
Nursing Care of Clients Experiencing Pain. Pain Pathway A-delta fibers: transmit pain quickly,...
66
Nursing Care of Clients Experiencing Pain
-
Upload
janel-benson -
Category
Documents
-
view
216 -
download
1
Transcript of Nursing Care of Clients Experiencing Pain. Pain Pathway A-delta fibers: transmit pain quickly,...

Nursing Care of Clients Experiencing
Pain

Pain Pathway • A-delta fibers: transmit pain quickly, associated with
acute pain• C-fibers: transmit pain more slowly, diffuse burning
pain and chronic pain• Inhibitory mechanisms: the analgesia system
stimulates a pain inhibitory center in the dorsal horns of the spinal cord (the exact mechanism is unknown)
• Endorphins: naturally occurring opioid peptides present in the neurons in the brain

Pain Pathway

Pain Pathway

Four Processes Involved in Nociception
• Transduction• Transmission• Perception• Modulation

Transmission of Pain

Gate Control Theory • Small diameter (a-delta or C) peripheral nerve fibers carry
signals of noxious stimuli to the dorsal horn• Signals are modified when they are exposed to the substantia
gelatinosa • Ion channels on the pre- and postsynaptic membranes serve
as gates• When open, permit positively charged ions to rush into the
second order neurons, sparking an electrical impulse and sending signals of pain to the thalamus
• Large diameter (A-delta) fibers have inhibitor effect• May activate descending mechanism that can inhibit
transmission of pain

Gate Control Theory

Clinical Application ofGate Control Theory
• Stop nociceptor firing • Apply topical therapies • Address client’s mood • Address client’s goals

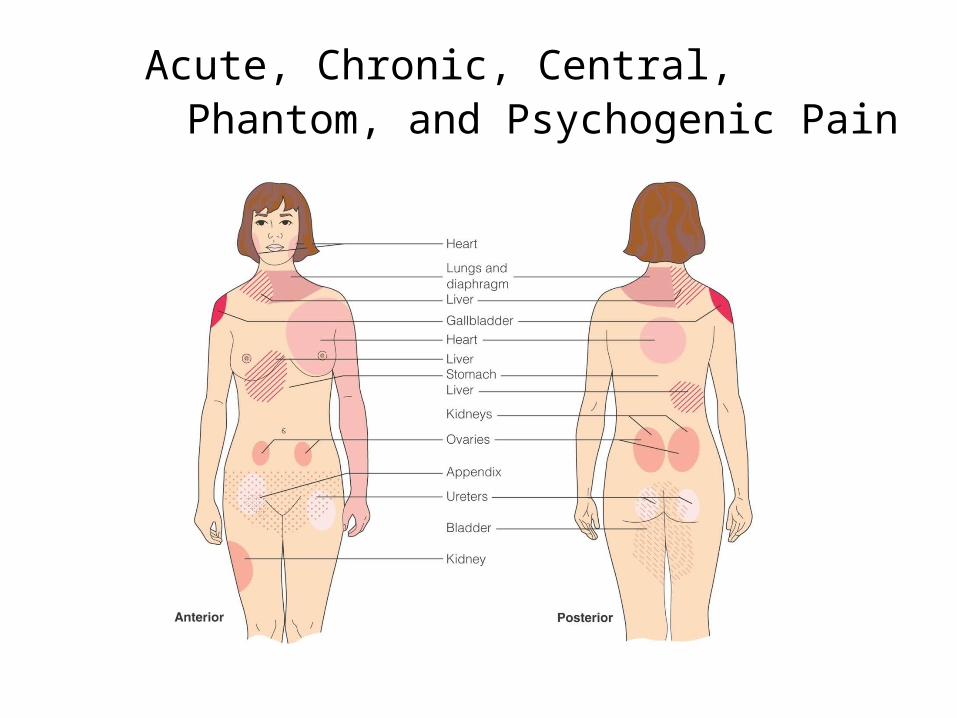
Acute, Chronic, Central, Phantom, and Psychogenic Pain
• Acute Pain– Somatic Pain
• May be sharp or diffused• May be accompanied by nausea and vomiting
– Visceral Pain• Arises from the body organs• Usually dull and poorly localized• May be referred or may radiate
– Referred Pain• Perceived in an area distant from the site of the stimuli
Acute, Chronic, Central, Phantom, and Psychogenic Pain

Acute, Chronic, Central, Phantom, and Psychogenic Pain
• Chronic Pain– Recurrent Acute Pain• Well-defined episodes of pain• Migraine headaches, sickle cell crisis
– Ongoing Time-limited Pain• Persists for a definite time period• Ends with control of the disease, rehabilitation, or
death

Acute, Chronic, Central, Phantom, and Psychogenic Pain
• Chronic Pain– Chronic Nonmalignant Pain• Not life-threatening but persists past expected time for
healing
– Chronic Intractable Nonmalignant Pain Syndrome• Client unable to cope well with the pain• Pain may be mild to severe• The pain itself becomes the pathologic process
Acute, Chronic, Central, Phantom, and Psychogenic Pain
• Central Pain– May be caused by a vascular lesion, tumor, or
inflammation
• Phantom Pain– Thought to be due to stimulation of severed nerves at the
amputation site
• Psychogenic Pain– Involves a long history of severe pain– The pain is real and can lead to physiologic changes

Factors Affecting Pain Response
• Age• Sociocultural influences• Emotional status • Past experiences with pain• Meaning associated with the pain • Lack of knowledge

Myths and Misconceptions Concerning Pain
• Pain is a result, not a cause• Chronic pain is really a masked form of depression• Narcotic medication is too risky to be used for
chronic pain• It is best to wait until a client has pain before giving
medication• Many client’s lie about the existence or severity of
pain• Pain relief interferes with diagnosis

Pain AssessmentSubjective Data
• Comprehensive pain history includes COLDERR– Character– Onset– Location– Duration– Exacerbation– Relief– Radiation

Additional Data to Obtain
• Associated symptoms• Effect on ADLs• Past pain experiences• Meaning of the pain to the person• Coping resources• Affective response

Nursing Process for Clients with Pain

Pain AssessmentObjective Data
• Nonverbal responses to pain– Facial expression– Vocalizations like moaning and groaning or crying
and screaming– Immobilization of the body or body part– Purposeless body movements– Behavioral changes such as confusion and
restlessness– Rhythmic body movements or rubbing

Pain AssessmentObjective Data
• Early physiologic responses– Increases BP, HR, RR– Pallor– Diaphoresis– Pupil dilation – May be absent in people with chronic pain
• Pain diary

NANDA Nursing Diagnoses
• Acute Pain and Chronic Pain• Specify the location• Related factors, when known, can include
physiologic and psychologic factors • Pain may be etiology of other nursing
diagnoses

NANDA Nursing Diagnoses
• Pain as etiology of other nursing diagnoses– Ineffective Airway Clearance– Hopelessness– Anxiety– Ineffective Coping– Ineffective Health Maintenance– Self-Care Deficit (Specify)– Deficient Knowledge (Pain Control Measures)– Disturbed Sleep Patterns
Nursing Process for Clients with Pain
• Assess the client’s pain level• Establish a nursing diagnosis • Plan and implement a care plan• Educate the client• Evaluate the patient’s response to the care
plan

Treatment Plan
• Goals vary according to the diagnosis and its defining characteristics
• Select pain relief measures appropriate for the client, based on assessment data and input from the client or support persons

Practice Guidelines
• Establish a trusting relationship• Consider client’s ability and willingness to
participate• Use a variety of pain relief measures• Provide pain relief before pain is severe• Use pain relief measures the client believe are
effective• Align pain relief measures with report of pain
severity

Practice Guidelines
• Encourage client to try ineffective measures again before abandoning
• Maintain unbiased attitude about what may relieve pain
• Keep trying• Prevent harm• Educate client and caregiver about pain

Pain Treatment Plan
• Include variety of pharmacologic and nonpharmacologic interventions
• Plan with wide range of strategies • Document plan in client record and for home
care• Involve client and support persons

Barriers to Effective Pain Management
• Lack of knowledge of the adverse effects of pain
• Misinformation regarding the use of analgesics
• Misconceptions about pain• May not report pain • Fear of becoming addicted
Addiction
• Primary, chronic, neurobiologic disease• Genetic, psychosocial, and environment are
influential factors• Behaviors can include:– Impaired control over drug use– Compulsive use– Craving– Continued use despite harm

Dependence
• State of adaptation• Manifested by withdrawal syndrome • Produced by abrupt cessation, rapid dose
reduction, decreasing blood level of the drug, and/or administration of an antagonist
Tolerance
• State of adaptation• Exposure to a drug induces changes• Result in a diminution of one or more of the
drug’s effects over time

Pharmacologic Interventions for Pain
• Opioids (narcotics)• Nonopioids/nonsteroidal anti-inflammatory
drugs (NSAIDS)• Co-analgesic drugs
Opioids (Narcotics)
• Full agonists– No ceiling on analgesia– Dosage can be steadily increased to relieve pain– E.g., morphine, oxycodone, hydromorphone

Opioids (Narcotics)
• Mixed agonist-antagonists– Act like opioids and relieve pain– Can block or inactivate other opioid analgesics– E.g. dezocine, petazocine hydrochloride,
butorphanol tartrate, nalbuphine hydrochloride• Partial agonist– Have a ceiling effect– E.g., buprenorphine

Nonopioids/NSAIDS
• Vary little in analgesic potency but do vary in anti-inflammatory effects, metabolism, excretions, and side effects
• Have a ceiling effect• Narrow therapeutic index• E.g. acetaminophen, ibuprofen, aspirin

Coanalgesic Drugs
• Antidepressants• Anticonvulsants• Local anesthetics• Others

WHO Ladder Step Approach for Cancer Pain Control

WHO Ladder Step Approach for Cancer Pain Control
• Step 1– For clients with mild pain (1-3 on a 0-10 scale)– Use of nonopioid analgesics (with or without a
coanalgesic)

WHO Ladder Step Approach
• Step 2– Client has mild pain that persists or increases – Pain is moderate (4-6 on a 0-10 scale) – Use of a weak opioid (e.g. Codeine, tramadol,
pentazocine) or a combination of opioid and nonopioid medicine (oxycodone with acetaminophen, hydrocodone with ibuprofen)
WHO Ladder Step Approach
• Step 3– Client has moderate pain that persists or increases– Pain is severe (7-10 on a 0-10 scale)– Strong opioids (e.g. Morphine, hydromorphone,
fentanyl)

Rational Polypharmacy
• Evolved from WHO three step approach• Demands health professionals be aware of all
ingredients of medications that alleviate pain • Use combinations to reduce the need for high doses
of any one medication• Maximize pain control with a minimum of side effects
or toxicity• Combined with multimodal therapy (e.g. nondrug
approaches)

Oral Administration
• Preferred because of ease of administration• Duration of action is often only 4 to 8 hours• Must awaken during night for medication• Long-acting preparations developed• May need rescue dose of immediate-release
medication

Transmucosa/Transnasal and Transdermal Administration
• Transmucosa and Transnasal– Enters blood immediately– Onset of action is rapid
• Transdermal – Delivers relatively stable plasma drug level– Noninvasive

Medication Administration
• Rectal– Useful for clients with dysphagia or
nausea/vomiting• Continuous subcutaneous infusion– Used for pain poorly controlled by oral
medications

Subcutaneous Infusion Placement

Medication Administration
• Intramuscular– Should be avoided– Variable absorption– Unpredictable onset of action and peak effect– Tissue damage
• Intravenous– Provides rapid and effective relief with few side
effects

Copyright 2008 by Pearson Education, Inc.
Medication Administration
• Intraspinal– Provides superior analgesia with less medication used

Benefits/Risk Routes and Technology
• Patient-controlled analgesia– Minimizes peaks of
sedation and valleys of pain that occur with prn dosing
– Electronic infusion pump– Safety mechanisms

Nonpharmacologic Pain Control Interventions
• Consists of variety of pain management strategies– Physical – Cognitive-behavioral– Lifestyle pain management
• Target body, mind, spirit, and social interactions

Physical Modalities
• Cutaneous stimulation• Immobilization or
therapeutic exercises• Transcutaneous
electrical nerve stimulation (TENS)

Cognitive-Behavioral(Mind-Body)
• Providing comfort• Eliciting relaxation
response• Repatterning thinking• Facilitating coping with
emotions

Lifestyle Management
• Stress management• Exercise, nutrition• Pacing activities• Disability management

Spiritual
• Feel part of a community• Bond with universe• Religious activities

Nonpharmacologic Invasive Techniques
• Cordotomy• Rhizotomy• Neurotomy• Sympathectomy• Spinal cord stimulation

Collaborative Care for Pain
• Surgery– Cordotomy: an incision into the anterolateral tracts of the
spinal cord to interrupt the transmission of pain– Neurectomy: removal of part of the nerve– Sympathectomy: destruction of the ganglia by incision or
injection– Rhizotomy: surgical severing of the dorsal spinal roots– Transcutaneous electrical nerve stimulation (TENS):
electrodes stimulate the A-beta touch fibers to close the “pain” gate

Collaborative Care for Pain

Body Interventions• Reducing pain triggers• Massage• Applying heat or ice• Electric stimulation (TENS)• Positioning and bracing (selective immobilization)• Acupressure• Diet and nutritional supplements• Exercise and pacing activities• Invasive interventions (e.g. blocks)• Sleep hygiene

Mind Interventions
• Relaxation and imagery• Self-hypnosis• Pain diary and journal writing• Distracting attention• Re-pattern thinking• Attitude adjustment• Reducing fear, anxiety, stress, sadness, and
helplessness• Providing information about pain

Spirit Interventions
• Prayer• Meditation• Self-reflection• Meaningful rituals• Energy work (therapeutic touch, Reiki)• Spiritual healing

Social Interaction
• Functional restoration• Improved communication• Family therapy• Problem-solving• Vocational training• Volunteering• Support groups
Collaborative Care for Pain
• Medications – NSAIDs: analgesic, antipyretic, and anti-
inflammatory action– Narcotics: opioids– Antidepressants: act on the retention of serotonin,
thus inhibiting the pain sensation– Anticonvulsants: used for headache and
neuropathic pain– Local anesthetics: blocks the transmission of nerve
impulses, therefore blocking pain

Collaborative Care for Pain

Collaborative Care for Pain
• Complementary Therapies– Acupuncture– Biofeedback– Hypnotism– Relaxation– Distraction– Cutaneous stimulation
Neuropathic Pain
• Experienced by people who have damaged or malfunctioning nerves
• Types– Peripheral – Central – Sympathetically maintained
Physiologic Pain
• Experienced when an intact, properly functioning nervous system signals that tissues are damaged, requiring attention and proper care
• Transient • Persistent• Subcategories– Somatic – Visceral


















