Nucleus cytoplasm extracellular fluid water Na+ K+ Cl- sugars proteins plasma intracellular fluid 7%...
44
nucleus cytoplasm extracell ular fluid water Na+ K+ Cl- sugars proteins plasma intracellular fluid 7% 26% 67%
-
Upload
norma-oconnor -
Category
Documents
-
view
215 -
download
0
Transcript of Nucleus cytoplasm extracellular fluid water Na+ K+ Cl- sugars proteins plasma intracellular fluid 7%...

nucleus
cytoplasm
extracellular fluid
waterNa+K+Cl-sugarsproteins
plasma
intracellular fluid
7%
26%
67%

Definitions
• Solute• Solvent• Osmosis• Osmotic Pressure• Osmolarity• Hyperosmotic• Hypoosmotic

Solutes are dissolved particles in solution (any type)
• Osmotic pressure depends on the number of solutes/unit volume (rather than chemical nature of solutes)

As this column rises higher, it will exert increasing pressure. At some point that hydrostatic pressure will reach an equilibrium, at which pointno more net water will move across thesemi-permeable membrane.
This pressure is the ‘osmotic pressure’of the starting solution on the right.
Osmotic flux of water: --which way will the water move?-- Why is there net water flux tothe right?

isosmotic
Solutes are dissolved particles in solution (any type)
(osmotic pressure is equal)

Solutes are dissolved particles in solution (any type)
hypersmotic(higher osmotic pressure)
hyposmotic(lower osmotic pressure)

Water always moves from an area of low osmotic pressure to an area of high osmotic pressure
Hyposmotic (lower osmotic pressure)
Hyperosmotic (higher osmotic pressure)
osmotic pressure: the pressure of water to enter, given the solute concentration
Osmosis: movement of water from anArea with lower osmotic pressure to Higher osmotic pressure

Osmolarity= concentration of solutes in a solution
Osmolarity vs. Molarity:
150 mMol sucrose= 150 mOsm sucrose
150 mMol NaCl = 300 mOsm NaCl
Osmotic pressures are generally described in osmolar units:

Definitions
• Solute:• Solvent:• Osmosis:• Osmotic Pressure:• Osmolarity:• Hyperosmotic:• Hypoosmotic:
Dissolved particles in a solution
movement of water from an area with lower osmotic pressure to higher osmotic pressure the pressure of water to enter,
given the solute concentration
Concentration of solutes in a solution
Higher osmotic pressure
Lower osmotic pressure
What the particles are dissolved in

The Mammalian Kidney
glomerulus
Bowman’scapsule
Proximal tubule
Loop of Henle
Distal tubule
Collectingduct
To bladderExtracellular Na+ conc.
Passive movement of water
H2O
Active movement of Na+
Na+
HIGH
LOW

What it actually looks like
Bowman’s capsule
Distal tubuleProximal tubule
Loop of Henle
glomerulus
Collecting duct

Osmotic ImbalanceHypovolemia

Baroreceptors in arteries of the heart
Causing an increase in secretion and release
of VP
VP2 major effects:1. Vasoconstriction2. Water retention in kidney

Collecting Duct Cell
glomerulus
Bowman’scapsule
Proximal tubule
Loop of Henle
Distal tubule
Collectingduct
To bladder
Passive movement of water
H2
O
The water pore is a protein called:aquaporin 2 (AQP2)

Collecting Duct:
n n
filtrate
to bladder
Basal side of cellapical side
of cell
Lower Na+
Higher Na+
Extracellular space

Collecting Duct:n n
to bladder
Lower Na+
Higher Na+
No Vasopressin:
basal aquaporins
Aquaporin 2
H2O
H2O
H2O
Add Vasopressin:

Collecting Duct:n n
to bladder
Lower Na+
Higher Na+
basal aquaporins
Aquaporin 2
H2O
H2O
H2O
Add Vasopressin:

Collecting Duct Cross-Section
Cells labeled with fluorescent antibodies made to the water channel

n n
Collecting Duct:

Collecting Duct:
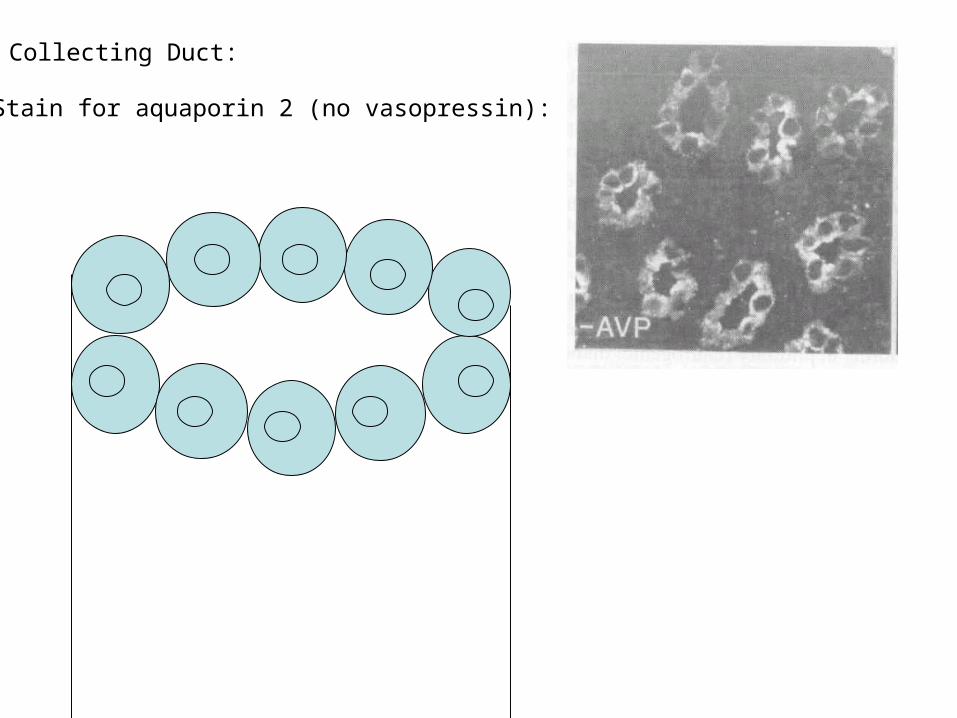
Stain for aquaporin 2 (no vasopressin):
Collecting Duct:

Collecting Duct:
Stain for aquaporin 2 (no vasopressin):
Add Vasopressin:

Collecting Duct:
Stain for aquaporin 2:
Add Vasopressin:

Collecting Duct:

2 major effects of vasopressin:1. Vasoconstriction2. Water retention in kidney:
Collecting Duct Cell
V2 receptor: localized to the kidney
VP
Gq
PLC
IP3
DAG
Smooth muscle cellIn arteries/capillaries
V1a receptor: localized to vascular smooth muscle cells
V1a receptorV2 receptor

Hypovolemia

Control of Aldosterone Secretion
ReninSecreted in response to low blood pressure
Cells in the capillary walls
ANGIOTENSIN I
ANGIOTENSIN II
angiotensin converting enzyme(ACE: secreted by the lungs)
IN THE BLOOD
ANGIOTENSINOGEN Made in the liver
aldosterone
Adrenal gland(cortex)

glomerulus
Bowman’scapsule
Proximal tubule
Loop of Henle
Distal tubule
Collectingduct
To bladderExtracellular Na+ conc.
Active movement of Na+
Na+
ALDOSTERONE:
Increases uptake of sodium from filtrate -Increases sodium in the blood -Decreases sodium in urine

Aldosterone and Angiotensin II productionIN THE BLOOD
ANGIOTENSINOGEN
ANGIOTENSIN I
ANGIOTENSIN II
angiotensin converting enzyme(ACE: secreted by the lungs)
Made in the liver
aldosteroneIncreases Na+ absorbtion in the kidney
Reninfrom glomerulus
Induce release of VP
Cause vasoconstriction
Stimulate drinking

REVIEW: hypovolemia
• Heart baroreceptors cause posterior pituitary to secrete VP– VP increases vasoconstriction– VP increases water pores in the
collecting duct, increasing water absorbtion from filtrate
• Cells in glomerulus secrete renin angiotensin II
• Increases aldosterone
• Increases vasoconstriction
• Increases VP
• Stimulates drinking
aldosterone• Increase sodium retention
A Decrease in Blood Pressure:

What about an increase in blood pressure?
• Baroreceptors in heart stop sending releasing signals to SON and PVN
• Glomerulosa cells produce less renin• Under conditions of excessively high blood
pressure:– The atria of the heart secrete Atrial Natriuretic
Peptide (ANP)– ANP:
• Shuts down secretion of VP, renin, and ALDO• Increases sodium excretion in the urine• Increases diuresis (water loss in urine)

Osmotic Imbalance

Osmoreceptors:-Present in cells in the hypothalamus-when dehydrated, cause secretion of VP from PVN and SON
VP
2 major effects:1. Vasoconstriction2. Water retention in kidney
Neural cells in hypothalamus containing osmoreceptors

Vasopressin and Osmolality

Angiotensin and Aldosterone?
Cells in the capillary walls
These cells are also sensitive to osmolality
-under low osmolality they secrete renin
-under high osmolality the shut down renin secretion

Under conditions of high osmolalityIN THE BLOOD
ANGIOTENSINOGEN
LESS ANGIOTENSIN I
LESS ANGIOTENSIN II
angiotensin converting enzyme(ACE: secreted by the lungs)
Made in the liver
LESS aldosteroneDecreases Na+ absorbtion in the kidney
LESS Renin from glomerulus
less VP
less vasoconstriction
less drinking

Osmotic Imbalance Review
• Osmoreceptors in the brain to signal SON and PVN nuclei to increase VP secretion– VP increases water retention in the
kidney
• Glomerular cells decrease secretion of Renin– Decrease Aldosterone secretion– Decrease Angiotensin II levels
High blood osmolality causes:

Pathophysiology of Osmoregulatory processes
• Adipsic hypernatremia– Dipsia is thirst, hypernatremia is high salt load– These patients do not have osmoreceptors in the brain, so they don’t
respond to hyperosmolality of the blood
No osmoreceptors in the brain
–No osmoreceptors, no VP secretion in response to cellular dehydration
–They need water, but they aren’t thirsty
–They do, however, have functional baroreceptors, and respond normally to changes in blood pressure

Pathophysiology of Osmoregulatory processes
• Adipsic hypernatremia– Dipsia is thirst, hypernatremia is high salt load– These patients do not have osmoreceptors in the brain, so they don’t
respond to hyperosmolality of the blood– No osmoreceptors, no VP secretion in response to cellular
dehydration– They need water, but they aren’t thirsty
• Diabetes Insipidus– Two types:
• Neurogenic DI:• Nephrogenic DI:

Neurogenic Diabetes Insipidus
VP is made but not transported
VP
1. no VP is secreted 2. Very little water is retained in the collecting duct Treatment with VP
can alleviate the problem

Nephrogenic Diabetes Insipidus
VP
Vasopressin is synthesized and secreted normally
Collecting Duct Cell
But there is a defect in the cellular mechanism that responds to VP

Pathophysiology of Osmoregulatory processes
• Adipsic hypernatremia– Dipsia is thirst, hypernatremia is high salt load– These patients do not have osmoreceptors in the brain, so they don’t
respond to hyperosmolality of the blood– No osmoreceptors, no VP secretion in response to cellular
dehydration– They need water, but they aren’t thirsty
• Diabetes Insipidus– Two types:
• Neurogenic DI: Problem with VP secretion• Nephrogenic DI: Problem with VP receptors in collecting duct
• Malignant hypertension

Pathophysiology of Osmoregulatory processes
• Adipsic hypernatremia– Dipsia is thirst, hypernatremia is high salt load– These patients do not have osmoreceptors in the brain, so they don’t
respond to hyperosmolality of the blood– No osmoreceptors, no VP secretion in response to cellular
dehydration– They need water, but they aren’t thirsty
• Diabetes Insipidus– Two types:
• Neurogenic DI: Problem with VP secretion• Nephrogenic DI: Problem with VP receptors in collecting duct
• Malignant hypertension– Causes a sudden and severe rise in blood pressure– Can lead to blindness, seizure, chest pain, heart failure

A B C
Hypothalamus
Posterior Pituitary