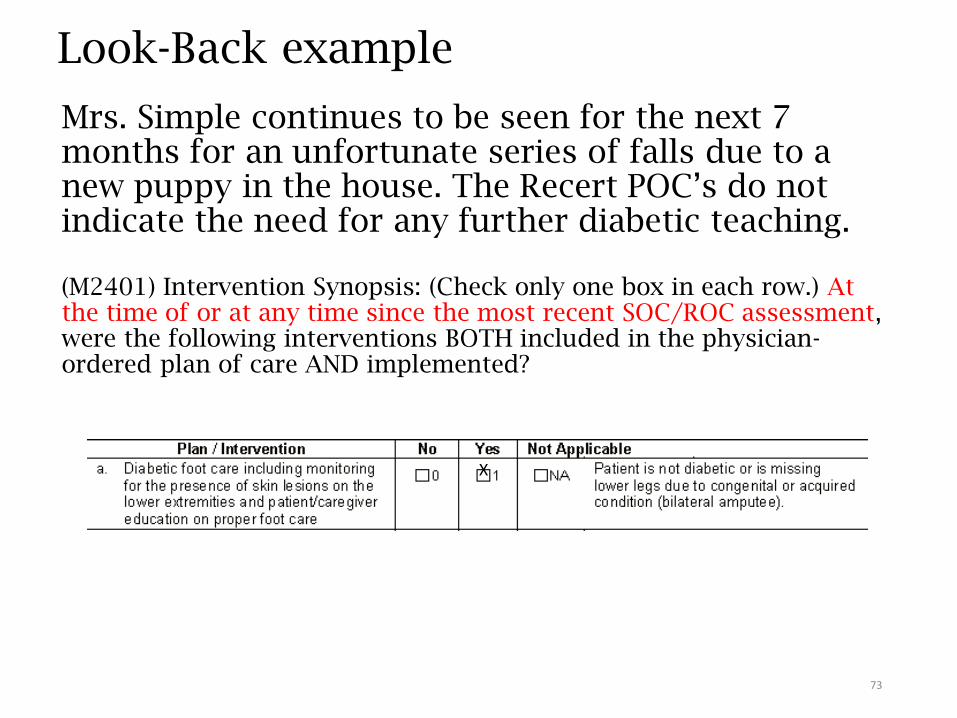
Look-Back example
Mrs. Simple continues to be seen for the next 7 months for an unfortunate series of falls due to a new puppy in the house. The Recert POC’s do not indicate the need for any further diabetic teaching.
(M2401) Intervention Synopsis: (Check only one box in each row.) At the time of or at any time since the most recent SOC/ROC assessment, were the following interventions BOTH included in the physician-ordered plan of care AND implemented?
73
X
74
Assessing Patient Status
• Combine observation, interview, and other relevant strategies to complete OASIS data items as needed. For example, it is acceptable to review the hospital discharge summary to identify inpatient procedures and diagnoses at SOC or to examine the care notes to determine if a physician-ordered intervention was implemented at Transfer or Discharge.
• Direct observation is the preferred strategy when assessing physiologic or functional health status.
• Ask the patient to perform specific tasks, and
• Observe the patient’s performance.
75
Understand Definitions
• “Specifically” means scoring of the item should be limited to only the circumstances listed.
• “For example” means clinician may consider other relevant circumstances or attributes when scoring the item.
• “Assistance” means assistance from another person, unless otherwise specified within the item.Includes verbal cues, supervision, and stand-by assist.
A service animal is not assistance; it is considered an assistive device.
• Minimize the use of “NA” and “Unknown” responses.
• Instead, do some searching to find the answers.
76
Standardized Tool Criteria
• “One that has been scientifically tested on a population with characteristics similar to that of the patient being assessed.”
• The standardized tool:• Must be appropriate for the patient
• Must be able to understand and participate
• Must have a standard response scale – e.g., TUG, numeric scales
• Must be appropriately administered, as indicated in the instructions
• Must be completed during the CMS-specified assessment time frame
SOC – within 5 days
ROC – within 48 hours following inpatient facility discharge or knowledge of discharge
77
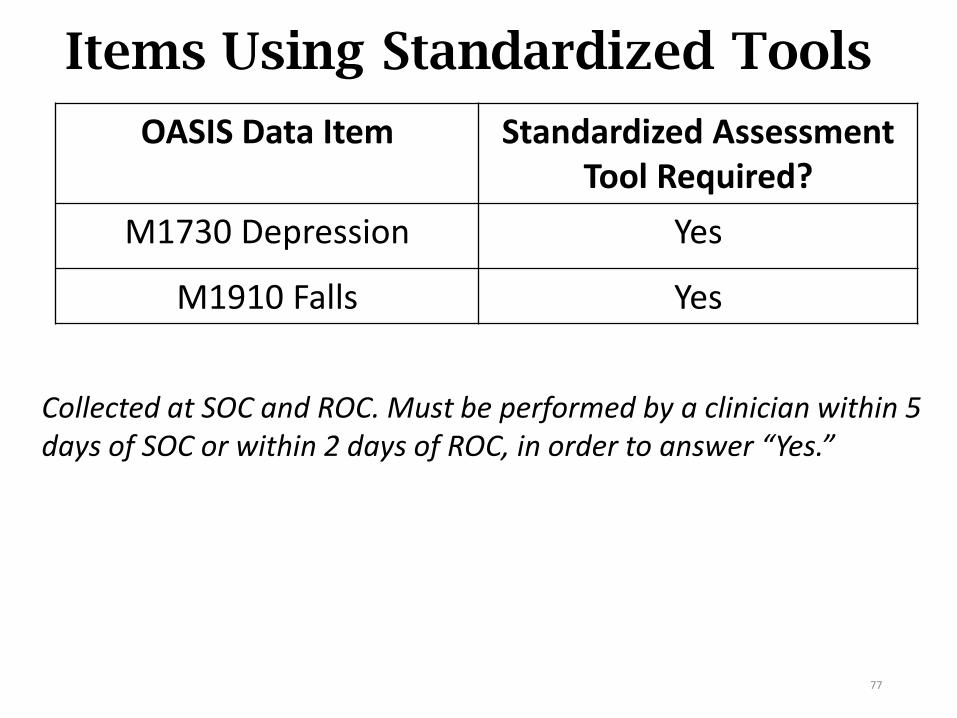
Items Using Standardized Tools
OASIS Data Item Standardized AssessmentTool Required?
M1730 Depression Yes
M1910 Falls Yes
Collected at SOC and ROC. Must be performed by a clinician within 5 days of SOC or within 2 days of ROC, in order to answer “Yes.”
Importance of Documentation
• Documentation is one of the central elements that underlies:The quality and skilled nature of patient care;
Coding and billing for the care provided; and
An effective compliance plan.
oSpecificity of diagnosis code assignment is essential in creating an accurate andcompliant medical record.
Creating a Compliant Record
• Begins at referral/intake with requests for:• F2F and/or the reason for referral to home care
• Dates and places of recent inpatient stays/surgeries
• Copies of the H&P, consultations, operative report, if applicable, discharge summary, etc.
• If referral is from the MD office – procure H&P, current medication list, and visit notes
• Continues with review of the documentation, then…
• A complete and thorough comprehensive assessment!
Assessment Strategies
Per the OASIS Guidance Manual, Chapter 3…
• Interview patient/caregiver to obtain past health history. Additional information may be obtained from the physician.
• Review current medications and other treatment approaches.
• Determine if additional diagnoses are suggested by the current treatment regimen.
• Verify this information with the patient/caregiver andphysician.
“What’s new or different?”
• Look for problems and changes in treatment. Remember, CHANGE IS YOUR FRIEND!
• For patients referred from physician, ask what’s worsened or changed. What prompted the referral NOW?
82
Patient Tracking ItemsM0030 – M0032
Completed at SOC and updated when a change occurs in the episode.
83
Timely Initiation of Care
Home Health Compare Quality Process Measure• How often the home health team began their patients’ care in
a timely manner.
OASIS items that contribute to the measure: M1005 Inpatient Discharge Date
M0030 SOC Date
M0032 ROC Date
M0102 Date of Physician-ordered SOC (ROC)
M0104 Date of Referral
But, what’s a “timely manner”?
P
84
Timely Initiation of Care
• If physician has specified a SOC/ROC date, then the SOC/ROC should be on or before that date.
• If no SOC/ROC date has been specified by the physician, then the SOC/ROC should be:
• Within two days of referral OR
• If the inpatient discharge is later than the referral, within two days of inpatient discharge.
P
85
(M0030)
• The start of care date is the date of the first billable visit
• A reimbursable (skilled) service must be delivered to be considered the start of care. A physician must specifically order that a covered service be furnished on the SOC date.
“Accuracy of this date is essential since many other aspects of data collection are based on this date.”
85
86
(M0032)
• The ROC date is the date of the first visit following an inpatient stay and may be conducted by any person providing a service under the agency’s home health plan of care – may be made by an aide, therapy assistant, or LPN.
• The ROC comprehensive assessment must be completed within 48 hours of discharge following a qualifying inpatient stay or within 48 hours of knowledge of the qualifying inpatient stay.
• At SOC, mark “NA.”
• There must be orders for the ROC and the visit performed.
86
87
How would you answer these?
Your patient was released from the hospital and needed an injection that evening (November 1st). The case manager was unavailable and planned to do the ROC assessment the following day (November 2nd).
Could the on-call nurse visit and give the injection before the ROC assessment is done?
Can an LPN do the ROC visit? The assessment?
M0032 (ROC date) is ________.
M0090 (Date assessment completed) is ________.
88
AnswersYour patient was released from the hospital and needed an injection that evening (November 1st). The case manager was unavailable and planned to do the ROC assessment the following day (November 2nd).
Could the on-call nurse visit and give the injection before the ROC assessment is done?
Yes
Can an LPN do the ROC visit?
Yes
The assessment?
No
M0032 (ROC date) is
November 1st.
M0090 (Date assessment completed) is
November 2nd.
89
M0080, M0090, M0090, M0150
90
(M0080)
• Specifies the discipline of the clinician completing the comprehensive assessment during an actual visit to the patient’s home at the specified OASIS time point or the clinician reporting the transfer to an inpatient facility or death at home.
91
M0080: Guidance
• Only one individual may complete and record the assessment, even when two disciplines are seeing the patient at the time of the assessment.
• The PT/SLP may visit after the initial RN visit, even if the RN has not completed the SOC comprehensive assessment.
• Clerical (office) staff may enter demographic data and agency ID items, but the assessing clinician must verify accuracy.
• When both the RN and qualified therapist are scheduled to conduct discharge visits on the same day, the last qualified clinician to see the patient is responsible for conducting the discharge comprehensive assessment.
92
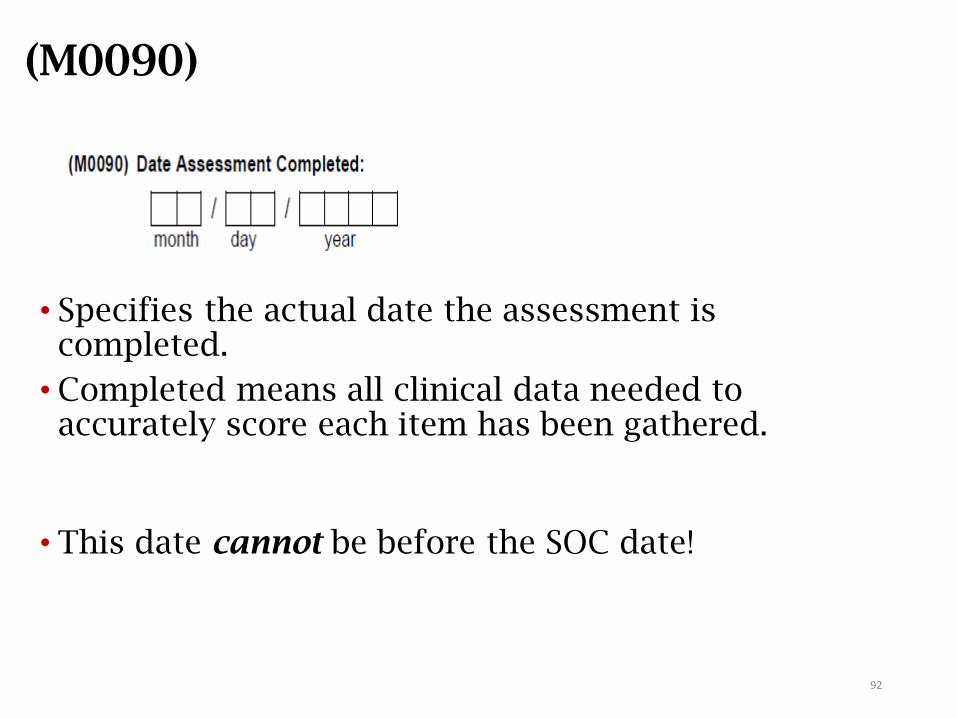
(M0090)
• Specifies the actual date the assessment is completed.
• Completed means all clinical data needed to accurately score each item has been gathered.
• This date cannot be before the SOC date!
93
M0090: Guidance
The OASIS typically takes more than one day to
complete. It actually may be completed on a day that
does NOT coincide with that clinician’s visit.
What can affect the M0090 date:
• Waiting for physician call back regarding medication
issues
• Physician clarification of prior diagnoses requiring a
code change
• Waiting to confer with the therapists regarding M2200
Therapy need and/or interventions for the POC
• Waiting to confer with the physician for interventions
on the POC
94
M0090: Guidance (cont.)
• If consulting with another discipline, or completing the OASIS over multiple visits, use the latest applicable date within range:
• Up to 5 days after SOC (day 0);
• Days 56-60 for Recertification;
• Within 48 hours of inpatient discharge (or knowledge of) for ROC.
• For Transfer and Death at home assessments:
• Record the date the agency completes the data collection after learning of the event.
• A visit might not be associated with these events.
• Do not change this date for OASIS corrections due to audits.
• If payer change requires re-creating a SOC OASIS, M0090 will be out of range:
• Disregard warning at OASIS submission; and
• Document circumstances in patient record.
95
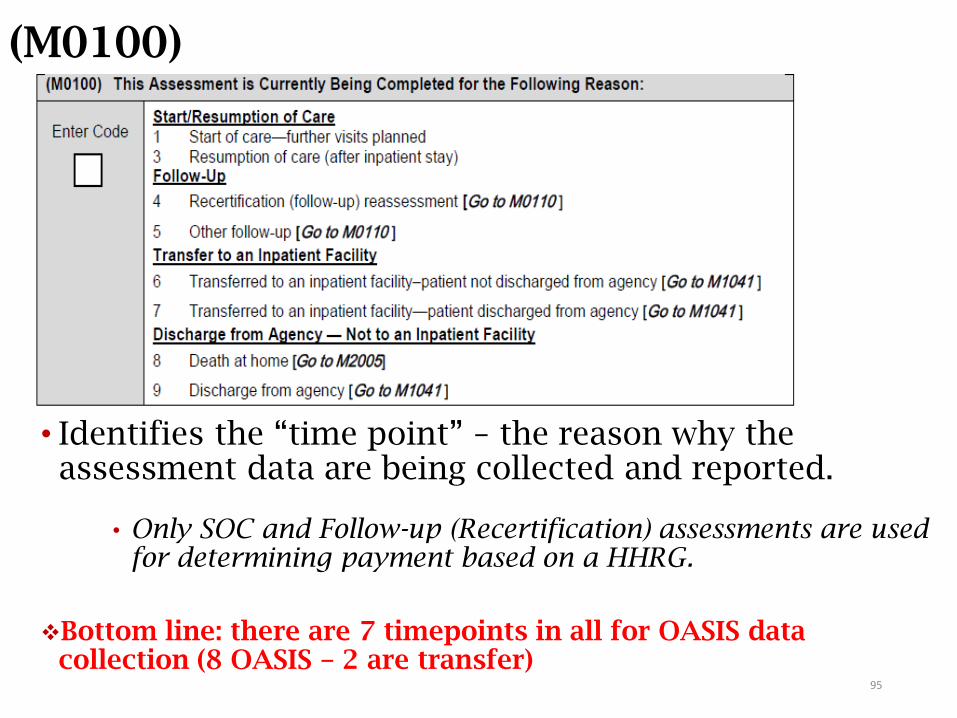
(M0100)
• Identifies the “time point” – the reason why the assessment data are being collected and reported.
• Only SOC and Follow-up (Recertification) assessments are used for determining payment based on a HHRG.
Bottom line: there are 7 timepoints in all for OASIS data collection (8 OASIS – 2 are transfer)
M0100 – RFA 1 (SOC Assessment)
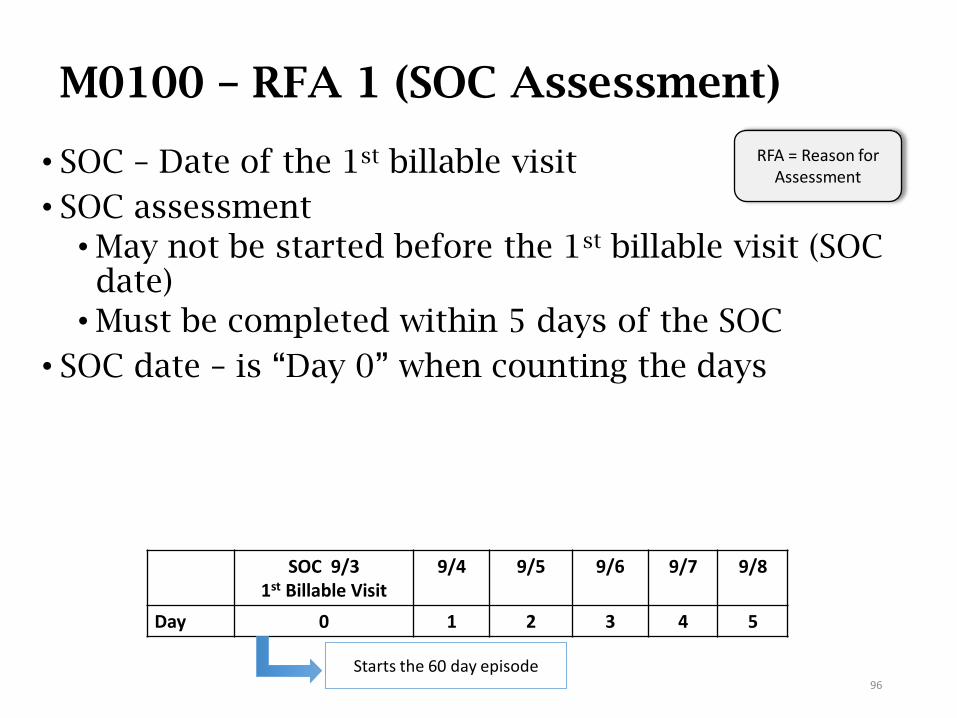
• SOC – Date of the 1st billable visit
• SOC assessment
• May not be started before the 1st billable visit (SOC date)
• Must be completed within 5 days of the SOC
• SOC date – is “Day 0” when counting the days
96
SOC 9/31st Billable Visit
9/4 9/5 9/6 9/7 9/8
Day 0 1 2 3 4 5
RFA = Reason for Assessment
Starts the 60 day episode
M0100 – RFA 3 (ROC Assessment)
• Conducted when patient resumes care after inpatient stay of 24 hrs. or longer for reasons other than diagnostic testing.
• The visit must be completed: • within 2 days of the patient’s discharge
• within 2 days of learning of the discharge
• or on the physician-ordered ROC date
• If recert is planned and the patient returns home in the last 5 days of the episode – only the ROC assessment is completed. A recertification assessment (RFA4) is not required, but the POC (485) is.
• Note: Physician orders are required to provide care. When an agency does not have orders within the 2 days from inpatient DC or knowledge of same, the agency should document efforts to obtain orders and complete ROC visit when orders are obtained.
97
When the ROC Comprehensive Assessment is Late
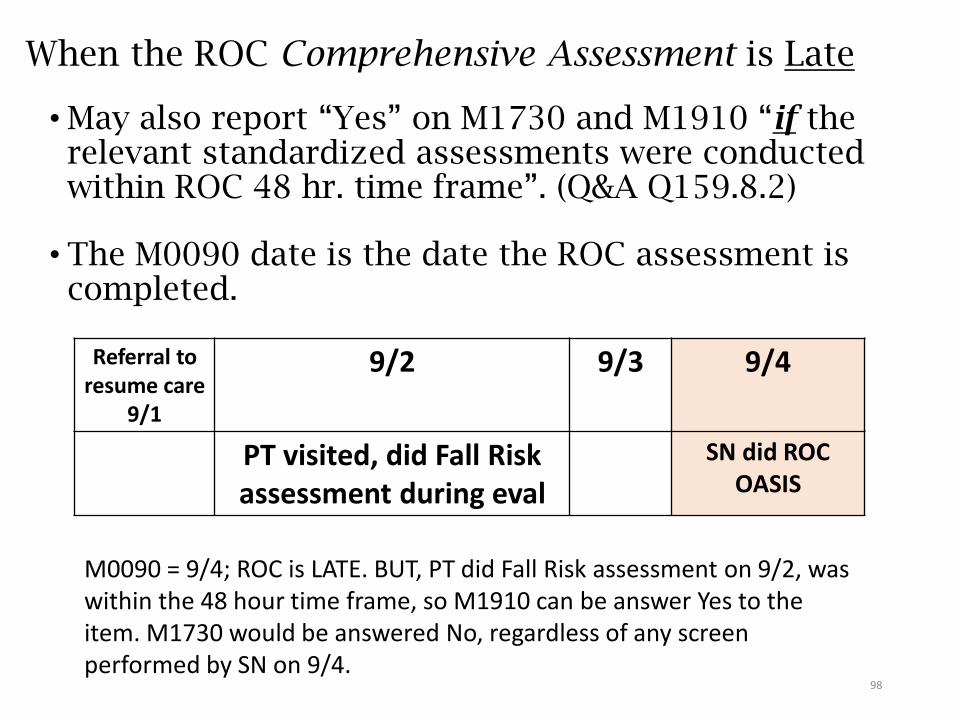
• May also report “Yes” on M1730 and M1910 “if the relevant standardized assessments were conducted within ROC 48 hr. time frame”. (Q&A Q159.8.2)
• The M0090 date is the date the ROC assessment is completed.
98
Referral to resume care
9/1
9/2 9/3 9/4
PT visited, did Fall Risk assessment during eval
SN did ROC OASIS
M0090 = 9/4; ROC is LATE. BUT, PT did Fall Risk assessment on 9/2, was within the 48 hour time frame, so M1910 can be answer Yes to the item. M1730 would be answered No, regardless of any screen performed by SN on 9/4.
M0100 - RFA 4 (Recertification)
• RFA 4 (Follow-Up / Recertification):• Completed on day 56 – 60 of the episode (last 5 days).
• May take more than 1 day and up to 5 days to complete.
• What if I miss the recert assessment window? • DO NOT D/C AND READMIT!!!!
• Complete the RFA 4 as soon as the error is found.
• Assign M0090 Date as the date the assessment is completed.
• Document reasons for late assessment in record.
99
100
RFA 5: Other follow-up
Comprehensive assessment (reassessment) due to a major decline or improvement in patient’s condition notenvisioned in the original plan of care
• Requires home visit
• Completed at time other than last 5 days of episode, when there has been no inpatient stay
• May indicate need to update patient’s plan of care
• Policies regarding criteria for RFA 5 determined by agency
• Must be completed within 2 days of identifying a major improvement or decline in patient’s health status
101
RFA 6: Transfer to Inpatient Facility –patient not discharged from agency
Transfer to inpatient facility – includes planned admissions• Transferred and admitted to inpatient bed of inpatient facility
• Stay of 24 hours or longer
• For reasons other than diagnostic tests
• Does not require home visit
• Must be completed within 2 days of transfer date (M0906) orknowledge of transfer that meets criteria
• If discovered later, complete RFA 6 within 2 days then complete RFA 3 (ROC).
• Complete RFA 6 for Medicare PPS patients you feel will return to agency.
• Other payers may have different requirements.
• If patient does not return to agency, do internal agency DC (no DC OASIS).
• M0906 (Transfer Date) = date patient admitted to inpatient bed, not the ER/observation unit.
102
RFA 7: Transfer to Inpatient Facility –patient discharged from agency
• Requirements for completing a transfer to inpatient facility with discharge from agency are the same as a RFA 6, except an RFA 7 is completed when a patient willNOT return to the agency – e.g., patient needs higher level of care, moves out of service area, etc.
• Do internal agency discharge (no discharge OASIS required).
• If patient dies in ER, outpatient surgery/recovery room, while under outpatient observation status, within 24 hours of admission to an inpatient facility, the usual transfer requirements are waived.
• Why? Because observation status is not a hospital admission.
103
RFA 8: Death at Home
• Patient died somewhere other than inpatient/outpatient facility or ER. For example:
• At home
• At church
• In an ambulance
• Pronounced dead on arrival (DOA) in ER
• A home visit is not required.
• Complete within 2 days of death date (M0906).
• M0906 (Death Date) = date patient actually died.
104
Completing Transfer and Death at Home
Can someone in the office who has never seen the patient complete
the Transfer and Death at Home OASIS?
• Yes
• Transfer and Death at home require data collection, not a visit.
• Includes no assessment findings
• Any RN, PT, OT, or SLP familiar with OASIS data collection
practices may collect the data, per agency policy.
• Data may be collected by phone and through record review.
• Guidance applies only to the Transfer and Death at Home
OASIS – not SOC, ROC, Follow-Up (Recertification), Other
Follow-up, and Discharge.
105
RFA 9: Discharge from Agency
• Requires home visit
• Does not include:• Death in an inpatient facility
• Death in an ambulance
• Dead on arrival (DOA) in ER
• Complete within 2 days of discharge date (M0906) or knowledge of need to discharge.
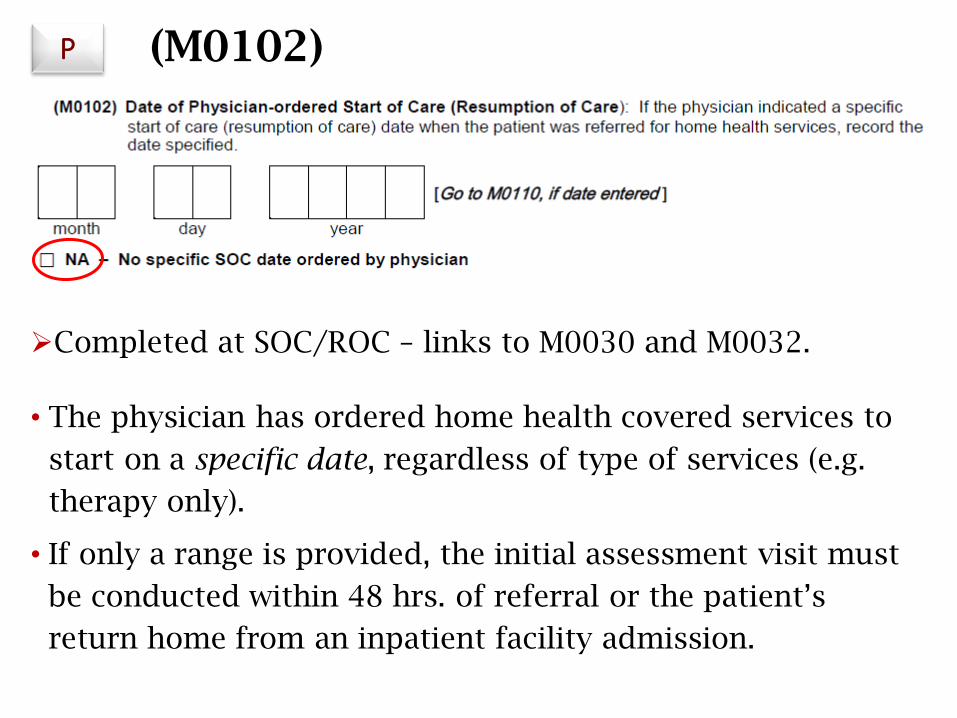
(M0102)
Completed at SOC/ROC – links to M0030 and M0032.
• The physician has ordered home health covered services to
start on a specific date, regardless of type of services (e.g.
therapy only).
• If only a range is provided, the initial assessment visit must
be conducted within 48 hrs. of referral or the patient’s
return home from an inpatient facility admission.
P
Physician-Ordered ROC
• With the update of the Conditions of Participation, the physician can now order a ROC date, even if it is greater than 48 hours after discharge from an inpatient facility
• The July 2018 OASIS Q&As, category 4b, Questions 4 and 5, elaborate further on this guidance, and the errata published July 30, 2018 and again January 25, 2019 corrects an error from the draft guidance
• When the physician specifies a date that homecare services must resume (a physician-ordered ROC date), the agency must conduct the ROC visit on that date
• The agency has up to 2 calendar days from the ROC date (M0032) to complete the ROC assessment document (M0090)
107
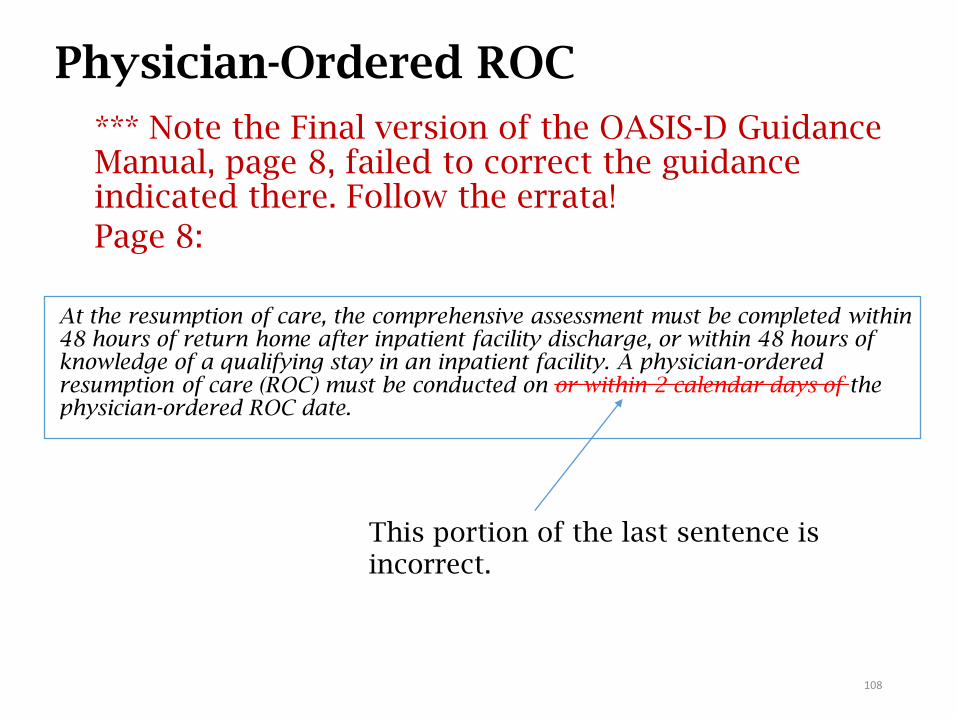
Physician-Ordered ROC
*** Note the Final version of the OASIS-D Guidance Manual, page 8, failed to correct the guidance indicated there. Follow the errata!
Page 8:
At the resumption of care, the comprehensive assessment must be completed within 48 hours of return home after inpatient facility discharge, or within 48 hours of knowledge of a qualifying stay in an inpatient facility. A physician-ordered resumption of care (ROC) must be conducted on or within 2 calendar days of the physician-ordered ROC date.
108
This portion of the last sentence is incorrect.
Physician Ordered ROC from July 2018 Q&As
• QUESTION 5: Now that the physician can order a ROC date that goes beyond 48 hours from hospital discharge, can that date ever be extended? Our patient was discharged from the hospital on Tuesday and the referral included orders to resume his care on Friday. When we called to arrange the time of the visit, he said he had other medical appointments on Friday and to come Monday. We called the ordering physician Friday requesting a delay in the ROC and received a call back on Monday approving the delay in ROC. How do we answer M0102?
• ANSWER 5: To report this new updated/revised physician’s ordered resumption of care date in M0102, it must have been received on or before the date of the previous physician’s ordered resumption of care. If the order to extend the physician’s ordered resumption of care date is received after the date of the previous physician’s ordered resumption of care date has passed, report NA for M0102 and report the original referral date in M0104. In your scenario, since you received the updated physician ordered resumption of care date after the original physician ordered resumption of care date had passed, report NA for M0102 and the original referral date (Tuesday) in M0104.
109
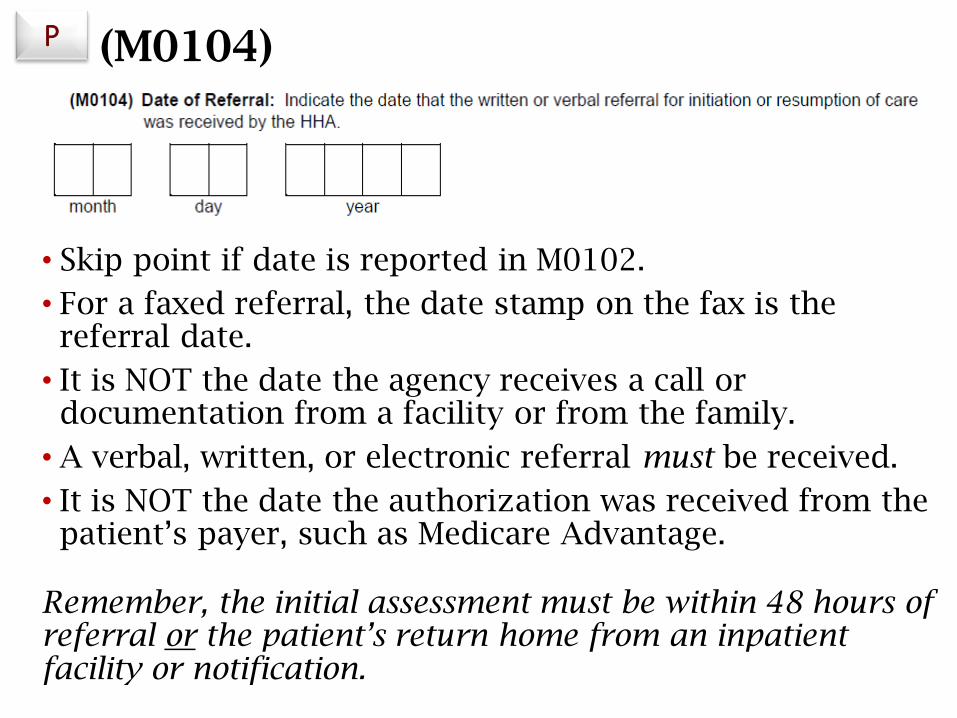
(M0104)
• Skip point if date is reported in M0102.
• For a faxed referral, the date stamp on the fax is the referral date.
• It is NOT the date the agency receives a call or documentation from a facility or from the family.
• A verbal, written, or electronic referral must be received.
• It is NOT the date the authorization was received from the patient’s payer, such as Medicare Advantage.
Remember, the initial assessment must be within 48 hours of referral or the patient’s return home from an inpatient facility or notification.
P
M0102/M0104: Guidance
• Referrals from hospital/SNF discharge planners on behalf of the physician may be considered when determining the SOC or referral date. (This should generate a verbal order.)
• There must be an order or change in patient condition to change the date. The request of the patient, family, or ALF staff to delay SOC is not included as a reason for delay of SOC/referral date.
• If the original SOC date is delayed due to patient condition or physician request (order), the date the agency receives the updated/revised referral order is the new referral date.
• To be considered a physician-ordered SOC date, the physician must give a specific date to initiate care, not a range of dates.
• If only a date range is provided, the initial assessment visit must be conducted within 48 hours of referral or patient’s return home from IP facility.
Consider this situation…
The hospital discharge planner notified your agency on 11/14 that Mrs. L was being discharged from the hospital that day. However, she developed a fever and remained hospitalized. On 11/18, the discharge planner called and said Mrs. L was going home that afternoon and needed a nursing visit that evening to administer IV antibiotics for a postoperative wound infection.
The RN performed the initial assessment and started the comprehensive assessment and OASIS that evening, but the patient was too tired for the nurse to complete the assessment. The nurse decided that the case manager could finish it the following morning, 11/19. PT was ordered for strengthening, and their eval was done on 11/21. The MD confirmed the nursing POC on 11/20 and the therapy POC on 11/21.

Which of the following is true?
a) The nurse who made the initial visit on 11/18 must complete the SOC OASIS on that day.
M0030 and M0090 = 11/18; M0102 = NA; M0104 = 11/14
b) The RN who made the visit on 11/19 may complete the SOC OASIS that was started the evening before.
M0030 = 11/18; M0090 = 11/19; M0102 = 11/18; skip M0104
c) The RN who visited on 11/19 must complete a new SOC OASIS.
M0030 and M0090 = 11/19; M0102 = NA; M0104 = 11/18
d) The RN who visited on 11/19 must complete a new SOC OASIS.
M0030 = 11/18; M0090 = 11/21; M0102 = 11/18; skip M0104
Answer
a) The nurse who made the initial visit on 11/18 must complete the SOC OASIS on that day.
M0030 and M0090 = 11/18; M0102 = NA; M0104 = 11/14
b) The RN who made the visit on 11/19 may complete the SOC OASIS that was started the evening before.
M0030 = 11/18; M0090 = 11/19; M0102 = 11/18; skip M0104
c) The RN who visited on 11/19 must complete a new SOC OASIS. M0030 and M0090 = 11/19; M0102 = NA; M0104 = 11/18
d) The RN who visited on 11/19 must complete a new SOC OASIS.
M0030 = 11/18; M0090 = 11/21; M0102 = 11/18; skip M0104
What constitutes a valid referral?
• The patient must be under the care of a physician.
• A valid referral exists if the referring physician, or another physician, will provide for the plan of care and ongoing orders and has provided adequate information regarding the patient.
• When the referring physician (i.e., hospitalist) is notgoing to provide a plan of care and ongoing orders and follow the patient, this is not a valid referral.
• The HHA must contact an alternate or attending physician who agrees to follow the patient and provide ongoing orders.
• The M0104 date is the date of the following physician’s agreement to provide a plan of care and ongoing orders for the patient.
More on Valid Referrals
• A general order to “Evaluate for Home Care services” (no discipline(s) specified) is a valid order if:
• It is received from a physician who will be following the patient and provide ongoing orders.
• Per CoP §484.55, the RN must conduct the initial assessment to determine immediate care and support needs and eligibility for the HH Benefit for Medicare patients.
• An order stating only to “eval for home safety” is not a valid referral per CMS.
SOC Scenario #1
• On 3/12, Dr. G wrote orders to admit Mr. T for home health services following discharge from the hospital. Mr. T was released from the hospital on 3/16. If the admitting clinician conducts a billable visit on 3/18, will the initiation of care be timely?
SOC Scenario #1
• On 3/12, Dr. G wrote orders to admit Mr. T for home health services following discharge from the hospital. Mr. T was released from the hospital on 3/16. If the admitting clinician conducts a billable visit on 3/18, will the initiation of care be timely?
• Yes
• M1005 Inpatient Discharge Date: 3/16
• M0030 SOC Date: 3/18
• M0102 Date of Physician-ordered SOC (ROC): N/A
• M0104 Date of Referral: 3/12
SOC Scenario #2a
• On 3/12, Dr. G wrote orders to admit Mr. T for home health services following discharge from the hospital. Mr. T was released from the hospital on 3/16; when the RN called to schedule the admit visit, he requested to be left alone until the 20th. The clinician notifies the physician on the 20th of the delay. If the admitting clinician conducts a billable visit on 3/20, will the initiation of care be timely?
• No
• M1005 Inpatient Discharge Date: 3/16
• M0030 SOC Date: 3/20
• M0102 Date of Physician-ordered SOC (ROC): N/A. The order to extend care must be received prior to the visit, within the allotted time frame (48 hrs from discharge).
• M0104 Date of Referral: 3/12
SOC Scenario #2b
• On 3/12, Dr. G wrote orders to admit Mr. T for home health services following discharge from the hospital. Mr. T was released from the hospital on 3/16; when the RN called to schedule the admit visit, he requested to be left alone until the 20th. The clinician notifies the physician on the 17th, and receives a verbal order to begin care on the 20th. If the admitting clinician conducts a billable visit on 3/20, will the initiation of care be timely?
• Yes
• M1005 Inpatient Discharge Date: 3/16• M0030 SOC Date: 3/20• M0102 Date of Physician-ordered SOC (ROC): 3/20
• M0104 Date of Referral: NA
Referral Scenario
Mr. B was seen in the ER on 9/2. Your agency received a faxed referral from the ER physician on 9/2 to admit the patient for skilled nursing services. The ER physician will not be following Mr. B. The record states that the patient’s PCP (Dr. Frank) will follow the patient.
The agency calls Dr. Frank to validate that he will provide a plan of care and ongoing orders for Mr. B. Dr. Frank states that he will not order HH services until he sees the patient on 9/4. On 9/5 Dr. Frank calls your agency and provides orders for HH services for Mr. B.
What is the appropriate response to M0104 (Date of Referral)?
9/5
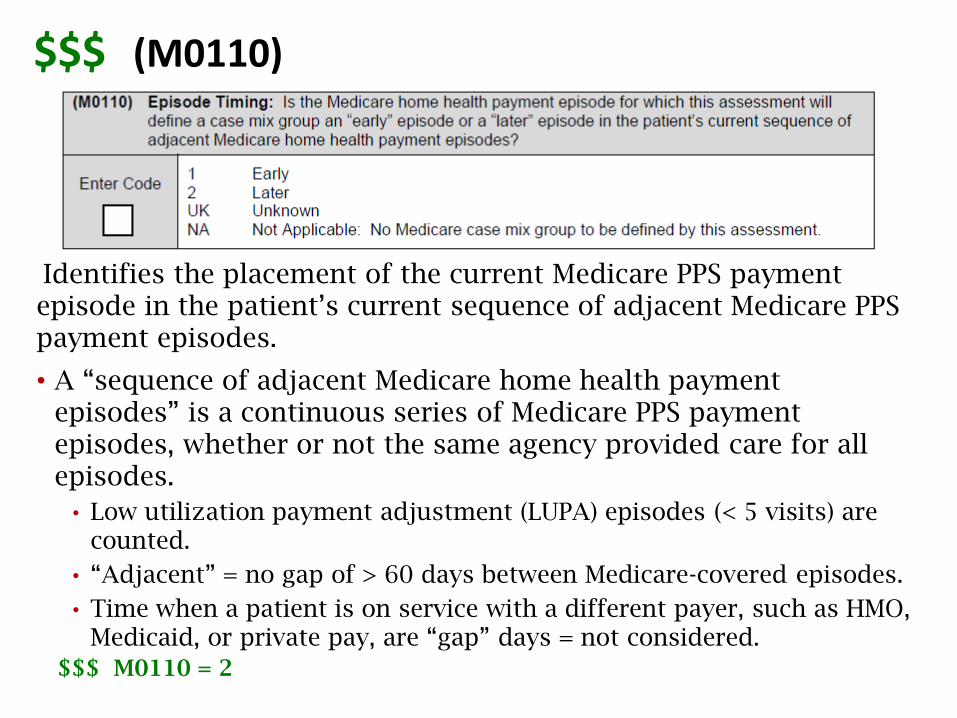
Identifies the placement of the current Medicare PPS payment episode in the patient’s current sequence of adjacent Medicare PPS payment episodes.
• A “sequence of adjacent Medicare home health payment episodes” is a continuous series of Medicare PPS payment episodes, whether or not the same agency provided care for all episodes.
• Low utilization payment adjustment (LUPA) episodes (< 5 visits) are counted.
• “Adjacent” = no gap of > 60 days between Medicare-covered episodes.
• Time when a patient is on service with a different payer, such as HMO, Medicaid, or private pay, are “gap” days = not considered.
$$$ M0110 = 2
$$$ (M0110)
M0110: Guidance
• “Early” includes the only PPS episode in a single episode case OR is the first or second PPS episode in a sequence of adjacent PPS episodes.
• “Later” means the third or later PPS episode in a sequence of adjacent episodes.
• Enter “UK - Unknown” if the placement of this PPS payment episode in the sequence of adjacent episodes is unknown. For the purposes of assigning a case mix code to the episode, this will have the same effect as entering the “Early” response.
M0110: Guidance
• Enter “NA” if no Medicare case mix group is to be defined for this episode.
• If no Medicare case-mix group is to be defined for this episode (ROC and Other Follow-up, other payers), select NA.
• If a non-Medicare FFS payer requires an HHRG for payment, select UK.
• If a Medicare FFS is secondary payer in M0150, complete M0110 as if Medicare is primary.
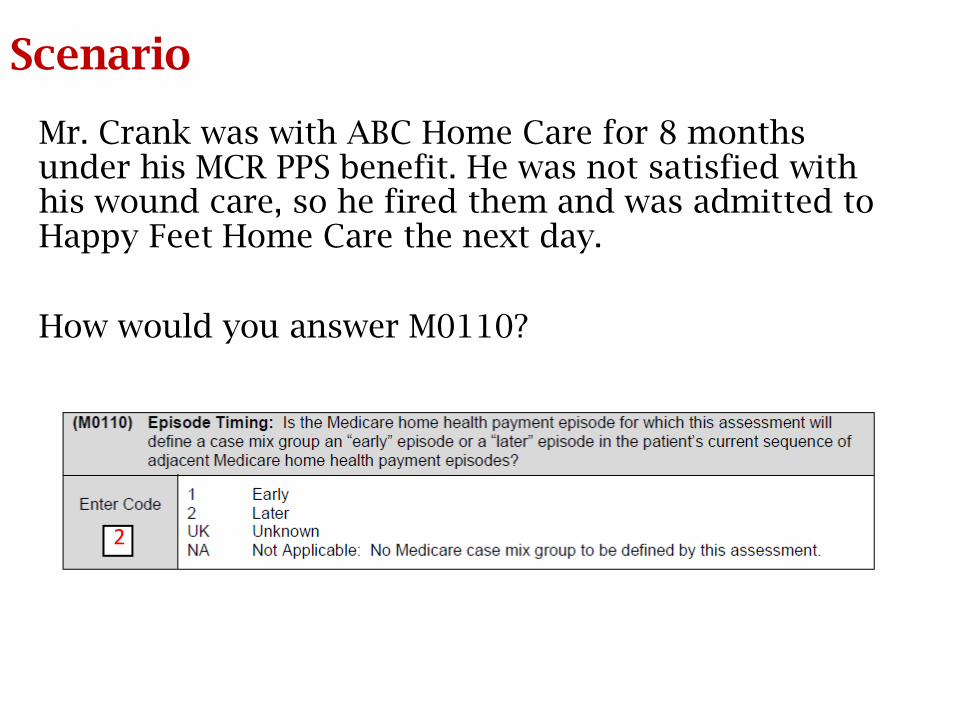
Scenario
Mr. Crank was with ABC Home Care for 8 months under his MCR PPS benefit. He was not satisfied with his wound care, so he fired them and was admitted to Happy Feet Home Care the next day.
How would you answer M0110?
2
126
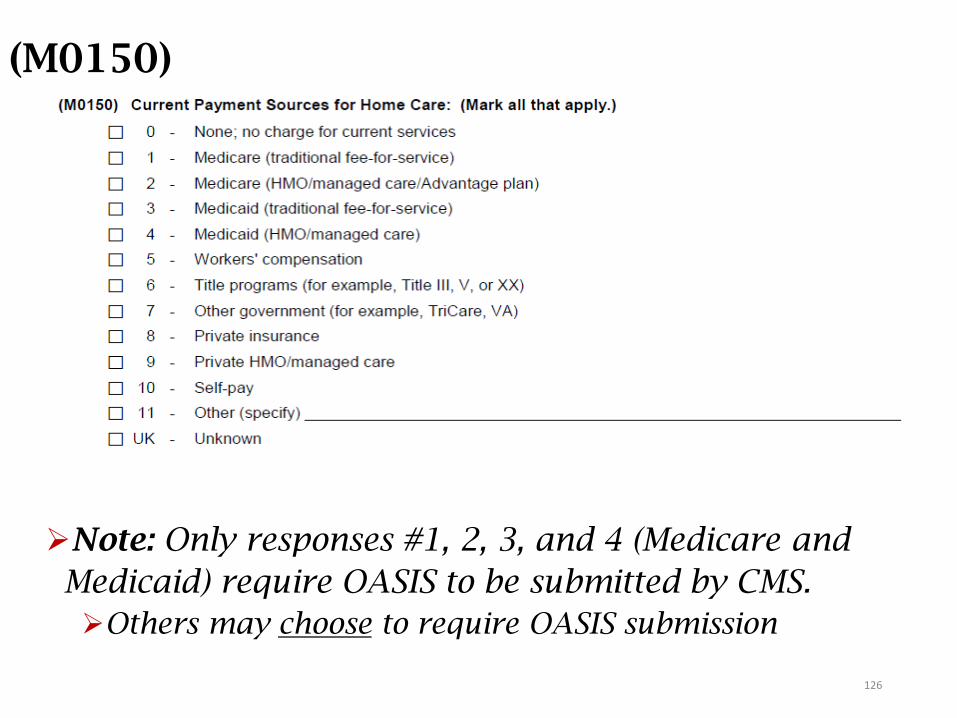
(M0150)
6 - Title programs (e.g., Title III, V, or XX)
7 - Other government (e.g., TriCare, VA, etc.)
8 - Private Insurance
9 - Private HMO/managed care
10 - Self-pay
11 - Other (specify) ____________________________
Note: Only responses #1, 2, 3, and 4 (Medicare and
Medicaid) require OASIS to be submitted by CMS.
Others may choose to require OASIS submission
127
M0150: Guidance
• This item is limited to identifying payers to which any services provided during this home care episode and included on the plan of care will be billed by your home health agency.
• Mark all that apply – those that may be billed by the agency – whether considered primary or secondary.
• Exclude “pending” payment sources.
• Do not consider any equipment, medications, or supplies being paid for by the patient, in part or in full.

128
MEDICARE as Payer
• If the payer is Medicare as primary or secondary, then Medicare must be checked.
• If the payer changes to Medicare, there must be a new SOC date.
• If the payer changes from Medicare to another payer, change M0150 at the next OASIS time point, unless the payer has other requirements.
See the response-specific instructions in Chapter 3 of the OASIS Guidance Manual for selection of the payment sources.
129
How would you mark M0150?
Your patient sustained injuries in an auto accident and the liability insurance is paying for home health. Most of the insurance money was spent on the hospitalization, though. Your patient has traditional Medicare and is eligible for the home health benefit (homebound, etc.).
What response(s) will you check on M0150?
130
Answer
Your patient sustained injuries in an auto accident and the liability insurance is paying for home health. Most of the insurance money was spent on the hospitalization, though. Your patient has traditional Medicare and is eligible for the home health benefit (homebound, etc.).
What will you check on M0150?1 - Medicare (traditional fee-for-service)
8 - Private insurance
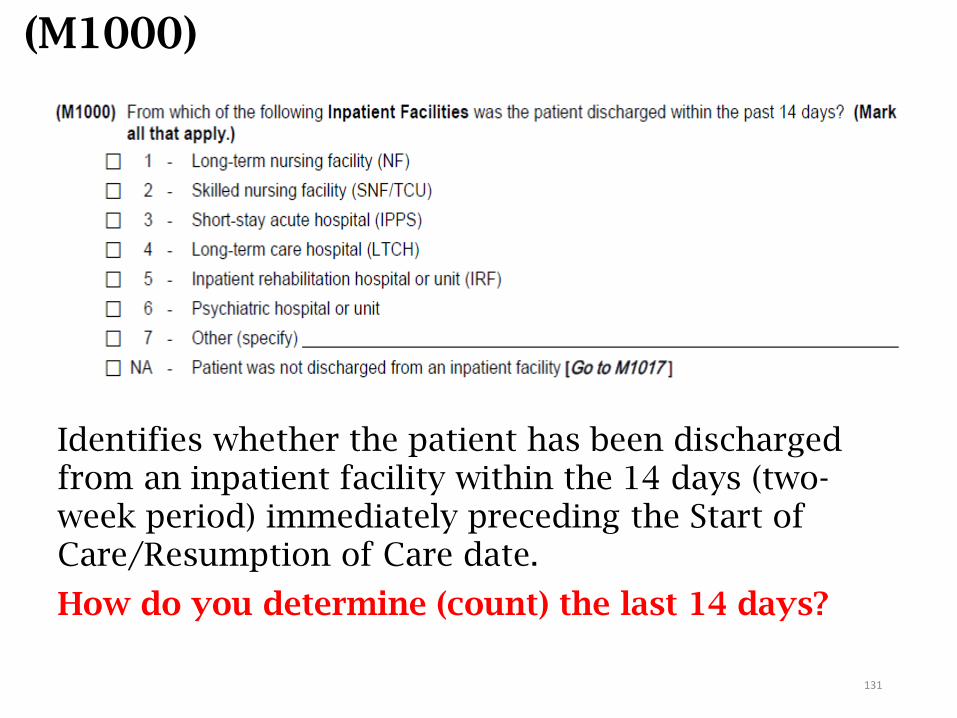
Identifies whether the patient has been discharged from an inpatient facility within the 14 days (two-week period) immediately preceding the Start of Care/Resumption of Care date.
How do you determine (count) the last 14 days?
(M1000)
131
M1000: Guidance
• A patient may have been discharged from more than one facility within the 14 days prior to SOC/ROC.
• An inpatient discharge on the day of assessment (day 0) falls within the 14-day period.
• The facility type is determined by the facility’s state license.
See Chapter 3 of the Guidance Manual for specifics regarding the responses.
132
How would you mark M1000?Mr. E was admitted to the hospital on 7/26 and discharged to
rehab on 8/1. He was discharged from rehab on 8/8 to an
assisted living facility where he did not receive skilled care. After
6 days in the ALF, he went to stay with his son because he didn’t
like living there. He was admitted to your agency on 8/16. Which
response(s) would you select for M1000?
1 - Long term nursing facility
2 - Skilled nursing facility
3 - Short-stay acute hospital
4 - Long-term care hospital
5 - Inpatient rehabilitation
6 - Psychiatric hospital
7 - Other (specify)
NA - Patient was not discharged from an inpatient facility
133
Answer
Mr. E was admitted to the hospital on 7/26 and discharged to rehab on 8/1. He was discharged from rehab on 8/8 to an assisted living facility where he did not receive skilled care. After 6 days in the ALF, he went to stay with his son, because he didn’t like living there. He was admitted to your agency on 8/16. Which response(s) would you select for M1000?
Select the correct response: 1 - Long term nursing facility 2 - Skilled nursing facility 3 - Short-stay acute hospital 4 - Long-term care hospital 5 - Inpatient rehabilitation 6 - Psychiatric hospital 7 - Other (specify) NA - Patient was not discharged from an inpatient
facility134
(M1005)
• Enter the date of only the most recent discharge:
• From an inpatient facility identified at M1000• Occurred within 14 days of SOC/ROC.
135
135
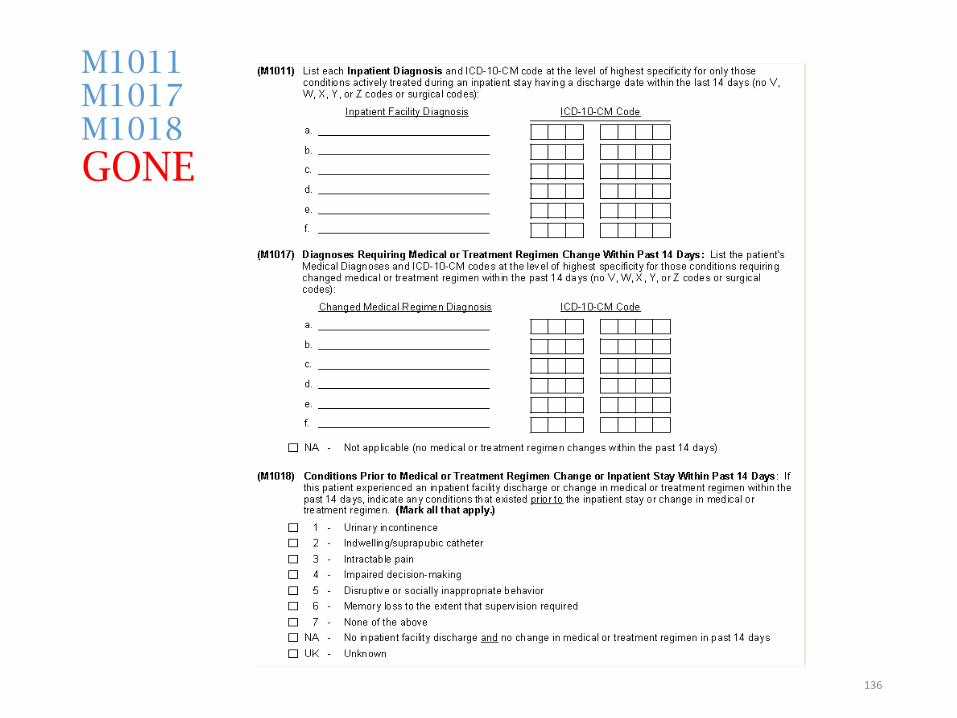
M1011M1017M1018
GONE
136
Impact
• Under OASIS-C2, completing the M1011/M1017 items allowed the agency to indicate in diagnosis format the patient’s recent medical concerns. This helped to support the need for current care.
• With these items gone, it is more crucial than ever for documentation to indicate what the patient was recently treated for, why continued care is necessary, and specifically what that care will consist of. A comprehensive admission narrative is of the utmost importance!
• This also ties in to the loss of M1018. As those may have been long-term conditions, if care is still rendered toward them, documentation must support why the care is needed – caregiver education, have there been any changes, are new diagnoses impacting the long-term issues, etc.
137
OASIS, Coding, and Relationships to PPS
• 2 OASIS-D coding items:
•M1021, M1023
• All diagnoses must match on:• OASIS, POC, and the final claim (UB-04)
• In OASIS, coding is governed by the ICD-10-CM Coding Conventions and Guidelines and by the response-specific guidance in Chapter 3 of the OASIS-D Guidance Manual.
• V, W, X, Y codes are only allowed in M1023.
• Z codes are allowed in M1021 and M1023.138
Official Coding Guidance Sources
• Official Coding Guidelines
• Coding Conventions
• OASIS Guidance Manual• Chapter 1: Conventions
• Chapter 3: Item-by-Item guidance
• Coding Clinic• Quarterly publication by the American Hospital
Association, whose guidance is approved by CMS
• Other CMS Guidance• Annual Final Rule
• CMS Q&As • https://www.qtso.com/hhatrain.html
139
Important Questions to AskWhy was the patient referred for home care? What does the F2F
say?
What problems are unresolved?
Are there any co-morbidities that may impact the outcome?
Is there more than one problem targeted for intervention?
If more than one discipline is ordered, is there a diagnosis common to multiple disciplines?
What services are needed to achieve the goals/outcomes?
Are there coding conventions that require additional codes or listing diagnoses in a specific order?
Often, the most challenging question of all is…140
What is the focus of care?
141
SOC narrative in a nutshell
• Indicate why the patient was hospitalized/visit to physician; surgeries performed
• Indicate primary diagnosis: the focus of care, need for home care
• State what other comorbidities will be addressed by the agency AND WHY
• Identify potential roadblocks to recovery/risk for rehospitalization
142
ROC narrative in a nutshell
• Indicate why the patient was re-hospitalized and when, what was addressed, surgeries performed
• Indicate (new) primary diagnosis, the focus of care, need for home care
• State what other comorbidities will be addressed by the agency AND WHY
• Identify potential roadblocks to recovery/risk for rehospitalization
143
Recert narrative in a nutshell
• The narrative is to recap the patient’s status at the beginning of the episode, compare it to the present status, and then state why continued skilled care is needed, as well as specify what that skilled care is.
• Fyi: SN is a discipline, not a skill
• Indicate (new) primary diagnosis, the focus of care
• State what other comorbidities will be continue to be addressed by the agency AND WHY
• Identify potential roadblocks to recovery/risk for rehospitalization
144
Identifying the Diagnoses
• Go beyond the checkmarks on the assessment.
• How is the patient functioning now?
• How about 3-6 months ago?
• Dig deep into the medications. Are there related diagnoses or a clue that there may be others?
• Consider what other illnesses or conditions the patient has that may impact the care plan.
145
Comorbidities add complexity!
• “Comorbidity” is the presence of one or more additional disorders (or diseases) co-occurring with a primary disease or disorder, that can worsen the course of both, even if the condition is well-managed, and is associated with:
• Worse health outcomes;
• More complex clinical management; and
• Increased health care costs.
• Identifying comorbidities that are relevant to the current POC helps support medical necessity!
146
Identifying the Diagnoses (cont.)
• Determine the level of the patient’s knowledge of his/her health conditions.
• Identify goals that are measurable, attainable, and appropriate for the patient, so the POC can be focused on what needs to be done and why.
• Collaborate with other disciplines who will be providing services to the patient.
• Select and sequence the diagnoses according to their “seriousness” related to the care plan.
147
Determining Diagnoses for the POC
• Diagnoses must support that services provided are reasonable and necessary.
• Select only those diagnoses that:• Comply with the coding guidelines and sequencing
requirements;
• Are relevant to the POC;
• Are unresolved;
• Are verified by current treatment regimen and the physician; and
• Are supported by documentation in the medical record, reflective of the F2F.
148
Assignment of Diagnoses
• Assignment of the diagnosis must be based on:
• Physician documentation or verification of ALLdiagnoses;
• Findings of the comprehensive assessment;
• Official Coding Guidelines; and
• OASIS guidance.
• The assessing clinician is responsible for:
• Selecting and sequencing the diagnoses, in conjunction with the physician; and
• Assigning the symptom control ratings (0-4).
149
More…
• Onset and exacerbation dates are not mandated by CMS.
• BUT: If used, they must be supported by the medical record.
• A coder may assign the codes.
• The assessing clinician must agree with any changes.
• Documentation of collaboration with the clinician is imperative!
150
• Physician verification is imperative!
• Verify diagnoses, medications, or treatments notdocumented or unclear.
• Confirm specific wound type and complications.
• Clarify cause of condition.
• Is the patient’s anemia due to CKD or a vitamin deficiency?
• Approve interventions for POC.
DOCUMENT all communication with the physician!
Physician MUST Verify POC!
151
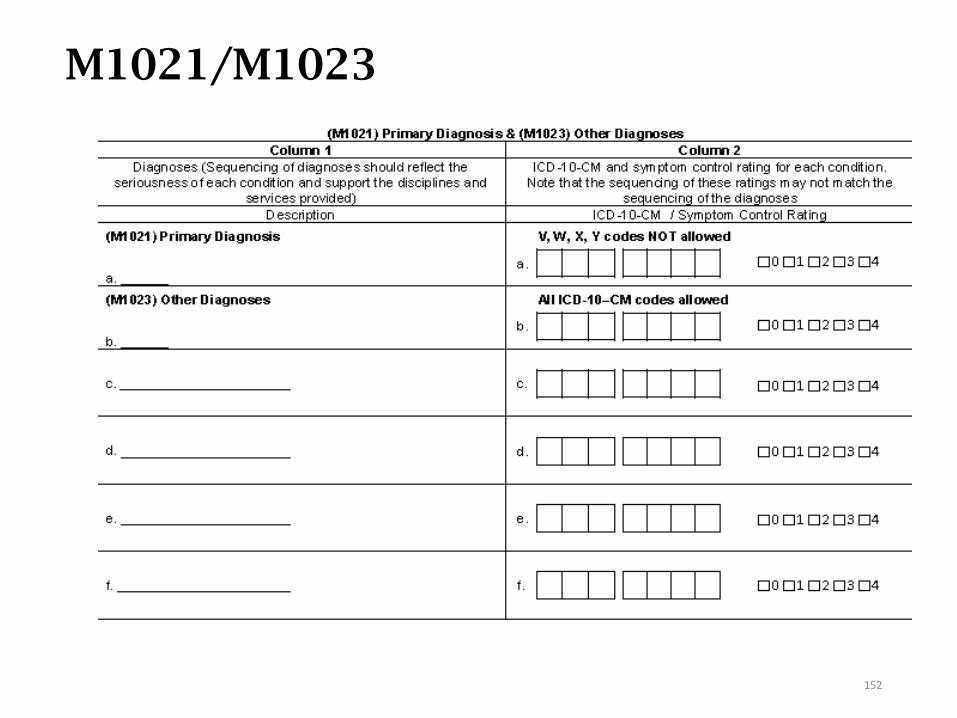
M1021/M1023
152
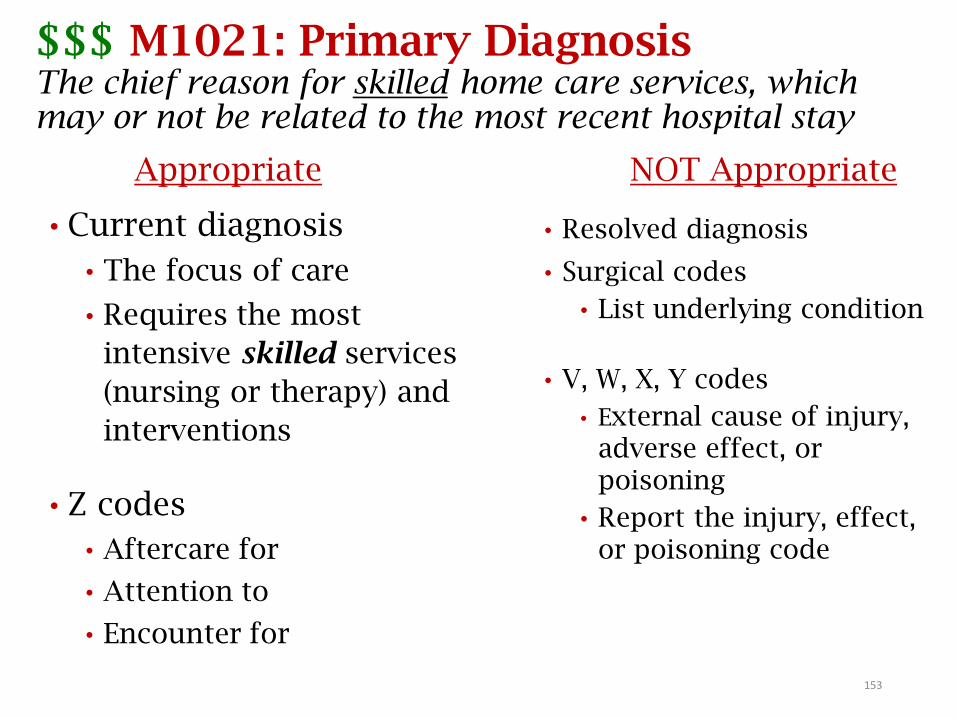
$$$ M1021: Primary DiagnosisThe chief reason for skilled home care services, which may or not be related to the most recent hospital stay
Appropriate
• Current diagnosis
• The focus of care
• Requires the most
intensive skilled services
(nursing or therapy) and
interventions
• Z codes
• Aftercare for
• Attention to
• Encounter for
NOT Appropriate
• Resolved diagnosis
• Surgical codes
• List underlying condition
• V, W, X, Y codes
• External cause of injury, adverse effect, or poisoning
• Report the injury, effect, or poisoning code
153
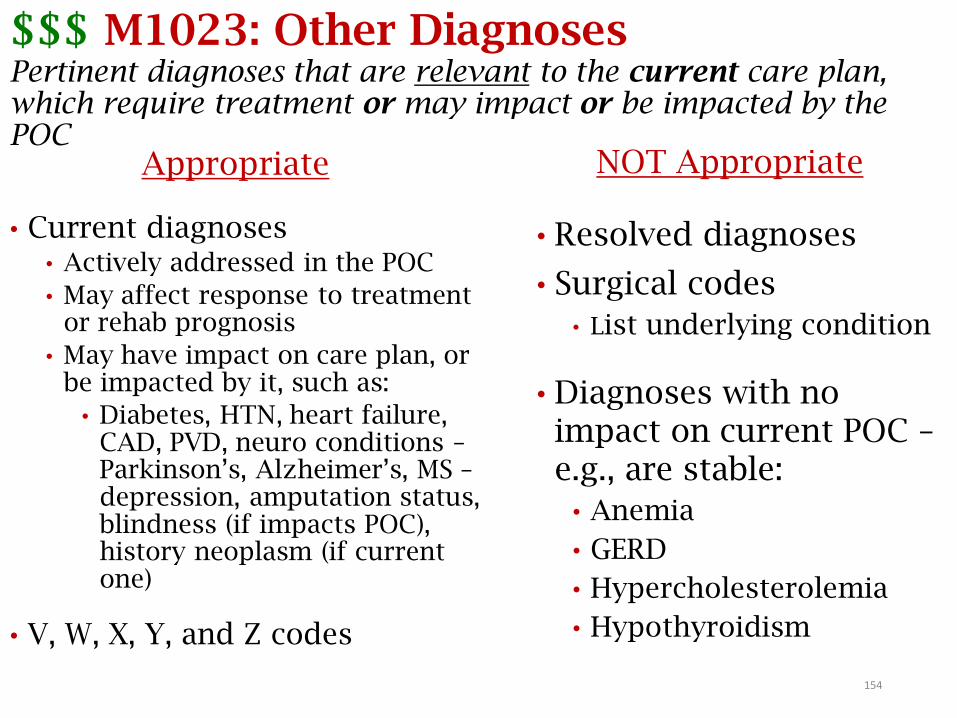
$$$ M1023: Other DiagnosesPertinent diagnoses that are relevant to the current care plan, which require treatment or may impact or be impacted by the POC
Appropriate
• Current diagnoses• Actively addressed in the POC
• May affect response to treatment or rehab prognosis
• May have impact on care plan, or be impacted by it, such as:
• Diabetes, HTN, heart failure, CAD, PVD, neuro conditions –Parkinson’s, Alzheimer’s, MS –depression, amputation status, blindness (if impacts POC), history neoplasm (if current one)
• V, W, X, Y, and Z codes
NOT Appropriate
• Resolved diagnoses
• Surgical codes
• List underlying condition
• Diagnoses with no impact on current POC –e.g., are stable:
• Anemia
• GERD
• Hypercholesterolemia
• Hypothyroidism
154
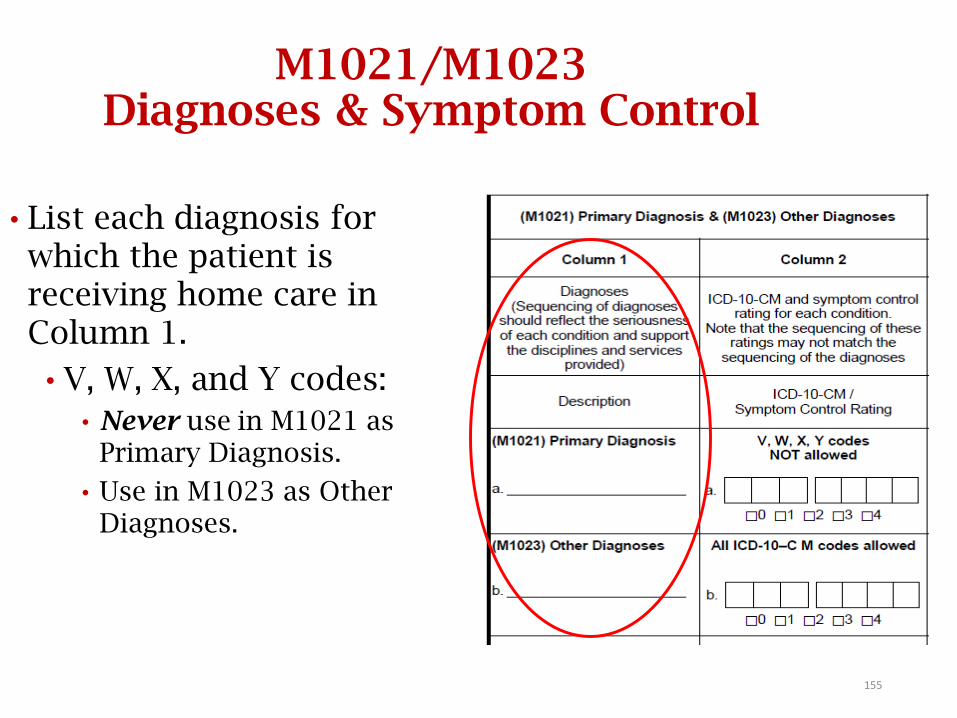
M1021/M1023 Diagnoses & Symptom Control
• List each diagnosis for which the patient is receiving home care in Column 1.
• V, W, X, and Y codes:
• Never use in M1021 as Primary Diagnosis.
• Use in M1023 as Other Diagnoses.
155
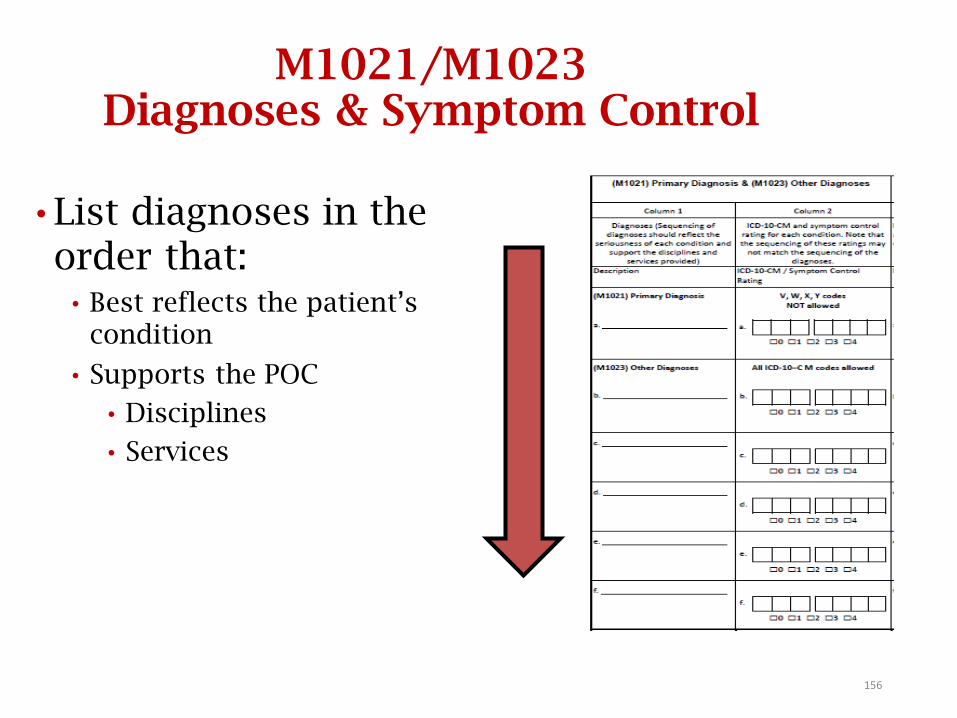
M1021/M1023 Diagnoses & Symptom Control
• List diagnoses in the order that:
• Best reflects the patient’s condition
• Supports the POC
• Disciplines
• Services
156
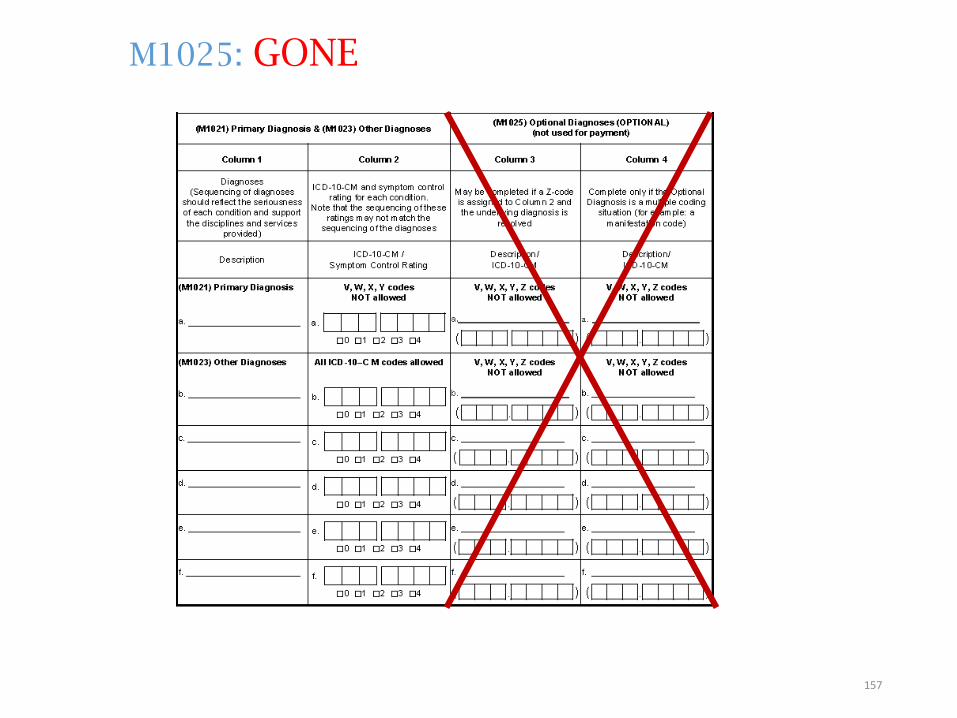
M1025: GONE
157
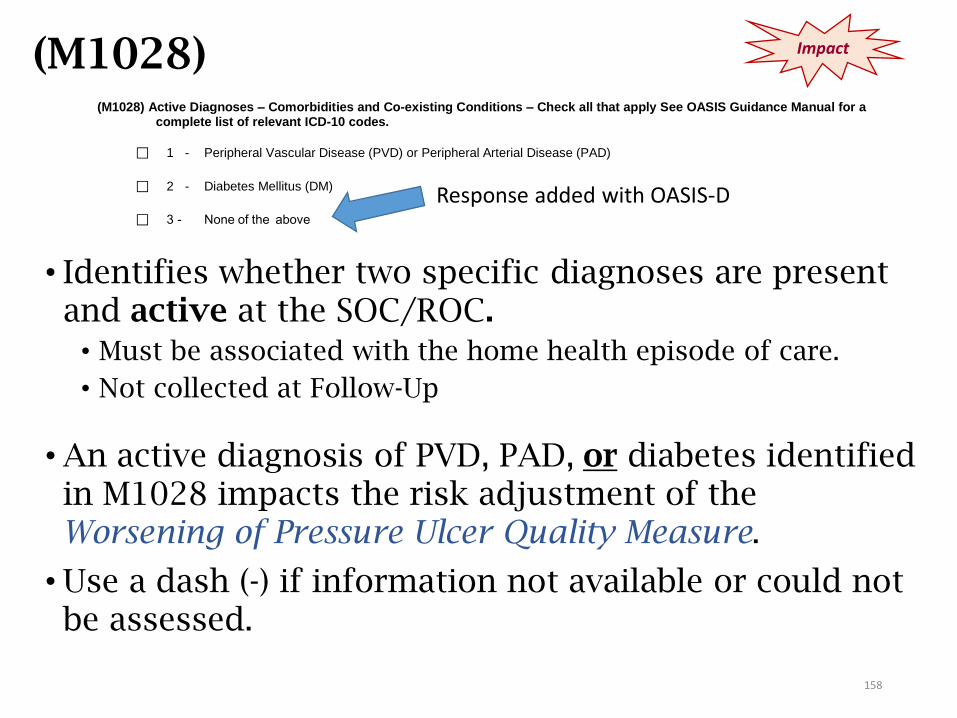
(M1028)
• Identifies whether two specific diagnoses are present and active at the SOC/ROC.
• Must be associated with the home health episode of care.
• Not collected at Follow-Up
• An active diagnosis of PVD, PAD, or diabetes identified in M1028 impacts the risk adjustment of the Worsening of Pressure Ulcer Quality Measure.
• Use a dash (-) if information not available or could not be assessed.
Impact
(M1028) Active Diagnoses – Comorbidities and Co-existing Conditions – Check all that apply See OASIS Guidance Manual for a complete list of relevant ICD-10 codes.
⃞ 1 - Peripheral Vascular Disease (PVD) or Peripheral Arterial Disease (PAD)
⃞ 2 - Diabetes Mellitus (DM)
⃞ 3 - None of the above
Response added with OASIS-D
158
(M1028) Active Diagnoses
• Active diagnoses are those diagnoses that have a direct
relationship to the patient’s current functional, cognitive, mood
or behavior status; medical treatments; nurse monitoring; or risk
of death at the time of assessment.
• “Nurse monitoring” includes clinical monitoring by a licensed
nurse (e.g., serial blood pressure evaluations, medication
management).
• DO NOT include diseases or conditions that have been
resolved.
• A diagnosis may not be inferred by association with other
conditions
• For example: Documentation of elevated blood sugar should not
be inferred to mean “diabetes”.
159
(M1028) Guidance and Tips
• Must be specific documentation in the medical record by the physician . . . that the disease or condition is an active diagnosis.
• The physician . . . may specifically indicate that a diagnosis is active.
• Specific documentation areas in the medical record may include, but are not limited to, progress notes, admission history and physical, transfer notes, and the hospital discharge summary.
• The physician . . . may document at the time of assessment that the patient’s condition is inadequately controlled and needs monitoring or adjustment of the medication regimen. (For example: diabetes)
160
Staff Training
• M1028: Capturing Diabetes and PVD/PAD. It is not enough to “just” code the diagnoses – there must be clear reference in the POC for how these active diagnoses impact or are impacted by the POC.
• Crucial that therapy staff get on board with this.
161
M1028: Active Diagnoses (Response 1)
• Select Response 1, if the patient has an active diagnosis of:
• Peripheral Vascular Disease (PVD) where the problem is arterial. Venous diseases are not associated with a risk of pressure ulcers.
• Codes that start with the first 3 characters of I73
• For example: I73.9, Peripheral vascular disease, unspecified
• If physician documents stasis ulcers, chronic venous insufficiency, or stasis dermatitis – assign diagnosis code I87.2, not I73.9.
OR
• Peripheral Arterial Disease (PAD)
• Codes that start with the first 4 characters of: I70.2, 170.3, 170.4, 170.5, 170.6, 170.7, and 170.91 and I70.92
Excludes: I70.90, (Unspecified atherosclerosis)
For example: I70.201, Unspecified atherosclerosis of native arteries of extremities, right leg
162
M1028: Active Diagnoses (Response 2)
• Select Response 2 if the patient has an active diagnosis of Diabetes Mellitus (DM) indicated by any one of the following diagnosis codes that start with:
• E08. – DM d/t underlying conditions
• E09. – Drug or chemical induced DM
• E10. – Type 1 DM
• E11. – Type 2 DM
• E13. – Other specified DM
For example: Diabetic PAD
E11.51 (Type 2 DM with peripheral angiopathy w/o gangrene))
E11.52 (Type 2 DM with peripheral angiopathy and gangrene)
163

(M1028) Examples of Active Diagnoses
Mr. A is prescribed insulin for diabetes mellitus. He requires regular blood glucose monitoring to determine whether blood glucose goals are achieved by the current medication regimen. The physician progress note documents diabetes mellitus.
164
(M1028) Examples of Active Diagnoses
Mr. A is prescribed insulin for diabetes mellitus. He requires regular blood glucose monitoring to determine whether blood glucose goals are achieved by the current medication regimen. The physician progress note documents diabetes mellitus.
• Response 2: Diabetes Mellitus would be checked.
• Rationale: Diabetes mellitus is considered an active diagnosis because the physician progress note documents the diagnosis and because there is ongoing medication management and glucose monitoring.
165
(M1028) Examples of Active Diagnoses
Your patient underwent a below the knee amputation due to gangrene associated with peripheral vascular disease. She requires dressing changes to the stump and monitoring for wound healing. In addition, peripheral pulse monitoring is ordered. The physician’s progress note documents peripheral vascular disease and a left below the knee amputation.
166
(M1028) Examples of Active Diagnoses
Your patient underwent a below the knee amputation due to gangrene associated with peripheral vascular disease. She requires dressing changes to the stump and monitoring for wound healing. In addition, peripheral pulse monitoring is ordered. The physician’s progress note documents peripheral vascular disease and a left below the knee amputation.
• Response 1: Peripheral vascular disease would be checked.
• Rationale: This would be considered an active diagnosis because the physician’s progress note documents the peripheral vascular disease diagnosis, with peripheral pulse monitoring and recent below the knee amputation, with dressing changes and wound status monitoring.
167
Coding Scenario
• The patient has multiple diagnoses that will be addressed in the POC: CHF, A-fib, COPD, anemia, hemiplegia as late effect of CVA, Parkinson’s disease, peripheral venous stasis. The clinician sequences these diagnoses as follows:
• M1021a: Heart failure, unspecified
• M1023b: Atrial fibrillation
• M1023c: COPD, unspecified
• M1023d: Anemia
• M1023e: Right-sided hemiplegia as a late effect of CVA
• M1023f: Parkinson’s disease
• Other pertinent diagnoses: Peripheral vascular disease, unspecified
Can the clinician check Response 1 (PVD) on M1028?
168
Coding Scenario
• The patient has multiple diagnoses that will be addressed in the POC: CHF, A-fib, COPD, anemia, hemiplegia as late effect of CVA, Parkinson’s disease, peripheral venous stasis. The clinician sequences these diagnoses as follows:
• M1021a: Heart failure, unspecified
• M1023b: Atrial fibrillation
• M1023c: COPD, unspecified
• M1023d: Anemia
• M1023e: Right-sided hemiplegia as a late effect of CVA
• M1023f: Parkinson’s disease
• Other pertinent diagnoses: Peripheral vascular disease, unspecified
• Can the clinician check Response 1 (PVD) on M1028?
Yes, if the PVD is addressed on the POC even if it is not listed in the top 6 coding places.
169
Scenario #1
Patient has a SOC assessment done on Monday. The H&P does not indicate a diagnosis of Diabetes, PVD or PAD, and M1028 is left blank. On Thursday the RN is notified that the patient was given a new diagnosis of PAD during her physician visit on Wednesday.
Since this is within the 5-day window, should M1028 be changed?
170
Scenario #1 – Answer
Patient has SOC assessment done on Monday. The H&P
does not indicate a diagnosis of Diabetes, PVD or PAD, and
M1028 is left blank. On Thursday, the RN is notified that
the patient was given a new diagnosis of PAD during her
physician visit on Wednesday.
Since this is within the 5-day window, should M1028 be
changed?
No. Per the Guidance Manual, the OASIS should NOT be
changed, and M1028 would be coded as 3 – None of the
above. The OASIS should reflect what was known and
documented at the time of the assessment.
171
Scenario #2
• Patient is seen for SOC on Monday. The H&P indicates a diagnosis of pre-diabetes. On Wednesday the RN is notified the patient was given the diagnosis of diabetes at her physician appointment Tuesday, and teaching will be needed for insulin use. Should the OASIS be changed?
172
Scenario #2 - Answer
• Patient is seen for SOC on Monday. The H&P indicates a diagnosis of pre-diabetes. On Wednesday the RN is notified the patient was given the diagnosis of diabetes at her physician appointment Tuesday, and teaching will be needed for insulin use. Should the OASIS be changed?
• Per the Q&A 7 (Oct 2016), the OASIS SHOULD be changed, and M1028 would be marked for the Diabetes. The diabetic condition was confirmed at the assessment (the pre-diabetic diagnosis) visit, and clarified within the 5 day assessment period.
173
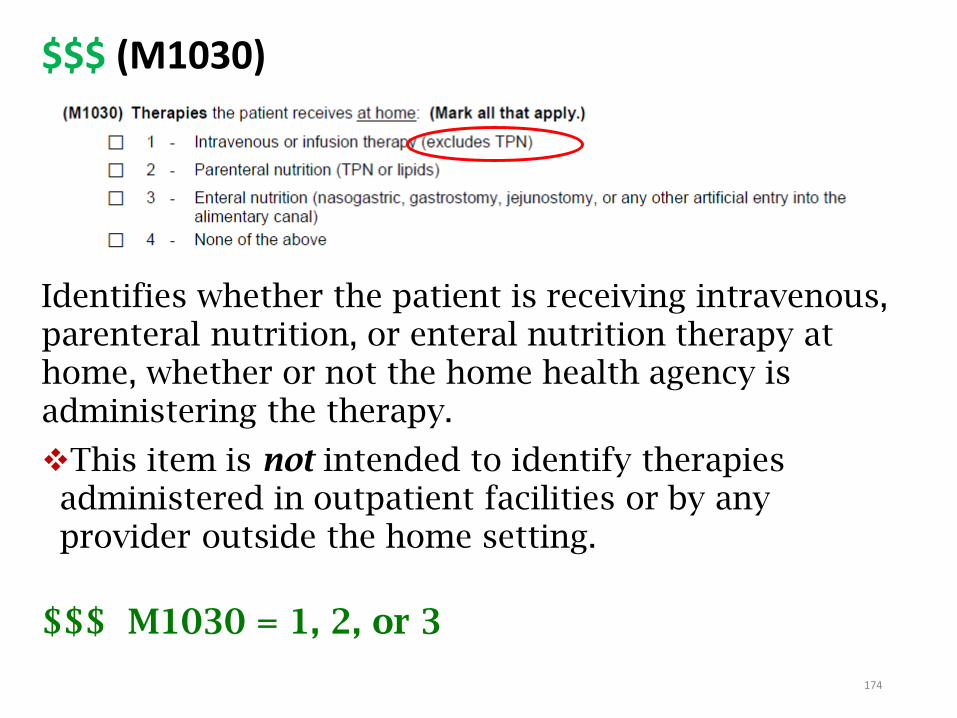
Identifies whether the patient is receiving intravenous, parenteral nutrition, or enteral nutrition therapy at home, whether or not the home health agency is administering the therapy.
This item is not intended to identify therapies administered in outpatient facilities or by any provider outside the home setting.
$$$ M1030 = 1, 2, or 3
174
$$$ (M1030)
174
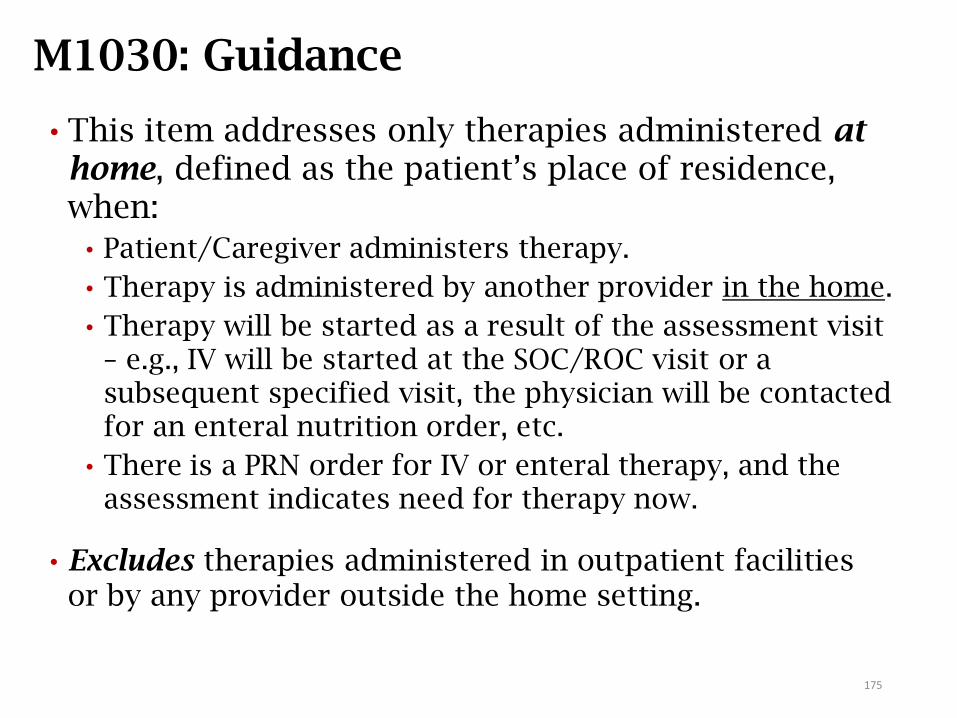
M1030: Guidance
• This item addresses only therapies administered at home, defined as the patient’s place of residence, when:
• Patient/Caregiver administers therapy.
• Therapy is administered by another provider in the home.
• Therapy will be started as a result of the assessment visit – e.g., IV will be started at the SOC/ROC visit or a subsequent specified visit, the physician will be contacted for an enteral nutrition order, etc.
• There is a PRN order for IV or enteral therapy, and the assessment indicates need for therapy now.
• Excludes therapies administered in outpatient facilities or by any provider outside the home setting.
175
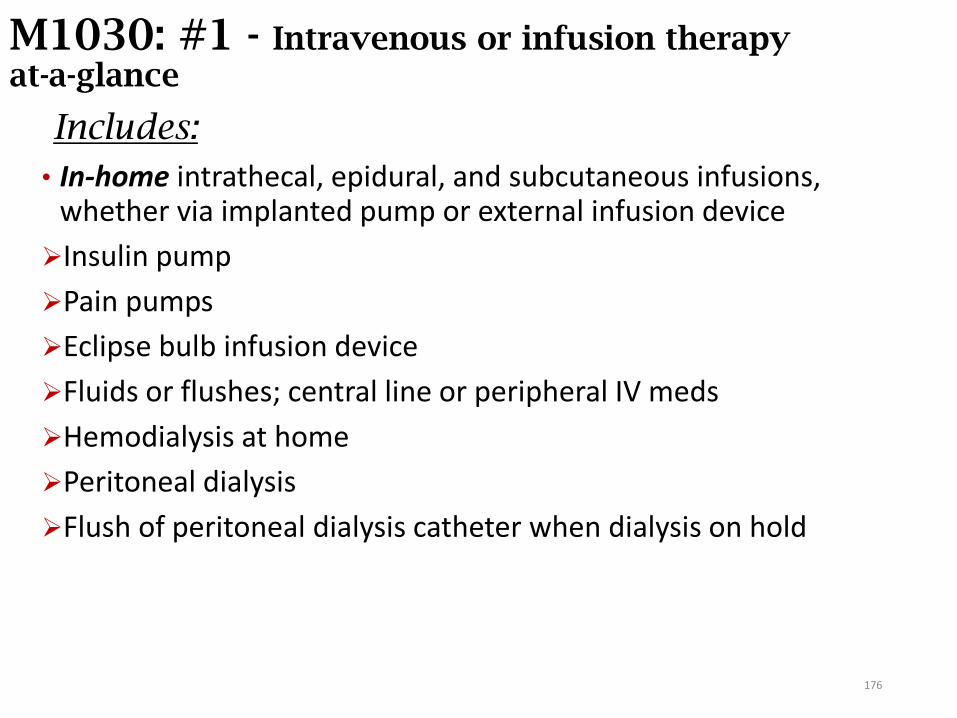
M1030: #1 - Intravenous or infusion therapy at-a-glance
Includes:
• In-home intrathecal, epidural, and subcutaneous infusions, whether via implanted pump or external infusion device
Insulin pump
Pain pumps
Eclipse bulb infusion device
Fluids or flushes; central line or peripheral IV meds
Hemodialysis at home
Peritoneal dialysis
Flush of peritoneal dialysis catheter when dialysis on hold
176
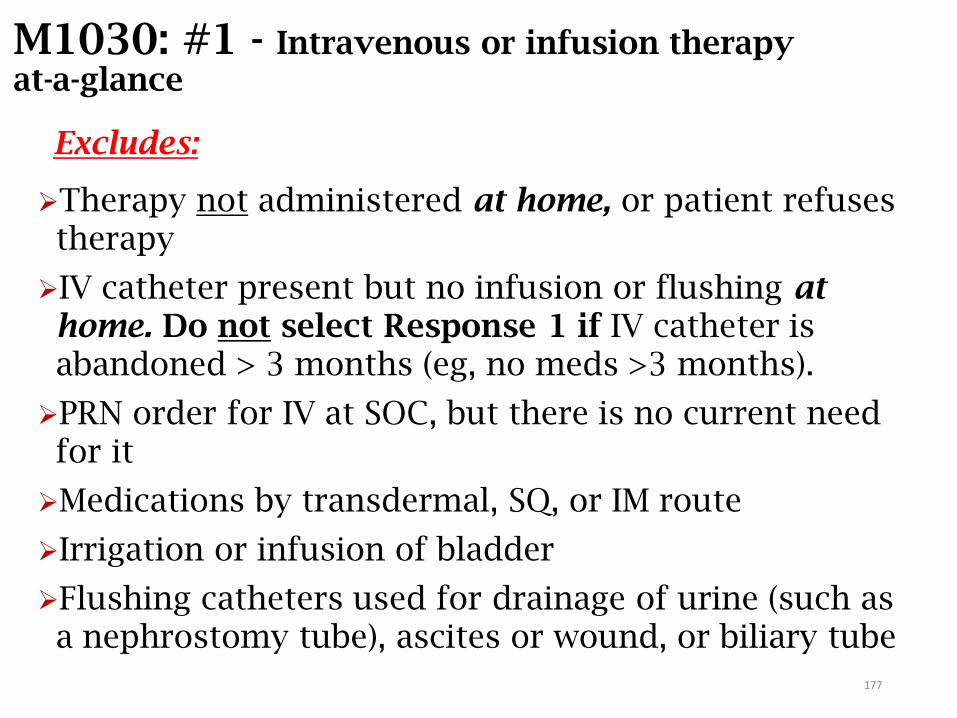
M1030: #1 - Intravenous or infusion therapy at-a-glance
Excludes:
Therapy not administered at home, or patient refuses therapy
IV catheter present but no infusion or flushing at home. Do not select Response 1 if IV catheter is abandoned > 3 months (eg, no meds >3 months).
PRN order for IV at SOC, but there is no current need for it
Medications by transdermal, SQ, or IM route
Irrigation or infusion of bladder
Flushing catheters used for drainage of urine (such as a nephrostomy tube), ascites or wound, or biliary tube
177
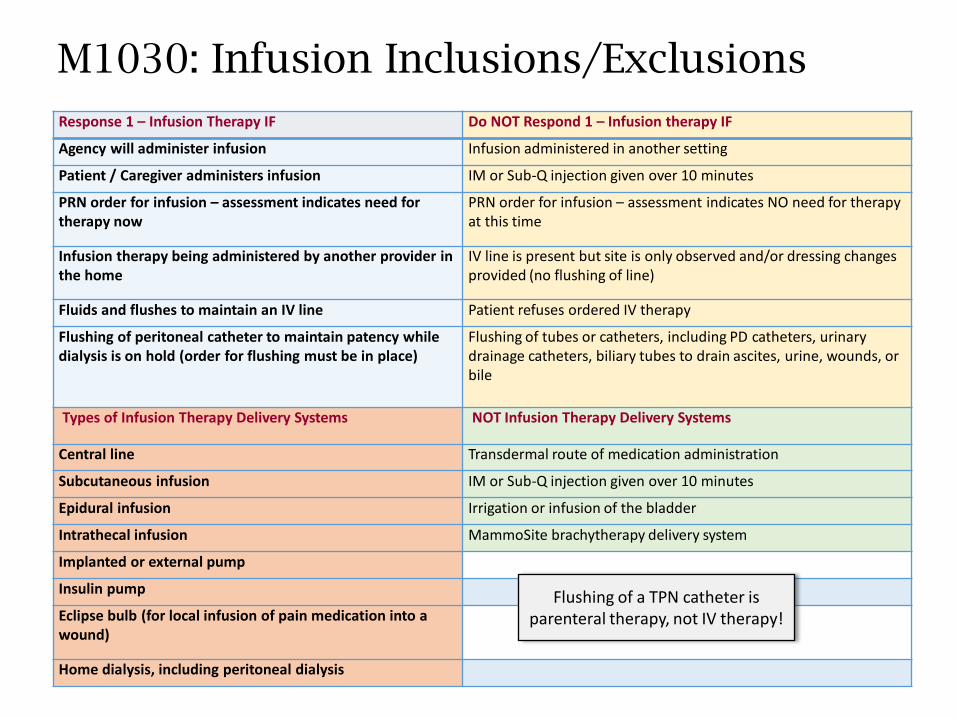
M1030: Infusion Inclusions/Exclusions
Response 1 – Infusion Therapy IF Do NOT Respond 1 – Infusion therapy IF
Agency will administer infusion Infusion administered in another setting
Patient / Caregiver administers infusion IM or Sub-Q injection given over 10 minutes
PRN order for infusion – assessment indicates need for therapy now
PRN order for infusion – assessment indicates NO need for therapy at this time
Infusion therapy being administered by another provider in the home
IV line is present but site is only observed and/or dressing changes provided (no flushing of line)
Fluids and flushes to maintain an IV line Patient refuses ordered IV therapy
Flushing of peritoneal catheter to maintain patency while dialysis is on hold (order for flushing must be in place)
Flushing of tubes or catheters, including PD catheters, urinary drainage catheters, biliary tubes to drain ascites, urine, wounds, or bile
Types of Infusion Therapy Delivery Systems NOT Infusion Therapy Delivery Systems
Central line Transdermal route of medication administration
Subcutaneous infusion IM or Sub-Q injection given over 10 minutes
Epidural infusion Irrigation or infusion of the bladder
Intrathecal infusion MammoSite brachytherapy delivery system
Implanted or external pump
Insulin pump
Eclipse bulb (for local infusion of pain medication into a wound)
Home dialysis, including peritoneal dialysis
Flushing of a TPN catheter is parenteral therapy, not IV therapy!
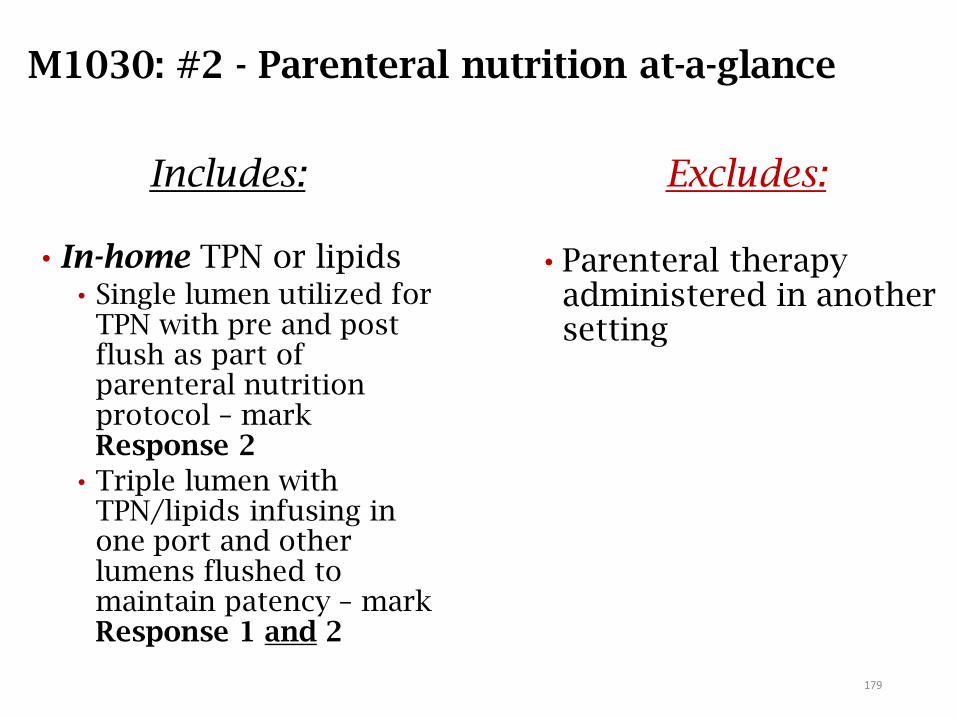
M1030: #2 - Parenteral nutrition at-a-glance
Includes:
• In-home TPN or lipids• Single lumen utilized for
TPN with pre and post flush as part of parenteral nutrition protocol – mark Response 2
• Triple lumen with TPN/lipids infusing in one port and other lumens flushed to maintain patency – mark Response 1 and 2
Excludes:
• Parenteral therapy administered in another setting
179
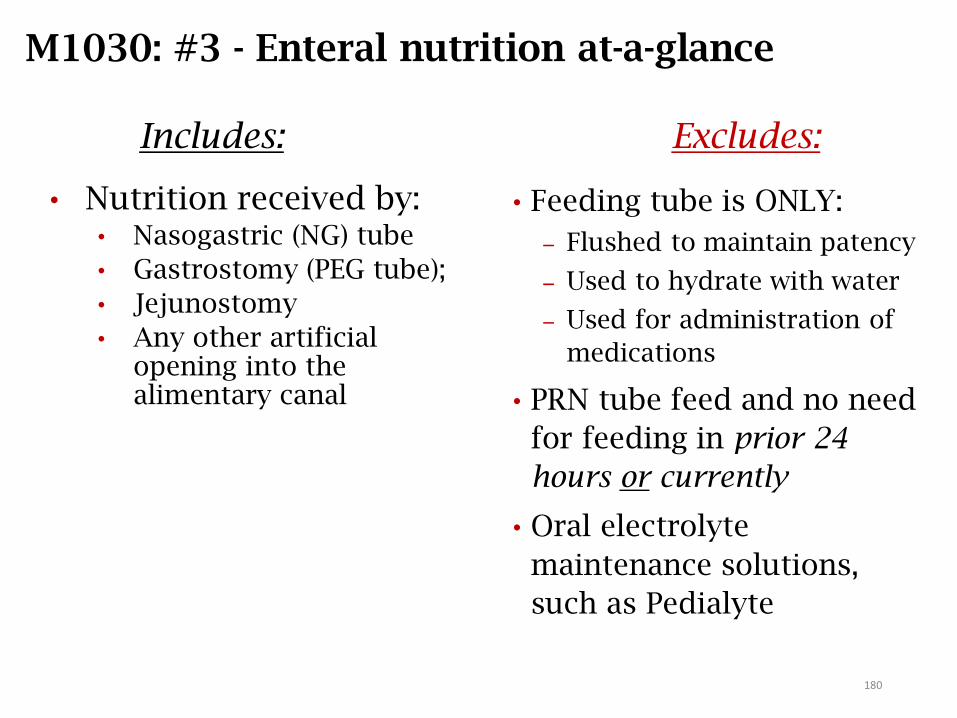
M1030: #3 - Enteral nutrition at-a-glance
Includes:
• Nutrition received by: • Nasogastric (NG) tube
• Gastrostomy (PEG tube);
• Jejunostomy
• Any other artificial opening into the alimentary canal
Excludes:
• Feeding tube is ONLY:
Flushed to maintain patency
Used to hydrate with water
Used for administration of
medications
• PRN tube feed and no need
for feeding in prior 24
hours or currently
• Oral electrolyte
maintenance solutions,
such as Pedialyte
180
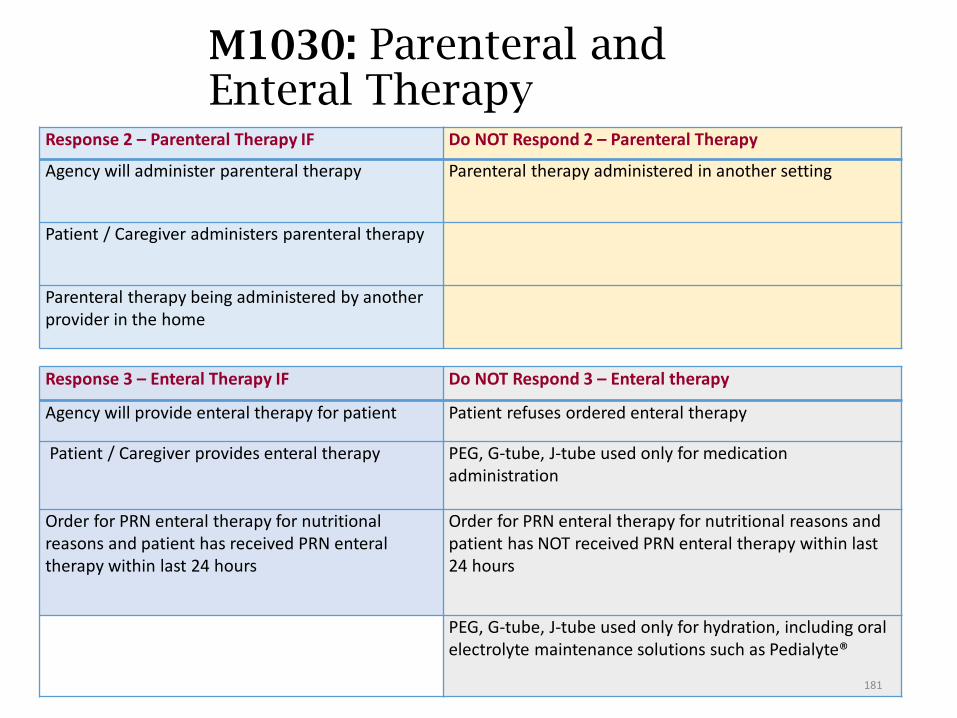
M1030: Parenteral and Enteral Therapy
Response 2 – Parenteral Therapy IF Do NOT Respond 2 – Parenteral Therapy
Agency will administer parenteral therapy Parenteral therapy administered in another setting
Patient / Caregiver administers parenteral therapy
Parenteral therapy being administered by another provider in the home
Response 3 – Enteral Therapy IF Do NOT Respond 3 – Enteral therapy
Agency will provide enteral therapy for patient Patient refuses ordered enteral therapy
Patient / Caregiver provides enteral therapy PEG, G-tube, J-tube used only for medication administration
Order for PRN enteral therapy for nutritional reasons and patient has received PRN enteral therapy within last 24 hours
Order for PRN enteral therapy for nutritional reasons and patient has NOT received PRN enteral therapy within last 24 hours
PEG, G-tube, J-tube used only for hydration, including oral electrolyte maintenance solutions such as Pedialyte®
181
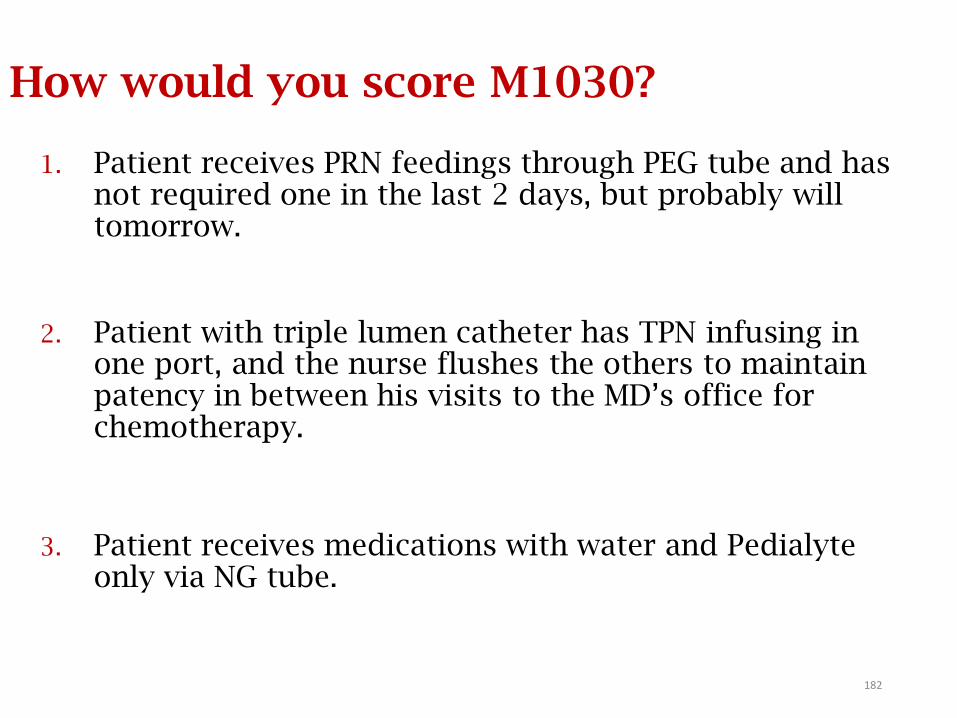
How would you score M1030?
1. Patient receives PRN feedings through PEG tube and has not required one in the last 2 days, but probably will tomorrow.
2. Patient with triple lumen catheter has TPN infusing in one port, and the nurse flushes the others to maintain patency in between his visits to the MD’s office for chemotherapy.
3. Patient receives medications with water and Pedialyte only via NG tube.
182
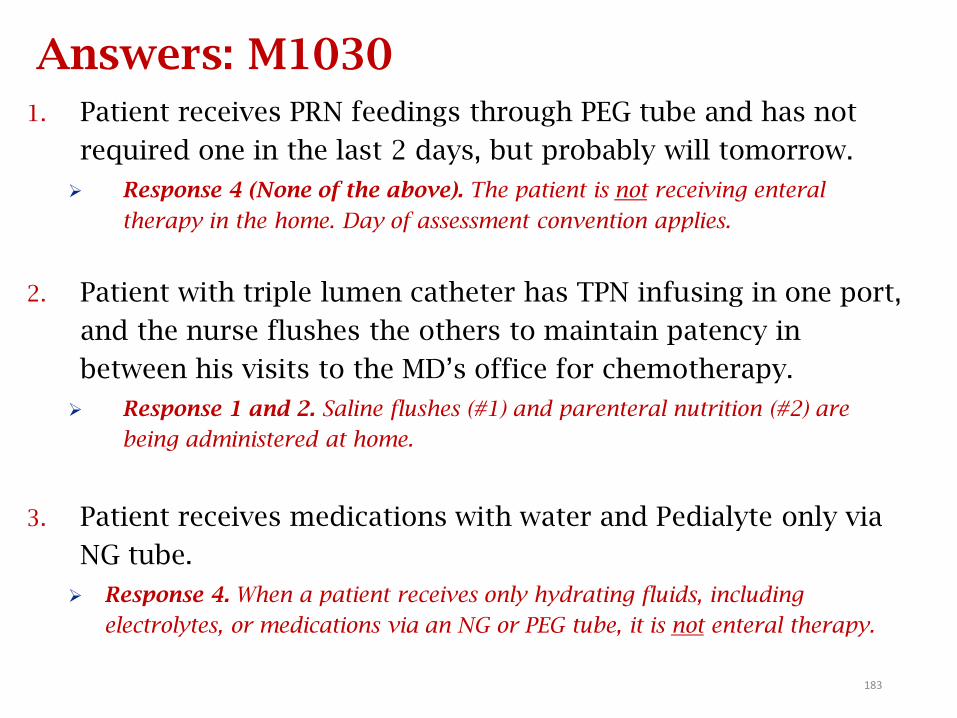
Answers: M1030
1. Patient receives PRN feedings through PEG tube and has not
required one in the last 2 days, but probably will tomorrow.
Response 4 (None of the above). The patient is not receiving enteral
therapy in the home. Day of assessment convention applies.
2. Patient with triple lumen catheter has TPN infusing in one port,
and the nurse flushes the others to maintain patency in
between his visits to the MD’s office for chemotherapy.
Response 1 and 2. Saline flushes (#1) and parenteral nutrition (#2) are
being administered at home.
3. Patient receives medications with water and Pedialyte only via
NG tube.
Response 4. When a patient receives only hydrating fluids, including
electrolytes, or medications via an NG or PEG tube, it is not enteral therapy.
183
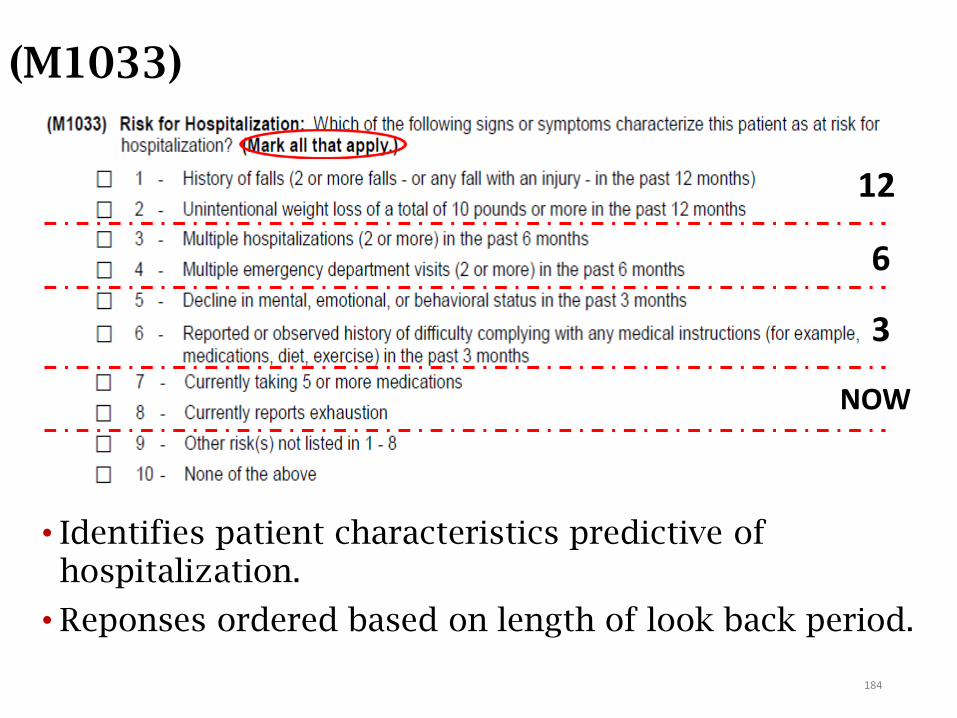
(M1033)
• Identifies patient characteristics predictive of hospitalization.
• Reponses ordered based on length of look back period.
184
12
6
3
NOW
M1033: Responses
• Response 1: includes witnessed and reported (unwitnessed) falls.
• Response 5: decline in mental, emotional, or behavioral status refers to significant changes occurring within the past 3 months that may impact the patient’s ability to remain safely in the home and increase the likelihood of hospitalization.
• Response 7: medications include OTC medications.
• Response 8: refers to physical and/or mental exhaustion at the current time (day of assessment).
• Response 9: Other risk(s), may be selected if the assessing clinician finds characteristics other than those listed in Responses 1-8 that may indicate risk for hospitalization (for example, slower movements during sit to stand and walking).
• Specify other risks in clinical documentation.185
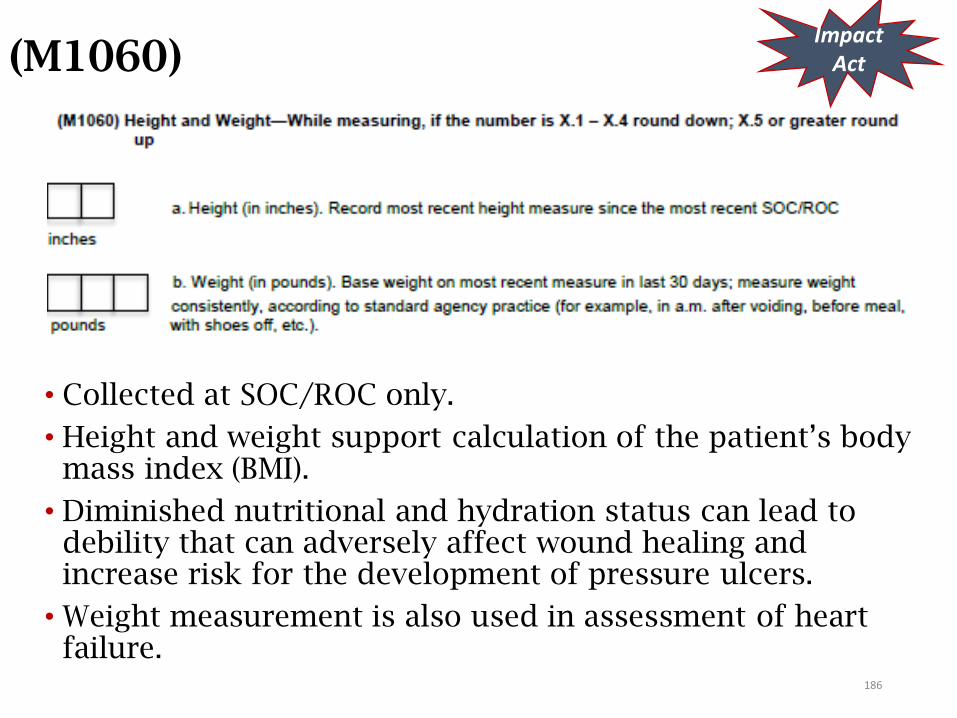
(M1060)
• Collected at SOC/ROC only.
• Height and weight support calculation of the patient’s body mass index (BMI).
• Diminished nutritional and hydration status can lead to debility that can adversely affect wound healing and increase risk for the development of pressure ulcers.
• Weight measurement is also used in assessment of heart failure.
ImpactAct
186
M1060a: Assessing Height
• Measure height in accordance with the agency’s policies and procedures, which should reflect current standards of practice (shoes off, etc.).
• Measure and record height to the nearest whole inch using mathematical rounding (i.e., if height measurement is X.5 inches or greater, round height upward to the nearest whole inch. If height measurement number is X.1 to X.4 inches, round down to the nearest whole inch).
• For example, a height of 62.5 inches would be rounded to 63 inches, and a height of 62.4 inches would be rounded to 62 inches.
• When reporting height for a patient with bilateral lower extremity amputation, measure and record the patient’s current height (i.e., height after bilateral amputation). If the height of the extremities varies, record the greatest measurement.
187
M1060b: Assessing Weight
• Measure weight in accordance with the agency’s policies and procedures, which should reflect current standards of practice (shoes off, etc.).
• Measure and record the patients weight in pounds using mathematical rounding (e.g., if weight is X.5 lbs. or more, round weight upward to the nearest whole pound. If weight is X.1 to X.4 lbs., round down to the nearest whole pound).
• For example, a weight of 152.5 lbs. would be rounded to 153 lbs. and a weight of 152.4 lbs. would be rounded to 152 lbs.
188
M1060 and the Dash (-)
• M1060 Height: A dash (–) value is a valid response for this item, when no information is available and/or it could not be assessed.
• OASIS submission specifications indicate height may only be entered between 50 and 80 inches.
• M1060 Weight: If a patient cannot be weighed, for example, because of extreme pain, immobility, or risk of pathological fractures, enter the dash value (–) and document the rationale on the patient’s medical record.
• OASIS submission specifications indicate weight may only be entered between 065 and 440 pounds.
(OASIS Q&As, Q2; Jan 2019)
189
M1060: Q&A GuidanceCMS Q&A #10, October 2016
Question:
For the new OASIS item M1060, can the agency gather the patient's height and weight by patient/caregiver report? M1060a requests most recent height measure since SOC/ROC, but M1060b allows most recent weight measurement in last 30 days. So does that mean that height must be actually measured after the home health admission, but weight can be entered based on hospital discharge paperwork documented within the last 30 days? Can we ask the patient or caregiver the patient’s height and/or weight?
190
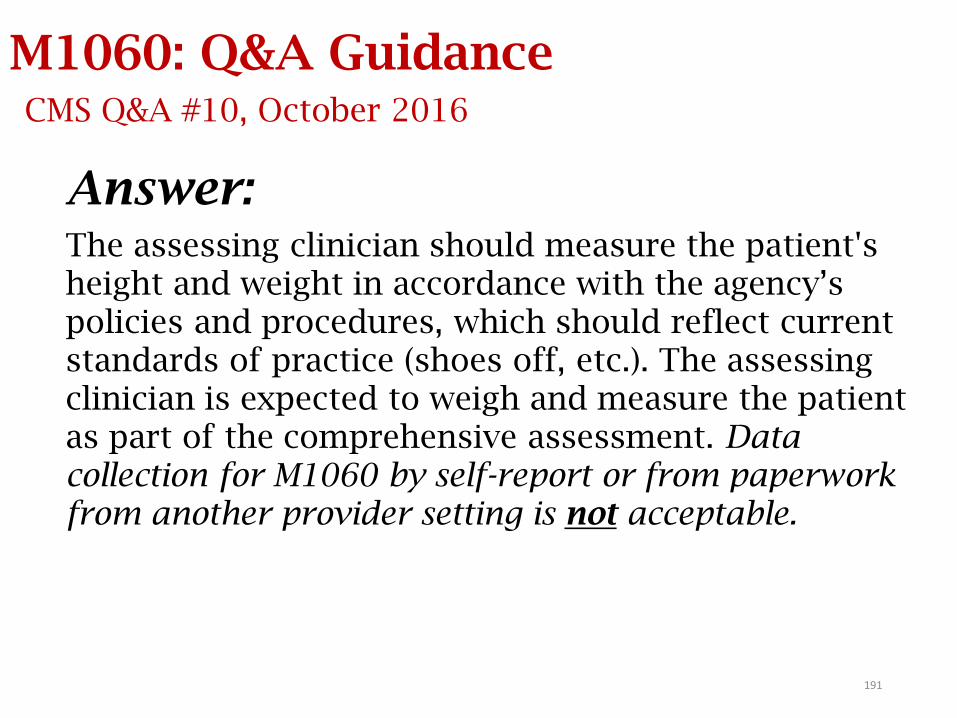
M1060: Q&A GuidanceCMS Q&A #10, October 2016
Answer:The assessing clinician should measure the patient's height and weight in accordance with the agency’s policies and procedures, which should reflect current standards of practice (shoes off, etc.). The assessing clinician is expected to weigh and measure the patient as part of the comprehensive assessment. Data collection for M1060 by self-report or from paperwork from another provider setting is not acceptable.
191
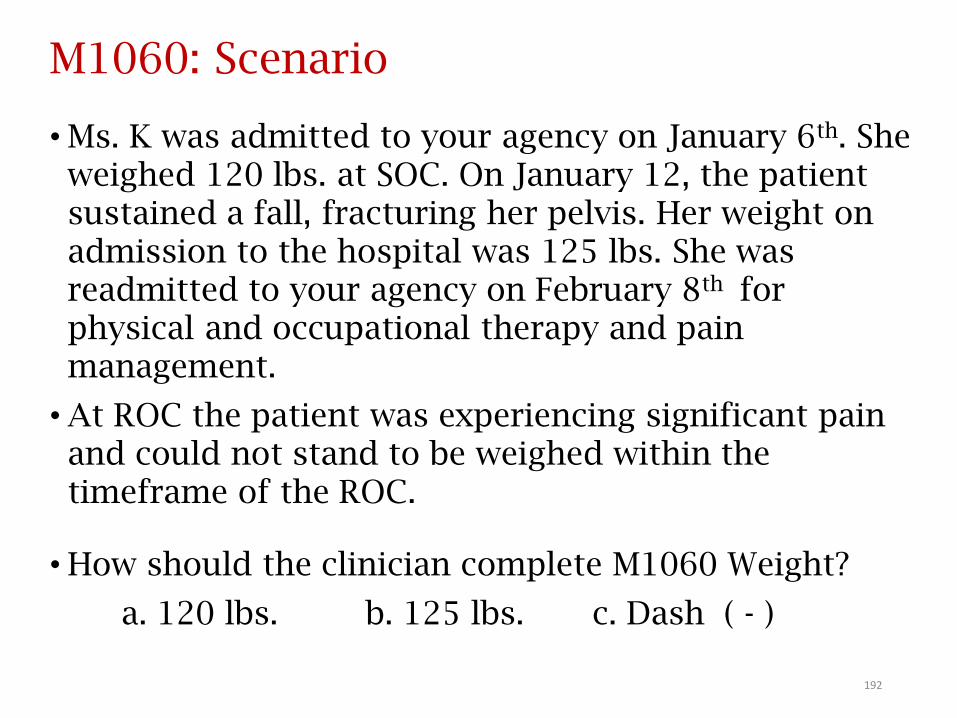
M1060: Scenario
• Ms. K was admitted to your agency on January 6th. She weighed 120 lbs. at SOC. On January 12, the patient sustained a fall, fracturing her pelvis. Her weight on admission to the hospital was 125 lbs. She was readmitted to your agency on February 8th for physical and occupational therapy and pain management.
• At ROC the patient was experiencing significant pain and could not stand to be weighed within the timeframe of the ROC.
• How should the clinician complete M1060 Weight?
a. 120 lbs. b. 125 lbs. c. Dash ( - )
192
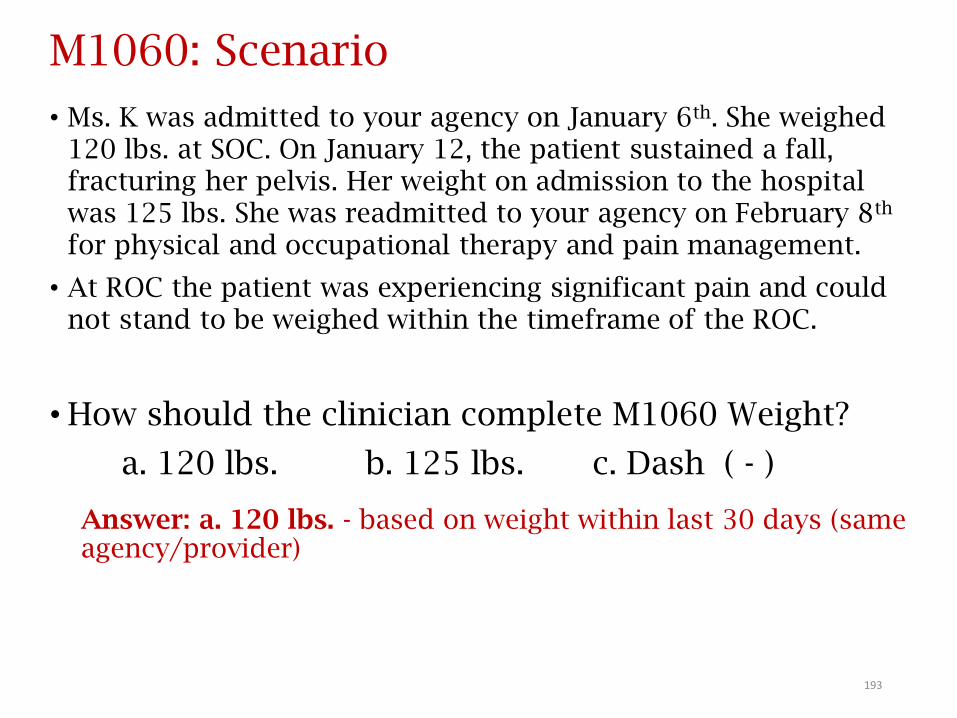
M1060: Scenario
• Ms. K was admitted to your agency on January 6th. She weighed 120 lbs. at SOC. On January 12, the patient sustained a fall, fracturing her pelvis. Her weight on admission to the hospital was 125 lbs. She was readmitted to your agency on February 8th
for physical and occupational therapy and pain management.
• At ROC the patient was experiencing significant pain and could not stand to be weighed within the timeframe of the ROC.
• How should the clinician complete M1060 Weight?
a. 120 lbs. b. 125 lbs. c. Dash ( - )
Answer: a. 120 lbs. - based on weight within last 30 days (same agency/provider)
193
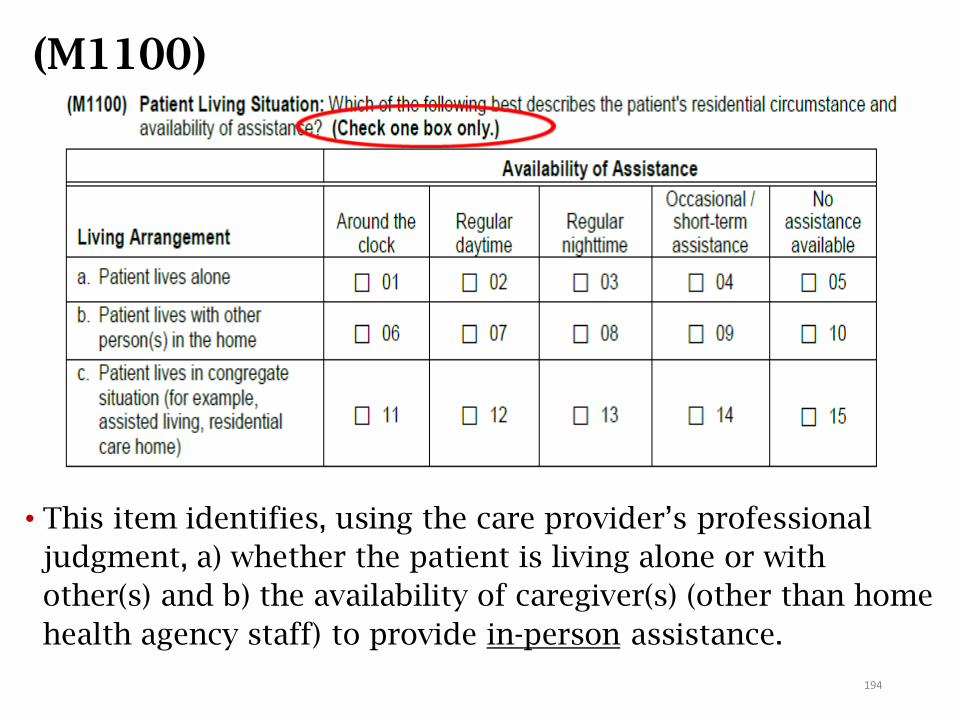
(M1100)
• This item identifies, using the care provider’s professional
judgment, a) whether the patient is living alone or with
other(s) and b) the availability of caregiver(s) (other than home
health agency staff) to provide in-person assistance.
194
M1100: Guidance
First: determine living arrangementa. Does the client live alone
• A client with only live-in paid help is considered to be living alone. If there are temporary caregivers, the client is still living alone
b. Does the client live with others in the home
c. Does the client live in congregate situation (eg. assisted living)
Second: determine availability of assistance How frequently is the caregiver in the home and available
AND capable
Only 1 box will be checked
195
“Usual” Status: For Living Arrangement determination
• Report the patient’s usual status prior to the current illness, exacerbation, or injury, unless there is a new arrangement that is expected to be permanent.
• If situation varies (e.g., temporarily staying with relative or caregiver travels out of town) – choose response that reflects the usual living arrangement.
196
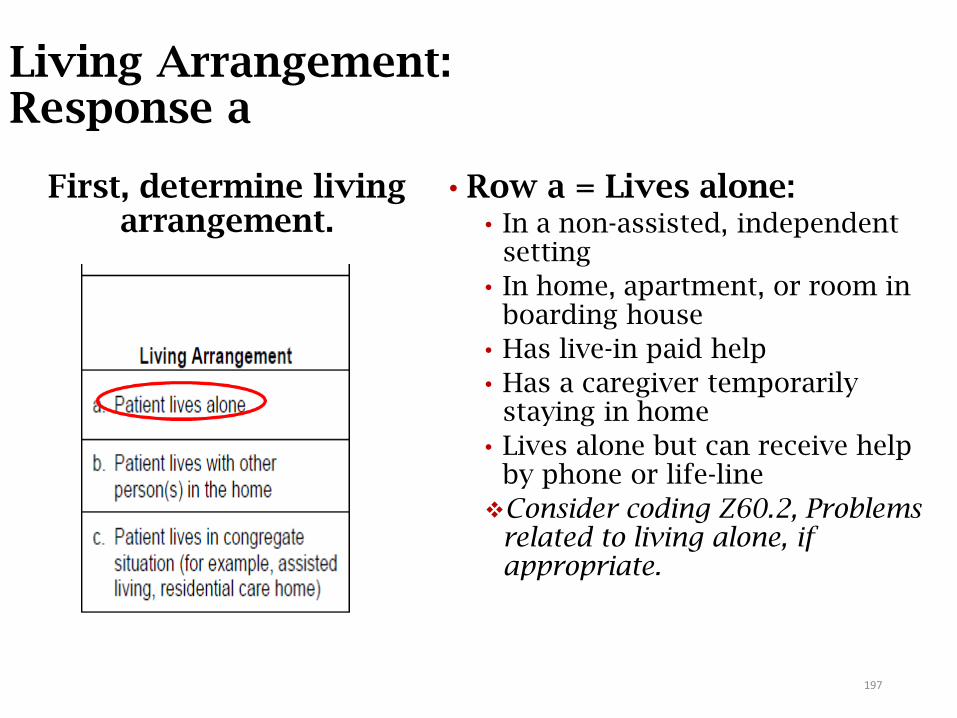
Living Arrangement: Response a
• Row a = Lives alone:• In a non-assisted, independent
setting
• In home, apartment, or room in boarding house
• Has live-in paid help
• Has a caregiver temporarily staying in home
• Lives alone but can receive help by phone or life-line
Consider coding Z60.2, Problems related to living alone, if appropriate.
First, determine living arrangement.
197
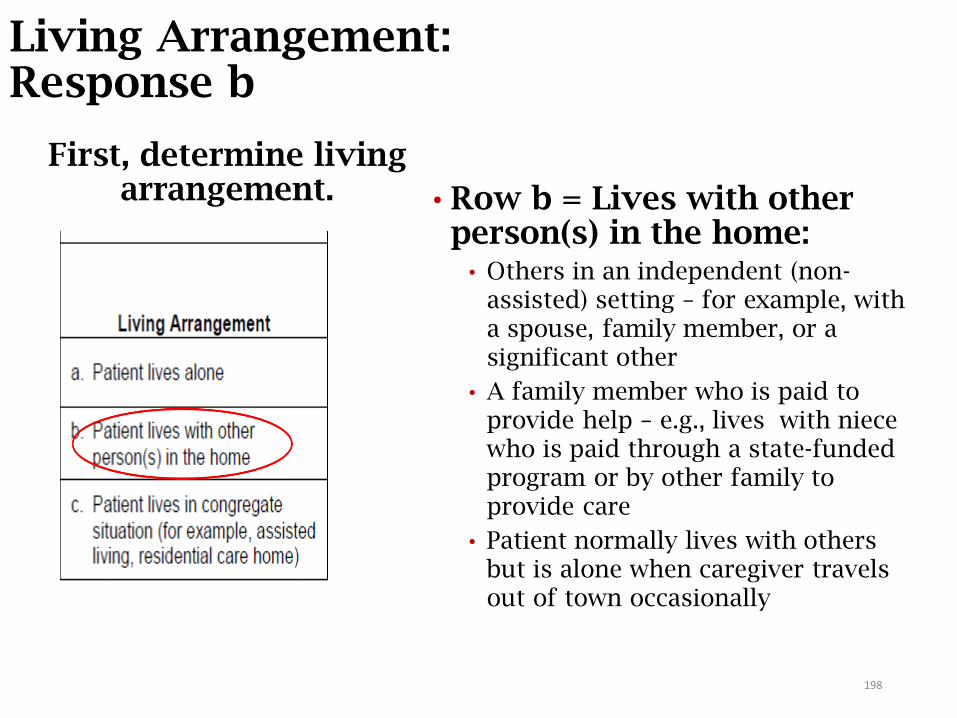
Living Arrangement: Response b
• Row b = Lives with other person(s) in the home:
• Others in an independent (non-assisted) setting – for example, with a spouse, family member, or a significant other
• A family member who is paid to provide help – e.g., lives with niece who is paid through a state-funded program or by other family to provide care
• Patient normally lives with others but is alone when caregiver travels out of town occasionally
First, determine living arrangement.
198

Living Arrangement: Response c
• Row c = Lives in an “assisted living” setting:
• Receives assistance, supervision, and/or oversight provided as part of living arrangement
• Includes patient who lives alone or with a spouse or partner in an apartment or room that is part of an assisted living facility, residential care home, or personal care home
First, determine living arrangement.
199
M1100: Next: Who is a caregiver?
Use your professional judgment to determine if the person the client lives with can/will provide physical assistance to the client if needed. If person living in the home is completely unable or
unwilling to provide any assistance, do not count them as a caregiver
Consider caregivers’ cognitive, physical, and emotional ability to provide assistance
If the client living situation varies (e.g., a caregiver temporarily staying with the client to provide care, a family member living with the client who occasionally travels out of town), select the response that best reflects the usual living arrangements.
200
Availability of Assistance
• Availability of assistance refers to the expected availability and willingness of caregiver(s) for the upcoming care episode.
• In-person assistance in the home of the patient:• Includes any type of in-person assistance including, but not
limited to ADLs and IADLs, including meal prep and medication management, and assistance available via a “call bell” 24 hours a day.
• Excludes phone or emergency assistance (Lifeline or 911).
• The caregiver(s) need not live in the home with the patient, but assistance via telephone is not included.
201
Availability of Assistance (cont.)
• In the large care continuum complexes, a patient is living in a congregate setting when “assistance, supervision and/or oversight are provided as part of the living arrangement” – e.g., housekeeping, meals, and laundry – even if living in an independent cottage or independent apartment.
• To determine the frequency of assistance, the clinician may refer to the ALF service contract or may gather information from the patient or family.
• In a congregate housing situation, if the patient has available in-person assistance in response to a call bell 24 hours a day, the correct answer would be "around the clock.”
202
Availability of Assistance (cont.)
Identify the frequency any in-person assistance is available:
• Around the clock• 24 hours a day (with infrequent exceptions)
• Regular daytime/nighttime
• During daytime/nighttime hours every day/night (with infrequent
exceptions)
• Regular daytime/nighttime is not defined by CMS
• Clinical judgment determines which hours constitute “regular”
daytime and nighttime for patient, based on patient’s specific
activities and routines
• Occasional/short-term assistance• Only for a few hours a day or on an irregular basis
• May be only able to help occasionally
• No assistance available• No one available to provide any in-person assistance
203
M1100: Scenarios
1. Patient underwent hip replacement. She lives alone, and her daughter is staying with her until she regains mobility. Her daughter is in the home most of the time, except for running occasional errands.
2. Patient lives in ALF with husband who requires supervision. She is independent with ADLs/IADLS and assists her husband. A call bell system is available during the day and night to summon help.
204
Answers: M1100
1. Patient underwent hip replacement. She lives alone, and her daughter is staying with her until she regains mobility. Her daughter is in the home most of the time, except for running occasional errands.Response 01 - Refers to patient’s usual living situation
prior to her surgery. She usually lives alone in her home, so row a; she currently has 24/7 help available, therefore [01].
2. Patient lives in ALF with husband who requires supervision. She is independent with ADLs/IADLS and assists her husband. A call bell system is available during the day and night to summon help.Response 11 - Patient lives in a congregate setting with 24-
hour help available – can be by call bell or other means.
205
Sensory StatusM1200 - M1242
206
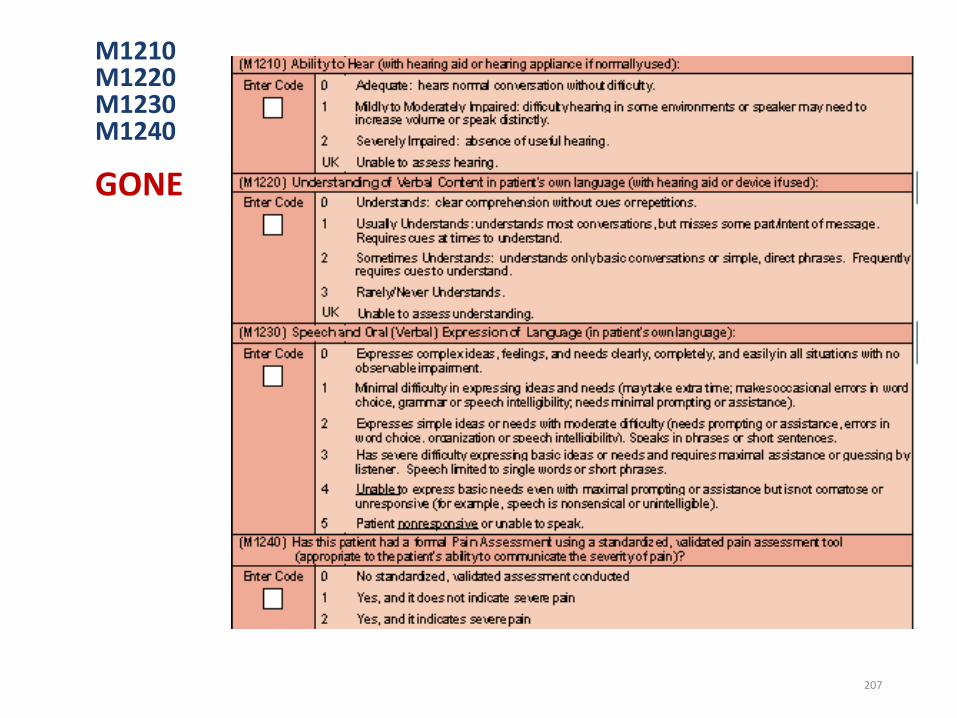
M1210M1220M1230M1240
GONE
207
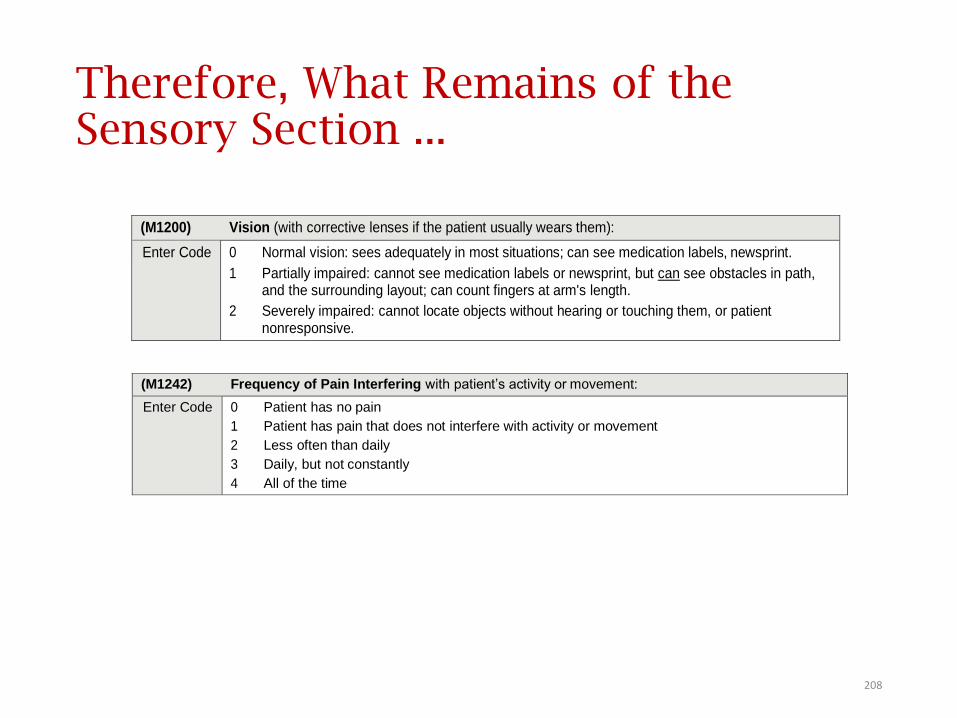
Therefore, What Remains of the Sensory Section ...
(M1200) Vision (with corrective lenses if the patient usually wears them):
Enter Code 0 Normal vision: sees adequately in most situations; can see medication labels, newsprint.
1 Partially impaired: cannot see medication labels or newsprint, but can see obstacles in path, and the surrounding layout; can count fingers at arm's length.
2 Severely impaired: cannot locate objects without hearing or touching them, or patient nonresponsive.
(M1242) Frequency of Pain Interfering with patient’s activity or movement:
Enter Code 0 Patient has no pain
1 Patient has pain that does not interfere with activity or movement
2 Less often than daily
3 Daily, but not constantly
4 All of the time
208
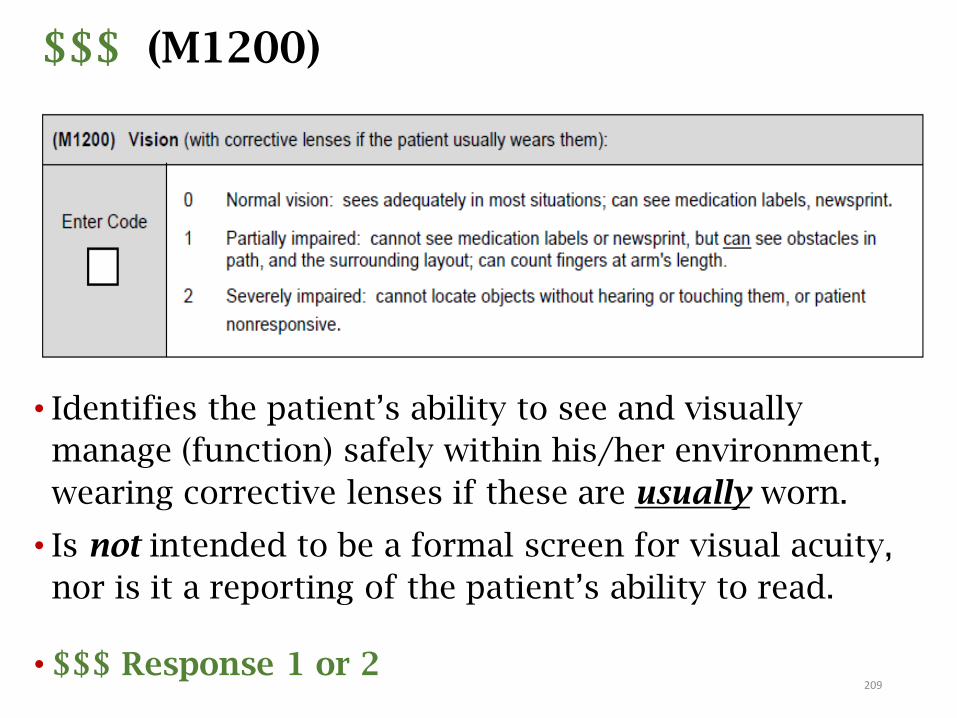
$$$ (M1200)
• Identifies the patient’s ability to see and visually
manage (function) safely within his/her environment,
wearing corrective lenses if these are usually worn.
• Is not intended to be a formal screen for visual acuity,
nor is it a reporting of the patient’s ability to read.
• $$$ Response 1 or 2209
M1200: Guidance
• Consider physical deficits/impairments that limit the patient’s ability to use vision in a functional way, such as limited ROM of neck due to an injury or kyphosis. If a patient is unable to see objects in path, affecting safe functioning in environment, M1200 should be “2 - severely impaired.”
• Clinician may use professional judgment to determine if the patient usually wears corrective lenses to see and visually manage safely within his/her environment. “For a patient with presbyopia who only requires reading glasses, there would be no expectation that they would wear their glasses greater than 50% of the time (hours).
• Eyeglasses (prescription or “grocery store”) and contact lenses are considered corrective lenses.
• Magnifying glasses and electronic magnifiers (“adaptive devices”) are not considered a corrective lens.
210
210
M1200: Guidance (cont.)
• When a patient is cognitively impaired, the clinician will need to observe the patient functioning within their environment and assess their ability to see functionally.
• Does it appear the patient can see adequately in most situations?
• Can they see eating and grooming utensils?
• Do they appear to see the buttons on their shirt/blouse?
• If so, the patient would be reported as a “0 - Normal vision” even though the constraints of the dementia may not allow the patient to communicate whether they can see newsprint or medication labels.
211
M1200: Responses
• Response 1: Based on the patient’s functional vision, not visual acuity. For example:
• Can patient read medication labels or differentiate pills?
• Can patient see obstacles in path?
• Can patient read medical equipment dials, gauges, scales?
• Does patient have glasses but refuse to wear them?
• Does patient need new prescription for glasses?
• Response 2: Severe impairment
• Patient is blind.
• Patient is unable to respond appropriately or is unresponsive.
Note: If selecting Response 1 or 2, ensure that impaired vision is addressed in documentation and on the POC.
212
How would you score M1200?
Patient is clearly visually impaired without his glasses, which he doesn’t wear because they’re too tight and hurt his nose He has a lighted magnifying glass that he uses when he needs to read something. The nurse assessed him using this and his glasses, and he’s able to read his medication labels and newsprint with both, which he’s unable to do without them.
How would you score M1200 (Vision)?
213

Answer: M1200
Patient is clearly visually impaired without his glasses, which he doesn’t wear because they’re too tight and hurt his nose. He has a lighted magnifying glass that he uses when he needs to read something. The nurse assessed him using this and his glasses, and he’s able to read his medication labels and newsprint with both, which he’s unable to do without them.
How would you score M1200 (Vision)?
Response 1 - Partially impaired: Patient doesn’t usually wear his glasses, and a magnifying glass is nota corrective lens.
214
How about this situation?
Patient with severe kyphosis limiting ROM in her neck. She cannot see obstacles in her path when ambulating but can read the newspaper and labels on her medication bottles.
What is the best response to M1200?
215
Answer: M1200
Patient with severe kyphosis limiting ROM in her neck. She cannot see obstacles in her path when ambulating but can read the newspaper and labels on her medication bottles.
What is the best response to M1200?
Response 2 - Severely impaired: Due to the patient’s limited ROM of her neck, she is unable to see objects in her path, which affects her ability to safely function in her environment.
216
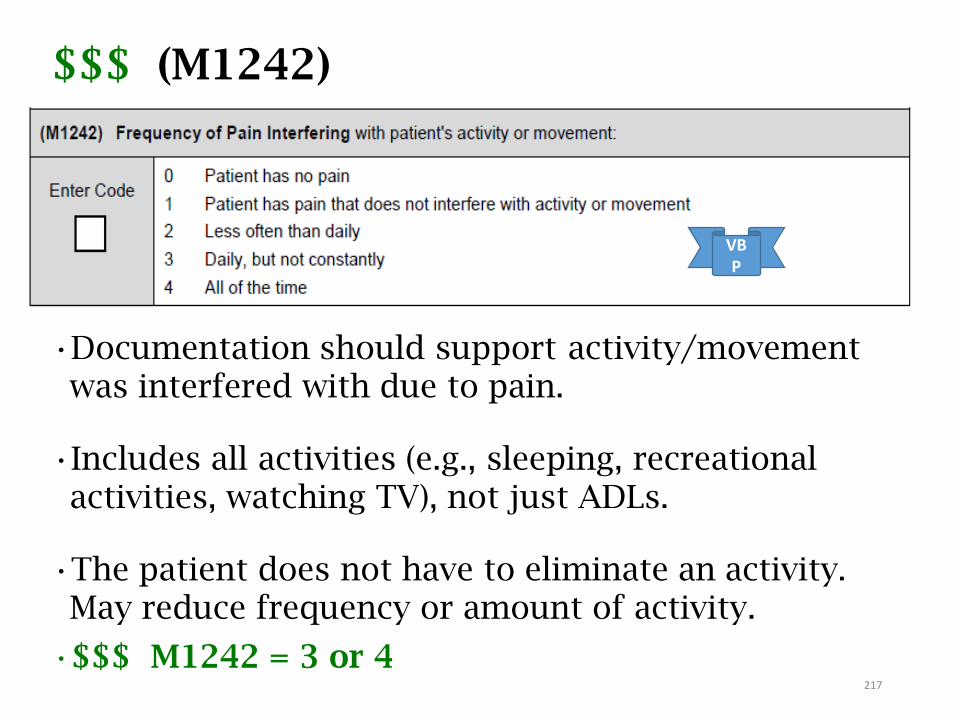
$$$ (M1242)
•Documentation should support activity/movement was interfered with due to pain.
•Includes all activities (e.g., sleeping, recreational activities, watching TV), not just ADLs.
•The patient does not have to eliminate an activity. May reduce frequency or amount of activity.
•$$$ M1242 = 3 or 4
VBP
217

M1242: Guidance
• Pain interferes with activity when the pain results
in the activity being performed less often than
otherwise desired, requires the patient to have
additional assistance in performing the activity, or
causes the activity to take longer to complete.
• Assess patient while moving. Include all activities (e.g.,
sleeping, recreational activities, watching television), not
just ADLs.
218
M1242: Time Frame Clarification
• If patient has stopped an activity to be free of pain, then the patient has pain interfering with activity.
• Time frame for M1242 is the day of the assessment and “recent pertinent past.”
• There must be a “reasonable expectation” the patient would perform activity again if the pain could be eliminated [or managed].
• Use clinical judgment – i.e., patient has not jogged in last 3 years since he has pain in his knee due to arthritis when he runs is not the recent pertinent past.
219
What does “All the Time” mean in M1242?
• Response “4 - All the time” means constantly throughout the day and night with little or no relief.
• If patient has stopped an activity, Response 4 is appropriate, if the frequency of the activity that was stopped in order to avoid pain collectively represent all the hours of the day/night.
• Pain must wake the patient frequently at night.
• Clinical judgment based on observation and patient interview must be used to determine if pain is interfering “all the time”.
(CMS Q&A #73.3, 10/16)
220
How would you score M1242?
•The patient has pain in her left arm following a mastectomy. She refuses to take pain medication because she says she cannot afford the medication. Her daughter helps her dress and comb her hair because the pain in her arm prevents her from doing so. When she takes her medication she gets relief from her pain.
•Patient who has daily arthritic pain, but does all her usual activities?
•Patient no longer cooks meals in her kitchen because her legs hurt when she stands on her feet.
221
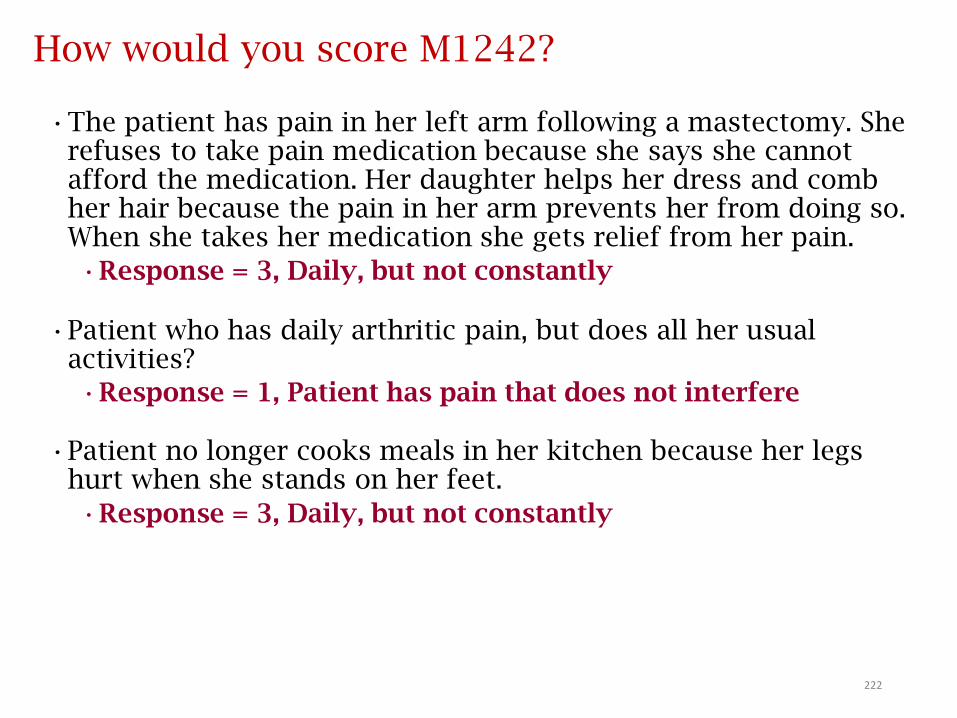
How would you score M1242?
•The patient has pain in her left arm following a mastectomy. She refuses to take pain medication because she says she cannot afford the medication. Her daughter helps her dress and comb her hair because the pain in her arm prevents her from doing so. When she takes her medication she gets relief from her pain.
•Response = 3, Daily, but not constantly
•Patient who has daily arthritic pain, but does all her usual activities?
•Response = 1, Patient has pain that does not interfere
•Patient no longer cooks meals in her kitchen because her legs hurt when she stands on her feet.
•Response = 3, Daily, but not constantly
222
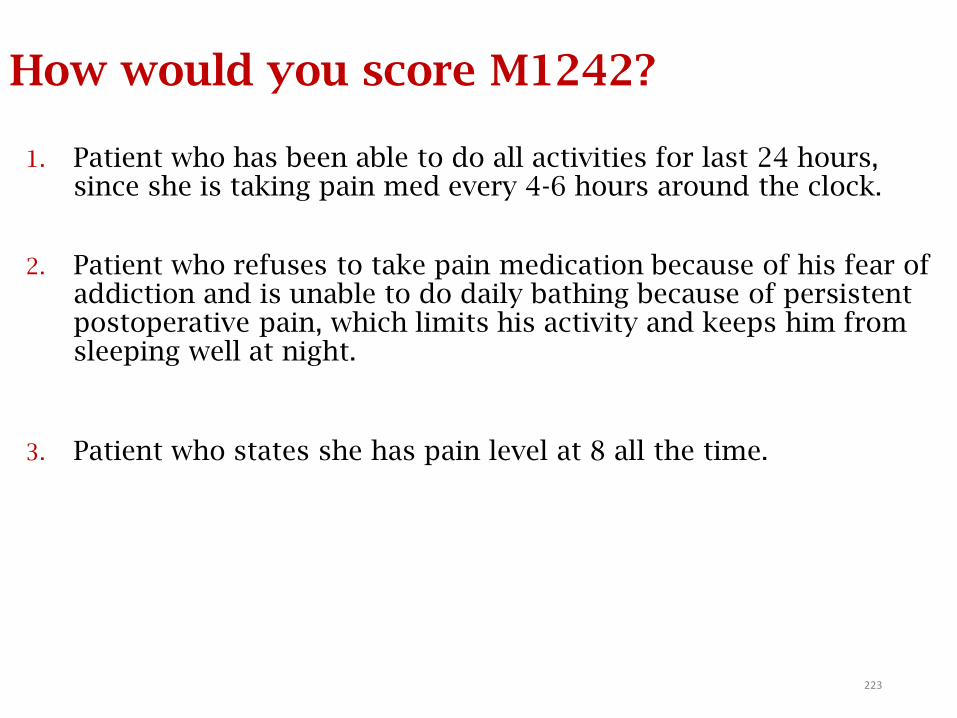
How would you score M1242?
1. Patient who has been able to do all activities for last 24 hours, since she is taking pain med every 4-6 hours around the clock.
2. Patient who refuses to take pain medication because of his fear of addiction and is unable to do daily bathing because of persistent postoperative pain, which limits his activity and keeps him from sleeping well at night.
3. Patient who states she has pain level at 8 all the time.
223
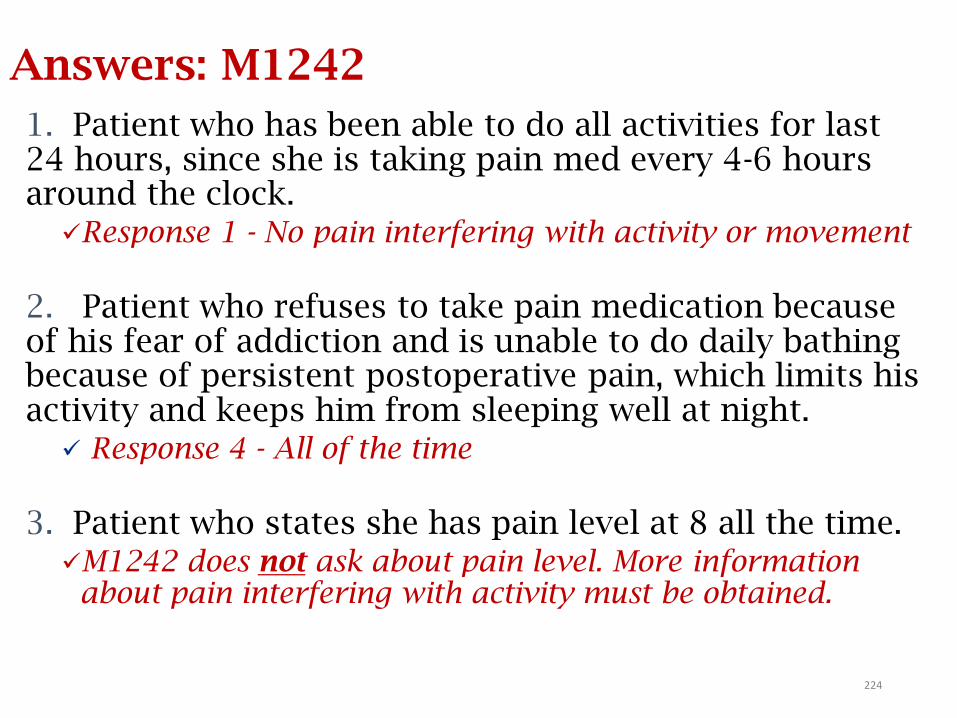
Answers: M1242
1. Patient who has been able to do all activities for last 24 hours, since she is taking pain med every 4-6 hours around the clock.Response 1 - No pain interfering with activity or movement
2. Patient who refuses to take pain medication because of his fear of addiction and is unable to do daily bathing because of persistent postoperative pain, which limits his activity and keeps him from sleeping well at night. Response 4 - All of the time
3. Patient who states she has pain level at 8 all the time. M1242 does not ask about pain level. More information
about pain interfering with activity must be obtained.
224
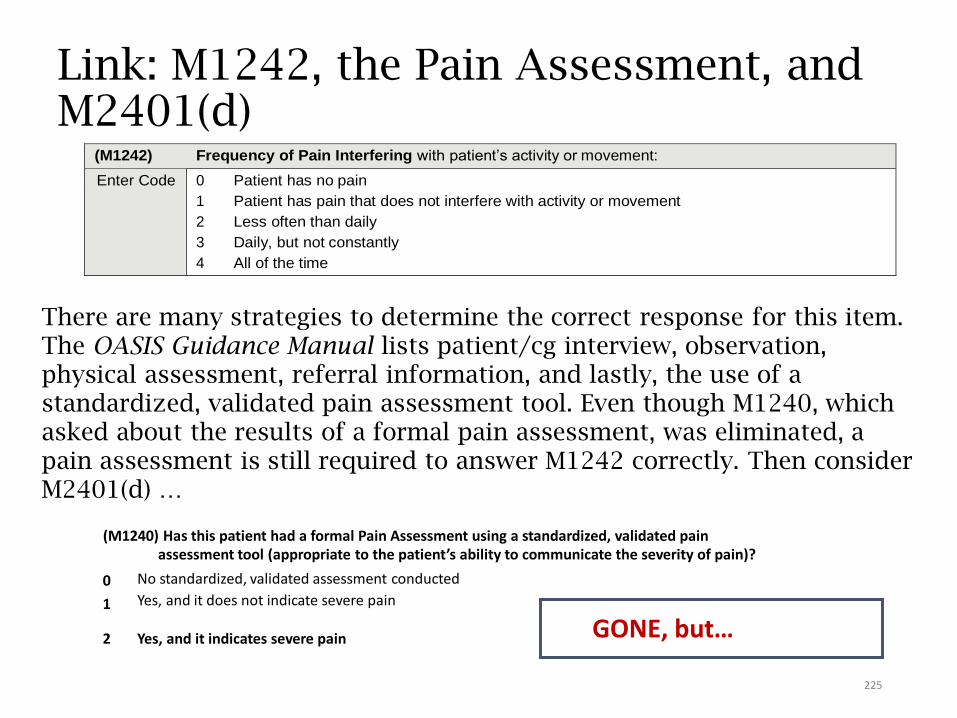
Link: M1242, the Pain Assessment, and M2401(d)
There are many strategies to determine the correct response for this item. The OASIS Guidance Manual lists patient/cg interview, observation, physical assessment, referral information, and lastly, the use of a standardized, validated pain assessment tool. Even though M1240, which asked about the results of a formal pain assessment, was eliminated, a pain assessment is still required to answer M1242 correctly. Then consider M2401(d) …
(M1240) Has this patient had a formal Pain Assessment using a standardized, validated pain assessment tool (appropriate to the patient’s ability to communicate the severity of pain)?
0
1
No standardized, validated assessment conducted
Yes, and it does not indicate severe pain
2 Yes, and it indicates severe pain GONE, but…
(M1242) Frequency of Pain Interfering with patient’s activity or movement:
Enter Code 0 Patient has no pain
1 Patient has pain that does not interfere with activity or movement
2 Less often than daily
3 Daily, but not constantly
4 All of the time
225
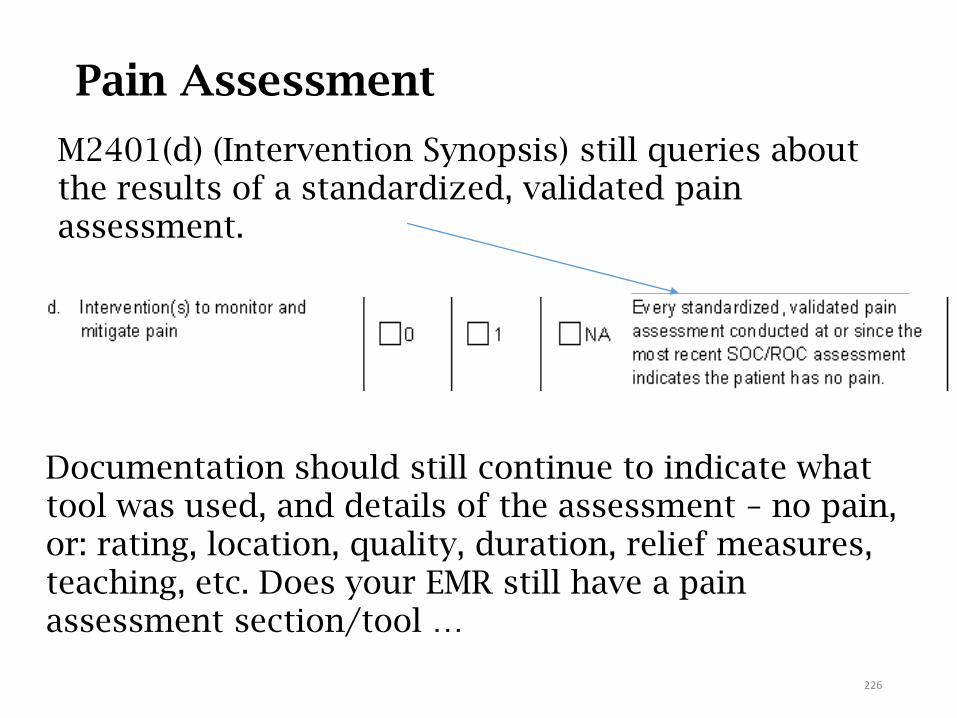
Pain Assessment
M2401(d) (Intervention Synopsis) still queries about the results of a standardized, validated pain assessment.
Documentation should still continue to indicate what tool was used, and details of the assessment – no pain, or: rating, location, quality, duration, relief measures, teaching, etc. Does your EMR still have a pain assessment section/tool …
226
See WOCN Guidance on OASIS-D Integumentary Items
Integumentary Status
M1306 – M1342
227
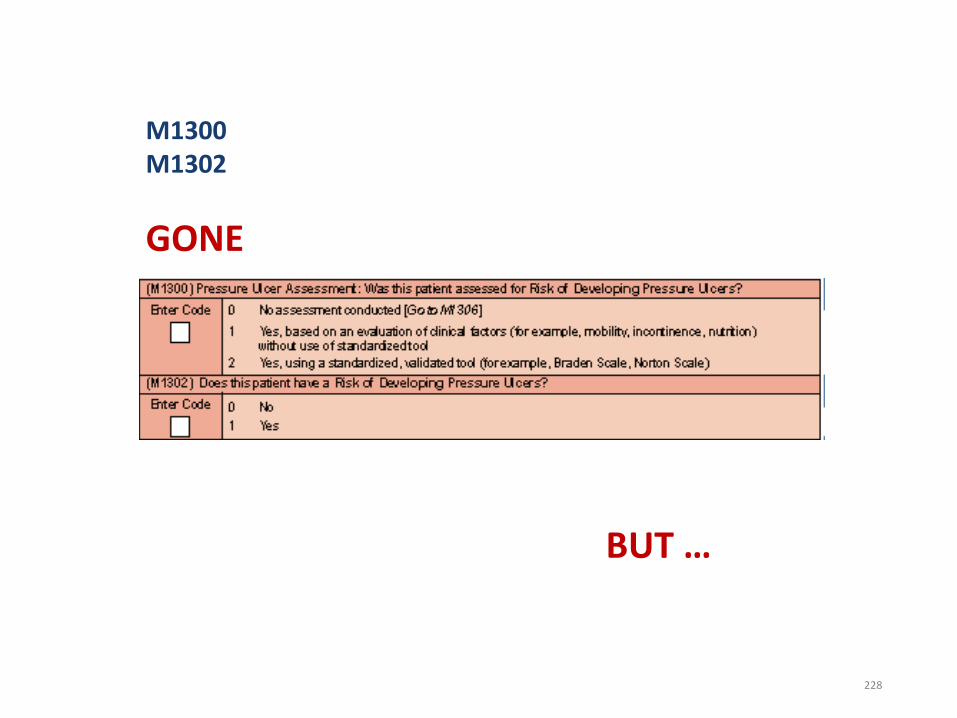
BUT …
M1300M1302
GONE
228
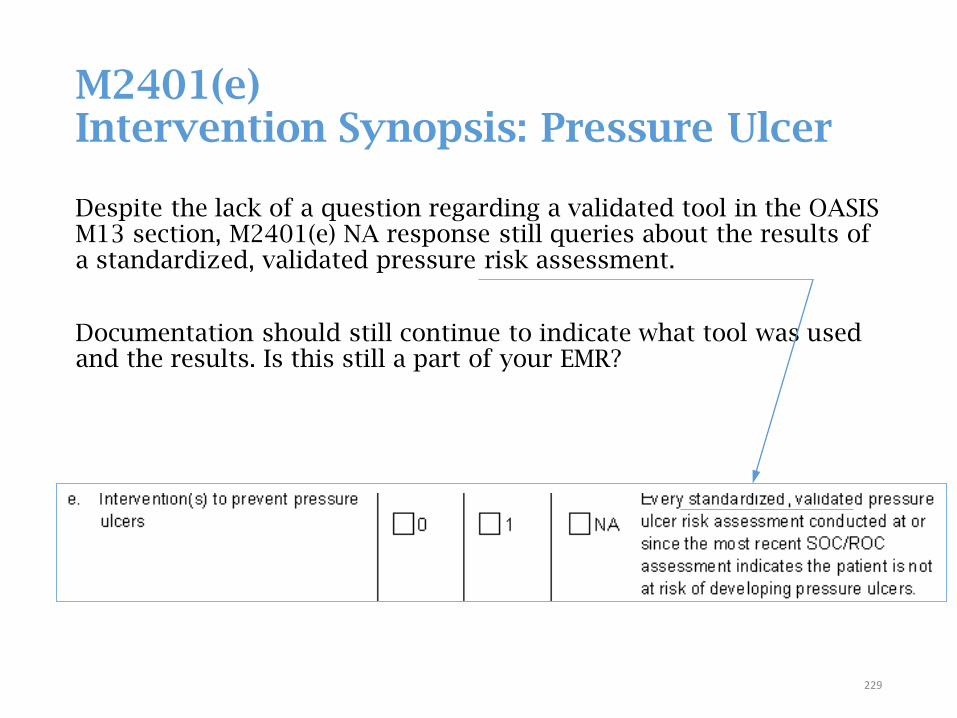
M2401(e) Intervention Synopsis: Pressure Ulcer
Despite the lack of a question regarding a validated tool in the OASIS M13 section, M2401(e) NA response still queries about the results of a standardized, validated pressure risk assessment.
Documentation should still continue to indicate what tool was used and the results. Is this still a part of your EMR?
229
Language Update
• Stage 1 pressure ulcers are to be designated as injuries, not ulcers per the OASIS-D Guidance Manual errata published July 30, 2018
• This appeared as a language change in items M1306, M1307, M1311, M1324
Old language: “Terminology referring to ‘healed’ vs. ‘unhealed’ ulcers can refer to whether the ulcer is ‘closed’ vs. ‘open’.”
New language: “Terminology referring to ‘healed’ vs. ‘unhealed’ ulcers/injuries can refer to whether the ulcer/injury is ‘closed’ vs. ‘open’.”
Summary: INJURY ↔ skin is intactULCER ↔ skin is broken
NEVER REVERSE STAGE230
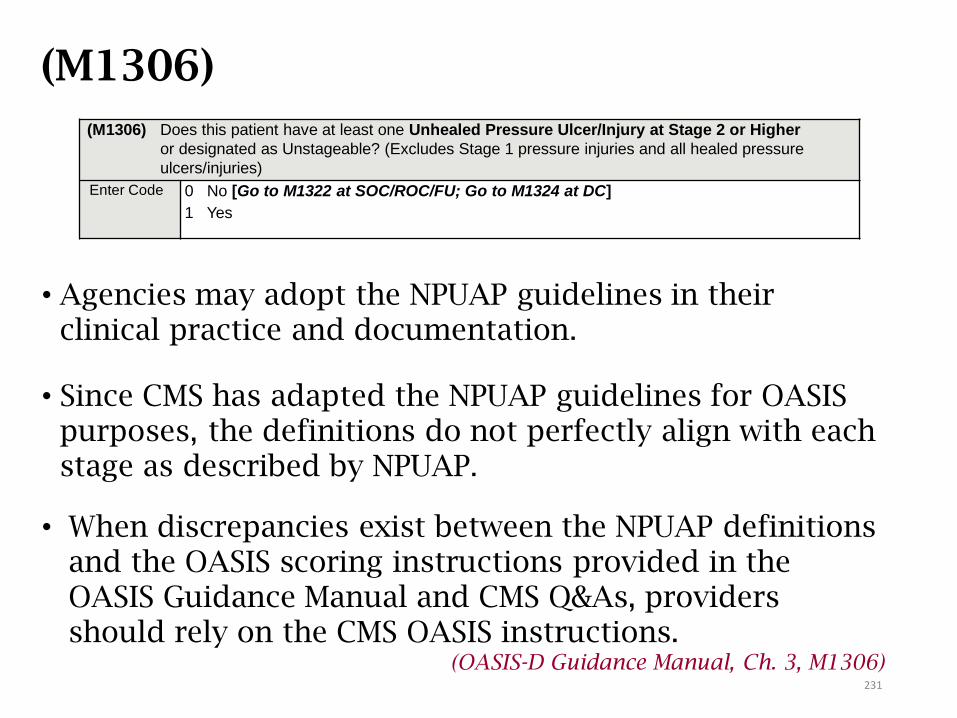
(M1306)
• Agencies may adopt the NPUAP guidelines in their clinical practice and documentation.
• Since CMS has adapted the NPUAP guidelines for OASIS purposes, the definitions do not perfectly align with each stage as described by NPUAP.
• When discrepancies exist between the NPUAP definitions and the OASIS scoring instructions provided in the OASIS Guidance Manual and CMS Q&As, providers should rely on the CMS OASIS instructions.
(OASIS-D Guidance Manual, Ch. 3, M1306)
(M1306) Does this patient have at least one Unhealed Pressure Ulcer/Injury at Stage 2 or Higher
or designated as Unstageable? (Excludes Stage 1 pressure injuries and all healed pressure
ulcers/injuries)
Enter Code 0 No [Go to M1322 at SOC/ROC/FU; Go to M1324 at DC]
1 Yes
231
(M1306) Response-Specific Guidance
• Pressure ulcers are defined as localized injury to the
skin and/or underlying tissue usually over a bony
prominence, as a result of pressure, or pressure in
combination with shear and/or friction.
• If pressure is not the primary cause of the lesion, do not
report the wound as a pressure ulcer. For example:
Blister of the heel due to rubbing of a new shoe on the
heel.
• Stage 2 (partial thickness) pressure ulcers heal through
the process of regeneration of epidermis across the
wound surface, known as “re-epithelialization”.
• Stage 2 ulcers do not granulate and are reported as unhealed until
they have epithelialized.
• Newly epithelialized Stage 2 ulcers are not reported or counted.232
(M1306) Response-Specific Guidance
• Pressure ulcers that are not considered healed:• Unstageable pressure ulcers
• Suspected Deep Tissue Injuries (DTIs)
• “Known” (documented in record) pressure ulcers covered with a nonremovable dressing.
• Known pressure ulcers where eschar or slough is obscuring visualization of Stage 4 structure.
• Stage 3 and 4 (full thickness) pressure ulcers heal through a process of granulation (filling of the wound with connective/scar tissue), contraction (wound margins contract and pull together), and re-epithelialization (covers with epithelial tissue from within wound bed and/or from wound margins).
233
(M1306) Response-Specific Guidance
• Once a stage 3 or 4 pressure ulcer has fully granulated and the wound surface is completely covered with new epithelial tissue, the wound is considered closed, and will continue to remodel and increase in tensile strength.
• For the purposes of scoring the OASIS, the wound is considered healed at this point, and should no longer be reported as an unhealed pressure ulcer.
• Tensile strength of the skin overlying a closed full thickness pressure ulcer is only 80% of normal skin tensile strength. Agencies should pay careful attention that preventative measures are put into place that will mitigate the re-opening of a closed ulcer. Consider the impact on M2401e.
234
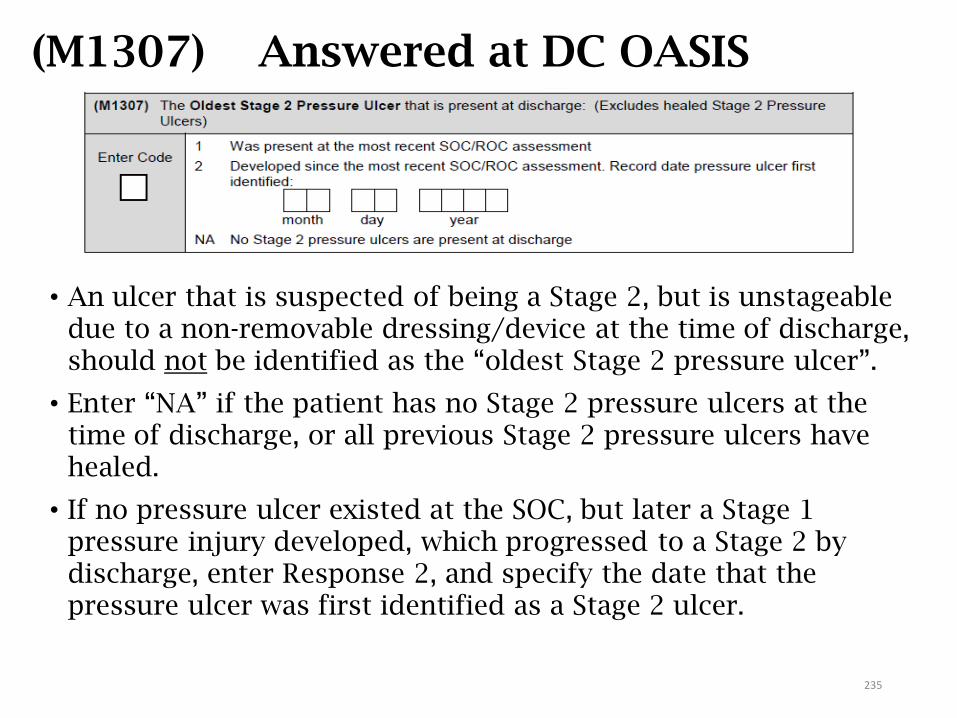
(M1307) Answered at DC OASIS
• An ulcer that is suspected of being a Stage 2, but is unstageable due to a non-removable dressing/device at the time of discharge, should not be identified as the “oldest Stage 2 pressure ulcer”.
• Enter “NA” if the patient has no Stage 2 pressure ulcers at the time of discharge, or all previous Stage 2 pressure ulcers have healed.
• If no pressure ulcer existed at the SOC, but later a Stage 1 pressure injury developed, which progressed to a Stage 2 by discharge, enter Response 2, and specify the date that the pressure ulcer was first identified as a Stage 2 ulcer.
235
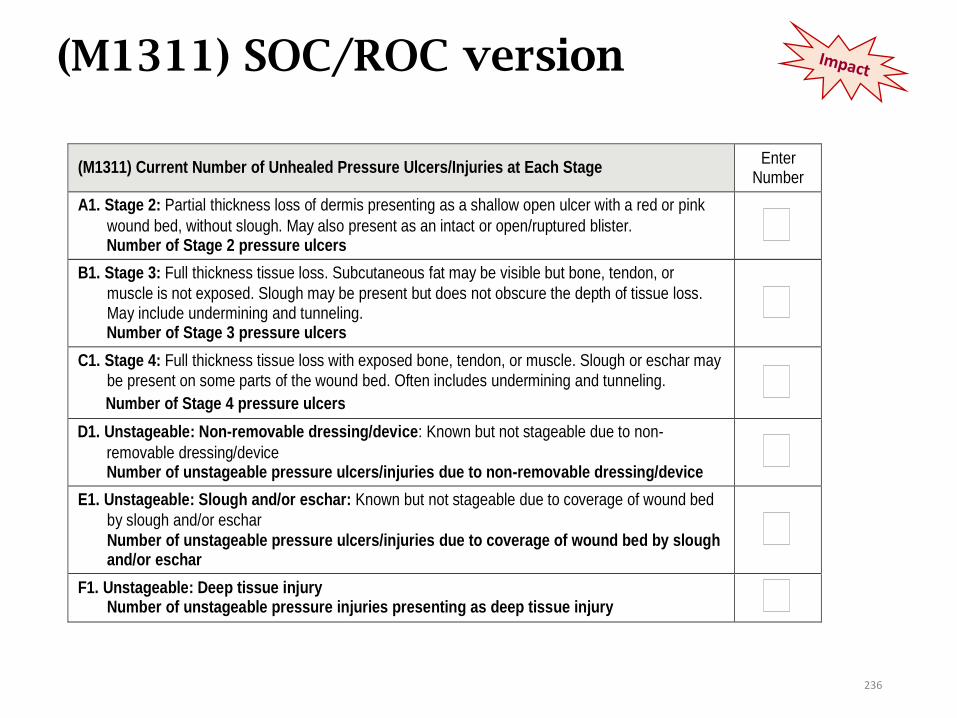
(M1311) SOC/ROC version
(M1311) Current Number of Unhealed Pressure Ulcers/Injuries at Each Stage Enter
Number
A1. Stage 2: Partial thickness loss of dermis presenting as a shallow open ulcer with a red or pink
wound bed, without slough. May also present as an intact or open/ruptured blister. Number of Stage 2 pressure ulcers
B1. Stage 3: Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon, or
muscle is not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining and tunneling. Number of Stage 3 pressure ulcers
C1. Stage 4: Full thickness tissue loss with exposed bone, tendon, or muscle. Slough or eschar may
be present on some parts of the wound bed. Often includes undermining and tunneling.
Number of Stage 4 pressure ulcers
D1. Unstageable: Non-removable dressing/device: Known but not stageable due to non-
removable dressing/device Number of unstageable pressure ulcers/injuries due to non-removable dressing/device
E1. Unstageable: Slough and/or eschar: Known but not stageable due to coverage of wound bed
by slough and/or eschar
Number of unstageable pressure ulcers/injuries due to coverage of wound bed by slough and/or eschar
F1. Unstageable: Deep tissue injury Number of unstageable pressure injuries presenting as deep tissue injury
236
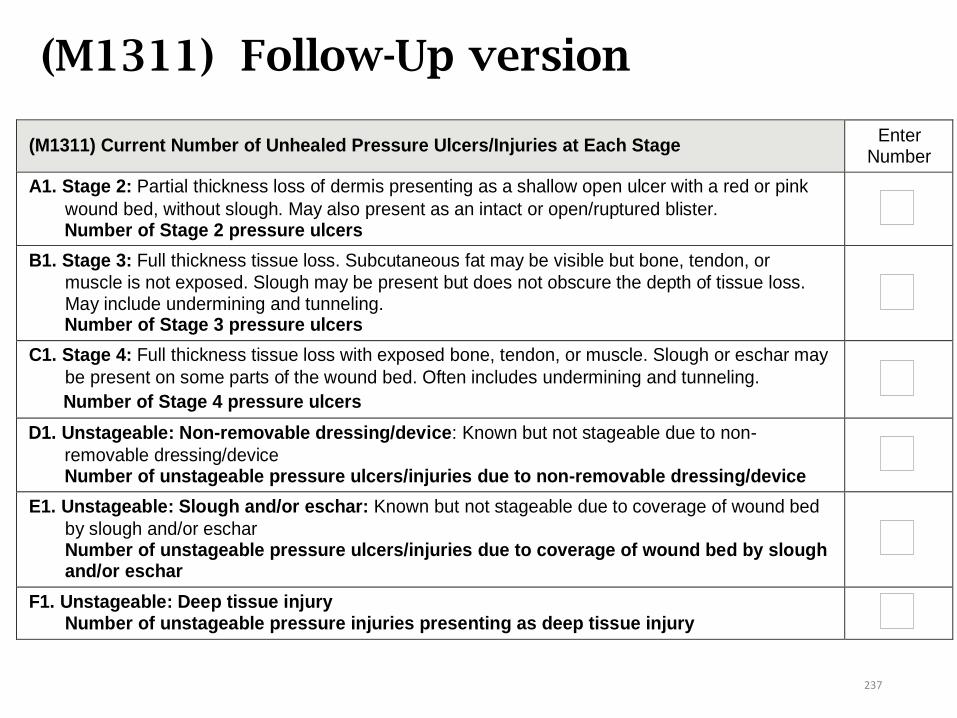
(M1311) Follow-Up version
(M1311) Current Number of Unhealed Pressure Ulcers/Injuries at Each Stage Enter
Number
A1. Stage 2: Partial thickness loss of dermis presenting as a shallow open ulcer with a red or pink
wound bed, without slough. May also present as an intact or open/ruptured blister. Number of Stage 2 pressure ulcers
B1. Stage 3: Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon, or
muscle is not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining and tunneling. Number of Stage 3 pressure ulcers
C1. Stage 4: Full thickness tissue loss with exposed bone, tendon, or muscle. Slough or eschar may
be present on some parts of the wound bed. Often includes undermining and tunneling.
Number of Stage 4 pressure ulcers
D1. Unstageable: Non-removable dressing/device: Known but not stageable due to non-
removable dressing/device Number of unstageable pressure ulcers/injuries due to non-removable dressing/device
E1. Unstageable: Slough and/or eschar: Known but not stageable due to coverage of wound bed
by slough and/or eschar Number of unstageable pressure ulcers/injuries due to coverage of wound bed by slough and/or eschar
F1. Unstageable: Deep tissue injury Number of unstageable pressure injuries presenting as deep tissue injury
237

(M1311) Discharge version, A-C
(M1311) Current Number of Unhealed Pressure Ulcers/Injuries at Each Stage Enter
Number
A1. Stage 2: Partial thickness loss of dermis presenting as a shallow open ulcer with a red or pink
wound bed, without slough. May also present as an intact or open/ruptured blister. Number of Stage 2 pressure ulcers [If 0 – Go to M1311B1, Stage 3]
A2. Number of these Stage 2 pressure ulcers that were present at most recent SOC/ROC
– enter how many were noted at the time of most recent SOC/ROC
B1. Stage 3: Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon, or
muscle is not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining and tunneling. Number of Stage 3 pressure ulcers [If 0 – Go to M1311C1, Stage 4]
B2. Number of these Stage 3 pressure ulcers that were present at most recent SOC/ROC
– enter how many were noted at the time of most recent SOC/ROC
C1. Stage 4: Full thickness tissue loss with exposed bone, tendon, or muscle. Slough or eschar may
be present on some parts of the wound bed. Often includes undermining and tunneling.
Number of Stage 4 pressure ulcers [If 0 – Go to M1311D1, Unstageable: Non-removable dressing/device]
C2. Number of these Stage 4 pressure ulcers that were present at most recent SOC/ROC
– enter how many were noted at the time of most recent SOC/ROC
238
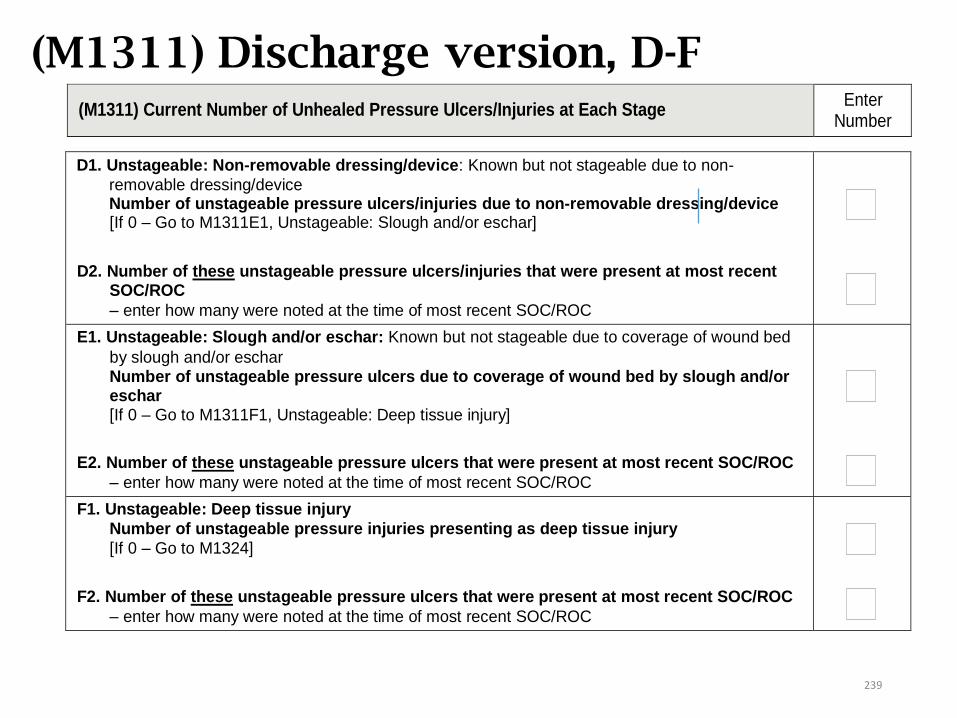
(M1311) Discharge version, D-F
D1. Unstageable: Non-removable dressing/device: Known but not stageable due to non-
removable dressing/device Number of unstageable pressure ulcers/injuries due to non-removable dressing/device [If 0 – Go to M1311E1, Unstageable: Slough and/or eschar]
D2. Number of these unstageable pressure ulcers/injuries that were present at most recent
SOC/ROC
– enter how many were noted at the time of most recent SOC/ROC
E1. Unstageable: Slough and/or eschar: Known but not stageable due to coverage of wound bed
by slough and/or eschar Number of unstageable pressure ulcers due to coverage of wound bed by slough and/or eschar [If 0 – Go to M1311F1, Unstageable: Deep tissue injury]
E2. Number of these unstageable pressure ulcers that were present at most recent SOC/ROC
– enter how many were noted at the time of most recent SOC/ROC
F1. Unstageable: Deep tissue injury
Number of unstageable pressure injuries presenting as deep tissue injury
[If 0 – Go to M1324]
F2. Number of these unstageable pressure ulcers that were present at most recent SOC/ROC
– enter how many were noted at the time of most recent SOC/ROC
(M1311) Current Number of Unhealed Pressure Ulcers/Injuries at Each Stage Enter
Number
239
(M1311) Guidance
• Not reported in M1311:• Stage 1 pressure injuries
• Pressure ulcers that have healed
• Not considered healed:• Stage 1 pressure injuries, although they are closed (intact
skin)
• Stage 2 pressure ulcers
• Suspected Deep Tissue Injury (sDTI), although closed (intact skin)
• Unstageable pressure ulcers covered by eschar or slough
240
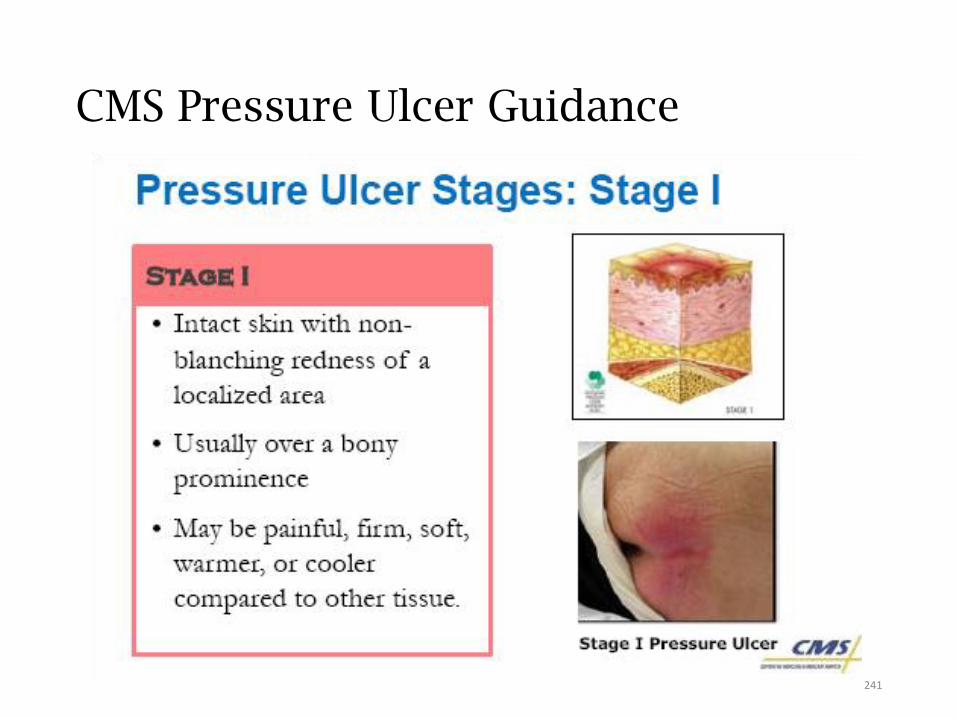
CMS Pressure Ulcer Guidance
241
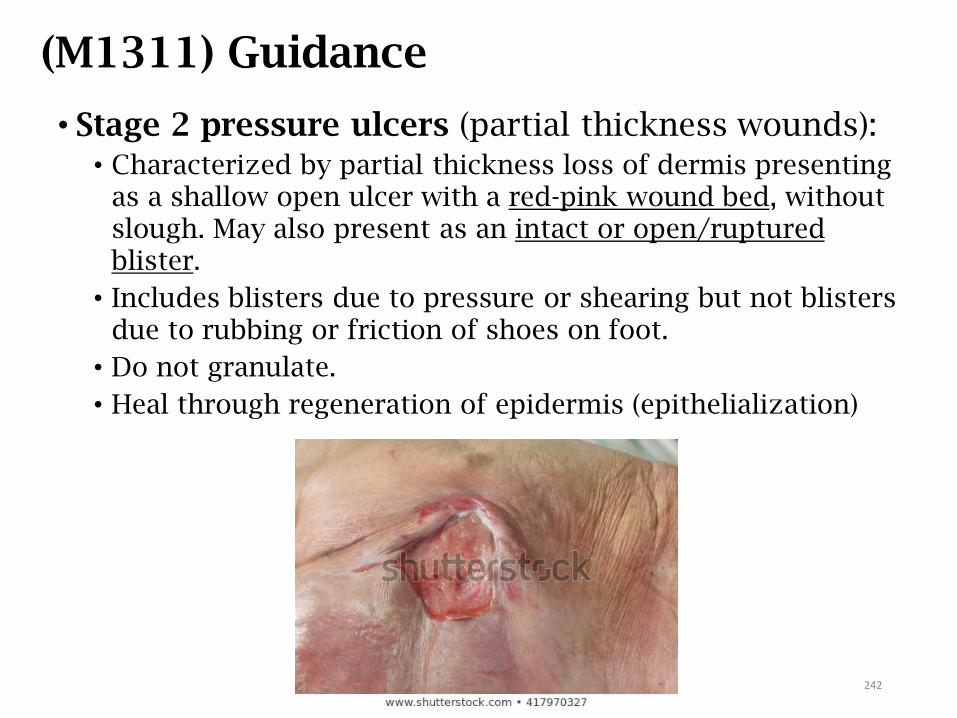
(M1311) Guidance
• Stage 2 pressure ulcers (partial thickness wounds):• Characterized by partial thickness loss of dermis presenting
as a shallow open ulcer with a red-pink wound bed, without slough. May also present as an intact or open/ruptured blister.
• Includes blisters due to pressure or shearing but not blisters due to rubbing or friction of shoes on foot.
• Do not granulate.
• Heal through regeneration of epidermis (epithelialization)
242
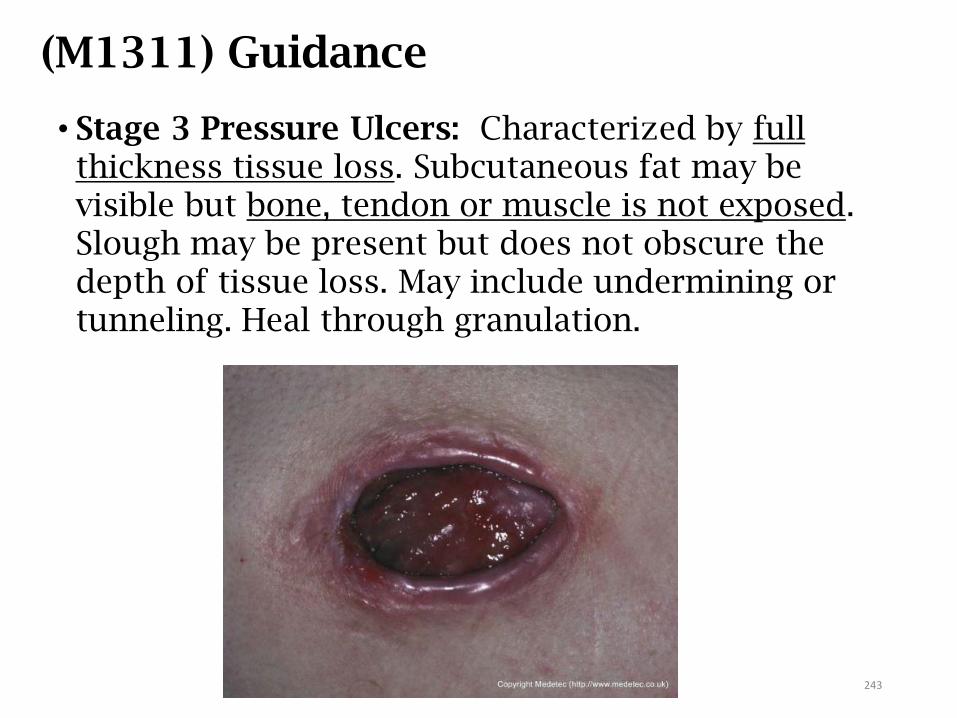
(M1311) Guidance
• Stage 3 Pressure Ulcers: Characterized by full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon or muscle is not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining or tunneling. Heal through granulation.
243
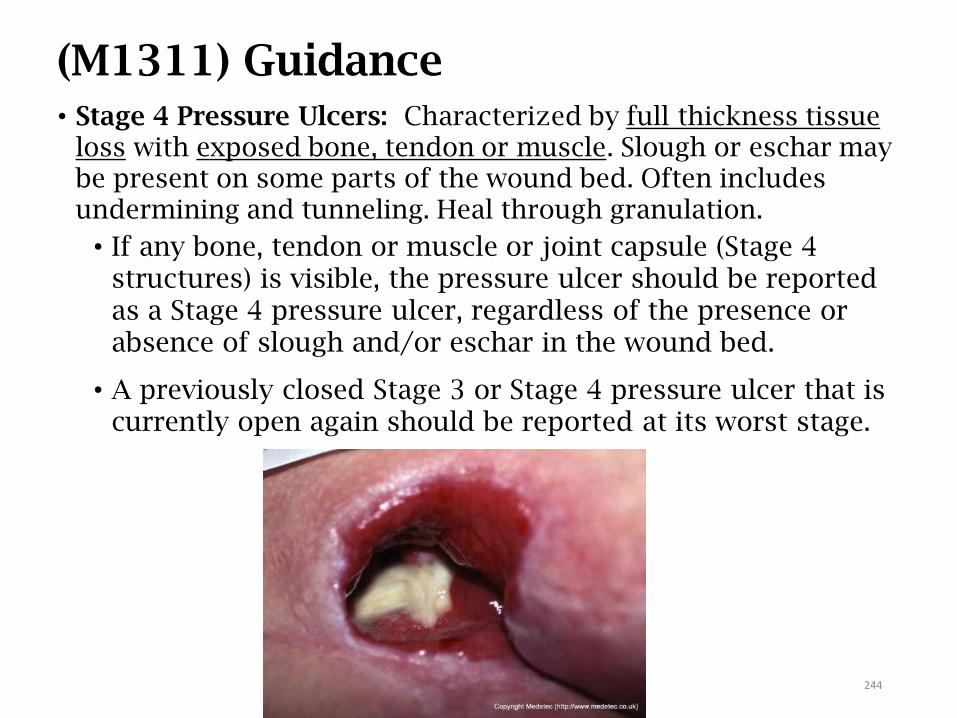
(M1311) Guidance• Stage 4 Pressure Ulcers: Characterized by full thickness tissue
loss with exposed bone, tendon or muscle. Slough or eschar may be present on some parts of the wound bed. Often includes undermining and tunneling. Heal through granulation.
• If any bone, tendon or muscle or joint capsule (Stage 4 structures) is visible, the pressure ulcer should be reported as a Stage 4 pressure ulcer, regardless of the presence or absence of slough and/or eschar in the wound bed.
• A previously closed Stage 3 or Stage 4 pressure ulcer that is currently open again should be reported at its worst stage.
244
M1311 Unstageable Pressure Ulcer
A pressure ulcer is considered Unstageable if:
• It is covered with a non-removable dressing/device, such as a
cast, that cannot be removed;
• It is a suspected deep tissue injury in evolution; or
• The wound bed is obscured by some degree of necrotic tissue
AND no bone, muscle, tendon, or joint capsule (Stage 4
structures) are visible.
• Pressure ulcers that have eschar (tan, black, or brown) or slough
(yellow, tan, gray, green or brown) tissue present such that the
anatomic depth of soft tissue damage cannot be visualized in
the wound bed, should be classified as unstageable.
• Any numerically stageable pressure ulcer/injury observed at
SOC/ROC, but at the time of discharge is unstageable due to
slough and/or eschar, should be considered new, and not coded
as present at the most recent SOC/ROC for M1311X2.245
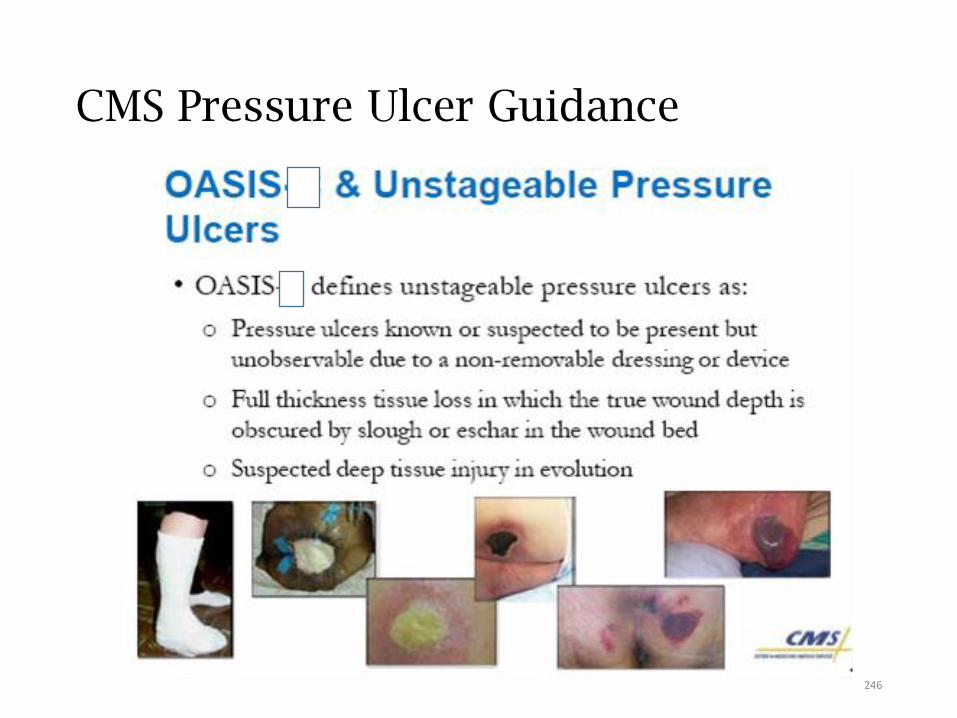
CMS Pressure Ulcer Guidance
246
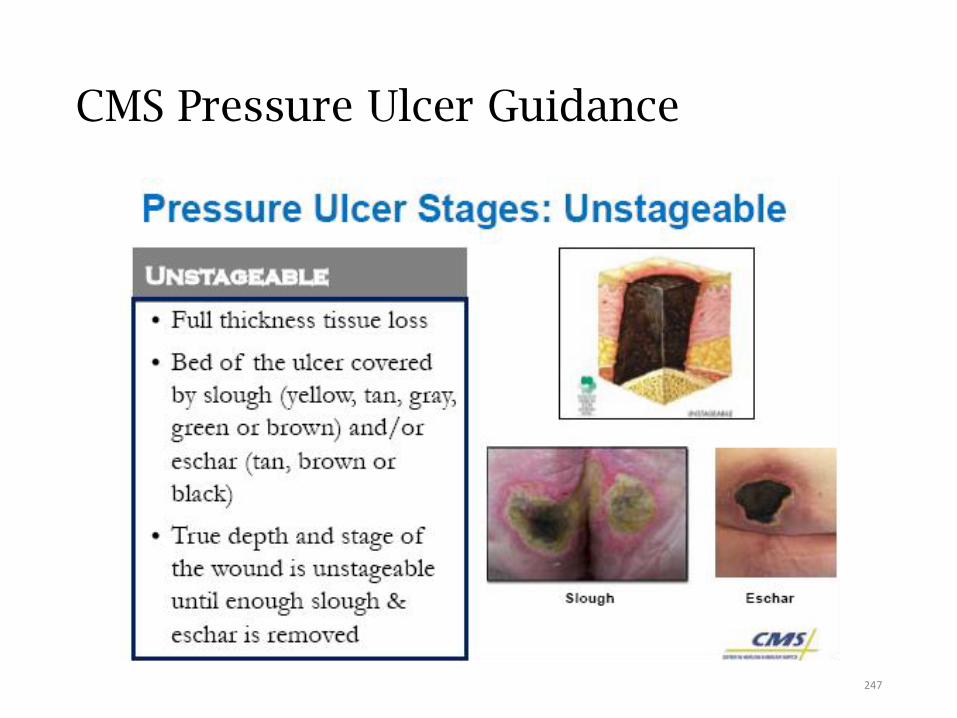
CMS Pressure Ulcer Guidance
247
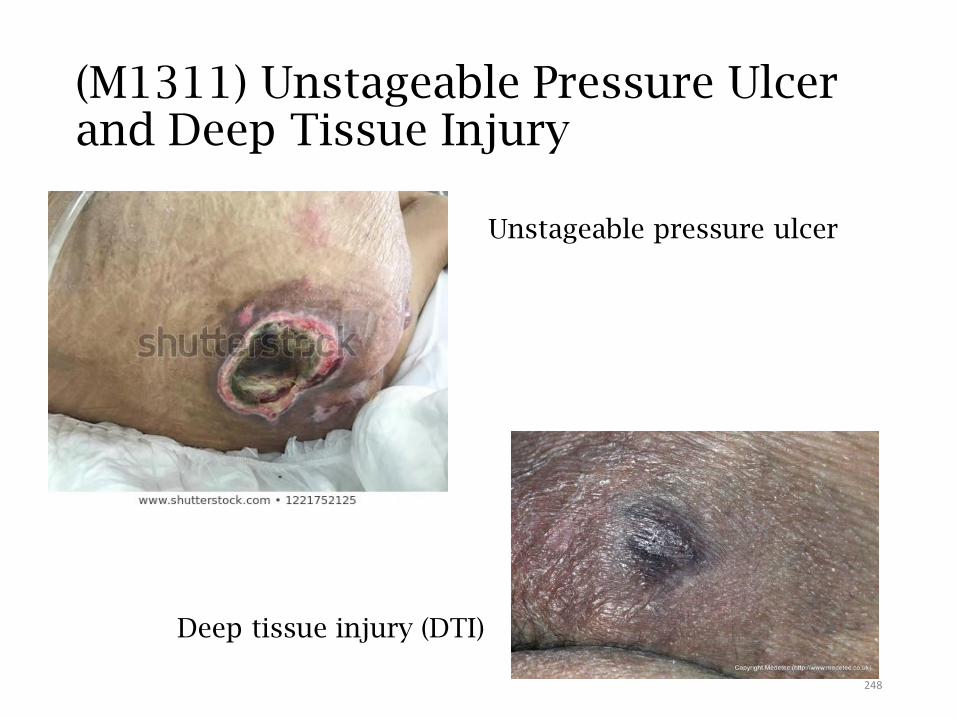
(M1311) Unstageable Pressure Ulcer and Deep Tissue Injury
Unstageable pressure ulcer
Deep tissue injury (DTI)
248
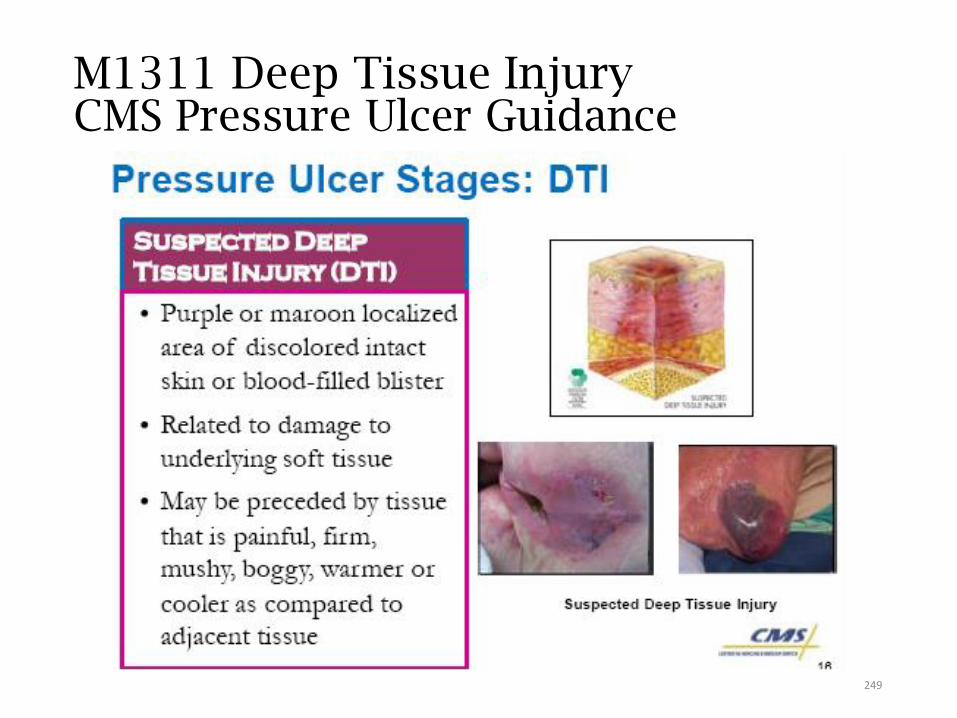
CMS Pressure Ulcer GuidanceM1311 Deep Tissue Injury
249
Medical Device Related Pressure Injury (NPUAP 2016)
Medical Device Related Pressure Injury:
This describes an etiology.
• Medical device related pressure injuries result from the use of devices designed and applied for diagnostic or therapeutic purposes. The resultant pressure injury generally conforms to the pattern or shape of the device. The injury should be staged using the staging system.
Mucosal Membrane Pressure Injury:
• Mucosal membrane pressure injury is found on mucous membranes with a history of a medical device in use at the location of the injury. Due to the anatomy of the tissue these ulcers cannot be staged.
250
(M1311) Guidance
• Surgically debrided pressure ulcers remain pressure ulcers. They are not surgical wounds.
• Pressure ulcers sutured closed are still considered pressure ulcers, not surgical wounds.
• Report these ulcers in M1311 as: D1 (unstageable d/t a nonremovable dressing or device
• Make and document every effort to contact previous providers (including patient’s physician) to determine the stage of the wound at its worst and report that stage.
• Do not reverse stage pressure ulcers as a way to document healing as it does not accurately characterize what is physiologically occurring as the ulcer heals.
• For example, over time, even though a Stage 4 pressure ulcer has been healing and contracting such that it is less deep, wide, and long, the tissues that were lost (muscle, fat, dermis) will never be replaced with the same type of tissue. Clinical standards require that this ulcer continue to be documented as a Stage 4 pressure ulcer until it has healed.
251
(M1311) Guidance: NOT a Pressure Ulcer
• A muscle flap, skin advancement flap, or rotational flap graft performed to surgically replace a pressure ulcer is not a pressure ulcer. It is a surgical wound, reported on M1340.
• Muscle flap, advancement flap, or rotational flap is defined as full thickness skin and subcutaneous tissue partially attached to the body by a narrow strip of tissue so that it retains its blood supply)
• A pressure ulcer treated with a skin graft (defined as transplantation of skin to another site) should not be reported as a pressure ulcer and, until the graft edges completely heal, should be reported as a surgical wound on M1340.
252
Present at SOC/ROC, row x1
• The general standard of practice for patients starting or resuming care is that patient assessments are completed as close to the actual time of the SOC/ROC (5-day/48-hr. window)
as possible. If a pressure ulcer that is identified on the SOC date increases in numerical stage (worsens) within the assessment time frame, the initial stage of the pressure ulcer would be reported in M1311 at the SOC.
• For example: At SOC on 8/1, patient has a Stage 2 pressure ulcer and no other pressure ulcers. At a routine visit on 8/3, the pressure ulcer has worsened to a Stage 3. Report the Stage 2 on M1311, A1.
253
Present at SOC/ROC, row X2
• If a pressure ulcer was unstageable at SOC/ROC, but becomes numerically stageable later, when completing the Discharge assessment, its “Present at the most recent SOC/ROC” stage should be considered the stage at which it first becomes numerically stageable.
• If the ulcer subsequently increases in numerical stage during the episode, do not report the higher stage ulcer as being “present at SOC/ROC” when completing the Discharge assessment.
254
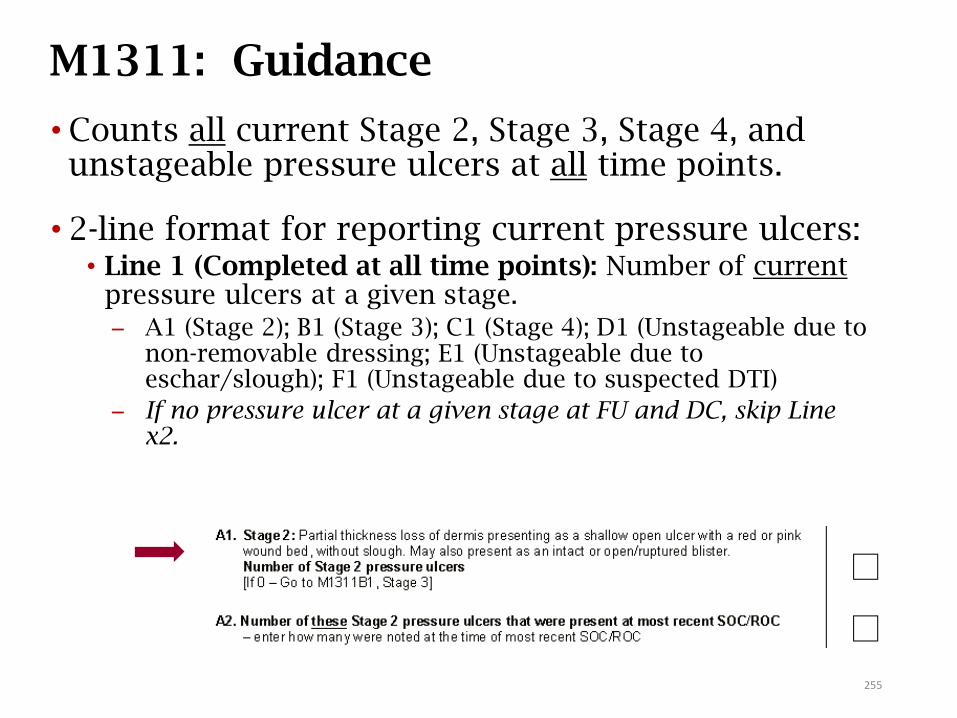
M1311: Guidance
• Counts all current Stage 2, Stage 3, Stage 4, and unstageable pressure ulcers at all time points.
• 2-line format for reporting current pressure ulcers:• Line 1 (Completed at all time points): Number of current
pressure ulcers at a given stage. A1 (Stage 2); B1 (Stage 3); C1 (Stage 4); D1 (Unstageable due to
non-removable dressing; E1 (Unstageable due to eschar/slough); F1 (Unstageable due to suspected DTI)
If no pressure ulcer at a given stage at FU and DC, skip Line x2.
255

M1311: Guidance
• 2-line format for reporting current pressure ulcers:• Line 2 (Completed at Follow-up and Discharge only):
Number of these ulcers at a given stage that were present at most recent SOC/ROC.
A2 (Stage 2); B2 (Stage 3); C2 (Stage 4); D2 (Unstageable due to non-removable dressing; E2 (Unstageable due to eschar/slough); F2 (Unstageable w/suspected DTI)
Interpretation: Was the current ulcer present AT THE SAME STAGE as at the most recent SOC/ROC assessment?
256
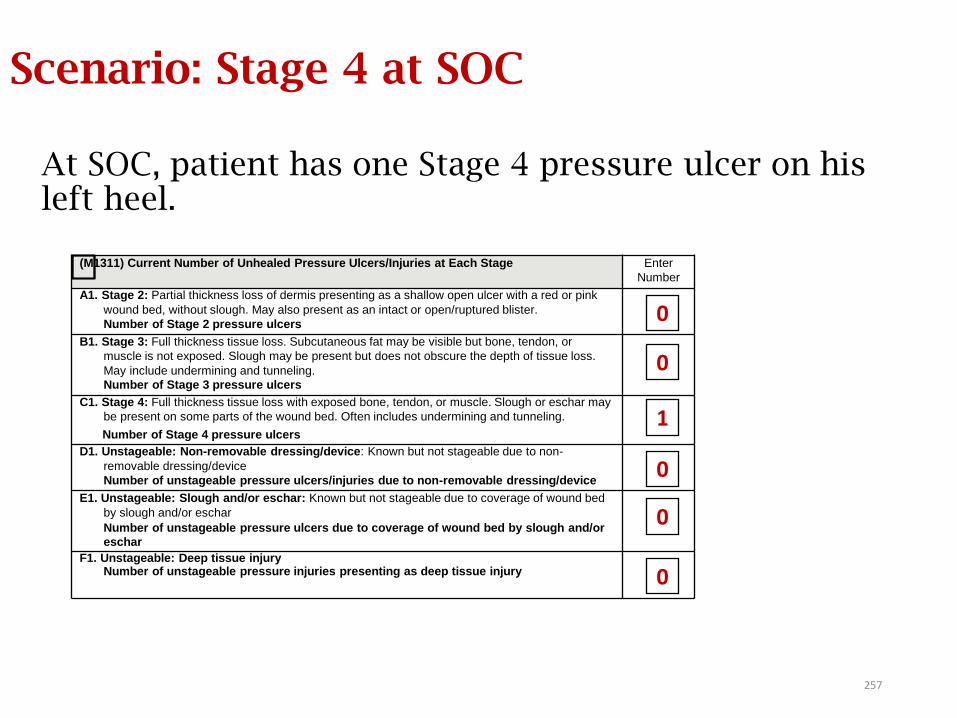
Scenario: Stage 4 at SOC
At SOC, patient has one Stage 4 pressure ulcer on his left heel.
0
1
(M1311) Current Number of Unhealed Pressure Ulcers/Injuries at Each Stage Enter
Number
A1. Stage 2: Partial thickness loss of dermis presenting as a shallow open ulcer with a red or pink
wound bed, without slough. May also present as an intact or open/ruptured blister.
Number of Stage 2 pressure ulcers
B1. Stage 3: Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon, or
muscle is not exposed. Slough may be present but does not obscure the depth of tissue loss.
May include undermining and tunneling.
Number of Stage 3 pressure ulcers
C1. Stage 4: Full thickness tissue loss with exposed bone, tendon, or muscle. Slough or eschar may
be present on some parts of the wound bed. Often includes undermining and tunneling.
Number of Stage 4 pressure ulcers
D1. Unstageable: Non-removable dressing/device: Known but not stageable due to non-
removable dressing/device
Number of unstageable pressure ulcers/injuries due to non-removable dressing/device
E1. Unstageable: Slough and/or eschar: Known but not stageable due to coverage of wound bed
by slough and/or eschar
Number of unstageable pressure ulcers due to coverage of wound bed by slough and/or
eschar
F1. Unstageable: Deep tissue injuryNumber of unstageable pressure injuries presenting as deep tissue injury
0
0
0
0
257
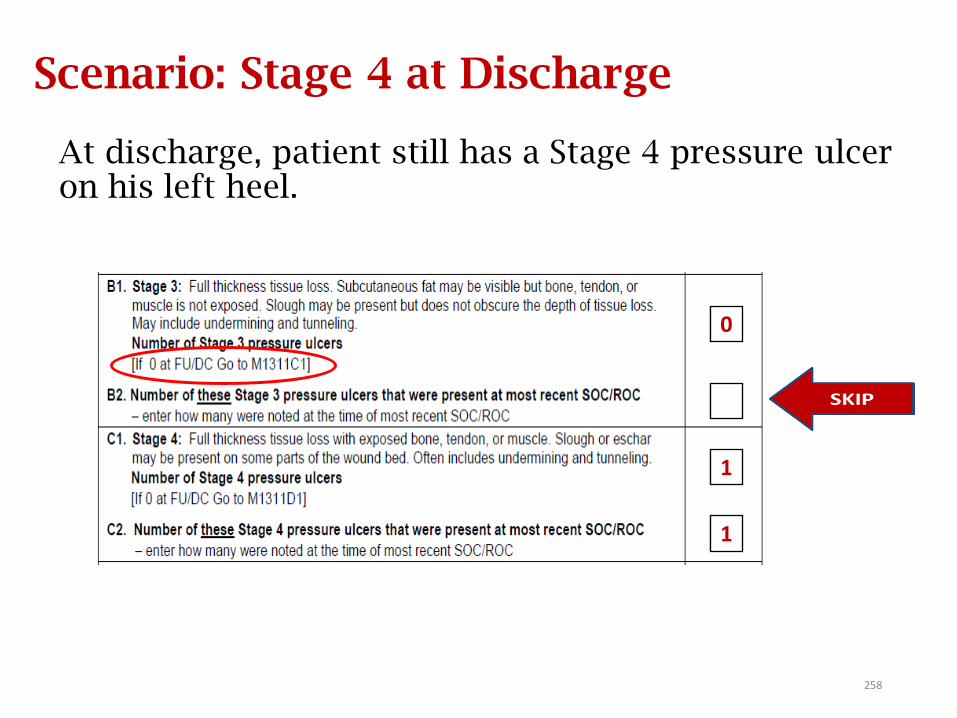
Scenario: Stage 4 at Discharge
At discharge, patient still has a Stage 4 pressure ulcer on his left heel.
0
1
1
258
Scenario: Eschar on the Heel
• Your patient had a pressure ulcer on his right heel that is unstageable due to black stable eschar. How should this be reported at SOC on M1311?
M1311: E1, Unstageable due to slough and/or eschar
259
During the episode the eschar peels off and leaves an area of fully granulated tissue. Assuming there is no documentation in the record that supports the most advanced stage of the ulcer, how should this ulcer be staged at Discharge on M1311?
Scenario: Eschar on the Heel (part 2)
260
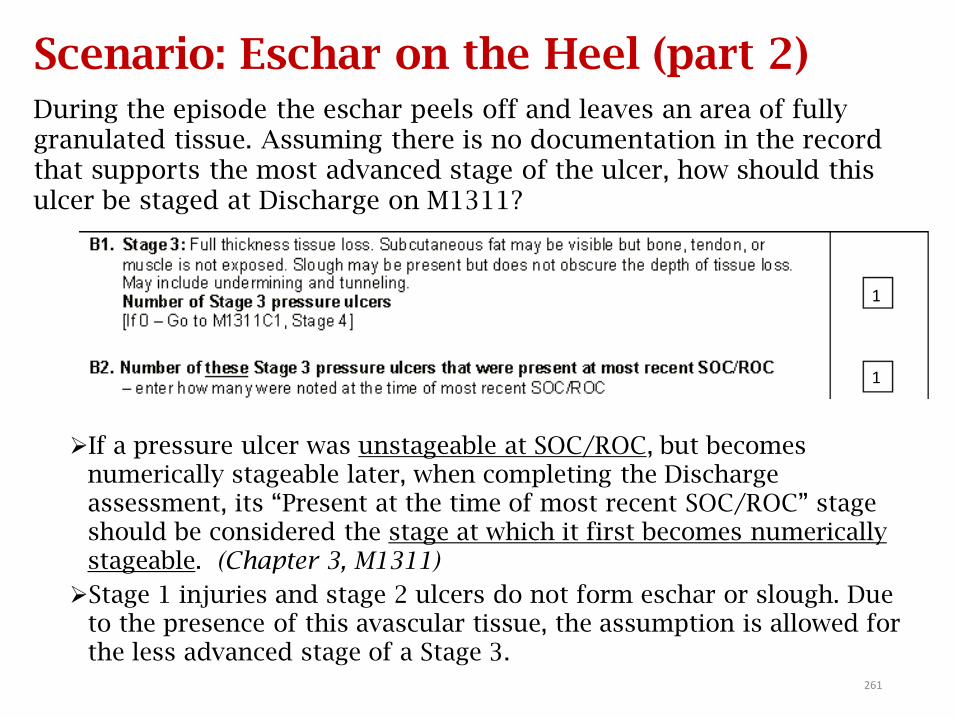
Scenario: Eschar on the Heel (part 2)During the episode the eschar peels off and leaves an area of fully granulated tissue. Assuming there is no documentation in the record that supports the most advanced stage of the ulcer, how should this ulcer be staged at Discharge on M1311?
If a pressure ulcer was unstageable at SOC/ROC, but becomes numerically stageable later, when completing the Discharge assessment, its “Present at the time of most recent SOC/ROC” stage should be considered the stage at which it first becomes numerically stageable. (Chapter 3, M1311)
Stage 1 injuries and stage 2 ulcers do not form eschar or slough. Due to the presence of this avascular tissue, the assumption is allowed for the less advanced stage of a Stage 3.
1
1
261
M1311: Scenario patient X
Patient X had a Stage 2 pressure ulcer on her left hip at SOC. Two weeks later she had an exacerbation of her CHF and was hospitalized for 5 days.
• At the ROC assessment, the pressure ulcer on her left hip had deteriorated to a Stage 3, and she had a new Stage 1 pressure injury on her right hip.
• At discharge, the Stage 3 pressure ulcer on her left hip was 80% granulated, and the Stage 1 pressure injury on her right hip had evolved to a stage 2 pressure ulcer.
Complete M1311 at SOC, ROC and DC
262
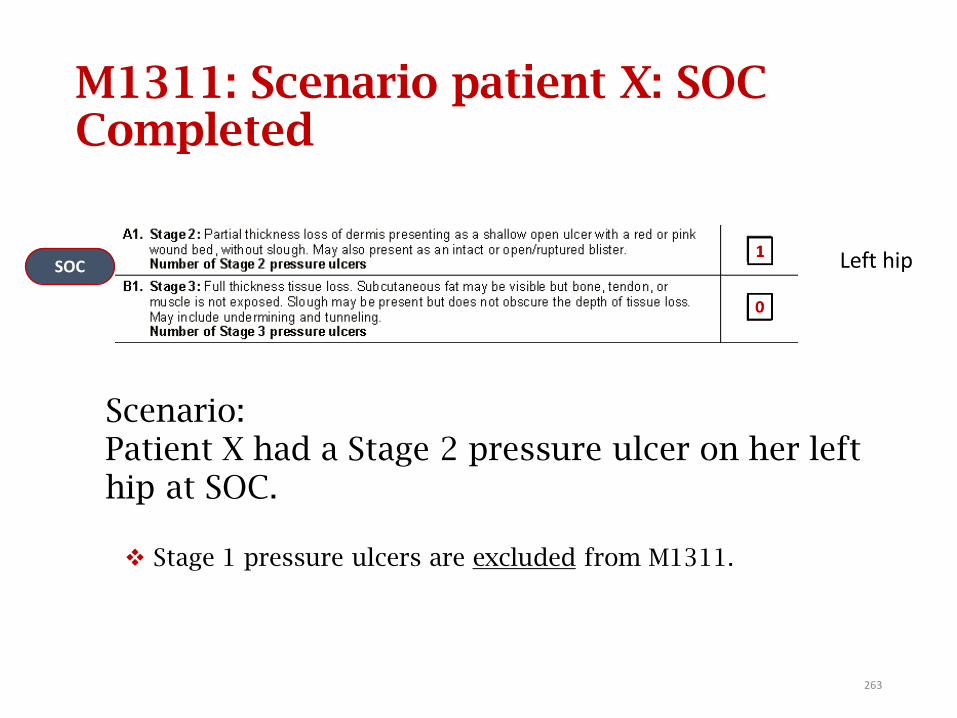
M1311: Scenario patient X: SOC Completed
Stage 1 pressure ulcers are excluded from M1311.
SOC
Scenario: Patient X had a Stage 2 pressure ulcer on her left hip at SOC.
Left hip
263
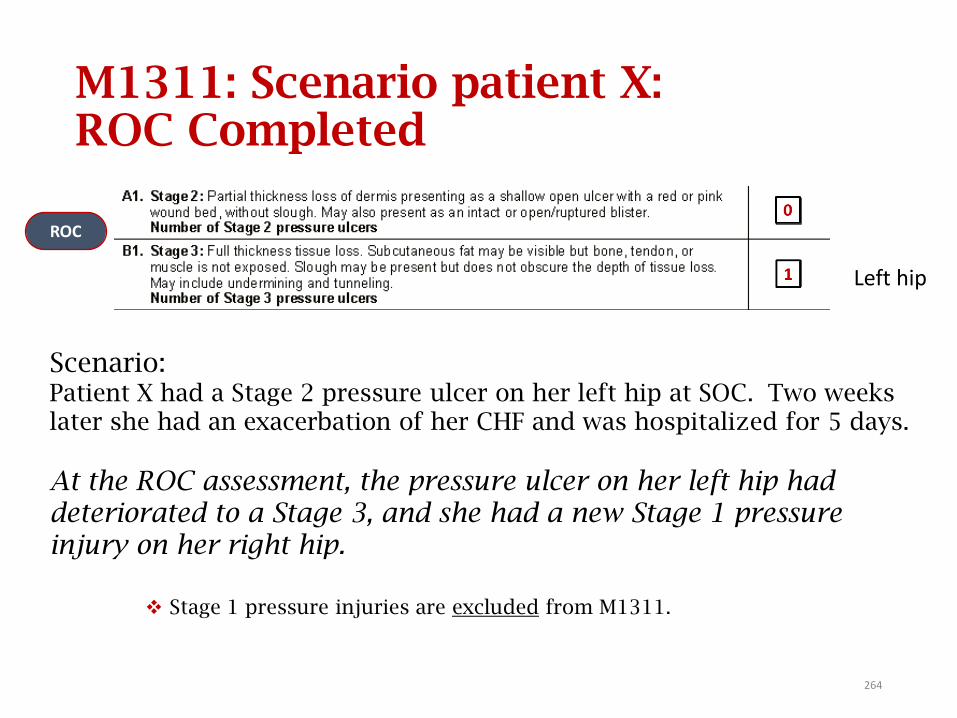
M1311: Scenario patient X: ROC Completed
Stage 1 pressure injuries are excluded from M1311.
ROC
Scenario:Patient X had a Stage 2 pressure ulcer on her left hip at SOC. Two weeks later she had an exacerbation of her CHF and was hospitalized for 5 days.
At the ROC assessment, the pressure ulcer on her left hip had deteriorated to a Stage 3, and she had a new Stage 1 pressure injury on her right hip.
Left hip
264
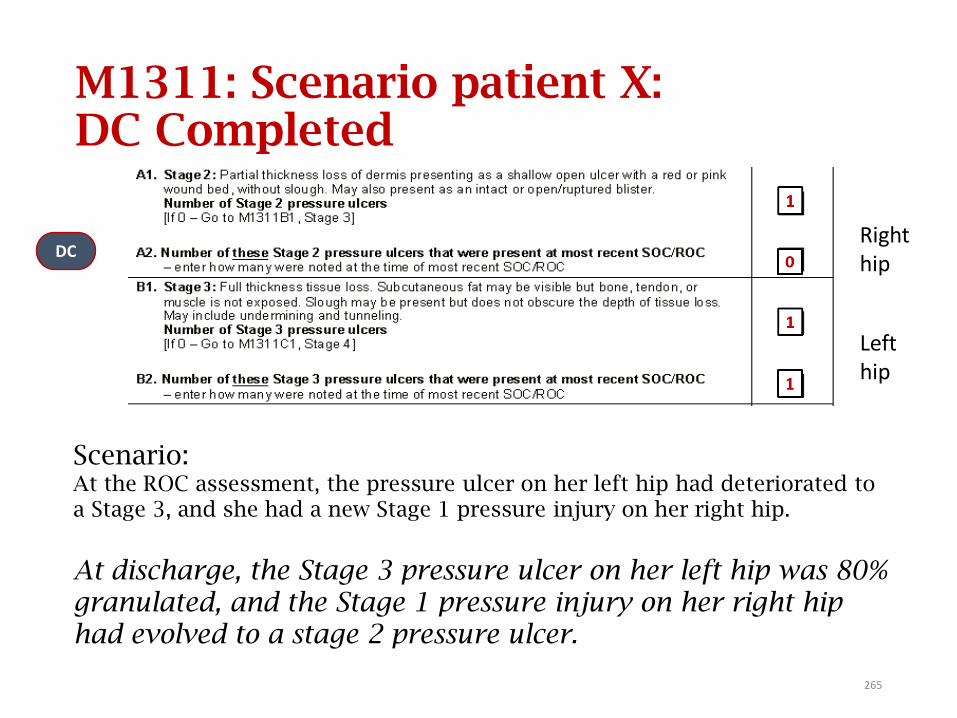
M1311: Scenario patient X: DC Completed
DC
Lefthip
Right hip
Scenario: At the ROC assessment, the pressure ulcer on her left hip had deteriorated to a Stage 3, and she had a new Stage 1 pressure injury on her right hip.
At discharge, the Stage 3 pressure ulcer on her left hip was 80% granulated, and the Stage 1 pressure injury on her right hip had evolved to a stage 2 pressure ulcer.
265
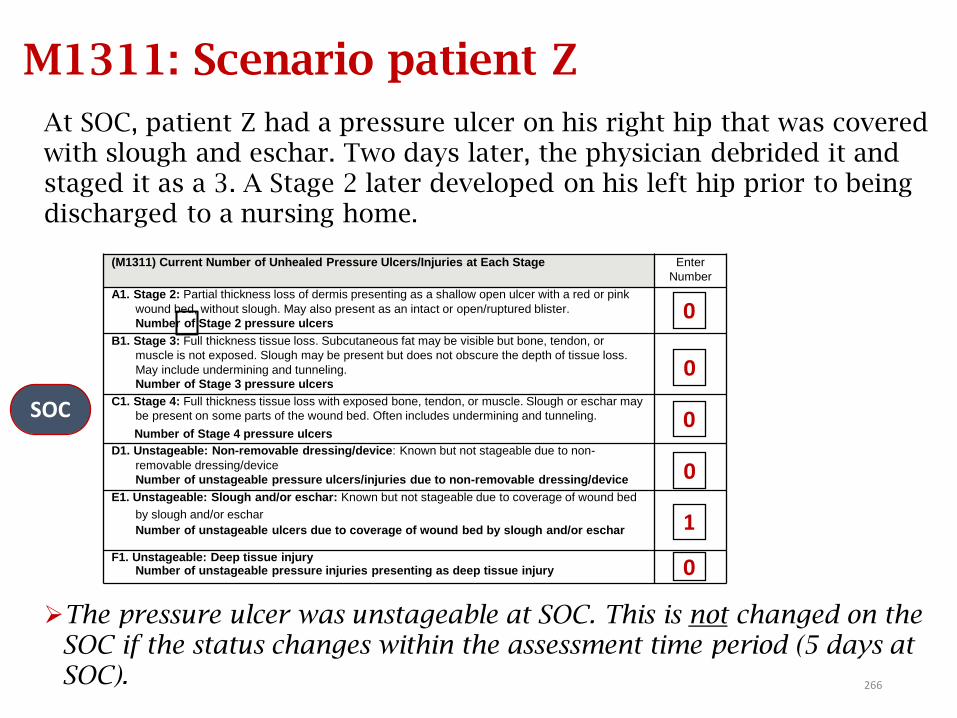
M1311: Scenario patient Z
At SOC, patient Z had a pressure ulcer on his right hip that was covered with slough and eschar. Two days later, the physician debrided it and staged it as a 3. A Stage 2 later developed on his left hip prior to being discharged to a nursing home.
The pressure ulcer was unstageable at SOC. This is not changed on the SOC if the status changes within the assessment time period (5 days at SOC).
0
SOC
(M1311) Current Number of Unhealed Pressure Ulcers/Injuries at Each Stage Enter
Number
A1. Stage 2: Partial thickness loss of dermis presenting as a shallow open ulcer with a red or pink
wound bed, without slough. May also present as an intact or open/ruptured blister.
Number of Stage 2 pressure ulcers
B1. Stage 3: Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon, or
muscle is not exposed. Slough may be present but does not obscure the depth of tissue loss.
May include undermining and tunneling.
Number of Stage 3 pressure ulcers
C1. Stage 4: Full thickness tissue loss with exposed bone, tendon, or muscle. Slough or eschar may
be present on some parts of the wound bed. Often includes undermining and tunneling.
Number of Stage 4 pressure ulcers
D1. Unstageable: Non-removable dressing/device: Known but not stageable due to non-
removable dressing/device
Number of unstageable pressure ulcers/injuries due to non-removable dressing/device
E1. Unstageable: Slough and/or eschar: Known but not stageable due to coverage of wound bed
by slough and/or eschar
Number of unstageable ulcers due to coverage of wound bed by slough and/or eschar
F1. Unstageable: Deep tissue injuryNumber of unstageable pressure injuries presenting as deep tissue injury
0
0
0
0
1
266
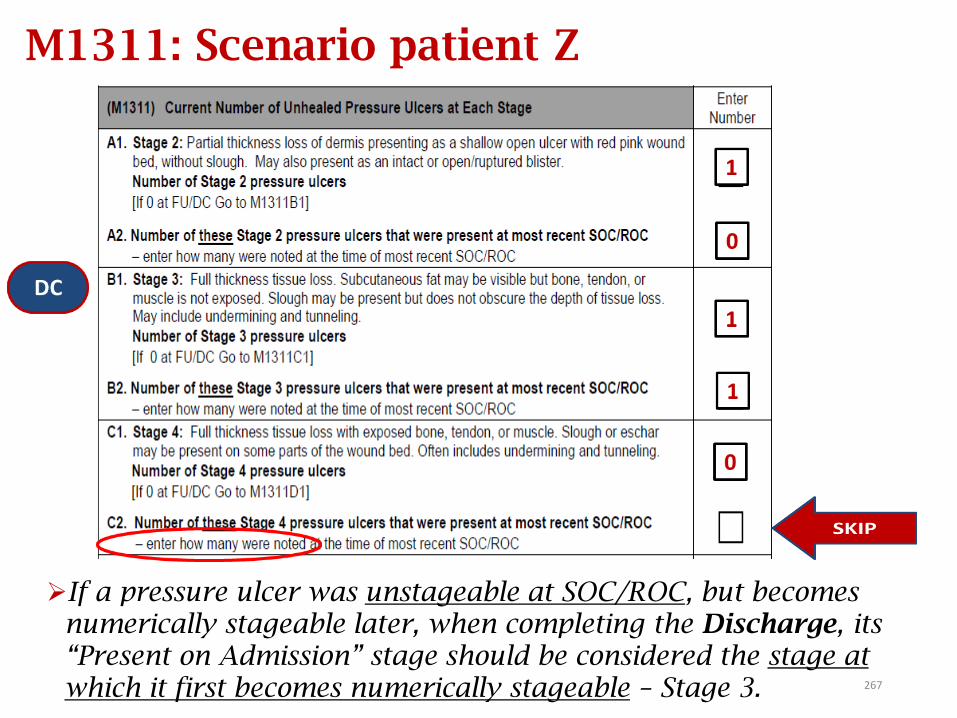
0
If a pressure ulcer was unstageable at SOC/ROC, but becomes numerically stageable later, when completing the Discharge, its “Present on Admission” stage should be considered the stage at which it first becomes numerically stageable – Stage 3.
M1311: Scenario patient Z
267
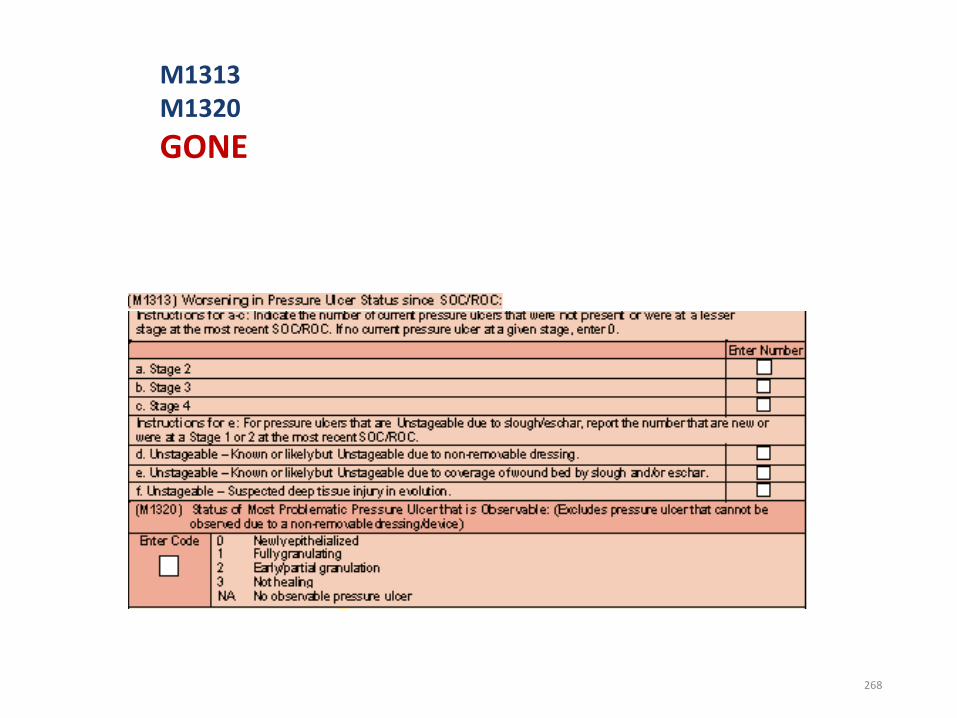
M1313M1320
GONE
268
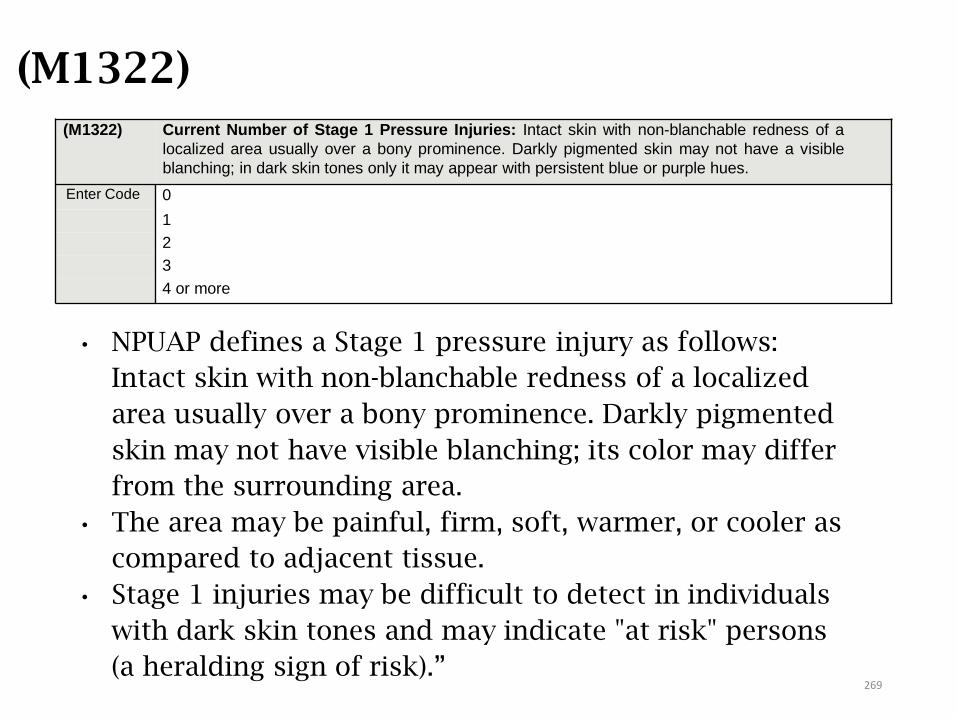
(M1322)
(M1322) Current Number of Stage 1 Pressure Injuries: Intact skin with non-blanchable redness of a
localized area usually over a bony prominence. Darkly pigmented skin may not have a visible
blanching; in dark skin tones only it may appear with persistent blue or purple hues.
Enter Code 0
1
2
3
4 or more
• NPUAP defines a Stage 1 pressure injury as follows:
Intact skin with non-blanchable redness of a localized
area usually over a bony prominence. Darkly pigmented
skin may not have visible blanching; its color may differ
from the surrounding area.
• The area may be painful, firm, soft, warmer, or cooler as
compared to adjacent tissue.
• Stage 1 injuries may be difficult to detect in individuals
with dark skin tones and may indicate "at risk" persons
(a heralding sign of risk).”269
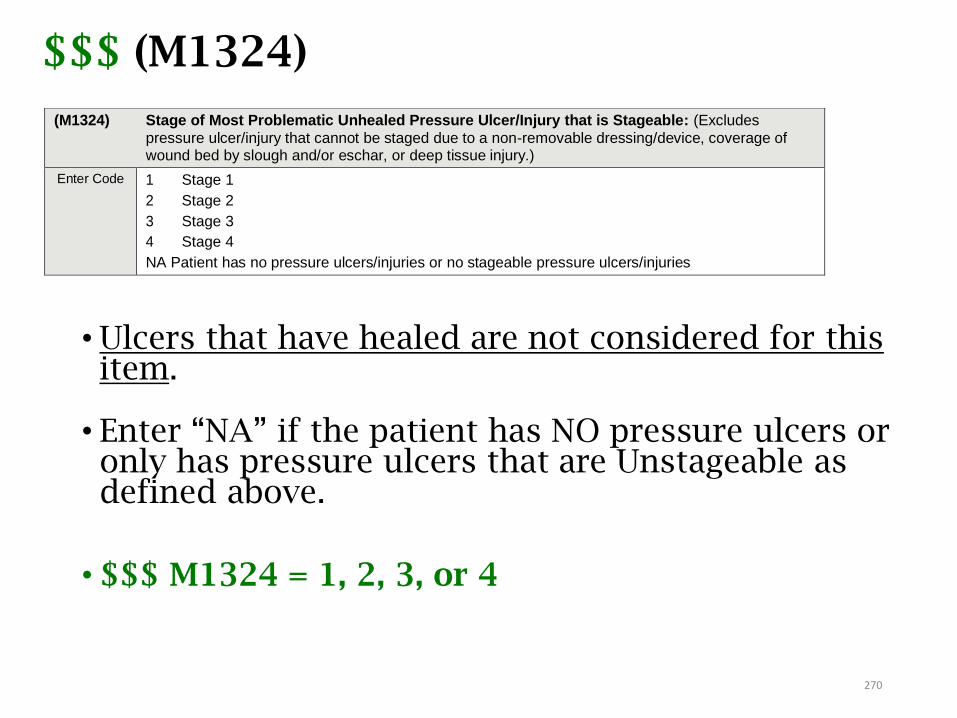
$$$ (M1324)
• Ulcers that have healed are not considered for this item.
• Enter “NA” if the patient has NO pressure ulcers or only has pressure ulcers that are Unstageable as defined above.
• $$$ M1324 = 1, 2, 3, or 4
(M1324) Stage of Most Problematic Unhealed Pressure Ulcer/Injury that is Stageable: (Excludes
pressure ulcer/injury that cannot be staged due to a non-removable dressing/device, coverage of wound bed by slough and/or eschar, or deep tissue injury.)
Enter Code 1 Stage 1
2 Stage 2
3 Stage 3
4 Stage 4
NA Patient has no pressure ulcers/injuries or no stageable pressure ulcers/injuries
270
Pressure Ulcer Scenario
On admission to your agency, patient had a Stage 2 pressure ulcer on his (L) hip. After 7 weeks of care, the SN notes that the Stage 2 ulcer has epithelialized. At discharge, the sacral area is noted to be reddened and non-blanchable, with no break in skin, and there are no other skin lesions.
How should the following OASIS items be answered?
M1306 – Does this patient have at least one Unhealed Pressure Ulcer at Stage 2 or Higher or designated as “unstageable”?
M1322 – Current Number of Stage 1 Pressure Ulcers
M1324 – Stage of Most Problematic Unhealed Pressure Ulcer
271
AnswersOn admission to your agency, patient had a Stage 2 pressure ulcer on his (L) hip. After 7 weeks of care, the SN notes that the Stage 2 ulcer has epithelialized. At discharge, the sacral area is noted to be reddened and non-blanchable, with no break in skin, and there are no other lesions.
How should the following OASIS items be answered at discharge?
• M1306 – Does this patient have at least one Unhealed Pressure Ulcer at Stage 2 or Higher or designated as “unstageable”?
Response 0 - No [Go to M1322]
• M1322 – Current Number of Stage 1 Pressure Ulcers
Response 1 – (1) Stage 1
• M1324 – Stage of Most Problematic Unhealed Pressure Ulcer
Response 1 - Stage 1272
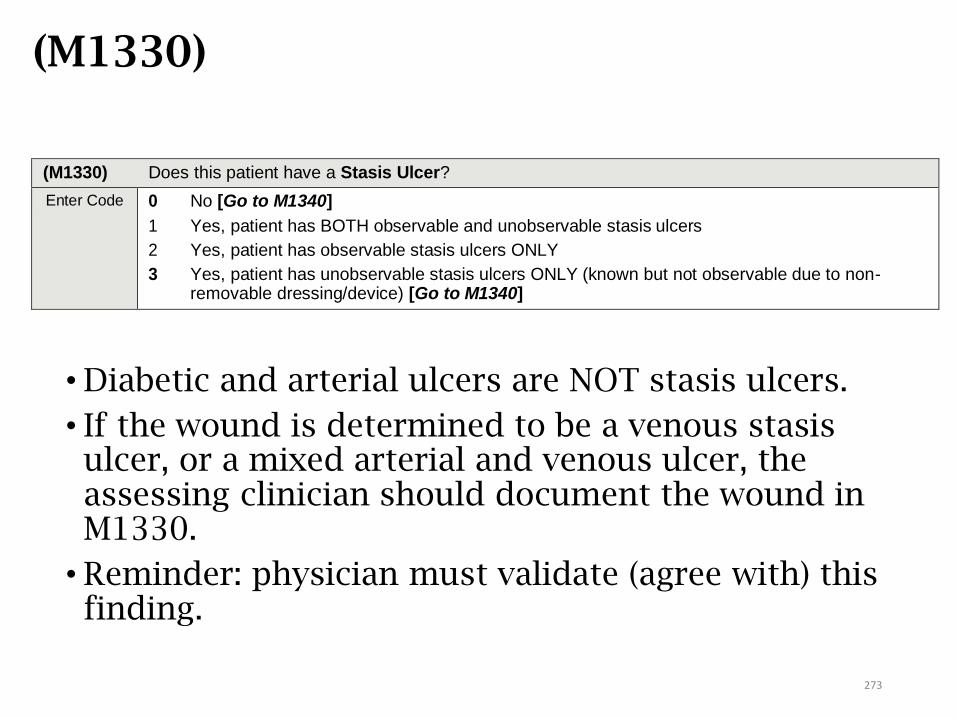
(M1330)
• Diabetic and arterial ulcers are NOT stasis ulcers.
• If the wound is determined to be a venous stasis ulcer, or a mixed arterial and venous ulcer, the assessing clinician should document the wound in M1330.
• Reminder: physician must validate (agree with) this finding.
(M1330) Does this patient have a Stasis Ulcer?
Enter Code 0 No [Go to M1340]
1 Yes, patient has BOTH observable and unobservable stasis ulcers
2 Yes, patient has observable stasis ulcers ONLY
3 Yes, patient has unobservable stasis ulcers ONLY (known but not observable due to non- removable dressing/device) [Go to M1340]
273
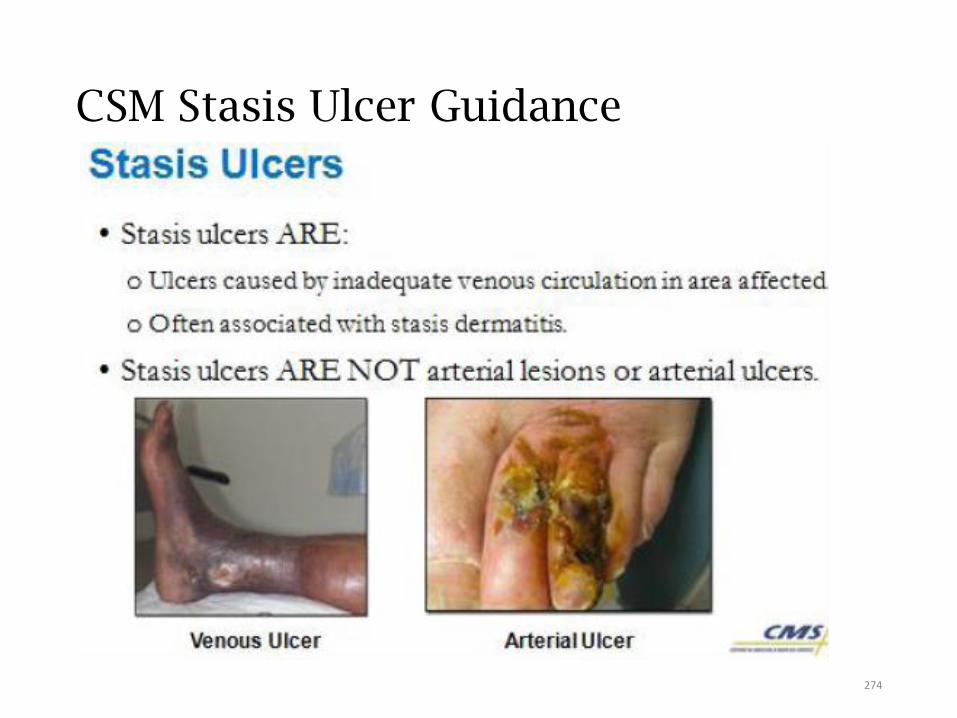
CSM Stasis Ulcer Guidance
274
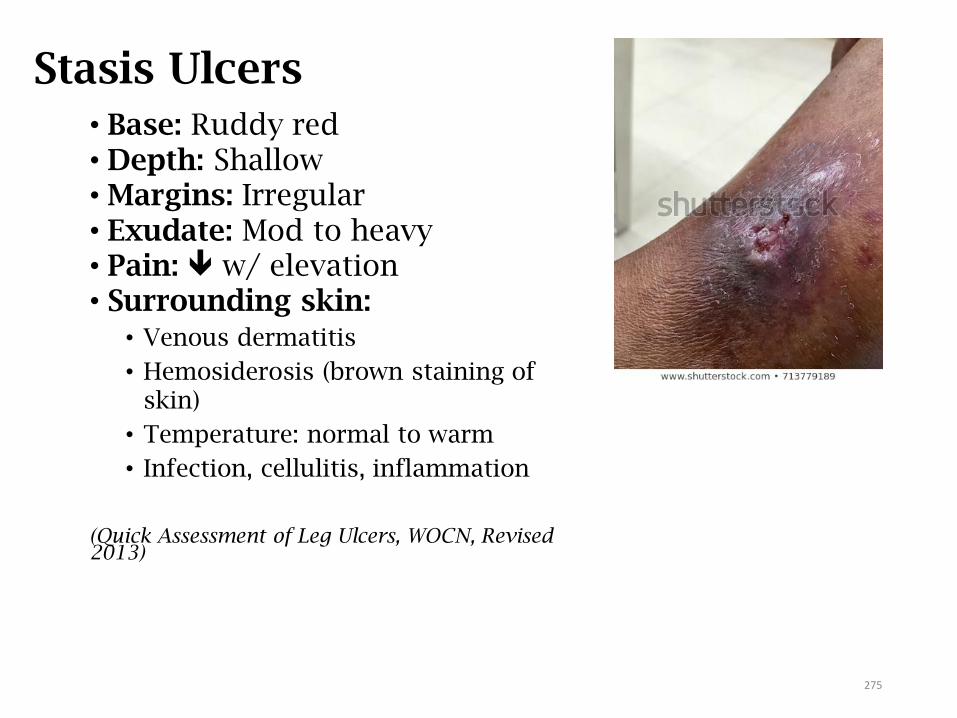
Stasis Ulcers• Base: Ruddy red• Depth: Shallow• Margins: Irregular• Exudate: Mod to heavy• Pain: w/ elevation• Surrounding skin:
• Venous dermatitis
• Hemosiderosis (brown staining of skin)
• Temperature: normal to warm
• Infection, cellulitis, inflammation
(Quick Assessment of Leg Ulcers, WOCN, Revised 2013)
275

Arterial Ulcers
• Base: pale• Depth: May be deep
• Margins: edges rolled• Exudate: Minimal• Pain: w/ elevation/ activity• Surrounding skin:
• Pale on elevation
• Temperature: decreased/cold
• Shiny, taut, thin, dry
• Hair loss over LE
• Necrosis, gangrene, eschar, cellulitis
(Quick Assessment of Leg Ulcers, WOCN, 2009)
276
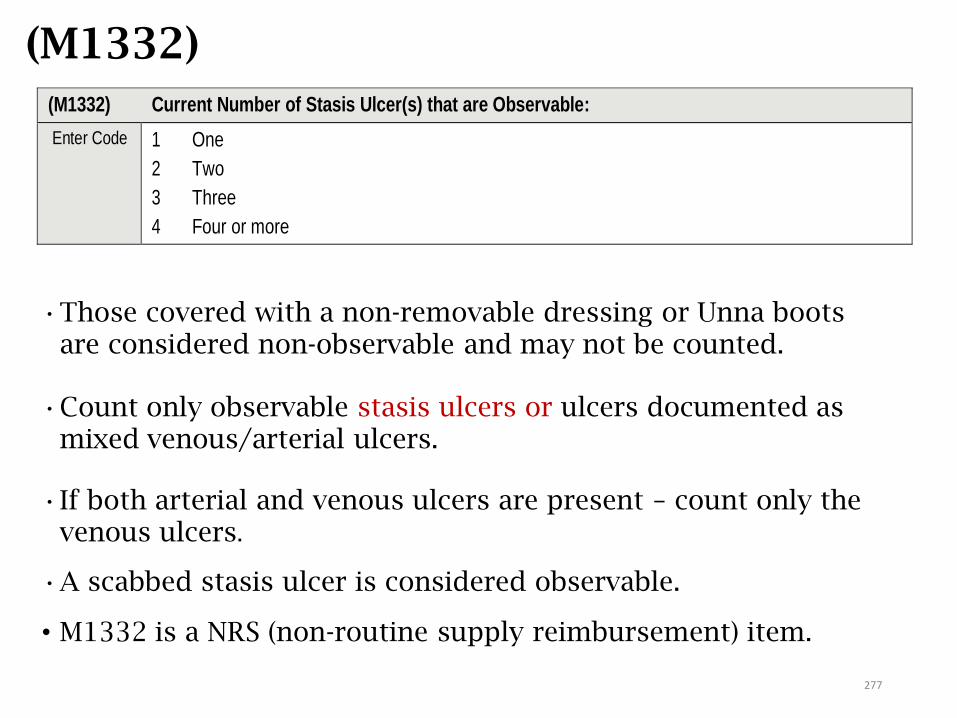
(M1332)
•Those covered with a non-removable dressing or Unna boots are considered non-observable and may not be counted.
•Count only observable stasis ulcers or ulcers documented as mixed venous/arterial ulcers.
•If both arterial and venous ulcers are present – count only the venous ulcers.
•A scabbed stasis ulcer is considered observable.
• M1332 is a NRS (non-routine supply reimbursement) item.
(M1332) Current Number of Stasis Ulcer(s) that are Observable:
Enter Code 1 One
2 Two
3 Three
4 Four or more
277
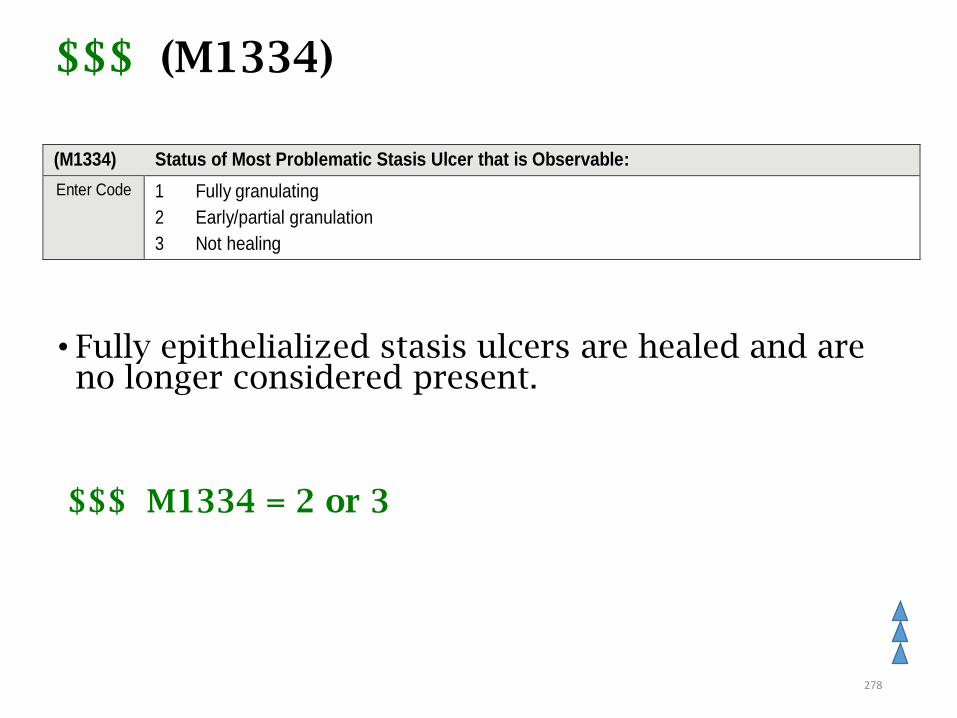
$$$ (M1334)
• Fully epithelialized stasis ulcers are healed and are no longer considered present.
$$$ M1334 = 2 or 3
(M1334) Status of Most Problematic Stasis Ulcer that is Observable:
Enter Code 1 Fully granulating
2 Early/partial granulation
3 Not healing
278
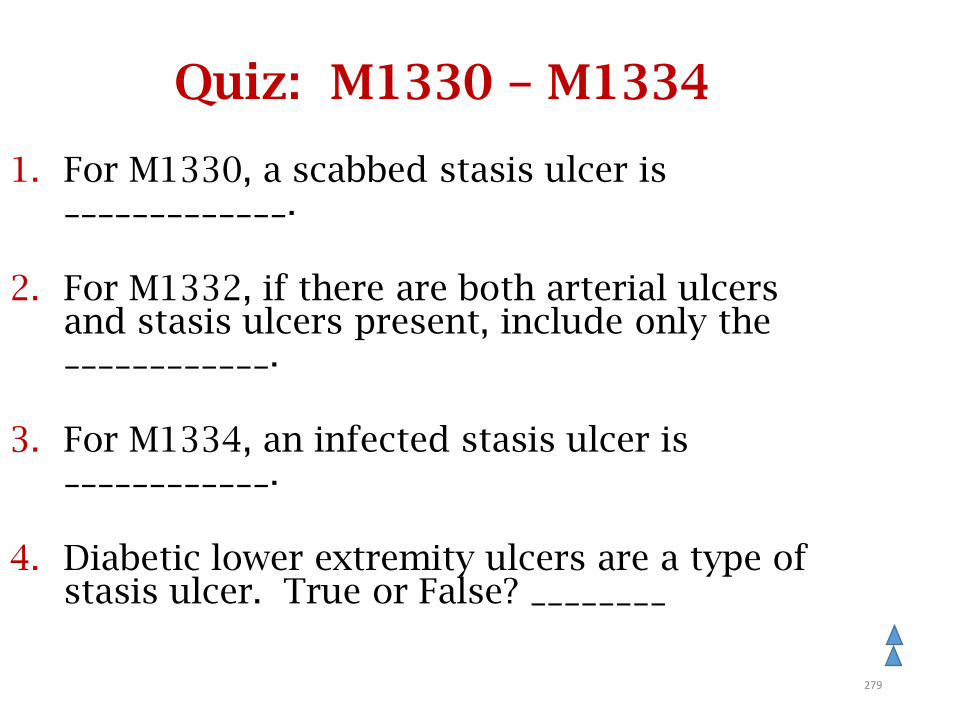
Quiz: M1330 – M1334
1. For M1330, a scabbed stasis ulcer is _____________.
2. For M1332, if there are both arterial ulcers and stasis ulcers present, include only the ____________.
3. For M1334, an infected stasis ulcer is ____________.
4. Diabetic lower extremity ulcers are a type of stasis ulcer. True or False? ________
279
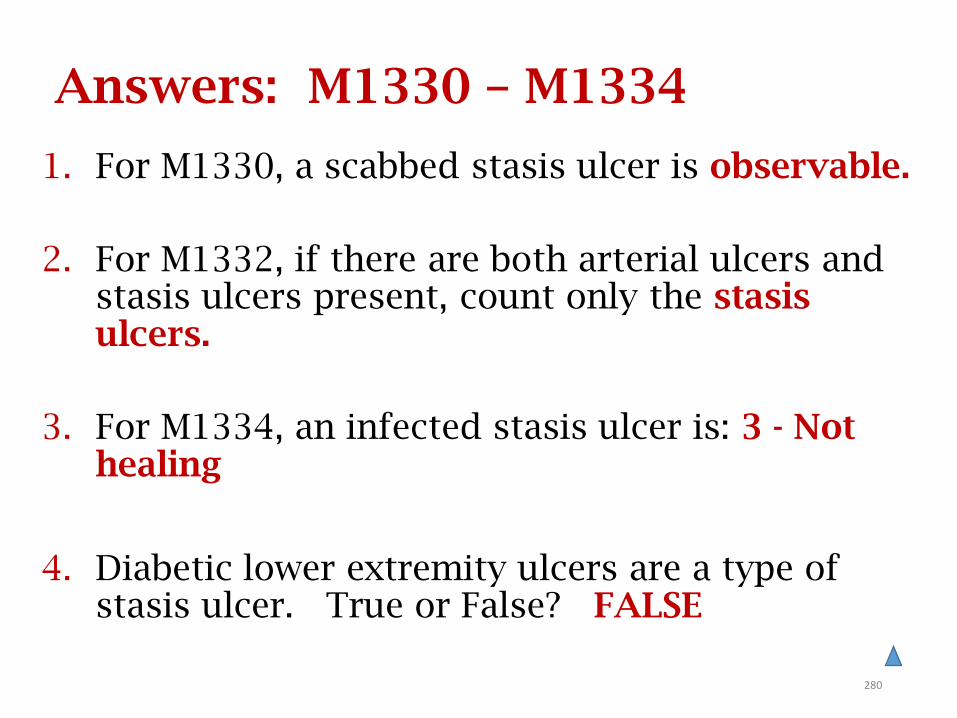
Answers: M1330 – M1334
1. For M1330, a scabbed stasis ulcer is observable.
2. For M1332, if there are both arterial ulcers and stasis ulcers present, count only the stasis ulcers.
3. For M1334, an infected stasis ulcer is: 3 - Not healing
4. Diabetic lower extremity ulcers are a type of stasis ulcer. True or False? FALSE
280
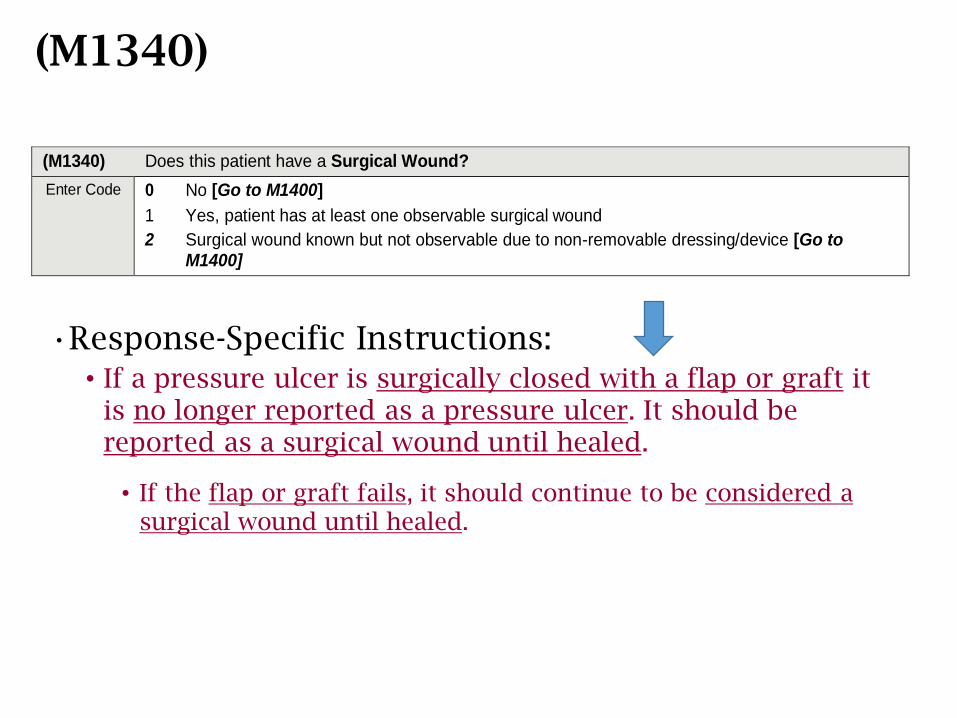
(M1340)
•Response-Specific Instructions:• If a pressure ulcer is surgically closed with a flap or graft it
is no longer reported as a pressure ulcer. It should be reported as a surgical wound until healed.
• If the flap or graft fails, it should continue to be considered a surgical wound until healed.
(M1340) Does this patient have a Surgical Wound?
Enter Code 0 No [Go to M1400]
1 Yes, patient has at least one observable surgical wound
2 Surgical wound known but not observable due to non-removable dressing/device [Go to M1400]
(M1340) Guidance
•A surgical site closed primarily (sutures, staples, or a chemical bonding agent) is generally described as a surgical wound until re-epithelialization has been present for approximately 30 days, unless the wound dehisces or presents signs of infection.
•If no evidence of dehiscence or infection, a wound becomes a scar 30 days after re-epithelialization.
•Incisional separation or disruption of wound edges of any surgical wound healing by primary intention results in a wound healing by secondary intention.
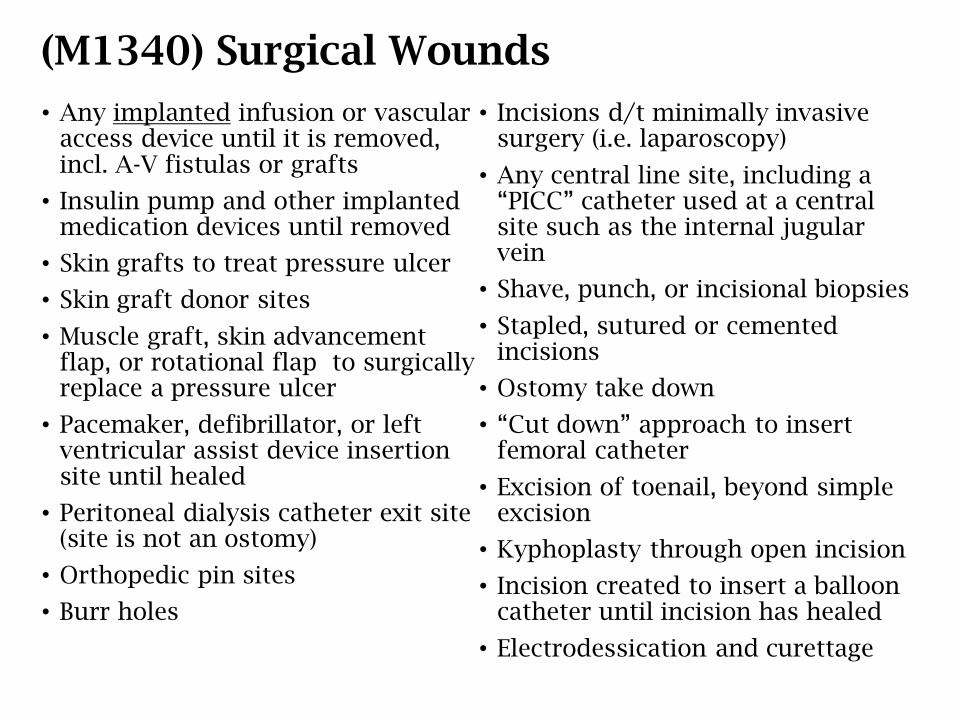
(M1340) Surgical Wounds
• Any implanted infusion or vascular access device until it is removed, incl. A-V fistulas or grafts
• Insulin pump and other implanted medication devices until removed
• Skin grafts to treat pressure ulcer
• Skin graft donor sites
• Muscle graft, skin advancement flap, or rotational flap to surgically replace a pressure ulcer
• Pacemaker, defibrillator, or left ventricular assist device insertion site until healed
• Peritoneal dialysis catheter exit site (site is not an ostomy)
• Orthopedic pin sites
• Burr holes
• Incisions d/t minimally invasive surgery (i.e. laparoscopy)
• Any central line site, including a “PICC” catheter used at a central site such as the internal jugular vein
• Shave, punch, or incisional biopsies
• Stapled, sutured or cemented incisions
• Ostomy take down
• “Cut down” approach to insert femoral catheter
• Excision of toenail, beyond simple excision
• Kyphoplasty through open incision
• Incision created to insert a balloon catheter until incision has healed
• Electrodessication and curettage
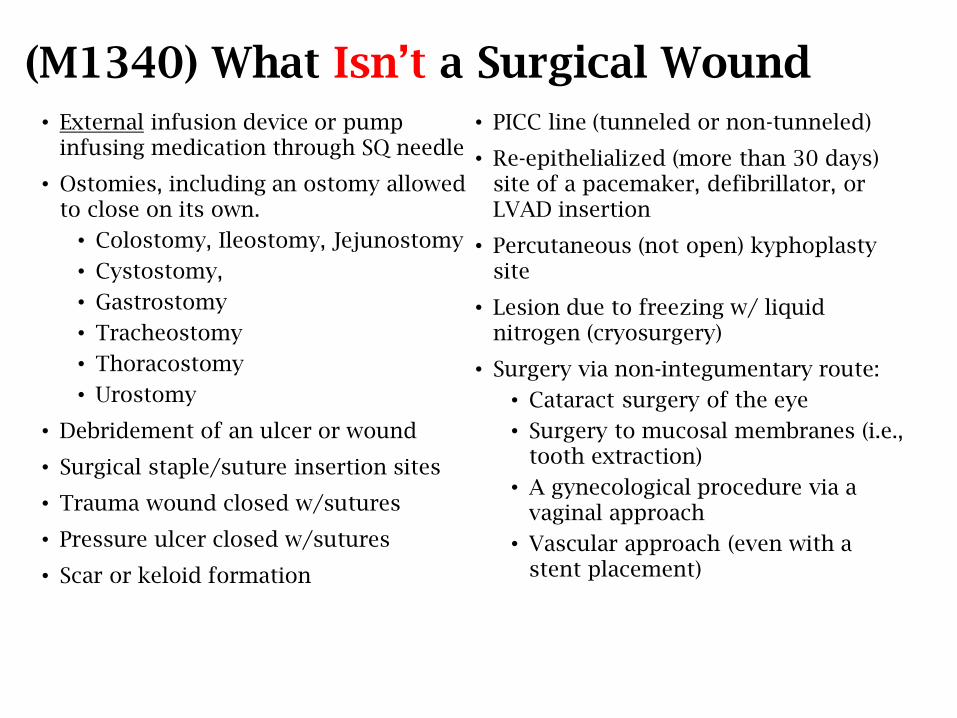
(M1340) What Isn’t a Surgical Wound• External infusion device or pump
infusing medication through SQ needle
• Ostomies, including an ostomy allowed to close on its own.
• Colostomy, Ileostomy, Jejunostomy
• Cystostomy,
• Gastrostomy
• Tracheostomy
• Thoracostomy
• Urostomy
• Debridement of an ulcer or wound
• Surgical staple/suture insertion sites
• Trauma wound closed w/sutures
• Pressure ulcer closed w/sutures
• Scar or keloid formation
• PICC line (tunneled or non-tunneled)
• Re-epithelialized (more than 30 days) site of a pacemaker, defibrillator, or LVAD insertion
• Percutaneous (not open) kyphoplasty site
• Lesion due to freezing w/ liquid nitrogen (cryosurgery)
• Surgery via non-integumentary route:
• Cataract surgery of the eye
• Surgery to mucosal membranes (i.e., tooth extraction)
• A gynecological procedure via a vaginal approach
• Vascular approach (even with a stent placement)
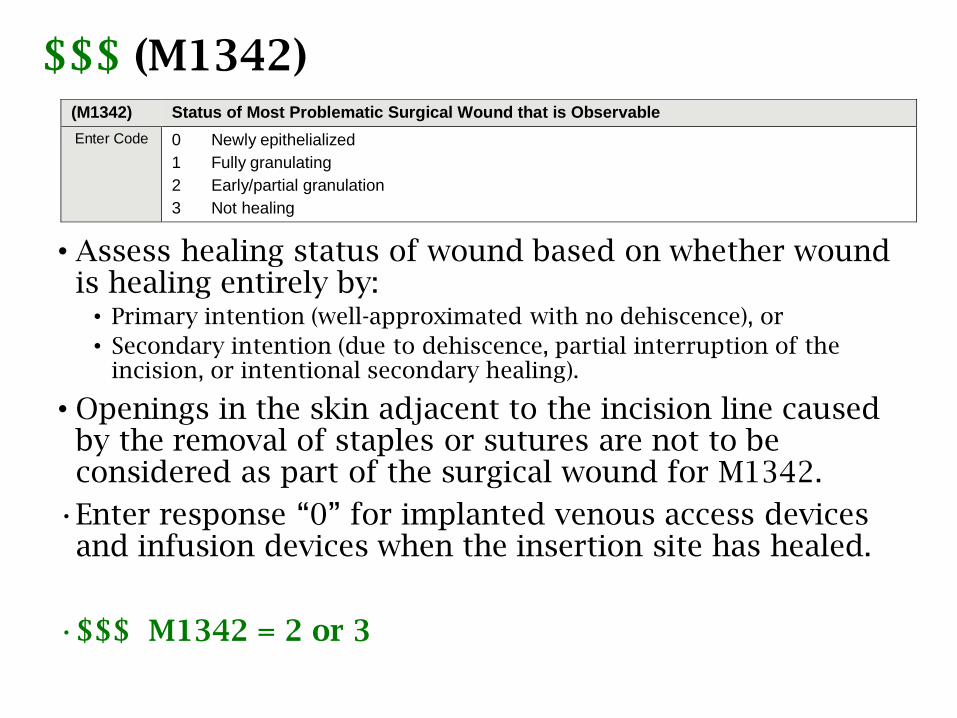
$$$ (M1342)
• Assess healing status of wound based on whether wound is healing entirely by:
• Primary intention (well-approximated with no dehiscence), or
• Secondary intention (due to dehiscence, partial interruption of the incision, or intentional secondary healing).
• Openings in the skin adjacent to the incision line caused by the removal of staples or sutures are not to be considered as part of the surgical wound for M1342.
•Enter response “0” for implanted venous access devices and infusion devices when the insertion site has healed.
•$$$ M1342 = 2 or 3
(M1342) Status of Most Problematic Surgical Wound that is Observable
Enter Code 0 Newly epithelialized
1 Fully granulating
2 Early/partial granulation
3 Not healing
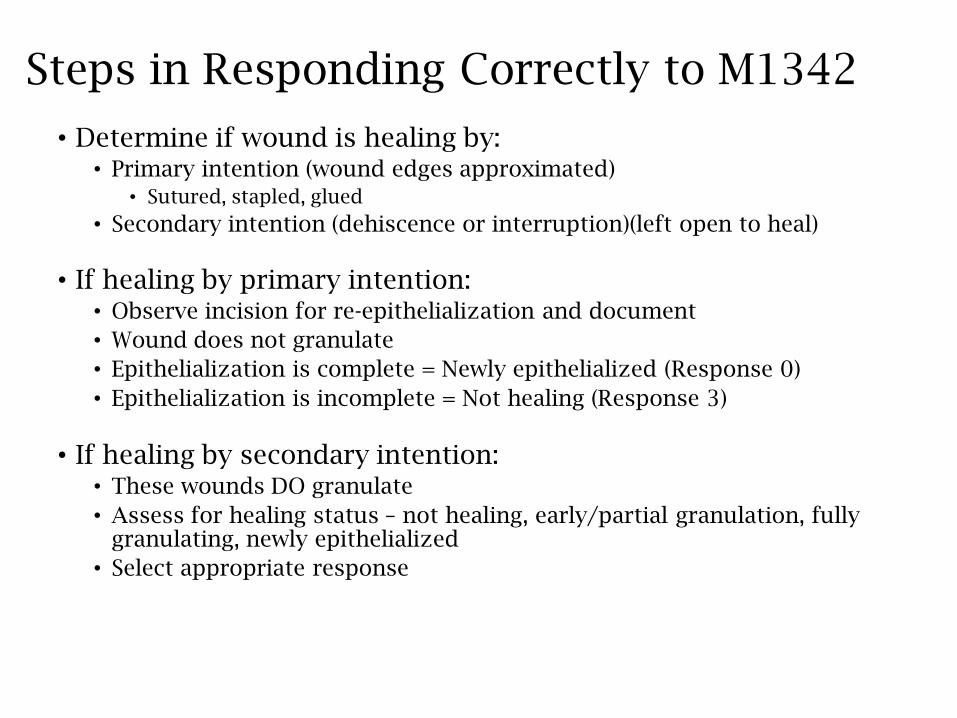
Steps in Responding Correctly to M1342
• Determine if wound is healing by:• Primary intention (wound edges approximated)
• Sutured, stapled, glued
• Secondary intention (dehiscence or interruption)(left open to heal)
• If healing by primary intention:• Observe incision for re-epithelialization and document
• Wound does not granulate
• Epithelialization is complete = Newly epithelialized (Response 0)
• Epithelialization is incomplete = Not healing (Response 3)
• If healing by secondary intention:• These wounds DO granulate
• Assess for healing status – not healing, early/partial granulation, fully granulating, newly epithelialized
• Select appropriate response
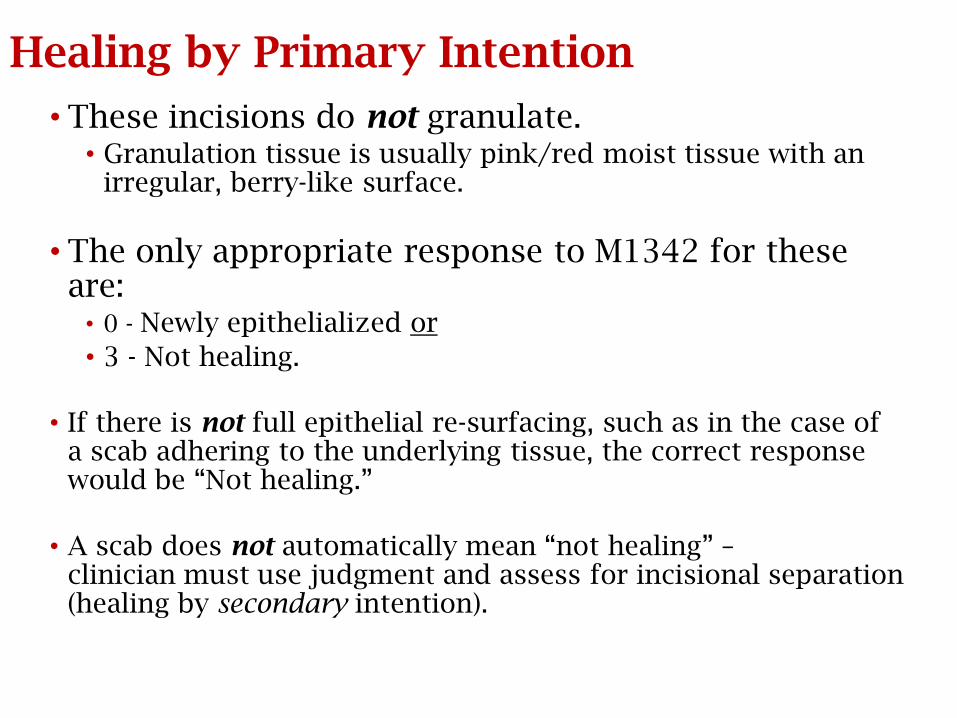
Healing by Primary Intention
• These incisions do not granulate.• Granulation tissue is usually pink/red moist tissue with an
irregular, berry-like surface.
• The only appropriate response to M1342 for these are:
• 0 - Newly epithelialized or
• 3 - Not healing.
• If there is not full epithelial re-surfacing, such as in the case of a scab adhering to the underlying tissue, the correct response would be “Not healing.”
• A scab does not automatically mean “not healing” –clinician must use judgment and assess for incisional separation (healing by secondary intention).
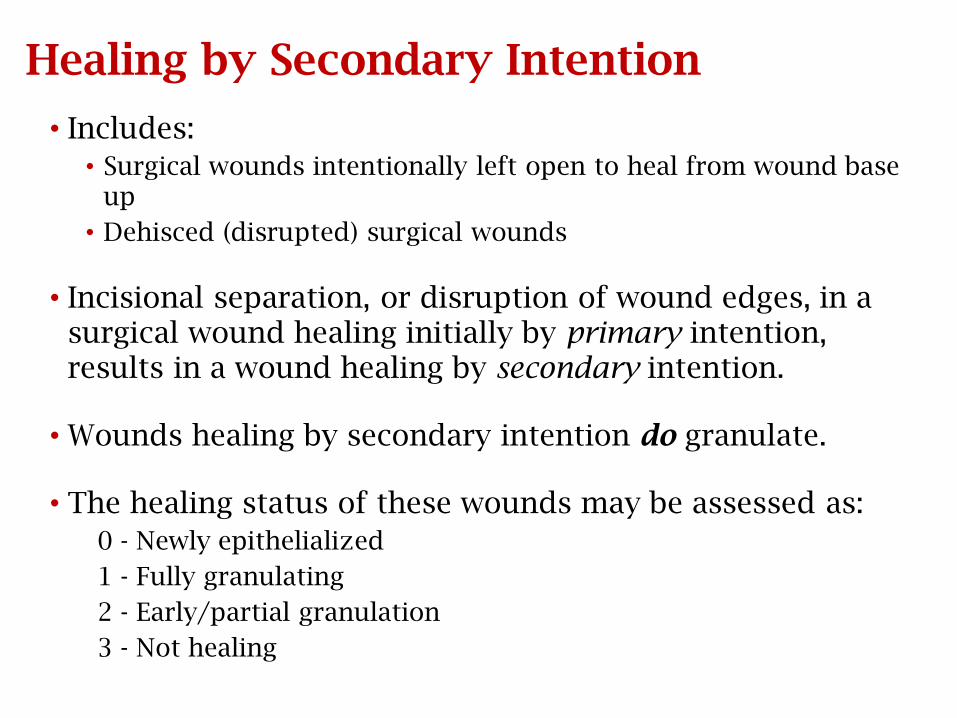
Healing by Secondary Intention
• Includes:
• Surgical wounds intentionally left open to heal from wound base up
• Dehisced (disrupted) surgical wounds
• Incisional separation, or disruption of wound edges, in a surgical wound healing initially by primary intention, results in a wound healing by secondary intention.
• Wounds healing by secondary intention do granulate.
• The healing status of these wounds may be assessed as:
0 - Newly epithelialized
1 - Fully granulating
2 - Early/partial granulation
3 - Not healing
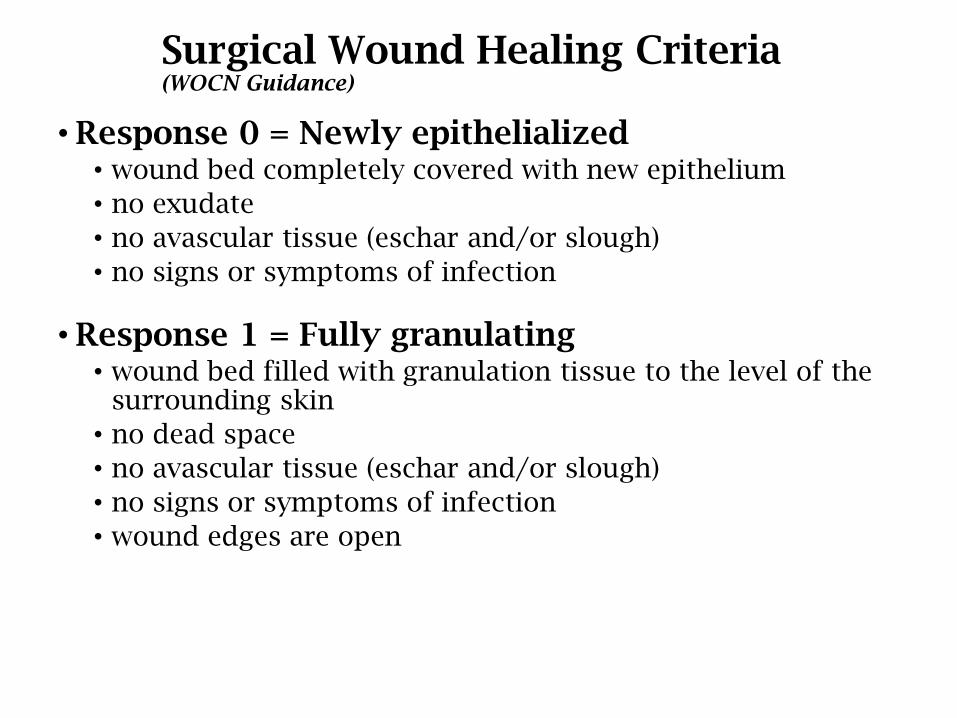
Surgical Wound Healing Criteria (WOCN Guidance)
• Response 0 = Newly epithelialized• wound bed completely covered with new epithelium
• no exudate
• no avascular tissue (eschar and/or slough)
• no signs or symptoms of infection
• Response 1 = Fully granulating• wound bed filled with granulation tissue to the level of the
surrounding skin
• no dead space
• no avascular tissue (eschar and/or slough)
• no signs or symptoms of infection
• wound edges are open
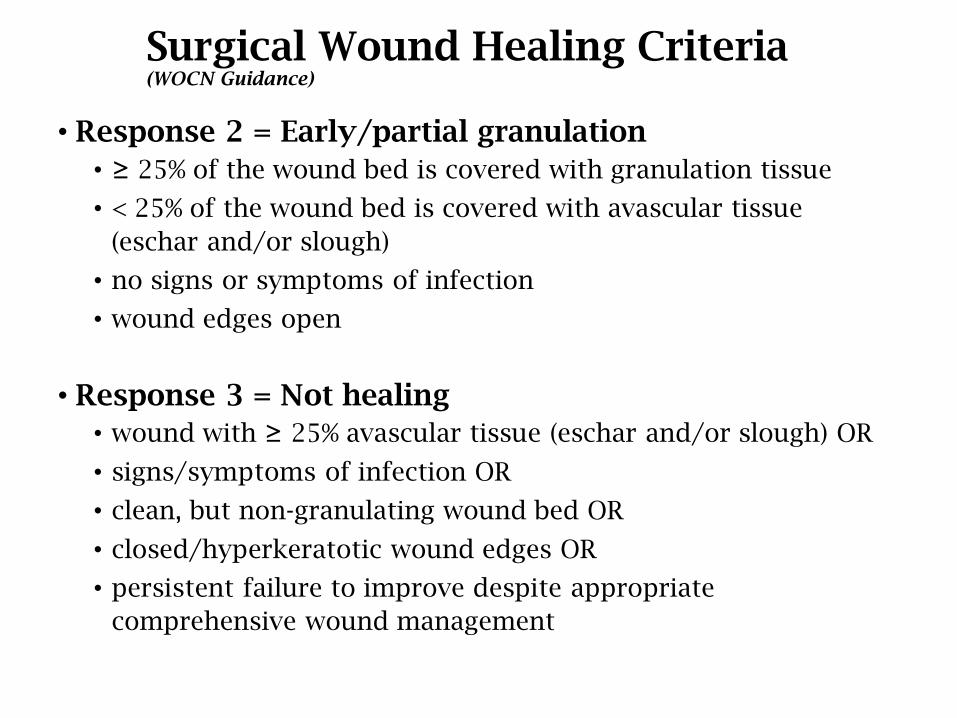
Surgical Wound Healing Criteria (WOCN Guidance)
• Response 2 = Early/partial granulation
• ≥ 25% of the wound bed is covered with granulation tissue
• < 25% of the wound bed is covered with avascular tissue
(eschar and/or slough)
• no signs or symptoms of infection
• wound edges open
• Response 3 = Not healing
• wound with ≥ 25% avascular tissue (eschar and/or slough) OR
• signs/symptoms of infection OR
• clean, but non-granulating wound bed OR
• closed/hyperkeratotic wound edges OR
• persistent failure to improve despite appropriate
comprehensive wound management
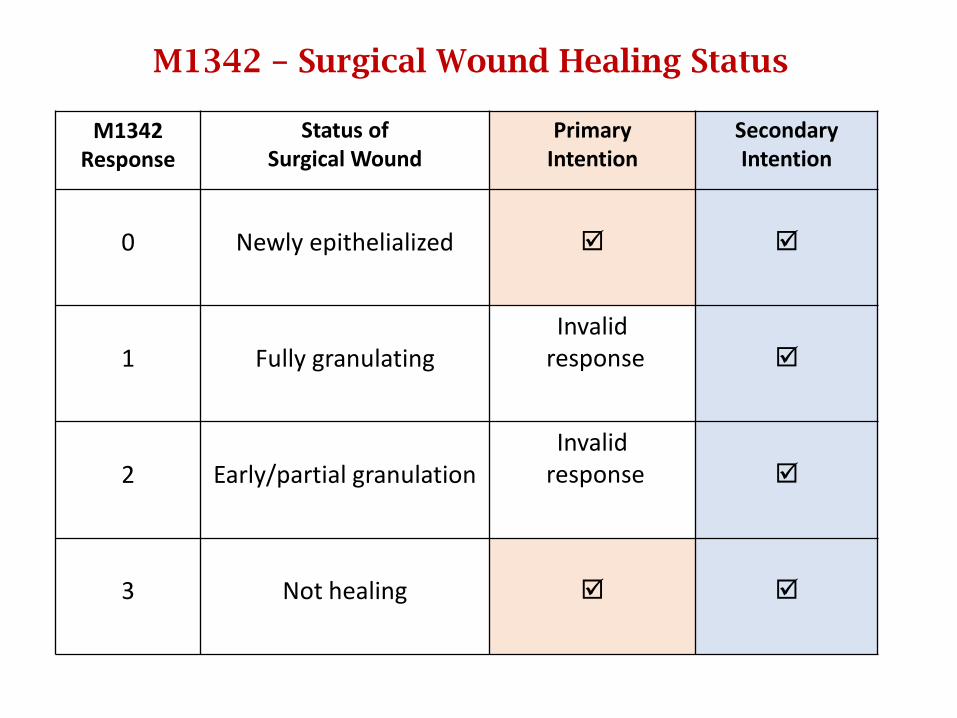
M1342 – Surgical Wound Healing Status
M1342 Response
Status of Surgical Wound
Primary Intention
SecondaryIntention
0 Newly epithelialized
1 Fully granulatingInvalid
response
2 Early/partial granulationInvalid
response
3 Not healing
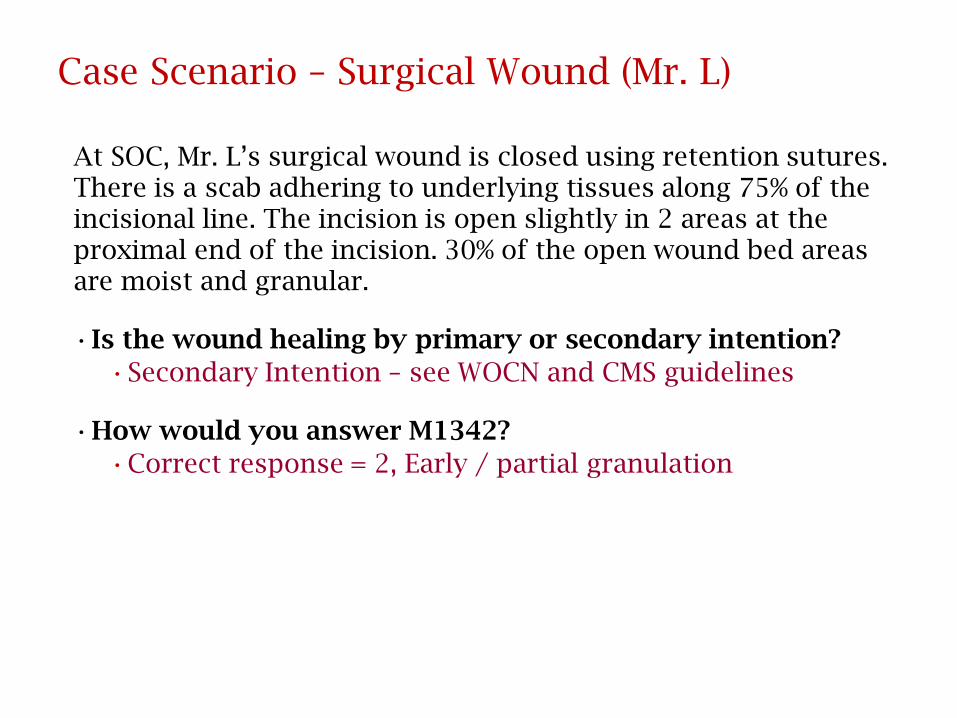
Case Scenario – Surgical Wound (Mr. L)
At SOC, Mr. L’s surgical wound is closed using retention sutures. There is a scab adhering to underlying tissues along 75% of the incisional line. The incision is open slightly in 2 areas at the proximal end of the incision. 30% of the open wound bed areas are moist and granular.
•Is the wound healing by primary or secondary intention?
•Secondary Intention – see WOCN and CMS guidelines
•How would you answer M1342?
•Correct response = 2, Early / partial granulation
Case Scenario – Surgical Wound (Mr. L)
• Mr. L’s surgical wound was noted to have re-epithelialized 2 weeks ago. The physician removed the retention sutures 3 days ago. The patient is being discharged because he is no longer homebound. At discharge, 4 of 16 former retention suture sites have become reddened. Two of the four are draining purulent material. The patient has been started on antibiotics. All 16 insertion points have scabs adhering to underlying tissue.
• What is the status of the most problematic surgical wound (M1342)?
• Newly epithelialized

Case Scenario – Surgical Wound (Mrs. H)
•Mrs. H is admitted for management of a COPD exacerbation. The patient also underwent an abdominal hysterectomy four days ago. At SOC the wound is clean, dry, and the edges are approximated but there is incomplete epithelial re-surfacing.
•Based on WOCN guidelines, how should you respond to M1342 (Status of most problematic observable surgical wound)?
•Response 3 (Not healing)
Scenario #1
Patient’s surgical incision is mostly approximated, but it is open slightly in 2 areas with some serous drainage. Minimal avascular tissue is present and open wound bed areas are smooth and red.
Is the wound healing by primary or secondary intention?
How would you answer M1342 (Status of most problematic (observable) surgical wound)?
0 - Newly epithelialized
1 - Fully granulating
2 - Early/partial granulation
3 - Not healing
Answers
Patient’s surgical incision is mostly approximated but it is open slightly in 2 areas with some serous drainage. Minimal avascular tissue is present and open wound bed areas are smooth and red.
Is the wound healing by primary or secondary intention?
Secondary Intention
How would you answer M1342?
Response 3 (Not healing) – smooth and red tissue is not granulation tissue
Strategies for Getting Wounds Right
Pay attention to item intent and skip patterns.
Know what the guidance is:Chapter 3 wound items
WOCN Guidance on OASIS Integumentary Items
CMS Q&As
Use tools to ensure you know what to answer and how to answer it correctly.
Re-educate yourself or others on wounds until you can ensure competency.
Education must be ongoing!
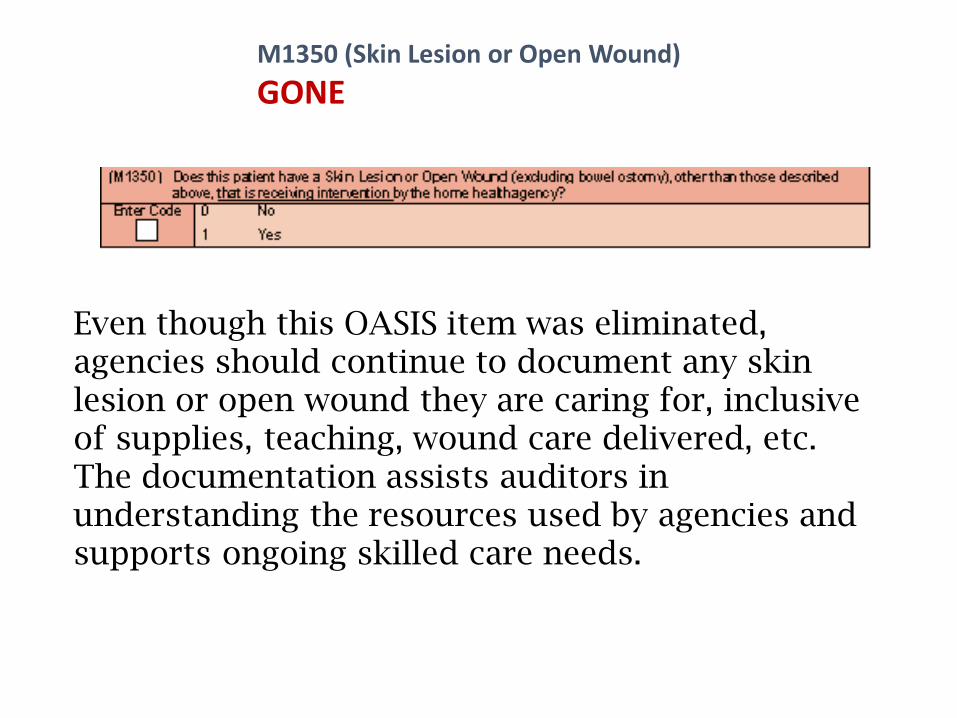
M1350 (Skin Lesion or Open Wound)
GONE
Even though this OASIS item was eliminated, agencies should continue to document any skin lesion or open wound they are caring for, inclusive of supplies, teaching, wound care delivered, etc. The documentation assists auditors in understanding the resources used by agencies and supports ongoing skilled care needs.
Respiratory StatusM1400
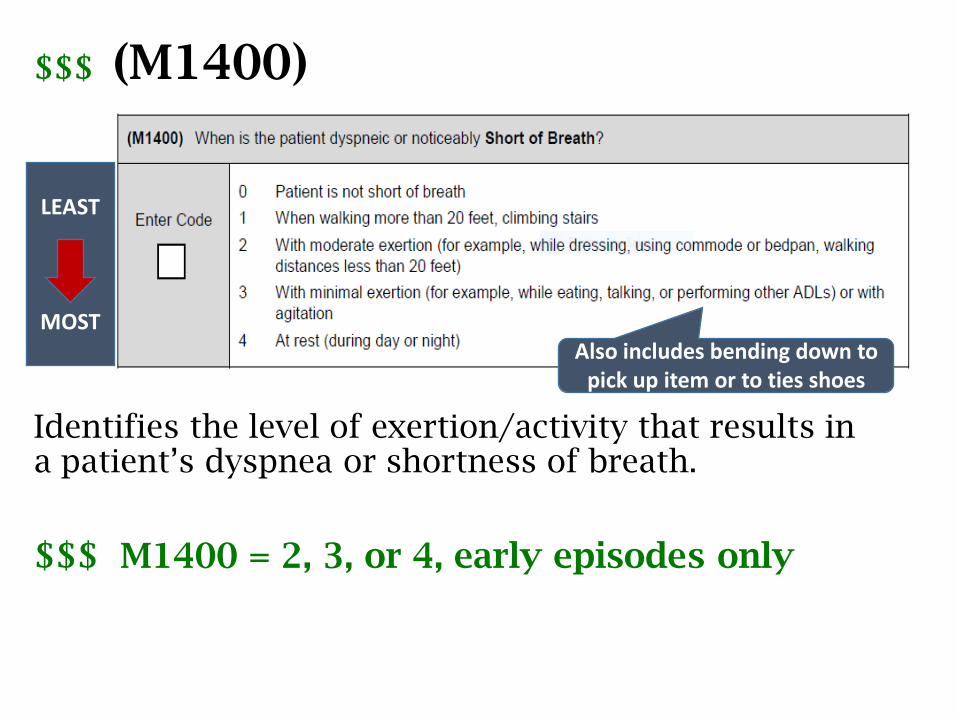
$$$ (M1400)
Identifies the level of exertion/activity that results in a patient’s dyspnea or shortness of breath.
$$$ M1400 = 2, 3, or 4, early episodes only
Also includes bending down to pick up item or to ties shoes
LEAST
MOST
M1400: Guidance
• If the patient uses oxygen:• Continuously – assess with oxygen ON.
• Intermittently – assess with oxygen OFF.
• Response is based on patient’s actual use of oxygen in the home, not on the physician’s oxygen order.
• For a chairfast or bedbound patient:• Evaluate the level of exertion required to produce SOB.
• Assess for dyspnea while performing ADLs, transferring or wheeling self, changing positions, or at rest.
M1400: Dyspnea
• Does the patient wear oxygen? Did you put it on the meds list?
• If oxygen worn at night when sleeping due to dyspnea: score is automatically [4] – this is the worst possible condition
• If a dx of CHF or COPD is present and they have oxygen – be careful about score of [0] – this is not typical
• Really listen to the patient when they are talking, moving around. Listen for frequent pauses in the conversation – are they catching a breath?
Elimination StatusM1600 – M1630
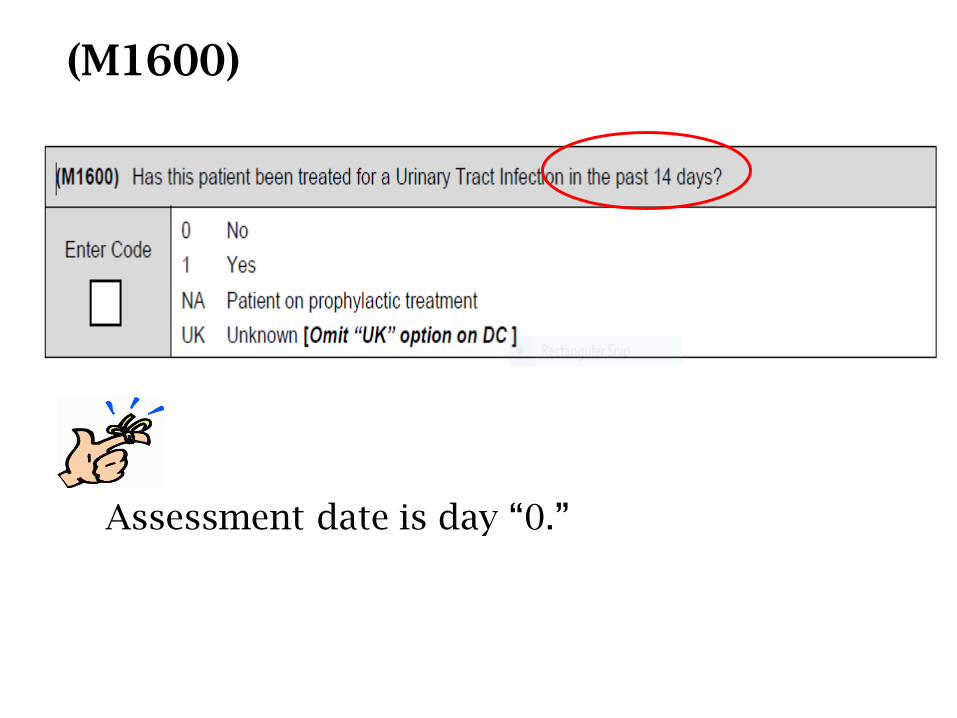
(M1600)
Assessment date is day “0.”
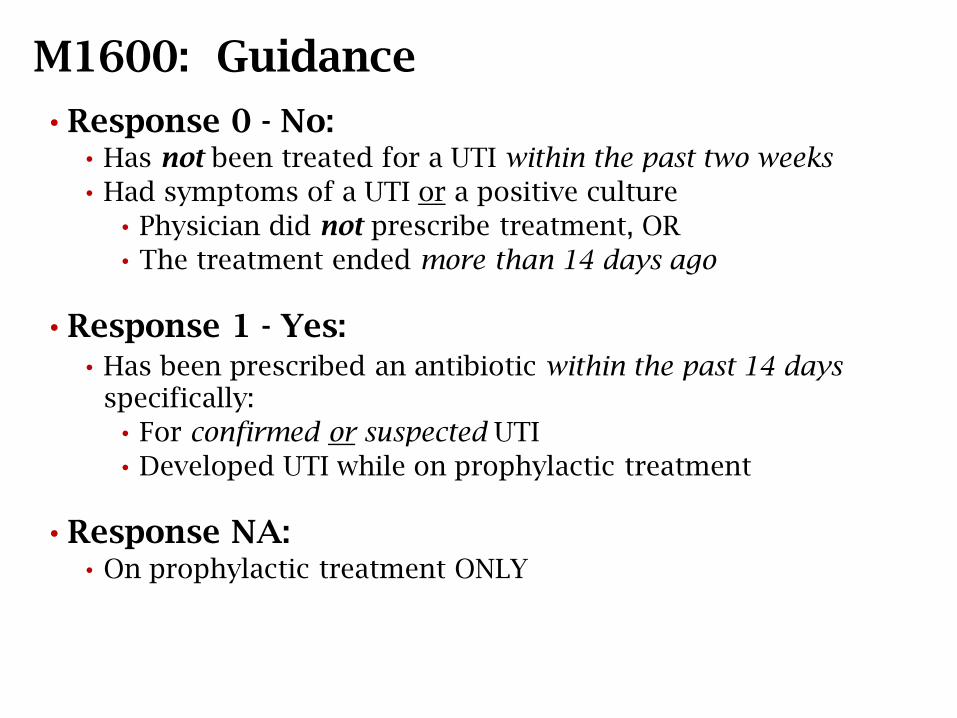
M1600: Guidance
• Response 0 - No:• Has not been treated for a UTI within the past two weeks
• Had symptoms of a UTI or a positive culture
• Physician did not prescribe treatment, OR
• The treatment ended more than 14 days ago
• Response 1 - Yes:• Has been prescribed an antibiotic within the past 14 days
specifically:
• For confirmed or suspected UTI
• Developed UTI while on prophylactic treatment
• Response NA: • On prophylactic treatment ONLY
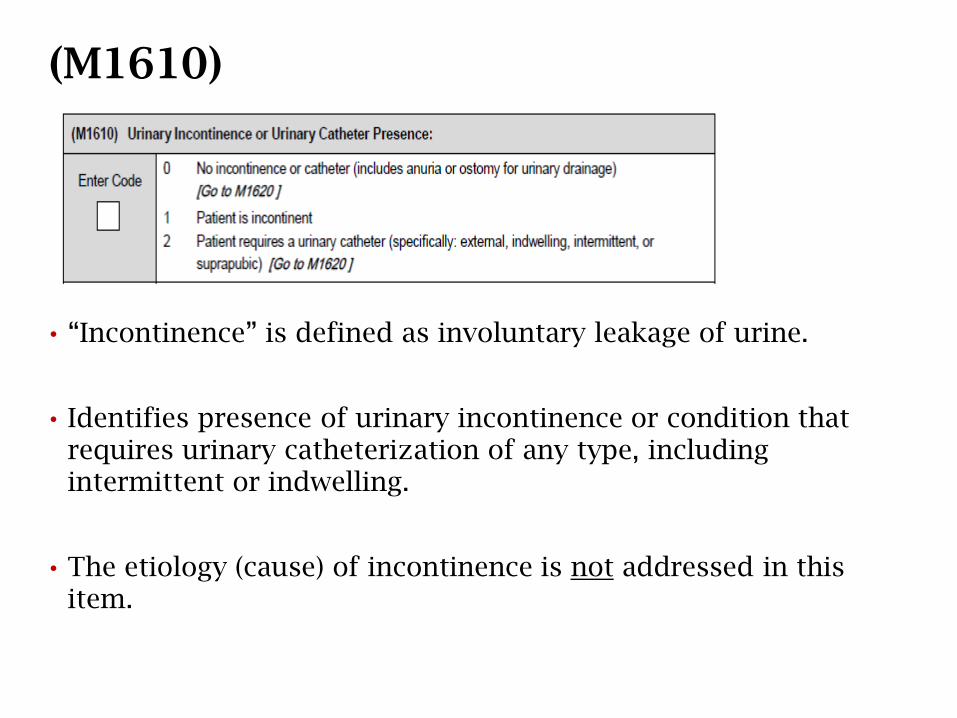
• “Incontinence” is defined as involuntary leakage of urine.
• Identifies presence of urinary incontinence or condition that requires urinary catheterization of any type, including intermittent or indwelling.
• The etiology (cause) of incontinence is not addressed in this item.
(M1610)
M1610: Guidance
• A leaking urinary appliance or drainage device is notincontinence.
• A catheter solely used for irrigation of the bladder or instillation of an antibiotic is not reported in this item.
• If catheter is discontinued or both inserted anddiscontinued during the comprehensive assessment, Response 0 or 1 is appropriate, depending on whether or not the patient is continent.
M1610: Responses• Response 0 - No incontinence, if the patient has:
• Anuria
• A urinary ostomy (e.g., an ileal conduit)
• A pouched urinary diversion (ileal conduit, urostomy, ureterostomy, nephrostomy), with or without a stoma
• Response 1 - Incontinent at any time• Includes patient on timed-voiding program
• Response 2 - Requires urinary catheter Specifically: (indwelling, external, suprapubic)
• Intermittent or continuous use of catheter for any reason –e.g., retention, incontinence
• Includes when patient is both incontinent and also requires a catheter
Responses (cont.)
Select Response 2 - Requires urinary catheter, if:• A catheter is inserted and left in place during the
comprehensive assessment, but not inserted and removed.
• A catheter or tube used to drain urine, even if intermittent, unless it is capped, with no plan to drain urine.
• A penis pouch is used – considered to be a device “like” an external catheter:
For example, a patient with a retracted penis who cannot effectively wear an external catheter.
Scenario: M1600 and M1610
Patient is admitted to home health following hospitalization for pneumonia. He complained of burning with urination, urinary frequency, and said his urine has a strong odor. The assessing clinician contacted the physician, who ordered a catheterization for a urine culture and an antibiotic for a possible UTI. He denied having any incontinence.
How would you score M1600 (Has this patient been treated for a Urinary Tract Infection in the past 14 days?) and M1610 (Urinary Incontinence or Urinary Catheter Presence)?
Answers: M1600 and M1610Patient admitted to home health following hospitalization for pneumonia. He complained of burning with urination, urinary frequency, and said his urine has a strong odor. The assessing clinician contacted the physician, who ordered a catheterization for a urine culture and an antibiotic for a possible UTI. He denied having any incontinence.
M1600 = Response 1 - YesThe patient was prescribed an antibiotic within the past 14 days specifically for a suspected UTI. The day of assessment counts, since the antibiotic was ordered as a result of the assessment.
M1610 = Response 0 - No incontinence or catheter. A catheter was inserted to obtain a urine culture and was then discontinued during the comprehensive assessment, and the patient denied being incontinent.
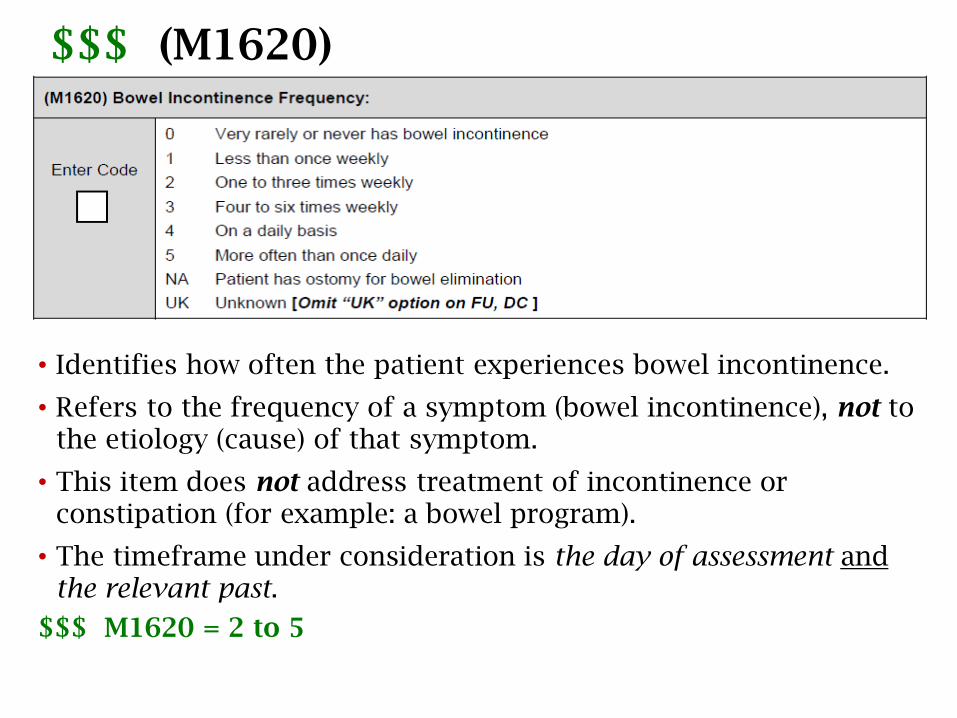
$$$ (M1620)
• Identifies how often the patient experiences bowel incontinence.
• Refers to the frequency of a symptom (bowel incontinence), not to the etiology (cause) of that symptom.
• This item does not address treatment of incontinence or constipation (for example: a bowel program).
• The timeframe under consideration is the day of assessment andthe relevant past.
$$$ M1620 = 2 to 5
$$$ M1620 = 2 to 5
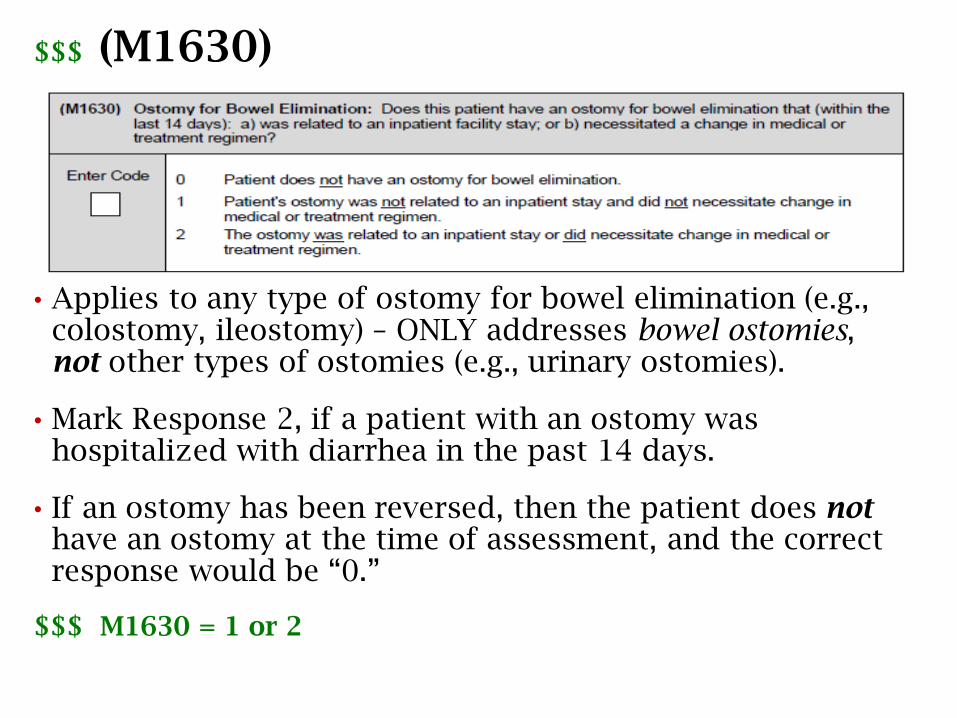
$$$ (M1630)
• Applies to any type of ostomy for bowel elimination (e.g., colostomy, ileostomy) – ONLY addresses bowel ostomies, not other types of ostomies (e.g., urinary ostomies).
• Mark Response 2, if a patient with an ostomy was hospitalized with diarrhea in the past 14 days.
• If an ostomy has been reversed, then the patient does nothave an ostomy at the time of assessment, and the correct response would be “0.”
$$$ M1630 = 1 or 2
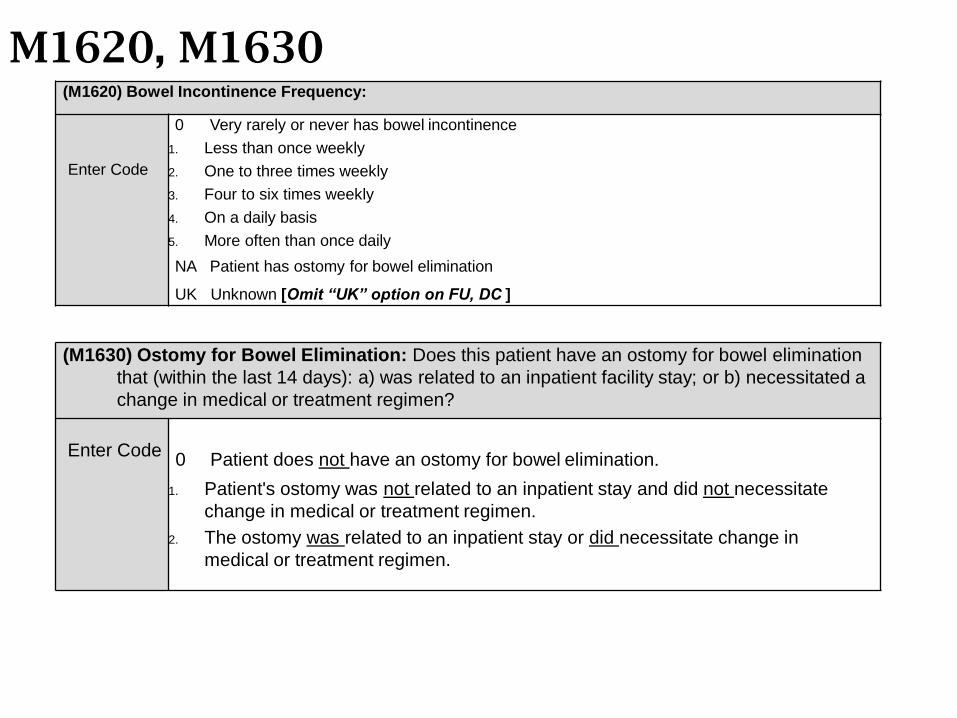
M1620, M1630(M1620) Bowel Incontinence Frequency:
Enter Code
0 Very rarely or never has bowel incontinence
1. Less than once weekly
2. One to three times weekly
3. Four to six times weekly
4. On a daily basis
5. More often than once daily
NA Patient has ostomy for bowel elimination
UK Unknown [Omit “UK” option on FU, DC ]
(M1630) Ostomy for Bowel Elimination: Does this patient have an ostomy for bowel elimination
that (within the last 14 days): a) was related to an inpatient facility stay; or b) necessitated a
change in medical or treatment regimen?
Enter Code0 Patient does not have an ostomy for bowel elimination.
1. Patient's ostomy was not related to an inpatient stay and did not necessitate
change in medical or treatment regimen.
2. The ostomy was related to an inpatient stay or did necessitate change in
medical or treatment regimen.
Scenario: M1620 and M1630
Patient was referred to home health from the hospital for continued treatment of an infected colostomy.
How should the clinician score M1620 (Bowel Incontinence Frequency) and M1630 (Ostomy for Bowel Elimination)?
Answers: M1620 and M1630
Patient was referred to home health from the hospital for continued treatment of an infected colostomy.
How should the clinician score M1620 and M1630?
M1620 = Response NA - Patient has ostomy for bowel elimination
M1630 = Response 2 - The ostomy was related to an inpatient stay or did necessitate change in medical or treatment regimen.
Neuro/Emotional/Behavioral StatusM1700 – M1745
M1700-M1745: Guidance
Assessment of the neuro/emotional/behavioral items includes:
• Observation of patient during assessment process:
− Posture and motor behavior
− Manner of dress
− Facial expressions
− Grooming and personal hygiene
− Affect and manner of speech
• Obtain information from patient, family, caregivers, physician, past health history
• Report any confusion or anxiety within last 14 days.
M1700-M1745: Guidance
• “Non-responsive” means the patient is unable to respond or responds in a way that you’re unable to make a clinical judgment. Attempt to obtain information from the caregiver or other source.
• Time span for assessment is specified in specific items.
Physician must confirm diagnoses associated with items!
What is confusion?
• “Confusion” is defined in Mosby's Medical Dictionary as "a mental state characterized by disorientation regarding time, place, person, or situation. It causes bewilderment, perplexity, lack of orderly thought, and inability to choose or act decisively and perform the activities of daily living. It is usually symptomatic of an organic mental disorder, but it may accompany severe emotional stress and various psychological disorders.”
• A “cognitive impairment,” such as forgetfulness, learning disabilities, concentration difficulties, or decreased intelligence, might NOT result in confusion.
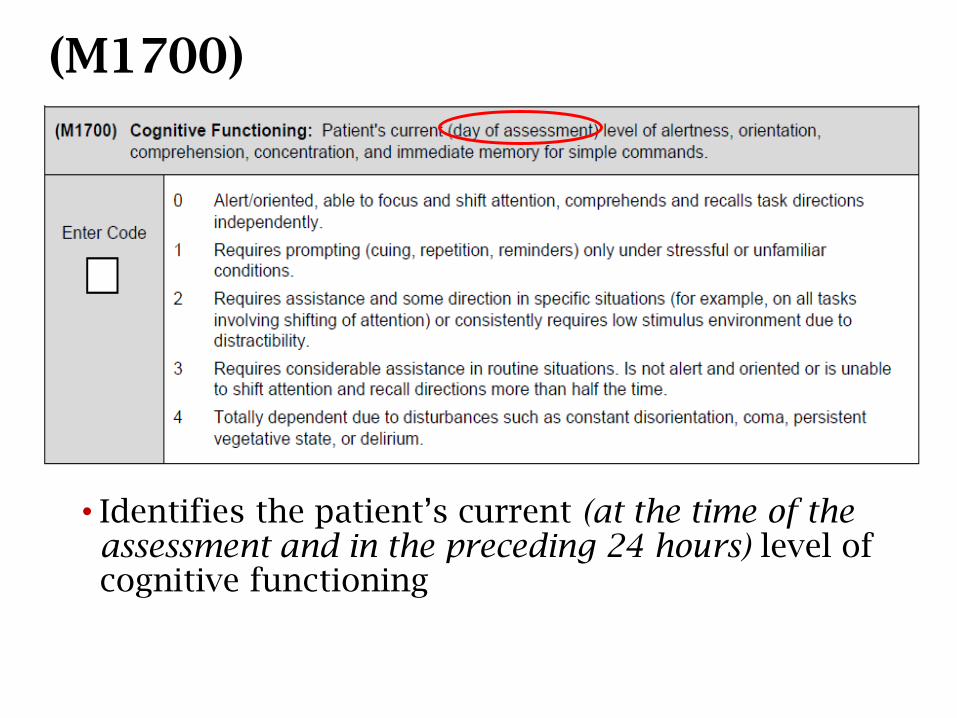
(M1700)
• Identifies the patient’s current (at the time of the assessment and in the preceding 24 hours) level of cognitive functioning
M1700: (cont.)
•When assessing, evaluate the amount of supervision and care the patient requires due to cognitive deficits.
•Be cognizant of repeating statements you make, if the patient asks you to write something down because they’ll forget, instructing on exercises they were taught in the hospital, etc. Remember, YOU being in the home is the “stressful or unfamiliar condition”.
•CMS feels that a score of [0] does not support repetitive teaching plans.
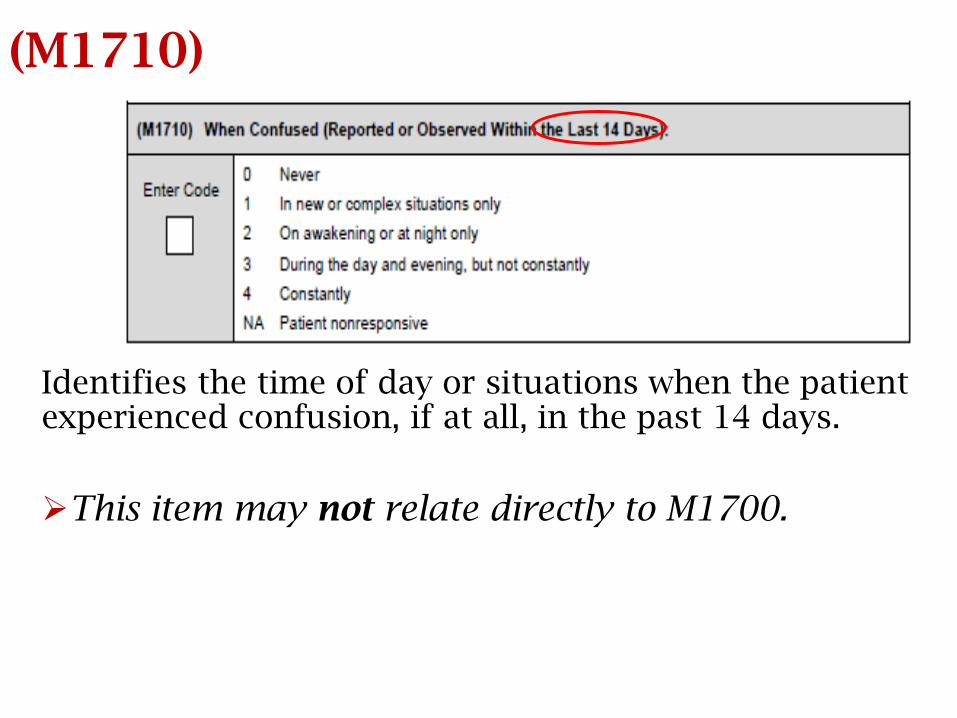
(M1710)
Identifies the time of day or situations when the patient experienced confusion, if at all, in the past 14 days.
This item may not relate directly to M1700.
M1700 and/or M1710?
• If a patient is confused on the day of the assessment, report it both in M1700 and M1710.
• If a patient is NOT confused on the day of assessment, but experienced confusion during the prior 14 days, report it only in M1710.
• If, on the day of the assessment, a patient has a cognitive impairment that does NOT result in confusion, report it only in M1700.
• For example: forgetfulness, learning disabilities, concentration difficulties, decreased intelligence
M1710: Responses
• Responses 1 - 4 are selected if the patient has experienced confusion, and each response represents a worsening of the confusion.
• Response 1 is selected when the patient's confusion is isolated to a new or a complex situation – e.g., when there is a new caregiver or when a new procedure is taught.
• Response 2, 3, and 4 are selected when confusion occurs without the stimulus of a new or complex situation, or when confusion persists after the new situation is routine.
• Responses 2, 3 & 4 differ from each other based on the time when the confusion occurred.
M1710 and M1720: Nonresponsive
• “Nonresponsive” means that the patient is unable to respond or responds in a way that you cannot make a clinical judgment about the patient’s level of orientation.
• If the patient is nonresponsive at the time of assessment, report whether there was any confusion during the past 14 days, if this information can be elicited from the caregiver or other source.
• If the patient is nonresponsive at the time of assessment and the information cannot be elicited, enter “NA - Patient nonresponsive.”
• Per CMS, a patient who simply refuses to answer questions should not automatically be considered “unresponsive.” The clinician should complete the comprehensive assessment and select the correct response based on observation and caregiver interview.
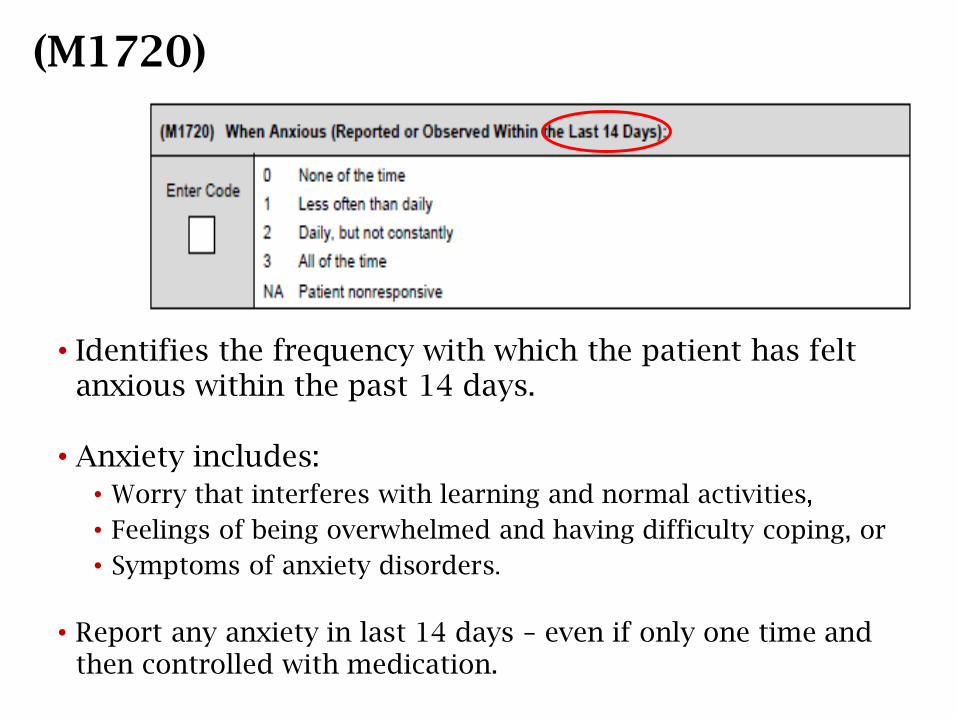
(M1720)
• Identifies the frequency with which the patient has felt anxious within the past 14 days.
• Anxiety includes:
• Worry that interferes with learning and normal activities,
• Feelings of being overwhelmed and having difficulty coping, or
• Symptoms of anxiety disorders.
• Report any anxiety in last 14 days – even if only one time and then controlled with medication.
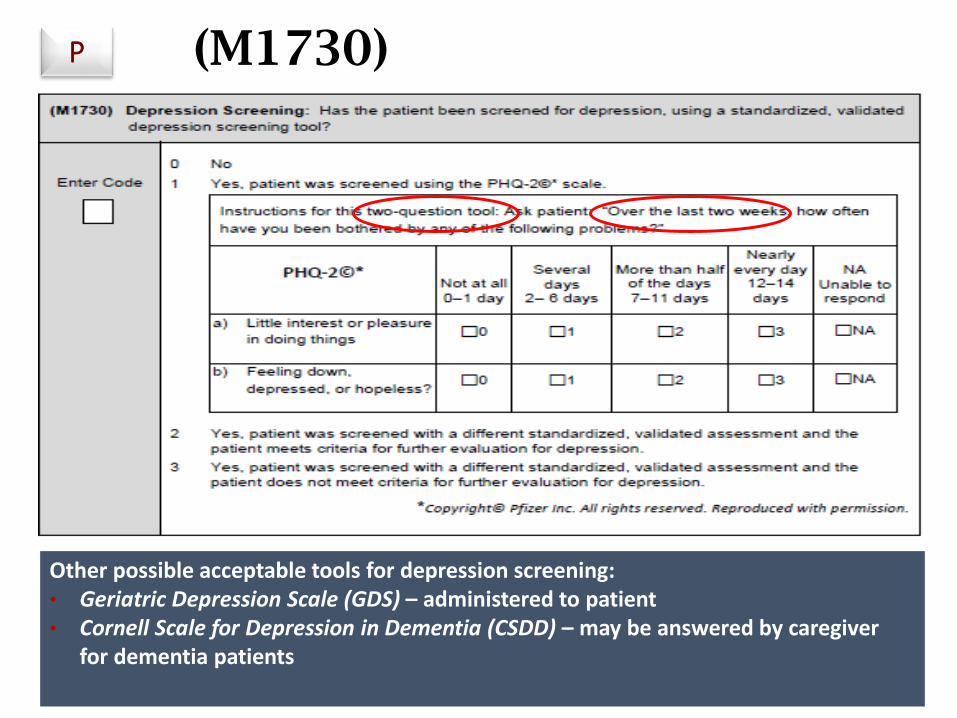
(M1730)P
Other possible acceptable tools for depression screening:• Geriatric Depression Scale (GDS) – administered to patient• Cornell Scale for Depression in Dementia (CSDD) – may be answered by caregiver
for dementia patients
Guidance for Depression Screening
Identifies if the home health agency screened the patient for depression using a standardized depression screening tool, which MUST:
• Include a standard response scale;
• Be administered to patient who is cognitively intact and physically able;
• Be appropriately administered, as indicated in the instructions; and
• Be administered by the clinician completing the OASIS in the time frame specified by CMS.
• Questions MUST be answered by the patient!
• A score of 3 or greater warrants further depression screening.
• Document and report to physician screening results, and include any ordered depression-related interventions in the POC.
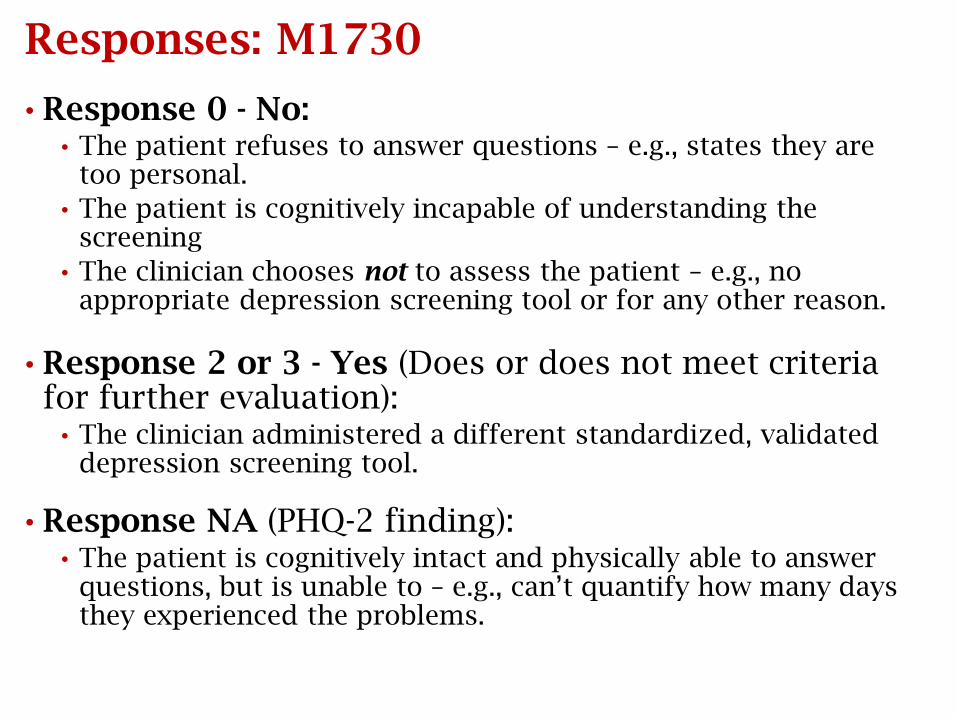
Responses: M1730
• Response 0 - No:• The patient refuses to answer questions – e.g., states they are
too personal.
• The patient is cognitively incapable of understanding the screening
• The clinician chooses not to assess the patient – e.g., no appropriate depression screening tool or for any other reason.
• Response 2 or 3 - Yes (Does or does not meet criteria for further evaluation):
• The clinician administered a different standardized, validated depression screening tool.
• Response NA (PHQ-2 finding):• The patient is cognitively intact and physically able to answer
questions, but is unable to – e.g., can’t quantify how many days they experienced the problems.
Scenario: M1730
Patient is sitting in a chair during her assessment and does not readily respond to any questions, including the ones on the PHQ-2. She seems tired, but is cognitively alert and oriented. Her daughter, who is her caregiver, says that her mother has been depressed and seems to have just given up.
How should the clinician answer M1730?
Answer: M1730
Patient is sitting in a chair during her assessment and does not readily respond to any questions, including the ones on the PHQ-2. She seems tired, but is cognitively alert and oriented. Her daughter, who is her caregiver, says that her mother has been depressed and seems to have just given up.
How should the clinician answer M1730?
Response 0 - No
Patient did not respond to PHQ-2 questions, and the response cannot be based on what anyone else says.
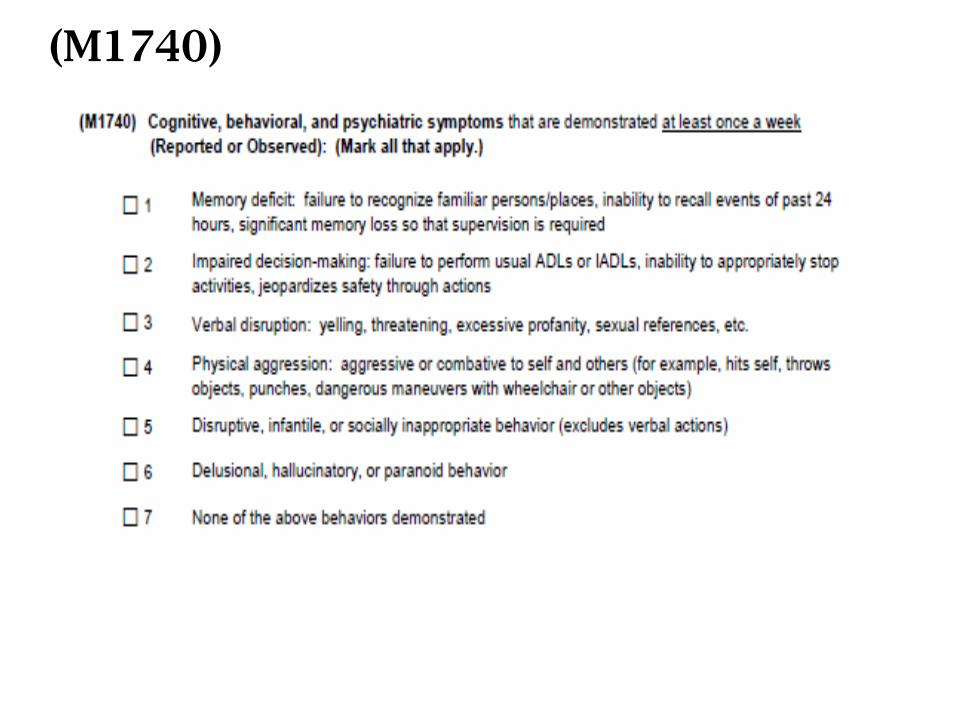
(M1740)
Time Frame for M1740
• The time frame under consideration for M1740 is defined in the wording of the item – "at least once a week,” which means that:
• A behavior was demonstrated multiple times in the recent, relevant past; and
• The frequency of the occurrence was at least one time a week prior to and including the day of assessment.
• The assessing clinician will determine "recent, relevant past" based on the patient/caregiver interview, referral information, assessment findings, diagnoses and recent history of medical treatment and its effectiveness.
M1740: Guidance
• Identifies specific behaviors associated with significantneurological, developmental, behavioral, or psychiatric disorders.
• May be determined either by diagnosis and/or in the assessing clinician’s clinical judgment.
• Include behaviors which are severe enough to:
• Make the patient unsafe to self or others;
• Cause considerable stress to the caregivers; or
• Require supervision or intervention.
• Behaviors may be observed by the clinician or reported by the patient, family, or others.
M1740: Guidance
•Score [1]: Do they have memory loss? Need supervision for safety? Are you grateful they do not live alone?
•Score [2]: smokes while on O2, forgets/refuses to use a.d., non-compliant with meds/treatment regime, won’t check their BS or follow prescribed diet, etc., and does not comprehend/appreciate the consequences of their actions.
It is not the intent of M1740 to report non-adherence or risky choices made by cognitively intact patients.
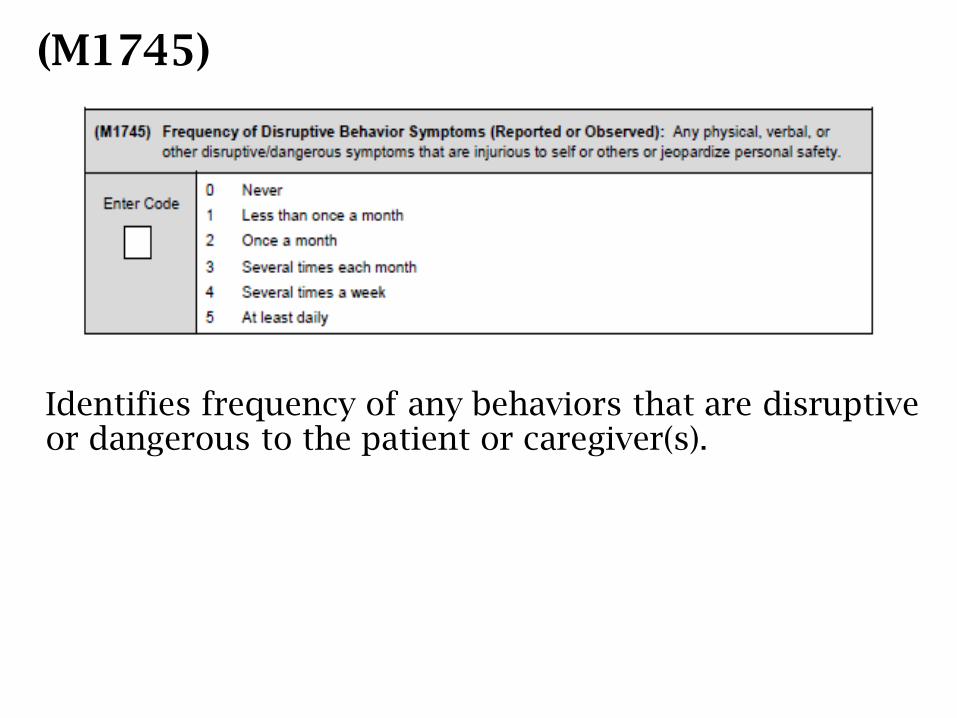
(M1745)
Identifies frequency of any behaviors that are disruptive or dangerous to the patient or caregiver(s).
M1745: Guidance
• Consider if the patient has any problematic behaviors – not just those listed in M1740 – which jeopardize or could jeopardize the safety and well-being of the patient or caregiver, such as:• wandering, sleeplessness, sun-downing, agitation, aggression,
combativeness, getting lost in familiar places, etc.
• Then, consider how frequently these behaviors occur.
• May be determined either by diagnosis and/or in the assessing clinician’s clinical judgment.
• Behaviors can be observed by the clinician orreported by the patient, family, or others.
Hoarding Disorder
If a hoarding disorder with associated behaviors results in concern for the patient and/or caregiver's safety, one or both of these M1740 responses may best describe it:
• [2] - Impaired decision-making: failure to perform usual ADLs or IADLs, inability to appropriately stop activities, jeopardizes safety through actions
• [5] - Disruptive, infantile, or socially inappropriate behavior (excludes verbal actions).
M1740 and M1745
• M1740 and M1745 are not directly linked to one another –may be behaviors reported in one and not the other.
• For example, a patient may express excessive profanity or sexual references that cause considerable stress to the caregivers and be reported in M1740, but, in the clinician's judgment, the behavior does not jeopardize the safety and well-being of the patient or caregiver, therefore is notreported in M1745.
• Answer each question individually. • M1740 lists specific behaviors associated with significant
neurological, developmental, behavioral or psychiatric disorders and asks if they are demonstrated at least once a week.
• M1745 is not reporting on a specific list of behaviors, but rather any behaviors that are disruptive or dangerous to the patient or caregivers.
M1740 and M1745
• The environment in which the patient lives and the skills of the caregiver may impact the scoring of M1740 and M1745.
• For example, patients with dementia may exhibit a number of behaviors listed in M1740, but may not be reported in this OASIS item if they live in a setting specifically designed to care for patients with dementia. The same would be true for M1745. Look to the descriptors for the behaviors that are reportable for both M1740 and M1745 to determine if the behavior would be reportable.
M1740 and M1745: Scenario
Patient was admitted for SN for management of his CHF and PT for strengthening. He was instructed to use his walker for safety due to his weakness. However, he refuses to do so…insists he walks fine without it. He doesn’t seem to have any cognitive impairment. His wife says he’s “as sharp as a tack, but is just stubborn.”
How should the clinician score M1740 and M1745?
Answers: M1740 and M1745
Patient was admitted for SN for management of his CHF and PT for strengthening. He was instructed to use his walker for safety due to his weakness. However, he refuses to do so…insists he walks fine without it. He doesn’t seem to have any cognitive impairment. His wife says he’s “as sharp as a tack, but is just stubborn.”
How should the clinician score M1740 and M1745?M1740 = 7 - None of the above behaviors demonstrated
M1745 = 0 - Never
Patient was cognitively intact and chose not to adhere to the instructions to use his walker.
ADL/IADLsM1800 – M1910
ADLs and IADLs
ADLs
• Defined as the tasks of everyday life
• Basic ADLs include:eating
dressing
getting into or out of a bed or chair
taking a bath or shower
using the toilet
IADLs
• Instrumental activities of daily living related to independent living
• Include:preparing meals
managing money
shopping
doing housework
using a telephone
346
ADLs
•To get the most accurate representation of the
patient shown in these ADL items, prior to scoring,
the clinician must know if the patient is considered a
falls risk. The consideration of the patient’s ability
to perform ADLs includes their ability to safely
ACCESS where the task occurs. If the patient needs
to ambulate to where the task occurs, then the falls
risk must be taken into account.
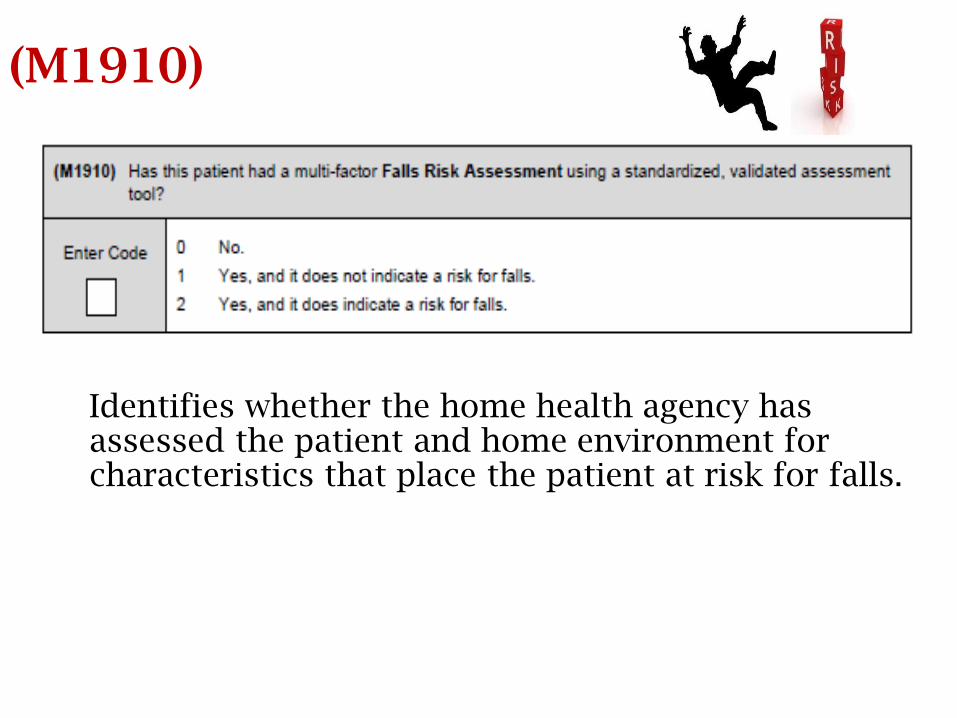
(M1910)
Identifies whether the home health agency has assessed the patient and home environment for characteristics that place the patient at risk for falls.
M1910: Guidance
• Multi-factor falls risk assessment must include at least one standardized tool that has been validated as effective in identifying falls risk in a population with characteristics of the patient being assessed and which includes a standardized response scale.
• A single comprehensive tool that meets criteria (MAHC-10) or several tools may be used.
• If only one tool is standardized and validated, it must be the one used to determine risk.
• If both tools used are standardized and validated:
• An at risk score on either = patient is at risk for falls
M1910: Guidance (cont.)
• Select Response 0 (No multi-factor falls risk assessment conducted) when: No standardized, validated multi-factor test done
Standardized, validated multi-factor test not done within the CMS time frame
Patient not able to participate in task required to allow completion and scoring of standardized assessment(s) that agency chooses to utilize
Bedfast
Chairfast
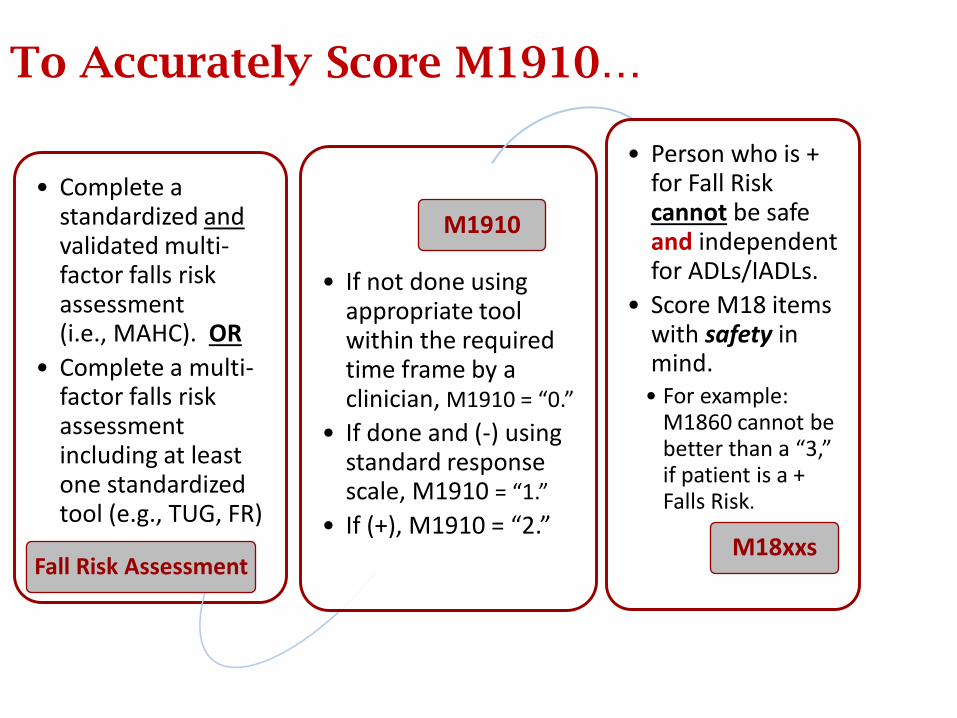
To Accurately Score M1910…
• Complete a standardized andvalidated multi-factor falls risk assessment (i.e., MAHC). OR
• Complete a multi-factor falls risk assessment including at least one standardized tool (e.g., TUG, FR)
Fall Risk Assessment
• If not done using appropriate tool within the required time frame by a clinician, M1910 = “0.”
• If done and (-) using standard response scale, M1910 = “1.”
• If (+), M1910 = “2.”
M1910
• Person who is + for Fall Risk cannot be safe and independent for ADLs/IADLs.
• Score M18 items with safety in mind.
• For example: M1860 cannot be better than a “3,” if patient is a + Falls Risk.
M18xxs
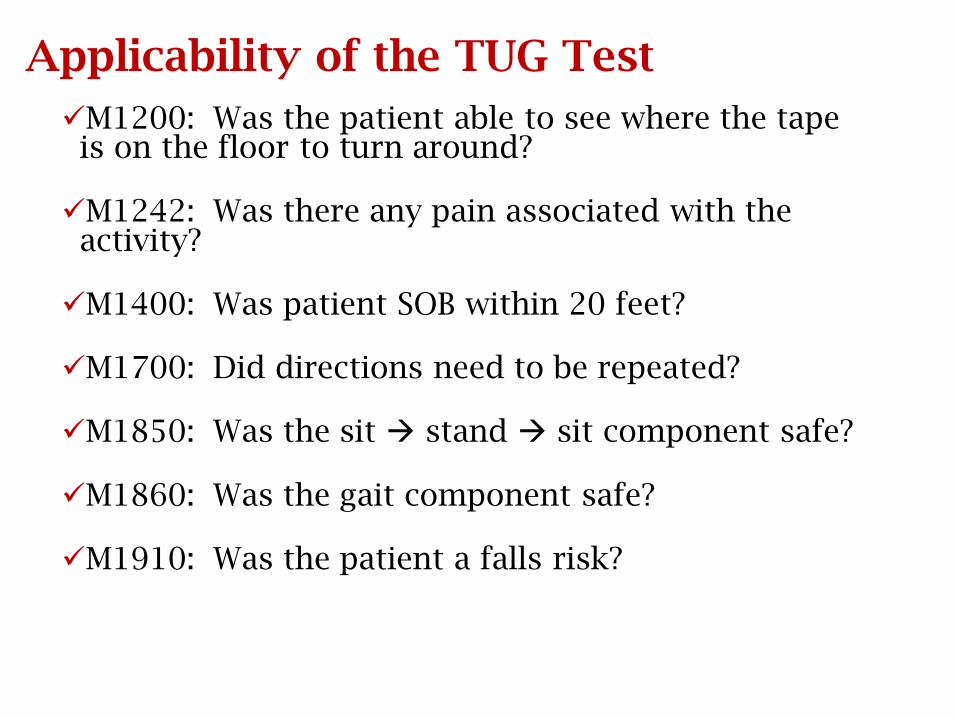
Applicability of the TUG Test
M1200: Was the patient able to see where the tape is on the floor to turn around?
M1242: Was there any pain associated with the activity?
M1400: Was patient SOB within 20 feet?
M1700: Did directions need to be repeated?
M1850: Was the sit stand sit component safe?
M1860: Was the gait component safe?
M1910: Was the patient a falls risk?
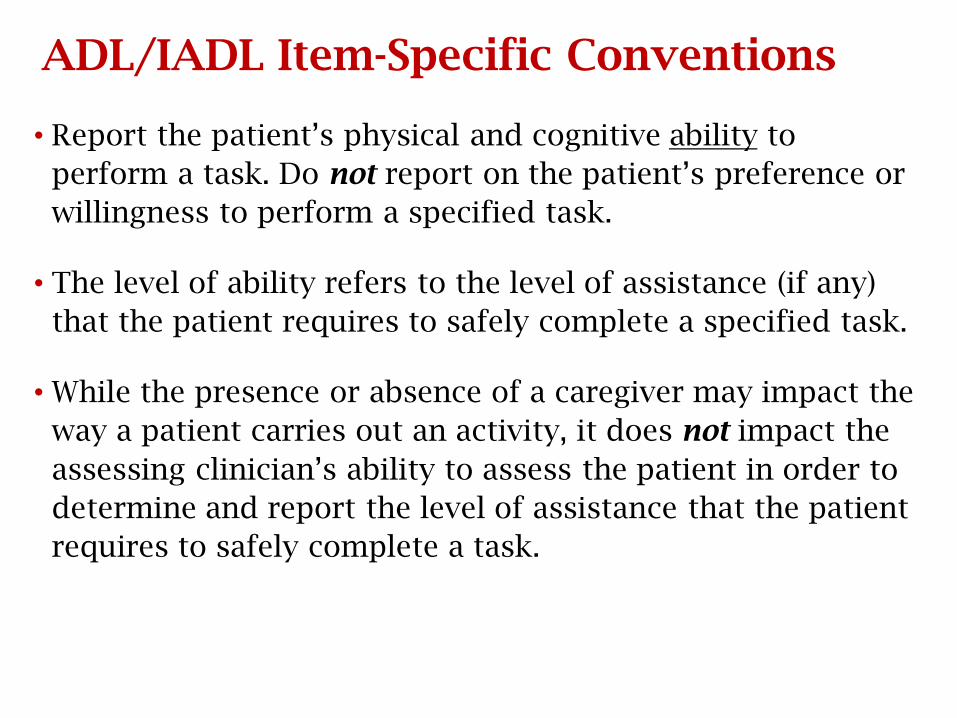
ADL/IADL Item-Specific Conventions
• Report the patient’s physical and cognitive ability to
perform a task. Do not report on the patient’s preference or
willingness to perform a specified task.
• The level of ability refers to the level of assistance (if any)
that the patient requires to safely complete a specified task.
• While the presence or absence of a caregiver may impact the
way a patient carries out an activity, it does not impact the
assessing clinician’s ability to assess the patient in order to
determine and report the level of assistance that the patient
requires to safely complete a task.
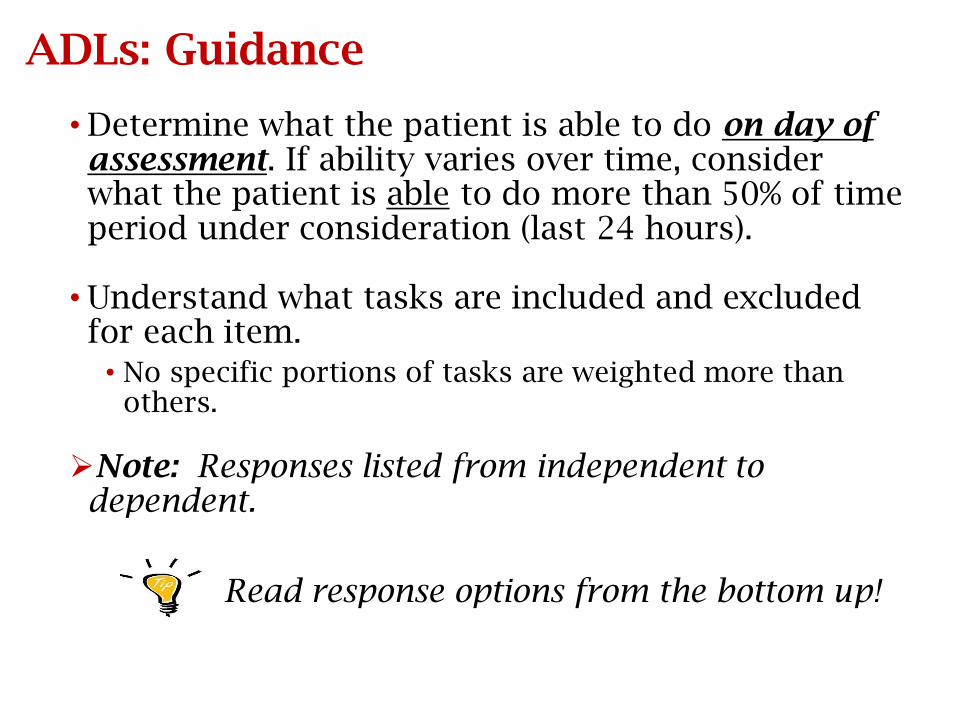
ADLs: Guidance
• Determine what the patient is able to do on day of assessment. If ability varies over time, consider what the patient is able to do more than 50% of time period under consideration (last 24 hours).
• Understand what tasks are included and excluded for each item.
• No specific portions of tasks are weighted more than others.
Note: Responses listed from independent to dependent.
Read response options from the bottom up!
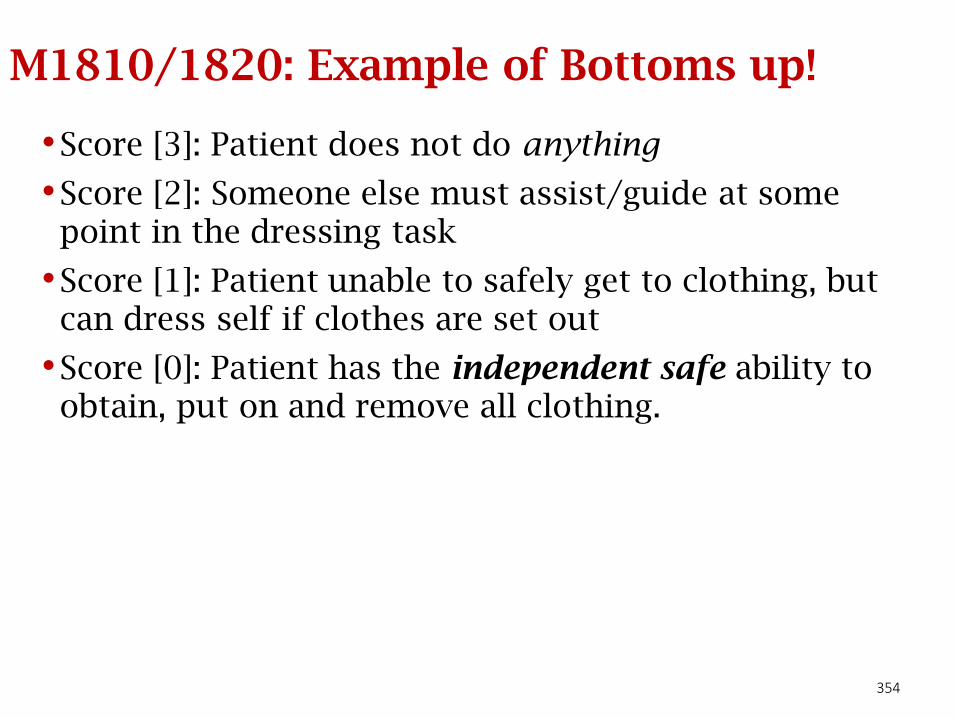
354
M1810/1820: Example of Bottoms up!
•Score [3]: Patient does not do anything
•Score [2]: Someone else must assist/guide at some point in the dressing task
•Score [1]: Patient unable to safely get to clothing, but can dress self if clothes are set out
•Score [0]: Patient has the independent safe ability to obtain, put on and remove all clothing.
ADL/IADL Item-Specific Conventions
• Consider medical restrictions when determining ability. For example, if the physician has ordered activity restrictions, consider this when selecting the best response to functional items related to ambulation, transferring, bathing, etc.
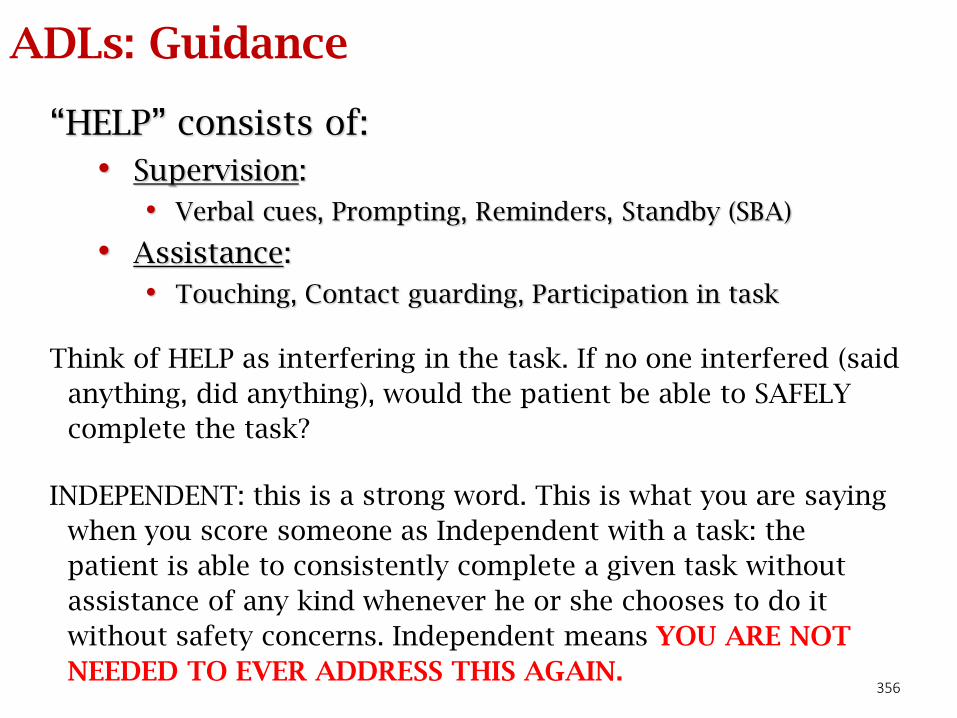
356
ADLs: Guidance
“HELP” consists of:
• Supervision:
• Verbal cues, Prompting, Reminders, Standby (SBA)
• Assistance:
• Touching, Contact guarding, Participation in task
Think of HELP as interfering in the task. If no one interfered (said
anything, did anything), would the patient be able to SAFELY
complete the task?
INDEPENDENT: this is a strong word. This is what you are saying
when you score someone as Independent with a task: the
patient is able to consistently complete a given task without
assistance of any kind whenever he or she chooses to do it
without safety concerns. Independent means YOU ARE NOT
NEEDED TO EVER ADDRESS THIS AGAIN.
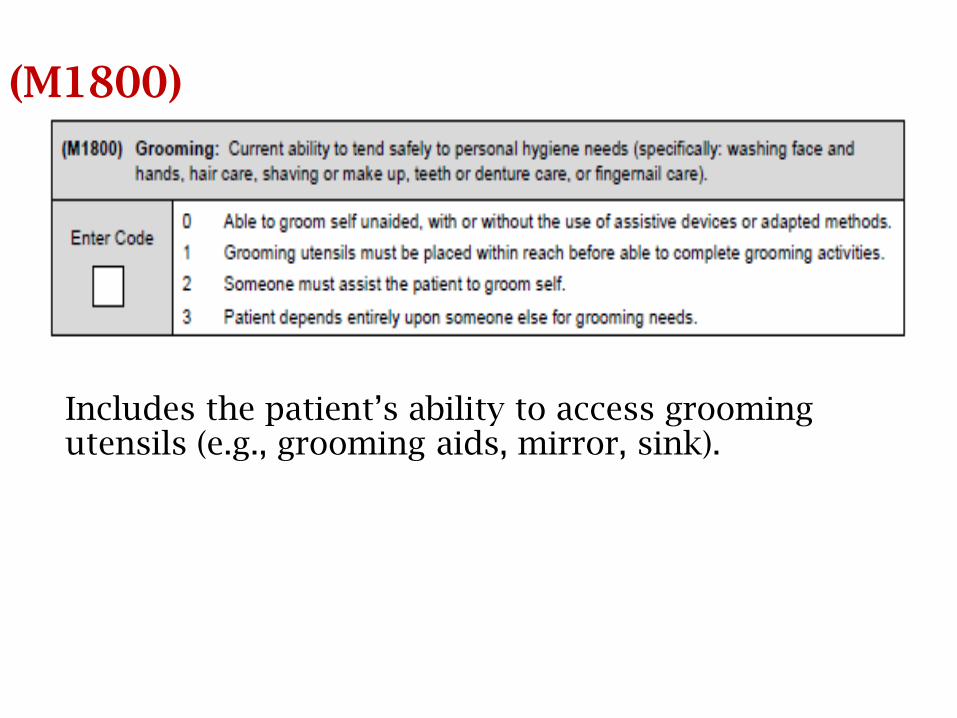
(M1800)
Includes the patient’s ability to access grooming utensils (e.g., grooming aids, mirror, sink).
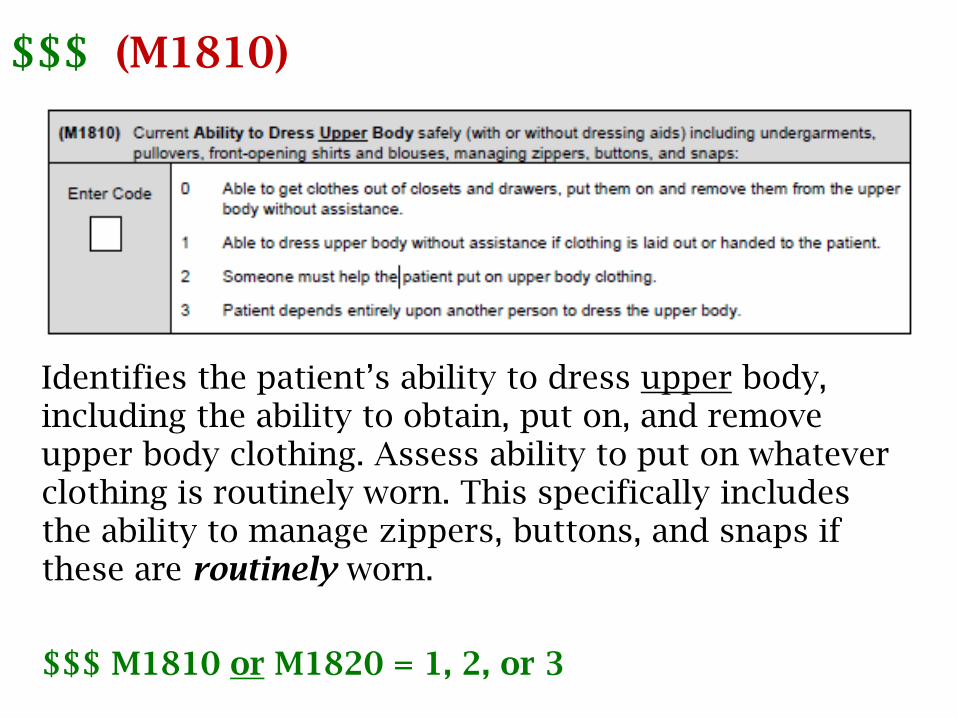
$$$ (M1810)
Identifies the patient’s ability to dress upper body, including the ability to obtain, put on, and remove upper body clothing. Assess ability to put on whatever clothing is routinely worn. This specifically includes the ability to manage zippers, buttons, and snaps if these are routinely worn.
$$$ M1810 or M1820 = 1, 2, or 3
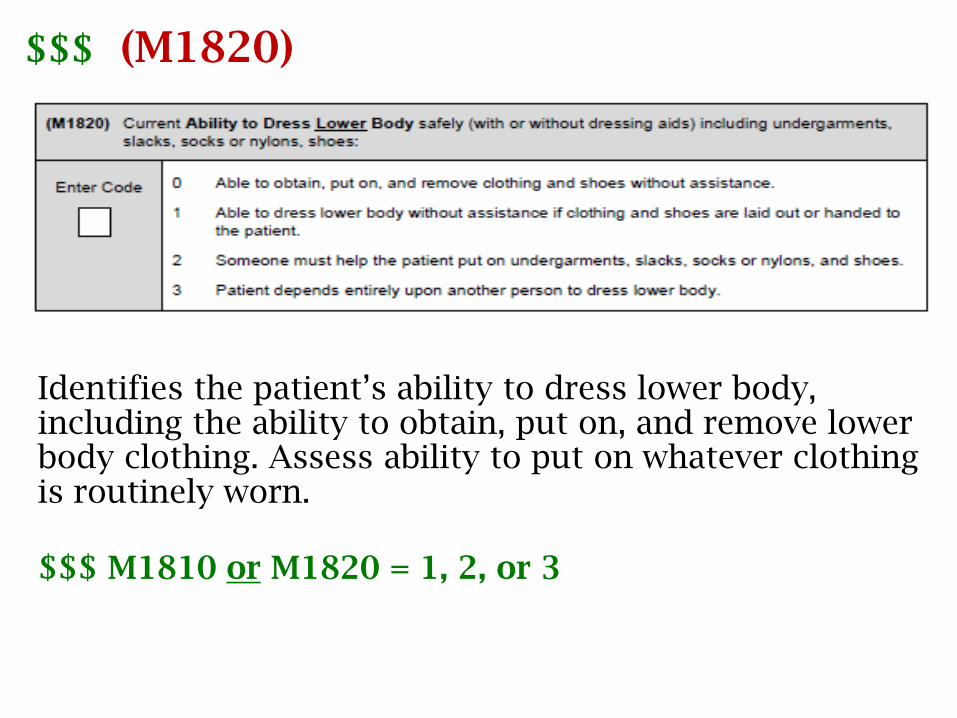
$$$ (M1820)
Identifies the patient’s ability to dress lower body, including the ability to obtain, put on, and remove lower body clothing. Assess ability to put on whatever clothing is routinely worn.
$$$ M1810 or M1820 = 1, 2, or 3
M1810 and M1820: Guidance
• There is no requirement to dress in a certain amount of time, as long as the patient can dress safely.
• Consider what the patient routinely wears (usual status).
• If clothing is modified, is there reasonable expectation that the patient could return to previous style of dressing? No time frame specified for when that may occur.
M1810 and M1820: Guidance (cont.)
• Elastic bandages (Ace wraps) worn for support and compression are considered a dressing item. Other wound dressings are not. Wraps used solely to secure a wound dressing are not considered in either M1810 or M1820.
• Consider prosthetic, orthotic, or other support devices applied as dressing items.
• Upper body – upper extremity prosthesis, cervical collar, or arm sling
• Lower body – prosthesis, ankle-foot orthosis (AFO), or TED hose
• Devices the patient is ordered to wear (e.g., a brace) are considered dressing items, even if not routinely worn.
• The majority rule does not refer to the individual steps the patient must take to collect, put on or take off clothing.
How would you score M1820?
Patient has compression stockings and needs assistance from another person with putting them on. He is able to put on all other lower body items as long as someone lays them out.
What is the most appropriate response to M1820?
Answer: M1820
Patient has compression stockings and needs assistance from another person with putting them on. He is able to put on all other lower body items as long as someone lays them out.
What is the most appropriate response to M1820?• Response 1 - Able to dress lower body without assistance if
clothing and shoes are laid out or handed to the patient.
Remember, the majority rules! Per Q&A 132.2, “select the response that represents the patient’s status in the “majority of tasks.” Do not consider which items are more important than others
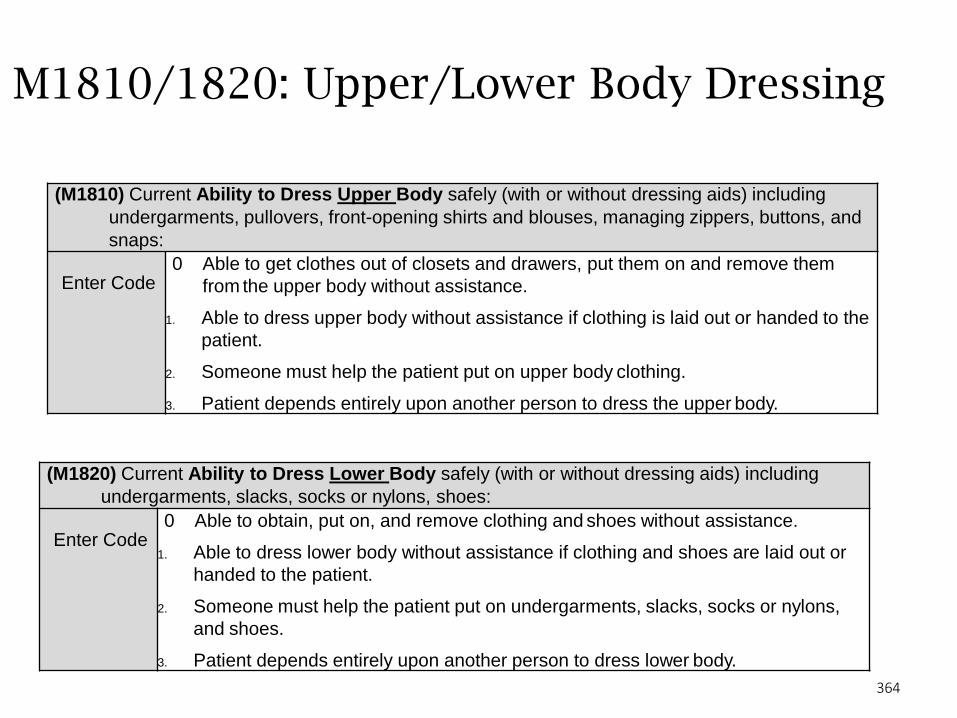
364
M1810/1820: Upper/Lower Body Dressing
(M1810) Current Ability to Dress Upper Body safely (with or without dressing aids) including
undergarments, pullovers, front-opening shirts and blouses, managing zippers, buttons, and
snaps:
Enter Code0 Able to get clothes out of closets and drawers, put them on and remove them
from the upper body without assistance.
1. Able to dress upper body without assistance if clothing is laid out or handed to the
patient.
2. Someone must help the patient put on upper body clothing.
3. Patient depends entirely upon another person to dress the upper body.
(M1820) Current Ability to Dress Lower Body safely (with or without dressing aids) including
undergarments, slacks, socks or nylons, shoes:
Enter Code0 Able to obtain, put on, and remove clothing and shoes without assistance.
1. Able to dress lower body without assistance if clothing and shoes are laid out or
handed to the patient.
2. Someone must help the patient put on undergarments, slacks, socks or nylons,
and shoes.
3. Patient depends entirely upon another person to dress lower body.
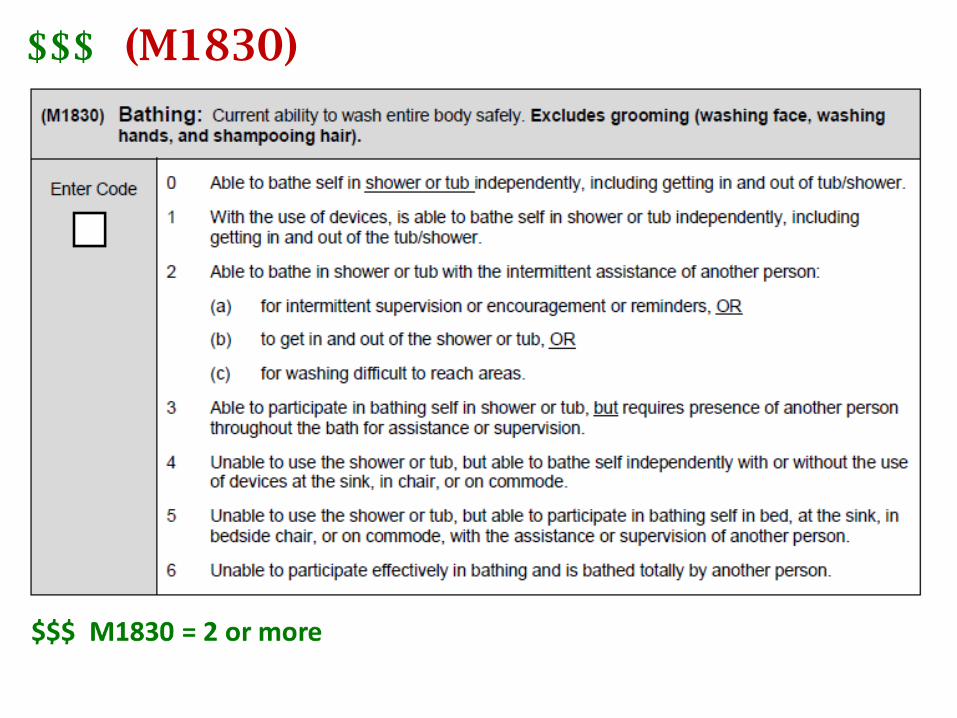
$$$ (M1830)
M1830: Guidance
• Identifies the patient’s ability to bathe entire body and the assistance that may be required to SAFELY bathe, including transferring in and out of the tub or shower.
For a patient with medical restrictions, select response 4, 5, or 6 depending on ability.
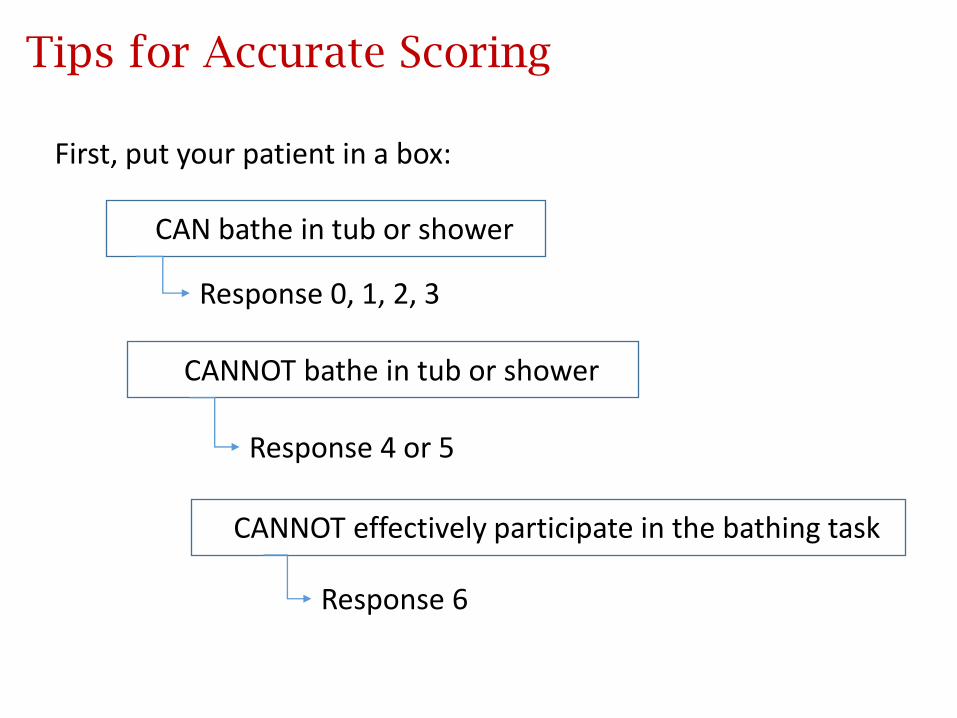
Tips for Accurate Scoring
CCAN bathe in tub or shower
Response 0, 1, 2, 3
CCANNOT bathe in tub or shower
CCANNOT effectively participate in the bathing task
Response 4 or 5
Response 6
First, put your patient in a box:
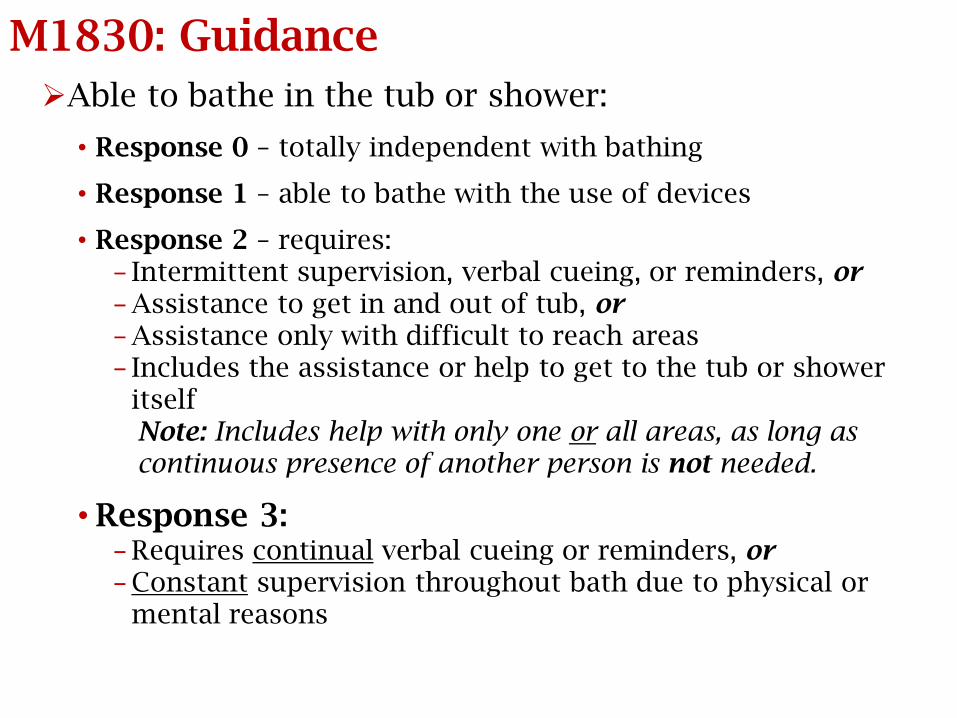
M1830: Guidance
Able to bathe in the tub or shower:
• Response 0 – totally independent with bathing
• Response 1 – able to bathe with the use of devices
• Response 2 – requires:− Intermittent supervision, verbal cueing, or reminders, or− Assistance to get in and out of tub, or− Assistance only with difficult to reach areas− Includes the assistance or help to get to the tub or shower
itselfNote: Includes help with only one or all areas, as long as continuous presence of another person is not needed.
• Response 3:− Requires continual verbal cueing or reminders, or− Constant supervision throughout bath due to physical or
mental reasons
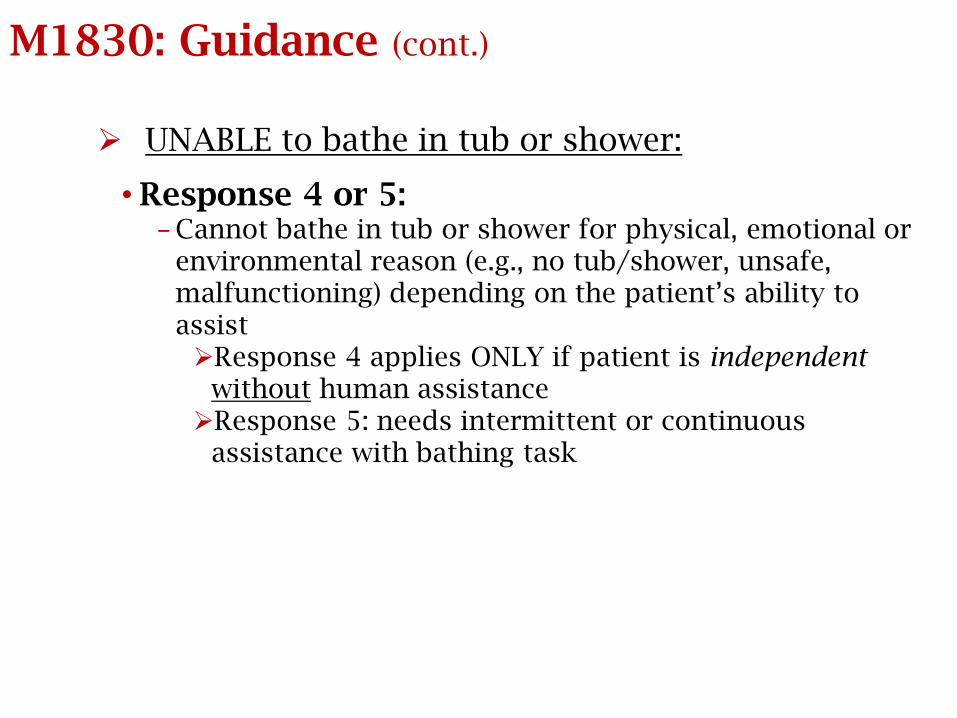
M1830: Guidance (cont.)
UNABLE to bathe in tub or shower:
• Response 4 or 5:− Cannot bathe in tub or shower for physical, emotional or
environmental reason (e.g., no tub/shower, unsafe, malfunctioning) depending on the patient’s ability to assistResponse 4 applies ONLY if patient is independent
without human assistanceResponse 5: needs intermittent or continuous
assistance with bathing task
M1830: Guidance (cont.)
• Response 6:−Totally dependent in bathing (unable to participate
and bathed entirely by another person)−Where the bathing task occurs does not matter
Strategies for M1830 Bathing
• If patient does not have a tub/shower, it is nonfunctioning, or is not accessible or safe for the patient to access, MUST mark [4] or greater
• Ex: shower is upstairs and patient cannot safely climb stairs
• Patients’ status should NOT be based on assumptions of ability with equipment if they do not currently have it
• Watch patient transfer into shower. If you do not want them to perform this because you are afraid they will fall…they probably are not safe!
• Consider restrictions:• Not permitted to climb steps
• Not permitted to get wound wet: MUST mark [4] or greater
• If there is an aide to assist with bathing: can be no better than a [3]
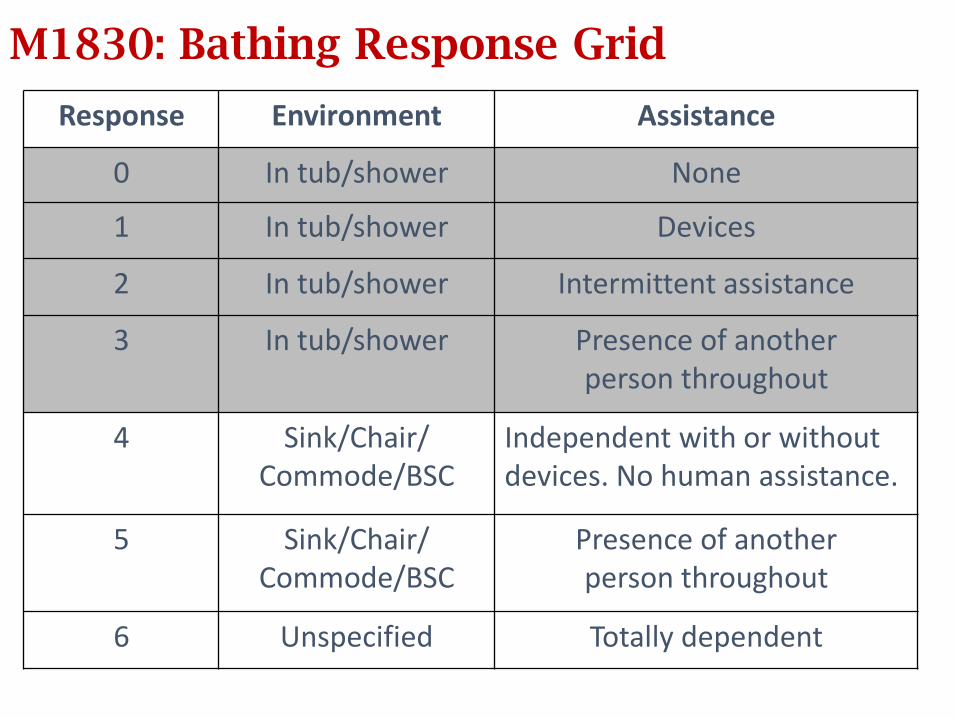
M1830: Bathing Response Grid
Response Environment Assistance
0 In tub/shower None
1 In tub/shower Devices
2 In tub/shower Intermittent assistance
3 In tub/shower Presence of another person throughout
4 Sink/Chair/ Commode/BSC
Independent with or without devices. No human assistance.
5 Sink/Chair/ Commode/BSC
Presence of another person throughout
6 Unspecified Totally dependent
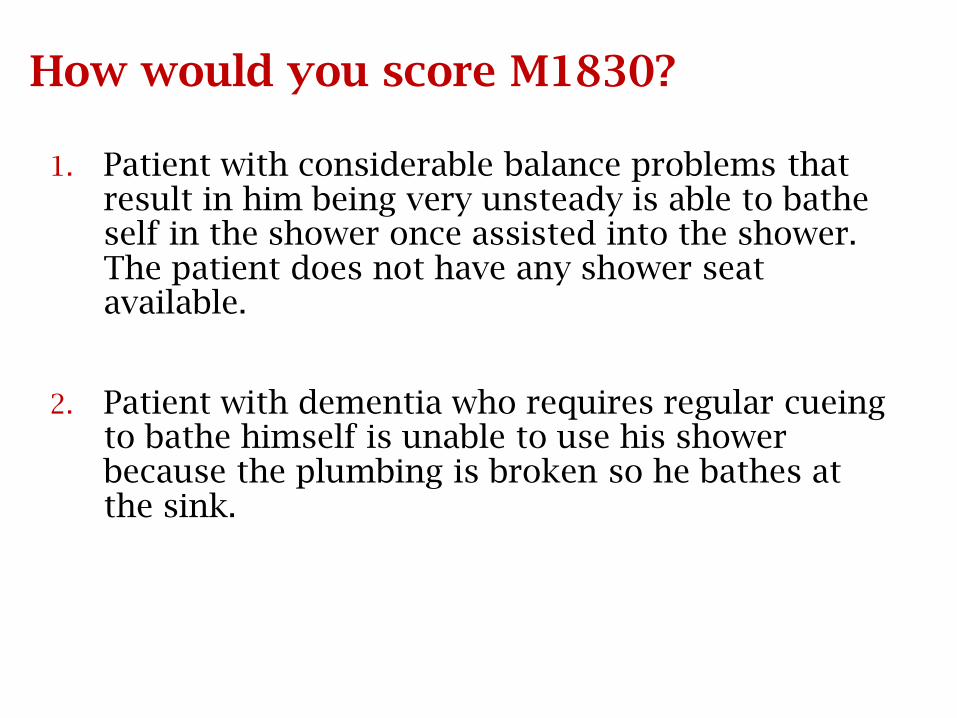
How would you score M1830?
1. Patient with considerable balance problems that result in him being very unsteady is able to bathe self in the shower once assisted into the shower. The patient does not have any shower seat available.
2. Patient with dementia who requires regular cueing to bathe himself is unable to use his shower because the plumbing is broken so he bathes at the sink.
Answers: M1830
1. Patient with considerable balance problems that result in him being very unsteady is able to bathe self in the shower once assisted into the shower. The patient does not have any shower seat available.
Response 3 - Patient not safe in shower by himself
2. Patient with dementia who requires regular cueing to bathe himself is unable to use his shower because the plumbing is broken so he bathes at the sink.
Response 5 - Unable to use tub/shower but able to participate in bathing at sink
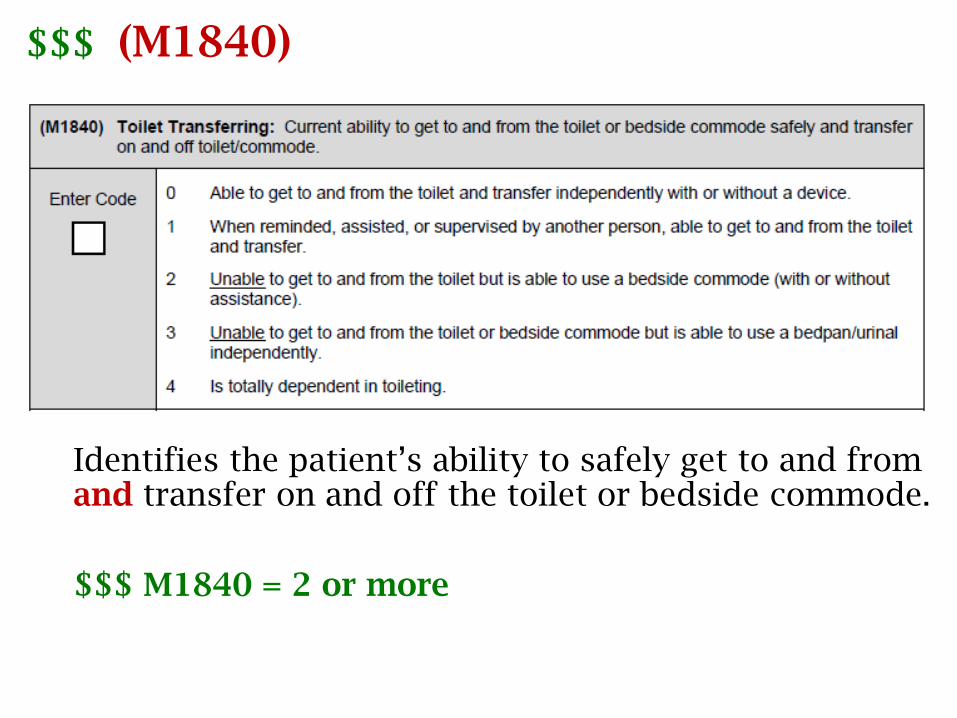
$$$ (M1840)
Identifies the patient’s ability to safely get to and from and transfer on and off the toilet or bedside commode.
$$$ M1840 = 2 or more
M1840: Guidance
• Excludes personal hygiene and management of clothing when toileting.
• Ability to use a bedpan/urinal independently (Response 3) does not include whether or not the patient needs assistance in emptying it.
• In absence of a toilet in the home, determine:• If patient is able to use a bedside commode (Response 2)
• If unable to use a bedside commode, is he/she able to use a bedpan/urinal independently (Response 3)
• If unable to use a bedside commode or bedpan/urinal or if such equipment is not present in the home to allow assessment (Response 4 - Dependent)
377
M1840: Toilet Transferring
• Response [0]: patient must be an independent, safe ambulator (not a falls risk)
• THR with hip precautions: if the required DME is not in place yet:
• E.g.: raised toilet seat or b/s/c, the patient should be scored as [3] or [4] because they are unable to SAFELY transfer on/off a regular toilet per THR restrictions on seat height.
• A patient who is hoyer lifted to a toilet or b/s/c is a [4].
M1840 Toilet Transfer tips
• Measures ability to get to/from the toilet AND ability to get on and off toilet/commode
• Consider that ability may be different during the day than at night or when the patient is fatigued
• What is their ambulation status?
• How did the patient do on the falls assessment?
• How accessible is the bathroom?
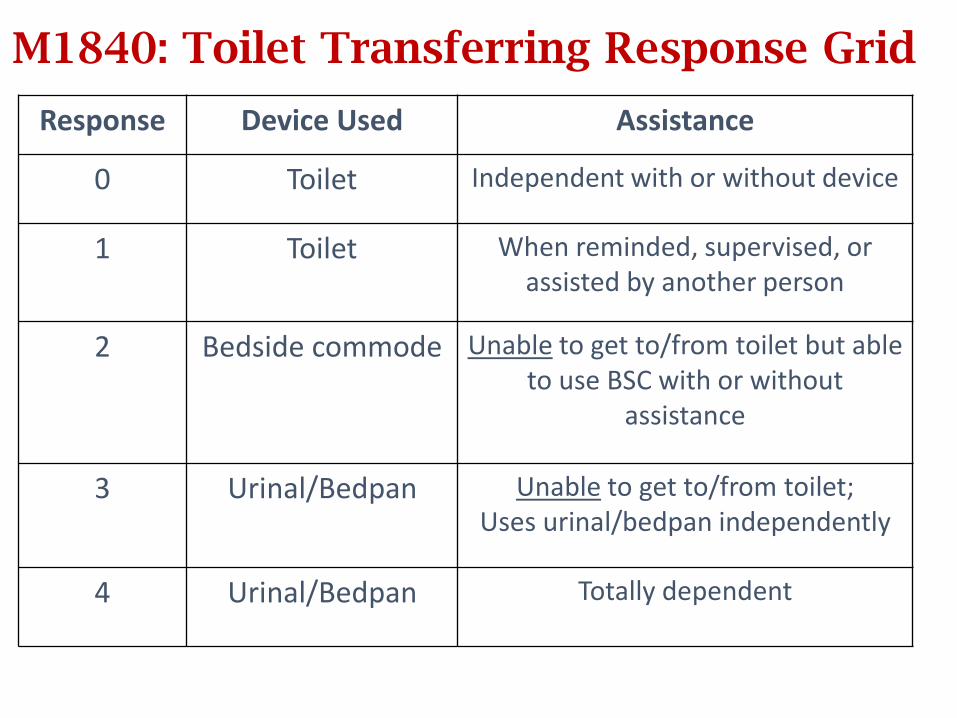
M1840: Toilet Transferring Response Grid
Response Device Used Assistance
0 Toilet Independent with or without device
1 Toilet When reminded, supervised, or assisted by another person
2 Bedside commode Unable to get to/from toilet but able to use BSC with or without
assistance
3 Urinal/Bedpan Unable to get to/from toilet;Uses urinal/bedpan independently
4 Urinal/Bedpan Totally dependent
How would you score M1840?
1. Patient uses a commode at night for convenience but can walk to and from the toilet and transfer safely during the day.
What is the most appropriate response for M1840?
2. Patient lives alone and walks to the bathroom using her cane, but is assessed to be safe only with assistance.
What response would you select for M1840?
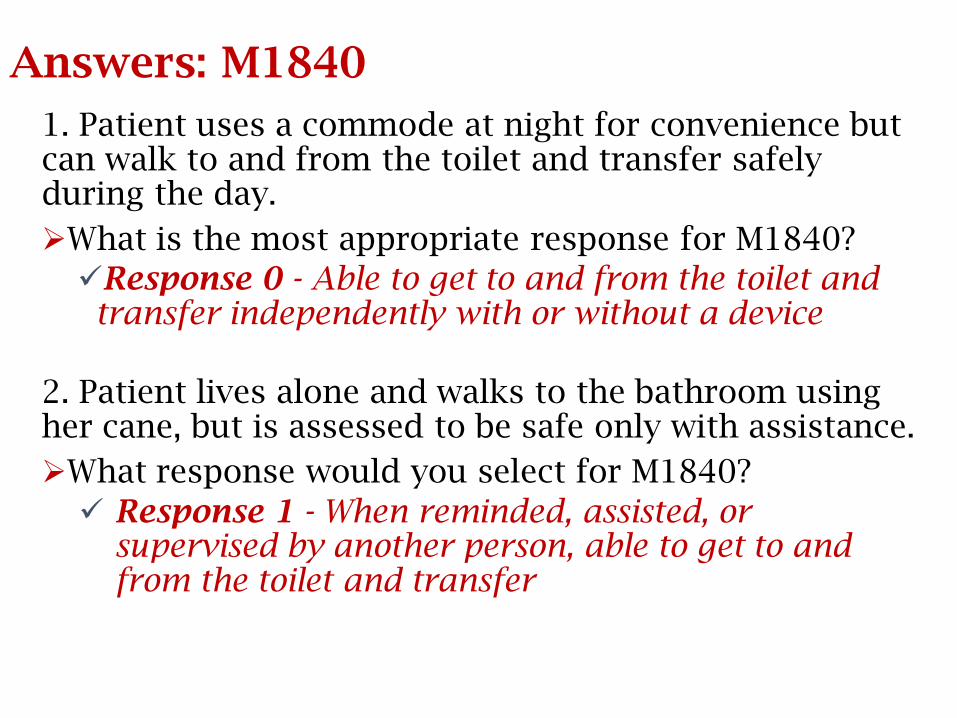
Answers: M1840
1. Patient uses a commode at night for convenience but can walk to and from the toilet and transfer safely during the day.
What is the most appropriate response for M1840?
Response 0 - Able to get to and from the toilet and transfer independently with or without a device
2. Patient lives alone and walks to the bathroom using her cane, but is assessed to be safe only with assistance.
What response would you select for M1840?
Response 1 - When reminded, assisted, or supervised by another person, able to get to and from the toilet and transfer
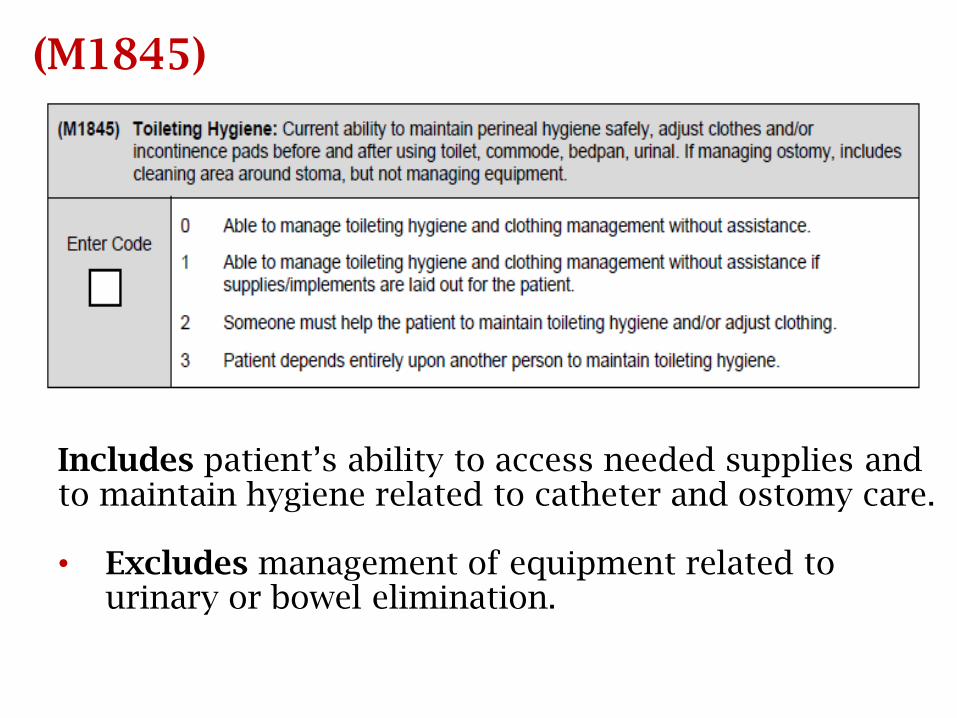
(M1845)
Includes patient’s ability to access needed supplies and to maintain hygiene related to catheter and ostomy care.
• Excludes management of equipment related to urinary or bowel elimination.
Scenario: M1840/M1845
Patient is post-op hip replacement and admitted to agency for rehab. At the time of admission, he is using a walker and his wife is walking with him to the toilet, assisting him on and off, and helping him adjust his clothing. The elevated commode seat, ordered by his surgeon, has not been delivered to the home yet.
What are the most appropriate responses for M1840 and M1845?
Answers: M1840/M1845
Patient is post-op hip replacement and admitted to agency for rehab. At the time of admission he is using a walker and his wife is walking with him to the toilet, assisting him on and off, and helping him adjust his clothing. The elevated commode seat, ordered by his surgeon, has not been delivered to the home yet.
• What are the most appropriate responses for M1840 and M1845?
M1840 = Response 4 – Totally dependent in toileting
M1845 = Response 2 - Someone must help patient to maintain perineal hygiene.
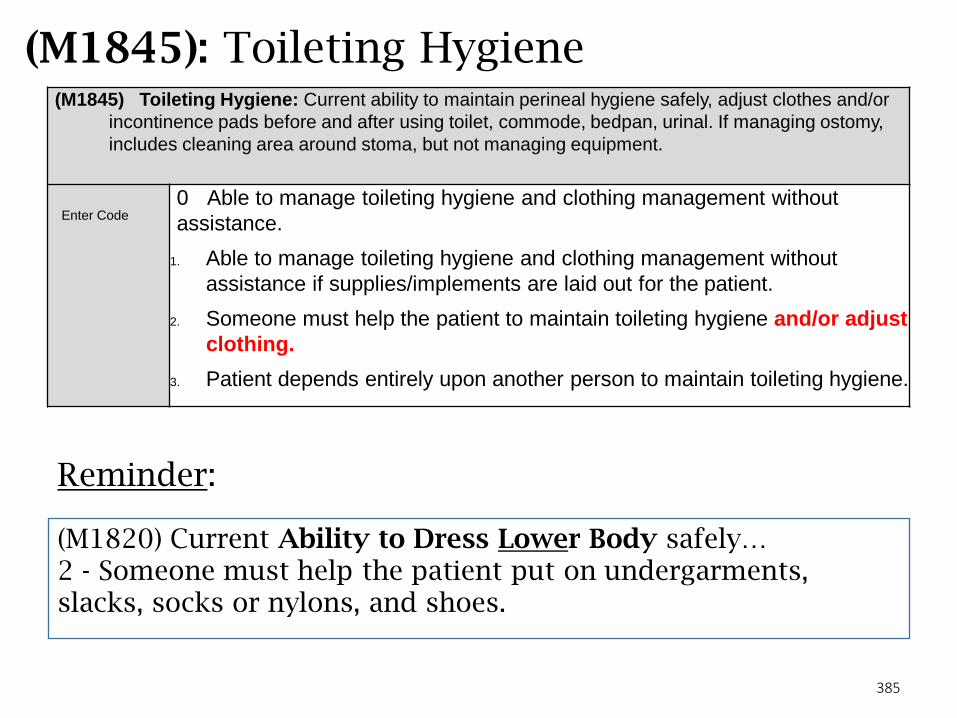
385
(M1845): Toileting Hygiene(M1845) Toileting Hygiene: Current ability to maintain perineal hygiene safely, adjust clothes and/or
incontinence pads before and after using toilet, commode, bedpan, urinal. If managing ostomy,
includes cleaning area around stoma, but not managing equipment.
Enter Code0 Able to manage toileting hygiene and clothing management without
assistance.
1. Able to manage toileting hygiene and clothing management without
assistance if supplies/implements are laid out for the patient.
2. Someone must help the patient to maintain toileting hygiene and/or adjust
clothing.
3. Patient depends entirely upon another person to maintain toileting hygiene.
Reminder:
(M1820) Current Ability to Dress Lower Body safely…2 - Someone must help the patient put on undergarments, slacks, socks or nylons, and shoes.
386
M1845: Toileting Hygiene
•Review your score on M1820 Lower body dressing first;
if the patient is scored [2] or [3] (they need assist), be
wary of scoring this item as [0] or [1]. You need to
consider what the lower body dressing deficit is –
panties, slacks, or is it socks, shoes, etc. Does it affect
the toileting hygiene task (look at score [2]).
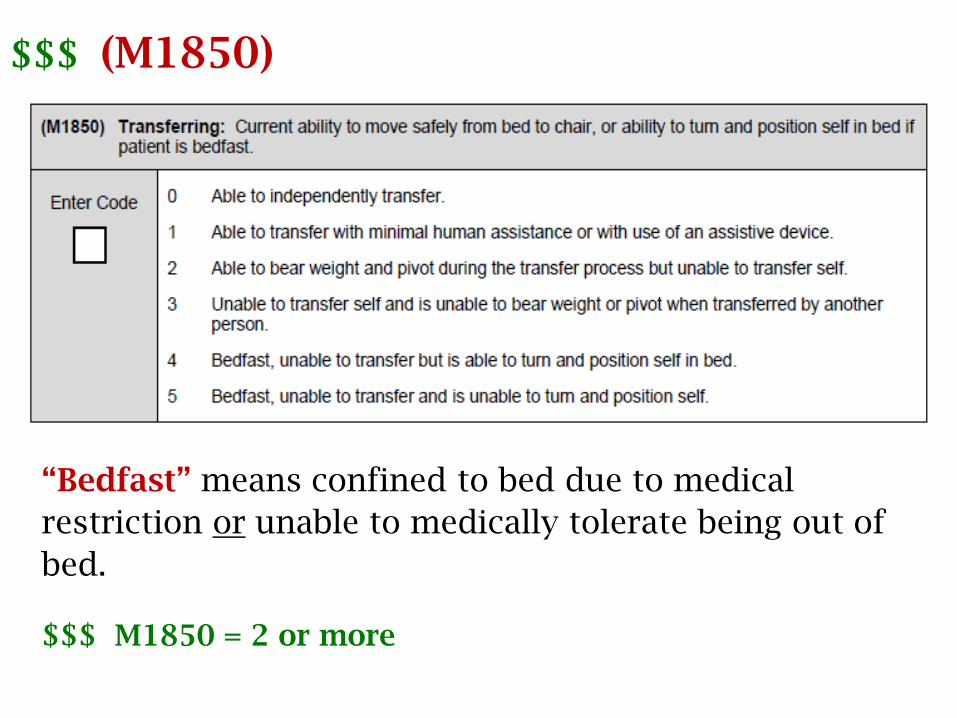
$$$ (M1850)
“Bedfast” means confined to bed due to medical
restriction or unable to medically tolerate being out of
bed.
$$$ M1850 = 2 or more

M1850: Responses
• Response 1 – if the patient requires “minimal human
assistance” – verbal cueing, environmental set-up, hands-on
assistance from another person who contributes < 25% of the
total effort required to perform the transfer
• or requires the use of an assistive device
• Response 2 – if the patient requires BOTH minimal human
assistance and an assistive device to transfer safely.
• Response 3 – if the patient unable both to bear weight or
pivot AND is not bedfast.
• Response 4 or 5 (patient is bedfast) – depends on ability to
turn AND position self in bed.
389
M1850: Transferring tips
• Ambulatory/w/c patients: the bed to chair transfer will include transferring from a supine position in bed to a sitting position at the bedside, then some type of standing, stand-pivot or sliding board transfer to a chair, return to the bed, and lie down.
• Note: The nearest chair might be the commode down the hall. That is the transfer that must be assessed! • If the patient is deemed a falls risk, they cannot be
scored [0]. • If they need more than minimal human assistance, or
need a human AND an a.d., they cannot be scored a [1].• Someone who is hoyered into a recliner or w/c is not
bedfast, therefore, their score can be no worse than a [3].Watch how GG0170c is scored! Do the 2 items make sense
when looked at side by side?
M1850 Transferring
• Bed to chair transfer includes transferring from supine in bed to sitting on nearest seating surface (complete cycle) and returning
• Score [1] is with human assistance OR assistive device…NOT BOTH.
• If both, must mark Score [2].
• If greater than min assist – cannot be [1].
• Remember that supervision = assist
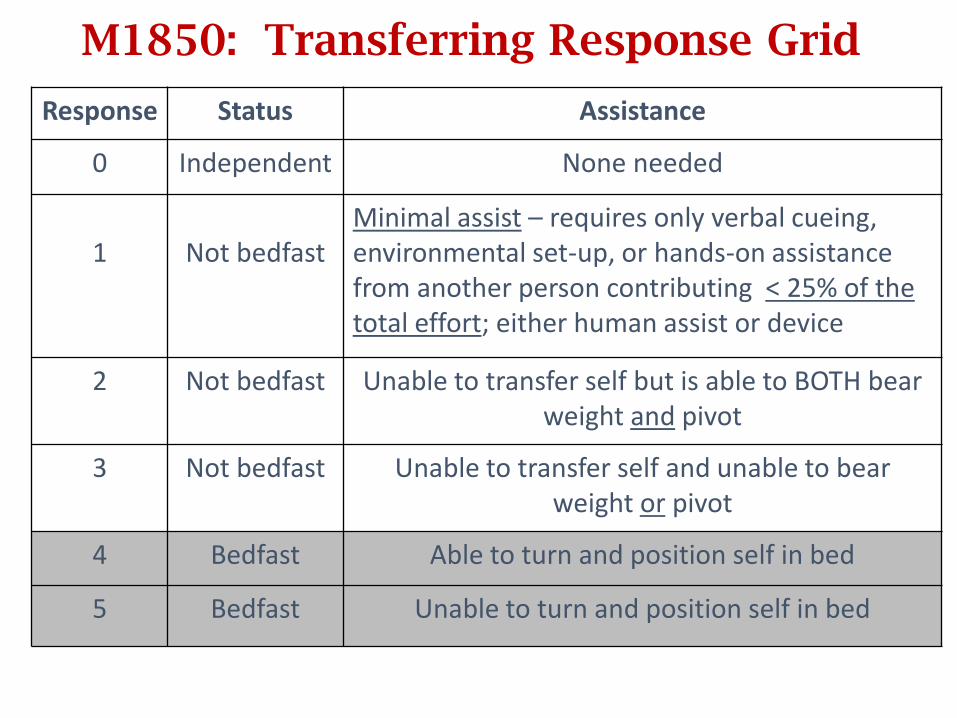
M1850: Transferring Response Grid
Response Status Assistance
0 Independent None needed
1 Not bedfast Minimal assist – requires only verbal cueing, environmental set-up, or hands-on assistance from another person contributing < 25% of the total effort; either human assist or device
2 Not bedfast Unable to transfer self but is able to BOTH bear weight and pivot
3 Not bedfast Unable to transfer self and unable to bear weight or pivot
4 Bedfast Able to turn and position self in bed
5 Bedfast Unable to turn and position self in bed
Scenario: M1850
Patient requires the assistance of his wife to come to a sitting position in bed. Once sitting on the bedside, he is able to use his walker to rise and transfer from his bed to his chair.
How would you score M1850?
Answer: M1850
Patient requires the assistance of his wife to come to a sitting position in bed. Once sitting on the bedside, he is able to use his walker to rise and transfer from his bed to his chair.
How would you score M1850?
Response 2 - Able to bear weight and pivot during the transfer process but unable to transfer self.
• Per CMS, when a patient requires BOTH an assistive device AND minimal human assistance to transfer, Response 2 is appropriate.
Minimal human assistance = any combination of verbal cueing, environmental set-up and/or hands on assist < 25% of total effort.
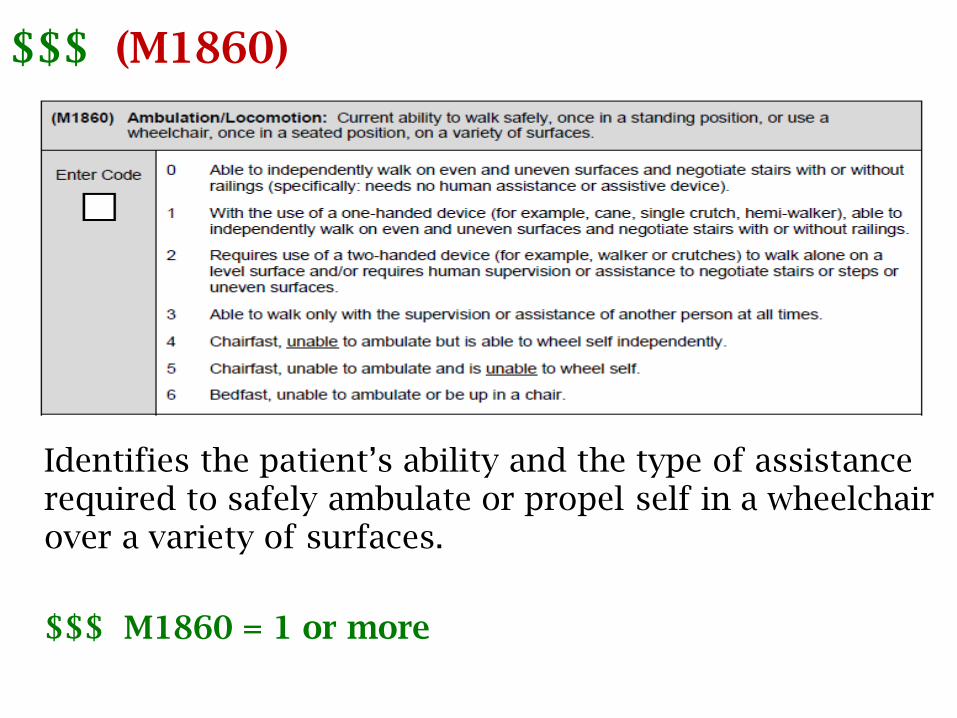
$$$ (M1860)
Identifies the patient’s ability and the type of assistance required to safely ambulate or propel self in a wheelchair over a variety of surfaces.
$$$ M1860 = 1 or more
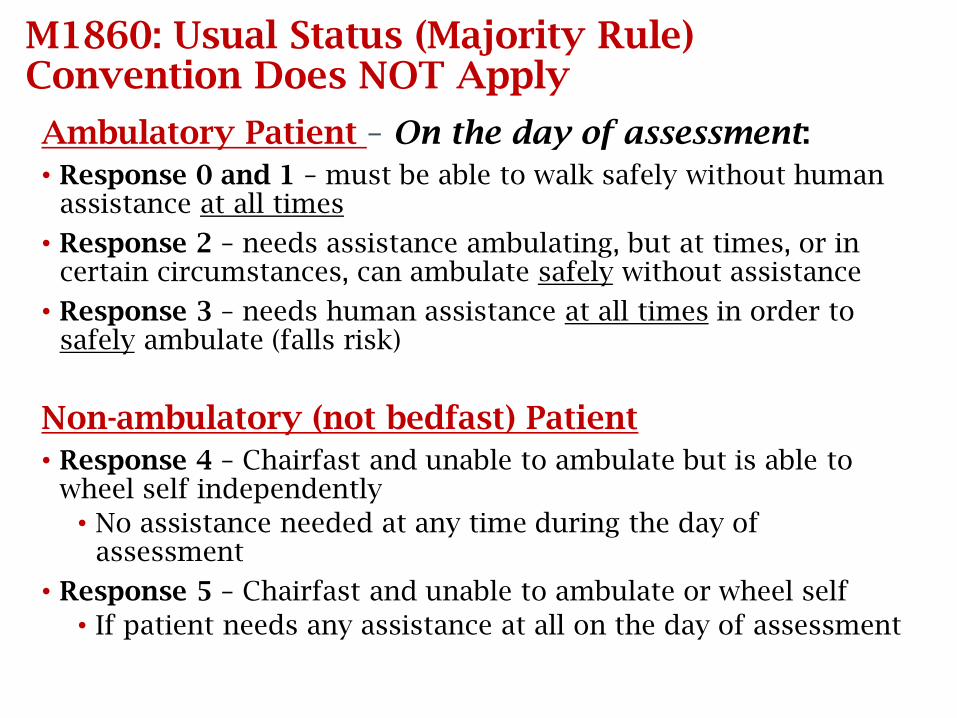
M1860: Usual Status (Majority Rule) Convention Does NOT Apply
Ambulatory Patient – On the day of assessment:
• Response 0 and 1 – must be able to walk safely without human assistance at all times
• Response 2 – needs assistance ambulating, but at times, or in certain circumstances, can ambulate safely without assistance
• Response 3 – needs human assistance at all times in order to safely ambulate (falls risk)
Non-ambulatory (not bedfast) Patient
• Response 4 – Chairfast and unable to ambulate but is able to wheel self independently
• No assistance needed at any time during the day of assessment
• Response 5 – Chairfast and unable to ambulate or wheel self
• If patient needs any assistance at all on the day of assessment
Dragulation/Ambudrag
• If you have a patient, that EVEN WITH an assist of
one or two people, you can not state they are
demonstrating safe ambulation, then you
CANNOT score them as a [3].
• They would have to be scored as [4] – [5],
dependent upon the availability of a w/c and
their ability to maneuver it.
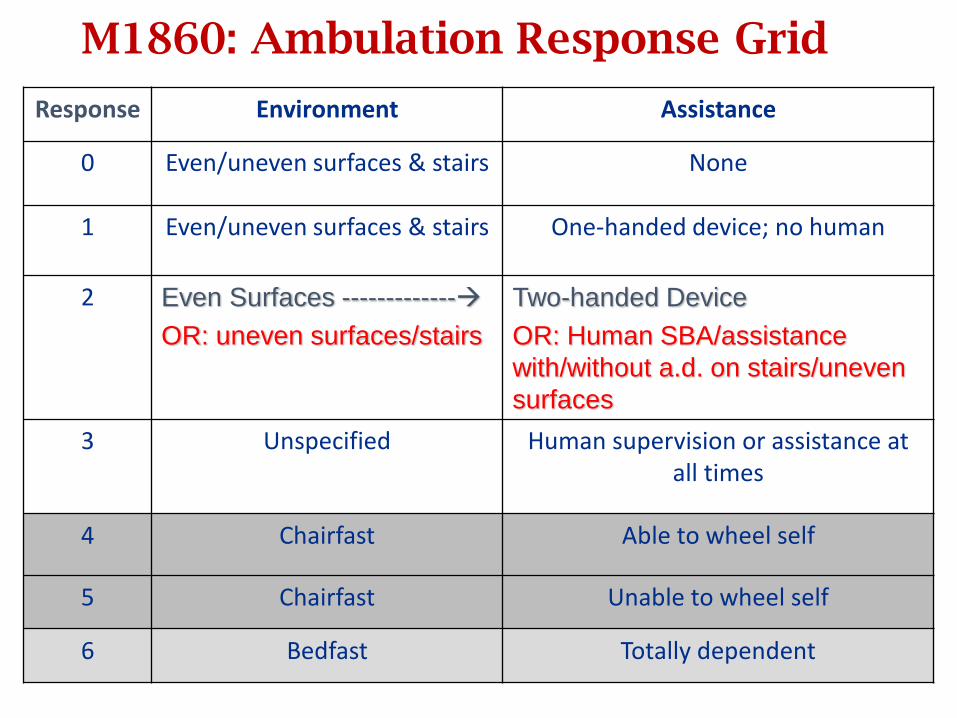
M1860: Ambulation Response Grid
Response Environment Assistance
0 Even/uneven surfaces & stairs None
1 Even/uneven surfaces & stairs One-handed device; no human
2 Even Surfaces -------------
OR: uneven surfaces/stairs
Two-handed Device
OR: Human SBA/assistance
with/without a.d. on stairs/uneven
surfaces
3 Unspecified Human supervision or assistance at all times
4 Chairfast Able to wheel self
5 Chairfast Unable to wheel self
6 Bedfast Totally dependent
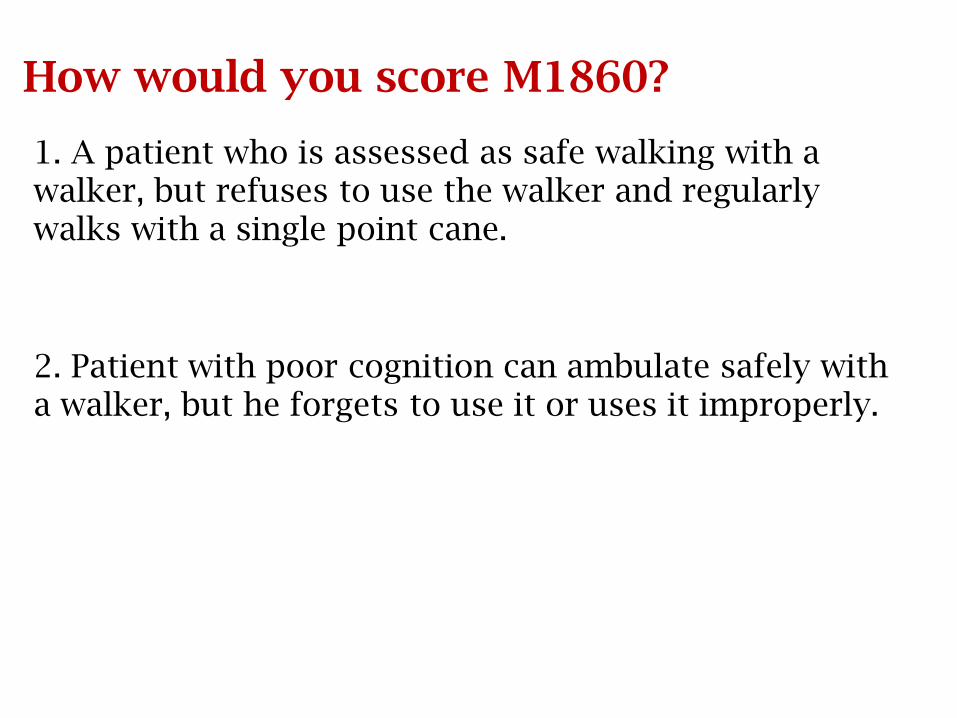
How would you score M1860?
1. A patient who is assessed as safe walking with a walker, but refuses to use the walker and regularly walks with a single point cane.
2. Patient with poor cognition can ambulate safely with a walker, but he forgets to use it or uses it improperly.
Answers: M1860
1. A patient who is assessed as safe walking with a walker, but refuses to use the walker and regularly walks with a single point cane.
Response 2 - Can only walk safely with a walker
2. Patient with poor cognition can ambulate safely with a walker, but he “forgets” to use it or uses it improperly.
Response 3 - Requires supervision/assistance at all times to ambulate safely
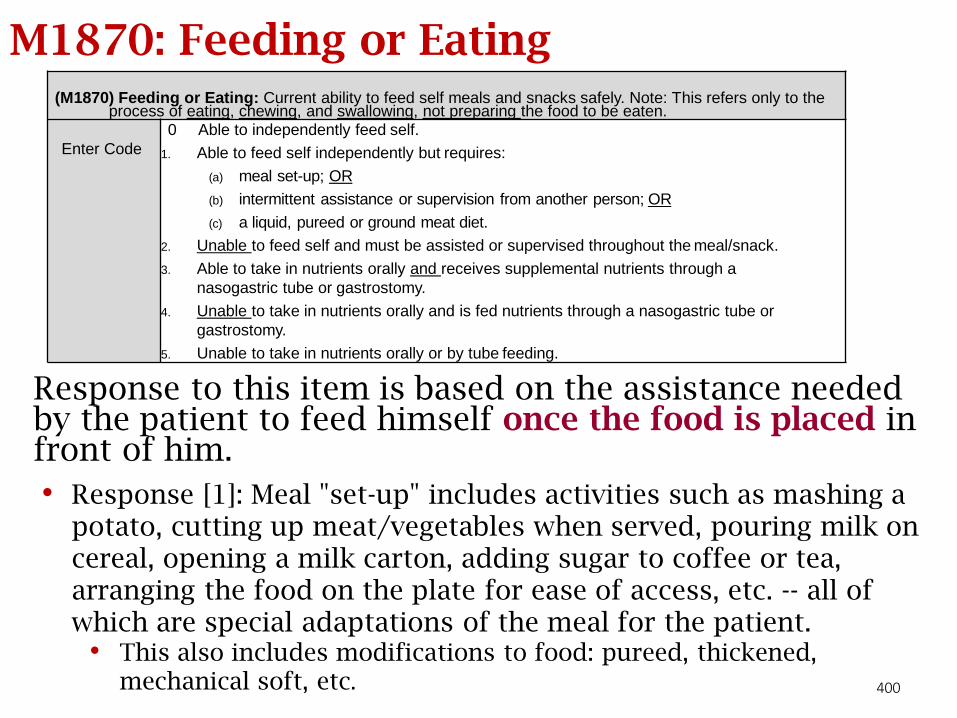
400
M1870: Feeding or Eating
Response to this item is based on the assistance needed by the patient to feed himself once the food is placed in front of him.
(M1870) Feeding or Eating: Current ability to feed self meals and snacks safely. Note: This refers only to the process of eating, chewing, and swallowing, not preparing the food to be eaten.
Enter Code
0 Able to independently feed self.
1. Able to feed self independently but requires:
(a) meal set-up; OR
(b) intermittent assistance or supervision from another person; OR
(c) a liquid, pureed or ground meat diet.
2. Unable to feed self and must be assisted or supervised throughout the meal/snack.
3. Able to take in nutrients orally and receives supplemental nutrients through a
nasogastric tube or gastrostomy.
4. Unable to take in nutrients orally and is fed nutrients through a nasogastric tube or
gastrostomy.
5. Unable to take in nutrients orally or by tube feeding.
• Response [1]: Meal "set-up" includes activities such as mashing a potato, cutting up meat/vegetables when served, pouring milk on cereal, opening a milk carton, adding sugar to coffee or tea, arranging the food on the plate for ease of access, etc. -- all of which are special adaptations of the meal for the patient.
• This also includes modifications to food: pureed, thickened, mechanical soft, etc.
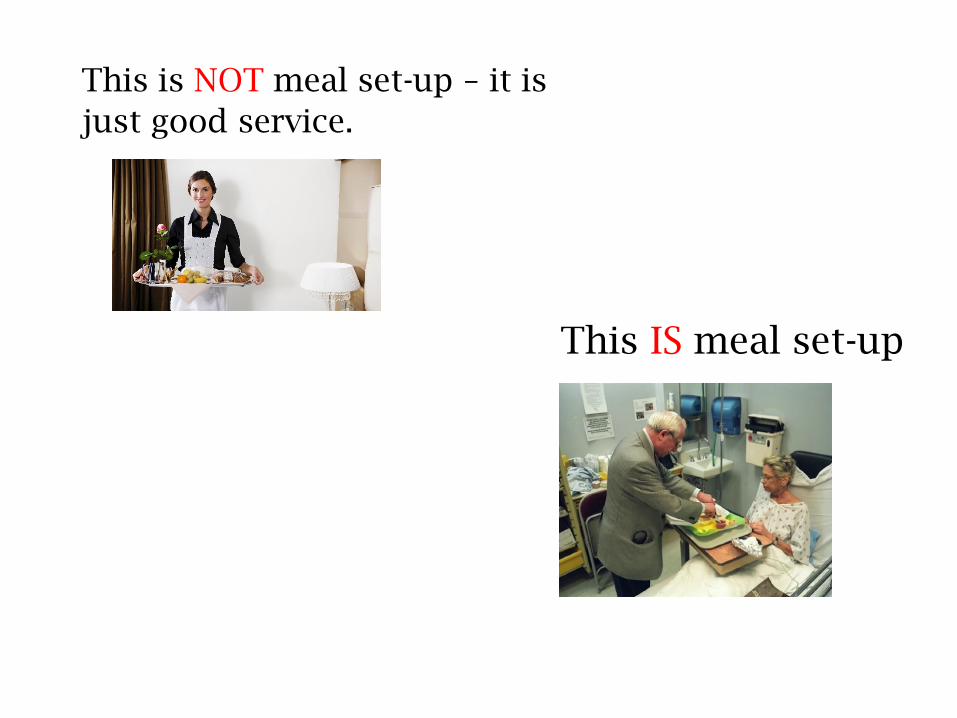
This is NOT meal set-up – it is
just good service.
This IS meal set-up
Medication ItemsM2001 – M2030
403
OASIS Medication Items
M2001: Drug regimen review
M2003: Medication follow-up
M2005: Medication intervention
M2010: High-risk drug education
M2016: Drug education intervention
M2020: Management of oral medications
M2030: Management of injectable medications
404
Drug Regimen Review Process
Assess / Review
Reconcile
Alert / Notify
Follow-up
Resolve
Implement / Educate
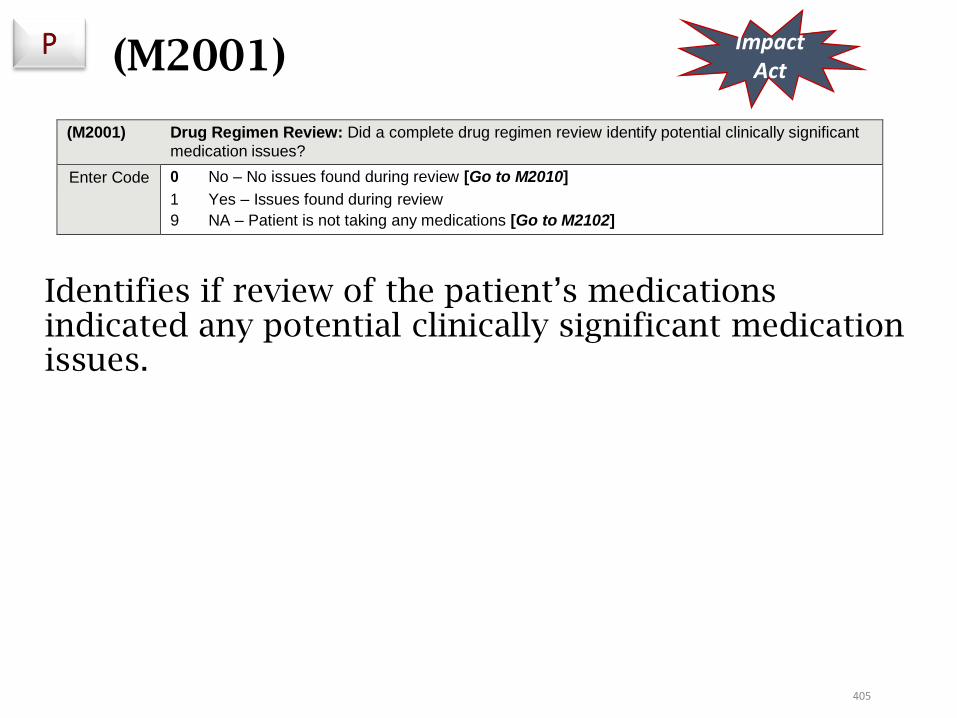
405
Identifies if review of the patient’s medications indicated any potential clinically significant medication issues.
P ImpactAct
(M2001) Drug Regimen Review: Did a complete drug regimen review identify potential clinically significant
medication issues?
Enter Code 0 No – No issues found during review [Go to M2010]
1 Yes – Issues found during review
9 NA – Patient is not taking any medications [Go to M2102]
(M2001)
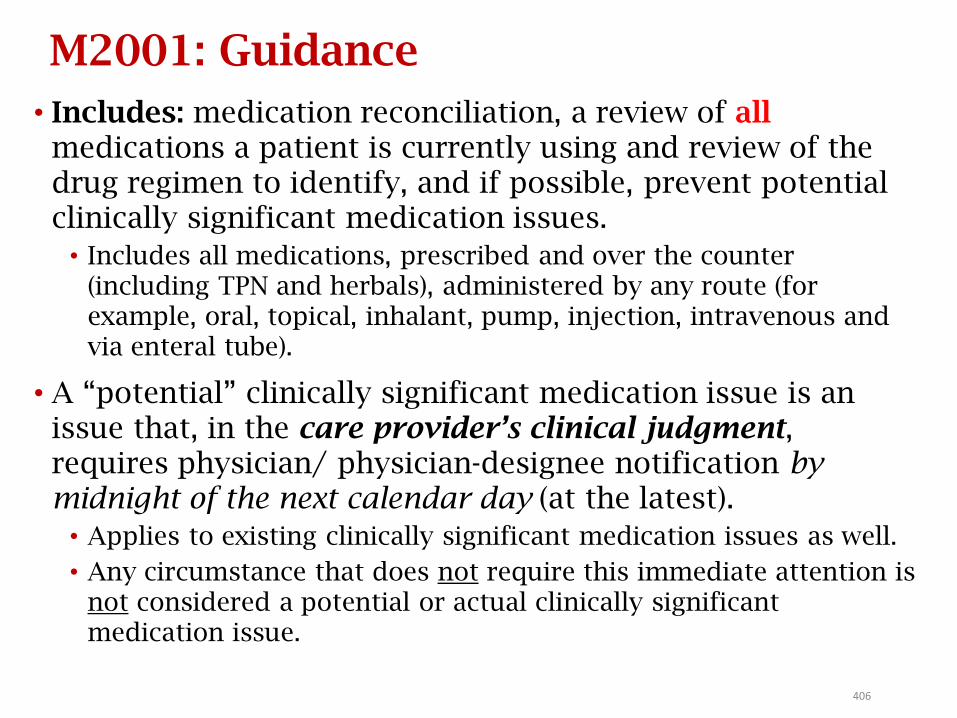
406
M2001: Guidance
• Includes: medication reconciliation, a review of allmedications a patient is currently using and review of the drug regimen to identify, and if possible, prevent potential clinically significant medication issues.
• Includes all medications, prescribed and over the counter (including TPN and herbals), administered by any route (for example, oral, topical, inhalant, pump, injection, intravenous and via enteral tube).
• A “potential” clinically significant medication issue is an issue that, in the care provider’s clinical judgment, requires physician/ physician-designee notification by midnight of the next calendar day (at the latest).
• Applies to existing clinically significant medication issues as well.
• Any circumstance that does not require this immediate attention is not considered a potential or actual clinically significant medication issue.

407
Medication Reconciliation
Must create the most accurate list possible of allmedications a patient is taking:
• Drug name, dosage, frequency, and route
• Identify which ones are new, changed, or long-standing
• Compare that list against the physician’s admission, transfer, and or discharge orders to ensure the patient is taking the correct medication at all transition points in care (or any time a comprehensive assessment is required)
• Reconciliation is not asking the patient what medications they are taking. It is putting your hands on the bottle!
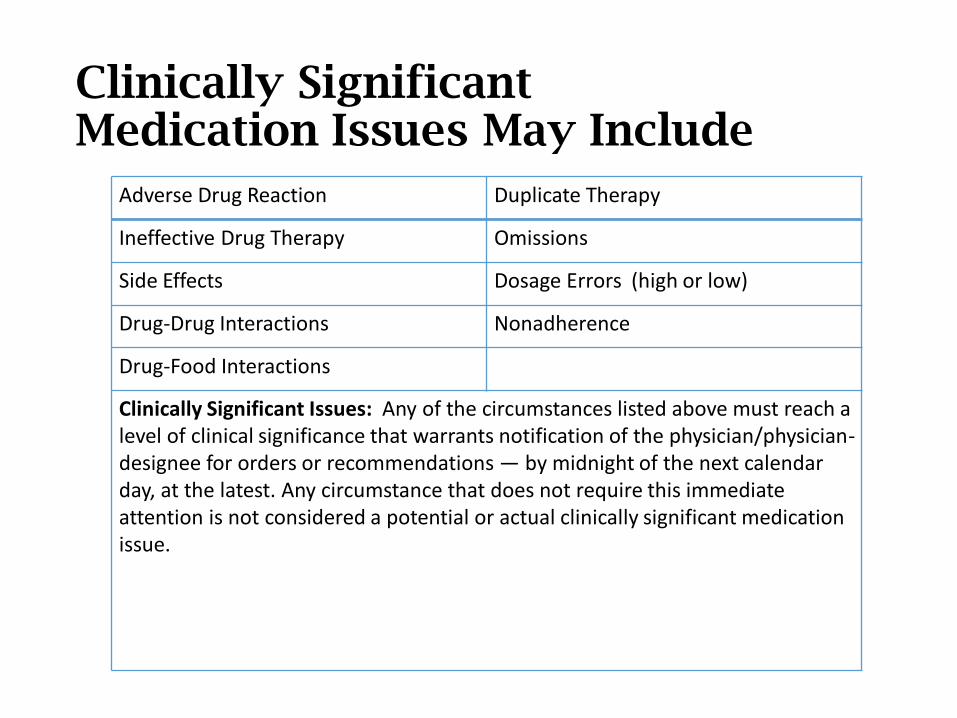
Clinically Significant Medication Issues May Include
Adverse Drug Reaction Duplicate Therapy
Ineffective Drug Therapy Omissions
Side Effects Dosage Errors (high or low)
Drug-Drug Interactions Nonadherence
Drug-Food Interactions
Clinically Significant Issues: Any of the circumstances listed above must reach a level of clinical significance that warrants notification of the physician/physician-designee for orders or recommendations — by midnight of the next calendar day, at the latest. Any circumstance that does not require this immediate attention is not considered a potential or actual clinically significant medicationissue.
409
M2001: Guidance
• Portions of the drug regimen review may be completed
by agency staff other than the clinician responsible for
SOC/ROC OASIS. The collaborating clinician must
communicate the findings to the assessing clinician. For
example, a “collaborating clinician” in the office might:
• Evaluate the medication list to identify possible duplicate drug
therapy or omissions, dosage errors, or potential drug
interactions.
• Contact the patient by phone to discuss issues regarding side
effects the patient may be experiencing or effectiveness of the
medication.
410
M2001:
• The M0090 date reports the date the assessment is completed and should include any time the assessing clinician took to collaborate with others in order to gather all needed assessment data and determine all relevant OASIS responses.
• If a medication-related problem is identified and resolved by the agency staff not requiring physician/physician-designee contact by midnight of the next calendar day, the problem does notneed to be reported as an existing clinically significant problem.
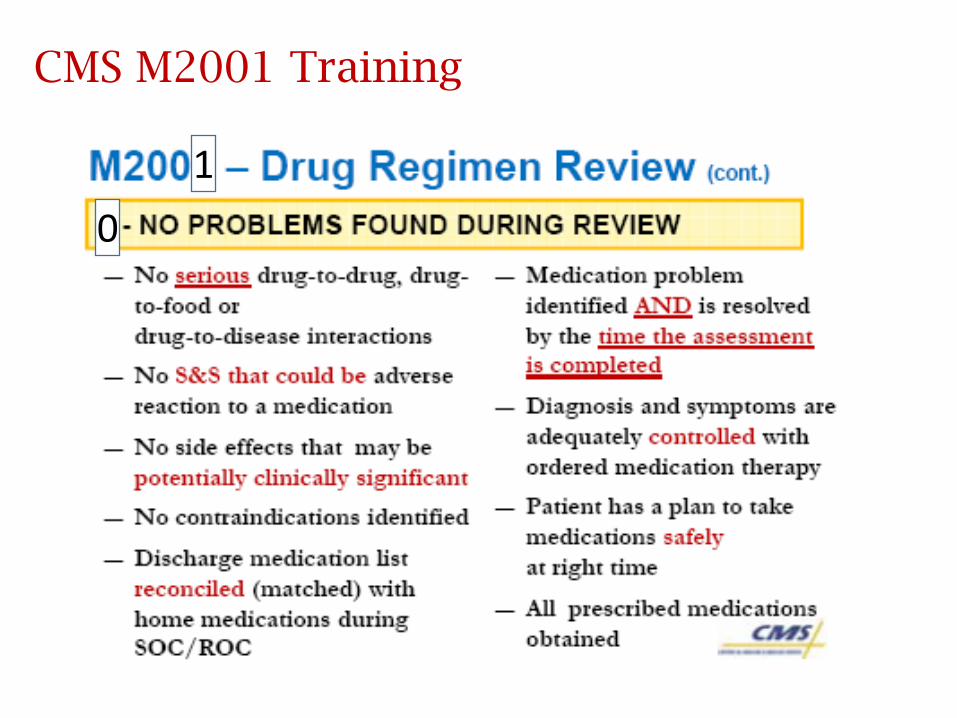
CMS M2001 Training
1
0
412
M2001: Response 0
Response 0 (no issues found during review) should be entered when:
• Patient’s list of medications from the inpatient facility discharge instructions matches the medications the patient shows the clinician at the SOC/ROC assessment visit.
• Assessment shows that diagnoses/symptoms for which the patient is taking medications are adequately controlled (as able to be assessed within the clinician’s scope of practice).
• Patient possesses all medications prescribed.
• Patient has a plan for taking medications safely at the right time.
• Patient is not showing signs/symptoms that could be adverse reactions caused by medications.
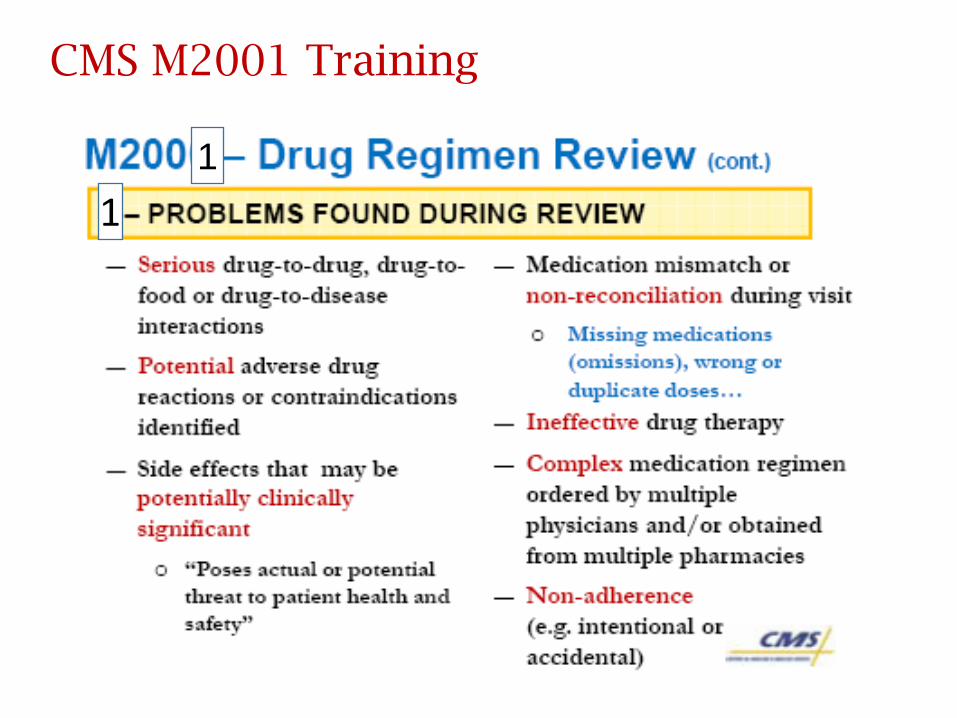
CMS M2001 Training
1
1
414
M2001: Response 1
Response 1 - issues found during review should be entered when:
• Patient’s list of medications from the inpatient facility discharge instructions DO NOT match the medications the patient shows the clinician at the SOC/ROC assessment visit.
• Assessment shows that diagnoses/symptoms for which the patient is taking medications are NOT adequately controlled (as able to be assessed within the clinician’s scope of practice).
• Patient seems confused about when/how to take medications indicating a high risk for medication errors.
415
M2001: Response 1 (cont.)
• Patient has not obtained medications or indicates that he/she will probably not take prescribed medications because of financial, access, cultural, or other issues with medications.
• Patient has signs/symptoms that could be adverse reactions from medications.
• Patient takes multiple non-prescribed medications (OTCs, herbals) that could interact with prescribed medications.
• Patient has a complex medication plan with medications prescribed by multiple physicians and/or obtained from multiple pharmacies so that the risk of drug interactions is high.
416
M2001: Dash (–)
A dash (–) value is a valid response for this item. A dash (–) value indicates that no information is available,
and/or an item could not be assessed. This most often occurs when the patient is unexpectedly transferred, discharged or dies before assessment of the item could be completed. However, providers should complete transfer and discharge assessments to the best of their ability when a care episode ends unexpectedly. CMS expects dash use to be a rare occurrence.
• If elements of the drug regimen review were skipped, for example, drug-to-drug interactions, a dash (–) should be reported, indicating the drug regimen review was not completed.
417
Are these clinically significant issues?
• Patient does not have transportation to pick up new
medication ordered at hospital discharge.
• Patient has Lasix 40 mg. 2x/day in one prescription bottle
(properly labeled) filled yesterday. Old prescription was for
Lasix 20 mg. 2x/day and filled a month ago. Bottle is stored
on top shelf in kitchen.•
• Patient has pain level of “8” and is taking pain medication
as ordered.•
• Patient prescription label states that patient is to take
Aricept® “as directed.”
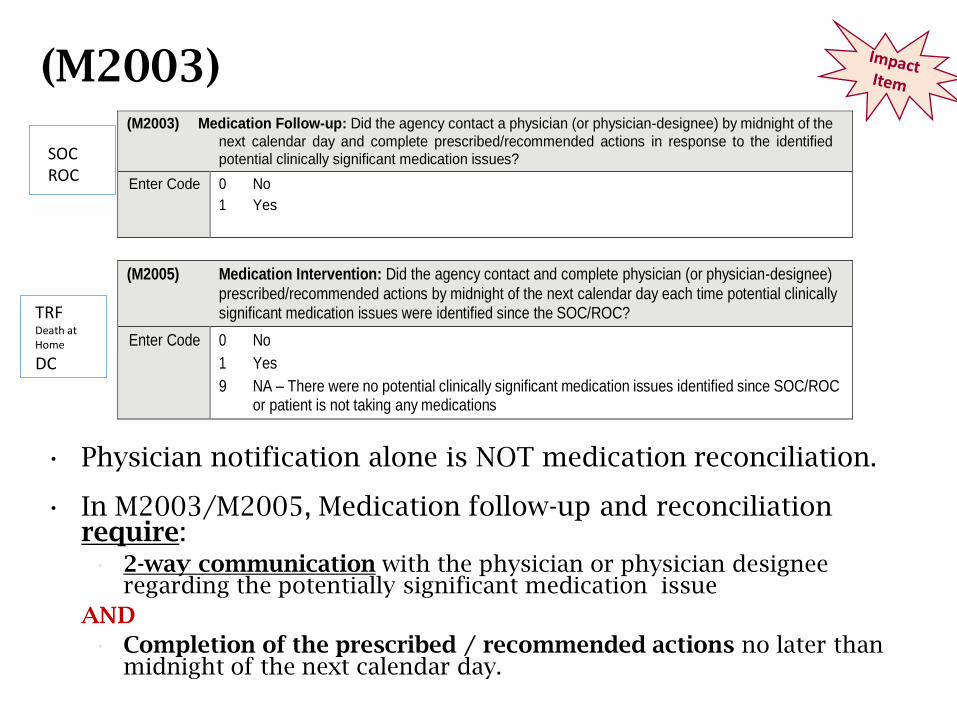
(M2003) (M2003) Medication Follow-up: Did the agency contact a physician (or physician-designee) by midnight of the
next calendar day and complete prescribed/recommended actions in response to the identified potential clinically significant medication issues?
Enter Code 0 No
1 Yes
(M2005) Medication Intervention: Did the agency contact and complete physician (or physician-designee)
prescribed/recommended actions by midnight of the next calendar day each time potential clinically significant medication issues were identified since the SOC/ROC?
Enter Code 0 No
1 Yes
9 NA – There were no potential clinically significant medication issues identified since SOC/ROC or patient is not taking any medications
SOC ROC
TRFDeath at Home
DC
• Physician notification alone is NOT medication reconciliation.
• In M2003/M2005, Medication follow-up and reconciliation require:• 2-way communication with the physician or physician designee
regarding the potentially significant medication issue
AND
• Completion of the prescribed / recommended actions no later than midnight of the next calendar day.
419
Definition: Physician Contact
• You cannot answer this item until you hear back from the physician and complete the orders. This will most likely affect the M0090 date!
• Contact with physician is defined as communication to the physician or physician-designee (made by telephone, voicemail, electronic means, fax, or any other means) that appropriately conveys the message of patient status.
• Communication can be directly to/from the physician or physician-designee, or indirectly through physician’s office staff on behalf of the physician or physician-designee, in accordance with the legal scope of practice.
420
Medication Reconciliation
• Medication follow-up and reconciliation require:• 2-way communication with the physician or physician-
designee regarding the potentially significant medication issue
AND
• Completion of the prescribed / recommended actions no later than midnight of the next calendar day, before the end of the allowed timeframe (5 days at SOC; 2 days at ROC).
• Physician notification alone is NOT reconciliation.
421
M2003: Responses
• If the physician/physician-designee recommends an
action that will take longer than the allowed time to
complete, enter Response 1 - Yes as long as the agency
has taken whatever recommended actions are possible to
comply with by midnight of the next calendar day.
• Includes when a weekend “on-call” physician unfamiliar with the
patient directs agency to call the PCP on Monday for further
orders.
• When multiple potential clinically significant medication
issues are identified at the SOC/ROC, all must be
communicated to the physician or designee, with
completion of ALL prescribed/recommended actions
occurring by midnight of the next calendar day in order to
enter Response 1 - Yes.
422
M2003: Responses
• If the physician/physician-designee provides no new orders or instruction in response to timely reported potential clinically significant medication issue(s), enter Response 1 - Yes, indicating that the physician/physician-designee was contacted and prescribed/recommended actions were completed.
• If a potential clinically significant medication issue was identified and the clinician attempted to communicate with the physician but did not receive communication back from the physician/physician designee until after midnight of the next calendar day, enter Response 0 -No.
• A dash (–) value is a valid response for this item.
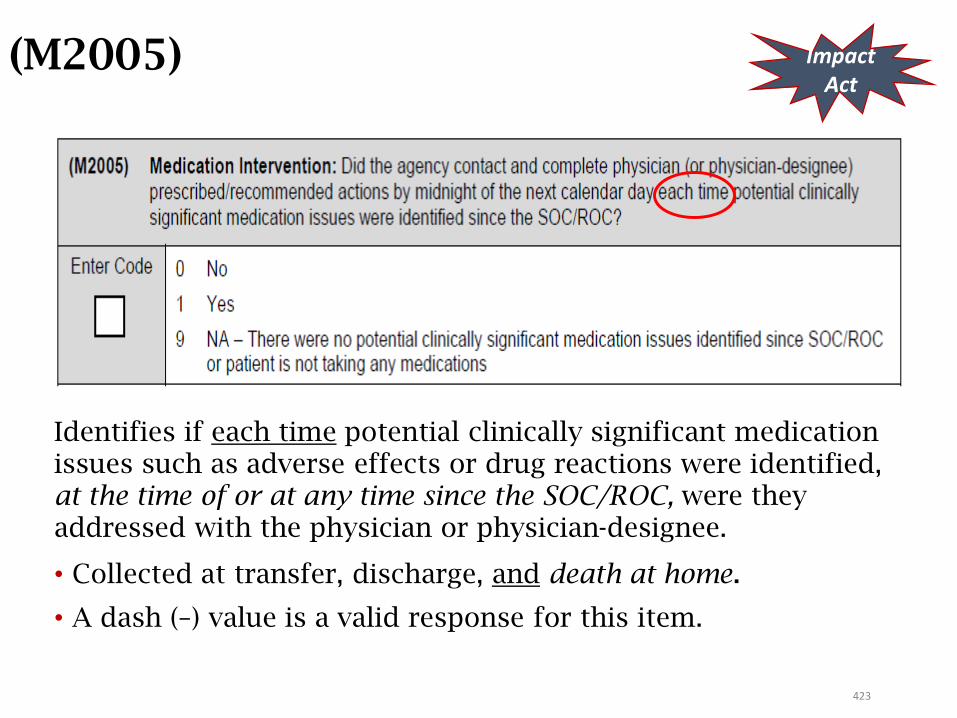
423
(M2005)
Identifies if each time potential clinically significant medication issues such as adverse effects or drug reactions were identified, at the time of or at any time since the SOC/ROC, were they addressed with the physician or physician-designee.
• Collected at transfer, discharge, and death at home.
• A dash (–) value is a valid response for this item.
ImpactAct
M2005 Tips
• Physician contact AND completion of prescribed/recommended actions are required
• It is critical, to be certain this item is answered correctly, that the ability to track contact and related teachings throughout the episode easily is possible. This is NOT a once and done item!
• Now completed on Death at Home OASIS
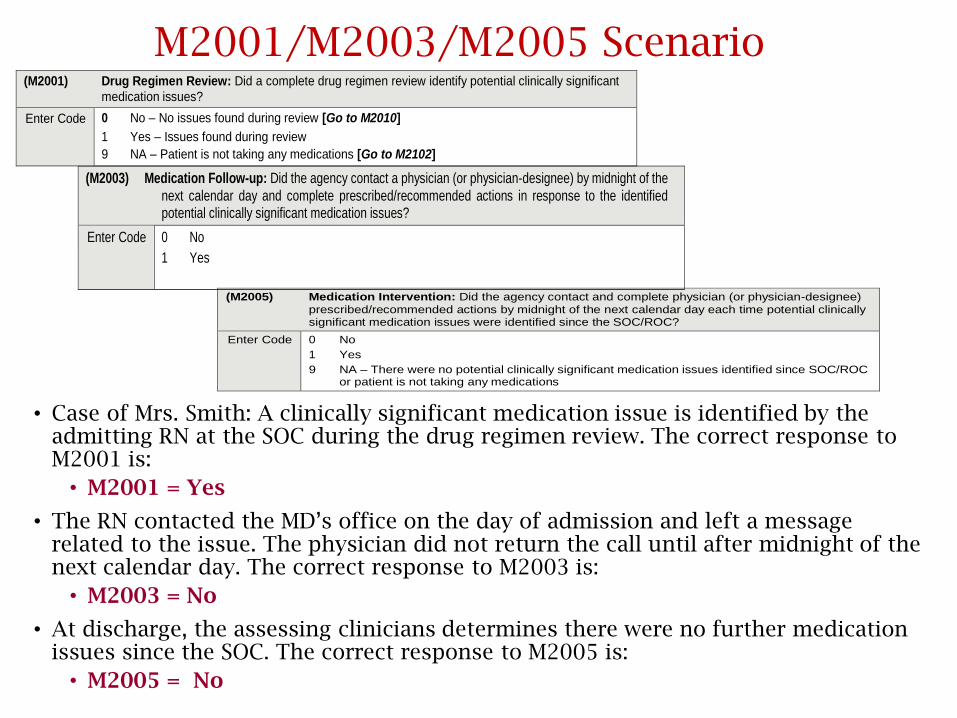
M2001/M2003/M2005 Scenario
• Case of Mrs. Smith: A clinically significant medication issue is identified by the admitting RN at the SOC during the drug regimen review. The correct response to M2001 is:
• M2001 = Yes
• The RN contacted the MD’s office on the day of admission and left a message related to the issue. The physician did not return the call until after midnight of the next calendar day. The correct response to M2003 is:
• M2003 = No
• At discharge, the assessing clinicians determines there were no further medication issues since the SOC. The correct response to M2005 is:
• M2005 = No
(M2005) Medication Intervention: Did the agency contact and complete physician (or physician-designee)
prescribed/recommended actions by midnight of the next calendar day each time potential clinically significant medication issues were identified since the SOC/ROC?
Enter Code 0 No
1 Yes
9 NA – There were no potential clinically significant medication issues identified since SOC/ROC or patient is not taking any medications
(M2003) Medication Follow-up: Did the agency contact a physician (or physician-designee) by midnight of the
next calendar day and complete prescribed/recommended actions in response to the identified potential clinically significant medication issues?
Enter Code 0 No
1 Yes
(M2001) Drug Regimen Review: Did a complete drug regimen review identify potential clinically significant
medication issues?
Enter Code 0 No – No issues found during review [Go to M2010]
1 Yes – Issues found during review
9 NA – Patient is not taking any medications [Go to M2102]
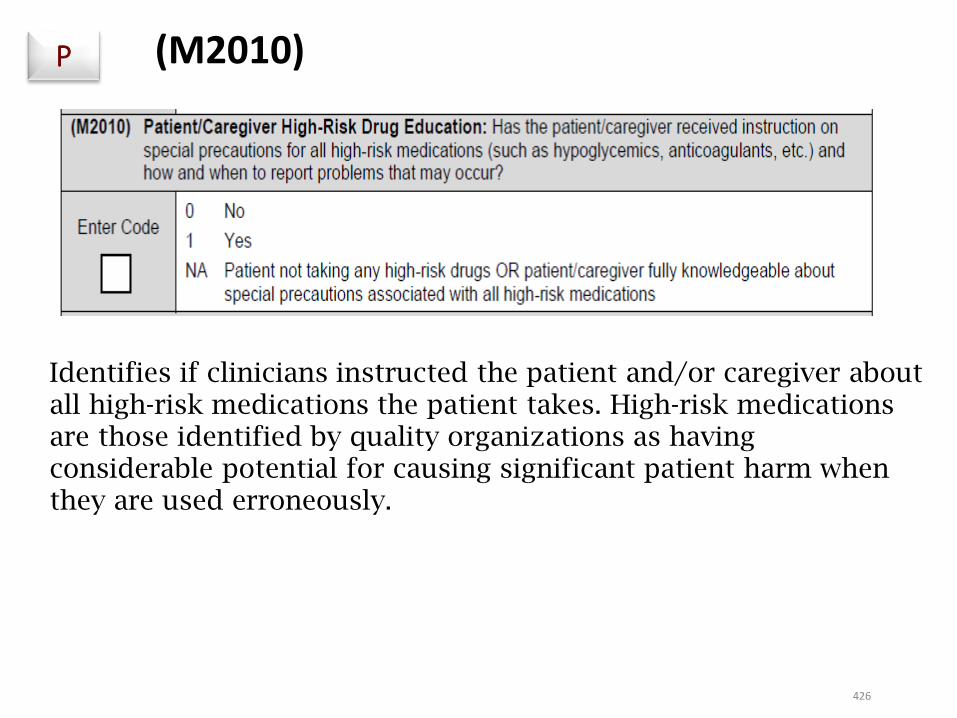
426
Identifies if clinicians instructed the patient and/or caregiver about all high-risk medications the patient takes. High-risk medications are those identified by quality organizations as having considerable potential for causing significant patient harm when they are used erroneously.
P (M2010)
427
M2010: Guidance
• This item is targeted to high-risk medications as it may be unrealistic to expect that patient education on all medications occurs on admission.
• Failure to provide patient education on high-risk medications at SOC/ROC could have severe negative impacts on patient safety and health.
• Examples: Coumadin, Insulin, Opiates and narcotics, Heparin, TPN, chemotherapy, Digoxin
• Includes discontinued high-risk meds that are being taken in error and staff had to educate patient / CG.
• If agency staff other than the clinician responsible for completing the SOC/ROC OASIS provided education to the patient/caregiver on high-risk medications:
• This information must be communicated to the clinician responsible for the SOC/ROC OASIS assessment so that the appropriate response for M2010 may be selected.
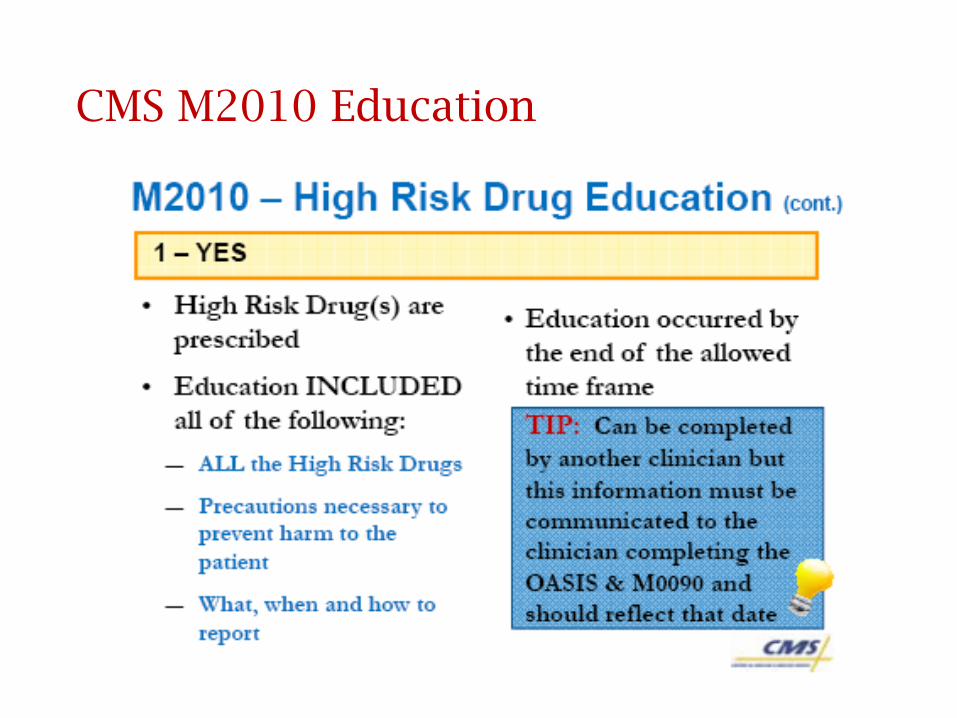
CMS M2010 Education
429429
M2010: High Risk Drug Education
If response [1] - Yes is chosen, you must have documentation indicating:
• who was instructed • which specific HR med• what was taught • their response to teaching (understanding, do
they need follow-up, etc.)
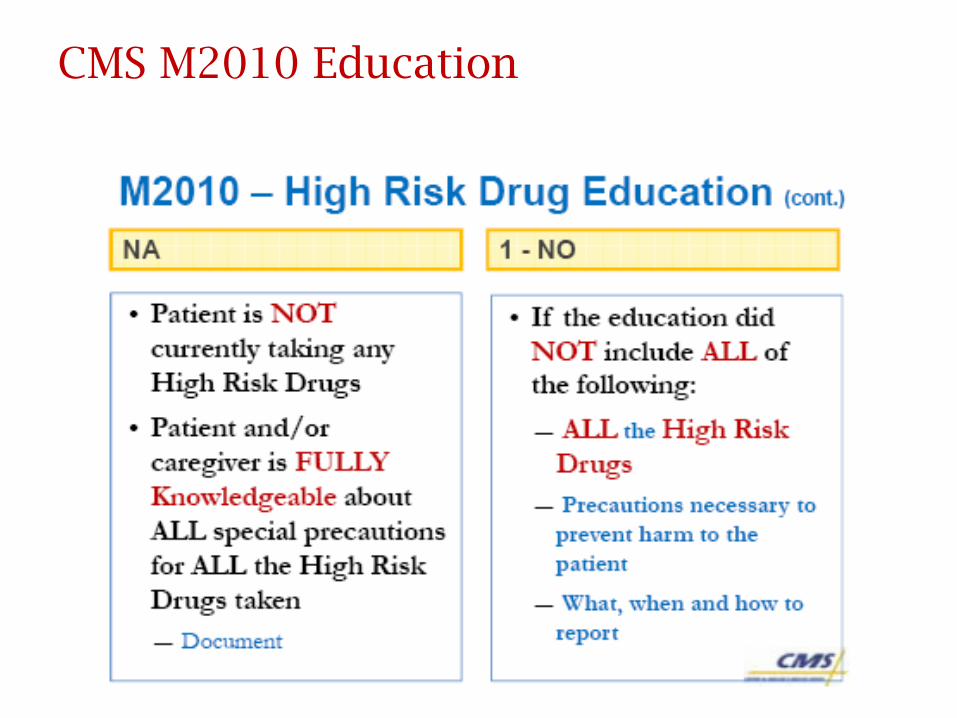
CMS M2010 Education
431
M2010: Scenario
Patient who has a history of HTN is being admitted for management of COPD following discharge from the hospital. The patient’s HTN is controlled now using a diuretic and a low salt diet.
During the medication review, the clinician finds that the patient is currently taking an antihypertensive which was discontinued before his discharge from the hospital. The clinician knows that the antihypertensive is a high-risk drug.
He validates with the physician that the drug should be discontinued and instructs the patient not to take the drug.
How should M2010 (High Risk Drug Education) be answered?
432
Answer: M2010
Patient who has a history of HTN is being admitted for management of COPD following discharge from the hospital. The patient’s HTN is controlled now using a diuretic and a low salt diet. During the medication review, the clinician finds that the patient is currently taking an antihypertensive which was discontinued before his discharge from the hospital. The clinician knows that the antihypertensive is a high-risk drug. He validates with the physician that the drug should be discontinued and instructs the patient not to take the drug.
How should M2010 (High Risk Drug Education) be answered?
Answer: Response 1 - Yes
Rationale: If the patient was taking a high-risk medication in error and was educated by Agency staff to discontinue the medication as well as the special precautions they need to take and how and when to report a problem that occurs as a result of taking
that medication, M2010 may be answered “Yes.”
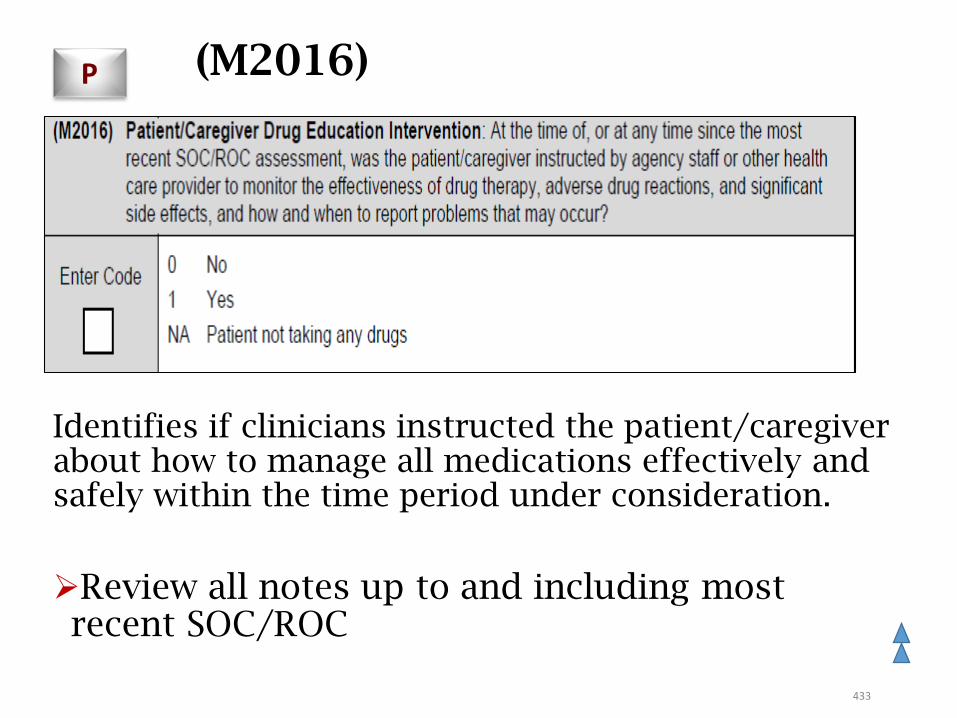
433
(M2016)
Identifies if clinicians instructed the patient/caregiver about how to manage all medications effectively and safely within the time period under consideration.
Review all notes up to and including most recent SOC/ROC
434
M2016: Guidance
• All prescribed and OTC medications by any route.
• Safe/effective management includes:
• Knowledge of effectiveness of drug therapy, including purpose
• Potential side effects and drug reactions
• When and how to contact the appropriate provider
• Specific medication(s) and teaching should be documented.
• The staff at an assisted living facility (ALF) can be considered patients’ caregivers, as can pharmacists, MD, etc.
• Documentation should support interventions to educate patient and caregiver or reason why interventions were not completed.
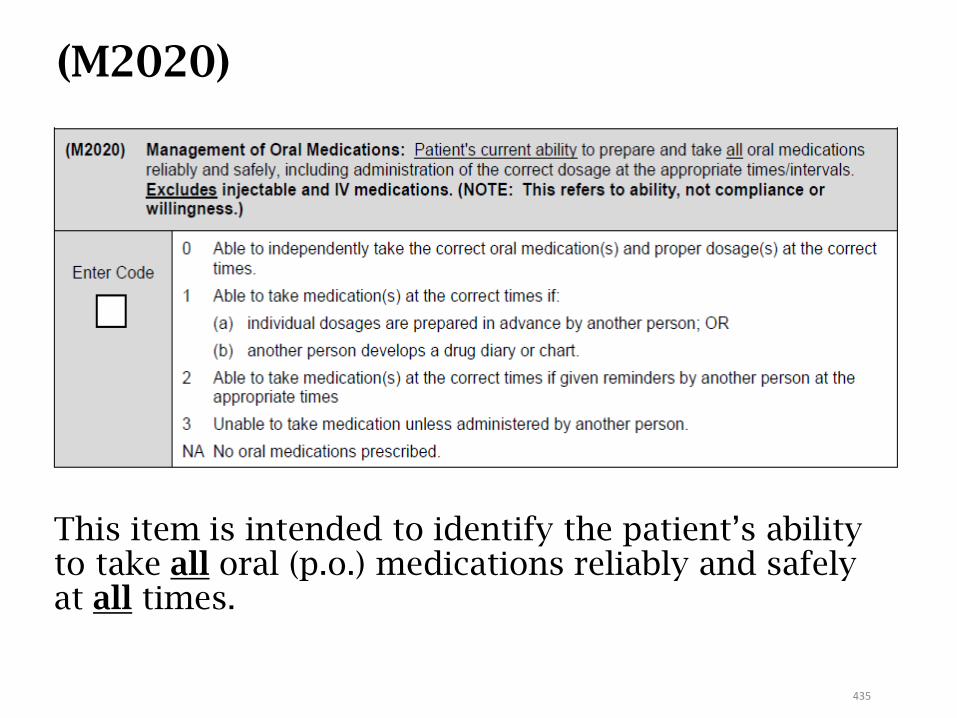
435
This item is intended to identify the patient’s ability to take all oral (p.o.) medications reliably and safely at all times.
(M2020)
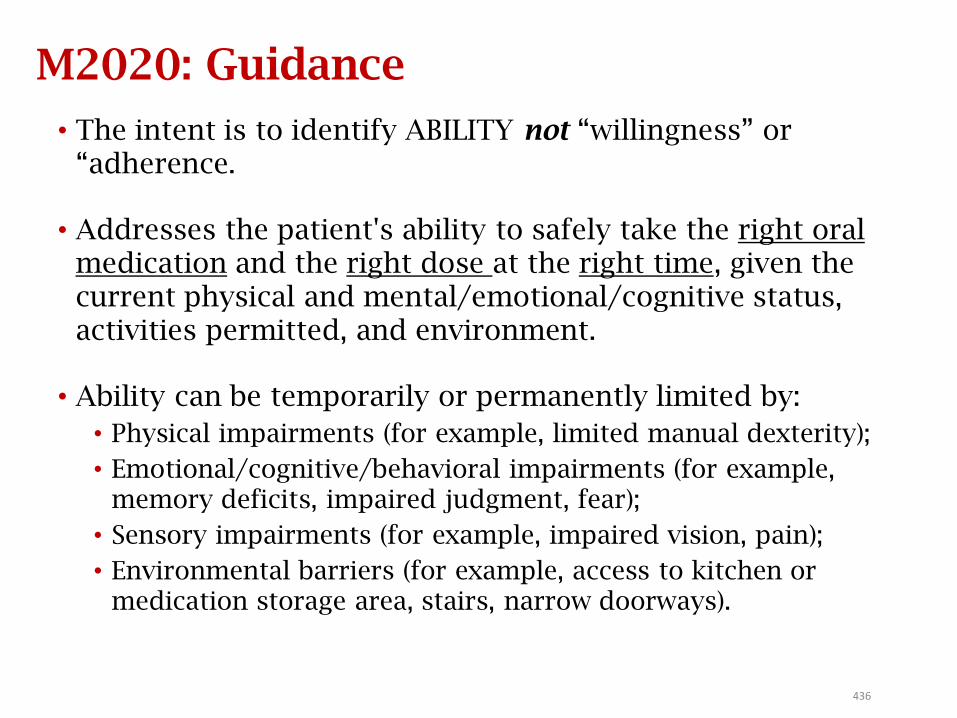
436
M2020: Guidance
• The intent is to identify ABILITY not “willingness” or “adherence.
• Addresses the patient's ability to safely take the right oral medication and the right dose at the right time, given the current physical and mental/emotional/cognitive status, activities permitted, and environment.
• Ability can be temporarily or permanently limited by:
• Physical impairments (for example, limited manual dexterity);
• Emotional/cognitive/behavioral impairments (for example, memory deficits, impaired judgment, fear);
• Sensory impairments (for example, impaired vision, pain);
• Environmental barriers (for example, access to kitchen or medication storage area, stairs, narrow doorways).
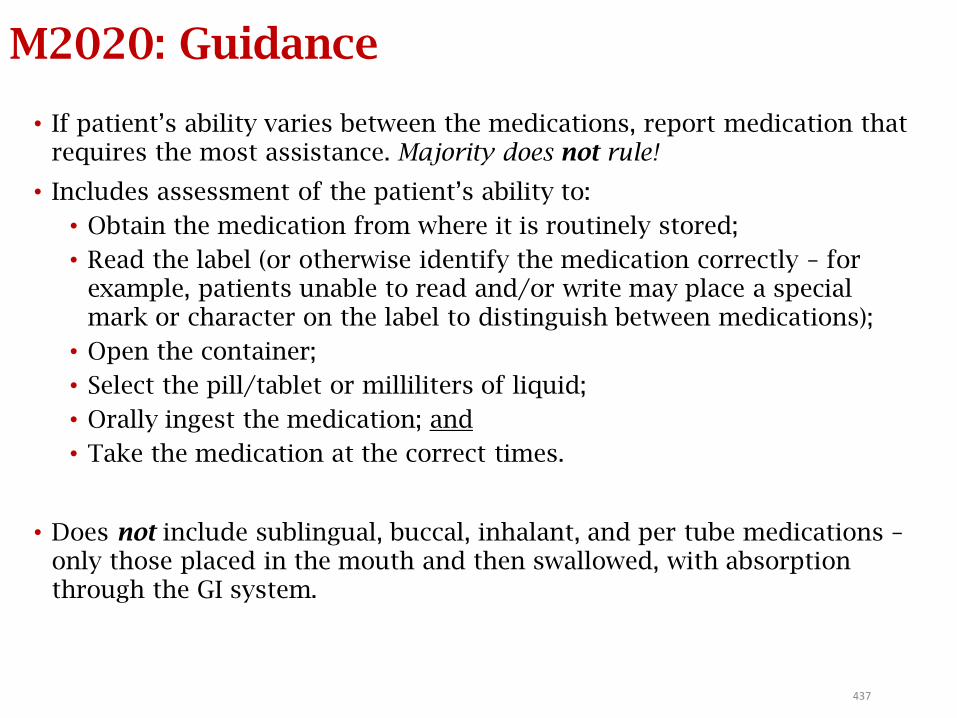
437
M2020: Guidance
• If patient’s ability varies between the medications, report medication that requires the most assistance. Majority does not rule!
• Includes assessment of the patient’s ability to:
• Obtain the medication from where it is routinely stored;
• Read the label (or otherwise identify the medication correctly – for example, patients unable to read and/or write may place a special mark or character on the label to distinguish between medications);
• Open the container;
• Select the pill/tablet or milliliters of liquid;
• Orally ingest the medication; and
• Take the medication at the correct times.
• Does not include sublingual, buccal, inhalant, and per tube medications –only those placed in the mouth and then swallowed, with absorption through the GI system.
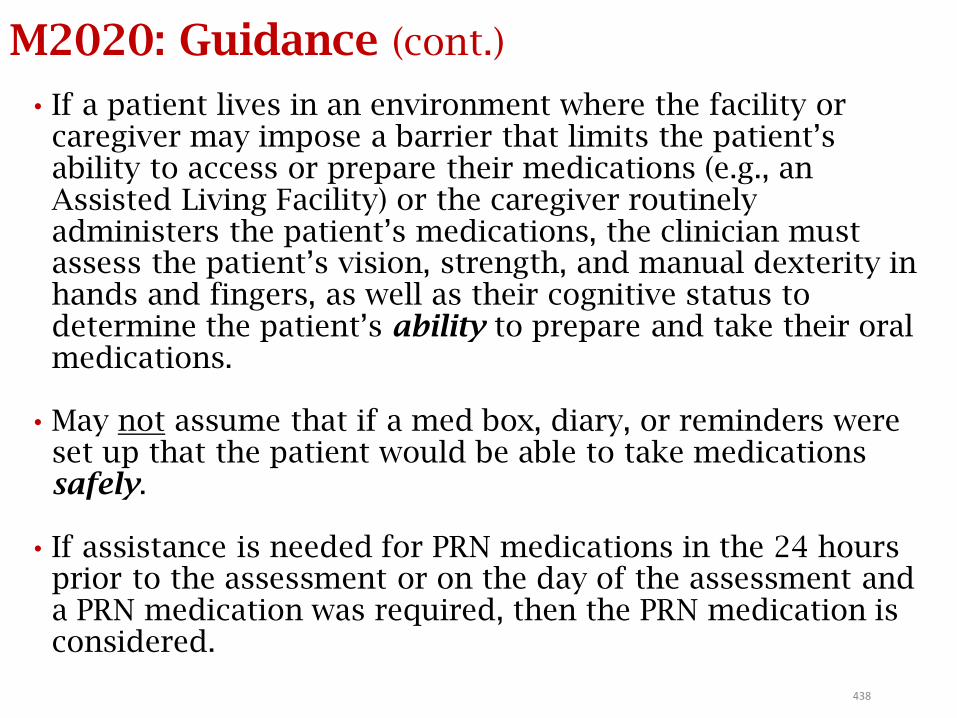
438
M2020: Guidance (cont.)
• If a patient lives in an environment where the facility or caregiver may impose a barrier that limits the patient’s ability to access or prepare their medications (e.g., an Assisted Living Facility) or the caregiver routinely administers the patient’s medications, the clinician must assess the patient’s vision, strength, and manual dexterity in hands and fingers, as well as their cognitive status to determine the patient’s ability to prepare and take their oral medications.
• May not assume that if a med box, diary, or reminders were set up that the patient would be able to take medications safely.
• If assistance is needed for PRN medications in the 24 hours prior to the assessment or on the day of the assessment and a PRN medication was required, then the PRN medication is considered.
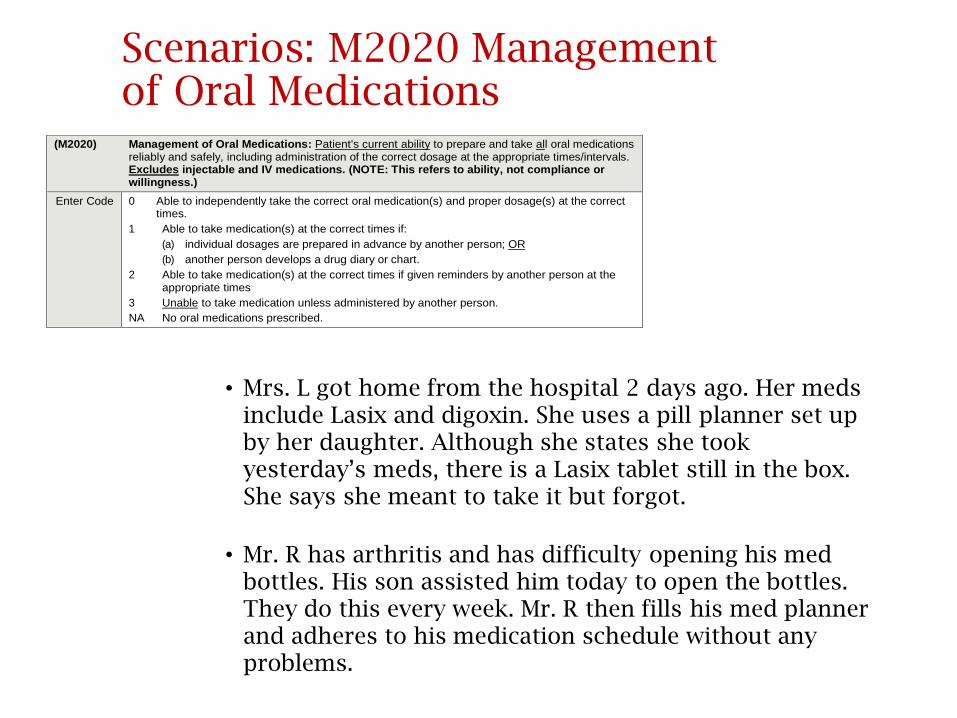
Scenarios: M2020 Management of Oral Medications
• Mrs. L got home from the hospital 2 days ago. Her meds include Lasix and digoxin. She uses a pill planner set up by her daughter. Although she states she took yesterday’s meds, there is a Lasix tablet still in the box. She says she meant to take it but forgot.
• Mr. R has arthritis and has difficulty opening his med bottles. His son assisted him today to open the bottles. They do this every week. Mr. R then fills his med planner and adheres to his medication schedule without any problems.
(M2020) Management of Oral Medications: Patient's current ability to prepare and take all oral medications reliably and safely, including administration of the correct dosage at the appropriate times/intervals. Excludes injectable and IV medications. (NOTE: This refers to ability, not compliance or willingness.)
Enter Code 0 Able to independently take the correct oral medication(s) and proper dosage(s) at the correct times.
1 Able to take medication(s) at the correct times if:
(a) individual dosages are prepared in advance by another person; OR
(b) another person develops a drug diary or chart.
2 Able to take medication(s) at the correct times if given reminders by another person at the appropriate times
3 Unable to take medication unless administered by another person.
NA No oral medications prescribed.
Scenarios: M2020 Management of Oral Medications
• Mrs. L got home from the hospital 2 days ago. Her meds include Lasix and digoxin. She uses a pill planner set up by her daughter. Although she states she took yesterday’s meds, there is a Lasix tablet still in the box. She says she meant to take it but forgot.
• Response 3 - Unable to take medication unless administered by another person
• Mr. R has arthritis and has difficulty opening his med bottles. His son assisted him today to open the bottles. They do this every week. Mr. R then fills his med planner and adheres to his medication schedule without any problems.
• Response 1 - Able to take medication(s) at the correct times if doses are prepared in advance or drug diary or chart is used.
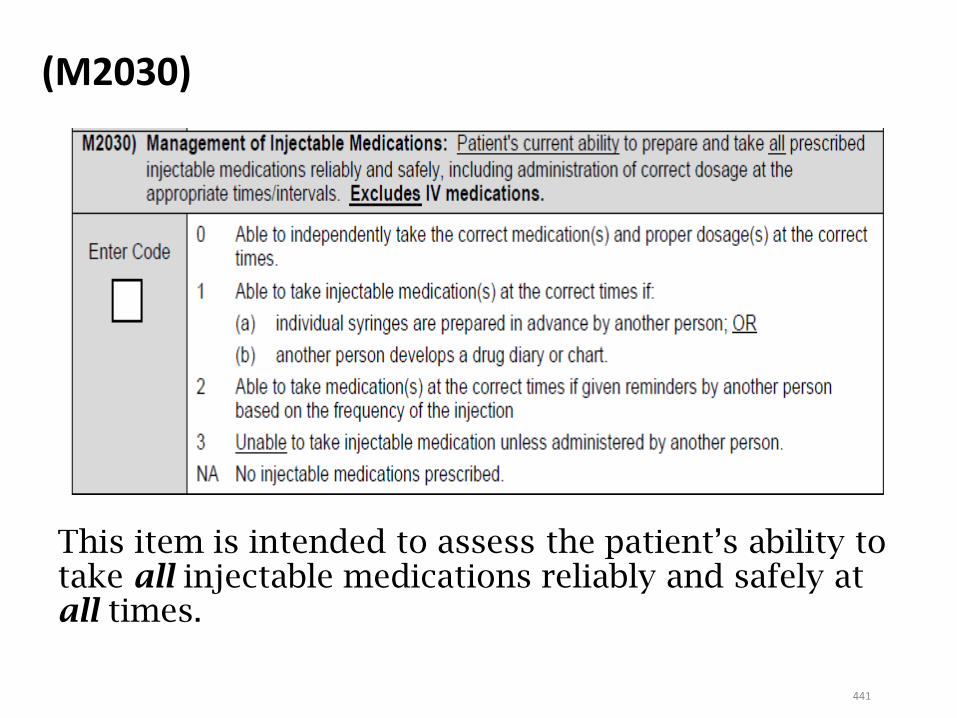
441
This item is intended to assess the patient’s ability to take all injectable medications reliably and safely at all times.
(M2030)

442
M2030: Guidance
• Assesses patient's current ability to prepare and take all prescribed injectable medications reliably and safely at all times. Majority does not rule!
• Excludes IV medication, infusions (i.e., medications given via pump), and medications given in the physician’s office or other settings outside of the home.
• Includes:• One-time injections administered in the home – e.g., flu
vaccine and B12 injections;
• Safe disposal of sharps; and
• PRN injectables included on the POC. If not needed at SOC, use clinical judgment regarding patient’s ability to self-administer.
443
M2030: Guidance (cont.)
• Includes assessment of the patient's ability to obtain the medication from where it is routinely stored, draw up the correct dose accurately using aseptic technique, inject in an appropriate site using correct technique, and dispose of the syringe properly.
• Select Response 3 (unable to administer medication), if the physician ordered the RN to administer an injection in the home – e.g., flu vaccine.
• At discharge, if there are no ongoing, current orders for an injectable medication, correct response = “NA.”
444
M2020/M2030 General Rules
• If a patient does not have the requisite knowledge of a drug’s dose and administration schedule to take the correct dose at the correct time (includes mental/emotional/cognitive ability):
• Response 3, Unable to take medication (oral or injectable) unless administered by another person, is appropriate.
• If a medication (oral or injectable) is not in the home (whether currently due, due at a future point during the episode, or PRN):
• Response 3, Unable to take medication (oral or injectable) unless administered by another person, is appropriate.
445
M2020/M2030 General Rules
• If medications are in the home but not needed or due at time of assessment, observe the patient’s ability based on asking patient to describe steps or simulate task.
• If patient requires assistance to walk to the place where medications are routinely stored or requires someone to retrieve medications for them:
• Response 3, Unable to take medication (oral or injectable) unless administered by another person, is appropriate.
446
M2020 and M2030: Scenarios
1. Patient got home from the hospital 2 days ago. Her meds include Lasix, Lisinopril, Digoxin, and an oral antibiotic. She is also on oxygen. She uses a pill planner set up by her daughter. Although she states she took yesterday’s meds, there is a Lasix tablet still in the box. She says she meant to take it but forgot.
How would you score M2020?
2. Patient, a long time diabetic, is independent in administration of his insulin. At SOC, post left total knee replacement, the nurse assesses that he is unsafe ambulating without supervision and his wife must get his insulin from the refrigerator for him.
How would you score M2030?
447
Answers: M2020 and M2030
1. Patient got home from the hospital 2 days ago. Her meds include Lasix, Lisinopril, Digoxin, and an oral antibiotic. She is also on oxygen. She uses a pill planner set up by her daughter. Although she states she took yesterday’s meds, there is a Lasix tablet still in the box. She says she meant to take it but forgot.
How would you score M2020?Response 3 - Unable to take medication unless administered
by another person
2. Patient, a long time diabetic, is independent in administration of his insulin. At SOC, post left total knee replacement, the nurse assesses that he is unsafe ambulating without supervision and his wife must get his insulin from the refrigerator for him.
How would you score M2030?Response 3 - Unable to take injectable medication unless
administered by another person
Care ManagementM2102
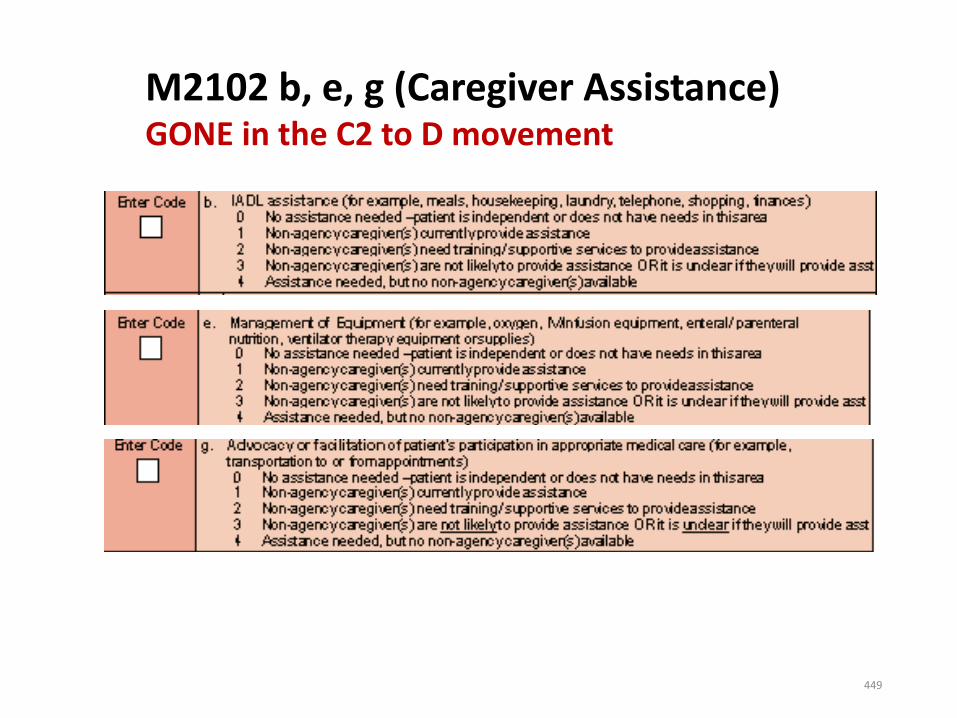
M2102 b, e, g (Caregiver Assistance)GONE in the C2 to D movement
449
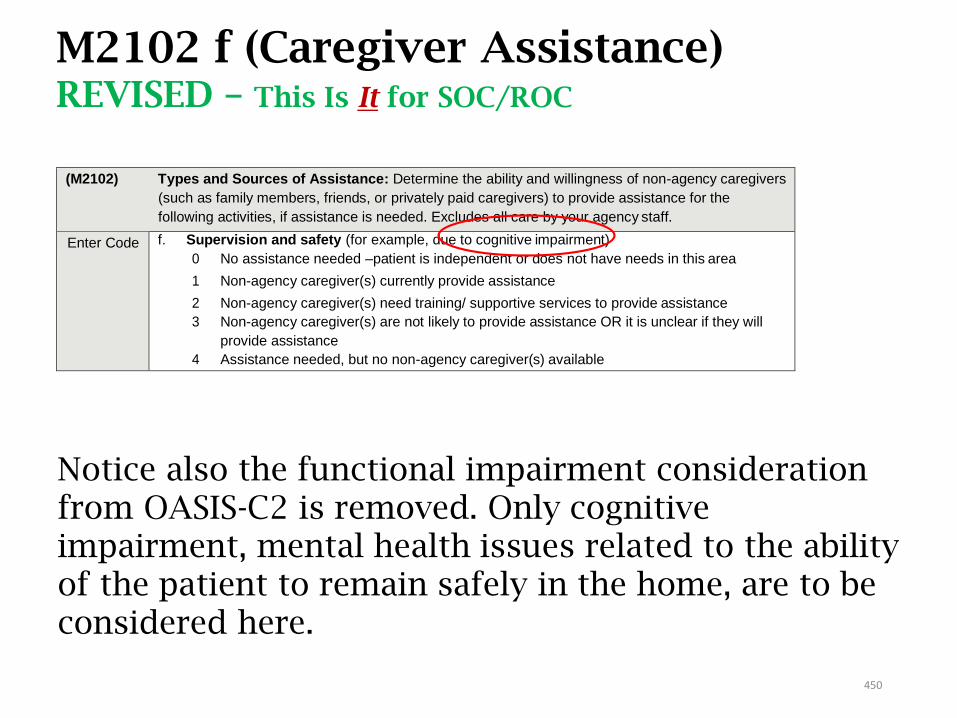
(M2102) Types and Sources of Assistance: Determine the ability and willingness of non-agency caregivers
(such as family members, friends, or privately paid caregivers) to provide assistance for the
following activities, if assistance is needed. Excludes all care by your agency staff.
Enter Code f. Supervision and safety (for example, due to cognitive impairment)
0 No assistance needed –patient is independent or does not have needs in this area
1 Non-agency caregiver(s) currently provide assistance
2 Non-agency caregiver(s) need training/ supportive services to provide assistance
3 Non-agency caregiver(s) are not likely to provide assistance OR it is unclear if they will
provide assistance
4 Assistance needed, but no non-agency caregiver(s) available
M2102 f (Caregiver Assistance)REVISED – This Is It for SOC/ROC
Notice also the functional impairment consideration from OASIS-C2 is removed. Only cognitive impairment, mental health issues related to the ability of the patient to remain safely in the home, are to be considered here.
450
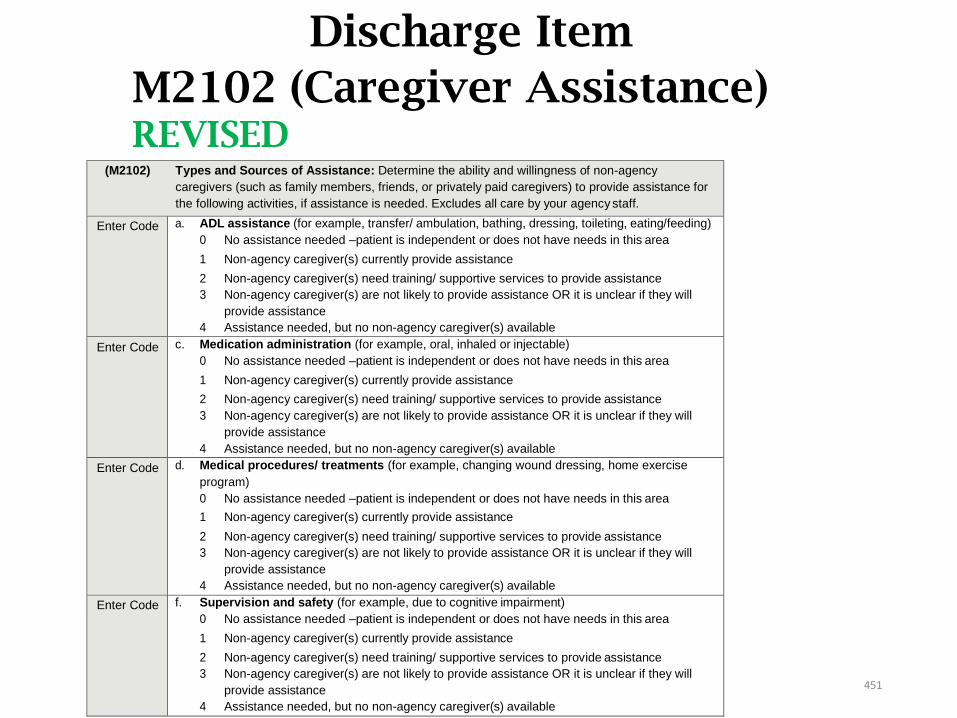
Discharge Item
M2102 (Caregiver Assistance)REVISED
(M2102) Types and Sources of Assistance: Determine the ability and willingness of non-agency
caregivers (such as family members, friends, or privately paid caregivers) to provide assistance for
the following activities, if assistance is needed. Excludes all care by your agency staff.
Enter Code a. ADL assistance (for example, transfer/ ambulation, bathing, dressing, toileting, eating/feeding)
0 No assistance needed –patient is independent or does not have needs in this area
1 Non-agency caregiver(s) currently provide assistance
2 Non-agency caregiver(s) need training/ supportive services to provide assistance
3 Non-agency caregiver(s) are not likely to provide assistance OR it is unclear if they will
provide assistance
4 Assistance needed, but no non-agency caregiver(s) available
Enter Code c. Medication administration (for example, oral, inhaled or injectable)
0 No assistance needed –patient is independent or does not have needs in this area
1 Non-agency caregiver(s) currently provide assistance
2 Non-agency caregiver(s) need training/ supportive services to provide assistance
3 Non-agency caregiver(s) are not likely to provide assistance OR it is unclear if they will
provide assistance
4 Assistance needed, but no non-agency caregiver(s) available
Enter Code d. Medical procedures/ treatments (for example, changing wound dressing, home exercise
program)
0 No assistance needed –patient is independent or does not have needs in this area
1 Non-agency caregiver(s) currently provide assistance
2 Non-agency caregiver(s) need training/ supportive services to provide assistance
3 Non-agency caregiver(s) are not likely to provide assistance OR it is unclear if they will
provide assistance
4 Assistance needed, but no non-agency caregiver(s) available
Enter Code f. Supervision and safety (for example, due to cognitive impairment)
0 No assistance needed –patient is independent or does not have needs in this area
1 Non-agency caregiver(s) currently provide assistance
2 Non-agency caregiver(s) need training/ supportive services to provide assistance
3 Non-agency caregiver(s) are not likely to provide assistance OR it is unclear if they will
provide assistance
4 Assistance needed, but no non-agency caregiver(s) available
451

Impact
• Reminder, at SOC/ROC, the only item was M2102(f), inquiring about the ability and willingness of non-agency caregivers to provide supervision and safety.
HOWEVER, at discharge, now the items for (M2102a) ADL assistance, (M2102c) med administration, and (M2102d) medical procedures/treatments are present as well.
It is imperative that clinicians query and document at SOC/ROC how the non-agency caregivers are handling these items and provide training/ interventions as needed to ensure a positive outcome at the time of discharge. Does your EMR have a trigger for this?
452
M2102: Sources of Assistance
•Report what is known on day of assessment regarding availability and ability of CGs to provide assistance for upcoming episode or at discharge.
•If patient needs assistance with any aspect of a category, consider the aspect that represents the most need and the availability of caregivers to meet the need.
•If more than one response in a row applies – select response that represents the greatest need(s).
•For example – CG provides assistance currently but also needs training/supportive services to provide assistance. Select Response 2 in appropriate row.
•Staff providing care employed by a Medicaid In-Home provider would be considered non-agency caregivers for the purpose of responding to M2102 if there are separate and distinct provider numbers for each provider type
453
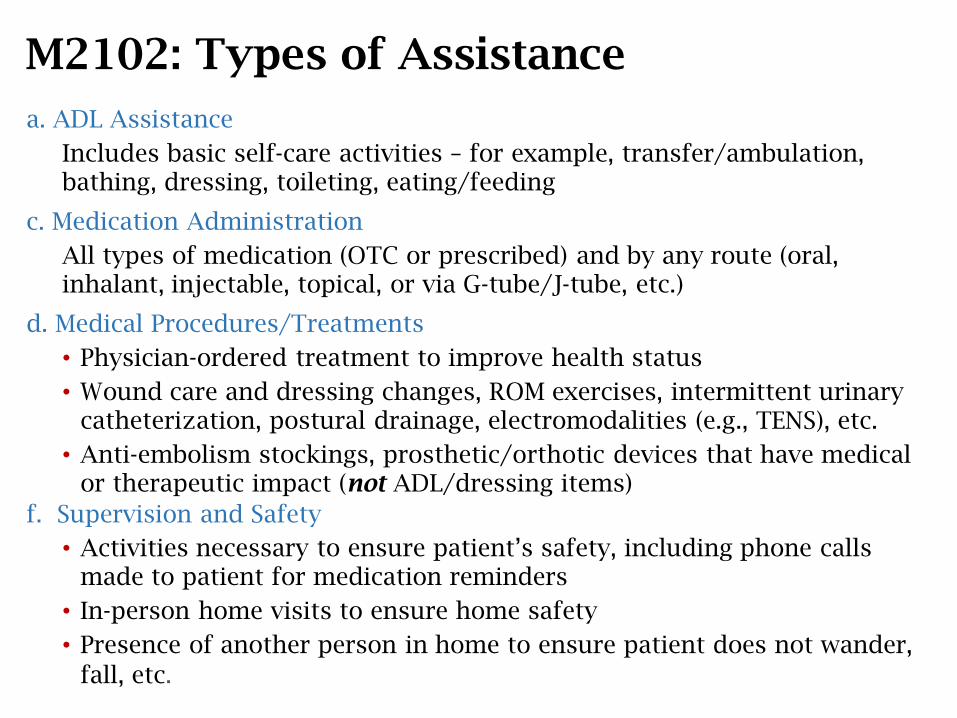
M2102: Types of Assistance
a. ADL Assistance
Includes basic self-care activities – for example, transfer/ambulation, bathing, dressing, toileting, eating/feeding
c. Medication Administration
All types of medication (OTC or prescribed) and by any route (oral, inhalant, injectable, topical, or via G-tube/J-tube, etc.)
d. Medical Procedures/Treatments
• Physician-ordered treatment to improve health status
• Wound care and dressing changes, ROM exercises, intermittent urinary catheterization, postural drainage, electromodalities (e.g., TENS), etc.
• Anti-embolism stockings, prosthetic/orthotic devices that have medical or therapeutic impact (not ADL/dressing items)
f. Supervision and Safety
• Activities necessary to ensure patient’s safety, including phone calls made to patient for medication reminders
• In-person home visits to ensure home safety
• Presence of another person in home to ensure patient does not wander,
fall, etc.
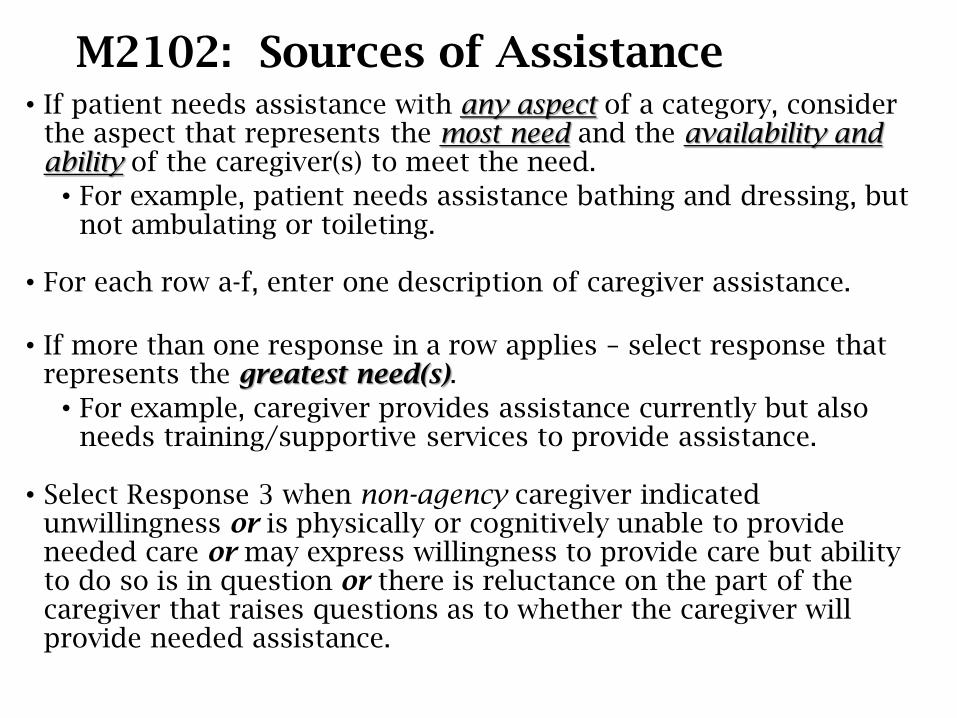
M2102: Sources of Assistance• If patient needs assistance with any aspect of a category, consider
the aspect that represents the most need and the availability and ability of the caregiver(s) to meet the need.
• For example, patient needs assistance bathing and dressing, but not ambulating or toileting.
• For each row a-f, enter one description of caregiver assistance.
• If more than one response in a row applies – select response that represents the greatest need(s).
• For example, caregiver provides assistance currently but also needs training/supportive services to provide assistance.
• Select Response 3 when non-agency caregiver indicated unwillingness or is physically or cognitively unable to provide needed care or may express willingness to provide care but ability to do so is in question or there is reluctance on the part of the caregiver that raises questions as to whether the caregiver will provide needed assistance.
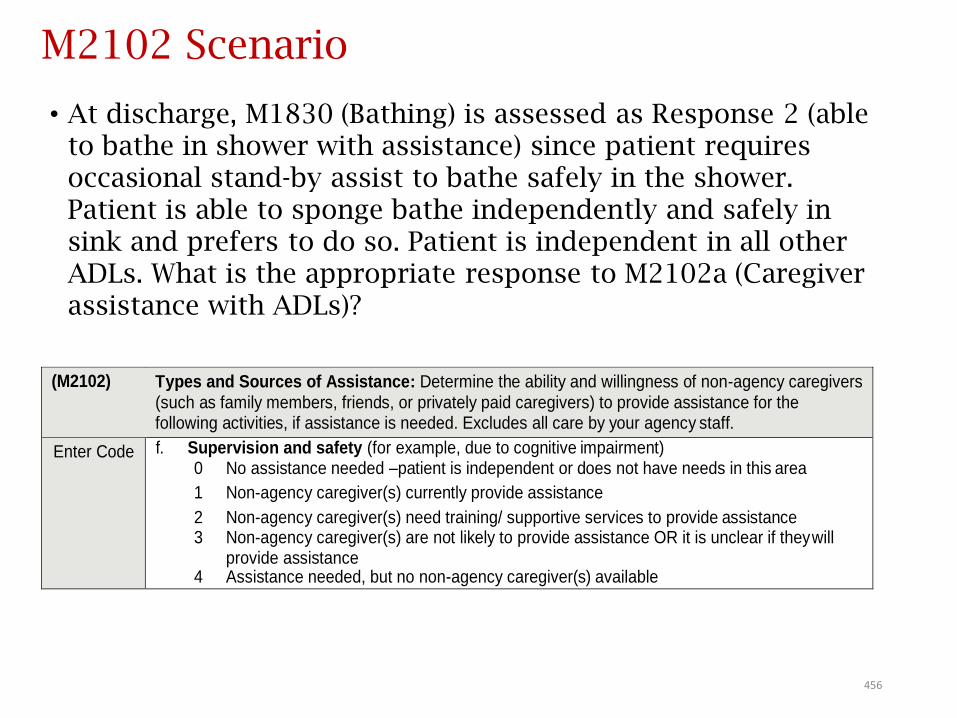
M2102 Scenario
• At discharge, M1830 (Bathing) is assessed as Response 2 (able to bathe in shower with assistance) since patient requires occasional stand-by assist to bathe safely in the shower. Patient is able to sponge bathe independently and safely in sink and prefers to do so. Patient is independent in all other ADLs. What is the appropriate response to M2102a (Caregiver assistance with ADLs)?
456
(M2102) Types and Sources of Assistance: Determine the ability and willingness of non-agency caregivers
(such as family members, friends, or privately paid caregivers) to provide assistance for the following activities, if assistance is needed. Excludes all care by your agency staff.
Enter Code f. Supervision and safety (for example, due to cognitive impairment) 0 No assistance needed –patient is independent or does not have needs in this area
1 Non-agency caregiver(s) currently provide assistance
2 Non-agency caregiver(s) need training/ supportive services to provide assistance 3 Non-agency caregiver(s) are not likely to provide assistance OR it is unclear if they will
provide assistance 4 Assistance needed, but no non-agency caregiver(s) available
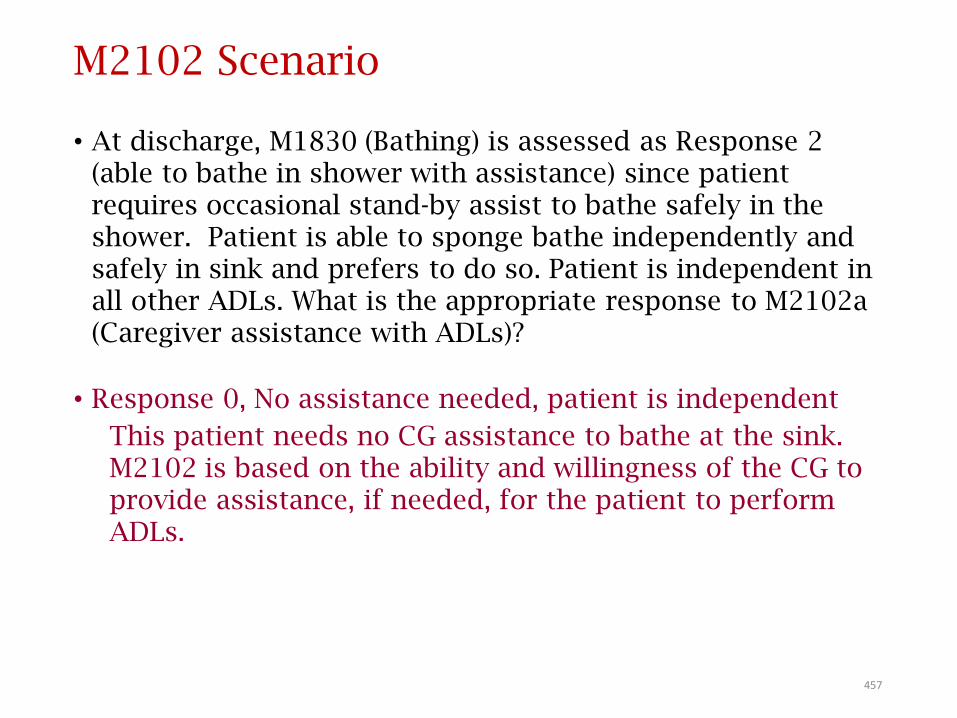
M2102 Scenario
• At discharge, M1830 (Bathing) is assessed as Response 2 (able to bathe in shower with assistance) since patient requires occasional stand-by assist to bathe safely in the shower. Patient is able to sponge bathe independently and safely in sink and prefers to do so. Patient is independent in all other ADLs. What is the appropriate response to M2102a (Caregiver assistance with ADLs)?
• Response 0, No assistance needed, patient is independent
This patient needs no CG assistance to bathe at the sink. M2102 is based on the ability and willingness of the CG to provide assistance, if needed, for the patient to perform ADLs.
457
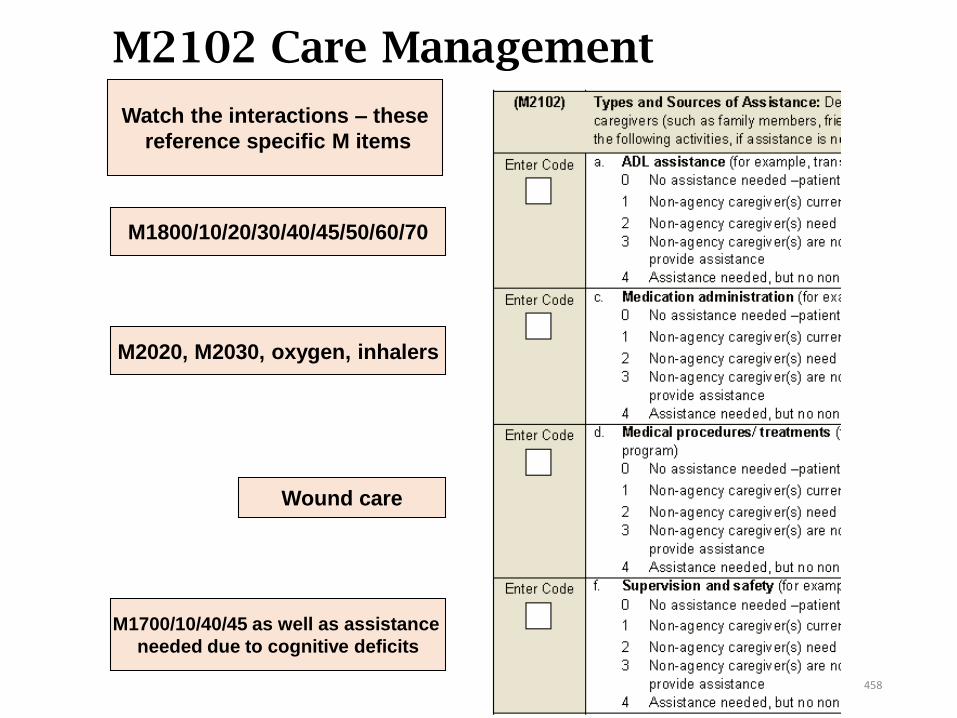
M2102 Care Management tipsWatch the interactions – these
reference specific M items
M1800/10/20/30/40/45/50/60/70
M2020, M2030, oxygen, inhalers
Wound care
M1700/10/40/45 as well as assistance
needed due to cognitive deficits
458
Therapy NeedM2200
459
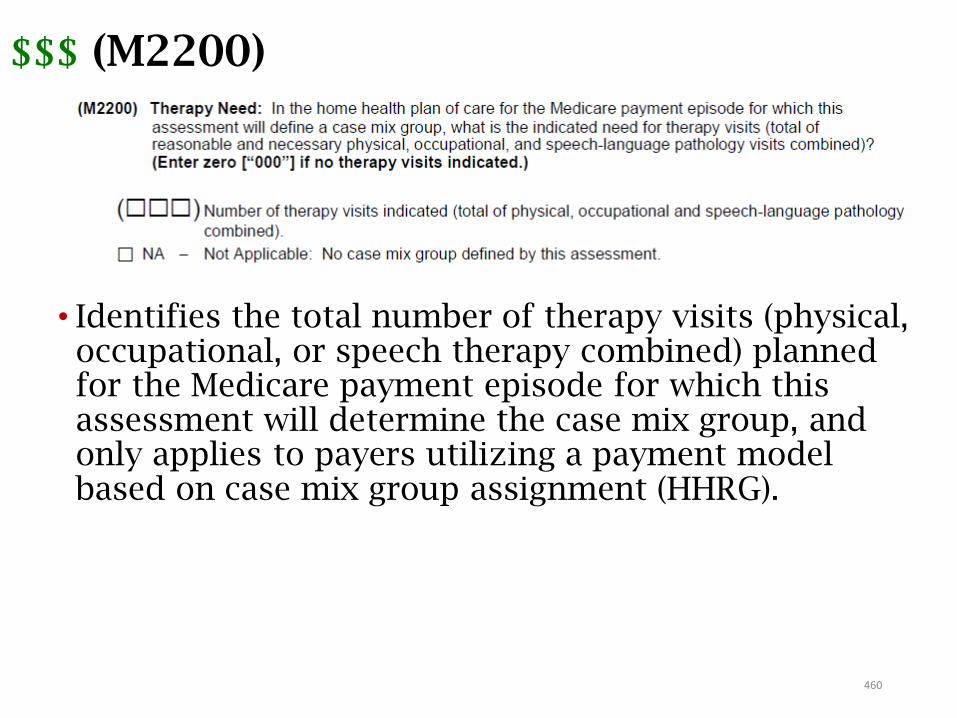
460
$$$ (M2200)
• Identifies the total number of therapy visits (physical, occupational, or speech therapy combined) planned for the Medicare payment episode for which this assessment will determine the case mix group, and only applies to payers utilizing a payment model based on case mix group assignment (HHRG).
461
$$$ (M2200)
• For multidisciplinary cases, therapists are responsible for informing the RN completing this item of the number of visits ordered. Coordination of patient care is a Condition of Participation.
• Per the Q&As, "If the number of visits that will be needed is uncertain, provide your best estimate."
• This could affect the M0090 date.
Only the SOC and FU (Recertification) result in a case mix assignment.
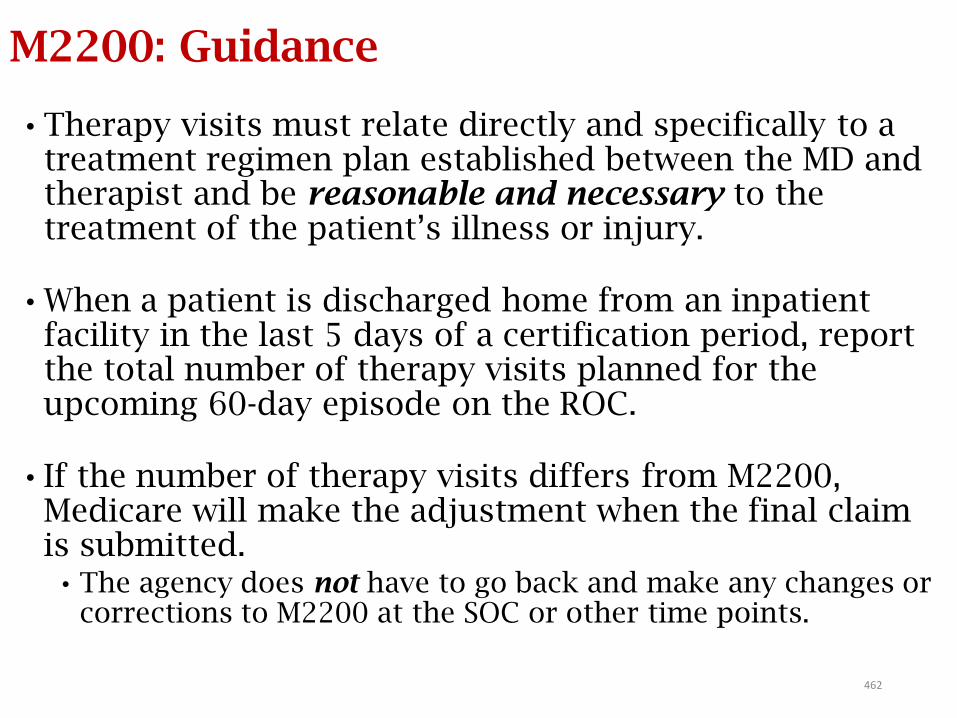
462
M2200: Guidance
• Therapy visits must relate directly and specifically to a treatment regimen plan established between the MD and therapist and be reasonable and necessary to the treatment of the patient’s illness or injury.
• When a patient is discharged home from an inpatient facility in the last 5 days of a certification period, report the total number of therapy visits planned for the upcoming 60-day episode on the ROC.
• If the number of therapy visits differs from M2200, Medicare will make the adjustment when the final claim is submitted.
• The agency does not have to go back and make any changes or corrections to M2200 at the SOC or other time points.
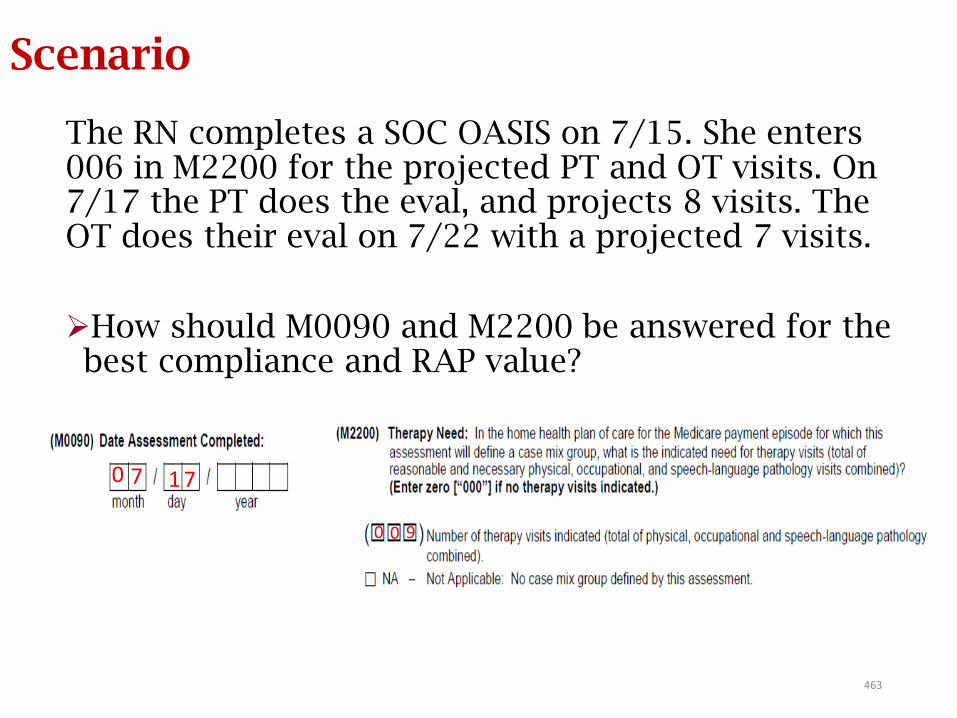
463
Scenario
The RN completes a SOC OASIS on 7/15. She enters 006 in M2200 for the projected PT and OT visits. On 7/17 the PT does the eval, and projects 8 visits. The OT does their eval on 7/22 with a projected 7 visits.
How should M0090 and M2200 be answered for the best compliance and RAP value?
0 7 1 7
900
Intervention SynopsisM2401
464
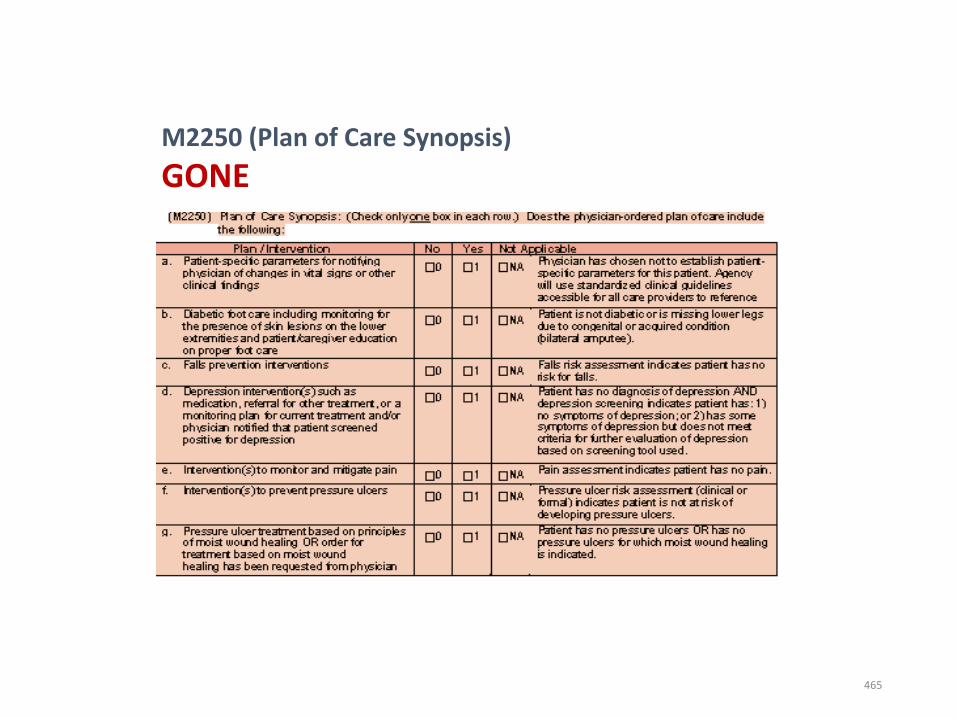
M2250 (Plan of Care Synopsis)
GONE
465
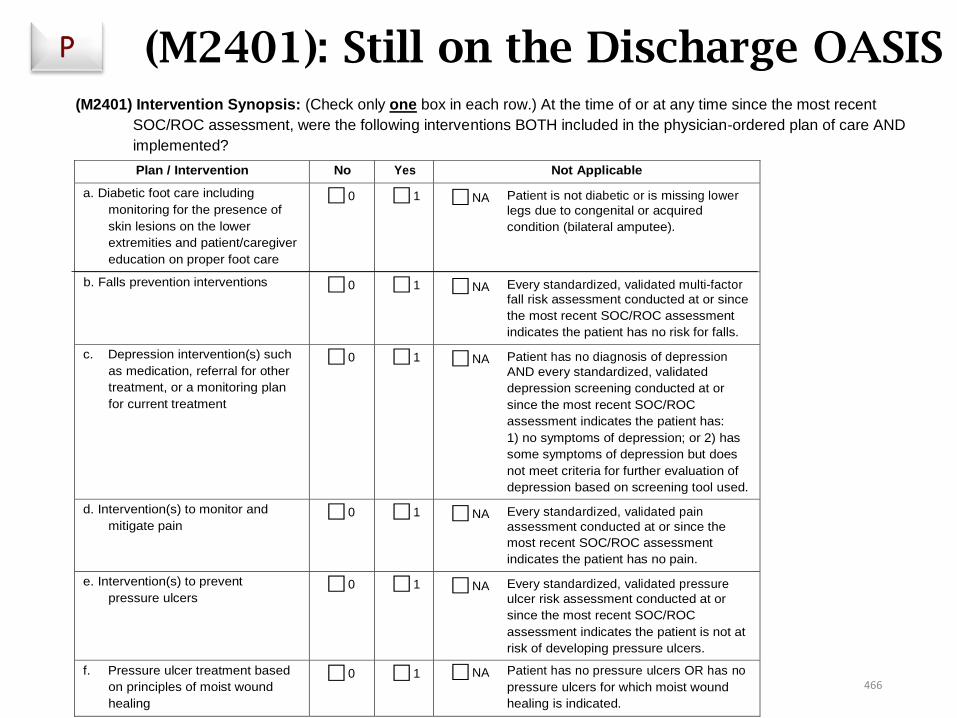
(M2401): Still on the Discharge OASIS …
Plan / Intervention No Yes Not Applicable
a. Diabetic foot care including
monitoring for the presence of
skin lesions on the lower
extremities and patient/caregiver
education on proper foot care
⃞ 0 ⃞ 1 ⃞ NA Patient is not diabetic or is missing lower
legs due to congenital or acquired
condition (bilateral amputee).
b. Falls prevention interventions ⃞ 0 ⃞ 1 ⃞ NA Every standardized, validated multi-factor
fall risk assessment conducted at or since
the most recent SOC/ROC assessment
indicates the patient has no risk for falls.
c. Depression intervention(s) such
as medication, referral for other
treatment, or a monitoring plan
for current treatment
⃞ 0 ⃞ 1 ⃞ NA Patient has no diagnosis of depression
AND every standardized, validated
depression screening conducted at or
since the most recent SOC/ROC
assessment indicates the patient has:
1) no symptoms of depression; or 2) has
some symptoms of depression but does
not meet criteria for further evaluation of
depression based on screening tool used.
d. Intervention(s) to monitor and
mitigate pain ⃞ 0 ⃞ 1 ⃞ NA Every standardized, validated pain
assessment conducted at or since the
most recent SOC/ROC assessment
indicates the patient has no pain.
e. Intervention(s) to prevent
pressure ulcers ⃞ 0 ⃞ 1 ⃞ NA Every standardized, validated pressure
ulcer risk assessment conducted at or
since the most recent SOC/ROC
assessment indicates the patient is not at
risk of developing pressure ulcers.
f. Pressure ulcer treatment based
on principles of moist wound
healing
⃞ 0 ⃞ 1 ⃞ NA Patient has no pressure ulcers OR has no
pressure ulcers for which moist wound
healing is indicated.
(M2401) Intervention Synopsis: (Check only one box in each row.) At the time of or at any time since the most recent
SOC/ROC assessment, were the following interventions BOTH included in the physician-ordered plan of care AND
implemented?
P
466
Impact: What Is the Potential Problem With M2250 POC No Longer Present?
Reminder: What “Yes” means for the M2401 Intervention
Synopsis items:
1. Interventions are on the POC to address the condition
AND
2. Documentation supports interventions were completed at
some point during the episode
SO … what’s the problem?
• M2250 is no longer present, with that item providing us a
checklist, a way to remind us to be accountable to these
conditions, to include them on the POC. It is crucial that
documentation (EMR, etc.) has a way to track these tasks for
accuracy in completion of the M2401 individual items.
467
Getting M2401 Right
• First: Can you answer “Yes” to a specific item?• Understand what must be included in the
interventions/orders.
• Understand the CMS guidance (including Q&As).
• Next: If item cannot be answered “Yes”, is “NA” appropriate?
• Understand NA criteria for the item.
• If “Yes” and “NA” are not appropriate, then “No” is the only option left.
468

M2401: General Guidance
(M2401): At the time of or at any time since the most recent SOC/ROC assessment, were the following interventions BOTH:
─ Included in the physician-ordered plan of care AND
─ Implemented
• Respond “Yes” when :
• Specific clinical intervention(s) is (are) included in the POC AND
• Specific clinical intervention(s) is (are) implemented at the time of the previous OASIS assessment or since that time
• Respond “No” if “Yes” and “NA” are not appropriate and when either:
• Specific intervention(s) is (are) not on POC OR
• Intervention(s) is (are) not implemented
• Document reason there were no interventions on POC or why ordered interventions were not implemented.
469
M2401: General Guidance
• M2401 – it’s OK to respond “yes” even if patient was not assessed to be at risk as long as interventions were in the physician-ordered POC and were implemented.
• For example:
• Orders to monitor and mitigate pain
• Orders to implement fall risk prevention measure
• Orders to prevent skin breakdown and improve skin integrity
470
M2401: General Guidance
• Clinical record documentation should detail:• The tool or clinical factors used to assess the patient.
• The findings as they relate to the assessment.
• An analysis to support the OASIS response selected.
• Standardized and validated tool(s) is (are):• Required to have been completed to respond “NA” to: pain,
fall risk, depression and pressure ulcer risk assessment in M2401.
• Required to respond “NA” in M2401.
471
What dressings qualify as moist wound healing treatments?
• A moist wound healing treatment is any primary dressing that hydrates or delivers moisture to a wound, thus promoting an optimal wound environment. This includes:
Films Negative wound pressure therapy
Alginates Unna boots
Hydrocolloids Medicated creams
Hydrogels Medicated ointments
Collagen
472
473
Physician-Ordered Plan of Care
• The “physician-ordered plan of care” means that the patient’s condition has been discussed and there is agreement as to the POC between the home health agency staff and the physician.
• Orders may be obtained ONLY from “physician.”• MDs, DOs, DPMs within legal scope of practice
• Measures initiated on the POC synopsis should be reflected in the physician-ordered POC.
• The physician plan of care includes all additional orders as an extension of the original POC.
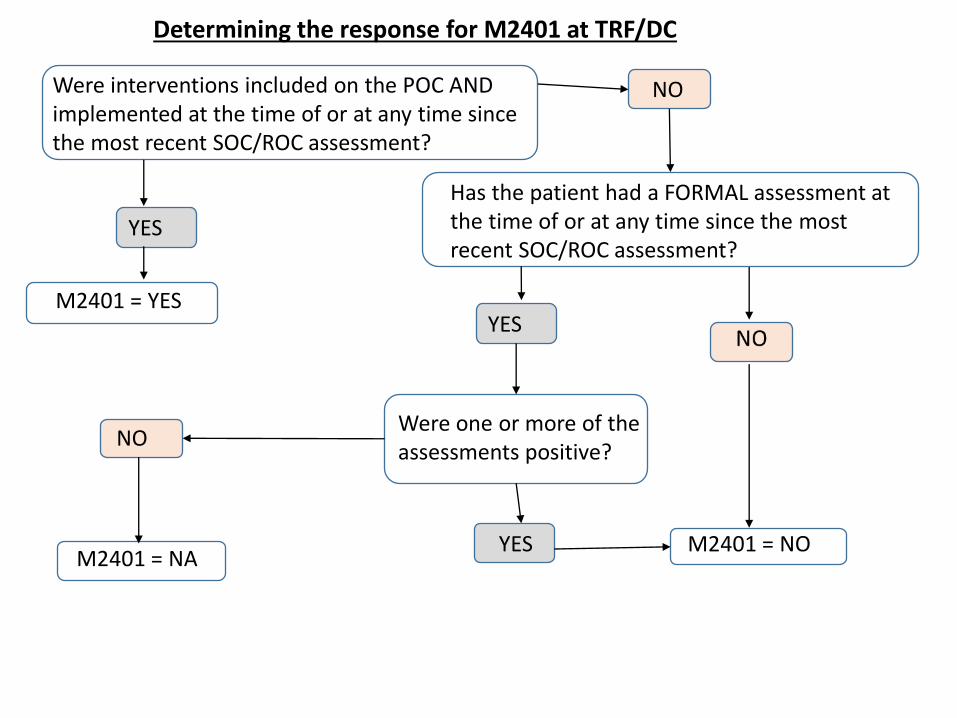
M2401 = NA
NO
YES M2401 = NO
Were one or more of the assessments positive?
Has the patient had a FORMAL assessment at the time of or at any time since the most recent SOC/ROC assessment?
Were interventions included on the POC AND implemented at the time of or at any time since the most recent SOC/ROC assessment?
Determining the response for M2401 at TRF/DC
YES
YES
NO
M2401 = YES
GG and J Items
475
GG Items
• As the IMPACT Act continues to evolve across all PAC settings, more GG items will be introduced into the OASIS. Unless noted otherwise, the scoring/“coding” for these items is the same.
• Be careful when coding these items and choosing the response for a similar task in the M18 section of the OASIS. Verbiage varies, as do parts of the task itself, and there are generally not direct crosswalks from the GG item to the OASIS item (see M18-GG Crosswalk Tool).
476
What are the GG items for?• QUESTION 30: The response-specific instructions in the OASIS
Guidance Manual for GG0130 and GG0170 state that the QRP only
requires coding a minimum of one self-care or mobility discharge
goal. If an agency decides to establish a discharge goal for just one
functional activity, how would the other remaining activities be
coded?
• ANSWER 30: Effective January 1, 2019, select activities from GG0130
and GG0170 are used to calculate the quality measure Application of
Percent of Patients with an Admission and Discharge Functional
Assessment and a Care Plan that Addresses Function (NQF #2631).
• The activities utilized in the measure are:
• GG0130. Self-care items (GG0130A. Eating, GG0130B. Oral hygiene, GG0130C. Toileting
hygiene).
• GG0170. Mobility Items (GG0170B. Sit to lying, GG0170C. Lying to sitting on side of bed,
GG0170D. Sit to stand, GG0170E. Chair/bed-to-chair transfer, GG0170F. Toilet Transfer,
GG0170J. Walk 50 feet with two turns, GG0170K. Walk 150 feet, GG0170R. Wheel 50 feet
with two turns, GG0170S. Wheel 150 feet).
477
OASIS-D Changes Summary:
OASIS-D Items ADDEDItem Description
GG0100 Prior Functioning
GG0110 Prior Device Use
GG0130 Self-Care
GG0170 Mobility
J1800 Any Falls Since SOC/ROC
J1900 Number of Falls Since SOC/ROC
478
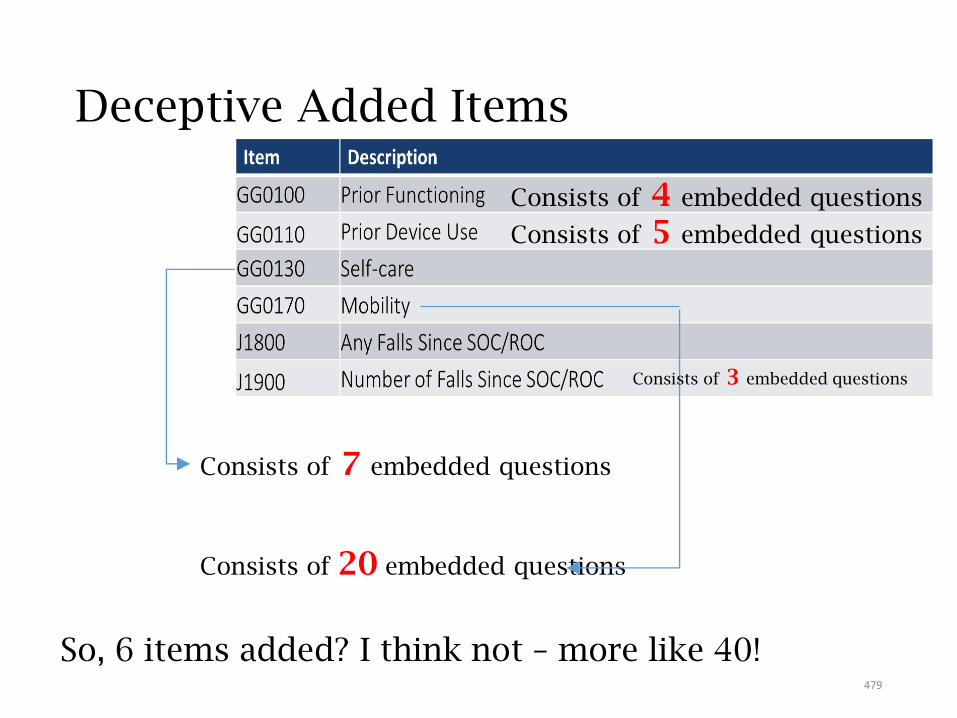
Deceptive Added Items
Consists of 7 embedded questions
Consists of 20 embedded questions
So, 6 items added? I think not – more like 40!
Consists of 4 embedded questions
Consists of 5 embedded questions
Consists of 3 embedded questions
479
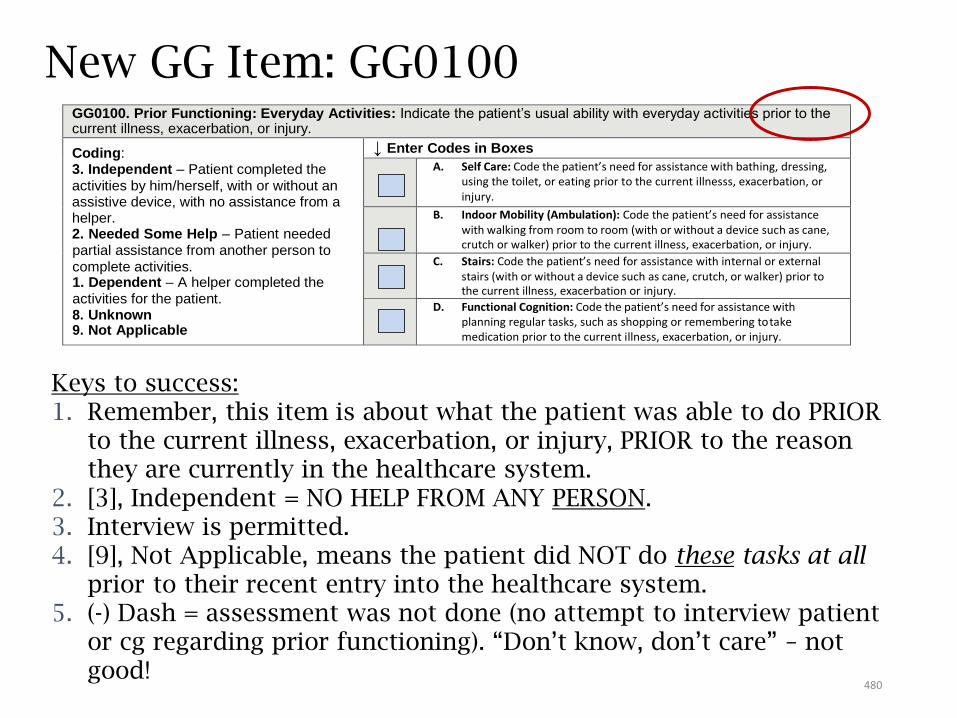
New GG Item: GG0100GG0100. Prior Functioning: Everyday Activities: Indicate the patient’s usual ability with everyday activities prior to the current illness, exacerbation, or injury.
Coding: 3. Independent – Patient completed the
activities by him/herself, with or without an assistive device, with no assistance from a helper. 2. Needed Some Help – Patient needed
partial assistance from another person to
complete activities. 1. Dependent – A helper completed the
activities for the patient. 8. Unknown 9. Not Applicable
↓ Enter Codes in Boxes
A. Self Care: Code the patient’s need for assistance with bathing, dressing, using the toilet, or eating prior to the current illnesss, exacerbation, or injury.
B. Indoor Mobility (Ambulation): Code the patient’s need for assistance with walking from room to room (with or without a device such as cane, crutch or walker) prior to the current illness, exacerbation, or injury.
C. Stairs: Code the patient’s need for assistance with internal or external stairs (with or without a device such as cane, crutch, or walker) prior to the current illness, exacerbation or injury.
D. Functional Cognition: Code the patient’s need for assistance with planning regular tasks, such as shopping or remembering to take medication prior to the current illness, exacerbation, or injury.
Keys to success:1. Remember, this item is about what the patient was able to do PRIOR
to the current illness, exacerbation, or injury, PRIOR to the reason they are currently in the healthcare system.
2. [3], Independent = NO HELP FROM ANY PERSON.3. Interview is permitted.4. [9], Not Applicable, means the patient did NOT do these tasks at all
prior to their recent entry into the healthcare system.5. (-) Dash = assessment was not done (no attempt to interview patient
or cg regarding prior functioning). “Don’t know, don’t care” – not good!
480
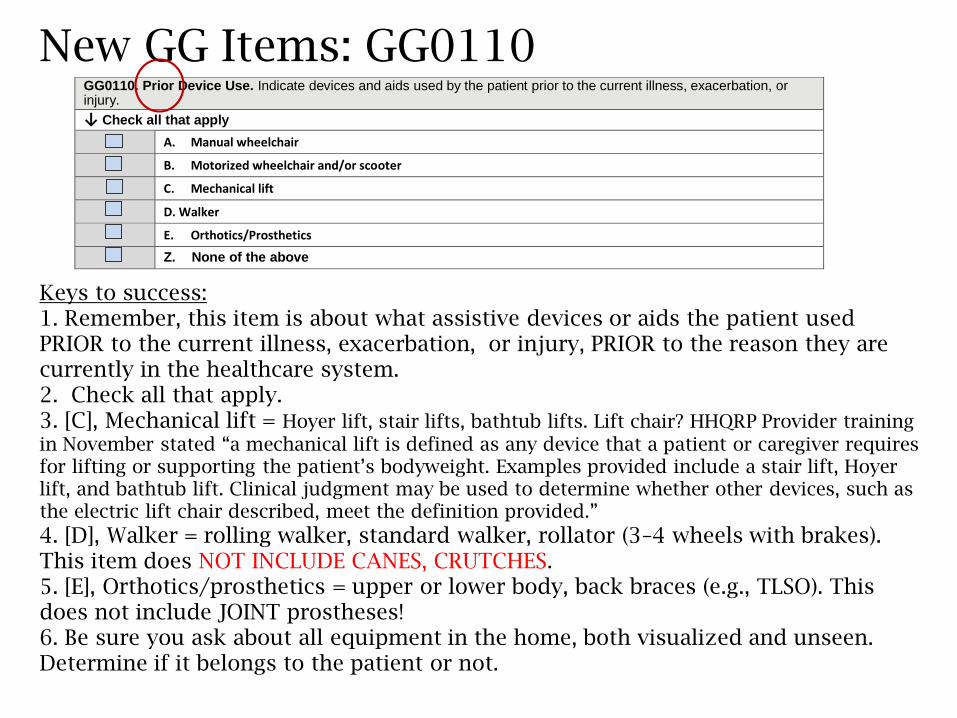
GG0110. Prior Device Use. Indicate devices and aids used by the patient prior to the current illness, exacerbation, or injury.
↓ Check all that apply
A. Manual wheelchair
B. Motorized wheelchair and/or scooter
C. Mechanical lift
D. Walker
E. Orthotics/Prosthetics
Z. None of the above
Keys to success:1. Remember, this item is about what assistive devices or aids the patient used PRIOR to the current illness, exacerbation, or injury, PRIOR to the reason they are currently in the healthcare system.2. Check all that apply.3. [C], Mechanical lift = Hoyer lift, stair lifts, bathtub lifts. Lift chair? HHQRP Provider training
in November stated “a mechanical lift is defined as any device that a patient or caregiver requires for lifting or supporting the patient’s bodyweight. Examples provided include a stair lift, Hoyer lift, and bathtub lift. Clinical judgment may be used to determine whether other devices, such as the electric lift chair described, meet the definition provided.”
4. [D], Walker = rolling walker, standard walker, rollator (3–4 wheels with brakes). This item does NOT INCLUDE CANES, CRUTCHES.5. [E], Orthotics/prosthetics = upper or lower body, back braces (e.g., TLSO). This does not include JOINT prostheses!6. Be sure you ask about all equipment in the home, both visualized and unseen. Determine if it belongs to the patient or not.
New GG Items: GG0110
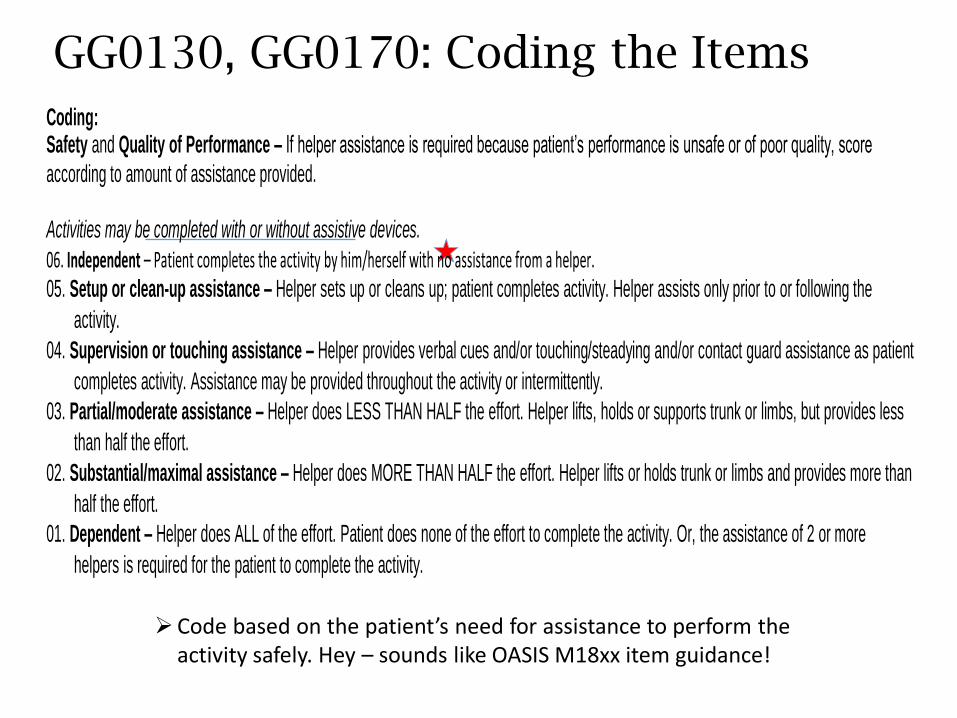
GG0130, GG0170: Coding the Items
Coding: Safety and Quality of Performance – If helper assistance is required because patient’s performance is unsafe or of poor quality, score
according to amount of assistance provided.
Activities may be completed with or without assistive devices.
06. Independent – Patient completes the activity by him/herself with no assistance from a helper. 05. Setup or clean-up assistance – Helper sets up or cleans up; patient completes activity. Helper assists only prior to or following the
activity.
04. Supervision or touching assistance – Helper provides verbal cues and/or touching/steadying and/or contact guard assistance as patient
completes activity. Assistance may be provided throughout the activity or intermittently.
03. Partial/moderate assistance – Helper does LESS THAN HALF the effort. Helper lifts, holds or supports trunk or limbs, but provides less
than half the effort.
02. Substantial/maximal assistance – Helper does MORE THAN HALF the effort. Helper lifts or holds trunk or limbs and provides more than
half the effort.
01. Dependent – Helper does ALL of the effort. Patient does none of the effort to complete the activity. Or, the assistance of 2 or more
helpers is required for the patient to complete the activity.
Code based on the patient’s need for assistance to perform the activity safely. Hey – sounds like OASIS M18xx item guidance!
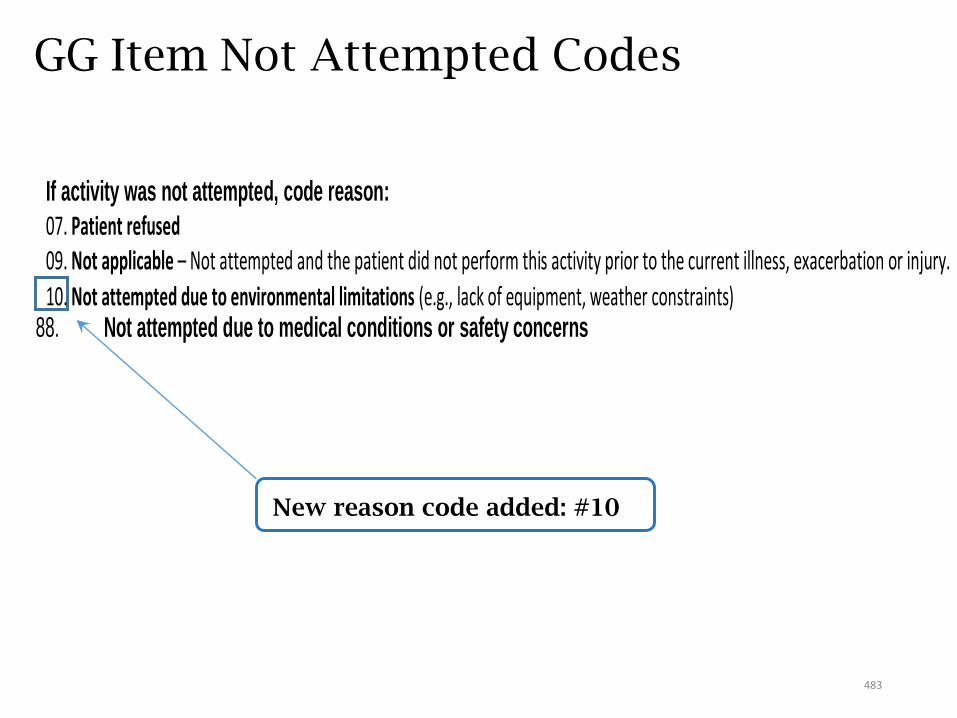
GG Item Not Attempted Codes
New reason code added: #10
If activity was not attempted, code reason:
07. Patient refused 09. Not applicable – Not attempted and the patient did not perform this activity prior to the current illness, exacerbation or injury.
10. Not attempted due to environmental limitations (e.g., lack of equipment, weather constraints) 88. Not attempted due to medical conditions or safety concerns
483
The “Danger of the Dash” – Lisa Selman-Holman, Jan 2019
• FB post: “Is it appropriate to score '88' (not attempted d/t medical conditions or safety concerns) as the discharge goal on the GG0170 question. Don't we want to 'hope' that the pt will be able to attempt by discharge? Of course if they have progressive disease process then patient may not be able to attempt. Thoughts?”
• I believe if you don’t anticipate the patient to be reasonably and safely able to perform the task, that is still the most appropriate response.
• Or, if no goal, is it a dash for DC goal?
• Reminder, what the dash means: (-) Dash = assessment was not done (no attempt to interview patient or cg regarding prior functioning). “Don’t know, don’t care”. Every attempt should be made to code the performance and discharge responses accurately! Use observation and interview!
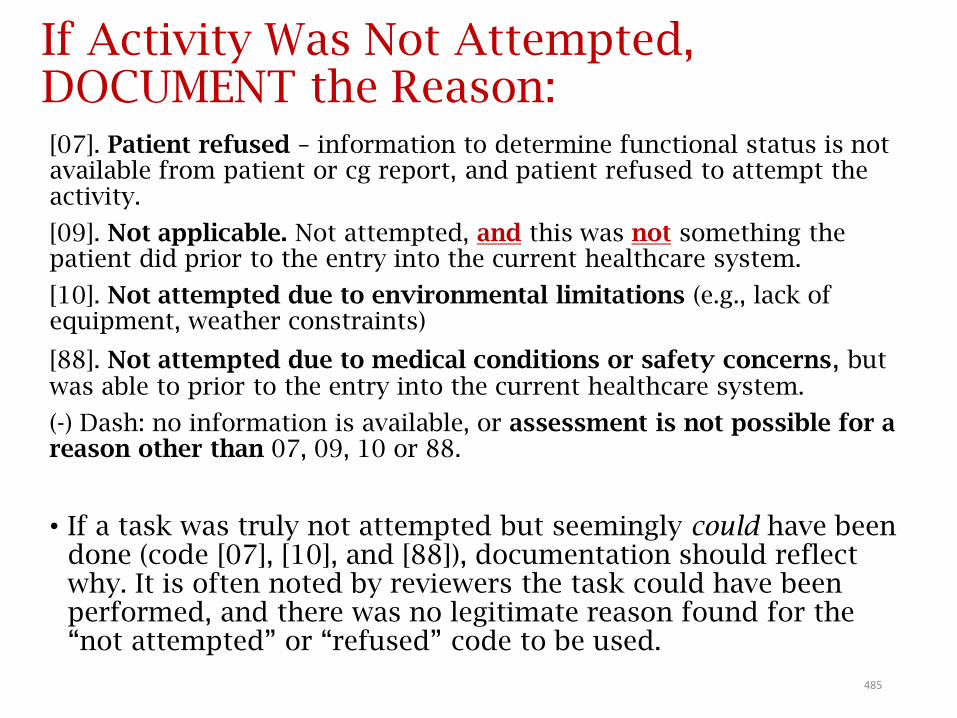
If Activity Was Not Attempted, DOCUMENT the Reason:[07]. Patient refused – information to determine functional status is not available from patient or cg report, and patient refused to attempt the activity.
[09]. Not applicable. Not attempted, and this was not something the patient did prior to the entry into the current healthcare system.
[10]. Not attempted due to environmental limitations (e.g., lack of equipment, weather constraints)
[88]. Not attempted due to medical conditions or safety concerns, but was able to prior to the entry into the current healthcare system.
(-) Dash: no information is available, or assessment is not possible for a reason other than 07, 09, 10 or 88.
• If a task was truly not attempted but seemingly could have been done (code [07], [10], and [88]), documentation should reflect why. It is often noted by reviewers the task could have been performed, and there was no legitimate reason found for the “not attempted” or “refused” code to be used.
485
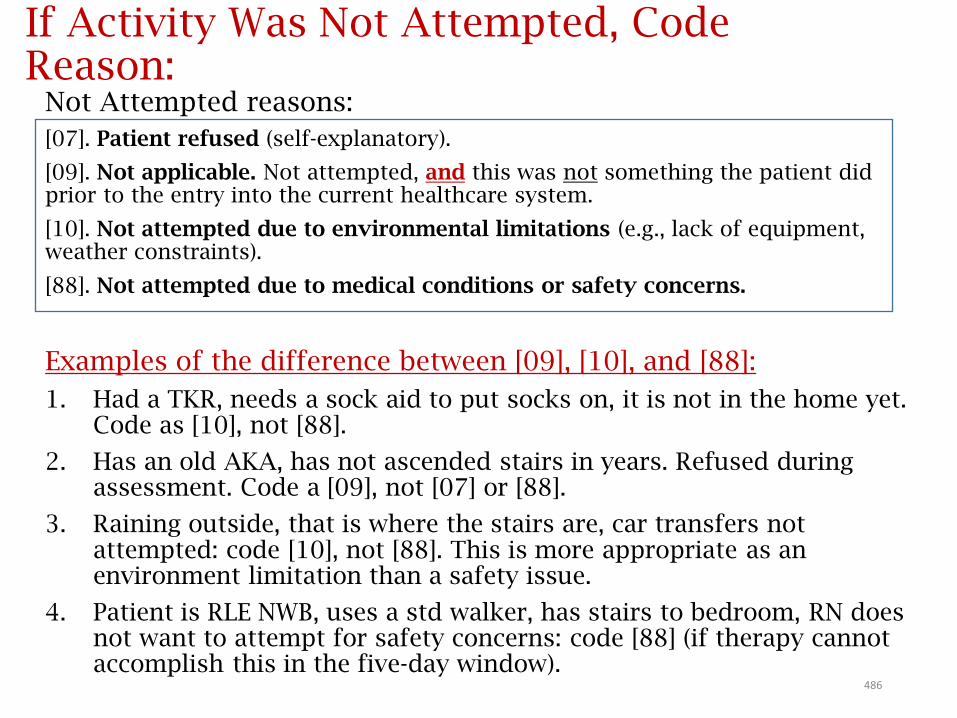
If Activity Was Not Attempted, Code Reason:
Not Attempted reasons:
[07]. Patient refused (self-explanatory).
[09]. Not applicable. Not attempted, and this was not something the patient did prior to the entry into the current healthcare system.
[10]. Not attempted due to environmental limitations (e.g., lack of equipment, weather constraints).
[88]. Not attempted due to medical conditions or safety concerns.
Examples of the difference between [09], [10], and [88]:
1. Had a TKR, needs a sock aid to put socks on, it is not in the home yet. Code as [10], not [88].
2. Has an old AKA, has not ascended stairs in years. Refused during assessment. Code a [09], not [07] or [88].
3. Raining outside, that is where the stairs are, car transfers not attempted: code [10], not [88]. This is more appropriate as an environment limitation than a safety issue.
4. Patient is RLE NWB, uses a std walker, has stairs to bedroom, RN does not want to attempt for safety concerns: code [88] (if therapy cannot accomplish this in the five-day window).
486
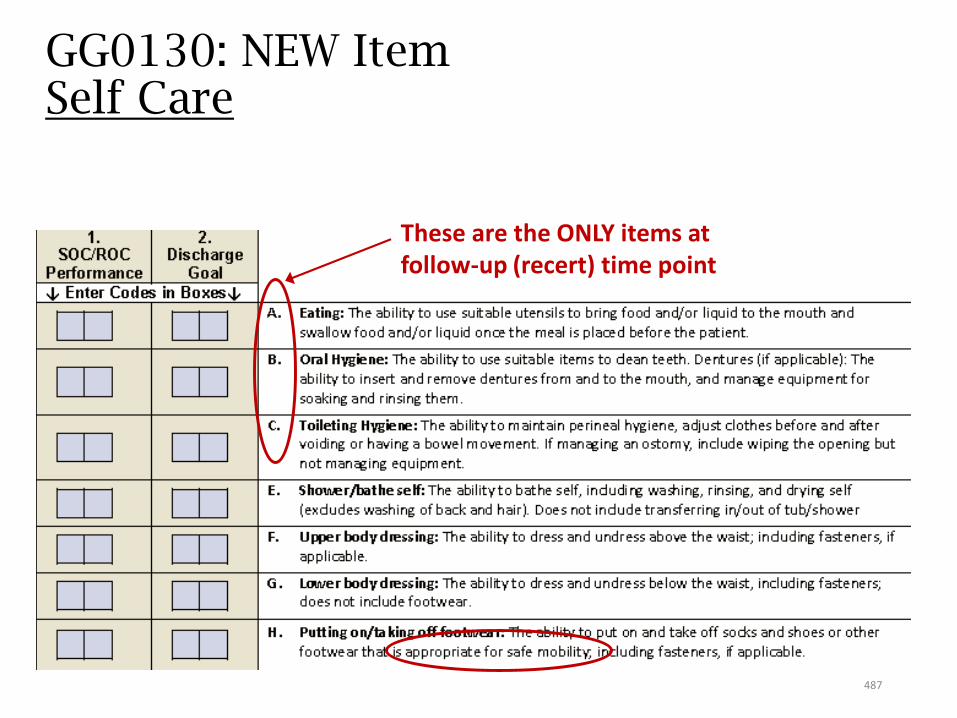
GG0130: NEW ItemSelf Care
These are the ONLY items at follow-up (recert) time point
487
GG0130 Response-Specific Instructions
• When possible, CMS invites a multidisciplinary approach to patient assessment (think one-clinician rule expansion).
• If the patient’s ability varies during the assessment time frame, record their usual ability to perform each activity; what is true greater than 50% of the assessment time frame.
• Licensed clinicians can establish a patient’s discharge goal(s) at the time of SOC/ROC based on the patient’s prior medical condition, SOC/ROC assessment, self-care and mobility status, discussions with the patient and family, professional judgment, the profession’s practice standards, expected treatments, patient motivation to improve, anticipated length of stay, and the discharge plan.
• Goals should be established as part of the patient’s care plan.
• Discharge performance: The discharge time period under consideration includes the last five days of care.
• This includes the date of the discharge visit plus the four preceding calendar days. Code the patient’s functional status based on a functional assessment that occurs at or close to discharge.
488
Selecting a Discharge Goal
• In general:• If the patient is expected to make progress, the Discharge
Goal would be higher than the SOC/ROC response.
• If the patient is not expected to make progress but would be expected to maintain the SOC/ROC functional level, the Discharge Goal would be the same as the SOC/ROC score.
• If the patient is expected to decline rapidly but skilled therapy services may slow decline of function, the Discharge Goal would be lower than the SOC/ROC score.
Discharge Goals per CMS
• Patient’s prior medical condition
• SOC/ROC assessment
• Self-care and mobility status
• Discussions with the patient and family
• Professional judgment
• Profession’s practice standards
• Expected treatments
• Patient motivation to improve
• Anticipated length of stay
• The discharge plan
Goals should be established as part of the patient’s care plan. Licensed clinicians can establish a patient’s discharge goal at the time of SOC/ROC based on:
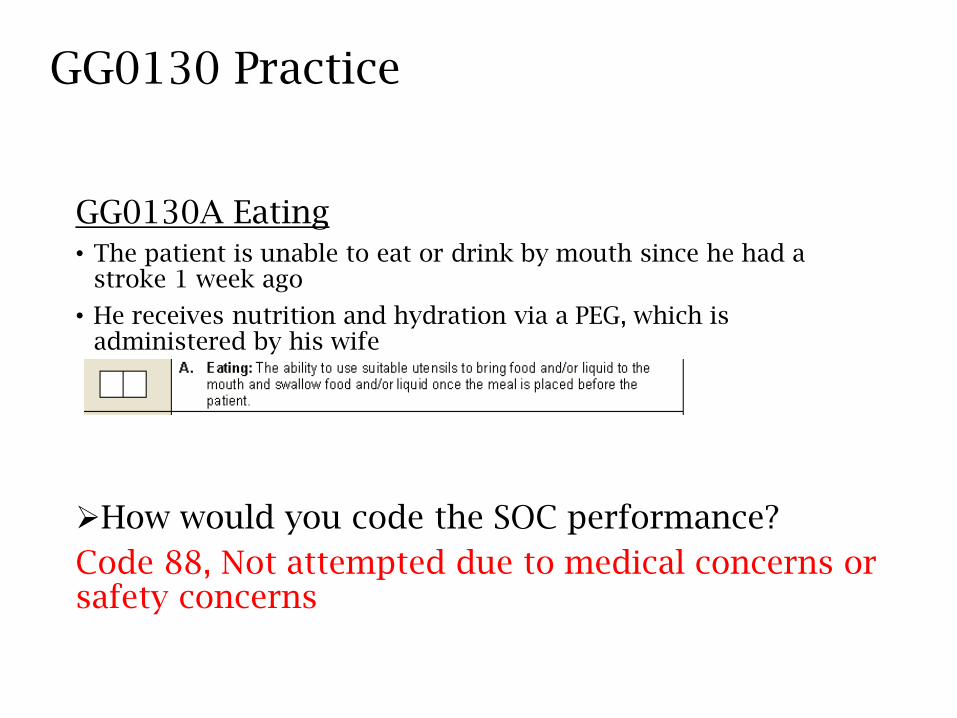
GG0130 Practice
GG0130A Eating• The patient is unable to eat or drink by mouth since he had a
stroke 1 week ago
• He receives nutrition and hydration via a PEG, which is administered by his wife
How would you code the SOC performance?
Code 88, Not attempted due to medical concerns or safety concerns
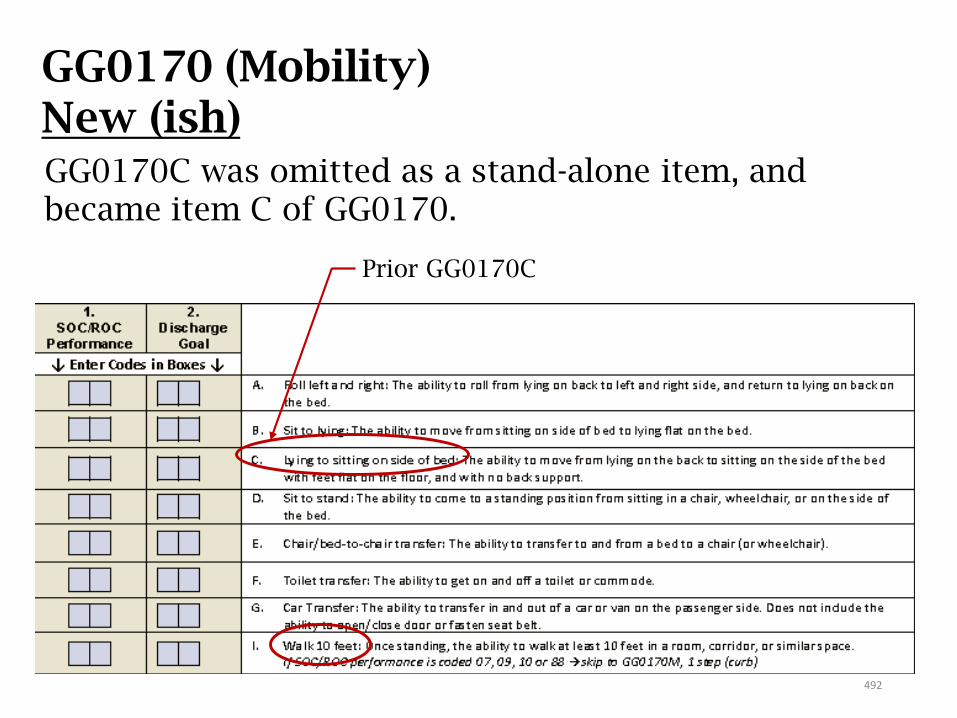
GG0170 (Mobility)New (ish)
Prior GG0170C
GG0170C was omitted as a stand-alone item, and became item C of GG0170.
492
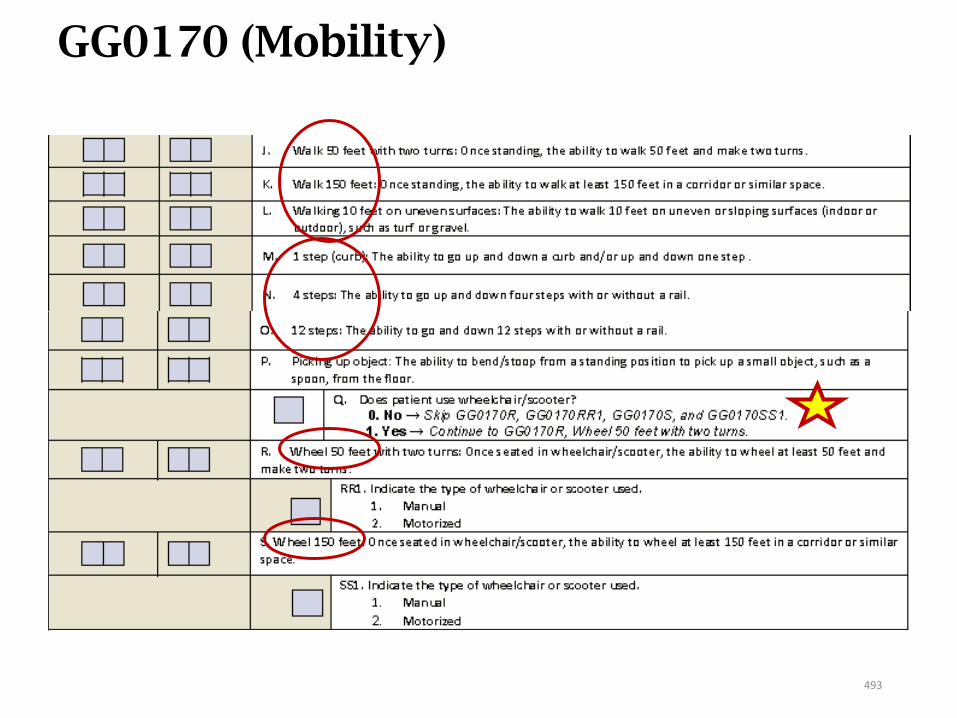
GG0170 (Mobility)
493
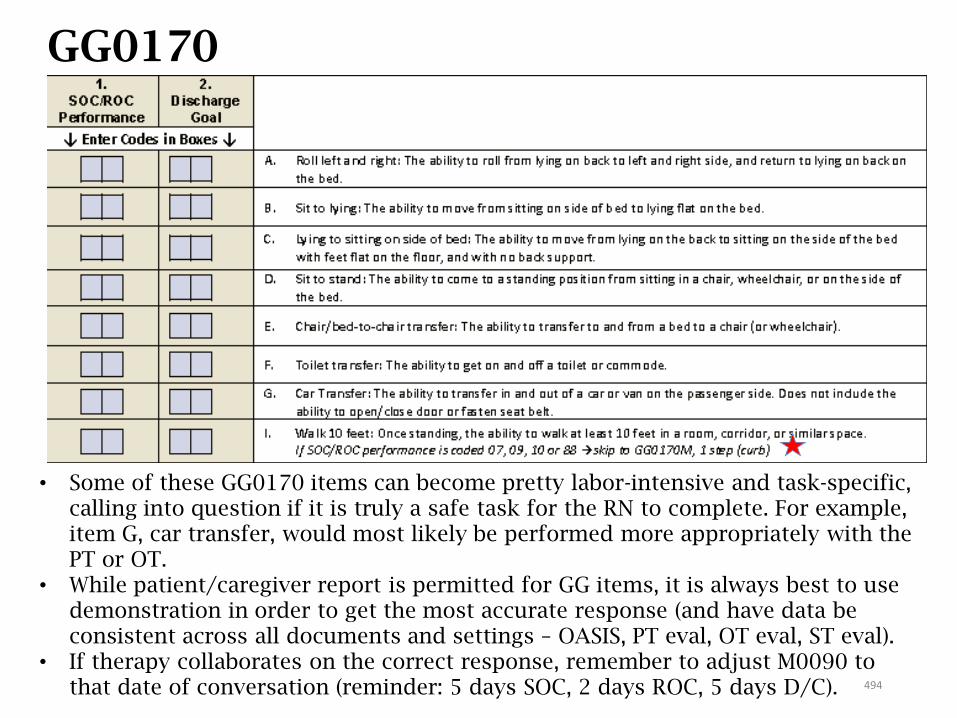
GG0170 (Mobility)
• Some of these GG0170 items can become pretty labor-intensive and task-specific, calling into question if it is truly a safe task for the RN to complete. For example, item G, car transfer, would most likely be performed more appropriately with the PT or OT.
• While patient/caregiver report is permitted for GG items, it is always best to use demonstration in order to get the most accurate response (and have data be consistent across all documents and settings – OASIS, PT eval, OT eval, ST eval).
• If therapy collaborates on the correct response, remember to adjust M0090 to that date of conversation (reminder: 5 days SOC, 2 days ROC, 5 days D/C). 494
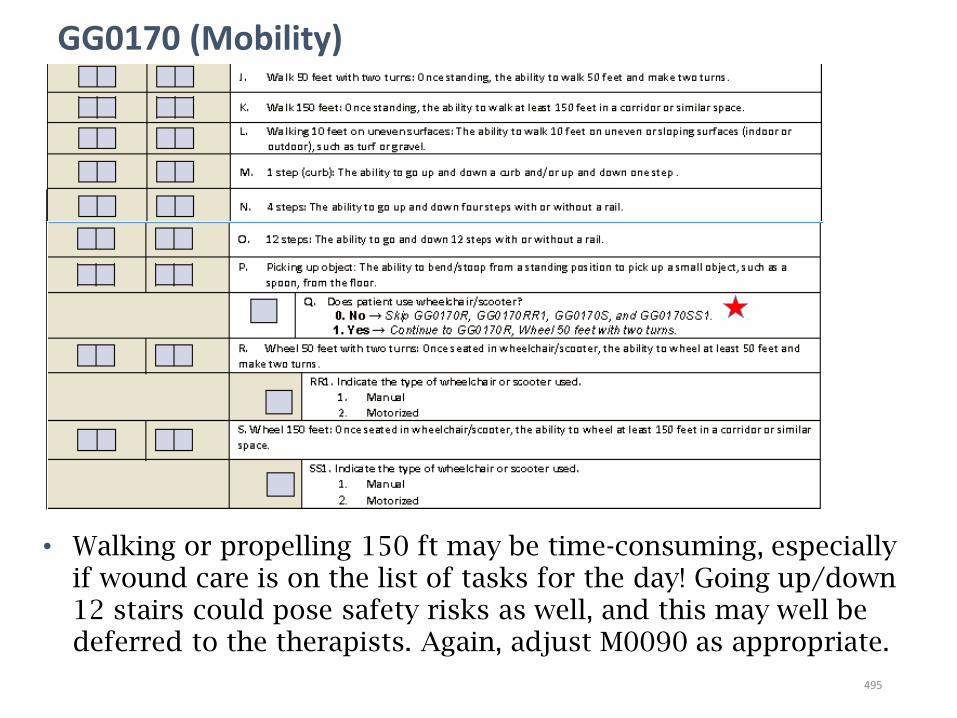
GG0170 (Mobility)
• Walking or propelling 150 ft may be time-consuming, especially if wound care is on the list of tasks for the day! Going up/down 12 stairs could pose safety risks as well, and this may well be deferred to the therapists. Again, adjust M0090 as appropriate.
495
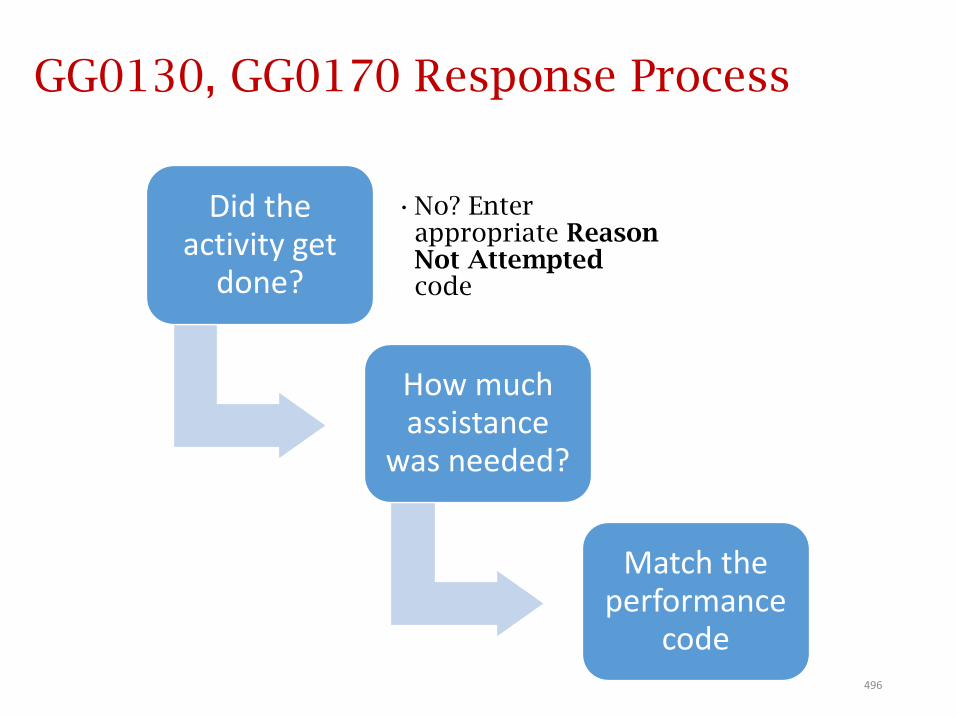
GG0130, GG0170 Response Process
Did the activity get
done?
•No? Enter appropriate Reason Not Attempted code
How much assistance
was needed?
Match the performance
code496
GG0170(O): Stairs question• GG0100C: Example from Guidance Manual for item-specific guidance: “When to
Code “Not Applicable:” Mr. S ambulates with a walker around his home, and uses a stair lift to negotiate the stairs to the second floor, where his bedroom is located.
• Coding: GG0100C, Stairs, would be coded 09, Not Applicable. Rationale: Mr. S is not able to go up and down stairs; he uses a stair lift. So, he did not perform this activity.”
• For GG0170(O): Completing the stair activities indicates that a patient goes up and down the stairs, by any safe means, with or without portable assistive devices and/or with or without some level of assistance.
• 06 – Independent would be coded if the stair activity of a patient going up and down steps (1, 4, or 12) is completed by any safe means (e.g., walking on their feet, scooting on their bottom), with or without a portable assistive device, and with no set-up assistance or assistance during the stair activity.
• The use of non-portable assistive devices (such as a stair chair with a track attached to the wall) would not be considered “completing the stair activity.” A patient that is not able to go up and down the stairs, with or without assistance, without the use of a non-portable stair lift would be coded with the appropriate “activity was not attempted” code.
The CMS Home Health Quality Help Desk Team
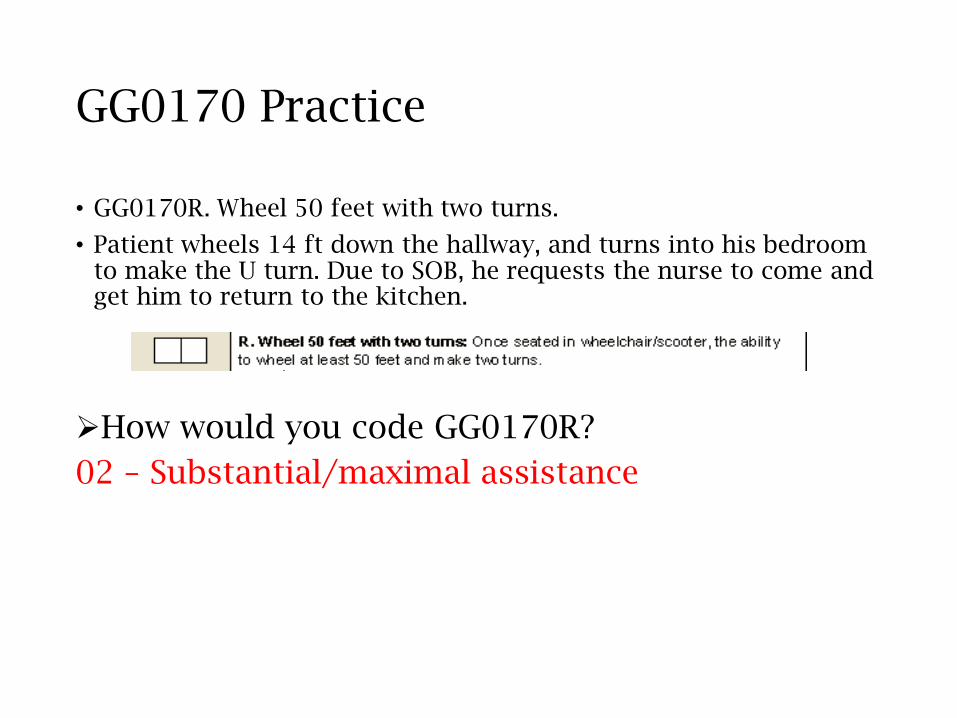
GG0170 Practice
• GG0170R. Wheel 50 feet with two turns.
• Patient wheels 14 ft down the hallway, and turns into his bedroom to make the U turn. Due to SOB, he requests the nurse to come and get him to return to the kitchen.
How would you code GG0170R?
02 – Substantial/maximal assistance
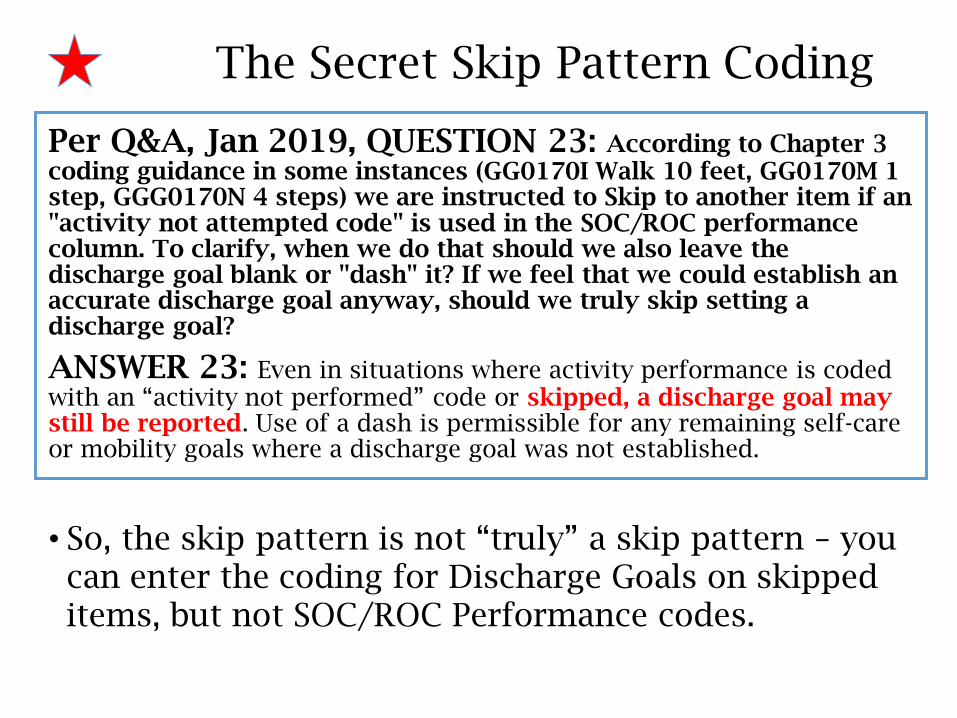
The Secret Skip Pattern Coding
Per Q&A, Jan 2019, QUESTION 23: According to Chapter 3 coding guidance in some instances (GG0170I Walk 10 feet, GG0170M 1 step, GGG0170N 4 steps) we are instructed to Skip to another item if an "activity not attempted code" is used in the SOC/ROC performance column. To clarify, when we do that should we also leave the discharge goal blank or "dash" it? If we feel that we could establish an accurate discharge goal anyway, should we truly skip setting a discharge goal?
ANSWER 23: Even in situations where activity performance is coded with an “activity not performed” code or skipped, a discharge goal may still be reported. Use of a dash is permissible for any remaining self-care or mobility goals where a discharge goal was not established.
• So, the skip pattern is not “truly” a skip pattern – you can enter the coding for Discharge Goals on skipped items, but not SOC/ROC Performance codes.
GG0170
Keys to success:1. Don’t try to equate the responses of the similar
M18xx Functional items to coding these items (see M18-GG Crosswalk Tool).
2. For multi-discipline cases, recommended to follow the agency policy for handling the OASIS items to be in compliance with the one-clinician rule. It may prove to have greater accuracy, safety, and efficiency to have many of the items within GG0130, GG0170 parceled out amongst the disciplines assessing in the five-day window.
3. Know what 10 ft (TUG test?), 50 ft, and 150 ft “look like.”
500
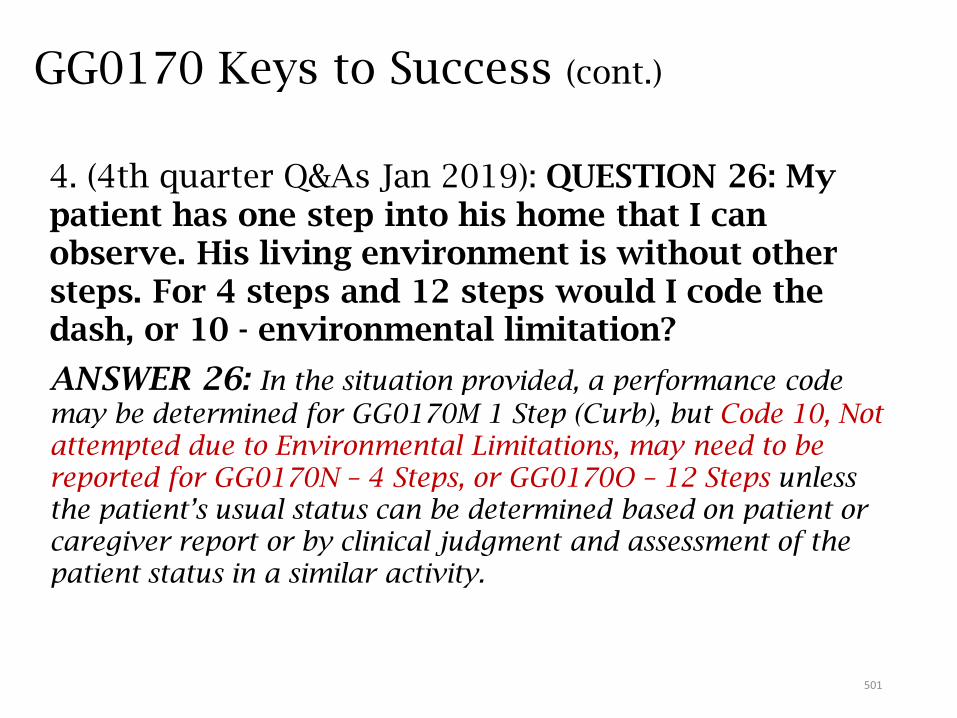
GG0170 Keys to Success (cont.)
4. (4th quarter Q&As Jan 2019): QUESTION 26: My patient has one step into his home that I can observe. His living environment is without other steps. For 4 steps and 12 steps would I code the dash, or 10 - environmental limitation?
ANSWER 26: In the situation provided, a performance code
may be determined for GG0170M 1 Step (Curb), but Code 10, Not attempted due to Environmental Limitations, may need to be reported for GG0170N – 4 Steps, or GG0170O – 12 Steps unless the patient’s usual status can be determined based on patient or caregiver report or by clinical judgment and assessment of the patient status in a similar activity.
501
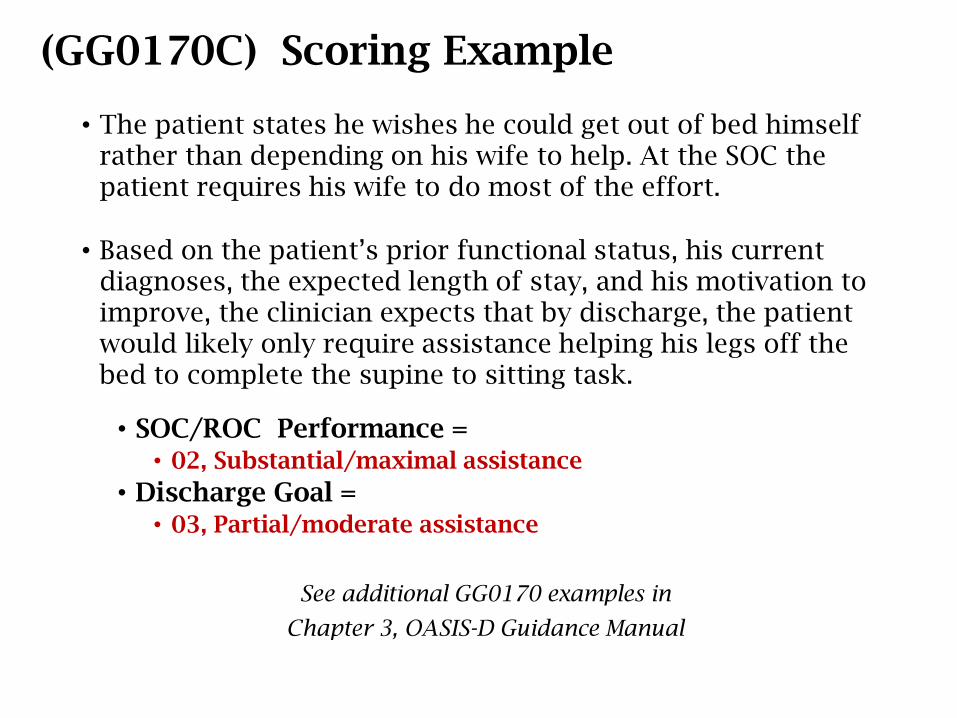
(GG0170C) Scoring Example
• The patient states he wishes he could get out of bed himself rather than depending on his wife to help. At the SOC the patient requires his wife to do most of the effort.
• Based on the patient’s prior functional status, his current diagnoses, the expected length of stay, and his motivation to improve, the clinician expects that by discharge, the patient would likely only require assistance helping his legs off the bed to complete the supine to sitting task.
• SOC/ROC Performance = • 02, Substantial/maximal assistance
• Discharge Goal = • 03, Partial/moderate assistance
See additional GG0170 examples in
Chapter 3, OASIS-D Guidance Manual
GG0170C: “What if?” Scenarios
The assessing clinician must exercise clinical judgment in reporting the help a patient needs to complete the lying to sitting transfer.
What if . . .
• Patient’s preferred (or necessary) sleeping surface is a recliner or a mattress on the floor?
• Patient’s feet do not reach the floor when sitting on side of bed?
GG0170C: “What if?” Scenarios
What if . . .
• Patient’s preferred (or necessary) sleeping surface is a recliner or a mattress on the floor?
• Assess the patient’s need for assistance using that sleeping surface
• Patient’s feet do not reach the floor when sitting on side of bed?
• If patient performs activity independently – score 06 (Independent)
• For safety, if patient needs help to lower bed or place stool under feet prior to transfer – score 05 (Setup or clean-up assistance
(CMS Q&A #151.21, 10/16)
GG0170C: “What if?” Scenarios(Source: CMS Home Health Provider Training Q&As, November 2016)
• Patient’s preferred sleeping surface is an electric powered recliner?
• Patient was bed bound prior to SOC/ROC?
• Patient’s bed bound status is new or temporary?
• Patient is bedbound (88) at SOC/ROC?
GG0170C: “What if?” Scenarios(Source: CMS Home Health Provider Training Q&As, November 2016)
• Patient’s preferred sleeping surface is an electric powered recliner?
• If the patient pushes a button to reach a sitting position, select 06 (Independent).
• Patient was bed bound prior to SOC/ROC?• Performance level at SOC/ROC = 09 (Not applicable)• If not expected to improve, a dash ( - ) is appropriate to report
Discharge Goal.
• Patient’s bed bound status is new or temporary?• Performance level at SOC/ROC = 88 (Not attempted due to
medical condition)
• Patient is bedbound (88) at SOC/ROC?• Use 01-06 as Discharge Goal if patient is expected to improve.
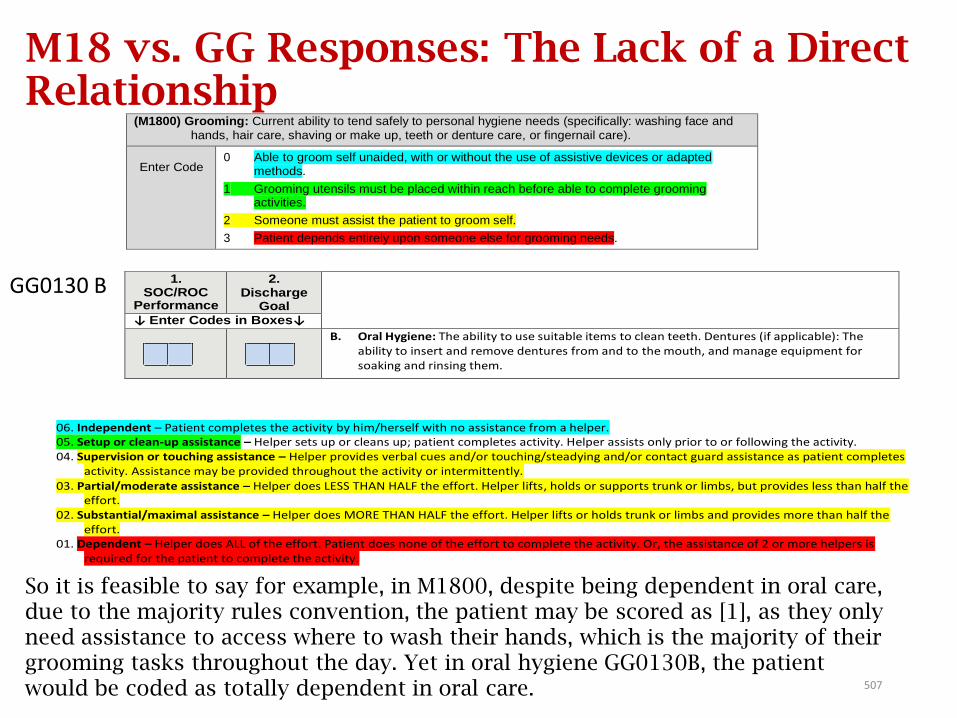
(M1800) Grooming: Current ability to tend safely to personal hygiene needs (specifically: washing face and
hands, hair care, shaving or make up, teeth or denture care, or fingernail care).
Enter Code 0 Able to groom self unaided, with or without the use of assistive devices or adapted
methods.
1 Grooming utensils must be placed within reach before able to complete grooming activities.
2 Someone must assist the patient to groom self.
3 Patient depends entirely upon someone else for grooming needs.
1. SOC/ROC
Performance
2. Discharge
Goal
↓ Enter Codes in Boxes↓
B. Oral Hygiene: The ability to use suitable items to clean teeth. Dentures (if applicable): The ability to insert and remove dentures from and to the mouth, and manage equipment for soaking and rinsing them.
06. Independent – Patient completes the activity by him/herself with no assistance from a helper. 05. Setup or clean-up assistance – Helper sets up or cleans up; patient completes activity. Helper assists only prior to or following the activity. 04. Supervision or touching assistance – Helper provides verbal cues and/or touching/steadying and/or contact guard assistance as patient completes
activity. Assistance may be provided throughout the activity or intermittently. 03. Partial/moderate assistance – Helper does LESS THAN HALF the effort. Helper lifts, holds or supports trunk or limbs, but provides less than half the
effort. 02. Substantial/maximal assistance – Helper does MORE THAN HALF the effort. Helper lifts or holds trunk or limbs and provides more than half the
effort. 01. Dependent – Helper does ALL of the effort. Patient does none of the effort to complete the activity. Or, the assistance of 2 or more helpers is
required for the patient to complete the activity.
M18 vs. GG Responses: The Lack of a Direct Relationship(M1800) Grooming: Current ability to tend safely to personal hygiene needs (specifically: washing face and
hands, hair care, shaving or make up, teeth or denture care, or fingernail care).
Enter Code 0 Able to groom self unaided, with or without the use of assistive devices or adapted
methods.
1 Grooming utensils must be placed within reach before able to complete grooming activities.
2 Someone must assist the patient to groom self.
3 Patient depends entirely upon someone else for grooming needs.
1. SOC/ROC
Performance
2. Discharge
Goal
↓ Enter Codes in Boxes↓
B. Oral Hygiene: The ability to use suitable items to clean teeth. Dentures (if applicable): The ability to insert and remove dentures from and to the mouth, and manage equipment for soaking and rinsing them.
06. Independent – Patient completes the activity by him/herself with no assistance from a helper. 05. Setup or clean-up assistance – Helper sets up or cleans up; patient completes activity. Helper assists only prior to or following the activity. 04. Supervision or touching assistance – Helper provides verbal cues and/or touching/steadying and/or contact guard assistance as patient completes
activity. Assistance may be provided throughout the activity or intermittently. 03. Partial/moderate assistance – Helper does LESS THAN HALF the effort. Helper lifts, holds or supports trunk or limbs, but provides less than half the
effort. 02. Substantial/maximal assistance – Helper does MORE THAN HALF the effort. Helper lifts or holds trunk or limbs and provides more than half the
effort. 01. Dependent – Helper does ALL of the effort. Patient does none of the effort to complete the activity. Or, the assistance of 2 or more helpers is
required for the patient to complete the activity.
GG0130 B
So it is feasible to say for example, in M1800, despite being dependent in oral care, due to the majority rules convention, the patient may be scored as [1], as they only need assistance to access where to wash their hands, which is the majority of their grooming tasks throughout the day. Yet in oral hygiene GG0130B, the patient would be coded as totally dependent in oral care. 507
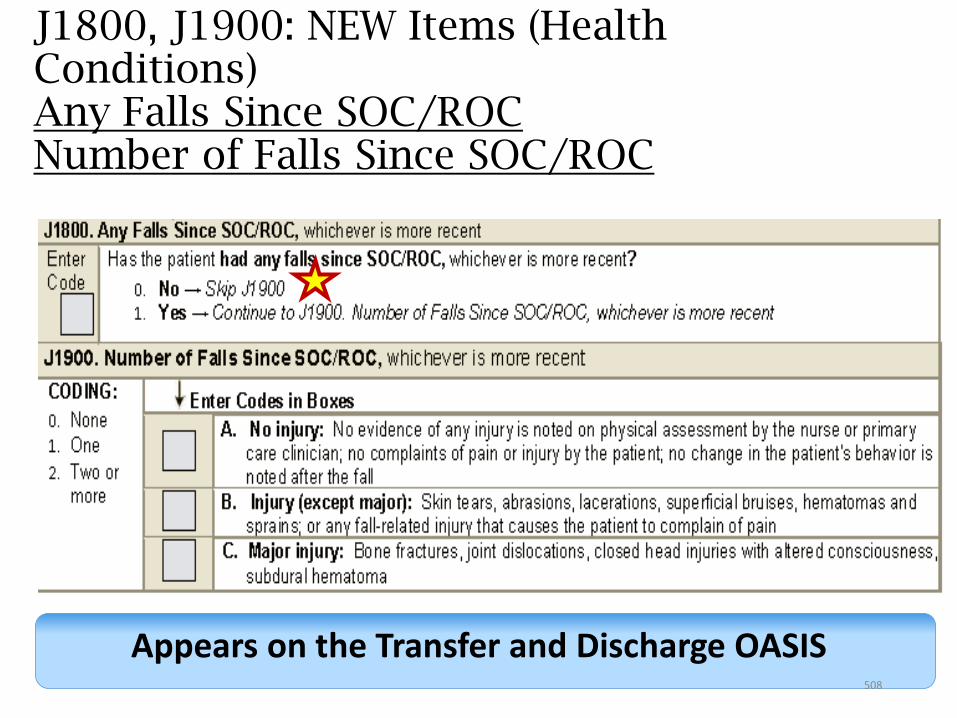
J1800, J1900: NEW Items (Health Conditions)Any Falls Since SOC/ROCNumber of Falls Since SOC/ROC
Appears on the Transfer and Discharge OASIS508
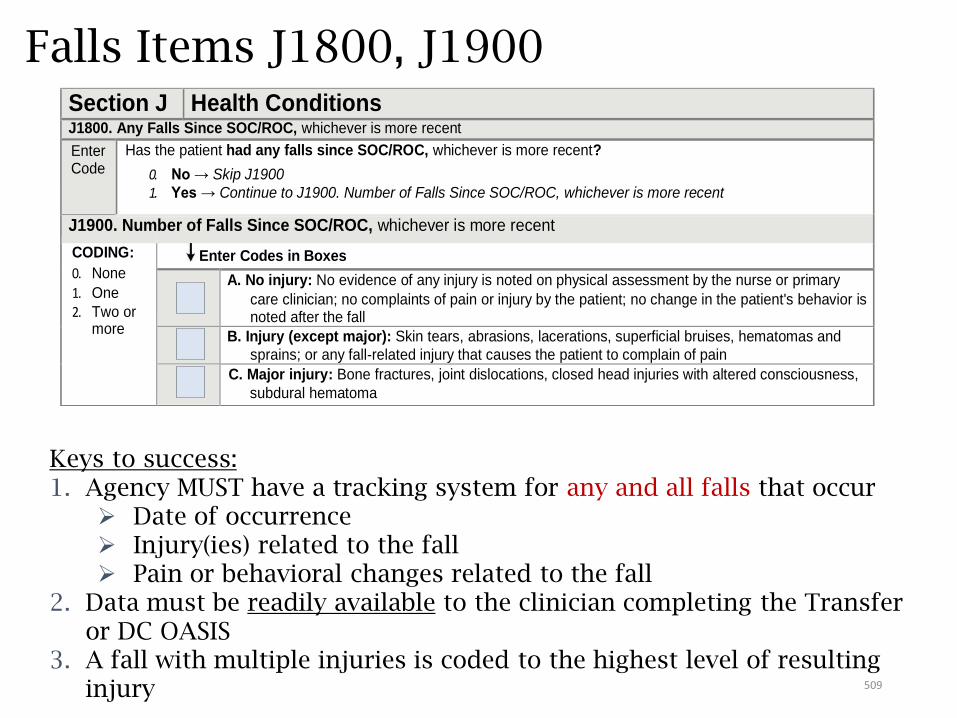
Falls Items J1800, J1900
Keys to success:1. Agency MUST have a tracking system for any and all falls that occur
Date of occurrence Injury(ies) related to the fall Pain or behavioral changes related to the fall
2. Data must be readily available to the clinician completing the Transfer or DC OASIS
3. A fall with multiple injuries is coded to the highest level of resulting injury
Section J Health Conditions J1800. Any Falls Since SOC/ROC, whichever is more recent
Enter Code
Has the patient had any falls since SOC/ROC, whichever is more recent?
0. No → Skip J1900
1. Yes → Continue to J1900. Number of Falls Since SOC/ROC, whichever is more recent
J1900. Number of Falls Since SOC/ROC, whichever is more recent
CODING:
0. None
1. One
2. Two or more
Enter Codes in Boxes
A. No injury: No evidence of any injury is noted on physical assessment by the nurse or primary
care clinician; no complaints of pain or injury by the patient; no change in the patient's behavior is noted after the fall
B. Injury (except major): Skin tears, abrasions, lacerations, superficial bruises, hematomas and
sprains; or any fall-related injury that causes the patient to complain of pain
C. Major injury: Bone fractures, joint dislocations, closed head injuries with altered consciousness,
subdural hematoma
509
Falls Guidance
The Guidance Manual has offered some insight into the consideration of falls.
Falls:
• An intercepted fall occurs when the patient would have fallen if he or she had not caught him/herself or had not been intercepted by another person—this is still considered a fall.
Not Falls:
• Falls are not a result of an overwhelming external force (such as a person pushing a patient).
• CMS understands that challenging a patient’s balance and training him/her to recover from a loss of balance is an intentional therapeutic intervention and does not consider anticipated losses of balance that occur during supervised therapeutic interventions as intercepted falls.
510
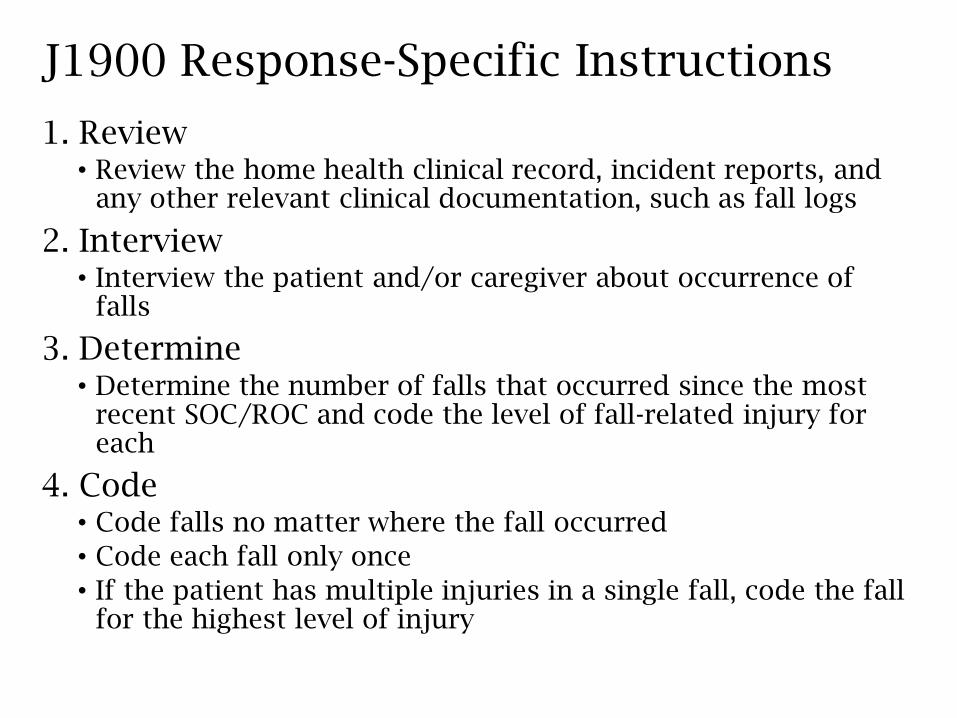
J1900 Response-Specific Instructions
1. Review• Review the home health clinical record, incident reports, and
any other relevant clinical documentation, such as fall logs
2. Interview• Interview the patient and/or caregiver about occurrence of
falls
3. Determine• Determine the number of falls that occurred since the most
recent SOC/ROC and code the level of fall-related injury for each
4. Code• Code falls no matter where the fall occurred
• Code each fall only once
• If the patient has multiple injuries in a single fall, code the fall for the highest level of injury
Other M items only at Transfer, Discharge
M1041 – M1056
512
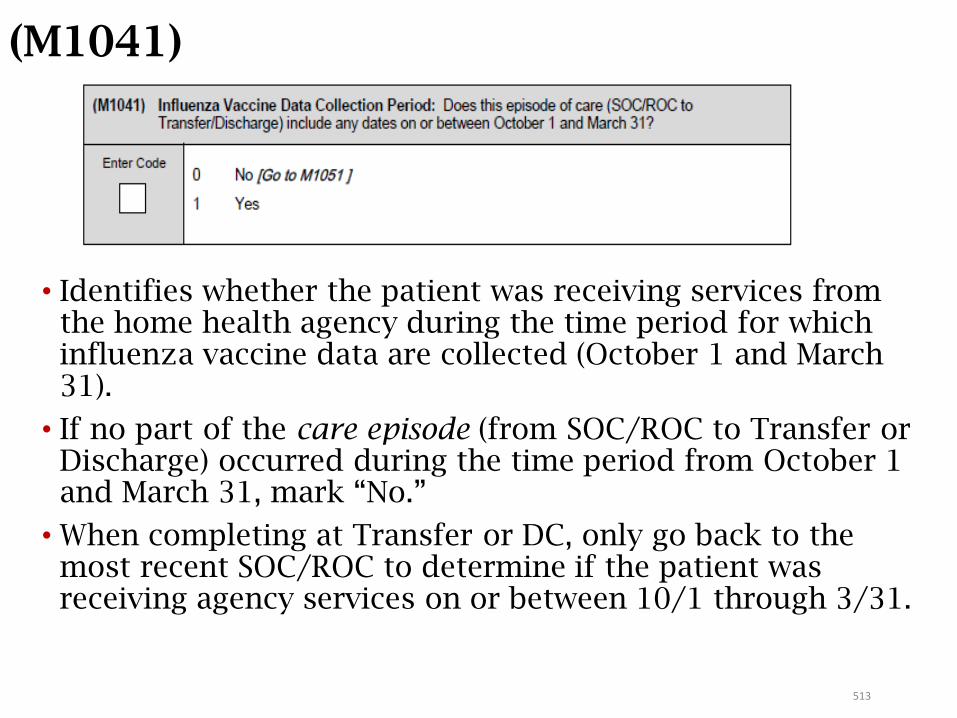
513
(M1041)
• Identifies whether the patient was receiving services from the home health agency during the time period for which influenza vaccine data are collected (October 1 and March 31).
• If no part of the care episode (from SOC/ROC to Transfer or Discharge) occurred during the time period from October 1 and March 31, mark “No.”
• When completing at Transfer or DC, only go back to the most recent SOC/ROC to determine if the patient was receiving agency services on or between 10/1 through 3/31.
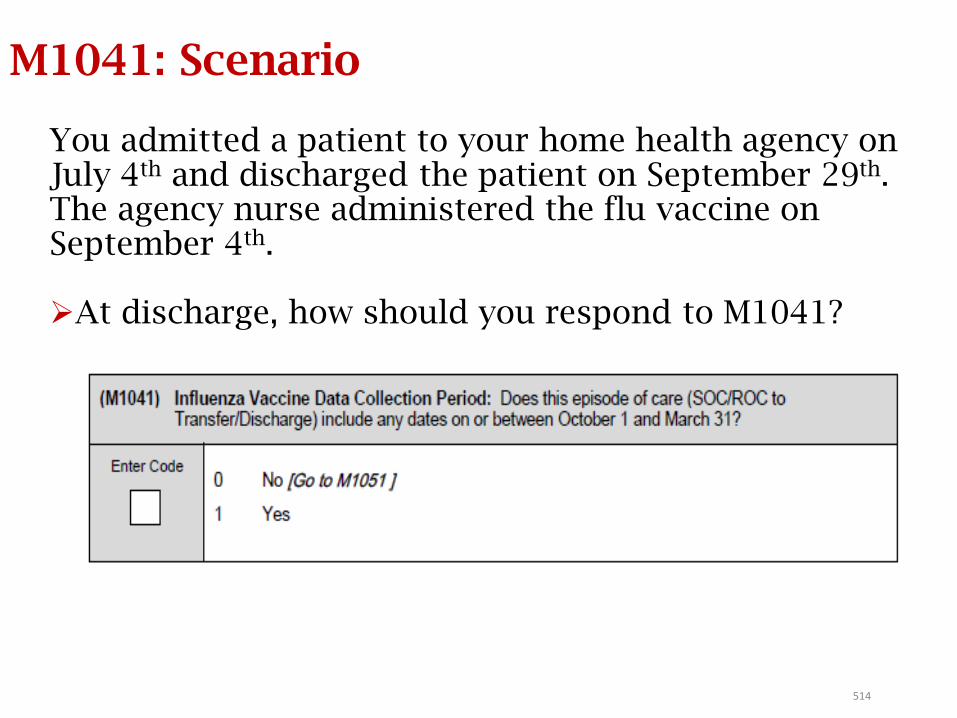
514
M1041: Scenario
You admitted a patient to your home health agency on July 4th and discharged the patient on September 29th. The agency nurse administered the flu vaccine on September 4th.
At discharge, how should you respond to M1041?
Answer: M1041
You admitted a patient to your home health agency on July 4th and discharged the patient on September 29th. The agency nurse administered the flu vaccine on September 4th.
• At discharge, how should you respond to M1041?
Response 0 (No)• The entire episode of care is outside the data collection
period (10/1 - 3/31).
• M1046 is skipped.
What if patient was discharged on October 1st?
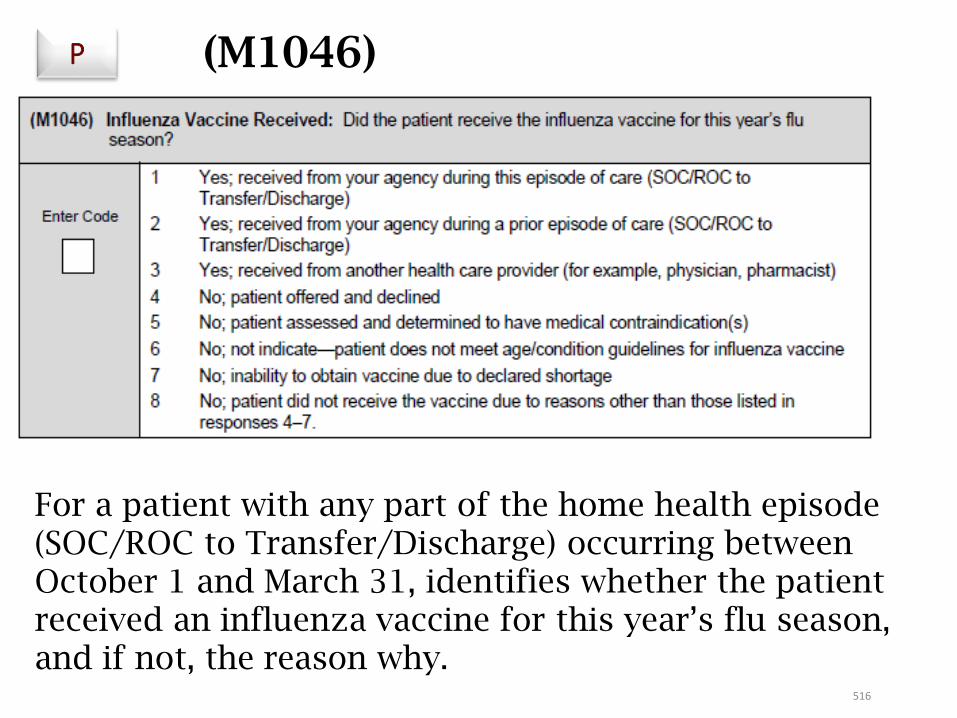
516
(M1046)
For a patient with any part of the home health episode (SOC/ROC to Transfer/Discharge) occurring between October 1 and March 31, identifies whether the patient received an influenza vaccine for this year’s flu season, and if not, the reason why.
P
517
M1046: Responses
• Response 1: your agency provided the influenza vaccine to the patient during this episode of care (SOC/ROC to Transfer/Discharge).
• Response 2: your agency provided the flu vaccine for this year’s flu season prior to this home health episode, (for example, if the SOC/ROC for this episode was in winter, but your agency provided the vaccine for the current flu season during a previous home health episode in the fall when the vaccine for the current flu season became available).
• You may enter Response 2 if a current patient was given a flu vaccine by your agency during a previous roster billing situation during this year’s flu season.
Roster billing is a simplified billing process that allows mass immunizers to submit one claim form with a list of several immunized beneficiaries.
518
M1046: Responses
• Response 3: the patient or caregiver reports (or there is documentation in the clinical record) that the patient received the influenza vaccine for the current flu season from another provider – e.g., the patient’s physician, a clinic, or health fair providing
influenza vaccines, etc.
• Response 1, 2, or 3 may be entered even if the flu vaccine for this year’s influenza season was provided prior to October 1 (that is, flu vaccine was made available early).
• Response 4: the patient was offered the vaccine and the patient or healthcare proxy (for example, someone with power of attorney) refused the vaccine.
Note: It is not required that the agency offer the vaccine. Enter Response 4 only if the patient was offered the vaccine and he/she refused.
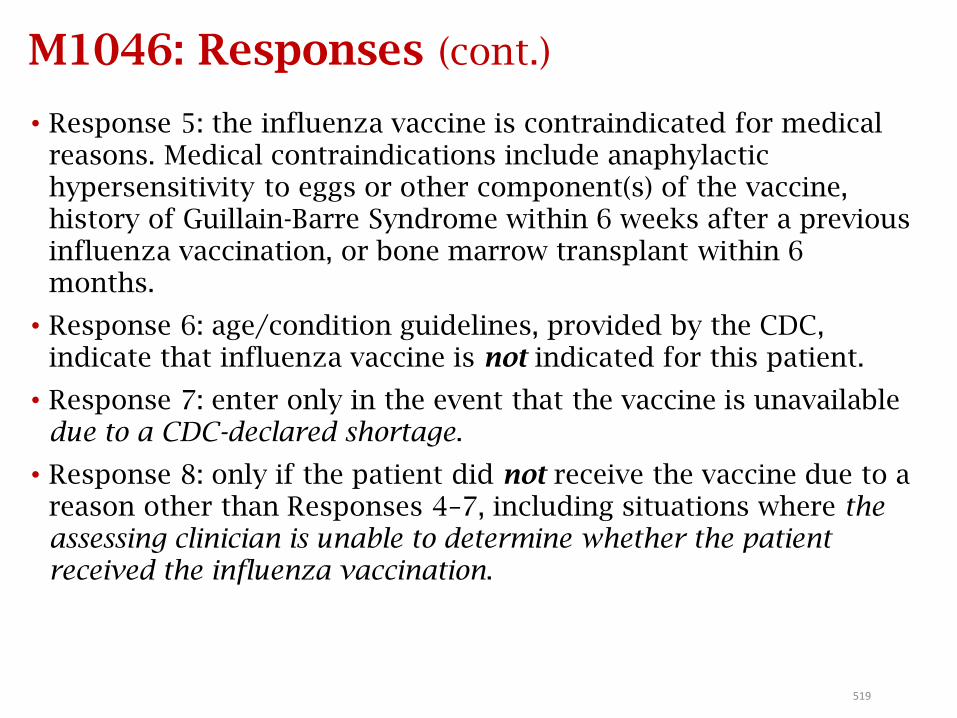
519
M1046: Responses (cont.)
• Response 5: the influenza vaccine is contraindicated for medical reasons. Medical contraindications include anaphylactic hypersensitivity to eggs or other component(s) of the vaccine, history of Guillain-Barre Syndrome within 6 weeks after a previous influenza vaccination, or bone marrow transplant within 6 months.
• Response 6: age/condition guidelines, provided by the CDC, indicate that influenza vaccine is not indicated for this patient.
• Response 7: enter only in the event that the vaccine is unavailable due to a CDC-declared shortage.
• Response 8: only if the patient did not receive the vaccine due to a reason other than Responses 4–7, including situations where the assessing clinician is unable to determine whether the patient received the influenza vaccination.
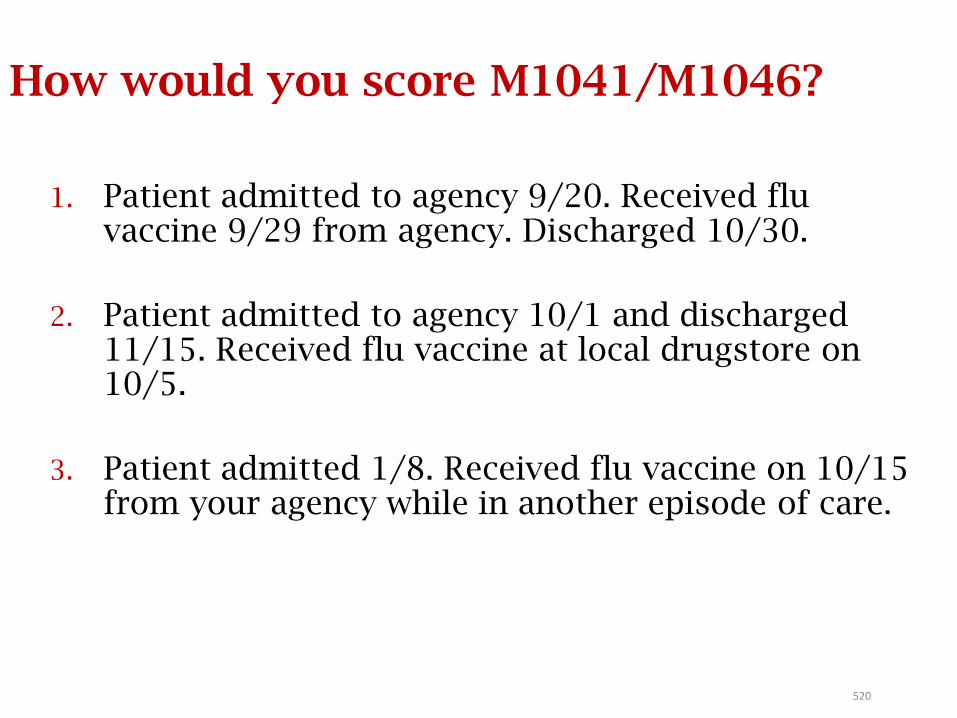
520
How would you score M1041/M1046?
1. Patient admitted to agency 9/20. Received flu vaccine 9/29 from agency. Discharged 10/30.
2. Patient admitted to agency 10/1 and discharged 11/15. Received flu vaccine at local drugstore on 10/5.
3. Patient admitted 1/8. Received flu vaccine on 10/15 from your agency while in another episode of care.
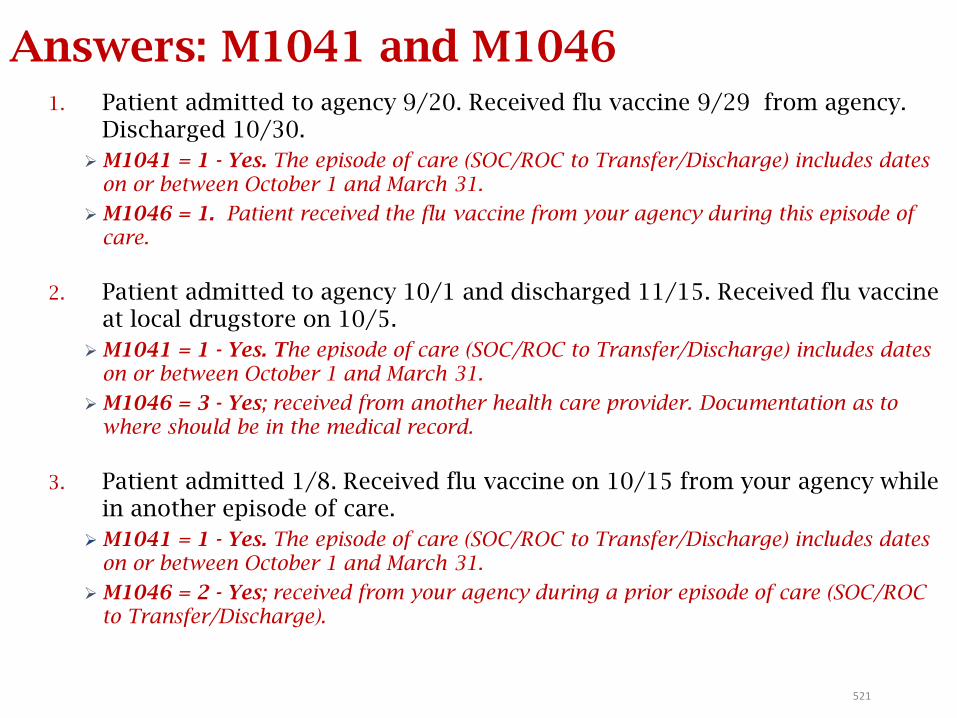
521
Answers: M1041 and M10461. Patient admitted to agency 9/20. Received flu vaccine 9/29 from agency.
Discharged 10/30.
M1041 = 1 - Yes. The episode of care (SOC/ROC to Transfer/Discharge) includes dates on or between October 1 and March 31.
M1046 = 1. Patient received the flu vaccine from your agency during this episode of care.
2. Patient admitted to agency 10/1 and discharged 11/15. Received flu vaccine at local drugstore on 10/5.
M1041 = 1 - Yes. The episode of care (SOC/ROC to Transfer/Discharge) includes dates on or between October 1 and March 31.
M1046 = 3 - Yes; received from another health care provider. Documentation as to where should be in the medical record.
3. Patient admitted 1/8. Received flu vaccine on 10/15 from your agency while in another episode of care.
M1041 = 1 - Yes. The episode of care (SOC/ROC to Transfer/Discharge) includes dates on or between October 1 and March 31.
M1046 = 2 - Yes; received from your agency during a prior episode of care (SOC/ROC to Transfer/Discharge).
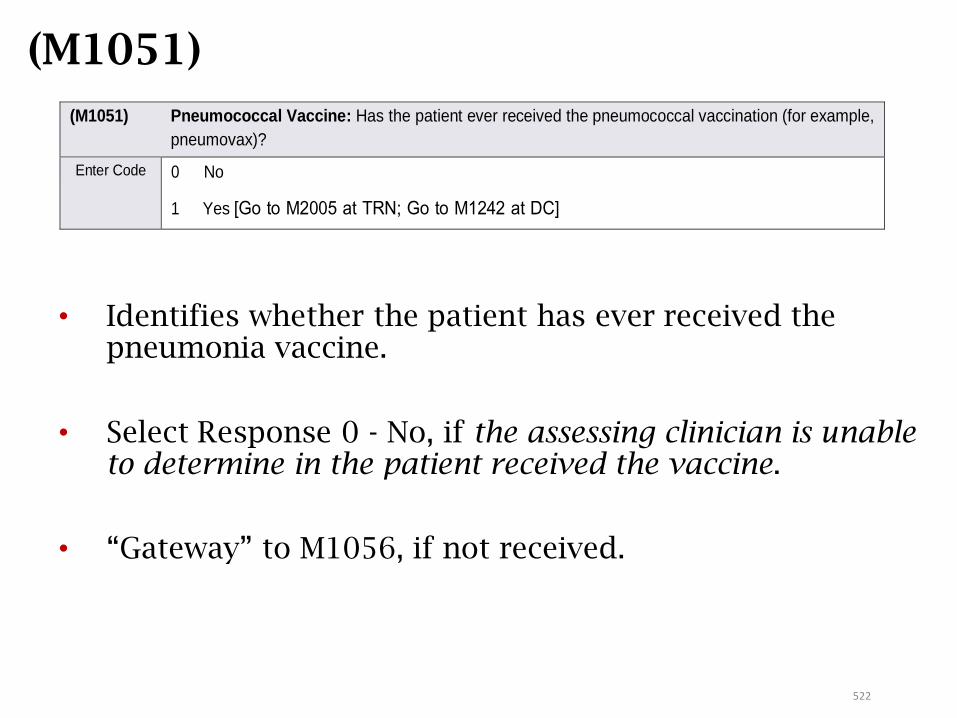
522
(M1051)
• Identifies whether the patient has ever received the pneumonia vaccine.
• Select Response 0 - No, if the assessing clinician is unable to determine in the patient received the vaccine.
• “Gateway” to M1056, if not received.
(M1051) Pneumococcal Vaccine: Has the patient ever received the pneumococcal vaccination (for example,
pneumovax)?
Enter Code 0 No
1 Yes [Go to M2005 at TRN; Go to M1242 at DC]
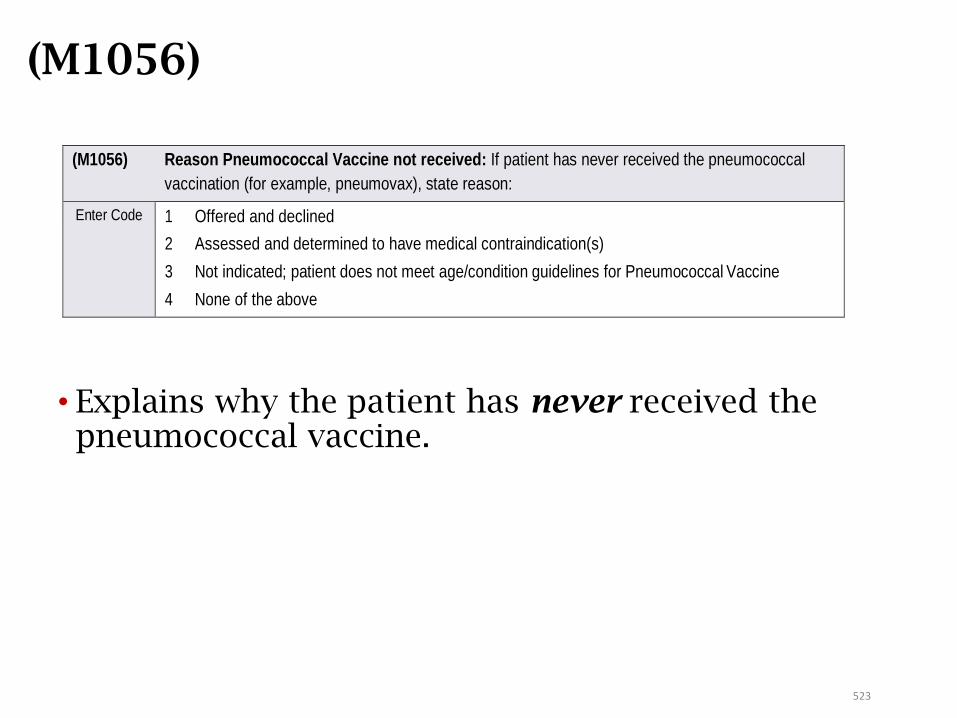
523
(M1056)
• Explains why the patient has never received the pneumococcal vaccine.
(M1056) Reason Pneumococcal Vaccine not received: If patient has never received the pneumococcal
vaccination (for example, pneumovax), state reason:
Enter Code 1 Offered and declined
2 Assessed and determined to have medical contraindication(s)
3 Not indicated; patient does not meet age/condition guidelines for Pneumococcal Vaccine
4 None of the above
524
M1056: Responses• Response 1: the patient and/or healthcare proxy (for example,
someone with power of attorney) refused the vaccine.
• Response 2: pneumococcal vaccine administration is medically contraindicated for this patient.
• Contraindications include anaphylactic hypersensitivity to component(s) of the vaccine, acute febrile illness, bone marrow transplant within past 12 months, or receiving course of chemotherapy or radiation therapy within past 2 weeks.
• Response 3: CDC age/condition guidelines indicate that pneumococcal vaccination is not indicated for this patient.
• Response 4: the agency did not provide the vaccine due to a reason other than Responses 1-3 including situations where the assessing clinician is unable to determine whether the patient has ever received the pneumococcal vaccine.
Guidelines for influenza and pneumococcal vaccine recommendations and contraindications are found on the CDC website.
525
How would you score M1051 and M1056?
Mr. B was transferred to the hospital. His record shows he has never had the PPV vaccine. It was not given by the home health agency due to his bone marrow transplant 3 months ago.
What would be the correct response for M1051 & M1056?
526
Answers: M1051 and M1056
Mr. B was transferred to the hospital. His record shows he has never had the PPV vaccine. It was not given by the home health agency due to his bone marrow transplant 3 months ago.
What would be the correct response for M1051 & M1056?
M1051 = 0 - No. Patient has never received the PPV vaccine.
M1056 = 2 - Assessed and determined to have medical contraindication(s). PPV is medically contraindicated in patients who have had a bone marrow transplant within the past 12 months.
Emergent CareM2301 – M2310
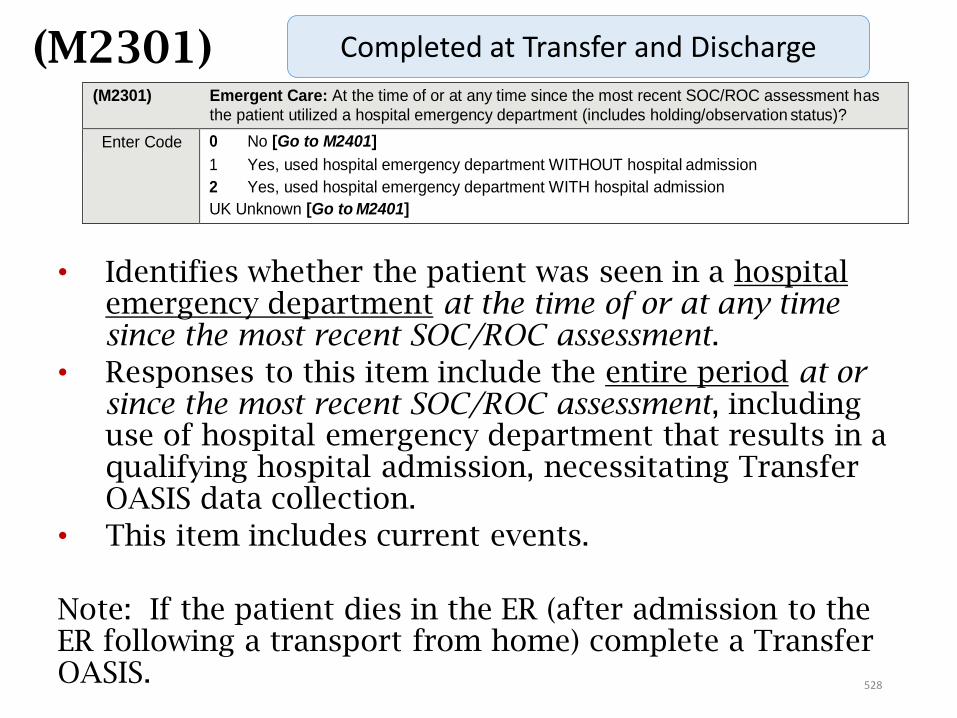
(M2301)
• Identifies whether the patient was seen in a hospital emergency department at the time of or at any time since the most recent SOC/ROC assessment.
• Responses to this item include the entire period at or since the most recent SOC/ROC assessment, including use of hospital emergency department that results in a qualifying hospital admission, necessitating Transfer OASIS data collection.
• This item includes current events.
Note: If the patient dies in the ER (after admission to the ER following a transport from home) complete a Transfer OASIS.
(M2301) Emergent Care: At the time of or at any time since the most recent SOC/ROC assessment has
the patient utilized a hospital emergency department (includes holding/observation status)?
Enter Code 0 No [Go to M2401]
1 Yes, used hospital emergency department WITHOUT hospital admission
2 Yes, used hospital emergency department WITH hospital admission
UK Unknown [Go to M2401]
Completed at Transfer and Discharge
528
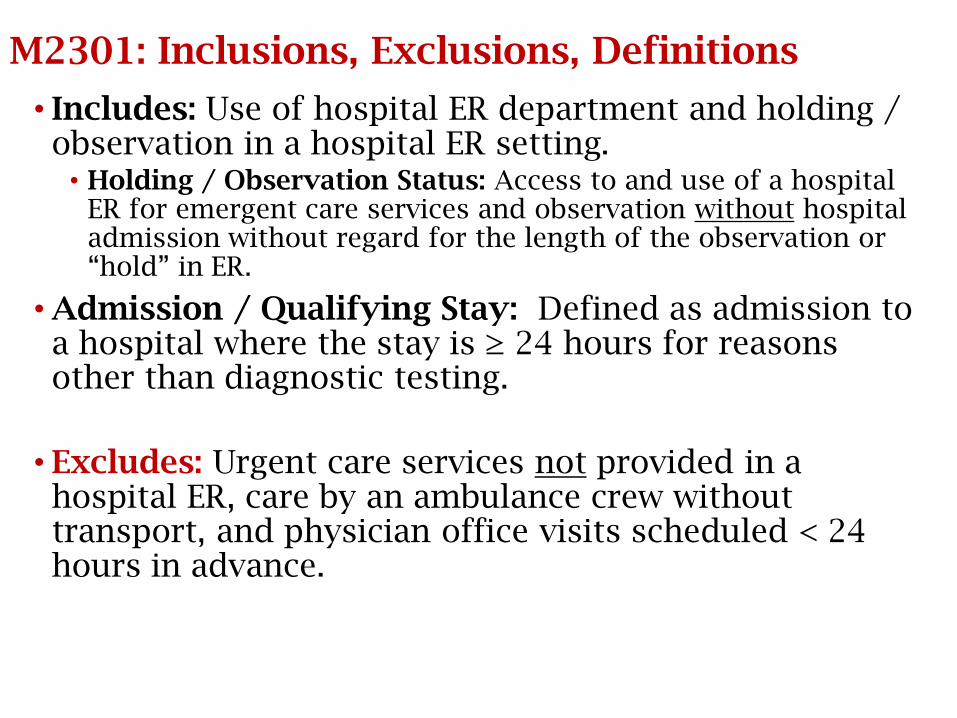
M2301: Inclusions, Exclusions, Definitions
• Includes: Use of hospital ER department and holding / observation in a hospital ER setting.
• Holding / Observation Status: Access to and use of a hospital ER for emergent care services and observation without hospital admission without regard for the length of the observation or “hold” in ER.
• Admission / Qualifying Stay: Defined as admission to a hospital where the stay is ≥ 24 hours for reasons other than diagnostic testing.
• Excludes: Urgent care services not provided in a hospital ER, care by an ambulance crew without transport, and physician office visits scheduled < 24 hours in advance.
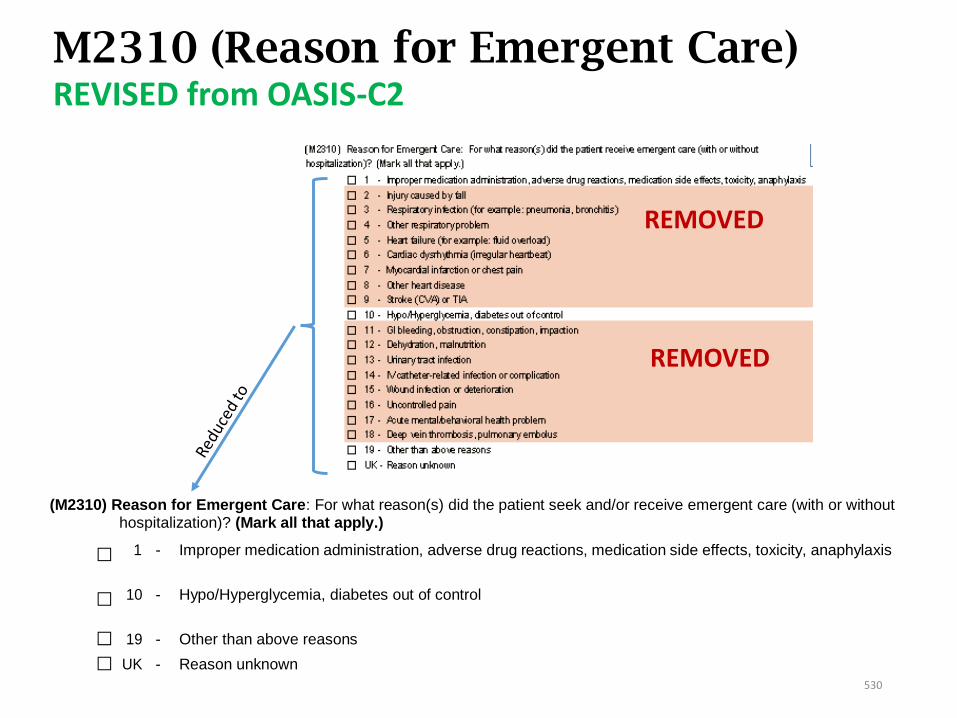
M2310 (Reason for Emergent Care)REVISED from OASIS-C2
REMOVED
REMOVED
(M2310) Reason for Emergent Care: For what reason(s) did the patient seek and/or receive emergent care (with or without hospitalization)? (Mark all that apply.)
⃞ 1 - Improper medication administration, adverse drug reactions, medication side effects, toxicity, anaphylaxis
⃞
10
- Hypo/Hyperglycemia, diabetes out of control
⃞
19
- Other than above reasons
⃞ UK - Reason unknown
530
(M2310)
• With the bulk of the conditions for rehospitalization removed, this presents a challenge for agencies to have the ability to track the reasons for returning to the hospital
• It is strongly recommended to have an internal process for continuing to track all rehospitalization reasons, as this information should be used for best practices, aiding agencies in determining where additional training and resources may be needed to prevent the reoccurrence
• The four response options needed for calculation of potentially avoidable event (PAE) measures were retained. In light of this, as 2 of the choices are “Other than the Above” and “Reason Unknown”, it is crucial for agencies to have documentation that clearly supports those 2 responses – what is the Other, or why is the reason Unknown?
531
532532
M2310: Guidance
• This item ONLY addresses services provided in a hospital emergency department – not urgent care, MD office, emergency crew without transport.
• If a patient seeks care in a hospital emergency department for a specific suspected condition, report that condition, even if the suspected condition was ruled out (e.g., patient was sent to the emergency department for suspected overdose, but was ruled out).
• If the patient has received emergent care in a hospital emergency department multiple times since the last time OASIS data were collected, include the reasons for all visits.
Transfer and DischargeM2410 – M2420
M0906
(M2410)
• Identifies the type of inpatient facility to which the patient was admitted.
• If the patient was admitted to more than one facility, indicate the facility type to which the patient was admitted first (for example, the facility type that they were transferred to from their home).
• When a patient dies in a hospital emergency department, the RFA 7 – Transfer to an Inpatient Facility OASIS is completed.
• In this unique situation, clinicians are directed to enter Response 1 – Hospital for M2410, even though the patient was not admitted to the inpatient facility.
534
(M2410) To which Inpatient Facility has the patient been admitted?
Enter Code 1 Hospital
2 Rehabilitation facility
3 Nursing home
4 Hospice
NA No inpatient facility admission [Omit “NA” option on TRN]
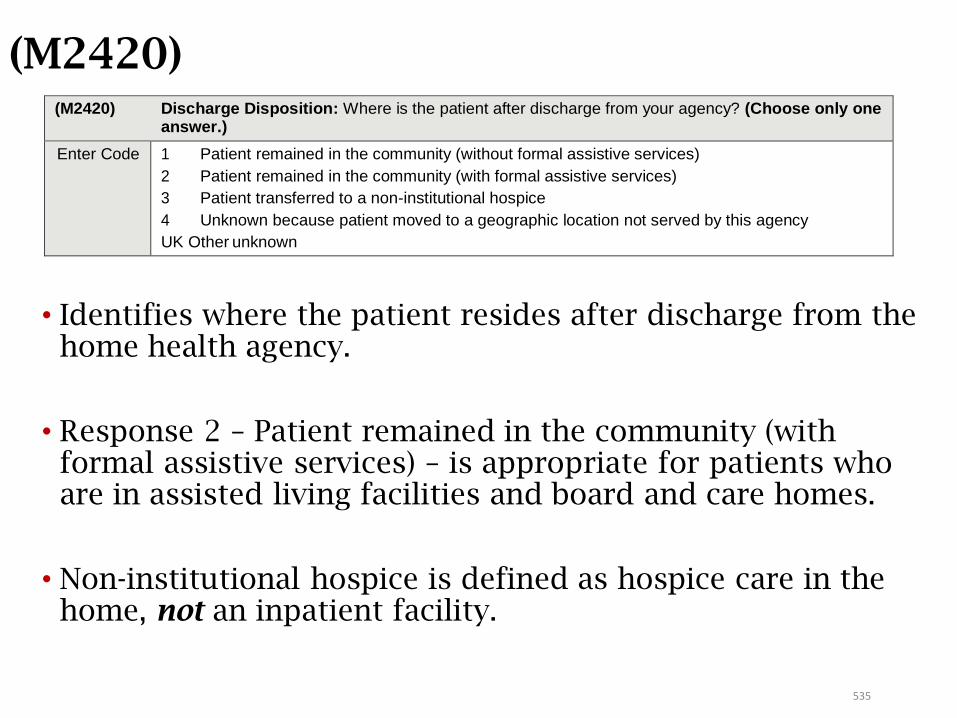
535
(M2420)
• Identifies where the patient resides after discharge from the home health agency.
• Response 2 – Patient remained in the community (with formal assistive services) – is appropriate for patients who are in assisted living facilities and board and care homes.
• Non-institutional hospice is defined as hospice care in the home, not an inpatient facility.
(M2420) Discharge Disposition: Where is the patient after discharge from your agency? (Choose only one answer.)
Enter Code 1 Patient remained in the community (without formal assistive services)
2 Patient remained in the community (with formal assistive services)
3 Patient transferred to a non-institutional hospice
4 Unknown because patient moved to a geographic location not served by this agency
UK Other unknown
M2420: Discharge Disposition
• Formal assistive services: community-based services provided through organizations or by paid helpers, such as:
• Homemaking services under Medicaid waiver programs, personal care services provided by a home health agency, paid assistance provided by an individual, home-delivered meals provided by organizations like Meals-on-Wheels.
• Therapy services provided in an outpatient setting are NOT considered formal assistance.
• Informal services: those provided by friends, family, neighbors, or other individuals in the community for which no financial compensation is provided. For example:
• Assistance with ADLs provided by a family member, transportation provided by a friend, meals provided by church members (specifically, meals not provided by the church organization itself, but by individual volunteers).
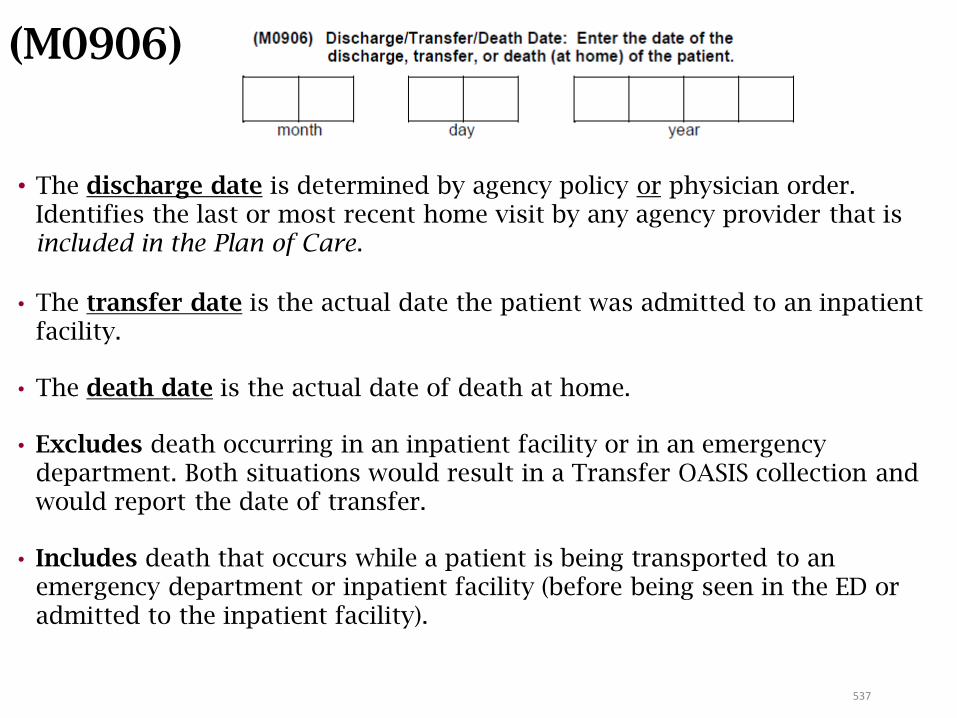
537
(M0906)
• The discharge date is determined by agency policy or physician order. Identifies the last or most recent home visit by any agency provider that is included in the Plan of Care.
• The transfer date is the actual date the patient was admitted to an inpatient facility.
• The death date is the actual date of death at home.
• Excludes death occurring in an inpatient facility or in an emergency department. Both situations would result in a Transfer OASIS collection and would report the date of transfer.
• Includes death that occurs while a patient is being transported to an emergency department or inpatient facility (before being seen in the ED or admitted to the inpatient facility).
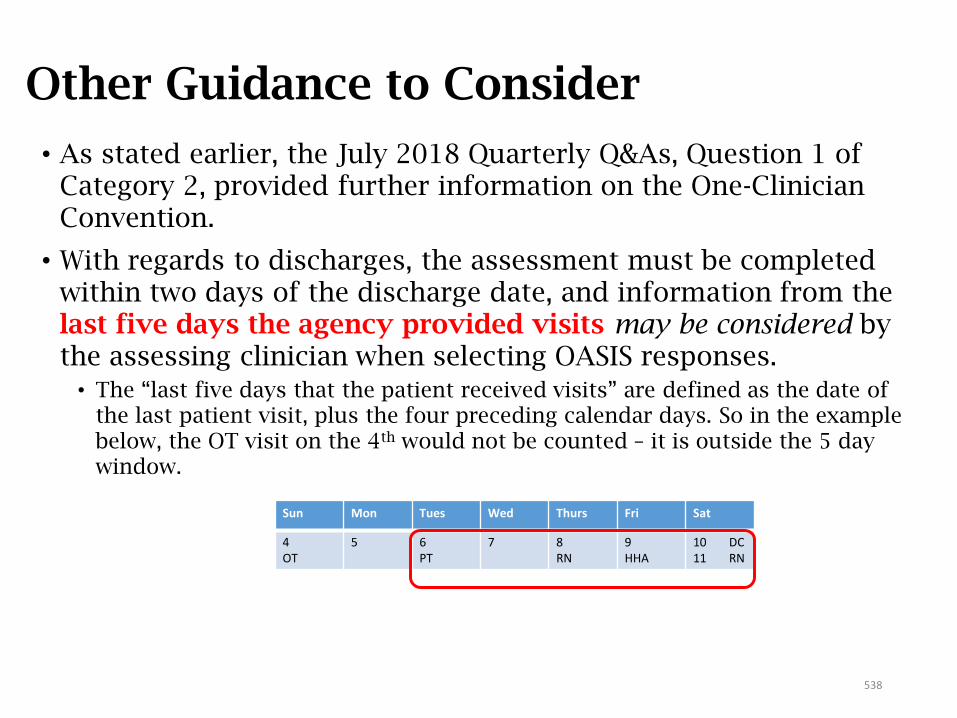
Other Guidance to Consider
• As stated earlier, the July 2018 Quarterly Q&As, Question 1 of Category 2, provided further information on the One-Clinician Convention.
• With regards to discharges, the assessment must be completed within two days of the discharge date, and information from the last five days the agency provided visits may be considered by the assessing clinician when selecting OASIS responses.
• The “last five days that the patient received visits” are defined as the date of the last patient visit, plus the four preceding calendar days. So in the example below, the OT visit on the 4th would not be counted – it is outside the 5 day window.
Sun Mon Tues Wed Thurs Fri Sat
4OT
5 6PT
7 8RN
9HHA
10 DC11 RN
538

Topics for Review
Dash values
Which answer is correct?
1. A dash may be used when responding to any OASIS item.
2. A dash may be used only on a SOC OASIS if the clinician runs out of time to complete the assessment.
3. CMS expects that using a dash will be a frequent response.
4. A dash is appropriate in M1060 Weight when a patient is too painful to stand to be weighed.
540
Dash values
Which answer is correct?
1. A dash may be used when responding to any OASIS item.
2. A dash may be used only on a SOC OASIS if the clinician runs out of time to complete the assessment.
3. CMS expects that using a dash will be a frequent response.
4. A dash is appropriate in M1060 Weight when a patient is too painful to stand to be weighed.
541
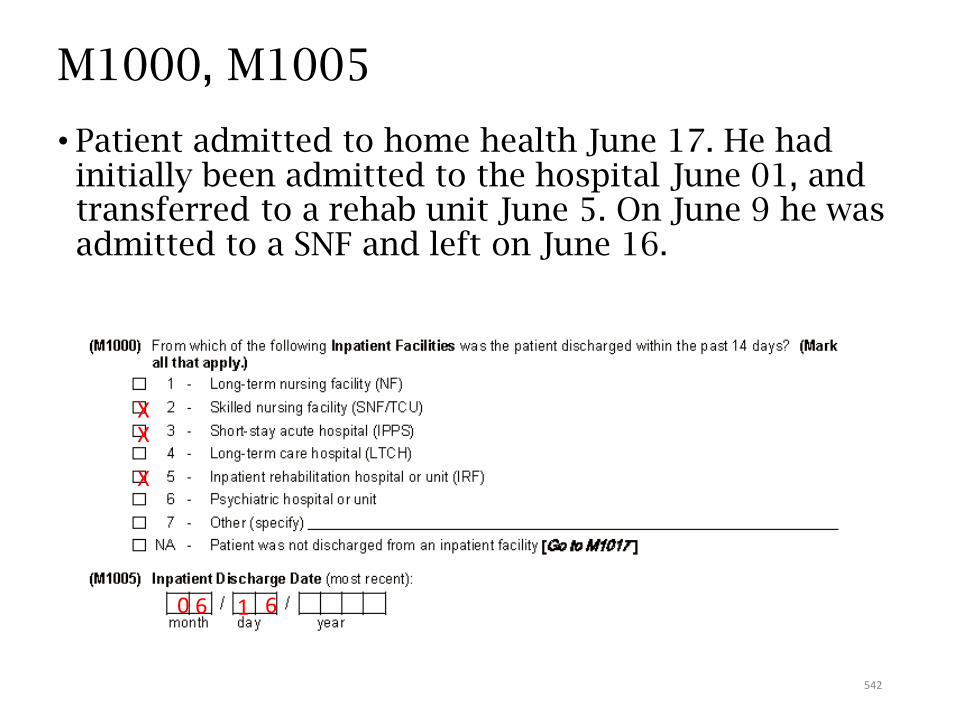
M1000, M1005
• Patient admitted to home health June 17. He had initially been admitted to the hospital June 01, and transferred to a rehab unit June 5. On June 9 he was admitted to a SNF and left on June 16.
XX
X
0 6 1 6
542
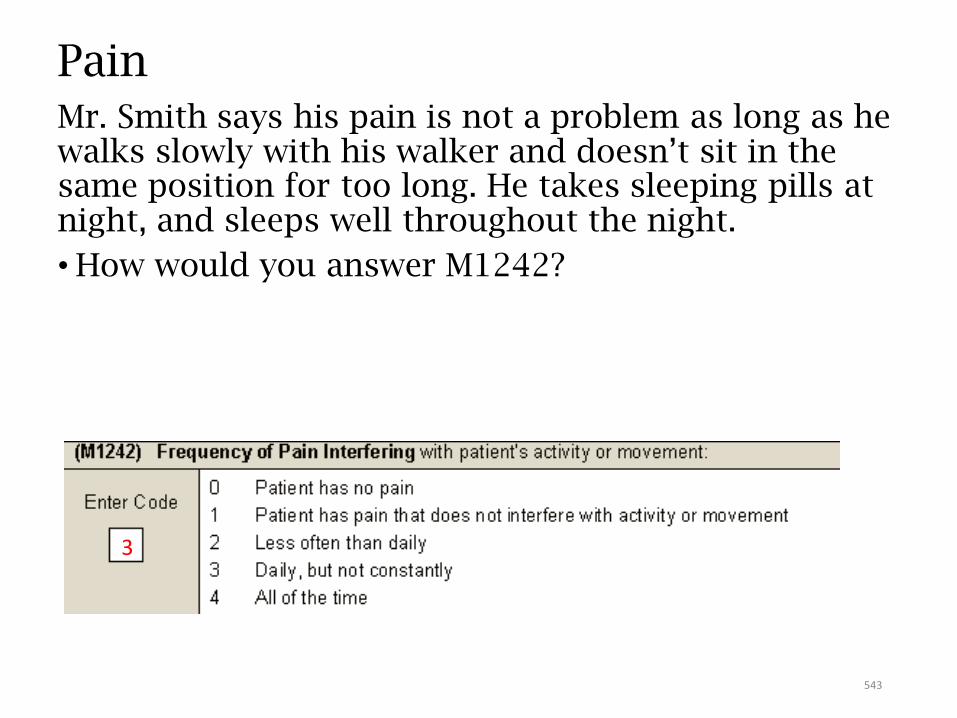
PainMr. Smith says his pain is not a problem as long as he walks slowly with his walker and doesn’t sit in the same position for too long. He takes sleeping pills at night, and sleeps well throughout the night.
• How would you answer M1242?
3
543
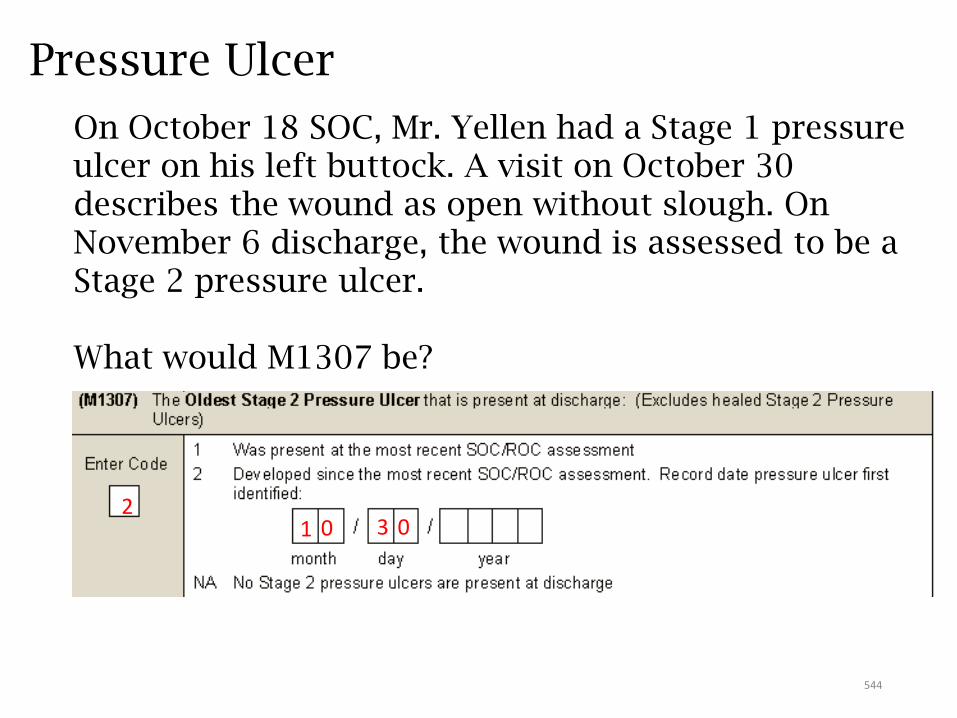
Pressure Ulcer
On October 18 SOC, Mr. Yellen had a Stage 1 pressure ulcer on his left buttock. A visit on October 30 describes the wound as open without slough. On November 6 discharge, the wound is assessed to be a Stage 2 pressure ulcer.
What would M1307 be?
21 0 03
544
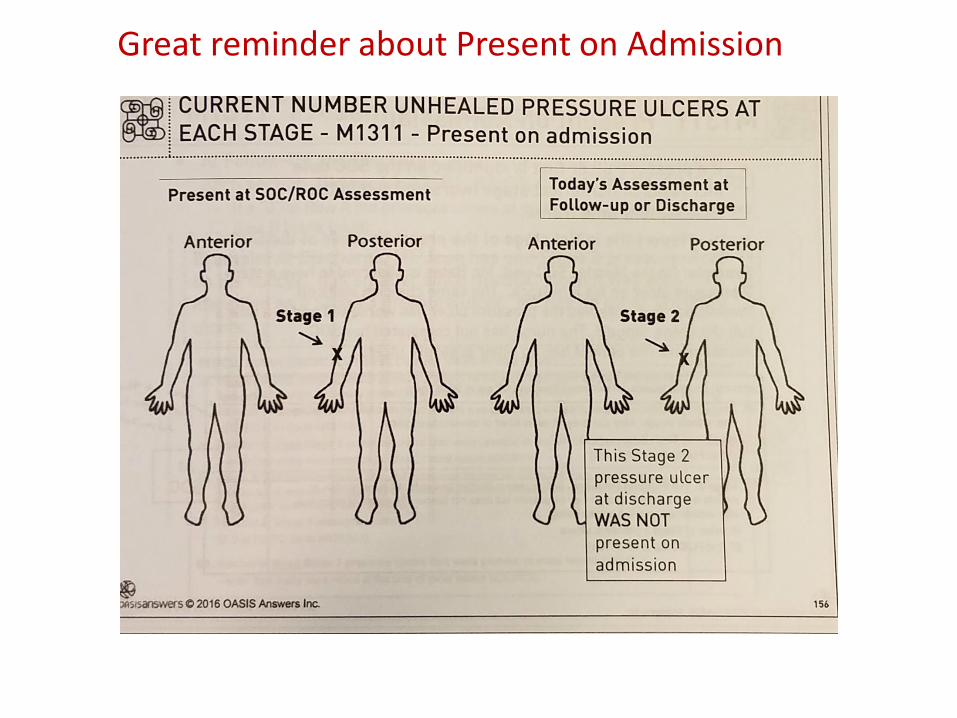
Great reminder about Present on Admission
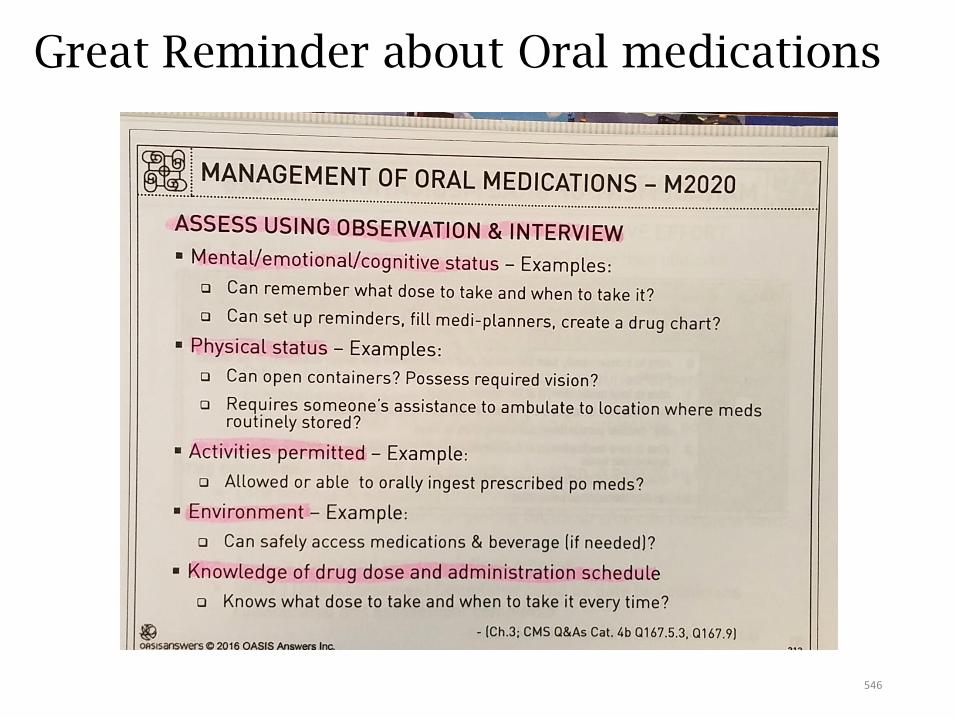
Great Reminder about Oral medications
546
Pressure Ulcer: Common Errors
NEVER reverse stage
Stage 2 are not healing until gone
547
Surgical Wounds: Common Errors
Generally takes 30 days for a surgical site to heal by primary intention
Sites healing by primary intention (incisions) can only be:[0] - newly epithelialized OR
[3] - not healing
Commonly missed: PAC (mediport), dialysis fistula, peritoneal dialysis access
Abscess or ulcer that gets I&D: NOT a surgical wound. Still classified as an abscess or ulcer.
548
M1030 Therapies received at home
Response [1] commonly missed:insulin pump
Hemodialysis or peritoneal dialysis in the home.
Feed Tube:Response [3]: used for nutrition
Response [4]: ONLY receiving flushes or meds
549
550
Facts to Know
551
OASIS and PPS• Time points for OASIS data collection:
• Start of Care (SOC)
• Resumption of Care (ROC) following an inpatient admission
• Follow up – at the end of a 60 day episode
• Other Follow up - when there is an unanticipated improvement or decline in patient’s condition
• Transfer to an inpatient facility
• Discharge, not to a facility
• Death at Home
Note: only SOC and Follow-up (Recertification) are used for determining payment based on a HHRG.
552
Purpose of OASIS
• Performs systematic comparative measurements of home health patient outcomes at two points in time.
• Identifies potentially avoidable outcomes of care.
• Identifies a HHA’s use of best practices in managing patients.
• Provides additional information about patient case-mix characteristics and utilization of resources.
• Risk adjusts outcome data when computing patient outcomes.
553
OASIS as a Payment Tool
• Patients receiving 5 or more visits are assigned one of 153 case mix weights based on equations that are determined by:
• Clinical severity score
• Functional status score
• Service utilization score
• Timing of Episode (early/later) – M0110
• Therapy visits – M2200
554
3 Dimensions or Domains
• Clinical Severity• Primary and secondary diagnosis codes
• Diagnosis to diagnosis interactions or combinations
• Diagnosis to case-mix item interactions or combinations
• Individual case mix items – e.g. M1030, M1242, M1400, M1830
• Functional Status• Functional items – dressing, bathing, toileting, transferring and
ambulation
• Service Utilization (based on therapy services)• 0-13
• 14-19
• 20 +
555
Definitions
• Active treatment
• Day of assessment
• At the time of or at any time since the most recent SOC/ROC
• Assistance
• Bedfast
556
OASIS Conventions
• Understand the time period under consideration for each item.
• Report what is true on the day of the assessment unless a different timeframe is specified in the item or related guidance.
• What is a care episode/quality episode?• Must have a beginning (i.e., a SOC or ROC assessment) and a
conclusion (i.e., a Transfer or Discharge assessment)
• If the patient’s ability varies on the day of the assessment, report the patient’s “usual status” or what is true greater than 50% of the assessment time frame, unless the item specifies differently.
557
More Conventions
• Responses to items documenting a patient’s current status should be based on independent observation of the patient’s condition and ability at the time of the assessment without referring back to previous assessments.
• Combine observation, interview, and other relevant strategies to complete OASIS data items as needed.
• Minimize use of NA and unknown responses.
About the HCS-O Exam
559
Purpose of the HCS-O Certification
• The exam assesses the knowledge of OASIS guidance for clinician’s collecting this data and the reviewer and their ability to apply guidance correctly in
patient-specific scenarios.
• The exam validates that the clinician is able to complete the OASIS an appropriate level of competence.
OASIS competency is a key component in attaining accurate clinical patient outcomes and reimbursement!
560
Exam and Competency AreasFor exam details, go to: https://ahcc.decisionhealth.com
• 80 questions; 3 hours
• Standard conventions and how OASIS works with the Payment System
• Clinical Items including diagnosis coding rules (as related to OASIS)
• Wound Items
• Functional Items
• Process Measures
561
Core Documents
–The OASIS-D Guidance Manual• Chapter 1
• Chapter 3
–CMS OASIS Q&As
–OASIS Considerations for Medicare PPS Patients
–WOCN OASIS-C2 Wound Guidance
•Other documents –Medicare HH CoPs
Test TakingSkills and Tips
Rule #1: Know the OASIS
Conventions!
563
Rule #2:Make Chapter 3 and the Q&As Your Best Friends!
564
565
Rule #3: Read Scenarios Carefully
Read everything…it all means something!
566
Rule # 4: Don’t Assume
Remember what they say about “assume.”
Don’t Do It!
567
Types of Questions
What is the appropriate response in the following scenario?
What is the appropriate date or episode equation?
Which of the following is true?
Which of the following is false ?
If any part of a statement is not true,then the whole thing is not true!

568
Selecting Your Answer
• Highlight important phrases and information, if taking a paper test.
If NOT taking the exam at an approved workshop, research PSI sites in your area.
• Answer the questions you’re sure of first – this helps to build your confidence.
• Hold the difficult questions for last and look at the guidance or Q&As to help you determine the correct answer, if you have time.
569
Resources Allowed for the Exam
• OASIS-D Guidance Manual - Chapters 1 and 3
• CMS OASIS Q&As
• OASIS Considerations for Medicare PPS Patients
• WOCN OASIS-D Wound Guidance
• OASIS Answers “Little Brown Book”
I think this means we’re done!
Thank you for attending!
571
Arlynn Hansell, PT, HCS-D, HCS-O, HCS-H, COS-COwner, Therapy and More, LLCCincinnati, [email protected]
ResourcesOASIS-D Guidance Manual https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-
Instruments/HomeHealthQualityInits/HHQIOASISUserManual.html
CMS OASIS Q&As: https://www.qtso.com/hhatrain.html
Medicare Benefit Policy Manual Chapter 7 https://www.cms.gov/Regulations-and-
Guidance/Guidance/Manuals/downloads/bp102c07.pdf
CY2019 HH PPS Final Rule https://www.cms.gov
572
Resources (cont.)
IMPACT Act of 2014 https://www.cms.gov/Medicare/Quality-Initiatives-Patient-
Assessment-Instruments/Post-Acute-Care-Quality-Initiatives/IMPACT-Act-of-2014-and-Cross-Setting-Measures.html
Quality Measures https://https://www.cms.gov/Medicare/Quality-Initiatives-Patient-
Assessment-Instruments/HomeHealthQualityInits/Home-Health-Quality-Measures.html
OASIS Outcome Measures https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-
Instruments/HomeHealthQualityInits/Downloads/Home-Health-Outcome-Measures-Table-OASIS-D-11-2018c.pdf
OASIS PBQI / Process Measures https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-
Instruments/HomeHealthQualityInits/Downloads/Home-Health-Process-Measures-Table_OASIS-D_11-2018c.pdf
Home Health Compare https://www.medicare.gov/homehealthcompare/search.html
573
Resources (cont.)
Home Health Star Ratings http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-
Instruments/HomeHealthQualityInits/HHQIHomeHealthStarRatings.html
Home Health Care CAHPS Survey https://homehealthcahps.org/
Home Health Value-Based Purchasing Model https://innovation.cms.gov/initiatives/home-health-value-based-
purchasing-model
OASIS Considerations for Medicare PPS Patients https://www.cms.gov/OASIS/Downloads/OASISConsiderationsforPPS
574
Resources (cont.)WOCN Guidance on OASIS-D Integumentary Items
www.wocn.org
NPUAP Pressure Ulcer Staging System www.npuap.org http://www.npuap.org/resources/educational-and-clinical-
resources/pressure-injury-staging-illustrations/
Pressure Ulcer risk Assessment www.bradenscale.com/images/bradenscale.pdf
Geriatric Depression Scale https://consultgeri.org/try-this/general-assessment/issue-4.pdf
Cornell Scale for Depression in Dementia http://geropsychiatriceducation.vch.ca/docs/edudownloads/depression/cornell_
scale_depression.pdf
575









![OASIS-D Handouts [Read-Only] · 11/06/2018 5 New items are added Different time point versions of some items Removal of items Revision of some items Updated Skip Patterns 9 Chapter](https://static.fdocuments.net/doc/165x107/5e5c7775b108056208748d8a/oasis-d-handouts-read-only-11062018-5-new-items-are-added-different-time-point.jpg)






![OASIS-D Handouts [Read-Only]€¦ · • Describe the major changes from OASIS-C2 to OASIS-D • Understand OASIS M-item coding instructions to accurately code new and revised OASIS](https://static.fdocuments.net/doc/165x107/5ec3637ace40ce0748747c2e/oasis-d-handouts-read-only-a-describe-the-major-changes-from-oasis-c2-to-oasis-d.jpg)
