NR-602: Primary Care of the Childbearing and Childrearing Family ...
23
Retrieved on 2/2/16 hf Syllabus Course Code: NR602 Course Title: Primary Care of the Childbearing and Childrearing Family Syllabus Top Information Course Number: NR602 Course Title: Primary Care of the Childbearing and Childrearing Family Course Credit: 3 (Theory 0.5; Clinical 2.5) Pre-requisite: NR503, NR507, NR508, NR509, NR510, NR511 Course Text Textbook 1 Hawkins, J. W., Roberto-Nichols, D. M., & Stanley-Haney, J. L. (2011). Guidelines for nurse practitioners in gynecologic settings (10th ed.). New York, NY: Springer Publishing Company. Textbook 2 Richardson, B. E. (2011). Pediatric primary care: Practice guidelines for nurses (2nd ed.). Sudbury, MA: Jones & Bartlett. (Ebook) Required across all FNP courses Textbook 3 American Psychological Association [APA]. (2010). Publication manual of the American Psychological Association (6th ed.). Washington, DC: Author Recommended across all FNP courses Textbook 4 NR602 Syllabus
Transcript of NR-602: Primary Care of the Childbearing and Childrearing Family ...
Retrieved on 2/2/16 hf
Syllabus
Course Code: NR602
Course Title: Primary Care of the Childbearing and Childrearing Family
Syllabus
Top Information
Course Number: NR602
Course Title: Primary Care of the Childbearing and Childrearing Family
Course Credit: 3 (Theory 0.5; Clinical 2.5)
Pre-requisite: NR503, NR507, NR508, NR509, NR510, NR511
Course Text
Textbook 1
Hawkins, J. W., Roberto-Nichols, D. M., & Stanley-Haney, J. L. (2011). Guidelines for nurse practitioners in gynecologic settings (10th ed.). New York, NY: Springer Publishing Company.
Textbook 2
Richardson, B. E. (2011). Pediatric primary care: Practice guidelines for nurses (2nd ed.). Sudbury, MA: Jones & Bartlett. (Ebook)
Required across all FNP courses
Textbook 3
American Psychological Association [APA]. (2010). Publication manual of the American Psychological Association (6th ed.). Washington, DC: Author
Recommended across all FNP courses
Textbook 4
NR602 Syllabus
Retrieved on 2/2/16 hf
Goroll, A. H. & Mulley, A. G. (2014). Primary care medicine: Office evaluation and management of the adult patient (7th ed.). Philadelphia, PA: Lippincott Williams & Wilkins. (Ebook)
Course Description
This course continues to expand the knowledge of health assessment principles specific to the role of the FNP, with a focus on the healthcare needs of women and families throughout reproductive and childrearing years. Students will further develop their skills related to health promotion, prevention of illness, diagnosis, and management of health problems commonly experienced. Care strategies will include patient education, protocol development, follow-up, and referral through a clinical practicum experience in a precepted primary care setting.
COs
1. Demonstrate effective leadership skills that support relationship-based caring with a family-centered focus to promote quality advanced practice nursing. (PO 2)
2. Identify current ethical and legal issues concerning the care of infants, children, adolescents, women, and child-bearing families. (PO 6)
3. Apply current evidence in health promotion, health protection, disease prevention, and primary care for infants, children, adolescents, women, and child-bearing families. (PO 1)
4. Apply developmental, cultural, and family theory to health promotion, health protection, disease prevention, and primary care for infants, children, adolescents, women, and child-bearing families. (PO 1)
5. Promote safe and quality patient outcomes in a teaching-coaching function through integration of developmentally appropriate anticipatory guidance in care of infants, children, adolescents, women, and child-bearing families. (PO 2)
6. Identify professional organizations active in the promotion of health for women and children. (PO 10)
7. Utilize principles of nursing informatics and technologies to plan, document, and professionally communicate in the care of infants, children, adolescents, women, and child-bearing families. (PO 11)
8. Incorporate patients’ cultural preferences, values, health beliefs, spirituality, and behaviors into a unique and relationship-based, holistic plan of care for infants, children, adolescents, women, and child-bearing families. (PO 1)
9. Create an appropriate and holistic plan of care for common primary care presentations in infants, children, adolescents, women, and child-bearing families. (PO 1)
10. Engage in routine appropriate inter-professional collaboration in caring for infants, children, adolescents, women, and child-bearing families. (PO 10)
11. Reflect on personal and professional growth toward achieving competence as a family nurse practitioner. (PO 5, 10)
Program Outcomes
The MSN program outcomes are aligned with the American Association of Colleges of Nursing
publication, The Essentials of Master’s Education in Nursing (2011). Upon completion of the MSN
degree program, the graduate will be able to:
Retrieved on 2/2/16 hf
1. Practice safe, high-quality advanced nursing care based on concepts and knowledge from
nursing and related disciplines.
2. Construct processes for leading and promoting quality improvement and safety in advanced
nursing practice and healthcare delivery.
3. Use contemporary communication modalities effectively in advanced nursing roles.
4. Evaluate the design, implementation and outcomes of strategies developed to meet
healthcare needs.
5. Develop a plan for lifelong personal and professional growth that integrates professional
values regarding scholarship, service and global engagement.
6. Apply legal, ethical and human-caring principles to situations in advanced nursing practice.
7. Design patient-centered care models and delivery systems using the best available scientific
evidence.
8. Manage human, fiscal and physical resources to achieve and support individual and
organizational goals.
9. Compose a plan for systematic inquiry and dissemination of findings to support advanced
nursing practice, patient-care innovation, and the nursing profession.
10. Collaborate interprofessionally in research, education, practice, health policy and leadership
to improve population health outcomes.
11. Apply principles of informatics to manage data and information in order to support effective
decision making.
Course Schedule
Week 1
Title: Caring for the family within the nurse practitioner paradigm: Applicable concept/ theories
COs: 1, 3, 4, 6, 9, 10
Reading: Allen, J., Ryan, M., Framer, E. (2013). Family wellness: The power is in being healthy together. American Journal of Health Promotion, 27(3), TAPH2-6.
Bermudez, J., Stinson, M., Kak-Hunter, L., & Abrams, B. (2011). Mejor sola que mal acompanada: Strengths and challenges of Mexican-origin mothers parenting alone.
Retrieved on 2/2/16 hf
Journal of Divorce and Remarriage, 52, (8), 622- 641. doi:10.1080/10502556.2011.619939
Higginbottom, G., Richter, M., Mogale, R., Ortiz, L., Young, S., & Mollel, O. (2011). Identification of nursing assessment models/tools validated in clinical practice for use with diverse ethno-cultural groups: An integrative review of the literature. BMC Nursing, 10(1), 16-26. doi:10.1186/1472-6955-10-16
Assignments: Clinical Encounter Log in eLogs (required, but not graded)
Case Study
Discussions
Yes
Other
Week 2
Title: Family assessment by the nurse practitioner: Assessment of the infant, child, and adolescent.
COs: 2, 3, 4, 5, 6, 8, 9, 10
Reading: Richardson, B. E. (2011). Pediatric primary care: Practice guidelines for nurses (2nd ed.). Sudbury, MA: Jones & Bartlett.
Chapter 1: Obtaining an Initial History
Chapter 2: Obtaining an Interval History
Chapter 3: Performing a Physical Examination
Chapter 6: Two-Week Visit
Chapter 7: One-Month Visit
Chapter 8: Two-Month Visit
Chapter 9: Four-Month Visit
Chapter 10: Six-Month Visit
Chapter 11: Nine-Month Visit
Chapter 12: Twelve-Month Visit
Chapter 13: Fifteen- to Eighteen-Month Visit
Chapter 14: Two-Year Visit
Chapter 15: Three-Year Visit (Preschool)
Chapter 16: Six-Year Visit

Retrieved on 2/2/16 hf
(School Readiness)
Chapter 17: Seven- to Ten-Year Visit (School Age)
Chapter 18: Eleven- to Thirteen-Year Visit (Preadolescent)
Chapter 19: Fourteen- to Eighteen-Year Visit (Adolescent)
Adachi, Y., Sato, C., Nishino, N., Ohryoji, F., Hayama, J., & Yamagami, T. (2009). A brief parental education for shaping sleep habits in 4-month-old infants. Clinical Medicine & Research, 7(3), 85–92. doi:10.3121/cmr.2009.814
American Academy of Pediatrics (AAP) (2011). Media use by children younger than 2 years. Pediatrics, 128(5). 1040–1045. doi:10.1542/peds.2011–1753
LeBlanc, A. G., Chaput, J., McFarlane, A., Colley, R. C., Thivel, D., Biddle, S. H., & ... Tremblay, M. S. (2013). Active Video Games and Health Indicators in Children and Youth: A Systematic Review. Plos ONE, 8(6), 1–20. doi:10.1371/journal.pone.0065351
O’Connor, N. (2009). Infant formula. American Family Physician 79(1), 565–570.
Assignments: Clinical Encounter Log in eLogs (required, but not graded)
Website Exploration:
Please go in and look at each of these websites and become familiar with them. You will use them this week and throughout the remainder of the course. Please open and download the CDC growth charts as you will need them to work this week and in future weeks.
Bright Futures:
Retrieved on 2/2/16 hf
http://brightfutures.aap.org/ American Academy of Pediatrics (AAP): http://aap.org CDC Growth Charts: http://www.cdc.gov/growthcharts/ Safety in Children: http://www.saf
Case Study
Discussions
Yes
Other
Week 3
Title: Health promotion, health protection, disease prevention, and treatment considerations in primary care pediatric assessment
COs: 1, 2, 3, 7, 9, 10
Reading: Richardson, B. E. (2011). Pediatric primary care: Practice guidelines for nurses (2nd ed.). Sudbury, MA: Jones & Bartlett.
Chapter 6 Two-Week Visit
Chapter 7 One-Month Visit
Chapter 8 Two-Month Visit
Chapter 9 Four-Month Visit
Chapter 10 Six-Month Visit
Chapter 11 Nine-Month Visit
Chapter 12 Twelve-Month Visit
Chapter 13 Fifteen- to Eighteen-
Month Visit
Chapter 14 Two-Year Visit
Chapter 15 Three-Year Visit
(Preschool)
Chapter 16 Six-Year Visit
(School Readiness)
Chapter 17 Seven- to Ten-Year
Visit (School Age)
Chapter 18 Eleven- to Thirteen-
Year Visit (Preadolescent)
Chapter 19 Fourteen- to
Eighteen-Year Visit (Adolescent)
Chapter 34-Behavioral Disorders
Chapter 35-Mental Health
Disorders
Retrieved on 2/2/16 hf
AAP Clinical Report. (2011). Supporting the health care transition from adolescence to adulthood in the medical home. Pediatrics, 128(1), 182–200. doi:10.1542/peds. 2011–0969
Beesdo, K., Knappe, S., Pine, S. (2009). Anxiety and anxiety disorders in children and adolescents: Developmental issues and implications for DSM-V. Psychiatric Clinics of North America, 32(3); 483–524. Retrieved from www.ncbi.nlm.nih.gov/pmc/articles/PMC3018839/
Glascoe, F., Schonwald, A., Trimm, F., & Marks, K. (2009). Making developmental-behavior screening work in your practice... part 2 of 3. Contemporary Pediatrics, 26(12), 38. Golnick, A., & MaCCabee-Ryavboy, N. (2010). Autism: Clinical pearls for primary care. Contemporary Pediatrics, 27(11), 42-60. Theoktisto, K. (2009). Pharmacokinetic considerations in the treatment of pediatric behavioral issues. Pediatric Nursing, 35(6), 369-374.
Assignments: Clinical Encounter Log in eLogs (required, but not graded)
Website Exploration:
Please read the ACOG opinion on adolescent contraception found below:
Adolescents and Long-Acting Reversible Contraception: Implants and Intrauterine Devices
IUDs and Contraceptive Implants Safe for Teens
Please go in and look at each of these websites and become familiar with them. You will use them this week and throughout the
Retrieved on 2/2/16 hf
remainder of the course.
CDC Adolescent Health:
CDC Pediatric Developmental Screening
Contraception
National Eating Disorder Association
NAMI
Immunizations
Office of Adolescent Health
Adolescent health goals of Healthy People 2020
Case Study
Discussions
Yes
Other
Week 4
Title: Health promotion, health protection, disease prevention, and treatment of selected pediatric diagnoses in primary care of children
COs: 1, 3, 7, 9, 10
Reading: Richardson, B. E. (2011). Pediatric primary care: Practice guidelines for nurses (2nd ed.). Sudbury, MA: Jones & Bartlett.
Chapter 20: Dermatologic
Problems
Chapter 21: Eye Disorders
Chapter 22: Ear Disorders
Chapter 23: Sinus, Mouth,
Throat, and Neck
Chapter 26: Gastrointestinal
Disorders
Chapter 27: Genitourinary
Disorders
Lightdale, J., Gresme, D. (2013). Gastroesophageal reflux: Management guidance for the
Retrieved on 2/2/16 hf
pediatrician. Pediatrics. doi: 10.1542/peds.2013-0421
Society of Pediatric Nurses. (2008). Position statement on fever in children. Retrieved from http://www.pedsnurses.org/pdfs/downloads/gid,126/index.pdf
Assignments: Clinical Encounter Log in eLogs (required, but not graded)
Quiz (required but not graded) Case Study
Discussions
Yes
Other
Week 5
Title: Health promotion, health protection, disease prevention, and treatment of unique childhood chronic, allergic, inherited, and autoimmune diseases.
COs: 1, 3, 7, 9, 10
Reading: Richardson, B. E. (2011). Pediatric primary care: Practice guidelines for nurses (2nd ed.). Sudbury, MA: Jones & Bartlett.
Chapter 24- Respiratory Disorders
Chapter 25- Cardiovascular
Disorders
Chapter 29- Endocrine Disorders
Chapter 30- Musculoskeletal
Disorders
Chapter 33- Pediatric Obesity
Everard, M. (2009). Acute bronchiolitis and croup. Pediatric Clinics of North America, 56(1), 119-133. doi:10.1016/j.pcl.2008.10.007
Fitzner, K., Greenwood, D., Payne, H., Thomson, J., Vukovljak, L., McCulloch, A., & Specker, J. (2008). An assessment of patient education and self-management in diabetes disease management--two case studies. Population Health Management, 11(6), 329-340. Hopkins, K., DeCristofaro, C., & Elliot, L.
Retrieved on 2/2/16 hf
(2011). How can primary care providers manage pediatric obesity in the real world? Journal of the American Academy of Nurse Practitioners, 23(6), 278-288. doi:10.1111/j.1745-7599.2011.00614.x Wierwille, L. (2011). Pediatric heart murmurs: Evaluation and management in primary care. Nurse Practitioner, 36(3), 22-30. doi:10.1097/01.NPR.0000393968.36683.f0
Assignments: Clinical Encounter Log in eLogs (required, but not graded)
Case Study
Discussions
Yes
Other
Week 6
Title: Health promotion, health protection, disease prevention, and treatment of selected women’s health, gynecologic, and obstetric diagnoses in primary care
COs: 1, 2, 3, 4, 5, 6, 7, 8, 9, 10
Reading: Hawkins, J. W., Roberto-Nichols, D. M., & Stanley-Haney, J. L. (2011). Guidelines for nurse practitioners in gynecologic settings (10th ed.). New York, NY: Springer Publishing Company
Chapter 1: Well Woman Exam
Chapter 5: Weight Management
Chapter 6: Guidelines for Assessing Victims of Abuse and Violence
Chapter 7: Methods of Family Planning
Chapter 10: Cervical Aberrations
Chapter 12: Genitourinary Conditions
Chapter 13: Infertility
Chapter 21: Vaginal Conditions
Booth, C. N., Bashleben, C., Filomena, C. A., Means, M. M., Wasserman, P. G., Souers, R. J., & Henry, M. R. (2013). Monitoring and Ordering Practices for Human Papillomavirus in Cervical
Retrieved on 2/2/16 hf
Cytology: Findings From the College of American Pathologists Gynecologic Cytopathology Quality Consensus Conference Working Group 5. Archives Of Pathology & Laboratory Medicine, 137(2), 214–219. doi:10.5858/arpa.2012-0114-CP
Bradbury-Jones, C., Duncan, F., Kroll, T., Moy, M., & Taylor, J. (2011). Improving the health care of women living with domestic abuse. Nursing Standard, 25(43), 35–40.
Eberl, M., Phillips, R. R., Lamberts, H., Okkes, I., & Mahoney, M. (2008). Characterizing breast symptoms in family practice. Annals of Family Medicine, 6(6), 528–533.
Edwards, M. (2008). Promoting breast awareness. Practice Nurse, 36(6), 35.
Hainer, B., & Gibson, M. (2011). Vaginitis: Diagnosis and treatment. American Family Physician, 83(7), 807-815.
Mishori, R., McClaskey, E., & Winklerprins, V. (2012). Chlamydia trachomatis infections: screening, diagnosis, and management. American Family Physician, 86(12), 1127–1132.
Stevens, P., & Keigher, S. (2009). Systemic barriers to healthcare access for U.S. women with HIV: The role of cost and insurance. International Journal of Health Services, 39(2), 225–243.
Tello, M., Yeh, H., Keller, J., Beach, M., Anderson, J., & Moore, R. (2008). HIV women's health: A study of gynecological healthcare service utilization in a U.S. urban clinic population. Journal of Women's Health, 17(10), 1609–1614. doi:10.1089/jwh.2008.0881
Assignments: Clinical Encounter Log in eLogs (required, but not graded)
Website Exploration:
Please go in and look at each of these
Retrieved on 2/2/16 hf
websites and become familiar with them. You will use them this week and throughout the remainder of the course.
CDC Center for STD Prevention
Women’s Health Resources
U.S. Medical Eligibility Criteria for Contraceptive Use
CDC STD Treatment Guidelines
Breast Cancer Screening Statements & Guidelines:
Link 1
Link 2
Link 3
Link 4
Screening for Cervical Cancer Statements & Guidelines:
Link 1
Link 2
Link 3
Ovarian Cancer Screening Guidelines:
Case Study
Discussions
Yes
Other
Week 7
Title: Health promotion, health protection, disease prevention, and treatment
of unique issues of the pregnant female and her family
COs: 2, 3, 4, 5, 8, 9, 10
Reading: Hawkins, J. W., Roberto-Nichols, D. M., & Stanley-Haney, J. L. (2011). Guidelines for nurse practitioners in
Retrieved on 2/2/16 hf
gynecologic settings (10th ed.). New York, NY: Springer Publishing Company.
Chapter 8: Preconception Care
Chapter 11: Emotional/Mental
Health Issues
Chapter 14: Loss of Integrity of
Pelvic Floor Structures
Chapter 15: Medical Abortion
Joseph, J., El-Mohandes, A., Kiely, M., El-Khorazaty, M., Gantz, M., Johnson, A., & ... Subramanian, S. (2009). Reducing psychosocial and behavioral pregnancy risk factors: Results of a randomized clinical trial among high-risk pregnant African American women. American Journal of Public Health, 99(6), 1053–1061.doi:10.2105/AJPH.2007.131425
Muzik, M., & Borovska, S. (2010). Perinatal depression: Implications for child mental health. Mental Health in Family Medicine, 7(4), 239–247.
Nichols, J., Curtis, E., & Rayman, M. (2008). Survey of total folate intake at conception and assessment of impact of fortification. Journal of Nutritional & Environmental Medicine, 17(1), 44–55.
O’Connor, N. (2009). Infant formula. American Family Physician 79(7), 565–570.
Oladapo, O., & Osiberu, M. (2009). Do sociodemographic characteristics of pregnant women determine their perception of antenatal care quality? Maternal & Child Health Journal, 13(4), 505–511. doi:10.1007/s10995-008-0389-2
Assignments: Clinical Encounter Log in eLogs (required, but not graded)

Retrieved on 2/2/16 hf
Website Exploration:
Find solid prenatal and gestational diabetes screening and guideline resources from reputable sources. You will use them this week and throughout the remainder of the course.
Case Study
Discussions
Yes
Other
Week 8
Title: Health promotion, health protection, disease prevention, and treatment of selected emergent conditions impacting the childbearing family
COs: 1, 7, 8, 9, 10, 11
Reading: Hawkins, J. W., Roberto-Nichols, D. M., & Stanley-Haney, J. L. (2011). Guidelines for nurse practitioners in gynecologic settings (10th ed.). New York, NY: Springer Publishing Company.
Chapter 18: Peri and Post
Menopause
Grant, K., & Ragsdale, K. (2008). Sex and the 'recently single': Perceptions of sexuality and HIV risk among mature women and primary care physicians. Culture, Health & Sexuality, 10(5), 495–511.
Sambamoorthi, U., Bean-Mayberry, B., Findley, P., Yano, E., & Banerjea, R. (2010). Organization of care and diagnosed depression among women veterans. American Journal of Managed Care, 16(9), 657–665.
Schroetter, S., & Peck, S. (2008). Women's risk of heart disease: Promoting awareness and prevention—a primary care approach.
Retrieved on 2/2/16 hf
MEDSURG Nursing, 17(2), 107–113.
Simmons, L., Anderson, E., & Braun, B. (2008). Health needs and healthcare utilization among rural, low-income women. Women & Health, 47(4), 53–69.
Stockdale, C., Boardman, L. (2011). Evaluation and treatment of postmenopausal dyspareunia. Journal of Clinical Outcomes Management, 18(9), 414–423
Assignments: Clinical Encounter Log in eLogs &
Clinical Performance Evaluation
(graded)
Final Exam
Case Study
Discussions
Yes
Other
Late Assignment Policy
Students are expected to submit assignments by the time they are due. Assignments submitted after the due date and time will receive a deduction of 10% of the total points possible for that assignment for each day the assignment is late. Assignments will be accepted, with penalty as described, up to a maximum of three days late, after which point a zero will be recorded for the assignment.
In the event of an emergency that prevents timely submission of an assignment, students may petition their instructor for a waiver of the late submission grade reduction. The instructor will review the student’s rationale for the request and make a determination based on the merits of the student’s appeal. Consideration of the student’s total course performance to date will be a contributing factor in the determination. Students should continue to attend class, actively participate, and complete other assignments while the appeal is pending.
This Policy applies to assignments that contribute to the numerical calculation of the course letter grade.
Evaluation Methods
The maximum score in this class is 1,000 points. The categories, which contribute to your final grade, are weighted as follows.
Assignment Points Weighting
Retrieved on 2/2/16 hf
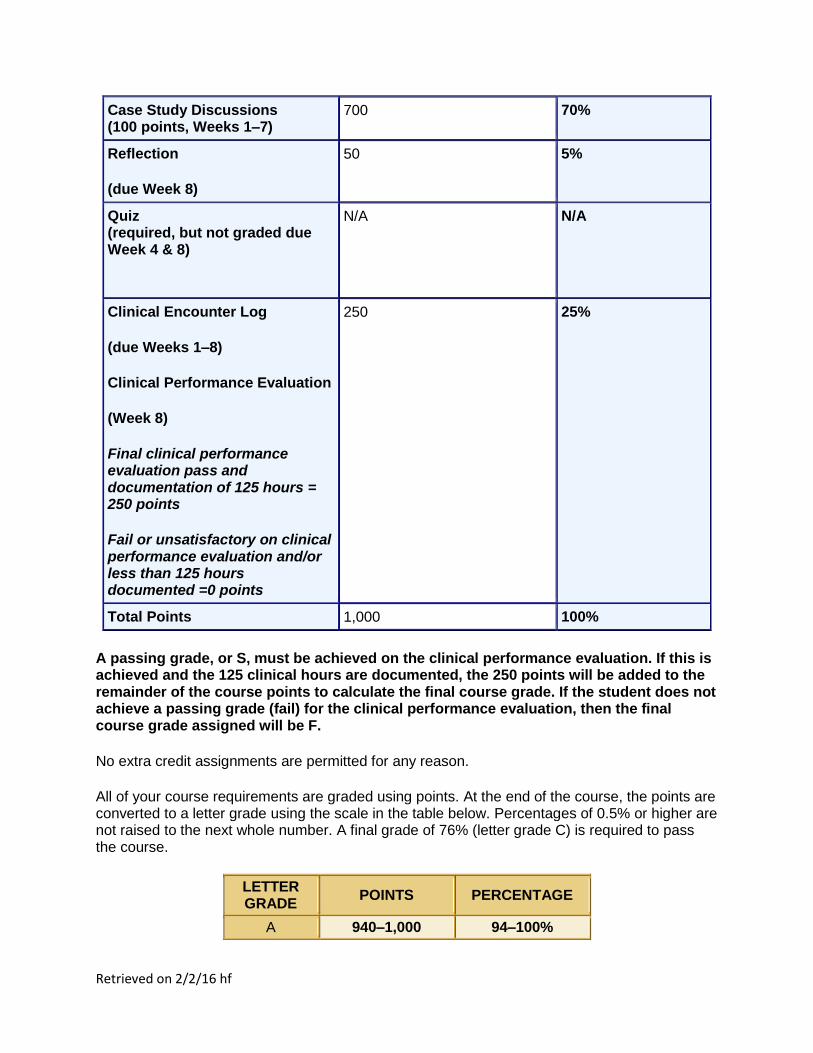
Case Study Discussions (100 points, Weeks 1–7)
700 70%
Reflection
(due Week 8)
50 5%
Quiz (required, but not graded due Week 4 & 8)
N/A N/A
Clinical Encounter Log
(due Weeks 1–8)
Clinical Performance Evaluation
(Week 8)
Final clinical performance evaluation pass and documentation of 125 hours = 250 points
Fail or unsatisfactory on clinical performance evaluation and/or less than 125 hours documented =0 points
250 25%
Total Points 1,000 100%
A passing grade, or S, must be achieved on the clinical performance evaluation. If this is achieved and the 125 clinical hours are documented, the 250 points will be added to the remainder of the course points to calculate the final course grade. If the student does not achieve a passing grade (fail) for the clinical performance evaluation, then the final course grade assigned will be F.
No extra credit assignments are permitted for any reason.
All of your course requirements are graded using points. At the end of the course, the points are converted to a letter grade using the scale in the table below. Percentages of 0.5% or higher are not raised to the next whole number. A final grade of 76% (letter grade C) is required to pass the course.
LETTER GRADE
POINTS PERCENTAGE
A 940–1,000 94–100%
Retrieved on 2/2/16 hf
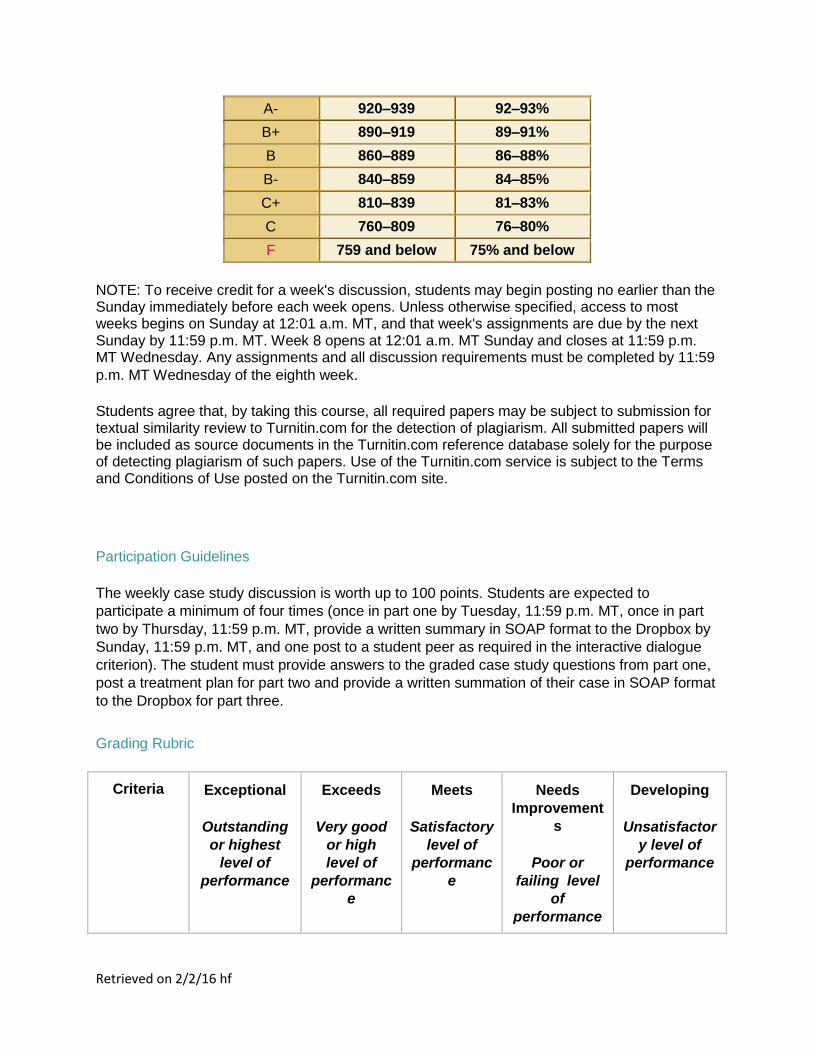
A- 920–939 92–93%
B+ 890–919 89–91%
B 860–889 86–88%
B- 840–859 84–85%
C+ 810–839 81–83%
C 760–809 76–80%
F 759 and below 75% and below
NOTE: To receive credit for a week's discussion, students may begin posting no earlier than the Sunday immediately before each week opens. Unless otherwise specified, access to most weeks begins on Sunday at 12:01 a.m. MT, and that week's assignments are due by the next Sunday by 11:59 p.m. MT. Week 8 opens at 12:01 a.m. MT Sunday and closes at 11:59 p.m. MT Wednesday. Any assignments and all discussion requirements must be completed by 11:59
p.m. MT Wednesday of the eighth week.
Students agree that, by taking this course, all required papers may be subject to submission for textual similarity review to Turnitin.com for the detection of plagiarism. All submitted papers will be included as source documents in the Turnitin.com reference database solely for the purpose of detecting plagiarism of such papers. Use of the Turnitin.com service is subject to the Terms and Conditions of Use posted on the Turnitin.com site.
Participation Guidelines
The weekly case study discussion is worth up to 100 points. Students are expected to
participate a minimum of four times (once in part one by Tuesday, 11:59 p.m. MT, once in part
two by Thursday, 11:59 p.m. MT, provide a written summary in SOAP format to the Dropbox by
Sunday, 11:59 p.m. MT, and one post to a student peer as required in the interactive dialogue
criterion). The student must provide answers to the graded case study questions from part one,
post a treatment plan for part two and provide a written summation of their case in SOAP format
to the Dropbox for part three.
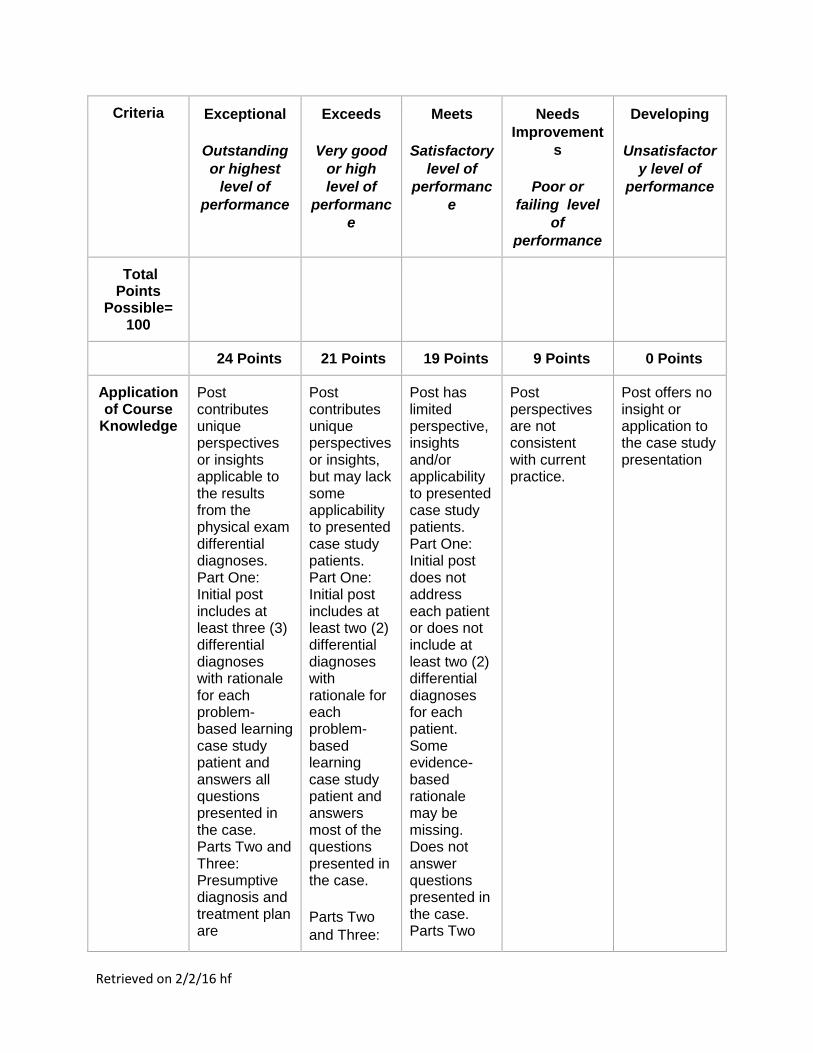
Grading Rubric
Criteria Exceptional
Outstanding
or highest
level of
performance
Exceeds
Very good
or high
level of
performanc
e
Meets
Satisfactory
level of
performanc
e
Needs
Improvement
s
Poor or
failing level
of
performance
Developing
Unsatisfactor
y level of
performance
Retrieved on 2/2/16 hf
Criteria Exceptional
Outstanding
or highest
level of
performance
Exceeds
Very good
or high
level of
performanc
e
Meets
Satisfactory
level of
performanc
e
Needs
Improvement
s
Poor or
failing level
of
performance
Developing
Unsatisfactor
y level of
performance
Total Points
Possible= 100
24 Points 21 Points 19 Points 9 Points 0 Points
Application of Course
Knowledge
Post contributes unique perspectives or insights applicable to the results from the physical exam differential diagnoses. Part One: Initial post includes at least three (3) differential diagnoses with rationale for each problem-based learning case study patient and answers all questions presented in the case. Parts Two and Three: Presumptive diagnosis and treatment plan are
Post contributes unique perspectives or insights, but may lack some applicability to presented case study patients. Part One: Initial post includes at least two (2) differential diagnoses with rationale for each problem-based learning case study patient and answers most of the questions presented in the case.
Parts Two
and Three:
Post has limited perspective, insights and/or applicability to presented case study patients. Part One: Initial post does not address each patient or does not include at least two (2) differential diagnoses for each patient. Some evidence-based rationale may be missing. Does not answer questions presented in the case. Parts Two
Post perspectives are not consistent with current practice.
Post offers no insight or application to the case study presentation
Retrieved on 2/2/16 hf
Criteria Exceptional
Outstanding
or highest
level of
performance
Exceeds
Very good
or high
level of
performanc
e
Meets
Satisfactory
level of
performanc
e
Needs
Improvement
s
Poor or
failing level
of
performance
Developing
Unsatisfactor
y level of
performance
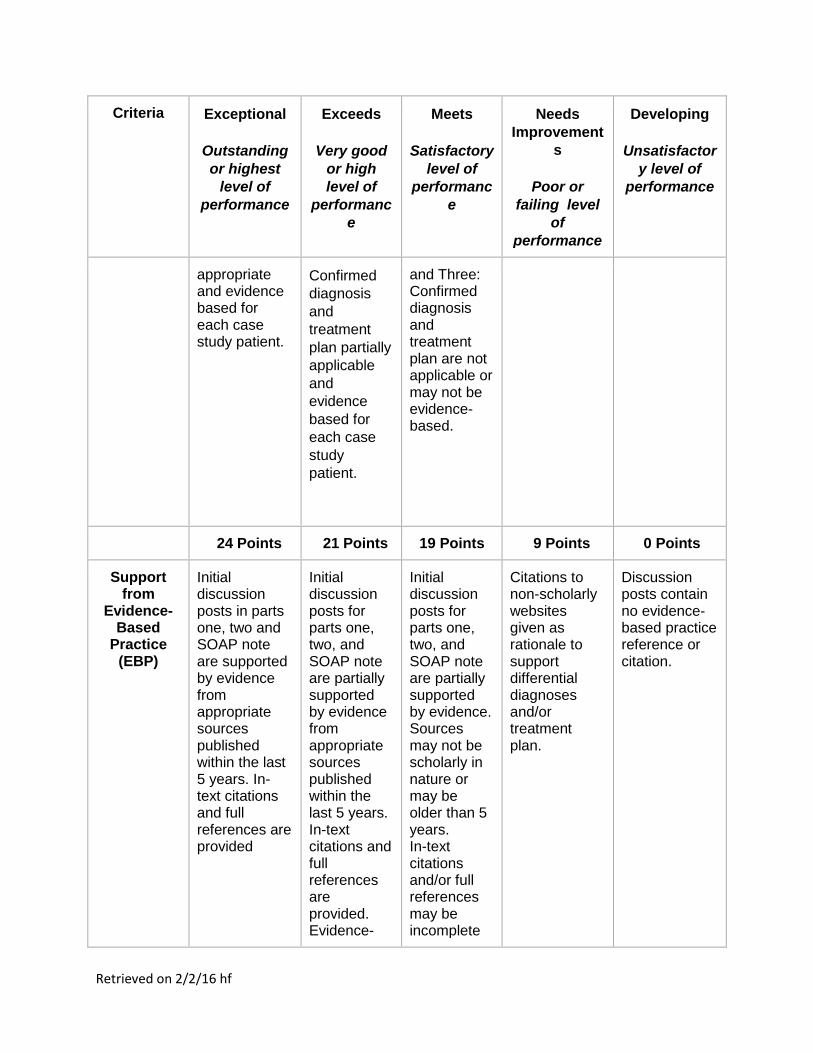
appropriate and evidence based for each case study patient.
Confirmed
diagnosis
and
treatment
plan partially
applicable
and
evidence
based for
each case
study
patient.
and Three: Confirmed diagnosis and treatment plan are not applicable or may not be evidence-based.
24 Points 21 Points 19 Points 9 Points 0 Points
Support from
Evidence-Based
Practice (EBP)
Initial discussion posts in parts one, two and SOAP note are supported by evidence from appropriate sources published within the last 5 years. In-text citations and full references are provided
Initial discussion posts for parts one, two, and SOAP note are partially supported by evidence from appropriate sources published within the last 5 years. In-text citations and full references are provided. Evidence-
Initial discussion posts for parts one, two, and SOAP note are partially supported by evidence. Sources may not be scholarly in nature or may be older than 5 years. In-text citations and/or full references may be incomplete
Citations to non-scholarly websites given as rationale to support differential diagnoses and/or treatment plan.
Discussion posts contain no evidence-based practice reference or citation.
Retrieved on 2/2/16 hf
Criteria Exceptional
Outstanding
or highest
level of
performance
Exceeds
Very good
or high
level of
performanc
e
Meets
Satisfactory
level of
performanc
e
Needs
Improvement
s
Poor or
failing level
of
performance
Developing
Unsatisfactor
y level of
performance
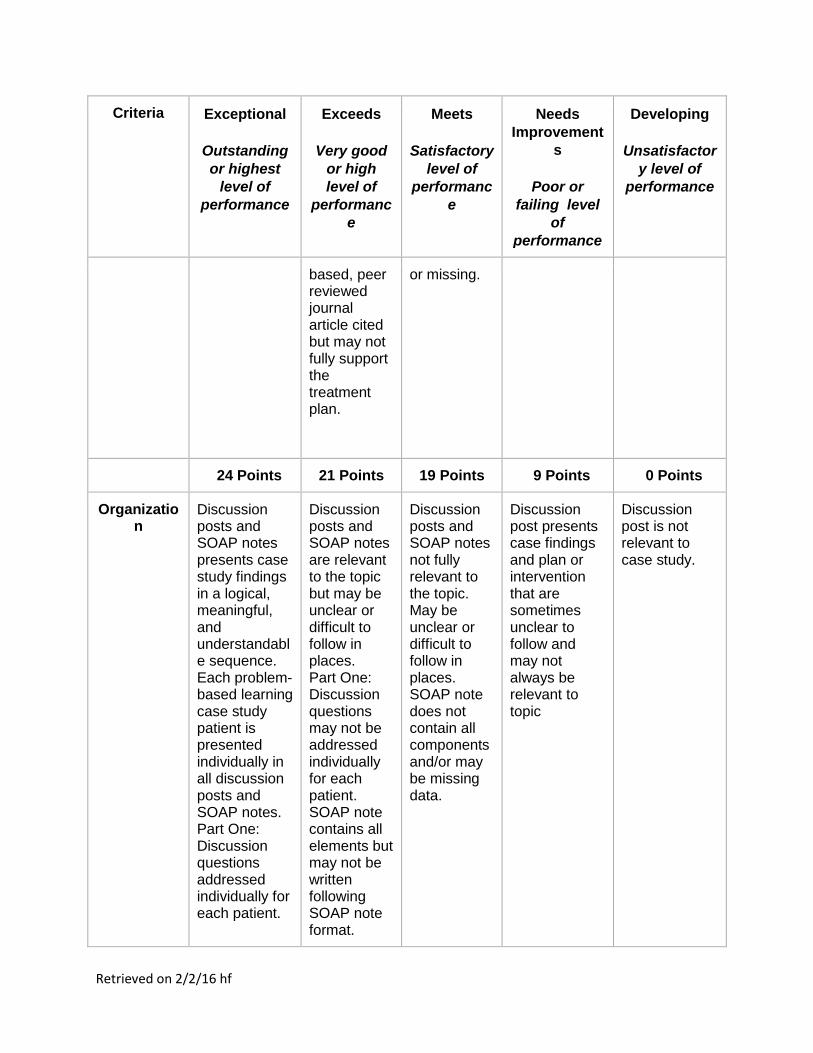
based, peer reviewed journal article cited but may not fully support the treatment plan.
or missing.
24 Points 21 Points 19 Points 9 Points 0 Points
Organization
Discussion posts and SOAP notes presents case study findings in a logical, meaningful, and understandable sequence. Each problem-based learning case study patient is presented individually in all discussion posts and SOAP notes. Part One: Discussion questions addressed individually for each patient.
Discussion posts and SOAP notes are relevant to the topic but may be unclear or difficult to follow in places. Part One: Discussion questions may not be addressed individually for each patient. SOAP note contains all elements but may not be written following SOAP note format.
Discussion posts and SOAP notes not fully relevant to the topic. May be unclear or difficult to follow in places. SOAP note does not contain all components and/or may be missing data.
Discussion post presents case findings and plan or intervention that are sometimes unclear to follow and may not always be relevant to topic
Discussion post is not relevant to case study.
Retrieved on 2/2/16 hf
Criteria Exceptional
Outstanding
or highest
level of
performance
Exceeds
Very good
or high
level of
performanc
e
Meets
Satisfactory
level of
performanc
e
Needs
Improvement
s
Poor or
failing level
of
performance
Developing
Unsatisfactor
y level of
performance
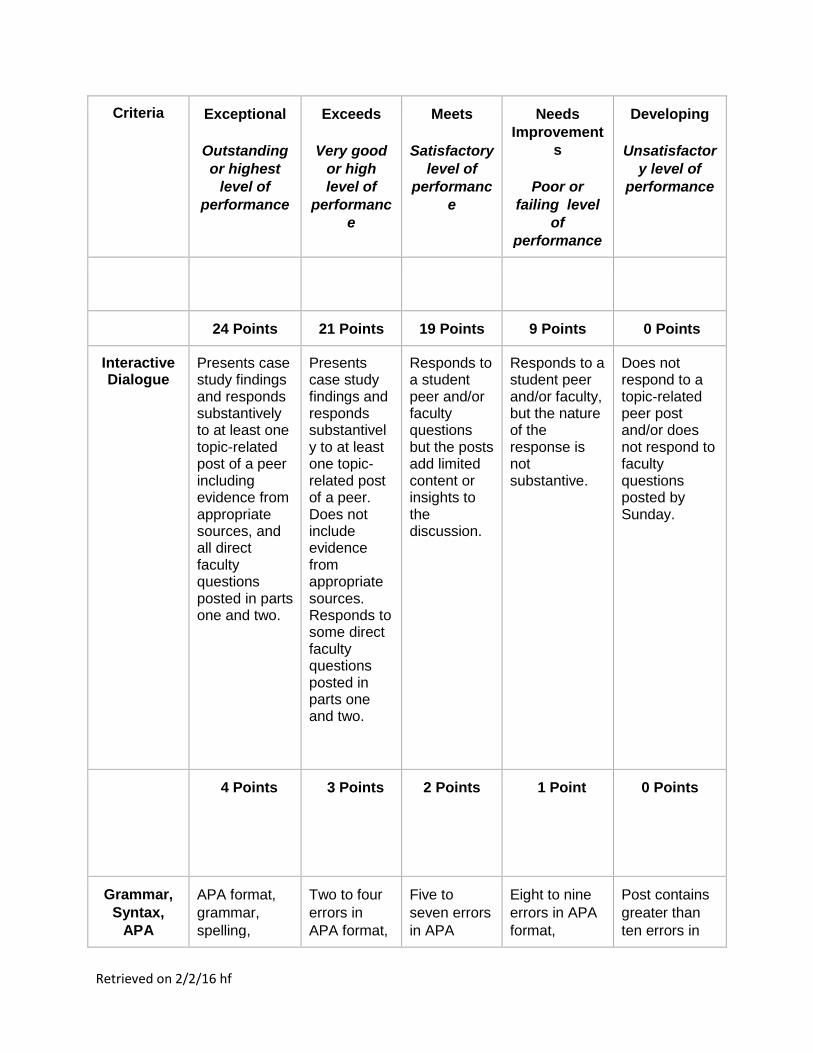
24 Points 21 Points 19 Points 9 Points 0 Points
Interactive Dialogue
Presents case study findings and responds substantively to at least one topic-related post of a peer including evidence from appropriate sources, and all direct faculty questions posted in parts one and two.
Presents case study findings and responds substantively to at least one topic-related post of a peer. Does not include evidence from appropriate sources. Responds to some direct faculty questions posted in parts one and two.
Responds to a student peer and/or faculty questions but the posts add limited content or insights to the discussion.
Responds to a student peer and/or faculty, but the nature of the response is not substantive.
Does not respond to a topic-related peer post and/or does not respond to faculty questions posted by Sunday.
4 Points 3 Points 2 Points 1 Point
0 Points
Grammar,
Syntax,
APA
APA format,
grammar,
spelling,
Two to four
errors in
APA format,
Five to
seven errors
in APA
Eight to nine
errors in APA
format,
Post contains
greater than
ten errors in
Retrieved on 2/2/16 hf
Criteria Exceptional
Outstanding
or highest
level of
performance
Exceeds
Very good
or high
level of
performanc
e
Meets
Satisfactory
level of
performanc
e
Needs
Improvement
s
Poor or
failing level
of
performance
Developing
Unsatisfactor
y level of
performance
and/or
punctuation
are accurate,
or with zero to
one errors.
grammar,
spelling, and
syntax
noted.
format,
grammar,
spelling, and
syntax
noted.
grammar,
spelling, and
syntax noted.
APA format,
grammar,
spelling,
and/or
punctuation or
repeatedly
makes the
same errors
after faculty
feedback.
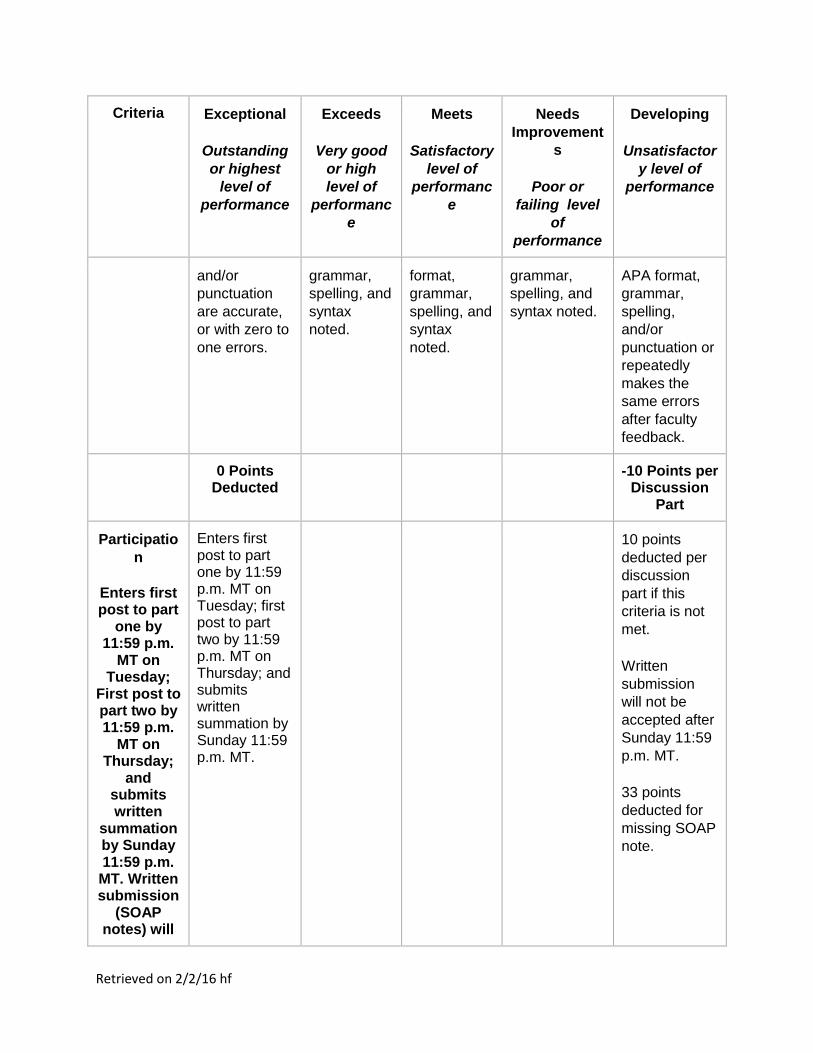
0 Points Deducted
-10 Points per Discussion
Part
Participatio
n
Enters first post to part
one by 11:59 p.m.
MT on Tuesday;
First post to part two by 11:59 p.m.
MT on Thursday;
and submits written
summation by Sunday 11:59 p.m. MT. Written submission
(SOAP notes) will
Enters first post to part one by 11:59 p.m. MT on Tuesday; first post to part two by 11:59 p.m. MT on Thursday; and submits written summation by Sunday 11:59 p.m. MT.
10 points
deducted per
discussion
part if this
criteria is not
met.
Written
submission
will not be
accepted after
Sunday 11:59
p.m. MT.
33 points
deducted for
missing SOAP
note.

Retrieved on 2/2/16 hf
Criteria Exceptional
Outstanding
or highest
level of
performance
Exceeds
Very good
or high
level of
performanc
e
Meets
Satisfactory
level of
performanc
e
Needs
Improvement
s
Poor or
failing level
of
performance
Developing
Unsatisfactor
y level of
performance
NOT be accepted
after Sunday
11:59 p.m. MT.
* 10 points deducted
per discussion part if this criteria is not met.
Webliography Disclaimer
The purpose of the Webliography is to provide students with annotated bibliographies of world wide websites relevant to their courses. These websites are not meant to be all inclusive of what is available for each course's subjects and have not been sanctioned as academically rigorous or scholarly by Chamberlain College of Nursing. Please exercise caution when using these websites for course assignments and references.
Professional Portfolio
Select assignments from courses across the FNP program will be compiled as artifacts within a Professional Portfolio to demonstrate your professional growth and expertise. Your final portfolio, which will be submitted in the final course NR661, will be assessed against the learning outcomes of the program. The Professional Portfolio will include the following:
Reflections from Week 8 for all FNP courses Five exemplar case studies (student selects top five) eLogs portfolio Curriculum vitae Professional development plan paper from NR510