Nutrigenomics White Paper

of 36
-
Upload
ana-raudhatul-jannah -
Category
Documents
-
view
229 -
download
0
Transcript of Nutrigenomics White Paper
-
7/25/2019 Nutrigenomics White Paper
1/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page1
The Power of Nutrigenomics:
A Practical Guide for Application in theTreatment of Chronic Illness
Advances in the understanding of genetics are changing the wayhealthcare professionals think about disease causes and prevention. It'snow accepted that a person's state-of-health arises from the dynamicinteraction of environmental factors with his or her genetic uniqueness.And, nutrition has emerged as a primary environmental factor that canpositively or negatively impact the extent to which a person will realize
his or her genetic potential.
Nutrition research in the past has focused on nutrient deficiencies andimpairment of health.1But the Human Genome Project has led to theconcept of personalized medicine not only with drugs(pharmocogenetics), but with nutritional modalities as well.1-4Nutritionalgenomicsor nutrigenomicsis the junction between health, diet, andgenomics.1In other words, nutrigenomics is the effect that nutritivesubstances and phytochemicals have on genetic expression withinhuman cells.
As a growing field of research, nutrigenomics is the recognition of theability to optimize nutrition for maintaining and extending a state ofoptimal health.5This growing field of research has demonstrated the
effects that nutrients and botanicals can have on modifying geneexpression, prompting the development of research-basednutraceuticals, functional foods, and dietary approaches to addressdisorders in genetically pre-disposed individals.2,3,5
The Future of Health CareHere Today
New developments in nutrigenomic research are predicted to offerenormous potential for the development of dietary optimizationapproaches.
5But you wont have to wait for therapies applying basic and
advanced nutrigenomic principals to benefit the health of your patients.Theyre already here.
Nutrigenomics in clinical practice entails using specified, defined
nutrients and nutritional programs to target genetic expression forimproved patient outcomes without serious adverse effects. These new,patient-centered approaches to health care rely upon nutrition and othermodifiable lifestyle factors to help people achieve optimal geneticexpression.
White Paper
Clinically effective modalities
for applying nutrigenomicsare already in use in a variety
of healthcare practices.
-
7/25/2019 Nutrigenomics White Paper
2/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page2
Table of Contents
The Nutrigenomics Matrix........... 3
3-Phase Plan for Implementing Nutrigenomics......... 4Phase 1AChanging Primary Dietary Signals with TLC.. 6
Help for Implementing Dietary Signal Changes... 7
Cardiovascular & Insulin Resistance Conditions.........8
Inflammatory, Gastrointestinal, Autoimmune & Fatigue
Disorders............................................................................... 8
Hormone Imbalances & Cyclerelated Symptoms.. 9
Phase 1BChanging Primary Dietary Signals with Medical Foods..10
The SKRM Effect: Creating the Next Generation of Medical
Foods 10
Metabolic Syndrome & Cardiovascular Disease....11
Inflammatory Bowel Disease (Autoimmune Support)... 13
Type 2 Diabetes.. 14
Chronic Fatigue Syndrome (Live Detoxification Support)15
Premenstrual Syndrome .. 16
Leaky Gut Syndrome . 17
Phase 2Modulating Kinase Signaling with SKRMs..18
Insulin SKRMs. 19
Inflammation & Autoimmune SKRMs.. 21
Future SKRMs........ 23
Phase 3Recommending Key Nutritional Support. 24
Cardiovascular Support. 24
Blood Sugar Metabolism Support 25
Liver Detoxification Support.. 25
Intestinal Support 26
Joint Inflammation Support... 27
Hormone Balance Support .. 27
Putting It All Together 29
Appendices
Applying Nutrigenomics for Children & Teens... 30
The Need for Therapeutic Lifestyle Changes 31
References.. 32
-
7/25/2019 Nutrigenomics White Paper
3/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page3
The Nutrigenomics Matrix
This chart is provided for your reference as a summary of how
nutrigenomics can easily be put into practice for the health of yourpatients. The combination of healthy dietary choices, medical foods,SKRMs, and other targeted nutrients can be a revolutionary avenue ofsupport for those suffering from a number of chronic illnesses.
This is the power of nutrigenomics.
ConditionsDietarySignal
ModificationMedical Food Support SKRMs
KeyNutritional
Support
MetabolicSyndrome &
CardiovascularDisease (CVD)
FirstLineTherapy
UltraMealPLUS 360
featuring SKRMs
UltraMeal
UltraMealPLUS
RIAA &Acacia
CoQ10EFAs
InflammatoryBowel Disease(IBD)
FirstLineTherapy
UltraInflamXPLUS
360 featuring SKRMs
UltraInflamX
RIAA GlucosamineChondroitinMSM
Type 2Diabetes
FirstLineTherapy
UltraGlycemX
PLUS360featuring SKRMs
RIAA &Acacia
CinnamonGreen Tea
ChronicFatigueSyndrome(liverdetoxificationsupport)
FirstLineTherapy
UltraClear
UltraClear PLUS
UltraClearPlus pH
Proteomicresearch inprogress
SilymarinCatechins
ArtichokeLeafWatercressEllagic Acid
Leaky GutSyndrome
FirstLineTherapy
UltraClear SUSTAIN
Probiotics
PremenstrualSyndrome(PMS)
FirstLineTherapy
Estrium Kudzu
Red CloverTurmericResveratrol
Stabilized I3C
The principles of
nutrigenomics can be appliedeasily in any healthcare
practice.
-
7/25/2019 Nutrigenomics White Paper
4/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page4
3-Phase Plan for ImplementingNutrigenomics
You can easily tailor and prescribe a program for patients presentingwith a variety of common and chronic health conditions. A nutrigenomicapproach to wellness can include any or all of the following:
1A. Dietary Signal Modification with TLCWestern diets, foods of convenience, and other unhealthydietary habits can muddle the signals sent to cells throughoutthe body, fostering negative genetic (phenotypic) expressionthat leads to premature aging and disease. What people eat,therefore, may have a direct influence on how they feel. Andaddressing those eating patterns allows your patients tomanage symptoms and even halt or reverse the progression oftheir illnesses.
You can help them make informed decisions that impact theirhealth by offering therapeutic lifestyle changes (TLC). TLC canprovide food plans that incorporate nutrigenomic principles for abroad population, then further customize these plans based onpatient response, individual concerns, and specific nutritionalneeds.
1B. Dietary Signal Modification with Medical FoodsMedical foods offer an adjunct approach to dietaryrecommendations to nutritionally manage specific conditions. Amedical food is formulated with macro- and micronutrients thatare recognized by scientific principles to support the dietarymanagement of a disease or condition, and is to beadministered under the supervision of a physician or licensedhealthcare practitioner.
Medical foods contain nutrients that typically cannot be acquiredthrough normal dietary measures. Some patients may require alevel of nutritional support that simply cannot be met by even afood plan with the best intentions. Medical foods offer apowerful tool, yet can be very simple to implement in yourpractice.
2. Selective Kinase Response Modulators (SKRMs)Dietary signals are translated by enzymes known as kinases atthe cellular level, helping to direct genetic expression. Selectivekinase response modulatorsor SKRMsare nutritionalsubstances that can work to modulate kinase signaling backinto balance, helping to restore healthy signaling to genes,favorably affect genetic expression, and reverse the effects ofchronic illness.
Adopt a simple, 3-phase plan
for applying nutrigenomics in
your practice.
-
7/25/2019 Nutrigenomics White Paper
5/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page5
Where an unhealthy diet makes the kinase signaling unclear,SKRMs help increase the volume of the message for positivegenetic expression and preservation or restoration of health.These research-based nutritional substances offer the newestavenue for a natural approach to wellness that embodies theideals of nutrigenomics.
3. Targeted Nutritional SupportEven the most comprehensive approach to wellness mayrequire additional nutritional support for maintaining health,addressing specific symptoms, or customizing approaches forpatients with multiple health concerns.
Outlined here are just a few approaches of the hundreds ofpossibilities for targeted nutritional applicationsfrom additionalsupport for joint protection and restoring healthy gut ecology tomaintaining healthy hormone balance and blood sugar levels.
-
7/25/2019 Nutrigenomics White Paper
6/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page6
Phase 1AChanging Primary Dietary Signals with TLC
The first step in a nutrigenomics intervention is changing primary dietarysignals. Foods contain nutrients serving as dietary signals that travel tocells throughout the body, where they are translated by kinases. Healthyfood choices foster healthy signaling. Poor food choices, however, cantrigger a disorder of kinase signaling, resulting in poor geneticexpression and, ultimately, chronic illness.6,7In fact, poor nutrition is oneof the three leading factors attributed to 70% to 90% of mortalities fromchronic illnesses in the U.S. alone.8
Prior to the commercialization of the Western diet, humans (overcenturies) developed a relationship with commonly eaten foods. Existingin harmony with these foods meant dietary signals that were adequate tomaintain health. Changing the diet with commercialized foods andintroducing foreign substances creates a state of cellular stress wheremessages can be distorted and negatively affect physiological function.6But these negative dietary signals dont have to be a part of modernliving, nor do the long-term costs of premature aging and chronicdisease development.
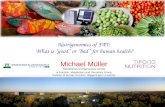
Figure 1. The nutrients (or lack thereof) and other foreign substances (xenobiotics) ina diet can both directly and indirectly influence genetic expression, impacting health.
Unhealthy diets are a leading
cause of chronic illness
fatalities.
Modifying Genetic Expression
Diet, Exercise& Lifest le
Nutrients &Xenobiotics
Metabolism
Gene Expression
Cell Phenotype
Signal Transduction
Direct Indirect
-
7/25/2019 Nutrigenomics White Paper
7/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page7
How can you help modify your patients dietary signals? This can beaccomplished through therapeutic lifestyle changes (TLC). Scientificevidence in support of TLC programs as a fundamental therapy forchronic conditionsincluding cardiovascular disease (CVD), type 2diabetes, and obesitycontinues to grow.7,9-21
An optimal TLC program should include recommendations for exercisefor a comprehensive approach. It should also provide the means andflexibility for further personalization of condition-specific support withnutrients that may not be possible to obtain through dietary measuresor difficult to obtain in therapeutic amounts. Medical foods (Phase 1B onpage 10) are designed to complement dietary approaches for thenutritional management of specific conditions.
Help for Implementing Dietary Signal Changes
The responsibilities of a patient change in the management of chronicdisease. Because the patient takes on a caretaker role in the treatmentprocess, greater educational efforts are needed for successfuloutcomes.
22,23Unfortunately, many practices are set up for acute
disease management rather than chronic illness care, and may not beprepared to institute efforts such as lifestyle modification programs.
23
FirstLine Therapyis an example of a TLC program that can helphealthcare practitioners teach their patients how to adopt dietarychanges that can positively affect kinase signaling to support geneticexpression, befitting a longer, healthier life.
The FirstLine Therapyfood plans are based on a traditionalMediterranean-style eating plan that has an overall low glycemic load(for balancing blood sugar), low in arachidonic acids (anti-inflammatory),and high in phytonutrients. Moreover, the foods have been screened fora history of safe use and for unique molecules that have the ability tomodulate kinase signaling in a positive manner. These foods affectsignal transduction to help increase the clarity of messages sent tokinases, creating a potential to combat chronic disease and restoreoptimal wellness. A disordered physiology will respond to these newsignal conductors, reducing the burden of prior unhealthy eating habits.
For optimal support, these dietary changes may be customizedthrough tailored food plans and medical foodsto meet the specificneeds of patients, such as those with conditions related to insulinresistance, cardiovascular disease, autoimmune disorders, inflammatoryconditions, fatigue syndromes, and hormone imbalances.
TLCthe first step in
harnessing the power of
nutrigenomics.
-
7/25/2019 Nutrigenomics White Paper
8/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page8
Cardiovascular & Insulin Resistance Conditions
Many conventional dietary programs recommended by leading
health organizations are lowfat, high-carbohydrate diets designed tolower elevated cholesterol levels. However, individuals on thesediets may eat high-glycemic-index foods that can cause spikes inblood sugarincreasing hunger, decreasing satiety (feeling offullness), and fostering insulin resistance and a variety of relatedhealth problems. Most importantly, these diets may not produce thedesired results.19
Dietary choices causing a high insulin response have been linked tothe development of metabolic syndrome, type 2 diabetes, andcardiovascular disease (CVD).12,24-26Research has demonstrated,for example, that the Western dietalso referred to as the StandardAmerican Diet (SAD)modulates kinases and insulin signaling.27
Science-based recommendations include reducing consumption ofhigh-glycemic-index foods (e.g., simple sugars, processed andsnack foods) and/or replacing them with low-glycemic-index fruits,vegetables, and whole grains.
12,28-30This also adds fiber for a lower
overall glycemic load (GL).26
A low-GL food plan promotes healthy blood sugar and energy levelsin your patients. Research also links insulin resistance to CVD risk(as is the case in metabolic syndrome), making this an appropriateeating plan for cardiovascular disease.13,19Low-GL diets have alsobeen shown useful in conditions involving inflammation andoxidative stress, reinforcing its application for CVD patients.
21,31
Inflammatory, Gastrointestinal, Autoimmune & Fatigue Disorders
Diet may also represent a significant immune-modulating part of apatients environmental exposure. An increasing body of researchsuggests that chronic or recurring inflammatory disorders may bereactions to substances that trigger an immune response from thegastrointestinal (GI) tract. Dietary changes may have a noticeableimpact on modifying the underlying inflammatory signals that areassociated with autoimmune disorders. Scientific studies havedemonstrated the effectiveness of dietary therapies in alleviating thesymptoms and even in altering the progression of inflammatory andautoimmune conditions.
31-49
Research suggests that many common inflammatory and
gastrointestinal conditions are triggered by sensitivities or reactionsto certain foods and that removing these offending foods mayprovide relief.32-49Broad guidelines for eliminating common foodsthat trigger inflammation can be customized as patients slowly
-
7/25/2019 Nutrigenomics White Paper
9/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page9
challenge the reintroduction of foods to determine those that mayexacerbate symptoms.
A low-GL diet has also been shown to be beneficial in reducingoxidative stressthe overproduction of damaging free radicalsassociated with chronic fatigue syndrome and conditions such asrheumatoid arthritis and inflammatory bowel disease (IBD).
31Low-
GL foods that are rich in antioxidantsberries, red grapes, garlic,spinach, whole grainscan help restore the bodys balance ofantioxidants and combat harmful free radicals generated byenvironmental toxins, inflammation, and unhealthy lifestyle habits.
While a modified elimination diet may provide an approach for long-term condition and symptom management, sometimes a moreaggressive, non-fasting dietary approach may be warranted. Somesymptoms of chronic fatigue syndrome, for example, may beimmediately relieved through a liver detoxification program featuringa more aggressive elimination diet for a shorter term.
Hormone Imbalances & Cyclerelated Symptoms
In both men and women, unhealthy diets are one of the manyfactors that influence the bodys ability to balance hormones.Additionally, foods and beverages can include exogenous sourcesof hormones that overload the bodys natural ability to detoxify andexcrete them.
Estrogen imbalance in women, for example, may manifest aspremenstrual syndrome, irregular menstrual cycles, fibrocysticbreast disease, endometriosis, or dysmenorrhea, as well as fostersymptoms that impact daily livinghot flashes, night sweats, anxietyattacks, and mood fluctuations.
Targeted dietary changessuch as the inclusion of cruciferousvegetables and adaptogenic phytoestrogens like soycan supportthe bodys production, use, and excretion of various hormones,particularly estrogen. These dietary changes can positively affectthe detoxification of circulating estrogens, thereby creating a positiveestrogenic influence on activities at the cellular level.
50-55
-
7/25/2019 Nutrigenomics White Paper
10/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page10
Phase 1BChanging Primary Dietary Signals with
Medical FoodsFood plans and other lifestyle changes may only provide part of therecommendations for changing dietary signals for optimal healthsupport. Medical foods, ever increasing in use, provide an idealcomplement to dietary changes to help modify kinase signaling forpatients presenting with a variety of conditions, such as those related todysglycemia and inflammation. Medical foods contain therapeutic levelsof nutrients that would be difficult, if not impossible, to achieve throughtraditional dietary means to support specific conditions.
For almost two decades, Metagenics has been one of the fewcompanies to develop and manufacture medical foods. The genesis ofthese medical foods was based on burgeoning research now known as
nutrigenomics. These medical foods are backed by numerous clinicalstudies and extensive peer-reviewed scientific support.
For added assurance and developmental research purposes, thesemedical foods undergo continual testing in a clinical setting at theFunctional Medicine Research CenterSM(FMRC), the clinical researcharm of Metagenics.
The SKRM Effect: Creating the Next Generation of Medical Foods
Medical Foods with the inclusion of SKRMs offer a multi-mechanisticapproach to offer even more opportunities for patient success. Theyrepresent the latest in medical food development, incorporating
nutrigenomic research and technology for a new degree of healthsupport. (For more information on SKRM research, please see Phase2Modulating Kinase Signaling with SKRMs on page 18.)
The following medical foods are intended to complement dietaryrecommendations to offer nutritional support for the management of
specific conditions. Healthcare practitioners, however, are best qualifiedto decide on a case-by-case basis when other patients may alsobenefit from the nutrients provided by formulas designed to address:
Metabolic syndrome
Cardiovascular disease
Inflammatory bowel disease (autoimmune support)
Type 2 diabetes Chronic fatigue syndrome (liver detoxification support)
Premenstrual syndrome (hormone balance)
Leaky gut syndrome
Medical foods provide
powerful signaling nutrients
not found in typical diets.
Medical foods containing
SKRMs offer a multi-
dimensional approach to
wellness.
-
7/25/2019 Nutrigenomics White Paper
11/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page11
Metabolic Syndrome & Cardiovascular Disease
UltraMeal
PLUS 360 Medical Foodis formulated with the additionof SKRMsin the form of reduced iso-alpha acids (RIAA, fromhops) and acacia extractto complement the formulas nutritionalsupport for the management of conditions associated withcardiovascular disease and metabolic syndrome. This advancedformula:
o Provides a proprietary soy protein and plant sterol blend thatcontains 2 grams of plant sterols (including beta-sitosterol) and15 grams of soy protein per serving. Foods containing at least0.65 g per serving of plant sterol esters, eaten twice a day withmeals for a daily total intake of at least 1.3 g as part of a dietlow in saturated fat and cholesterol, may reduce the risk of heartdisease.
o Provides 5-methyl-tetrahydrofolate (5-MTHF)a body-ready,nature-identical folateto promote healthy homocysteine levelsfor cardiovascular health.
o Offers a low-glycemic-index meal option to encourage healthyinsulin and blood sugar levels.
o Supplies high quality foundation nutrition for patients with CVD.
In individuals with metabolic syndrome and high cholesterol, thisadvanced medical food formula and accompanying program hasbeen clinically shown to improve the following importantcardiovascular risk factors:
56
o Lower the apolipoprotein Bto-apolipoprotein A1 (apoB/ApoA1)ratio
o Reduce total cholesterol, LDL cholesterol, and triglyceride levelso Increase HDL (good) cholesterol levelso Lower homocysteine levels
(See Table 1 on the following page for clinical results.)
Also available without SKRMs as UltraMealand UltraMeal
PLUS.
-
7/25/2019 Nutrigenomics White Paper
12/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page12
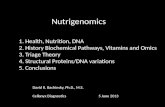
* These results are statistically significant.
Table 1.The summary of lab value changes from a 12-week, 2-arm study aboveillustrates the additive affect of a medical food and SKRMs on markers ofcardiovascular health. Metabolic outcomes were improved more significantly with amedical food and SKRMs than with a low-GL diet and exercise alone.
56
Medical Food with SKRMs Shows Greater Resultsvs. Dietary Signal Modification & Exercise Alone
Measurement Arm 1: UltraMeal PLUS360 with Low-GL Diet
Plan & Exercise
Arm 2: Low-GL DietPlan & Exercise Only
Total Cholesterol -36.74* -16.33*
Triglycerides -89.39* -30.89
HDL-C 2.65* 1.06
LDL-C -28.38* -15.06*
TChol/HDL-C -1.35* -.61*
TG/HDL -3.01* -1.01
ApoA1 -4.00 -8.44
ApoB -25.70* -15.06*
ApoB/ApoA1 -.12* -.05*
Greater Improvement in CV Health Markers
-
7/25/2019 Nutrigenomics White Paper
13/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page13
Inflammatory Bowel Disease (Autoimmune Support)
UltraInflamX
PLUS 360Medical Food is formulated with SKRMsin the form of reduced iso-alpha acids (RIAA, from hops)tocomplement the formulas nutritional support for the management ofinflammatory bowel disease (IBD), such as Crohns disease orulcerative colitis. This unique medical food:
Provides a low-allergenic-potential protein base in the form ofrice protein concentrate.
Supplies L-glutamine, a valuable energy source for intestinalmucosal cells.
Provides ginger and rosemary, which may help support healthyeicosanoid and cytokine metabolism.
Supplies generous levels of turmeric extract, which has beenshown to inhibit the activity of a wide variety of enzymes,cytokines, eicosanoids, and reactive species implicated in pain
and inflammation. Offers an excellent source of antioxidants with a very high
oxygen radical absorbance capacity (ORAC) value.
Advantages of the addition of SKRMs include:
Shown to beneficially influence the function of kinases involvedin inflammatory processes.
Suggested by research to positively influence inflammation-
signaling molecules such as NF-B, COX-2, and PGE2.
Also available without SKRMs as UltraInflamXMedical Food.
-
7/25/2019 Nutrigenomics White Paper
14/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page14
Type 2 Diabetes
UltraGlycemXMedical Foodis formulated to meet the specialized
nutritional needs of patients with type 2 diabetes, insulin resistance,and hypoglycemia by providing a low-glycemic-index blend thatincludes high amylose starch (a resistant starch), targeted plantnutrients from green coffee beans and cinnamon, and heart-healthysoy protein and barley ingredients. UltraGlycemX:
o Supports healthy heart function by providing 15 grams of soyprotein per serving. Diets low in saturated fat and cholesterolthat include 25 grams of soy protein a day may reduce the riskof heart disease.
o Provides 11 grams of specialized dietary fibers per serving tohelp maintain healthy blood glucose levels in type 2 diabetics.
o Includes green coffee bean extract (containing chlorogenic acid)and barley beta-glucans for support of healthy glucose, lipid,and insulin metabolism.
o Offers a low-glycemic-index meal option to encourage healthyinsulin and blood sugar levels.
o Supplies resistant starch that resists digestion and ismetabolized much like dietary fiber, with positive implications forglucose and insulin metabolism.
o Provides beneficial levels of cinnamon, chromium, biotin, andmagnesium to promote healthy glucose uptake and insulinfunction.
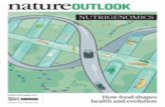
Figure 2.A preliminary, randomized, 2-arm clinical study of 37 insulin-resistantpatients showed a greater average decrease when supplementing with an
UltraGlycemX formula.57
111
71.5
0
50
100
150
Before Program After 8 Weeks on
UltraGlycemX
Program
Insulin(IU/mL)
36% Average Decrease in 2-hr Postprandial Insulin
-
7/25/2019 Nutrigenomics White Paper
15/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page15
Chronic Fatigue Syndrome (Liver Detoxification Support)
UltraClearMedical Foodis formulated to provide readily
assimilable macronutrients (protein, carbohydrates, and fats) to helpaddress altered energetic function in patients with chronic fatiguesyndrome.
o Designed for those patients who may benefit from specificnutritional support for hepatic detoxification function.
o Provides nutrients and antioxidants that support hepaticdetoxification processes.
o Provides low-allergenic-potential protein in the form of riceprotein concentrate, which may be beneficial during times ofincreased hepatic detoxification burden.
o The rice protein concentrate has been prepared via a uniqueprocess that reduces its already low allergenic potential.
UltraClear PLUSMedical Food
o Provides the same low-allergenic-potential rice protein base andmacronutrients, but designed for those patients who may benefitfrom specific nutritional support for Phase II hepaticdetoxification function with the addition of:
Glycine to support Phase II glycine conjugation Magnesium sulfate and L-cysteine to support Phase II
sulfationo Also provides green tea catechins and mixed carotenoids to
protect against reactive species generated during hepaticdetoxification.
UltraClearPlus pHMedical Food
o Provides the same low-allergenic-potential rice protein base andmacronutrients, but designed for those patients who may benefitfrom specific nutritional support to promote alkalinization ofurine and Phase II hepatic detoxification function with theaddition of:
Potassium citrate to promote alkalinization of urine Sesame (a source of sesamin) to help support Phase II
hepatic metabolism of lipids (including cholesterol) andother substances
Glycine and taurine to support Phase II amino acidconjugation
Magnesium sulfate to support Phase II sulfation
Further personalize an
approach by identifying those
patients with needs for
additional detoxification
support.
-
7/25/2019 Nutrigenomics White Paper
16/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page16
Premenstrual Syndrome (PMS)
EstriumMedical Foodis formulated to provide specialized
nutritional support for premenstrual syndrome by supplying flaxseed,isoflavones, and targeted nutrients. This targeted formula:
o Supports healthy estrogen metabolism and balance withflaxseed and non-soy isoflavones (from kudzu).
o Supplies generous levels of vitamin E, vitamin B6, calcium,magnesium, and chromium to address particular concernsassociated with PMS.
o Offers a low-glycemic-index meal option to help support healthyenergy and insulin metabolism.
o Provides turmeric extract, which has been shown in research toinhibit the activities of a wide variety of enzymes, cytokines,eicosanoids, and reactive species implicated in pain andinflammation.
Figure 3. In a clinical study of 40 PMS patients following the Estrium program for twomenstrual cycles there was a significant improvement in symptoms as measured bythe Shortened Premenstrual Assessment Form (scores from 10 to 30 indicatesymptomatology in the last half of the cycle).
58
0
20
40
60
Before Program After Estrium
Program
SPAFTotalScore
59% Reduction in PMS Symptoms
-
7/25/2019 Nutrigenomics White Paper
17/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page17
Leaky Gut Syndrome
UltraClear SUSTAINMedical Foodis formulated to provide
specialized nutritional support, including L-glutamine and readilyassimilable, low-allergenic-potential macronutrients for patients withleaky gut syndrome.
o Provides L-glutamine, a valuable energy source for intestinalmucosal cells.
o Addresses dysbiosis associated with leaky gut syndrome byproviding inulin and fructooligosaccharides (FOS) to promotethe growth of healthy intestinal bacteria.
o Provides prebiotic factors, which encourage the production ofshort-chain fatty acids (SCFAs) that promote intestinal mucosalhealth and a healthy intestinal environment.
o The rice protein concentrate has been prepared via a uniqueprocess that reduces its already low allergenic potential.
Medical Food Nutritional Profiles & Research
Nutritional information for the medical foods mentioned in this documentis available at www.metagenics.com. In addition to extensivedevelopmental research and clinical studies, these medical foodsundergo continual testing in a clinical setting at the Functional MedicineResearch Center.
Individual case management studies with medical foods are available forviewing at www.metagenics.com in the resources section:www.metagenics.com/science/case_studies.asp?sect=2
-
7/25/2019 Nutrigenomics White Paper
18/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page18
Phase 2Modulating Kinase Signaling with SKRMs
Nutrigenomic research, such as that conducted by the MetaProteomicsNutrigenomics Research Center, attempts to discover highly activesubstances from food and other natural sources that can serve as potentdietary signaling molecules to positively affect genetic expression.Optimally, this yields the development of unique food ingredient extractsfrom which individual bioactive molecules can be isolated and tested fortheir ability to modify cellular function related to various diseaseprocesses.
Many prevalent health issues have been found to have specificunderlying kinase signaling components. This is due to the ability ofkinases to translate dietary signals in a positive or negative manner toinfluence health. For example, research has shown that impaired kinase
signaling can lead to impaired insulin response and hyperlipidemiaassociated with type 2 diabetes.59
Kinases are enzymes that chemically modify other proteins and regulatethe majority of cellular pathwaysparticularly those involved in thetransmission of intracellular signals. These enzymes also help regulateeicosanoids, cytokines, reactive oxygen species, and other mediatorsthat may negatively impact the body both locally and systemically.
Figure 4. SKRMs positively affect kinase signaling for optimal genetic and phenotypicexpression for wellness. SKRMs are an ideal complement to positive dietary changesfor restoration of healthy kinase activities.
Diet, Exercise& Lifestyle
Nutrients &Xenobiotics
Metabolism
Gene Expression
Cell Phenotype
Signal Transduction
Direct Indirect SKRMs
SKRMs provide another
nutritional modality to
modulate cellular signals.
Modifying Genetic Expression with SKRMS
-
7/25/2019 Nutrigenomics White Paper
19/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page19
As mentioned previously, SKRMs are nutritional substances that canwork to modulate kinase signaling back into balance. This balance helpsrestore healthy signaling to genes for positive genetic expression andreversal of illness.
Proprietary research has yielded the discovery of food-derived SKRMsthat specifically inhibit kinase-mediated processes associated withinsulin resistance and inflammation. SKRMs may offer therapeuticadvantages over dietary modifications alone.
Insulin SKRMs
Groundbreaking preliminary research suggests the identification ofSKRMs that have the ability to improve insulin sensitivity by modulatingspecific kinase enzymes that serve as hubs for insulin-signalingprocesses.
More than 200 natural substances and extracts were tested for theirinfluence on insulin responses and adipocyte (fat-storing) cells at theMetaProteomics Nutrigenomics Research Center. A combination ofreduced iso-alpha acids (RIAA) derived from hops (Humulus lupulus)and acacia extract (Acacia nilotica) was shown via in vitrotesting toinhibit inflammatory markers that influence insulin function.
60
Research has implicated dysregulated inflammatory processes in thedevelopment of insulin resistance, and several inflammation-inducedcytokines have been shown to be expressed during insulin resistanceand metabolic syndrome.61-63Cytokinessuch as interleukin-1 beta (IL-
1), tumor necrosis factor alpha (TNF-), and interferon gamma (IFN-
)have been shown to play a role in cytokine-induced -celldysfunction in diabetes.64,65
In human clinical testing at the Functional Medicine Research Center,supplementation of metabolic syndrome subjects with a combination ofRIAA and acacia led to greater reduction of 2 h pp insulin levels, ascompared to placebo. Furthermore, greater decreases of fasting insulin,fasting and 2 h pp glucose, fasting triglyceride, and HOMA scores wereobserved in subjects taking RIAA/acacia supplement versus subjectstaking placebo. These collective results indicate RIAA/acaciasupplementation might be useful in maintaining insulin homeostasis insubjects with metabolic syndrome.
60
-
7/25/2019 Nutrigenomics White Paper
20/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page20
Insulin SKRM Research
Figure 5. The Homeostasis Model Assessment (HOMA) estimates steady state betacell function and insulin sensitivity, and is a published measure of insulin resistance. Asignificant decrease was observed for the RIAA/acacia group as compared to the
placebo group in an 8-week clinical trial.60
Figure 6. In the same blinded, placebo-controlled study of 91 patients, theRIAA/acacia blend showed a greater improvement in triglyceride levels than
placebo.60
-1.48
-48.97-55
-45
-35
-25
-15
-5
Placebo RIAA/Acacia Blend
Triglycerides
0.16
0.78
0
0.2
0.4
0.6
0.8
1
Placebo RIAA/Acacia Blend
HOMA
Increased Insulin Sensitivity with SKRMs
Improvement in Triglycerides with SKRMs
-
7/25/2019 Nutrigenomics White Paper
21/36
-
7/25/2019 Nutrigenomics White Paper
22/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page22
Inflammation & Autoimmune SKRM Research
PGE2
(pg/ml)
Concentration (g/ml)
0
500
1000
1500
2000
2500
2.5 5.0
Control
THIAA
RIAA
PGE2
(pg/ml)
Concentration (g/ml)
0
500
1000
1500
2000
2500
2.5 5.0
Control
THIAA
RIAA
Figure 7. Cells were pre-incubated with THIAA or RIAA, followed by lipopoly-saccharide (LPS)-induced stimulation of PGE2production. The data show thatcompared to the control and RIAA, THIAA inhibits PGE2expression more effectively.
Figure 8. Cells were pre-incubated with THIAA and then stimulated with LPS to induceTNF-production. Results show that THIAA can lead to greater inhibition of TNF-expression in a dose-dependent manner.
0
500
1000
1500
2000
2500
10.0 20.0
TNF-(pg/ml)
Concentration (g/ml)
Control
THIAA
PGE2 Inhibition with SKRMs
TNF-Inhibition with SKRMs
-
7/25/2019 Nutrigenomics White Paper
23/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page23
Future SKRMs
Nutrigenomic research continues to focus on naturally derived
substances that act as SKRMs to beneficially influence health in otherareas, such as liver detoxification, bone resorption, and hormonebalance.
For more information on nutrigenomic research and the development ofinnovative nutritional protocols, please visit:www.metaproteomicslabs.com
-
7/25/2019 Nutrigenomics White Paper
24/36
-
7/25/2019 Nutrigenomics White Paper
25/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page25
Blood Sugar Metabolism Support
Ever-growing research continues to show the newly discovered benefitsof green tea and cinnamon in complementing dietary approaches toblood sugar management. Insulin resistance conditions can also induceoxidative stress that can lead to vascular complications, such asneuropathy.
CinnamonCinnamon has been shown to display insulin-enhancingactivity in vitro and shown in human clinical trials to positivelyinfluence glucose levels.
106-108Extracts of cinnamon have also been
shown to activate insulin receptor kinase and inhibitdephosphorylation of the insulin receptorleading to increasedinsulin sensitivity.
Green Tea (EGCG)Green tea contains epigallocatechin gallate(EGCG), a bioflavonoid shown to protect pancreatic islet cells and
enhance insulin sensitivity.
109
Catechins from green tea also providestrong antioxidant protection.110
Liver Detoxification Support
There are two primary phases in the detoxification process. In Phase I,fat-soluble toxins are transformed into intermediate compounds that aremore reactive, but will bind more easily to non-toxic, water-solublemolecules in Phase II. In Phase II, formation between the reactiveintermediates and water-soluble molecules make the entire compoundready for excretion out of the body. Targeted nutrients can influencedetoxification activities in either phaseor sometimes both.
SilymarinThis active constituent of milk thistle (Silybum marianum)is well-recognized for its beneficial effects on protecting the liverfrom toxins and stimulating liver regeneration, as well as itsantioxidant properties. Preliminary research also indicates that itmay influence Phase I and Phase II enzymes, and therefore may becalled a bifunctional modulator.
111,112
CatechinsThese strong antioxidants have the capacity toscavenge most oxygen free radicals.
110Also derived from green tea
(Camilla sinensis, see above), catechins enhance the induction ofPhase II enzymesglutathione S-transferase and quininereductaseand inhibit the overinduction of specific cytochromeP450 Phase I biotransformation enzymes.
113,114
WatercressGlucosinolates found in watercress (Nasturtiumofficinale) are precursors of phenythyl isothicynate (PEITC), whicheffectively inhibits the overinduction of specific sytochrome P450
-
7/25/2019 Nutrigenomics White Paper
26/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page26
enzymes and enhances Phase II glutathione S-transferase andquinine reductase.115-117
Ellagic AcidNaturally found in pomegranate fruit (Punicagranatum), ellagic acid beneficially modulates Phase Ibiotransformation and enhances Phase II glutathione S-transferaseand quinine reductase enzyme induction.
118-120Also scavenges
superoxide radicals and hydroxyl radicals, reducing hepaticoxidative stress.
120,121
Note: Catechins, watercress, and ellagic acid also influence geneticexpression of enzymes that control Phase II conjugationreactions.113-120
Artichoke LeafExtracts from artichoke (Cynara scolymus) have along history of traditional use in promoting liver function. Researchsuggests that several constituents of artichoke, including
chlorogenic acid and cynarin, have marked antioxidant andhepatoprotective properties.122-124
Intestinal Support
Probiotic strains have specific characteristics that determine whetherthey have the ability to benefit the intestinal environment. But not allgenera, species, and strains are suitable for all purposes. Following arebeneficial bacteria shown to adhere to the intestinal lining and support ahealthy balance of microflora.
125-130
Lactobacillus acidophilus NCFMThis strain of human origin has
been proven safe and effective by more than 60 scientific studies
and almost 30 years of commercial use. It produces lactic acid,hydrogen peroxide, and other natural substances while modulating
the activity of enzymessuch as -glucuronidase, nitroreductase,and azoreductaseto positively influence the balance of intestinalbacteria and support intestinal tissue health.
125Its also one of a
limited number of Lactobacillus species shown to adhere in theintestines.
131
BifidobacteriumThis major group of carbohydrate-metabolizingbacteria in the intestines (including B. lactis) is 1000 times moreabundant than lactobacilli in healthy adults (and some researchersbelieve more important as well).
132 Bifidobacteria have proven
effectiveness as immunosupportive agents that enhance hostresistance, as well as produce strong acids (e.g., acetic, lactic) that
positively affect intestinal pH; thereby, playing a critical role inmodulating ammonia, phenol, steroidal, and other toxin levels tomaintain health and support intestinal microbial balance.
125-127
-
7/25/2019 Nutrigenomics White Paper
27/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page27
Note: Scientific identification of strains is not only an indicator ofpredicted safety, but assures the means for providing optimal healthbenefits.
Joint Inflammation Support
Many inflammatory and autoimmune conditions are characterized bypain and motility concerns related to the joints. Glucosamine andchondroitin sulfates, as well as MSM, offer widely accepted approachesfor maintaining healthy connective tissue and relieving pain associatedwith concerns that affect a growing number of patients.
Glucosamine & ChondroitinThese nutrients are naturally found inhealthy tissue and work together in forming healthy joint matrixcartilage and enhancing joint lubrication.133,134They may alsopromote the incorporation of sulfur into cartilage. Sulfur is necessaryfor the synthesis of collagen and improves the moisture content ofcartilage, supporting its shock-absorbing ability.135Supplementationwith glucosamine and chondroitin can help restore normal jointmotility and relieve pain.
133,135-138Continued use is required to
maintain benefits.
Methyl-Sulfonyl-Methane (MSM)This natural compoundcomplements glucosamine and chondroitin sulfates, and alsoprovides a highly biologically valuable source of sulfur. MSM hasbeen widely used to support joint health and relieve pain as aneffective natural analgesic and anti-inflammatory agent.
139A
randomized, placebo-controlled trial showed that MSM improvedsymptoms of pain and physical function in patients withosteoarthritis.140Another randomized, double-blind, parallel,
placebo-controlled trial also showed that MSM significantly improvedthe signs and symptoms of osteoarthritis. Furthermore, thecombination of glucosamine and MSM showed better efficacy inreducing pain and swelling and in improving the functional ability ofjoints than the individual agents.139
Hormone Balance Support
Phytoestrogens are plant compounds that have structural and functionalsimilarities to estrogen.
55,141Selective estrogen receptor modulators
(SERMsnot to be confused with SKRMs) are non-steroidalcompounds capable of binding to the estrogen receptors and influencingtheir activities. Specifically, SERMs are noted as being both agonists (in
cases of low estrogen levels, such as with menopause) and antagonists(in cases of high estrogen). Because they support a moderate level ofestrogen activity, upon binding to the estrogen receptors they inhibitendogenous estrogen when too much is present, but can still supportestrogens important functions.142-144
-
7/25/2019 Nutrigenomics White Paper
28/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page28
Kudzu & Red CloverProvide a varied profile of non-soyisoflavones and isoflavone glycosidesincluding daidzein,genistein, puerarin, and fromononetinthat bind to the estrogenreceptor and may act as weaker estrogens, resulting in an inhibitionof the estrogenic effect.50,144-146
TurmericCurcuminoids, the active component in turmeric(Curcuma longa), induce glutathione production and glutathione-Stransferase activityhelping to protect tissues from reactiveestrogen metabolites.
147In combination with isoflavones, curcumin
shows in vitro evidence of reducing xenoestrogens-induced growthin estrogen receptor-positive and negative cancer cells, therebypromoting breast health.55,148
Resveratrol (from Polygonum cuspidatum)Classified as a SERMbased on its ability to bond to estrogen receptors and act as both anestrogen agonist and antagonist. Resveratrol provides many other
benefits, including cardioprotective properties.
149
Resveratrol hasbeen shown to promote healthy cytokine production by influencingthe cyclooxygenase and 5-lipoxygenase pathways. It is alsoassociated with reduced activity of nuclear factor kappaB (NF-B)a transcription factor that may promote the expression ofundesirable genes. Resveratrol has potent antioxidant activity(especially in lipids that are highly concentrated in brain tissue),promotes healthy blood flow, and induces hepatic phase IIdetoxification activity.
Stabilized Indole-3-Carbinole (I3C)This naturally occurringcompound found in cruciferous vegetables protects estrogen-sensitive tissues by promoting the formation of 2-hydroxyestrone,diindolymethane (DIM), and other beneficial estrogen metabolites. It
supports the detoxification of estrogens, other steroid hormones,and xenoestrogens by enhancing the activity of enzymes involved intheir metabolism and excretion. Research indicates great promiseas a natural hormone-balancing agent.
150-157
Note: Natural-source I3C may be an important consideration whenrecommending supplementation to patients.
-
7/25/2019 Nutrigenomics White Paper
29/36
-
7/25/2019 Nutrigenomics White Paper
30/36
-
7/25/2019 Nutrigenomics White Paper
31/36
-
7/25/2019 Nutrigenomics White Paper
32/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page32
References
1. Alffman L, Muller M. Nutrigenomics: from molecular nutrition to prevention of disease. J M Diet Assoc.2006;106(4):569-576.
2. Subbiah MT. Nutrigenetics and nutraceuticals: the next wave riding on personalized medicine. Transl Res.2007;149(2):55-61.
3. Mariman EC. Nutrigenomics and nutrigenetics: the omics revolution in nutritional science. Biotechnol ApplBiochem. 2006;44(Pt 3):119-128.
4. Kaput J. Nutrigenomics2006 update. Clin Chem Lab Med.2007;45(3):279-287.5. Ferguson LR. Nutrigenomics: integrating genomic approaches into nutrition research, Mol Diag Ther.
2006;10(2):101-108.6. Bland JS. What role has nutrition been playing in our health? The xenohormesis connection. 2007 [In press.]7. Roberts CK, Barnard RJ. Effects of exercise and diet on chronic disease. J Appl Physiol.2005;98:3-30.8. Aldan SG, Greenlaw RL, Diehl HA, et al. The behavioral and clinical effects of therapeutic lifestyle changes
on middle-aged adults. Preventing Chronic Disease.2006;3(1):1-16.9. Ashley JM, St. Jeor ST, Schrage JP, et al. Weight control in the physicians office.Arch Intern Med
2001;161:1599-1604.10. Woollard J, Burke V, Beilin LJ, et al. Effects of a general practice-based intervention on diet, body mass
index and blood lipids in patients at cardiovascular risk. J Cardiovasc Risk2003;10(1):31-40.11. Mattila R, Malmivaara A, Kastarinen M, et al. Effectiveness of multidisciplinary lifestyle intervention for
hypertension: a randomized controlled trial. J Hum Hypertens2003;17(3):199-205.12. Hu FB, Manson JE, Stampfer MJ, et al. Diet, lifestyle, and the risk of type 2 diabetes mellitus in women. N
Engl J Med2001;345(11):790-97.13. Case CC, Jones PH, Nelson K, et al. Impact of weight loss on the metabolic syndrome. Diabetes Obes
Metab2002;4(6):407-14.14. OReilly S, Doherty M. Lifestyle changes in the management of osteoarthritis. Best Pract Res Clin
Rheumatol2001;15(4):559-68.15. The North American Menopause Society. Management of osteoporosis in postmenopausal women: 2006
position statement of The North American Menopause Society. Menopause2006;13(3):340-67.16. Preuss HG, Bagchi D, Bagchi M. Protective effects of a novel niacin-bound chromium complex and a grape
seed proanthocyanidin extract on advancing age and various aspects of syndrome X.Ann N Y Acad Sci2002;957:250-59.
17. Gordon NF, Salmon RD, Franklin BA, et al. Effectiveness of therapeutic lifestyle changes in patients withhypertension, hyperlipidemia, and/or hyperglycemia. Am J Cardiol.2004;94:1558-1561.
18. Aldana SG, Greenlaw RL, Diehl HA, et al. Effects of an intensive diet and physical activity modificationprogram on the health risks of adults. J Am Diet Assoc.2005;105:371-381.
19. Wannamethee SG, Sharper AG, Whincup PH. Modifiable lifestyle factors and the metabolic syndrome inolder men: effects of lifestyle changes. J Am Geriatr Soc. 2006;54:1909-1914.
20. Tuomilehto J, Lindstrom J, Eriksson JG, et al. Prevention of type 2 diabetes mellitus by changes in lifestyleamong subjects with impaired glucose tolerance. N Engl J Med.2201;344:1343-1350.
21. Esposito K, Marfella R, Ciotola M, et al. Effects of a Mediterranean-style diet on endothelial dysfunction andmarkers of vascular inflammation in the metabolic syndrome: a randomized trial. JAMA. 2004;292(12):1440-1446.
22. Holman H. Chronic diseasethe need for a new clinical education. JAMA.2004;292(9):1057-1059.23. Casalino LP. Disease management and the organization of physician practice. JAMA. 2005; 293(4):485-
488.24. Roche HM, Phillips C, Gibney MJ. The metabolic syndrome: the crossroads of diet and genetics. Proc Nutr
Soc.2005;64:371-377.25. Kendal CW, Augustin LS, Emam A, Josse AR, Saxena N, Jenkins DJ. The glycemic index: methodology and
use. Nestle Nutr Workshop Ser Clin Perform Programme.2006;11:43-56.
26. Hyman, Mark. UltraMetabolism: The Simple Plan for Automatic Weight Loss. New York: Scribner, 2006.27. Prada PO. Gottardello, Zecchin H, Lia Gaspaparetti A, et al. Western diet modulates insulin signaling, c-Jun
N-terminal kinase activity, and insulin receptor substrate-1 [ser307] phosphorylation in a tissue-specificfashion. Endocrinology.2005;146(3):1576-1587.
28. Pins JJ, Keenan JM. Dietary and nutraceutical options for managing the hypertriglyceridemic patient. ProgCardiovasc Nurs. 2006;21(2):89-93.
29. Deen D. Metabolic syndrome: time for action.Am Fam Physician.2004;69(12):2875-882.30. Deedwania PC, Volkova N. Current treatment options for the metabolic syndrome. Curr Treat Options
CardiovascMed.2005;7(1):61-74.31. Hu Y, Block G, Norkus EP, Morrow JD, Dietrich M, Hudes M. Relations of glycemic index and glycemic load
with plasma oxidative stress markers.Am J Clin Nutr.2006;84(1):70-76.32. Stamp LK, James MJ, Cleland LG. Diet and rheumatoid arthritis: a review of the literature. Semin Arthritis
Rheum2005;35(2):77-94.33. van de Laar, MA, van der Korst JK. Food intolerance in rheumatoid arthritis. I. A double blind, controlled trial
of the clinical effects of elimination of milk allergens and azo dyes.Ann Rheum Dis1992;51(3):298-302.34. Pena AS, Crusius JB. Food allergy, coeliac disease and chronic inflammatory bowel disease in man. Vet Q
1998;20 Suppl 3:S49-52.35. Stark ME, Tremaine WJ. Maintenance of symptomatic remission in patients with Crohns disease. Mayo Clin
Proc1993;68(12):1183-90.36. Khan S, Orenstein SR. Eosinophilic gastroenteritis: epidemiology, diagnosis and management. Paediatr
Drugs2002;4(9):563-70.37. Ebo DG, Stevens WJ. IgE-mediated food allergyextensive review of the literature.Acta Clin Belg
2001;56(4):234-47.38. Sullivan PB. Food allergy and food intolerance in childhood. Indian J Pediatr 199;66(1 Suppl):S37-45.39. Caffarelli C, Cavagni G, Menzies IS, Bertolini P, Atherton DJ. Elimination diet and intestinal permeability in
atopic eczema: a preliminary study. Clin Exp Allergy1993;23(1):28-31.40. Atherton DJ. Role of diet in treating atopic eczema: elimination diets can be beneficial. BMJ
1988;277(6661):1458,1460.41. Veien NK, Hattel T, Justesen O, Norholm A. Dietary restrictions in the treatment of adult patients with
eczema. Contact Dermatitis1987;17(4):223-28.
-
7/25/2019 Nutrigenomics White Paper
33/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page33
42. Fogg MI, Spegel JM. Management of food allergies. Expert Opin Pharmacother 2003;4(7):1025-1037.43. Garcia-Careaga M Jr, Kerner JA Jr. Gastrointestinal manifestations of food allergies in pediatric patients.
Nutr Clin Pract2005;20(5):526-35.44. Veien NK, Hattel T, Justesen O, Norholm A. Oral challenge with food additives. Contact Dermatitis
1987;17(2)100-103.45. Burr ML, Fehily AM, Stott NC, Merrett TG. Food-allergic asthma in general practice. Hum Nutr Appl Nutr
1985;39(5)349-355.46. Atkinson W, Sheldon Tam Shaath N, Whorwell PJ. Food elimination based on IgG antibodies in irritable
bowel syndrome: a randomised controlled trial. Gut2004;53(10):1459-1464.47. Hafstrom I, Ringertz B, Spanberg A, et al. A vegan diet free of gluten improves the signs and symptoms of
rheumatoid arthritis: the effects on arthritis correlate with a reduction in antibodies to food allergens.Rheumatology (Oxford) 2001;40(10):1175-1179.
48. Galli E, Cicconi R, Rossi P, Casati A, Brunetti E, Mancino G. Atopic dermatitis: molecular mechanisms,clinical aspects and new therapeutic approaches. Curr Mol Med2003;3(2):127-138.
49. Darlington LG, Ramsey NW. Review of dietary therapy for rheumatoid arthritis. Br J Rheumatol1993;32(6):507-14.
50. Cassidy A. Potential tissue selectivity of dietary phytoestrogens and estrogens. Curr Opin Lipid.1999:10:47-52.
51. Keck AS, Finley JW. Cruciferous vegetables: cancer protective mechanisms of glucosinolate hydrolysisproducts and selenium. Integr Cancer Ther.2004;3(1):5-12.
52. Setchell KD. Soy isoflavonesbenefits and risks from natures selective estrogen receptor modulators(SERMs). J Am Coll Nutr. 2001;20(5 Suppl):354S-362S.
53. Ganry O. Phytoestrogen and breast cancer prevention. Eur J Cancer Prev. 2002;11(6):519-522.54. Xu X, Duncan AM, Wangen KE, Kurzer MS. Soy consumption alters endogenous estrogen metabolism in
premenopausal women. Cancer Epidemiol Biomarkers Prev.200;9(8):781-786.55. Cos P, DeBruyne T, Apers S, Vanden Burrghe D, Pieters L, Vlietinck AJ. Phytoestrogens: recent
developments. Planta Med.2003;69:589-599.56. Lerman RH, Bland JS, Darland G, Lamb JJ, Minich DM, Schiltz B, Trip ML. Supplementation with a novel
selective kinase response modulator (SKRM) nutraceutical and medical food significantly enhances thebenefits of a diet and exercise program in subjects with metabolic syndrome. Functional Medicine ResearchCenter, Gig Harbor, WA. [In preparation.]
57. Lukaczer D, Lerman R, Schiltz B, et al. A pilot trial comparing the effects of identical weight loss dietprograms with or without additional nutrient supplementation in subjects with insulin resistance andhyperinsulinemia. Gig Harbor, WA: Functional Medicine Research Center; Research Report No. 105, 2000.
58. Lukaczer D, Liska DJ, Darland G, et al. Improvement in symptoms and estrogen metabolism in women withpremenstrual syndrome using a newly formulated medical food. Gig Harbor, WA: Functional MedicineResearch Center; Research Report No. 110, 2001.
59. Luo J, Sobkiw CL. Hirshman MF, Logsdon MN, et al. Loss of class IA PI3K signaling in muscle leads toimpaired muscle growth, insulin response, and hyperlipidemia. Cell Metab.2006;3(5):355-366.
60. Lerman RH, Tripp ML, Bland JS. Double-blind, placebo-controlled trial examining the effects of RIAA/acaciasupplementation on insulin homeostasis. Functional Medicine Research Center, Gig Harbor, WA.
61. Yudkin JS, Stehouwer CD, Emeis JJ, Coppack SW. C-reactive protein in healthy subjects: associations withobesity, insulin resistance, and endothelial dysfunction: a potential role for cytokines originating fromadipose tissue?Arterioscle Thromb Vasc Biol.1999;19:972-978.
62. Mohamed-Ali V, Goodrick S, Rawesh A, et al. Subcutaneous adipose tissue releases interleukin-6, but nottumor necrosis factor-, in vivo. Endocrinol Metab.1997;82:4196-4200.
63. Lundgren CH, Brown SL, Nordt TK, Sobel BE, Fujii S. Elaboration of type-1 plasminogen activator inhibitorfrom adipocytes. A potential pathogenetic link between obesity and cardiovascular disease. Circulation.1996;93:106-110.
64. Heitmeier MR, Kelly CB, Ensor NJ, et al. Role of cyclooxygenase-2 in cytokine-induced -cell dysfunction
and damage by isolated rat and human islets. J Biol Chem.2004;279:53145-53151.65. McDaniel ML, Kwon G, Hill JR, Marshall CA, Corbett JA.Cytokines and nitric oxide in islet inflammation anddiabetes. Proc Soc Exp Biol Med.1996;211:24-32.
66. Elenkov IJ, Iezzoni DG, Daly A, et al. Cytokine dysregulation, inflammation and well-being.Neuroimmunomodulation. 2005;12(5):255-269.
67. Cook ME. Regulation of eicosanoid pathways: a pathway to health and development. Pakistan J Nut.2002;1(2):103-105.
68. Kidd P. Th1/Th2 balance: the hypothesis, its limitations, and implications for health and disease.Altern MedRev.2003;8(3):223-246.
69. Skapenko A, Leipe J, Lipsky PE, et al. The role of the T cell in autoimmune inflammation.Arthritis Res Ther.2005;7(Suppl 2):S4-S14.
70. Liska D, Garland G,Tripp M. Proprietary Clinical Research Report. Gig Harbor,WA: Functional MedicineResearch Center; 2004.
71. Lukaczer D, Lerman RH, Darland G, et al. Effects of a reduced iso-alpha acids (RIAA), rosemary extract,and oleanolic acid supplement on pain in subjects with osteoarthritis (OA), Proprietary Clinical ResearchReport. Gig Harbor,WA: Functional Medicine Research Center;2004.
72. Tripp M, Darland G, Lerman RH, et al. Development of Meta050, a natural anti-inflammatory targetinginhibition of cyclooxygenase gene induction instead of direct cyclooxygenase enzyme inhibition, resulting inan anti-inflammatory with low-predicted GI toxicity. Presented at: Fed Am Soc Experimental Biol. 2003: April.
73. Lerman RH, Liska D, Tripp M, et al. Summary of effects of a reduced iso-alpha acids (RIAA), rosemaryextract, and oleanolic acid supplement on parameters of cardiovascular health. Proprietary ClinicalResearch Report. Gig Harbor,WA: Functional Medicine Research Center;2004.
74. Lerman RH, Liska D, Tripp M, et al. Clinical trial evaluating the effect of Meta050 on parameters of plateletfunction and blood coagulation. Proprietary Clinical Research Report.Gig Harbor,WA: Functional MedicineResearch Center;2004.
75. Tripp M, Babish J, Darland G, et al. Hop and modified hop extracts have potent in vitro anti-inflammatoryproperties. Published Proceedings from 1st International Symposium on Humulus. Editors K.E. Hummer andJ.A. Henning.Acta Horiculturae. 668, ISHS 2005.
76. Babish JG, Howell T. Proprietary Research Report. San Clemente, CA: MetaProteomics, Inc. 2003.
-
7/25/2019 Nutrigenomics White Paper
34/36
___________________________________________________
Version 1.4 2007 Metagenics, Inc. Page34
77. Lukaczer D, Lerman RH,Tripp M, et al. A randomized cross-over study to assess the effects of a proprietaryreduced iso-alpha acid (RIAA), rosemary extract, and oleanolic acid supplement on gastrointestinal integrityusing the fecal calprotectin assay. ProprietaryClinical Research Report. Gig Harbor, WA: FunctionalMedicine Research Center;2004.
78. Yamamoto K, Wang J, Yamamoto S, et al. Suppression of cyclooxygenase-2 gene transcription by humulonof beer hop extract studied with reference to glucocorticoid. FEBS Lett. 2000;465:103-06.
79. Cantorna MT, Zhu Y, Froicu M, et al. Vitamin D status, 1,25-dihydroxyvitamin D3, and the immune system.Am J Clin Nutr.2004;80(6 Suppl):1717S-1720S.
80. Peterlik M, Cross HS. Vitamin D and calcium deficits predispose for multiple chronic diseases. Eur J ClinInvest.2005;35(5):290-304.
81. Holick MF. The vitamin D epidemic and its health consequences. J Nutr.2005;135(11):2739S-2748S.82. Prabhu KS, Zamamiri-Davis F, Steward JB, et al. Selenium deficiency increases the expression of inducible
nitric oxide synthase in RAW 264.7 macophages: role of nuclear factor-B in up-regulation. Biochem J.2002;366:203-209.
83. Tarp U. Selenium and the selenium-dependent glutathione peroxidase in rheumatoid arthritis. Dan Med Bull.1994;41(3):264-274.
84. Zamamiri-Davis F, Lu Y, Thompson JT, et al. Nuclear factor-kappaB mediates over-expression ofcyclooxygenase-2 during activation of RAW 264.7 macrophages in selenium deficiency. Free Radic BiolMed.2002;32(9):890-897.
85. Rosenstein ED, Caldwell JR. Trace elements in the treatment of rheumatic conditions. Rheum Dis Clin NorthAm.1999;25(4):929-935.
86. Peretz A, Cantinieaux B, Neve J, et al. Effects of zinc supplementation on the phagocytic functions ofpolymorphonuclears in patients with inflammatory rheumatic diseases. J Trace Elem Electrolytes Health Dis.1994;8(3-4):189-194.
87. Bahagavan HN, Chopra RK. CoQ10: absorption, tissue uptake, metabolism and pharmacokinetics. FreeRadic Res.2006;40(5):445-453.
88. Crane FL. Biochemical functions of coenzyme Q10. J Am Coll Nutr.2001;20(6):591-598.89. Wolters N, Hahn A. Plasma ubiquinone status and response to six-month supplementation combined with
multivitamins in healthy elderly womenresults of a randomized, double-blind, placebo-controlled study. IntJ Vitam Nutr Res.2003;73(3):207-214.
90. Lu WL, Zhang Q, Lee SH, et al. Total coenzyme Q10concentrations in Asian men following multiple oral 50-mg doses administered as coenzyme Q10sustained release tablets or regular tablets.Biol Pharm Bull.2003;26(1):52-55.
91. Singh RB, Niaz MA, Rastogi V, Rastogi SS. Coenzyme Q in cardiovascular disease. J Assoc PhysiciansIndia.1998;46(3):299-306.
92. Weant KA, Smith KM. The role of coenzyme Q20 in heart failure.Ann Pharmacother. 2005;39(9):1522-1526.93. Mortensen SA. Perspectives on therapy of cardiovascular disease with coenzyme Q10(ubiquinone). Clin
Investig.1993;71(8 Suppl):S116-S123.94. Folkers K, Langsjoen P, Willis R, Richardson P, Xia LJ, Ye CQ, Tamagawa H. Lovastatin decreases
coenzyme Q levels in humans. Proc Natl Acad Sci USA.1990;87(22):8931-8934.95. Passi S, Stancato A, Aleo E, Dmitrieva A, Littarru GP. Statins lower plasma and lymphocyte
ubiquinol/ubiquinone without affecting other antioxidants and PUFA. Biofactors.2003;18(1-4):113-124.96. Bargossi AM, Battino M, Gaddi A, Fiorella PL, Grossi G, Barozzi G, Di Giulio R, Descovich G, et al.
Exogenous CoQ10preserves plasma ubiquinone levels in patients t reated with 3-hydroxy-3-methylglutarylcoenzyme A reductase inhibitors. Int J Clin Lab Res. 1994;24(3):171-176.
97. Langsjoen PH, Langsjoen AM. The clinical use of statins and the associated depletion of the essential co-factor coenzyme Q10: a review of the pertinent human and animal data. Biofactors. 2003;18(1-4)101-111.
98. Harris WS, Park Y, Isley WL. Cardiovascular disease and long-chain omega-3 fatty acids. Curr Opin Lipidol.2003;14(1):9-14.
99. Carroll DN, Roth MT. Evidence of the cardioprotective effects of omega-3 fatty acids.Ann Pharmacother.
2002;36(12):1950-1956.100. Schrepf, R. Clinical prevention of sudden cardiac death by n-3 polyunsaturated fatty acids and mechanismof prevention of arrhythmias by n-3 fish oils. The Lancet 2004;363:1441-1442.
101. Biscione F, Totteri A, De Vita A, Lo Bianco F, Altamura G. Effect of omega-3 fatty acids on the prevention ofatrial arrhythmias. Ital Heart J Suppl.2005;6(1):53-59.
102. Leaf A, Kang JX, Xiao YF, Billman GE. Clinical prevention of sudden cardiac death by n-3 polyunsaturatedfatty acids and mechanism of prevention of arrhythmias by n-3 fish oils. Circulation.2003;107(21):2646-2652.
103. Mozaffarian D, Psaty BM, Rimm EB, et al. Fish intake and risk of incident atrial fibrillation. Circulation.2004;110(4):368-373.
104. He K, Rimm EB, Merchant A, et al. Fish consumption and risk of stroke in men. JAMA.2002;288(24):3130-3136.
105. Siscovick DS, Raghunathan TE, King I, et al. Dietary intake and cell membrane levels of long-chain n-3polyunsaturated fatty acids and the risk of primary cardiac arrest. JAMA.1995;274:1363-1367.
106. Khan A, Safdar M, Ali Khan MM, Khattak KN, Anderson RA. Cinnamon improves glucose and blood lipids ofpeople with type 2 diabetes. Diabetes Care.2003;26(12):3215-3218.
107. Khan A, Bryden NA, Polanshy MM, Anderson RA. Insulin potentiating factor and chromium content ofselected foods and spices. Bio Trace Element Res.1990;24:183-188.
108. Broadhurst CL, Polansky MM, Anderson RA. Insulin-like biological activity of culinary and medicinal plantaqueous extracts in vitro. J Agric Food Chem.2000;48:849-852.
109. Anderson RA, Polansky M. Tea enhances insulin activity. J Agric Food Chem.2002;50:7182-7186.110. Dreosti IE. Bioactive ingredients: antioxidants and polyphenols in tea. Nutr Rev. 1996;54:S51-S58.
111. Saller R, Meier R, Brignoli R. The use of silymarin in the treatment of liver diseases. Drugs.2001;61(14):2035-2063.112. Wellington K, Jarvis B. Silymarin: a review of its clinical properties in the management of hepatic disorders.
Bio Drugs.2001;15(7):465-489.113. Steel VE, Kelloff GJ, Balentine D, et al. Comparative chemopreventive mechanisms of green tea, black tea,
and selected polyphenol extracts measured by in vitro bioassays. Carcinogenesis. 200;21(1):63-67.114. Ahmad N, Muktar H. Green tea polyphenols and cancer: biological mechanisms and practical implications.
Nutr Rev. 1999;57(3):78-83.
-
7/25/2019 Nutrigenomics White Paper
35/36
-
7/25/2019 Nutrigenomics White Paper
36/36
154. Taioli E, Bradlow HL, Garbers SV, et al. Role of estradiol metabolism and CYP1A1 polymorphisms in breastcancer risk. Cancer Detect Prev.1999;23(3):232-237.
155. Rosen CA, Woodson GE, Thompson JW, Hengesteg AP, Bradlow HL. Preliminary results of the use ofindole-3-carbinol for recurrent respiratory papillomatosis. Otolaryngol Head Neck Surg.1998;118(6):810-815.
156. Bradlow HL, Michnovicz JJ, Halper M, Miller DG, Wong GY, Osborne MP. Long-term responses of women
to indole-3-carbinol or a high fiber diet. Cancer Epidemiol Biomarkers Prev.1994;3(7):591-595.157. Michnovicz JJ, Adlercreutz H, Bradlow HL. Changes in levels of urinary estrogen metabolites after oral
indole-3-carbinol treatment in humans. J Natl Cancer Inst.1997;89:718-723.
MET1547 12/07