Nutrition Information and Analysis Systems in Yemen
80
1 Nutrition Information and Analysis Systems in Yemen Volume 1 Key Findings & Recommendations Submission Date: 30 April 2021 Prepared under the Technical Assistance to Strengthen Capabilities (TASC) Project Submitted by: DAI Global Health 3 rd floor, Block C, Westside London Road, Apsley HP3 9TD, United Kingdom Tel: +44 1442 202400 Disclaimer: This report was produced by TASC through support provided by UK aid and the UK Government; however, the views expressed do not necessarily reflect the UK Government’s official policies. Noreen Mucha, Team Leader Nutrition & Monitoring and Evaluation Advisor Christopher Coffey, Co-Team Leader Nutrition & Monitoring and Evaluation Advisor Peter Hailey, Nutrition Information Systems Technical Advisor Rita Abi Akar, Nutrition Advisor, TASC Core Team
Transcript of Nutrition Information and Analysis Systems in Yemen

1
Nutrition Information and Analysis Systems in Yemen
Volume 1 Key Findings & Recommendations
Submission Date: 30 April 2021 Prepared under the Technical Assistance to Strengthen Capabilities (TASC) Project Submitted by: DAI Global Health 3rd floor, Block C, Westside London Road, Apsley HP3 9TD, United Kingdom Tel: +44 1442 202400 Disclaimer: This report was produced by TASC through support provided by UK aid and the UK Government; however, the views expressed do not necessarily reflect the UK Government’s official policies. Noreen Mucha, Team Leader Nutrition & Monitoring and Evaluation Advisor
Christopher Coffey, Co-Team Leader Nutrition & Monitoring and Evaluation Advisor
Peter Hailey, Nutrition Information Systems Technical Advisor
Rita Abi Akar, Nutrition Advisor, TASC Core Team

i
Table of Contents
EXECUTIVE SUMMARY ........................................................................................................................ 1
Scope of Work ....................................................................................................................................... 1
Nutrition Programming in Yemen ........................................................................................................ 1
Overview of the Main Sources of Nutrition Information ................................................................... 1
Key Findings and Recommendations ................................................................................................. 2 National Nutrition Monitoring and Evaluation Accountability Framework ....................................................... 2 Harmonizing and Standardising Monitoring and Reporting .............................................................................. 2 Capacity Development for NIS within the Health Workforce ............................................................................ 3 Strengthening Reporting through the DHIS-2 and Mobile Applications ............................................................ 4 Analysis and Use of Available Data .................................................................................................................... 4 Joint Nutrition Data Repository and Dashboard ................................................................................................ 5 Use of Routine Data Sub-National Level to Increase Effectiveness and Coverage ............................................ 5 Health Facility Level Data Use and Analysis ....................................................................................................... 6
1. INTRODUCTION ................................................................................................................................. 7
1.1 Background Context ....................................................................................................................... 7
1.2 Scope of Work Objectives and Methodology ............................................................................... 8
1.3 Key Limitations ............................................................................................................................... 9
2. OVERVIEW OF CURRENT NUTRITION INFORMATION SYSTEMS IN YEMEN .......................... 10
2.1 Data Sources, Service Delivery Entry Points, and Data Users ................................................ 10
2.2 Existing Data Flows, Monitoring and Data Collection Forms................................................... 11
2.3 Quality (Accuracy and Completeness) of nutrition data, data cleaning and feedback mechanisms ........................................................................................................................................ 16
2.4 Nutrition Information Systems in Humanitarian Settings ......................................................... 18
3. STREAMLINING THE SYSTEM: PRIORITISATION AND HARMONISATION OF NUTRITION DATA & INFORMATION COLLECTION AND REPORTING MECHANISMS .......................... 20
3.1 Overview & Current Situation and Key Challenges ................................................................... 20 3.1.1 Developing a Framework for Action and Standardising Monitoring and Reporting (Recommendations 1.1 – 1.3) .......................................................................................................................................................... 20 3.1.2 Capacity Development within the Health Workforce (Recommendations 1.5 – 1.9) ............................. 23 3.1.3 Short Message Service (SMS) and Web-based Messaging Applications (Recommendations 1.10) ....... 23 3.1.4 Strengthening Reporting and Analysis through the DHIS-2 (Recommendation 1.11) ............................ 24
3.2 Streamlining the Data Collection and Reporting Mechanisms Systems ................................ 25 National Nutrition Monitoring and Evaluation Accountability Framework for Action .................................... 25 Harmonizing and Standardising Monitoring and Reporting ............................................................................ 26 Capacity Development for NIS within the Health Workforce .......................................................................... 29

ii
Strengthening Reporting through the DHIS-2 and Mobile Applications .......................................................... 31
4. MAXIMISING DATA VALUE: OPPORTUNITIES FOR TRANSFORMING THE NUTRITION DATA ANALYSIS AND USE................................................................................................................. 34
4.1 Overview & Current Situation and Key Challenges ................................................................... 34
4.2 Current Analysis of Programme Data to Guide Decision-Making ........................................... 34 4.2.1 Facility and Community Level (Recommendation 2.6) ........................................................................... 34 4.2.2 District and Governorate Level Analysis and Use of Data (Recommendations 2.3 – 2.5) ...................... 35 4.2.3 National level Analysis and Use of Data (Recommendations 2.3 – 2.5) ................................................. 36
4.3 Opportunities for Expanded Use of NIS Programme Data for Improved Programme Coverage and Quality ......................................................................................................................... 38
4.3.1 Current Analysis of CMAM and Related Nutrition Data (Recommendations 2.3 – 2.5) ......................... 38 4.3.2 Factors Influencing Interpretation of Programme Data in Yemen (Recommendations 2.2 – 2.6) ......... 39 4.3.4 Using Acute Malnutrition Admissions data to Determine Effective Programme Functioning and the Impact of COVID-19 (Recommendations 2.2 – 2.5) ......................................................................................... 40 4.3.5 Monitoring how the Number of Programmes Impacts Programme Performance and Reporting (Recommendations 2.2 – 2.6) .......................................................................................................................... 40
4.4 Recommendations for Maximising Data Value: Opportunities for Transforming the Analysis and Use of Nutrition Data ................................................................................................................... 41
Defining and Expanding the Analysis and Use of NIS Data in Yemen .............................................................. 41 Facilitating Real-Time Analysis Clearly Linked to Actions for Improving Programme Performance ................ 43 Routine Analysis of Data at the Sub-national Level to Increase Programme Effectiveness and Coverage ..... 44 Increasing Data Analysis and Use at Health Facility Level ............................................................................... 45
5. CONCLUDING REMARKS............................................................................................................... 47
ANNEX 1: STAKEHOLDERS FOR KEY INFORMANT INTERVIEWS ............................................... 48
ANNEX 2: AGENDA OF CONSULTATIVE MEETING FEBRUARY 16-17, 20201 ............................. 56
ANNEX 3: TECHNICAL CONSULTATIONS POWERPOINTS & LINKS TO SESSIONS .................. 58
ANNEX 4: KEY NUTRITION-SPECIFIC INTERVENTIONS IN YEMEN ............................................. 59
ANNEX 5: EXISTING TRAININGS ....................................................................................................... 61
ANNEX 6: YEMEN NUTRITION DATA COLLECTION FORMS AND COLLECTION DETAILS ....... 63
ANNEX 7: INDICATOR REFERENCE GUIDE INDICATOR REFERENCE SHEET EXAMPLE ........ 67
ANNEX 8: STAKEHOLDERS (BY LEVEL) MANAGEMENT OF NUTRITION DATA COLLECTION AND REPORTING ...................................................................................................................... 69
ANNEX 9: PROPOSED DRAFT SUB-NATIONAL SCORECARD INDICATORS .............................. 70
ANNEX 10: LEVEL OF HEALTHCARE, TYPE OF HEALTH FACILITIES, CATCHMENT AREA, STAFFING AND NUTRITION SERVICES OFFERED ............................................................... 71

iii

iv
Tables Table 1: Overview of Main Data Sources of Information for Nutrition................................................... 10 Table 2: Immediate Recommendations (immediate-1 year) ................................................................. 25 Table 3: Immediate Recommendations (immediate-1 year) ................................................................. 26 Table 4:Short-Term Recommendations (1-2 years) ............................................................................. 26 Table 5: Longer-Term Recommendations (1-3 years) .......................................................................... 27 Table 6: Immediate Recommendations (Immediate-1 year) ................................................................. 29 Table 7: Short-Term Recommendations (Immediate-1 year) ............................................................... 30 Table 8: Longer-Term Recommendations (1-3 years) .......................................................................... 31 Table 9: Immediate Recommendations (Immediate-1 year) ................................................................. 32 Table 10: Immediate Recommendations (Immediate-1 year) ............................................................... 32 Table 11: Immediate Recommendations (Immediate-1 year) ............................................................... 41 Table 12: Immediate Recommendations (Immediate-1 year) ............................................................... 43 Table 13: Immediate Recommendations (Immediate-1 year) ............................................................... 44 Table 14: Long-Term Recommendations (1-3 years) ........................................................................... 45 Table 15: List of Stakeholders Consulted for Key Informant Interviews (KIIs) (Updated April, 29th, 2021) ..................................................................................................................................................... 48 Table 16: Training Cadres for Nutrition ................................................................................................. 61 Table 17: Existing Training.................................................................................................................... 62 Table 18: Yemen Nutrition Data Collection Forms and Collection Details .......................................... 64 Table 19: Stakeholders (by Level) Management of Nutrition Data Collection and Reporting .............. 69 Table 20: Yemen Proposed Draft Sub-National Scorecard Indicators ................................................. 70 Table 21: Level of Healthcare, Type of Health Facilities, Catchment Area, Staffing and Nutrition Services Offered ................................................................................................................................... 71 Figures Figure 1: Yemen Nutrition Information Systems Review & Recommendations Process ....................... 8 Figure 2: Community Management of Acute Malnutrition (CMAM) Health Facility Sites Data Flows and Data Collection Forms ........................................................................................................................... 13 Figure 3: Infant and Young Child Feeding (IYCF) Data Flows and Data Collection Forms ................. 14 Figure 5: Integrated Nutrition Outreach Services Data Flows and Data Collection Forms................... 14 Figure 6: Health and Nutrition Mobile Teams Reporting Template and Nutrition Capacity Building Field Information Report ................................................................................................................................ 15 Figure 7: Community Health and Nutrition Volunteer (CHNV) Management Data Flows and Data Collection Forms ................................................................................................................................... 15 Figure 8: Data Collection: Reporting & Data Cleaning ......................................................................... 17 Figure 9: The Nutrition Data Value Chain ............................................................................................. 21 Figure 10: Data Assessment/Collection, Analysis, and Use for Decision-Making (Action) .................. 22 Figure 11: Nutrition-Specific Interventions in Yemen ............................................................................ 59 Figure 12: Community Management of Acute Malnutrition (CMAM) components, and main service delivery entry points .............................................................................................................................. 60
v
Acronyms
ACF Action contre la Faim (Action Against Hunger)
AM Acute Malnutrition
BSFP Blanket Supplementary Feeding Programme
CFSS Comprehensive Food Security Survey
CHV Community Health Volunteer
CHNV Community Health and Nutrition Volunteers (CHNVs) (previously Community Health Volunteers (CHV)
CMAM Community Management of Acute Malnutrition
CRF Common Results Framework
CSO Central Statistics Office
CSO Civil Society Organisation
DAI Development Associates International
DG-ECHO Directorate General for European Civil Protection and Humanitarian Aid Operations. (previously European Commission Humanitarian Office)
DHO District Health Office & District Health Officer
DHS Demographic and Health Surveys
DHIS2 District Health Information System
EBF Exclusive Breastfeeding
EPI Expanded Programme of Immunization
e-IYCF Emergency Infant and Young Child Feeding
eDEWS Electronic Disease Early Warning System
eIDEWS Electronic Integrated Disease Early Warning and Response System
EU European Union
FAO Food and Agriculture Organization of the United Nations
FCDO Foreign, Commonwealth & Development Office (United Kingdom)
FEWSNET Famine Early Warning Systems Network
FSLA Food Security and Livelihoods Assessment
GAM Global Acute Malnutrition
GHO Governorate Health Office & Governorate Health Officer
GMP Growth Monitoring and Promotion
HCs Health Centres
HF Health Facility
HMIS Health Management Information System
HNO Humanitarian Needs Overview
HRP Humanitarian Response Plan
HUs Health Units
IFA Iron Folic Acid
IM/IS Information Management/Information Systems
IMCI Integrated Management of Childhood Illness
IMO Information Management Officers
vi
INGO International Non-Governmental Organisations
IP Implementing Partner
IPC Integrated Food Security Phase Classification
IPC AMN Integrated Food Security Phase Classification Acute Malnutrition
IPG Implementing Partners Group
IYCF Infant and Young Child Feeding
IYCF-C Infant and Young Child Feeding Corners
JMP WHO/UNICEF Joint Monitoring Program for Water Supply and Sanitation (JMP) standards
KII Key Informant Interviews
M & M Monitoring and mentoring
MAM Moderate Acute Malnutrition
MEAL Monitoring, Evaluation, Accountability and Learning
M&E Monitoring and Evaluation
MICS Multiple Indicator Cluster Survey
MIYCN Maternal and Infant Young Child Nutrition
MNP Micronutrient Powder
MOPHP Ministry of Public Health and Population
MoPIC Ministry of Planning and International Cooperation
MTs Mobile Teams
MSNAP Multisectoral Nutrition Action Plan (Yemen)
MUAC Mid Upper Arm Circumference
NC Nutrition Cluster
NCC Nutrition Cluster Coordinator
NIS Nutrition Information System
NITWG Nutrition Information Technical Working Group
NGO Non-governmental Organisation
NSS National Surveillance System
OCHA Office for the Coordination of Humanitarian Affairs (United Nations)
ODA Overseas Development Assistance
ORS Oral Rehydration Salts
ORT Oral Rehydration Therapy
OTP Outpatient Therapeutic Programme (now referred to as ‘outpatient’)
PBS Population-Based Surveys
PHC Primary Health Care
PIN People in Need
PLW Pregnant and Lactating Women
PNC Postnatal Care
SAM Severe Acute Malnutrition
SC Stabilization Centres
SD Standard Deviation

vii
SDG Sustainable Development Goal
SFP Supplementary Feeding Programme
SMART Standardized Monitoring and Assessment of Relief and Transitions
SO Strategic Objective
SQUEAC Semi-Quantitative Evaluation of Access and Coverage
SUN Scaling Up Nutrition (Movement)
TASC Technical Assistance to Strengthen Capabilities
TEAM UNICEF/WHO Technical and Expert Advisory Group on Nutrition Monitoring
TFC Therapeutic Feeding Centre (inpatient)
TWG Technical Working Group
TSFP Targeted Supplementary Feeding Programme
UN United Nations
UNICEF United Nations Children’s Fund
UNOCHA United Nations Office for the Coordination of Humanitarian Affairs
USAID United States Agency for International Development
USD United States Dollar
VitA Vitamin A
WASH Water, Sanitation and Hygiene
WFP World Food Programme
WH Weight-for-Height
WHA World Health Assembly
WHO World Health Organization
WRA Women of Reproductive Age
WHZ Weight-for-Height Z score
YHC Yemen Health Cluster
YHNO Yemen Humanitarian Needs Overview
YCFSS Yemen Comprehensive Food Security Survey
YDHS Yemen Demographic Health Survey
YNC Yemen Nutrition Cluster

1
Executive Summary
Scope of Work
TASC was requested to review the Nutrition Information and Analysis Systems (NIS) including indicators, data collection, analysis and use in Yemen through a situational analysis exercise. The assignment aimed to systematically identify factors which affect the collection, analysis, dissemination, and utilization of timely, accurate and representative nutrition information in Yemen, through in-depth consultation with relevant stakeholders and an additional desk-based scoping review. The results of this exercise are intended to help stakeholders to clearly define a set of sequential actions (immediate, short-term and long-term) to address key challenges and barriers in the NIS to help improve the overall availability, quality, analysis and utilization of data.
Nutrition Programming in Yemen
The size of the nutrition response in Yemen has increased every year since 2016 up until 2019, with preliminary data from the United Nations Office for the Coordination of Humanitarian Affairs (UNOCHA) Financial Tracking Service showing a decline in funding in 2020. By the end of January 2021, UN OCHA reported that USD$1.9 billion, 56 percent of the $3.38 billion needed for the overall 2020 Humanitarian Response Plan, had been committed by international donors.1 Nonetheless, the humanitarian response in Yemen remains the largest humanitarian response globally in history. The Nutrition Cluster in Yemen is led by the United Nation Children’s Fund (UNICEF) and co-chaired by the Ministry of Public Health and Population (MOPHP). As of October 2020, there were 42 active Nutrition Cluster implementing partners including 17 national non-governmental organizations (NGOs), 20 international NGOs, four United Nations (UN) agencies and one government agency.2
A major component of nutrition programming in Yemen is Community Management of Acute Malnutrition (CMAM) which is administered at the health facility level with some community outreach and mobile services. CMAM includes: the management of moderate acute malnutrition (MAM) through both an outpatient targeted supplementary feeding program (TSFP), the management of severe acute malnutrition (SAM) without complications through outpatient therapeutic treatment programme (OTP) services and the management of SAM with complications through an inpatient Therapeutic Feeding Centre (TFC) Program also referred to as ‘stabilization centres (SC)’ in hospitals. and some health centres and through community mobilization via the community Health and Nutrition Volunteers. In addition, there are Infant and young child feeding (IYCF) corners, counselling services and breastfeeding support available at some health facilities, as well as nutrition preventive services including the Blanket Supplementary Feeding Programme (BSFP), and micronutrient interventions, including micronutrient supplementation services-such as Iron Folic Acid (IFA) supplementation for pregnant women, Vitamin A supplementation and micronutrient powders (MNP) supplementation.
Overview of the Main Sources of Nutrition Information
The nutrition information system in Yemen comprises a range of data sources, including periodic Population Based Surveys (PBS), periodic nutrition assessments, routine nutrition programme monitoring data from health facilities and mobile service delivery teams, and data generated through nutrition programmes within health facilities and villages. Data are collected and managed by a combination of MOPHP staff, UN Agencies, and NGOs (both local and international). In addition, there is third-party monitoring for nutrition programming that is managed by several UN agencies, where contracted companies provide a range of monitoring services on humanitarian and development projects and programmes across Yemen. Most of the nutrition data comes from the CMAM programme sites located at primary health care (PHC) units (fixed health units and temporary health units), PHC health centres, district hospitals, general governorate hospitals, and specialist referral hospitals. Attached to the PHC units are Community Based Health Services including the newly recognised community health and nutrition-based volunteers (CHNVs). There are a number of paper-based data collection forms, including daily registers, monthly reports, and referral forms that are also filled out by health workers and CHNVs at the health facility and community level that feed into the data bases. In
1 UNOCHA. Financial Tracking Service https://reliefweb.int/sites/reliefweb.int/files/resources . 2 “Yemen: Nutrition Cluster, Partners Operational Presence (Jan-October 2020).” Yemen Nutrition Cluster. https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/4w_yemen_nc_operational_presence_jan-oct2020.pdf (accessed January 3, 2021).

2
addition, there is compiled data by the Yemen Nutrition Cluster that is maintained and reported on monthly.
Population based surveys and assessments play a vital role within the NIS. The people in need estimates in the integrated phase classification (IPC) analysis and caseload calculations for Nutrition Cluster programming use the results of SMART assessments, either upper confidence interval or point prevalence of previous survey estimates of acute malnutrition.
The District Health Information System (DHIS)-2 is currently being piloted in Yemen and is in the ‘system preparation phase’ with the nutrition module under development. The MOPHP, with support of the UNICEF,are working on piloting a nutrition DHIS-2 module that is planned to be implemented at scale to record key facilities-based data. Existing health records and tools are being reviewed to see what nutritional data should be included.
Key Findings and Recommendations
In response to the severe humanitarian crisis in Yemen, there has been a vast scaling-up of the nutrition response in Yemen in recent years. A range of stakeholders deliver nutrition services in the country, including direct service provision by the MOPHP, UN agencies (including UNICEF, WHO, FAO and WFP) and national and international NGOs. A range of information is produced on nutrition conditions and nutrition programme results.
The set of recommendations outlined in sections below and in sections three and four of this report describe a set of sequential and related steps to address identified issues within the NIS to further strengthen the system for better programme coverage and performance and ultimately improved nutrition and health outcomes for the people of Yemen. Individual organisational stakeholders are proposed alongside each recommendation as being most suitable for holding accountability to oversee their implementation. Developing a workplan to delineate roles and responsibilities in more detail and within a more detailed timeframe is beyond the scope of this report. This process needs to be led by stakeholders in country through an appropriate platform. The Nutrition Information Technical Working Group in Yemen is suggested as the most appropriate platform for development of such a workplan.
National Nutrition Monitoring and Evaluation Accountability Framework
The set of recommendations outlined in this report need to be situated within an overall Framework for Monitoring and Evaluation through the NIS in Yemen as recommendations are inter-related and should be acted upon and followed up and monitored together with clearly designated roles, responsibility and accountabilities.
Such a framework does not necessarily need new targets and does not need to be overly complicated. It can use the existing national targets that the nutrition stakeholders already use. Instead, it would act as a tool to formalize and document roles and responsibilities and clearly define how and when and who will be prioritizing, collecting analysing and acting upon information within the country.
The following recommendations can thus be thought of as suggested elements of this framework, covering roles and responsibilities for developing human resources and capacity development, and documenting a set of agreed harmonized indicators and available standardized reporting and monitoring tools.
Recommendations
No. Timeframe Recommendation
1.1 0-1 year Develop a National Nutrition Monitoring and Evaluation Accountability Framework (including clearly defined Nutrition Reporting Roles and Responsibilities).
Harmonizing and Standardising Monitoring and Reporting
With the rapid scale up of nutrition programming in recent years, the number and type of nutrition indicators collected, and the variety of forms and reporting procedures used by stakeholders involved in nutrition programming have also increased. There is a need for harmonisation and standardisation of indicators, data collection forms, and agreed-upon standard operating and reporting procedures.

3
Recommendations:
No. Timeframe Recommendation
1.2 0-1 year Finalize Sub-National Nutrition Scorecard Set of Key Performance Indicators (KPI), Thresholds and Review Process
1.3 1-2 years Facilitate Harmonization of Indicators and Data Collection Forms
1.4 2-3 years Develop a National Nutrition Indicator Reference Guide
Capacity Development for NIS within the Health Workforce
The production of nutrition information, especially nutrition programme information, is heavily reliant upon the workforce within health facilities and communities, along with district and governorate health offices (DHO and GHO) which are facing severe human, physical and financial resource constraints.
While there are a number of regular trainings for health workers and CHNVs, none of these contain a monitoring and reporting component. Refresher training for MOPHP monitoring and evaluation focal persons for nutrition at the district and governorate level takes place on an annual basis only.
DHOs and GHOs play a key role in the NIS in Yemen acting as the first administrative point of contact that health facilities report to within the health system. Trainings for DHO and GHO staff are on an annual basis. It is not clear what impact trainings have as there is no clear system of tracking quality and completeness of reporting before and after trainings take place. The set of criteria provided for DHO and GHO for assessing data quality could be more clearly defined by Information Management Officers (IMOs) at the zonal and national level in the Nutrition Cluster, and mechanisms are lacking which can systematically identify where there are data quality issues and trigger support through increased capacity building or other efforts.
At both the national and the sub-national levels, we recommend a rapid human resource assessment that informs the standardisation and strengthening of available training for health workers and monitoring and evaluation focal persons for nutrition (including IMOs) throughout the nutrition data value chain.
It will be useful to monitor the quality and completeness of reporting both before and after capacity building exercises. Ideally, the impact of capacity building would be tracked across all governorates and districts where trainings take place, but if that is not feasible, a subsection could be identified, e.g., on the issues with reporting and the completeness and quality of reporting. These actions can support the MOPHP alongside a longer term set of actions to increase the available human, physical and financial resources targeted to Monitoring and Evaluation for Nutrition.
Recommendations:
No. Timeframe Recommendation
1.5 0-1 year Conduct a Rapid Human/Infrastructure Capacity Assessment for Data Management to Inform Trainings/Capacity Development Strategy.
1.6 0-1 year Introduce Regular Quality Improvement Teams at Governorate and District Level Data Review Meetings to Review Progress Against Targets for KPIs in Scorecards and Feedback Mechanisms
1.7 1-2 years Introduce routine monitoring and reporting on the effectiveness of capacity building/ training exercises with GHO, DHO and facility/programme staff utilizing available data from nutrition programme databases.
1.8 1-2 years Implement Training in Monitoring and Reporting for Nutrition across cadre of the health workforce.
1.9 2-3 years Strengthen the Monitoring and Evaluation Department within Nutrition Department of MOPHP

4
Strengthening Reporting through the DHIS-2 and Mobile Applications
In the medium to longer term, the development and roll out the DHIS-2 in Yemen presents an important effort for more systematic collection, management and analysis of nutrition information in the country. However, this review found that development of the system is not visible or well understood by many nutrition stakeholders inside and outside of the country, including key donor agencies and some UN agency staff. How nutrition will be incorporated within the DHIS-2 and what proportion of nutrition programming data will be migrated to the system is also not yet well defined.
In the shorter term, further formalising the use and analysis of messaging services for communication from the facility and district levels upwards could increase accountability and help identify and address recurrent issues, especially related to availability of stock, human resources, and reporting.
Recommendations
No. Timeframe Recommendation
1.10 0-1 year Increase and further systemize use of Mobile Technologies to improve feedback and real time analysis of information from primary health care facilities
1.11 0-1 year Develop and disseminate a clear plan for to further Define How Nutrition will be Integrated with the District Health Information Systems (DHIS-2) and Increase Awareness and Engagement from Nutrition Stakeholders.
Analysis and Use of Available Data
Mainstreaming nutrition data into information systems is not only about improving the quality, availability, and accessibility of data, but also requires building capacity and transforming information into input for sound decision-making.
There also is a lack of a clearly defined set of actions that should be taken in response to observed data trends, or to flag a need for action when thresholds are surpassed. There is limited routine analysis of trends in nutrition programme data at governorate and district levels, which could assist in interpretation of trends in acute malnutrition admissions and discharge patterns, health facility reporting performance, and trends in the availability of services and the supply chain on nutrition commodities. This lack of real-time nutrition programme data analysis slows the decision-making process on course corrections to improve the quality and effectiveness of nutrition services.
Defining and Expanding the Purpose of Analysis of NIS Data in Yemen At present, the focus of the nutrition information and analysis products produced by the Nutrition Cluster
in Yemen tends to be more focused on use of data for implementing partner accountability and
monitoring of outputs produced rather than for direct programmatic use. Further targeted analysis of
available data could be used to improve the programme effectiveness and coverage.
There is also a lack of a clear strategy for communicating analysis of data to different stakeholders in a form tailored to their specific needs in a routine and timely manner. There is a need for nutrition stakeholders to come together to collectively agree upon and articulate a strategy for data use and communication, outlining the needs of stakeholders across the data value chain, what data they currently use in their roles and how more in-depth analysis and routine analysis and dissemination can help them increase programme coverage and quality. Given the current constraints in human resources for nutrition information systems, it will be important, specifically for the Nutrition Cluster and UNICEF, to foremost mobilize human resources at the national level to commit to subsequent actions.

5
Recommendations:
No. Timeframe Recommendation
2.1 0-1 year Develop a data use and communication strategy through the Nutrition Information Technical Working Group.
2.2 0-1 year Introduce additional human resources dedicated to undertaking and coordinating analysis and facilitating use data in decision making.
Joint Nutrition Data Repository and Dashboard
The mechanisms in place to provide stakeholders who produce and use data across the data value chain, with feedback and analysis on the data they produce (e.g., at facility, district or governorate level) are not well defined across contexts in Yemen. For instance, no routine or systematized analysis is produced for use by MOPHP staff or NGOs at the Governorate, or District levels.
There is a lack of routine analysis of trends in programme data by Governorate or District provided to zonal Clusters, GHO or DHO which could help them understand trends over time or between indicators, or to compare trends to other districts or governorates. The lack of routine subnational analysis limits the scope for triangulation of indicators such as admissions, screening data, stock use, and number and location of programmes for identification of programming bottlenecks. Instead, it is up to the discretion and capacity of the GHO or relevant other Nutrition Cluster staff to identify this, act upon it and follow up.
To address this, it is recommended to develop a joint data repository reflecting the breadth of available data generated through nutrition programmes in the country. This would facilitate the development of a nutrition data dashboard capable of generating real-time information products for analysis and feedback with sub-national staff and producers of data and can feed into a scorecard system to track progress at the sub-national levels.
Data generated through such a data repository dashboard can also provide vital outputs to inform feedback and information to those generating and using nutrition information throughout the nutrition data value chain and inform subnational scorecards to track progress on key indicators. At the national (central) level, a web-based data dashboard including indicator registry to facilitate access to information on agreed upon Yemen indicators can help to reduce duplication and misalignment of reporting procedures. The overview of nutrition data collection forms and collection details outlined in Table 9 of this report can provide a starting point for this process.
Recommendation:
No. Timeframe Recommendation
2.3 0-1 year Develop a National Data Repository linked to Joint Dashboard to facilitate increased analysis and feedback at the Governorate and District levels
Use of Routine Data Sub-National Level to Increase Effectiveness and Coverage
The nutrition programme data collated through the proposed dashboard needs to be positioned within a wider analytic process, using indicator tracking against set thresholds and targets as defined in the proposed subnational scorecard system.
Routinely producing an analysis of admissions data alongside reporting, screening and number of active programmes and triangulated with other information such as reports of increased food insecurity, insecurity or natural disasters or disease outbreak could provide a deeper understanding of programme performance and drivers of service utilization, as well as programme performance in community mobilisation and coverage. Such an analysis should be linked from its inception and design to how it can inform decision-making, drawing upon other NIS sources such as estimates from PBS, health facility nutrition monitoring, and data from other clusters and sectors to provide a wider picture of drivers to ensure early action is taken in response to discerned trends.
Such a system of analysis could be used within national and zonal Nutrition Cluster meetings, Nutrition Information Technical Working group meetings and more broadly. In order to link analysis to

6
decision making, an integral part of each analysis would be reporting on what actions were taken upon the previous analysis findings, for instance, through systematically identifying and flagging for follow up issues such as stock outs, low or decreasing screening numbers, large, continuous or cyclical changes in admissions, or programme outcome indicators.
Recommendation:
No. Timeframe Recommendation
2.4 0-1 year
Routine and Systematic Analysis of Available Nutrition Data to inform Nutrition Cluster Strategy: Implement, disseminate, and monitor use of routine and systematic analysis of available nutrition data to inform Nutrition Cluster strategy.
Health Facility Level Data Use and Analysis
While there are standard trainings in place for CHNVs and facility-based health workers (as described in section 2.4 ‘Existing Training’), there are no existing instances of facility-level approaches to encourage analysis and use of data at the facility level, such as the CMAM surge approach3 or District Health System Strengthening approaches.
Several key informant interviews (KIIs) and participants within consultative meetings stressed that there is a need for more engagement and training for health facility workers and CHNVs to facilitate responsive nutrition programming that feeds back into the higher levels (e.g., district, governorate, central). There was broad consensus among KII that there is room for further mobilization and leveraging of health facility level data and knowledge to increase rapid screening and referral to programmes and identify and address limiting factors in service utilization.
Recommendation:
No. Timeframe Recommendation
2.5
2-3 years Integrate Facility and Community-Based Approaches to Increase Qualitative Analysis of Nutrition Information
3 The CMAM Surge approach complements routine CMAM services by improving health staffs' use of facility data and knowledge of the local context to better anticipate, plan for, respond to, and bounce back from these increases in demand for acute malnutrition treatment services.

7
1. Introduction
1.1 Background Context
Before the beginning of the current crisis in 2015, Yemen had not been a major recipient of overseas development assistance (ODA). In 2006 ODA accounted for just 1.2% of GNI. Between 1995 and 2009 only 5% of ODA to the country was in the form of humanitarian assistance.4 Domestic funding for health and nutrition programming was limited.5 Between 2016 and 2019, the total budget for the nutrition response in Yemen increased year on year, with preliminary data showing funding levels were declining in 2020.6 By the end of January 2021, only US$ 1.9 billion was committed by donors, amounting to 56 percent of the $3.38 billion needed for the 2020 Humanitarian Response Plan. 7 Nonetheless, the humanitarian response in Yemen remains the largest humanitarian response in history.
As part of public sector governance reforms introduced in 2001, much of the responsibility for executing health budgets shifted to governorates and local government authorities, particularly for recurrent spending.8 A lack of clearly defined responsibilities at the central and local levels, unclear administrative responsibilities between health offices and local councils led to interference from many parties in the leadership of health districts.9 This combined with a lack of adequate financial tracking contributed to widespread reports of budget shortfalls, misallocation of funds and reduced funding availability for health services at district, and facility levels.10 Out of pocket expenditure increased substantially from 43% in 2000 to 81% in 2015.11
Until 2001, the global emergency response to severe acute malnutrition was predominantly through Therapeutic Feeding Centres (TFCs) in hospital settings. In Yemen, the first SAM management protocol was developed in 2005. In order to improve coverage and impact, Yemen began implementing emergency nutrition interventions through Community-based Therapeutic Care (CTC) from 2008 onwards. Treatment programmes were funded under area specific projects with the support of various international organisations including the United Nations Children’s Fund (UNICEF) and the World Bank.12 In 2013,MOPHP introduced the national community management of acute malnutrition (CMAM) guidelines, which were revised in 2017.13 Nutrition and health education including breastfeeding child feeding support, Vitamin A supplementation and deworming along with other basic maternal and child health services were delivered through the country’s Community Health Volunteer programme guided by the National Guidelines for Community Volunteer Programme adopted in 2011.14 The Community Health and Nutrition Volunteers (CHNVs) actively screen and identify children with acute malnutrition and use a referral slip to refer them to a specific CMAM service and site. They follow-up admitted children that are absent, defaulted or as determined by the health worker. They provide feedback to the health facilities on problems related to the children’s home environment. CHNVs also promote appropriate health, nutrition (including infant and young child feeding practices (IYCF) and hygiene practices through key messages. The government established the Yemen Nutrition Cluster in 2009. The Nutrition Cluster is led by UNICEF and co-chaired by the MOPHP. The Nutrition Cluster currently coordinates MOPHP and NGO partner programmes in over 4,000 health facilities, over 3,600 blanket and supplementary feeding programme (BSFP) distribution points and through mobile teams nationally.
4 OECD. OECD DAC Data: Yemen. http://www.oecd.org/countries/yemen/ Published 2018. Accessed January 2, 2020 5 Government of Yemen. Ministry of Planning and Development. National Health Strategy. 2010-2025.; 2010 6 UNOCHA. Financial Tracking Service https://reliefweb.int/sites/reliefweb.int/files/resources. 7 Relief Web. “Yemen Humanitarian Response Plan Extension, June - December 2020 [EN/AR] - Yemen.” Accessed November 3, 2020. https://reliefweb.int/report/yemen/yemen-humanitarian-response-plan-extension-june-december-2020-enar. 8 Elgazzar, Heba. “Raising Returns: The Distribution of Health Financing and Outcomes in Yemen,” February 2011. http://documents1.worldbank.org/curated/en/904741468334310999/pdf/596160WP01publ1omesinYemen01PUBLIC1.pdf. 9 WHO. Assessing the regulation of the private health sector in the Eastern Mediterranean Region: Egypt. 2014. https://apps.who.int/iris/bitstream/handle/10665/250541/EMROPUB_2014_EN_1757.pdf?sequence=1&isAllowed=y 10 Elgazzar HA. Raising returns: The distribution of health financing and outcomes in Yemen. 2011. https://openknowledge.worldbank.org/bitstream/handle/10986/13595/596160WP01publ1omesinYemen01PUBLIC1.pdf?sequence=1 11 WHO. Out-of-pocket expenditure (% of current health expenditure). https://data.worldbank.org/indicator/SH.XPD.OOPC.CH.ZS Published 2020. Accessed October 27, 2020. 12 World Bank. Project Appraisal for a Health and Population Project.; 2010. http://documents1.worldbank.org/curated/en/283341468340753068/text/537660PAD0Revi1rd10IDA1R20111001011.txt 13 Al-Dheeb N, et al. Experiences of Implementing CMAM in Yemen and Number of Deaths Averted. Emerg Nutr Netw. 2018. 14 Wright J. Essential Health Services: Yemen. Essential Health Services Snapshots Series. 2015. Washington DC; 2015. https://www.hfgproject.org/essential-package-of-health-services-country-snapshot-yemen/

8
The institutional and operational characteristics of nutrition programming is explored in more depth throughout relevant sections of this report.15
1.2 Scope of Work Objectives and Methodology
The objectives guiding this work was threefold: 1) to conduct an overall review of the current situation and state of nutrition information systems and data collection/management in Yemen; 2) to hold a consultative meeting led by the MOPHP along with UNICEF/Yemen in order to learn about the current state of nutrition information systems in Yemen as well as the use of nutrition information products and discuss successes, challenges and gaps; and finally: 3) to hold a series of follow-up technical consultations for identification of key immediate (immediate-to one year), short-term (1-2 years), and medium-term actions (2-3 years).
The process is outlined in Figure 1. The consultant team conducted a key document16 review, then conducted more than 38 key informant interviews (KIIs) with more than 70 participants (See Annex 1 for a list of KII). The key findings were presented in a draft scoping report, the contents of which were presented and discussed during a consultative meeting February 16-17, 2021 with over 58 participants in-country and 63 participants online over the course of the two-day meeting (see Annex 2 for the meeting agenda). Following this meeting we had three focused technical consultations: 1st meeting) March 8, 2021: ‘Capacity building & training in monitoring and reporting for nutrition’, 2nd meeting) March 17, 2021: ‘Streamlining and harmonization of national nutrition data collection forms, indicators & reporting mechanisms’ and 3rd meeting) March 22, 2021: ‘Improving nutrition data quality, use and analysis & real-time data including through digitalization/information system’. Technical Consultation Presentations can be found in Annex 3 of this report. This report presents the key results from the literature review, the KIIs, the consultative meeting, and the three follow-up technical consultations.
Figure 1: Yemen Nutrition Information Systems Review & Recommendations Process
Source: Authors of this report, 2021.
15 UNOCHA Yemen Humanitarian Response Plan. 2021. https://reliefweb.int/sites/reliefweb.int/files/resources/Final_Yemen_HRP_2021.pdf

9
1.3 Key Limitations
This technical review of nutrition information systems in Yemen has several important limitations. The review was based on a document review, key informant interviews and group technical consultations.
▪ Due to the ongoing civil conflict in Yemen and the impacts of the COVID-19 pandemic on travel globally, the authors were unable to travel to Yemen for field work. As such, all primary data collection through KII’s and technical workshops was online virtually vis-a-via Zoom, skype, email and other online communication.
▪ The lack of face-to-face communication and observation of the nutrition information system “in the field” has implications for the breadth and depth of the report and the authors ability to accurately reflect all aspects of the situation on the ground in country.
▪ While the authors engaged stakeholders at both the national and sub-national levels to contribute to the review, engaging stakeholders at the health facility and district levels was challenging, and the lack of KII or observation at these levels constitutes an important limitation to this work.
▪ KII interviews were sought with a wide range of stakeholders both within and outside of the country. The contribution from KII’s was backed up by triangulation with other KII and document review. However, some of the review findings are based upon the sometimes-subjective viewpoints and opinions of KII. As such, it should be noted that the review may represent some viewpoints over other possible interpretations among stakeholders in the country.
▪ The scale of the humanitarian response in Yemen is unprecedented. Reflecting the points of view and processes of all actors and actions part of the humanitarian nutrition response in the country was not feasible given the time and resources available for this review.

10
2. Overview of Current Nutrition Information Systems in Yemen
2.1 Data Sources, Service Delivery Entry Points, and Data Users
As of December 2020, per district in Yemen, there are between zero to 48 active health facilities with CMAM services, with median number of nine per District.17 The primary service delivery entry point for nutrition-specific programming in the health sector in Yemen is through Community Management of Acute Malnutrition (CMAM) Sites (Figure 5) for the following services:
1) Primary Health Care (PHC) Unit (fixed site)
2) Primary Health Care Unit (Temporary health unit site)
3) Primary Health Care Centre
4) Governorate/District /Authority or Referral Hospitals
5) Primary Health Care Extension Services ▪ Mobile Health & Nutrition Services ▪ Nutrition Integrated Outreach Services ▪ Community Outreach through Community Health and Nutrition Volunteers (CHNVs) ▪ Community-Based Distribution points for BSFP
See Table 1 for a summary of the main nutrition data sources, service delivery entry points and the users of the data.
Table 1: Overview of Main Data Sources of Information for Nutrition
Data Sources
Service Delivery Entry Points
Data Users
Health Facility-Based Data
Sources (Routine)
Community Management of Acute Malnutrition
(CMAM) database-for both treatment of SAM and
MAM (Access and Excel)
▪ PHC units ▪ PHC Centres ▪ PHC Community Supported
Shared Temporary Health Unit ▪ Outreach-Mobile Health Services ▪ District Hospital ▪ Governorate Hospital ▪ Specialized
Care/Teaching/Referral Hospitals
▪ MOPHP ▪ Implementing
partners ▪ GHO-N ▪ DHO-N
The new Inpatient Therapeutic Feeding
Centres (TFC) database (piloting with ASP.net
with Excel sheet reporting)
▪ District Hospital ▪ Governorate Hospital ▪ Specialized
Care/Teaching/Referral Hospitals
▪ MOPHP ▪ WHO
Infant and Young Child Feeding (IYCF)
Corners monthly report database (Excel)
▪ PHC units ▪ PHC Centres ▪ Outreach-Mobile Health Services ▪ Community outreach ▪ District Hospital ▪ Governorate Hospital ▪ Specialized
Care/Teaching/Referral Hospitals
▪ MOPHP ▪ Implementing
partners ▪ GHO-N ▪ DHO-N ▪ Health workers
Community Health and Nutrition (CHNV)
monthly database (Excel)
▪ PHC units ▪ PHC Centres ▪ Community outreach ▪ Community-Based Health and
Nutrition Volunteers (female health worker is called Murshada)
▪ Expanded programme for immunization (EPI) campaigns
▪ Mass nutritional screening programmes
▪ MOPHP ▪ Implementing
partners (forthcoming)
▪ GHO-N ▪ DHO-N ▪ Health workers
Community-Based Health & Nutrition Mobile
teams Reporting Template (Excel)
▪ PHC Outreach-Mobile Health Services
▪ MOPHP ▪ Implementing
partners ▪ GHO-N ▪ DHO-N ▪ Health workers
Nutrition Outreach Database for Governorate
Health Offices (Excel)
▪ Governorate Health Offices ▪ MOPHP ▪ GHO-N
17 Yemen Nutrition Cluster. Monthly Summary Database. January to December 2020. https://www.humanitarianresponse.info/en/document/nutrition-cluster-monthly-update-december-2020

11
Table 1: Overview of Main Data Sources of Information for Nutrition
Data Sources
Service Delivery Entry Points
Data Users
Nutrition Surveillance System (NSS) ▪ WHO/MOPHP Nutrition
Surveillance Sites ▪ MOPHP ▪ WHO ▪ Health workers
Nutrition Cluster Source Compiled Data
▪ Nutrition Cluster Caseload Calculations &
Targets
▪ Nutrition Cluster Assessments Summary
▪ Nutrition Cluster Monthly Summary Analysis
▪ Nutrition Cluster 4 W’s matrix (Who Does What, When and where)
▪ MOPHP ▪ Implementing partners
▪ MOPHP ▪ Implementing
partners
Population Based Surveys
(PBS) (Periodic)
▪ Comprehensive Food Security Survey (CFSS)
▪ Multiple Indicator Cluster Survey (MICS) ▪ Yemen Demographic Health Survey (YDHS) ▪ Yemen Comprehensive Food Security
Survey (CFSS)
▪ Population and site survey representative sample
▪ MOPHP ▪ Implementing
partners
Nutrition Assessments
(Periodic)
▪ Emergency Food Security and Nutrition Assessment Food Security Livelihood Assessment (FSLA)
▪ Standardized Monitoring and Assessment of Relief and Transitions (SMART)
▪ Semi-Quantitative Evaluation of Access and Coverage (SQUAEC) Assessment Method18
▪ Yemen Food Security Outlook Updates-FEWS NET (Famine Early Warning Systems Network)
▪ Population and site survey representative sample
▪ MOPHP ▪ Implementing
partners
Third Party Monitoring
World Bank Emergency Health and Nutrition Programme internal third part monitoring
▪ All nutrition programming ▪ MOPHP ▪ UN Agencies
Annex 10 also depicts the level of healthcare, type of health facilities, catchment area, staffing and nutrition services offered.
2.2 Existing Data Flows, Monitoring and Data Collection Forms
Yemen collects data primarily through public health facilities19 that participate in the CMAM programme. and through community-based distribution points. Data are collected from visitors of health facilities and children who are admitted into the CMAM program and other preventive interventions through either routine primary healthcare, via referrals, through routine vaccination and growth monitoring or through mass health campaigns, mass expanded programme for immunization (EPI) campaigns and/or mass malnutrition screenings.
At the health facility level, the health worker—generally a nurse/medical/doctor assistant enters the data into the paper register books since there is no electronic data entry immediately available at the health facility level unless they are WHO-supported therapeutic feeding centres (TFCs). The Yemen Nutrition Cluster consolidates data on CMAM for the health facility (HF) sites that are primarily supported by either UN agency or national and international non-governmental organizations (NNGOs/INGOs), as well as some government-only operated HF sites.
At the District level the District Health Officer (DHO)-Nutrition Coordinator collates the paper forms into the respective nutrition programme Excel-based databases:
1. CMAM database-for both SAM and MAM (Access and Excel) (managed by UNICEF/MOPHP for SAM and WFP/MOPHP for MAM)
2. The new Inpatient Therapeutic Feeding Centres (TFC) database (piloting with ASP.net with Excel sheet reporting) (managed by WHO/MOPHP)
3. The IYCF Corners monthly report database (managed by UNICEF/MOPHP);
4. Nutrition Surveillance System (NNS) (managed by WHO)
18 Al-Ros, Belad. “Semi-Quantitative Evaluation of Access and Coverage (SQUAEC) REPORT Sana’a, Beni Matar, Sanhan.” Coverage Monitoring Network (CMN), January 2013. https://www.coverage-monitoring.org/wp-content/uploads/2015/07/Sanaa_-Jan-2013_-Yemen_-SQUEAC.pdf. 19 Public Health Facilities include: Primary Healthcare (PHC) Centres, PHC fixed Units, PHC community-supported shared temporary health units (i.e., schools, sheik in village house room, etc.), PHC outreach-mobile health services, community-based health services (community outreach), district, governorate and specialized hospitals)
12
5. The Community Health and Nutrition (CHNV) monthly database (managed by UNICEF/MOPHP;
6. The Community-Based Health & Nutrition Mobile teams Reporting Template managed by UNICEF/MOPHP);
7. The Nutrition Outreach Database for Governorate Health Offices managed by UNICEF/MOPHP);
8. Forthcoming District Information Health Systems Database (DHIS-2) managed by UNICEF & WHO/MOPHP); In terms of a health management information system (HMIS), Yemen is starting to scale-up the District Health Information Systems (DHIS-2) which is currently being piloted including for nutrition but it will take time to roll out in Yemen and reach scale
At present, at the sub-national level, data are disaggregated by Governorates and Districts, with continual data collection into a number of Excel spreadsheets from cumulative reports submitted on a monthly basis from the health facilities at the district-level by the District Health Officer-Nutrition Focal person (DHO-N). In Volume 2, the details for the Yemen nutrition data collection forms can be found including the name of the data collection form, the type of form, the individuals who fills out the form at the entry point, the service delivery entry point, the frequency of data submission (i.e., daily, weekly monthly), who the form/database is submitted to for approval, and if available the date that the form is due to be updated. On a monthly basis, the following Excel spreadsheets from each CMAM health facility site are collated by the DHO-N for the following categories of services:
• CMAM programme and Blanket Supplementary Feeding Programme (BSFP)
• IYCF corners
• Mobile integrated health & nutrition outreach teams
• Activities by CHNVs
The DHO-N then submits to a Governorate Health Officer-Nutrition Coordinator (GHO-N). The GHO-N thereby submits to UN agency zonal20 hubs and the central level MOPHP.
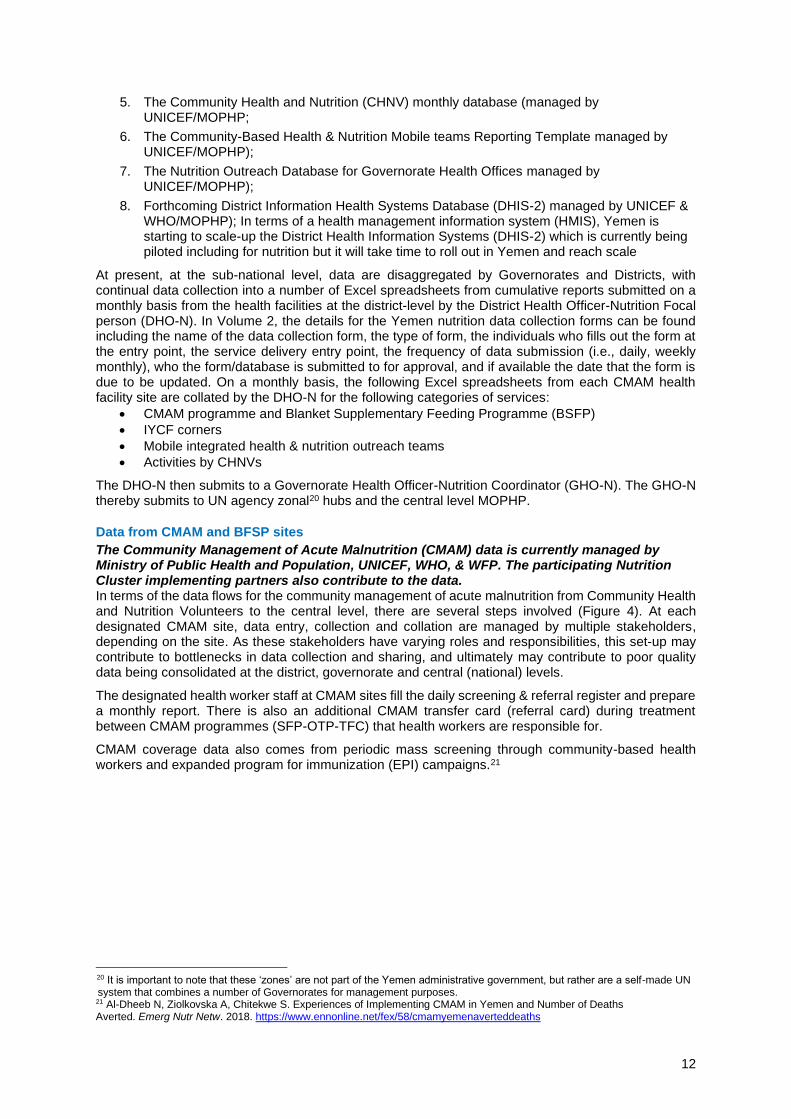
Data from CMAM and BFSP sites
The Community Management of Acute Malnutrition (CMAM) data is currently managed by Ministry of Public Health and Population, UNICEF, WHO, & WFP. The participating Nutrition Cluster implementing partners also contribute to the data. In terms of the data flows for the community management of acute malnutrition from Community Health and Nutrition Volunteers to the central level, there are several steps involved (Figure 4). At each designated CMAM site, data entry, collection and collation are managed by multiple stakeholders, depending on the site. As these stakeholders have varying roles and responsibilities, this set-up may contribute to bottlenecks in data collection and sharing, and ultimately may contribute to poor quality data being consolidated at the district, governorate and central (national) levels.
The designated health worker staff at CMAM sites fill the daily screening & referral register and prepare a monthly report. There is also an additional CMAM transfer card (referral card) during treatment between CMAM programmes (SFP-OTP-TFC) that health workers are responsible for.
CMAM coverage data also comes from periodic mass screening through community-based health workers and expanded program for immunization (EPI) campaigns.21
20 It is important to note that these ‘zones’ are not part of the Yemen administrative government, but rather are a self-made UN system that combines a number of Governorates for management purposes.
21 Al-Dheeb N, Ziolkovska A, Chitekwe S. Experiences of Implementing CMAM in Yemen and Number of Deaths Averted. Emerg Nutr Netw. 2018. https://www.ennonline.net/fex/58/cmamyemenaverteddeaths

13
Figure 2: Community Management of Acute Malnutrition (CMAM) Health Facility Sites Data Flows and Data Collection Forms
Source: Authors of this report, 2021.
For the management of MAM, there is a specific MAM database that is managed by the MOPHP/WFP, which is drawing from a paper-based MAM treatment daily register for targeted supplementary feeding programme (TSFP). In addition, for the prevention of malnutrition, there is a paper-based daily register and monthly report for the Blanket Supplementary Feeding Programme (BSFP), also managed primarily through WFP and MOPHP. WFP organizes its commodities through their MAM commodities distribution plan (Excel sheets), and a commodities tool for TSFP and BSFP together. The MAM programme information is compiled in a cooperating partners' monthly distribution report (CPDR) – this only covers MAM treatment services covered by their implementing partners.
For the management of SAM without complications through the Out-Patient Therapeutic Programme (OTP) there is a daily register, and monthly reporting tool that feeds into the SAM database. There is a stock database at the Governorate Health Office (GHO) level to manage therapeutic foods, but it is not used regularly.
In terms of CMAM sites that have inpatient care for the management of SAM with complications, there is a Therapeutic Feeding Centre (TFC) daily register, a monthly report and a separate TFC case reporting dashboard database system managed by WHO/MOPHP. In addition, WHO also uses a TFC assessment tool to ensure that their sites are regularly supervised and delivering quality services. Select sentinel sites (currently scaling-up) managed by WHO have a facility-based nutrition surveillance system (NSS) for their sentinel sites (soon to be scaled-up) with a health facility-based daily register.
Data from Infant and Young Child Feeding (IYCF Corners)
In CMAM sites that have Infant and Young Child Feeding (IYCF) corners there are daily registers: one for mothers and one general register for children. Also, there are daily tally sheet and a daily report for team supervisors. A monthly report is submitted to the District Health Office (DHO)-Nutrition at end of every month. The DHO-N fills in the cumulate IYCF corner data from multiple sites (attached to health facilities) into a monthly Excel-based database.
Data on Mobile Integrated Health and Nutrition Outreach Services
There are two daily registers-one register for mothers and one general register for children, plus a daily tally sheet and daily report for team supervisors. For mobile teams nutrition services there is a monthly reporting template. In terms of integrated nutrition services outreach there is an overall excel-based database for Governorate Health Offices.

14
.
Figure 4: Integrated Nutrition Outreach Services Data Flows and Data Collection Forms
Source: Authors of this report, 2021.
Figure 3: Infant and Young Child Feeding (IYCF) Data Flows and Data Collection Forms
15
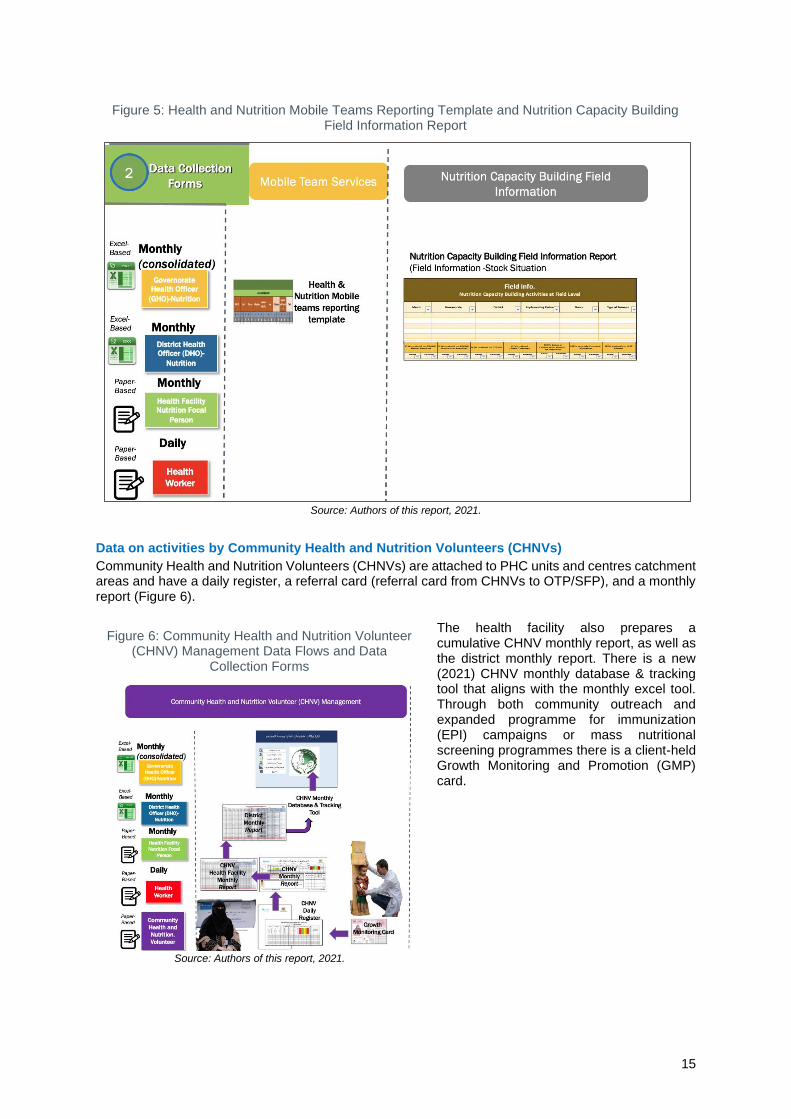
Figure 5: Health and Nutrition Mobile Teams Reporting Template and Nutrition Capacity Building Field Information Report
Source: Authors of this report, 2021.
Data on activities by Community Health and Nutrition Volunteers (CHNVs)
Community Health and Nutrition Volunteers (CHNVs) are attached to PHC units and centres catchment areas and have a daily register, a referral card (referral card from CHNVs to OTP/SFP), and a monthly report (Figure 6).
The health facility also prepares a cumulative CHNV monthly report, as well as the district monthly report. There is a new (2021) CHNV monthly database & tracking tool that aligns with the monthly excel tool. Through both community outreach and expanded programme for immunization (EPI) campaigns or mass nutritional screening programmes there is a client-held Growth Monitoring and Promotion (GMP) card.
Figure 6: Community Health and Nutrition Volunteer (CHNV) Management Data Flows and Data
Collection Forms
Source: Authors of this report, 2021.

16
2.3 Quality (Accuracy and Completeness) of nutrition data, data cleaning and feedback mechanisms
At the health facility level, the HF nutrition focal point collates and cleans health facility data into a consolidated monthly report (paper-based). Key criteria for cleaning data at health facility level is for case outcomes (cured, defaulting, non-response, and deaths) to match total programme discharges.
Reviewing the use of data at a health facility level through interviews with health facility staff in country was beyond the scope of this assignment. However, some KII reported that in some cases health facilities face challenges in submitting forms complete and in a timely manner, and analysis or use of data at health facility level is often limited.
Hard copy written paper-based forms are collected by DHO-N staff. At the district level from days 1-5 at the beginning of each month (submission by the fifth of month), the DHO-N, consolidates the paper-based forms from health facilities, and assesses data according to the catchment area. In some governorates where there is no established DHO, this role is undertaken by sub-governorate health offices, which may cover several districts. DHO staff manually enter the ledges from health facility CMAM sites data into Excel.
The district monthly report forms are sent monthly (in principle by the first week of the subsequent month) to the governorate level via consolidated Excel spreadsheets. Submission occurs through a range of methods, depending on the context and availability of internet within districts, most often via email, WhatsApp and other messaging services as attachment, or in some cases via USB memory stick.
The level of human, physical and human resources are limited at the DHO level. In some cases’ UNICEF supports by provision of laptops. Allowances have been provided to some DHO staff through the World Bank funded Emergency Health and Nutrition Programme (EHNP). However, interviewees have noted that such allowances to DHOs for information management stopped in early 2020, resulting in more delays in reporting of data in some instances.
Relevant DHO staff are trained on an annual basis on how to assess the quality of data submitted (checklist is included in Annex 11). This is part of a yearly training for District Health Offices which is centring around the following:
• Review of districts performance in terms of data and reporting.
• Refresher training on using the reporting tools and addressing common issues.
• Refresher training on data management skills (data collection, data cleaning, data compilation, data presentation, and data analysis)
At the Governorate level the Governorate Health Officer-Nutrition Coordinator (GHO-N), manually combines all district level programme data in one Excel spreadsheet. They clean the data by looking for red flags, discharge and outcome figures that do not line up, etc. These data are due on the 10th of each month and then emailed to MOPHP focal persons and United Nations (UN) (i.e., UNICEF, WHO, WFP) zonal offices at the same time.
At both District and Governorate level, the manual entry of data into Excel was flagged during the KIIs as being vulnerable to data entry errors. A list previously was provided to both DHO and GHO with data flagged as red (i.e., potentially erroneous), but this approach is no longer in active use. The focus in this list was on:
• Very high defaulters / cure / death / non-respondents numbers comparing to total discharges22.
• Comparing screening results with admission figures.
• Irregularities in screening data (e.g., having higher SAM number than MAM)
• Questions around the standardized entries of health facility name, health facility statue, etc).
• Comparing supplies used with admissions23.
22 As per Sphere standards, the denominator in the performance indicators for acute malnutrition treatment programmes consists of the total number of discharged but this is not happening in Yemen. See: https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/7.minimum-standards-in-food-secutity-and-nutrition.pdf 23 A logical comparison however would be between supplies used and attendance so that is includes both new admissions and cases who were admitted in previous months.

17
• Trends in supply needs in comparison with past months.
• Checking any unusual figures in admission categories (e.g., high number of oedema cases)
Finding any of the above is not flagged as erroneous per se, rather where a flag occurs, all data for health facility or district is to be reviewed and followed up on through feedback during district and governorate health office meetings.
These criteria are primarily to verify the validity of the data in the monthly report, and to assist the identification of potential errors. It has been noted that the checklist for nutrition programme data quality does not provide DHO with any analytical tools to flag where facilities report unlikely programme outcome indicators or static figures over time. For instance, a health facility with high defaulting in a given month is flagged as red for DHO in their data entry sheet, however, another facility reporting very low defaulting (say less than 1%) on a continuous basis, even with high numbers of admissions, is not flagged as potentially problematic.
Where application of data quality criteria flags data as potentially erroneous or of concern in a given district by zonal UN agency / NC IMO, this will usually be communicated to the GHO, who then feeds back to the DHO. Direct contact between the national or zonal Nutrition Cluster staff and DHO and programmes tends to be limited to defined capacity building, training or supportive outreach activities rather than around routine data issues.
Information management staff in GHO use the same set of criteria used by DHO. Many of the same issues appear to be present at the GHO level, in terms of a lack of guidance provided to recognize or report unlikely, problematic or static figures reported over time.
Figure 7: Data Collection: Reporting & Data Cleaning
Source: Authors of this report, 2021.
The IMOs at the UN agency hubs are located in a ‘zone24’. There five zonal hubs in Yemen based in Aden, Sana, Taiz, Sa'ada and Hodeidah (Al-Hodeida), covering between two and eight governorates. The zonal Nutrition Cluster Hubs report to the national Cluster but coordinates actions within their given governorates. As such, they are often a first point of contact between GHO and the wider National Nutrition Cluster. It is understood that subnational zonal Nutrition Cluster IMO utilise a similar set of data quality criteria as DHO and GHO for assessing data quality and completeness.
The IMOs located in each zonal hub, upon receiving data from governorates undertake another round of data cleaning, mainly looking for red flags, based upon the criteria outlined above. They (UN agency IMOs/Governorate Health Offices) submit nutrition data to the Sanaa and Aden MOPHP and Cluster level from the 10-15th of each month.
24 It is important to note that these ‘zones’ are not part of the Yemen administrative government, but rather are a self-made UN system that combines a number of Governorates for management purposes.

18
Finally, the national Nutrition Cluster/UNICEF/WHO/WFP offices conduct another round of data cleaning for UN-supported interventions to ensure they have the same numbers for a quality check.
The agreed timeframe to have the reports submitted to the Nutrition Cluster is by 10th of each subsequent month. However, most of the timely it is delayed to the 20th, or to the end of the month. NGOs operating OTP, TSFP, BSFP, IYCF, MNP submit to the DHO in their respective districts. These are then consolidated to the GHOs and subsequently to the National level. The NC coordinator informed the team that 40% of the TSFP services are covered by NGOs that submit their report to WFP and then to the cluster, while NGO OTP coverage accounts for just 10% of the OTP coverage in the country.
Most of data/reports submitted to the cluster directly by the NGO on monthly are: supplies tracking tool at the health facility level, funding status, constraints and challenges that are not part of the MOPHP information chain established collection and reporting system.
Key informants reported that they receive little direct feedback and only hear about their joint progress as reported through the monthly Nutrition Cluster meetings through a PowerPoint presentation entitled ‘Nutrition Cluster Monthly Analysis25’ and the monthly Nutrition Cluster Summary Analysis consolidated database. KII reported that the lack of other more forms of direct feedback was at least partly due to limited human resource capacity with limited availability of IMOs within the Nutrition Cluster managing a large number and variety of Excel files with reporting data.
2.4 Nutrition Information Systems in Humanitarian Settings
Global acute malnutrition (GAM) prevalence estimates from assessments such as SMART, and the IPC acute malnutrition analysis have the most commonly used nutrition indicators used to prioritise action in non-nutrition specific clusters namely in WASH, food security, livelihoods and health,26 and through the Yemen multisectoral famine risk reduction strategy.27 Nutrition data is also used in the IPC acute food insecurity analysis. However, this review found little evidence of the systematic use of nutrition data to drive prioritization or convergence of programming across clusters, outside of the IPC and famine risk reduction strategy.
Following the IPC-acute malnutrition analysis results, the Nutrition Cluster conducted multisectoral gap analyses at hub level with health/ WASH and food security and livelihood clusters. This led to joint agreement that scaling up of the health/WASH response and increased allocation of resources to be focused on areas with gaps in programming.
Intersectoral analysis was also conducted to prioritize districts for multisectoral responses for prevention of famine in 2018, 2019 and 2021. A joint monitoring framework (JMF)28 - a concept for monitoring the integrated phase classification (IPC) assumptions intends to incorporate data from across several clusters is under conception in Yemen, as part of wider efforts for famine risk reduction, however this is at a nascent stage. The framework came about in 2019 as it became apparent to be necessary to inform decision makers in a better way in between the IPC rounds. It is planned that an on-going monitoring framework would be able to identify hotspots and produce information to guide on what set of actions can best be put in place to reduce vulnerabilities. It was mentioned by some that progress towards the development of the joint framework had slowed down in recent months. The Nutrition Information
25 The ‘Nutrition Cluster Monthly Analysis’ reports on: The Nutrition Cluster, partners operational presence in the form of a map differentiating three main nutrition programmes: 1) management of severe acute malnutrition (SAM), 2) management of moderate acute malnutrition (MAM) and 3) counseling for mothers or care of children under 2 on infant and young child feeding (IYCF). It reports on coverage of partners by Governorate and differentiates partners by national NGOs, international NGOs, UN agencies and government. It also reports on a Nutrition Cluster dashboard which illustrates the people in need (PIN), overall target and reach as well as outlines a number of activities and their progress in relation to these targets. It also depicts geographic coverage of both SAM achievements and MAM achievements. Finally, it reports on Admissions & reporting rate trends for SAM and MAM, new admission coverage for SAM and MAM, new admission and reporting rates for SAM/MAM, SAM and MAM performance indicators, SAM and MAM treatment coverage against targets, IYCF, BFSP, MNP, VitA coverage against targets, supply availability, impact of covid-19, Reasons for decrease and mitigation measures (by NGOs), 26 see for example: Yemen Humanitarian Fund (YHF) First Standard Allocation 2020 – Strategy. https://www.unocha.org/sites/unocha/files/dms/YHF_SA1%20-%20Strategy%20Paper.pdf; Yemen WASH Cluster; Coordination Meeting 1st December 2020. Available at: https://www.humanitarianresponse.info/en/operations/yemen/water-sanitation-
hygiene; Food Security and Nutrition Clusters prioritisation of the geographical locations for the 2017 humanitarian response. https://www.humanitarianresponse.info/en/operations/yemen/document/fs-nut-prioritisation-v6-external . 27 Integrated Famine Risk Reduction: An Inter-Cluster Strategy To Prevent Famine In Yemen. A Case Study July 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/Yemen_Integrated_Famine_Risk_Reduction_CaseStudy_July2020.pdf 28 The JMF is a concept for monitoring the integrated phase classification (IPC) assumptions, identifying hotspots and triggering actions such as IPC update, data collection or even direct programme interventions. Recently the Food and Agriculture Organization of the United Nations (FAO) included it as a deliverable within the information system project in order to house the process with the aim of involving of partners. It is still in inception/conceptual phase as of April 2021.

19
Technical Working Group (NITWG), under the auspices of the Nutrition Cluster – is in the process of development of a Results Monitoring Framework which will be streamlined within the wider inter-cluster joint monitoring framework.
The Integrated Phase Classification (IPC) analysis, both for acute malnutrition and food insecurity, which informs targeting across nutrition related clusters in Yemen, uses a range of nutrition data from various available sources, including survey estimates of acute malnutrition, programme data on CMAM admissions data and other nutrition data as deemed relevant, alongside information on food consumption and security, mortality and disease data (diarrhoea, malaria, acute respiratory infection, measles etc.) collected through PBSs and programme-based data. The IPC analysis is also used to inform priority districts targeted by the nutrition and other clusters, and to provide guide people in need estimates. The people in need estimates in the IPC- analysis uses the results of SMART assessments, either upper confidence interval or point prevalence of previous survey estimates of acute malnutrition.
Where CMAM new admissions data are used in the analysis to characterize the new admission trend (increasing, stable or decreasing), a cut-off of 80% or above of programmes reporting per district is applied. The process of developing IPCs is flexible in terms of decision-making on the indicators to cover within it. The IPC is not based upon a set calculation. It is rather based upon an evidence informed decision-making process through which geographic areas are judged to be in a given IPC class based upon available evidence from relevant sectors. Key informants involved in the IPC in Yemen agreed that if more in-depth district level analysis of NIS data were available, the IPC could potentially incorporate other forms of nutrition information alongside or in place of the data that is currently used.
Key informants from other clusters noted that the Nutrition Cluster currently produces a large amount of information but that this information is not in a form which is readily usable for decision-making around the prioritisation of geographic or population groups. Reported nutrition programme coverage numbers against caseload targets was seen to provide only limited value for use in this respect. One interviewee said that “further investigation of the data, instead of just reporting it” would be beneficial to inform planning and monitoring in other sectors. During the interviews, it was also stated that further analysis which could identify where programme data may point to deterioration of the nutrition situation could facilitate improved joint targeting of preventative actions from other clusters.
Within Nutrition Cluster information products, the most cited non-nutrition specific information is from the IPC analysis. Within Nutrition Cluster information products, there is little reporting of information from other clusters by governorate or UN zones to triangulate with nutrition information to identify hotspots and provide a picture of potential drivers of the nutrition situation.

20
3. STREAMLINING THE SYSTEM: Prioritisation and Harmonisation
of Nutrition Data & Information Collection and Reporting
Mechanisms
3.1 Overview & Current Situation and Key Challenges
3.1.1 Developing a Framework for Action and Standardising Monitoring and Reporting (Recommendations 1.1 – 1.3)
With the rapid scale up of nutrition programming in recent years, the number and type of nutrition indicators collected, and the variety of forms and reporting procedures used by stakeholders involved in nutrition programming have also increased. There is a need for harmonisation and standardisation of indicators, data collection forms, and agreed-upon standard operating and reporting procedures.
Indicators and their data sources—routine data collection forms need to be streamlined and endorsed so that everyone uses the same forms with clearly defined monitoring and reporting roles and responsibilities for each cadre. Data collection sources need also to be identified to avoid duplication. Please see Annex 6 for more details on Yemen nutrition data collection forms and management of nutrition data collection and reporting which helped map out all of the data collection forms that identified quite a few bottlenecks for taking other actions to improve.
We present the current situation, key findings and recommendations by priority-ones we think should be initiated immediately (immediately up to 1 year), short-term recommendations that should be initiated in at least 1-2 years) and longer-term recommendations that should be initiated and implemented at least after two years (thus May 2023) up until 3 years (May 2025).
The job descriptions and roles and responsibilities for monitoring, reporting and data collection for nutrition workforce at each level in Yemen (central (national), governorate, district, health facility and community) are not currently clearly documented leading to a confusion of daily role and responsibilities, lines of reporting and approval processes.
Furthermore, there has not been any capacity assessment of human resources for the data and information management for nutrition. However, the lack of capacity for sub-national staff to collect and submit quality data at sub-national levels in a timely manner was noted by KII and consultations. There are a number of nutrition trainings available for health workers and Community Health and Nutrition Volunteers (CHNVs) but these trainings lack a monitoring and reporting component.
There are also low levels of capacity and limited training on monitoring and reporting which is, in addition, compounded by a lack of infrastructure (technology and equipment) to compile information in a timely-‘real-time’ manner.
Data quality is key to nutrition programme credibility and when implementing the recommended activities, best practice resources are necessary in the design and use of dashboards (e.g., learning from other countries). It is important to understand that dashboards are only tools and their effectiveness depends on their use.
Thus, it will be imperative to begin the improvement of the nutrition information systems by clearly defining the data users and roles and responsibilities through a ‘Yemen Nutrition Monitoring, Evaluation and Reporting Accountability Framework’.
Otherwise, it is imperative to do the following in Yemen: ▪ Immediately develop a Yemen Nutrition Monitoring, Evaluation and Reporting Accountability
Framework ▪ Define Governorate/District key performance indicators & thresholds and regular reporting
mechanisms for a sub-national nutrition scorecard to track progress/results/against targets ▪ Harmonize indicators and data collection forms ▪ Harmonize Data Sources /existing databases, Excel spreadsheets into one central
interoperable database that is managed by MOPHP in addition to ONE UN agency approach ▪ Harmonize existing nutrition data dashboards into ONE nutrition data dashboard based on
joint data, revise priorities, define automatically generated data visualization tools (DVTs) for Governorate, District, and Health Facility use (situation maps, dashboards). This can be done manually until a national nutrition dashboard is consolidated.

21
Figure 8: The Nutrition Data Value Chain
Source: Piwoz, Ellen, Rahul Rawat, Patrizia Fracassi, and David Kim. “Strengthening the Nutrition Data Value Chain for Accountability and Action” 33 (2019): 6. https://www.anh-
academy.org/sites/default/files/SightandLifeMagazine_2019_Data_in_Nutrition_StrengtheningtheDataValueChain-AccountabilityandAction.pdf

22
Figure 9: Data Assessment/Collection, Analysis, and Use for Decision-Making (Action)
Source: Authors of this report, 2021.

23
Learning from other countries lessons from using data dashboards within governments we present Figure 11 as an overview of the suggested flow of how the nutrition information system needs to be improved in Yemen as well all of the four pieces of the nutrition data value chain working together: 1) data prioritization, 2) data collection, 3) data accessibility and 4) data use. In line with these key areas of the nutrition data value chain there needs to be a full range of activities implemented to create and use nutrition quality data.
Figure 9 presents the data flow and outputs of the proposed database and how it would feed into subnational scorecards outlining key indicators and thresholds, and support feedback across the data value chain and decision making is shown.
3.1.2 Capacity Development within the Health Workforce (Recommendations 1.5 – 1.9)
The production of nutrition information, especially nutrition programme information, is heavily reliant upon the workforce within health facilities and communities, along with district and governorate health offices which are facing severe human, physical and financial resource constraints.
While there are a number of regular trainings for health workers and Community Health and Nutrition Volunteers (CHNVs), none of these contain a monitoring and reporting component. Refresher training for MOPHP monitoring and evaluation focal persons for nutrition at the district and governorate level takes place on an annual basis only.
District and Governorate Health Offices play a key role in the NIS in Yemen acting as the first administrative point of contact that health facilities report to within the health system. Trainings for DHO and GHO staff are on an annual basis. It is not clear what impact trainings have as there is no clear system of tracking quality and completeness of reporting before and after trainings take place. The set of criteria provided for DHOS and GHO for assessing data quality could be more clearly defined by IMO at the zonal and national level in the Nutrition Cluster, and mechanisms are lacking which can systematically identify where there are data quality issues and trigger support through increased capacity building or other efforts.
At both the national and the sub-national levels, we recommend a rapid human resource assessment that informs the standardisation and strengthening of available training for health workers and monitoring and evaluation focal persons for nutrition (including information management officers) throughout the nutrition data value chain.
It will be useful to monitor the quality and completeness of reporting both before and after capacity building exercises. Ideally, the impact of capacity building would be tracked across all governorates and districts where trainings take place, but if that is not feasible, a subsection could be identified, e.g., on the issues with reporting and the completeness and quality of reporting. These actions can support the MOPHP alongside a longer term set of actions to increase the available human, physical and financial resources targeted to Monitoring and Evaluation for Nutrition.
3.1.3 Short Message Service (SMS) and Web-based Messaging Applications (Recommendations 1.10)
Several KII felt that there are opportunities for increasing digitization of reporting from facilities utilizing short message service (SMS) based systems. There was no consensus on what system could be used, although several key informants with experience in other low resource settings felt there are examples which could be leveraged for us in Yemen (examples which can be found online are SMS based CMAM stock reporting in Nigeria29, the RapidPro community nutrition monitoring in Zimbabwe.30
WhatsApp is used across programming in nutrition programming in Yemen, for instance to submit data programme data, to communicate information on stock use and supply issues at GHO/DHO level. While WhatsApp is used extensively in a non-formalised way across different areas of nutrition programming, the WHO have implemented a somewhat more systematised process to analysing data communicated through messaging. WhatsApp groups for “TFC grievance reporting” are also used by the WHO supported TFC staff. Some 39 groups are currently active as of March 2021. Staff at the facility level
29 Tuffrey, Veronica, et al. "Assessment of monitoring systems in the management of severe acute malnutrition in northern Nigeria." BMC nutrition 7.1 (2021): 1-13. 30 Munikwa, Nakai, et al. "Use of RapidPro for remote collection of nutrition data during the drought emergency and COVID-19 pandemic in Zimbabwe." Field Exchange 64 (2021): 67.

24
provide feedback through the groups to relevant stakeholders at Governorate, Zonal and National level on issues such as stock, staffing and allowances, technical issues and case follow up.
The WHO at a national level undertake a routine analysis of messages, with counts provided on the number and location of group, most common issues brought and flagged as important (stock, allowances, staffing etc.). Some interviewees noted that that the groups, while not following a formal reporting template per se, do allow for concerns and stock issues at the facility level to be quickly acted upon.
In the shorter term, further formalising the use and analysis of messaging services for communication from the facility and district levels upwards could increase accountability and help identify and address recurrent issues, especially related to availability of stock, human resources, and reporting rates.
3.1.4 Strengthening Reporting and Analysis through the DHIS-2 (Recommendation 1.11)
As previously described, for OTP CMAM programming both CHNV reporting to facilities and reporting from facilities to DHO is via hardcopy paper-based reporting sheets and written data collection forms.
The most cited efforts towards digitization of nutrition reporting in Yemen is via the district health information system (DHIS-2). The DHIS-2 is a health management information system for collection, storage, validation, analysis, visualization and presentation of health information data operated in 73 low- and middle-income countries. The system provides a range of mobile solutions for data collection and transfer such as SMS-functions and Android and low-end Java-apps for offline data collection.31
In the medium to longer term, the development and roll out the DHIS-2 in Yemen presents an important for more systematic collection, management and analysis of nutrition information in the country. However, this review found that development of the system is not visible or well understood by many nutrition stakeholders inside and outside of the country, including key donor agencies and some UN agency staff. How nutrition will be incorporated within the DHIS-2 and what proportion of nutrition programming data will be migrated to the system is also not yet well defined.
While modules with indicators for various health services are in-built, it is adaptable to country contexts allowing for real-time data visualization through dashboards, scorecards, pivot tables, maps and charts. The DHIS-2 was first piloted Yemen in 2017. The Sana’a MOPHP has formed a committee-for DHIS-2, led by MOPHP with support from WHO, and UNICEF. Progress in the roll of the system has been slow due to both limited funds and a lack of clarity around how a digitized system will function in areas lacking necessary infrastructure, especially rural areas which often lack mobile connectivity, computers, or reliable electricity. Inputting data via smart phones android app, at a cost of $100 per mobile, is an option being explored in low resource facilities, allowing data input and storage offline. The WHO noted that they plan for health facilities currently submitting data to the WHO-supported health facility nutrition surveillance system to transition to DHIS-2, but no solid timeline has been agreed.
What other aspects of nutrition programming will be included in the system is not yet well defined. What aspects of CMAM and preventive programming will be included and how this relates to existing databases and analysis systems will need to be further clarified. There was a lack of clarity from the key informants on how CMAM and preventative nutrition programme reporting would be incorporated into the system. Some key informants noted that reporting all nutrition programming via DHIS-2 would not feasible or desirable and dual reporting on nutrition programming will continue to be necessary even when DHIS-2 is operating.
Many key informants, including donor agencies and UN staff, were either unaware or unclear on plans for the rollout of DHIS-2. There does not appear to of been any significant consultations on how the system will be integrated with existing nutrition programme reporting databases, analysis and feedback mechanisms. Currently, there is little digitized CMAM facility reporting largely due to the rurality and lack of connectivity of many facilities providing services. However, as noted elsewhere in this report WhatsApp is used in several places throughout the NIS at present. For instance, data submitted through DHO to GHO is in some cases via WhatsApp and feedback is often also provided via WhatsApp. The WHO is currently working with the MOPHP on the TFC based case reporting dashboard (as of January 2021) but the lay-out and contents are yet to be finalized.
31 District Health Information Software 2 (DHIS2). DHIS-2 Overview. https://dhis2.org.

25
3.2 Streamlining the Data Collection and Reporting Mechanisms Systems
Indicators and their data sources—routine data collection forms need to be streamlined and endorsed so that everyone uses the same forms with clearly defined monitoring and reporting roles and responsibilities for each cadre. Data collection sources need also to be identified to avoid duplication. Please see Annex 6 for more details on Yemen nutrition data collection forms and management of nutrition data collection and reporting which helped map out all of the data collection forms that identified quite a few bottlenecks for taking other actions to improve.
We present the current situation, key findings and recommendations by priority-ones we think should be initiated immediately (immediately up to 1 year), short-term recommendations that should be initiated in at least 1-2 years) and longer-term recommendations that should be initiated and implemented at least after two years (thus May 2023) up until 3 years (May 2025).
National Nutrition Monitoring and Evaluation Accountability Framework for Action
Table 2: Immediate Recommendations (immediate-1 year)
Current Situation Summary
& Key Findings Key Proposed Activity(s)
Key Stakeholder Responsible
& Stakeholders Involved Recommendation 1.1: Develop a National Nutrition Monitoring and Evaluation Accountability Framework (including Clearly Define Nutrition Reporting Roles and Responsibilities)
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making (Analysis &
Action) ▪ Roles and
responsibilities for monitoring, reporting and data collection for nutrition at each level (central (national), Governorate, District, Health Facility and Community) are not currently clearly documented leading to a confusion of role and responsibilities, lines of reporting and approval processes.
▪ There are often many ad hoc information reporting requests for the Nutrition Cluster based on needs, which takes staff away from other responsibilities.
▪ Timeliness of Data Collection: There is difficulty with timely submissions and the amount of time it takes to compile information.
Develop a National Nutrition Monitoring and Evaluation Accountability Framework (including Clearly Define Nutrition Reporting Roles and Responsibilities)-this will clearly defined roles and responsibilities for nutrition reporting, data collection, data collection forms-contributing to a robust multisectoral national nutrition reporting and monitoring system for Yemen. Learning from Kenya the Nutrition M & E framework32 the framework should include: ▪ The goal and objectives ▪ Guiding principles on quality for monitoring and reporting-
including and data quality assessments (DQA) ▪ Clearly defined components of the nutrition information
system (NIS) data dashboard and data depository ▪ Sources of nutrition data and information ▪ How data will be analysed and disseminated, as well as
defining the basic M & E concepts. ▪ Clearly defined roles and responsibilities for a unified
approach to reporting and monitoring. ▪ Clearly defined Reporting due dates and approval process
of data and any data cleaning processes. ▪ Clearly defined framework for capacity building for nutrition
information/reporting and monitoring ▪ Clearly defined plan for the dashboards about who will use
the data (who are the users), when it will be used for communication and how it will influence decision-making
▪ Real-Time Tracking of programme information (admissions, discharge, outcomes, screening, stock etc.): There needs to be a process put into place for flagging the evolving situation for in relation to these indicators in real time. This includes flagging unusual events, outbreaks, etc.
The M & E framework will not only reiterate the national nutrition definitions but it will go into more detail about the key result areas and priorities aligning with the national nutrition response. It is proposed all other recommendations in this report would contribute to and be situated within such a framework.
▪ Targeted Technical Assistance Team (Consultancy)
▪ MOPHP ▪ Nutrition Cluster ▪ WHO Information
Management Officers ▪ UNICEF Information
Management Officers ▪ WFP Information
Management Officers ▪ SUN Secretariat/Yemen
32“Kenya Nutrition Monitoring and Evaluation Framework: 2018 to 2022.” Nairobi, Kenya: Government of Kenya, Ministry of Health, July 2020.

26
Harmonizing and Standardising Monitoring and Reporting
Table 4:Short-Term Recommendations (1-2 years)
Current Situation Summary & Key Findings
Key Proposed Activity(s)
Key Stakeholder Responsible
& Stakeholders Involved
Recommendation 1.3: Facilitate Harmonization of Indicators and Data Collection Forms
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making
(Analysis & Action)
Indicators ▪ Most nutrition/data
information is coming from routine data collection from many data collection forms collected by the MOPHP & UN agencies (WFP/WHO/UNICEF).
▪ Very little data is being submitted by INGOs and data harmonization needs to be increased.
▪ WHO has been working with MOPHP to develop a key compendium of national
Hire a consultant or a consultant team to harmonize and simplify indicators and data collection tools. This consultancy will work directly with MOPHP and UN agencies to define priorities & standard indicators, then update the data collection forms based on this, eliminating excess indicators or data fields from data collection forms. ** Focus on reducing and simplifying indicators for action Facilitate a 1-day validation workshop to agree on harmonized and simplify indicators and data collection tools ▪ As a starting point, consultants can use the mapping
the consultants conducted through this consultancy.
▪ Targeted Technical Assistance Team (Consultancy)
▪ MOPHP ▪ Nutrition Cluster ▪ UNICEF/IMOs ▪ WFP/IMOs ▪ WHO/IMOs
Table 3: Immediate Recommendations (immediate-1 year) Current Situation Summary
& Key Findings Key Proposed Activity(s)
Key Stakeholder Responsible & Stakeholders Involved
Recommendation 1.2: Finalize Sub-National Nutrition Scorecard Set of Key Performance Indicators (KPI), Thresholds and Review Process
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making (Analysis & Action)
▪ There is currently no way to track performance at the national, or sub-national levels and no established feedback mechanisms
▪ There are some performance indicators for quality and for initial utilization but no others and very little for other nutrition services.
▪ This suggestion is based on the March 17 Technical Session on Streamlining and Harmonization of National Nutrition Data Collection Forms, Indicators & Reporting Mechanisms
Facilitate a 1-2 -day workshop to finalize scorecard key performance indicators-focusing on programme coverage, all nutrition services use core nutrition outcomes, Along with this define clear scorecard thresholds to measure and track performance against targets ▪ A scorecard is a web-based tool
that displays periodic snapshots of performance on indicators and targets associated with a country’s nutrition strategies and plans.
▪ Decide on 10-15 key performance indicators and pre-defined targets for performance tracking of all nutrition services at the Governorate/District levels
▪ Select initial indicators based on priorities and available data.
▪ Clearly define agreed upon ranges of threshold limit or boundaries for the ‘traffic lights’ system (i.e., green, yellow and red) at regular intervals (i.e., every quarter).
▪ Agree upon proposed reporting & accountability mechanisms to monitor and collect scorecard data.
▪ Define clear corrective actions for each indicator based on traffic light score.
▪ Clearly decide on regular management review processes to review the scorecard
▪ A Technical Assistance Consultant Team
▪ UNICEF, IMO leading ▪ MOPHP ▪ UNICEF Nutrition Cluster

27
Table 4:Short-Term Recommendations (1-2 years)
Current Situation Summary & Key Findings
Key Proposed Activity(s)
Key Stakeholder Responsible
& Stakeholders Involved
impact indicators aligned with the World Health Assembly Targets for 203033
▪ There was an effort to consolidate indicators through the Yemen Multisectoral Nutrition Action Plan (MSNAP) Monitoring and Evaluation Plan (M&E Plan) 2020-2023: An Accompanying Document to the Republic of Yemen’s Common Results Framework and Multisectoral Nutrition Action Plan34.” –however it did not map all data sources.
▪ There are a set of proposed District Health Information System (DHIS-2) indicators that need to be reviewed/revised and agreed upon.
▪ Data Collection Forms: There is currently a major burden of having to fill out multiple registers within the same health facility by the same person
▪ Harmonize, consolidate and clearly define and mainstream a set of recommended nutrition-specific indicators (facility and community-based) their data sources, and frequency of data collection.
▪ Agreed to “streamline and simplify” and significantly reduce the number of indicators reported on.
▪ The Yemen Nutrition Cluster is collecting a lot of nutrition indicators—need to analyze these and see which ones are most useful
▪ Need to clearly define/revise core indicators that can be integrated into DHIS-2
▪ Prioritize indicators, especially Emergency infant and young child feeding (e-IYCF) and acute malnutrition treatment]
▪ Disaggregation: Ensure the indicators are disaggregated into males/females as well as into geographic level of reporting - national, governorate and district
▪ Consider additional indicators as appropriate for support of midwives and CHNVs and for supportive supervision at all levels.
▪ Consider harmonizing with other related programming indicators such as child health/expanded programme for immunization (EPI), child health register/PLW register, etc.
▪ This workshop can be used to critically review and triangulate data, standardize tools and methods as well as develop national harmonized guidance.
▪ Please see Volume 2 for all of the existing data collection tools and some of the issues with the data collection tools.
Table 5: Longer-Term Recommendations (1-3 years)
Current Situation Summary
& Key Findings Key Proposed Activity(s)
Key Stakeholder Responsible
& Stakeholders Involved
Recommendation 1.4: Develop a National Nutrition Indicator Reference Guide
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making
(Analysis & Action)
▪ There are no standardized comprehensive indicator definitions available.
▪ The “Yemen Multisectoral Nutrition Action Plan (MSNAP) Monitoring and Evaluation Plan (M&E Plan) 2020-2023: An Accompanying Document to the Republic of Yemen’s Common Results
Develop a web-based indicator registry (housed on the Nutrition Cluster) to facilitate access to information about the agreed upon Yemen indicators. Include: ▪ Both the global and national standards
(guidelines/policies) that are referenced ▪ The number in the results framework ▪ The indicator ▪ The indicator definition ▪ The unit of measurement ▪ Indicator disaggregation ▪ Method of estimation including:
▪ Targeted Technical Assistance Team (Consultancy)
▪ MOPHP ▪ Nutrition Cluster ▪ WHO Information
Management Officer ▪ UNICEF Information
Management Officer ▪ WFP Information
Management Officer
33 Key High-Level Impact Indicators (WHA 2030) include: 1. Stunting in Children under Five Years of Age, 2. Anaemia in Women of Reproductive Age (WRA), 3. Low Birth Weight (LBW), 4. Overweight in Children under Five Years of Age, 5. Exclusive Breastfeeding in Infants Ages Six Months or Less, 6. Wasting in Children under 5 Years of Age, and a few additional indicators have been added: 1. Women’s Minimum Dietary Diversity (W-MDD), 2. School age children anaemia, 3. School age children acute malnutrition screening, 4. Women/Adolescent overweight, 5. Complementary Feeding for Children 34“Yemen Multisectoral Nutrition Action Plan (MSNAP) Monitoring and Evaluation Plan (M&E Plan) 2020-2023: An Accompanying Document to the Republic of Yemen’s Common Results Framework and Multisectoral Nutrition Action Plan.” Republic of Yemen, March 2020. https://mqsunplus.path.org/wp-content/uploads/2020/08/Yemen-MSNAP-ME-Plan-FINAL_29April2020.pdf.

28
Table 5: Longer-Term Recommendations (1-3 years)
Current Situation Summary
& Key Findings Key Proposed Activity(s)
Key Stakeholder Responsible
& Stakeholders Involved
Framework and Multisectoral Nutrition Action Plan35 is available with some data sources defined.
o the numerator o the denominator,
▪ Data availability ▪ Data source(s) ▪ Information/caveats about data quality ▪ Frequency of data collection ▪ Guidance if applicable on reporting Normative global, regional and local indicators should be considered36 National data sources should also be considered—prioritizing the routine data sources from daily and monthly data collection forms.37 Both routine information indicators should be defined as well as periodic population-based surveys and assessments core set of indicators to help establish indicators that can be quality and measure trends over time.
▪ SUN Secretariat/Yemen
35 “Yemen Multisectoral Nutrition Action Plan (MSNAP) Monitoring and Evaluation Plan (M&E Plan) 2020-2023: An Accompanying Document to the Republic of Yemen’s Common Results Framework and Multisectoral Nutrition Action Plan.” Republic of Yemen, March 2020. https://mqsunplus.path.org/wp-content/uploads/2020/08/Yemen-MSNAP-ME-Plan-FINAL_29April2020.pdf 36 These include: The Scaling Up Nutrition Movement Monitoring, Evaluation, Accountability and Learning – SUN MEAL (SUN. “Monitoring, Evaluation, Accountability and Learning - MEAL.” Accessed December 16, 2020. http://scalingupnutrition.org/progress-impact/monitoring-evaluation-accountability-and-learning-meal/.; “Indicators for Assessing Infant and Young Child Feeding Practices: Conclusions of a Consensus Meeting Held 6–8 November 2007 in Washington D.C.” Washington, D.C.: World Health Organization (WHO), 2007. http://www.unicef.org/nutrition/files/IYCF_updated_indicators_2008_part_1_definitions.pdf DHS-8 Questionnaires: https://dhsprogram.com/publications/publication-DHSQ8-DHS-Questionnaires-and-Manuals.cfm “Meeting Emerging Nutrition Data Needs in DHS-8 | The DHS Program Blog.” Accessed December 16, 2020. https://blog.dhsprogram.com/nutrition-data-in-dhs-8/.; “WHO/UNICEF Discussion Paper: The Extension of the 2025 Maternal, Infant and Young Child Nutrition Targets to 2030.” World Health Organization (WHO) and United Nations Children’s Fund (UNICEF). Accessed October 12, 2020. https://www.who.int/nutrition/global-target-2025/discussion-paper-extension-targets-2030.pdf?ua=1 WHO, “WHO | Global Targets 2025.” World Health Organization. Accessed August 19, 2020. http://www.who.int/nutrition/global-target-2025/en/. “Feed the Future Indicator Handbook, Originally Published March 2018, Revised Version Published September 2019.” The U.S. Government’s Global Hunger & Food Security Initiative, Feed the Future, March 2018.; https://www.agrilinks.org/sites/default/files/revised_ftf_indicator_handbook_clean_version_20190926.pdf Progress on Drinking Water, Sanitation and Hygiene: Update and SDG Baselines: 2017.” Joint Monitoring Program (JMP), WHO and UNICEF, July 12, 2017. https://data.unicef.org/wp-content/uploads/2017/07/JMP-2017-report-launch-version_0.pdf Drinking Water | JMP.” Accessed October 25, 2020. https://washdata.org/monitoring/drinking-water.; “STANDARDISED CATEGORIES AND INDICATORS FOR BETTER CMAM REPORTING FINAL Apr 2015.Pdf.” Accessed December 16, 2020. https://www.cmamreport.com/sites/all/themes/stc/cmam-assets/STANDARDISED%20CATEGORIES%20AND%20INDICATORS%20FOR%20BETTER%20CMAM%20REPORTING%20%20FINAL%20Apr%202015.pdf.; Global Nutrition Monitoring Framework: Operational Guidance for Tracking Progress in Meeting Targets for 2025.” Accessed August 6, 2020. https://www.who.int/publications-detail-redirect/9789241513609.; “SDG Indicators — SDG Indicators.” Accessed November 22, 2020. https://unstats.un.org/sdgs/indicators/indicators-list/.; “Recommendations for Data Collection, Analysis and Reporting on Anthropometric Indicators in Children under 5 Years Old.” WHO &(UNICEF, 2019. https://apps.who.int/iris/bitstream/handle/10665/324791/9789241515559-eng.pdf?ua=1 37 “Yemen Multisectoral Nutrition Action Plan (MSNAP) 2020-2023.” Republic of Yemen, March 29, 2020. https://mqsunplus.path.org/wp-content/uploads/2020/08/Yemen-MSNAP-FINAL_29April2020.pdf.; “Yemen Multisectoral Nutrition Action Plan (MSNAP) Monitoring and Evaluation Plan (M&E Plan) 2020-2023: An Accompanying Document to the Republic of Yemen’s Common Results Framework and Multisectoral Nutrition Action Plan.” Republic of Yemen, March 2020. https://mqsunplus.path.org/wp-content/uploads/2020/08/Yemen-MSNAP-ME-Plan-FINAL_29April2020.pdf.; “Yemen Multiple Indicator Cluster Survey 2006.” Ministry of Public Health and Population & UNICEF, 2006. https://mics-surveys-prod.s3.amazonaws.com/MICS3/Middle%20East%20and%20he%20Africa/Yemen/2006/Final/Yemen%202006%20MICS_English.pdf.; All “Standardized Monitoring and Assessment of Relief and Transitions (SMART)Survey Preliminary Results; “Yemen National Health and Demographic Survey (DHS) 2013.” Rockville, Maryland, USA: Ministry of Public Health and Population (MOPHP), Central Statistical Organization (CSO) [Yemen], Pan Arab Program for Family Health (PAPFAM), and ICF International., 2015. https://www.dhsprogram.com/pubs/pdf/FR296/FR296.pdf.; “Yemen: IPC Acute Food Insecurity Analysis - January - December 2020 (Issued October 2020).” Integrated Food Security Phase Classification, October 2020. https://reliefweb.int/sites/reliefweb.int/files/resources/IPC_Yemen_Acute_Malnutrition_2020JanDec.pdf .

29
Capacity Development for NIS within the Health Workforce
Table 6: Immediate Recommendations (Immediate-1 year)
Current Situation Summary & Key Findings
Key Proposed Activity(s) Key Stakeholder Responsible & Stakeholders Involved
Recommendation 1.5: Conduct a Rapid Human/Infrastructure Capacity Assessment for Data Management to Inform Trainings/Capacity Development Strategy
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making (Analysis &
Action) ▪ There is currently a lack of capacity for
sub-national staff to collect and submit quality data at sub-national levels in a timely manner.
▪ There has not been any capacity assessment of data management for nutrition.
▪ There are a number of trainings available for health workers, managers and Community Health and Nutrition Volunteers (CHNVs), but none of have a monitoring and reporting component.
▪ There is a lack of quality of data, often due to the fact that individuals have not been sufficiently trained on how to use the data collection forms and the value-added of the data, and use of data at the national and sub-national levels for decision-making.
▪ There is a lack of infrastructure (technology and equipment) to compile information in a timely manner.
▪ Assessment for capacity building should be for all implementing partners and not just for MOPHP
Conduct a rapid human /infrastructure capacity assessment for data management to inform training. The capacity should be assessed for: 1. MOPHP central level 2. MOPHP Governorate level 3. MOPHP District level 4. Health workers***(most important)-both community health and nutrition volunteers (CHNVs) and facility-based health workers 5. Implementing partners in nutrition and health staff instead of just M&E staff. ▪ Include a rapid assessment on what
infrastructure is available for human use including technology and equipment to compile information in a timely manner.
▪ Suggestion to adapt capacity assessment using IYCF-E Individual Capacity Assessment tool for Health and Nutrition Service Providers38
▪ Can be a part of the broader Capacity development framework/strategy MOPHP/UNICEF is working on
▪ Suggest a system to monitor the impact of the capacity development training to track effectiveness of training.
▪ A Technical Assistance Consultant Team
▪ MOPHP ▪ Nutrition Cluster
Dividing text Current Situation
Summary & Key Findings
Key Proposed Activity(s) Key Stakeholder
Responsible & Stakeholders Involved
Recommendation 1.6: Introduce Regular Quality Improvement Teams at Governorate and District-Level Data Review Meetings to Review Progress Against Targets for Key Performance Indicators in Scorecards and Feedback Mechanisms
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making (Analysis &
Action) ▪ There currently lacks any
kind of formal platform/process to use data for decision-making for nutrition at the sub-national level to monitor nutrition programming through available data consolidated from existing data collection forms and provide
▪ Quality data collection is driven by better systems through streamlined and harmonized indicators and collation systems and secondly by people being held accountable for quality
▪ To increase accountability for quality we suggest facilitating and institutionalizing regular GHO/N and DHO/N nutrition data review meetings (i.e., monthly or quarterly) through Nutrition Quality Review Teams (team members TBD).
▪ This is an open forum to provide peer-feedback on challenges, to conduct problem solving and look at what is working to make course changes.
▪ Targeted Technical Assistance Team (Consultancy)
▪ MOPHP Nutrition monitoring and reporting focal persons
▪ Governorate health Officers -Nutrition Coordinators (GHO-N)
38 “IYCF-E Individual Capacity Assessment Tool for Health and Nutrition Service Providers | Nutrition Cluster.” Accessed March 23, 2021. https://www.nutritioncluster.net/IYCF-E_Ind_Cap_Assessment

30
Current Situation Summary
& Key Findings Key Proposed Activity(s)
Key Stakeholder Responsible
& Stakeholders Involved feedback and conduct programme course correction
▪ Roles of Sub-National Nutrition Data Quality Improvement Teams
o Regularly review and clean nutrition data o Flag data errors and barriers to nutrition data
collection and integration o Analyse data to determine effectiveness of
changes o Ensured replenishment of nutrition commodities
and supplies o Scale up changes that led to improvement
Develop and use of job aids to inform GHO/Ns and DHO/Ns on appropriate nutrition reporting and monitoring practices Job aids also can be developed for health workers and CHNVs to reinforces collecting quality data-look at experience from EPI—empty posters with a data chart with key indicators where they can chart their progress- (Can link with scorecards) ---a quality improvement process. Can track key CMAM trends, etc.
▪ District health Officers -Nutrition Coordinators (DHO-N)
▪ Health Workers ▪ Community Health and
Nutrition Volunteers (CHNVs)
Table 7: Short-Term Recommendations (Immediate-1 year)
Current Situation Summary
& Key Findings Key Proposed Activity(s)
Key Stakeholder Responsible
& Stakeholders Involved Recommendation 1.7: Introduce routine monitoring and reporting on the effectiveness of capacity building/ training exercises with GHO, DHO and facility/programme staff utilizing available data from nutrition programme databases.
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making (Analysis &
Action) ▪ Yearly training for GHO and
DHO are undertaken to strengthen data collection and collation processes, and the use of data to feedback to health facilities. It is unclear what impact these trainings have on issues such as high numbers of districts with <1% defaulting and incomplete reporting from some districts.
▪ With available information in country, the dates for capacity building can be used to monitor the quality and completeness of reporting both before and after capacity building exercises. The impact of capacity building could be tracked in this way in all governorates and districts where trainings take place or a subsection identified as having issues with reporting and completeness and quality of reporting.
▪ Where capacity building does not lead to improvement, this could foster further engagement and/or further refinement of trainings and tools used, identifying where challenges remain, i.e., are trainings adequately focused on relevant material; are trainings adequately imparting knowledge; is the uptake of knowledge gained being translated into action to actually, impact data quality or effectiveness of programmes. Such analysis can also be used to assist in determining whether other types of training approaches would be better suited and to measure the impact of staff turn-over and capacities of the monitoring and supportive supervisory teams.
▪ Where issues which inhibit the effectiveness of capacity building exercises can then be addressed and the impact of changes made monitored through tracking changes in the quality and completeness of reporting within NIS programme data.
▪ Nutrition Cluster ▪ MOPHP Nutrition
monitoring and reporting focal persons
▪ UNICEF ▪ Governorate health Officers
-Nutrition Coordinators (GHO-N)
▪ District health Officers -Nutrition Coordinators (DHO-N)
Current Situation Summary & Key Findings
Key Proposed Activity(s) Key Stakeholder
Responsible & Stakeholders Involved
Recommendation 1.8: Implement Training in Monitoring and Reporting for Nutrition
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making (Analysis &
Action)

31
Table 7: Short-Term Recommendations (Immediate-1 year)
Current Situation Summary
& Key Findings Key Proposed Activity(s)
Key Stakeholder Responsible
& Stakeholders Involved ▪ There is no standardized
monitoring and reporting for nutrition training/module.
▪ Need to identify the key people to train for data quality
▪ Need to also consider the financing/infrastructure gaps also needed for those who are trained such as equipment-laptops, Internet, modems, printers and other incentives for data workers.
▪ Nutrition Cluster will soon facilitate broad level nutrition capacity discussion soon. On the job training and coaching training is very important.
Yemen needs more support for monitoring and evaluation competencies across all levels (central, Zone, Governorate, District, health facility levels). ** There is an urgency to monitor and report now at least at the national level—and this should be prioritized as soon as possible In order to institutionalize skills in M & E, we are proposing a routine M & E training every year. The intention of the training will be so that by the end of the session, participants will be able to: 1. Understand the monitoring and reporting for nutrition
programming in Yemen (i.e., CMAM, therapeutic feeding program)
2. Understand the indicators, data entry and data collection forms, etc.
3. Be able to accurately fill out the data collection forms and report as appropriate.
The nutrition monitoring and reporting module M & E training proposed participants are: ▪ MOPHP Central staff ▪ Nutrition Implementing partner staff ▪ Governorate Health Officers (Nutrition focal person) ▪ District Health Officers (Nutrition focal person) ▪ Health Workers39 ▪ Community Health and Nutrition Volunteers (CHNVs) ▪ Need to map out all of the existing trainings and
evaluate the monitoring/reporting components. This module should be integrated into the CMAM and CHNV training
▪ Need to develop the nutrition monitoring and reporting training module
▪ Consider on-the-job training as when on-the-job training was implemented for Therapeutic Feeding Centres there was a decrease in defaulter rate in TFCs
▪ Targeted Technical Assistance Team (Consultancy)
▪ MOPHP ▪ MOPHP Nutrition
monitoring and reporting focal persons
▪ Nutrition Cluster implementing partners
▪ Governorate health Officers -Nutrition Coordinators (GHO-N)
▪ District health Officers -Nutrition Coordinators (DHO-N)
▪ Health Workers ▪ Community Health and
Nutrition Volunteers (CHNVs)
Table 8: Longer-Term Recommendations (1-3 years)
Current Situation Summary
& Key Findings Key Proposed Activity(s)
Key Stakeholder Responsible
& Stakeholders Involved
Recommendation 1.9: Strengthen Monitoring and Evaluation Department within Nutrition Department of MOPHP
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making
(Analysis & Action) There are only 2-3 staff working in MoPHP in Sana’a who are designated for M & E and no staff in MoPHP in Aden
Strengthening the M and E department at MoPHP at the subnational level in terms of continued hands-on mentoring and provision of tools to support M and E. e.g., computers
Consider secondment of an M & E for Nutrition Advisor (1-3 years
▪ MOPHP
Strengthening Reporting through the DHIS-2 and Mobile Applications
39 The Primary Healthcare Health Unit and health facility---only have 1-2 staff in the unit and have competing duties and high demand. They are in charge of integrated activities for registration.

32
Table 9: Immediate Recommendations (Immediate-1 year)
Current Situation Summary
& Key Findings Key Proposed Activity(s)
Key Stakeholder Responsible
& Stakeholders Involved
Recommendation 1.10: Increase and further systemize use of Mobile Technologies to improve feedback and real time analysis of information from primary
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making
(Analysis & Action)
While relatively rudimentary, WhatsApp and other messaging services are currently used widely used among nutrition stakeholders for real time communication of issues faced at facility or district level, including issues around stock, staffing and technical feedback and follow up. There is substantial room to further formalise the analysis and use of information reported through WhatsApp, for increased accountability through the collation and quantification of reported issues to identify and prioritise actions to address bottlenecks.
• Expand and routinise the grievance reporting system used by staff in TFC to staff working OTP and preventive programming to increase accountability and allow for faster response from the DHO, GHO and Cluster level to respond to needs of programmes.
• Carry out regular analysis of the number and seriousness of grievances and requests submitted through WhatsApp groups and messages on a regular basis can improve an understanding of common bottlenecks and inform actions to address them.
• The “TFC grievance reporting” used by WHO supported TFC staff provides an effective and feasible option for increasing real time feedback and information on key issues such stock supply levels, staffing and incentives, as well as providing a channel for communication on technical issues.
▪ Nutrition Cluster, UNICEF, WFP, MOPHP and Nutrition Cluster partner NGOs.
Table 10: Immediate Recommendations (Immediate-1 year)
Current Situation Summary
& Key Findings Key Proposed Activity(s)
Key Stakeholder Responsible
& Stakeholders Involved
Recommendation 1.11: Develop and disseminate a clear plan to further Define How Nutrition will be Integrated with the District Health Information Systems (DHIS-2) and Increase Awareness and Engagement from Nutrition Stakeholders.
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making
(Analysis & Action) The scale-up of the existing District Health Information System (DHIS-2)40 information systems’ platform-through a nutrition-focused module will facilitate relevant facility and community-based nutrition data collection and analysis. Current efforts to further develop and roll out the DHIS-2 are not visible or well understood by many stakeholders inside and outside of the country, including key donor agencies and some UN agency staff. How nutrition will be incorporated within the DHIS-2 and what proportion of nutrition programming data will be
• Mapping relevant stakeholders and undertaking an awareness and engagement campaign to leverage resources and skills of humanitarian Clusters, UN and donor agencies.
• Undertake a series of workshops and wider discussions to define what aspects of current nutrition reporting will be migrated to the DHIS-2 and how this will occur will be vital to ensure optimum integration of nutrition within the system while avoiding overburdening of the system.
• Wide engagement of nutrition stakeholders in the country towards defining what can be incorporated and how the current data value chain and related databases and information products would be integrated or interoperable will increase uptake and use.
• In the interim, before the DHIS-2 is rolled out, encouraging use of nutrition and health data, be it through existing or planned databases, data
▪ MOPHP, WHO, UNICEF, and engagement from Nutrition Cluster, and donor agencies.
40 DHIS2 is an open-source platform for national health management information systems (HMIS). It is a flexible, web based scalable HMIS solution, enabling data entry, management, validation, analysis and visualization of aggregate, event and individual level data. The software has been field-tested and continuously improved for over 15 years. As of 2018, DHIS2 has been implemented in over 57 low-income and middle-income (LMIC) countries, and has become the HMIS software of choice in these contexts and has also been adopted for education, WASH, nutrition and other sectors in some countries.

33
Table 9: Immediate Recommendations (Immediate-1 year)
Current Situation Summary
& Key Findings Key Proposed Activity(s)
Key Stakeholder Responsible
& Stakeholders Involved
migrated to the system is not yet well defined.
visualization tools and scorecards should increase uptake when the system is rolled out.

34
4. MAXIMISING DATA VALUE: Opportunities for Transforming the
Nutrition Data Analysis and Use
4.1 Overview & Current Situation and Key Challenges
A conceptual framework for the nutrition data value chain is included in Figure 10 of this report. It charts the value chain from data prioritization and collection through to analysis and use of data to influence decision making. The diagram presents the flow of nutrition data in a circle from prioritization and creation through to decision making, although in practice the steps within the data value chain are not strictly sequential, they are more overlapping.
Applying the framework to this review of the information systems for nutrition Yemen, there appears to be a strong focus on the early stages of the data value chain centred on the creation, collection, and curation of data, with somewhat less focus on the routine and systematic analysis, translation and dissemination and decision making.
Among several key informants consulted for this review, it was widely understood that the primary value of information products. These products act as a tool for accountability through which the Cluster can communicate how available resources have been allocated to result in an agreed set of outputs, namely a given number of admissions (relative to calculated caseloads) into programmes which achieve outcome indicators that are within the Sphere standards thresholds (e.g., achieved coverage and cure rates over 75% and low non-response, death and defaulter rates).
These information products tend to provide little indication of how information presented has been or will be used to inform decision making or to identify potential underlying reasons for trends presented, for example through triangulation among indicators presented or with other information from other related clusters, such as WASH, food security or health.
At a subnational level, the mechanisms to provide those involved in the production and collation of data throughout the data value chain, or those tasked with decision making around resource allocation and prioritization, with feedback and analysis on the data they produce, and use are also not well defined. As such, the data value chain in Yemen remains primarily one-directional and accountability focused.
Data is created, curated, and fed upwards from the facility to the district, governorate, zonal and finally national levels. While programme data is used to provide feedback to GHO, DHO, facilities and partner NGOs? NOGs, this does not occur in a systematic or routine way and it is not clear how feedback directly promotes specific actions in response discernible trends.
This is in part due to the division of labour within the cluster. The primary mandate of staff involved in information management of nutrition data can be broadly characterised as ensuring the timely production of data to be used for ensuring accountability of the cluster against agreed targets. However, no one individual or contracted organisation has a mandate to ensure available data is analysed and disseminated in a form which adds direct value to decision makers seeking to effectively allocate resources for maximum impact on increasing programme quality and coverage.
The following section describes in some detail how nutrition data is currently analysed and used, and outlines some of the specific complexities and challenges which currently inhibit its use.
4.2 Current Analysis of Programme Data to Guide Decision-Making
4.2.1 Facility and Community Level (Recommendation 2.6)
While there are standard trainings in place for CHNV’s and facility-based health workers (as described in section 2.4 ‘Existing Training’), there are no existing instances of facility-level approaches to encourage analysis and use of data at the facility level, such as the CMAM surge approach41 or District Health System Strengthening approaches.
41 The CMAM Surge approach complements routine CMAM services by improving health staffs' use of facility data and knowledge of the local context to better anticipate, plan for, respond to, and bounce back from these increases in demand for acute malnutrition treatment services.

35
Several KIIs and participants within consultative meetings stressed that there is a need for more engagement and training for health facility workers and CHNV’s to facilitate responsive nutrition programming that feeds back into the higher levels (e.g., district, governorate, central).
In many country contexts, recent years have seen increased efforts to mobilise community and frontline health worker knowledge to assist in early detection of spikes in of acute malnutrition and use data produced at the facility level, for instance through the CMAM Surge approach42 developed by Concern International, the District Health System Strengthening Approach developed by Action Contre La Faim (ACF),43 and various similar country and organizational programming approaches.
These approaches use facility health worker knowledge and facility and/or district level data to identify what constitutes “normal” caseloads of admissions which can be managed with available resources. The aim being to provide the most appropriate support to health facilities capacity to cope with increases in caseload and empower health facility and district level staff to utilize available data from their programme or district, alongside local knowledge to identify drivers of seasonal trends, including both demand side (e.g., distance to health facility, women’s workload etc.) and supply side factors (e.g., stock outs and health worker absenteeism in facilities etc.).
While information produced through facility level analyses may also feed into the wider sub-national and national NIS, they constitute a valuable source of nutrition information in and of themselves When undertaken and effectively acted upon at the facility level. Analysis can also feed into the wider national and sub-national NIS providing information on seasonal and context specific drivers of malnutrition and service utilization to inform annual planning for increased screening, pre-positioning of supplies and human resources to enable timely and preventative actions. This review did not find any instances of the use of such approaches in Yemen.
There was consensus among KII that there is room for further mobilization and leveraging of health facility level data and knowledge to increase rapid screening and referral to programmes and identify and address limiting factors in service utilization.
4.2.2 District and Governorate Level Analysis and Use of Data (Recommendations 2.3 – 2.5)
DHOs are the first government administrative level point of contact that health facilities report to within the health system. DHOs play a vital role not just in their role in collecting data from health facilities but also in providing feedback to programme staff about issues reported within programme data, such as changes in acute malnutrition admissions44, community and health facility-based acute malnutrition screening, nutrition programme outcomes and issues around supply chain management for both inpatient and outpatient nutrition services. They act as the primary connectors from the health facility/nutrition programme level to the GHO and wider sub-national and Sanaa and Aden MOPHP and Nutrition Clusters at hub/zonal level.
Downstream feedback from GHO to DHO and implementing partner NGOs and upstream feedback from GHO to zonal and national Nutrition Cluster are meant to occur on a regular, usually monthly, basis. Feedback should be provided on both the quality and content of monthly reporting from DHOs. However, it was understood that no set analysis or feedback tool is consistently used for this feedback process. Instead, the picture is that feedback tends to be context specific, focusing on progress towards targets, admissions, reporting, programme outcomes, and other indicators flagged as necessary for follow-up by the Sanaa and Aden MOPHP or zonal/IMO or national cluster coordinators, etc.
This review did not find evidence of readily available tools or guidance which supports the use of data to I) identify trends or breaches of agreed thresholds in specific indicators, 2) trigger a set of related commensurate actions where trends or breaches of agreed thresholds are identified, 3) track the impact of actions taken within the NIS.
In practical terms, this means that where programme data shows patterns such as: large or continuous changes in admissions; low or decreasing numbers of screening; low or consistently unrealistically high cure rates; repeated stock outs or low reporting rates etc. this is not systematically flagged within the NIS to trigger commensurate actions and follow up in response.
42 Concern International, Evaluations of CMAM Surge Approach. 2020. https://www.concern.net/insights/evaluations-cmam-surge 43 ACF International. Health System Strengthening: From Diagnosis to Planning. 2017. https://www.actionagainsthunger.org/sites/default/files/publications/Action_Against_Hunger_HSS_Approach_Summary_2017.pdf 44 Attendance data is not included in the aggregated database.

36
Current tools and training for zonal Cluster Coordinators and Governorate and District Health Offices are more focused on ensuring a measure or accountability through meeting predefined data quality criteria and reporting progress against targets and thresholds for programme outcome indicators. As such, the analysis of data and the linking of analysis to commensurate actions occurs in an ad-hoc fashion, depending upon the capacity and motivation of data users across the data value chain.
There is a lack of routine analysis of trends in programme data by Governorate or District provided to zonal Clusters, GHO or DHO which could help them understand trends over time or between indicators, or to compare trends to other districts or governorates. The lack of routine subnational analysis limits the scope for triangulation of indicators such as admissions, screening data, stock use, and number and location of programmes for identification of programming bottlenecks.
As such, in a particular district, there may be patterns such as reduced screening numbers alongside reductions in admissions, continuous stock outs and increasing defaulter rates, or steady screening numbers and reporting rates alongside large or continuous increases in admissions yet there is no system which would necessarily flag or highlight this. Rather it is up to the discretion and capacity of the GHO or relevant other Nutrition Cluster staff to identify this, act upon it and follow up.
Further to this, the criteria currently used by zonal and national Nutrition Cluster IMOs, and GHO and DHO flag programmes reporting poor programme outcome indicators such as low cure rates / high defaulting and non-response rates. However, there is no means through which reporting of unrealistic outcome indicators such as consistent or very high cure or low default rates are flagged as potentially problematic.
While the approach for data processing, collation and sharing follows a set routine, the use of data at the zonal Nutrition Cluster level and how analysis undertaken at the zonal level is shared with other zonal UN hubs and the national level vary.
Routine sharing of analysis occurs through Nutrition Cluster meetings. However, during interviews with zonal cluster IMO coordinators, it was mentioned that the level of analysis varies across zonal clusters and clusters in one area are not necessarily aware of the level or type of analysis that informs other zonal clusters.
A review of data Nutrition Cluster monthly summary databases from 2017 to 2020 shows a substantial number of districts reporting 0% defaulting45, often over prolonged periods. While 0% defaulting is possible in a well-managed programme with few demand or supply side issues and low numbers of admissions, 0% defaulting across an entire district with high numbers of admissions over several months is highly unlikely. Current tools and training for data quality criteria do not equip those producing or analysing programme outcome data to identify and mark such cases as potential indicators of poor reporting rather than exceptional performance.
4.2.3 National level Analysis and Use of Data (Recommendations 2.3 – 2.5)
Nutrition Summary Monthly Databases files are provided to iMMAP46, an organisation contracted by the Nutrition Cluster since the last quarter of 2020, to support humanitarian data work in the WASH, health and Nutrition Clusters in Yemen, to produce information products such as coverage maps, graphs for use in PowerPoint presentations, etc. The methodology and content of these products has been largely consistent over time, both before iMMAP were contracted to support and previous to 2019 when the Nutrition Cluster produced these information products themselves.
There is a monthly trends analysis PowerPoint and ‘Monthly Summary Database Excel files’ normally shared with all Nutrition Cluster stakeholders/implementing partners on the Nutrition Cluster distribution list and posted on the Nutrition Cluster webpage. There is also usually a quarterly Nutrition Cluster- donor meeting where donors are updated on the nutrition situation in the country and response, funding, challenges, and key issues. The focus of these information products tends to be on the estimated caseloads, targets and coverage of various nutrition services provided by the cluster. Coverage against targets was a key factor in the identification of priority districts for the Nutrition Cluster in 2020. Priority districts being those districts with high to very high prevalence of acute malnutrition, and districts with low treatment coverage against
45 For instance, 28 districts with over 100 children discharged with less than 1% defaulting in 2020, as reported in the Yemen Nutrition Cluster Monthly Summary Analysis. January – December 2020. 46 About iMMAP. https://immap.org/who-we-are/

37
target of ≤49 percent, alongside districts where IPC for acute malnutrition projected deterioration of nutrition situation or particularly high burden of IDPs.47
In keeping with Global Nutrition Cluster standard practice, the Yemen Nutrition Cluster calculates the expected caseload in need of treatment for SAM through OTP using three data sources: Population estimates of the number of children under 5 years of age; Prevalence estimates of AM from survey data, and an incidence correction factor. The expected caseload against which coverage is measured is generally imprecise, and all variables included in the calculations for expected caseloads can contribute to a disparity between the expected caseload based on available information for estimating caseload, and subsequent actual caseload treated over a planning period. Imprecision can be due to a range of factors, including a lack of timely and accurate population size and malnutrition prevalence, and incidence estimates.
The monthly summary reports are also made publicly available via UNOCHA website48 alongside the finalised information products. The main indicators covered in the information products are coverage against targets for curative programming for acute malnutrition, preventative micronutrient and blanket supplementary feeding programming and related trends in admission, and reporting rates trends, alongside percentage of stockouts-the supply availability analysis (only for ready to use supplementary foods (RUSF) and Wheat Soy Blend Plus (WSB+)-a supplementary food) and key acute malnutrition treatment outcome indicators (cure, defaulter, death rates) in CMAM programmes.
From KII’s and analysis of Nutrition Cluster information products, it appears the primary value of these products produced from the monthly summary reports is as tools for accountability and advocacy for the Nutrition Cluster, where the cluster can communicate how resources received and distributed have resulted in a set of outputs such as services available and utilized relative to a measure of population need.
Some interviewed stakeholders/participants in consultations revealed dissatisfaction in the focus in these information products on coverage targets and the output-oriented presentation of data, without any wider analysis of trends, contextualisation of figures presented or cross tabulation of figures to reveal underlying and potentially causative factors. While the Nutrition Cluster analyses and responds to trends in service use due to seasonality or climate or conflict related shocks and disease outbreaks, this is not always systematically or clearly communicated to a wider set of stakeholders, both downstream to GHO, DHO and facility staff, and upstream at national level to donor agencies and programme staff in other clusters/ sectors.
A key limiting factor in this respect is that the Nutrition Cluster information products produced through the existing information systems are designed to primarily function as a means of providing accountability regarding a set of outputs having been achieved, rather than as a possible means to decipher differences in programme performance or nutrition population-based changes/improvements.
A secondary and related factor are limitation with regards to available human resources, such as a dedicated member of staff within the Nutrition Cluster on nutrition information systems, or contracted agency or implementing partner, tasked with facilitating analysis, dissemination and use of available data with an objective of producing a sound information base for programmatic/operational decision making.
At present, the zonal IMOs and national Nutrition Cluster staff tend to be mandated to work in either producing and collating information in a form suitable to inform current global standardized Nutrition Cluster information products, or programme and operational tasks. The challenging work context and high workloads make it difficult for staff to make time for additional or more exploratory analysis and communicating it to promote action on the findings when this does not fall specifically within the mandate of any one staff member.
A key source of data used within the Nutrition Cluster remains population-based surveys (PBS) and the routine (Standardised Monitoring and Assessment of Relief and Transitions (SMART) assessments, which are especially key in the planning process to determine the People in Need (PIN) estimates for acute malnutrition (SAM, MAM and SAM with complications and BSFP). Other PIN estimates in the Nutrition Cluster for interventions such as IYCF, MNP, vitamin A do not rely on SMART surveys data.
47 Yemen Humanitarian Fund (YHF) First Standard Allocation 2020 – Strategy. https://www.unocha.org/sites/unocha/files/dms/YHF_SA1%20-%20Strategy%20Paper.pdf 48 “Nutrition | Humanitarian Response.” Accessed April 25, 2021. https://www.humanitarianresponse.info/en/operations/yemen/nutrition.

38
However, challenges around the timely availability of survey data in Yemen, severely hamper their use for programmatic decision-making. The two IPC acute malnutrition analyses undertaken in the northern and southern governorates of the country in 2020 have progressed in some ways towards addressing the sparsity of available PBS data. The use of other forms of data such as routine nutrition programme data remains underexploited for programming purposes, while data produced through the WHO supported health facility nutrition monitoring (through their national surveillance system sites) is also yet to be incorporated into PIN analysis within the cluster, or to be triangulated with other sources of nutrition information through a clearly articulated framework or strategy around the use of data use for decision making.
A key limitation regarding use of prevalence estimates from representative population-based surveys such as SMART surveys is that they provide only a snapshot of the nutrition situation while the prevalence of various forms of malnutrition in a population often tends to be dynamic and changes over time. Information on population size in Yemen also faces limitations, as it has relied on modelled projections since 2004 when the last census was carried out in the country. Coverage data from Nutrition Cluster programme data in Yemen, as in other contexts, should thus be interpreted with caution.
Much of the cluster coverage reporting materials made available through online UNOCHA humanitarian response and Nutrition Cluster websites is typically against targets, a proportion of the overall and target caseload for each intervention, deemed within the capacity of the cluster to reach, used for planning and monitoring.
As stated above, the key informants consulted for this review pointed to the value of available information products as important tools for accountability through which the Nutrition Cluster can present how resources received and distributed have resulted in a set of outputs such as services available and utilized relative to a measure of population need. However, the restricted use of data primarily for monitoring and accountability purposes, without further context or analysis, results in limited utility for decision makers who wish to use data produced through the NIS for programmatic decision making at a more granular level to expand the reach and quality of services.
4.3 Opportunities for Expanded Use of NIS Programme Data for Improved Programme Coverage and Quality
The aim and priority in community-based services for the management of acute malnutrition is to reach as many of those affected, at an early stage, and ensure attendance until discharge criteria are met. Analysis of programme data such as admissions, reporting rates, community screening and mobilization, supply chain use and the number and type of active programmes by district, can together support efforts to support the achievement of these aims.
An expanded focus within Nutrition Cluster information products and reporting incorporating more analytical focus and contextualization, clearly linking how data is being used to inform decisions may increase the relevance and usefulness of information products for use both within and outside of the Nutrition Cluster. The following section outlines the potential value and some of the complexities of using programme data produced through the NIS to inform decision making to achieve increased coverage and quality of programmes.
4.3.1 Current Analysis of CMAM and Related Nutrition Data (Recommendations 2.3 – 2.5)
CMAM admissions for MAM and SAM, and numbers of beneficiaries reached for preventative nutrition services, are key indicators in nutrition information systems in Yemen. New Admissions figures provide the numerator for coverage calculations which make up a key component of monthly Nutrition Cluster reporting information products such as coverage maps and trend analysis.
The Yemen Nutrition Cluster information products, in keeping with Global Nutrition Cluster norms for reporting, also chart admissions for CMAM services alongside reporting rates to aid interpretation of admission trends. New admissions are presented on monthly basis as a marker of performance against targets and marker of changes in the burden in the population.
The Yemen Nutrition Cluster, at a national level has also undertaken more in-depth analysis of admissions trends, examining changes in admissions alongside changes in reporting rates and community mobilisation at a district level to determine where changes in admission may have been due to changes in reporting, community screening and mobilisation, or actual changes in burden in the community.

39
These deep dive analyses were undertaken in 2019 and 2020 and presented in the form of a Power Point presentation. The analyses only examine year on year trends and provide only counts of districts for cross tabulation and trend analyses, rather than identifying potential causes of change in admissions in specific districts. In addition to these national deep dives, IMO at the subnational level also sporadically produce more in-depth analysis of admissions, depending on capacity, time and motivation. No routine triangulation of trends in programme data was with other sectoral information was noted as being undertaken within the Nutrition Cluster.
Routine analysis of nutrition programme data presented in Nutrition Cluster Information products are not situated within a clearly defined or communicated framework or theory of change for how they should be used to inform decision making on how resources are directed to increase support or expand Nutrition Cluster programming within the country.
While prevalence estimates of GAM from PBS are used by clusters such as food security, WASH and health cluster for geographic prioritisation of the sectoral humanitarian response, this review found only limited evidence of programme data being used by other clusters for prioritization of programming. The WASH cluster routinely presents nutrition admissions data alongside health and WASH specific data to explain programmatic decision making.49
4.3.2 Factors Influencing Interpretation of Programme Data in Yemen (Recommendations 2.2 – 2.6)
The use of programme data to determine the actual burden of malnutrition in the population relative to other factors related to programme performance and utilization is complicated by several factors. These limitations are explored in some detail below. These limitations and the potential for confounding in interpretation of programme data is presented not as an argument against interpretation of available data but rather as justification for why further analysis and triangulation of available data is both possible and warranted.
Among potential explanatory factors for changes in acute malnutrition admissions in each area are:
1) Changes in the number and characteristics of programmes reporting data.
2) Changes in the number of programmes active.
3) Changes in community mobilisation and screening.
4) Other factors, such as community uptake of services, an example being the widespread decrease in nutrition service utilization globally due to COVID-19; or duplication or non-registration of admissions.
In any given context, it is likely that in changes in admissions over time may be due in part to a combination of the above factors, as well as being due to changes in the actual burden in the community. Even where changes in admissions can be linked to a change in burden, the change in burden itself could be due to changes in incidence or in the size and spread of populations within the capture area of programmes.
At present the variable most often used to contextualize admissions in Nutrition Cluster information products is the reporting rate. The reporting rate is particularly vital to understand trends in admissions as low reporting prevents an understanding of actual service utilization. Reporting can also be interpretated alongside other information, such as past trends in a given district on stock use, screening and admissions to give an indication if it may reflect whether programmes are operational, and clients are using the service.
Community screening is also a vitally important indicator of programme performance and can be used to contextualize admissions numbers through cross tabulation to discern potential causes of changes and determine changes in indicators of programme performance (i.e., changes in community screening), versus changes in burden. Information is reported and available of screening at district level but is far less reported in Nutrition Cluster information products.
The primary use of the acute malnutrition admissions, reporting, screening and outcome data should be to measure the functioning of the services and make adaptations to improve its efficiency assuming that changes in efficiency will eventually result in positive changes in impact. While the multiple potential confounding factors explored above limit the interpretation of changes in admissions
49 See for example: Yemen WASH Cluster; Coordination Meeting 1st December 2020. Available at: https://www.humanitarianresponse.info/en/operations/yemen/water-sanitation-hygiene

40
numbers, they by no means prevent it. Data is available in Yemen on three of the most important potential explanatory factors at a district level and can be used to analyse admission data to determine where they may indicate a change in population burden and where they may point to other factors such as improvements in community screening and referral or number of programmes active or reporting in a given district.
Other figures reported from nutrition programmes such as screening numbers, reporting rates, stock use and outcome indicators provide valuable information to help understand where programmes are performing well or may need further support and follow up.
All of this information can be further contextualized and interpreted in light of information from other relevant sectors and qualitative information from staff throughout the various levels of the nutrition and wider health and humanitarian system in country.
4.3.4 Using Acute Malnutrition Admissions data to Determine Effective Programme Functioning and the Impact of COVID-19 (Recommendations 2.2 – 2.5)
As previously noted, acute malnutrition admissions data can help us understand issues around programme performance and utilization: e.g., a decrease in admissions, while other factors such as reporting, community screening and number of programmes active remain unchanged, may point to other factors related to supply and demand side factors impacting service utilization.
An example of where such an analysis could aid decisions makers is the impact of COVID-19 on programme admissions over the last three quarters of 2020. Globally programme admission to nutrition programmes and health and other services fell drastically. In Yemen, admission in December 2020 were down approximately 25% for January through December 2020, compared to 2019. Some key informants hypothesised that this decrease was partly due to the impact of COVID-19, which led to fear of accessing services from communities, increased health worker absenteeism and supply disruptions as a similar phenomenon was seen in other contexts globally,
However, it was also noted that the onset of COVID occurred alongside an unrelated issue within the MOPHP and Nutrition Cluster reporting lines which led to a large decrease in percentage of programmes reporting data to the cluster (reporting rates). In addition to this the Yemen Nutrition Cluster experienced a decrease in funding relative to estimated need in 2020 (71% of appeal funded) compared to 2019 (81% of appeal funded).50
This could also be expected to have resulted in changes in the scale and quality of services provided and effective coverage. However, the lack of any available analysis of how changes in funding may explain or relate to changes in data reported through the NIS (such as number of active programmes, stock use, screening or outcome indicators) makes it difficult to determine the impact of reduced funding relative to other factors.
In March, 2020 the Nutrition also introduced adapted nutrition protocols for outpatient Treatment for Acute Malnutrition including simplified admission criteria using mid-upper arm circumference (MUAC) rather than weight for height with further implications for effective programme functioning.51
Some key informants voiced frustration at the lack of analysis of these issues in ways which could have disentangled the various potential drives of decreased admissions. Real time in-depth analysis of changes in admissions, accounting for changes in reporting and screening and triangulated with other factors such as use of other services (e.g., education, food security programming, other health services) could have helped disaggregate real decreases in admissions versus unrelated decreases in reporting or other factors to inform an appropriate programmatic response.
The lack of real time analysis of how COVID-19 and other factors converged to impact programme utilization and effective coverage and reporting provides an indication of the wider underlying weaknesses in the system of analysis of available data within the NIS.
4.3.5 Monitoring how the Number of Programmes Impacts Programme Performance and Reporting (Recommendations 2.2 – 2.6)
50 UNOCHA. Financial Tracking Service. Yemen. 2020. https://fts.unocha.org/countries/248/summary/2020 51 Yemen Country Office Humanitarian Situation Report. Reporting Period 1 January – 31 Dec, 2020. https://www.unicef.org/media/93126/file/Yemen%20Humanitarian%20Situation%20Report,%20End%20of%20Year%202020.pdf

41
A potential related use of admission data is to evaluate how changes in the number of programmes active impacts admissions, outcomes, and related measures of programme quality such as screening. For instance, we may intuitively expect that for every additional programme active in a district this would, all other things being constant, result in an increase in the number of admissions in the district. A brief examination of monthly summary databases in Yemen over the years 2017 to 2020 shows a surprisingly weak relationship between changes in the number of OTP programmes active in a given district and changes in the number of admissions.
This may be due other factors with a significant impact on admissions trends. A range of both supply and demand side issues can impact service utilization, for instance programmes may not be adequately close to populations with most need or changes in the nutrition situation within populations may impact the need for services, repeated stock outs of health worker absenteeism may impact client confidence, or low levels of screening or community mobilisation may mean cases are not being identified and referred within the community, or an improvement. Analysing how changes in the number of programmes active impact on admissions, reporting rates, screening numbers and stock use, can provide an important measures’ of how and where programmes are performing well or may need greater support.
4.4 Recommendations for Maximising Data Value: Opportunities for Transforming the Analysis and Use of Nutrition Data
Defining and Expanding the Analysis and Use of NIS Data in Yemen
Table 11: Immediate Recommendations (Immediate-1 year)
Current Situation Summary
& Key Findings
Key Proposed Activity(s) Key Stakeholder Responsible
& Stakeholders Involved
Recommendation 2.1: Develop a data use and communication strategy through the Nutrition Information Technical Working Group.
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making
(Analysis & Action)
Current Situation Summary & Key Findings
• There is a lack any clear framework or theory of change for how data generated through the NIS should be acted upon, or how it does or should impact resource allocation for nutrition programming within the country.
• In particular, there is a lack of any common understanding among nutrition stakeholders on what information available is or should be being used to identify, address and follow up on supply side issues in programming which limit programme quality and coverage (e.g., low programme availability, low screening rates, stock outs, staff absenteeism and capacity constraints etc.)
• There is currently a lack of a clear strategy for communicating data to different stakeholders in a form tailored to their specific needs in a routine and timely manner.
Key Proposed Activity(s) The nutrition information technical working group provides a suitable platform through which nutrition stakeholders in Yemen can collectively agree upon and articulate a strategy for data use and communication, outlining the needs of stakeholders across the data value chain, what data they currently use in their roles and how more in-depth analysis and routine analysis and dissemination can help them increase programme coverage and quality.
More specifically such a strategy should: 1. What information is currently used to identify and address supply side issues in programming
and to mobilize (internally and externally) and target resources (be it qualitative information shared within the cluster, programme data, PBS, etc.).
2. What stakeholders (from the district, governorate, zonal, national, and international UN and donor agency levels) use what information,
3. what indicators and level of analysis should be communicated to them on routine basis?
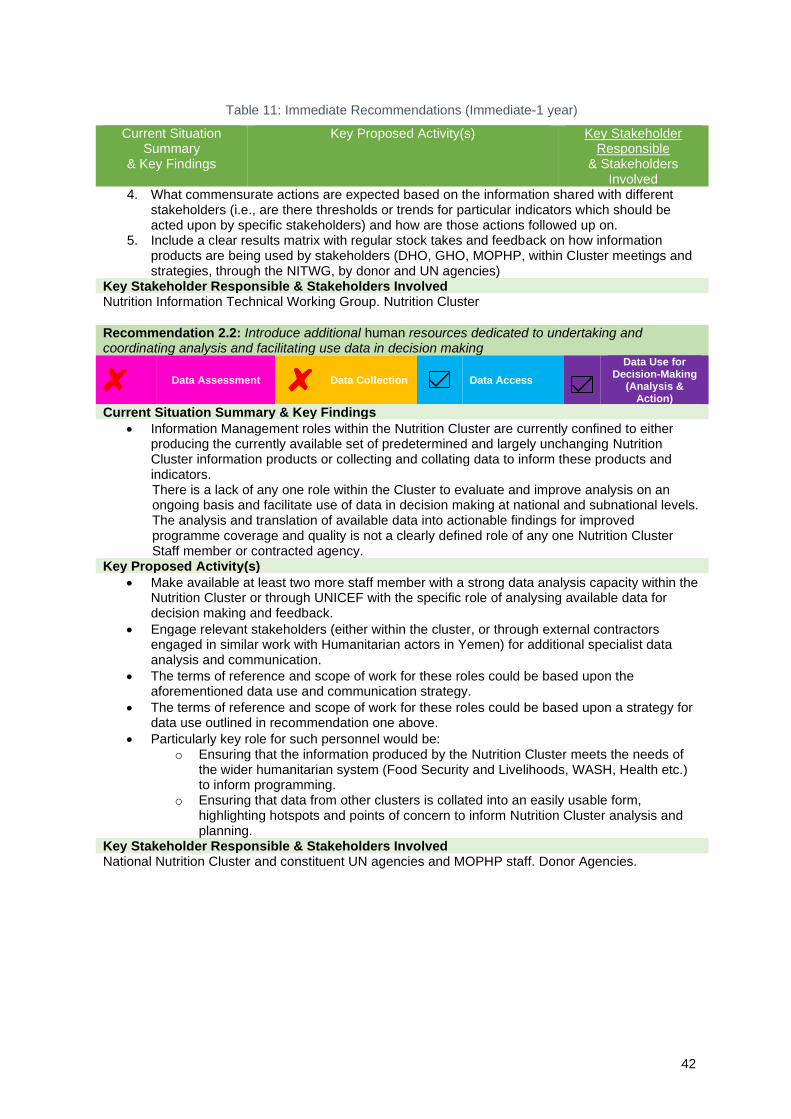
42
Table 11: Immediate Recommendations (Immediate-1 year)
Current Situation Summary
& Key Findings
Key Proposed Activity(s) Key Stakeholder Responsible
& Stakeholders Involved
4. What commensurate actions are expected based on the information shared with different stakeholders (i.e., are there thresholds or trends for particular indicators which should be acted upon by specific stakeholders) and how are those actions followed up on.
5. Include a clear results matrix with regular stock takes and feedback on how information products are being used by stakeholders (DHO, GHO, MOPHP, within Cluster meetings and strategies, through the NITWG, by donor and UN agencies)
Key Stakeholder Responsible & Stakeholders Involved Nutrition Information Technical Working Group. Nutrition Cluster
Recommendation 2.2: Introduce additional human resources dedicated to undertaking and coordinating analysis and facilitating use data in decision making
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making
(Analysis & Action)
Current Situation Summary & Key Findings
• Information Management roles within the Nutrition Cluster are currently confined to either producing the currently available set of predetermined and largely unchanging Nutrition Cluster information products or collecting and collating data to inform these products and indicators. There is a lack of any one role within the Cluster to evaluate and improve analysis on an ongoing basis and facilitate use of data in decision making at national and subnational levels. The analysis and translation of available data into actionable findings for improved programme coverage and quality is not a clearly defined role of any one Nutrition Cluster Staff member or contracted agency.
Key Proposed Activity(s)
• Make available at least two more staff member with a strong data analysis capacity within the Nutrition Cluster or through UNICEF with the specific role of analysing available data for decision making and feedback.
• Engage relevant stakeholders (either within the cluster, or through external contractors engaged in similar work with Humanitarian actors in Yemen) for additional specialist data analysis and communication.
• The terms of reference and scope of work for these roles could be based upon the aforementioned data use and communication strategy.
• The terms of reference and scope of work for these roles could be based upon a strategy for data use outlined in recommendation one above.
• Particularly key role for such personnel would be: o Ensuring that the information produced by the Nutrition Cluster meets the needs of
the wider humanitarian system (Food Security and Livelihoods, WASH, Health etc.) to inform programming.
o Ensuring that data from other clusters is collated into an easily usable form, highlighting hotspots and points of concern to inform Nutrition Cluster analysis and planning.
Key Stakeholder Responsible & Stakeholders Involved National Nutrition Cluster and constituent UN agencies and MOPHP staff. Donor Agencies.

43
Facilitating Real-Time Analysis Clearly Linked to Actions for Improving Programme Performance
Table 12: Immediate Recommendations (Immediate-1 year)
Current Situation Summary
& Key Findings
Key Proposed Activity(s) Key Stakeholder Responsible
& Stakeholders Involved
Recommendation 2.3: National Data Repository linked to Joint Dashboard to facilitate increased analysis and feedback at the Governorate and District levels
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making
(Analysis & Action)
Current Situation Summary & Key Findings
• The mechanisms in place to provide stakeholders who produce and use data across the data value chain, with feedback and analysis on the data they produce (e.g., at facility, district or governorate level) are not well defined across contexts in Yemen. For instance, no routine or systematized analysis is produced for use by MOPHP staff or NGOs at the Governorate, or District Levels.
Key Proposed Activity(s) Develop a national data repository comprising all routinely updated nutrition data and a dashboard utilizing this combined database, capable of autogenerating district and governorate level reports with district and governorate level trend analysis of routine programme data, alongside other relevant key indicators, such as data from health facility nutrition surveillance. Such a dashboard should include relevant indicators currently reported within the Nutrition Cluster monthly summary reports, with suggested key indicators of focus being: admissions; percent national burden of admissions; reporting rate; number of children screened; stockouts; number of programmes; coverage against caseload and targets. Display could be searchable by:
• Services (SAM; MAM; PLW SFP etc.); Zone/ Governorate/District/Combination thereof and by time trends with figures displayed by time trend lines and graphs and tables and should be available in Arabic as well as English. The database should reflect all relevant available indicators currently available through the monthly summary database, as well as additional relevant available information such as screening numbers and information on stock use and stock outs,
• A set of rules can be applied to data to discern trends by Geographic region. For instance. flags could be applied where there are:
▪ Repeated or cyclical increases or decreases in any one indicator (e.g., for four consecutive months) to be flagged;
▪ Large increases or decreases (e.g., a percentage change in a districts admission twice that of the average variation normally observed in that district, or similar) to be flagged;
▪ X number of stock outs flagged; ▪ Stock used. ▪ Screening numbers fall below a set threshold (based upon population burden and
number of programmes) for a given number of months. The above indicators are just a suggestion of potential indicators provided to highlight the approach of identification of patterns of particular concern in each area of analysis.
The database can also be used to produce the subnational score card tracking progress against agreed criteria (see section two of this report on Streamlining and Harmonization of Nutrition Data Collection Indicators, Forms and Reporting Mechanisms).
Given the lack of access to fast, stable internet at subnational level, especially at district level and below, the dashboard could be used to autogenerate reports which can be shared via email, WhatsApp or other messaging services, or printed PDF reports.
These autogenerated reports can be used to inform the analysis, feedback and monitoring and evaluation processes throughout the programme data. Autogenerated reports at District and

44
Governorate level could be shared at these levels and used to build a sense of ownership and understanding around data produced.
Training and guidance would be vital to ensure stakeholders can interpret and act upon the data presented in the dashboard and reports better interpret information to improve district and governorate level decision making and feedback with facility and community level programme staff could be incorporated into training for Nutrition Cluster staff and GHO and DHO. Figure 9 presents the data flow and outputs of the proposed database and how it would feed into subnational scorecards outlining key indicators and thresholds, and support feedback across the data value chain and decision making is shown. Key Stakeholder Responsible & Stakeholders Involved Nutrition Cluster, constituent UN agency and MOPHP, at national and subnational levels.
Routine Analysis of Data at the Sub-national Level to Increase Programme Effectiveness and Coverage
Table 13: Immediate Recommendations (Immediate-1 year)
Current Situation Summary
& Key Findings
Key Proposed Activity(s) Key Stakeholder Responsible
& Stakeholders Involved
Recommendation 2.4: Routine and Systematic Analysis of Available Nutrition Data to inform Nutrition Cluster Strategy
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making
(Analysis & Action)
Current Situation Summary & Key Findings There is limited routine analysis of trends in Nutrition Cluster data at national, governorate and district level, which could inform interpretation of trends in admissions, reporting rates, community screening and mobilisation, and availability of services and stock, which could inform decision making, for instance through systematically identifying and flagging for follow up issues such as stock outs, low or decreasing screening numbers, large, continuous or cyclical changes in admissions. Key Proposed Activity(s) Routinely producing an analysis of admissions data alongside reporting, screening and number of active programmes and triangulated with other information such as reports of increased food insecurity, insecurity or natural disasters or disease outbreak could provide a deeper understanding of programme performance and drivers of service utilization, as well as programme performance in community mobilisation and coverage. Such an analysis should be linked from its inception and design to how it can inform decision making drawing upon other NIS sources such as estimates from PBS, health facility nutrition monitoring, and data from other clusters and sectors to provide a wider picture of drivers to identify ensure early action is taken in response to discerned trends.
Such a system of analysis could be used within national and zonal Nutrition Cluster meetings, Nutrition Information Technical Working group meetings and more broadly. In order to link analysis to decision making, an integral part of each analysis would be reporting on what actions were taken upon the previous analysis findings for instance through systematically identifying and flagging for follow up issues such as stock outs, low or decreasing screening numbers, large, continuous or cyclical changes in admissions, or programme outcome indicators.
The cycle to produce such analyses would therefore be:
1. Collect available data such as monthly summary database analysis or data repository and dashboard analysis, alongside additional information from the Facility Based Nutrition Monitoring System, other cluster reports (from WASH, Food Security and Livelihoods, Health and other Clusters as appropriate) as well as relevant available information on climate, conflict or economic shocks.

45
Table 13: Immediate Recommendations (Immediate-1 year)
Current Situation Summary
& Key Findings
Key Proposed Activity(s) Key Stakeholder Responsible
& Stakeholders Involved
2. Analyse available nutrition specific data over the time period of interest, looking at time trends. In order to set the scope of such analyses and to increase usability, the focus could be upon identifying only a set number of districts of concern where issues should be followed up. This could be for instance:
• x number of districts with largest proportion increases in national population burden of admissions,
• x number of districts with largest number of stock outs reported,
• x number of districts with percentage of programmes reporting,
• x number of districts with lowest levels of community screening relative to population size
• x number of districts with lowest and highest defaulter rates reported.
The above indicators are just a suggestion of potential indicators provided to highlight the approach of identification of only those districts of particular concern in each area of analysis.
3. Triangulate nutrition data with other information from other clusters
4. Dissemination based upon an agreed communication strategy of analysis through presentation to relevant platforms (National and zonal Nutrition Cluster meetings, Nutrition Information Technical Working group meetings, quarterly or ad hoc donor nutrition situation and program update -led by the Nutrition Cluster, other cluster and sectoral meetings as appropriate etc.) 5. Collect information on feedback to previous analysis and how findings were acted upon (for instance, contact with MOPHP staff and NGO partners to further investigate trends discerned etc.). Incorporate the findings on actions taken into next analysis.
6. Begin Cycle again.
In this way, an integral part of analyses would be reporting on how previous analyses have been used. Where they have not been helpful or resulted in erroneous conclusions, this could also be enacted upon
Tools and trainings could be further streamlined to assist those involved in the data production process (from programme to DHO, GHO, Zonal and National levels) to apply a set of predefined criteria to flag potentially erroneous data, including very high or static cure rates over time, and to facilitate interpretation of relationships between numbers and trends in admissions and cure rates.
Key Stakeholder Responsible & Stakeholders Involved Nutrition Cluster, UNICEF, Wider Cluster System in Yemen (to provide multi-sectoral information, and for uptake and feedback on analysis.
Increasing Data Analysis and Use at Health Facility Level
Table 14: Long-Term Recommendations (1-3 years)
Current Situation Summary
& Key Findings
Key Proposed Activity(s) Key Stakeholder Responsible
& Stakeholders Involved
Recommendation 2.5: Integrate Facility and Community-Based Approaches to Increase Qualitative Analysis of Nutrition Information
Data Assessment
Data Collection
Data Access
Data Use for Decision-Making
(Analysis & Action)
Current Situation Summary & Key Findings
• No evidence was found of use of facility or community-based approaches to analyse
seasonal trends in admissions, drawing upon facility, district level summary databases and

46
Table 14: Long-Term Recommendations (1-3 years)
Current Situation Summary
& Key Findings
Key Proposed Activity(s) Key Stakeholder Responsible
& Stakeholders Involved
triangulated with information from community level and qualitative knowledge or context
specific seasonal drivers of malnutrition.
Key Proposed Activity(s)
• Utilize data produced through the NIS at the District level within facility and district health
system strengthening approaches, such as the Concern CMAM surge approach and ACF
District Health System Strengthening Approach.
At a community level, this approach can facilitate identification of high burden or otherwise high burden communities, which can then be targeted for increased community mobilisation and outreach accordingly. At a facility or district level, such an approach can increase preparedness for cyclical or otherwise predictable climate, conflict, economic shocks as well as seasonal spikes in malnutrition and disease, and empower health facility/programme staff to analyse and act upon the data they produce. The introduction or scale up of such approaches could be initiated by the MOHP or other NOG Nutrition Cluster partners with the support of national and zonal Nutrition Cluster in a limited number of districts or facilities, alongside other efforts to improve programme performance.
Key Stakeholder Responsible & Stakeholders Involved Nutrition Cluster. NGO partners to support in their own programming and in MOPHP facilities

47
5. CONCLUDING REMARKS In response to the severe humanitarian crisis in Yemen, the scale up of the nutrition response in Yemen in recent years has been significant. A range of stakeholders deliver nutrition services in the country, spanning MOPHP, UN agencies and national and international NGOs. Large volumes of valuable information are produced on the nutrition situation, both in terms of nutrition dynamics within the population and the performance and effectiveness of nutrition programmes.
However, the production of nutrition information, especially programmatic information, is heavily reliant upon a health work force within health facilities and district and governorate health offices who face severe human, physical and financial resource constraints. There has been a lack of commensurate capacity assessment or measures to put in place for targeted support for those working in the production of nutrition information.
With the rapid and vast scale up of nutrition programming in recent years, the number and type of nutrition indicators collected, and forms and reporting procedures used by stakeholders involved in nutrition programming have also increased. Roles and responsibilities for monitoring, reporting and data collection for nutrition at each level (central (national), Governorate, District, Health Facility and Community) have not been clearly documented leading to a confusion of role and responsibilities, lines of reporting and approval processes. There is a need for review, harmonisation and standardisation of indicators, data collection forms, and agreed-upon standard operating and reporting procedures.
At both the national and the sub-national levels, a rapid human resource assessment is also required that can help to inform a process of standardisation and strengthening of available training for health workers and monitoring and evaluation focal persons for nutrition (including information management officers) throughout the nutrition data value chain.
The use of information generated is the final goal of a nutrition information system. Population based surveys and assessments remain the most used sources of nutrition information used for decision making in Yemen. There is limited routine analysis of trends in nutrition programme data at governorate and district level, which could assist in interpretation of trends in admissions, reporting rates, community screening and mobilisation, and availability of services and stock, and inform decisions making to improve the effectiveness of the services.
A theory of change for how nutrition programme data, alongside other forms of nutrition data and from other sectors, is used for targeting human, physical and financial resources for maximum programme effectiveness and coverage is not clearly defined or understood. Furthermore, the mechanisms in place to provide stakeholders who produce and use data across the data value chain with feedback, analysis or guidance what actions should be taken in response to observed trends within data, are not well defined across contexts in Yemen. Further targeted analysis of available data should be used to improve the design and application of data quality criteria and related capacity building to better address and follow up on recurrent issues in data quality.
In the longer term, the scale-up of the existing District Health Information System (DHIS-2) information systems’ platform-through a nutrition-focused module will facilitate relevant facility and community-based nutrition data collection and analysis. As slow but steady progress is made towards further development and roll out of the system, there is a need to increase visibility of these efforts. This would presumably increase interest and engagement and hasten rollout.
The set of recommendations outlined in sections three and four of this report describe a set of sequential and related steps to address these issues and further strengthen the system for better programme coverage and performance and ultimately improved nutrition and health outcomes for the people of Yemen.
Individual organisational stakeholders are proposed alongside each recommendation as being most
suitable for holding accountability to oversee their implementation. Developing a work plan to delineate
roles and responsibilities in more detail and within a more detailed timeframe is beyond the scope of
this report. This process needs to be led by stakeholders in country through an appropriate platform.
The Nutrition Information Technical Working Group in Yemen is suggested as the most appropriate
platform for development of such a workplan.

48
Annex 1: Stakeholders for Key Informant Interviews
Table 15: List of Stakeholders Consulted for Key Informant Interviews (KIIs) (Updated April, 29th, 2021)
# Organization Name Position Telephone Email
Emailed Date/
Meeting Date
Key Informant Interviews (KIIs)
1
Action Against Hunger (AAH)
Hassan Ali Ahmed
SMART Secretariat Yemen for the AAH SMART
Meeting January 11, 2021
2
Action Against Hunger (AAH) Action Against Hunger / Action contre la Faim 500-720 rue Bathurst St, Toronto, ON M5S 2R4
Hailu Wondim Emergency Nutrition Assessment Manager
PHONE: +251936983444 / Skype: wondim.hailu
Meeting January 11, 2021
3
Afcar Consulting Adnan Qatinah Founder & CEO Haddah, Iran Street, Of Al-Bostan Hotel Sana'a, Yemen
Mobile: (+967) 711 811 151 Tel.: (+ 967-1) 414 636
Meeting Jan 21, 2021
5
Deem for Development | Aden www.deemyemen.org
Saleem Al-Basha Deem for Development
Branch Manager : +967-1428732 m: +967-733089826
Meeting February 4, 2021
6
European Commission Humanitarian Aid (ECHO)
Roselyn Mullo
Thematic Expert Cash Transfers and Food Security (RO Amman)
+962775526255
Meeting January 13, 2021
7
European Commission Humanitarian Aid (ECHO)
Javier Rio Navarro European Commission - DG ECHO Technical Assistant, Yemen
Mobile Yemen: +967 73 5377791 Mobile Amman: +962 77 6104569 ECHO website in Arabic http://echo-arabic.eu
Meeting January 13, 2021
8 Field Medical Foundation (FMF)
Abdulgalil Al-Dafary
770840260
Meeting February 4, 2021
9
Food and Agriculture Organization of the United Nations (FAO)
Kamal - Wanjohi, Kamau (FAOYE)
Joint Monitoring Framework As you have not yet interviewed Kamal maybe you could Kamal for the framework – if you don’t get no problem, I will share
Meeting Feb 2, 2021
10
Food and Agriculture Organization of the United Nations (FAO)
Joel Munywoki Nutrition Officer at Food and Agriculture Organization
[email protected] Meeting January 18, 2021
11
iMMAP https://immap.org/ Elijah Odundo | Information Management Officer & Data Analyst (Yemen)
Elijah Odundo Nutritionist IMMAP
739775173 [email protected]
Meeting December 8, 2020 Scheduled second

49
Table 15: List of Stakeholders Consulted for Key Informant Interviews (KIIs) (Updated April, 29th, 2021)
# Organization Name Position Telephone Email
Emailed Date/
Meeting Date
Better Data, Better Decisions, Better Outcomes M: +(962) 790932082 | Skype: Elijah.odundo1 iMMAP MENA Regional Office Husseini Center, 145 Mecca St., Amman, Jordan www.immap.org
Meeting 2021
12 iMMAP
Mehtab Khan [email protected]
Meeting January 27, 2021
13 iMMAP
Fridon Japaridze
Meeting January 27, 2021
14 International Medical Corps (IMC)
Suzanne Brinkmann
Meeting January 5, 2021
15 International Medical Corps (IMC)
Samuel Mbuto [email protected]
Meeting January 5, 2021
16 International Medical Corps (IMC)
Sibida George [email protected]
Meeting January 5, 2021
17
Ministry of Public Health and Population (MOPHP)/Yemen -Sana’a
Dr. Abdulfattah M.Al-Mahdi
Child Health Specialist /Community Medicine Specialist Rapporteur of the Supervisory Committee of SMART Surveys Deputy Technical Committee of SMART surveys National Nutrition Cluster coordinator / MOPHP Former UN Dispensary Doctor General Director of preventive and curative Nutrition PHC Sector, MOPH&P/Yemen
Mobile: +967 77105 99 33 office: +967 1 239211
Meeting December 6, 2020
18 Ministry of Public Health and Population (MOPHP) -Sana’a
Arafat Nutrition Data in the MOPHP
Meeting December 15, 2020
19 Ministry of Public Health and Population (MOPHP) -Sana’a
Houssein Managerial Role for this in MOPHP
Meeting December 15, 2020

50
Table 15: List of Stakeholders Consulted for Key Informant Interviews (KIIs) (Updated April, 29th, 2021)
# Organization Name Position Telephone Email
Emailed Date/
Meeting Date
20
Ministry of Public Health and Population (MOPHP), Information and Research 52
Najeeb Yahya Ali
Director of Information and Research in the MOPHP
777770100 [email protected] [email protected]
Meeting planned February 4, 2021
21
Ministry of Public Health & Population (MoPHP)- Aden
Manar Wadea 737796323 [email protected]
Meeting February 2, 2021
22
Ministry of Public Health and Population (MOPHP) -Aden
Dr. Mahfood Ali Head of the Nutrition Department MOPHP- Aden
Meeting January 25, 2021
23 Qatar Red Crescent (QRCS)- Nutrition partners
Dr. Wafa Mohammed Al-Shaibani
733570043
Meeting January 25, 2021
24
REACH Initiative Juliet Stein Country Coordinator - Yemen at IMPACT Initiatives
December 9, 2020; Meeting December 15, 2020
25
REACH Initiative Noortje GERRITSMA
Assessment Officer for Health and Nutrition (Based in Amman)
Meeting December 15, 2020
26
REACH Initiative53 Alexander WARD
Research Manager (Based in Amman)
Meeting December 15, 2020v
27 Relief International Abdirahman Ali Country Director [email protected] Meeting
February 3, 2021
28
Relief International Edith Muturi Health and Nutrition Technical Advisor
[email protected] Meeting February 3, 2021
52 Director of Health Information and Research in the MOPHP- Najeeb Yahya Ali. It was also agreed it is important to share his knowledge and understanding of DHIS 2 that is under his supervision and how is linked with the nutrition information system- would very much enrich the NIS consultation meeting and future improvements. In view of this, we all agreed that should interviewed as of the one of the key informants and be among the NIS participant. He is very much interested also in sharing his experience in the DHIS 2 during the consultation. I am copying Najeeb so that you can follow up with him directly. He can also be reached over his mobile phone: 53 REACH Initiative is a leading humanitarian initiative providing granular data, timely information and in-depth analysis from contexts of crisis, disaster and displacement.
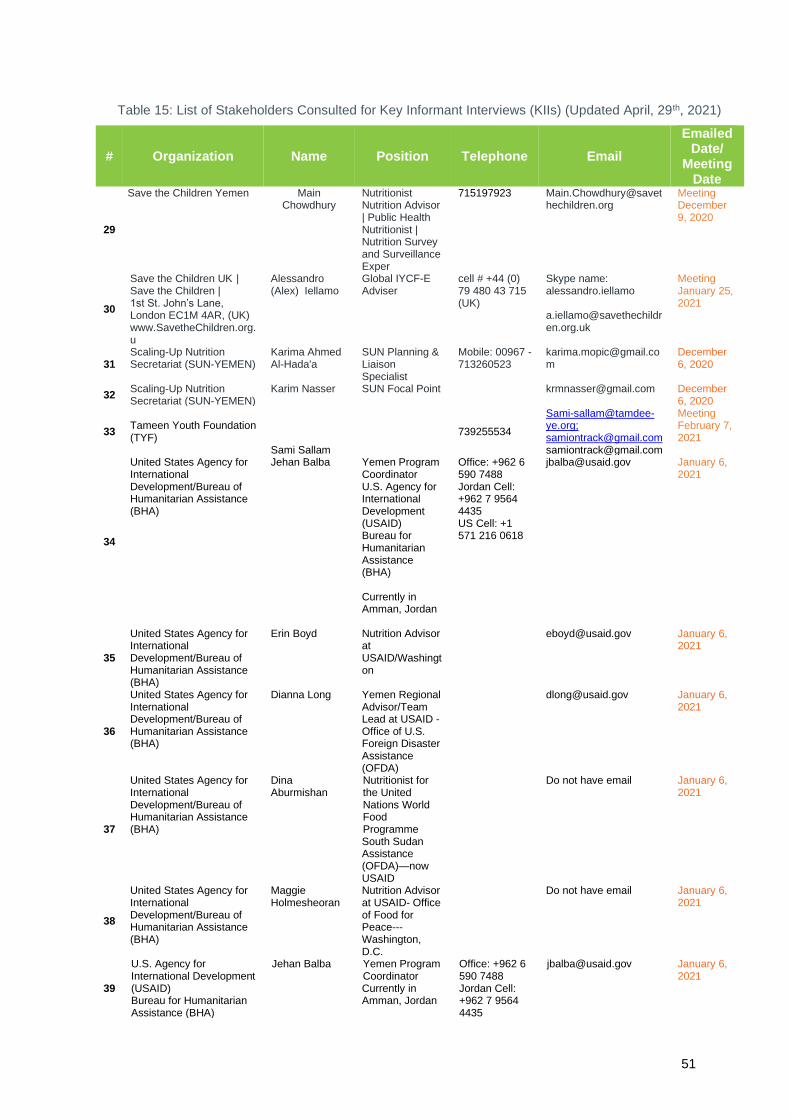
51
Table 15: List of Stakeholders Consulted for Key Informant Interviews (KIIs) (Updated April, 29th, 2021)
# Organization Name Position Telephone Email
Emailed Date/
Meeting Date
29
Save the Children Yemen Main Chowdhury
Nutritionist Nutrition Advisor | Public Health Nutritionist | Nutrition Survey and Surveillance Exper
715197923 [email protected]
Meeting December 9, 2020
30
Save the Children UK | Save the Children | 1st St. John’s Lane, London EC1M 4AR, (UK) www.SavetheChildren.org.u
Alessandro (Alex) Iellamo
Global IYCF-E Adviser
cell # +44 (0) 79 480 43 715 (UK)
Skype name: alessandro.iellamo [email protected]
Meeting January 25, 2021
31 Scaling-Up Nutrition Secretariat (SUN-YEMEN)
Karima Ahmed Al-Hada'a
SUN Planning & Liaison Specialist
Mobile: 00967 - 713260523
December 6, 2020
32 Scaling-Up Nutrition Secretariat (SUN-YEMEN)
Karim Nasser SUN Focal Point [email protected] December 6, 2020
33 Tameen Youth Foundation (TYF)
Sami Sallam
739255534
[email protected]; [email protected] [email protected]
Meeting February 7, 2021
34
United States Agency for International Development/Bureau of Humanitarian Assistance (BHA)
Jehan Balba
Yemen Program Coordinator U.S. Agency for International Development (USAID) Bureau for Humanitarian Assistance (BHA) Currently in Amman, Jordan
Office: +962 6 590 7488 Jordan Cell: +962 7 9564 4435 US Cell: +1 571 216 0618
[email protected] January 6, 2021
35
United States Agency for International Development/Bureau of Humanitarian Assistance (BHA)
Erin Boyd Nutrition Advisor at USAID/Washington
[email protected] January 6, 2021
36
United States Agency for International Development/Bureau of Humanitarian Assistance (BHA)
Dianna Long Yemen Regional Advisor/Team Lead at USAID - Office of U.S. Foreign Disaster Assistance (OFDA)
[email protected] January 6, 2021
37
United States Agency for International Development/Bureau of Humanitarian Assistance (BHA)
Dina Aburmishan
Nutritionist for the United Nations World Food Programme South Sudan Assistance (OFDA)—now USAID
Do not have email January 6, 2021
38
United States Agency for International Development/Bureau of Humanitarian Assistance (BHA)
Maggie Holmesheoran
Nutrition Advisor at USAID- Office of Food for Peace---Washington, D.C.
Do not have email January 6, 2021
39
U.S. Agency for International Development (USAID) Bureau for Humanitarian Assistance (BHA)
Jehan Balba
Yemen Program Coordinator Currently in Amman, Jordan
Office: +962 6 590 7488 Jordan Cell: +962 7 9564 4435
January 6, 2021

52
Table 15: List of Stakeholders Consulted for Key Informant Interviews (KIIs) (Updated April, 29th, 2021)
# Organization Name Position Telephone Email
Emailed Date/
Meeting Date
US Cell: +1 571 216 0618 Email : [email protected] Office : +962 6 590 7488 Jordan Cell: +962 7 9564 4435 US Cell: +1 571 216 0618
40
United Nations Children’s Fund (UNICEF)/Yemen
Nagib Abdulbaqi
Nutrition Specialist, *Technical Working Group-UNICEF
Tel: +967-1-211-400 (331) Mobile: +967 712223457 Skype for Business (Email address)
[email protected] meeting January 7, 2021
41
United Nations Children’s Fund (UNICEF)/Yemen
Emma Tuck إيما
توكWASH Cluster focal person Yemen WASH Cluster Coordinator
Tel / WhatsApp: +967 712 223 122
[email protected] Meeting December 14, 2020
42
UNICEF Yemen, P.O.Box: 725 - Sana'a – Yemen – مكتب
Ahmed A. Al-Shami
Programme Officer (Data Management and Monitoring) – Health & Nutrition Section
Tel: +967-1-211-400 (335) Fax: +967-1-206-092 Mobile: +967-712223181
Meeting December 8, 2020
43
United Nations Children’s Fund (UNICEF) New York 3 United Nations Plaza New York, NY10017
Louise Mwirigi DHIS-2 : Nutrition Indicators Louise M Mwirigi,
Nutrition Specialist (Information) Programme Division, UNICEF DHIS2 Nutrition *Technical Working Group-UNICEF
Tel : +1 212 326 7405 Cel: +1 718 644 3523 Skype ID : louisem.mwirigi
[email protected] Meeting December 1, 2020
44
United Nations Children’s Fund (UNICEF)/Yemen
Nagib Abdulbaqi
Nutrition Specialist, *Technical Working Group-UNICEF
Tel: +967-1-211-400 (331) Mobile: +967 712223457 Skype for Business (Email address)
Meeting Jan 7, 2021
45 United Nations Children’s Fund (UNICEF)/Yemen
Boniface (Boni) Kalanda
Chief Planning, Monitoring and Evaluation
Mobile +967 71222 3113
[email protected] November 11, 2020
46 United Nations Children’s Fund (UNICEF)/Yemen
Kennedy Ongwae
Chief of Health and Nutrition at UNICEF Yemen
[email protected] November 11, 2020
47 United Nations Children’s Fund (UNICEF)/Yemen
Vivienne Forsythe
*Technical Working Group-UNICEF
[email protected] November 11, 2020
48 United Nations Children’s Fund (UNICEF)/Yemen
Koki (Mary) Kyalo
Nutrition Cluster deputy
[email protected] [email protected]
Meeting January 21, 2021
49 United Nations Children’s Fund (UNICEF)/Yemen
Adeniyi Olaleye Planning, Monitoring & Evaluation
[email protected] November 11, 2020

53
Table 15: List of Stakeholders Consulted for Key Informant Interviews (KIIs) (Updated April, 29th, 2021)
# Organization Name Position Telephone Email
Emailed Date/
Meeting Date
Specialist at UNICEF *Technical Working Group-UNICEF
50
UNICEF Yemen P.O.Box: 725 - Sana'a – Yemen – اليمن اليونيسيف مكتب
Abdulkawie Moharram
Information Management Officers' (IMO) IMO Nutrition Cluster
[email protected] Meeting January 19, 2021
51 United Nations Children’s Fund (UNICEF)/Yemen
Boniface (Boni) Kalanda
Chief Planning, Monitoring and Evaluation
Mobile +967 71222 3113
[email protected] November 11, 2020
52 United Nations Children’s Fund (UNICEF)/Yemen
Kennedy Ongwae
Chief of Health and Nutrition at UNICEF Yemen
[email protected] November 11, 2020
53 United Nations Children’s Fund (UNICEF)/Yemen
Vivienne Forsythe
*Technical Working Group-UNICEF
[email protected] November 11, 2020
54 United Nations Children’s Fund (UNICEF)/Yemen
Koki Kyalo
Deputy Nutrition Cluster Coordinator at UNICEF
771589500 [email protected] Meeting January 21, 2021
55 United Nations Children’s Fund (UNICEF)/Yemen Aden
Dr. Gamil Gamila Hibatullah
Health and Nutrition (H&N) Specialist
[email protected] PENDING
56 United Nations Children’s Fund (UNICEF)/Yemen Aden
Dr. Waddah Alwan
Health and Nutrition (H&N) Officer
[email protected] ENDING
57 United Nations Children’s Fund (UNICEF)/Yemen Aden
Dr. Lina Albaz Health and Nutrition (H&N) Officer
[email protected] PENDING
58 United Nations Children’s Fund (UNICEF)/Yemen Hodeida54
Dr. Khaled Khaled Al-Shaibani
Health and Nutrition (H&N) Specialist
[email protected] PENDING
59 United Nations Children’s Fund (UNICEF)/Yemen
Yasmin Algodemh
Health and Nutrition (H&N) Officer
[email protected] PENDING
60 United Nations Children’s Fund (UNICEF)/Yemen Hodeida
Waleed Almadhaji Waleed Almadhaji Health & Nutrition Officer – UNICEF Hodediah office UNICEF Yemen, P.O.Box: 725 - Sana'a - Yemen Tel: +967-3-205-785/7 (ext. 808) Fax: +967-3-206-834 Mobile: +967-712223490 Email: [email protected]
Health and Nutrition (H&N) Officer
54 From Hodeida; Dr. Khaled H&N specialist & Dr Yasmin & Dr Waleed (H&N officers)

54
Table 15: List of Stakeholders Consulted for Key Informant Interviews (KIIs) (Updated April, 29th, 2021)
# Organization Name Position Telephone Email
Emailed Date/
Meeting Date
Follow us on Facebook, Twitter, YouTube, unicef.org
61 World Food Programme (WFP)
Trust Mlambo Nutrition Manager, World Food Program
[email protected] Meeting December 14, 202055
62 World Food Programme (WFP)
Yukimi Ogaki [email protected] Meeting December 14, 2020
63 World Food Program (WFP)
Esmail Alyagori
Information Management Officer
Tuesday, February 2, 2021
64
World Health Organization (WHO)/Yemen
Marina Adrianopoli
Technical Officer for Nutrition at World Health Organization WHO Health Emergencies Programme | WHO Yemen| Amman outpost Based out of Amman
GPN: 64059| cell in Jordan: +962 7 9847 8348 | cell in Yemen: +967 739 888 405 http://www.emro.who.int/countries/yem/
[email protected] Meeting January 4, 2020
65
World Health Organization (WHO)/Yemen
Eshrak Naji Mohammed Al-Falahi
Eshrak Naji Alfalahi Nutrition Officer Nutrition Department World Health Organization Country Office Sana’a, Yemen
Office t/p: 1470095/4/3 Mobile: +967 739 712 220 GPN: 67343 Skype name: live:e.alfalahi_2 Web: www.who.int Follow WHO Yemen on: www.facebook.com/WHOYemen www.twitter.com/WHOYemen http://www.emro.who.int/countries/yem/
[email protected] Meeting January 5, 2020
66 World Health Organization (WHO)/Yemen
Ferima Coulibaly-Zerbo
733570043
[email protected] Meeting December 29, 2020
67 World Health Organization (WHO)/Yemen
Mr Arafat Al Khshbi,
DHIS-2 focal person
Meeting January 28, 2021
68
Nutrition Cluster Zonal Nutrition Coordinator
Mutahar Al-Falahi Hameed Awn Henry Sebuliba Al-Hajj Murad Abdullah Dahan Jemal Seid Mohammed
Nutrition Cluster Zonal Nutrition Coordinators. UNICEF Yemen.
[email protected] [email protected] [email protected] [email protected] [email protected]
Meeting March 13 2021
55 Thank you very much for your email. Kindly note I am out of office with limited access to email between 17th January to 7th February, 2021. Kindly refer all CO Nutrition communication to Ms. Habiba Abdi email [email protected] and Dr Salem Mufta email [email protected].
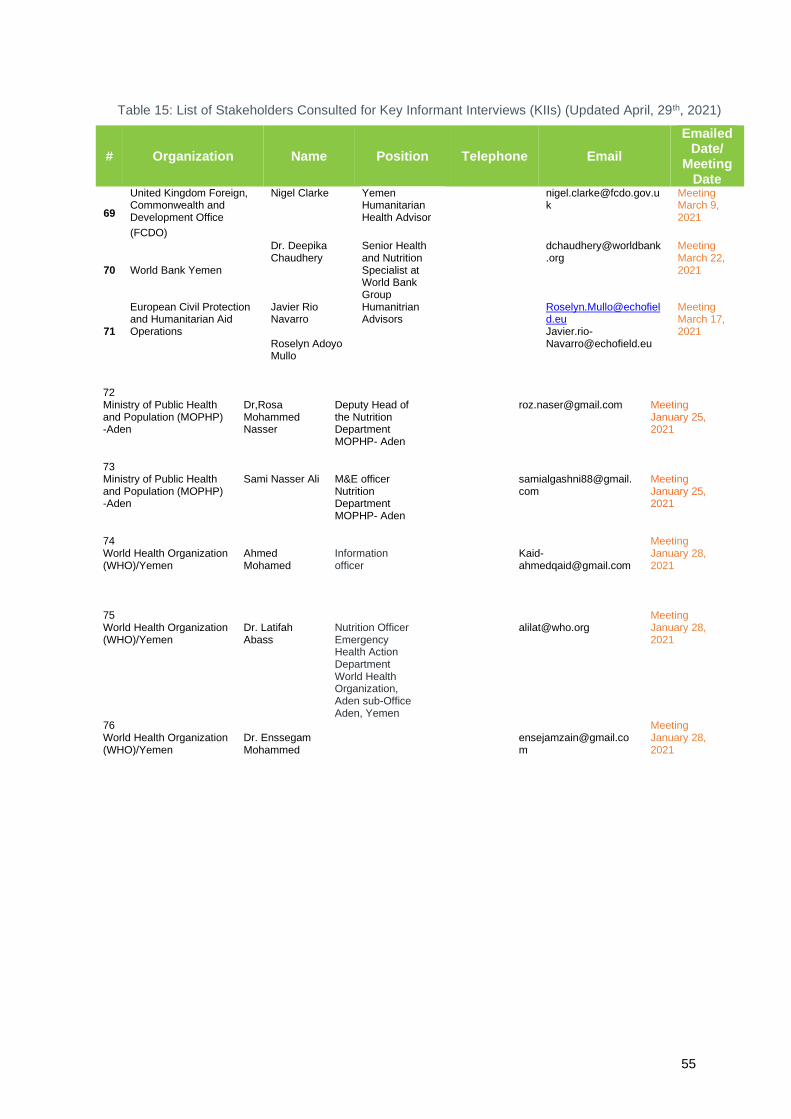
55
Table 15: List of Stakeholders Consulted for Key Informant Interviews (KIIs) (Updated April, 29th, 2021)
# Organization Name Position Telephone Email
Emailed Date/
Meeting Date
69
United Kingdom Foreign, Commonwealth and Development Office
(FCDO)
Nigel Clarke Yemen Humanitarian Health Advisor
Meeting March 9, 2021
70
World Bank Yemen
Dr. Deepika Chaudhery
Senior Health and Nutrition Specialist at World Bank Group
Meeting March 22, 2021
71
European Civil Protection and Humanitarian Aid Operations
Javier Rio Navarro Roselyn Adoyo Mullo
Humanitrian Advisors
[email protected] [email protected]
Meeting March 17, 2021
72 Ministry of Public Health and Population (MOPHP) -Aden
Dr,Rosa Mohammed Nasser
Deputy Head of the Nutrition Department MOPHP- Aden
Meeting January 25, 2021
73 Ministry of Public Health and Population (MOPHP) -Aden
Sami Nasser Ali
M&E officer Nutrition Department MOPHP- Aden
Meeting January 25, 2021
74 World Health Organization (WHO)/Yemen
Ahmed Mohamed
Information officer
Kaid- [email protected]
Meeting January 28, 2021
75 World Health Organization (WHO)/Yemen
Dr. Latifah Abass
Nutrition Officer Emergency Health Action Department World Health Organization, Aden sub-Office Aden, Yemen
Meeting January 28, 2021
76 World Health Organization (WHO)/Yemen
Dr. Enssegam Mohammed
Meeting January 28, 2021

56
Annex 2: Agenda of Consultative Meeting February 16-17, 20201
Nutrition Information Systems in Yemen: Consultative Technical Meeting
February 16 & 17, 2021 9:00 AM-1:30 PM
Objectives of Consultative Meeting Objective 1. Stakeholders learn about the current state of Nutrition Information Systems in Yemen including
▪ Information systems
▪ Data collection forms
▪ Nutrition-specific indicators
▪ Date data flows
▪ Use of nutrition information products Objective 2. Discuss successes, challenges and gaps, to contribute to the identification of areas for improvement and strengthening of the NIS in Yemen
Day 1 Time Session and Content 9:00-9:15 AM Welcome from Nutrition Cluster & Ministry of Public Health and
Population 9:15 - 9:30 AM 1-Overview of Scope of Work
▪ Overview of the scope of work and aims of consultative meeting (FCDO/TASC Team) (15 min)
▪ Introduction of participants in the meeting rooms (in the chat box on Zoom)
▪ Explanation of meeting participation virtually and in person 9:30 -10:15 AM 2-Overview of NIS/Monitoring and Reporting Systems for Nutrition
in Yemen ▪ Overview of Nutrition Information System ▪ Nutrition Information Data Flows ▪ Main Sources of nutrition data and how they are used for
decision making. ▪ Open Discussion/Questions
10:15 - 10:30 AM Break B10:30 – 1:30 PM (continued into Tuesday)
3-Facility & Community -Based Data, Monitoring and Reporting (Routine)
Community Management of Acute Malnutrition (CMAM) Sites & Database
10:30-10:50 AM (20 min)
Community Management of Acute Malnutrition (CMAM) Sites & Database
10:50-11:05 AM (15 min)
1.a. Severe Acute Malnutrition (SAM) database (outpatient) for SAM without complications
11:05-11:20 AM (15 min)
1.b. Moderate Acute Malnutrition (MAM) database (outpatient) for MAM
11:20-11:40 AM (20 min)
1.c. Therapeutic Feeding Centres Database System (inpatient) for SAM with Complications
11:40-12:00 PM (20 min)
▪ Targeted Questions on CMAM (SAM, MAM & TFC)
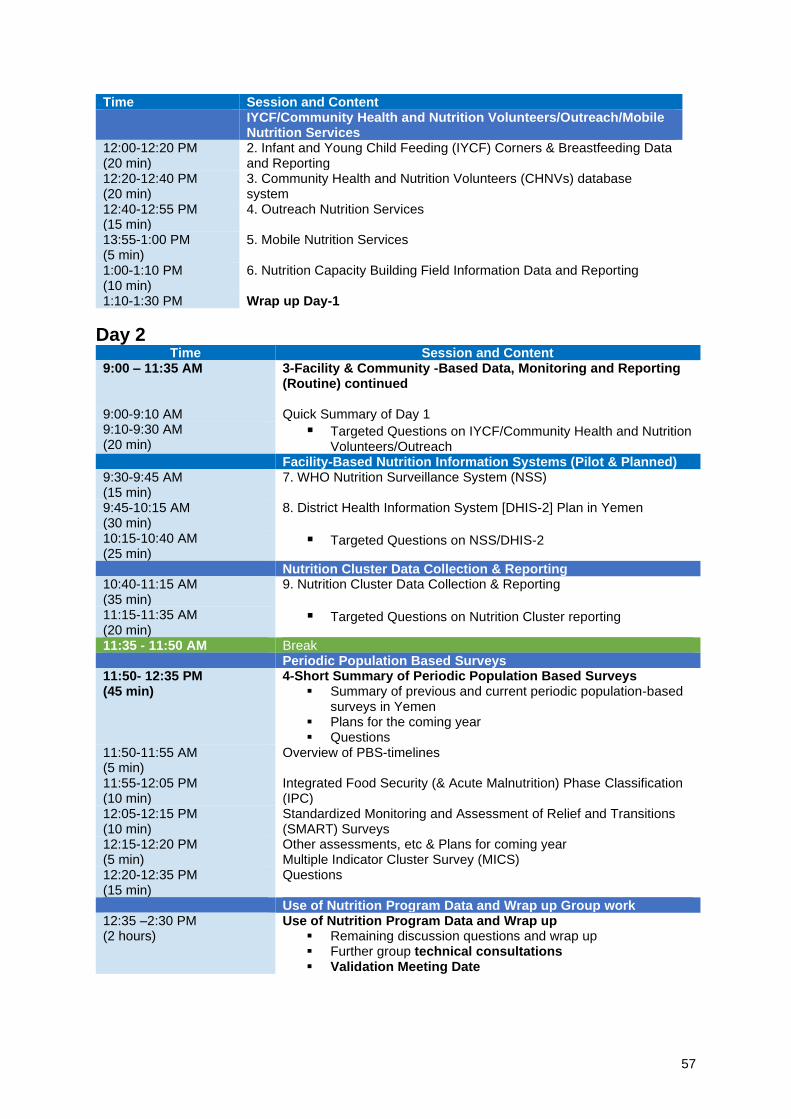
57
Time Session and Content IYCF/Community Health and Nutrition Volunteers/Outreach/Mobile
Nutrition Services 12:00-12:20 PM (20 min)
2. Infant and Young Child Feeding (IYCF) Corners & Breastfeeding Data and Reporting
12:20-12:40 PM (20 min)
3. Community Health and Nutrition Volunteers (CHNVs) database system
12:40-12:55 PM (15 min)
4. Outreach Nutrition Services
13:55-1:00 PM (5 min)
5. Mobile Nutrition Services
1:00-1:10 PM (10 min)
6. Nutrition Capacity Building Field Information Data and Reporting
1:10-1:30 PM Wrap up Day-1
Day 2 Time Session and Content
9:00 – 11:35 AM 3-Facility & Community -Based Data, Monitoring and Reporting (Routine) continued
9:00-9:10 AM Quick Summary of Day 1 9:10-9:30 AM (20 min)
▪ Targeted Questions on IYCF/Community Health and Nutrition Volunteers/Outreach
Facility-Based Nutrition Information Systems (Pilot & Planned) 9:30-9:45 AM (15 min)
7. WHO Nutrition Surveillance System (NSS)
9:45-10:15 AM (30 min)
8. District Health Information System [DHIS-2] Plan in Yemen
10:15-10:40 AM (25 min)
▪ Targeted Questions on NSS/DHIS-2
Nutrition Cluster Data Collection & Reporting 10:40-11:15 AM (35 min)
9. Nutrition Cluster Data Collection & Reporting
11:15-11:35 AM (20 min)
▪ Targeted Questions on Nutrition Cluster reporting
11:35 - 11:50 AM Break Periodic Population Based Surveys 11:50- 12:35 PM (45 min)
4-Short Summary of Periodic Population Based Surveys ▪ Summary of previous and current periodic population-based
surveys in Yemen ▪ Plans for the coming year ▪ Questions
11:50-11:55 AM (5 min)
Overview of PBS-timelines
11:55-12:05 PM (10 min)
Integrated Food Security (& Acute Malnutrition) Phase Classification (IPC)
12:05-12:15 PM (10 min)
Standardized Monitoring and Assessment of Relief and Transitions (SMART) Surveys
12:15-12:20 PM (5 min)
Other assessments, etc & Plans for coming year Multiple Indicator Cluster Survey (MICS)
12:20-12:35 PM (15 min)
Questions
Use of Nutrition Program Data and Wrap up Group work 12:35 –2:30 PM (2 hours)
Use of Nutrition Program Data and Wrap up ▪ Remaining discussion questions and wrap up ▪ Further group technical consultations ▪ Validation Meeting Date
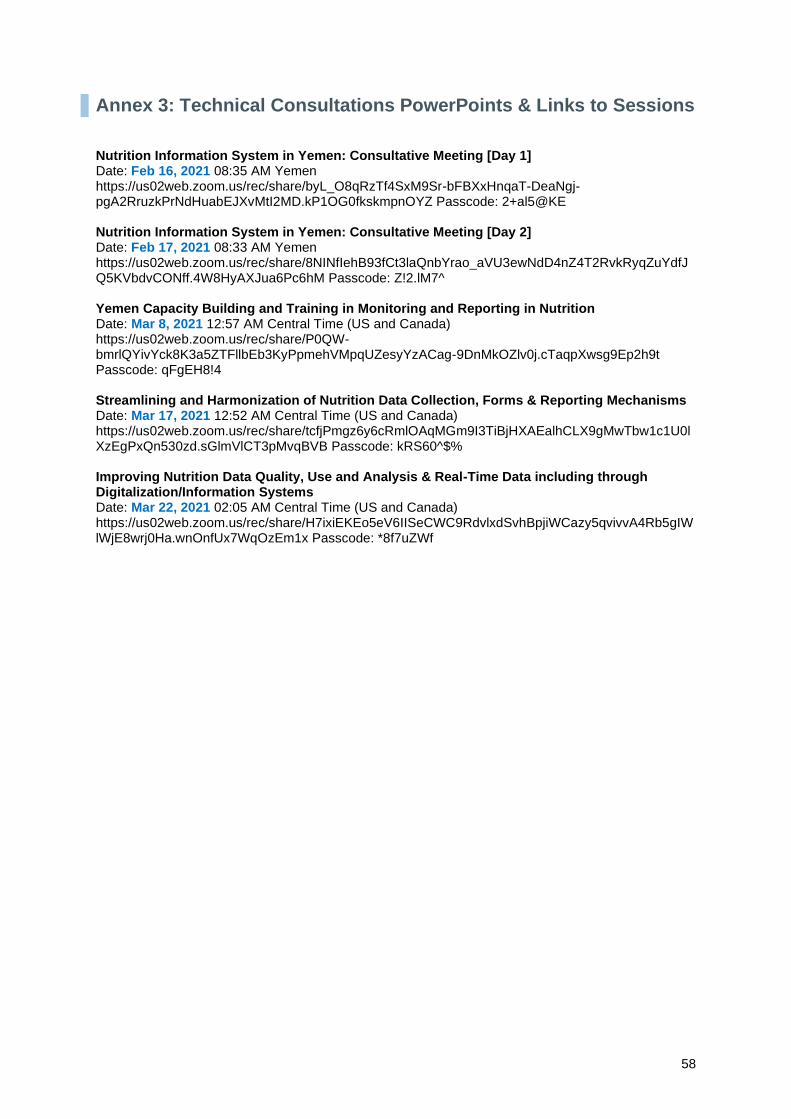
58
Annex 3: Technical Consultations PowerPoints & Links to Sessions Nutrition Information System in Yemen: Consultative Meeting [Day 1] Date: Feb 16, 2021 08:35 AM Yemen https://us02web.zoom.us/rec/share/byL_O8qRzTf4SxM9Sr-bFBXxHnqaT-DeaNgj-pgA2RruzkPrNdHuabEJXvMtI2MD.kP1OG0fkskmpnOYZ Passcode: 2+al5@KE Nutrition Information System in Yemen: Consultative Meeting [Day 2] Date: Feb 17, 2021 08:33 AM Yemen https://us02web.zoom.us/rec/share/8NINfIehB93fCt3laQnbYrao_aVU3ewNdD4nZ4T2RvkRyqZuYdfJQ5KVbdvCONff.4W8HyAXJua6Pc6hM Passcode: Z!2.lM7^ Yemen Capacity Building and Training in Monitoring and Reporting in Nutrition Date: Mar 8, 2021 12:57 AM Central Time (US and Canada) https://us02web.zoom.us/rec/share/P0QW-bmrlQYivYck8K3a5ZTFllbEb3KyPpmehVMpqUZesyYzACag-9DnMkOZlv0j.cTaqpXwsg9Ep2h9t Passcode: qFgEH8!4 Streamlining and Harmonization of Nutrition Data Collection, Forms & Reporting Mechanisms Date: Mar 17, 2021 12:52 AM Central Time (US and Canada) https://us02web.zoom.us/rec/share/tcfjPmgz6y6cRmlOAqMGm9I3TiBjHXAEalhCLX9gMwTbw1c1U0lXzEgPxQn530zd.sGlmVlCT3pMvqBVB Passcode: kRS60^$% Improving Nutrition Data Quality, Use and Analysis & Real-Time Data including through Digitalization/Information Systems Date: Mar 22, 2021 02:05 AM Central Time (US and Canada) https://us02web.zoom.us/rec/share/H7ixiEKEo5eV6IISeCWC9RdvlxdSvhBpjiWCazy5qvivvA4Rb5gIWlWjE8wrj0Ha.wnOnfUx7WqOzEm1x Passcode: *8f7uZWf

59
Annex 4: Key Nutrition-Specific Interventions in Yemen This consultancy looked at nutrition information systems for interventions in the health sector only -focusing on nutrition-specific interventions56 57, illustrated in Figure 17.
Figure 10: Nutrition-Specific Interventions in Yemen
Source: Authors of this report, 2021.
56 Nutrition-specific interventions address the immediate causes of undernutrition, such as a poor or inadequate diet, disease, and related underlying factors such as lack of access to food, sub-optimal feeding practices, inadequate health care, and an unhealthy environment. 57 “FY 2018 Annual Performance Report | FY 2020 Annual Performance Plan.” United States Department of State United States Agency for International Development, May 2019. https://www.usaid.gov/sites/default/files/documents/1870/FY_20_APP_FY_18_APR_FINAL_5-20-2019_508-Compliance_1.pdf

60
The nutrition-specific intervention with the most financial and human resources in Yemen is the Community Management of Acute Malnutrition (CMAM) which has four main components (Figure 3).
Figure 11: Community Management of Acute Malnutrition (CMAM) components, and main service delivery entry points
Source: Authors of this report, 2021.

61
Annex 5: Existing Trainings There are a number of trainings in Yemen for nutrition-in three main categories: 1) technical nutrition training (for different nutrition program focal points), 2) Health Workers training and 3) Community Health and Nutrition Volunteers (CHNVs) (Table 2). These trainings train the cadres in at the different levels (Central/National Level, Governorate, District and Health Facility and Community Level) in Table 16. In order to track capacity building activities for all nutrition interventions there is a ‘Nutrition Capacity Building Field Information Data and Reporting’ report.
Training is implemented and managed by a combination of UN agencies and Nutrition Cluster implementing partners. Currently the ‘Nutrition Capacity Building Field Information Report’ managed by UNICEF/Yemen reports the following on training, along with other identified training. Health Worker training on SAM with Complications (managed by WHO) Health Worker (HW) Training on CMAM
▪ HWs trained on CMAM (Basic Training) (Male, Female) ▪ HWs trained on CMAM (Refresher training) (Male, Female) ▪ HWs trained on TFC/SC (Male, Female) ▪ CHVs trained (Basic Training) (Male, Female) ▪ CHVs trained (Training on growth monitoring) (Male, Female) ▪ CHVs attended review Meetings (Male, Female)
Health Worker (HW) Training on Infant and Young Child Feeding ▪ HWs trained on IYCF (Basic) (Male, Female) ▪ HWs trained on IYCF (Refresher) (Male, Female)
Other ▪ People trained on SMART Surveys (Male, Female)
Training of Trainer (TOT) Meetings ▪ Male TOT ▪ Female TOT ▪ Type of TOT Training
However, it is important to note that not all implementing partners conducting training are necessarily reporting into this. Currently, due to the COVID-19 pandemic trainings and refresher trainings did not happen in 2020.
Support is needed to ensure the quality training and refresher training of relevant human resources at all levels (central, governorate, district and health facility/community health and nutrition volunteers (CHNVs) for monitoring and reporting.
Table 16: Training Cadres for Nutrition
Human Resources
Central/National Level
1.1 Ministry of Public Health and Planning (MOPHP) Central/National Level Management
1.2 UN Agency Information Management Officer (IMO) Staff (UNICEF, WHO, WFP)
1.3 Implementing Partner Monitoring & Evaluation Staff
Governorate Level
1.4 Ministry of Public Health and Planning (MOPHP) Governorate Level Nutrition Staff/Nutrition Coordinator
District Level
1.5 Ministry of Public Health and Planning (MOPHP) District Level Nutrition Staff/Nutrition Coordinator
Health Facility and Community Level
1.6 Ministry of Public Health and Planning (MOPHP) Service Delivery level: Health Facilities –Health Workers-Nutrition Focal person staff
1.7 Ministry of Public Health and Planning (MOPHP) Service Delivery level: Health Facilities –Community Health and Nutrition Volunteers (CHNVS)

62
Table 17: Existing Training
TRAINING
1.1 Technical Nutrition Training (Nutrition program focal points)
1.1.1 Nutrition Information Management/ Information Systems (IM/IS) Training
1.1.2 Standardized Monitoring and Assessment of Relief and Transitions (SMART) Surveys Training-Manager level
1.1.3 Standardized Monitoring and Assessment of Relief and Transitions (SMART) Master level training of trainers (TOT) Central Staff to lower-level staff
1.1.4 Nutrition Data Clinic Workshop (all data, looking at data quality) higher level staff for data analysis/data quality improvement
1.1.5 Master Inpatient Therapeutic Feeding Centre Training-TOT Cascade (WHO)
1.1.6 Integrated Food Security Phase Classification (IPC) Acute Malnutrition Training-Level 1
1.1.7 Nutrition Monitoring and Supervision Training
1.1.8 Nutrition Surveillance Training
1.1.9 Emergency Nutrition Training
1.1.10 Training of Trainers (TOT) for Nutrition Training
1.2 Health Workers Training
1.2.1 Community-Based Management of Acute Malnutrition (CMAM) Training-Basic Training [Health Workers]
1.2.3 Community-Based Management of Acute Malnutrition (CMAM) Training-Refresher Training [Health Workers]
1.2.4 Therapeutic Feeding Centres/ Stabilization Centres (TFC/SC) Training [Health Workers]
1.2.5 SAM with Medical Complications Management withing DTCs and ICUs /e SAM/MC for DTC and ICU is not the full package like in TFC [Health Workers]
1.2.6 Infant and Young Child Feeding (IYCF) Training-Basic [Health Workers]
1.2.7 Infant and Young Child Feeding (IYCF) Training-Refresher [Health Workers]
1.2.8 CMAM-Outpatient Therapeutic Treatment Programme] (OTP) Training –Basic [Health Workers]
1.2.9 CMAM-Outpatient Therapeutic Treatment Programme] (OTP) Training –Refresher [Health Workers]
1.3 Community Health and Nutrition Volunteers (CHNVs)
1.3.1 Master Trainers for CMAM CHNVs
1.3.2 Community-Based Management of Acute Malnutrition (CMAM) Training-Basic Training for Community Health and Nutrition Volunteers (CHNVs) Basic Training (with Growth Monitoring Training for Community Health and Nutrition Volunteers (CHNVs))
1.3.3 Review Meeting for CHNVs---review training gaps--Attended a Review for Community Health and Nutrition Volunteers (CHNVs)
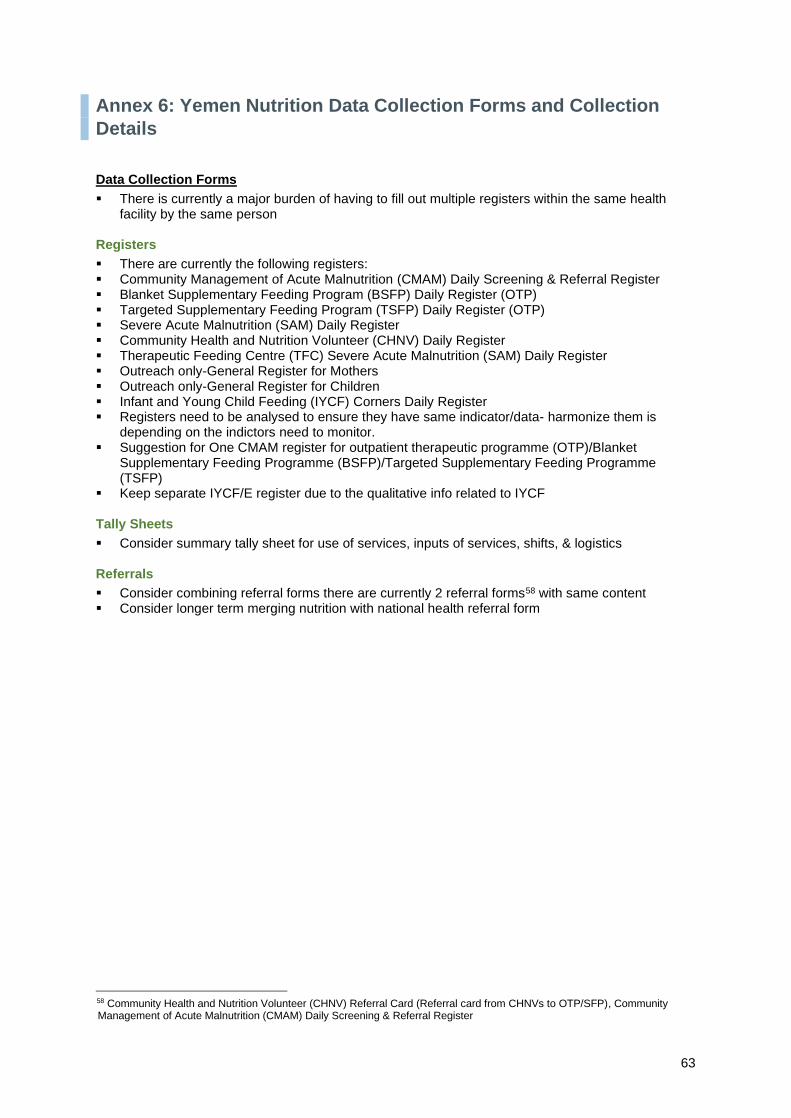
63
Annex 6: Yemen Nutrition Data Collection Forms and Collection
Details
Data Collection Forms
▪ There is currently a major burden of having to fill out multiple registers within the same health facility by the same person
Registers
▪ There are currently the following registers: ▪ Community Management of Acute Malnutrition (CMAM) Daily Screening & Referral Register ▪ Blanket Supplementary Feeding Program (BSFP) Daily Register (OTP) ▪ Targeted Supplementary Feeding Program (TSFP) Daily Register (OTP) ▪ Severe Acute Malnutrition (SAM) Daily Register ▪ Community Health and Nutrition Volunteer (CHNV) Daily Register ▪ Therapeutic Feeding Centre (TFC) Severe Acute Malnutrition (SAM) Daily Register ▪ Outreach only-General Register for Mothers ▪ Outreach only-General Register for Children ▪ Infant and Young Child Feeding (IYCF) Corners Daily Register ▪ Registers need to be analysed to ensure they have same indicator/data- harmonize them is
depending on the indictors need to monitor. ▪ Suggestion for One CMAM register for outpatient therapeutic programme (OTP)/Blanket
Supplementary Feeding Programme (BSFP)/Targeted Supplementary Feeding Programme (TSFP)
▪ Keep separate IYCF/E register due to the qualitative info related to IYCF Tally Sheets
▪ Consider summary tally sheet for use of services, inputs of services, shifts, & logistics Referrals
▪ Consider combining referral forms there are currently 2 referral forms58 with same content ▪ Consider longer term merging nutrition with national health referral form
58 Community Health and Nutrition Volunteer (CHNV) Referral Card (Referral card from CHNVs to OTP/SFP), Community Management of Acute Malnutrition (CMAM) Daily Screening & Referral Register

64
Table 18: Yemen Nutrition Data Collection Forms and Collection Details
Name of Data Collection Form Type of Form Individual who fills the form
Service Delivery Entry Points
Frequency Submitted to Updated Date
1. Community Management of Acute Malnutrition (CMAM) Sites
Community Management of Acute Malnutrition (CMAM) Daily Screening & Referral Register (for both outpatient therapeutic care (OTP) and Targeted Supplementary Feeding Program (TSFP)
Register Paper-based
Health Worker at HF
CMAM Health Facility site
Daily Stays at HF During the month
OTP & TSFP
Community Management of Acute Malnutrition (CMAM) Monthly Report
Monthly Report Paper-Based
Health Worker at HF
CMAM Health Facility site
Monthly District Health Office (DHO)-Nutrition
At end of the month
Moderate Acute Malnutrition (MAM) OTP Daily Register Register Paper-based
Health workers
CMAM Health Facility site Daily Stays at HF During the month
MAM OTP
Cooperating Partners' Monthly Distribution Report (CPDR) (for MAM)
Monthly Report Excel-based
Mobile Teams tracking (mobile team supervisor) Monthly Field Info (Governorate Health Officer (GHO) Nutrition Coordinator or L/INGOs focal persons
CMAM Health Facility site MAM OTP
Monthly
MAM WFP IMO
Severe Acute Malnutrition (SAM) OTP Daily Register Register Paper-based
Health workers
CMAM Health Facility site Daily Stays at HF During the month
SAM OTP
Severe Acute Malnutrition (SAM) OTP Monthly Reporting Tool Monthly report Excel-Based
District Health Officer (DHO)-Nutrition
CMAM Health Facility site Monthly
Governorate Health Office – Nutrition (GHO)
5th of every month
SAM OTP
Therapeutic Feeding Center (TFC) SAM Daily Register Register Paper-based
Health workers Therapeutic Feeding Center (TFC)
Daily Stays at HF During the month
2. Community Health and Nutrition Volunteer (CHNV)
Community Health and Nutrition Volunteer (CHNV) Daily Register
Register Paper-based, This is used to screen all U5 children who attend to the HF/MT to identify the nutrition status and refer the child to the appropriate program.
Community Health and Nutrition Volunteer
Community Daily Stays with CHNV for daily record
During the month
Community Health and Nutrition Volunteer (CHNV) Monthly Report
Register Community Health and Nutrition Volunteer
Monthly Health Facility at end of the month
Paper-based
CHNVs Monthly Report Summary at HF level Register Paper-based Health worker Monthly DHO 5th of every month
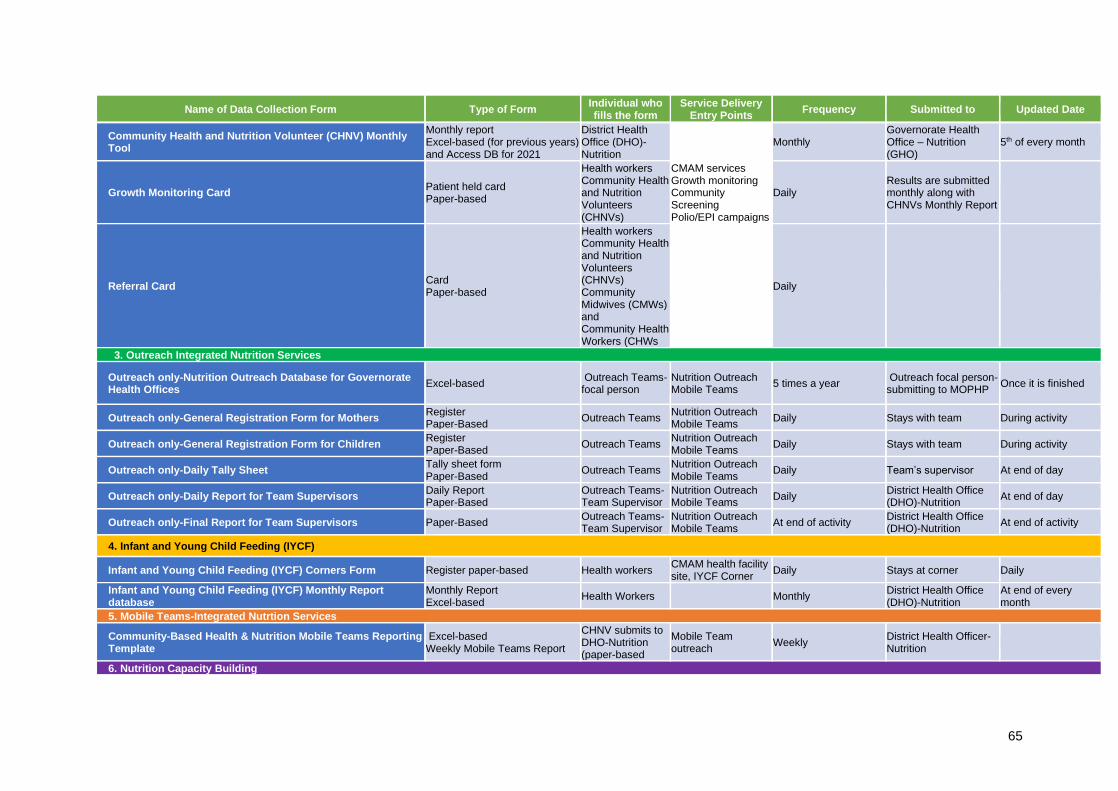
65
Name of Data Collection Form Type of Form Individual who fills the form
Service Delivery Entry Points
Frequency Submitted to Updated Date
Community Health and Nutrition Volunteer (CHNV) Monthly Tool
Monthly report Excel-based (for previous years) and Access DB for 2021
District Health Office (DHO)-Nutrition
Monthly Governorate Health Office – Nutrition (GHO)
5th of every month
Growth Monitoring Card Patient held card Paper-based
Health workers Community Health and Nutrition Volunteers (CHNVs)
CMAM services Growth monitoring Community Screening Polio/EPI campaigns
Daily Results are submitted monthly along with CHNVs Monthly Report
Referral Card Card Paper-based
Health workers Community Health and Nutrition Volunteers (CHNVs) Community Midwives (CMWs) and Community Health Workers (CHWs
Daily
3. Outreach Integrated Nutrition Services
Outreach only-Nutrition Outreach Database for Governorate Health Offices
Excel-based Outreach Teams-focal person
Nutrition Outreach Mobile Teams
5 times a year Outreach focal person-submitting to MOPHP
Once it is finished
Outreach only-General Registration Form for Mothers Register Paper-Based
Outreach Teams Nutrition Outreach Mobile Teams
Daily Stays with team During activity
Outreach only-General Registration Form for Children Register Paper-Based
Outreach Teams Nutrition Outreach Mobile Teams
Daily Stays with team During activity
Outreach only-Daily Tally Sheet Tally sheet form Paper-Based
Outreach Teams Nutrition Outreach Mobile Teams
Daily Team’s supervisor At end of day
Outreach only-Daily Report for Team Supervisors Daily Report Paper-Based
Outreach Teams-Team Supervisor
Nutrition Outreach Mobile Teams
Daily District Health Office (DHO)-Nutrition
At end of day
Outreach only-Final Report for Team Supervisors Paper-Based Outreach Teams-Team Supervisor
Nutrition Outreach Mobile Teams
At end of activity District Health Office (DHO)-Nutrition
At end of activity
4. Infant and Young Child Feeding (IYCF)
Infant and Young Child Feeding (IYCF) Corners Form Register paper-based Health workers CMAM health facility site, IYCF Corner
Daily Stays at corner Daily
Infant and Young Child Feeding (IYCF) Monthly Report database
Monthly Report Excel-based
Health Workers Monthly District Health Office (DHO)-Nutrition
At end of every month
5. Mobile Teams-Integrated Nutrtion Services
Community-Based Health & Nutrition Mobile Teams Reporting Template
Excel-based Weekly Mobile Teams Report
CHNV submits to DHO-Nutrition (paper-based
Mobile Team outreach
Weekly District Health Officer-Nutrition
6. Nutrition Capacity Building

66
Name of Data Collection Form Type of Form Individual who fills the form
Service Delivery Entry Points
Frequency Submitted to Updated Date
Nutrition Capacity Building Field Information Report Quarterly Report Excel-based
Governorate/ District Health – Nutrition Offices Implementing Partners
Nutrition capacity building/training events
Quarterly MoPHP/UNICEF
7.Nutrition Cluster Reporting
Nutrition Cluster Caseload Calculations & Targets Excel-based UNICEF Implementing Partners
Nutrition Cluster Bi-annual
Share it with NC partners and Publish it on the NC webpage on ten HR.info
During preparing the HRP and after midyear review,
Nutrition Cluster Assessments Summary Excel-based Implementing Partners
Nutrition Cluster At end of activity (Survey conducted)
Share it with NC partners and Publish it on the NC webpage on ten HR.info
After the Survey preliminary or final report published,
Nutrition Cluster Monthly Summary Analysis Excel-based Implementing Partners
Nutrition Cluster Monthly
Share it with NC partners and Publish it on the NC webpage on ten HR.info
End of the next month
Nutrition Cluster 4 W’s matrix (Who Does What, When and where)
Excel-based Implementing Partners
Nutrition Cluster Monthly
Share it with NC partners and Publish it on the NC webpage on ten HR.info
Every month

67
Annex 7: Indicator Reference Guide Indicator Reference Sheet
Example GLOBAL TARGET GLOBAL TARGET 1 By 2030, a 50% reduction globally of the number of children under five who are stunted
Standards World Health Assembly Targets (WHA) Indicators and Targets
World Health Organization (WHO) United Nations Children’s Fund (UNICEF) Scaling up Nutrition (SUN) Indicator Yemen standard here
Results Framework
Indicator Prevalence of Stunted Children: Children under 5 years who are stunted (moderate and severe): Percentage of stunted (moderate and severe) children aged 0–59 months (moderate stunting = length/height-for-age between <-2 and >-3 SD of the WHO Child Growth Standards median; severe stunting = height-for-age below -3 SD of the WHO Child Growth Standards median) x under-five population at the time of the survey.
Definition Stunting is a height-for-age measurement that is a reflection of chronic undernutrition. This indicator measures the proportion of children under 2 years of age below -2 standard deviations (-3 standard deviations for severe stunting) from the median height-for-age of WHO/NCHS reference population. Height-for-age: Height-for-age reflects achieved linear growth and its deficits indicate long-term cumulative health or nutritional inadequacies. Two related terms – length and stature – are also used. Length refers to measurement in a recumbent (horizontal) position, as often done for children below 2 years of age, who cannot stand well. Standing height measurement is often referred to as stature. Z-score or standard deviation value system: the most preferred measuring system of anthropometric indices. The Z-score system expresses the anthropometric value as a number of standard deviations or Z-scores below or above the reference mean or median value. A fixed Z-score interval implies fixed height or weight differences for children of a given age. For population-based uses, a major advantage is that a group of Z-scores can be subjected to summary statistics, such as the mean and the standard deviation of the Z-scores. World Health Organization/ National Centre for Health Statistics (WHO/NCHS) Reference population is a
general guide for individual-based screening and population-based monitoring; it is not intended to be a rigid diagnostic criterion for defining malnutrition. Proper application requires that a number of local and external sources of information be taken into account. If the reference population is utilized in such a flexible manner, a single reference can be used for a wide range of populations with diverse environmental conditions and nutritional status.
This indicator will be used to measure cumulative deficient growth associated with long-term factors including chronic insufficient dietary intake, frequent infection, poor feeding practices over a sustained period, and possibly low socio-economic status of the household.
To classify levels of stunting for global monitoring, the prevalence ranges shown in this table are recommended by WHO.
Height-for-age stunting prevalence ranges
Group Children below -2 standard deviations from the median
Low Less than 20%
Medium 20 – 29%
High 30 – 39%
Very high 40% and over
Unit of Measurement
Percentage, Outcome
Disaggregation ▪ Sex (male, female) ▪ Ages: 0-6 months of age, 6-23 months of age, 24-59 months of age
METHOD OF ESTIMATION Numerator Percent of stunted children =
Number of children aged 0–59 months1 who were stunted.
Denominator Total number of children aged 0–59 months who were measured. Children aged 0–59 months who are stunted for age Total number of children aged 0–59 months who were measured Percent of stunted children = *100

68
Data Availability Since 1989, WHO maintains the Global Database on Child Growth and Malnutrition (available at: http://www.who.int/nutgrowthdb/en/). This global database aggregates population-based surveys that include anthropometric measurements of representative samples of children less than 5 years of age.
Data Sources Main sources of data are population-based household surveys with anthropometry and nutrition surveillance systems.
Data Quality Population-based surveys that fulfil a set of criteria. Data are checked for validity and consistency and raw data sets are analysed according to a standard procedure to obtain comparable results. The main criteria for including surveys in the database are: (i) a defined population-based sampling frame; (ii) a probabilistic sampling procedure involving at least 400 children; (iii) use of standard anthropometric measurement techniques; and (iv) presentation of results in z-scores in relation to the WHO child growth standards. To facilitate re-running of nutritional survey data, WHO recommends using either the new software WHO Anthro or the statistical macros. Both can be downloaded together with manuals and Readme files (available at: http://www.who.int/childgrowth/software/en/). The WHO Anthro "Nutritional survey" software module enables analysis of existing data sets. The macros are available for SPSS, SAS, STATA and S-Plus; And they are particularly recommended for analysis of large survey data sets. Both the software and the macros allow the user to produce result tables in the standard data-entry format ready for submission to the Global Database.
Frequency of Data Collection
Every 3–5 years
Guidance for Anthropometric Data Collection
Determination of a child’s age is the first and most important step in anthropometric assessment. Accurate age is required for sampling whether a child should be included in the survey and to determine whether a child’s recumbent length or standing height should be measured. A child’s age plays a role when deriving correct z-scores for age-related indicators (the WHO growth standards are expressed in units of days).
Length/Height Recumbent length should be measured for children less than 24 months of age and standing height should be measured for children 24 months and above. Detailed descriptions on length/ height board, training and standardization procedures for anthropometry and essential steps of measurements are presented iby WHO/UNICEF. For further details on anthropometric measurements, see also the WHO Training Course on Child Growth Assessment 59 60 DHS guidance61 and Cogill 200362.
Guidance on Reporting
Prevalence of stunting in children less than 5 years of age should be presented for the total sample and disaggregated by age, sex, place of residence, region, socioeconomic status and mothers’ education. It is useful to present stunting data by severity – moderate (z-score between <-2 and >-3 SD) and severe (z-score below -3 SD).
59 “WHO | Training Course on Child Growth Assessment.” Accessed November 3, 2020. https://www.who.int/nutrition/publications/childgrowthstandards_trainingcourse/en/ 60 WHO. “WHO | Physical Status: The Use and Interpretation of Anthropometry.” World Health Organization. Accessed November 3, 2020. https://www.who.int/childgrowth/publications/physical_status/en/ 61 “Collecting Quality Anthropometric Data in The DHS Program | The DHS Program Blog.” Accessed July 6, 2020. https://blog.dhsprogram.com/collecting-quality-anthropometric-data-in-the-dhs-program/ 62 Cogill, Bruce. “Anthropometric Indicators Measurement Guide.” Washington, D.C. USA, 2001.

69
Annex 8: Stakeholders (by Level) Management of Nutrition Data Collection and Reporting
Table 19: Stakeholders (by Level) Management of Nutrition Data Collection and Reporting
Health Workers
Community Health and Nutrition Volunteers (CHNVs)
District Health Officers (DHO) Nutrition
Coordinators
Governorate Health Officers (GHO)
Nutrition Coordinators
MOPHP Central/ National Level
UN Agencies Information Management Officers
(IMOs) & INGO Nutrition M & E Focal Persons
Data Entry & Data Collection
▪ Daily Registers ▪ Growth Monitoring
Card ▪ CMAM Daily
Screening & Referral Register (for both OTP and TSFP)
▪ MAM OTP Daily Register
▪ SAM OTP Daily Register
▪ TFC SAM Daily Register
▪ IYCF Corners Form ▪ Referral Card
▪ Daily Registers ▪ Growth Monitoring
Card ▪ Referral Card
Multiple Databases: ▪ CMAM Database ▪ SAM Database ▪ MAM Database ▪ TFC Database ▪ Nutrition Site
Surveillance Database
▪ IYCF Database
Multiple Databases: ▪ CMAM
Database ▪ SAM Database ▪ MAM Database ▪ TFC Database ▪ Nutrition Site
Surveillance Database
▪ IYCF Database ▪ Nutrition
Capacity Building Field Information database
Multiple Databases: ▪ CMAM Database ▪ SAM Database ▪ MAM Database ▪ TFC Database ▪ Nutrition Site
Surveillance Database
▪ IYCF Database ▪ Nutrition Capacity
Building Field Information database
Multiple Databases: ▪ CMAM Database ▪ SAM Database ▪ MAM Database ▪ TFC Database ▪ Nutrition Site
Surveillance Database
▪ IYCF Database ▪ Nutrition Capacity
Building Field Information database
Daily, Weekly & Monthly Reporting
▪ Monthly Reports ▪ Multiple Databases ▪ CHNVs Monthly
Report Summary at HF level
▪ CMAM Monthly Report
▪ TFC Monthly Report ▪ IYCF Monthly Report
database
▪ Monthly Reports ▪ CHNV Monthly
Report ▪ CHNVs Monthly
Report Summary at HF level
▪ CHNV Monthly Tool
▪ Community-Based Health & Nutrition Mobile Teams Reporting Template
▪ Monthly Reports ▪ Multiple Databases ▪ CMAM Monthly Report ▪ CHNV Monthly Tool ▪ SAM OTP Monthly
Reporting Tool ▪ TFC Monthly Report ▪ Outreach only- Daily
Report for Team Supervisors
▪ Outreach only- Final Report for Team Supervisors
▪ IYCF Monthly Report database
▪ Nutrition Capacity Building Field Information Report
▪ Community-Based Health & Nutrition Mobile Teams Reporting Template
▪ Monthly Reports ▪ Multiple Databases ▪ SAM OTP Monthly
Reporting Tool ▪ Outreach only -
Nutrition Outreach Database for Governorate Health Offices
▪ Nutrition Capacity Building Field Information Report
▪ Multiple Databases ▪ MAM WFP IMO: Cooperating Partners' Monthly Distribution Report (CPDR) (for MAM)
▪ Nutrition Capacity Building Field Information Report

70
Annex 9: Proposed Draft Sub-National Scorecard Indicators
Table 20: Yemen Proposed Draft Sub-National Scorecard Indicators
Individuals Assessed/ Screened for Acute Malnutrition
Management of Acute Malnutrition (Wasting) Coverage
Acute Malnutrition Defaulter Rate
Community Management of Acute Malnutrition (CMAM) Coverage
Targeted Supplementary Feeding Programmes
Iron-Folic Acid (IFA) Supplementation Coverage for Pregnant Women
Supply Chain Management
1. Acute Malnourished Individuals Assessed: Number of acutely malnourished children under 5 (0-59 months of age) assessed/screened by community health and nutrition workers and referred to sites providing integrated management of acute malnutrition
2. Moderate Acute Malnutrition (MAM) Coverage (Admissions): Percentage of (Proportion) of children under 5 who were admitted for treatment of moderate acute malnutrition 3. Severe Acute Malnutrition (SAM) Coverage (Admissions): Percentage (Proportion) of children 6–59 months of age with severe acute malnutrition (SAM) admitted for treatment Number of children treated in OTP and SFP
4. Moderate Acute Malnutrition (MAM) Defaulter Rate: Percentage of (Proportion) children under 5 years of age (6-59 months of age) with MAM defaulting 5. Severe Acute Malnutrition (SAM) Defaulter Rate: Percentage of (Proportion) children under 5 years of age (6-59 months of age) with SAM defaulting
6. Community Management of Acute Malnutrition Outpatient Sites: Total number of fixed Outpatient Therapeutic Programme (OTP) CMAM sites (disaggregated by MAM and SAM sites) 7. Therapeutic Feeding Centres (TFC)/ Stabilization Centre: Number of fixed Therapeutic Feeding Centres/Stabilization Centres (TFCs/SCs) (inpatient sites).
8. Targeted Supplementary Feeding Programmes Admissions for MA: Number of individuals enrolled in services for Targeted Supplementary Feeding Programmes for treatment of MAM
9. Iron Folic Acid Supplementation: Number of mothers who received micronutrient supplementation (Folic Acid + Iron tablets) Common Results Framework (CRF)
10. Specialized Food Products: Number of and Percentage of children under 5 (6-59 months of age) who received ready to use specialized food products (supplementary plumpy SUP) or ready to use therapeutic foods (RUTF) (Plumpy’ Nut) 11.No Stock Outs: Number of health facilities that do not experience stock-outs
Infant and Young Child Feeding (IYCF) Multisectoral Nutrition Governance
Exclusive breastfeeding for children under 6 months
Infant & Young Child Feeding Support
Trainings for Nutrition District Nutrition Multisectoral Plans
Multisectoral Nutrition Information System
12: Exclusive Breastfeeding: Prevalence of exclusive breastfeeding of children under six months of age: Percentage of infants <6 months of age who are fed exclusively with breast milk
13. Estimated number of individuals receiving Infant & Young Child Feeding Support
14. Nutrition Trainings: Number of individuals (disaggregated by technical/management, trainer of trainers, health workers and community health and nutrition volunteers) trained by type of training (CMAM, IYCF, CHNV)
15. District Nutrition Multisectoral
Plans: Percentage of Districts with
(Annual) Operational District
Nutrition Multisectoral plans
developed and operationalized (Annual)
16. Nutrition Scorecard Completed and Used for
Decision-Making: Percentage of Districts with
indicators completed in the Nutrition Scorecard
with Nutrition Data at a Specific Reporting Period (quarterly) and used for quarterly nutrition meetings at the GHO and DHO levels.

71
Annex 10: Level of Healthcare, Type of Health Facilities, Catchment
Area, Staffing and Nutrition Services Offered
Table 21: Level of Healthcare, Type of Health Facilities, Catchment Area, Staffing and Nutrition Services Offered
Level of Healthcare
Type of Health Facility Geographic Area Population Catchment
Area
Staffing Nutrition Services Offered
Primary Health Care
PHC Center Groups of villages ▪ Urban ▪ Rural (rarely) ▪ Outpatients
clinics and polyclinics (urban only)
Population up to 10,000 households
Health worker nutrition M & E focal person (who has other responsibilities)
1. Acute malnutrition screening 2. CMAM Services (both moderate acute malnutrition and severe acute malnutrition including Outpatient for acute malnutrition and inpatient (inpatient services (TFCs) 3. Outpatient supplementary feeding programme (SFP) 4. IYCF Corners 5. Nutrition Preventive Services
Primary Health Care
PHC Units -Fixed Health Care Unit
▪ Urban ▪ Rural ▪ A cluster of
villages
Population up to 5,000 households
1-2 Health Workers Nurse/Midwifes Health worker nutrition M & E focal person (who has other responsibilities)
1. Acute malnutrition screening 2. CMAM Services (not all PHC units) 3. IYCF Corners 4. Nutrition Preventive Services
Primary Health Care
PHC Community Supported Shared Temporary Health Unit (i.e., schools, sheik in village house room, etc.)
▪ Urban ▪ Rural ▪ A group of
villages (Hamlets)
Population up to 1,000 households
3-4 staff 1. Acute malnutrition screening 2. CMAM Services (not all PHC temporary units) 3. Nutrition Preventive Services
Primary Health Care
PHC Outreach-Mobile Health Services
Mobile outreach Health worker nutrition M & E focal person (who has other responsibilities)
1. Acute malnutrition screening 2. CMAM Services 3. Nutrition Preventive Services 4. IYCF 5. Health services (Expanded Programme of Immunization (EPI), integrated management for childhood illness

72
Table 21: Level of Healthcare, Type of Health Facilities, Catchment Area, Staffing and Nutrition Services Offered
Level of Healthcare
Type of Health Facility Geographic Area Population Catchment
Area
Staffing Nutrition Services Offered
(IMCI), and reproductive health (RH)
Primary Health Care
Community-Based Health Services (Community Outreach)
Village level (Hamlet63)
▪ Community-Based Health and Nutrition Volunteers (female health worker is called Murshada
▪ Traditional Birth Attendants (TBAs)
▪ Community Educators (Murshadaat) and
▪ Community Based Distributors of contraceptives.
1. Acute malnutrition screening 2. CMAM referral 3. IYCF 4. Nutrition preventive services 5. Growth Monitoring for Children Under 2 years of age
Secondary Health Care
District Hospital (referral care)
▪ Urban ▪ Main town of
the District
40-60 beds with 4 specialists and 78-82 technical staff members
4 specialists and 78-82 technical staff members Health worker nutrition M & E focal person (who has other responsibilities)
1. Acute malnutrition screening 2. CMAM Services including OTPs and TSFPs. 3. Inpatient TFC 4. IYCF Corners 5. Nutrition preventive services.
Secondary Health Care
Governorate Hospital (referral care)
▪ Urban ▪ Capital of
Governorate
Governorate Hospital (up to 200 beds and up to 200 technical staff members)
200 technical staff members Health worker nutrition M & E focal person (who has other responsibilities)
1. Acute malnutrition screening 2. CMAM Services including OTPs and TSFPs. 3. Inpatient TFC 4. IYCF Corners 5. Nutrition preventive services.
Tertiary Health Care
Specialized Care/Teaching/Referral Hospitals Authority Hospital
Sana’a and Aden ▪ Urban ▪ Main town of
the District
Specialized and University Hospitals with all specialties (up to 500 bed with 410 technical staff members)
410 technical staff members Health worker nutrition M & E focal person (who has other responsibilities)
1. Acute malnutrition screening 2. CMAM Services including OTPs and TSFPs. 3. Inpatient TFC 4. IYCF Corners 5. Nutrition preventive services.
63That is, tribes are sub-divided into "quarters" comprised of clusters of hamlets