NPUAP Mission Mission The National Pressure Ulcer ... NEW Educational Slide Sets ... point zig-zag...
32
6/5/2017 1 ©2017 National Pressure Ulcer Advisory Panel | www.npuap.org Why is this Wound Not Healing? June 8, 2017 Aimee Garcia, MD, CWS, FACCWS Mary Litchford, PhD, RDN, LDN npuap.org NPUAP Mission The National Pressure Ulcer Advisory Panel (NPUAP) is the nation’s leading scientific expert in pressure injury prevention and treatment. Our goal is to insure improved patient health, and to advance public policy, education and research. ©2017 National Pressure Ulcer Advisory Panel | www.npuap.org
Transcript of NPUAP Mission Mission The National Pressure Ulcer ... NEW Educational Slide Sets ... point zig-zag...
6/5/2017
1
©2017 National Pressure Ulcer Advisory Panel | www.npuap.org
Why is this Wound Not Healing?June 8, 2017
Aimee Garcia, MD, CWS, FACCWSMary Litchford, PhD, RDN, LDN
npuap.org
NPUAP MissionThe National Pressure Ulcer
Advisory Panel (NPUAP) is
the nation’s leading
scientific expert in pressure
injury prevention and
treatment. Our goal is to
insure improved patient
health, and to advance
public policy, education
and research.
©2017 National Pressure Ulcer Advisory Panel | www.npuap.org

6/5/2017
2
Reduced Price for theInternational Guideline!
NPUAP in collaboration with the
European Pressure Ulcer Advisory
Panel (EPUAP) and the Pan Pacific
Pressure Injury Alliance (PPPIA) has
worked to develop a pressure injury
prevention and treatment the Clinical
Practice Guideline and Quick
Reference Guide. The price of these
books have recently been reduced.
Purchase your copy today at
www.npuap.org
npuap.org©2017 National Pressure Ulcer Advisory Panel | www.npuap.org
NPUAP Monograph
Released in November 2012, the 254-page,
24 chapter monograph, Pressure Ulcers:
Prevalence, Incidence and Implications for the
Future was authored by 27 experts from NPUAP
and invited authorities and edited by NPUAP
Alumna Dr. Barbara Pieper.
The monograph focuses on pressure ulcer rates
from all clinical settings and populations; rates in
special populations; a review of pressure ulcer
prevention programs; and a discussion of the
state of pressure ulcers in America over the last
decade.
Purchase the monograph today at www.npuap.org
• E-version $49
• Individual Chapters $19npuap.org
©2017 National Pressure Ulcer Advisory Panel | www.npuap.org

6/5/2017
3
NEW Educational Slide Sets
npuap.org©2017 National Pressure Ulcer Advisory Panel | www.npuap.org
• Pressure Injury Definition and
Stages
• Prevention of Pressure Injury
• Treatment of Pressure Injury
Each downloadable slide set includes
presentations, speaker notes and
handouts
Purchase the slide sets today at www.npuap.org
©2016 National Pressure Ulcer Advisory Panel | www.npuap.org

6/5/2017
4
THANK YOU to the following companies that have provided support for this webinar!
• Acelity
• American Medical
Technologies
• ArjoHuntligh
• Coloplast
• Dabir Surfaces
• HoverTech
International
• Leaf Healthcare
• Medline
The NPUAP webinar commercial supporters
did not have any input regarding the
content of this presentation.
THANK YOU to the following companies that have provided support for this webinar!
• Molnlycke
• Permobil
• Position Health
• Select Medical
• Sizewise
• Span America
• Stryker
• Tamarack Habilitation
Technologies
• Wellsense
The NPUAP webinar commercial supporters
did not have any input regarding the
content of this presentation.

6/5/2017
5
Faculty Disclosure
©2016 National Pressure Ulcer Advisory Panel | www.npuap.org
• Aimee Garcia, MD, CWS, FACCWSNo disclosures
Past President, NPUAP
• Mary Litchford, PhD, RDN, LDNPresident CASE Software & Books
Author of:•Nutrition Focused Physical Assessment: Making Clinical
Connections;
•Laboratory Assessment of Nutritional Status: Bridging Theory &
Practice
•Nutrition & Pressure Injuries: Putting New Guidelines into Practice
•Common Denominators of Declining Nutritional Status
Consultant for Prosynthesis Labs
Speaker’s Bureau Abbott Labs
Speaker’s Bureau Nestle Nutrition
President National Pressure Ulcer Advisory Panel
Planning Committee Disclosures
• Jeffrey Levine, MD
• Mary Litchford, PhD, RD, LDN
• Sally O’Neill, PhD
• Mary Sieggreen, MSN, CNS, NP, CVN
The planning committee members have listed
no financial interest/arrangements that would
be considered a conflict of interest.
©2017 National Pressure Ulcer Advisory Panel | www.npuap.org

6/5/2017
6
Objectives
• Understand the factors that might impact
wound healing
• Identify what work-up is required to
assess a non-healing wound
• Discuss the nutrition recommendations
for pressure injury treatment in a chronic
wound.
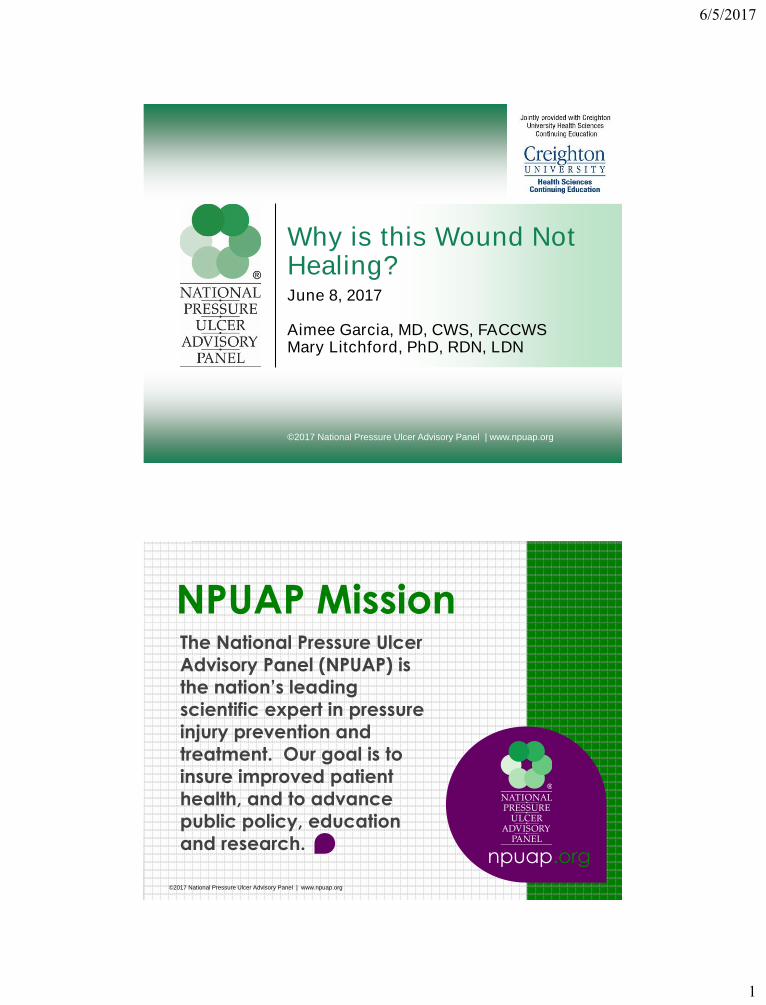
Non-healing wound
• A non-healing or chronic wound is defined
as a wound that does not improve after four
weeks or does not heal in eight weeks.
• Many factors can impact wound healing
6/5/2017
7

6/5/2017
8
Factors that Impact Wound Healing
• Medications
• Immobility
• Radiation Therapy/Chemotherapy
• Arterial / Venous Insufficiency
• Diabetes & Other Chronic Medical Diseases
• Aging
• Smoking
• Infection
• Nutrition
Medications
• Any medication that impacts the
inflammatory phase
– NSAIDS
– Steroids
– Immunosuppressive medications
6/5/2017
9
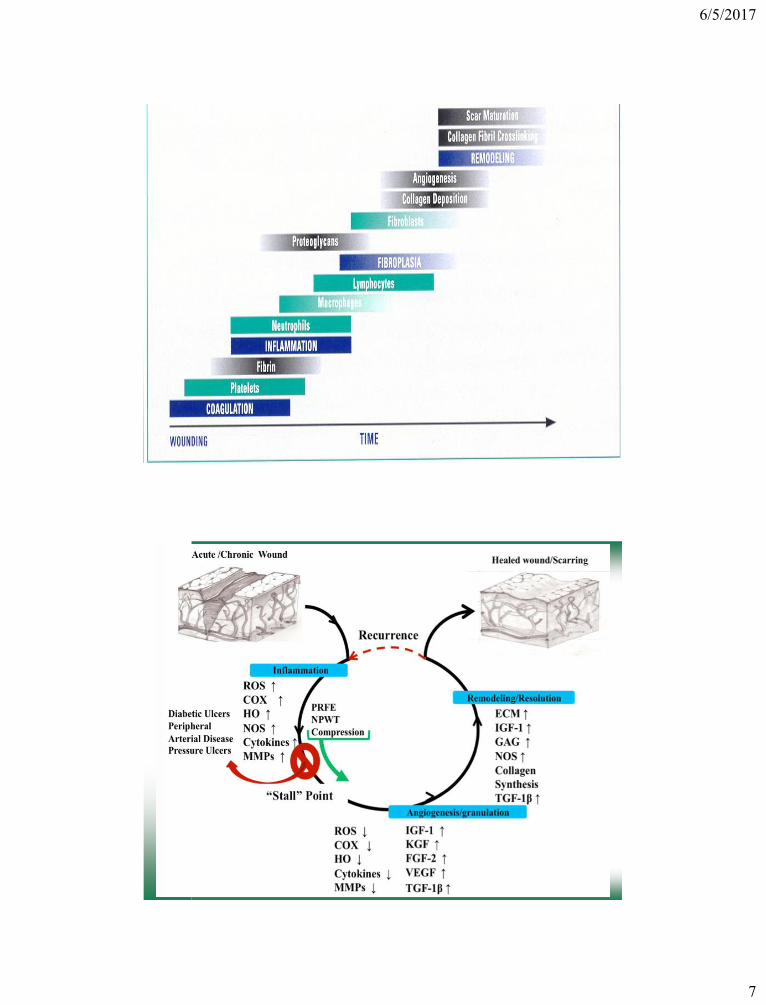
PRESSURE POINTS
Factors that impact wound healing
• Radiation Therapy/Chemotherapy
• Arterial / Venous Insufficiency
• Diabetes & Other Chronic Medical
Diseases
6/5/2017
10
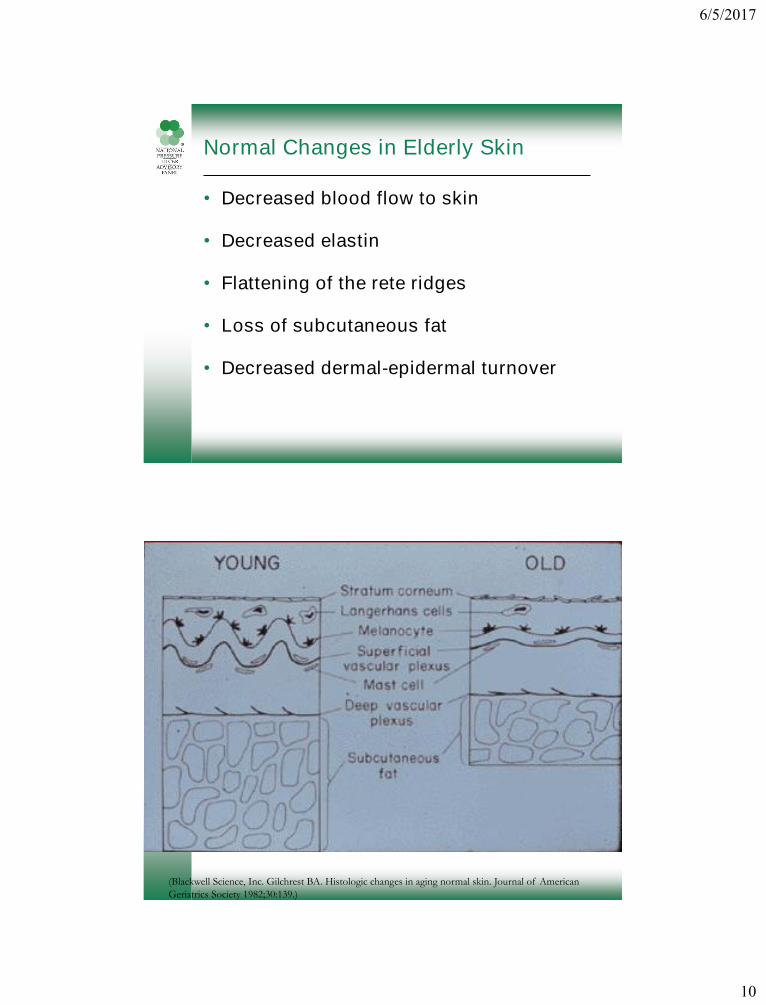
Normal Changes in Elderly Skin
• Decreased blood flow to skin
• Decreased elastin
• Flattening of the rete ridges
• Loss of subcutaneous fat
• Decreased dermal-epidermal turnover
(Blackwell Science, Inc. Gilchrest BA. Histologic changes in aging normal skin. Journal of American
Geriatrics Society 1982;30:139.)
6/5/2017
11
Smoking
• Nicotine
• Carbon Monoxide
• Hydrogen cyanide
• Effects last for 1 hour after smoking
Bacterial Burden Negative Impact on Wound Healing
• Prolongs the inflammatory stage
• Induces additional tissue destruction
• Delays collagen synthesis
• Prevents epithelialization
6/5/2017
12
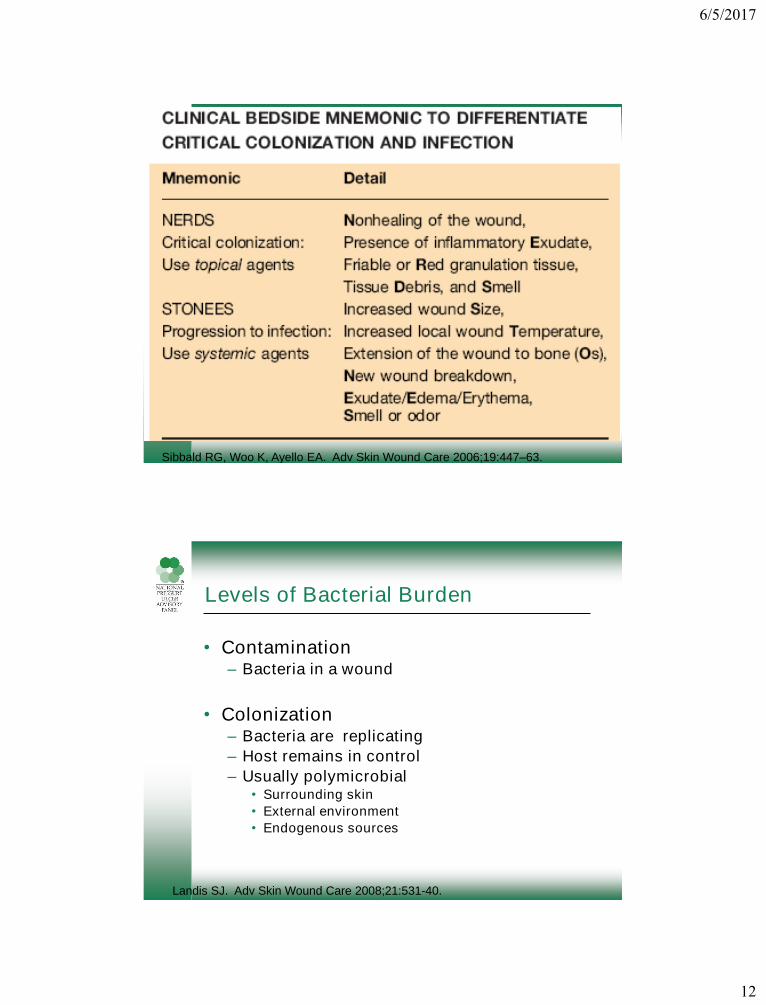
Sibbald RG, Woo K, Ayello EA. Adv Skin Wound Care 2006;19:447–63.
Levels of Bacterial Burden
• Contamination– Bacteria in a wound
• Colonization– Bacteria are replicating
– Host remains in control
– Usually polymicrobial• Surrounding skin
• External environment
• Endogenous sources
Landis SJ. Adv Skin Wound Care 2008;21:531-40.

6/5/2017
13
Landis SJ. Adv Skin Wound Care 2008;21:531-40.
Levels of Bacterial Burden
• Critical Colonization– wounds with more than 100,000 organisms/gram
will not heal
– Suspect bacterial burden if a clean wound shows no improvement after 14 DAYS of topical therapy
• Infection– Invasion of the soft tissues

6/5/2017
14
Probability of Host Infection
P (Infection) = Bacterial burden x Virulence
Host resistance
Landis SJ. Adv Skin Wound Care 2008;21:531-40.
Wound Cultures
• Traditional swab culture detects only surface
bacterial colonization/contamination
– may not reflect the invasive organism causing
infection
• Quantitative Wound Culture recommended for
determining infection
– documents bacterial burden
– identifies bacteria actually invading wound tissue
6/5/2017
15
Quantitative Analysis
• Superficial Swab
– Z swab
– Levine technique
• Needle aspiration
• Punch Biopsy
• Tissue sample
Z swab
• Swabs using the Z-stroke entail rotating the
swab between the fingers as the wound is
swabbed from margin to margin in a 10
point zig-zag fashion.

6/5/2017
16
Levine technique
• The Levine Technique consists of rotating
the swab over a 1 cm square area with
enough pressure to express fluid from within
the wound tissue
• The Levine Technique is best used when in
the wound is first cleaned and there is no
necrotic tissue or eschar
Tissue hypoxia
• Inhibition of oxidative burst activity in
polymorphonuclear leukocytes
– ↓ intracellular production of antimicrobial
metabolites
• Reduced leukocyte killing capacity
• Fecal contamination contains high
numbers of anaerobes
Hohn DC et al. Surg Forum 1976; 27: 18-20.

6/5/2017
17
Complications
• Osteomyelitis
• Fistulas
• Carcinoma
• Sepsis
Osteomyelitis
• Can occur in 1/3rd of pressure ulcers
• Osteomyelitis most common in:
– Pelvis
– Femoral head
– Ischial bones
– Calcaneus
• If bone is visible or palpable, likelihood
of osteomyelitis is >90%

6/5/2017
18
Osteomyelitis
• Work up
– Plain x-rays
– Lab analysis
• ESR, CRP
– Bone scans
– MRI
– Biopsy
©2011 National Pressure Ulcer Advisory Panel | www.npuap.org
Fistulas
• Abnormal passage between two
epithelialized surfaces that connect one
viscera to another or to the body surface
http://www.nhstaysideadtc.scot.nhs.uk/wound%20Formulary/Section%2010/Section%2011%20fistula%20as
%20attachment.pdf

6/5/2017
19
Fistulas
• Management goals:
– Management and free drainage of exudate
– Protection of surrounding skin
– Prevention of infection
– Removal of necrosis or slough
– Promotion of granulation from the base of the
wound
Sinus Tracts
• Discharging, blind-ended track that
extends from the surface of the skin to
an underlying abscess/cavity. May be
caused by infection, liquefaction or a
foreign body
http://www.nhstaysideadtc.scot.nhs.uk/wound%20Formulary/Section%2010/Section%2011%20fistula%20as
%20attachment.pdf
6/5/2017
20
Sinus Tracts
• Management goals:
– Allow cleansing and draining
– Do not plug
– Protection of surrounding skin
– Prevention of infection
– Removal of necrosis or slough
– Promotion of granulation from the base of the
wound
Carcinoma in Pressure Ulcers
• Marjolin’s ulcer
– Most commonly found in burn wounds and
osteomyelitis
– Most common type: squamous cell
carcinoma
– Other types:
• Basal cell
• Melanoma
• Fibrosarcoma
• Angiosarcoma
• Osteosarcoma
• Others
6/5/2017
21
Occurrence
• Most malignancies in pressure ulcers
occur in the sacral or iliac areas
• Rich lymphatic drainage to the pelvic
region
– Higher rates of metastasis
• Little support for chemo; Radiation can
be effective for palliation
Marjolin’s Ulcer
• Occurs in 1.7% of chronic wounds
• Incidence of SCCa in pressure ulcers is
0.5%
• Very aggressive
• Metastatic rate in pressure ulcers is 60%– Burns (38%)
– Osteo (14%)
• Biopsy if wound present for >6 months

6/5/2017
22
Prognosis
• Factors affecting prognosis
– Tumor type
– Location
– Rate of metastasis
• Survival rates
– 65-75% in 3 years
– 35-50% if metastatic disease present
SIRS
• Defined as a systemic response to
infection
• Criteria:– Fever of more than 38°C (100.4°F) or less than 36°C
(96.8°F)
– Heart rate of more than 90 beats per minute
– Respiratory rate of more than 20 breaths per minute or
arterial carbon dioxide tension (PaCO 2) of less than 32
mm Hg
– Abnormal white blood cell count (>12,000/µL or <
4,000/µL or >10% immature [band] forms)

6/5/2017
23
SIRS
• Non-specific
• Can be caused by multiple conditions:
– Infection
– Ischemia
– Trauma
– Inflammation
– Combination of above
Sepsis
• Bacteremia
– Not always related to SIRS or sepsis
• Sepsis
– Systemic response to infection
– SIRS + infection
• Associated with:
– Hypoperfusion
– Organ dysfunction
– Hypotension

6/5/2017
24
©2017 National Pressure Ulcer Advisory Panel | www.npuap.org
Nutrition
Mary Litchford, PhD, RDN, LDN
Two observations:
1. “Healing is a matter of time, but sometimes also a matter of opportunity.”
2. “Let food be thy medicine and medicine be thy food.”
48
Does Nutrition Really Make a Difference?
HippocratesImage from Dreamtime Photos

6/5/2017
25
Undernutrition-Malnutrition Continuum
49
• Organ function
• Food-Meds Issues
• Adapted from: Litchford, M. Nutr Clin Prac. Aug 2014 29:428.
• Food intake
• Weight loss
• Fat stores
• Muscle mass
• Physical strength
• Illness
• Injury or surgery
• Loss of reserves
• Too tired to shop or cook
• Too tired to eat
• Limited food budget
Poor dietary intake
Increased nutrient needs
Impaired nutrient transport
Undernutrition & malnutrition
2014 NPUAP-EPUAP & Pan Pacific Pressure Injury Alliance (PPPIA) CPG
Nutrition Recommendations
• Nutrition screening
• Nutrition assessment
• Care planning
• Energy intake
• Protein intake
• Hydration
• Vitamins and minerals
50
Image by Dreamtime
6/5/2017
26
Provide 30 to 35 kcalories/kg body weight for adults
with a pressure ulcer who are assessed as being at
risk of malnutrition.
Adjust energy intake based on weight change or level
of obesity. Adults who are under weight, or who have
had significant unintended weight loss, may need
additional energy intake.
Reassess Energy Requirements
© CSB, 201651
2014 NPUAP-EPUAP & Pan Pacific Pressure Injury Alliance (PPPIA) CPG
Reassess Energy Requirements: Action Plan
52
1.Collect more data on
actual food intake
over 2-4 days
2.Determine amount
and quality of protein
eaten per meal
3.Recheck height &
weight
4.Assess for chewing &
swallowing problems
5.Reassess need for
therapeutic diets
Image by Dreamtime

6/5/2017
27
Reassess Hydration Status
Provide and encourage adequate daily fluid intake for hydration for an individual assessed to be at risk of or with a pressure ulcer. This must be consistent with the individual’s comorbid conditions and goals.
Monitor individuals for s and sx of dehydration, including change in weight, skin turgor, urine output, serum Na, and/or calculated serum osmolality.
53
2014 NPUAP-EPUAP & Pan Pacific Pressure Injury Alliance (PPPIA) CPG
Images from Dreamtime Photos
Reassess Water Requirements: Action Plan
54
1. Collect more data on
actual intake water
over 2-4 days
2. NFPA for s/s
dehydration
3. Recheck weight
history
4. Assess for
swallowing problems
5. Assess need for
thickened liquids if
ordered
Image by Dreamtime
6/5/2017
28
Reassess Protein Requirements
Offer 1.25 to 1.5 gms protein/kg
body weight daily for adults with an
existing pressure ulcer and who are
assessed to be at risk of
malnutrition when compatible with
goals of care, and reassess as
condition changes.
Provide adequate protein for
positive nitrogen balance for adults
with a pressure ulcer.
Images from Dreamtime Photos
55
2014 NPUAP-EPUAP & Pan Pacific Pressure Injury Alliance (PPPIA) CPG
Reassess Protein Requirements:Action Plan
56
1. Collect more data on
actual protein intake
over 2-4 days
2. Determine amount
and quality of protein
eaten per meal
3. Assess for chewing
& swallowing
problems
4. Reassess need for
therapeutic diets
Image by Dreamtime

6/5/2017
29
Protein Sources are Not Nutritionally Equal
57
Incomplete Protein Complete
Protein
Food For Thought
Which menu promotes tissue synthesis?
Menu 1 (no B, light L, heavy S)
Menu 2 (equal at each meal)
Menu 3 (light B, light L, heavy S)
No difference in outcomes
0
20
40
60
Breakfast Lunch Dinner
PR
O g
m
Meal
Protein Distribution at Meals
Menu 1
Menu 2
Menu 3
58

6/5/2017
30
Leucine Triggers Tissue Synthesis
0
20
40
60
80
100
120M
g l
eu
cin
e p
er
gm
pro
tein
Leucine ( mg/gm PRO)
Source Protein in Dietary Supplements per Selected Manufacturers' Websites & USDA Nutrient Analysis
Database
59
Options when Intake is Insufficient
Offer high calorie, high protein nutritionalsupplements in addition to the usual diet to adults with nutritional risk and pressure ulcer risk if nutritional requirements cannot be achieved by dietary intake.
Supplement with high protein, arginine, and micronutrients for adults with a pressure ulcer Category/Stage III or IV or multiple pressure ulcers when nutritional requirements cannot be met with traditional high calorie and protein supplements.
Images from Dreamtime Photos
60
2014 NPUAP-EPUAP & Pan Pacific Pressure Injury Alliance (PPPIA) CPG
6/5/2017
31
New Nutrition Prescription: Action Plan
61
1. Address each
problem:
2. Small appetite: use
fortified foods
3. Insufficient protein
intake: 30 gm protein
meal, supplements
4. Chewing/swallowing
problems:
consistency modified
diet
5. Fatigue: mealtime
assistantImage by Dreamtime
References1. Posthauer ME, Banks M, Dorner B, et al. The role of nutrition for pressure ulcer management:
National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel, and Pan Pacific
Pressure Injury Alliance white paper. Adv Skin Wound Care 2015 Apr;28(4):175-88; quiz 189-90.
http://journals.lww.com/aswcjournal/Fulltext/2015/04000/The_Role_of_Nutrition_for_Pressure_Ulcer.7
.aspx. Accessed June 10, 2016.
2. Litchford, MD. Counteracting the Trajectory of Frailty and Sarcopenia in Older Adults. Nutr Clin Prac.
Aug 2014 29:428-434.
3. Litchford M, Dorner B, Posthauer ME. Malnutrition as a precursor of pressure ulcers. Wound
2014;3(1):54-63. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3899999/. Accessed June 10, 2016.
4. Evidence-based recommendations for optimal dietary protein intake in older people: a position
paper from the PORT-AGE study group. J Am Med Dir Assoc 2013;14(8):542-59.
http://www.sciencedirect.com/science/article/pii/S1525861013003265. Accessed June 10, 2016.
5. 2014 National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan
Pacific Pressure Injury Alliance. Prevention and treatment of pressure ulcers: clinical practice
guideline. Haesler E, ed. Cambridge Media: Osborne Park, Western Australia.
6. Dorner B, Friedrich EK, Posthauer ME; American Dietetic Association. Position of the American
Dietetic Association: individualized nutrition approaches for older adults in health care communities.
J Am Diet Assoc 2010;110:1549-53.
7. Lim SL, Ong KC, Chan YH, et al. Malnutrition and its impact on cost of hospitalization, length of stay,
readmission and 3-year mortality. Clin Nutr 2012;31(3):345-50.
http://www.sciencedirect.com/science/article/pii/S0261561411001993. Accessed June 10, 2016.
8. Rojer AG, Kruizenga HM, Trappenburg MC, et al. The prevalence of malnutrition according to the new
ESPEN definition in four diverse populations. Clin Nutr 2015;35(3):758-62.
http://www.sciencedirect.com/science/article/pii/S0261561415001740. Accessed June 20, 2016.
62
6/5/2017
32
References9. White J, Guenter P, Jensen G, et al.; Academy of Nutrition and Dietetics Malnutrition Work Group;
A.S.P.E.N. Malnutrition Task Force; A.S.P.E.N. Board of Directors. Consensus statement of the Academy
of Nutrition and Dietetics/American Society of Parenteral and Enteral Nutrition: characteristics
recommended for the identification and documentation of adult malnutrition (undernutrition). J Acad
Nutr Diet 2012:112(5):730-8. http://www.andjrnl.org/article/S2212-2672(12)00328-0/fulltext. Accessed
June 20, 2016.
10.Edsberg L, Langemo D, Baharestani M, et al. Unavoidable pressure injury: state of the science and
consensus outcomes. J Wound Ostomy Continence Nurs 2014 Jul-Aug;41(4):313-34.
11.van Anholt RD, Sobotka L, Meijer EP, et al. Specific nutritional support accelerates pressure ulcer
healing and reduces wound care intensity in non-malnourished patients. Nutrition 2010;26(9):867-72.
http://www.sciencedirect.com/science/article/pii/S089990071000167X. Accessed June 10, 2016.
12.Cereda E, Klersy C, Serioli M, et al.; Oligo Element Sore Trial Study Group. A nutritional formula
enriched with arginine, zinc, and antioxidants for the healing of pressure ulcers: a randomized,
controlled trial. Ann Intern Med 2015;162(3):167-74.
63
CE Test Information
To earn the 1.0 CE credit for today’s
webinar please visit the link below.
This information will also be emailed out to
webinar registrants ONE HOUR after the
conclusion of the webinar.
https://blueq.co1.qualtrics.com/jfe/form/SV
_1ChUkJSaolcDrGl