

NPfIT: The Biggest Computer Programme in the World Ever ! Sean Brennan Clinical Matrix.
53
NPfIT: The Biggest Computer Programme in the World Ever ! Sean Brennan Clinical Matrix
-
Upload
tracy-perry -
Category
Documents
-
view
213 -
download
0
Transcript of NPfIT: The Biggest Computer Programme in the World Ever ! Sean Brennan Clinical Matrix.

NPfIT:The Biggest Computer
Programme in the World
Ever !
Sean BrennanClinical Matrix
Why do the cows in the Isle of Man have better computers that
the NHS?

But…………………..
• Daisy’s Record is a by-product.• The Primary objective is to milk her.

Why does my dog have a better electronic health record than I
have?
Clinical History
Doggie Health Record
So why do we need clinical IT?
Today in the NHS (England)
• Will spend £170 million• £2000 every second• £10 million settling litigation claims• 110 people will die due to ‘adverse events’• 1230 people will suffer an adverse event• 270 people will catch a hospital acquired infection• £2.8 million on treating patients who have MRSA• £1.3 million on treating patients who have had an
adverse drug event
Today in the NHS (England)
• 200,000 people will get help in their home from the NHS• 1.2 million will visit their GP’s• 160,000 will be treated in NHS Outpatients• 140,000 will visit an NHS dentist• Over 1400 babies will be born• NHS Direct will receive 3,500 calls seeking advice• Labs will perform millions of tests
The NHS is a very BUSY organisation.• 3 million critical processes each and every day.• If totally supported by electronic records that would be approx 30 MILLION30 MILLION new transactions
each day!
So
• Computerising the NHS is a very big and very difficult project.
• But lets NOT just add technology to existing workflow…….Isn’t there a better way?

Spanish Brasero – wasted opportunity?
A.A. Milne 1926
Illustration E.H.Shepard 192614
“Here is Edward Bear,coming
downstairs now, bump, bump, bump,
on the back of his head, behind
Christopher Robin. It is, as far as
he knows, the only way of coming
downstairs, but sometimes he feels
that there really is another way,
if only he could stop bumping for
a moment and think of it”

It’s about change
• We need to change the way care is delivered
• IT enables change to happen• The current model is no longer
appropriate
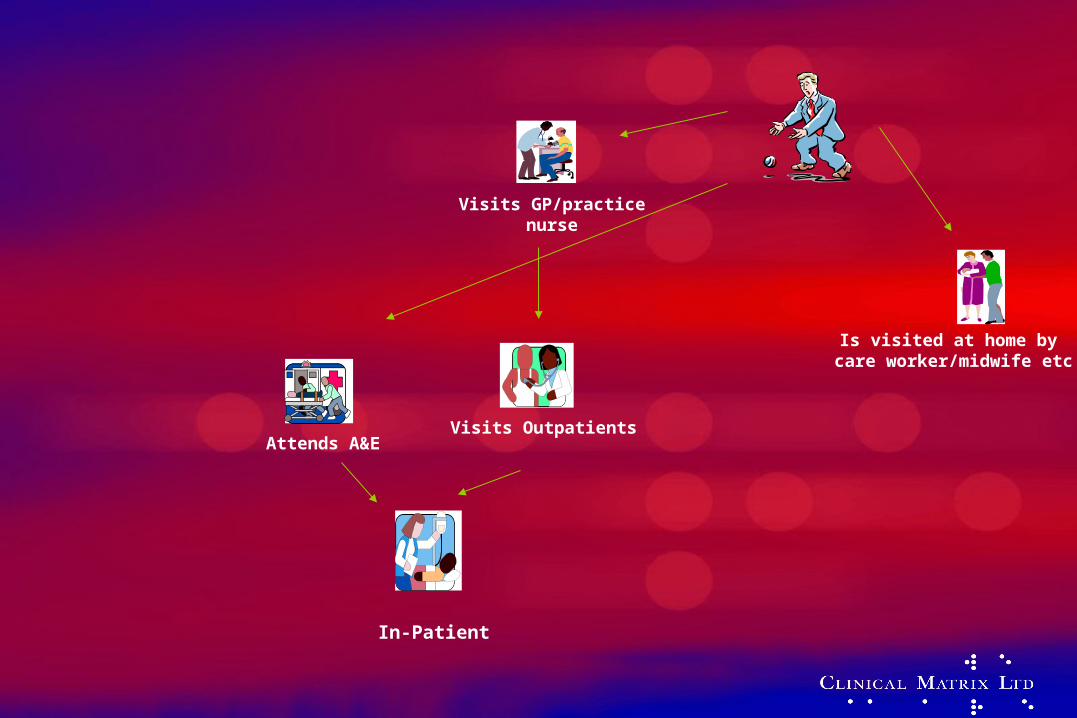
Visits GP/practicenurse
Visits OutpatientsAttends A&E
Is visited at home by care worker/midwife etc
In-Patient

Visits OutPatients
VisitsGP/practice
nurse
Attends A&E
Calls NHSDirect
Uses theHome HealthCare Guide
Calls OOHservice
Is visited at homeby GP, nurse, social
/ care worker,midwife etc
Goes to thepharmacy
Visits thedentist
Attends as
in-patient
Calls 999
Use NHSDirect.online
Visits awalk-incentre

We must use technology to support change
Not just add technology to existing ways of working


LSP
iSoft i.EPR / Lorenzo
Integration Bus
EM
IS P
CS
Torex P
SE
InPractise V
ision
Niche C
linicals
Portal
LSP
iSoft i.EPR / Lorenzo
Integration Bus
EM
IS P
CS
Torex P
SE
InPractise V
ision
Niche C
linicals
Portal
LSP
iSoft i.EPR / Lorenzo
Integration BusE
MIS
PC
S
Torex P
SE
InPractise V
ision
Niche C
linicals
Portal
LSP
Cerner
Integration Bus
EM
IS P
CS
Torex P
SE
InPractise V
ision
Niche C
linicals
Portal
LSP
IDX
Integration Bus
EM
IS P
CS
Torex P
SE
InPractise V
ision
Niche C
linicals
Portal
Blo
od
Gro
up
A+
, Allerg
ic to p
enic
illin
NH
S C
are Record S
ervice
Cluster wide Data Repository
Cluster wide Data Repository
Cluster wide Data Repository
Cluster wide Data Repository
Cluster wide Data Repository

NASP
LSP
iSoft i.EPR / LorenzoCerner Or IDX
Integration Bus
EM
IS P
CS
Torex P
SE
InPractise V
ision
Niche C
linicals
National Data Repository
Portal
What does it look like?
eBooking PDS PSIS eTP
Transaction Messaging Service
Cluster wide Data Repository

What will it do?NASP
LSP
iSoft i.EPR / Lorenzoor IDX or ?
Integration Bus
EM
IS P
CS
Torex P
SE
InPractise V
ision
Niche C
linicals
National Data Repository
Portal
eBooking PDS PSIS eTP
Transaction Messaging Service
Cluster wide Data Repository
Patient IndexPACS
Prescribing &Pharmacy
Scheduling
ClinicalDocumentation
Request & OrderCommunication
Decision Support
Assessment
ResultsReporting
DocumentManagement
eBooking
Care Management
Care Pathways & Planning
User Tools
Prevention, scheduling
& surveillance

So what’s in it for you and your patients?
•This is the biggest national clinical change programme ever carried out in the NHS
•It will affect you and all your clinical colleagues•It will impact the way that you practice and improve the way
you treat your patients by:
– Ensuring that the right information is always available at the point of care
– Making it easier and faster to book appointments order tests and see results, anywhere
– Helping to ensure consistent good practice treatments– Reducing prescribing errors– Stops the paper chase. Making huge savings on the 30% of
all NHS costs that are associated with recording, transporting, storing, and looking for information!
OK – so what do I get out of it?
• Access to knowledge/guidelines• Real-time decision support• Access to ALL the patients information• Reduction in administrative data collection• Provide clinical information for secondary
analysis• Reduce inappropriate referrals• Plan discharge• Opportunities to re-design the service
NCRS: What are the benefits?
Benefits……….
• Access to clinical knowledge• Access to all the patients information• Better communications• Decision support• Easier ordering and prescribing• Access to digital images (X-Rays)• Care pathways and protocols• Quality clinical information for audit and research

Hospital discharge letters
• Illegible• Written in haste• Arrive two weeks after discharge

Benefits: Access to knowledge

T’Internet
The Good, the Bad and the Ugly

Benefits
Reduce Illegibility

Illegible Writing kills Patients!
• Doctors writing illegibly are still killing patients Advise doctors to write in CAPITAL LETTERS• It is writing in lower case in a hurry which
causes mistakes Medical Defense Union in BMJ 1992;305:604

Benefits
Decision Support
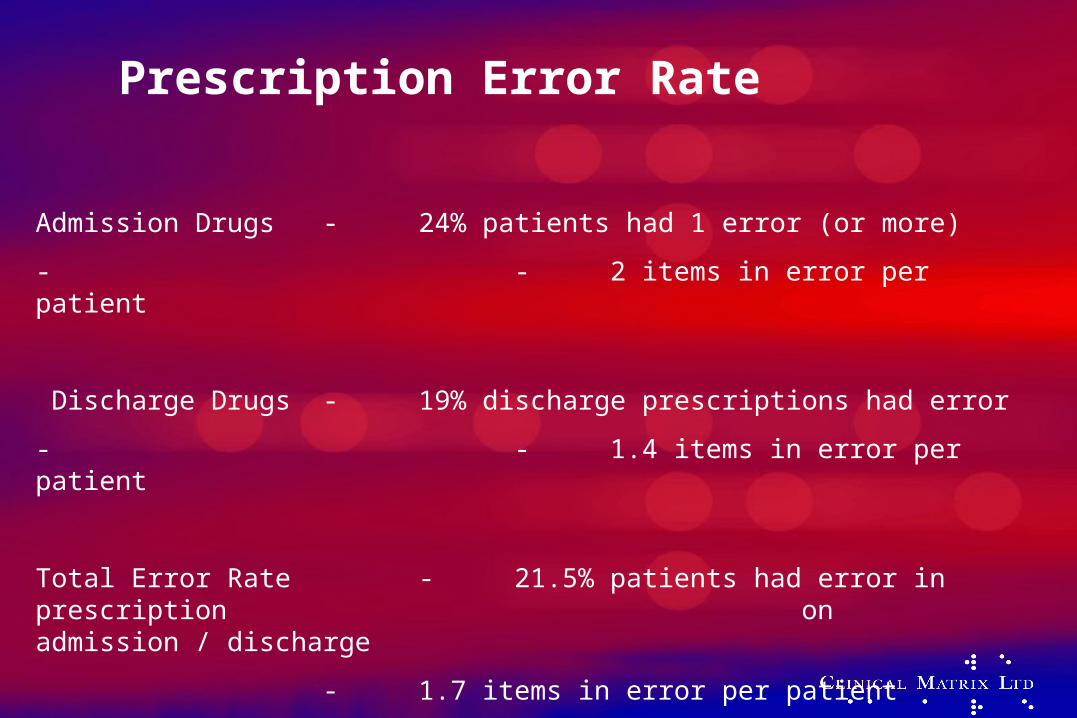
Prescription Error Rate
Admission Drugs - 24% patients had 1 error (or more)
- - 2 items in error per patient
Discharge Drugs - 19% discharge prescriptions had error
- - 1.4 items in error per patient
Total Error Rate - 21.5% patients had error in prescription on admission / discharge
- 1.7 items in error per patient
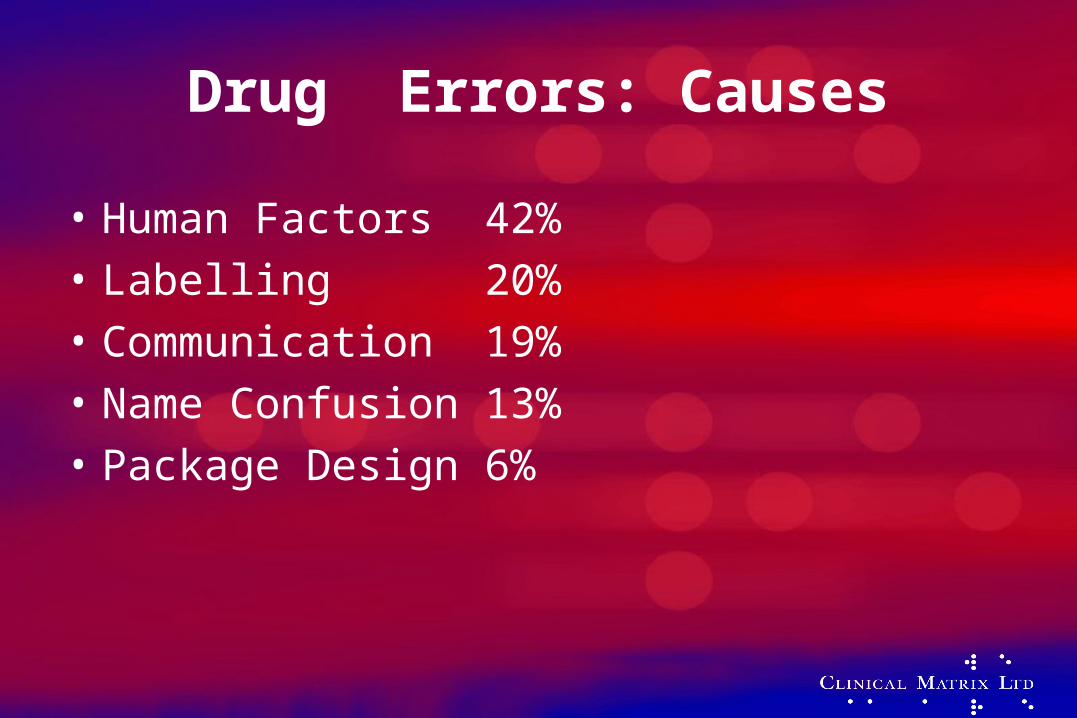
Drug Errors: Causes
• Human Factors 42%• Labelling 20%• Communication 19%• Name Confusion 13%• Package Design 6%

Advantages of Electronic Medicines Administration
• Clarity• Schedule compliance• Audit trail• Alerts/Warnings

But……..• Computer errors on the increase!
– 46% errors in transcription and documentation phase– 36% errors at drug dispensing– 13% errors at prescription phase– 4% errors at drug administration
• Automation does not equal safety. Training is an issue
• Don Detmer: Properly structured automated systems can reduce error rates substantially. However, simply installing an automated system will not magically eliminate errors.

Benefits:
Warnings
Useful Warnings !
• The drug you are about to give the patient will react with one they are already on.
• The dose you are about to give the patient is incorrect for their body mass.
• On bottom of Coke bottles –– Open other end
What will make it work?
• What’s in it for me ?– Benefits to me as a clinician– Benefits to my patients– Benefits to my organisation
• Is it easy to use?• Is it responsive? (i.e. quick!)
Making it easy to use
The Interface: The London Underground



Ways to improve clinical data capture

User Interface
• Touch Screens• Handwriting Recognition• Bar Codes• OCR Forms• Light Pens• Voice Recognition

Touch Screens for clinicians
• In certain conditions excellent– Operating Theatres– Sterile Stores– Reception areas
Bar Codes
• Invented in1948 by Bernard Silver and Norman Woodland
• 1949 first patent issued 1952• Trial by Bar Codes?• But…….was it the Irish who invented it?
Bar Codes: Uses in healthcare
• Drugs• Laboratories• Meals• Fluids• Positive Patient ID• X-Ray films
Light Pens
• Rapid• Easy to use• Used at Wirral • Removes need for keyboard• Rapid (Did I say rapid?)
Optical Character Recognition
• Useful for patients use– Complete data before consultation
• Good for surveys• Where multiple data items are collected –
Anaesthetic information in theatre• Paper is good !
Voice Recognition
• Opportunities– Radiology– Pathology– Clinician Reporting
• Discharge letters• Outpatient letters
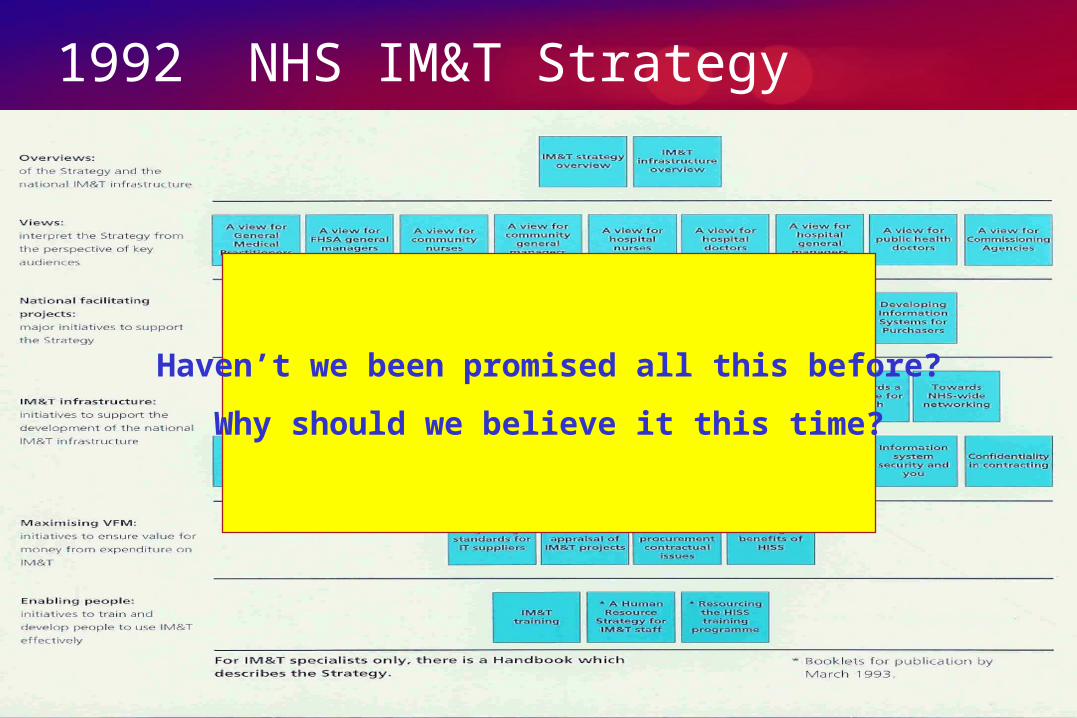
1992 NHS IM&T Strategy
Haven’t we been promised all this before?
Why should we believe it this time?

This time…..
• Top of the office commitment• Huge increase in resources• Tight contracts• Buying a service not a single system• Local Service Providers accountable• Recognition that it is NOT just an IT project
But………………..
• Local Vs.. National• We MUST engage clinicians• We MUST be open and honest about timetable• We MUST acknowledge it is difficult AND
different• We SHOULD ensure we have the right focus• We MUST learn from history
What annoys clinicians?
• Change for the sake of change• Dodgy evidence• Quicker doesn’t always mean better• Systems that don’t fit clinical workflow• Feeding the beast• Slow systems• Not enough workstations• Interfering computers• Too many alerts• Complicated systems/poor user interface


















