
Nurses' experiences of caring for burn injured children in ...392093/FULLTEXT01.pdf ·...
33
Institutionen för folkhälso- och vårdvetenskap Enheten för vårdvetenskap Nurses' experiences of caring for burn injured children in pain. Author : Supervisor : Andrea Olsson Khadija Innocencia Yahaya-Malima Dr. Clara Aarts Examensarbete i Vårdvetenskap 15 hp Examinator : Sjuksköterskeprogrammet 180 hp Dr. Pranee Lundberg VT 2011
Transcript of Nurses' experiences of caring for burn injured children in ...392093/FULLTEXT01.pdf ·...
Institutionen för folkhälso- och vårdvetenskap
Enheten för vårdvetenskap
Nurses' experiences of
caring for burn injured children in pain.
Author: Supervisor:
Andrea Olsson Khadija Innocencia
Yahaya-Malima
Dr. Clara Aarts
Examensarbete i Vårdvetenskap 15 hp Examinator:
Sjuksköterskeprogrammet 180 hp Dr. Pranee Lundberg
VT 2011

Sammanfattning:
Syfte: Syftet med studien var att ta reda på sjusköterskors erfarenheter av att vårda barn
på brännskadeenheten med smärta under omläggningar och vilka förhållanden och
hinder de uttrycker för att utföra sitt jobb inom smärtlindring Metod: Åtta
sjuksköterskor intervjuades med semistrukturerade öppna frågor på brännskadeenheten
för barn i Dar es Salaam. Intervjuerna spelades in med diktafon, transkriberades och
analyserades genom innehålls manifest. Resultat: Tre kategorier framkom genom
analysen, smärtskattning, smärtlindringsmetod och faktisk smärtbehandling.
Sjuksköterskorna uttryckte att smärtlindringsmetoderna och smärtskattningen de utför
fungerade utan anmärkning. De uttryckte att smärtskattningen fungerade som en
indikator på hur de brännskadade barnen uppförde sig och hur de påverkades under
dagliga omläggningar av sina brännskador. Resultaten från observationsstudien visade
att det inte fanns någon specifikt smärtskattningsinstrument som sjuksköterskorna
använde sig av, mera än ett kliniskt begrundande och erfarenhetsmässigt konstaterande
att barnen var smärtpåverkade under aktuell omläggning. Smärtbehandlingen som
användes mest frekvent var Panodil och sjuksköterskorna uttryckte sina rädslor för att
barnen skulle utveckla beroende till opiater om det användes i för stor utsträckning.
Slutsats: Smärtlindring är ett ämne som visar att sjuksköterskor som jobbar inom
området med brännskadade barn har goda kunskaper av smärtlindring. Däremot är det
rutinmässigt standardiserande av utsträckt smärtbehandling ett område som måste
belysas.
Nyckelord: omvårdnads erfarenheter, sjuksköterskor, brännskadade barn, smärta, Tanzania.

Abstract:
Aim: To illuminate how nurses working with burn injured children describe their
care for burn injured children in pain during dressing procedures and which
conditions and obstacles nurses express they are working under in order to proceed
with giving care. Method: Semi-structured qualitative interviews with eight nurses at
a pediatric burn ward in Dar es Salaam. Interviews were recorded, transcribed and
processed by manifest content analysis. Result: Three themes were derived and
identified as, pain assessment, pain management and pain treatment. Nurses
experienced the pain management as satisfactory and expressed pain assessment as
indication to how the burn injured children behaved and were affected upon daily
dressing of burn wounds. Results also showed from observations that there is no
specific pain assessment tool being used at the ward, more than the nurse’s clinical
eye and work experience at the dressing occasion. The main pain treatment used at
the ward was Panadol and nurses described their fear of children becoming tolerant
to opiates as reason why Panadol being used so extensively. Conclusion: This is a
topic that shows that nurses in dealing with pediatric burn injured patients have good
skills in pain management. However the routine use of pain treatment during
dressings as an extensive standard treatment needs to be illuminated.
Keywords: experience of caring, nurses, burn injured children, pain, Tanzania.
CONTENTS:
1. INTRODUCTION .............................................................................................................................. 5
1.1 Burn injuries in Tanzania ............................................................................................................... 5
1.2 Trauma of being burn injured ......................................................................................................... 6
1.3 Dressing of burn wounds ................................................................................................................ 6
1.4 Pain assessment ............................................................................................................................... 7
1.5 Pain management ............................................................................................................................ 7
1.6 Problem area ................................................................................................................................... 8
1.7 Aim of study ................................................................................................................................... 8
2. METHOD Burn injury background ................................................................................................. 9
2.1 Design ............................................................................................................................................ 9
2.2 Selection ......................................................................................................................................... 9
2.3 Data collection method ................................................................................................................... 9
2.4 Procedure ...................................................................................................................................... 10
2.5 Analysis ......................................................................................................................................... 10
2.6 Ethical consideration ..................................................................................................................... 12
3. RESULTS ...................................................................................................................................... 12
3.1 Pain assessment ............................................................................................................................. 14
3.2 Pain management .......................................................................................................................... 15
3.3 Pain treatment ............................................................................................................................... 16
3.4 Extent of burn injury and pain treatment prior to dressing of burn from observation .................. 17
4. DISCUSSION ................................................................................................................................ 18
4.1 Summary of results ....................................................................................................................... 18
4.2 Result discussion ........................................................................................................................... 18
4.3 Method discussion ......................................................................................................................... 20
4.4 Conclusion ................................................................................................................................... 22
5. REFERENCES................................................................................................................................ 22
APPENDIX I. INTERVIEW GUIDE ................................................................................................ 26
APPENDIX II. OBSERVATION GUIDE .......................................................................................... 27
APPENDIX III. LETTER OF CONSENT .......................................................................................... 28
5
INTRODUCTION:
1.1 Burn injuries in Tanzania
This thesis and the minor field study have been conducted in a hospital in Dar es
Salaam, Tanzania where large numbers of burn injured children are admitted to
hospitals in each year (Mbembati, Museru and Leshabari, 1999). Burn injured
children are a common patient category in Tanzanian hospitals due to the extent of
open fire cooking, along with the lack of preventative measures taken to keep burn
injuries at low numbers. Other reasons for children being admitted in hospitals
researchers from Tanzania found is because of the mentality of parents which is an
initial problem as to why children get burn injured. Over 50% of parents
participating in a study from Dar es Salaam hospitals have the idea that it is difficult
to control children and that accidents are unpreventable (Mbembati, Museru and
Leshabari, 1999). However there is evidence that parents suffer from feelings of
guilt, depression or post traumatic stress syndrome along with their child sustaining
burn injuries (Jansson and Gustavsson, 2005). Children under the age of three are the
most frequent age group of burn injured children where as older children are more
prone to have larger extents of their burn injuries supporting the fact that child safety
and prevention is needed (Serour, Gorenstein, and Boaz, 2008). Burn injured
children being admitted to pediatric burn wards need to be attended to accordingly
and ensured they get appropriate quality care for the time being hospitalized to
minimize future problems. There is more burn-prevention work to be developed
specifically for households with young children as children under six years still
sustain largely disproportional injuries (D’Souza, Nicholas, Nelson and McKenzie,
2009).
Problems related in burn injured children include post traumatic stress syndrome
(PTSD), burn injury dressing, infections related to burn injuries along with sufficient
or appropriate pain management where pain assessment is included.

6
1.2 Trauma and being burn injured
Symptoms of trauma have been recognized in pre-school children together with
physiological reactivity. Children admitted to pediatric burn injury unit’s
demonstrated there was a relation between the smiles and vocalization frequency,
how much the children spoke and laughed after the burn injury. One of the measures
was by heart rate at 24 hours, after seven days and one month after the injury. The
higher the heart rate was at the time of measure the less the spontaneous smiles were.
The pain rating the child him or she did at 24 hours resulted in decreased frequency
in vocalization at one month post hospitalization (Stoddard et al., 2006). Pathways of
how the children’s symptoms of PTSD were expressed. One pathway concerned the
size of the burn together with the level of pain related to the burn along with a child’s
level of acute anxiety due to separation followed by the PTSD. Making the size of
the burn, level of pain estimated from the burn, related to the child’s level of acute
separation anxiety to PTSD. A second pathway showed the relation between burn
size and a child’s own measured level of acute dissociation at three months following
the burn to PTSD (Saxe et al., 2005).
1.3 Dressing of burn wounds
Children who have been admitted to hospitals often suffer from infections related to
their burn wounds and skin damage. Infections are a problem that can cause longer
hospitalization due to staphylococcus aureus and pseudomonas amongst other skin
organism that is commonly found contaminating granulation of burn wounds
(Hackett, 1971). This is a topic which is debated and there are many ways to carry
out dressing of burn wounds. When speaking of dressings the term itself covers
many treatments and can be sorted into categories: on admission, later treatment and
other procedures. Specifically these categories include everything from removal of
clothing, canulation for intravenous fluids, catheterization on admission to re-
dressing of burnt area, change of catheter in later treatment and cleaning of infected
areas for preparation for reception of upcoming skin grafts (Davies, 1971). To
prevent infections and long term scaring related to burn injuries the use of amnion
from new born children has been proved to have anti-inflammatory characteristics
7
and the need for antibiotics can be reduced (Ley-Chavez, Martines-Pardo, Roman,
Oliveros-Lonzano, and Canchola-Martines, 2003).
1.4 Pain assessment
Another aspect of suffering a burn injury is the pain experience and pain
management needed. Pain in a most subjective experience and when dealing with
children there are different skills to apply that differ from those used in adults when
performing pain assessment and pain management. Pain assessment for pediatric
patients can be carried out using different methods. Scales which are commonly used
when pain assessing pediatric patients are faces pain scales (FPS) where the primal
face of pain (PFP) offers explanation to the use and deficiency of face pain scales
and the face, leg, activity, cry, consolability scale (FLACC) (Schiavento, 2007). The
validity of these scales has been evaluated in different studies. Facial expressions of
a child when pain assessing, is considered to be a determinant and a highly reliable
cue when measuring child’s experience of pain (Schiavenato, 2007). These scales are
considered to be easily comprehensive for children (Silva and Thuler, 2008). The
Visual Analogue Scale (VAS) as well as the Faces Rating Scale (FRS) is two other
pain assessment tools that can be used interchangeably for evaluating acute
postoperative pain which is relevant in the skin grafting procedure (Fadaizadeh,
Emami and Samii, 2009). One consideration of using faces pain scales is that of
cross-cultural aspects. The ethnic background and culture may encourage or
discourage facial expressions and facial phenotypes and hence recognizing faces of
pain differently (Newman, et al., 2005). It is also concluded that children who are
undergoing surgery or painful procedures wish to have for them, comprehensive
information about the procedure, anesthesia and pain together with the complications
they might have ahead of them (Fortier et al., 2009).
1.5 Pain management
There are a number of methods to pain manage children with burn injuries of
different degrees. The use of topic analgesia Lidocain-Prilocaine cream (LPC) has
been studied with positive results for pediatric burn victims with burn degrees of the
first to third degree (Kargi and Tekerekoglu, 2010). The use of opiates in general for
burn victims is highly thought of, as many burn injured patients need skin grafting or
8
other surgery the use of intravenous opiates are often use for pre-operation pain
management (Dadure, Acosta and Capdevila, 2004). Opiates are also used in
inflammatory pain which is a common state of burn victims (Watterson, Howard and
Goldman, 2004). Methoxyflurane is also used to pain manage children with burn
injuries especially in general terms for burn dressing (Packer, 1972). The person who
gives pain management is a topic rarely discussed but brings light on to how children
experience pain and how parents acknowledges their child in pain prior to going to
the hospital (Spedding, Harley, Dunn and McKinney, 1999). Methadone compared to
morphine has shown to be a good substitute when dealing with the morphine tolerant
pediatric patient and leading to lower doses of needed analgesia (Williams,
Sarginson and Ratcliffe, 1998).
1.6 Problem area
Research have shown that children, especially children up to five years old are more
frequently victims of burn injuries also suffer psychological aspects related to the
burn (Membati et al., 1999). Not only is the burn a physically painful trauma such as
the pain related to daily dressings as is the child exposed to post traumatic stress
syndromes (Stoddard et al., 2006). There is a need to pain manage the individual
who is suffering from burn injuries in a scientifically supported manner along with
the nurse´s different experiences of a child in pain. The study was conducted in
Tanzania as this is one of the countries in the world where these problems arise and
are more frequent. The nurses at a city hospital in Dar es Salaam, work alongside
these problems when dressing burn injuries on a daily basis at a pediatric burn ward.
1.7 Aim of the study
The aim of the study is to illuminate how nurses working with burn injured children
describe their work with burn injured children in pain and which conditions and
obstacles nurses express they are working under in order to manage children’s pain
from a holistic view.
9
2. METHOD
2.1 Design
The study is empirical and has a descriptive qualitative study design with semi-
structured interviews and observations. The design allows a phenomenon to be
studied and described in a matter that presents valuable reflections of individuals
(Polit, & Beck, 2008).
2.2 Sample
The sample group consisted of registered and enrolled nurses from the pediatric burn
ward at a hospital in Dar es Salaam, Tanzania. This ward is admitting children up to
the age of sixteen and treats all children with various burn degrees as well as patients
undergoing surgery such as skin grafting as a post-burn treatment. A selection
criterion for nurses to take part in the study was that they were enrolled or registered
nurses working in the ward for at least six months and English speaking. There were
approximately thirteen nurses both male and female working during the conduction
of the study. A number of ten nurses were requested to join and eight nurses were
included in the final interviews. The author limited herself to ten nurses considering
the interviews were transcribed by one relatively inexperienced person. The nurses
who did not consent to the study had reason of language skills and lack of
collaboration concerning work schedule and leave. The work experience variation of
the participating nurses varied from over one year to over ten years. All interviewed
nurses were female and the ages varied from 26 to 53 years of age.
2.3 Data collection method
Semi structured interviews were used. This method is commonly used and
considered to be revealing and to bring insight to what the individual experiences.
An interview guide (Appendix 2) was used in the field to bring background
information, experience of pain management and acknowledging the child in pain,
and work related problems with burn injured children on every day basis. The
10
interview guide was being based on the literature of interviewing methods and finally
established by the interviewer considering language differences and native spoken
language that might lead to misinterpretations (Dalen, 2008). The observation part of
the study took part during the daily dressing occasions of the children, following one
patient and nurse at the time prior to the interview. An observation guide to collect
background data (Appendix 1) was used to serve the purpose of recalling the type of
patient and the pain management scene. The observer used the FLACC-scale
(Schiavento, 2007) when observing the burn injured children undergoing dressings.
This scale is considered to be appropriate to use for objective measurements of pain
in children including children with cognitive impairment (Voepel-Lewis, Merkel,
Tait, Trzinka and Malviya, 2002).
2.4 Procedure
Before the study took place, permission had been granted by the ethical committee to
proceed with the study. The dean of school of nursing informed the head nurse at the
pediatric burn ward about the study. The head nurse of the pediatric burn ward
informed the nurses concerning the study. A letter of consent was handed out to all
nurses working in the pediatric burn ward stating all information in written version to
be signed if their wish was to partake in the study. A field study was undertaken by
the author prior to the interviews to get insight and understanding of the work and
management of the pediatric burn ward. The interview guide was tested prior to the
actual interview with one of the nurses to ensure its functionality as well as to test the
recording instrument being used. Data was collected on two consecutive days with a
number of four nurses per day. The interviews took place at the ward during the
nurse’s work hours in a secluded area to ensure privacy from fellow colleagues and
other hospital staff. Open ended questions were used and of a general matter. The
observation part of the study was based on ten patients, one for each nurse that was
first sought. Observations took place on the same day as the interviews were
conducted and took as long as the dressing of the child took which could vary in
time, pending on seize of each burn injury and level of healing process in the actual
burn injury being dressed. Observations were carried out prior to the interview with
the observer following the nurse in her daily routine and dressing of the children.

11
2.5 Analysis
Data was analyzed according to Qualitative content analysis in nursing research:
concepts, procedures and measures to achieve trustworthiness proposing qualitative
content analysis by using a manifest content analysis (Graneheim and Lundman,
2004). Through this type of manifest the text appears gradually whilst being worked
on. The text content proposed the informants different experiences. The parts of the
text which brought information in line with the aim of the study and questions asked
were taken out and constructed meaning bearing units being strictly quoted.
Condensed meaning units were used to shorten the text yet keep the substance of the
content. By abstracting the condensed meaning unit a code could be derived giving a
description of the meaning units’ content. Codes were then combined into sub-
themes and finally a theme. All steps of the content analysis was been done by the
author and over several weeks allowing reflection and consideration to various
interpretation possibilities and abstracting levels. To enable consensus the author
engaged a second colleague with more experience in the field to discuss the meaning,
interpretations and derived themes of the performed data analysis. Example of the
analyzing process is shown in table 1. Data gathered from the observations is shown
in table 3. This data was analyzed from the observation guide which was filled out by
the observer. This data shows the age, gender, percentage of burn, reason for burn
injury of the ten observed children together with the pain management used at the
occasion.
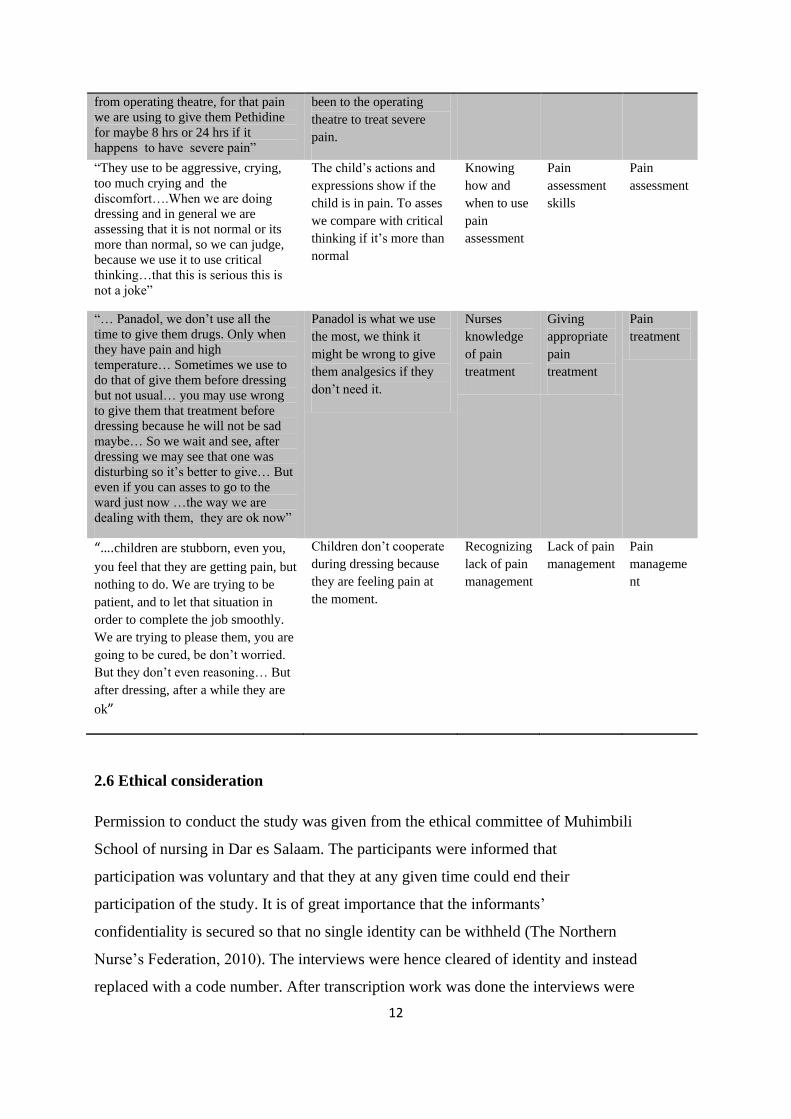
Table 1. Example of meaning units, condensed meaning units, sub-themes and
themes.
Meaning unit Condensed
meaning unit
Code Sub-theme Theme
“Sometimes it’s very difficult to
cope with these things…Because in
treating burn it takes very long
time…We don’t use to give
sedation…because we are afraid of
addiction. But after dressing we use
to give them analgesics like Panadol
and so forth. maybe when they come
It’s difficult to cope with
as treating burns take a
long time. We are afraid
of addiction so we don’t
use sedation. We give
Panadol after dressing or
Pethidine if they have
Difficulty in
finding
good pain
management
Appropriate
pain
management
Pain
manageme
nt
12
from operating theatre, for that pain
we are using to give them Pethidine
for maybe 8 hrs or 24 hrs if it
happens to have severe pain”
been to the operating
theatre to treat severe
pain.
“They use to be aggressive, crying,
too much crying and the
discomfort….When we are doing
dressing and in general we are
assessing that it is not normal or its
more than normal, so we can judge,
because we use it to use critical
thinking…that this is serious this is
not a joke”
The child’s actions and
expressions show if the
child is in pain. To asses
we compare with critical
thinking if it’s more than
normal
Knowing
how and
when to use
pain
assessment
Pain
assessment
skills
Pain
assessment
“… Panadol, we don’t use all the
time to give them drugs. Only when
they have pain and high
temperature… Sometimes we use to
do that of give them before dressing
but not usual… you may use wrong
to give them that treatment before
dressing because he will not be sad
maybe… So we wait and see, after
dressing we may see that one was
disturbing so it’s better to give… But
even if you can asses to go to the
ward just now …the way we are
dealing with them, they are ok now”
Panadol is what we use
the most, we think it
might be wrong to give
them analgesics if they
don’t need it.
Nurses
knowledge
of pain
treatment
Giving
appropriate
pain
treatment
Pain
treatment
“….children are stubborn, even you,
you feel that they are getting pain, but
nothing to do. We are trying to be
patient, and to let that situation in
order to complete the job smoothly.
We are trying to please them, you are
going to be cured, be don’t worried.
But they don’t even reasoning… But
after dressing, after a while they are
ok”
Children don’t cooperate
during dressing because
they are feeling pain at
the moment.
Recognizing
lack of pain
management
Lack of pain
management
Pain
manageme
nt
2.6 Ethical consideration
Permission to conduct the study was given from the ethical committee of Muhimbili
School of nursing in Dar es Salaam. The participants were informed that
participation was voluntary and that they at any given time could end their
participation of the study. It is of great importance that the informants’
confidentiality is secured so that no single identity can be withheld (The Northern
Nurse’s Federation, 2010). The interviews were hence cleared of identity and instead
replaced with a code number. After transcription work was done the interviews were
13
deleted. Observation demands respect of privacy and integrity of the patient. The
observer asked permission to stand by on dressing occasion from both nurse and
relative if being at the location. The children being observed were unnamed to secure
their identity.
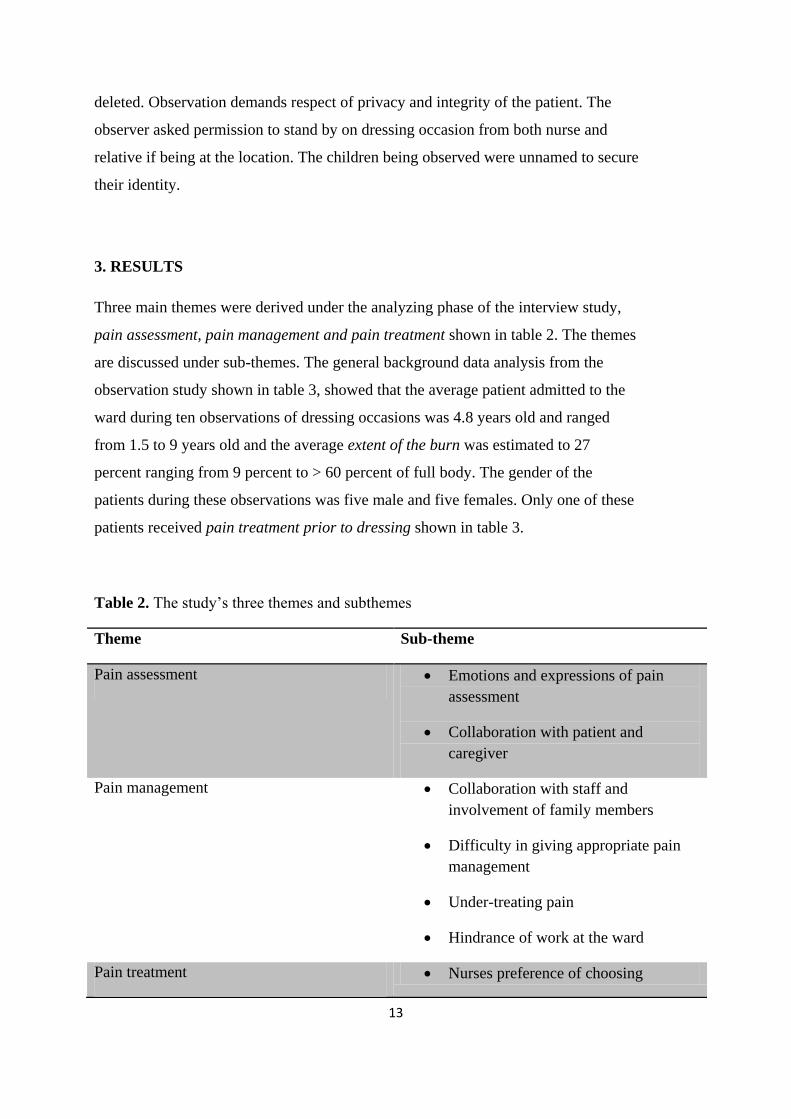
3. RESULTS
Three main themes were derived under the analyzing phase of the interview study,
pain assessment, pain management and pain treatment shown in table 2. The themes
are discussed under sub-themes. The general background data analysis from the
observation study shown in table 3, showed that the average patient admitted to the
ward during ten observations of dressing occasions was 4.8 years old and ranged
from 1.5 to 9 years old and the average extent of the burn was estimated to 27
percent ranging from 9 percent to > 60 percent of full body. The gender of the
patients during these observations was five male and five females. Only one of these
patients received pain treatment prior to dressing shown in table 3.
Table 2. The study’s three themes and subthemes
Theme Sub-theme
Pain assessment Emotions and expressions of pain
assessment
Collaboration with patient and
caregiver
Pain management Collaboration with staff and
involvement of family members
Difficulty in giving appropriate pain
management
Under-treating pain
Hindrance of work at the ward
Pain treatment Nurses preference of choosing
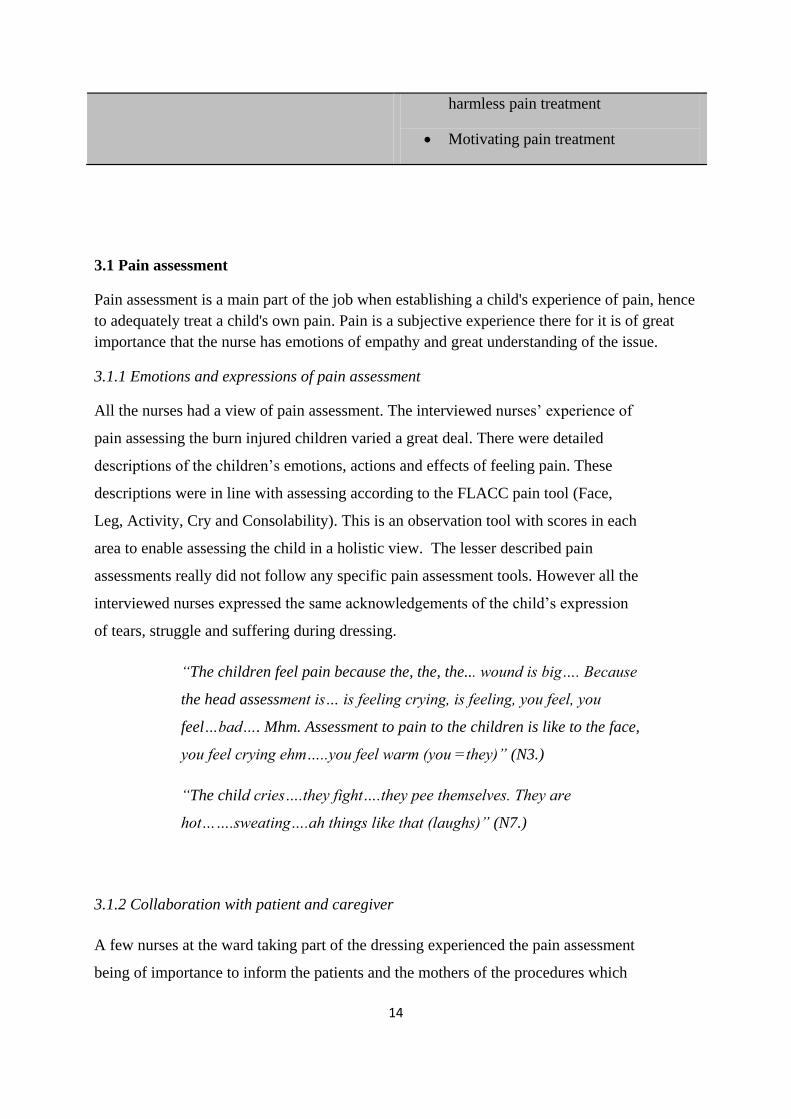
14
harmless pain treatment
Motivating pain treatment
3.1 Pain assessment
Pain assessment is a main part of the job when establishing a child's experience of pain, hence
to adequately treat a child's own pain. Pain is a subjective experience there for it is of great
importance that the nurse has emotions of empathy and great understanding of the issue.
3.1.1 Emotions and expressions of pain assessment
All the nurses had a view of pain assessment. The interviewed nurses’ experience of
pain assessing the burn injured children varied a great deal. There were detailed
descriptions of the children’s emotions, actions and effects of feeling pain. These
descriptions were in line with assessing according to the FLACC pain tool (Face,
Leg, Activity, Cry and Consolability). This is an observation tool with scores in each
area to enable assessing the child in a holistic view. The lesser described pain
assessments really did not follow any specific pain assessment tools. However all the
interviewed nurses expressed the same acknowledgements of the child’s expression
of tears, struggle and suffering during dressing.
“The children feel pain because the, the, the... wound is big…. Because
the head assessment is… is feeling crying, is feeling, you feel, you
feel…bad…. Mhm. Assessment to pain to the children is like to the face,
you feel crying ehm…..you feel warm (you =they)” (N3.)
“The child cries….they fight….they pee themselves. They are
hot…….sweating….ah things like that (laughs)” (N7.)
3.1.2 Collaboration with patient and caregiver
A few nurses at the ward taking part of the dressing experienced the pain assessment
being of importance to inform the patients and the mothers of the procedures which
15
was about to take place, regardless of the child’s daily experience of dressing
procedure. In order to get a good pain assessment nurses described the need for
cooperation and calm of the patient and relative.
“…Because we have many children and we are few so we don’t have
space, when you finish one you clean the table you continue. Also
mothers they are standby they want to be treated, everybody want…
ehe… everyone wants to be that one you are dressing (laughs) they
think that maybe the instrument can be finished and they, they can,
think they can stand without treatment, changing that dressing”. (N 4)
3.2 Pain management
Pain management in this case is viewed upon as a holistic way of caring for a patient
in pain admitted to the ward due to their burn injuries. To manage the patient there is
a need to consider how to care for the specific patient and which the best treatment
for the specific patient may be.
3.2.1 Collaboration with staff and involvement of family members
Nurses expressed routines and pain management according to their work situation.
From the gathered information the nurses expressed a satisfied opinion of their work
routine concerning pain management. They work along the side of a medical doctor
and interns at the ward and wishing to involve the patient and their relative.
“Treatment for pain, pain killer. The treatment, you must reassure the
mother what you are going to do. A nurse who was in duty she should be able
to know if the child she or he is in pain. And you give or administer the proper
drug which is it administered or prescribed by the specialist or intern Dr,
whichever is the administer” (N 1.)
3.2.2 Difficulties to give appropriate pain management
A few nurses expressed the difficulty to find an appropriate pain management
scheme and to cope with the situation accordingly, seeing the patient in pain. As
patients are there for a very long time suffering extensive injuries a number of nurses
16
expressed on several occasion that they are afraid of addiction to opiates of the
patients, leaving the child un-sedated on occasions when otherwise needed. Most
nurses rarely expressed urgent need for analgesics on dressing occasions or seeked
more administration from the doctors on the ward.
“Sometimes it is very difficult to cope with these things. Because in
treating burn it takes long time, it can take months…even a year if a
burn injury is big in percent. So….we don’t use to give sedation. We
don’t use sedation because we are afraid of addiction, to be addicted.
(N 4.)
Only one nurse expressed spontaneously she had not worked there for very long and
that she would like to give more pain treatment.
“Children you (they) feel pain because…because, because the wound is
bad. Mm, yeah I did not do this for a very long time. I like to give
medicine.” (N3.)
3.2.3 Under -treating pain.
Majority of the nurses expressed similar acknowledgements of children being
uncooperative during daily dressings due to the lack of appropriate pain management
resulting in nurses not being able to do their work in a wishful manner. Recognizing
the child in pain is to be considered as the child not being sufficiently pain managed
for the dressing occasion.
“…children are stubborn, even you, you feel that they are getting pain,
but nothing to do. We are trying to be patient, and to let that situation
in order to complete the job smoothly. We are trying to please them…
But they don’t even reasoning. But after dressing, after a while they
are ok (laughs)…” (N4.)
3.2.4 Hindrance of work at the ward.
A few nurses experienced the facility of the ward to be of hindrance as the children
suffered from the heat of the surroundings leaving the children impatient and stressed
17
with the situation prior to the dressing occasion as well as the work load for the
nurses with number of patients waiting in line for dressings.
“The children are crying, it is hot….and children are suffering…eh. I
want more time for information to patient…inform the mother and,
and…work together with…mmm” (N 7.)
“For example dressing or caring about one and a half to two hours for
one patient…ah…which is long time of hours. Which is long, tough job
because there is between fifteen to nineteen children” (N 1.)
3.3 Pain treatment
Pain treatment at the ward was available and prescribed by the physician or intern at
the ward. There was a variety of analgesics which could be used for different
situations. Panadol as a regular analgesic was used for fever or pain conditions in
general. Pethidine, opiates and non steroid analgesic drugs such as Diklofenak was
prescribed for serious pain conditions or when the pediatric has undergone surgery
recently.
3.3.1 Nurses preference of using harmless pain treatment
Pain treatment is shown by the study results to be generalized to Panadol. Most of
the nurses expressed few alternative analgesics to be used in the purpose to pain
relieve burn injured children specifically during the daily occurring dressing of
wounds. The use of stronger drugs or opiates was combined with the child having
undergone surgery such as skin grafting or recently being admitted to the ward. More
than half of the eight participating nurses expressed Panadol on several occasions as
the most appropriate analgesic to use as it has little side effects, expressing fear of
children being addicted to opiates.
“Panadol, as there is little side effects.” (N1.)
“Medicine to use for pain….ah …of pain...Paracetamol…. if you are
going to do…for doing the skin grafting…. Pethidine. If the wound is
clean you can use cream sometimes.” (N3.)
18
3.3.2. Motivating pain treatment
The majority of nurses discussed the children's need for pain treatment and their
motivation why and when the child would need pain treatment. When comparing
data results shown in table 3 from the observation part of the study with the nurses’
transcribed interviews, the burn injured children did not receive more pain treatment
than observed and in line with the expressed frequency of the nurses.
“For me to say which one is the best…..I say Panadol ah…..we have
Panadol many times. Sometimes if the child is very much in pain….the
Dr may prescription Diklofenak….lakini (but in Swahili) for regular
patients who did not go to the operating theatre….we… ah… give them
Panadol.” (N8.)
“….after dressing we use to give them analgesics like Panadol and so
forth. But we are not giving them sedation…maybe when they come
from operating theatre, for that pain we are using to give them
Pethidine for maybe 8 hrs or 24 hrs., if it happens to have severe pain”
(N 4.)
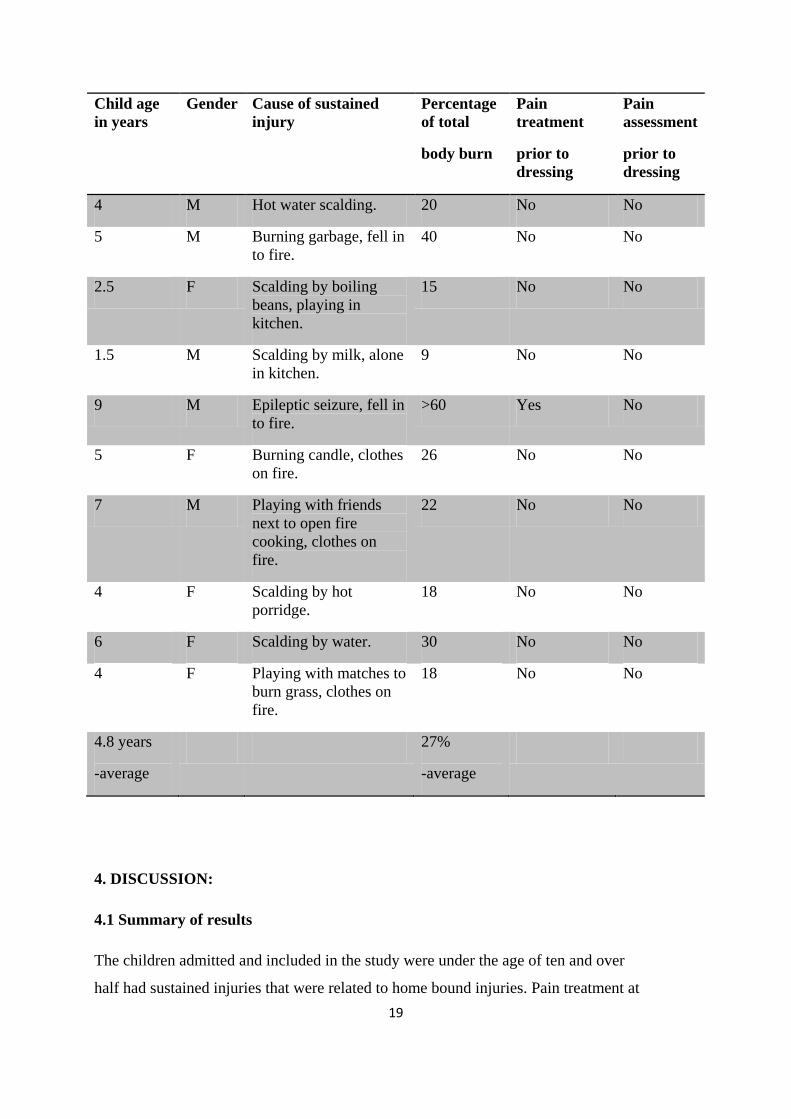
3.4 Extent of burn injury and pain treatment prior to dressing from observation
This result is showing data collected from the observation part of the study which
was carried out prior to the interviews. On average the children’s summed up burn
extent injury was 27% from the observation study. The sustained injuries are caused
due to clothes catching on fire or being soaked in hot liquids. This leaves injuries
over torsos and genital areas in general as a result of clothes being centered on these
parts of the child’s body. This percentage should be taken in to consideration of the
individual’s age and size. Regardless of age and size the degree of burn should also
be accounted for, which can tell a lot of the pain the child will feel during dressing.
The observation study showed that in one case the one child with over 60% burn
injury was given pain treatment prior to the dressing.
Table 3. Observation study results.
19
Child age
in years
Gender Cause of sustained
injury
Percentage
of total
body burn
Pain
treatment
prior to
dressing
Pain
assessment
prior to
dressing
4 M Hot water scalding. 20 No No
5 M Burning garbage, fell in
to fire.
40 No No
2.5 F Scalding by boiling
beans, playing in
kitchen.
15 No No
1.5 M Scalding by milk, alone
in kitchen.
9 No No
9 M Epileptic seizure, fell in
to fire.
>60 Yes No
5 F Burning candle, clothes
on fire.
26 No No
7 M Playing with friends
next to open fire
cooking, clothes on
fire.
22 No No
4 F Scalding by hot
porridge.
18 No No
6 F Scalding by water. 30 No No
4 F Playing with matches to
burn grass, clothes on
fire.
18 No No
4.8 years
-average
27%
-average
4. DISCUSSION:
4.1 Summary of results
The children admitted and included in the study were under the age of ten and over
half had sustained injuries that were related to home bound injuries. Pain treatment at
20
the pediatric burn ward included Panadol on regular occasions but not frequently
prior to dressings. Stronger drugs such as Pethidine was more commonly used related
to skin grafting procedures or when extensive pain relief was considered necessary
due to severity of burn injury. The analysis of the interviews resulted in three themes,
pain assessment, pain management and pain treatment under which the specific
objectives could be answered.
The nurses at the burn ward expressed assessment skills that cannot be compared
with a specific pain assessment tool. The results expressed the nurse’s experiences
of pain management as well as their work routines concerning pain management.
Nurses’ experience having satisfying pain management skills and work according to
their set ward routines. Further the observations showed that the nurses did not use
any pain assessment tools before and during burn dressings and the children were not
pain treated on most occasions prior to their upcoming dressing. The observation
part of the study showed that children regardless of degree of burn did not receive
pain treatment in majority of the ten observed dressing occasions.
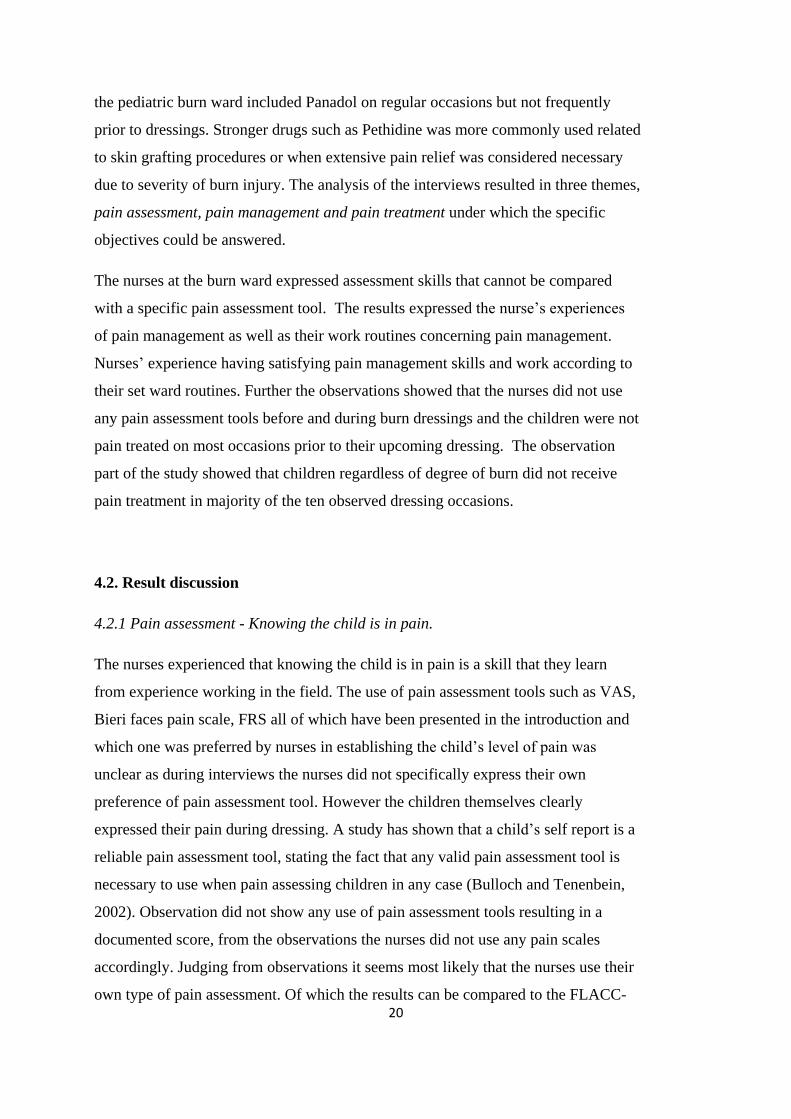
4.2. Result discussion
4.2.1 Pain assessment - Knowing the child is in pain.
The nurses experienced that knowing the child is in pain is a skill that they learn
from experience working in the field. The use of pain assessment tools such as VAS,
Bieri faces pain scale, FRS all of which have been presented in the introduction and
which one was preferred by nurses in establishing the child’s level of pain was
unclear as during interviews the nurses did not specifically express their own
preference of pain assessment tool. However the children themselves clearly
expressed their pain during dressing. A study has shown that a child’s self report is a
reliable pain assessment tool, stating the fact that any valid pain assessment tool is
necessary to use when pain assessing children in any case (Bulloch and Tenenbein,
2002). Observation did not show any use of pain assessment tools resulting in a
documented score, from the observations the nurses did not use any pain scales
accordingly. Judging from observations it seems most likely that the nurses use their
own type of pain assessment. Of which the results can be compared to the FLACC-
21
scale if that would that have been used. Using the FLACC-scale can be supported as
valid tool even when pain assessing cognitive impaired children (Voepel et al.,
2002). It has been discussed that pain assessment motivation may vary to a greater
extent than predicted when a person is pain assessing others. Meaning that some pain
assessments might be under scored or leaving a patient insufficiently pain managed
due to the pain assessing persons own beliefs of pain and motivation to follow
through on pain assessment and management. Although more research in the subject
is required (Franck and Bruce, 2009). The author however finds it interesting to find
that the ability and motivation might actually be a matter of culture, personality and
skills combined.
4.2.2 Pain management - Treating pain from a holistic view in burn injured children.
Nurses expressed little use of analgesic drugs in general, although they named a
variety. The variety of pain treatment and ways of administering pain treatment for
burn injured children is broad and are effective and proven to suit their purpose such
as morphine tablets, morphine administered intravenously and also topically
(Watterson et al., 2004). The main objective is to individualize pain assessment and
the given pain treatment to ensure adequate pain treatment is given the specific child
to soothe their condition to the fullest extent possible. It seems to be a matter of
opinion from the interviewed that the child apparently will manage and cope with the
burn dressing under the existing circumstance and that nurses more often treat pain
after dressing if the child still complains or suffer from pain. The results from this
study shows that more work is needed to pain manage children at the pediatric burn
ward, and the study can be used to illuminate the lack of administered pain treatment
to improve the situation for children undergoing painful daily dressings.
4.2.3 Problems in proceeding with daily dressing of burn injured children.
Nurses in the pediatric burn ward repeatedly expressed the patient’s lack of
cooperation during dressing occasions as being a hindrance in their work process.
This indicates that the burn injured children are insufficiently pain managed prior to
the dressing occasion. A child undergoing dressing of their burn injuries may
experience the situation so stressful that it possibly could disturb their biological
stress system leading to inherent temperamental traits (Stoddard et al, 2006). It is
22
already proven that burn injured children suffer from PTSD. This supports the fact
that burn injured children should be sufficiently pain managed in all aspects of their
condition, referring to burn dressings being a general term for what the burn injured
patient has to undergo (Davies, 1971). Supporting the fact that children suffer from
distress and anxiety related to dressing of the sustained burn injury as well as this
being state can prolong the time needed for the burn management procedure. It is
also shown that children can be distracted by games during dressing in some
situations leading to lower pain scores (Debashish, Grimmer, Sparnon, MacRae and
Thomas, 2005).
4.2.4 Pain treatment - The best pain management for burn injured children.
The study showed that the nurses at the pediatric burn ward had good facilities to
care for children suffering from burn injuries in the sense of stating availability of
appropriate pain treatment. The theoretical practice of individualizing pain treatment
should lead to a number of analgesic methods to be used. Such as opiates in general,
topical analgesic treatment or peripheral analgesics. Considering the majority of
nurses expressed that Panadol being the best pain management for burn injured
children leaves a lot of room for improvement in the area. The nurses expressed fear
of addiction appearing in children as one of the reasons to their preference of
Panadol. Pain management when administered, assessed and monitored properly
leaves little indication to assume the burn injured child will be showing tolerance
immediately. Meaning there is a number of options to turn to and precautions to take
should a child show signs of tolerance to opiates. The use of morphine can for
example be exchanged with methadone to reduce unwished for side effects (Williams
et al., 1998).
4.2.5 Observation study
The observation part of the study was valuable for the author in writing the thesis.
The observations served as background data to recall the dressing situation when
later interviewing the nurses. Although the author did consider some ethical aspects
of conducting observations as having an observer during dressing occasion can be of
conflict of ethical aspects. Having an observer also might affect the behavior of
23
children undergoing dressing as well as the nurses paying more attention to the work
situation, feeling uncomfortable or simply being distracted.
4.3 Method discussion
4.3.1 Credibility - how reliable are the results in relation to the objectives of the study.
Credibility was established due to the nurses answering the same questions. This
gave all the nurses the same opportunity to express their views on each question
asked. Semi-structured qualitative interview open ended questions were used since
this reveals the informants own experience (Polit, & Beck, 2008). Communicative
validity may be discussed since the author is not a trained interviewer as a
profession, leaving more room for improved interview skills or methods. The nurses
who took part in the interviews may have experienced the situation stressful
considering their workload. However nurses were not extracted from their work
situation and the author gave the nurses time to gather information and themselves
prior to the interview session.
Since the interview questions were of a general matter and open ended the nurses
seemed at times unsure of how to answer, this leaves consideration for experienced
language difficulties. With more specific question the informants may have been able
to express themselves more or even the use of a questionnaire form so the nurses
could take the questionnaire home and reply with written answers. The internal
validity of this matter can be questioned. As the author did not execute participant
self control of the interview material to avoid or be able to correct misunderstandings
on behalf of the author. The questions used however gave valuable information as of
how nurses experience pain management and their feelings at the working moment
extending credibility to the study.
From the discussion of the three derived themes it became clear as to which themes
fell in to the aim of the study in a natural manner. Something which pleased the
author as it was not predicted. The nurse’s description of knowing the burn injured
child is in pain fell in to the pain assessment theme. Nurses describing the objectives
concerning treating pain in burn injured children and problems in proceeding with
24
daily dressing of burn injured children underwent the theme of pain management.
Pain treatment as one theme covered the objective of what nurses considered to be
the best pain treatment. The themes illuminate the core of pain management as a
holistic aspect, and support the ways of scientifically proven methods of pain
management.
4.3.2 Dependability - how reliable is the conclusion compared to the extracted material.
Dependability was reached through showing a clear line throughout the text to the
derived themes. The author chose to proceed with a manifest content analysis to
identify similarities and differences in the informant’s opinions (Graneheim and
Lundman, 2004). The analysis process is accounted for via the meaning units,
condensed meanings and way of abstractions in text and examples shown in table1.
Every step of the analysis process has been reflected upon concerning interpretation
possibilities and abstraction levels. Reaching the codes and themes are then
considered to help strengthen the analysis result. Validity in this sense is considered
to be reached as the author took precautions during the analyzing part before stating
the codes, themes and sub-themes. This was a precaution taken since the author was
inexperienced compared to other experienced interviewers who might reach
abstraction levels faster.
4.3.3 Transferability - in what way can the results be used.
Data collected from the study was withheld from ten observations and eight
interviews. All interviews were used in the result. No particular exclusion needed to
be done as the author depended on all the informants whom could be used in terms of
the informant’s language skills and available staff that suited the selection criteria.
The informants limited language skills and limited variation of work experience
ranging from over one year to ten is a limit in itself to illuminate the specific
objectives from a variety of experience.
As a qualitative study it cannot be generalized over all pediatric burn wards in
Tanzania as other wards might have different solutions to their dealing with pain
management. On the other hand the study illuminates how the nurses working at
Muhimbili university hospital and the pediatric burn ward experience their given
pain management. The study can be of clinical relevance when looking at extended

25
development and educational matters for the staff. It can be of interest to extend the
study to see whether there are more aspects to the lack of pain management in
general being used at the pediatric burn ward.
4.4 Conclusion
Pain management among nurses caring for burn injured children is a subject that
needs to be paid more attention to. The nurses express both experience and
knowledge of how to assess pain and manage pain. Yet there is a lack of routines to
fulfill the duty of ever existing need for pain management.
4.4.1 Nursing implications
These findings provide good reason the potential role for interventions to be carried
out in the purpose to improve the dressing occasions for the burn injured children
concerning their experienced pain as well as improving the work situation for the
nurses.
References:
Bulloch, B. & Tenenbein, M. (2002). Validation of 2 Pain Scales for Use in the
Pediatric Emergency Department. Pediatrics.110 (33), DOI: 10.1542/peds.110.3.e33
Dalen, M. (2008). Intervju som metod. Malmö: Glerups utbildning AB
Davies, M. (1971). Burns. Section of Plastic Surgery. (64).
Dadure, C., Acosta, C. & Capdevila, X. (2004). Perioperative Pain Management of a
Complex Orthopedic Surgical Procedure with Double Continuous Nerve Blocks in a
Burned Child. Anesthetist Analgesics. (98), 1653–5.
DOI:10.1213/01.ANE.0000114084.01266.E5
26
Debashish. D. A., Grimmer, K.A., Sparnon, A.L., McRae, S.E. & Bruce H Thomas,
B. H. (2005). The efficacy of playing a virtual reality game in modulating pain for
children with acute burn injuries: A randomized controlled trial. BMC Pediatrics
5(1), doi:10.1186/1471-2431-5-1
D’Souza, A.L., Nicholas, G., & McKenzie, L.B., N. (2009). Pediatric Burn Injuries
Treated in US Emergency Departments Between 1990 and 2006. Pediatrics
(124), 1424-1430. DOI: 10.1542/peds.2008-2802.
Fadaizadeh, L., Emami, H., Samii, K. (2009). Comparison of Visual Analogue Scale
and Faces Rating Scale in Measuring Acute Postoperative Pain. Archives of Iranian
Medicine. 12(1), 73 – 75
Fortier, M.A., MacLaren Chorney, J., Rony, R.Y.Z., Perret-Karimi, D., Rinehart,
J.B., Camilon, F.S. & Kain, Z.N. (2009). Children’s Desire for Perioperative
Information. Anesthetist Analgesics. 109(4), 1085–1090.
doi:10.1213/ane.0b013e3181b1dd48.
Franck. S.L. & Bruce, E. (2009). Putting pain assessment into practice: Why is it so
painful? Pain Res Manage. 14(1), 13-20.
Graneheim, U.H. & Lundman, B. (2004). Qualitative content analysis in nursing
research: concepts, procedures and measures to achieve trustworthiness. Nurse
Education Today. (24) 105-112.
Hackett, M.E. (1971). Burns. Section of Plastic Surgery. (64).
Jansson, L., & Gustavsson, M., (2005). Ett brännskadat barn. Examensarbete.
Malmö högskola, sjuksköterskeprogrammet.
Kargi, E., & Tekerekoglu, B. (2010). Usage of lidocaine-prilocaine cream in the
treatment of post burn pain in pediatric patients. Turkish Journal of Trauma &
Emergency Surgery. 16 (3), 229-232.
27
Ley-Chavez, E., Martines-Pardo, M.E., Roman, R., Oliveros-Lonzano, F., &
Canchola-Martines, E. (2003). Application of Biological Dressings from
Radiosterilized Amnios with Cobalt 60 and Serologic Studies on the Handling of
Burns in Pediatric Patients. Annals of transplantation. 8(4), 46-49.
Mbembati, N.A.A., Museruand, M., Leshahari, M. T. (1999). Childhood Burn
Injuries in Children in Dar es Salaam: Patterns and Perceptions of prevention.
Study. Muhimbili University, Collage of Health sciences.
Newman, C.J., Lolekha, R., Limkittikul, K., Luanxay, K., Chotpitayasunondh, T., &
Chantavanich, P. (2005). A comparison of pain scales in Thai children. Archives of
Disease in Childhood. (90), 269–270. doi: 10.1136/adc.2003.044404.
Packer, K. J., (1972). Methoxyflurane analgesia for burns dressings. Postgraduate
Medical Journal. (48), 128-132.
Polit, D.F. & Beck, C.T. (2008). Nursing Research. Generating and Assessing
Evidence for Nursing Practice (8th
ed.). Philadelphia: Lippincott Williams &
Wilkins.
Saxe, G., Stoddard, F.J., Hall, E., Chawla, N., Lopez, C., Sheridan, R.L., King, D.,
King, L & Yahuda, R. (2005). Pathways to PTSD, Part I: Children With Burns.
American Journal of Psychiatry. (162), 1299–1304.
Schiavenato, M. (2007). Facial Expression and Pain Assessment in
The Pediatric Patient: The Primal Face of Pain. Journal for Specialists in Pediatric Nursing.
13 (2).
Serour, F., Gorenstein, A. & Boaz, M. (2008). Characteristics of Thermal Burns in
Children Admitted to an Israeli Pediatric Surgical Ward. Israel Medical Association
Journal. (10), 282–286.
28
Silva, F.C. & Thuler, L.C. (2008). Cross-cultural adaptation and translation of two
pain assessment tools in children and adolescents. Journal of Pediatrics. 84(4), 344-
349. doi:10.2223/JPED.1809.
Spedding, R.L., Harley, D., Dunn, F.J. & McKinney, L.A. (1999). Who gives pain
relief to children? Journal of Accident Emergency Medicine. (16), 261-264.
Stoddard, F.J., Ronfeldt, H., Kagan, J., Drake, J.E., Snidman, N., Murphy, J.M.,
Saxe, G., Burns, J., & Sheridan, R.L. (2006). Young Burned Children: The Course of
Acute Stress and Physiological and Behavioral Responses. American Journal of
Psychiatry. (163), 1084–1090.
The Northern Nurses´ Federation. (2003). Etiska riktlinjer för omvårdnadsforskning i
norden. Stockholm: vård i norden. Hämtad 9 december, 2010, från
www.vardinorden.org/ssn/etikk.pdf
Voepel-Lewis, T., Merkel, S., Alan R. Tait, A.R., Trzcinka, A., & Malviya, S.
(2002) The Reliability and Validity of the Face, Legs, Activity, Cry, Consolability
Observational Tool as a Measure of Pain in Children with Cognitive Impairment.
Anesthesist Analgesics. (95), 1224 –9.
Watterson, G., Howard, R., & Goldman, A. (2004). Peripheral opioids in
inflammatory pain. Archives of Disease in Childhood. (89), 679–681. Doi:
10.1136/adc.2003.032003.
Williams, P.I., Sarginson, R.E. & Ratcliffe, J.M. (1998). Use of methadone in
morphine-tolerant burned pediatric patients. British Journal of Anaesthesia. (80), 90-
92.
29
Appendix 1.
Observation guide
Patient data: For background information only
Ward: Date: Time:
Patient/Gender: Age:
Type of burn injury: degree of injury
Cause of injury: Time since injury and time spent in hospital
Analgesic method:
Time for analgesia:
Time of dressing burn wound:
Pain evaluation:
Nurse at dressing occasion uses pain evaluation tool Yes/No
Patient expresses pain (observer uses FLACC) Yes/No
Nurse acknowledges patients pain. (i.e. talks to patient, gives analgesia) Yes/No
observation notes: (short notes to remember the occasion)
30
Appendix 2.
Interview guide: Open ended questions of a general matter with a nurse during
approximately 20 min.
Background fact on nurse:
Enrolled or registered nurse.
How many months or years experience at the pediatric burn ward.
How would you like to provide good pain management for or treat children with burn
injuries with pain? e.g
- What is your experience of treating pain in children?
- Which is the best pain treatment for burn injured children?
- How do you know the child is in pain? In your opinion do you feel you have a good
assessment tool?
- What kind of problems do you meet in your daily work with burn injured child patients?
31
Appendix 3.
Participant information and consent form
Study regarding nurse’s experience of pain management in caring for burn injured children.
My name is Andrea Olsson and I am a third year nursing student from Uppsala University in
Sweden. Muhimbili University of Health and Allied Sciences and Uppsala University have a
co-operation offering student exchange. I am writing my thesis in the period September
through December. I will conduct a small study entitled; Nurses experience of pain
management in caring for burn injured children. Permission for the study is given by the Dean
of school of nursing.
Purpose of the Study
The aim of the study is to investigate how nurses at Muhimbili University Hospital in Dar Es
Salaam, Tanzania experience and work with pain management of burn patients at a paediatric
ward.
Participants
Ten nurses at Muhimbili University hospital in Dar es Salaam will be asked to voluntary
participate on one occasion each.
What Participation Involves
Participants will be asked questions about their experience of caring for paediatric patients
with pain due to burn injuries. The interview will be recorded with a tape recorder and the
information used to write a study report. The interview will take approximately 20-30
minutes. The interviewer and nurse will agree on a appropriate time related to a patient care
situation for reflection and interview.
Participants full rights
Participation in this study is voluntary. Participants are free to withdraw from the study
without expressing their reason. I will be sincerely grateful for all participation however.
32
Confidentiality
I will assure that strict confidentiality will be assessed for the study. No names will be
mentioned or left traceable in the study. All documents will be kept among me and my
supervisor in Tanzania and Sweden.
Benefits
There will be no economic benefit to the voluntary participants in this study. However, the
results of the study might be of interest for nurses involved in their future work as a health
care professionals dealing with pain management. A copy of the finished report will be sent to
the participants either by mail or email and the school of nursing.
Who to Contact
Voluntary nurse participants with questions concerning this study are welcome to contact me
at site or via e- mail:
Andrea Olsson; [email protected]
Consent to participate in a research project:
Participant agrees………………………… Participant does NOT agree ……………….........
I, _________________________________have read the contents in this form. My questions
have been answered. I agree to participate in this study.
Signature of participant_________________________________
Signature of researcher__________________________ Date of signed consent:

33


















