
Nursing Care of the Low-Risk Postpartum Family. Clinical Assessment Review antepartum and...
100
Nursing Care of the Low-Risk Postpartum Family
-
date post
19-Dec-2015 -
Category
Documents
-
view
215 -
download
2
Transcript of Nursing Care of the Low-Risk Postpartum Family. Clinical Assessment Review antepartum and...

Nursing Care of the Low-RiskPostpartum Family

Clinical Assessment
• Review antepartum and intrapartum histories• Receive report from labor room personnel • Client may want to review birth experience• Education• Consider religious and cultural factors• Assess language barriers

Physical Assessment
• Vital signs• Breasts• Uterus, level of fundus• Amount and type of lochia• Uterine pain• Bladder

Physical Assessment (continued)
• Bowels, hemorrhoids• Episiotomy• Extremities• Emotional status

Postpartum Assessment
• B – Breasts• U – Uterus• B – Bowel• B – Bladder• L – Lochia• E – Episiotomy/Lacerations

Postpartum Assessment (continued)
• H – Homans’/Hemorrhoids• E – Emotions

Distended Bladder Postpartum

Uterine Involution

Figure 34–1 Involution of the uterus. (A) Immediately after delivery of the placenta, the top of the fundus is in the midline and approximately two thirds to three-fourths of the way between the symphysis pubis and the umbilicus (B). About 6 to 12 hours after birth, the fundus is at the level of (or one fingerbreadth below) the umbilicus. The height of the fundus then decreases about one fingerbreadth (approximately 1 cm) each day.

Other Assessments
• Hemodynamic status– WBC, H&H, coagulation factors
• Integumentary system– Striae, perspiration, acne, hair loss
• Musculoskeletal system– Diastasis
• Activity, exercise, and weight loss• Sexuality and contraception
Postpartum Changes in Lab Values
• Nonpathologic leukocytosis occurs in the early postpartum period
• Blood loss averages 200-500 mL (vaginal), 700-1000 mL (cesarean)
• Plasma levels reach the prepregnant state by 4-6 weeks postpartum
• Platelet levels will return to normal by the 6th week• Diuresis• Cardiac output returns to normal by 6-12 weeks

Immunizations
• Rubella– Rubella nonimmune clients– Safe for nursing mothers– Transient rash, fever, joint symptoms
• Rho(D) immune globulin– Mother Rh negative, infant Rh positive– Negative Coombs’ test– 300 mcg IM within 72 hours of delivery– Card issued to client
Family Considerations
• Maternal-infant attachment
• Maternal adjustment and role attainment– Taking-in phase– Taking-hold phase– Letting-go phase
• Paternal adjustment• Sibling adjustment• Grandparent adjustment

Postpartum Uterine Changes
• Decrease in weight 100g • Spongy layer of the decidua is sloughed off• Basal layer differentiates into two layers – Outer layer sloughs off – Inner layer begins the foundation for the new
endometrium• Placental site heals by exfoliation
Postpartum Uterine Changes (continued)
• Uterine cells will atrophy• Uterine debris in the uterus is discharged
through lochia– Lochia rubra is red (first 2-3 days) – Lochia serosa is pink (day 3 to day 10)– Lochia alba is white (continues until the cervix is
closed)

Factors Retarding Involution

Postpartal High-Risk Factors
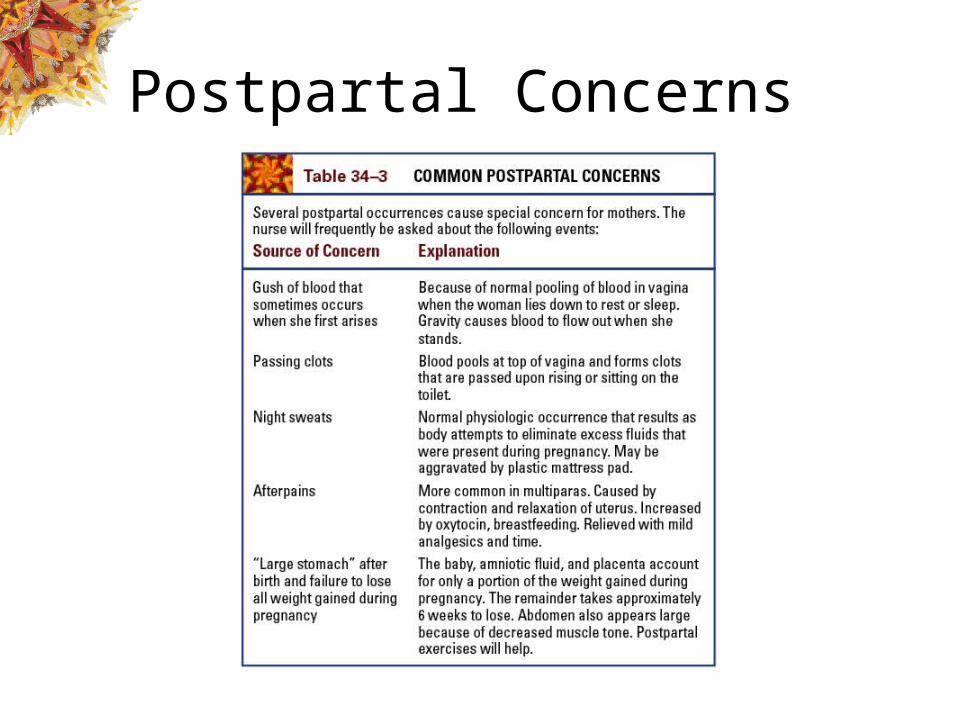
Postpartal Concerns

Lochia Rubra
Scant amount
Large amount with clots
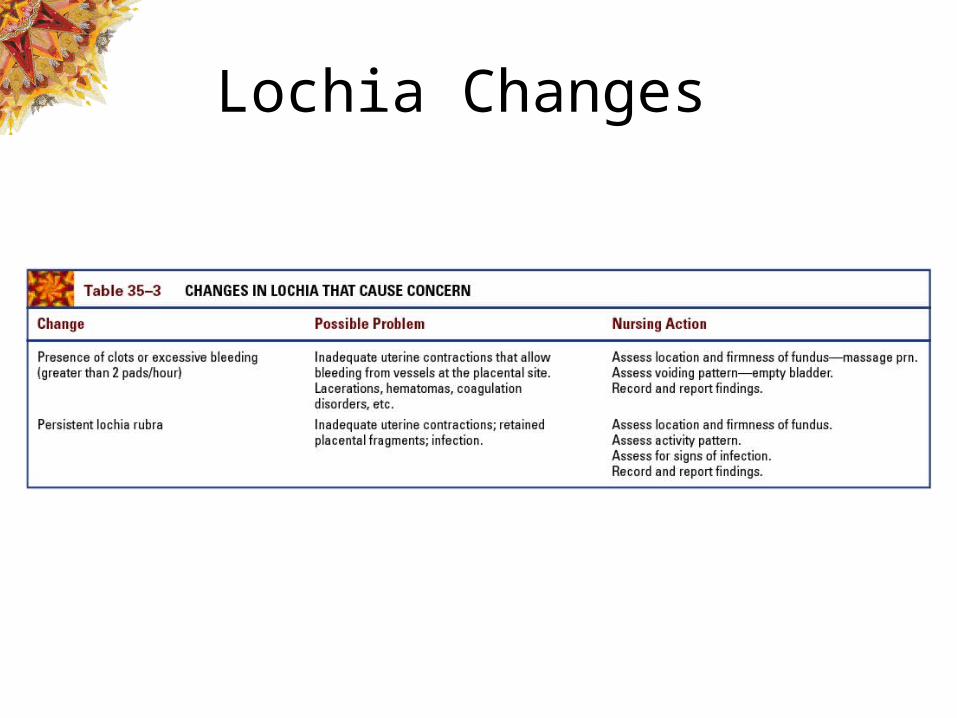
Lochia Changes

Postpartum Cervical and Vaginal Changes
• Cervix is spongy, flabby, and may appeared bruised• External os may have lacerations and is irregular and
closes slowly• Shape of the external os changes to a lateral slit• Vagina may be edematous, bruised with small
superficial lacerations• Size decreases and rugae reappear within 3-4 weeks• Returns to prepregnant state by 6 weeks

Perineal Changes and Return of Menstruation
• Perineum may be edematous, with bruising• Lacerations or an episiotomy may be present• Menstruation generally returns between 6 and
10 weeks (nonbreastfeeding)

Postpartum Abdominal and Breast Changes
• Loose and flabby but will respond to exercise • Uterine ligaments will gradually return to their
prepregnant state• Diastasis recti abdominis• Striae will take on different colors based on
the mother’s skin color • Breasts are ready for lactation

Figure 34–3 Diastasis recti abdominis, a separation of the musculature, commonly occurs after pregnancy.

Postpartum Bowel Changes
• Bowels will be sluggish • Episiotomy, lacerations, or hemorrhoids may
delay elimination

Postpartum Bladder Changes
• Increased bladder capacity• Swelling and bruising of tissues around the
urethra• Decrease in sensitivity to fluid pressure• Decrease in sensation of bladder filling • Urinary output is greater due to puerperal
diuresis• Increased chance of infection due to dilated
ureters and renal pelves

Postpartum Changes in Vital Signs
• Temperature may be elevated to 38C for up to 24 hours after birth
• Temperature may be increased for 24 hours after the milk comes in
• BP rises early and then returns to normal• Bradycardia occurs during first 6-10 days

Postpartum Weight Changes
• Initial weight loss of 10-12 lbs• Postpartum diuresis causes a loss of 5 lbs• Return to their prepregnant weight by the 6th
to 8th week

Postpartal Nutrition

Maternal Psychological Adjustment
• “Taking In”• “Taking Hold”
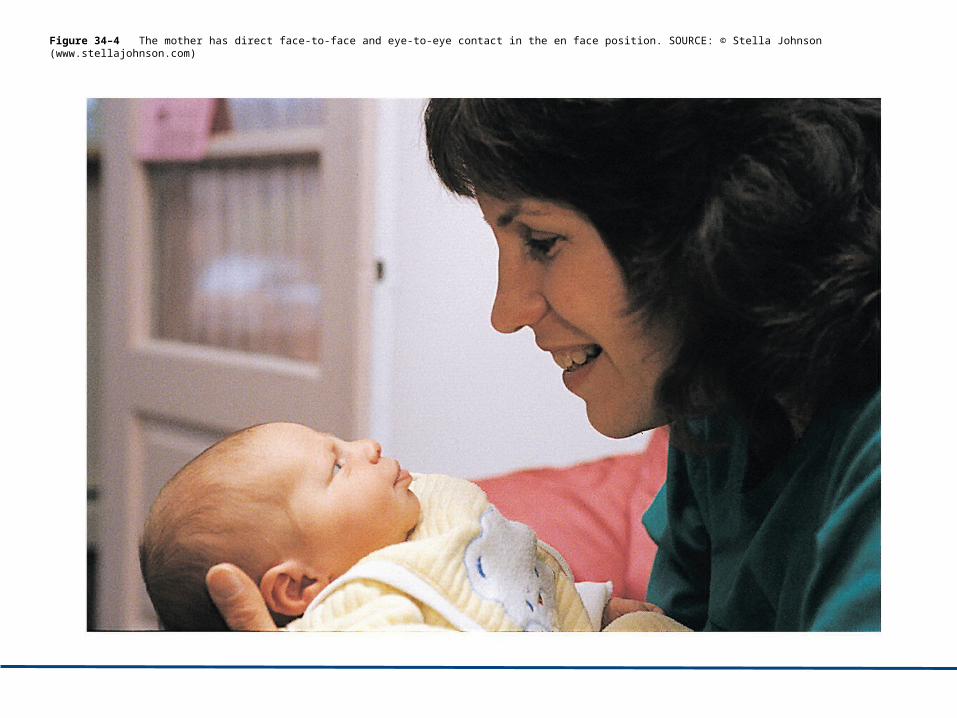
Figure 34–4 The mother has direct face-to-face and eye-to-eye contact in the en face position. SOURCE: © Stella Johnson (www.stellajohnson.com)

Maternal Role Attainment
• Anticipatory stage• Formal stage• Informal stage• Personal stage

Postpartum Blues
• Transient periods of depression; sometimes occurs during the first few days postpartum– Mood swings – Anger– Weepiness– Anorexia– Difficulty sleeping– Feeling let down

Causes of Postpartum Blues
• Changing hormones• Lack of supportive enviornment

Cultural Influence in the Postpartum Period
• Non-Western cultures emphasize postpartum period
• Food and liquids after birth• Hot-cold balance• Role of grandmother

Principles of Conducting a Postpartum Assessment
• Selecting the time that will provide the most accurate data
• Providing an explanation of the purpose of the assessment
• Ensuring that the woman is relaxed before starting
• Recording and reporting the results clearly • Body fluid precautions

Breast Assessment
• Size and shape• Abnormalities, reddened areas, or
engorgement• Presence of breast fullness due to milk
presence• Assess nipples for cracks, fissures, soreness, or
inversion

Abdominal Assessment
• Position of fundus related to umbilicus• Position of fundus to midline• Firmness• Assess incision for bleeding, approximation,
and signs of infection

Figure 34–6 Measuring the descent of the fundus for the woman having a vaginal birth. The fundus is located two fingerbreadths below the umbilicus. Always support the bottom of uterus during any assessment of fundus.

Figure 34–2 The uterus becomes displaced and deviated to the right when the bladder is full.

Assessment of Lochia and Perineum
• Assess lochia for amount, color, and odor• Presence of any clots • Wound is assessed for approximation,
redness, edema, ecchymosis, and discharge• Presence of hemorrhoids• Level of comfort/discomfort • Efficacy of any comfort measures

Figure 34–8 Intact perineum with hemorrhoids.

Assessment of Extremities, Bowel, and Bladder
• Homan’s sign• Assess calf for redness and warmth • Adequacy of urinary elimination• Bladder distention and pain during urination• Intestinal elimination • Maternal concerns regarding bowel
movements

Assessment of Psychological Adaptation and Nutrition
• Adaptation to motherhood • Fatigue• Nutritional status• Cesarean birth– Return of bowel function– Tolerance of dietary progression

Physical and Developmental Tasks
• Gain competence in caregiving• Confidence is role as parent• Return of all physical systems to prepregnant
state

Factors that Influence Parent-Infant Attachment
• Family of origin• Relationships• Stability of the home environment• Communication patterns• The degree of nurturing the parents received
as children

Nursing Responsibilities for Client Teaching
• Assess educational needs• Develop and implement a teaching plan• Evaluate client learning• Revise plan as needed

Postpartal Teaching

Postpartal Teaching

Postpartal Teaching

Postpartal Teaching

Postpartal Teaching

Postpartal Teaching

Postpartal Uterine Monitoring

Postpartum Drugs

Postpartum Drugs
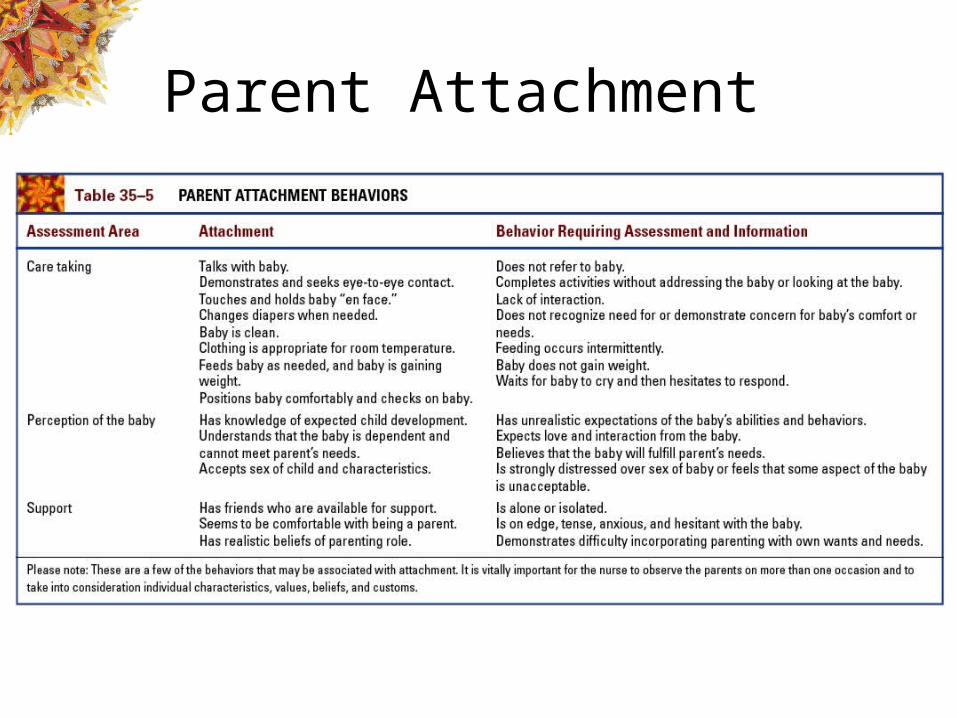
Parent Attachment

Uterine Well-Being and Comfort Measures
• Assess uterus• Assess lochia• Afterpains– Positioning– Ambulation– Analgesics

Perineal Well-Being and Comfort Measures
• Assess perineum• Perineal care• Ice packs• Surgigator®• Analgesics

Comfort Measures
• Diaphoresis• Suppression of lactation– Well-fitting bra– Cold compresses or cabbage leaves– Anti-inflammatory medication

Pharmacologic Interventions
• Rubella vaccine• RhoGAM

Emotional Stress Interventions
• Encourage mothers to tell birth stories• Maternal role attainment

Rest and Activity
• Provide opportunities for rest• Encourage frequent rest periods• Resumption of activity– Avoid heavy lifting– Avoid frequent stair climbing– Avoid strenuous activity

Postpartal Family Wellness
• Family-centered care• Information• Time for interaction• Supportive environment

Figure 35–3 The nurse provides discharge instructions to the mother and father before discharge.

Resumption of Sexual Activity
• Resume after episiotomy healed and lochia stopped
• Lubrication may be required• Contraception• Potential limiting factors– Fatigue– Demands of the infant

Parent-Infant Attachment
• Incorporate family goals in care plan• Postpone eye prophylaxis for 1 hour after
delivery • Provide private time for the family to become
acquainted• Encourage skin-to-skin contact• Encourage mother to tell her birth story

Parent-Infant Attachment
• Encourage involvement of the sibling• Prepare parents for potential problems with
adjustment• Initiate and support measures to minimize
fatigue • Help parents identify, understand, and accept
feelings

Care of the Mother after Cesarean Birth
• Minimize complications– Deep breathing and incentive spirometry– Ambulation– Pain management
• Rest• Minimize gas pains

Pharmacologic Management of Pain
• Epidural analgesia• PCA

Needs after Discharge
• Increased need for rest and sleep• Incisional care• Assistance with household chores• Infant and self-care• Relief of pain and discomfort

Parent-Infant Attachment
• Factors that hinder attachment– Physical condition of the mother and the newborn– Maternal reactions to stress– Anesthesia– Medications
• Newborn safety

Nursing Care of the Adolescent
• Postpartum hygiene• Contraceptive counseling• Newborn care• Include family in teaching• Positive feedback

Post-discharge Adolescent Needs
• Child care • Transportation • Financial support• Nonjudgmental emotional support• Education regarding newborn care and illness• Education regarding self-care
Care of the Mother who Relinquishes her Infant
• Active listening• Provide nonjudgmental support• Show concern and compassion• Personalize care for the mother

Early Discharge
• Signs of possible complications• Rest and activity• Resumption of sexual activity• Referral numbers for questions• Contact information about local agencies or
support groups• Bottle or breastfeeding information

Early Discharge (continued)
• A scheduled postpartal and newborn well-baby visit
• Procedure for obtaining the birth certificate• Newborn care• Signs and symptoms of infant complications

Lactation and Newborn Nutrition

American Academy of Pediatrics Recommendations
• Newborns should be nursed when they show signs of hunger
• No supplements should be given unless there is a medical indication
• Exclusive breastfeeding is sufficient for approximately six months

American Academy of Pediatrics Recommendations (continued)
• Gradual introduction of iron-rich solids should begin after six months
• Breastfeeding should continue for at least 12 months

Nutrients in Breast Milk
• Protein– Source of amino acids for growth– Whey fraction more easily digested and promotes
gastric emptying• Fat– Greatest concentration in hind milk– Necessary for brain development
• Carbohydrates– Enhance immunity and brain development

Nutrients in Breast Milk (continued)
• Water and electrolytes• Minerals• Trace elements• Fat-soluble and water-soluble vitamins

Anatomy of the Breast
Pectoralis major muscle
Lobes(glandular tissue)
Adipose tissue
Cooper’s ligament
Areola
Nipple
Lactiferous duct
Opening of lactiferous duct
Clavicle
Ribs
Areola
Nipple

Lactogenesis
• Estrogen and progesterone levels fall• Prolactin triggers
milk production• Oxytocin elicits the
let-down reflex• Milk production depends
on supply and demand– Feed often (every two to three hours)– Avoid supplements– Encourage night feedings

Interferences with Lactation
• Poor nutrition, inadequate fluid intake
• Maternal anxiety• Medical conditions• Pendulous breasts• Flat or inverted nipples• Postoperative pain• Deficient knowledge

Promoting Successful Breastfeeding
• Maternal comfort and relaxation• Positioning of mother and infant• Correct latching on of the infant• Removal of the infant from the breast• Burping

Promoting Successful Breastfeeding (continued)
• Timing– Feed immediately after delivery if possible– Offer both breasts at each feeding– 15 minutes on each breast– Offer the breast every two to three hours

Positioning for Breastfeeding

Techniques for Successful Breastfeeding
Breaking suction
Rooting reflex
Proper latching-on technique

Benefits of Breastfeeding
• Maternal benefits– Contraception– Less anemia– Weight loss– Involution of the uterus– Prevention against breast and ovarian cancer

Benefits of Breastfeeding (continued)
• Infant benefits– Bonding between mother/infant– Optimal nutrition – Prevention against infection– Enhanced cognitive development– Prevention against disease (diabetes, SIDS,
asthma)

Nursing Implications: Barriers to Successful Breastfeeding
• Maternal barriers– Diet, medications, smoking, fatigue– Prior breast surgery– Nipple abnormalities– Contraceptives– Psychologic issues, modesty
• Infant barriers– Prematurity– Illness and disability– Hypoglycemia– Jaundice
Nipple shields
Breastfeeding the preterm infant

Assessment forInsufficient Lactation
• Low urination pattern• Low stooling frequency• Minimal breast changes after delivery• Irritable or sleepy infant• Nursing less than seven times a day• Weight loss of more than 10% of the birth
weight• Continued weight loss after day 10 of life

Contraindications to Breastfeeding
• Maternal disease– Hepatitis B, C– HIV
• Maternal medications• Infant– Severe illness– Inborn errors of metabolism

Common Breastfeeding Problems
• Cracked or sore nipples– Change positions– Assess for proper latching on– Apply breast milk after nursing – Cabbage leaves, tea bags
• Mastitis– Antibiotics

Common Breastfeeding Problems (continued)
• Engorgement– Feed frequently, avoid supplements– Good support bra– Apply warmth (towels, shower) before nursing

Breast Pumps

Resources for Breastfeeding Mothers
• Lactation consultants• La Leche League• International
Lactation Consultant Association

Formula Feeding
• Available in powder, concentrate, ready-to-feed forms– Ensure that parents know how to mix formula– Ensure cleanliness in preparation
• Cow- or soy-based preparations• Monitor for food allergy symptoms– Rash, colic, diarrhea, bloody stool, respiratory
symptoms

Formula Feeding (continued)
• Solids usually introduced at about four months– One new food at a time– Wait at least three days between new foods


















