
CASE REPORT A Rare Case of Broad Ligament Fibroid: A Case ...
NOT SIMPLY A FIBROID UTERUS: A RARE DIAGNOSTIC DISCOVERY
Resident(s): Bhumin Patel, MD PYG-3
Attending(s): Henry Dalsania, MD, Phillip Zeni, MD, and Jim Machin, MD
Program/Dept(s): Diagnostic & Interventional Radiology

Laparotomy Pelvic
angiogram Repeat
Laparotomy
Repeat Pelvic
Angiogram Pathology
Surgical removal
CHIEF COMPLAINT AND TIMELINE OF EVENTS
31 y/o AAF with complaints of menometrorrhagia and was initially admitted for total abdominal hysterectomy. Initial abdominal laparotomy demonstrated a highly vascular, unresectable pelvic mass
Initial pelvic angio to assess vascularity and Gelfoam of Right iliac supply, non-diagnostic
Repeat laparotomy for biopsy was unsuccessful due to hemorrhage
Repeat pelvic angio for complete vascular embolization

RELEVANT HISTORY
Past Medical History G2P2 female
Past Surgical History Bilateral tubal ligation
Family & Social History Nonsmoker, 1-2 alcoholic drinks per day, single sexual partner
Review of Systems Fatigue
Pelvic pain
Abdominal distention
INITIAL IR INTERVENTION QUESTION
What is the abnormality demonstrated on the CT A/P coronal images ?
A) Multifibroid Uterus
B) Pelvic AVM
C) Enlarged Uterus
D) Hypervascular Pelvic Mass
E) Uncertain
CORRECT!
What is the abnormality demonstrated on the CT A/P coronal images ?
A) Multifibroid Uterus
B) Pelvic AVM
C) Enlarged Uterus
D) Hypervascular pelvic Mass
E) Uncertain
At this point in the diagnostic workup, all possibilities are correct. No tissue diagnosis could be made. Although, an enlarged hypervascular uterus is demonstrated, which is most commonly secondary to leiomyoma.
Return to Case

Sorry, That’s not the best answer.
What is the abnormality demonstrated on the CT A/P coronal images ?
A) Multifibroid Uterus
B) Pelvic AVM
C) Enlarged Uterus
D) Hypervascular pelvic Mass
E) Uncertain
At this point in the diagnostic workup, all possibilities are correct. No tissue diagnosis could be made. Although, an enlarged hypervascular uterus is demonstrated, which is most commonly secondary to leiomyoma.
Return to Case

DIAGNOSTIC DILEMMA
Biopsy could not be completed despite multiple laparotomy attempts secondary to hemorrhage
Multiple imaging modalities were performed to possibly indicate diagnosis Including CT with & without IV contrast, CTA of the pelvis,
MRI/MRA
CT w/ contrast demonstrated a large hypervascular mass concerning fro a high-grade sarcoma, possibly angiosarcoma versus vascular malformation. Of note, hemoperitoneum was also present.

DIAGNOSTIC WORKUP QUESTION
T2 coronal images are presented and the large pelvic mass is obvious. What do the serpiginous T2 hypointense areas demonstrate?
A) Fat
B) Hemorrhage
C) Packed Tumor cells
D) Flow voids

CORRECT!
T2 coronal images are presented and the large pelvic mass is obvious. What do the serpiginous T2 hypointense areas demonstrate?
A) Fat
B) Hemorrhage
C) Packed Tumor cells
D) Flow voids
These hypointense regions are due to flow voids interspersed within the hypervascular pelvic mass.
Return to Case

Sorry, that’s incorrect.
T2 coronal images are presented and the large pelvic mass is obvious. What do the serpiginous T2 hypointense areas demonstrate?
A) Fat
B) Hemorrhage
C) Packed Tumor cells
D) Flow voids
These hypointense regions are due to flow voids interspersed within the hypervascular pelvic mass.
Return to Case

REVIEW OF INTERVENTIONAL DIAGNOSTIC WORKUP
Roberts catheter was used to isolate each illiac artery
Right iliac artery is preferentially demonstrated on these images
Multiple small branches are visualized originating from multiple internal illiac a. branches
DIAGNOSTIC WORKUP QUESTION
Initial pelvic angiogram was performed and gelfoam was used for Right Iliac branch vessel embolization. Why was gelfoam chosen over other embolization techniques?
A) Large Mass
B) Acute Hemorrhage
C) Large Vessel Extravasation
D) Multivascular Supply

CORRECT!
Initial pelvic angiogram was performed and gelfoam was used for Right Iliac branch vessel embolization. Why was gelfoam chosen over other embolization techniques?
A) Large Mass
B) Acute Hemorrhage
C) Large Vessel Extravasation
D) Multivascular Supply
While in emergency situations embolization with coils is preferred if a single vessel injury is identified, multiple arterial malformations/injuries are better managed with gelfoam
Return to Case

Sorry, That’s not the best answer
Initial pelvic angiogram was performed and gelfoam was used for Right Iliac branch vessel embolization. Why was gelfoam chosen over other embolization techniques?
A) Large Mass
B) Acute Hemorrhage
C) Large Vessel Extravasation
D) Multivascular Supply
While in emergency situations embolization with coils is preferred if a single vessel injury is identified, multiple arterial malformations/injuries are better managed with gelfoam
Return to Case
DIAGNOSIS
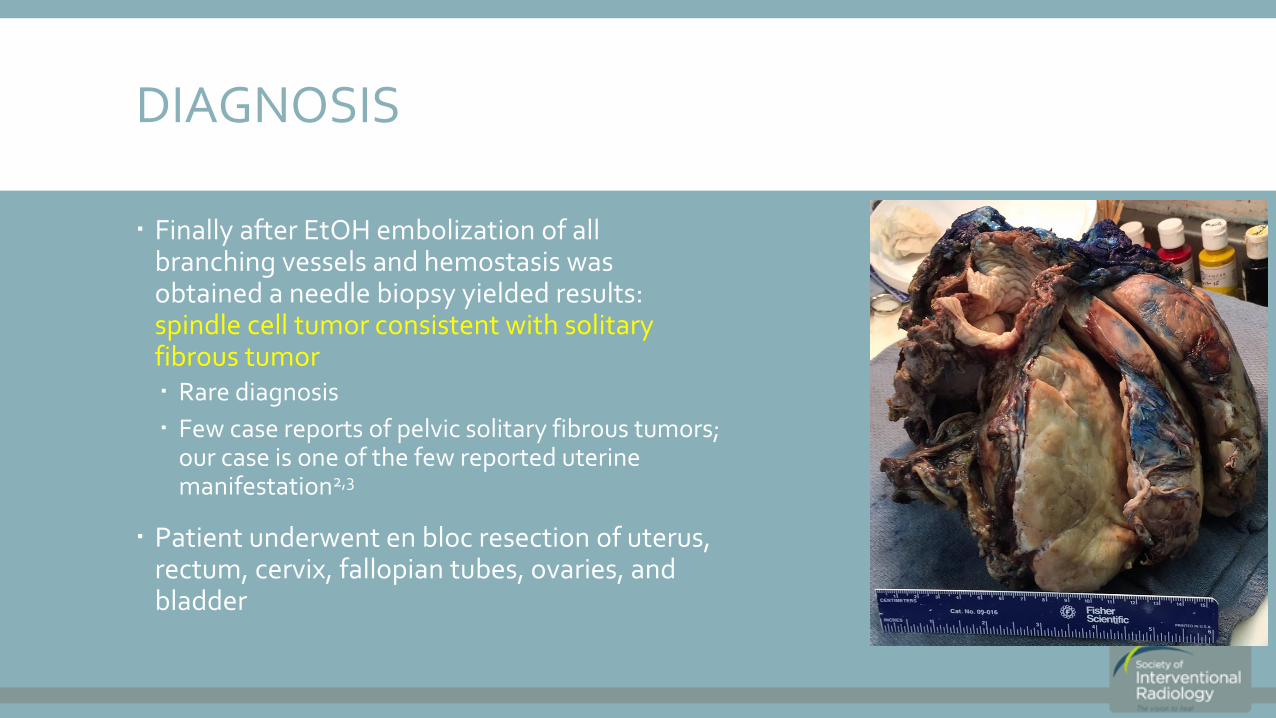
Finally after EtOH embolization of all branching vessels and hemostasis was obtained a needle biopsy yielded results: spindle cell tumor consistent with solitary fibrous tumor Rare diagnosis
Few case reports of pelvic solitary fibrous tumors; our case is one of the few reported uterine manifestation2,3
Patient underwent en bloc resection of uterus, rectum, cervix, fallopian tubes, ovaries, and bladder

SUMMARY & TEACHING POINTS
In summary, our case demonstrates a rare diagnosis, which could have been easily masked for a common finding
A multimodality approach helped to guide our diagnosis and eventual surgical cure for this patient
Angiography contraindications 5
Anaphlaxis to contrast media, uncorrectable coagulopathy, severe renal insufficiency
Pregnancy, active pelvic infection, prior pelvic radiation, connective tissue disease
Gelfoam is a good embolization technique with a multivascular case such as this
Solitary fibrous tumor of the uterus is a rare finding Most have a benign course4 but can cause extensive mass effect and require large
anatomical resection, as in our case
REFERENCES
1. Chen, HY, et al. Aterial Embolization for controlling Life-Threatening Traumatic Pelvic Hemorrhage. Mid Taiwan J. Med. 2009; 14: 16-26.
2. Katsuno, H, et al. Trans-sacral resection of a solitary fibrous tumor in the pelvis: report of a case. Surg. Today. 2011; 41 (11): 1548-51.
3. Kawamura, S, et al. Advanced malingnant solitary fibrous tumor in pelvis responding to radiation therapy. Pathology International. 2007; 57 (11): 213-18.
4. Hasegawa, T, et al. Extrathoracic solitary fibrous tumors: Their histological variability and potentially aggressive behavior. Human Pathology. 1999; 30 (12): 1464-73
5. Spies JB, Spector A, Roth AR et-al. Complications after uterine artery embolization for leiomyomas. Obstet Gynecol. 2002;100 (5 Pt 1): 873-80







![Competency Based Training Programme - NBE · • Formulate a relevant scientific clinical question and transform it into a research ... Multiple pregnancy [MP] ... Fibroid uterus,](https://static.fdocuments.net/doc/165x107/5b9226b909d3f26a278d4d11/competency-based-training-programme-nbe-formulate-a-relevant-scientific.jpg)









