NSW INJURY RISK MANAGEMENT RESEARCH CENTRE · 2014-05-16 · NSW INJURY RISK MANAGEMENT RESEARCH...
84
NSW INJURY RISK MANAGEMENT RESEARCH CENTRE IRMRC Caroline Finch, Soufiane Boufous, Rebecca Dennis Sport/leisure injury hospitalisation episodes in NSW, 2003-2004: Socio- demographic and geographic patterns and sport-specific profiles SPORTS INJURY REPORT ll AUGUST 2007
Transcript of NSW INJURY RISK MANAGEMENT RESEARCH CENTRE · 2014-05-16 · NSW INJURY RISK MANAGEMENT RESEARCH...

NSW INJURY RISK MANAGEMENTRESEARCH CENTRE
IRM
RC
Caroline Finch, Soufiane Boufous, Rebecca Dennis
Sport/leisure injury hospitalisationepisodes in NSW, 2003-2004: Socio-demographic and geographic patternsand sport-specific profiles
SPO
RTS
INJU
RY R
EPOR
T llA
UG
US
T 2007

ISBN 978-0-9580633-9-5
Published by: NSW INJURY RISK MANAGEMENT RESEARCH CENTRE
UNSW, SYDNEY NSW 2052, AUSTRALIATelephone: +61 (2) 9385 4207 Facsimile: +61 (2) 9385 6040 http://www.irmrc.unsw.edu.au
Design and Production: Lawton Design pty ltd

List of Tables i
List of Figures vi
Acknowledgements vii
Executive Summary viii
Background 01
About This Report 02
Part A: Socio-Demographic and Geographic Characteristics of Sport/Leisure Hospitalisation
Episode Rates 05
A.1 INTRODUCTION 05
A.2 SOCIOECONOMIC STATUS 05
A.3 GEOGRAPHIC LOCATION 07
A.4 STATE MAPS 09
A.5 IMPLICATIONS 14
A.6 RECOMMENDATIONS 15
Part B: Coding Issues Associated With the Identification of Sport/Leisure Injuries 16
B.1 INTRODUCTION 16
B.2 ACTIVITY CODES AND THE IDENTIFICATION OF SPORT/LEISURE INJURIES 17
B.3 PLACE CODES AND THE IDENTIFICATION OF SPORT/LEISURE INJURIES 19
B.4 RELATIONSHIP BETWEEN ACTIVITY AND PLACE CODES 21
B.5 IMPLICATIONS OF THESE CODING ISSUES 24
B.6 RECOMMENDATIONS 25
Part C: Profiles of Injury Hospitalisation Episodes Associated with Selected Sport and
Leisure Activities 26
C.1 INTRODUCTION 26
C.2 SPORT SPECIFIC PROFILES 26
C.2.1. RUGBY (league and union) 26
C.2.2. SOCCER 30
C.2.3. CYCLING 34
C.2.4. SKATING AND BLADING 37
C.2.5. MOTORCYCLE RIDING 40
C.2.6. AUSTRALIAN FOOTBALL 43
C.2.7. EQUESTRIAN SPORTS 46
C.2.8. ICE AND SNOW SPORTS 48
C.2.9. BASKETBALL 51
C.2.10. NETBALL 54
C.3 IMPLICATIONS 56
C.4 RECOMMENDATIONS 57
References 58
Appendix 1: ICD-10-AM Codes 59
Appendix 2: Legends for the Maps of Sport/Leisure Injury Hospitalisation Episode Rates
and Counts, NSW, 2003-2004 66
Contents

Table A.1: Summary profile of sport/leisure injury hospitalisation episodes in Yallarooi, Walgett and Bland, 2003-2004, NSW residents 10
Table B.1: Distribution of activity codes across common categories of mechanisms of injury, NSW hospitalisation episodes of NSW residents, 2003-2004 18
Table B.2: Impact of different assumptions about the proportion of missing/unspecified activity codes that may be truly sports/athletics cases on the overall sport/leisure injury frequency estimates, NSW hospitalisation episodes, 2003-2004 19
Table B.3: Distribution of place codes across common categories of mechanisms of injury, NSW hospitalisation episodes, 2003-2004 20
Table B.4: Impact of different assumptions about the proportion of missing/unspecified place codes that may be truly sport/leisure cases on the overall sports/athletics injury frequency estimates, NSW hospitalisation episodes, 2003-2004 21
Table B.5: Proportion of NSW-based hospitalisation episodes of NSW residents identified as being associated with sports/athletics according to the ICD-10-AM activity and place codes, 2003-2004 22
Table C.1: Broad mechanisms leading to rugby injury hospitalisation, NSW, 2003-2004 27
Table C.2: Place of occurrence of incidents leading to hospitalisation episodes for rugby injury, NSW, 2003-2004 27
Table C.3: Nature of rugby injury associated with hospitalisation episodes, NSW, 2003-2004 27
Table C.4: Injured body regions associated with hospitalisation episodes for rugby injury, NSW, 2003-2004 28
Table C.5: Most commonly specified ICD external causes leading to hospitalised rugby injuries, NSW, 2003-2004 28
Table C.6: Most commonly specified ICD external causes of rugby upper limb injuries leading to hospitalisation, NSW, 2003-2004 28
Table C.7: Most commonly specified ICD external causes of rugby lower limb injuries leading to hospitalisation, NSW, 2003-2004 28
Table C.8: Most commonly specified ICD external causes of rugby head injuries leading to hospitalisation, NSW, 2003-2004 29
Table C.9: Most commonly specified ICD diagnosis codes for rugby injuries treated in hospital, NSW, 2003-2004 29
Table C.10: Most commonly specified ICD diagnoses associated with rugby upper limb injuries leading to hospitalisation, NSW, 2003-2004 29
Table C.11: Most commonly specified ICD diagnoses associated with rugby lower limb injuries leading to hospitalisation, NSW, 2003-2004 30
Table C.12: Most commonly specified ICD diagnoses associated with rugby head injuries leading to hospitalisation, NSW, 2003-2004 30
Table C.13: Broad mechanisms leading to soccer injury hospitalisation, NSW, 2003-2004 30
Table C.14: Place of occurrence of incidents leading to hospitalisation episodes for soccer injury, NSW, 2003-2004 30
Table C.15: Nature of soccer injury associated with hospitalisation episodes, NSW, 2003-2004 31
Table C.16: Injured body regions associated with hospitalisation episodes for soccer injury, NSW, 2003-2004 31
Table C.17: Most commonly specified ICD external causes leading to hospitalised soccer injuries, NSW, 2003-2004 31
Table C.18: Most commonly specified ICD external causes of soccer upper limb injuries leading to hospitalisation, NSW, 2003-2004 32
Table C.19: Most commonly specified ICD external causes of soccer lower limb injuries leading to hospitalisation, NSW, 2003-2004 32
Table C.20: Most commonly specified ICD external causes of soccer head injuries leading to hospitalisation, NSW, 2003-2004. 32
Table C.21: Most commonly specified ICD diagnosis codes for soccer injuries treated in hospital, NSW, 2003-2004 33
Table C.22: Most commonly specified ICD diagnoses associated with soccer upper limb injuries leading to hospitalisation, NSW, 2003-2004. 33
List
of
tabl
es
i

ii
Table C.23: Most commonly specified ICD diagnoses associated with soccer lower limb injuries leading to hospitalisation, NSW, 2003-2004 33
Table C.24: Most commonly specified ICD diagnoses associated with soccer head injuries leading to hospitalisation, NSW, 2003-2004 33
Table C.25: Broad mechanisms leading to cycling injury hospitalisation, NSW, 2003-2004 34
Table C.26: Place of occurrence of incidents leading to hospitalisation episodes for cycling injury, NSW, 2003-2004 34
Table C.27: Nature of cycling injury associated with hospitalisation episodes, NSW, 2003-2004 34
Table C.28: Injured body regions associated with hospitalisation episodes for cycling injury, NSW, 2003-2004 35
Table C.29: Most commonly specified ICD external causes leading to hospitalised cycling injuries, NSW, 2003-2004 35
Table C.30: Most commonly specified ICD external causes of cycling upper limb injuries leading to hospitalisation, NSW, 2003-2004 35
Table C.31: Most commonly specified ICD external causes of cycling lower limb injuries leading to hospitalisation, NSW, 2003-2004 35
Table C.32: Most commonly specified ICD external causes of cycling head injuries leading to hospitalisation, NSW, 2003-2004 36
Table C.33: Most commonly specified ICD diagnosis codes for cycling injuries treated in hospital, NSW, 2003-2004 36
Table C.34: Most commonly specified ICD diagnoses associated with cycling upper limb injuries leading to hospitalisation, NSW, 2003-2004 36
Table C.35: Most commonly specified ICD diagnoses associated with cycling lower limb injuries leading to hospitalisation, NSW, 2003-2004 36
Table C.36: Most commonly specified ICD diagnoses associated with cycling head injuries leading to hospitalisation, NSW, 2003-2004 37
Table C.37: Broad mechanisms leading to skating and blading injury hospitalisation, NSW, 2003-2004 37
Table C.38: Place of occurrence of incidents leading to hospitalisation episodes for skating and blading injury, NSW, 2003-2004 37
Table C.39: Nature of skating and blading injury associated with hospitalisation episodes, NSW, 2003-2004 38
Table C.40: Injured body regions associated with hospitalisation episodes for skating and blading injury, NSW, 2003-2004 38
Table C.41: Most commonly specified ICD external causes leading to hospitalised skating and blading injuries, NSW, 2003-2004 38
Table C.42: Most commonly specified ICD external causes of skating and blading upper limb injuries leading to hospitalisation, NSW, 2003-2004 38
Table C.43: Most commonly specified ICD external causes of skating and blading lower limb injuries leading to hospitalisation, NSW, 2003-2004 39
Table C.44: Most commonly specified ICD external cause of skating and blading head injuries leading to hospitalisation, NSW, 2003-2004 39
Table C.45: Most commonly specified ICD diagnosis codes for skating and blading injuries treated in hospital, NSW, 2003-2004 39
Table C.46: Most commonly specified ICD diagnoses associated with skating and blading upper limb injuries leading to hospitalisation, NSW, 2003-2004 39
Table C.47: Most commonly specified ICD diagnoses associated with skating and blading lower limb injuries leading to hospitalisation, NSW, 2003-2004 39
Table C.48: Most commonly specified ICD diagnoses associated with skating and blading head injuries leading to hospitalisation, NSW, 2003-2004 40
Table C.49: Broad mechanisms leading to motorcycle riding injury hospitalisation, NSW, 2003-2004 40
Table C.50: Place of occurrence of incidents leading to hospitalisation episodes for motorcycle riding injury, NSW, 2003-2004 40
Table C.51: Nature of motorcycle riding injury associated with hospitalisation episodes, NSW, 2003-2004 41
List of tables

Table C.52: Injured body regions associated with hospitalisation episodes for motorcycle riding injury, NSW, 2003-2004 41
Table C.53: Most commonly specified ICD external causes leading to hospitalised motorcycle riding injuries, NSW, 2003-2004 41
Table C.54: Most commonly specified ICD external causes of motorcycle riding upper limb injuries leading to hospitalisation, NSW, 2003-2004 42
Table C.55: Most commonly specified ICD external causes of motorcycle riding lower limb injuries leading to hospitalisation, NSW, 2003-2004 42
Table C.56: Most commonly specified ICD external causes of motorcycle riding head injuries leading to hospitalisation, NSW, 2003-2004 42
Table C.57: Most commonly specified ICD diagnosis codes for motorcycle riding injuries treated in hospital, NSW, 2003-2004 42
Table C.58: Most commonly specified ICD diagnoses associated with motorcycle riding upper limb injuries leading to hospitalisation, NSW, 2003-2004 42
Table C.59: Most commonly specified ICD diagnoses associated with motorcycle riding lower limb injuries leading to hospitalisation, NSW, 2003-2004 42
Table C.60: Most commonly specified ICD diagnoses associated with motorcycle riding head injuries leading to hospitalisation, NSW, 2003-2004 43
Table C.61: Broad mechanisms leading to Australian football injury hospitalisation, NSW, 2003-2004 43
Table C.62: Place of occurrence of incidents leading to hospitalisation episodes for Australian football injury, NSW, 2003-2004 43
Table C.63: Nature of Australian football injury associated with hospitalisation episodes, NSW, 2003-2004 43
Table C.64: Injured body regions associated with hospitalisation episodes for Australian football injury, NSW, 2003-2004 44
Table C.65: Most commonly specified ICD external causes leading to hospitalised Australian football injuries, NSW, 2003-2004 44
Table C.66: Most commonly specified ICD external causes of Australian football upper limb injuries leading to hospitalisation, NSW, 2003-2004 44
Table C.67: Most commonly specified ICD external causes of Australian football lower limb injuries leading to hospitalisation, NSW, 2003-2004 44
Table C.68: Most commonly specified ICD external causes of Australian football head injuries leading to hospitalisation, NSW, 2003-2004 45
Table C.69: Most commonly specified ICD diagnosis codes for Australian football injuries treated in hospital, NSW, 2003-2004 45
Table C.70: Most commonly specified ICD diagnoses associated with Australian football upper limb injuries leading to hospitalisation, NSW, 2003-2004 45
Table C.71: Most commonly specified ICD diagnoses associated with Australian football lower limb injuries leading to hospitalisation, NSW, 2003-2004 45
Table C.72: Most commonly specified ICD diagnoses associated with Australian football head injuries leading to hospitalisation, NSW, 2003-2004 46
Table C.73: Broad mechanisms leading to equestrian sports injury hospitalisation, NSW, 2003-2004 46
Table C.74: Place of occurrence of incidents leading to hospitalisation episodes for equestrian sports injury, NSW, 2003-2004 46
Table C.75: Nature of equestrian sports injury associated with hospitalisation episodes, NSW, 2003-2004 46
Table C.76: Injured body regions associated with hospitalisation episodes for equestrian sports injury, NSW, 2003-2004 47
Table C.77: Most commonly specified ICD external causes leading to hospitalised equestrian sports injuries, NSW, 2003-2004 47
Table C.78: Most commonly specified ICD external causes of equestrian sports upper limb injuries leading to hospitalisation, NSW, 2003-2004 47
Table C.79: Most commonly specified ICD external causes of equestrian sports lower limb injuries leading to hospitalisation, NSW, 2003-2004 47
Table C.80: Most commonly specified ICD external causes of equestrian sports head injuries leading to hospitalisation, NSW, 2003-2004 48
Table C.81: Most commonly specified ICD diagnosis codes for equestrian sports injuries treated in hospital, NSW, 2003-2004 48
List
of
tabl
es
iii

iv
Table C.82: Most commonly specified ICD diagnoses associated with equestrian sports upper limb injuries leading to hospitalisation, NSW, 2003-2004 48
Table C.83: Most commonly specified ICD diagnoses associated with equestrian sports lower limb injuries leading to hospitalisation, NSW, 2003-2004 48
Table C.84: Most commonly specified ICD diagnoses associated with equestrian sports head injuries leading to hospitalisation, NSW, 2003-2004 48
Table C.85: Broad mechanisms leading to ice and snow sports injury hospitalisation, NSW, 2003-2004 49
Table C.86: Place of occurrence of incidents leading to hospitalisation episodes for ice and snow sports injury, NSW, 2003-2004 49
Table C.87: Nature of injury associated with hospitalisation episodes for ice and snow sports injury, NSW, 2003-2004 49
Table C.88: Injured body regions associated with hospitalisation episodes for ice and snow sports injury, NSW, 2003-2004 49
Table C.89: Most commonly specified ICD external causes leading to hospitalised ice and snow sports injuries, NSW, 2003-2004 50
Table C.90: Most commonly specified ICD external causes of ice and snow sports upper limb injuries leading to hospitalisation, NSW, 2003-2004 50
Table C.91: Most commonly specified ICD external causes of ice and snow sports lower limb injuries leading to hospitalisation, NSW, 2003-2004 50
Table C.92: Most commonly specified ICD external causes of ice and snow sports head injuries leading to hospitalisation, NSW, 2003-2004 50
Table C.93: Most commonly specified ICD diagnosis codes for ice and snow sports injuries treated in hospital, NSW, 2003-2004 50
Table C.94: Most commonly specified ICD diagnoses associated with ice and snow sports upper limb injuries leading to hospitalisation, NSW, 2003-2004 51
Table C.95: Most commonly specified ICD diagnoses associated with ice and snow sports lower limb injuries leading to hospitalisation, NSW, 2003-2004 51
Table C.96: Most commonly specified ICD diagnoses associated with ice and snow sports head injuries leading to hospitalisation, NSW, 2003-2004 51
Table C.97: Broad mechanisms leading to basketball injury hospitalisation, NSW, 2003-2004 51
Table C.98: Place of occurrence of incidents leading to hospitalisation episodes for basketball injury, NSW, 2003-2004 52
Table C.99: Nature of basketball injury associated with hospitalisation episodes, NSW, 2003-2004 52
Table C.100: Injured body regions associated with hospitalisation episodes for basketball injury, NSW, 2003-2004 52
Table C.101: Most commonly specified ICD external causes leading to hospitalised basketball injuries, NSW, 2003-2004 52
Table C.102: Most commonly specified ICD external causes of basketball upper limb injuries leading to hospitalisation, NSW, 2003-2004 53
Table C.103: Most commonly specified ICD external causes of basketball lower limb injuries leading to hospitalisation, NSW, 2003-2004 53
Table C.104: Most commonly specified ICD external causes of basketball head injuries leading to hospitalisation, NSW, 2003-2004 53
Table C.105: Most commonly specified ICD diagnosis codes for basketball injuries treated in hospital, NSW, 2003-2004 53
Table C.106: Most commonly specified ICD diagnoses associated with basketball upper limb injuries leading to hospitalisation, NSW, 2003-2004 53
Table C.107: Most commonly specified ICD diagnoses associated with basketball lower limb injuries leading to hospitalisation, NSW, 2003-2004 54
Table C.108: Most commonly specified ICD diagnoses associated with basketball head injuries leading to hospitalisation, NSW, 2003-2004 54
Table C.109: Broad mechanisms leading to netball injury hospitalisation, NSW, 2003-2004 54
Table C.110: Place of occurrence of incidents leading to hospitalisation episodes for netball injury, NSW, 2003-2004 54
Table C.111: Nature of netball injury associated with hospitalisation episodes, NSW, 2003-2004 54
List of tables

List
of
tabl
es
v
Table C.112: Injured body regions associated with hospitalisation episodes for netball injury, NSW, 2003-2004 55
Table C.113: Most commonly specified ICD external causes leading to hospitalised netball injuries, NSW, 2003-2004 55
Table C.114: Most commonly specified ICD external causes of netball upper limb injuries leading to hospitalisation, NSW, 2003-2004 55
Table C.115: Most commonly specified ICD external causes of netball lower limb injuries leading to hospitalisation, NSW, 2003-2004 55
Table C.116: Most commonly specified ICD external causes of netball head injuries leading to hospitalisation, NSW, 2003-2004 56
Table C.117: Most commonly specified ICD diagnosis codes for netball injuries treated in hospital, NSW, 2003-2004 56
Table C.118: Most commonly specified ICD diagnoses associated with netball upper limb injuries leading to hospitalisation, NSW, 2003-2004 56
Table C.119: Most commonly specified ICD diagnoses associated with netball lower limb injuries leading to hospitalisation, NSW, 2003-2004 56
Table C.120: Most commonly specified ICD diagnoses associated with netball head injuries leading to hospitalisation, NSW, 2003-2004 56

vi
List of figuresFigure A.1 Age-standardised NSW-based sport/leisure hospitalisation rates across
quintiles of social disadvantage as defined by SEIFA codes, NSW residents hospitalised in NSW, all ages, 2003-2004 05
Figure A.2 Age-standardised NSW-based sport/leisure specific hospitalisation rates across quintiles of social disadvantage as defined by SEIFA codes, NSW residents hospitalised in NSW, all ages, 2003-2004 06
Figure A.3 Age-standardised NSW-based sport/leisure hospitalisation rates across regions as defined by ARIA codes, NSW residents hospitalised in NSW, all ages, 2003-2004 07
Figure A.4 Age-standardised sport/leisure specific hospitalisation rates across regions as defined by ARIA codes, NSW residents hospitalised in NSW, all ages, 2003-2004 08
Figure A.5 Age-standardised NSW-based sport/leisure injury hospitalisation rates per 100,000 population across NSW, by Local Government Areas (LGAs), 2003-2004 09
Figure A.6 Number of NSW-based sport/leisure injury hospitalisation episodes of NSW residents across NSW, by Local Government Areas, 2003-2004 11
Figure A.7 Age-standardised NSW-based sport/leisure injury hospitalisation rates of NSW residents per 100,000 population across Sydney region Local Government Areas, 2003-2004 12
Figure A.8 Number of NSW-based sport/leisure injury hospitalisation episodes of NSW residents across Sydney region Local Government Areas, 2003-2004 13
Figure B.1 NSW-based sports/athletics related drowning - relationship between activity and place codes 23
Figure B.2 NSW-based sports/athletics related overexertion and strenuous or repetitive movements - relationship between activity and place codes 23
Figure B.3 NSW-based sports/athletics related struck by/against - relationship between activity and place codes 23
Figure B.4 NSW-based sports/athletics related falls - relationship between activity and place codes 24

vii
Ack
now
ledg
emen
ts ACKNOWLEDGEMENTS
This project was funded by the NSW Sporting Injuries Committee (NSWSIC) under its Research andInjury Prevention Scheme.
Prof Caroline Finch was supported by an NHMRC Principal Research Fellowship. Dr SoufianeBoufous was supported by the NSWSIC Grant and the NSW Injury Risk Management ResearchCentre (IRMRC) Core Funding, which is provided by the NSW Department of Health, the NSWRoads and Traffic Authority and the NSW Motor Accidents Authority. Dr Rebecca Dennis wassupported by an NHMRC Population Health Capacity Building Grant in Injury Prevention, Traumaand Rehabilitation.
Prof Caroline Finch and Dr Rebecca Dennis worked on this report in their capacity as ProfessionalVisiting Fellow and Visiting Fellow in the NSW Injury Risk Management Research Centre (Universityof New South Wales (UNSW)), respectively. They both work full time in the School of HumanMovement and Sport Sciences at the University of Ballarat.
The hospitalisation episodes data, and information related to socio-economic status and geographiclocation were accessed via the NSW Department of Health's Health Outcomes InformationStatistical Toolkit (HOIST), maintained by the Centre for Epidemiology and Research.
The National Centre for Classification in Health provided the list of ICD-10-AM Third Editionexternal causes of injury codes reproduced in this report.
The authors also would like to thank Ms Shanley Chong for her contribution in preparing the mapsin this report and Ms Henny Oentojo for her work on preparing the manuscript.
Comments on the draft report were received with thanks from:
> Dr Carolyn Broderick (Sports Medicine Unit, UNSW)
> Ms Rosemary Green (NSW Sport and Recreation)
> Ms Sonya Jenkins (NSW Sporting Injuries Committee)
> A/Prof Andrew McIntosh (School of Safety Science, UNSW)
> Ms Claire Monger (NSW Health)
> Mr Mike Stratton (Australian Bureau of Statistics)
> Ms Karina Ryan (NSW Sporting Injuries Committee)
> A/Prof Ann Williamson (NSW Injury Risk Management Research Centre, UNSW)

viii
Executive Sum
mary
EXECUTIVE SUMMARY
Government and other agencies encourage participation in sport and other active pursuits for arange of reasons including improved health, reduced obesity levels and social and communitydevelopment. Unfortunately, if injuries occur during sport/leisure, there is a risk of both short andlong-term inactivity which could lead to these benefits not being realised. For this reason, it isimperative that all groups involved in encouraging sport and physical activity promote activity that issafe and encourage measures to reduce injury risk.
Planning for sports safety policy and injury prevention initiatives needs to be informed by high-quality, relevant data. Policy decisions need to be based on compelling arguments about the publichealth burden of health conditions and the lack of this information to date for NSW has meant thatsport/leisure injuries have not received the level of attention they perhaps deserve.
In 2006, we provided the first detailed epidemiological profile of severe sport/leisure injury in NSW;a rate of 190.3 hospitalised sport/leisure injuries per 100,000 population was reported for2003–2004. In response to the interest generated by the last report, this report now provides a moredetailed analysis of injury hospitalisation episodes associated with commonly represented categoriesof sport/leisure. In addition, social determinants of sport/leisure injury hospitalisation risk, as ameasure of health inequalities across all age groups, are presented for NSW for the first time. Thisinformation is important for the further identification of priority population groups and the targetingof injury prevention and sports medicine services.
This report provides:
1. information about socio-demographic and geographic characteristics of sport/leisure injury hospitalisation episodes in NSW, including maps of sports injury rates across the State (Part A);
2. an analysis of the relationships between the International Classification of Diseases (ICD) activity and place of injury coding systems for identifying sports injuries (Part B); and
3. a detailed profile of injuries associated with the ten sport/leisure activity groups most commonly associated with injury hospitalisation episodes (Part C).
The focus of this report is solely on injuries associated with admission episodes to hospital in NSWduring the two year period 2003–2004. It does not include interstate hospitalisations of NSWresidents.
There has been increasing recognition of the impact of social disadvantage on the rate of injuries inAustralia. However, the impact of health inequalities on the incidence of sport/leisure injuries acrossall ages has not been examined in detail to date. Part A of this report examines the relationshipbetween selected socio-demographic and geographic characteristics of the incidence of sport/leisurehospitalisation episodes across the entire NSW population for the first time. Maps across the state ofNSW are presented to highlight geographic variations in sport/leisure injury hospitalisation episodes.
A very strong rurality gradient in sports/leisure injury hospitalisation episodes rates across the state ofNSW was identified, with people resident in remote and very remote areas having a significantlyhigher rate. In contrast, there was no clear relationship between socioeconomic status andsport/leisure hospitalisation rates across sports, though rates were significantly higher towards thedisadvantaged end of the scale. Reasons for this may include differences in sporting/leisureinfrastructure across regions. An alternative explanation could be differential participation in sportacross regions.
In 2003-2004, there were high numbers of sport/leisure injury hospitalisation cases in metropolitanSydney and the east coast of NSW. Whilst these high numbers are related to the population levels inthose areas, and the associated level of participation in sport/leisure, they do have implications forhealth service delivery in these areas.
Sports/leisure injury cases were identified on the basis of ICD-10-AM activity codes. The ICD-10-AM also allows for the coding of place of occurrence of injury, which includes, among othercategories, sports/athletics areas. However, the relationship between the activity codes indicatingsport/leisure activities and place of occurrence codes indicating sports/athletics areas has not beenpreviously reported. Part B of this report presents a sensitivity analysis of the range of possibleimpacts that the underreporting of activity codes, has on estimates of the frequency of sports injuryhospitalisation episodes. It also explores the relationship between the activity and place codes forthe identification of sports/leisure injuries, including an assessment of the degree of concordancebetween the two sets of codes.

ix
Exec
utiv
e S
umm
ary Unfortunately, not all hospitalisation episodes have valid activity codes assigned to them. This
almost certainly means that the number of sport/leisure injury hospitalisation episodes identified onthe basis of activity codes, is an underestimate. After adjusting for potential underreportingassociated with undefined activity codes, it is likely that sport/leisure injuries may really account forup to one in five injury hospitalisation episodes and over 40% of all overexertion and strenuous orrepetitive movements, drowning and struck by/against hospitalisation episodes. Selecting sportsinjuries on the basis of activity codes alone, yields a larger number of cases than a place-basedselection criterion. Together, these data issues highlight limitations in the ability to identify allpriority sports/leisure activity injuries based on ICD-10-AM codes for the identification anddevelopment of appropriate injury prevention strategies.
Part C of this report provides a detailed profile of the ten sport/leisure activity groups most commonlyassociated with hospitalisation episodes due to injury. This profile includes information pertaining tothe mechanism, place of occurrence, nature, body region, diagnosis and external cause of injuryacross each of the ten sports. The ten categories of sport/leisure activity focussed on are, in order ofdecreasing frequency: rugby (league and union), soccer, cycling, motorcycling, skating/rollerblading,Australian football, equestrian sports, ice and snow sports, basketball and netball. The relatively highnumber of missing cases (i.e. activity and place of injury codes) and unspecified codes suggest thatfurther improvements to ICD-10-AM coded routine data relating to sport/leisure injuries is needed.
RECOMMENDATIONS
For sports safety practice
1. The profiles of injury associated with specific sport/leisure activities should be presented to therelevant State Sporting Associations and the implications of the findings discussed with them.
2. It is well known that sport/leisure hospitalisations represent fewer than 30% of all sports injurycases. Given the number of hospitalisations highlighted in this report, it is likely that there aremany more cases that do not receive treatment at a hospital. These high numbers of sportinginjuries may warrant a review by organisations such as the NSW Sporting Injuries Committee andSports Medicine Australia of the delivery and availability of community-wide sports medicineservices aimed at treating moderate injuries, including those focusing on prevention both inclinical settings and directly linked to sports delivery systems across metropolitan Sydney and theeast coast of NSW.
For priority target groups
1. The high excess rate of sport/leisure injury in remote and very remote areas needs consideration.Further investigations are justified into determining why these areas have such high rates,identifying what the major issues may be and exploring what infrastructure needs and otherlocally-based issues could be addressed to reduce injury rates in these areas. Collection ofappropriate participation data to determine if the high rates are due to large numbers ofparticipants or to an increased injury risk in these areas will be important.
2. Sport/leisure injury rates should continue to be monitored across social/demographic groups. Amajor gap is information about how rates differ in areas with a high Aboriginal population.Research is required to quantify sports participation rates and describe the nature and extent ofsports injuries amongst Aboriginal people.
For identifying sports injury cases based on ICD-coded data
1. Future studies using ICD-10-AM coded routine data collections should continue to use theactivity variable to select sport/leisure cases.
2. Estimates of sport/leisure frequency based on such data need to be recognised as being anunderestimate of the true frequency.
3. Those interested in hospitalisation rates for injuries related to rugby need to be aware that rugbyleague and rugby union are often not differentiated in the hospitalisation data, despite specificICD-10-AM activity codes being available for each type of rugby. It would be useful to identifythe reasons why there are relatively large numbers of "rugby unspecified" coded cases in areaswhere both forms of football are popular, as this lack of specificity limits the information forpreventive purposes.

x
Executive Sum
mary
For improvements to data collection and coding practices
Sports participation data
1. Bodies such as the Australian Bureau of Statistics and the NSW Sporting Injuries Committee couldgive consideration towards the collection and reporting of sports participation survey data across Local Government Areas (LGAs) so that regional estimates of injury rates can be adjusted for participation in sport/leisure activities and not just for population density.
Routinely collected hospitalisation data
1. Improvements in the information recorded for cases of sport-related hospitalisation in routinelycollected hospitalisation data appear warranted. The identification of sport/leisure relatedhospitalisation depends upon the recording of accurate and specific information about the natureof the activity being undertaken at the time of injury. In addition, specific information about themechanism (external cause) of an injury and the type of place where the injury occurred is ofgreat value to injury prevention efforts. Reasons for the relatively high levels of missing orunspecified activity and place information need to be determined to identify what solutions couldbe implemented to address these information gaps.
ICD-10-AM coding
1. Further refinement of ICD-10-AM codes may be required to enable data coders to more easilyclassify the activity being undertaken at the time of injury as well as the type of place in whichthe injury occurred. Given the strong association of the causes of sports injuries with the externalcause categories of overextention and strenuous or repetitive movements, drowning and struckby/against, efforts should perhaps first be directed at these categories. The detail and quality ofinformation available to coders from hospital medical records will need to be considered.
2. Continued development of the ICD-10-AM codes should include consultation with experts in theuse and interpretation of sport/leisure injury data to ensure that coding guidelines and trainingprocedures enable the recorders and coders to more easily classify the activity being undertakenat the time of injury.
3. Consideration could be given to enhancements to the ICD-10-AM coding procedures that wouldallow the phase of play/actual activity at the time of injury to be reported (such as during trainingor in competitive games) and for the type of activity to be properly differentiated betweenorganised sport, informal sport and general play.

01
Bac
kgro
und BACKGROUND
Government and other agencies encourage participation in sport and other active pursuits for arange of reasons including improved health, reduced obesity levels and social and communitydevelopment. Unfortunately, if injuries occur during sport/leisure, there is a risk of both shortand long-term inactivity which could lead to these benefits not being realised. For this reason,it is imperative that all groups involved in encouraging sport and physical activity promoteactivity that is safe and encourage measures to reduce injury risk.
Planning for sports safety policy and injury prevention initiatives needs to be informed by high-quality, relevant data. Like most other jurisdictions across Australia, New South Wales (NSW)does not currently have a systematic reporting of sport/leisure injury trends across the broadcommunity level. This means that there are no overarching estimates of sport/leisure injuryrates across the state nor identification of sport/leisure injury priority attention areas, from ahealth inequalities perspective. Policy decisions need to be based on compelling argumentsabout the public health burden of health conditions (generally in terms of mortality andhospitalisation episodes) and the lack of this information for NSW has meant that, to date,sport/leisure injuries have not received the level of attention they perhaps deserve.
At present, in NSW, as in other Australian states and territories, only deaths and hospitalisationepisodes relating to sport/leisure can be routinely identified and monitored over time toprovide population estimates of the incidence of sport/leisure injuries. In 2006, we providedthe first detailed epidemiological profile of severe sport/leisure injury in NSW (A profile ofhospitalisation episodes and deaths due to sport and leisure injuries in New South Wales, 2000-2004) [1]. Injury data were obtained from existing routine databases that contain informationon sport/leisure related deaths and hospitalisation episodes in NSW. Mortality data wereobtained from the Australian Bureau of Statistics' deaths dataset for the three-year period 2000-2002 and information pertaining to hospitalisation episodes was retrieved from the NSWInpatient Statistics Collection for the two calendar-year period 2003-2004.
The previous report presented an overall mortality rate of 0.85 deaths per 100,000 populationduring the three year period. The death rate for males was almost four times higher than infemales and people aged 15-24 years had the highest age-specific rate of death in sport; peopleaged over 35 years had the highest age-specific rate of death in leisure activities. In addition, arate of 190.3 hospitalised sport/leisure injury episodes per 100,000 population was reported for2003-2004, with similar age and sex differentials.
In response to the interest generated by the last report, this report now provides a moredetailed analysis of injury hospitalisation episodes associated with commonly representedcategories of sport/leisure. In addition, the socio-demographic and geographic characteristicsof injury risk, as a measure of health inequality, are presented for NSW for the first time. Thisinformation is important for the further identification of priority population groups for thetargeting of injury prevention and sports medicine services.

02
About This R
eport
ABOUT THIS REPORT
This report is the second in a series presenting an epidemiological profile of serious injuriesrelated to participation in sport/leisure activities in NSW. The first report in the series,published in 2006 (A profile of hospitalisation episodes and deaths due to sport and leisureinjuries in New South Wales, 2000-2004), provided estimates of the population-level rate ofserious sport/leisure injury incidence in NSW in terms of deaths and hospitalisation episodesand compared sport/leisure injury rates in particular subgroups of interest, such as males versusfemales and different age groups.
The objectives of this report are to provide:
1. information about socio-demographic and geographic characteristics of sport/leisure injuryhospitalisation episodes in NSW, including maps of sports injury rates across the State (Part A);
2. an analysis of the relationships between the International Classification of Diseases (ICD)activity and place of injury coding systems for identifying sports injuries (Part B); and
3. a detailed profile of injuries associated with the ten sport/leisure activity groups mostcommonly associated with injury hospitalisation episodes (Part C).
INJURY DATA USEDThe focus of this report is solely on injuries associated with admission to hospital in NSW. Itdoes not include interstate hospitalisations of NSW residents. While it is recognised that suchinjuries only represent a small amount of the overall burden of all relevant injuries [2], they areamong the most serious of all sport/leisure injuries and should therefore be the target of injuryprevention strategies, at least in the first instance.
Injury hospitalisation episode data were extracted from routinely collected datasets from theHealth Outcomes Information Statistical Toolkit (HOIST) provided by the Centre forEpidemiology and Research, NSW Health.
The NSW Inpatient Statistics Collection (ISC) includes details of all hospitalisation episodes inNSW. It records all inpatient separations (discharges, transfers and deaths) from all public,private and repatriation hospitals, private day procedures centres and public nursing homes inNSW. Hospitals are required to submit details for every inpatient and for every episode of care.An episode of care either ends by the patient ending a period of stay in hospital (by discharge,transfer or death) or by the patient becoming a different type of patient within the same periodof stay in hospital (e.g. the patient is admitted for an acute injury then later becomes arehabilitation patient) [3].
Due to the nature of the hospital data, the number of hospital episodes for sport/leisure injuriesis not equivalent to the number of incident cases. Patients who had been readmitted ortransferred from one hospital to another for treatment of the same injury, in some instanceseven within the same hospital, may be recorded more than once. In the absence of a directmeans to identify incident cases in the dataset, we have used the 'mode of separation' variableto exclude transfers and statistical discharges or transfers within the same hospital in order tominimise multiple counting of cases relating to the same injury incident.
The ICD-10-AM third edition was used to select appropriate cases for the analyses in thisreport. Cases selected included all NSW-based hospital separations in NSW, of NSW residentsof any age, with an ICD-10-AM principal diagnosis indicating an injury (S00-T35, T66-T71,T73, T75, T95-T99) and an 'Activity at the time of injury' code referring to sport/leisure activity(U50-U72) [4]. This version of the ICD-10-AM includes over 200 different categories providedby the ICD-10-AM 'activity while injured'. This definition of injury excludes poisonings.
Data extraction was restricted to the two calendar years of 2003-2004, due to the availabilityof full calendar year data at the time of preparing this report. The data for the last six months of2004 was coded according to the fourth edition of the ICD-10-AM but this is unlikely to haveimpacted on case selection.
A detailed list of all ICD-10-AM third edition activity codes used to select cases is provided inAppendix 1. Cases assigned these codes were included on the assumption that the majority ofinjury cases they select would be related to participation in a sport/leisure activity. Forexample, cycling was included, as it was assumed the majority of cases would be related toparticipation in cycling as a sport/leisure activity, rather than to transportation for work. Thisassumption has been used in previous analyses of sports injury cases treated at hospital.

03
Abo
ut T
his
Rep
ort CALCULATION OF HOSPITALISATION RATES
The frequency and rates of sport/leisure hospitalisation episodes were calculated in each yearand in subgroups of interest, such as age, gender and sport/leisure type. The denominators usedwere the mid-year NSW population estimate (in the relevant age/gender subgroup) obtainedfrom the Australian Bureau Statistics (ABS). Year-specific hospitalised rates were agestandardised to the 2001 Australian population to adjust for any differences that may havearisen from a change in the age structure of the population [3]. All of the population data, usedin both numerators and denominators, were restricted to NSW residents.
Ninety-five percent confidence intervals (95% CI) were calculated for various rates. Cells withtotal case numbers less than five have not been shown in the tables in order to maintainconfidentiality. All analyses were carried out using SAS, version 8.02 [5].
SPORT SPECIFIC INJURY PROFILESThe ten sport/leisure categories with the highest population-adjusted hospitalisation rates wereidentified from Table 9 of the previous report [1]. Hospitalisation episodes for each of thesecategories are described in detail in Part C to demonstrate the particular priorities forprevention in each of these activities. All data is given as frequencies, or the proportion of thetotal number of cases, associated with a given sport.
SOCIO-DEMOGRAPHIC CHARACTERISTICS OF SPORT/LEISURE INJURYStandardised hospitalisation rates for all sport/leisure activities, as well as for the ten mostcommonly injury associated sports/activities in 2003-2004, were examined by socioeconomicstatus (SES) and remoteness of various geographical areas in NSW, for NSW residents only.
Socioeconomic status Socioeconomic status was derived from the Socio-Economic Indexes for Areas (SEIFA) which isbased on data from the 2001 ABS population census. The SEIFA is a composite measurederived from multiple weighted variables relating to education, occupation, ethnicity and theeconomic resources of households [6]. The SEIFA is derived from attributes such as income,education, employment, occupation, and variables that measure aspects of disadvantage (e.g.number of bedrooms in home; rental versus home ownership) as well as variables that areassociated with disadvantage (e.g. the proportion of indigenous persons, single parent families,etc) [6]. It is a single score available for any configuration of geographical census areas, withlower scores indicating lower SES.
The ABS divides NSW into 198 statistical local areas (SLAs). Sport/leisure injury hospitalisationepisodes were assigned to SLAs on the basis of the usual residence of the injured person. Thetotal number of cases, and the age standardised rate, for each SLA was calculated for theperiod 2003-2004. The SLAs were then ranked into one of five quintiles, such that eachquintile contained approximately 20% of the total population of NSW (Part A).
NSW residents hospitalised in other states/territories have been excluded from these analyses.
LocationThe Accessibility/Remoteness Index of Australia (ARIA) is an index of the accessibility of placesto service centres, or conversely of remoteness of places. Population localities are given a score(from 0 to 15) based on the road distance to service towns of different sizes. Scores for regionsare derived by averaging scores for localities [7]. The index scores are classified into thefollowing categories according to the SLA of residence:
> Highly Accessible (Major Cities of Australia): average Accessibility/Remoteness Index of Australia (ARIA) index value of 0 to 0.2
> Accessible (Inner Regional Australia): average ARIA index value >0.2 and < 2.4
> Moderately Accessible (Outer Regional Australia): average ARIA index value >2.4 and <5.92
> Remote Australia: average ARIA index value >5.92 and < 10.53
> Very Remote Australia: average ARIA index value >10.53
Age-standardised sport/leisure injury hospitalisation rates were calculated for each of the fiveARIA categories for NSW residents hospitalised in NSW (Part A).

04
About This R
eport
MapsAge-standardised hospitalisation rates for all sport/leisure activities by gender, 2003-2004, werecomputed for each SLA across the state and for each Statistical Sub Division (SSD) in theSydney metropolitan region. These areas were then modified to the corresponding LocalGovernment Areas (LGAs) and presented in the form of maps using Mapinfo software [8].MapInfo was also used to generate the appropriate shading categories for the maps.
CODING ISSUESAs a follow-up to some of the ICD-10-AM activity and place coding issues identified on page25 of the previous report [1], a sensitivity analysis of the range of possible impacts that theunderreporting of activity codes in general, has on estimates of the frequency of sports injuryhospitalisation episodes is presented. All data are presented as the proportion of allhospitalisation episodes in NSW in 2003-2004 or the proportion of all cases identified as asport/leisure hospitalisation, as appropriate (Part B).

05
Par
t A
: S
ocio
-Dem
ogra
phic
and
Geo
grap
hic
Cha
ract
eris
tics
of
Spo
rt/L
eisu
re H
ospi
talis
atio
n Ep
isod
e R
ates PART A: SOCIO-DEMOGRAPHIC AND GEOGRAPHIC CHARACTERISTICS OF
SPORT/LEISURE HOSPITALISATION EPISODE RATES
A.1 INTRODUCTIONThere has been increasing recognition over recent years that health inequalities, as measuredby various measures of social disadvantage, have an impact on the rate of both fatal and nonfatal injuries in Australia [9-11]. However, the impact of health inequalities on the incidence ofsport/leisure injuries has not been examined in detail to date.
Only one Australian study has previously examined socioeconomic and geographic differenceson sport/leisure-related injury [12]. This NSW-based study considered ICD-9 codedhospitalisation episodes in people aged 5-19 years, for the period 1996 to 2000. A limitationof the study was that it used ICD-9 codes for sports injuries, which are known to underenumerate the numbers of sport/leisure injuries, relative to the ICD-10-AM codes we have usedin this report. The earlier study found no association between socioeconomic status andsport/leisure-related hospitalisation episodes. In contrast, it identified a significantly higher riskof hospital admission in people from rural areas, than those in metropolitan areas. This isconsistent with previous views that sport/leisure injury rates were likely to be higher in ruralareas [13].
The aim of this part of the report is to provide an examination of the relationship betweenselect socio-demographic and geographic characteristics of health and the incidence ofsport/leisure hospitalisation episodes across the entire NSW population for the first time. Theindices used have been described on page 4 and include both measures of social disadvantageand remoteness. Finally, maps across the state of NSW are presented to highlight geographicvariations in sport/leisure injury hospitalisation episodes. In all cases, the geographic locationis based on the place of usual residence of the injured case.
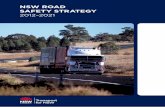
A.2 SOCIOECONOMIC STATUSFigure A.1 presents the overall sport/leisure injury hospitalisation rates across the state of NSW,for all ages, across quintiles of SES. The first quintile represents areas of most disadvantage andthe fifth quintile areas of least disadvantage. There is no clear trend between the SEIFA indexand sport/leisure hospitalisation rates. Across quintiles the rates of sport/leisure hospitalisationrange from a low of 150.3/100,000 population in the quintile of most disadvantage to a high of201.8/100,000 population in the middle quintile. The rates of hospitalised sport/leisure injurywere significantly higher in the second and third quintile groups, than all other groups.Residents from the most disadvantaged areas had hospitalisation rates similar to those from the4th quintile of disadvantage (i.e. more advantaged people).
Figure A.1 Age-standardised NSW-based sport/leisure hospitalisation rates across quintiles ofsocial disadvantage as defined by SEIFA codes, NSW residents hospitalised inNSW, all ages, 2003-2004.
1st quintile = most disadvantaged 5th quintile = least disadvantaged
150.3
197.4 201.8
147.4
172.1
0
50
100
150
200
250
1st quintile 2nd quintile 3rd quintile 4th quintile 5th quintile
SEIFA quintiles
Rat
e pe
r 10
0,00
0 po
pula
tion
0.00
50.0
100.
150.
200.
250.
1st quintile = most disadvantaged, 5th quintile = least disadvantaged95% confidence intervals for rates shown

06
Part A
: Socio-D
emographic and G
eographic Characteristics of
Sport/Leisure H
ospitalisation Episode Rates
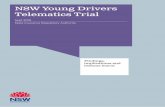
Figure A.2 shows selected sport/leisure category specific hospitalised injury rates across SEIFAcategories. Generally, the trend across the sports categories is similar to the overall trend. Thethree sport/leisure activities where the most advantaged people have the higher rates ofhospitalised injury than all others are ice/snow sport, soccer and netball. The differential acrossSEIFA categories was greatest for rugby injuries.
Figure A.2 Age-standardised NSW-based sport/leisure specific hospitalisation rates acrossquintiles of social disadvantage as defined by SEIFA codes, NSW residents hospitalised in NSW, all ages, 2003-2004.
0 5 10 15 20 25 30
Rugby
Soccer
Motorcycling
Cycling
Skating/blading
Equestrian
Australian football
Basketball
Ice/snow sports
Netball
5th quintile 4th quintile 3rd quintile 2nd quintile 1st quintile
Rate per 100,000 population
Spor
t/le
isur
e ac
tivi
ty
5th quintile 4th quintile 3rd quintile 2nd quintile 1st quintile
1st quintile=most disadvantaged, 5th quintile=least disadvantaged

02
Par
t A
: S
ocio
-Dem
ogra
phic
and
Geo
grap
hic
Cha
ract
eris
tics
of
Spo
rt/L
eisu
re H
ospi
talis
atio
n Ep
isod
e R
ates A.3 GEOGRAPHIC LOCATION
Figure A.3 presents the overall all-age sport/leisure injury hospitalisation rates across the state ofNSW, across ARIA categories. These ARIA categories can be interpreted as covering major cities,inner regional areas, outer regional areas, remote and very remote areas, respectively.
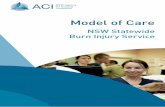
There is a strong positive relationship between the sport/leisure hospitalisation rates and increasingrurality as shown by comparisons of the confidence intervals for the rates across ARIA categories.The rates of sport/leisure hospitalisation range from a low of 156.2/100,000 population in the mosturban areas to a high of 335.5/100,000 population in remote areas. Even though they are based onsmaller numbers of cases (as shown by the wider confidence limits), the rates of hospitalisedsport/leisure injury are significantly higher in remote and very remote areas than in other parts of thestate.
07
Figure A.3 Age-standardised NSW-based sport/leisure hospitalisation rates across regions asdefined by ARIA codes, NSW residents hospitalised in NSW, all ages, 2003-2004.
Highly
accessible Accessible Moderately
accessible Remote Very
remote
Rat
e pe
r 10
0,00
0 po
pula
tion
400
350
300
250
200
150
100
50
0
ARIA groups95% confidence intervals for rates shown
The ARIA-specific rates for selected sport/leisure categories are shown in Figure A.4. For most sports,there is no clear relationship with ARIA. The exception to this is Australian Football when injury ratesgenerally increased with increasing remoteness. The two sports with the highest rates of injuries invery remote communities are cycling and soccer. The former may represent a higher risk of injury ona road network that is less well maintained than that in high traffic areas or longer distancestravelled. Soccer also is the only sport to have higher rates of injury in highly accessible areas.

03
Part A
: Socio-D
emographic and G
eographic Characteristics of
Sport/Leisure H
ospitalisation Episode Rates
08
Figure A.4 Age-standardised sport/leisure specific hospitalisation rates across regions asdefined by ARIA codes, NSW residents hospitalised in NSW, all ages, 2003-2004.
0 10 20 30 40 50 60 70
Rugby
Soccer
Motorcycling
Cycling
Skating/blading
Equestrian
Australian football
Basketball
Ice/snow sports
Netball
Very remote Remote Moderately Accesible
Accessible Highly accessible
Rate per 100,000 population
Spor
t/le
isur
e ac
tivi
ty
Spor
t/le
isur
e ac
tivi
ty
Rate per 100,000 population

09
Par
t A
:Soc
io-D
emog
raph
ic a
nd G
eogr
aphi
c C
hara
cter
isti
cs o
f S
port
/Lei
sure
Hos
pita
lisat
ion
Epis
ode
Rat
es
Figure A.5 Age-standardised NSW-based sport/leisure injury hospitalisation rates per 100,000 population across NSW, by Local Government Areas (LGAs), 2003-2004.
A.4 STATE MAPS
Figure A.5 shows age-standardised sport/leisure injury hospitalisation rates in each of the 164LGAs across NSW. Just under half of all LGAs (46.4%) had sport/leisure injury rates in therange 0-200/100,000 population; 38.4% (n=61) had rates in the range 200-300/100,000 and11.7% (n=22) had rates in the range 300-500/100,000 population; 3 LGAs had rates in therange 500-850/100,000.
Three non-metropolitan LGAs had particularly high rates (range: 500 to 850 per 100,000population): Yallaroi (161 on the map), Walgett (149 on the map) and Bland (16 on the map).Table A.1 provides a summary of the types of injury cases in these three areas. It should benoted that rates tend to be more variable and unstable in smaller areas and so these area-specific results need to be interpreted with caution.
Refer to Appendix 2 for LGA labels.In the legend, the bracketed numbers give the number of LGAs in each range

10
Part A
: Socio-D
emographic and G
eographic Characteristics of
Sport/Leisure H
ospitalisation Episode Rates
The greatest proportion of LGAs (30.1%) had 0-30 injury cases (Figure A.6). However, the nexthighest proportion (22.6%, n=42 LGAs) had counts between 220 and 1140 sport/leisurehospitalisation episodes over the two year period. Eight percent (14) of LGAs had 30-40 cases,17.7% (n=29) had 40-90 cases and the remaining 21.3% (n=35) were associated with 90-220cases. Comparison of Figure A.5 and Figure A.6 shows that none of the three LGAs with highrates also had a high number of sport/leisure hospitalisation episodes during 2003–2004.
Most of the LGAs with very high counts of sport/leisure hospitalisation episodes were fromalong the east coast of the state and metropolitan Sydney (Figure A.6 and A.8). Comparisons ofFigure A.5 with Figure A.7 and Figure A.6 with Figure A.8, shows that these large counts can beaccounted for by population size and are therefore unlikely to be related to particularlyhazardous environments or participation contexts in those areas.
Table A.1: Summary profile of sport/leisure injury hospitalisation episodes in Yallarooi, Walgettand Bland, 2003-2004, NSW residents.
Yallarooi (n=35) Walgett (n=132) Bland (n=89) Gender male 78 79 65 Age 0-14 years 35 33 21 15-34 years 44 47 42 35+ years 21 20 27 Sport/leisure activity 1st ranked Rugby (17) Leisure, nec (20) Leisure, nec (74) 2nd ranked # Soccer (13) Rugby (7) 3rd ranked # Cycling (11) #
all figures are % of the total cases
nec= not elsewhere classified; #= fewer than 5 cases

11
Par
t A
: S
ocio
-Dem
ogra
phic
and
Geo
grap
hic
Cha
ract
eris
tics
of
Spo
rt/L
eisu
re H
ospi
talis
atio
n Ep
isod
e R
ates
Figure A.6 Number of NSW-based sport/leisure injury hospitalisation episodes of NSW residents across NSW, by Local Government Areas, 2003–2004.
Refer to Appendix 2 for LGA labels.In the legend, the bracketed numbers give the number of LGAs in each range.
Figures A.7 and A.8 show detailed maps for the Sydney metropolitan region. None of themetropolitan LGAs had a very high sport/leisure injury hospitalisation rate in 2003–2004. TheLGAs with the highest rates were Wollongong (158 on the map) and Manly (97 on the map). Incontrast, many of the metropolitan LGAs had high injury counts, reflecting their population size(Figure A.8). Three metropolitan LGAs had relatively low counts: Clarence Valley (36 on themap), Burwood (21 on the map) and Hunters Hill (76 on the map).

12
Part A
: Socio-D
emographic and G
eographic Characteristics of
Sport/Leisure H
ospitalisation Episode Rates
Figure A.7 Age-standardised NSW-based sport/leisure injury hospitalisation rates of NSWresidents per 100,000 population across Sydney region Local Government Areas,2003–2004.
Refer to Appendix 2 for LGA labels.In the legend, the bracketed numbers give the number of LGAs in each range.

13
Par
t A
: S
ocio
-Dem
ogra
phic
and
Geo
grap
hic
Cha
ract
eris
tics
of
Spo
rt/L
eisu
re H
ospi
talis
atio
n Ep
isod
e R
ates
Figure A.8 Number of NSW-based sport/leisure injury hospitalisation episodes of NSW residents across Sydney region Local Government Areas, 2003–2004.
Refer to Appendix 2 for LGA labels.In the legend, the bracketed numbers give the number of LGAs in each range.

14
Part A
: Socio-D
emographic and G
eographic Characteristics of
Sport/Leisure H
ospitalisation Episode Rates
A.5 IMPLICATIONS
This section has described sport/leisure hospitalisation rates across sub-groups of the totalpopulation of NSW. A particular strength of the analysis is the fact that it has a large populationbase and covers all hospitalisation episodes in both the public and the private hospital systemin NSW. Differential access to hospital care on the basis of SES is unlikely, since data fromboth the public and private systems have been included, and because everyone has access tofree public hospital inpatient care under the Medicare system.
Some caution needs to be given when interpreting the results, however. Injuries wereattributed to the area of usual residence of the injured person, but may have occurred inanother location with a different level of disadvantage, and by inference, social andenvironmental risk factors. We based our analyses on SLAs, even though they do notrepresent socioeconomically homogenous areas. Smaller areas, such as collector districts,would have been preferable, but data at this level are currently unavailable. Use of SLAs in ourstudy may therefore have masked larger gradients in injury rates.
Interstate hospitalisations of NSW residents were not included in the analysis. This may havehad an impact on the total number of injury hospitalisation episodes, particularly amongresidents of LGAs on the NSW border. However, this impact is likely to be small as usuallyfewer than 2% of all hospitalisations of NSW residents occur outside NSW.
The major finding is a very strong rurality gradient in sports/leisure injury hospitalisation ratesacross the state of NSW, with people resident in remote and very remote areas having asignificantly higher rate. The difference has implications because people from remote areashave less access to health facilities and are less likely to be hospitalised as a result of injury,compared to people in other parts of the state. Reasons for the rurality gradient need to beexplored further, as they do not seem to be accounted for on the bases of particularly riskysports, alone. The ARIA findings are consistent with the previous findings reported by Lamamongst children in NSW [12]. In contrast, there was no clear relationship between the SEIFAindex and sport/leisure hospitalisation episode rates across activities, though rates weresignificantly higher (in the second and third quintiles) of disadvantage.
Without further relevant information, the reasons for these trends are not clear but may well berelated to differences in sport/leisure infrastructure across regions. For example, people frommore affluent areas are more likely to participate in sporting activities that are supported by agood infrastructure including well maintained grounds, provision of appropriate and goodcondition equipment, better funded sporting clubs, wider use of personal protectiveequipment, better provision of first aid services and access to more qualified coaches andofficials. These infrastructure items have all been shown to contribute to the provision of safersporting environments [14, 15]. Rural communities are known to have poorer sportinginfrastructure [13] and it has been suggested that the same is particularly true of Aboriginalcommunities in these areas [16]. It would seem reasonable to hypothesise that people whoparticipate in sport/leisure contexts with good infrastructure would be at reduced risk of injurycompared to other areas which cannot afford or have access to this full infrastructure.Alternatively, a lack of sport infrastructure could lead to a reduction in participation.Unfortunately, there is currently no readily available information about the availability ofsports/leisure infrastructure across regions and so these hypotheses cannot be formallyassessed.
An alternative explanation for some of the SEIFA findings, in particular, could be differentialparticipation in sport across the quintiles. The financial burden of playing sport, in terms ofmembership fees, equipment, etc, means that some people may not be able to afford toparticipate in sport/leisure activities; this is most likely to affect the most disadvantaged people.Hence, the overall rate of injury in the first quintile may be lower than that of most othergroups because there are fewer participants. A similar interpretation could also explain thehigher rate of injury in the fifth quintile, relative to the fourth. It is possible that more affluentpeople participate in more sport/leisure activity than other people and so the higher rate ofinjury reflects more people playing sport and being at risk of injury. Unfortunately, there iscurrently no available sports participation data available at the SLA level that would allow thisto be explored further or for participant-adjusted rates to be determined.

15
Par
t A
: S
ocio
-Dem
ogra
phic
and
Geo
grap
hic
Cha
ract
eris
tics
of
Spo
rt/L
eisu
re H
ospi
talis
atio
n Ep
isod
e R
ates
The presented injury maps show high numbers of sport/leisure injury hospitalisation cases inmetropolitan Sydney and the east coast. Whilst these high numbers are related to thepopulation levels in those areas, they do have implications for health service delivery in theseareas because of the high case load. Unlike other injury issues, such as road trauma andviolence, the vast majority of sport/leisure injuries do not present to hospital for treatment. Ithas been estimated that fewer than 30% of all cases receive medical treatment. Considerationcould therefore be given towards reviewing other health care support, such as that provided bysports medicine professionals and first aid services in high case member areas, as it may alsobe expected that a high overall incidence of sport/leisure injury (not just that beinghospitalised) may be occurring in these areas too.
In the ICD-10-AM codes, which were used to identify cases in this report, there is no simpledelineation between sport and leisure. This makes it impossible to identify injuries solelyrelated to participation in organised sports. For example, if someone was injured whileparticipating in football, it is not known if this was as a team member in a competitive game oras part of a kick-to-kick session in the backyard. Further research could be undertaken todetermine the extent to which the geographical variations across the state are due to factorsrelated to organised sport or to more leisure type pursuits.
A.6 RECOMMENDATIONS
The high excess rate of sport/leisure injury in remote and very remote areas needsconsideration. Further investigations into determining why these areas have such high rates,identifying what the major issues may be and exploring what infrastructure needs and otherlocally-based issues could be addressed to reduce injury rates in these areas would bebeneficial. Collection of appropriate participation data to determine if the high rates are due tolarge numbers of participants or to an increased injury risk in these areas will be important.
Sport/leisure injury rates should continue to be monitored across social/demographic groups. Amajor gap is information about how rates differ in areas with a high Aboriginal population.Research is required to quantify sports participation rates and describe the nature and extent ofsports injuries amongst Aboriginal people.
It is well known that sport/leisure hospitalisations represent fewer than 30% of all sports injurycases. Given the number of hospitalisations highlighted in this report, it is likely that there aremany more cases that do not receive treatment at a hospital. These high numbers of sportinginjuries may warrant a review by organisations such as the NSW Sporting Injuries Committeeand Sports Medicine Australia of the delivery and availability of community-wide sportsmedicine services aimed at treating moderate injuries, including those focusing on preventionboth in clinical settings and directly linked to sports delivery systems across metropolitanSydney and the east coast of NSW.
Bodies such as the Australian Bureau of Statistics and the NSW Sporting Injuries Committeecould give consideration towards the collection and reporting of sports participation surveydata across Local Government Areas (LGAs) so that regional estimates of injury rates can beadjusted for participation in sport/leisure activities and not just for population density.

16
Part B
: Coding Issues A
ssociated With the Identification of S
port/Leisure Injuries
B.1 INTRODUCTION
As stated on page 2, sports/athetics injury cases have been identified in this report on thebasis of ICD-10-AM activity codes. These activity codes represent over 200 categories andcan be used to specifically identify different types of sport/leisure activity associated withinjury. Australia has led the world in the development and use of these ICD activity codes.Unfortunately, as stated in the previous sport/leisure injury report [1], the quality of theICD-10-AM sports/athletics activity coding is unknown because previous studies haveinvestigated the validity of the principal injury and external cause codes, but not activitycodes.
The ICD-10-AM also allows for the coding of place of occurrence of injury, whichincludes, among other categories, a category of sports/athletics areas. The relationshipbetween the activity codes indicating sports/athletics activities and place of occurrencecodes indicating sports/athletics areas has not been fully explored to date. In the absenceof this information, and the higher presumed specificity of the activity code for indicatingsports/athletics activity associated with injury, sport/leisure injury studies, including ours,have selected cases based on this variable.
In the ICD-10-AM, activity codes are used with categories V01 to Y34 (i.e. for all injurycauses except complications of care and sequelae) according to specific rules. Whenmultiple codes apply, the code appearing highest in the tabular list is assigned. Forexample, when sport is undertaken during school or as part of paid work, an activity codefor sports/athletics (U50-U71) should be assigned. The place of occurrence code is for usewith categories V01 to Y89 (i.e. for all injury causes including complication of care), toidentify the place where the injury or poisoning occurred. The place of occurrence isassigned to the activity code. As with the activity codes, when multiple codes apply, thecode appearing highest on list is applied [4]. The ISC provides up to three fields for therecording of activity and place of occurrence codes. Despite these ICD-10-AM codingprinciples, a large number of cases are assigned either an unspecified or a missing activitycode. Furthermore, less than 1% of cases have codes in the second and third field. Inpractice, there is very little difference in the interpretation of unspecified and missingcodes. In theory, unspecified means that the coder tried but could not find anyinformation related to where the injury had occurred in the medical/hospital notes. Asmissing indicates that no information was provided by the coder, it is not clear whether theinformation on place was missing from the medical notes or that the coder just failed toextract the information.
This section presents a sensitivity analysis of the range of possible impacts that theunderreporting of activity codes in general, has on estimates of the frequency ofsport/leisure injury hospitalisation episodes. In addition, it presents an exploration of therelationship between the activity and place codes for the identification of sports/athleticsinjuries, including an assessment of the degree of concordance between the two sets ofcodes. The assessment is for NSW hospitalisation episodes of NSW residents during the 2years 2003–2004.
PART B: CODING ISSUES ASSOCIATED WITH THE IDENTIFICATION OF SPORT/LEISURE INJURIES

17
Par
t B
: C
odin
g Is
sues
Ass
ocia
ted
Wit
h th
e Id
enti
fica
tion
of
Spo
rt/L
eisu
re In
juri
es B.2 ACTIVITY CODES AND THE IDENTIFICATION OF SPORT/LEISURE INJURIES
Table B.1 shows the distribution of activity codes across the ICD external causecategories most commonly associated with sport/leisure injury.
Overall, in 2003–2004, there was a total of 182,951 hospital separations. Of these,55.6% had activity codes that were not related to sport/leisure and 13.9% could bespecifically identified as being associated with sport/leisure. Almost one third of cases(30.5%) either had a missing or an unspecified (i.e. U73.9) activity code. This hassignificant implications for the identification of sports/athletics injuries and estimationof their frequency, as one third of the overall set of hospitalisation episodes wouldhave to be removed from consideration.
Table B.1 also shows variations across the external cause categories. As a proportionof all external cause cases, the rates of also having a valid sports/athletics activitycode was highest for overexertion and strenuous or repetitive movements (39.9%),followed by drowning (37.9%) and struck by/against (33.4%). It was lowest for theothers, falls and transport accident categories.
There were relatively low levels of missing activity codes but the frequency ofunspecified activity codes ranged from a low of 12.3% of all overexertion andstrenuous or repetitive movements to 38.9% of all exposure to unknown factor cases.The high rate of unspecified activity codes in the falls category has been previouslynoted and is considered to be most relevant to the problem of falls in older people[17].
Tables B.1 and B.2 only relate to the first activity field. While there are three fields foractivity codes allowed, fewer than 0.5% of cases had a second activity code and onlyabout 3 cases had a third activity code. Even for these cases, a scan of the codes inthe secondary and third activity fields showed that they were either the same as theone in the first activity field or seemed to refer to a secondary injury. There were nocases with codes in the second and third activity field when the codes in the first fieldwere missing.

Sport/athletics activity code
Unspecified activity code
Missing activity code
Not sport/athletics activity code
ICD external cause category
ICD code range
Total number of cases assigned to ICD code range
n % n % n % n %
Overexertion and strenuous or repetitive movements
X50 4854 1938 39.9 596 12.3 20 0.4 2300 47.4
Drowning
W65-W74, V90, V91, V21
346 131 37.9 68 19.7 0 0 147 42.5
Struck by/against W20-W23, W50-W52
11400 3805 33.4 2296 20.1 25 0.2 5274 46.3
Transport accidents V01-V99 28998 4308 14.9 9403 32.4 125 0.4 15162 52.3
Fall W00-W19 71879 10510 14.6 21581 30.0 281 0.4 36507 55.0
Exposure to unknown factor
X59 19708 2790 14.2 7666 38.9 230 1.1 9022 45.8
Others All other codes
45766 1864 4.1 12718 27.8 854 1.9 30330 66.3
Total 182951 25346 13.9 54328 29.7 1535 0.8 101742 55.6
18
Part B
: Coding Issues A
ssociated With the Identification of S
port/Leisure Injuries
Table B.1: Distribution of activity codes across common categories of mechanisms of injury,NSW hospitalisation episodes of NSW residents, 2003–2004
Given the high level of unspecified and missing activity codes, it is pertinent to ask what impactthis may have on estimates of the frequency of sport/leisure injury hospitalisation episodes. TableB.2 shows the results of a sensitivity analysis which considers the impact of the following varyingassumptions:
1. None of the cases with unspecified and missing activity codes are actually sport/leisureinjuries.
2. A number of the cases with unspecified and missing activity codes are actually sport/leisureinjuries and the % of sport/leisure cases in the unknown cases is equivalent to that amongstthe cases with a known activity code.
3. A number of the cases with unspecified and missing activity codes are actually sport/leisureinjuries and the % of sport/leisure cases in the unknown cases is 75%.
These assumptions therefore provide a range from very conservative (i.e. assumption 1) to beingmost likely (assumption 2) to providing a maximal bound (assumption 3). Assumption 2, assumesthat there is no differential misclassification rate amongst actual sport/leisure cases and true non-sport/leisure cases, though this is could not be verified. The maximal bound of assumption 3 isrelatively arbitrary but has been chosen to be less than 100% because it is extremely unlikely thatall cases with missing/unspecified activity codes would be associated with sports/athletics.
Overall, under assumption 1, sports/athletics leisure hospitalisation episodes would comprise13.9% of all injury hospitalisation episodes. At the maximal bound end of the scale, this could beas high as 38.3% of all cases. It is most likely, however, that the true frequency of sport/leisureinjury hospitalisation episodes lies in the range covered by assumptions 1-2, i.e. in the range of13.9-19.9% of all hospitalisation episodes.
This sensitivity analysis example serves to show how incomplete data coding can have asignificant impact on conclusions about the frequency of sports/athletics injuries.

19
Par
t B
: C
odin
g Is
sues
Ass
ocia
ted
Wit
h th
e Id
enti
fica
tion
of
Spo
rt/L
eisu
re In
juri
es
B.3 PLACE CODES AND THE IDENTIFICATION OF SPORT/LEISURE INJURIES
Table B.3 shows the distribution of place codes across the ICD external causecategories most commonly associated with sports/athletics injury. There were notmany instances of missing codes but the level of unspecified place codes ranged from8.1% for drowning to 81.8% of all X59: Exposure to unknown factors cases. Theexternal category causes most likely to have a sport and athletics area place codeindicated were overexertion and strenuous or repetitive movements (27.3%) andstruck by/against (22.2%) cases. Transport accidents were least likely to be coded toan area for sport/athletics.
Table B.2: Impact of different assumptions about the proportion of missing/unspecified activity codes that may be truly sports/athletics cases on theoverall sport/leisure injury frequency estimates, NSW hospitalisationepisodes, 2003–2004
% of all cases related to
sports/athletics under different assumptions about the
missing/unknown activity code cases ICD external cause category
ICD code range
Total number of cases assigned to ICD code range
0% % amongst
known activity cases
75%
Drowning
W65-W74, V90, V91, V21
346 37.9 47.1 53.6
Fall W00-W19 71879 14.6 21.0 39.0
Overexertion and strenuous or repetitive movements
X50 4854 39.9 45.7 50.1
Transport accidents V01-V99 28998 14.9 22.1 41.1
Struck by/against W20-W23, W50-W52
11400 33.4 41.9 49.7
Exposure to unknown factor X59 19708 14.2 23.6 46.2
Others All other codes
45766 4.1 5.8 27.8
Total 182951 13.9 19.9
38.3

20
Part B
: Coding Issues A
ssociated With the Identification of S
port/Leisure InjuriesTable B.3: Distribution of place codes across common categories of mechanisms of injury, NSW
hospitalisation episodes, 2003–2004
Sports/athletics place code
Unspecified place code
Missing place code
Not sports/athletics
place code ICD external cause category
ICD code range
Total number of
cases assigned to ICD code
range n % n % n % n %
Overexertion and strenuous or repetitive movements
X50 4854 1325 27.3 1778 36.6 20 0.4 1731 35.7
Drowning W65-W74, V90, V91, V21
346 42 12.1 28 8.1 0 0.0 276 79.8
Struck by/against
W20-W23, W50-W52
11400 2527 22.2 4794 42.1 8 0.1 4071 35.7
Transport accidents V01-V99 28998 986 3.4 7409 25.6 64 0.2 20539 70.8
Fall W00-W19 71879 5249 7.3 22146 30.8 84 0.1 44400 61.8
Exposure to unknown factor
X59 19708 1775 9.0 16116 81.8 48 0.2 1769 9.0
Others All other codes
45766 585 1.3 21955 48.0 191 0.4 23035 50.3
Total 182951 12489 6.8 74226 40.6 399 0.2 95837 52.4
Given the high level of unspecified and missing place codes, it is pertinent to ask what impact this mayhave on estimates of the frequency of sports/athletics injury hospitalisation episodes. Table B.4 showsthe results of a sensitivity analysis which considers the impact of the following varying assumptions:
1. None of the cases with unspecified and missing place codes are actually sport/leisure injuries.
2. A number of the cases with unspecified and missing place codes are actually sport/leisure injuriesand the % of sport/leisure cases in the unknown cases is equivalent to that amongst the cases witha known place code.
3. A number of the cases with unspecified and missing place codes are actually sport/leisure injuriesand the % of sport/leisure cases in the unknown cases is 75%.
These assumptions therefore provide a range from very conservative (i.e. assumption 1) to being mostlikely (assumption 2) to providing a maximal bound (assumption 3). Assumption 2, assumes that thereis no differential misclassification rate amongst actual sport/leisure cases and true non-sport/leisurecases, though this is could not be verified. The maximal bound of assumption 3 is relatively arbitrarybut has been chosen to be less than 100% because it is extremely unlikely that all cases withmissing/unspecified activity codes would be associated with sports/athletics.
Overall, under assumption 1, sports/athletics injury hospitalisation episodes would comprise 6.8% ofall injury hospitalisation episodes. At the maximal bound end of the scale, this could be as high as37.4% of all cases. It is most likely, however, that the true frequency of sports/athletics injuryhospitalisation episodes lies in the range covered by assumptions 1-2, i.e. in the range of 6.8-11.5% ofall hospitalisation episodes.
This sensitivity analysis example serves to show how incomplete data coding can have a significantimpact on conclusions about the frequency of sports/athletics injuries.
It is worth noting that the proportion of cases identified as being related to sport/leisure on the basis ofplace codes is less than the equivalent proportion based on activity codes (comparison of Tables B.2and B.4).

21
Par
t B
: C
odin
g Is
sues
Ass
ocia
ted
Wit
h th
e Id
enti
fica
tion
of
Spo
rt/L
eisu
re In
juri
es
B.4 RELATIONSHIP BETWEEN ACTIVITY AND PLACE CODES
The previous two sections considered the usefulness of the activity and place codesfor estimating the frequency of injury hospitalisation episodes individually. Theactivity code selection identified a larger number of cases than the place codeselection. This section considers the relationship between the two selection criteria todetermine if some combination of the two selection processes would be moreoptimal.
Table B.5 summarises the proportion of hospitalisation episodes identified as beingassociated with sport/leisure according to the ICD-10-AM activity and place codesacross major ICD external cause categories for hospitalisation episodes during 2003and 2004.
Table B.4: Impact of different assumptions about the proportion of missing/unspecified place codes that may be truly sport/leisure cases on the over-all sports/athletics injury frequency estimates, NSW hospitalisationepisodes, 2003–2004
% of all cases related to sport/leisure under different assumptions about the missing/unknown activity code cases
ICD external cause category
ICD code range
Total number of cases assigned to ICD code range
0% % amongst
known activity cases
75%
Drowning W65-W74, V90, V91, V21
346 27.3 43.4 55.1
Fall W00-W19 71879 12.1 13.2 18.2
Overexertion and strenuous or repetitive movements
X50 4854 22.2 38.3 53.8
Transport accidents V01-V99 28998 3.4 4.6 22.7
Struck by/against W20-W23, W50-W52
11400 7.3 10.6 30.5
Exposure to unknown factor
X59 19708 9.0 50.1 70.5
Others All other codes
45766 1.3 2.5 37.6
Total 182951 6.8 11.5 37.4

22
Part B
: Coding Issues A
ssociated With the Identification of S
port/Leisure Injuries
Overall, 85.2% of hospitalisation episodes could not be positively identified as a sport/leisureinjury on the basis of either an activity or place code. Almost twice as many hospitalisationepisodes were identified on the basis of a sport/leisure activity code than on the basis of aplace code selection (13.8% versus 7.1%). Adding a place code selection criterion, onlyadded an additional 1% to the estimate of overall frequency of sport/leisure injury cases thatwould be based on activity codes alone (i.e. 14.8% vs 13.8%).
Table B.5: Proportion of NSW-based hospitalisation episodes of NSW residents identified asbeing associated with sports/athletics according to the ICD-10-AM activity and placecodes, 2003–2004
CASES IDENTIFIED AS BEING ASSOCIATED WITH SPORT AND LEISURE
ICD code range n
% with ONLY a
sports/athletics activity code
A
% with ONLY a
sports/athletics place code
B
% with BOTH a
sports/athletics activity code
AND a sports/athletics
place code
C
% with EITHER a sports/athletics
activity code OR a sports/athletics
place code
A+B+C
% not sport related *
100-(A+B+C)
W65-W74, V90, V91,
V21
346 30.1 6.4 7.8 44.2 55.8
X50 4854 13.3 0.9 26.6 40.8 59.2
W20-W23, W50-W52 11400 12.4 1.5 20.9 34.9 65.1
V01-V99 28998 12.2 1.4 2.6 16.3 83.7
W00-W19 71879 8.0 0.9 6.7 15.5 84.5
X59 19708 5.7 0.6 8.5 14.8 85.2
All other codes
45766 3.1 0.5 0.9 4.6 95.4
182951 7.6 0.9 6.2 14.8 85.2
* cases with no mention of a sports/athletics activity code or a sport/recreation place code (includes cases for
which these variables have missing or unspecified values).
Note – The overall % with a sports/athletics activity code is the sum of the numbers in columns A and C. The overall % with a sport/recreation place code is the sum of the numbers in columns B and C.

23
Par
t B
: C
odin
g Is
sues
Ass
ocia
ted
Wit
h th
e Id
enti
fica
tion
of
Spo
rt/L
eisu
re In
juri
es
Figures B.1-B.4, explore the activity and place code relationships for four major external causegroups. In each instance, the proportion of cases with only a sport/athletics place is small.
The concordance between the two types of codes also varied across mechanisms with 28.6%of all sports-related overexertion and strenuous or repetitive movements having both an activityand place code indicating sport. A large proportion of all struck by/against sport/leisureinjuries also had both an activity and place code indicating sport/leisure. For drowning andfalls, sport/leisure related cases were twice as likely to be identified by activity codes thanplace codes (37.9% vs 14.2% for drowning and 14.7% vs 7.6% for falls). For overexertion andstrenuous or repetitive movements and struck by/against cases, activity code identification wasabout 1.5 times more common than place code identification (39.9% vs 27.5%, and 33.3% vs22.4%, respectively).
Figure B.1 NSW-based sports/athletics related drowning – relationship between activity andplace codes
Figure B.2 NSW-based sports/athletics related overexertion and strenuous or repetitivemovements – relationship between activity and place codes
Note: Numbers are the % of all drowning NSW hospitalisation episodes, 2003–2004 and add to 44.2%
Note: Numbers are the % of all overexertion and strenuous or repetitive movements NSW hospitalisation episodes,2003–2004 and add to 40.8%
Figure B.3 NSW-based sports/athletics related struck by/against – relationship between activityand place codes
Note: Numbers are the % of all struck by/against NSW hospitalisation episodes, 2003–2004 and add to 34.9%
Activity codeonly
30.1%
7.8%both
6.4% Place code only
Activity codeonly
13.3%
26.6%both
0.9% Place code only
Activity codeonly
12.4%
20.9%both
1.5% Place code only

24
Part B
: Coding Issues A
ssociated With the Identification of S
port/Leisure Injuries
Figure B.4 NSW-based sports/athletics related falls – relationship between activity and placecodes
Note: Numbers are the % of all falls NSW hospitalisation episodes, 2003–2004 and add to 15.5%
B.5 IMPLICATIONS OF THESE CODING ISSUES
Currently, not all hospitalisation episodes have valid or useable activity codes; over 30% of allinjury hospitalisation episodes have either a missing or unspecified activity code. This almostcertainly means that the number of sports/athletics injury hospitalisation episodes identified onthe basis of activity codes, is an underestimate. This also severely limits the ability to identify allpriority sports and activities for the development of injury prevention strategies for these cases.It would seem that more effort may be needed, in close collaboration with health informationstakeholders, in order to ensure the appropriate training of coders and data recorders regardingthe use of injury-related codes, including those specific to sport/leisure, and the informationneeded to assign them.
After adjusting for potential underreporting associated with undefined activity codes, it is likelythat sports/athletics injuries may really account for up to one in five injury hospitalisationepisodes and over 40% of all overexertion and strenuous or repetitive movements, drowningand struck by/against hospitalisation episodes.
The external cause categories of overexertion and strenuous or repetitive movements, drowningand struck by/against hospitalisation episodes are most commonly associated with sport/leisureactivity and should be the focus of further coding developments and refinements.
Selecting sports/athletics injuries on the basis of activity codes alone, yields a larger number ofcases than a place-based selection criterion. This suggests, in terms of frequency estimation,that defining sports/athletics injury cases on the basis of activity alone, is appropriate, albeit aslight underestimate.
Selecting cases on the basis of the place of injury is clearly an underestimate. This is perhapsnot surprising, given that not that all sport/leisure injuries will occur only in sports/athleticsareas and many will also occur in schools, at homes, and in natural settings etc. Anotherproblem with case selection based on place is that some cases injured in a sport ground mightnot necessarily have been actually participating in a sport at the time; they may have beenspectators, coaches, referees or passers-by, for example. This provides further support for theplace of occurrence codes not being adequate for identifying sports/athletics hospitalisations.
Activity codeonly
8.0%
6.7%both
0.9% Place code only

25
Par
t B
: C
odin
g Is
sues
Ass
ocia
ted
Wit
h th
e Id
enti
fica
tion
of
Spo
rt/L
eisu
re In
juri
es B.6 RECOMMENDATIONS
Future studies using ICD-10-AM coded routine data collections should continue to use theactivity variable to select sport/leisure cases.
Estimates of sport/leisure frequency based on such data need to be recognised as being anunderestimate of the true frequency.
Improvements in the information recorded for cases of sport-related hospitalisation in routinelycollected hospitalisation data appear warranted. The identification of sport/leisure relatedhospitalisation depends upon the recording of accurate and specific information about thenature of the activity being undertaken at the time of injury. In addition, specific informationabout the mechanism (external cause) of an injury and the type of place where the injuryoccurred is of great value to injury prevention efforts. Reasons for the relatively high levels ofmissing or unspecified activity and place information need to be determined to identify whatsolutions could be implemented to address these information gaps.
Further refinement of ICD-10-AM codes may be required to enable data coders to more easilyclassify the activity being undertaken at the time of injury as well as the type of place in whichthe injury occurred. Given the strong association of the causes of sports injuries with theexternal cause categories of overextention and strenuous or repetitive movements, drowningand struck by/against, efforts should perhaps first be directed at these categories. The detail andquality of information available to coders from hospital medical records will need to beconsidered.
Continued development of the ICD-10-AM codes should include consultation with experts inthe use and interpretation of sport/leisure injury data to ensure that coding guidelines andtraining procedures enable the recorders and coders to more easily classify the activity beingundertaken at the time of injury.

26
C.1 INTRODUCTION
Part C of this report provides a detailed profile of the ten sports most commonly associatedwith NSW-based hospitalisations of NSW residents due to injury. This profile describes themechanism, place of occurrence, nature, body region, diagnosis and external cause of injuryacross each of the ten sports. As this report focuses on injuries that result in hospitalisation,only the most severe injuries are described. Unfortunately, it is not possible to delineate thoseinjuries that occurred during formal organised sport from those that were incurred during morerecreational activity. This limits the recommendations that can be made for injury preventionstrategies in specific contexts.
It is also beyond the scope of this report to review and recommend potential preventivemeasures for these, and less severe, injuries. Nonetheless, the information presented in thissection enables the identification of the priority areas for injury prevention across all forms ofparticipation in the particular activity category.
The ten categories of sport/leisure activity focussed on here are those with the highest overallinjury rates in our earlier report (Table 9) [1]. Hospitalisation cases are categorised according tothe principal injury diagnosis only.
Importantly, these profiles present the frequency of cases only and are not participation-adjusted. Hence they do not necessarily reflect participation rates in particular sports. Thismeans that the data presented here cannot be used to conclude whether increased numbers ofinjuries in a specific sport/leisure activity are due to higher participation, a higher risk forparticipants or both.
C.2 SPORT SPECIFIC PROFILES
C.2.1. RUGBY (league and union)
This section provides a description of the hospitalised injuries associated with participation inrugby league or union. Unfortunately, the use of the ICD codes used to identify rugby injuriesdoes not allow an adequate identification of particular rugby codes (eg league versus union)because of the very large number of ‘rugby unspecified’ cases and so the data here covers allcodes of rugby football in NSW.
With a total of 3052 hospitalisation episodes over the 2 year period, 2003–2004, rugby wasthe highest ranking sport with respect to the frequency of injury. The mechanisms of theseinjuries are summarised in Table C.1. More than half of all injuries were associated with a falland a further 21% were associated with tackling and other collisions in the sport.
Part C
: Profiles of Injury H
ospitalisation Episodes Associated w
ith Selected S
port and Leisure A
ctivitiesPART C: PROFILES OF INJURY HOSPITALISATION EPISODES ASSOCIATEDWITH SELECTED SPORT AND LEISURE ACTIVITIES

27
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s Table C.1: Broad mechanisms leading to rugby injury hospitalisation, NSW, 2003–2004
Mechanism n % Fall 1734 56.8
Struck by or struck against 646 21.2
Overexertion and strenuous or repetitive movements 186 6.1
Other 75 2.5
Unspecified 409 13.4
Total 3052 100.0
As would be expected, the vast majority of rugby injuries occurred in a sports andathletics area (Table C.2). The place of injury was unknown for about one in eight cases.
Table C.2: Place of occurrence of incidents leading to hospitalisation episodes for rugby injury,NSW, 2003–2004
Place of occurrence n % Sports and athletics area 2509 82.2
School 96 3.1
Home 17 0.6
Other 34 1.1
Unknown 394 12.9
Total 3052 100.0
Table C.3 shows that the most common principal diagnosis of the rugby injuries was afracture, accounting for nearly 55% of all hospitalised rugby injuries. This was followedby dislocation, and sprain/strain. Intracranial injuries, including concussion, accountedfor 7% of all hospitalised cases. This distribution is consistent with the fact that these datarelate to hospitalisation episodes only and so the injuries would be expected to be severein nature.
Table C.3: Nature of rugby injury associated with hospitalisation episodes, NSW, 2003–2004
Nature of injury n % Fracture 1671 54.8
Dislocation 288 9.4
Sprain or strain 259 8.5
Intracranial injury (including concussion) 213 7.0
Injury to muscle and tendon 90 2.9
Superficial injury 70 2.3
Open wound 72 2.4
Injury to internal organ 37 1.2
Other 352 11.5
Total 3052 100.0
The most commonly injured body region was the upper limb, accounting for more thanone-third of all injuries. This was followed by the lower limb and head (Table C.4).
n %
n %
n %

28
Part C
: Profiles of Injury H
ospitalisation Episodes Associated w
ith S
elected Sport and Leisure A
ctivitiesTable C.4: Injured body regions associated with hospitalisation episodes for rugby injury, NSW,
2003–2004
Injured body region n % Upper limb 1187 38.9
Lower limb 761 24.9
Head 708 23.2
Neck 223 7.3
Trunk 155 5.1
Other 18 0.6
Total 3052 100.0
The most frequently reported ICD individual external causes of rugby injury are shown inTable C.5. Just over half of the injuries were caused by a fall on the same level as part ofa collision during the game. Contact in the game was also associated with a further 19%of injuries (W50+W51). These injuries are consistent with the nature of rugby, which iscomprised of frequent tackling and pushing.
Table C.5: Most commonly specified ICD external causes leading to hospitalised rugby injuries,NSW, 2003–2004.
ICD external causes n % W03 Other fall on same level due to collision with, or pushing by,
another person 1593 52.2
W50 Hit, struck, kicked, twisted, bitten or scratched by another person 325 10.6
W51 Striking against or bumped into by another person 258 8.5
X50 Overexertion and strenuous or repetitive movements 186 6.1
W18 Other fall on same level 90 2.9
W21 Striking against or struck by sports equipment 49 1.6
W01 Fall on same level from slipping, tripping and stumbling 28 0.9
Y04 Assault by bodily force 9 0.3
Table C.6, Table C.7 and Table C.8 list the most common external causes of injury codesfor each of the major body regions: upper limb, lower limb and head. For each of thethree body regions, the most common cause of injury was a fall on the same level due tocollision with, or pushing by, another person (W03). As stated earlier, this is notunexpected given the nature of rugby, which is a full body contact sport.
Table C.6: Most commonly specified ICD external causes of rugby upper limb injuries leading tohospitalisation, NSW, 2003–2004.
ICD external cause n W03 Other fall on same level due to collision with, or pushing by, another person 650
W51 Striking against or bumped into by another person 69
W18 Other fall on same level 62
W50 Hit, struck, kicked, twisted, bitten or scratched by another person 62
Table C.7: Most commonly specified ICD external causes of rugby lower limb injuries leading tohospitalisation, NSW, 2003–2004.
ICD external causes n W03 Other fall on same level due to collision with, or pushing by, another person 370X50 Overexertion and strenuous or repetitive movements 150W50 Hit, struck, kicked, twisted, bitten or scratched by another person 40W51 Striking against or bumped into by another person 31
n
n
n %
n %

29
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s Table C.8: Most commonly specified ICD external causes of rugby head injuries leading to hospitalisation, NSW, 2003–2004.
ICD external cause n W03 Other fall on same level due to collision with, or
pushing by, another person 475
W50 Hit, struck, kicked, twisted, bitten or scratched by another person
191
W51 Striking against or bumped into by another person 140 W21 Striking against or struck by sports equipment 15
As shown in Table C.9, a fracture of the forearm was the most commonly recordeddiagnosis code for rugby injury, representing 15% of all cases. In fact, the top fourdiagnosis codes related to fractures, across all regions of the body.
Table C.10, Table C.11 and Table C.12 list the five most common ICD diagnoses for eachof the major body regions: upper limb, lower limb and head. Consistent with the findingsrelating to the nature of rugby injuries presented in Table C.3, fractures were the leadingdiagnosis for all three body regions.
Table C.9: Most commonly specified ICD diagnosis codes for rugby injuries treated in hospital, NSW,2003–2004
ICD diagnosis codes n % S52 Fracture of forearm 457 15.0 S82 Fracture of lower leg, including ankle 383 12.5 S62 Fracture at wrist and hand level 298 9.8 S02 Fracture of skull and facial bones 290 9.5 S06 Intracranial injury 213 7.0 S83 Dislocation, sprain and strain of joints and
ligaments of knee 203 6.7
S43 Dislocation of shoulder joint 152 5.0 S42 Fracture of shoulder and upper arm 127 4.2
Table C.10: Most commonly specified ICD diagnoses associated with rugby upper limb injuriesleading to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S52 Fracture of forearm 457S62 Fracture at wrist and hand level 298S43 Dislocation of shoulder joint 152S42 Fracture of shoulder and upper arm 127S63 Dislocation, sprain and strain of joints and ligaments at wrist and hand
level 60
n
n
n
%

30
Part C
: Profiles of Injury H
ospitalisation Episodes Associated w
ith S
elected Sport and Leisure A
ctivitiesTable C.11: Most commonly specified ICD diagnoses associated with rugby lower limb injuries leading
to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S82 Fracture of lower leg, including ankle 383
S83 Dislocation, sprain and strain of joints and ligaments of knee 203
S72 Fracture of femur 33
S86 Injury of muscle and tendon at lower leg level 30
S93 Dislocation, sprain and strain of joints and ligaments at ankle and foot level 24
Table C.12: Most commonly specified ICD diagnoses associated with rugby head injuries leading tohospitalisation, NSW, 2003–2004.
p
ICD principal diagnosis codes n S02 Fracture of skull and facial bones 290
S06 Intracranial injury 213
S01 Open wound of head 57
Table C.13: Broad mechanisms leading to soccer injury hospitalisation, NSW, 2003–2004
Mechanism n % Fall 1209 41.8
Struck by or struck against 827 28.6
Overexertion and strenuous or repetitive movements 317 11.0
Unspecified 458 15.9
Other 78 2.7
Total 2889 100.0
C.2.2. SOCCER
There were a total of 2889 hospitalisation episodes for soccer injury over the 2 year period2003–2004. As shown in Table C.13, the majority of these injuries (41.8%) were as a result of a fall.This was followed by injuries caused by being struck by or against (28.6%). As with rugby football,which had a large number of injuries for which the mechanism of injury was unclear, nearly one insix soccer injuries was coded as exposure to an unspecified factor (15.9%).
Almost 75% of soccer injuries occurred in a sports and athletics area, as shown in Table C.14.However, the place of injury was unknown for a relatively large proportion of injuries.
Table C.14: Place of occurrence of incidents leading to hospitalisation episodes for soccer injury, NSW,2003–2004
Place of occurrence n % Sports and athletics area 2141 74.1School 149 5.2Home 21 0.7Other 63 2.1Unknown 515 17.8Total 2889 100.0
The vast majority of soccer injuries were fractures, representing more then 60% of all cases. Thesecond most common nature of injury was a sprain or strain. The proportion of intracranial injuriesin soccer (3.1%) was far smaller as compared with rugby (7.0%), which most likely reflects thediffering styles of body contact in these sports.
n %
n
n
n
%

31
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s Table C.15: Nature of soccer injury associated with hospitalisation episodes, NSW, 2003–2004
Nature of injury n % Fracture 1803 62.4 Sprain or strain 336 11.6 Dislocation 234 8.1 Injury to muscle and tendon 151 5.2 Intracranial injury (including concussion) 90 3.1 Superficial injury 43 1.5 Open wound 31 1.1 Injury to internal organ 26 0.9 Other 175 6.1 Total 2889 100.0
The body region that was most commonly injured in soccer was the lower limb, with half of allinjuries, as shown in Table C.19. This is consistent with the specific demands of soccer, whichprimarily involves contact with the ball and other players when kicking the ball.
Table C.16: Injured body regions associated with hospitalisation episodes for soccer injury, NSW,2003–2004
Injured body region n % Lower limb 1447 50.1Upper limb 975 33.7Head 319 11.0Trunk 95 3.3Neck 40 1.4Other 13 0.4Total 2889 100.0
The most frequently reported ICD external causes of soccer injury are presented in Table C.17. Themost frequent external cause of injury was a fall on the same level due to collision with, or pushingby, another person (W03). Combined with those injuries that were caused by contact with anotherperson (W50, W51), these three external causes accounted for 42.9% of all injuries. Unfortunatelyone in six injuries was classified as being due to exposure to an unspecified factor.
Table C.17: Most commonly specified ICD external causes leading to hospitalised soccer injuries,NSW, 2003–2004.
ICD external causes n % W03 Other fall on same level due to collision with, or pushing by,
another person 619 21.4
W50 Hit, struck, kicked, twisted, bitten or scratched by another person 383 13.3W18 Other fall on same level 351 12.1X50 Overexertion and strenuous or repetitive movements 317 11.0W51 Striking against or bumped into by another person 237 8.2W21 Striking against or struck by sports equipment 193 6.7W01 Fall on same level from slipping, tripping and stumbling 178 6.2W19 Unspecified fall 60 2.1
Table C.18, Table C.19 and Table C.20 list the most commonly specified external cause of injurycodes for each of the major body regions: upper limb, lower limb and head injury. For upper limbinjuries, falls accounted for the top three causes of injury.
n %
n %
n %

32
Part C
: Profiles of Injury H
ospitalisation Episodes Associated w
ith S
elected Sport and Leisure A
ctivitiesTable C.18: Most commonly specified ICD external causes of soccer upper limb injuries leading to hospitalisation, NSW, 2003–2004.
ICD external cause n W03 Other fall on same level due to collision with, or pushing by, another person 260
W18 Other fall on same level 257
W01 Fall on same level from slipping, tripping and stumbling 114
W21 Striking against or struck by sports equipment 101
The most common cause of soccer lower limb injury was overexertion and overuse, closelyfollowed by a fall resulting from contact with another player, as shown in Table C.19.
Table C.19: Most commonly specified ICD external causes of soccer lower limb injuries leading to hospitalisation, NSW, 2003–2004.
ICD external causes n X50 Overexertion and strenuous or repetitive movements 297
W03 Other fall on same level due to collision with, or pushing by, another person 291
W50 Hit, struck, kicked, twisted, bitten or scratched by another person 195
W51 Striking against or bumped into by another person 105
Following a similar pattern to upper limb injuries, the most common cause of head injury in soccerwas due to contact with another player, as presented in Table C.20.
Table C.20: Most commonly specified ICD external causes of soccer head injuries leading to hospitalisation, NSW, 2003–2004.
ICD external cause n W50 Hit, struck, kicked, twisted, bitten or scratched by another person 104
W51 Striking against or bumped into by another person 80
W03 Other fall on same level due to collision with, or pushing by, another person 53
W21 Striking against or struck by sports equipment 44
One in four soccer injuries was a fracture of the lower leg, including the ankle (Table C.21). Asdescribed earlier, this is consistent with the playing demands of soccer, which primarily focuses onattempting to kick the ball, which can sometimes involve sudden change of direction. Thesemovements would increase the likelihood of these lower leg fractures. The second most commonlyrecorded ICD diagnosis code for soccer injury was a fracture of the forearm. As a large proportion ofall soccer injuries were caused by a fall, it is possible that these forearm fractures are the result of aplayer attempting to break their fall with their arms and hands.
n
n
n

33
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s Table C.21: Most commonly specified ICD diagnosis codes for soccer injuries treated in hospital, NSW,2003–2004
ICD diagnosis codes n % S82 Fracture of lower leg, including ankle 742 25.7S52 Fracture of forearm 617 21.4S83 Dislocation, sprain and strain of joints and ligaments of knee 409 14.2S02 Fracture of skull and facial bones 145 5.0S86 Injury of muscle and tendon at lower leg level 130 4.5S62 Fracture at wrist and hand level 126 4.4S06 Intracranial injury 90 3.1S42 Fracture of shoulder and upper arm 82 2.8S43 Dislocation of shoulder joint 67 2.3S92 Fracture of foot, except ankle 34 1.2
Table C.22, Table C.23 and Table C.24 list the most commonly specified ICD diagnoses for each ofthe major body regions: upper limb, lower limb and head. Consistent with the findings relating tothe nature of soccer injuries presented in Table C.15, fractures were the leading ICD diagnosis forall three body regions. For the upper and lower limb, there were also a large proportion ofdislocations.
Table C.22: Most commonly specified ICD diagnoses associated with soccer upper limb injuries leading to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S52 Fracture of forearm 617
S62 Fracture at wrist and hand level 126
S42 Fracture of shoulder and upper arm 82
S43 Dislocation of shoulder joint 67
S63 Dislocation, sprain and strain of joints and ligaments of wrist and hand 29
Table C.23: Most commonly specified ICD diagnoses associated with soccer lower limb injuries leading to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S82 Fracture of lower leg, including ankle 742
S83 Dislocation, sprain and strain of joints and ligaments of knee 409
S86 Injury of muscle and tendon at lower leg level 130
S92 Fracture of foot, except ankle 34
Table C.24: Most commonly specified ICD diagnoses associated with soccer head injuries leading tohospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S02 Fracture of skull and facial bones 145
S06 Intracranial injury 90
S01 Open wound of head 18
% n
n
n
n

34
Part C
: Profiles of Injury H
ospitalisation Episodes Associated w
ith S
elected Sport and Leisure A
ctivities
Table C.25: Broad mechanisms leading to cycling injury hospitalisation, NSW, 2003–2004
Mechanism n % Transport 1137 93.2 Fall 20 1.6 Struck by or struck against 12 1.0 Overexertion and strenuous or repetitive movements 5 0.4 Other 35 2.9 Unspecified 11 0.9 Total 1220 100.0
C.2.3. CYCLING
There were a total of 1220 hospitalisation episodes for injury associated with cycling over the 2 yearperiod 2003–2004. It can sometimes be difficult to determine whether injury is the result ofparticipation in cycling as a sport and leisure activity or as a mode of transport (Table C.25).However, the data that has been extracted for this report has an ‘activity at the time of injury’ codereferring to sport/leisure activity. Therefore, it is expected that the vast majority of cases described inthis report were related to participation in cycling for the purposes of sport and leisure, and not as amode of transport.
As shown in Table C.26, the majority of cycling injuries were recorded as occurring in an unknownplace, accounting for nearly half of all cases. The second most common place of occurrence forcycling injury was a street and highway with 26% of hospitalised injuries, followed by a sports andathletics area with 10% of injuries. This is not unexpected given that only cycling in the context offormal sport would be conducted in a sports and athletics area. However, it is likely that themajority of people participating in cycling are doing so for a recreational or leisure activity, ratherthan formal organised sport.
Table C.26: Place of occurrence of incidents leading to hospitalisation episodes for cycling injury,NSW, 2003–2004
Place of occurrence n % Street and highway 322 26.4
Sports and athletics area 124 10.2
Home 54 4.4
Other 158 12.9
Unknown 562 46.1
Total 1220 100.0
More than half of all cycling injuries were a fracture, 13% were an open wound and 8% were ahead injury (Table C.27).
Table C.27: Nature of cycling injury associated with hospitalisation episodes, NSW, 2003–2004
Nature of injury n % Fracture 674 55.2
Open wound 161 13.2
Intracranial injury (including concussion) 98 8.0
Superficial injury 65 5.3
Injury to internal organ 38 3.1
Dislocation 31 2.5
Injury to muscle and tendon 19 1.6
Sprain or strain 15 1.2
Other 119 9.8
Total 1220 100.0
Table C.28 shows that the upper limb was the body region with the greatest frequency ofhospitalised cycling injuries. However, one in four injuries occurred to the head, which is importantto consider with respect to helmets as a mandatory injury prevention measure.
n %
n %
n %

35
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s Table C.28: Injured body regions associated with hospitalisation episodes for cycling injury, NSW,2003–2004
Injured body region n % Upper limb 556 45.6
Head 293 24.0
Lower limb 205 16.8
Trunk 134 11.0
Neck 22 1.8
Other and unspecified 10 0.8
Total 1220 100.0
More than half of all hospitalised cycling injuries were as a result of a non-collision transportaccident, as shown in Table C.29. Unfortunately, for more than one in four cases, the external causeof injury was listed as being an ‘other and unspecified transport accident’, which does not provideadequate information to fully understand the circumstances surrounding many cycling injuries.
Table C.29: Most commonly specified ICD external causes leading to hospitalised cycling injuries,NSW, 2003–2004.
ICD external causes n % V18 Pedal cyclist injured in non-collision transport accident 640 52.5V19 Pedal cyclist injured in other and unspecified transport accident 333 27.3V13 Pedal cyclist injured in collision with car, pick-up truck or van 69 5.7V17 Pedal cyclist injured in collision with stationary object 48 3.9V11 Pedal cyclist injured in collision with other pedal cycle 31 2.5W22 Striking against or struck by other objects 7 0.6V14 Pedal cyclist injured in collision with heavy transport vehicle 6 0.5W03 Other fall on same level due to collision with, or pushing by, another
person 5 0.4
Table C.30: Most commonly specified ICD external causes of cycling upper limb injuries leading tohospitalisation, NSW, 2003–2004.
ICD external cause n V18 Pedal cyclist injured in non-collision transport accident 293
V19 Pedal cyclist injured in other and unspecified transport accident 175
V13 Pedal cyclist injured in collision with car, pick-up truck or van 18
V17 Pedal cyclist injured in collision with stationary object 15
V11 Pedal cyclist injured in collision with other pedal cycle 11
Table C.31: Most commonly specified ICD external causes of cycling lower limb injuries leading tohospitalisation, NSW, 2003–2004.
ICD external causes n V18 Pedal cyclist injured in non-collision transport accident 94
V19 Pedal cyclist injured in other and unspecified transport accident 53
V13 Pedal cyclist injured in collision with car, pick-up truck or van 24
V11 Pedal cyclist injured in collision with other pedal cycle 8
V17 Pedal cyclist injured in collision with stationary object 6
As shown in Table C.30, Table C.31 and Table C.32, the most commonly specified causes of injuryfor each of the three major body regions was V18: Pedal cyclist injured in non-collision transportaccident.
n %
n
n
n
%

36
Part C
: Profiles of Injury H
ospitalisation Episodes Associated w
ith S
elected Sport and Leisure A
ctivitiesTable C.32: Most commonly specified ICD external causes of cycling head injuries leading to
hospitalisation, NSW, 2003–2004.
ICD external cause n V18 Pedal cyclist injured in non-collision transport accident 168
V19 Pedal cyclist injured in other and unspecified transport accident 81
V17 Pedal cyclist injured in collision with stationary object 18
V13 Pedal cyclist injured in collision with car, pick-up truck or van 14
V11 Pedal cyclist injured in collision with other pedal cycle 5
The two most commonly recorded diagnosis codes for cycling injury were fractures of the forearm,shoulder and upper arm, accounting for nearly one in three hospitalised injuries. The third mostcommon diagnosis was an intracranial injury, as shown in Table C.33.
Table C.33: Most commonly specified ICD diagnosis codes for cycling injuries treated in hospital,NSW, 2003–2004
ICD diagnosis codes n % S52 Fracture of forearm 277 22.7S42 Fracture of shoulder and upper arm 120 9.8S06 Intracranial injury 98 8.0S82 Fracture of lower leg, including ankle 78 6.4S62 Fracture at wrist and hand level 71 5.8S01 Open wound of head 67 5.5S09 Other and unspecified injuries of head 52 4.3S02 Fracture of skull and facial bones 43 3.5S81 Open wound of lower leg 36 3.0S00 Superficial injury of head 31 2.5
Not surprisingly, the most frequently occurring cycling upper limb injury was a fracture of theforearm, as presented in Table C.34. In fact, fractures accounted for the three most common upperlimb hospitalised injuries in cycling.
Table C.34: Most commonly specified ICD diagnoses associated with cycling upper limb injuries leading to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S52 Fracture of forearm 556
S42 Fracture of shoulder and upper arm 277
S62 Fracture at wrist and hand level 120
S43 Dislocation of shoulder joint 71
S51 Open wound of forearm 18
As shown in Table C.35, the most common lower limb injuries were fractures and open wounds.
Table C.35: Most commonly specified ICD diagnoses associated with cycling lower limb injuries leading to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S82 Fracture of lower leg, including ankle 78
S81 Open wound of lower leg 36
S72 Fracture of femur 23
S92 Fracture of foot except ankle 12
S71 Open wound of hip and thigh 11
Table C.36 presents the five most common ICD diagnoses associated with head injuries in cycling.
%
n
n
n
n

37
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s
C.2.4. SKATING AND BLADING
This section describes the hospitalised injuries associated with participation in skating and blading.There was a total of 970 hospitalised cases recorded over the 2 year period 2003-2004, with thevast majority (86%) of these being due to a fall (Table C.37).
Table C.37: Broad mechanisms leading to skating and blading injury hospitalisation, NSW, 2003–2004
Mechanism n % Fall 836 86.2
Transport 74 7.6
Struck by or struck against 11 1.1
Overexertion and strenuous or repetitive movements 6 0.6
Others 28 2.9
Unspecified 15 1.5
Total 970 100.0
More than two in three skating and blading injuries were recorded as occurring in an unknownplace (Table C.38), which severely hampers the ability to suggest appropriate injury preventionmeasures in specific contexts/locations. For example, if it were known that the majority of injuriesoccurred in specific skating facilities, such as skate parks, suggestions could be made as to strategiesthat could be implemented to reduce injuries occurring in these places. Only 15% of injuriesoccurred in a sports and athletics area, which is most likely a skate park or rollerblading path.
Place of occurrence n % Sports and athletics area 142 14.6
Street and highway 62 6.4
Home 25 2.6
School 7 0.7
Other 54 5.6
Unknown 680 70.1
Total 970 100.0
As was the case for the three other sports described so far in this section of the report (Rugbyfootball, soccer and cycling), the most frequently occurring hospitalised injury for skating andblading was a fracture, accounting for nearly 4 in 5 injuries (Table C.39).
Table C.36: Most commonly specified ICD diagnoses associated with cycling head injuries leading tohospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S06 Intracranial injury 98
S01 Open wound of head 67
S02 Fracture of skull and facial bones 43
S00 Superficial injury of head 31
Table C.38: Place of occurrence of incidents leading to hospitalisation episodes for skating and bladinginjury, NSW, 2003–2004
% n
% n
n

38
Part C
: Profiles of Injury H
ospitalisation Episodes Associated w
ith S
elected Sport and Leisure A
ctivities
Nature of injury n % Fracture 758 78.1 Intracranial injury (including concussion) 42 4.3 Dislocation 37 3.8 Open wound 34 3.5 Superficial injury 26 2.7 Sprain or strain 15 1.5 Injury to muscle and tendon 12 1.2 Injury to internal organ 8 0.8 Other 38 3.9 Total 970 100.0
As shown in Table C.40, two-thirds of all hospitalised skating and blading injuries occurred to theupper limb. This was followed by the lower limb and head.
Injured body region n % Upper limb 636 65.6
Lower limb 195 20.1
Head 107 11.0
Trunk 24 2.5
Other and unspecified body part 8 0.8
Total 970 100.0
Consistent with the findings reported in Table C.37, the majority of skating and blading injuries werecaused by a fall, as demonstrated in Table C.41.
ICD external causes n % W02 Fall involving ice-skates, skis, roller-skates or skateboards 606 62.5W18 Other fall on same level 93 9.6V98 Other unspecified transport accidents 60 6.2W03 Other fall on same level due to collision with, or pushing by,
another person 48 4.9W01 Fall on same level from slipping, tripping and stumbling 35 3.6W19 Unspecified fall 32 3.3W17 Other fall from one level to another 10 1.0W25 Contact with sharp objects 9 0.9
Table C.42: Most commonly specified ICD external causes of skating and blading upper limb injuriesleading to hospitalisation, NSW, 2003–2004.
ICD external cause n W02 Fall involving ice-skates, skis, roller-skates or skateboards 393
W18 Other fall on same level 71
V98 Other unspecified transport accidents 41
W03 Other fall on same level due to collision with, or pushing by, another person 33
W01 Fall on same level from slipping, tripping and stumbling 26
Accordingly, for each of the three major body regions (upper limb, lower limb and head), the mostcommon external cause of injury was W02: Fall involving ice-skates, skis, roller-skates orskateboards, as shown in Table C.42, Table C.43 and Table C.44.
Table C.39: Nature of skating and blading injury associated with hospitalisation episodes, NSW,2003–2004
Table C.40: Injured body regions associated with hospitalisation episodes for skating and bladinginjury, NSW, 2003–2004
Table C.41: Most commonly specified ICD external causes leading to hospitalised skating and bladinginjuries, NSW, 2003–2004.
n
n %
% n
% n

39
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s
ICD diagnosis codes n % S52 Fracture of forearm 518 53.4S82 Fracture of lower leg, including ankle 139 14.3S06 Intracranial injury 42 4.3S62 Fracture at wrist and hand level 31 3.2S02 Fracture of skull and facial bones 23 2.4S09 Other and unspecified injuries of head 23 2.4S42 Fracture of shoulder and upper arm 22 2.3S43 Dislocation of shoulder joint 16 1.6S61 Open wound of wrist and hand 14 1.4S92 Fracture of foot, except ankle 12 1.2
Consistent with the previous table, the most common diagnosis of skating and blading upper limbinjury was a fracture of the forearm, followed by fractures of the wrist, hand, shoulder and upperarm, as demonstrated in Table C.46.
ICD principal diagnosis codes n S52 Fracture of forearm 636
S62 Fracture at wrist and hand level 518
S42 Fracture of shoulder and upper arm 31
S43 Dislocation of shoulder joint 22
S61 Open wound of wrist and hand 16
Fractures also accounted for three of the most common ICD diagnoses associated with lower limbinjuries in skating and blading, with the vast majority of these fractures occurring to the lower leg,including the ankle (Table C.47).
Table C.47: Most commonly specified ICD diagnoses associated with skating and blading lower limbinjuries leading to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S82 Fracture of lower leg, including ankle 139
S92 Fracture of foot, except ankle 12
S83 Dislocation, sprain and strain of joints and ligaments of knee 11
S72 Fracture of femur 9
S93 Dislocation, sprain and strain of joints and ligaments at ankle and foot level 8
ICD external cause n W02 Fall involving ice-skates, skis, roller-skates or skateboards 79
As shown in Table C.45, the most commonly recorded ICD diagnosis code for skating and bladinginjury was a fracture of the forearm. This has potential implications for the recommended use ofprotective equipment, such as elbow and wrist guards.
Table C.43: Most commonly specified ICD external causes of skating and blading lower limb injuriesleading to hospitalisation, NSW, 2003–2004.
ICD external causes n W02 Fall involving ice-skates, skis, roller-skates or skateboards 115
W18 Other fall on same level 15
W03 Other fall on same level due to collision with, or pushing by, another person 12
W01 Fall on same level from slipping, tripping and stumbling 7
Table C.44: Most commonly specified ICD external cause of skating and blading head injuries leadingto hospitalisation, NSW, 2003–2004.
Table C.45: Most commonly specified ICD diagnosis codes for skating and blading injuries treated inhospital, NSW, 2003–2004
Table C.46: Most commonly specified ICD diagnoses associated with skating and blading upper limbinjuries leading to hospitalisation, NSW, 2003–2004.
n
n
n
n
n
%

40
Part C
: Profiles of Injury H
ospitalisation Episodes Associated w
ith S
elected Sport and Leisure A
ctivities
Table C.49: Broad mechanisms leading to motorcycle riding injury hospitalisation, NSW, 2003–2004
Mechanism n % Transport 1025 97.0
Struck by or struck against 8 0.8
Fall 5 0.5
Other 19 1.8
Total 1057 100.0
It is perhaps more indicative of the sport/leisure participation focus of this report, that the mostfrequent place of occurrence of motorcycle riding injury was in a sports and athletics area, asshown in Table C.50.
Place of occurrence n % Sports and athletics area 357 33.8
Home 40 3.8
Street and highway 47 4.4
Other 280 26.5
Unknown 333 31.5
Total 1057 100.0
As with the previous four sports described in this section of the report, the most frequently occurringinjury requiring hospitalisation was a fracture, accounting for two in every three motorcycle ridinginjuries. This was followed by an open wound and intracranial injury, as demonstrated in TableC.51.
ICD principal diagnosis codes n S06 Intracranial injury 42
S02 Fracture of skull and facial bones 23
S09 Other and unspecified injuries of head 23
S00 Superficial injury of head 11
S01 Open wound of head 8
As shown in Table C.48, the most commonly occurring head injury was an intracranial injury,followed by a fracture of the skull and facial bones.
C.2.5. MOTORCYCLE RIDING
Over the period 2003–2004 there was a total of 1057 hospitalisation episodes associated withparticipation in motorcycle riding. As was described with cycling, participation in motorcycle ridingcan potentially be for sport and leisure purposes, or as a mode of transport. However, the cases inthis report were selected on the basis of having an ‘activity at the time of injury’ code referring tosport/leisure activity and therefore it is expected that the majority of the injuries described here arerelated to participation in the sport and leisure context. It can therefore be somewhat misleadingthat nearly all injuries were coded with the mechanism of transport, as shown in Table C.49.
Table C.48: Most commonly specified ICD diagnoses associated with skating and blading head injuriesleading to hospitalisation, NSW, 2003–2004.
Table C.50: Place of occurrence of incidents leading to hospitalisation episodes for motorcycle ridinginjury, NSW, 2003–2004
n %
n
n
%

41
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s
Table C.52: Injured body regions associated with hospitalisation episodes for motorcycle riding injury,NSW, 2003–2004
Injured body region n % Upper limb 390 36.9Lower limb 345 32.6Trunk 162 15.3Head 108 10.2Neck 28 2.6Unspecified body part 12 1.1Other 12 1.1Total 1057 100.0
Table C.53 presents the most commonly specified external causes of hospitalised motorcycle ridinginjuries. As with cycling, the majority of injuries are the result of a non-collision transport accident.
ICD external causes n % V28 Motorcycle rider injured in non-collision transport accidents 594 56.2V29 Motorcycle rider injured in other and unspecified traffic accidents 251 23.7V27 Motorcycle rider injured in collision with fixed or stationary objects 82 7.8V22 Motorcycle rider injured in collision with two- or three-wheeled motor
vehicle 43 4.1V23 Motorcycle rider injured in collision with car, pick-up truck or van 16 1.5V86 Occupant of other motor vehicle designed primarily for off-road use
injured in transport accident 16 1.5V20 Motorcycle rider injured in collision with pedestrian or animal 7 0.7W22 Striking against or struck by other objects 7 0.7
Table C.54 to C.56 list the most commonly specified external causes of injury codes for each of themajor body regions: upper limb, lower limb and head. For each of the three body regions, the mostcommon cause of injury was a motorcycle rider being injured in a non-collision transport accident(V28).
ICD external cause n V28 Motorcycle rider injured in non-collision transport accidents 238
V29 Motorcycle rider injured in other and unspecified traffic accidents 88
V27 Motorcycle rider injured in collision with fixed or stationary objects 29
V22 Motorcycle rider injured in collision with two- or three-wheeled motor vehicle 13
V18 Occupant of other motor vehicle designed primarily for off-use road use injured in transport accident
5
There was a similar distribution of injuries to the upper and lower limb, with two-thirds of allinjuries occurring to these two body regions, as shown in Table C.52
Nature of injury n % Fracture 699 66.1 Open wound 81 7.7 Intracranial injury (including concussion) 54 5.1 Superficial injury 44 4.2 Injury to internal organ 35 3.3 Dislocation 33 3.1 Sprain or strain 17 1.6 Injury to muscle and tendon 7 0.7 Other 87 8.2 Total 1057 100.0
Table C.51: Nature of motorcycle riding injury associated with hospitalisation episodes, NSW,2003–2004
Table C.53: Most commonly specified ICD external causes leading to hospitalised motorcycle ridinginjuries, NSW, 2003–2004.
Table C.54: Most commonly specified ICD external causes of motorcycle riding upper limb injuriesleading to hospitalisation, NSW, 2003–2004.
n
n %
n
n
%
%

42
Part C
: Profiles of Injury H
ospitalisation Episodes Associated w
ith S
elected Sport and Leisure A
ctivities
ICD external cause n V28 Motorcycle rider injured in non-collision transport accidents 81
V29 Motorcycle rider injured in other and unspecified traffic accidents 28
V27 Motorcycle rider injured in collision with fixed or stationary objects 8
As shown in Table C.57, the most commonly recorded diagnosis code for motorcycle riding was afracture of the lower leg, closely followed by a fracture of the forearm.
ICD diagnosis codes n % S82 Fracture of lower leg, including ankle 198 18.7 S52 Fracture of forearm 181 17.1 S42 Fracture of shoulder and upper arm 86 8.1 S62 Fracture at wrist and hand level 58 5.5 S06 Intracranial injury 54 5.1 S22 Fracture of rib(s), sternum and thoracic spine 54 5.1 S92 Fracture of foot, except ankle 43 4.1 S72 Fracture of femur 31 2.9 S43 Dislocation of shoulder joint 26 2.5 S81 Open wound of lower leg 24 2.3
ICD principal diagnosis codes n S52 Fracture of forearm 181
S42 Fracture of shoulder and upper arm 86
S62 Fracture at wrist and hand level 58
S43 Dislocation of shoulder joint 26
S51 Open wound of forearm 9
Table C.59: Most commonly specified ICD diagnoses associated with motorcycle riding lower limbinjuries leading to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S82 Fracture of lower leg, including ankle 198
S92 Fracture of foot, except ankle 43
S72 Fracture of femur 31
S81 Open wound of lower leg 24
S91 Open wound of ankle and foot 9
Table C.58, Table C.59 and Table C.60 list the most common ICD diagnoses for each of the majorbody regions: upper limb, lower limb and head. Fractures were the three most common diagnosesfor upper and lower limb injuries, and for the head, an intracranial injury was the most common.Unfortunately, the second most common diagnosis for a head injury was ‘other and unspecifiedinjuries of head’, which provides little information about the injury that occurred.
ICD external causes n V28 Motorcycle rider injured in non-collision transport accidents 177
V29 Motorcycle rider injured in other and unspecified traffic accidents 93
V27 Motorcycle rider injured in collision with fixed or stationary objects 23
V22 Motorcycle rider injured in collision with two- or three-wheeled motor vehicle
17
V23 Motorcycle rider injured in collision with car, pick-up truck or van 8
Table C.55: Most commonly specified ICD external causes of motorcycle riding lower limb injuriesleading to hospitalisation, NSW, 2003–2004.
Table C.56: Most commonly specified ICD external causes of motorcycle riding head injuries leadingto hospitalisation, NSW, 2003–2004.
Table C.57: Most commonly specified ICD diagnosis codes for motorcycle riding injuries treated inhospital, NSW, 2003–2004
Table C.58: Most commonly specified ICD diagnoses associated with motorcycle riding upper limbinjuries leading to hospitalisation, NSW, 2003–2004.
n
n
n %
n
n

43
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s
C.2.6. AUSTRALIAN FOOTBALL
Whilst it is not possible to differentiate well between rugby league and rugby union injuries due tolarge numbers of unspecified cases, it is possible to specifically identify Australian football.Following a similar pattern to rugby, the most frequent mechanism of Australian football injury wasa fall, which accounted for over 40% of all injuries (Table C.61). Consistent with the frequenttackling and grappling for the ball, almost 30% of injuries were caused by being struck.Unfortunately, one in five injuries was coded as being due to exposure to an unspecified factor.
Table C.60: Most commonly specified ICD diagnoses associated with motorcycle riding head injuriesleading to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S06 Intracranial injury 54
S09 Other and unspecified injuries of head 20
S01 Open wound of head 17
S12 Fracture of neck 13
S02 Fracture of skull and facial bones 11
Mechanism n % Fall 393 43.6
Struck by or struck against 264 29.3
Overexertion and strenuous or repetitive movements 42 4.7
Others 26 2.9
Unspecified 177 19.6
Total 902 100.0
The vast majority of Australian football injuries occurred in a sports and athletics area, as shown inTable C.62.
Table C.62: Place of occurrence of incidents leading to hospitalisation episodes for Australian footballinjury, NSW, 2003–2004
Place of occurrence n % Sports and athletics area 649 72.0
School 32 3.5
Home 10 1.1
Other 9 1.0
Unknown 202 22.4
Total 902 100.0
As presented in Table C.63, fractures accounted for three in every five Australian football injuries,which was by far the most frequently occurring injury.
Table C.63: Nature of Australian football injury associated with hospitalisation episodes, NSW, 2003–2004
Nature of injury n % Fracture 557 61.8 Dislocation 68 7.5 Sprain or strain 58 6.4 Intracranial injury (including concussion) 56 6.2 Injury to muscle and tendon 26 2.9 Superficial injury 16 1.8 Injury to internal organ 16 1.8 Open wound 14 1.6 Other 91 10.1 Total 902 100.0
Table C.61: Broad mechanisms leading to Australian football injury hospitalisation, NSW, 2003–2004
n
n %
n %
n %

44
Part C
: Profiles of Injury H
ospitalisation Episodes Associated w
ith S
elected Sport and Leisure A
ctivities
Table C.65: Most commonly specified ICD external causes leading to hospitalised Australian footballinjuries, NSW, 2003–2004.
ICD external causes n % W03 Other fall on same level due to collision with, or pushing by, another
person 314 34.8
W50 Hit, struck, kicked, twisted, bitten or scratched by another person 121 13.4W51 Striking against or bumped into by another person 81 9.0W21 Striking against or struck by sports equipment 50 5.5X50 Overexertion and strenuous or repetitive movements 42 4.7W18 Other fall on same level 41 4.5W01 Fall on same level from slipping, tripping and stumbling 26 2.9
Accordingly, for all three major body regions, the most common external cause of injury was a fallon same level due to collision with, or pushing by, another person (Table C.66, Table C.67 andTable C.68).
ICD external cause n W03 Other fall on same level due to collision with, or pushing by, another person 140
W21 Striking against or struck by sports equipment 33
W50 Hit, struck, kicked, twisted, bitten or scratched by another person 31
W18 Other fall on same level 30
Overexertion and strenuous or repetitive movements was the second most common external causeof lower limb injury in Australian football, followed by being hit or struck (Table C.67).
ICD external causes n W03 Other fall on same level due to collision with, or pushing by, another person 98
X50 Overexertion and strenuous or repetitive movements 32
W50 Hit, struck, kicked, twisted, bitten or scratched by another person 18
W01 Fall on same level from slipping, tripping and stumbling 12
Whilst the most frequent external cause of head injury in Australian football was a fall (W03), thiswas closely followed by being hit or struck (Table C.68).
The most frequently reported ICD external causes of Australian football injury are shown in TableC.65. As with the other football codes of rugby and soccer, the most common external cause ofhospitalised Australian football injury was coded as W03: other fall on same level due to collisionwith, or pushing by, another person. This represented approximately one-third of all injuries.Consistent with the contact encountered in Australian football, there was also a large number ofinjuries cause by being hit or struck.
Table C.64: Injured body regions associated with hospitalisation episodes for Australian football injury,NSW, 2003–2004
Injured body region n % Upper limb 378 41.9Lower limb 260 28.8Head 195 21.6Trunk 41 4.5Neck 23 2.5
Other and unspecified 5 0.5
Total 902 100.0
Other and
The most commonly injured body region was the upper limb, with more than 40% of all injuries.There was a similar proportion of lower limb and head injuries, as shown in Table C.64.
Table C.66: Most commonly specified ICD external causes of Australian football upper limb injuriesleading to hospitalisation, NSW, 2003–2004.
Table C.67: Most commonly specified ICD external causes of Australian football lower limb injuriesleading to hospitalisation, NSW, 2003–2004.
n
n
n
n
%
%

45
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s
ICD diagnosis codes n % S62 Fracture at wrist and hand level 137 15.2S82 Fracture of lower leg, including ankle 132 14.6S52 Fracture of forearm 123 13.6S02 Fracture of skull and facial bones 93 10.3S83 Dislocation, sprain and strain of joints and ligaments of knee 62 6.9S06 Intracranial injury 56 6.2S42 Fracture of shoulder and upper arm 42 4.7S43 Dislocation of shoulder joint 33 3.7S09 Other and unspecified injuries of head 30 3.3S63 Dislocation, sprain and strain of joints and ligaments at wrist
and hand level 18 2.0
ICD principal diagnosis codes n S62 Fracture at wrist and hand level 137S52 Fracture of forearm 123S42 Fracture of shoulder and upper arm 42S43 Dislocation of shoulder joint 33S63 Dislocation, sprain and strain of joints and ligaments of wrist and hand 18
Table C.71: Most commonly specified ICD diagnoses associated with Australian football lower limbinjuries leading to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S82 Fracture of lower leg, including ankle 132S83 Dislocation, sprain and strain of joints and ligaments of knee 62S72 Fracture of femur 13S86 Injury of muscle and tendon at lower leg level 8
The most common ICD diagnoses for each of the major body regions, upper limb, lower limb andhead, are listed in Table C.70, Table C.71 and Table C.72. The upper and lower limb injuriesprimarily consisted of fractures and dislocations. There was also a large proportion of fractures whenconsidering the head injuries encountered in Australian football. However, as with many of the tensports listed in this section of the report, there are many head injuries that are coded into a categorywhich includes unspecified injuries.
Table C.68: Most commonly specified ICD external causes of Australian football head injuries leadingto hospitalisation, NSW, 2003–2004.
ICD external cause n W03 Other fall on same level due to collision with, or pushing by, another person 59
W50 Hit, struck, kicked, twisted, bitten or scratched by another person 57
W51 Striking against or bumped into by another person 50
W21 Striking against or struck by sports equipment 12
Fractures accounted for five of the ten most commonly recorded ICD diagnosis codes for Australianfootball, most often occurring at the wrist, hand, lower leg, forearm, skull and face (Table C.69). Thefact that there were a large number of fractures reflects the severity of injuries that are treated in thehospital setting.
Table C.69: Most commonly specified ICD diagnosis codes for Australian football injuries treated inhospital, NSW, 2003–2004
Table C.70: Most commonly specified ICD diagnoses associated with Australian football upper limbinjuries leading to hospitalisation, NSW, 2003–2004.
n
n
n
n
%

46
Part C
: Profiles of Injury H
ospitalisation Episodes Associated w
ith S
elected Sport and Leisure A
ctivitiesTable C.72: Most commonly specified ICD diagnoses associated with Australian football head injuries
leading to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S02 Fracture of skull and facial bones 93 S06 Intracranial injury 56 S01 Open wound of head 7
One in five equestrian sports injuries occurred in a sports and athletics area. However, more thanhalf of all injuries occurred in an unknown location, as shown in Table C.74.
Table C.75 shows that the most common principal diagnosis of the equestrian sports injuries was afracture, with more than half of all cases. The second most common injury was an intracranialinjury, including concussion.
Table C.73: Broad mechanisms leading to equestrian sports injury hospitalisation, NSW, 2003–2004
Mechanism n % Transport 800 91.5
Fall 11 1.3
Other 63 7.1
Total 874 100.0
Place of occurrence n % Sports and athletics area 175 20.0Home 37 4.2Street and highway 22 2.5Other 167 19.1Unknown 473 54.1Total 874 100.0
C.2.7. EQUESTRIAN SPORTS
There were a total of 874 hospitalised injuries associated with equestrian sports over the period ofinterest. The vast majority of these were listed with the mechanism of transport (Table C.73).
Table C.75: Nature of equestrian sports injury associated with hospitalisation episodes, NSW,2003–2004
Nature of injury n % Fracture 466 53.3 Intracranial injury (including concussion) 102 11.7 Superficial injury 73 8.4 Open wound 28 3.2 Dislocation 28 3.2 Injury to internal organ 28 3.2 Sprain or strain 17 1.9 Injury to muscle and tendon 10 1.1 Other 122 14.0 Total 874 100.0
Table C.74: Place of occurrence of incidents leading to hospitalisation episodes for equestrian sportsinjury, NSW, 2003–2004
n
n %
n %
n %

47
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s
The most frequently specified ICD external causes of equestrian sports injury are shown in TableC.77. The considerable majority of injuries was coded as V80: ‘animal rider or occupant of animal-drawn vehicle injured in transport accident’. However, the third most commonly recorded ICDexternal cause was V28, which is ‘motorcycle rider injured in non-collision transport accidents’.This is obviously a coding error and demonstrates that incorrect coding can hamper the ability tounderstand the pattern of injuries in specific sports.
Table C.76: Injured body regions associated with hospitalisation episodes for equestrian sports injury,NSW, 2003–2004
Injured body region n % Upper limb 296 33.9Trunk 205 23.5Head 180 20.6Lower limb 148 16.9Neck 34 3.9Other and unspecified
11 1 3Total 874 100.0
11 1.3
Table C.78, Table C.79 and Table C.80 list the top external cause of injury codes for each of themajor body regions: upper limb, lower limb and head. For all three body regions, the most commoncause of injury was V80: ‘animal rider or occupant of animal-drawn vehicle injured in transportaccident’. As discussed for Table C.77, there are several coding errors, and these are again listed inthe external causes of upper and lower limb equestrian sports injuries.
ICD external causes n % V80 Animal rider or occupant of animal-drawn vehicle injured in transport
accident 743 85.0W55 Bitten or struck by other mammals 36 4.1V28 Motorcycle rider injured in non-collision transport accidents 30 3.4V06 Pedestrian injured in collision with other non-motor vehicle 9 1.0W23 Caught, crushed, jammed or pinched in or between objects 6 0.7
n %
Table C.78: Most commonly specified ICD external causes of equestrian sports upper limb injuriesleading to hospitalisation, NSW, 2003–2004.
ICD external cause n V80 Animal rider or occupant of animal-drawn vehicle injured in transport accident 262
W17 Other fall from one level to another 12
Table C.79: Most commonly specified ICD external causes of equestrian sports lower limb injuriesleading to hospitalisation, NSW, 2003–2004.
ICD external causes n V80 Animal rider or occupant of animal-drawn vehicle injured in transport
accident 106
W55 Bitten or struck by other mammals 14
V28 Motorcycle rider injured in noncollision transport accidents 11
One in three injuries occurred to the upper limb, as demonstrated in Table C.76. This was followedby injuries to the trunk and head, which each accounted for approximately 20% of all injuries.
Table C.77: Most commonly specified ICD external causes leading to hospitalised equestrian sportsinjuries, NSW, 2003–2004.
n %
n
n

48
Part C
:P
rofiles of Injury Hospitalisation Episodes A
ssociated with
Selected S
port and Leisure Activities
Accordingly, the most common diagnoses for upper limb (Table C.82) and lower limb (Table C.83)injuries were fractures. As described earlier, there are many injuries to the head that are notspecified (Table C.84).
C.2.8. ICE AND SNOW SPORTS
Ice and snow sports include activities such as alpine skiing, cross-country skiing, snowboarding andtobogganing. Over 2003–2004, 841 people were hospitalised for an injury sustained during one ofthese activities. The vast majority of these injury cases were the result of a fall (Table C.85).Unspecifieds were the second most commonly recorded mechanism category.
Table C.81: Most commonly specified ICD diagnosis codes for equestrian sports injuries treated in hospital, NSW, 2003–2004
ICD diagnosis codes n % S52 Fracture of forearm 149 17.0S06 Intracranial injury 102 11.7S42 Fracture of shoulder and upper arm 82 9.4S82 Fracture of lower leg, including ankle 70 8.0S22 Fracture of rib(s), sternum and thoracic spine 48 5.5S32 Fracture of lumbar spine and pelvis 45 5.1S30 Superficial injury of abdomen, lower back and pelvis 30 3.4S62 Fracture at wrist and hand level 21 2.4
Table C.82: Most commonly specified ICD diagnoses associated with equestrian sports upper limbinjuries leading to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S52 Fracture of forearm 149
S42 Fracture of shoulder and upper arm 82
S62 Fracture at wrist and hand level 21
S43 Dislocation of shoulder joint 15
ICD principal diagnosis codes n S52 Fracture of forearm 149
S42 Fracture of shoulder and upper arm 82
S62 Fracture at wrist and hand level 21
S43 Dislocation of shoulder joint 15
ICD principal diagnosis codes n S06 Intracranial injury 102
S09 Other and unspecified injuries of head 32
S02 Fracture of skull and facial bones 18
S01 Open wound of head 16
As with many other sports in this section of the report, the most common diagnosis of injury was afracture of the forearm (Table C.81). In fact, the majority of the top ten diagnoses for equestriansports injury were fractures.
Table C.80: Most commonly specified ICD external causes of equestrian sports head injuries leading tohospitalisation, NSW, 2003–2004.
ICD external cause n V80 Animal rider or occupant of animal-drawn vehicle injured in transport accident 195
W55 Bitten or struck by other mammals 9
Table C.83: Most commonly specified ICD diagnoses associated with equestrian sports lower limbinjuries leading to hospitalisation, NSW, 2003–2004.
Table C.84: Most commonly specified ICD diagnoses associated with equestrian sports head injuriesleading to hospitalisation, NSW, 2003–2004.
n
n
n
n
n
%

49
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s
As most ice and snow sports and leisure activities are undertaken in alpine ski resorts, it is notsurprising that more than three-quarters of all injuries were coded as occurring in a place for sportand athletics (Table C.86).
Consistent with the major injury mechanism, the most common injuries were fractures orsprains/strains which, together, accounted for three-quarters of all injuries (Table C.87).
The lower limb accounted for more than half of all principal diagnoses for ice and snow sportrelated injuries.
Table C.86: Place of occurrence of incidents leading to hospitalisation episodes for ice and snow sportsinjury, NSW, 2003–2004
Place of occurrence n % Sports and athletics area 640 76.1Other 129 15.3Unknown 72 8.6Total 841 100.0
Nature of injury n % Fracture 346 41.1 Sprain or strain 285 33.9 Dislocation 46 5.5 Injury to muscle and tendon 35 4.2 Intracranial injury (including concussion) 28 3.3 Open wound 21 2.5 Injury to internal organ 15 1.8 Superficial injury 14 1.7 Other 51 6.1 Total 841 100.0
The most commonly specified external causes are shown in Table C.89 and are consistent with theresults of Table C.85. As would be expected, the most common external cause was W02: Fallinvolving ice-skates, skis, roller-skates or skateboards.
Injured body region n % Lower limb 438 52.1Upper limb 219 26.0Trunk 88 10.5Head 77 9.2Neck 14 1.7Other 5 0.6Total 841 100.0
Table C.85: Broad mechanisms leading to ice and snow sports injury hospitalisation, NSW, 2003–2004
Mechanism n % Fall 535 63.6
Overexertion and strenuous or repetitive movements 60 7.1
Struck by or struck against 41 4.9
Transport 13 1.5
Other 27 3.2
Unspecified 165 19.6
Total 841 100.0
Table C.87: Nature of injury associated with hospitalisation episodes for ice and snow sports injury,NSW, 2003–2004
Table C.88: Injured body regions associated with hospitalisation episodes for ice and snow sportsinjury, NSW, 2003–2004
n %
n %
n %
n %

50
Part C
: Profiles of Injury H
ospitalisation Episodes Associated w
ith S
elected Sport and Leisure A
ctivities
Tables C.90, C.91 and C.92 present the main external causes across the major body regions.Although falls feature prominently in each table. A significant number of cases were coded as“unspecified” or exposure to unspecified factor.
ICD external causes n % W02 Fall involving ice-skates, skis, roller-skates or skateboards 405 48.2X50 Overexertion and strenuous or repetitive movements 60 7.1W03 Other fall on same level due to collision with, or pushing by, another
person 37 4.4W01 Fall on same level from slipping, tripping and stumbling 27 3.2W22 Striking against or struck by other objects 17 2.0W00 Fall on same level involving ice and snow 13 1.5W18 Other fall on same level 13 1.5
ICD diagnosis codes n % S83 Dislocation, sprain and strain of joints and ligaments of knee 283 33.7S82 Fracture of lower leg, including ankle 104 12.4S52 Fracture of forearm 84 10.0S42 Fracture of shoulder and upper arm 52 6.2S32 Fracture of lumbar spine and pelvis 29 3.4S06 Intracranial injury 28 3.3S62 Fracture at wrist and hand level 24 2.9S09 Other and unspecified injuries of head 23 2.7S22 Fracture of rib(s), sternum and thoracic spine 18 2.1S63 Dislocation, sprain and strain of joints and ligaments at wrist
and hand level 17 2.0
In contrast to fractures being the number one nature of injury (Table C.87), the single most commoninjury diagnosis was a dislocation, sprain and strain of joints and ligaments of knee and this wasreported in a third of all cases (Table C.93). This injury diagnosis is quite common in severe skiinjuries where torsional forces on the knee during a fall can lead to ACL rupture. Lower legfractures in this context may be related to the ski binding system and inadequate releasemechanisms. One in ten injury hospitalisation episodes was for a forearm facture, probably as theresult of the attempt of a person putting out their arm/s to stabilise themselves during a fall.
Table C.92: Most commonly specified ICD external causes of ice and snow sports head injuries leadingto hospitalisation, NSW, 2003–2004.
ICD external cause n W02 Fall involving ice-skates, skis, roller-skates or skateboards 46
W01 Fall on same level from slipping, tripping and stumbling 10
W03 Other fall on same level due to collision with, or pushing by, another person 8
ICD external cause n W02 Fall involving ice-skates, skis, roller-skates or skateboards 103
W01 Fall on same level from slipping, tripping and stumbling 12
W03 Other fall on same level due to collision with, or pushing by, another person 12
Table C.91: Most commonly specified ICD external causes of ice and snow sports lower limb injuriesleading to hospitalisation, NSW, 2003–2004.
ICD external causes n W02 Fall involving ice-skates, skis, roller-skates or skateboards 204
X50 Overexertion and strenuous or repetitive movements 45
W03 Other fall on same level due to collision with, or pushing by, another person 14
Table C.89: Most commonly specified ICD external causes leading to hospitalised ice and snow sportsinjuries, NSW, 2003–2004.
Table C.90: Most commonly specified ICD external causes of ice and snow sports upper limb injuriesleading to hospitalisation, NSW, 2003–2004.
Table C.93: Most commonly specified ICD diagnosis codes for ice and snow sports injuries treated inhospital, NSW, 2003–2004
n
n
n
n
n %
%

51
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s Tables C.94, C.95 and C.96 present the most common ICD diagnoses associated with ice and snowsports injuries to the major body regions. Forearm factures were the most common upper limbinjury and injuries to the knee, the most common lower limb injury. Intracranial injuries were themajor type of head injury, but there was also a large number of cases with an unspecified headinjury diagnosis.
ICD principal diagnosis codes n S52 Fracture of forearm 84
S42 Fracture of shoulder and upper arm 52
S62 Fracture at wrist and hand level 24
S63 Dislocation, sprain and strain of joints and ligaments at wrist and hand level
17
S43 Dislocation of shoulder joint 9
Table C.95: Most commonly specified ICD diagnoses associated with ice and snow sports lower limbinjuries leading to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S83 Dislocation, sprain and strain of joints and ligaments of knee 283
S82 Fracture of lower leg, including ankle 104
S72 Fracture of femur 14
S86 Injury of muscle and tendon at lower leg level 7
C.2.9. BASKETBALL
Like most other sporting activities considered in this part of the report, the majority of basketballinjuries were the result of a fall (Table C.97). Basketball is often rated as a non-collision sport butone-in five hospitalised cases sustained their injuries as a result of being stuck by or struck against aperson or object.
ICD principal diagnosis codes n S06 Intracranial injury 28
S09 Other and unspecified injuries of head 23
S02 Fracture of skull and facial bones 14
S01 Open wound of head 9
S13 Dislocation, sprain and strain of joints and ligaments at neck level
5
Not surprisingly, given the nature of the activity, the majority of basketball hospitalisation episodeswere the result of an injury event in a sports and athletics area (Table C.98).
Table C.97: Broad mechanisms leading to basketball injury hospitalisation, NSW, 2003–2004
Mechanism n % Fall 245 41.9
Struck by or struck against 124 21.2
Overexertion and strenuous or repetitive movements 80 13.7
Other 31 5.3
Unspecified 105 17.9
Total 585 100.0
Table C.94: Most commonly specified ICD diagnoses associated with ice and snow sports upper limb injuries leading to hospitalisation, NSW, 2003–2004.
Table C.96: Most commonly specified ICD diagnoses associated with ice and snow sports head injuriesleading to hospitalisation, NSW, 2003–2004.
n
n
n
n %

52
Part C
:P
rofiles of Injury Hospitalisation Episodes A
ssociated with
Selected S
port and Leisure Activities
The major nature of injury was a fracture (Table C.99), consistent with the major mechanisms ofinjury in Table C.97.
Place of occurrence n % Sports and athletics area 361 61.7
School 49 8.4
Home 9 1.5
Other 11 1.9
Unknown 155 26.5
Total 585 100.0
In contrast to most published studies of basketball injuries, the upper limb accounted for more thanhalf of all injuries (Table C.100). This is probably due to the severity of the sustained injuries andthe fact that most lower limb injuries in basketballers do not require hospitalisation.
Table C.99: Nature of basketball injury associated with hospitalisation episodes, NSW, 2003–2004
Nature of injury n % Fracture 319 54.5 Sprain or strain 66 11.3 Dislocation 60 10.3 Injury to muscle and tendon 46 7.9 Intracranial injury (including concussion) 18 3.1 Superficial injury 14 2.4 Open wound 12 2.1 Other 50 8.5 Total 585 100.0
Table C.101 shows that the major external cause of basketball hospitalisation episodes was a fall ona same level. However, overexertion and strenuous and repetitive movements and strikesagainst/from sports equipment were also common.
Injured body region n % Upper limb 300 51.3Lower limb 187 32.0Head 70 12.0Trunk 16 2.7Neck and other 12 2.1Total 585 100.0
ICD external causes n % W18 Other fall on same level 115 19.7
X50 Overexertion and strenuous or repetitive movements 80 13.7
W21 Striking against or struck by sports equipment 80 13.7
W03 Other fall on same level due to collision with, or pushing by, another person
58 9.9
W01 Fall on same level from slipping, tripping and stumbling 55 9.4
W50 Hit, struck, kicked, twisted, bitten or scratched by another person 45 7.7
W51 Striking against or bumped into by another person 23 3.9
Table C.98: Place of occurrence of incidents leading to hospitalisation episodes for basketball injury, NSW, 2003–2004
Table C.100: Injured body regions associated with hospitalisation episodes for basketball injury, NSW, 2003–2004
Table C.101: Most commonly specified ICD external causes leading to hospitalised basketball injuries, NSW, 2003–2004.
n %
n %
n
n %
%

53
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s
ICD external cause n W18 Other fall on same level 82
W21 Striking against or struck by sports equipment 40
W03 Other fall on same level due to collision with, or pushing by, another person 36
W01 Fall on same level from slipping, tripping and stumbling 31
ICD external causes n X50 Overexertion and strenuous or repetitive movements 64
W18 Other fall on same level 19
W03 Other fall on same level due to collision with, or pushing by, another person 9
Table C.104: Most commonly specified ICD external causes of basketball head injuries leading to hospitalisation, NSW, 2003–2004.
ICD external cause n W21 Striking against or struck by sports equipment 16
W50 Hit, struck, kicked, twisted, bitten or scratched by another person 14
W18 Other fall on same level 12
W01 Fall on same level from slipping, tripping and stumbling 10
W51 Striking against or bumped into by another person 9
ICD diagnosis codes n % S52 Fracture of forearm 146 25.0
S62 Fracture at wrist and hand level 92 15.7
S83 Dislocation, sprain and strain of joints and ligaments of knee 68 11.6
S82 Fracture of lower leg, including ankle 40 6.8
S86 Injury of muscle and tendon at lower leg level 38 6.5
S02 Fracture of skull and facial bones 25 4.3
S43 Dislocation of shoulder joint 21 3.6
S06 Intracranial injury 18 3.1
S63 Dislocation, sprain and strain of joints and ligaments at wrist and hand level
14 2.4
ICD principal diagnosis codes n S52 Fracture of forearm 146S62 Fracture at wrist and hand level 92S43 Dislocation of shoulder joint 21S63 Dislocation, sprain and strain of joints and ligaments of wrist and hand
level 14
S42 Fracture of shoulder and upper arm 11
Interestingly, factures of the forearm and wrist/hand accounted for over 40% of all injuries (TableC.105). Dislocations, sprains and strains of joints and ligaments of the knee were the third mostcommon injury diagnosis overall. Tables C.106, C.107 and C.108 summarise the major diagnosesin each of the major body regions.
The most common external causes of injury, according to the major body region injured, are shownin Tables C.102, C.103 and C.104. Upper limb injuries were most commonly caused by falls, thelower limb injuries by overexertion and strenuous and repetitive movements and the head injuriesby strikes against/from sports equipment.
Table C.102: Most commonly specified ICD external causes of basketball upper limb injuries leadingto hospitalisation, NSW, 2003–2004.
Table C.103: Most commonly specified ICD external causes of basketball lower limb injuries leading to hospitalisation, NSW, 2003–2004.
Table C.105: Most commonly specified ICD diagnosis codes for basketball injuries treated in hospital, NSW, 2003–2004
Table C.106: Most commonly specified ICD diagnoses associated with basketball upper limb injuries leading to hospitalisation, NSW, 2003–2004.
n
n
n
n
n
%

54
Part C
: Profiles of Injury H
ospitalisation Episodes Associated w
ith S
elected Sport and Leisure A
ctivities
ICD principal diagnosis codes n S83 Dislocation, sprain and strain of joints and ligaments of knee 68S82 Fracture of lower leg, including ankle 40S86 Injury of muscle and tendon at lower leg level 38S93 Dislocation, sprain and strain of joints and ligaments at ankle and foot level 13
ICD principal diagnosis codes n S02 Fracture of skull and facial bones 25 S06 Intracranial injury 18 S00 Superficial injury of head 6
Table C.109: Broad mechanisms leading to netball injury hospitalisation, NSW, 2003–2004
Mechanism n % Fall 195 36.0
Overexertion and strenuous or repetitive movements 140 25.9
Struck by or struck against 58 10.7
Other 14 2.6
Unspecified 134 24.8
Total 541 100.0
The vast majority of injuries occurred in a place for sport and athletics (Table C.110), which isconsistent with the need for the game to be placed on a netball court. A large number of cases didnot have the place of injury specified.
Place of occurrence n % Sports and athletics area 434 80.2
School 15 2.8
Other 11 2.0
Unknown 81 15.0
Total 541 100.0
The major nature of injury was a fracture (Table C.111), followed by a sprain/strain or injury tomuscle/tendon.
C.2.10. NETBALL
Falls were the major cause of netball related hospitalisation episodes (Table C.109). Overexertionand strenuous or repetitive movements accounted for a quarter of all injuries; strikes were much lesscommon a cause of netball injury than they were for basketball injury. Almost a quarter of allinjuries were coded as exposure to unspecified factor.
Table C.107: Most commonly specified ICD diagnoses associated with basketball lower limb injuries leading to hospitalisation, NSW, 2003–2004.
Table C.108: Most commonly specified ICD diagnoses associated with basketball head injuries leading to hospitalisation, NSW, 2003–2004.
Table C.110: Place of occurrence of incidents leading to hospitalisation episodes for netball injury, NSW, 2003–2004
Table C.111: Nature of netball injury associated with hospitalisation episodes, NSW, 2003–2004
Nature of injury n % Fracture 209 38.6 Sprain or strain 136 25.1 Injury to muscle and tendon 114 21.1 Dislocation 37 6.8 Intracranial injury (including concussion) 8 1.5 Open wound 5 0.9 Other 32 5.9 Total 541 100.0
n %
n %
n %
n
n

55
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s In contrast to the basketball injuries, the lower limb was the most commonly injured body region inhospitalised netball players (Table C.112).
Table C.112: Injured body regions associated with hospitalisation episodes for netball injury, NSW, 2003–2004
Injured body region n % Lower limb 307 56.7Upper limb 189 34.9Head 33 6.1Trunk 7 1.3Neck and other 5 0.9Total 541 100.0
Table C.113 shows that the major external cause of the hospitalised netball cases was ‘overexertionand strenuous or repetitive movements’, consistent with the high level of soft tissue injuries shownin Table C.111. Whilst body contact injuries were not common, a significant number of injurieswere associated with falls as the result of body contact.
ICD external causes n % X50 Overexertion and strenuous or repetitive movements 140 25.9W18 Other fall on same level 75 13.9W01 Fall on same level from slipping, tripping and stumbling 53 9.8W03 Other fall on same level due to collision with, or pushing by, another
person 50 9.2W21 Striking against or struck by sports equipment 25 4.6W51 Striking against or bumped into by another person 16 3.0W50 Hit, struck, kicked, twisted, bitten or scratched by another person 15 2.8
ICD external cause n W18 Other fall on same level 54
W01 Fall on same level from slipping, tripping and stumbling 33
W03 Other fall on same level due to collision with, or pushing by, another person 33
W21 Striking against or struck by sports equipment 21
ICD external causes n X50 Overexertion and strenuous or repetitive movements 127
W18 Other fall on same level 16
W01 Fall on same level from slipping, tripping and stumbling 12
W03 Other fall on same level due to collision with, or pushing by, another person 12
Tables C.114, C.115 and C.116 list the most commonly specified external causes across major bodyregions. Falls featured prominently on the list for upper limb injuries and overexertion andstrenuous or repetitive movements for the lower limbs. Head/neck injuries, whilst uncommon, weregenerally associated with falls.
Table C.113: Most commonly specified ICD external causes leading to hospitalised netball injuries, NSW, 2003–2004.
Table C.114: Most commonly specified ICD external causes of netball upper limb injuries leading to hospitalisation, NSW, 2003–2004.
Table C.115: Most commonly specified ICD external causes of netball lower limb injuries leading to hospitalisation, NSW, 2003–2004.
n %
n
n
n
%

56
Part C
: Profiles of Injury H
ospitalisation Episodes Associated w
ith S
elected Sport and Leisure A
ctivities
ICD diagnosis codes n % S83 Dislocation, sprain and strain of joints and ligaments of knee 139 25.7S52 Fracture of forearm 112 20.7S86 Injury of muscle and tendon at lower leg level 110 20.3S62 Fracture at wrist and hand level 46 8.5S82 Fracture of lower leg, including ankle 29 5.4S09 Other and unspecified injuries of head 11 2.0S63 Dislocation, sprain and strain of joints and ligaments at wrist
and hand level 10 1.8S93 Dislocation, sprain and strain of joints and ligaments at ankle
and foot level 10 1.8S06 Intracranial injury 8 1.5S02 Fracture of skull and facial bones 7 1.3
Table C.118: Most commonly specified ICD diagnoses associated with netball upper limb injuries leading to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S52 Fracture of forearm 112
S62 Fracture at wrist and hand level 46
S63 Dislocation, sprain and strain of joints and ligaments of wrist and hand 10
S42 Fracture of shoulder and upper arm 7
S43 Dislocation of shoulder joint 5
Table C.119: Most commonly specified ICD diagnoses associated with netball lower limb injuries leading to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S83 Dislocation, sprain and strain of joints and ligaments of knee 139
S86 Injury of muscle and tendon at lower leg level 110
S82 Fracture of lower leg, including ankle 29
S93 Dislocation, sprain and strain of joints and ligaments at ankle and foot level 10
Table C.120: Most commonly specified ICD diagnoses associated with netball head injuries leading to hospitalisation, NSW, 2003–2004.
ICD principal diagnosis codes n S06 Intracranial injury 8
S02 Fracture of skull and facial bones 7
The most common upper limb injuries were fractures (Table C.118) and dislocations, sprains andstrains of joints and ligaments of knee were the most common lower limb injuries (Table C.119).Although a number of head injury cases were identified, the majority of these had other andunspecified diagnoses (Table C.120).
Table C.117 lists the most common principal diagnoses of injury in the hospitalised netballers,which are consistent with the common natures of injury and injury mechanisms.
ICD external cause n W01 Fall on same level from slipping, tripping and stumbling 7
W03 Other fall on same level due to collision with, or pushing by, another person 5
W50 Hit, struck, kicked, twisted, bitten or scratched by another person 5
W51 Striking against or bumped into by another person 5
Table C.116: Most commonly specified ICD external causes of netball head injuries leading to hospitalisation, NSW, 2003–2004.
Table C.117: Most commonly specified ICD diagnosis codes for netball injuries treated in hospital, NSW, 2003–2004
n
n
n
n
n
%

57
Par
t C
: P
rofi
les
of In
jury
Hos
pita
lisat
ion
Epis
odes
Ass
ocia
ted
wit
h S
elec
ted
Spo
rt a
nd L
eisu
re A
ctiv
itie
s C.3 IMPLICATIONS
This part of the report has presented detailed information about the nature and diagnoses of theinjuries leading to hospitalisation across a range of sport and leisure activities. The presented analysesare based on the principal diagnosis only, and hence underestimate the actual number of most of theinjury categories and diagnoses because multiple injuries have not been taken into account.
Only cases positively identified as being associated with one of the sport/leisure categories describedin this report have been included here. Many more sports injuries occur and are either coded to otheractivities or to non-specific codes such as “football unspecified”. A further limitation of the data forrugby is that the use of the ICD-10-AM codes does not differentiate well between different codesbecause of large numbers cases with unspecified rugby code. Improvement in the specificity ofreporting of football codes, particularly the rugby codes in a state like NSW, would enhance the abilityof ICD-coded data to identify particular priority groups.
The detailed analyses in this report serve to emphasise the limitations of incomplete and non-specificdetail. In some instances, up to almost half of all cases had missing data or an “unspecified”categorisation on variables such as external cause of injury and place of injury. These data fields arecritical for understanding about the factors likely to be surrounding an injury event, and hence arenecessary for prevention purposes. This lack of detail hinders the ability to identify priority areas forinjury prevention strategies and reiterates the need for the recording of more detailed clinicalinformation and the improved coding of hospitalisation episodes data.
No attempt has been made here to suggest specific injury prevention measures based on the profilespresented here. Interpretation of this data needs to be made within the context of each specificactivity and the physical manoeuvres it requires. Furthermore, it is not possible, with this data, toidentify whether or not the injuries were sustained during organised sport, informal sport of justgeneral play. This is an unfortunate limitation of the ICD-10-AM system because such informationwould also further enhance the potential to properly inform prevention efforts.
The data presented in this report is also limited in that it does not provide very specific details aboutthe chain of events leading to the injury and, in many instances, the true mechanistic reason for theinjury occurrence. This is a limitation of the ICD that hinders the use of this data for sports injuryprevention efforts. For example, without knowing what particular activity the injured person wasparticipating in at the time (eg. in rugby union the injured person may have been injured as a result ofbeing tackled, or because they slipped over whilst running, or because of ball mishandling, or scrumengagement/disengagement), it is not possible to suggest sports-specific injury prevention strategies forany sport, but to only talk in generalities.
More needs to be done in order to improve the coding of sport-related cases routinely collected inlarge administrative databases, such as hospital and death data. While the validity of the ICD-10-AMdiagnosis codes is well established due to their value in health service utilisation applications, verylittle is known of the validity of external causes of injury codes. These latter are vital to theidentification of the sport/leisure cases and to the overall injury prevention efforts as they indicate themechanism and the circumstances in which injury occurs. In addition, the relatively high number ofmissing cases (i.e. activity and place of injury codes) and unspecified codes suggest that more effort isneeded, in close collaboration with health information stakeholders, in order to ensure the appropriatetraining of coders regarding the use of injury-related codes, including those specific to sport andphysical activity.
C.4 RECOMMENDATIONS
The profiles of injuries associated with specific sport/leisure activities should be presented to therelevant state sporting associations and the implications of the findings discussed with them.
Consideration could be given to the enhancements to the ICD-10-AM coding procedures that wouldallow the phase of play/actual activity at the time of injury to be reported (such as during training or incompetitive games) and for the type of activity to be properly differentiated between organised sport,informal sport and general play.
Those interested in hospitalisation rates for injuries related to rugby need to be aware that rugbyleague and rugby union are often not differentiated in the hospitalisation data, despite specific ICD-10-AM activity codes being available for each type of rugby. It would be useful to identify the reasonswhy there are relatively large numbers of “rugby unspecified” coded cases in areas where both formsof football are popular, as this lack of specificity limits the information for preventive purposes.

58
REFERENCES
1. Boufous, S., Dennis, R. and Finch, C.(2006). A profile of hospitalisationepisodes and deaths due to sport andleisure injuries in New South Wales,2000–2004. Sydney, Australia: Universityof New South Wales.
2. Australian Bureau of Statistics. (2003).National Health Survey: Injuries, Australia2001. (Report number 4384.0).Canberra, Australia: Australian Bureau ofStatistics.
3. Centre for Epidemiology and Research.(2006). Health Outcomes and InformationStatistical Toolkit (HOIST). InpatientStatistics Collection. Sydney, Australia:NSW Department of Health.
4. National Centre for Classification inHealth. (2002). The InternationalStatistical Classification of Diseases andRelated Health Problems, 10th Revision,Australian Modification (ICD-10-AM). 3rdEdition. Sydney, Australia: National Centrefor Classification in Health.
5. SAS Institute. (2000). SAS: statistical soft-ware. Version 8.02. Cary, USA: SASInstitute.
6. Australian Bureau of Statistics. (2003).Information Paper: Census of Populationand Housing _ Socio-Economic Indexesfor Areas, Australia, 2001. (Report num-ber 2039.0). Canberra, Australia:Australian Bureau of Statistics.
7. Australian Bureau of Statistics. (2003).ASGC Remoteness Classification: Purposeand Use (Census paper number 03/01).Canberra, Australia: Australian Bureau ofStatistics.
8. MapInfo Corporation. (2006). MapInfoProfessional, Version 8.5. Retrieved 23February, 2007, from http://www.mapin-fo.com.au/
9. Draper, G., Turrell, G. and Oldenburg, B.(2004). Health inequalities in Australia:Mortality. Canberra, Australia: AustralianInstitute of Health and Welfare.
10.Jolly, D.L., Moller, J.N. and Volkmer, R.E.(1993). The socio-economic context ofchildhood injury in Australia. Journal ofPaediatrics & Child Health, 29, 438-44.
11.Al-Yaman, F., Bryant, M. and Sargeant, H.(2002). Australia's children: Their healthand wellbeing 2002. Canberra, Australia:Australian Institute of Health and Welfare.
12.Lam, L.T. (2005). Hospitalisation due tosports-related injuries among children andadolescents in New South Wales,Australia: an analysis on socioeconomicand geographic differences. Journal ofScience & Medicine in Sport, 8 (4), 433-40.
13.Finch, C., Mahoney, M., Townsend, M.and Zazryn, T. (2003). Rural sports andrecreational injuries in Australia: what dowe know? Australian Journal of RuralHealth, 11 (3), 151-8.
14.Finch, C. and McGrath, A. (1997).SportSafe Australia: A national sports safe-ty framework. A report prepared for theAustralian Sports Injury PreventionTaskforce. Canberra, Australia: AustralianSports Commission.
15.Australian Government Department ofHealth and Ageing. (2004). Sports safety inAustralia: An update. Canberra, Australia:Commonwealth of Australia.
16.Finch, C. (2004). Sports injury inAboriginal and Torres Strait Islander com-munities – a priority problem. SportsHealth, 22 (3), 17-8.
17.Langley, J.D., Davie, G.S. and Simpson,J.C. (2007). Quality of hospital dischargedata for injury prevention. InjuryPrevention, 13 (1), 42-4.
References

App
endi
x 1:
ICD
-10-
AM
Cod
esR
epro
duce
d w
ith
perm
issi
on f
rom
the
Nat
iona
l Cen
tre
for
Cla
ssif
icat
ion
in H
ealt
h.
59
APPENDIX 1: ICD-10-AM CODESREPRODUCED WITH PERMISSION FROM THE NATIONAL CENTRE FOR CLASSIFICATION IN HEALTH.

60
Appendix 1: IC
D-10-A
M C
odesR
eproduced with perm
ission from the N
ational Centre for C
lassification in Health.
APPENDIX 1: ICD-10-AM CODESREPRODUCED WITH PERMISSION FROM THE NATIONAL CENTRE FOR CLASSIFICATION IN HEALTH.

61
App
endi
x 1:
ICD
-10-
AM
Cod
esR
epro
duce
d w
ith
perm
issi
on f
rom
the
Nat
iona
l Cen
tre
for
Cla
ssif
icat
ion
in H
ealt
h.
APPENDIX 1: ICD-10-AM CODESREPRODUCED WITH PERMISSION FROM THE NATIONAL CENTRE FOR CLASSIFICATION IN HEALTH.

62
Appendix 1: IC
D-10-A
M C
odesR
eproduced with perm
ission from the N
ational Centre for C
lassification in Health.
APPENDIX 1: ICD-10-AM CODESREPRODUCED WITH PERMISSION FROM THE NATIONAL CENTRE FOR CLASSIFICATION IN HEALTH.

63
App
endi
x 1:
ICD
-10-
AM
Cod
esR
epro
duce
d w
ith
perm
issi
on f
rom
the
Nat
iona
l Cen
tre
for
Cla
ssif
icat
ion
in H
ealt
h.
APPENDIX 1: ICD-10-AM CODESREPRODUCED WITH PERMISSION FROM THE NATIONAL CENTRE FOR CLASSIFICATION IN HEALTH.

64
Appendix 1: IC
D-10-A
M C
odesR
eproduced with perm
ission from the N
ational Centre for C
lassification in Health.
APPENDIX 1: ICD-10-AM CODESREPRODUCED WITH PERMISSION FROM THE NATIONAL CENTRE FOR CLASSIFICATION IN HEALTH.

65
App
endi
x 1:
ICD
-10-
AM
Cod
esR
epro
duce
d w
ith
perm
issi
on f
rom
the
Nat
iona
l Cen
tre
for
Cla
ssif
icat
ion
in H
ealt
h.
APPENDIX 1: ICD-10-AM CODESREPRODUCED WITH PERMISSION FROM THE NATIONAL CENTRE FOR CLASSIFICATION IN HEALTH.

66
Appendix 2: Legends for the M
aps of Sport/Leisure Injury
Hospitalisation Episode R
ates and Counts, N
SW
, 2003-2004
Map label LGA Name N Rates* 95% CI 1 Albury 243 271.3 237.2 305.32 Armidale Dumaresq 107 217.2 176.1 258.33 Ashfield 98 121.6 97.5 145.74 Auburn 129 104.1 86.1 122.15 Ballina 179 227.1 193.9 260.46 Balranald # 72.8 1.5 144.07 Bankstown 425 121.4 109.9 133.08 Barraba 15 341.6 169.0 514.29 Bathurst 123 146.9 121.0 172.810 Baulkham Hills 591 189.2 174.0 204.411 Bega Valley 153 241.1 203.0 279.312 Bellingen 85 333.3 262.5 404.013 Berrigan 20 122.3 68.7 175.914 Bingara 11 270.2 110.7 429.715 Blacktown 1137 206.1 194.1 218.016 Bland 89 676.5 536.5 816.617 Blayney 43 322.4 226.2 418.618 Blue Mountains 324 209.7 186.9 232.519 Bogan 13 208.4 95.2 321.620 Bombala 13 254.1 116.1 392.021 Boorowa 5 101.5 12.6 190.522 Botany Bay 138 184.8 154.0 215.623 Bourke 17 216.2 113.6 318.924 Brewarrina 18 419.6 226.2 613.025 Broken Hill 34 82.7 54.9 110.526 Burwood 88 142.1 112.5 171.827 Byron 101 165.2 133.0 197.428 Cabonne 68 269.3 205.4 333.329 Camden 190 190.5 163.4 217.530 Campbelltown 405 134.8 121.6 147.931 Canada Bay 111 84.8 69.1 100.632 Canterbury 316 116.8 103.9 129.633 Carrathool 30 452.7 291.1 614.334 Central Darling 9 187.1 65.0 309.235 Cessnock 198 196.4 169.1 223.836 Clarence Valley 203 164.2 141.7 186.837 Cobar 37 366.5 248.6 484.438 Coffs Harbour 270 208.7 183.9 233.639 Coolah 21 269.8 154.6 385.040 Coolamon 31 377.4 244.8 509.941 Cooma-Monaro 25 132.7 80.7 184.742 Coonabarabran 36 268.0 180.6 355.4
APPENDIX 2: LEGENDS FOR THE MAPS OF SPORT/LEISURE INJURY HOSPITALISATION EPISODE RATES AND COUNTS, NSW, 2003-2004

67
App
endi
x 2:
Leg
ends
for
the
Map
s of
Spo
rt/L
eisu
re In
jury
H
ospi
talis
atio
n Ep
isod
e R
ates
and
Cou
nts,
NS
W,
2003
-200
4
43 Coonamble 21 221.4 126.8 316.044 Cootamundra 40 263.1 181.7 344.545 Corowa 24 139.6 83.8 195.346 Cowra 39 148.5 102.0 195.147 Culcairn 23 286.0 169.3 402.748 Deniliquin 20 121.3 68.1 174.449 Dubbo 133 170.5 141.5 199.450 Dungog 41 244.0 169.4 318.551 Eastern Capital City Regional 40 163.5 112.9 214.252 Eurobodalla 177 248.6 212.0 285.253 Evans 12 144.2 62.7 225.754 Fairfield 336 89.3 79.8 98.955 Forbes 42 209.2 146.0 272.556 Gilgandra 12 127.4 55.4 199.457 Glen Innes 37 310.1 210.3 409.958 Gloucester 20 203.8 114.6 293.059 Gosford 755 232.0 215.5 248.660 Greater Argyle 56 98.5 72.7 124.361 Greater Queanbeyan 69 62.2 47.5 76.862 Greater Taree 239 259.0 226.2 291.863 Great Lakes 119 175.6 144.1 207.164 Griffith 160 322.0 272.2 371.865 Gundagai 20 265.3 149.2 381.466 Gunnedah 55 223.0 164.1 281.867 Guyra 14 157.4 75.0 239.768 Harden 15 198.0 97.9 298.169 Hastings 335 242.4 216.5 268.370 Hawkesbury 315 247.4 220.2 274.771 Hay 22 308.6 179.8 437.472 Holbrook 16 324.0 165.5 482.473 Holroyd 268 147.5 129.8 165.174 Hornsby 670 214.1 197.9 230.375 Hume 38 235.0 160.4 309.776 Hunter's Hill 56 202.9 149.8 256.077 Hurstville 222 147.1 127.8 166.578 Inverell 49 155.5 112.0 199.079 Jerilderie # 105.9 2.2 209.780 Junee 30 254.7 163.7 345.781 Kempsey 99 176.9 142.1 211.782 Kiama 141 348.7 291.3 406.283 Kogarah 163 149.8 126.8 172.884 Ku-ring-gai 474 217.8 198.2 237.485 Kyogle 38 196.9 134.3 259.486 Lachlan 58 389.1 289.1 489.087 Lake Macquarie 740 195.6 181.5 209.788 Lane Cove 147 227.5 190.8 264.289 Leeton 63 262.0 197.4 326.690 Leichhardt 188 144.3 123.7 164.991 Lismore 199 230.7 198.6 262.792 Lithgow 62 58.7 44.1 73.393 Liverpool 393 117.8 106.2 129.594 Lockhart 12 169.7 73.8 265.6
APPENDIX 2: LEGENDS FOR THE MAPS OF SPORT/LEISURE INJURY HOSPITALISATION EPISODE RATES AND COUNTS, NSW, 2003-2004
Map label LGA Name N Rates* 95% CI

68
Appendix 2: Legends for the M
aps of Sport/Leisure Injury
Hospitalisation Episode R
ates and Counts, N
SW
, 2003-2004
95 Maitland 210 176.6 152.8 200.596 Manilla 15 229.7 113.6 345.997 Manly 206 264.6 228.5 300.798 Marrickville 215 141.6 122.7 160.599 Merriwa 17 365.7 192.2 539.3100 Moree Plains 82 254.8 199.7 309.9101 Mosman 110 194.4 158.1 230.7102 Mudgee 75 203.4 157.4 249.3103 Murray # 15.3 0.6 36.5104 Murrumbidgee 20 378.7 213.1 544.4105 Murrurundi 8 184.9 56.9 313.0106 Muswellbrook 51 167.3 121.4 213.2107 Nambucca 56 152.7 112.8 192.7108 Narrabri 77 269.0 209.0 329.0109 Narrandera 47 355.2 253.8 456.5110 Narromine 25 177.8 108.2 247.4111 Newcastle 501 172.8 157.6 187.9112 North Sydney 213 176.3 152.6 199.9113 Nundle # 152.2 3.2 301.3114 Oberon 27 264.9 165.1 364.7115 Orange 213 283.7 245.7 321.8116 Parkes 77 255.8 198.7 312.8117 Parramatta 367 122.3 109.8 134.8118 Parry 52 202.7 147.6 257.7119 Penrith 762 214.2 199.0 229.4120 Pittwater 270 237.3 209.0 265.6121 Port Stephens 246 198.7 173.9 223.5122 Quirindi 27 273.3 170.4 376.3123 Randwick 467 185.0 168.2 201.8124 Richmond Valley 78 93.8 73.0 114.7125 Rockdale 218 115.2 99.9 130.5126 Ryde 292 146.6 129.8 163.4127 Rylstone 12 156.8 68.2 245.5128 Scone 60 304.6 227.6 381.5129 Severn 20 350.6 197.2 504.0130 Shellharbour 384 309.9 279.0 340.9131 Shoalhaven 391 214.3 193.1 235.5132 Singleton 97 222.3 178.1 266.4133 Snowy River 23 157.0 92.9 221.1134 Sydney 402 146.4 96.0 151.7135 Strathfield 76 123.9 223.0 252.1136 Sutherland Shire 1021 237.5 132.1 160.7137 Tamworth 164 220.5 186.7 254.2138 Temora 33 261.9 172.6 351.1139 Tenterfield 24 176.6 106.0 247.2140 Tumbarumba 24 329.5 197.9 461.1141 Tumut 49 213.6 153.9 273.4142 Tweed 255 161.2 141.5 181.0143 Upper Lachlan 15 107.7 53.2 162.2144 Uralla 28 232.1 146.2 317.9145 Urana 8 284.8 87.7 481.9146 Wagga Wagga 230 200.3 174.5 226.2
APPENDIX 2: LEGENDS FOR THE MAPS OF SPORT/LEISURE INJURY HOSPITALISATION EPISODE RATES AND COUNTS, NSW, 2003-2004
Map label LGA Name N Rates* 95% CI

69
App
endi
x 2:
Leg
ends
for
the
Map
s of
Spo
rt/L
eisu
re In
jury
H
ospi
talis
atio
n Ep
isod
e R
ates
and
Cou
nts,
NS
W,
2003
-200
4
147 Wakool 8 82.5 25.4 139.7148 Walcha 14 213.8 101.9 325.7149 Walgett 132 809.7 672.1 947.2150 Warren 16 243.0 124.1 361.9151 Warringah 615 222.6 205.0 240.2152 Waverley 259 209.4 183.9 234.8153 Weddin 25 327.3 199.2 455.4154 Wellington 34 195.6 129.9 261.3155 Willoughby 227 178.6 155.4 201.8156 Wingecarribee 120 427.5 351.2 503.9157 Wollondilly 167 207.4 176.0 238.9158 Wollongong 960 250.5 234.7 266.4159 Woollahra 174 162.5 138.3 186.6160 Wyong 635 225.1 207.6 242.6161 Yallaroi 35 553.6 370.7 736.5162 Yass Valley 5 23.4 2.9 43.9163 Young 31 129.9 84.2 175.6164 Unincorporated NSW # 180.1 2.4 383.7*rates per 100,000 population # less than 5 cases
APPENDIX 2: LEGENDS FOR THE MAPS OF SPORT/LEISURE INJURY HOSPITALISATION EPISODE RATES AND COUNTS, NSW, 2003-2004
Map label LGA Name N Rates* 95% CI

SPORTS AND LEISURE INJURY REPORT llAUGUST 2006IRMRC
NSW INJURY RISK MANAGEMENT RESEARCH CENTREUNSW, SYDNEY NSW 2052, AUSTRALIATelephone: +61 (2) 9385 4207 Facsimile: +61 (2) 9385 6040 http://www.irmrc.unsw.edu.auABN 57 195 873 179

NS
W IN
JUR
Y RIS
K MA
NA
GEM
ENT
RES
EAR
CH CEN
TRE
SPO
RTS
INJU
RY R
EPOR
T llA
UG
US
T 2006IR
MR
C