Nurturing a Culture of Patient Safety and Achieving Lower ... · Nurturing a Culture of Patient...
17
Nurturing a Culture of Patient Safety and Achieving Lower Malpractice Risk Through Disclosure: Lessons Learned and Future Directions RICHARD C. BOOTHMAN, SARAH J. IMHOFF, AND DARRELL A. CAMPBELL JR. SUMMARY • In mid-2001 and early 2002, the University of Michigan Health System systematically changed the way it responded to patient injuries and medical malpractice claims. Michigan adopted a proactive, principle-based approach, described as an "open disclosure with offer" model, built on a com- mitment to honesty and transparency. Implementation was followed by steady reduction in the number of claims and various other metrics, such as elapsed time for processing claims, defense costs, and average settlement amounts. Though the model continues to evolve, it has retained its core components and the culture it nurtured while spurring other initiatives such as a unique approach to peer review. In this article we review our experience, identify the essential practical components of our model, offer suggestions for tailoring the approach to other settings, and present some thoughts as to the future of this approach. Richard C. Boothman, JD, is the chief risk officer at the University of Michigan Health System. Sarah J. Imhoff, MHSA, is a JD candidate (2014) at Georgetown University Law Center. Darrell A. Campbell Jr., MD, is the chief medical officer and Henry King Ransom Professor of Surgery at the University of Michigan Health System. RICHARD C. BOOTHMAN; SARAH J. IMHOFF; AND DARRELL A. CAMPBELL JR. • 13
Transcript of Nurturing a Culture of Patient Safety and Achieving Lower ... · Nurturing a Culture of Patient...

Nurturing a Culture of Patient Safety andAchieving Lower Malpractice RiskThrough Disclosure: Lessons Learnedand Future Directions
RICHARD C . BOOTHMAN, SARAH J. IMHOFF, AND
DARRELL A. CAMPBELL JR.
S U M M A R Y • In mid-2001 and early 2002, the University of MichiganHealth System systematically changed the way it responded to patient injuriesand medical malpractice claims. Michigan adopted a proactive, principle-basedapproach, described as an "open disclosure with offer" model, built on a com-mitment to honesty and transparency. Implementation was followed by steadyreduction in the number of claims and various other metrics, such as elapsedtime for processing claims, defense costs, and average settlement amounts.Though the model continues to evolve, it has retained its core components andthe culture it nurtured while spurring other initiatives such as a unique approachto peer review. In this article we review our experience, identify the essentialpractical components of our model, offer suggestions for tailoring the approachto other settings, and present some thoughts as to the future of this approach.
Richard C. Boothman, JD, is the chief risk officer at the University of Michigan Health System.
Sarah J. Imhoff, MHSA, is a JD candidate (2014) at Georgetown University Law Center.
Darrell A. Campbell Jr., MD, is the chief medical officer and Henry King Ransom Professor ofSurgery at the University of Michigan Health System.
R I C H A R D C. B O O T H M A N ; S A R A H J. I M H O F F ; A N D D A R R E L L A. C A M P B E L L JR. • 13

As a result of being
stonewalled by their
caregivers, patients reach
conclusions about their
care without all of the facts
and often lack the medical
For decades, the medical community hasbitterly complained about the adversarialclimate surrounding adverse clinicaloutcomes, but this community has offeredno suitable alternatives (Mello, Studdert,and Brennan 2003). Today's generation ofhealthcare leaders has known nothing elseand has been offered few other ways ofhandling adverse outcomes. Before 2001,University of Michigan Health System(UMHS) was like many self-insured healthsystems in the country. Historically, itadhered to a deny-and-defend approach
to claims arising fromunanticipated medicaloutcomes. The UMHSchanged its approach afterquestioning whether denyand defend best served allof its interests. Despite thefact that the state of Michi-
gan had enacted no recentknowledge to make sense of ^^^ ^^^^ ^^ University
what happened. of Michigan shifted itsapproach in late 2001 and
early 2002 to favor honesty, transparency,and proactivity. This approach has shownpromising results.
UMHS HISTORY: PRE 2001The University of Michigan became self-insured in 1985 and has since internallycontrolled its defenses. With the exceptionof a brief period during which risk manage-ment controlled litigation, litigation man-agement was largely the province of thehealth system legal office, staffed by lawyersin the university's Office of General Goun-sel. Throughout this time, the UMHS hadrelationships with multiple private defensetrial law firms in the belief that competitionwould yield more favorable hourly rates.Independent trial lawyers were regularlyassigned new lawsuits and were expected
to investigate cases, retain independentexperts, and prepare defenses to liability,causation, and damage components of theircases. For the most part, their work wasoverseen and "managed" by lawyers (orearlier, risk managers) who had no personaltrial experience in the defense of malprac-tice actions. Despite a compulsory pre-suitnotice period instituted in Michigan in thespring of 1994, potential claims were rarelyworked up before litigation was filed. Mostassignments to trial lawyers occurred onlyafter the suit's notice period had expired.Before 2001, trial lawyers routinely deniedand defended the vast majority of the UM-HS's claims, consistent with the expecteddeny-and-defend approach.
The internal claims managementarchitecture refiected the commitment todeny and defend: Two commiftees revieweddaims at the end of the process, typicallyjust before cases were set to start trial.One committee reviewed medical defensestrategies, and the other, a traditional daimscommittee, approved settlements or trialdecisions. The UMHS was consciously ethi-cal and risk-averse in responding to patientdaims. Those responsible sought to do "theright thing" in decisions to settle daims,though most decisions occurred near theend of lengthy and costly litigation and mostcases were settled, not tried, regardless ofthe daims' merits.
Deny and Defend:Communication BarriersThe prevalence of deny and defend hasoften been blamed on trial lawyers, butmultiple factors may have spawned theapproach (Boothman et al. 2009). Thehealthcare community, hardwired as all hu-mans with a fight-or-fiight refiex, may havegravitated too eagerly to the trial lawyers'natural instinct to defend assigned claims.
14 • F R O N T I E R S O F H E A L T H S E R V I C E S M A N A G E M E N T 2 8 : 3

Physicians and healthcare executives whowere advised not to talk about adverseevents with a patient or family willinglyobliged, but at the expense of stimulating arobust climate in which patient safety is theprevailing priority. Trial lawyers' perspec-tives and advice largely go unchallengedwhen litigation is managed internally byrisk managers or lawyers with no trialexperience, as they give little considerationto the way in which deny and defend mightinhibit patient safety goals. Regardless ofthe reason, it is no secret that the medicalcommunity has avoided disclosing medicalerrors to patients, with an estimated onein four errors disclosed (Wu et al. 1993;Blendon et al. 2002; Lamb et al. 2003;Gallagher et al. 2003; Kronman, Paasche-Orlow, and Orlander 2011; Kaldjian et al.2008). In addition, it is estimated that lessthan 2 percent of negligent medical errorslead to malpractice litigation, suggestingthat litigation is not as pervasive as mostphysicians believe and patients injuredby medical errors are infrequently com-pensated through litigation (Meyers 1987;Localio et al. 1991; Studdert et al. 2000). Asthe competing interests swirled, the UM H Sopenly questioned whether deny and de-fend was the strategy to serve its needs.
The foundational assumptions support-ing deny and defend create a self-perpetuat-ing spiral that suppresses consideration ofalternative approaches. Underpinning denyand defend are the dual assumptions that(a) when a patient is injured in the courseof an adverse event, a fight is inevitableand (b) a fight is the institution's mostprudent way of responding to the patient'scomplaints. However, patients mainly hirelawyers because of the lack of knowledgethey have about their adverse event (Vin-cent, Young, and Phillips 1994). As a resultof being stonewalled by their caregivers.
patients reach conclusions about their carewithout all of the facts and often lack themedical knowledge to make sense of whathappened. Caregivers and hospitals rarelyact to correct patients' and families' mis-conceptions about their care or attempt tofill in gaps to promote understanding. Themedical community more often views acomplaint as a threat, not an opportunity toreach an understanding based on honestyand openness. Because deny and defendcannot envision communication with ag-grieved parties while the issues are fresh,it is not surprising that patients find silentreinforcement for their own conclusionsand instinctively turn to their own lawyersfor answers (Studdert and Brennan 2001).
Trial lawyers also act on incompleteinformation. They see themselves as advo-cates, not mediators, and aggressively lookto create a case in the context of an asstimedadversarial relationship with those they viewas prospective defendants. These lawyers,governed in part by the exigencies of run-ning a law firm, are compelled to considerthe costs and benefits of taking a case. Law-suits are filed before either side knows ifthey have a true confiict, and hospital execu-tives rarely stop to analyze whether litigatingeach case actually serves their organization'sinterests. Clinicians seem relieved to learnfrom their trial lawyers that they shouldnot talk to aggrieved patients or families,but that short-term liberation comes atthe cost of longer-term misunderstanding.This failure of communication predictablyresults in litigation of questionable necessitywith significant costs to both sides. A recentstudy (Golann 2011) showed that plaintiffsdrop 58.6 percent of medical malpracticecases, mainly due to information accumu-lated during investigation that shows theplaintift^has a weak or frivolous case. In theend, the dearth of communication among
R I C H A R D C . B O O T H M A N ; S A R A H J. I M H O F F ; A N D D A R R E L L A. C A M P B E L L J R . • 15

caregivers, patients, and trial lawyers affordslittle chance that the parties will achieve anunderstanding short of litigation; the factthat the understanding occurs in the courseof litigation only reinforces the visceralimpression in the healthcare communitythat unanticipated clinical outcomes spawnadversarial proceedings. The spiral isself-sustaining.
Deny and Defend: Safety BarriersThe adversarial posturing between pa-tients and their caregivers under the
deny-and-defend approachCasting apology as a is especially unfortunate
claims management tactic 8^^^" *^ seriousness andprevalence of injuries that
only undervalues the • r r • l A-
model and the pivotal role dne. The Institiite of Medi-honesty plays in patient cines pronouncement that
f f. f f- II nearly 100,000 lives werebeing lost through medi-
and culturally. ^al error each year helpedcreate national awareness
about the prevalence of medical errors,and based on this knowledge the UMHSstarted investing more resources intopatient safety efforts (Kohn, Gorrigan,and Donaldson 2000). In fall 2002, Dar-rell Gampbell Jr., MD, (an author of thispiece), then chief of staff, publicly pro-nounced his aspiration for the UMHS "tobecome the safest hospital in the UnitedStates" (Anstett 2004). Deny and defendwas a barrier to that goal.
One of the most significant costs ofdeny and defend is the chilling effect ithas on patient safety. Deny and defend el-evates the goal of protecting the institutionagainst the anticipated claim at the cost ofputting present and future patients at riskfor similar injuries. Trial lawyers, drivenmyopically by their instinct to control theflow of information in order to maximize
their courtroom chances, routinely defendclinical care that should not be defendedand instruct caregivers not to talk withanyone about their claim for fear of havingan unprotected admission find its wayinto evidence. Thus, any impulse to use amedical injury to improve care and pre-vent future similar errors is snuffed. Denyand defend chills even the most robustsafety intentions.
Patient safety efforts are ftirther com-promised by poor communication amongcaregivers, their patients, and attorneys. Un-like other types of personal injury litigation,medical outcomes caused by medical errorrarely are immediately distinguishable firomthose that occurred despite reasonable care.A paradigm that discourages communica-tion breeds needless litigation, as the patient,caregivers, and health system all act on anincomplete understanding of the event.Litigation focuses energy away firom improv-ing care and preventing future errors. Inmid-2001, deny and defend no longer madesense to an organization that viewed itselfas ethical and determined to be the safesthospital in the nation. Thus, in early 2002,having already started the change in itsclaims management approach, the UMHSmoved to recondle its twin goals by creatingthe Michigan Model.
THE MICHIGAN MODEL:BEGINNINGS
Greating the Michigan Model was stimu-lated by a set of simple but forcefulrealizations:
• By relying on trial lawyers to drive theinstitution's response to patient inju-ries, the UMHS predictably found itselfin a fight in the majority of claims.
• With its resources, the UMHS didnot need litigation to determine the
l 6 • F R O N T I E R S O F H E A L T H S E R V I C E S M A N A G E M E N T 2 8 : 3

difference between reasonable andunreasonable care.
• Litigation, with its uncertainty and highfinancial, emotional, and productivitycosts, should be avoided except as a lastresort.
• Seftling cases in which the clinical carewas reasonable or did not cause injuryblurred core corporate principles andleft clinical staff demoralized.
• Most important, defending care thatwas below the UMHS's standard ofpractice generated both significant un-necessary costs and undermined insti-tutional quality and safety culture goals,sending the wrong message to the staffand public.
Beginning in the fall of 2001, threeprinciples were circulated for approvalamong those involved in UMHS claimsmanagement:
1. Compensate patients quickly andfairly when unreasonable medical carecaused injury.
2. If the care was reasonable or did notadversely affect the clinical outcome,support caregivers and the organizationvigorously.
3. Reduce patient injuries (and thereforeclaims) by learning through patients'experiences.
The principles drew no opposition, andthey remain universally incontestable. Adecade into the UMHS's experience, theycontinue to serve as the foundation of theUMHS's response to patient injury andmedical errors.
The Michigan Model: BackboneThe Michigan Claims Management Modelhas been well-described in journals (see
Boothman et al. 2009 for further detail).The model has also been described inthe popular press, although it is almostinvariably shortchanged by headlines thatcarry some derivation of "Apologies SaveMoney" (Tanner 2009; Gotbaum 2007;Koranda 2010; Arbogast 2004). Apologiescan save money and an honest approachdoes work to improve claims manage-ment numbers, but highlighting the roleof apology in that way cheapens it as littlemore than a claims management strategy.Casting apology as a claims managementtactic only undervalues the model and thepivotal role honesty plays in patient safety,functionally and culturally. To understandthe Michigan Model, it is critical to under-stand that the claims management pro-cess is only the public face of an organicculture shift that seeks to elevate patientsafety to the foreground and relegateclaims considerations to the background.
The UMHS's approach was molded bymany intrinsic and extrinsic factors. Itshistory, culture, idiosyncrasies, resources,jurisdiction, and the relationship the insti-tution has with the courts and the plain-tiffs' bar all affect its architecture (Booth-man et al. 2009). Every healthcare systemwill create an approach that meets its ownneeds, but after ten years, the UMHS'sapproach can be distilled to identifiableelements that, if included in any approachfor handling adverse medical outcomes,should yield similar results. (See Kachaliaet al. 2010 for results.) Before reviewingthe model's elements, an organizationinterested in designing its own alternativeto deny and defend would be well-servedby minding some basic realities.
Accountability: At the heart of the MichiganModel is a difterent mindset about patientinjuries—one that lifts heads previously m
R I C H A R D C . B O O T H M A N ; S A R A H J. I M H O F F ; A N D D A R R E L L A. C A M P B E L L JR. • 17

Leadership's flrmcommitment to change
can temper resistance fromthe considerable body of
doubters embedded in anysystem subscribed to deny
and defend.
cowering in the trenches waiting for a law-suit to drop, and states unflinchingly: "Weown patient injuries. News of a patient'sinjury does not represent a threat to us butcreates an obligation we must meet andaddress in a straightforward, principledway so it never happens again."
Caregivers have convinced themselvesthat they are victims of a perverse and bro-ken system (Sage 2005; Studdert, Mello, andBrennan 2004). The sense of victimhoodis strong and causes stress and palpablefear (Wu 2000). Accoimtability requires adetermination to take control over the dia-logue surrounding adverse patient outcomes
within the firamework ofethical, corporate, andprofessional principles. Itviscerally recoils firom theold practice of deferring toothers (e.g., lawyers, regula-tors) for an assessment ofwhether an outcome oc-curred through negligenceor reasonable care. Seizingcontrol over this dialogue
diminishes anxiety and encovurages a posi-tive culture of patient safety. In this mindset,defense attorneys are valuable tools to beused selectively when warranted, not ersatzleaders driving corporate ethics.
Honesty: At the very core of the model ishonesty. The model's three foundationalprinciples demand an assessment as towhether the care giving rise to an unan-ticipated clinical outcome was reasonable;therefore, the prerequisite commitmentmust be to honesty in these evaluations.The first disclosure is always the one wemake to ourselves. This is not a new con-cept: Alcoholics Anonymous led its 12-stepprogram with that commitment to per-sonal honesty in the 1930s (AA 2002).
Neither claim gains nor patient safetyimprovements are possible withouthonesty. Litigating claims that should beresolved is abusive to all concerned—pa-tients, healthcare providers, and institu-tions. Denying and defending claims thatarise from true medical errors wastesopportunities to lower malpractice costs,freezes initiatives for improving care, andundermines attempts to instill a rigor-ous culture promoting safety and clinicalquality. Conversely, paying on groundlessclaims also undermines efforts at culturechange. The practice erodes the moraleof healthcare providers who work in anintrinsically risky environment. It encour-ages patients to believe that every undesir-able outcome was the result of medicalerror, encourages plaintiffs' lawyers tosee lawsuits as risk-free, and encouragescourts to believe that the most effectiveway of clearing their dockets is to lean onthe healthcare institution to pay regardlessof merit. Worse, the practice reinforces theidea that malpractice claims are inevi-table, simply a cost of doing business andvalueless as a barometer of patient safety.Paying groundless claims erodes account-ability just as effectively as misguidedlydefending medical errors does.
Principles: The approach requires cou-rageous, though not blind, adherenceto the model's three central principles.Generally, adherence to principles createsconsistency and predictability in behavior,processes, and operations, which are im-portant in redirecting all those with a stakein unanticipated outcomes. The benefits ofconsistency and predictability to frontlinestakeholders, such as the patient, family,and caregivers, are obvious, but a consid-erable number of others also benefit froma predictable institutional response to
i 8 • F R O N T I E R S O F H E A L T H S E R V I C E S M A N A G E M E N T 2 8 : 3

adverse medical events. That list includesthe local legal community, judges, regula-tory and accrediting agencies, lienholders,medical and claims staffs of other hos-pitals, and the surrounding community.It is easy to miss the broad audience andthe degree to which one health system'spattern of response to medical injuries canaffect other caregivers and other healthsystems. Predictability becomes credibility,which stimulates robust engagement ofall stakeholders and feeds both the patientsafety and claims management activities.
Dismissing Fear: Fear is the single mostpowerful factor suppressing explorationof more constructive alternatives (Lambet al. 2003)—fear of inviting litigation,fear of complicating litigation, and fearof making a mistake that will lead to acatastrophic claims outcome. Physiciansfear the patient's reaction, and somerationalize away the need to tell a patientabout an error if the patient does not seemaware of it already—essentially, the doc-trine of "Let sleeping dogs lie" (Wu et al.1997; Gallagher et al. 2003; Studdert et al.2000). Fear prompts the medical com-munity to rely almost exclusively on a legalsystem that does not serve their needs andis expensive financially and emotionally.Overcoming fear is always a prerequisiteto paradigm shifting. Leadership mustcommunicate priorities clearly and createa safe environment for its claims manage-ment professionals to explore an approachthey've spent their careers avoiding. Lead-ership's firm commitment to change cantemper resistance from the considerablebody of doubters embedded in any systemsubscribed to deny and defend. Securingsolid expertise in the trenches amelioratesfears by building confidence of those whorely on institutional claims management.
Gaining Support for Implementing aNew ModelGonsider the following before creating yourinstitution's version of the Michigan Model.
Board of Directors: Gonsider presentingthe paradigm shift to the board first. Ifthe program is seen as a low priority or ifthe board resists, build evidence by start-ing small and publicizing the gains. Withenough success, support for the programshould rise because "leadership" followssuccess in many institutions. As boardsgenerally feel compelled to be moreinvolved in an issue when presented withdata, building board support can lessenfear among medical staff and those inclaims management of doing somethingconsidered dangerous or counterintuitiveto the institution's goals.
Medical Leadership: Identify caregiverchampions. Align the program withmedical leadership. One of the first casesto come up for trial after the UMHS shiftinvolved the chair of a major department,who assumed his case would be settledconsistent with the traditional deny-and-defend approach. Once the chairunderstood the importance of adheringto principles, the case, deemed ground-less, proceeded through a lengthy butsuccessful trial. The department chairsaw the value of the program and imme-diately communicated the new paradigmto other physician leaders in the system.Additionally, Dr. Gampbell, the incomingchief of staff at the time, openly pro-moted the program among the medicalstaff and hospital leadership while fight-ing for its implementation politically.Support from medical leadership waskey in overcoming objections from theuniversity's legal circles.
m
m
R I C H A R D C. B O O T H M A N ; S A R A H J. I M H O F F ; A N D D A R R E L L A. C A M P B E L L JR. • 19

Quickly engaging
patients and families with
accurate information can
help them understand
what happened before
misimpressions form and
they feel the need foran advocate.
Department chairs must understandhow the model supports the quality andsafety missions of their departments.Patient safety trends should be discussedto develop annual goals of improvementand strategies for achieving those goals.Cultivating a sense of control and ac-countability feeds departmental safetygoals and aligns them with claims reduc-tions. At the UMHS, that clear alignmenthelped direct the medical department toproactively tailor departmental patientsafety and educational efforts.
Communicating themodel to the medicalstaff at large is impor-tant. Reassuring the staffthat meritorious claimswill be resolved andnon-meritorious claimsavoided should appeal totheir immediate interests.Connecting directiy withpatient safety improve-ment appeals to the very
reason they entered their profession. Overtime, as data accumulates and confidenceincreases, medical staff will support theinitiative. Without support from keyphysician leaders, the UMHS would havelapsed to the security of the status quo.
ESSENTIAL ELEMENTS OF THEMODELIn The Seven Habits of Highly EffectivePeople, Stephen R. Covey (1989) admon-ishes us to "begin with the end in mind."If there were an ideal system for resolvingpatient disputes that arise from clinicalcare without the vagaries and expense ofthe legal system, while instilling a cul-ture focused on patient safety and qualityclinical care, what would it look like? TheUMHS has seen promising results as it
works to answer that question. Though themanner in which they are created mightdiffer from institution to institution, afterten years of experience, the followingelements seem indispensable to the dualpurposes of enhancing patient safety andreducing litigation costs.
i: Capturing Clinical Issues. Problemscannot be fixed if problems are not known.The problem's magnitude is not clear ifclose calls and adverse events are not col-lected and analyzed. Thus, it is importantto strategically approach data collection.
Voluntary reporting is limited by a vari-ety of factors, including caregivers' reluc-tance to report due to fear of implicatingthemselves or their peers, lack of trainingon what should be reported, insensitiv-ity to the importance of reporting, and ahistory of unresponsiveness that damp-ens any sense that reporting a complaintwill lead to improvement in the qualityof care (Levinson 2012; Farley et al. 2010;Rowlin et al. 2008; Kaldjian et al. 2008).AU healthcare systems have pockets ofinformation that can and should be tappedproactively.
Healthcare providers themselves are avaluable source of safety data, but they arefamously reluctant to complain proactivelyabout their colleagues' behavior (Levinson2012; Kaldjian et al. 2008). Witness therelatively anemic performance of mostpeer review systems, which too often donot engage until a provider proves toodangerous to be ignored (Baldwin et al.1999). All caregivers have personal lists ofprocesses and people that represent genu-ine, potential patient safety threats; howcan that information be tapped.-* Billingdata that tap patient safety indicators suchas blood loss, hemorrhage after surgery,and readmission rates are fertile sources
2 0 • F R O N T I E R S O F H E A L T H S E R V I C E S M A N A G E M E N T 2 8 : 3

of safety information. Seeing the vastpotential for further safety improvements,the UMHS has been working on systemsfor effectively capturing clinical data (Bahlet al. 2008). Tapping unused pockets ofinformation can reveal potential safety is-sues and unlock valuable opportunities forimprovement.
Speed is important. Collecting informa-tion as soon as the adverse event or closecall occurs is critical because it promotesimmediate action to correct the root causeof an event and prevents errors fromrepeating. Speed also provides a valuableclaims management opportunity, becausequickly engaging patients and familieswith accurate information can help themunderstand what happened before misim-pressions form and they feel the need foran advocate.
2: Identification of Medical Errors. Health-care providers work in a dangerous worldwith no promises that their clinical inter-ventions will have the intended effect orthat they won't cause harm as they try tohelp. Unanticipated outcomes alone donot equate to medical mistake. Organi-zations need a reliable means of distin-guishing unfortunate clinical outcomesthat warrant compensation from adverseoutcomes that occurred despite reasonablecare. In a deny-and-defend model, unrea-sonable and reasonable care are eventuallydistinguished through litigation, but theresult is vulnerable to irrelevant factorssuch as how vwtnesses perform for thejury, and results come with extiaordinarycost and delay. Determining when care hasmet professional and institutional expec-tations is fundamentally a clinical, not alegal, question; the most reliable assess-ments are derived from robust and honestevaluations by clinicians who subscribe
to the critical importance of honesty, notdefensiveness. Making credible determina-tion of reasonable or unreasonable care iscential to the model and key to developinga sense of contiol and accountability.
3: Gommunication. Communicationamong patients, families, and caregiv-ers demands a mix of skills. In the acutephase following an adverse event, com-passionate and careful listening is vitalto understand the patient's or family'sperspective and help them realize theinstitution will suppori their needs. Set-ting reasonable expectations is also key,as too much unexplained delay creates asense that critical information is beingconcealed. The same challenges apply tocommunications with caregivers, mostof whom experience a complex mix ofemotions that includes betrayal, guilt, fear,and shame (Wolf et al. 2000; Newman1996; Wu 2000). Sensitive listening andclear and compassionate communicationare essential to moving the adverse eventsto constructive grounds. The UMHS riskmanagement consultants all have formalmediation training and legal resourcesreadily available.
Once a disclosure is made, however, itis difficult to undo if it is later discoveredto be inaccurate or false. Admissions canrarely be retracted; denials that turn out tobe erroneous undermine credibility goingforward. The UMHS risk managementconsultants have learned the importanceof being disciplined about sharing facts,not speculation.
4: Gompensation. Ludan L. Leape (2009)has said, "Apology without compensationis like taking a shower in a raincoat. You'redoing the right thing, but you don't get wetand you're still dirty." Gompensating patients
C
R I C H A R D C . B O O T H M A N ; S A R A H J. I M H O F F ; A N D D A R R E L L A . C A M P B E L L J R . • 21

The greatest value of
proactivity is to ensure
that future patients are
not harmed while an
individual's claim is being
adjusted.
for injuries caused by medical errors isan important component of the model. Itavoids expensive and needless litigation,provides patients and staff needed closure,and quickly establishes critical organiza-tional credibility. Unwillingness or in-ability to provide compensation signifies alack of sincerity, suggesting that apologiesare liftle more than a claims managementstratagem.
Valuing a case can be difficult. Casevalue is affected by many intangible ele-ments, such as the strength of liability and
causation elements, shockvalue, subjective pain andsuffering, and economiccomponents affected bya myriad of assumptions.Valuing cases is an art,not a science. The UMHSuses economic experts,financial planners, life care
planners, and benefit specialists in thepatients' areas of need to calculate a justmonetary figure. Adequacy of compensa-tion is often measured against a sense forwhat a case might bring in a courtroom, sothere must be understanding of the claim'svalue in the context of litigation. This neednot bind any program, but failing to heedthis value could cause aggrieved patientsto feel the hospital is taking advantage ofthem with an attempt at early but cheapintervention.
5: Learning from Mistakes. The patientinjured by medical error represents animmediate financial exposure to theorganization. The greatest value of proac-tivity is to ensure that future patients arenot harmed while an individual's claim isbeing adjusted. Submitting future patientsand caregivers to the same risk of injury isnot just imprudent, it is unethical. When
preventable injury occurs, the organiza-tion and its staff are changed. None arenaïve to the risk that a patient can beinjured. That new knowledge imposesan urgent duty to ensure that future pa-tients are not similarly injured. The sys-tem must be hard-wired so that knowl-edge of the safety risk is disseminatedto those who can implement change andbe accountable for taking steps to ame-liorate the risk as quickly as possible.Doing so in a legally protected way willensure that addressing the root causesof medical errors becomes an organiza-tional habit, not a risk in itself.
6: Measurement. Data collection drivesmodern medicine. It provides evidenceof effective change and facilitates return-on-investment analyses that enable anorganization to determine whether todevote resources to an approach, changeaspects of the tactic, or pursue anothermodel. The UMHS collected data on theparameters of its model and has con-stantly tweaked the model and gaugedits effect on improvements (Kachalia etal. 2010). With each year of data, newfive-year plans are developed to furtherlower the number of claims filed, di-minish costs, and reduce patient safetyevents. Without measurement, analyzingthe success of a new approach on costreduction or quality of care outcomeswould not be possible.
7: Resources. The resources needed toimplement an institution's version of theMichigan Model will vary by institutionand evolve over time. One can start bysimply deploying defense counsel dif-ferently without increasing overhead. Inimplementing the model, ensure the rightpeople are in the right roles.
2 2 • F R O N T I E R S O F H E A L T H S E R V I C E S M A N A G E M E N T 2 8 : 3

MICHIGAN'S EXPERIENCE WITHTHE MODELIn one of the most famous momentsin US presidential debate history, Ron-ald Reagan turned to the audience andbluntly posed a memorable question:"Ask yourself, are you better off nowthan you were four years ago.'" Thechanges the UMHS has enacted havenot completely rid the health system ofmalpractice claims and lawsuits, but itis clear that the health system is betteroff now than it was ten years ago. As forits claims experience, between 1995 and2007, when comparing before and afterimplementation of the Michigan Model, theUMHS lowered its average monthly costrates for total liability, patient compensation,reserves, and non-compensation legalcosts (Kachalia et al. 2010). The UMHSalso reduced its average monthly rate ofnew claims from 7.03 to 4.52 claims per
100,000 patient encounters, decreasedthe average monthly rate of lawsuitsfrom 2.13 to 0.75 per 100,000 patientencounters, and reduced the time betweenclaim reporting and resolution (Kachaliaet al. 2010).
The UMHS widely communicated itsapproach to the plaintiffs' bar and Michi-gan courts at the outset. In the program'sfirst year, plaintiffs' lawyers changed theway they approached the UMHS aboutclaims. They now openly engage theUMHS before claims are asserted and be-fore a suit is contemplated. With open dia-logue, plaintiffs' lawyers are able to makebetter choices about the cases they elect tofile and the UMHS is able to resolve mostmeritorious claims without litigation.
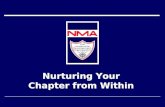
Settlements of non-meritorious (casesin which the UMHS felt the standard ofcare was met) claims occurred frequentlybefore 2001 as depicted in Exhibit i. Since
E X H I B I T 1 U M H S FY claims by incident Date; Number of Settlements Paid by UMHS Standardof Care Assessment
SOC = Standard of Care
m
C
75
R I C H A R D C. B O O T H M A N ; S A R A H J. I M H O F F ; A N D D A R R E L L A. C A M P B E L L J R . • 23

the adoption of a principled approach,the number of non-meritorious settle-ments has significantly decreased, leavingmeritorious claims (in which the UMHSagrees the standard of care was not met)to make up the majority of settlements.This experience has resulted in overalllower claims numbers because the UMHSis now largely spared the need to defendnon-meritorious claims. The importanceof this experience transcends claims sav-ings alone. Unlike other institutions thatregard malpractice as an inevitable cost of
doing business and not anIsolating legitimate claims indication of the quality
allows the health system ° ' ' ' *^ ^^"^ ^ ' ^strong sense of account-
to precisely examine ability for the remainingpatterns of behavior, staff claims. Though the finan-members, and processes i l cost of true medical
, , , ,. , , errors is sobering andthat signal fixable ¿i^^pp^inting, the clarity
problems. that results from analysispresents opportunities
for positive change. We can delve deeplyinto the remaining claims for patterns tostrategically target those areas in which er-rors have occurred and further reduce thenumber of claims through patient safetyimprovements.
The UMHS can no longer blame preda-tory lawyers and opportunistic patientsfor its malpractice losses. Isolating legiti-mate claims allows the health system toprecisely examine patterns of behavior,staff members, and processes that signalfixable problems. The UMHS can at leastput a partial price tag on the cost of failureto provide patients the quality of care theydeserve. This engenders a sense of ac-countability and a greater sense that thehealth system can control its malpracticecosts through improvements in patientsafety. The direct link between patient
safety and medical malpractice has histori-cally been elusive for most institutions;one of the most salient benefits derivedfrom the Michigan Model is the graphicdemonstration ofthat clear link, which isoften obscured by the "noise" of litigationover complications that arise in spite ofreasonable clinical care.
FUTURE INITIATIVES
Aside from focusing on specific clinicalissues and problematic staff membersidentified through analysis of claims,broader realizations have emerged fromthe UMHS's decade of experience.
New Process to Effectuate ChangingCultureThe UMHS has made measurable prog-ress toward its overall goals of changingculture, improving patient safety, andfurther reducing malpractice costs. Themodel has contributed to a culture ofpatient safety that is presently driving aradical redesign of the institution's patientsafety architecture along a functional fiowintended to
• strategically collect clinical information,• methodically assess and analyze that
information to establish institutionalpriorities,
• assign responsibility for change,• measure effectiveness and communi-
cate institutional priorities, and• share successful changes to stimulate
greater understanding of and interestin our priorities and efforts throughoutthe organization.
The work is moving apace without de-fensiveness. The old distinctions betweenrisk management, quality improvement,and customer relations have blurred as
2 4 • F R O N T I E R S O F H E A L T H S E R V I C E S M A N A G E M E N T 2 8 : 3

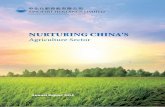
the health system tackles patient safetyenterprise-wide. Focusing on safe andhigh-quality clinical care strongly suggeststhat these concepts, previously consideredseverable, are actually inseparable ideasalong a continuum of care. As a conse-quence of the UMHS's clearer focus onsafer patient care, a functional fiow forisolating and approaching clinical safetj?concerns has emerged, which transcendsthe old definitions and boundaries withthe promise of true clinical improvement.The algorithm is shown in Exhibit 2.
Shared Decision MakingThe experience of hundreds of "disclo-sures" graphically proves that caregivercommunication lags behind patientneeds and expectations. As the healthcarecommunity moves at a glacial pace fromphysician-centric to patient-centric care,patients' expectations about their owndirect involvement with healthcare deci-sions are moving much faster, hastened byaccess to information through the Internetand media. From a medical malpracticeperspective, greater patient control overmedical decision making should yieldgreater patient accountability for clini-cal outcomes, but clarifying physicians'personal accountability depends directiyon the quality of the communication. TheUMHS experience highlights the urgency
to adopt an organically different view ofthe relationship among patients, caregiv-ers, and the healthcare system. Embed-ding concepts of shared decision makingseems to be the inevitable step towardstrengthening the notion that "we're inthis together," a cultural shift that can onlystrengthen the therapeutic relationshipand lower the likelihood that patients turnto the legal system first to deal with unex-pected outcomes.
Peer ReviewMost healthcare systems struggle with peerreview. Historically considered a disciplinetool, peer review too often is invoked onlyafter a caregiver bottoms ouf and becomesa problem that can no longer be ignored(Brennan 1999). As a direct consequenceof its embrace of honesty and transparency,the UMHS continues to boldly refine itsinnovative approach to peer review. Rea-soning that peer review should be relevantand proactive, departments were chal-lenged to identify events particular to theirpractice that would mark potential patientsafety concerns. Those events, describedas patient safety indicators, are keyed tobilling and other retrievable data (Bahl et al.2008). In many departments, caregivers'clinical performances are measured di-rectly against those of their colleagues, andoutiiers can be identified and corrected
E X H I B I T 2 Flow for Capturing, Prioritizing, and Addressing Safety Concerns
Recognition/Capture of the Clinical Problems and Risks
Dissemination/Communication of Successes
Assessment and Response with Clinical Care Improvements
Assessment of Performance/Capturing Metrics onImprovement and Unintended Consequences
m
-i
C
m
R I C H A R D C. B O O T H M A N ; S A R A H j . I M H O F F ; A N D D A R R E L L A. C A M P B E L L J R . • 25

Recent studiesdemonstrate that despitethe attention created by
the Institute of Medicine'sestimates of needless
human injury and death,the quality of medical care
in the United States hasnot improved.
earlier than ever before. As the metrics areclinically relevant, the system is embracedas an integral pari of departmental qualityinitiatives. The approach loses its disci-plinary feel with earlier intervention andits promise to embrace and improve. Thiskind of peer review would not be possiblein a deny-and-defend environment.
Health System Cultural BenefitsThe tangible benefits of the UMHS ap-proach to medical liability claims maybe linked to a profoundly more impor-
tant, but less tangible,benefit concerning aninstitution's overall safetyculture. Many aspects ofthe UMHS approach to
visible to the thousandsof UMHS employeeswho care for patients andarguably set the tone forother drcumstances inwhich the core values ofhonesty and trust are of
paramount medical importance. Onecould argue that if implementation ofthe UMHS approach to liability had animportant ripple effect on other aspectsof medical care within the system, itshould be manifest in an improvingsafety culture. Indeed, overall safetyculture scores at UMHS, as measuredby the biannual Safety Attitudes Ques-tionnaire, have improved steadily overthe past six years. While admittedly it ishard to prove cause and effect, an im-proving safety culture is another impor-tant metric, in addition to claims data,that supports the value of the UMHSapproach to liability. If this is true, theliability approach has value far in excessof its impact on claims.
HEALING MEDICINEThe collateral damage from deny anddefend has been underappreciated. Itsimpact has long obscured the direct con-nection between lapses in patient safetyand medical malpractice litigation. Itsdirect, albeit unintended, consequencesinclude a fundamental failure to accept re-sponsibility for patient injuries caused bytrue medical error, and that failure in turnaccounts for decades of needless litigationand all of its attendant personal, financial,and ethical costs. Recent studies demon-strate that despite the attention createdby the Institute of Medicine's estimatesof needless human injury and death,the quality of medical care in the UnitedStates has not improved (Landrigan et al.2010). Abandoning deny and defend canbe a critical first step to recovery.
REFERENCESAlcoholics Anonymous (AA). 2002. Twelve
Steps and Twelve Traditions. New York:Alcoholics Anonymous World ServicesInc.
Anstett, P. 2004. "U-M Hospital's Goal:Safest in the Nation." The Detroit FreePress February 24.
Arbogast, C. R. 2004. "Can ApologizingAvoid Malpractice Suits. " MSNBC.Updated November 11. www.msnbc.msn.com/id/6462162.
Bahl, V., M. A. Thompson, T.Y. Kay, H. M.Hu, and D. A. Campbell. 2008. "Do theAHRQ Patient Safety Indicators FlagConditions That Are Present at the Timeof Hospital Admission?" Medical Care 46(5): 516-22.
Baldwin, L .M., L. G. Hart, R. E. Oshel, M.A. Fordyce, R. Cohen, and R. A. Rosen-blatt. 1999. "Hospital Peer Review andthe National Practitioner Data Bank."Journal of the American Medical Associa-tion 281 (4): 349-55.
Blendon, R. J., C. M. DesRoches, M. Brodie,J. M. Benson, A. B. Rosen, E. Schneider,
26 • F R O N T I E R S OF H E A L T H SERVICES M A N A G E M E N T 2 8 : 3

D. E. Altman, K. Zapert, M. J. Herrmann,and A. E. Steffenson. 2002. "Views ofPracticing Physicians and the Public onMedical Errors." New England Journal ofMedicine 347 (24): 1933-40.
Boothman, R. C, A. C. Blackwell, D. A.Campbell Jr., E. Commiskey, and S.Anderson. 2009. "A Befter Approach toMedical Malpractice Claims? The Univer-sity of Michigan Experience."/oumai ofHealth and Life Sciences Law 2 (2): 125-59.
Brennan, T. A. 1999. "Hospital Peer Reviewand Clinical Privileges Actions: To Reportor Not Report." Jowmai of the AmericanMedical Association 281 (4): 381-82.
Covey, S. R. 1989. The Seven Habits of HighlyEffective People. New York: Fireside.
Farley, D. 0., A. M. Haviland, A. C. Haas,and C. Pham. 2010. "Adverse EventReporting Practices by US Hospitals:Survey Results from 2005 and 2009."RAND Health. Published July 2010. www.rand.org/pubs/working_papers/2Oio/RAND_WR752.sum.pdf
Gallagher, T. H., A. D. Waterman, A. G.Ebers, V. J. Fraser, and W. Levinson.2003. "Patients' and Physicians' AttitudesRegarding the Disclosure of MedicalErrors." Journal of the American MedicalAssociation 289 (8): 1001-07.
Golann, D. 2011. "Dropped Medical Malprac-tice Claims: Their Surprising Frequency,Apparent Causes, and Potential Rem-edies." Health Affairs }0 (7): 1343-50.
Gotbaum, R. 2007. "Practice of HospitalApologies Is Gaining Ground." NationalPublic Radio. Published October 6.www. npr. org/templates/story/ story.
KachaHa, A., S. R. Kaufhian, R. Boothman, S.Anderson, K. Welch, S. Saint, and M. A.Rogers. 2010. "liability Claims and CostsBefore and After Implementation of aMedical Error Disclosure Program." Annalsof Internal Medicine 153 (4): 213-21.
Kaldjian, L C, E. W. Jones, B. J. Wu, V. LForman-Hoffinan, B. H. Levi, and G. E.Rosenthal. 2008. "Reporting MedicalErrors to Improve Patient Safety: A Surveyof Physicians in Teaching Hospitals."Archives of Internal Medicine 168 (i): 40-46.
Kohn, L. T, J. M. Corrigan, and M. S. Donald-son, (eds). 2000. To Err Is Human. Wash-ington, DC: National Academy Press.
Koranda, J., 2010. "Apologies Might SaveDocs From Being Sued." The WichitaEagle. Published February 7. www.kansas.com/2010/02/07/1170371/ght-save-docs-from-being-sued.html.
Kronman, A. C, M. Paasche-Orlow, and J. D.Orlander. 2011. "Factors Associated withDisclosure of Medical Errors by Hous-estaff." BMJ Quality <? Safety September22 (Online ahead of print). doi:io.ii36/bmjqs-2011-000084.
Lamb, R. M., D. M. Studdert, R. M. J.Böhmer, D. M. Berwick, and T. A.Brennan. 2003. "Hospital DisclosurePractices: Results of a National Survey."Health Affairs 22 (2): 73-83.
Landrigan, C. P., G. J. Parry, C. B. Bones, A.D. Hackbarth, D. A. Goldmann, and P. J.Sharek. 2010. "Temporal Trends in Ratesof Patient Harm Resulting from MedicalCare." New England Journal of Medicine363 (22): 2124-34.
Leape, L. L. 2009. "Fulfilling the Promise:Keynote." Speech at Fulfilling the Prom-ise: Advancing Patient Safety and MedicalLiability Reform Innovations Forum,Common Good. December 10.
Levinson, D. R. 2012. "Hospital IncidentReporting Systems Do Not Capture MostPatient Harm." Report number OEI-06-09-00091. Washington, DC: Office ofInspector General, US Department ofHealth and Human Services.
Localio, A. R., A. G. Lawthers, T. A. Bren-nan, N. M. Laird, L. E. Hebert, L. M.Peterson, J. P. Newhouse, P. C. Weiler,and H. H. Hiatt. 1991. "RelationBetween Medical Malpractice Claimsand Adverse Events Due to Negligence:Results of a Harvard Medical PracticeStudy III." New England Journal ofMedicine 325 (4): 245-51.
Mello, M. M., D. M. Stiiddert, and T. A.Brennan. 2003. "The New MedicalMalpractice Crisis." New England Journalof Medicine 348 (23): 2281-4.
Meyers, A. R. 1987. "Lumping It: TheHidden Denominator of the Medical
>
- i
R I C H A R D C . B O O T H M A N ; S A R A H J. I M H O F F ; A N D D A R R E L L A. C A M P B E L L JR. • 27

Malpractice Crisis." American Journal ofPublic Health 77 (12): 1544-48.
Newman, M. C. 1996. "The Emotional Impactof Mistakes on Family Physicians." ArchivesofEamily Medicine 5 (2): 71-5.
Rowlin, E. J., D. Lucier, S. G. Pauker, S.Kumar, J. Chen, and D. N. Salem. 2008."Does Error Reporting by Physicians andNurses Diner}" Joint Commission Journalon Quality and Patient Safety 34 (9):537-45-
Sage, W. 2005. "Medical Malpractice Insur-ance and Üie Emperor's Clothes." 54DePaul Law Review 54 (March 24): 463-64.
Studdert, D. M., andT. A. Brennan. 2001."No-fault Compensation for MedicalInjuries: The Prospect for Error Preven-tion." Journal of the American MedicalAssociation 286 (2): 217-23.
Stiiddert, D. M., M. M. Mello, and T. A.Brennan. 2004. "Medical Malpractice."New England Journal of Medicine 350 (3):283-92.
Studdert, D. M., E. J. Thomas, H. R. Burstin,B. I. Zbar, E. J. Orav, and T. A. Brennan.2000. "Negligent Care and MalpracticeClaiming Behavior in Utah and Colo-rado." Medical Care 38 (3): 250-60.
Tanner, L. 2009. "Doctors Urged to Say 'I'mSorry.'" CBS News. PubHshed February 11.www.cbsnews.com/st0ries/2004/11/11/health/main6552i9.shtml.
Vincent, C., M. Young, and A. Phillips.1994. "Why Do People Sue Doctors.-* AStudy of Patients and Relatives TakingLegal Action." Lancet 343 (8913):1609-13.
Wolf, Z. R., J. F. Serembus, J. Smetzer, H.Cohen, and M. Cohen. 2000. "Responsesand Concerns of Healthcare Providers toMedication Errors." Clinical NurseSpecialist 14 (6): 278-87.
Wu, A. W. 2000. "Medical Error: TheSecond Victim. The Doctor Who MakesMistakes Needs Help Too." BritishMedical Journal }2O (7237): 726-7.
Wu, A. W, T. A. Cavanaugh, S. J. McPhee, B.Lo, and G. P. Micco. 1997. "To Tell theTruth: Ethical and Practical Issues inDisclosing Medical Mistakes to Patients."Journal of General Internal Medicine 12(12): 770-5.
Wu, A. W, S. Folkman, S. J. McPhee, and B.Lo. 1993. "How House Officers Copewith Their Mistakes." Western Journal ofMedicine 159 (5): 656-69..
2 8 • F R O N T I E R S O F H E A L T H S E R V I C E S M A N A G E M E N T 2 8 : 3

Copyright of Frontiers of Health Services Management is the property of American College of Healthcare
Executives and its content may not be copied or emailed to multiple sites or posted to a listserv without the
copyright holder's express written permission. However, users may print, download, or email articles for
individual use.