O Oral Maxillolac $ur9 Orthognathic Surgery Versus...
7
OOral Maxillolac $ur9 53:572-578, "1995 Orthognathic Surgery Versus Orthodontic Camouflage in the Treatment of Mandibular Deficiency MYRON R. TUCKER, DDS* Although there have been significant advances in the combined surgical and orthodontic treatment of patients with mandibular deficiency, many patients continue to be treated by orthodontics alone without consideration for surgical correction. The correction of Class II maloc- clusion due to mandibular deficiency can be accom- plished in a variety of ways. Proffit and Akerman de- scribed three primary treatment approaches for correction of mandibular deficiency and the associated Class II malocclusion] These approaches include: 1) growth modification so that the jaw discrepancy is elimi- nated as a result of mandibular growth; 2) compensation of the dentition with retraction of the upper incisors and proclination of the lower incisors, or both, in an effort to camouflage rather than correct the skeletal problem; or 3) surgical correction of the jaw abnormality. In the case of mandibular deficiency, this is usually accom- plished by mandibular advancement. A fourth option that could be considered includes orthodontic treatment of the malocclusion, compensating the dentition, com- bined with genioplasty. This option is intended to cor- rect the malocclusion with orthodontic compensation and improve facial esthetics with a somewhat simpler surgical procedure. 2 Each of these treatment approaches is associated with controversy, including which patients benefit most from a specific treatment and the timing of treat- ment, particularly when considering growing patients. During the past two decades correction of Class II malocclusions with surgical advancement of the man- dible has improved dramatically. This is due in part to significant advances in technology, as well as increased Received from University Oral and Maxillofacial Surgery, Char- lotte, NC. * In private practice. Address correspondence and reprint requests to Dr Tucker: Uni- versity Oral and Maxillofacial Surgery, 8738 University City Blvd, Charlotte, NC 28213. © 1995 American Association of Oral and Maxillofacial Surgeons 0278-2391/95/5305-001453.00/0 experience on the part of both orthodontists and sur- geons in treating mandibular deficiency. Both orth- odontic and surgery residents generally get adequate exposure to patients receiving this type of treatment during their training. The use of rigid fixation techniques, and the trend toward shorter inpatient hospital stays have dramati- cally decreased the impact of surgery on patients. Whereas 15 years ago patients frequently spent 2 nights and nearly 3 days in the hospital, patients now routinely stay only overnight to as little as a few hours in an outpatient surgical facility. Instead of having their teeth wired together for 6 to 8 weeks, patients routinely undergo mandibular advancement surgery with no maxillomandibular fixation. All of this results in more rapid recovery from surgery, earlier return to work, and much less disruption of the lives of patients and their families. There do continue to be risks that are associated with surgery, including adverse outcomes such as neu- rosensory abnormalities, failure to achieve the antici- pated occlusal result, nonunion, malunion, and the as- sociated risks of general anesthesia. However, the low frequency and lack of severity of most complications has made surgical treatment much more commonplace in the correction of Class II malocclusions. Whereas surgical treatment was once viewed as a "last resort" reserved for those with the most severe abnormalities, it is now be considered a routine treatment for correc- tion of mandibular deficiency in indicated cases. Patient Evaluation Much of the controversy related to treatment may actually result from each practitioner's assessment of the clinical problem. A recent study documented sig- nificant disagreement between trained orthodontists and surgeons when evaluating patients with dentofacial deformities. 3 The differences in assessment of the pa- tient's deformity included the specific nature of the 572
Transcript of O Oral Maxillolac $ur9 Orthognathic Surgery Versus...

O Oral Maxillolac $ur9 53:572-578, "1995
Orthognathic Surgery Versus Orthodontic Camouflage in the Treatment of
Mandibular Deficiency MYRON R. TUCKER, DDS*
Although there have been significant advances in the combined surgical and orthodontic treatment of patients with mandibular deficiency, many patients continue to be treated by orthodontics alone without consideration for surgical correction. The correction of Class II maloc- clusion due to mandibular deficiency can be accom- plished in a variety of ways. Proffit and Akerman de- scribed three primary treatment approaches for correction of mandibular deficiency and the associated Class II malocclusion] These approaches include: 1) growth modification so that the jaw discrepancy is elimi- nated as a result of mandibular growth; 2) compensation of the dentition with retraction of the upper incisors and proclination of the lower incisors, or both, in an effort to camouflage rather than correct the skeletal problem; or 3) surgical correction of the jaw abnormality. In the case of mandibular deficiency, this is usually accom- plished by mandibular advancement. A fourth option that could be considered includes orthodontic treatment of the malocclusion, compensating the dentition, com- bined with genioplasty. This option is intended to cor- rect the malocclusion with orthodontic compensation and improve facial esthetics with a somewhat simpler surgical procedure. 2
Each of these treatment approaches is associated with controversy, including which patients benefit most from a specific treatment and the timing of treat- ment, particularly when considering growing patients.
During the past two decades correction of Class II malocclusions with surgical advancement of the man- dible has improved dramatically. This is due in part to significant advances in technology, as well as increased
Received from University Oral and Maxillofacial Surgery, Char- lotte, NC.
* In private practice. Address correspondence and reprint requests to Dr Tucker: Uni-
versity Oral and Maxillofacial Surgery, 8738 University City Blvd, Charlotte, NC 28213.
© 1995 American Association of Oral and Maxillofacial Surgeons
0278-2391/95/5305-001453.00/0
experience on the part of both orthodontists and sur- geons in treating mandibular deficiency. Both orth- odontic and surgery residents generally get adequate exposure to patients receiving this type of treatment during their training.
The use of rigid fixation techniques, and the trend toward shorter inpatient hospital stays have dramati- cally decreased the impact of surgery on patients. Whereas 15 years ago patients frequently spent 2 nights and nearly 3 days in the hospital, patients now routinely stay only overnight to as little as a few hours in an outpatient surgical facility. Instead of having their teeth wired together for 6 to 8 weeks, patients routinely undergo mandibular advancement surgery with no maxillomandibular fixation. All of this results in more rapid recovery from surgery, earlier return to work, and much less disruption of the lives of patients and their families.
There do continue to be risks that are associated with surgery, including adverse outcomes such as neu- rosensory abnormalities, failure to achieve the antici- pated occlusal result, nonunion, malunion, and the as- sociated risks of general anesthesia. However, the low frequency and lack of severity of most complications has made surgical treatment much more commonplace in the correction of Class II malocclusions. Whereas surgical treatment was once viewed as a "last resort" reserved for those with the most severe abnormalities, it is now be considered a routine treatment for correc- tion of mandibular deficiency in indicated cases.
Patient Evaluation
Much of the controversy related to treatment may actually result from each practitioner's assessment of the clinical problem. A recent study documented sig- nificant disagreement between trained orthodontists and surgeons when evaluating patients with dentofacial deformities. 3 The differences in assessment of the pa- tient's deformity included the specific nature of the
572

MYRON R. TUCKER 5 7 3
deformity, as well as the severity of the deformity. The differences in opinion regarding the severity of the deformity may be compounded by each practitioner's interest or focus on a specific component of the maloc- clusion, ie, skeletal versus dental. In a study assessing patients who were evaluated for orthodontic and surgi- cal treatment, Proffit et al 4 found fewer Class II patients with severe overjet than with significant skeletal defi- ciency. This is probably due to significant dental com- pensation (lower incisor protrusion and upper incisor retraction) reducing the degree of dental abnormality despite a significant skeletal deformity. Focusing more on the occlusal relationship and less on the skeletal position may result in different treatment approaches than would be generated if more attention was placed on the skeletal component.
Most patients seek orthognathic surgical treatment based on the recommendation of the treating orthodon- tist. 5 Because many orthodontists may not focus on the skeletal component of mandibular deficiency, or consider it severe enough to warrant treatment, many patients with Class II malocclusions may never receive a surgical consultation or have this treatment alterna- tive discussed as a viable option.
At the present time there are no widely accepted guidelines, nor is there a "gold standard," for determin- ing which cases of Class lI malocclusion would best be treated with surgery versus orthodontic camouflage. Proffit and Akerman, I have described the envelope of discrepancy, which can help serve as a guide when se- lecting appropriate treatment modalities for patients with a variety of maxillofacial abnormalities of varying sever- ity. This envelope of discrepancy is based on the severity of the abnormal occlusal relationships (Fig 1). Using this concept, three asymmetric circles are used to help visualize the range of correction that can be accom- plished by orthodontic tooth movement alone, a larger range of correction that can be accomplished by func- tional appliance therapy in combination with orthodontic treatment, and an even larger range of correction that uses surgery as part of the treatment. Using this concept, the outer limits of correction for each type of treatment can be clearly visualized. However, in this diagram, the limits of treatment are represented by a finite line sepa- rating each type of treatment. In actual clinical practice such strict division of patients into types of treatment cannot and does not occur. A variety of treatment options continues to exist for each patient based on his or her primary goals for treatment, as well as practitioner pref- erence and experience.
Patient Motivations for Treatment
All medical and dental treatment should initially be based on the patient's chief complaint. In the case of patients who may be candidates for orthodontic and
T
FIGURE 1. The envelope of discrepancy. The limits of tooth movement that can be accomplished by various types of treatment are shown diagramatically in the asymmetric circles. Orthodontic tooth movement is represented by the inner circle or envelope. Changes that can occur as a result of orthopedic or functional appli- ance therapy in growing patients is shown in the middle envelope and the limits of surgical change are represented by the outer envelope. (Reprinted with permission.~)
surgical treatment, there is a wide variety of chief com- plaints expressed by patients and significant differ- ences in patient goals for outcomes of treatment. Pa- tient's goals for treatment can include: 1) Enhanced dental esthetics; 2) Improved dental function; 3) Better facial esthetics; 4) Resolution or improvement of tem- poromandibular joint or muscle pain; and 5) Improved long-term maintenance of the dentition when factors such as periodontal problems are exacerbated by real- occlusions. Each of these concerns must be prioritized by the patient, orthodontist, and surgeon to insure that the most important goals for the patient are achieved as a result of treatment.
The importance of facial esthetic improvement can-

574 ORTHOGNATHIC SURGERY VS ORTHODONTIC CAMOUFLAGE
not be underestimated in patients who are considering orthodontic and surgical treatment. In one study, a sig- nificant percentage of females (53%) and males (41%) indicated that esthetics and improvement in appearance were a major factor in their goal for seeking treatment. 6 Flanary et al 7 found that facial esthetics was of signifi- cant importance in 78% of patients electing to undergo orthodontic and surgical treatment.
When patients describe improvement in facial es- thetics as a high priority goal for treatment, the exact nature of their concerns and goals must be carefully evaluated. Variation in patients' evaluation of their own facial esthetics may eventually have a significant impact on the type of treatment. For instance, two patients may present with nearly identical facial ap- pearance, a mild mandibular deficiency and Class II malocclusion. Each patient may list improvement in facial esthetics as a primary goal for seeking treatment. One patient may describe dentoalveolar protrusion as the primary facial abnormality. In many cases this will be amenable to orthodontic treatment only. On the other hand, a patient who describes deficiency in pro- jection of the lower jaw as the facial abnormality, may be treated best with a combination of orthodontics and surgery.
Even when nearly identical clinical situations exist, some patients view their deformity as being much more severe than others. Bell et al8 found that patients who opted for surgical treatment were significantly less likely to perceive themselves to be in the normal range when evaluating their own profile. For this reason it is important to specifically identify this group of pa- tients, so that the treatment plan can be aimed at ad- dressing all of their concerns in order to achieve their goals for treatment in the best possible way.
Treatment Planning
The data collection and analysis for treatment plan- ning of mandibular deficient patients are relatively standardized in both the orthodontic and surgical com- munities. Data collection includes a patient interview, clinical examination, radiographs, photographs, study models and, in some practices, computerized video imaging. The data analysis includes interpretation of cephalometric radiographic data, model analysis, and treatment projections using cephalometric prediction tracings and, in some cases, trial setup of occlusal models. The importance of each aspect of the decision- making process is well known, has been discussed in the companion article in this issue, 9 and will not be discussed further in this article.
The use of video imaging has increased as a result of improved computer technology, decreased cost, more accurate imaging projection, and increased acceptance as a treatment-planning modality, l° In the absence of
growth, tracings generated from cephalometric radio- graphs, can be used with reasonable accuracy to predict surgical outcome. However, it is extremely difficult for most patients to clearly understand the impact of treatment on facial esthetics when viewing cephalo- metric profile tracings. The recent use of video imaging has enhanced the patient's ability to perceive projected surgical changes and make a more informed decision related to possible treatment options.
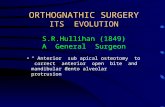
It is obvious that patients with nearly identical man- dibular deficiency and Class II malocclusions will have dramatic differences in facial appearance as a result of orthodontic versus surgical treatment, l~ Variations in orthodontic treatment options can also produce marked differences in facial profile. Paquette et alx2 described differences in facial profile as a result of correction of Class II malocclusions with or without extraction. Although they are not as dramatic as changes some- times seen with surgical treatment, facial profile changes as a result of various orthodontic options may also be of significant importance to patients. The ability to show patients the effect on the facial profile of both orthodontic and surgical treatment options provides better information regarding treatment outcome. This allows patients to interact and participate in their own treatment planning by providing an assessment of their own perception of facial esthetic changes (Fig 2). At the present time the computerization of predicted changes is limited to two-dimensional images. In the future, computer technology will most likely provide the ability to generate predicted facial images in three dimensions.
Efficacy of Surgical Treatment
The efficacy of treatment can be judged using a variety of parameters including improvement in occlu- sal characteristics such as overbite, overjet, and buccal interdigitation, and improvement in facial esthetics and long-term stability. Very few studies have been de- signed that directly compare similar homogeneous populations of patients divided into surgical and orth- odontic treatment groups. Proffit et a113 compared out- comes of orthodontic and surgical orthodontic treat- ment of Class II malocclusions in 57 adult patients treated for similar occlusal and skeletal problems using cephalometric data and dental casts to evaluate the relative success of treatment. The outcome of each individual treatment was evaluated in two separate ways. First, the result was judged based on whether the final measurement of a particular result of treatment fell within a normal range. In this study acceptable results were similar in both groups when evaluating overbite and buccal interdigitation. However, there were two obvious differences between the surgical and orthodontic groups: in the surgical group acceptable

MYRON R. TUCKER 5 7 5
Pretreatment Orthodontic Prediction Surgical Prediction
FIGURE 2. Video imaging treatment options. A, Pretreatment photograph. B, Cephalometric superimposition showing pretreatment profile and results obtained with orthodontic treatment only (extraction of upper and lower premolar teeth) and with surgical treatment. C, Video image of orthodontic only treatment plan. D, Video image of surgical treatment plan.
overjet was achieved in 95% of cases versus 74% in the orthodontic treatment group, and an acceptable ANB difference was achieved in 81% of the surgical patients versus 52% of patients who received only orthodontic treatment.
In the same study, ~3 the efficacy of treatment was also measured by evaluating the actual change oc- curring in a measurement after treatment expressed as a percentage of the change needed to give an ideal post-treatment value. The closer a post-treatment value was to 100% of the ideal, the more "successful" the treatment. When evaluating treatment efficacy in this manner, a significantly greater percentage of the ideal goal was achieved in surgery patients when evaluating the skeletal ANB difference, soft tissue AB difference, the location of the maxillary incisor, and overjet. The
percentage differences of the goals achieved for overjet and ANB difference are shown in Figures 3 and 4.
Patients with mandibular deficiency who undergo orthodontic and surgical correction have greater im- provement in facial esthetics when compared with pa- tients undergoing orthodontic treatment only. In the Proffit et al study ~3 previously described, the esthetic outcomes of patients were evaluated by orthodontists and surgeons, comparing orthodontic only treatment with surgical advancement of the mandible in combi- nation with orthodontic treatment. There was no sig- nificant disparity between the opinions of orthodontists and surgeons when evaluating these patients. The es- thetic changes from orthodontic treatment only ap- peared to be small and the changes were as likely to be negative as positive (Fig 5A). However, the surgical

5 7 6 ORTHOGNATHIC SURGERY VS ORTHODONTIC CAMOUFLAGE
OVERJET CORRECTION-PERCENTAGE OF GOAL ACHIEVED
Percent of patients 80
70
60
50
30
2O
10
0 <20% 21-40% 41-60% 61-80% >80%
Percent of goal achieved 1~3Orthodontics mmSurgery
FIGURE 3. Graphic representation of the percentage of an ideal goal for overjet correction achieved as the result of orthodontics only and surgical and orthodontic treatment. (Reprinted with permis- sion. 14)
group had significant improvement in esthetic ratings for 11 of 13 patients (Fig 5B). As would be expected, the improvement appeared to be greatest in patients with the lowest pretreatment ratings. Although the es- thetic changes were evaluated by orthodontists and sur- geons who may evaluate these features more critically, it has been shown that the lay public can also detect changes in facial esthetics as a result of surgical treat- ment. In a study by Dunlevy et a114 there was general agreement among laypersons, orthodontists, and oral and maxillofacial surgeons when asked to evaluate pa- tients' improvement in facial appearance after ortho- gnathic surgery.
It has also been shown that patients undergoing or- thognathic surgical treatment experience greater im- provement in facial body image scores when compared with patients undergoing orthodontic treatment only or patients who decline any type of treatment whatsoever (Fig 6). As with professionals' judgement of facial esthetics, overall body image and facial image appear to be lowest at the initial assessment for patients who elect to undergo surgery, when compared with patients undergoing orthodontic treatment only. Over the time of treatment there is some improvement, but this is less in patients receiving orthodontic treatment only than in those undergoing surgical correction.
Special Considerations in Adolescents
Unlike adult patients, developing adolescents will continue to have some facial growth, which can play a part in treating Class II malocclusions. In a recent study, surgical versus orthodontic treatment of Class II malocclusions was evaluated in adolescent pa- tientsJ 5 In this study three groups were identified: those treated successfully with orthodontics alone,
those treated with orthodontic and surgical correction, and those whose orthodontic treatment was judged to be unsuccessful. In this study, successful orthodontic treatment resulted from a combination of retraction of the maxillary incisors and protraction of the mandibu- lar incisors in combination with some continued facial growth. Forty percent of these patients had greater than 2 mm of anterior-posterior growth during the treatment period. The unsuccessful treatment group initially had greater overjet, more severe mandibular deficiency, in- creased anterior facial height, and less retraction of maxillary incisors and less growth during treatment. The recommendation of this study was that in Class II adolescents who are beyond the growth spurt, sur- gery is most likely to be needed for successful correc- tion of the malocclusion if the overjet is greater than 10 mm, if the distance from pogonion to nasion perpen- dicular is 18 mm or more, if mandibular body length is less than 70 mm, or if facial height is greater than 125 mm.
Other Considerations
In addition to the functional, occlusal, and facial esthetic considerations, several other factors must be considered when developing a treatment plan for cor- rection of Class II mandibular deficient malocclu- sions. Patient compliance may be a significant factor in the outcome of any type of treatment. Some types of treatment require much more compliance or partici- pation on the part of the patient to achieve the desired goal. Maxillary retraction dependent on use of a head- gear is an important part of orthodontic treatment to eliminate overjet in many patients. Headgear must be worn consistently and for the appropriate amount of time each day to maximize the effect of this type of treatment. Patients who are unable or unwilling to
ANB ANGLE CORRECTION-PERCENTAGE OF GOAL ACHIEVED
Percent of patients 60
50
40
30
lO
o - ,r <20% 21-40% 41-80% 61-80% >80%
Percent of goal achieved E3Orthodontics BIBSurgery
FIGURE 4. Percentage of ideal goal for ANB correction achieved as a result of orthodontics only or orthodontic-surgical treatment. (Reprinted with permission. 13)

MYRON R. TUCKER 577
ESTHETIC RATING A BEFORE AND AFTER ORTHODONTIC TREATMENT
MEAN ESTHETIC RATING 80
ESTHETIC RATING B BEFORE AND AFTER SURGICAL TREATMENT
MEAN ESTHETIC RATING 80
60
40 ¸
20 2 3 4 5 6 7 8 9 ' 10 '11 ' 12 ' 13
SUBJECT NUMBER
- - - PRETREATMENT - - POST TREATMENT
60
40
20
. . . . . . . . . . . . . . . . . . = . . . . . . . .
1 2 3 4 5 6 7 8 9 ' 1 0 '11 ' 12 ' 13 ' SUBJECT NUMBER
- - - PRETREATMENT - - POST TREATMENT
FIGURE 5. Esthetic ratings before and after treatment. A, The orthodontics-only patients started at a slightly higher level than patients undergoing orthodontic and surgical treatment. B, Surgical patients had greater increase in facial esthetic ratings as a result of treatment. (Adapted with permission. 13)
comply with this type of treatment are less likely to achieve the treatment goals. In many cases, patients would prefer to undergo surgical correction as op- posed to committing themselves to participation in headgear therapy.
Patients undergoing orthodontic treatment alone may be in treatment for shorter periods than patients undergoing surgery in combination with orthodon- tics. L3 There are however, several situations where a combined orthodontic-surgical therapy may decrease treatment time. An example would be when orthodon- tic treatment only will require extractions and space closure as part of the orthodontic camouflage therapy. The same patient might be treated quicker without ex- traction, allowing for surgery at an earlier time in treat- ment followed by final orthodontic detailing.
The risks of surgery must always be considered and balanced against the benefits of surgical treatment. Sur- gery will always be associated with some pain, swell-
FACIAL-BODY IMAGE
Presurg ' 1 -2 d postop ' 4 - 6 w postop '24 mo postop ' Interval during t reatment
- - O r t h o - S u r g e r y - - Orthodont ics only
FIGURE 6. Facial body-image scores for patients undergoing sur- gical-orthodontic treatment, orthodontics only, and no treatment. (Reprinted with permission. 5)
ing, and the possibility of intraoperative or postopera- tive bleeding. Other long-term complications such as neurosensory abnormality, nonunion, malunion, post- operative malocclusion, and relapse must also be con- sidered. Current technology and practitioner experi- ence have greatly reduced the complications resulting from this type of treatment and increased the level acceptance by patients and orthodontists. When pro- viding patients with information regarding surgical treatment, it is important to make it as accurate as possible. In some cases this can be provided by an orthodontist with wide experience with surgical pa- tients who is familiar with all aspects of surgical treat- ment; however, in most cases, this information is best provided by an oral and maxillofacial surgeon who routinely performs the procedure.
As a part of informed consent, patients should also be counseled about alternative treatments and the risks and benefits associated with each of these alternatives. While, in general, orthodontic treatment may be per- ceived as less risky than surgical treatment, there are occasions where certain problems may occur as the result of orthodontic treatment that may be less likely to happen with orthodontic treatment in combination with surgical correction. One example would be the possibility of severe resorption of maxillary incisor roots resulting from retraction during orthodontic cam- ouflage treatment. Kaley et all6 recently described a 20 times greater risk of resorption in maxillary incisor roots when they are torqued against the palatal cortical plate, the exact movement required when retracting maxillary incisors in correction of Class II malocclu- sions.
The current medicolegal environment requires that patients be fully counseled regarding all of their alter- natives for treatment of a specific problem. When surgeons discuss the possibility of surgical treatment of mandibular deficiency it is imperative that they

5 7 8 ORTHOGNATHIC SURGERY VS ORTHODONTIC CAMOUFLAGE
also discuss the possibilities of no treatment and orth- odontic treatment only, presenting their assessment of the advantages and disadvantages of each treatment. Orthodontists discussing correction of Class II maloc- clusion and mandibular deficiency also should present the possibility of surgical treatment to the patient along with a realistic assessment of the risks and ben- efits and projected outcome of each type of treatment. Failure to provide adequate information that would allow the patient to make an informed decision re- garding type of treatment may have medicolegal im- plications if the patient is not satisfied with the out- come of treatment.
Finances appear to be one of the disadvantageous factors when a patient is considering surgery as part of the corrective treatment for a Class II malocclusion. Because surgery requires operating room time, a same- day admission or overnight hospital stay, and anesthe- sia and other ancillary fees in addition to the surgical fee, this obviously increases the cost of treatment. The effect of decreased third-party payment for this type of surgical treatment has become a major" factor in influencing many patients to elect nonsurgical treat- ment. Although surgical treatment will always increase the cost to some degree, efforts to reduce operating time and hospitalization have resulted in significant cost reduction. Further efforts in this regard will hope- fully ease the financial burden associated with surgical treatment.
Summary
Surgical correction of Class II malocclusions, when associated with mandibular deficiency, often has im- proved results with combined orthodontic and surgical correction compared with orthodontic treatment alone. Strong consideration of surgical correction of mandib- ular deficiency should be based on the following ques- tions:
1) Do the patient's goals for treatment place a high priority on improvement in facial esthetics? As a corollary, even patients who are not particularly concerned with facial esthetics, but who may have a worsening in facial appearance as a result of orthodontic camouflage, should be considered for surgical correction. This may include patients with lack of upper lip support, an obtuse nasola- bial angle, a large nose, and a long lower face height, all of which may become more apparent as a result of orthodontic camouflage treatment.
2) Are the orthodontic movements required in ex- cess of the envelope of discrepancy so that
adequate orthodontic correction may not be achieved?
3) Could orthodontic-surgical treatment result in a significant decrease in treatment time? An exam- ple would be when surgical treatment in combi- nation with orthodontics could be accomplished without extraction, whereas orthodontic treat- ment alone would require extraction and space closure.
4) Is there adequate patient compliance? Would orthodontic treatment alone be as ineffective without adequate patient cooperation?
5) Are the risks of surgery within acceptable levels? Are the benefits of surgical treatment, as pre- viously described, obvious?
References
1. Proffit WR, Ackerman JL: Diagnosis and treatment planning, in Graber M, Vanarsdall RL Jr (eds): Orthodontics: Current Principals and Treatment. St Louis, MO, Mosby, 1994
2. Proffit WR, Turvey TA, Moriarty J: Augmentation genioplasty as an adjunct to conservative orthodontic treatment. Am J Orthod 79:473, 1983
3. Phillips C, Bailey LJ, Sieber RP: Level of agreement in clini- cians perception of Class II malocclusions. J Oral Maxillofac Surg 52:565, 1994
4. Proffit WR, Phillips C, Dann C: Who seeks surgical-orthodontic treatment. Int J Adult Orthod Orthognath Surg 5:153, 1990
5. Kiyak HA, Bell R: Psychosocial considerations in surgery and orthodontics, in Proffit WR, White RP Jr (eds): Surgical Orth- odontic Treatment. St Louis, MO, Mosby, 1991, pp 71-94
6. Kiyak HA, Hohl T, Sherrick P, et al: Sex differences and motives for and outcomes of orthognathic surgery. J Oral Surg 39:757, 1981
7. Flanary CM, Batnwell GM, Alexander JM: Patient perceptions of orthognathic surgery. Am J Orthod 88:137, 1985
8. Bell R, Kiyak HA, Joondeph DR, et al: Perceptions of facial profile and their influence on the decision to undergo ortho- gnathic surgery. Am J Orthod 88:323, 1985
9. Thomas PM: Camouflage versus surgery and the treatment of mandibular deficiency. J Oral Maxillofac Surg 53:579-587, 1995
10. Sarver DM, Johnston MW, Matukas VJ: Video imaging for planning and counseling for orthognathic surgery. J Oral Maxillofac Surg 46:939, 1988
11. Cassidy DW Jr, Herbosa EG, Rotskoff KS, et al: A comparison of surgery and orthodontics in "Borderline" adults with Class II, division I malocclusions. Am J Orthod Dentofac Orthop 104:455, 1993
12. Paquette DE, Beattie JR, Johnston LE Jr: A long-term compari- son of nonextraction and premolar extraction edgewise ther- apy in "borderline" Class II patients. Am J Orthod Dentofac Orthop 102:1, 1992
13. Proffit WR, Phillips C, Douvartzidis N: A comparison of out- comes of orthodontic and surgical-orthodontic treatment of Class II malocclusions in adults. Am J Adult Orthod Dentofac Orthop 101:556, 1992
14. Dunlevy HA, White RP Jr, Proffit WR, et al: Professional and lay judgment of facial esthetics following orthognathic sur- gery. Int J Adult Orthod Orthognath Surg 3:151, 1987
15. Proffit WR, Phillips C, Tulloch JFC, et al: Surgical versus orth- odontic correction of skeletal Class II malocclusion in adoles- cents: Affects and indications. Int J Adult Orthod Orthognath Surg 7:209, 1992
16. Kaley JA, Phillips C: Factors related to root resorption in edge- wise practice. Angle Orthod 61:125, 1991

![Maxillarydistractionosteogenesisversusorthognathic ... · [Intervention Review] Maxillary distraction osteogenesis versus orthognathic surgery for cleft lip and palate patients Dimitrios](https://static.fdocuments.net/doc/165x107/5f8b909b25543c1aa612fc00/maxillarydistractionosteogenesisversusorthognathic-intervention-review-maxillary.jpg)