
Novedades en el tratamiento de la hepatitis C: noticias desde la … · 2016-06-03 · Novedades en...
37
Novedades en el tratamiento de la hepatitis C: noticias desde la EASL Rafael Esteban Hospital Universitario Valle Hebrón Barcelona
Transcript of Novedades en el tratamiento de la hepatitis C: noticias desde la … · 2016-06-03 · Novedades en...

Novedades en el tratamiento de la hepatitis C: noticias desde la EASL
Rafael Esteban
Hospital Universitario Valle Hebrón
Barcelona

Real-World Data
2

94 96 96 96 97
020406080
100
Category 1
Real-World Effectiveness and Safety of LDV/SOF for HCV GT1
3
Interim real-world analysis of 2,308 HCV GT1 patients receiving LDV/SOF
Spanish HEPA-C Cohort
Patients N=2,308
Mean age, years 59 (±11)
Mean viral load, log 6.07 (±0.72)
Genotype, n (%) 1 1a 1b
91 (3.9)
672 (29.1) 1526 (66.1)
Fibrosis stage (N=2,258), n (%) F0-1 F2 F3 F4
147 (6.5)
425 (18.8) 480 (21.3)
1206 (53.4)
+RBV, n (%) 631 (44.7)
Treatment duration, n (%) 8 weeks 12 weeks 24 weeks
118 (5.2)
1708 (74.6) 464 (20.3)
Treatment experienced, n (%) 1150 (51.4)
Baseline Demographics
N=1,721
Virologic failure, n (%) 39 (2.2)
W/D or LTFU, n (%) 4 (0.2)
D/C due to AE, n (%) 30 (1.7)
SAEs, n (%) 96 (5.6)
Death, n 10 (0.6)
High effectiveness and safety of LDV/SOF in real-life clinical practice
Cabezas, EASL 2016, Poster LBP511
‡
*1/1 patient (100%) treated w/ RBV achieved SVR
Interim SVR12, N=1,060
32/34 335/ 349
459/ 476
159/ 166
33/ 34
w/o RBV w/ RBV 8 wk* 12 wk 24 wk

SVR Among Those Who Qualified for 8 Week Treatment
4 Cabezas, EASL 2016, Poster LBP511
Spanish HEPA-C Cohort
98 98
0
20
40
60
80
100
8 Weeks 12 Weeks
SVR
4/1
2, %
423/2308 Qualified for 8 Weeks Therapy*
*Qualified = GT1, treatment-naïve, no cirrhosis, HCV RNA ≤ 6 million IU/mL
LDV/SOF 8 week is underused although it provides comparably high SVR12 rates in GT 1, TN, non-cirrhotic patients with baseline HCV RNA
≤ 6 million IU/mL
SVR4/12 Interim Analysis
‡
20% (86/423) received 8 weeks 74% (314/423) received 12 weeks 4% (18/423) received 24 weeks

LDV/SOF in GT1 Patients from Real-World Setting
Buggisch, EASL 2016, Poster SAT-241 5
German Hepatitis C-Registry (DHC-R)
SVR analysis of 1,956 LDV/SOF patients treated for 8 weeks or 12 weeks Baseline Demographics (N=2,509)
Patients
LDV/SOF 8 wk
N=828*
LDV/SOF 12 wk
N=1,320
LDV/SOF+ RBV
12 wk N=358
Male, n (%) 395 (56) 767 (74) 223 (80)
Mean age, years 50.2 53.9 59.1
Age >70 years, % 7.0 9.8 17.9
Treatment naïve, % 91.7 39.4 33
Fibroscan, mean (kPa) 6.5 9.3 21.2
Liver cirrhosis, % 2.5 13.6 69.3
Baseline viral load >6 million, % 2.9 14.1 8.9
HIV coinfection, n (%) 59 (9.2) 121 (11.7) 17 (5.9)
98 99 97
0
20
40
60
80
100
SVR
12, %
631 644
SVR12 (PP)
Under real world conditions, LDV/SOF±RBV for 8 or 12 weeks in GT 1 patients achieved high SVR
1021 1033
271 279
*Including 3 patients who received LDV/SOF+RBV 8 weeks
LDV/SOF 8wk*
LDV/SOF 12wk
LDV/SOF +RBV 12wk
‡

LDV/SOF±RBV for 8, 12, and 24 Weeks in a Large Integrated Health Care System
6 Lai, EASL 2016, Poster SAT-177
Real-World Data (Kaiser Permanente, Northern California)
Real world outcomes in 1,235 HCV GT1 patients
Patients
LDV/SOF 8, 12 or 24
weeks N=852
LDV/SOF+RBV 12 weeks
N=383
Median age, years 60 61
Male, % 62 69
Treatment experienced, % 14 81
Cirrhotic, % 21 49
Baseline Demographics 92 93 95 93
0
20
40
60
80
100
LDV/SOF 8weeks
LDV/SOF 12weeks
LDV/SOF+RBV12 weeks
LDV/SOF 24weeks
%
SVR12 (PP)
High SVR rates (92–95%) in HCV GT 1 patients treated with LDV/SOF-based therapy, which are comparable to results in
published studies
328 347
238 258
403 433
14 15
‡

SVR12 in ION-3 Compared to Real-World Cohorts
7
GT 1: LDV/SOF 8 weeks GT 1: LDV/SOF 8 weeks
SVR
12 (%
)
97 93 98 98 99
92 98 97 97 99
0
20
40
60
80
100
ION-3 VeteransAffairs
DHCR Burman'spharmacy
TRIOCohort
KaiserPermanente
NorthernCalifornia
KaiserPermanenteLos Angeles
GECCO HCVTarget
ifi
631/ 644
119/ 123
271/ 275
150/ 154
155/ 159
127/ 128
238/258
236/ 240
331/338
LDV/SOF 8 weeks ‡
Kowdley. ION-3. NEJM * Backus, VA, Hepatology 2016 ***
Terrault. HCV-TARGET. AASLD 2015 **
Afdhal. TRIO. LBP-519 *** EASL 16 ** Buggisch. IFI. SAT-243 *** Curry. GECCO. AASLD 2015 *** Latt. Kaiser. SAT-227 ** Buggisch. DHC-R. SAT-241 *** Qureshi. Burman’s. SAT-192 ** Lai. Kaiser. SAT-177 ***
*Post hoc analysis ** Per Protocol *** ITT analysis ; patients were primarily treatment-naive non-cirrhotic patients with BL viral load < 6 million IU/mL
Real-World Data across >3,000 patients treated with LDV/SOF 8 weeks achieved high and comparable SVR to LDV/SOF 12 weeks
1138/1227

No effect of PPI use on LDV/SOF SVR in GT1 Patients
Afdhal, EASL 2016, LBP519 8
98 97
0
20
40
60
80
100
SVR
12, %
1495/ 1525
441/ 454
Daily PPI use did not have an effect on SVR in a heterogeneous real-world US population when used according to LDV/SOF US
prescribing information
98 98 99 100 97 97
0
20
40
60
80
100
8 Weeks 12 Weeks 24 Weeks
SVR
12, %
No PPIOn PPI
230/ 234
41/ 41
1024/ 1045
287/ 297
243/ 246
113/ 116
Overall (PP)
No PPI On PPI
By LDV/SOF Duration (PP)
TRIO Real-World Cohort ‡

No effect of PPI use on LDV/SOF SVR in GT1 Patients Predictors of response
9 Afdhal, EASL 2016, LBP519
80% 85% 90% 95% 100%
PPI Drug Name Dexlansproprazole (n=10) Esomeprazole (n=48)
Lansoprazole (n=26) Omeprazole (n=228)
Pantoprazole (n=77)
Rabeprazole (n=5)
Low (n=282)
High (n=172)
Once Daily (n=420) Twice Daily (n=34)
PPI Dose
PPI Frequency
p=0.030
p=0.965
p=0.799
97% N=454
TRIO Real-World Cohort
Daily PPI use did not have an effect on SVR in a heterogeneous real-world US population when used according to US prescribing information
38% (172/454) of the patients who were taking high-dose, and 7% (34/454) were on twice daily PPIs (omeprazole, esomeprazole, or pantoprazole)
‡

SOF+DCV±RBV or LDV/SOF±RBV for 12 weeks in Patients with Advanced HCV Cirrhosis
Cheung, EASL 2016, Oral PS097 10
Event, n (%) All Treated
(n=409) Untreated
(n=261)
Deaths 13 (3.2%) 15 (5.7%)
Decompensation 72 (17.6%) 73 (28.0%)*
New HCC 19 (4.6%) 21 (8.0%)
Sepsis 27 (6.6%) 15 (5.7%)
New OLT 27 (6.6%) 10 (3.8%)
Hospital admissions 133 (32.5%) 83 (31.8%)
MELD worsening >2 94 (23.0%) 99 (37.9%)*
Total adverse outcomes 213 (52.1%) 166 (63.6%)*
English Access Program
329/409
Adverse Events – first 6 months (3 months Rx, 3 months post-Rx)
*P< 0.05 between treated and untreated
180/200 118/172
50 60
100
88
71
82 85
40
91
65
91
0
20
40
60
80
100
G1 G3 others
%
SVR12
SOF-based treatment was associated with short term improvements in clinical outcomes
For patients with decompensated cirrhosis N=409 – Overall SVR = 80.4%
SOF+DCV LDV/SOF
SOF+DCV+RBV LDV/SOF+RBV
‡
2 4
30 34
11 13
136 149
3 5
75 105
2 5
37 57
3 3
9 11
21 23

SOF/DCV±RBV or LDV/SOF±RBV for 12 weeks in Patients with Advanced HCV Cirrhosis
Overall in 329 patients over 15 months: Decompensation 21.3% (n=70) HCC 6.4% (21) Liver transplant 12.2% (40) Deaths 4.9% (16)
Cheung, EASL 2016, Oral PS097 11
English Access Program
-20
-10
0
10
20
Cha
nge
in M
ELD
sco
re
MELD Changes 0 – 6 months
33% of patients
55% of patients
10% of patients
Patients with less severe baseline liver disease (MELD <15 and Child-Pugh A/B) had a higher
frequency of event-free survival at 15 months post-treatment than patients with advanced liver disease
(MELD >15 and Child-Pugh C)
Adverse Events Over Time for Virological Responders
- 15 months
‡
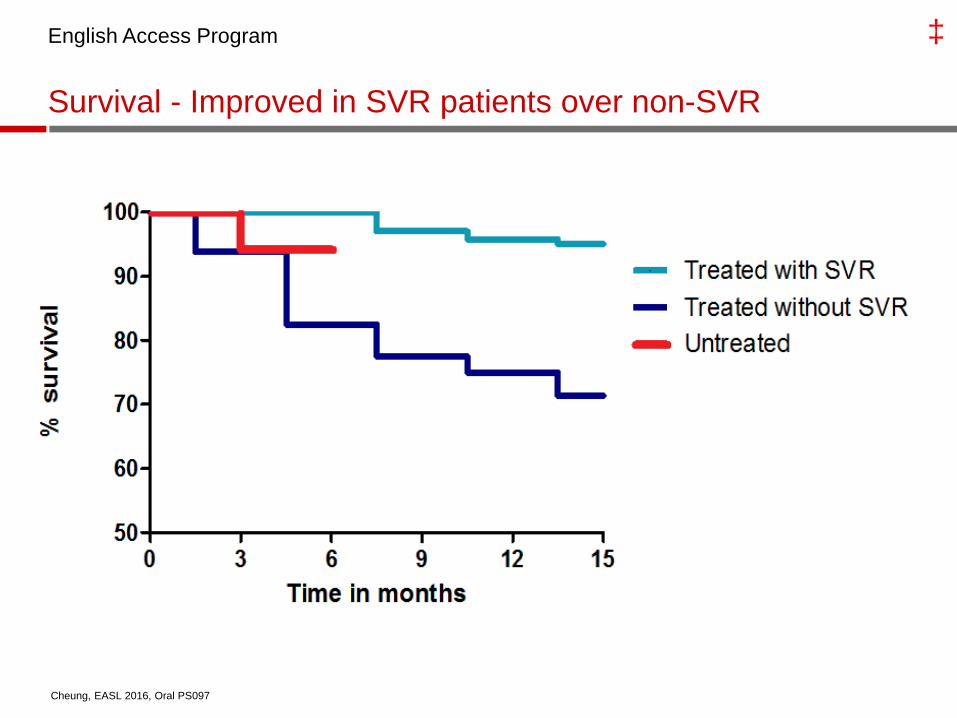
Survival - Improved in SVR patients over non-SVR
English Access Program
Cheung, EASL 2016, Oral PS097
‡

Real-world safety and effectiveness of ombitasvir/paritaprevir/R with dasabuvir and/or ribavirin in the German Hepatitis C Registry
HCV GT1 or GT4, treated with 3D or 2D +/-R
Data collection between Feb 2014 and Dec 2015
1017 patients
Adopted from Hinrichsen H., ICL 2016, GS07
Moderador
Notas de la presentación
Background and Aims: Approximately 400,000 adults in Germany have chronic HCV infection, of whom 63% are infected with HCV genotype (GT) 1 and 3% with GT4. We report the safety and effectiveness of the direct-acting antiviral (DAA) regimen of ombitasvir (OBV), paritaprevir (identified by AbbVie and Enanta, co-dosed with ritonavir [PTV/r]) + dasabuvir (DSV) ± ribavirin (RBV) in patients with GT1 or GT4 infection participating in the real-world German Hepatitis C Registry (DHC-R). Methods: The DHC-R is a non-interventional prospectiv Results: As of September 15, 2015, 902 patients received OBV/PTV/r + DSV ± RBV treatment, with 389 patients having reached end of treatment. Patients included 233 (26%) with GT1a, 544 (60%) with GT1b, 110 (12%) with GT4 infection, respectively, and 15 (2%) with an unspecified, mixed or alternative GT1-subgenotype infection. Patients included 201 (22%) with cirrhosis and 511 (60%) with prior HCV treatment experience. Adverse events (AEs) occurred in 45% of patients (26% of which were patients with cirrhosis), the majority being mild or moderate in severity. The most common AEs were fatigue (21%), pruritus (9%), headache (8%) and insomnia (5%). Serious AEs (SAEs) were reported in 4/418 (1.0%) patients receiving DAAs without RBV and in 11/484 (2.3%) patients receiving DAAs + RBV. No commonality was observed among SAEs, with anemia only occurring in 2 patients. To date, 14 patients have discontinued treatment and of 92 GT1 patients with available follow-up data (mITT/PP), 83 achieved SVR12 with 7 treatment discontinuations and 2 patients experiencing virologic failure, resulting in an SVR rate of 90%. Conclusions: In this large, real-world cohort of HCV GT1 and GT4-infected patients, treatment with OBV/PTV/r + DSV ± RBV was safe and achieved high rates of sustained virologic response. Upcoming SVR12/24 data retrieved in December 2015 will be presented at the meeting and will include data from patients with GT4 infection.

Real-world safety and effectiveness of ombitasvir/paritaprevir/R with dasabuvir and/or ribavirin in the German Hepatitis C Registry
Adopted from Hinrichsen H., ICL 2016, GS07

SAT-156 Safety and efficacy of OBV/PTV/r +
DSV + SOF in DAA-experienced patients with HCV GT1 infection
Chronic HCV GT1 infection (HCV RNA > 10 000 IU/mL)
History of previous DAA treatment failure without discontinuation for reasons other than virologic failure
95% SVR12 with the multi-targeted regimen of OBV/PTV/r + DSV + SOF ± RBV
Irrespective of baseline RAVs, suggesting that resistance testing is not needed
Ombitasvir/Paritaprevir/r, Dasabuvir, and Sofosbuvir Treatment of Patients With HCV Genotype 1-Infecti on Who Failed a Prior Course of DAA Therapy: The QUARTZ-I Study
15 Adapted from Poordad F., ILC 2016, SAT-156
Moderador
Notas de la presentación
Background and Aims: Optimal strategies for retreatment of patients with prior direct-acting antiviral (DAA) treatment failure are still not clear. We investigated the safety and efficacy of ombitasvir/ paritaprevir (identified by AbbVie and Enanta)/ritonavir (OBV/PTV/r) and dasabuvir (DSV) plus sofosbuvir (SOF) with or without ribavirin (RBV) in DAA-experienced patients with HCV genotype 1 (GT1) infection. Methods: Patients with GT1a infection were to receive OBV/PTV/r + DSV + SOF + RBV for 12 (without cirrhosis) or 24 weeks (with cirrhosis). Patients with GT1b infection received 12 weeks of OBV/PTV/r + DSV + SOF. All patients had a history of DAA treatment failure either due to on-treatment breakthrough or relapse. Presence of resistance-associated variants (RAVs) was assessed by deep sequencing. Efficacy was assessed by sustained virologic response at post-treatment week 12 (SVR12), defined as an HCV RNA <15 IU/mL. Safety and efficacy were assessed in all patients receiving at least 1 dose of study drugs. Results: Among 22 GT1 DAA-experienced patients enrolled, 20 had GT1a infection and 6 had compensated cirrhosis. Prior DAA experience included OBV/PTV/r + DSV (n = 14), OBV/PTV/r (n = 2), telaprevir + pegIFN/RBV (n = 2), SOF + pegIFN/RBV (n = 1), SOF + RBV (n = 1), simeprevir + samatasvir (n = 1), and simeprevir + SOF (n = 1). At baseline, 18/22 patients had RAVs in at least 1 of the 3 DAA targets, 6 of whom had RAVs in 2 targets, and 4 of whom had RAVs in all 3 targets. All but 1 patient had HCV RNA <15 IU/mL by treatment week 4. The non-cirrhotic GT1a patient with detectable viral load atweek 4 extended treatment to 24 weeks. SVR12 was achieved in 14/15 (93%) patients treated for 12 weeks, and SVR4 was achieved in 7/7 patients receiving 24 weeks treatment. One GT1a patient with prior telaprevir + pegIFN/RBV experience and no baseline RAVs relapsed at post-treatmentweek 12. Two patients experienced serious adverse events (pneumonia and cellulitis), neither assessed as being related to study drugs. The patient with pneumonia discontinued study drug atweek 10 but still achieved SVR12. Grade 3 laboratory abnormalities were rare. Conclusions: High SVR12 rates were achieved with the multitargeted regimen of OBV/PTV/r + DSV + SOF ± RBV in patients with DAA treatment experience, including those who previously failed the 3-DAA regimen and those with NS5A RAVs. Complete SVR12 data will be presented.

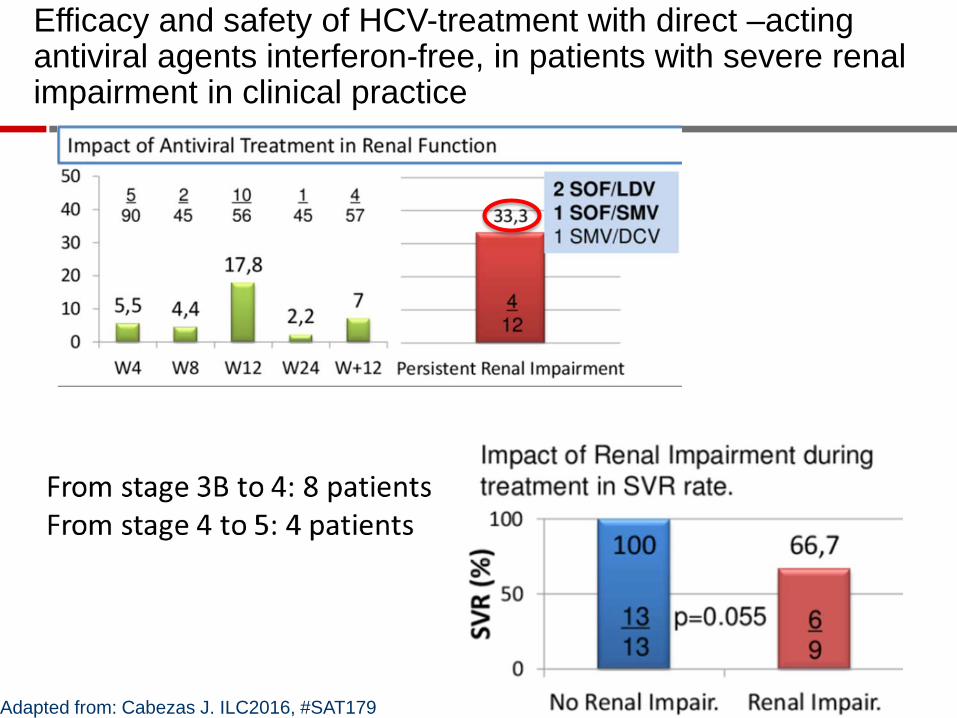
Efficacy and safety of HCV-treatment with direct –acting antiviral agents interferon-free, in patients with severe renal impairment in clinical practice
• 116 patients with advanced CKD from the Spanish Hepa-C registry
• 55 with stage 3B • 21 with stage 4 • 40 with stage 5
Adapted from: Cabezas J. ILC2016, #SAT179
Moderador
Notas de la presentación
EFFICACY AND SAFETY OF HCV-TREATMENT WITH DIRECT-ACTING ANTIVIRAL AGENTS INTERFERON-FREE, IN PATIENTS WITH SEVERE RENAL IMPAIRMENT IN CLINICAL PRACTICE J. Cabezas1,2, M.C. Londono3, S. Llerena1,2, R. Munoz4, C. Baliellas5, M. Buti6, J.M. Pascasio7, F. Saez-Royuela8, J. Garcia-Samaniego9, J. de la Vega10, P. Sanchez-Pobre11, C. Alvarez-Navascues12, J.A. Carrion13, F. Gea14, R.M. Morillas15, M. Fernandez-Bermejo16, A. Castro17, M. Rivero18, J.R. Fernandez19, M. Berenguer20, J.J. Moreno21, D. Rincon22, J.L. Calleja23, J. Crespo1,2. E-mail: [email protected] Background and Aims: Chronic hepatitis C virus infection (CHC) increases the risk of death in patients with chronic kidney disease (CKD) stage 4–5. However, patients with hepatitis C and CKD are considered a special population who are difficult to treat, and information about the efficacy and safety of IFN -free treatment regimens is limited. The aim of this study is to analyze the effectiveness and safety of the free IFN therapy in a large number of patients with CHC and CKD in clinical practice in Spain. Methods: We carried out an observational, ambispective, multicenter study that included 1,343 Hep-C patients from the Spanish Association for the Study of the Liver (AEEH) database. Among those patients, 100 have advanced CKD data: 45 patients are stage 3b(Cl cret 30–44 mL/min),18 are stage 4 (Cl cret 15–30 mL/min) and 37 are stage 5 (Cl cret <15 mL/min, with/without hemodialysis). All patients began treatment before October 2015. Demographic, clinical, virological, pretreatment type, antiviral regimen and renal function variables were analyzed. Results: Patients with CKD were mostly men (74%) with a mean age of 57.6 years. Of the 100 patients, only 33 (33%) had undergone a previous antiviral therapy, compared with 760 (61.3%) patients without CKD (p < 0.001). Genotype distribution: G1 (86%); G3 (5%); G4 (9%). Fibrosis distribution: F0-F1: 22/F2-F3: 28/F4: 50. CKD patients were treated with SOF + SIM + RBV (8), SOF + LDV + RBV (16), SOF + DCV + RBV (16;), SIM + DCV + RBV (48), 3D Abbvie + RBV (9) SOF + RBV (3). The SVR4 (CKD 35/39; 89.7%) and SVR12 (42/47; 89.3%) were similar to patients without CKD (405/449; 90.2%). Dependant on the type of treatment, the SVR12 was: SOF + SIM +/− RBV (7/8; 87.5%), SOF + LDV +/− RBV (2/2, 100%), SOF + DCV +/− RBV (16/16; 100%), SIM + DCV +/− RBV (14/17; 82.3%), 3D Abbvie (1/1; 100%) SOF + RBV (2/3; 66,6%). SVR was lower in patients with cirrhosis (19/22, 86.3%) than in the rest of the cohort (18/18; 100%; p = 0.024). The stage of CKD did not influence the possibility of obtaining an SVR. Similarly, the SVR was independent of the CV [N1], genotype, duration of therapy, and whether or not RBV was used. No significant safety problems occurred, however treatment was discontinued in two patients due to a progression in renal impairment. Conclusions: This multicenter clinical practice study demonstrates the remarkable effectiveness and safety of the combination of different IFN-free regimens in patients with CHC and CKD.

Baseline creatinine clearance is a predictor of worsening renal function while on HCV treatment with sofosbuvir-ledipasvir
Retrospective cohort study – N=91
Baseline eGFR < 60 ml/min was a predictor for worsening of renal function while on LED/SOF
Rosenblatt R., ICL 2016, SAT -262
Moderador
Notas de la presentación
BASELINE CREATININE CLEARANCE IS A PREDICTOR OF WORSENING RENAL FUNCTION WHILE ON HCV TREATMENT WITH SOFOSBUVIR-LEDIPASVIR R. Rosenblatt1, A. Mehta1, M. Wagner1, S. Kumar1. E-mail: [email protected] Background and Aims: Sofosbuvir-ledipasvir (SOF/LDV) is a highly effective and safe hepatitis C virus (HCV) treatment regimen. The aim of this study is to evaluate if patients with pre-existing renal dysfunction are at higher risk for worsening kidney disease during treatment. Methods: This is a retrospective cohort study of patients treated with SOF/LDV. Creatinine and CrCl were collected at baseline, 4 weeks into therapy, end of therapy, 4 weeks after therapy, and 12 weeks after therapy. Abnormal baseline renal function was defined as CrCl <60. Patients with lower CrCl at completion of therapy compared to baseline were considered to have worsening renal function while on HCV treatment. All statistical analysis was performed by SAS 9.4. Results: Ninety patients treated with SOF/LDV had complete data and included in analysis. 15 patients were treated for 8 weeks, 67 patients with 12 weeks, and 8 patients with 24 weeks. 17 patients had abnormal baseline renal function, with 42% having worsening CrCl while on treatment. Univariate analysis demonstrated baseline CrCl < 60 to be significantly associated with worsening renal function on treatment (p = 0.016). Baseline CrCl < 60 remained significantly associated with worsening renal function (p = 0.04) in multivariate logistic regression controlling for age, duration of treatment and presence of advanced fibrosis. Changes in renal function after completion of therapy will also be reported. Conclusions: This was a retrospective study of the effect of SOF/LDV on CrCl during treatment for HCV. Patients with an abnormal baseline CrCl were more likely than those with normal CrCl to have worsening kidney function while on HCV treatment. Based on this data, it worth exercising caution when using SOF/LDV with patients with preexisting renal dysfunction. Future studies are needed with larger patient cohorts to verify this finding. This was a retrospective study of the effect of SOF/LDV on CrCl on patients with normal and abnormal baseline kidney function. The data shows that patients with an abnormal baseline CrCl were more likely than those with normal CrCl to have worsening kidney function, even when controlled for age, treatment duration, and advanced fibrosis. The effect of SOF/LDV on renal function was not discussed or noted on trials conducted prior to the medication’s approval. Based on this data, it worth exercising caution when using SOF/LDV with patients with pre-existing renal dysfunction. Future studies are needed with larger patient cohorts to verify this finding.
Efficacy and safety of HCV-treatment with direct –acting antiviral agents interferon-free, in patients with severe renal impairment in clinical practice
Adapted from: Cabezas J. ILC2016, #SAT179

Observational Spanish study (n=1055) • Across the age groups, anti-infective (67.8%) and CNS (68.8%) drugs were the most used • Anti-acids, anxiolytic and analgesic the most common > 44 y • Comorbidity index (CCI) increases with age • Average number of drugs 2.9 (1.7) • Co-medication with potential DDI: 62% • Contra-indication: 20%
Comorbidities, comedication and potential drug-drug interaction in chronic HCV patients
Therapeutic groups (≥20% overall) A02 Anti-acids, peptic ulcer drugs 55% N02 Analgetics 51% J01 Systemic use antibiotics 47% N05 Psycholeptics – anxiolytics 45% M01 Anti-inflammatory and anti-rheumatic drugs 43%
N06 Psychoanaleptics – anti-depressants 35% C09 Renin-angiotensin system blocking drugs 30% R03 Anti-asthmatics 24% C10 Lipid lowering drugs 22% C03 Diuretics 21% Drug-drug interactions Contraindicated 62% Potential interaction 20%
Adapted from: Sicras A , ILC2016, #SAT-116
Moderador
Notas de la presentación
Background and Aims: With the approval of new direct‐acting antiviral agents (DAA) significant health gains may be obtained; however, there is evidence of different levels of potential for drugdrug interactions (DDI). We investigated the demographics, prevalence of co‐morbidities and co‐medications, and potential for DDIs with licensed DAAs among chronic hepatitis C patients in Spain. Methods: Observational, retrospective study of chronic hepatitis C patients ≥18 years, registered in the electronic prescriptions database, with a minimum of 12 months of active follow-up (≥2 contacts with the healthcare system) in the 2010–2013 period. Comorbidities were analyzed using the International Classification of Primary Care (ICPC-2) and aggregated by means of the Charlson comorbidity index (CCI) and the individual case mix index by bands resource utilization (BUR). Comedication was classified by ATC system. DDI potential with licensed DAA regimens was assessed according to thewebsite: http://www.hep‐druginteractions.org/. The analysis was performed by age group. Results: 1,055 HCV infected patients were enrolled, with the following age distribution: 18–44 (19%), 45–64 (43%), 65–74 (10%) and ≥75 years (18%). Summary results are presented in Table 1. CCI and BUR increased with age (p < 0.001). The most frequent comorbidities by age group were: pain and hypertension in ≥75 years; hypertension and dyslipidemia in 65–74 years; while smoking and dyslipidemiawere most frequent for 64 years or younger. Across age groups, the most used drugswere anti-infectives (67.8%) and CNS drugs (66.8%). Antacids, anxiolytics and analgesics were the most common classes in older than 44 years. The average number of drugs was 2.9 (SD 1.7) patient/year. 61.6% of comedications had potential for DDI and 19.5% had contraindication. Conclusions: HCV infection is associated with a high comorbidity and concomitant medication consumption, which increases with age. Given the high potential for drug-drug interactions, careful selection of HCV treatment is advised.

SIX WEEKS OF SOFOSBUVIR/LEDIPASVIR (SOF/LDV) ARE SUFFICIENT TO TREAT ACUTE HEPATITIS C VIRUS GENOTYPE 1 MONOINFECTION: THE HEPNET ACUTE HCV IV STUDY
Material and Methods: The German HepNet Acute HCV IV Study was designed as a single arm, prospective multicenter pilot study to evaluate the efficacy and safety of treatment with SOF/LDV for 6 weeks without ribavirin in patients with acute genotype 1 HCV monoinfection.
20 patients were included by 10 centers between November 2014 and October 2015. Central HCV RNA testing was performed with the Cobas AmpliPrep/Cobas TaqMan assay version 2.0 (limit of quantification 15 IU/mL).
Detering K, ICL 2016, # LB08
Moderador
Notas de la presentación
Introduction: Early treatment of acute hepatitis C virus (HCV) infection with interferon alfa monotherapy for 12–24weeks is highly effective but is associated with frequent unfavorable side effects. There is no fully published study yet exploring the safety, efficacy and required treatment duration of interferon-free treatment of acute hepatitis C virus monoinfection. Material and Methods: The German HepNet Acute HCV IV Studywas designed as a single arm, prospective multicenter pilot study to evaluate the efficacy and safety of treatment with SOF/LDV for 6 weeks without ribavirin in patients with acute genotype 1 HCV monoinfection. 20 patients were included by 10 centers between November 2014 and October 2015. Central HCV RNA testing was performed with the Cobas AmpliPrep/Cobas TaqMan assay version 2.0 (limit of quantification 15 IU/mL). Results: Most patientswere male (60%) and had a mean age of 46 ± 12 years. Risk factors for HCV infection were sexual transmission in 11 (55%) patients (including 5 men having sex with men), medical procedures/needle stick injury in 5 (25%) patients, drug use in 1 (5%) patient, nail treatment in 1 (5%) patient and unspecified in the remaining 2 (10%) patients. Mean alanine aminotransferase (ALT) and mean bilirubin levels before start of antiviral treatment were 882 U/L and 3.1 mg/dL, respectively. The mean HCV-RNA viral load was 4.9 log10 IU/mL (range 3.3–6.7) at screening; 11 patients were infected HCV genotype 1a and 9 patients with genotype 1b. All 20 patients (100%) completed 6weeks of antiviral treatment and followup week 4, 18 patients completed at least follow-up week 12; the last two patients are still in follow-up, SVR-12 data will be available at time of presentation. Fatigue was the most frequent adverse event reported during antiviral treatment (30%). There was one SAE which was unrelated to the study drugs. At follow-up week 12, 16 (89%) patients had normalized ALT and all patients had normal bilirubin values. HCV RNA response rates at different time points are shown in the table. At follow-up weeks 4 and 12, all patients had undetectable HCV RNA (SVR-4 20/20 (100%), SVR-12 18/18 (100%)). Conclusion: Treatment for 6 weeks with SOF/LDV was safe, well tolerated and highly effective in HIV-negative HCV genotype 1-infected patients with acute hepatitis C. Short-duration treatment of acute hepatitis C may be cost-saving as compared to treatment of chronic hepatitis C and could prevent the spread of HCV in high risk populations.

EUROPEAN RAVS DATABASE: FREQUENCY AND CHARACTERISTICS OF RAVS IN TREATMENT-NAïVE AND DAA-EXPERIENCED PATIENTS
Adapted by Simone Susser, ILC2016, #PS007
Methods: Serum samples of 3305 European HCV infected patients
were collected and population-based sequencing of HCV NS3, NS5A and NS5B genes was performed. RAVs were considered as relevant if they were associated with treatment failure or were shown to confer a >2-fold changed drug susceptibility in comparison to the reference strain. RAVs were analysed in NS3 (positions 36, 43, 54, 55, 56, 80,122, 155, 156,158,168, 170, 175), NS5A (24, 28, 30, 31, 58, 92, 93) and NS5B (159, 282, 321, 316, 368, 411, 414, 448, 553, 554, 556, 558, 559, 561).
Moderador
Notas de la presentación
Background and Aims: Interferon-free combination therapies are the new standard for treatment of chronic hepatitis C virus (HCV) infection. The frequency of HCV RAVs (resistance associated variants) to direct antiviral agents (DAAs) varies between HCV genotypes, but pre-existing RAVs are often associated with virologic treatment failure. In this study frequencies of NS3, NS5A and NS5B RAVs were investigated in treatment-naïve and -experienced patients and consequences for DAA treatment options were evaluated.� �Methods: Serum samples of 3305 European HCV infected patients were collected and population-based sequencing of HCV NS3, NS5A and NS5B genes was performed. RAVs were considered as relevant if they were associated with treatment failure or were shown to confer a >2-fold changed drug susceptibility in comparison to the reference strain. RAVs were analysed in NS3 (positions 36, 43, 54, 55, 56, 80,122, 155, 156,158,168, 170, 175), NS5A (24, 28, 30, 31, 58, 92, 93) and NS5B (159, 282, 321, 316, 368, 411, 414, 448, 553, 554, 556, 558, 559, 561).� �Results: Treatment-naïve and treatment-experienced patients infected with HCV genotype 1a (n = 1417), 1b (n = 1300), 1c-e (n = 5), 2 (n = 49), 3 (n = 389), 4 (n = 119), 5 (n = 7), 6 (n = 1), and 2k/1b (n = 18) were studied. Pre-existing RAVs could be observed in 38% of treatment-naïve patients. The proportion of selected RAVs in telaprevir, boceprevir and PEG/RBV pre-treated patients was 36%, 26%, and 34%, respectively. After failure to SOF/RBV ± PEG no RAVs could be detected. In patients treated with SOF in combination with SMV, DCV, or LDV a much higher incidence of RAVs was observed (64%, 84%, and 60%) only exceeded by PTV/OMB/DSV failure patients who all selected RAVs (100%). Re-/treatment without RAVs with currently approved regimens would be possible in 99% of the naïve patients and in 96% (TVR), 95% (BOC), 83% (SOF/RBV), 90% (SOF/PEG/RBV), 88% (SOF/SMV) 49% (SOF/DCV), 62% (SOF/LDV), 28% (PTV/OMB/DSV), and 98% (PEG/RBV) of pre-treated patients.� �Conclusions: For treatment naïve patients RAVs against NS3, NS5A or NonNuc NS5B inhibitors are observed with moderate frequency (5-57%) and RAVs-free treatment options are available for almost all patients. However, in patients with failure to multiple DAA combination regimens, RAVs were found in 36-100% of patients which may impose restrictions on effective retreatment options with currently approved DAA regimens.

FREQUENCY AND CHARACTERISTICS OF RAVS IN TREATMENT-NAïVE AND DAA-EXPERIENCED PATIENTS
Adapted by Simone Susser, ILC2016, #PS007

Development of hepatocellular carcinoma in HCV cirrhotic patients treated with direct acting antivirals
344 consecutive CPA or CPB cirrhosis – HIV negative – No active alcohol consumption – Treated with different DAA regimens – Followed for 12-24 weeks after end of therapy – Contrast-enhanced US performed at baseline to exclude active HCC. If no definite result, CT-scan and/or MRI was performed to confirm the absence of
active HCC – Contrast-enhanced US performed between 12 and 24 week post-treatment follow-up Suspected HCC was confirmed by CT-scan and/or MRI
Adapted from: Buonfiglioli F. ILC2016, #LB506
Moderador
Notas de la presentación
DEVELOPMENT OF HEPATOCELLULAR CARCINOMA IN HCV CIRRHOTIC PATIENTS TREATED WITH DIRECT ACTING ANTIVIRALS F. Buonfiglioli1, F. Conti1, P. Andreone1, C. Crespi2, F.G. Foschi3, M. Lenzi1, G. Mazzella1, G. Verucchi1, S. Brillanti1. E-mail: [email protected] Introduction: Therapy of chronic hepatitis C with direct-acting antivirals (DAAs) is able to induce a sustained virological response (SVR) in over 85% of patients, even if liver cirrhosis is present. Eradication of HCV infection should prevent the development of major complications, including hepatocellular carcinoma (HCC). At our referral centre, we analysed the whole cohort of patients with liver cirrhosis treated with DAAs in order to evaluate whether HCV eradication affects the development of HCC. Material and Methods: Between March and November 2015, 344 consecutive HIV negative patients with HCV-related Child-Pugh A/B cirrhosis, without active HCC, were treated with DAAs: Sofosbuvir + Simeprevir (34%), 3D combination (22%), SOF + Ribavirin (17%), SOF + Daclatasvir (16%), SOF + Ledipasvir (10%). Ribavirin (RBV) was added at the physician’s discretion according to weight. Occurrence of HCC was assessed by contrast enhanced-ultrasonography and MR/CT-scan during the six-month post-treatment follow-up period. Results: Median age was 63 years (29–85) and 60% were males. The majority (69%) had genotype 1 infection; 55% had experienced previous treatment failure to PegIFN + RBV. History of previous HCC, treated with TACE and/or RFA, without evidence of active neoplastic lesion by MR and/or CT-scan, was present in 59 patients (17%). At 12- week follow-up, SVR was achieved in 89% of patients. Between treatment end and 24-week follow-up, active HCCwas detected in 26 patients (7.6%): median agewas 58 years (48–82), M/F ratiowas 19/7 and Child-Pugh class was A in 19 (73%). A single nodulewas detected in 21 (81%) and multiple nodules in 5 (19%). HCV genotype 1 infection was found in 13 patients (1a/1b: 6/7), genotype 2 in 5, genotype 3 in 4, and genotype 4 in 4. 22/26 (85%) had SVR. HCC developed in 17 (29%) of the 59 patients with a history of previous HCC. Among those without history of HCC, novel HCC was detected in 9 (3.2%). At the time of HCC detection, alphafetoprotein (AFP) was increased (>50 ng/mL) in only 2/26 (8%). Conclusion: In this large retrospective cohort study on cirrhotic patients treated with DAAs, we observed a high rate of HCC recurrence and a standard rate of HCC occurrence in a relatively short follow-up observation. Development of HCC was rarely associated with increase in AFP levels. Cirrhotic patients should be closely monitored after treatment, and the biological significance of our findings deserve further investigations

The ASTRAL Phase 3 Program (N=1408)
24
ASTRAL-1 GT 1, 2, 4‒6
TN, TE NC, CC
ASTRAL-2 GT 2
TN, TE NC, CC
ASTRAL-3 GT 3
TN, TE NC, CC
ASTRAL-4 GT 1‒6 TN, TE
CTP-B Cirrhosis
‡
Primary endpoints – SVR12 – Discontinuations due to AEs
n=624
n=116
Wk 0 Wk 12
n=134
n=132
Wk 0 Wk 12
n=277
n=275
Wk 0 Wk 12
SOF + RBV
SOF/VEL
Wk 24 Wk 0
Wk 12
SOF/VEL
Wk 24
n=90
n=87
n=90
SOF/VEL + RBV
SOF/VEL
SOF/VEL
Placebo
SOF/VEL
SOF+RBV
ASTRAL-5 GT 1‒4 TN, TE NC, CC
HIV/HCV Co-Infection
n=106
Wk 0 Wk 12
SOF/VEL
Feld, AASLD, 2015, LB-2. Feld JJ, et al. N Engl J Med. 2015; Sulkowski, AASLD, 2015, 205. Foster GR, et al. New Engl J Med. 2015.; Mangia, AASLD, 2015, 249. Foster GR, et al. New Engl J Med. 2015, Charlton, AASLD, 2015, LB-13. Curry MP, et al. New Engl J Med.2015. Wyles, EASL 2016, PS104

Integrated Efficacy Analysis of SOF/VEL for 12 Weeks
Agarwal, EASL 2016, Poster SAT-195 25
ASTRAL-1, -2, -3
Retrospective integrated analysis of data from 1,035 SOF/VEL patients in ASTRAL-1, -2, and -3
Baseline Demographics
The ASTRAL-1, -2, and -3 studies enrolled patients with baseline characteristics historically associated with poor response
Patients, n (%) GT1 n=328
GT2 n=238
GT3 n=277
GT4 n=116
GT5 n=35
GT6 n=41
Total N=1035
Cirrhosis 73 (22) 29 (12) 80 (29) 27 (23) 5 (14) 6 (15) 220 (21)
Platelets <100 x 103/µL 21 (6) 4 (2) 25 (9) 8 (7) 1 (3) 3 (7) 62 (6)
Albumin <3.5 mg/dL 6 (2) 1 (<1) 8 (3) 6 (5) 0 0 21 (2)
Fibroscan ≥15 kPa 30 (16) 9 (7) 40 (20) 17 (19) 4 (17) 5 (19) 105 (16)
HCV RNA ≥800,000 IU/mL 255 (78) 186 (78) 191 (69) 74 (64) 26 (74) 31 (76) 763 (74)
Treatment experienced 110 (34) 44 (18) 71 (26) 52 (45) 11 (31) 3 (7) 291 (28)
Black race 25 (8) 19 (8) 3 (1) 14 (12) 0 0 61 (6)
Age ≥65 years 36 (11) 53 (22) 7 (3) 11 (10) 16 (46) 0 123 (12)
BMI ≥35 kg/m2 20 (6) 18 (8) 21 (8) 8 (7) 3 (9) 0 70 (7)
HbA1c ≥6.5% 21 (6) 9 (4) 13 (5) 10 (9) 3 (9) 4 (10) 60 (6)
NS5A RAVs (15% cut off) 50 (15) 146 (61) 31 (11) 69 (59) 3 (9) 19 (46) 318 (31)
‡

Integrated Efficacy: SVR12
Agarwal, EASL 2016, Poster SAT-195 26
ASTRAL-1, -2, -3 SV
R12
(%)
98 99 95 100 97 100
0
20
40
60
80
100 98
Total
1015 1035
323 328
264 277
116 116
34 35
41 41
237 238
GT 1 GT 2 GT 3 GT 4 GT 5 GT 6
‡
2 relapse 2 LTFU 1 D/C 1 D/C
11 relapse 2 D/C 1 death

SOF/VEL+RBV for 24 Weeks for Patients Who Failed Prior SOF/VEL-Containing Regimens
Gane, EASL 2016, Oral PS024 27
Retreatment Study
Interim analysis of safety and efficacy of SOF/VEL + RBV for 24 weeks in patients who had failed prior Phase 2 HCV treatment with SOF/VEL-containing regimens
SOF/VEL + RBV N=69
Mean age, y (range) 57 (31‒74)
Male, n (%) 53 (77)
White, n (%) 61 (88)
Cirrhosis, n (%) 18 (26)
Mean HCV RNA, log10 IU/mL (range) 6.5 (4.4‒7.4)
Genotype, % 1 / 1a / 1b / 2 / 3
54 / 46 / 7 / 20 / 26
Duration of prior treatment
4 or 6 weeks 25 (36)
8 weeks 26 (38)
12 weeks 18 (26)
Mean time to retreatment, days (range) SOF/VEL Phase 2 non-SVR (n=41) SOF/VEL + GS-9857 Phase 2 (LEPTON) non-SVR (n=28)
441 (309-600) 138 (101-172)
Demographics
‡

SOF/VEL+RBV for 24 Weeks for Patients Who Failed Prior SOF/VEL-Containing Regimens
11/13 GT 3 patients with RAVs had Y93H; 9 (82%) achieved SVR12
5 patients had 2 NS5A RAVs; all 5 achieved SVR12
3 patients had NS3 RAVs; all 3 achieved SVR12
28
Retreatment Study
GT 2 (n=13*) GT 1 (n=34) GT 3 (n=16)
100% SVR
96% SVR
100% SVR
100% SVR
38% No RAVs
5/13
62% RAVs 8/13
82% No RAVs
28/34
18% RAVs 6/34
19% No RAVs
3/16
81% RAVs 13/16
100% SVR 77%
SVR
10/13 3/3 8/8 5/5 6/6 27/28
Results: SVR12 by NS5A RAVs
Gane, EASL 2016, Oral PS024
‡
1% deep sequencing cut-off. *1 patient could not be sequenced; 1 patients who withdrew consent was excluded.

Efficacy and safety of elbasvir/grazoprevir in patients with chronic hepatitis C virus infection and inherited blood disorders
Randomized, parallel-group, multisite, placebo-controlled trial – Stratification by cirrhosis (yes/no) and disease status (sickle cell anemia vs ß-
thalassemia vs hemophilia/von Willebrand disease
12 weeks of EBR/GRZ, no ribavirin
Elbasvir/grazoprevir: C-EDGE IBLD
Adapted from: Hezode C. ILC2016, #SAT128
Moderador
Notas de la presentación
Background and Aims: Complications from chronic hepatitis C virus (HCV) infection remain a major cause of morbidity and mortality among individuals with inherited blood disorders (IBLD), including those with haemophilia (HEM), beta thalassemia (BTHAL), von Willebrand disease (VWD) and sickle cell anaemia (SCA). Inability to tolerate ribavirin and frequent comorbidities have limited HCV treatment options in these patients. The efficacy and safety of a oncedaily, fixed-dose combination of EBR 50 mg (NS5A inhibitor) and GZR 100 mg (NS3/4A protease inhibitor) has been demonstrated in a broad population of HCV-infected patients and supported evaluation in the IBLD population. Methods: C-EDGE-IBLD is a double-blind, placebo-controlled study that randomized treatment-naive (TN) and peg-IFN/RBV treatmentexperienced (TE) HCV genotype (GT)1, 4 or 6-infected patients in a 2:1 ratio to either an immediate treatment group (ITG; 12 weeks of EBR/GZR) or deferred treatment group (DTG; 12 weeks of placebo, followed by EBR/GZR). Randomization was stratified according to cirrhosis status and IBLD group, defined as 1)HEM(A or B) or VWD, 2) BTHAL and 3) SCA. The primary endpoints for this study are proportion of patients in the ITG who achieved an SVR12 (HCV RNA <15 IU/mL 12 weeks after study treatment completion) and a comparison of the safety and tolerability of EBR/GZR in the ITG relative to placebo treatment in the DTG. Results: 158 of 159 randomized patients have unblinded treatment allocation (106, ITG; 52, DTG); treatment arm is still blinded for 1 patient. Mean agewas 44 years; 75% male; 18% black; 40% GT1a; 44% GT1b; 11% GT4; 26% cirrhotic; 50% TE; 6% HIV/HCV co-infected; 43% HEM/VWD; 38% BTHAL; 18% SCA). All 106 patients in the ITG and 50 of 52 patients in the DTG completed 12 weeks of treatment. Available HCV RNA results at follow-up week 4 (SVR4) for patients in the ITG (n = 105) are summarized in Table 1. Therewere 3 (2.9%) patients with serious adverse events (SAEs) (1 drug-related, 2 related to IBLD) in the ITG. In the DTG, 1 patient discontinued due to AE, and 1 withdrew consent; 6/52 (11.5%) had SAEs (1 drug-related, 3 related to IBLD). No patient in either arm prematurely discontinued from the trial due to worsening of underlying IBLD. There was 1 hepatic event of clinical interest (ALT >3× baseline and >100 U/L) in each arm. SVR12 results will be presented. Conclusions: Preliminary data indicate that EBR/GZR iswell tolerated and effective in patients with HCV GT1, 4 or 6 with and without cirrhosis with IBLD.

Elbasvir/grazoprevir: C-EDGE IBLD
Adapted from: Hezode C. ILC2016, #SAT128
SVR12 primary efficacy analysis
Factor replacement therapy, blood transfusions, and chelation events

Elbasvir/grazoprevir: C-EDGE CO-STAR
Efficacy of elbasvir/grazoprevir fixed-dose for 12 weeks in HCV-infected persons who inject drugs on opioid agonist therapy
Phase 3, randomized, parallel-group, placebo-controlled, double-blind
Treatment-naïve, GT1, 4, or 6; mixed genotypes of 1, 4, and 6 allowed
On OAT for at least 3 months, and consistently kept at least 80% of scheduled appointments while on OAT
Patients with a positive urine drug screen at baseline were not excluded from the trial
Goal of 20% with cirrhosis; may be co-infected with HIV
Adapted from: Dore GJ. ILC2016, #SAT163
Moderador
Notas de la presentación
Background and Aims: The fixed-dose combination of elbasvir 50 mg, an NS5A inhibitor and grazoprevir 100 mg, an NS3/4 protease inhibitor (EBR/GZR), is a highly effective and well-tolerated all-oral, once-daily regimen in diverse populations of HCV GT1, 4, or 6- infected patients, including PWID on OAT. However, data on HCV reinfection rates after successful HCV treatment are limited, particularly in the interferon-free treatment era. Methods: The double-blind, placebo-controlled CO-STAR study evaluated the efficacy of EBR/GZR for 12 weeks in treatment-naive HCV GT1/4/6-infected patients ± cirrhosis ± HIV receiving OAT. Patients were randomized 2:1 to an immediate treatment group (ITG) or a deferred treatment group. HCV reinfection was evaluated among ITG patients with undetectable HCV RNA at end of treatment (EOT). In patients with viremia recurrence following EOT, population sequencing and phylogenetic analysis of the NS3 and NS5A regions were performed on baseline and post-treatment samples to distinguish relapse from reinfection. Results: 301 patients were randomized, with 201 in the ITG (mean age 47 yrs; 76% male; 15% black; 76% GT1a; 20% cirrhotic, 8% HIV+). Baseline OAT included methadone (81%) and buprenorphine (19%), and 62% had detectable illicit drugs on urine drug screen. A total of 197/200 patients had undetectable HCV RNA at EOT. Post-treatment viremia was detected in 14 patients, with 7 virological relapses, and 7 probable HCV reinfections; 5 through follow-up week (FW)12 and an additional 2 at FW24 (GT1a to 6a, GT1a to 1a, GT1a to GT3a, GT6a to GT1b, GT6a to 6a, GT1a to 1a, GT1b to 1b). Two subjects previously identified as reinfections had subsequent clearance of HCV RNA at FW24. An estimate of reinfection incidence from EOT through FW12 is 10.6 (95%CI: 3.42, 24.6) per 100 person years. Follow-up analysis, including next generation sequencing of baseline/post-treatment viremic samples to determine if any probable reinfection cases were due to relapse of non-dominant baseline variants rather than reinfection, will be presented. The CO-STAR population will be followed for 3 years post-FW24 for ongoing evaluation of reinfection. Conclusions: Several HCV reinfection cases were detected among PWID on OAT following successful EBR/GZR therapy. Further followup is required to determine the natural course of HCV reinfection in the setting of interferon-free HCV treatment, and the impact of viral persistence following reinfection on long-term response rates in this population.

Elbasvir/grazoprevir: C-EDGE CO-STAR
Adapted from: Dore GJ. ILC2016, #SAT163
SVR 12 and 24, mFAS Urine drug screen results.
Incidence of reinfection Immediate treatment group through FW12: • 5 reinfections out of 201 total patients
• 47.4 person-years of follow-up • 10.5 reinfections per 100 person-years (95% CI: 3.4, 24.6)
Immediate treatment group and deferred treatment group from EOT through FW24: • 6 reinfections out of 296 total patients
• 175.3 person years • 3.4 reinfections per 100 person years (95% CI: 1.3, 7.5)

Elbasvir/grazoprevir/sofosbuvir/ribavirin: C-SWIFT retreatment
Treatment of GT-1 infected patients who failed 4, 6, or 8 weeks of EBR/GZR + SOF – Retreatment with 12 weeks of EBR/GRZ plus SOF and ribavirin
Adapted from: Lawitz E. ILC2016, #SAT148
Moderador
Notas de la presentación
Background and Aims: Therapies to retreat patients who have failed prior all-oral, direct-acting antiviral therapies have not been defined. The purpose of this study was to assess a retreatment regimen for subjects who had failed therapy with elbasvir/grazoprevir (EBR/GZR, an NS5A inhibitor + potent NS3/4A protease inhibitor fixed-dose combination) + sofosbuvir (SOF). Methods: Genotype 1-infected patients who relapsed after therapy with EBR/GZR + SOF for 4, 6 or 8weekswere offered retreatment with 12 weeks of EBR/GZR + SOF + ribavirin (RBV). The primary endpoint was the proportion of patients achieving hepatitis C virus RNA < 15 IU/mL 12 weeks after end of treatment (SVR12). Population sequencing was used to detect resistance-associated variants (RAVs) in NS3, NS5A and NS5B. Results: Twenty-five of 29 eligible patients were enrolled: 88% (22/ 25) with G1a infection; 20% (5/25) with cirrhosis; baseline viral load mean 6.6 log10 IU/mL (range: 4.3–7.4 log10 IU/mL). At baseline of retreatment, 80% (20/25) patients had NS5A RAVs, 52% (13/25) had an NS3 RAV and 0/25 had an NS5B RAV. NS5A variants at the following positions occurred in 16–32% of the retreatment population, M28, Q30, L31, H58 and Y93. Nine subjects had both an NS5A and NS3 RAV at baseline. Twenty-three of 25 subjects completed therapy. Two patients were lost to follow-up; one after treatment day 3 and one after treatment week 4, at which time viral load was 363 IU/mL and target not detected, respectively. SVR12 was achieved in 100% of the 23 patients who completed therapy. One patient discontinued RBV only due to pruritus. Rash, fatigue and nauseawere the most frequent adverse events occurring in 8% of patients. Conclusions: 100% SVR12 was achieved with a 12-week regimen of EBR/GZR + SOF + RBV regardless of cirrhosis and high prevalence of RAVs (including two class RAVs). Final SVR24 results will be presented.

Elbasvir/grazoprevir/sofosbuvir/ribavirin: C-SWIFT retreatment
SVR24, overall and by subgroup (mFAS)
Efficacy in patients with or without baseline NS5A R
Adapted from: Lawitz E. ILC2016, #SAT148

High SVR Rates With the Combination of ABT-493 + ABT-530 for 8 Weeks in Non-Cirrhotic Patients with HCV Genotype 1 or 2 Infection
Patients with HCV GT1 (n=34) or GT2 (n=54) infection without cirrhosis received once-daily ABT-493 (300 mg) + ABT-530 (120 mg) for 8 weeks
Adapted from: Poordad F. ILC2016, #SAT157
Moderador
Notas de la presentación
Background and Aims: Hepatitis C virus (HCV) direct-acting antivirals (DAAs), ABT-493 (NS3/4A protease inhibitor identified by AbbVie and Enanta) and ABT-530 (NS5A inhibitor), demonstrated potent pangenotypic antiviral activity in vitro, with a high barrier to resistance and maintenance of activity against common variants. In Part 1 of the SURVEYOR-I and SURVEYOR-II studies, ABT-493 + ABT- 530 for 12 weeks was well tolerated and achieved sustained virologic response (SVR) rates between 97–100% in non-cirrhotic patients with HCV genotype (GT) 1 or 2 infection. In Part 2 of these studies, ABT- 493 + ABT-530was co-administered for a shorter duration of 8weeks. Methods: Non-cirrhotic treatment-naive patients or pegylated interferon/ribavirin treatment-experienced non-responders received once-daily ABT-493 300 mg + ABT-530 120 mg for 8 weeks. HCV RNA <25 IU/mL at post-treatment weeks 4 (SVR4) and 12 (SVR12) and safety are reported. Results: In Part 2 of SURVEYOR-I and -II, 34 patients with GT1 infection (71% GT1a; 68% non-CC IL28B genotype; 15% treatmentexperienced) and 54 patients with GT2 infection (70% GT2b; 59% non-CC IL28B genotype; 13% treatment-experienced) were enrolled, respectively. Mean baseline HCV RNA log10 IU/mL ± standard deviation was 6.3 ± 1.1 for GT1-infected patients and 6.6 ± 0.8 for GT2-infected patients, with 38% and 57% of patients who had baseline levels ≥6 M IU/mL, respectively. SVR12 was achieved by 97% (33/34) of GT1-infected patients. SVR4 was achieved by 98% (53/ 54) of GT2-infected patients (SVR12 data will be available for presentation). There have been no virologic failures to date. One GT1-infected patient discontinued study prematurely atweek 4 (with undetectable HCV RNA) due to a non-DAA related serious adverse event (AE) of abdominal cancer of unknown origin and subsequently died prior to reaching the SVR12 time point. The GT2-infected patient without SVR4 was lost to follow up after week 6, when HCV RNAwas not detected. Therewere no other discontinuations due to AEs. Across both studies, AEswere mostly mild (Grade 1), with the most common AEs being fatigue and headache. Conclusions: The combination of ABT-493 and ABT-530 administered for 8 weeks in non-cirrhotic patients with HCV GT1 or GT2 infectionwaswell tolerated and achieved SVR rates of 97–98%, with no virologic failures to date, regardless of baseline viral load or prior treatment history.

ABT-530 Co-Administrati on for 12 Weeks in HCV Genotype 1-Infected Patients With Cirrhosis (SURVEYOR-I)
GT1-infected patients with compensated
cirrhosis received once-daily
ABT-493 200 mg + ABT-530 120 mg for
12 weeks
Eligible patients were treatment-naïve
or pegylated interferon (pegIFN)/ribavirin (RBV) treatment-experienced with compensated cirrhosis
Adapted from: Gane E, ILC2016, #SAT-135
Moderador
Notas de la presentación
Background and Aims: Next generation direct-acting antivirals (DAAs), including ABT-493, an NS3/4A protease inhibitor (identified by AbbVie and Enanta) and ABT-530, an NS5A inhibitor, have demonstrated potent antiviral activity against all major HCV genotypes (GTs) in vitro, with little or no loss of potency against common resistance-associated variants. Furthermore, the ABT-493/ ABT-530 combination was well-tolerated and achieved high sustained virologic response (SVR) rates in patients with HCV GT1, GT2 and GT3 infection without cirrhosis (SURVEYOR-I/II, Part 1). Here we present data from Part 2 of the SURVEYOR-I study, evaluating the safety and efficacy of ABT-493 and ABT-530 administered for 12 weeks in HCV GT1-infected patients with compensated cirrhosis. Methods: Treatment-naive or pegylated interferon/ribavirin treatment-experienced patients with cirrhosis received ABT-493 200 mg + ABT-530 120 mg once daily for 12 weeks. Cirrhosis was determined by either liver biopsy (Metavir F4), Fibroscan (liver stiffness >14.6 KPa) or serum markers (Fibrotest score ≥0.75 and an APRI > 2). SVR at post-treatment week 12 (SVR12; HCV RNA levels determined using Roche COBAS TaqManR RT-PCR assay [lower limit of detection of 15 IU/mL and lower limit of quantification of 25 IU/ mL]) and safety are reported. Results: A total of 27 patients were enrolled and the population was 74% male, 89% white, 74% GT1a, 85% non-CC IL28B, 26% HCV treatment-experienced, and all reported baseline fibrosis scores of F4. The median (range) HCV RNA log10 IU/mL was 6.7 (5.6–7.3), and 93% had HCV RNA ≥6,000,000 IU/mL at baseline. SVR12was achieved in 26 out of 27 (96%) patients, with one patient experiencing relapse at post-treatmentweek 4. All adverse events (AEs)were deemed mild or moderate in severity, with no patients reporting severe or serious AEs considered related to study drugs. No patients discontinued treatment prematurely due to AEs and the most frequent AEs reported in >10% of patients were fatigue (11%) and headache (11%). No clinically meaningful abnormal liver function or other laboratory results were observed. Conclusions: Treatment with the IFN- and ribavirin-free combination of next generation HCV DAAs, ABT-493 and ABT-530, was welltolerated and achieved high SVR12 rates of 96% following a 12-week treatment regimen in GT1-infected patients with compensated cirrhosis regardless of baseline viral load or prior treatment history.

100% SVR12 With ABT-493 + ABT-530 With or Without Ribavirin in Treatment-Naïve HCV Genotype 3-Infected Patients With Cirrhosis
18 to 70 years of age
HCV GT3 infection
HCV RNA >10 000 IU/mL
Presence of compensated cirrhosis
Key exclusion criteria – Any prior HCV treatment
– Any prior history of hepatic decompensation – HIV co-infection, albumin <LLN, platelet count <90 x 109/L – Herbal supplements and potent P-gp inducers were prohibited
Patients received once-daily ABT-493 300 mg + ABT-530 120 mg for 12 weeks +/- 900 mg RBV
Adapted from: Kwo P. ILC2016#LB01
Moderador
Notas de la presentación
Introduction: Patients with HCV genotype 3 (GT3) infection and cirrhosis remain difficult-to-cure in the current era of direct-acting antiviral (DAA) therapy. ABT-493 (NS3/4A protease inhibitor identified by AbbVie and Enanta) and ABT-530 (NS5A inhibitor) have shown good tolerability and high response rates in GT3-infected patients without cirrhosis. Here,we evaluate the efficacyand safety of ABT-493 + ABT-530 with or without ribavirin (RBV) in GT3-infected patients with cirrhosis. Material and Methods: Treatment-naive GT3-infected patients with compensated cirrhosis were randomised to receive once-daily 300 mg ABT-493 + 120 mg ABT-530, either with or without oncedaily 800 mg RBV for 12 weeks. Efficacy was assessed by sustained virologic response (HCV RNA <25 IU/mL) at post-treatment week 12 (SVR12). Baseline samples were sequenced to assess the presence of resistance-associated variants (RAVs) in NS3 or NS5A. Safety is reported in all patients. Results: Forty-eight patients with cirrhosis were enrolled (65% non- CC IL28B genotype, 65% male, mean age 55, mean viral load 6.3 log10 IU/mL). Baseline sequencing results were available for samples from 46 patients: 7 (15%) had variants in NS3 only, 7 (15%) had variants in NS5A only, and 3 (7%) had variants in both targets. SVR4 was achieved in 24/24 (100%) and 24/24 (100%) of patients following 12 weeks of treatment with and without RBV, respectively. To date, no patient has relapsed after the post-treatmentweek 4 visit. The most common adverse events (AEs) were more frequently observed in the RBV-containing arm than the RBV-free arm (headache 33 vs 13%, fatigue 25 vs 8%, and nausea 21% vs 8%, respectively). Three patients experienced serious AEs, of which 1 event (delusional disorder) was considered related to DAAs and RBV (in a patient with admitted amphetamine and alcohol use) and 1 event (anaemia) was considered related to RBV. There were no discontinuations due to AEs and no patients experienced aminotransferase elevations above baseline. Conclusion: ABT-493 + ABT-530 with or without RBV for 12 weeks was well tolerated in treatment-naive GT3-infected patients with cirrhosis, achieving SVR4 rates of 100% regardless of the presence of baseline NS3 and/or NS5A variants. SVR12 results will be presented. Based on these promising results, the combination of 300 mg ABT- 493 + 120 mg ABT-530 without RBV is now being examined in a larger cohort of GT3-infected patients with cirrhosis, including treatment-experienced patients.


















