
NURS 2410 Unit 4 Nancy Pares, RN, MSN Metro Community College.
108
NURS 2410 Unit 4 Nancy Pares, RN, MSN Metro Community College
-
Upload
cordelia-booth -
Category
Documents
-
view
217 -
download
0
Transcript of NURS 2410 Unit 4 Nancy Pares, RN, MSN Metro Community College.

NURS 2410 Unit 4
Nancy Pares, RN, MSNMetro Community College

Identification of At-risk Newborn
• Low socioeconomic level of the mother • Limited or no prenatal care• Exposure to environmental dangers• Preexisting maternal conditions

Identification of At-risk Newborn (continued)
• Maternal factors such as age or parity• Medical conditions related to pregnancy • Pregnancy complications

Feeding Guidelines

Early Feeding Skills (EFS)
Congenital Anomalies

Congenital Anomalies

Congenital Anomalies

Congenital Anomalies

Congenital Anomalies

Congenital Anomalies

Congenital Anomalies

Congenital Anomalies

Nursing Care of the Drug-Exposed Newborn
• Neonatal abstinence scoring• Monitoring VS and pulse oximetry until stable• Small frequent feedings• IV therapy if needed• Positioning on the right side-lying or semi-
Fowler’s • Monitoring frequency of diarrhea and
vomiting

Nursing Care of the Drug-Exposed Newborn
• Weigh infant every 8 hours during withdrawal• Swaddle infant• Protect face and extremities from excoriation • Place infant in quiet, dimly lighted area of the
nursery• Administration of medications

Infants Born to HIV/AIDS Infected Mothers: Consequences
• Prematurity• SGA• Failure to thrive• Enlarged spleen and liver• Swollen glands

Infants Born to HIV/AIDS Infected Mothers: Consequences
• Recurrent respiratory infection• Rhinorrhea• Recurrent GI problems• Persistent or recurrent candidiasis

Nursing Care of the Infant Born to HIV/AIDS Infected Mothers
• Provide comfort• Keep the newborn well nourished• Keep the infant protected from infections• Facilitate growth, development, and
attachment

Newborn Withdrawal

Neonatal Abstinence

Neonatal Abstinence

Infants at Risk for HIV/AIDS

Cardiac Defects

Cardiac Defects

Cardiac Defects

Cardiac Defects

Cardiac Defects

Small-for-gestational-age
• Maternal factors• Maternal disease• Environmental factors• Placental factors• Fetal factors

Triplets Manifesting Different Rates of Growth

• Infants <10th percentile for weight at birth• May be symmetric or asymmetric • Factors may be fetal, maternal, or placental• Complications
– Hypoxia, hypothermia, hypoglycemia, polycythemia, hyperbilirubinemia, meconium aspiration
Intrauterine Growth Restriction

• Nursing implications– Prevent heat loss– Monitor blood glucose, feed early– Monitor for respiratory complications– Management of hyperbilirubinemia
Intrauterine Growth Restriction (continued)

• Infants >90th percentile for weight at birth• Factors
– Maternal diabetes, parental obesity
• Complications– Difficult delivery, birth trauma, hypoglycemia
• Nursing implications– Assess for birth injury– Monitor for hypoglycemia
Large for Gestational Age Infant

Impact of Maternal Diabetes Mellitus (DM) on the Newborn
• LGA• SGA• Hypoglycemia• Hypocalcemia• Hyperbilirubinemia

Impact of Maternal Diabetes Mellitus (DM) on the Newborn
• Birth trauma• Polycythemia• RDS• Congenital malformations

• Risk factors– Congenital anomalies– Macrosomia (>4,000 gm)– Hypoglycemia– Respiratory distress syndrome
Infants of Diabetic Mothers

• Prevention of complications– Normoglycemia during gestation and labor– Deliver when lungs are mature– Prepare for delivery of large infant– Monitor for hypoglycemia
Infants of Diabetic Mothers (continued)

Hypoglycemia Symptoms
• Lethargy or jitteriness• Poor feeding and sucking• Vomiting• Hypothermia and pallor• Hypotonia, tremors• Seizure activity, high pitched cry, exaggerated
moro reflex

Hypoglycemia: Nursing Care
• Routine screening for all at risk infants• Early feedings• D10W infusion

Figure 33–14 Potential sites for heel sticks. Avoid shaded areas to prevent injury to arteries and nerves in the foot and the important longitudinally oriented fat pad of the heel, which in later years could impede walking.

Figure 33–15 Heel stick. With a quick, piercing motion, puncture the lateral heel with a microlance. Be careful not to puncture too deeply.

Postmaturity Syndrome
• Hypoglycemia• Meconium aspiration and oligohydramnios• Polycythemia• Congenital anomalies• Seizures• Cold stress

The Premature Infant
• Delivery prior to 37 weeks’ gestation
• Factors– Multiple gestation,
PROM, incompetent cervix

Assessment of the Preterm Newborn
• Physical characteristics• Gestational age• Maternal prenatal risk factors• Delivery risk factors• Physical assessment• Family assessment

• Assessment– Gestational age assessment– Neurologic assessment– Physical characteristics
• Thin skin, soft cartilage, absent plantar creases• Abundant lanugo and vernix• Genitalia characteristic of prematurity
The Premature Infant (continued)

Review of Systems and Potential Complications
• Cardiovascular– Patent ductus arteriosis– Hypotension
• Central nervous system– Intraventricular hemorrhage– Posthemorrhagic hydrocephalus
• Hematologic system– Anemia– Polycythemia
• Hepatic system– Hyperbilirubinemia
Phototherapy

Risk Factors for Hyperbilirubinemia

Lab Evaluation of Jaundice

Checklist for in-room Phototherapy

• Excess bilirubin in the blood resulting in jaundice
• Can be caused by physiologic or pathologic processes– Normal RBC breakdown – Rh or ABO incompatibility
Hyperbilirubinemia

• Complications– Kernicterus– Erythroblastosis fetalis– Hydrops fetalis
• Assessment findings– Jaundice, elevated bilirubin levels
Hyperbilirubinemia (continued)

• Encourage frequent feedings• Exposure to sunlight• Phototherapy
– Shield infant’s eyes– Monitor body temperature– Monitor weight– Monitor fluid intake– Weigh diapers– Note frequency of stools
Management of Hyperbilirubinemia

Physiologic Hyperbilirubinemia
• Appears after first 24 hours of life• Disappears within 14 days• Due to an increase in red cell mass

Pathologic Hyperbilirubinemia
• Appears within first 24 hours of life• Serum bilirubin concentration rises by more
than 0.2 mg/dL per hour• Bilirubin concentrations exceed the 95th
percentile• Conjugated bilirubin concentrations are
greater than 2 mg/dL • Clinical jaundice persists for more than 2
weeks in a term newborn

Causes of Pathologic Hyperbilirubinemia
• Hemolytic disease of the newborn• Erythroblastosis fetalis• Hydrops fetalis• ABO incompatibility

Treatment of Pathologic Hyperbilirubinemia
• Resolving anemia• Removing maternal antibodies and sensitized
erythrocytes• Increasing serum albumin levels• Reducing serum bilirubin levels• Minimizing the consequences of
hyperbilirubinemia

Phototherapy: Nursing Care
• Maximize exposure of the skin surface to the light• Periodic assessment of serum bilirubin levels• Protect the newborn’s eyes with patches• Measure irradiance levels with a photometer• Good skin care and reposition infant at least every 2
hours• Maintain an NTE and adequate hydration and
nutrition

Figure 33–18 Infant receiving phototherapy. The phototherapy light is positioned over the incubator. Bilateral eye patches are always used during photo light therapy to protect the baby’s eyes. SOURCE: Courtesy of Lisa Smith-Pedersen, RNC, MSN, NNP.

Review of Systems (continued)
• Gastrointestinal system– Dysmotility– Necrotizing enterocolitis– Gastroesophageal reflux
• Immune system– Infection
• Integumentary system– Epidermal stripping– Absorption of chemical
agentsCrib with head elevated for reflux

Preterm Infant: GI Alterations
• Poorly developed gag reflex• Incompetent esophageal cardiac sphincter• Poor sucking and swallowing reflexes• Difficulty meeting caloric needs for growth • Inability to handle the increased osmolarity of
formula protein • Difficulty with absorbing saturated fats

Preterm Infant: GI Alterations (continued)
• Difficulty with lactose digestion• Deficiency of calcium and phosphorous • Increased basal metabolic rate and increased
oxygen requirements • Feeding intolerance• Potential for the development of necrotizing
enterocolitis (NEC)

Review of Systems (continued)
Ophthalmologic system◦ Retinopathy of prematurity
Renal system◦ Oliguria◦ Glycosuria
Respiratory system◦ Respiratory distress syndrome◦ Bronchopulmonary dysplasia◦ Apnea of prematurity◦ Pneumonia
Preterm infant in an oxygen hood

Preterm Infant: Respiratory Alterations
• Inadequate surfactant production• Muscular coat of pulmonary blood vessels is
not completely developed• Greater risk for the ductus arteriosis to remain
open

Fetal/Neonatal Risk Factors for Resuscitation
• Nonreassuring fetal heart rate pattern• Difficult birth • Fetal scalp/capillary blood sample-acidosis
pH<7.20• Meconium in amniotic fluid• Prematurity• Macrosomia or SGA

Respiratory Distress Assessment

Respiratory Distress Assessment

Respiratory Distress Assessment

Fetal/Neonatal Risk Factors for Resuscitation (continued)
• Male infant • Significant intrapartum bleeding• Structural lung abnormality or
oligohydramnios• Congenital heart disease• Maternal infection• Narcotic use in labor

Fetal/Neonatal Risk Factors for Resuscitation (continued)
• An infant of a diabetic mother• Arrhythmias• Cardiomyopathy• Fetal anemia

Respiratory Distress Syndrome (RDS)
• Deficiency or absence of surfactant• Atelectasis• Hypoxemia, hypercarbia, academia• May be due to prematurity or surfactant
deficiency

Figure 33–5 RDS chest x-ray. Chest radiograph of respiratory distress syndrome characterized by a reticulogranular pattern with areas of microatelectasis of uniform opacity and air bronchograms. SOURCE: Courtesy of Carol Harrigan, RNC, MSN, NNP.

RDS: Nursing Care
• Maintain adequate respiratory status• Maintain adequate nutritional status• Maintain adequate hydration• Education and support of family

Figure 33–9 Premature infant under oxygen hood. Infant is nested and has a nonnutritive sucking pacifier. SOURCE: Courtesy of Lisa Smith-Pedersen, RNC, MSN, NNP.

Transient Tachypnea of the Newborn (TTN)
• Failure to clear lung fluid, mucus, debris• Exhibit signs of distress shortly after birth• Symptoms
– Expiratory grunting and nasal flaring– Subcostal retractions– Slight cyanosis

TTN: Nursing Care
• Maintain adequate respiratory status• Maintain adequate nutritional status• Maintain adequate hydration• Support and educate family

Meconium Aspiration Syndrome (MAS)
• Mechanical obstruction of the airways• Chemical pneumonitis• Vasoconstriction of the pulmonary vessels• Inactivation of natural surfactant

MAS: Nursing Care
• Assess for complications related to MAS• Maintain adequate respiratory status• Maintain adequate nutritional status• Maintain adequate hydration

Persistent Pulmonary Hypertension (PPHN)
• Blood shunted away from lungs• Increased pulmonary vascular resistance (PVR)• Primary
– Pulmonary vascular changes before birth resulting in PVR
• Secondary– Pulmonary vascular changes after birth resulting
in PVR

PPHN: Nursing Care
• Minimize stimulation• Maintain adequate respiratory status• Observe for signs of pneumothorax• Maintain adequate nutritional status• Maintain adequate hydration status• Support and educate family

Figure 33–10 Chest x-ray of a left-sided pneumothorax. A rupture of the alveoli sacs allows air to leak through the pleura, forming collections of air outside the lung (air shows on x-ray as dark area over lung). SOURCE: Courtesy of Carol Harrigan, RNC, MSN, NNP.

Nutrition and Fluid Management
• Fluids– Strict I&O, weigh diapers
• Electrolyte management– Management of sodium
and potassium levels
• Glucose homeostasis• Feeding
– Gavage or nipple method– Types: formula or breast milk
Gavage feeding tube

Developmental Care of the Preterm Infant
LightSoundTemperaturePositioning and
containment strategiesHandling and touchingNonnutritive sucking

• Fractures– Clavicle, long bones, skull most common– Risks
• Large infant, breech, difficult labor
– Assessment• Impaired mobility
– Management• Immobilization, traction, casting
Trauma and Birth Injuries

• Facial Palsy– Usually related to use of forceps
• Brachial Palsy– Usually related to difficult delivery such as
shoulder dystocia– Assessment
• Impaired mobility of arm
– Paralysis may be temporary or permanent
Trauma and Birth Injuries (continued)

Preterm Infant: Alterations in Thermogenesis
• Unavailability of glycogen and brown fat• Inability to increase oxygen consumption• High ratio of body surface area to body weight• Extended position increases body surface area• Decreased ability to vasoconstrict superficial
blood vessels

Preterm Infant: Kidney Alterations
• Lower glomerular filtration rate (GFR)• Limited ability to concentrate urine or excrete
large amounts of fluid• Excrete glucose at a lower serum glucose level • Buffering capacity is reduced • Excretion time of drugs is longer

Preterm Infants: Liver Alterations
• Glycogen stores are used rapidly• Glycogen stores are affected by asphyxia and
cold stress• Low iron stores• Conjugation is impaired

Preterm Infants: Other Alterations
• Immunologic– Lack of passive IgG antibodies– Skin is easily excoriated
• Neurologic– Increased risk for IVH & ICH– Delayed or absent reactivity

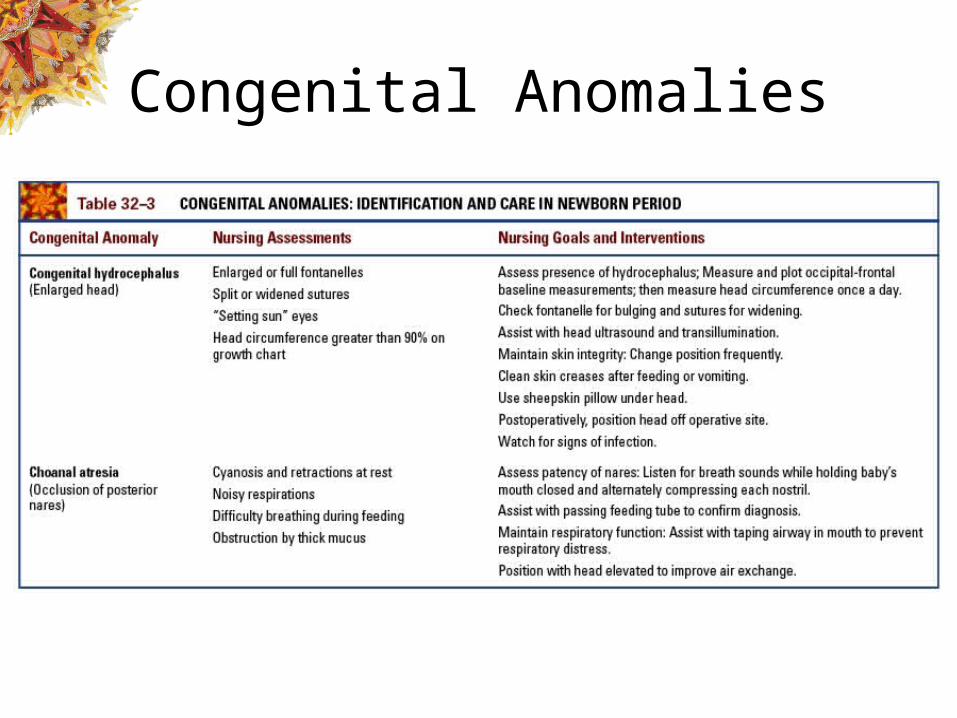
Hydrocephalus: Nursing Assessments
• Occipital-frontal baseline measurements• Daily head circumferences• Skin integrity• Signs and symptoms of infection• Signs of widening of suture lines

Hydrocephalus: Nursing Interventions
• Assist with head ultrasounds and transillumination
• Change position frequently• Clean skin creases• Keeping a sheepskin under the head• Postoperatively position head off the
operative site

Maternally TransmittedInfections

Maternally TransmittedInfections

Antibiotic/antiviral Therapy

Cold Stress
• Increase in oxygen requirements• Increase in utilization of glucose• Acids are released in the bloodstream• Surfactant production decreases

Figure 33–13 Cold stress chain of events. The hypothermic, or cold-stressed, newborn attempts to compensate by conserving heat and increasing heat production. These physiologic compensatory mechanisms initiate a series of metabolic events that result in hypoxemia and altered surfactant production, metabolic acidosis, hypoglycemia, and hyperbilirubinemia.

Cold Stress: Nursing Care
• Observe for signs of cold stress• Maintain NTE• Warm baby slowly• Frequent monitoring of skin temperature• Warming IV fluids• Treat accompanying hypoglycemia

• Risk factors– Maternal infection (group B streptococcus most
common)– Long labor, prolonged rupture of the membranes– Maternal fever, chorioamnionitis– Fetal distress, aspiration
Sepsis

• Assessment findings– Unstable temperature, poor tone, poor sucking
• Management– Antibiotics– Supportive care
Sepsis (continued)

Signs and Symptoms of Sepsis (continued)
• Temperature instability• Feeding intolerance• Hyperbilirubinemia• Tachycardia followed by apnea/bradycardia

Signs and Symptoms of Sepsis
• Lethargy or irritability• Hypotonia• Hypotension• Pallor, duskiness, or cyanosis• Cool and clammy skin

Symptoms of Syphilis
• Rhinitis• Red rash around the mouth and anus• Irritability• Generalized edema and hepatosplenomegaly• Congenital cataracts• SGA and failure to thrive

Syphilis: Nursing Management
• Initiate isolation • Administer penicillin• Provide emotional support for the family

Gonorrhea
• Symptoms– Conjunctivitis– Corneal ulcerations
• Nursing management– Administration of ophthalmic antibiotic ointment– Referral for follow-up

Symptoms of Herpes
• Small cluster vesicular skin lesions over the entire body
• DIC• Pneumonia• Hepatitis• Hepatosplenomegaly• Neurologic abnormalities

Herpes: Nursing Management
• Careful hand washing and gown and glove isolation
• Administration of IV vidarabine or acyclovir• Initiation of follow-up referral• Support and education of parents

Chlamydia
• Symptoms– Pneumonia– Conjunctivitis
• Nursing management– Administration of ophthalmic antibiotic ointment– Referral for follow-up

Facilitating Parental Attachment
• Facilitating family visits• Allowing the family to hold and touch the
baby• Giving the family a picture of the baby• Liberal visiting hours• Encouraging the family to get involved in the
care

Figure 33–20 Mother of a 26 weeks’ gestational age infant with respiratory distress syndrome on a ventilator is getting acquainted with her baby. Physical contact is vital to the bonding process and should be encouraged whenever possible. SOURCE: Courtesy of Lisa Smith-Pedersen, RNC, MSN, NNP.

Needs of Parents of At-risk Infants
• Realistically perceiving the infant’s medical condition and needs
• Adapting to the infant’s hospital environment• Assuming primary caretaking role• Assuming total responsibility for the infant
upon discharge• Possibly coping with the death of the infant if
it occurs


















