Not for publication or presentation
125
Not for publication or presentation AGENDA CIBMTR WORKING COMMITTEE FOR IMMUNOBIOLOGY Grapevine, TX Friday, February 28, 2014, 12:15 pm – 4:45 pm Co‐Chair: Carlheinz Müller, MD, PhD, German National Bone Marrow Donor Registry Telephone: +49‐731‐1507‐10; Fax: +49‐731‐1507‐51; E‐mail: [email protected] Co‐Chair: Michael Verneris, MD, University of Minnesota Medical Center ‐ Fairview Telephone: 612‐626‐2961; Fax: 612‐626‐3941; E‐mail: [email protected] Co‐Chair: Marcelo Fernandez‐Vina, PhD, Stanford University Telephone: 650‐723‐7968; Fax: 650‐725‐4470; E‐mail: [email protected] Statisticians: Michael Haagenson, MS, CIBMTR Statistical Center Telephone: 612‐884‐8609; Fax: 612‐884‐8661; E‐mail: [email protected] Hailin Wang, MPH, CIBMTR Statistical Center Telephone: 414‐805‐0647; Fax: 414‐805‐0714; E‐mail: [email protected] Tao Wang, PhD, CIBMTR Statistical Center Telephone: 414‐955‐4339; Fax: 414‐955‐6513; E‐mail: [email protected] Co‐Scientific Dir: Stephanie Lee, MD, MPH, Fred Hutchinson Cancer Research Center Telephone: 206‐667‐5160; Fax: 206‐667‐1034; E‐mail: [email protected] Co‐Scientific Dir: Stephen Spellman, MBS, CIBMTR Immunobiology Research Telephone: 612‐617‐8334; Fax: 612‐884‐8677; E‐mail: [email protected] 1. Welcome and introduction (C Müller) 12:15 pm a. Minutes of Immunobiology Working Committee at Tandem 2013 12:20 pm (Attachment 1) b. Newly appointed chair: Katharina Fleischhauer, MD; Essen University Hospital, Telephone: +49‐201‐723‐4582, Fax: +49‐201‐723‐4546, E‐mail: Katharina.Fleischhauer@uk‐essen.de 2. Completed project summary (published or submitted work) 12:25 pm a. R04‐76 Petersdorf EW, Malkki M, Horowitz MM, Spellman SR, Haagenson MD, Wang T. Mapping MHC haplotype effects in unrelated donor hematopoietic cell transplantation. Published. Blood. 2013 Mar 7; 121(10):1896‐1905. b. IB09‐08 Dobbelstein C, Ahn KW, Haagenson M, Hale GA, van Rood JJ, Miklos D, Waller EK, Spellman SR, Fernandez‐Vina M, Ganser A, Aljurf M, Bornhaeuser M, Gupta V, Marino SR, Pollack MS, Reddy V, Eder M, Lee SJ. Birth order and transplant outcome in HLA‐identical sibling stem cell transplantation – an analysis on behalf of the Center for International Blood and Marrow Transplantation (CIBMTR). Published. Biology of Blood & Marrow Transplantation. 2013 May 1; 19(5):741‐745. 1
Transcript of Not for publication or presentation
Not for publication or presentation
A G E N D A CIBMTR WORKING COMMITTEE FOR IMMUNOBIOLOGY Grapevine, TX Friday, February 28, 2014, 12:15 pm – 4:45 pm Co‐Chair: Carlheinz Müller, MD, PhD, German National Bone Marrow Donor Registry Telephone: +49‐731‐1507‐10; Fax: +49‐731‐1507‐51; E‐mail: [email protected] Co‐Chair: Michael Verneris, MD, University of Minnesota Medical Center ‐ Fairview Telephone: 612‐626‐2961; Fax: 612‐626‐3941; E‐mail: [email protected] Co‐Chair: Marcelo Fernandez‐Vina, PhD, Stanford University Telephone: 650‐723‐7968; Fax: 650‐725‐4470; E‐mail: [email protected] Statisticians: Michael Haagenson, MS, CIBMTR Statistical Center Telephone: 612‐884‐8609; Fax: 612‐884‐8661; E‐mail: [email protected] Hailin Wang, MPH, CIBMTR Statistical Center Telephone: 414‐805‐0647; Fax: 414‐805‐0714; E‐mail: [email protected] Tao Wang, PhD, CIBMTR Statistical Center Telephone: 414‐955‐4339; Fax: 414‐955‐6513; E‐mail: [email protected] Co‐Scientific Dir: Stephanie Lee, MD, MPH, Fred Hutchinson Cancer Research Center Telephone: 206‐667‐5160; Fax: 206‐667‐1034; E‐mail: [email protected] Co‐Scientific Dir: Stephen Spellman, MBS, CIBMTR Immunobiology Research Telephone: 612‐617‐8334; Fax: 612‐884‐8677; E‐mail: [email protected] 1. Welcome and introduction (C Müller) 12:15 pm
a. Minutes of Immunobiology Working Committee at Tandem 2013 12:20 pm (Attachment 1)
b. Newly appointed chair: Katharina Fleischhauer, MD; Essen University Hospital, Telephone: +49‐201‐723‐4582, Fax: +49‐201‐723‐4546, E‐mail: Katharina.Fleischhauer@uk‐essen.de
2. Completed project summary (published or submitted work) 12:25 pm a. R04‐76 Petersdorf EW, Malkki M, Horowitz MM, Spellman SR, Haagenson MD, Wang T.
Mapping MHC haplotype effects in unrelated donor hematopoietic cell transplantation. Published. Blood. 2013 Mar 7; 121(10):1896‐1905.
b. IB09‐08 Dobbelstein C, Ahn KW, Haagenson M, Hale GA, van Rood JJ, Miklos D, Waller EK,
Spellman SR, Fernandez‐Vina M, Ganser A, Aljurf M, Bornhaeuser M, Gupta V, Marino SR, Pollack MS, Reddy V, Eder M, Lee SJ. Birth order and transplant outcome in HLA‐identical sibling stem cell transplantation – an analysis on behalf of the Center for International Blood and Marrow Transplantation (CIBMTR). Published. Biology of Blood & Marrow Transplantation. 2013 May 1; 19(5):741‐745.
1

Not for publication or presentation
c. IB11‐03 Hurley CK, Woolfrey A, Wang T, Haagenson M, Umejiego J, Aljurf M, Askar M, Battiwalla M, Dehn J, Horan J, Oudshoorn M, Pidala J, Saber W, Turner V, Lee SJ, Spellman SR. The impact of HLA unidirectional mismatches on the outcome of myeloablative hematopoietic stem cell transplantation with unrelated donors. Published. Blood. 2013 Jun 6; 121(23):4800‐4806.
d. IB05‐03 Shamim Z, Spellman S, Haagenson M, Wang T, Lee SJ, Ryder LP, Müller K. Polymorphism in the interleukin‐7 receptor‐alpha and outcome after allogeneic hematopoietic cell transplantation with matched unrelated donor. Published. Scandinavian Journal of Immunology. 2013 Aug 1; 78(2):214‐220.
e. IB07‐05 Morishima Y, Kawase T, Malkki M, Morishima S, Spellman S, Kashiwase K, Kato S, Cesbron A, Tiercy JM, Senitzer D, Verlardi A, Petersdorf EW. Significance of ethnicity in the risk of acute graft‐versus‐host disease and leukemia relapse after unrelated donor haematopoietic cell transplantation. Published. Biology of Blood & Marrow Transplantation. 2013 Aug 1; 19(8):1197‐1203.
f. R04‐74 Venstrom JM, Pittari G, Gooley TA, Chewning J, Spellman S, Haagenson M, Gallagher MM, Malkki M, Petersdorf E, Dupont B, Hsu KC. HLA‐C dependent prevention of leukemia relapse by donor activating KIR2DS1. Published. N Engl J Med, 2013 August 30, 367(9):805‐816.
g. IB06‐02 Fernández‐Viña MA, Klein JP, Haagenson M, Spellman SR, Anasetti C, Noreen H, Baxter‐Lowe LA, Cano P, Flomenberg N, Confer DL, Horowitz MM, Oudshoorn M, Petersdorf EW, Setterholm M, Champlin R, Lee SJ, de Lima M. Multiple mismatches at the low expression HLA loci DP, DQ, and DRB3/4/5 associate with adverse outcomes in hematopoietic stem cell transplantation. Published. Blood. 2013 May 30; 121(22):4603‐4610.
h. IB11‐04 Pidala J, Wang T, Haagenson M, Spellman SR, Askar M, Battiwalla M, Baxter‐Lowe LA, Bitan M, Fernandez‐Viña M, Gandhi M, Jakubowski AA, Maiers M, Marino SR, Marsh SG, Oudshoorn M, Palmer J, Prasad VK, Reddy V, Ringden O, Saber W, Santarone S, Schultz KR, Setterholm M, Trachtenberg E, Turner EV, Woolfrey AE, Lee SJ, Anasetti C. Amino acid substitution at peptide‐ binding pockets of HLA class I molecules increases risk of severe acute GVHD and mortality. Published, Blood. Epub 2013 Aug 27, DOI:10.1182/blood‐2013‐05‐501510.
i. IB06‐13/R04‐80 Eapen M, Klein JP, Ruggeri A, Spellman S, Lee SJ, Anasetti C, Arcese W, Barker JN, Baxter‐Lowe LA, Brown M, Fernandez‐Vina MA, Freeman J, He W, Paola Iori A, Horowitz MM, Locatelli F, Marino S, Maiers M, Michel G, Sanz GF, Gluckman E, and Rocha V. Impact of allele‐level HLA matching on outcomes after myeloablative single unit umbilical cord blood transplantation for hematologic malignancy. Published. Blood. 2013 October 18; Epub, DOI:10.1182/blood‐2013‐05‐506253
j. IB11‐06 Fernandez‐Vina M, Wang T, Lee S, Haagenson M, Aljurf M, Askar M, Battiwalla M, Baxter‐Lowe LA, Gajewski J, Jakubowski A, Marino S, Oudshoorn M, Marsh S, Petersdorf E, Schultz K, Turner EV, Waller E, Woolfrey A, Umejiego JB, Spellman S, and Setterholm MI. Identification of a Permissible HLA Mismatch in Hematopoietic Stem Cell Transplantation. In press.
2
Not for publication or presentation
k. R02‐40/R03‐63 Cooley S, Weisdorf DJ, Guethlein LA, Klein JP, Wang T, Marsh SGE, Spellman S, Haagenson MD, Saeturn K, Ladner M, Trachtenberg E, Parham P, Miller JS. Recipient HLA‐C1 enhances the clinical advantage of killer‐cell immunoglobulin‐like receptor B haplotype donors in unrelated transplantation for acute myelogenous leukemia. Submitted.
l. IB09‐02 Fleischhauer K, Fernandez‐Viña MA, Wang T, Haagenson M, Battiwalla M, Baxter‐Lowe LA, Ciceri F, Dehn J, Gajewski J, Hale GA, Heemskerk MBA, Marino SR, McCarthy PL, Miklos D, Oudshoorn M, Pollack MS, Reddy V, Senitzer D, Shaw BE, Waller EK, Lee SJ, and Spellman SR. Risk‐associations between HLA‐DPB1 T cell epitope matching and outcome of unrelated hematopoietic cell transplantation are independent from HLA‐DPA1. Submitted.
m. IB11‐02 Sengsayadeth S, Wang T, Lee SJ, Haagenson MD, Spellman S, Fernandez‐Viña MA, Muller CR, Verneris MR, Savani BN, Jagasia M. Cytotoxic T‐Lymphocyte Antigen‐4 (CTLA‐4) Single Nucleotide Polymorphisms Do Not Impact Outcomes after Unrelated Donor Transplant: A Center for International Blood and Marrow Transplant Research Analysis. Submitted.
n. IB11‐05 Gleason MK, Ross JA, Warlick ED, Lund TC, Verneris MR, Wiernik A, Spellman S, Haagenson MD, Lenvik AJ, Litzow MR, Epling‐Burnette PK, Weiner LM, Weisdorf DJ, Vallera DA, Miller JS. CD16xCD33 bispecific killer cell engager (BiKE) activates NK cells from MDS patients against primary MDS and MDSC CD33+ targets. Submitted.
4. Research Repository update and accrual tables (S Spellman) (Attachment 2) 12:25 pm
5. Proposed studies and discussion for Immunobiology Working Committee 12:35 pm a. Voting guidelines (M Verneris) b. PROP 1303‐04/1312‐08 The prognostic impact of somatic mutations and levels of
CXC chemokine ligands on post hematopoietic cell transplantation (HCT) outcomes in patients with myelodysplastic syndromes (MDS) / The prognostic impact of somatic point mutations in patients with myelodysplastic syndromes (MDS) undergoing allogeneic hematopoietic stem cell transplantation (HSCT) (W Saber/ RC Lindsley/BL Ebert) (Attachment 3)
d. PROP 1309‐02 Donor‐Specific anti HLA antibodies, Allele and Antigen level HLA mismatches in the outcomes of Transplantation of Non‐Malignant Diseases with Unrelated Donors (M Fernandez‐Vina/A Woolfrey) (Attachment 4)
e. PROP 1310‐14 Structural/Functional Models of HLA for Data Mining of Permissive Mismatching in Allogeneic Hematopoietic Stem Cell Transplantation (L Gragert) (Attachment 5)
f. PROP 1310‐24 Indirectly recognizable HLA epitopes (PIRCHES): a retrospective validation study on the role of indirect recognition of mismatched HLA in hematopoietic stem‐cell transplantation outcome (E Spierings) (Attachment 6)
g. PROP 1311‐20/1311‐37 Impact of human leukocyte antigen (HLA) haplotypes on outcomes of allogeneic transplantation for B‐cell non‐Hodgkin lymphomas (B‐NHL) / A Retrospective Assessment of Outcomes of Follicular Lymphoma Patients who have Undergone Allogeneic Stem Cell Transplant Based on Human Leukocyte Antigen (HLA) Type (B William/M de Lima/M Fernandez‐Vina/B Hill) (Attachment 7)
3

Not for publication or presentation
h. PROP 1311‐72 Assessing the similarity of the T cell receptor repertoire in allogeneic hematopoietic stem cell recipients with the same single human leukocyte mismatches (EH Meyer) (Attachment 8)
i. PROP 1312‐10 mtDNA haplotypes and unrelated donor transplant outcomes (M Verneris/J Ross) (Attachment 9)
j. Dropped Proposals: PROP 1304‐02 Evaluation of rapid predictive test for response to cytarabine
chemotherapy using Acute Myeloid Leukaemia (AML) patient peripheral blood or bone marrow samples (V Salisbury/E Anderson/MA Smith) ‐ This proposal was dropped because the approach was not feasible. PROP 1312‐12 The impact of HLA‐Class I and Class II mismatch combinations in double mismatched unrelated hematopoietic stem cell transplantations (D Fürst / J Mytilineos / C Müller / H Schrezenmeier) – PROP 1312‐13 The interaction between age‐associated risk and HLA mismatches in HSCT from unrelated donors (D Fürst / J Mytilineos / C Müller) –
k. Proposal voting
6. BREAK – 30 minutes 2:30 pm 7. Studies in progress (Attachment 10) 3:00 pm
HLA GENES – CLASSICAL MATCHING (Chair: C Müller)
3:00 pm
a. IB12‐03 Effect of genetic ancestry matching on HSCT outcomes (A Madbouly/M Maiers/N Majhail) – update
Typing
b. IB12‐01 Impact of unrelated donor HLA‐mismatch in reduced‐intensity conditioning allogeneic hematopoietic stem cell transplantation outcomes (J Koreth) (Attachment 11) – no update
Manuscript preparation
c. IB12‐02 Impact of unrelated donor HLA‐mismatch in myeloablative conditioning allogeneic hematopoietic stem cell transplantation outcomes (J Pidala/C Anasetti) (Attachment 12) – no update
Manuscript preparation
d. IB13‐01 The effect of allele‐level HLA‐matching on survival after umbilical cord blood transplantation for non‐malignant diseases in children. (P Veys/M Eapen) – no update
Protocol development
e. IB13‐02 Effects of HLA Class I Amino Acid Mismatches on Stem Cell Transplant Outcomes (SR Marino/SM Lee/T Karrison/TA Binkowski/A Artz) – no update
Protocol development
f. IB13‐03 Significance of HLA Class I and II Allelic Mismatching Within and Outside of HLA Supertypes among Recipients of Single‐Allele Mismatched Unrelated Allogeneic Hematopoietic Stem Cell Transplantation: A CIBMTR and NMDP Research Study (A Lazaryan/D Weisdorf/M Arora) – no update
Protocol development
g. IB13‐08 Interaction between SNPs and clinical data using predictive modeling on a Bayesian network framework./ Short and long term survival assessment of post HSCT transplantation using predictive modeling on a Bayesian network framework. (R Abdi/G Alterovitz/D McDermott) – no update
Protocol development
4
Not for publication or presentation
h. IB13‐09 The development of Machine Learning based classifiers to define the alloreactivity of HLA mismatches in unrelated donor hematopoietic stem cell transplantation (Y Louzoun) – no update
Protocol development
CYTOKINE/CHEMOKINE
(Chair: M Fernandez‐Vina) No updates.
3:10 pm
NK/KIR
(Chair: M Verneris) 3:10 pm
a. R02‐40/R03‐63 KIR Program Project/NK receptor acquisition (J Miller/E Trachtenberg) ‐ update
Ongoing
b. IB11‐05 KIR genotyping and immune function in MDS patients prior to unrelated donor transplantation (E Warlick/J Miller) (Attachment 13)– no update
Typing
c. IB12‐06 Natural killer cell genomics and outcomes after allogeneic transplantation for lymphoma (V Bachanova/J Miller/D Weisdorf/L Burns) – no update
Analysis
d. IB12‐04 Determining the Effects of HLA‐C KIR Ligand Expression on Outcomes of Unrelated Hematopoietic Stem Cell Transplantation (J Venstrom) – update
Analysis
e. IB13‐05 The Impact Of MHC Class I Chain‐Related Gene A (MICA) Donor‐Recipient Mismatches and MICA‐129 Polymorphism On Unrelated Donor Hematopoietic Stem Cell Transplants (HSCT) For Hematological Malignancies (M Askar/R Sobecks) ‐ update
Analysis
f. IB07‐03 Analysis of Killer Immunoglobulin‐like Receptor(KIR) ligands in reduced intensity conditioning (RIC)allogeneic hematopoietic stem cell transplantation (HSCT) (R Sobecks/K Hsu/M Askar) (Attachment 14) – no update
Analysis
g. IB08‐06 Analysis of Killer Immunoglobulin‐Like Receptor (KIR) ligands in umbilical cord blood transplantation (R Sobecks/V Rocha/M Eapen) – no update
Analysis
h. R04‐74 KIR functional significance (IHWG) (K Hsu/J Venstrom) – no update
Ongoing
i. IB12‐04B Effect of HLA‐C allele matching in the context of recipient HLA‐C‐encoded KIR ligand grouping (C1 or C2) on the outcome of unrelated hematopoietic stem cell transplantation (HSCT) (J Fischer/M Uhrberg) – no update
Analysis
OTHER GENES
(Chair: M Fernandez‐Vina) 3:30 pm
a. R04‐76 Identification of functional SNPs (IHWG) (E Petersdorf) ‐ update
Ongoing
b. IB09‐06/RT09‐04 Genetic polymorphisms and HCT related mortality Re: Pre‐HCT conditioning in matched unrelated donor
Analysis
5

Not for publication or presentation
HCT (T Hahn) – update c. IB12‐05/RT10‐01 Plasma YKL‐40 and CHI3L1 genotype to predict
mortality after allogeneic hematopoietic cell transplantation (HCT) (B Kornblit) – update
Analysis
d. IB08‐08 Genome‐Wide Association in Unrelated Donor Transplant Recipients and Donors: A Pilot Study (R Goyal) – no update
Manuscript preparation
e. IB09‐04 Association of donor and recipient gene polymorphisms of drug metabolisms [GSTP, GSTT, GSTM and UGT (2B17, 2B7, 2B28)] and innate immune response [CD14, TIRAP, and NALPs (1 and 3)] with outcomes after allele matched unrelated hematopoietic stem cell transplantation (V Rocha) – no update
Analysis
f. IB10‐01 Donor and Recipient Telomere Length as Predictors of Outcomes after Hematopoietic Stem Cell Transplant in Patients with Acquired Severe Aplastic Anemia (S Gadalla) (Attachment 15) – no update
Analysis
g. IB10‐03 TLR and HMGB1 gene polymorphisms in unrelated haematopoietic stem cell transplantation (K Müller/B Kornblit) – no update
Manuscript preparation
h. IB10‐04 A validation study of the role of base excision repair pathway as a predictor of outcome after hematopoietic stem cell transplant (B Thyagrajan /M Arora) – no update
Analysis
i. IB13‐04/PROP1302‐01 Discrepancy analysis of microsatellite loci as a proxy measure for ancestral differentiation between donors and recipients: correlation between high scores and poorer overall survival in high resolution matched unrelated donor transplantation (J Harvey/C Steward/ V Rocha) (Attachment 16) – no update
Typing
SENSITIZATION/TOLERANCE
(Chair: M Fernandez‐Vina)3:50 pm
a. R03‐65 HY antigen (D Miklos) (Attachment 17) – no update Manuscript preparationb. IB11‐01 Analysis of the NIMA effect on the outcome of
unrelated PBSC/BM transplantation (G Ehninger/JJ van Rood/ A Schmidt) – no update
Typing
c. IB06‐09 Detection of HLA antibody to the mismatched antigen in single antigen HLA‐mismatched unrelated donor transplants: Is it a predictor of graft‐versus‐host disease outcome? (S Arai/D Miklos) – no update
Manuscript preparation
d. IB11‐07 Effect of Pretransplant Rituximab upon ABO Mismatch Hematopoietic Cell Transplantation (D Miklos/A Logan) – no update
Manuscript preparation
8. Deferred studies pending accrual/funding 3:50 pm
a. IB06‐10 Evaluation of the impact of the exposure to NIMA
during fetal life and breast feeding and to the IPA during pregnancy on the clinical outcome of HSCT from
Deferred
6
Not for publication or presentation
haploidentical family members (J van Rood) – no update b. IB08‐04 Immune response gene polymorphisms in unrelated
donor stem cell transplantation in children (K Müller) – no update
Deferred
c. IB12‐07 Telomeres and incidence of leukemia recurrence and survival after hematopoietic stem cell transplantation (M Eapen) – no update
Pending funding
d. IB13‐06 Role of the complement system in graft‐versus‐host disease (V Afshar‐Kharghan /J Belmont/C Amos)
Pending funding
e. IB13‐07 Impact of donor signal‐regulatory protein alpha (SIRPα) polymorphism on outcome of allogeneic hematopoietic stem cell transplantation (allo‐HSCT) (A Gassas/J Danska/S Rajakumar)
Pending funding
9. Other business 3:55 pm
Handling of overlapping research sample requests
10. Closing remarks (M Fernandez‐Vina) 4:10 pm
7

Not for publication or presentation Attachment 1
MINUTES AND OVERVIEW PLAN CIBMTR WORKING COMMITTEE FOR IMMUNOBIOLOGY Salt Lake City, Utah Saturday, February 16, 2013, 12:15 pm– 4:45 pm Co‐Chair: Carlheinz Müller, MD, PhD, German National Bone Marrow Donor Registry Telephone: +49‐731‐1507‐10; Fax: +49‐731‐1507‐51; E‐mail: [email protected] Co‐Chair: David Miklos, MD, PhD, Stanford University Telephone: 650‐725‐4626; Fax: 650‐724‐6182; E‐mail: [email protected] Co‐Chair: Marcelo Fernandez‐Vina, PhD, Stanford University Telephone: 650‐723‐7968; Fax: 650‐725‐4470; E‐mail: [email protected] Statisticians: Michael Haagenson, MS, CIBMTR Statistical Center Telephone: 612‐884‐8609; Fax: 612‐884‐8661; E‐mail: [email protected] John Klein, PhD, CIBMTR Statistical Center Telephone: 414‐955‐8379; Fax: 414‐955‐6513; E‐mail: [email protected] Tao Wang, PhD, CIBMTR Statistical Center Telephone: 414‐955‐4339; Fax: 414‐955‐6513; E‐mail: [email protected] Co‐Scientific Dir: Stephanie Lee, MD, MPH, Fred Hutchinson Cancer Research Center Telephone: 206‐667‐5160; Fax: 206‐667‐1034; E‐mail: [email protected] Co‐Scientific Dir: Stephen Spellman, MBS, CIBMTR Immunobiology Research Telephone: 612‐617‐8334; Fax: 612‐884‐8677; E‐mail: [email protected] 1. Welcome and introduction
Dr. Marcelo Fernandez‐Vina opened the meeting at 12:20 pm. Minutes of the Immunobiology Working Committee (IBWC) at Tandem 2012 were then approved as written. Dr. David Miklos was thanked as the outgoing Chair, and Dr. Michael Verneris was introduced as the incoming Chair. Dr. Fernandez‐Vina then presented the list of publications and submissions from the past year. The IBWC chairs, scientific directors and statisticians of the Immunobiology working committee then introduced themselves.
2. Completed project summary (published or submitted work)
a. IB07‐02 Marino SR, Lin S, Maiers M, Haagenson M, Spellman S, Klein JP, Binkowski TA, Lee
SJ, van Besien K. Identification by Random Forest method of HLA class I amino acid substitutions associated with lower survival at day 100 in unrelated donor hematopoietic cell transplantation. Published. Bone Marrow Transplantation, 47:217‐226, February 2012.
b. IB07‐06 Fleischhauer K, Shaw B, Gooley T, Malkki M, Bardy P, Bignon JD, Dubois V, Horowitz M, Madrigal JA, Morishima Y, Oudshoorn M, Ringden O, Spellman S, Velardi A, Zino E, Petersdorf E. Effect of T‐cell‐epitope matching at HLA‐DPB1 in recipients of unrelated‐donor
8
Not for publication or presentation Attachment 1
haemopoietic‐cell transplantation: a retrospective study. Published. Lancet Oncology, 13(4):366‐374, April 2012.
c. IB10‐05 Spellman S, Klein JP, Haagenson M, Askar M, Baxter‐Lowe LA, He J, Hsu S, Blasczyk
R, Hurley CK. Scoring HLA Class I Mismatches by HistoCheck Does Not Predict Clinical Outcome in Unrelated Hematopoietic Stem Cell Transplantation. Published. Biol Blood Marrow Transplant, 18(5):739‐746. May 2012.
d. IB07‐09 Pearce KF, Lee SJ, Haagenson M, Petersdorf EW, Norden J, Collin MP, Klein JP,
Spellman SR, Lowerson SA, Davies S, Dickinson AM. Analysis of non‐HLA genomic risk factors in HLA‐matched unrelated donor hematopoietic cell transplantation for chronic myeloid leukemia. Published. Haematologica, 97(7):1014‐1019. July 2012.
e. IB08‐02 Horan J, Wang T, Haagenson M, Spellman SR, Dehn J, Eapen M, Frangoul H, Gupta
V, Hale GA, Hurley CK, Marino S, Oudshoorn M, Reddy V, Shaw P, Lee SJ, Woolfrey A. Evaluation of HLA matching in unrelated hematopoietic stem cell transplantation for non‐malignant disorders. Published. Blood, 120(14):2918‐2924. October 4, 2012.
f. IB06‐11s Rocha V, Spellman S, Zhang MJ, Ruggeri A, Purtill D, Brady C, Baxter‐Lowe LA,
Baudoux E, Bergamaschi P, Chow R, Freed B, Koegler G, Kurtzberg J, Larghero J, Lecchi L, Nagler A, Navarette C, Prasad V, Prasath A, Price T, Pouthier F, Ratanatharathorn V, van Rood JJ, Horowitz MM, Gluckman E, Eapen M. Effect of HLA‐matching recipients to donor non‐inherited maternal antigens on outcomes after mismatched umbilical cord blood transplantation for hematologic malignancies. Published. Biol Blood Marrow Transplant, 18(12):1890‐1896. December 2012.
g. R04‐76s Petersdorf EW, Malkki M, Gooley TA, Spellman S, Haagenson M, Horowitz MM,
Wang T. MHC‐resident variation affects risks after unrelated donor hematopoietic cell transplantation. Published. Science Translational Medicine, 4(144):144ra101, July 25, 2012
h. R04‐74s Venstrom JM, Pittari G, Gooley TA, Chewning J, Spellman S, Haagenson M,
Gallagher MM, Malkki M, Petersdorf E, Dupont B, Hsu KC. HLA‐C dependent prevention of leukemia relapse by donor activating KIR2DS1. Published. N Engl J Med 2012, 367(9):805‐816, August 30, 2012.
i. IB07‐05 Morishima Y, Kawase T, Malkki M, Morishima S, Spellman S, Kashiwase K, Kato S,
Cesbron A, Tiercy JM, Senitzer D, Verlardi A, Petersdorf EW. Significance of ethnicity in the risk of acute graft‐versus‐host disease and leukemia relapse after unrelated donor haematopoietic cell transplantation. Submitted.
j. IB09‐08 Dobbelstein C, Ahn KW, Haagenson M, Hale GA, van Rood JJ, Miklos D, Waller EK,
Spellman SR, Fernandez‐Vina M, Ganser A, Aljurf M, Bornhaeuser M, Gupta V, Marino SR, Pollack MS, Reddy V, Eder M, Lee SJ. Birth order and transplant outcome in HLA‐identical sibling stem cell transplantation – an analysis on behalf of the Center for International Blood and Marrow Transplantation (CIBMTR). In press, Biol Blood Marrow Transplant.
9
Not for publication or presentation Attachment 1
3. Research Repository update and accrual tables
Mr. Steve Spellman discussed the Research Sample Repository. Unrelated donors, cord blood and transplant recipient pre‐transplant and pre‐conditioning samples from NMDP facilitated transplants are being collected as well as pre‐transplant and pre‐conditioning samples from related donors and recipients under the SCTOD. There are 41 sites participating in the related sample collection process, and they are BMTCTN Core and Ancillary centers. Last year, over 13,000 sample aliquots were distributed.
Mr. Spellman also mentioned that post‐transplant samples are being collected as part of BMTCTN 12‐02. CIBMTR has also submitted a NHLBI R24 grant to increase the ability to collect post‐transplant samples for recipients and donors. The grant is going to committee in March. The R24 would be prospectively enrolling patients for the post‐transplant samples. There will be no attempt to collect post‐transplant samples from previously transplanted patients.
Prior to 2002, sample types collected were B‐LCL, PBMC, granulocytes and serum. Starting in the Summer of 2008, 2 ml of ACT‐A plasma were collected. Currently, 10‐20 ml of whole blood and any source of DNA from infused cord blood units are stored as frozen aliquots (‐80° C and Liquid Nitrogen) and whole blood spotted on filter paper.
There are currently over 26,000 pairs overall with over 17,500 being first transplants and most with high resolution HLA typing. For umbilical cord blood transplants, there are 1096 single unit cord blood transplant pairs and 220 double unit cord blood triplets. For related samples, there are 1689 related pairs, 1952 related recipients and 1820 related donors. There are demographics on 1,167 pairs because data submission lags behind sample submission.
All investigators using samples are required to submit the interpreted results of all testing to the CIBMTR/NMDP. This makes the data available to the HCT research community, and it eliminates or reduces duplicative testing to preserve resources and sample inventory. The resulting data are stored in the NMDP Immunobiology database and linked to the sample inventory.
The quality control at the NMDP is very robust. For laboratory testing that is conducted elsewhere, we work with the investigators and labs to be sure their techniques are also robust.
A question was raised about collecting relapse samples which would help the post‐transplant community. Mr. Spellman felt that the CIBMTR would have the infrastructure to capture these samples effectively if the necessary funding were secured.
4. Proposed studies and discussion for Immunobiology Working Committee
10
Not for publication or presentation Attachment 1
a. Voting guidelines – Dr. Carlheinz Müller discussed the voting procedures for the proposals. Using the yellow handout, committee members were told to vote “1” for good and “9” for bad. It is not a ranking system. The committee was asked to base their votes on if the study has an impact; if the study is interesting to the transplant community; if it will lead to clinical decisions; and if it is publishable in a high ranked journal.
b. PROP 0212‐01/0712‐01 Interaction between SNPs and clinical data using predictive modeling on a Bayesian network framework/ Short and long term survival assessment of post HSCT transplantation using predictive modeling on a Bayesian network framework. (R Abdi/G Alterovitz/D McDermott) ‐ Dr. Stephanie Lee presented this proposal in the absence of Dr. Reza Abdi and colleagues. This proposal started off in the Immunobiology working committee because it was initially looking at genetic predictors. The main goal of this study is to identify the major determinants of short and long term survival post hematopoietic stem cell transplantation (HSCT) and to examine their interaction using novel Bayesian Network Analysis. All the relevant clinical information including the characteristics of donor and recipients and transplant risk factors will be considered in the model. Dr. Abdi would like to have a heterogeneous population to evaluate the clinical outcomes. Both an internal and external validation will be performed. The accuracy of the model will be judged by the area under the receiver operator characteristic curve (AUROC), with >70% considered a successful model. Potential problems with Bayesian techniques include overfitting the model and the highly intensive computational requirements to develop the model. The investigators will not be using a multi‐state model; their model will only look at baseline predictors. The Bayesian model will likely be compared to the traditional Cox regression models, although deciding which is better may be difficult. Bayesian techniques have been used in other areas of medicine, but this is new to the BMT transplant community. If the Bayesian model is validated, it would provide more precise risk estimates for individual patients. The investigators would eventually like to include genetic information as potential predictors to refine their model further.
c. PROP 0712‐02/IB13‐01 The Impact Of MHC Class I Chain‐Related Gene A (MICA) Donor‐Recipient Mismatches and MICA‐129 Polymorphism On Unrelated Donor Hematopoietic Stem Cell Transplants (HSCT) For Hematological Malignancies (M Askar/R Sobecks) ‐ Dr. Medhat Askar presented this proposal. He started by reviewing some of the background. It has been found that a higher rate of severe acute GvHD (grade III‐IV) and severe gastrointestinal
11

Not for publication or presentation Attachment 1
acute GvHD was reported in MICA‐mismatched patients regardless of degree of HLA matching by Parmar et al in 2009. At the 2012 BMT Tandem meeting, Dr. Askar reported a significant association between 1‐2 MICA mismatches and severe acute GvHD that was augmented by the presence of HLA‐DPB1. Anderson et al did not observe similar effects when 38 12/12 HLA matched donor/recipient pairs were typed evaluated for MICA mismatch effects. At the Cleveland Clinic, Dr. Askar found that 1‐2 MICA mismatches and no HLA‐DP mismatches had approximately 10% severe acute GvHD, while the group with no MICA mismatches but 1 to 2 HLA‐DP mismatches had almost 20% severe aGvHD, and the group with 1 to 2 MICA mismatches and 1 to 2 HLA‐DP mismatches had almost 40% severe aGvHD. This was presented at last year’s Tandem BMT meetings. Specific aims include: 1) investigating the impact MICA mismatches on clinical outcomes, particularly acute and chronic GvHD of unrelated donor HCT in a homogeneous population of patients diagnosed with ALL, AML or MDS; 2) investigating the interaction between mismatches at the MICA locus with mismatches at other HLA loci particularly low expression loci, such as HLA‐DQB1, DQA1, DPB1, and DPA1 in influencing the above outcomes; and 3) investigating the impact of MICA position 129 polymorphism (as a surrogate marker of NK cell activation through its cognate receptor NKG2D) of HCT recipients and donors on the above clinical outcomes. The proposed study will be a retrospective cohort study of 9/10 HLA‐B mismatches and 10/10 (enriched with B alleles with weaker MICA associations). Donors and recipients will be genotyped for MICA. A question was raised about looking at HLA‐DPA and DPB and incorporating the TCE3 epitope data that Dr. Katharina Fleischhauer and Dr. Bronwen Shaw published. It was also mentioned that approximately 10 percent of cases that are matched for HLA‐B and –C are mismatched for MICA. A question was raised wondering if the 10 percent has been checked in the Cleveland Clinic dataset. The information was based on unrelated patients who have high resolution typing for MICA in that dataset. This study is already funded to genotype 700 pairs. One grant came from the NMDP for retrieval of the samples.
d. PROP 0312‐01 Role of the complement system in graft‐versus‐host disease (V Afshar‐Kharghan /J Belmont/C Amos) ‐ Dr. Amin Alousi presented the proposal in Dr. Afshar‐Kharghan’s absence. The hypothesis of this proposal is that polymorphisms in genes encoding complement proteins may affect the severity of GvHD. There are epidemiologic and murine evidence to support this hypothesis. The investigators will genotype both donor and recipients for complement polymorphisms and correlate the genotypes with the presence or absence of severe GvHD. Genotyping will be conducted in two stages: 1) Discovery stage ‐ 2522 tagged SNP’s in 59 complement genes using 2000 DNA samples (500 patients with severe GvHD, 500 patients with no/mild GVHD and 1000 respective donors); and 2) Replication Stage: Genotype an additional 2000 DNA samples for the most promising 20 SNP’s identified in stage 1. Assuming a severe acute GvHD rate of 25% in patients, a power calculation was conducted under different strengths of linkage disequilibrium.
12
Not for publication or presentation Attachment 1
If the genotype frequencies (GF) are 50%, then the Odds Ratio (OR) to detect a difference is OR=1.27; if GF=40%, then OR=1.29; if GF=30%, then OR=1.35; if GF=20%, then OR=1.41; and if GF=10%, then OR=1.55. This would use banked samples and would be a retrospective study. Dr. Afshar‐Kharghan is applying for NIH funding. He was planning to restrict to well‐matched donor/recipient pairs and needs a discovery set to determine the top 20 SNPs between the donor/recipient pairs. A suggestion was made to make the replication stage blinded.
e. PROP 0712‐03 The development of Machine Learning based classifiers to define the alloreactivity of HLA mismatches in unrelated donor hematopoietic stem cell transplantation (Y Louzoun) Mr. Steve Spellman presented this proposal in Dr. Louzoun’s absence. The proposal is based on the idea that when a cell presenting a foreign MHC class I is introduced to a host T cells, the host T cells may recognize it and react to it for two main reasons: 1) direct TCR‐MHC interaction – The parts of the TCR that directly bind the MHC molecule interact strongly enough with the foreign MHC to induce a T cell response; and 2) peptide epitope repetoire differences – TCR interaction with foreign epitopes, not presented by self‐MHC. Dr. Louzoun will use bioinformatics based estimates of the MHC and TCR interaction and epitope repertoire differences to translate HLA mismatches between donor and recipient to a pair of distances. He will then use these distances to produce machine learning based classifiers for mismatched transplant outcomes. Distance matrices will be used to define a distance between mismatched HLA allele pairs. Then machine learning tools will be applied to evaluate correlation with HCT outcome of mortality, TRM, relapse and acute GvHD III‐IV. The current study population available is N=2464 and would include first unrelated allo HCT for ALL, AML, CML or MDS that are 9/10 with a single HLA‐A, ‐B or ‐C mismatch (allele or antigen). There will be a testing cohort first, and then a blinded validation cohort for this study. It was suggested that this study use a homogeneous population possibly restricting to a T‐cell replete, myeloablative preparative regimen, and calcineurin‐based GvHD prophylaxis. The goal is to find an algorithm that will select better HLA mismatches, and this may be one way that will help. He doesn’t need samples; all he needs is the HLA typing, which is already generated. The committee will need to confirm how homogeneous of data that Dr. Louzoun will want. Another suggestion was to explore cord blood transplants in the future if the algorithm is successful. A suggestion was made to exclude the CD34+ selected and T cell depleted patients.
f. PROP 1112‐16 Effect of HLA‐C allele matching in the context of recipient HLA‐C‐encoded KIR ligand grouping (C1 or C2) on the outcome of unrelated hematopoietic stem cell transplantation (HCT) (J Fischer/M Uhrberg) – Dr. Johannes Fischer presented this proposal. One objective of this proposal is to determine the role of KIR ligands in unrelated HCT since it is a matter of current debate, and common rules for selecting patients according to KIR ligand matching are not well established. The second objective is to investigate the degree of four‐digit HLA‐C allele matching in the context of recipients HLA‐C defined KIR ligand groups (C1/C1, C1/C2, C2/C2), which may help to better define immunogenetic low and high risk constellations associated with differential outcome of HCT. Dr. Fischer has shown in 2007 that for a small cohort that of PBSC cases, C1/C1 cases have
13
Not for publication or presentation Attachment 1
better survival than C1/C2 which is better than C2/C2. The hypotheses of this proposal is that if the donor HLA‐C allele is matched and the recipient KIR ligand is C1/C1, then there is a relapse control; if the donor HLA‐C allele is matched and the recipient KIR ligand is C1/C2 or C2/C2, then there are increased risks of relapse and TRM; if the donor HLA‐C allele is mismatched and the recipient KIR ligand is C1/C1, then there increased risks of relapse and TRM; and if the donor HLA‐C allele is mismatched and the recipient KIR ligand is C1/C2 or C2/C2, then there is a relapse control. Dr. Fischer would like to test this HLA‐C‐based risk assignment on a larger matched unrelated HCT cohort. There would not be any KIR genotyping required for this study. It was suggested to remove the CML cases from this cohort because the relapse rates are low. A question was asked as to how often a mismatch is at HLA‐C, which is about 80% of the time in 7/8 matched cases.
g. PROP 1112‐68 The effect of allele‐level HLA‐matching on survival after umbilical cord blood transplantation for non‐malignant diseases in children. (P Veys/M Eapen) – Dr. Paul Veys presented this study which has the goal of determining the effect of allele‐level HLA‐match on graft failure and survival after umbilical cord blood transplantation for non‐malignant diseases. The primary hypothesis is better HLA‐match (allele‐level HLA‐match and matching at HLA‐C locus) lowers graft failure and improves overall survival. The justification for this study includes a study that looked at adult donor HCT by Horan in Blood 2012, which stated that HLA‐mismatch is associated with lower survival and higher graft failure as well as the determination that after UCB HCT for acute leukemia, HLA‐mismatched transplants are associated with higher TRM while after 8/8 UCB HCT, TRM rates are ≈ 10%. The primary objective would be survival, both 100 day and 1 year. The selection criteria would include first allo‐HCT for non‐malignant diseases of SCID, non‐SCID diseases, IEM, Fanconi anemia and SAA from 2000 through 2010. Eligible patients include a total N of 597 where the disease population includes SAA (13%); Haemoglobinopathies (13%); SCID/non‐SCID (25%); IEM (31%); histiocytic disorders (16%); other (2%). The available HLA matching is currently 8/8 = 15%, 7/8 = 19%, 6/8 = 23%, 5/8 = 24%, 4/8 = 14%, (2/8 or 3/8) = 5%. A suggestion was made to make sure that conditioning regimen is sorted out, since outcomes differ according to regimen. A question was raised wondering if there was data on donor‐specific anti‐HLA antibody. Another question was raised about the level of HLA typing. Much of this data shown was already high resolution typed or is going through retrospective typing. Dr. Mary Eapen was considering removing the severe aplastic anemia (SAA) cases for this study since most are heavily transfused and may have a higher rate of HLA pre‐sensitization.
h. PROP 1112‐27 Impact of donor signal‐regulatory protein alpha (SIRPα) polymorphism on outcome of allogeneic hematopoietic stem cell transplantation (allo‐HCT) (A Gassas/J Danska/S Rajakumar) – Dr. Adam Gassas presented this proposal, which would evaluate the impact of donor SIRPα polymorphisms on HCT outcome. Polymorphisms in SIRPα IgV domain confers differential
binding to human CD47. In murine studies, SIRP is a potent regulator of interactions between human hematopoietic cells and the recipient bone marrow microenvironment and engraftment. CD47 is highly expressed on AML and its interaction with SIRPα on macrophages inhibits phagocytosis.
14
Not for publication or presentation Attachment 1
Objectives of this study are to determine whether there is an association between HCT donor and donor‐recipient SIRP alpha polymorphism and survival in malignant and non‐malignant diseases; and to test for an association between HSCT donor SIRP alpha polymorphism and donor‐recipient association with hematologic malignancy relapse post allo‐HSCT. The current sample size required is 234 pairs. However, the committee felt that the investigators should consider a higher number of pairs for their analysis. The top three causes of death are graft failure, GvHD and infection. The primary outcome will be overall survival. A question was raised about specifying ethnicity during their analysis, but the sample size is too small to adjust for ethnicity. Two other suggestions were to look at engraftment and to limit the study to AML cases.
i. PROP 1212‐04 Effects of HLA Class I Amino Acid Mismatches on Stem Cell Transplant Outcomes (SR Marino/SM Lee/T Karrison/TA Binkowski/A Artz) – Dr. Andrew Artz presented this proposal in Dr. Susana Marino’s absence. This study is a validation study of IB07‐02, which looked at the Random Forest techniques of HLA Class I amino acid mismatches on HSCT outcomes. The aim of this study is to validate the effect of the HLA class I amino acid substitutions and associated alleles on HCT outcomes. The current study would include cases from 2004 through 2011. The population would be matched “8/8” or single HLA Class I “7/8” cases of AML, ALL, CML and MDS patients in early or intermediate stage. This validation study would evaluate the Random Forest Importance Scores that came out during the first analysis and have been divided into “High risk” and “Low risk”. Outcomes would include 1 year overall survival, 1 year disease‐free survival, TRM and GvHD. The C*03:03/C*03:04 mismatch may need to be pulled out due to being potentially being considered “permissive”. The investigators may want to include “8/8” matched, unrelated donor transplants as a reference group for the “Low risk” and “High risk” categories. The audience commented that the analysis should be adjusted for cytogenetic risk. Cytogenetic data for AML is messy and requires a lot of physician time to clean it up. The CIBMTR statisticians would conduct this analysis since it is a straightforward validation of Dr. Marino’s previous findings.
j. Proposal voting
The committee was asked to fill out the voting sheets and turn them in before the break.
5. Studies in progress HLA GENES – CLASSICAL MATCHING IB06‐13/R04‐80s HLA matching in unrelated cord blood transplants (S Rodriguez‐Marino/LA Baxter‐Lowe/V Rocha/M Eapen) –
15

Not for publication or presentation Attachment 1
Dr. Mary Eapen began the second half of the IBWC session with an update to the analysis of whether allele‐level HLA matching in myeloablative, single unit cord blood transplants are associated with outcome. This study uses both CIBMTR and Eurocord data for acute leukemia and MDS patients. Dr. Eapen showed a table comparing the antigen‐level HLA typing results versus the actual allele‐level HLA typing for those cases. It was evident that allele‐level typing discovers at least one additional mismatch over antigen‐level typing in over half of the cases. She also showed that 8/8 allele‐level typed cases have approximately 9% Treatment‐related Mortality (TRM) rates, which is significantly less that 6/8 and 7/8 cases, and 6/8 and 7/8 have significantly less TRM than the 3/8, 4/8 and 5/8 cases. Multivariate results of TRM showed that HLA‐A, ‐C and –DRB1 have a significant higher rate of TRM when there is a single HLA‐locus mismatch. HLA‐B did not show an effect. Dr. Eapen also showed that TRM varies in the 7/8 cord blood population when considering TNC counts ≤ 3 x 107/kg, > 3 to 5 x 107/kg and > 5 x 107/kg. The ≤ 3 x 107/kg group has significantly higher TRM than the other two 7/8 groups, and all three 7/8 groups have significantly higher TRM than the 8/8 group. This is also true for the 6/8 groups when dividing TNC by the same three groups and comparing against the 8/8 group. Conclusions of the analysis are: 1) a single mismatch detected by low resolution or allele‐level HLA typing was associated with higher TRM; 2) the effect of TNC is independent of HLA‐mismatch and a TNC of > 3 x 107/kg is optimal; 3) the data do not support the hypothesis that increasing TNC to 5 x 107/kg or higher can overcome higher TRM seen with HLA disparity; and 4) single mismatch at HLA–B is better tolerated than a single mismatch at HLA–A, ‐C or –DRB1. Dr. Eapen also commented that an overall survival effect was not seen, except in the 3/8 cases. A question was raised about the conclusion that TRM is not as detrimental for HLA‐B mismatches as it is for the other three loci. The concern was the fact that the study may be underpowered in HLA‐B mismatches. Relapse did not show a difference in any of the loci. However, the primary cause of death for these cases is recurrent leukemia. The HLA‐C typing data was determined retrospectively. There are approximately 1200 donor/recipient pairs in this analysis. These cases were confirmatory typed using molecular methods as well as retrospectively typed to get the allele‐level typing described. This study does not have the cases to compare isolated HLA‐A vs. HLA‐B vs. HLA‐C vs. HLA‐DRB1. It can only compare 8/8 vs. 7/8 vs. 6/8 vs. 5/8 vs. 4/8 vs. 3/8. IB11‐03 Evaluation of the impact of allele homozygosity at HLA loci on outcome (C Hurley/A Woolfrey/M Maiers) – Mr. Spellman mentioned that this study was reviewed by Blood and requested a major revision. IB11‐04 Impact of amino acid substitutions at peptide binding pockets of HLA class I molecules on hematopoietic cell transplantation (HCT) outcomes (J Pidala/C Anasetti) – Dr. Joseph Pidala presented his study update, which assessed the impact of amino acid substitutions (AAS) at peptide binding positions 9, 99, 116 and 156 as well as the KIR binding position 77 of the HLA Class I molecule on HSCT outcome and was presented at ASH 2012. This study included all ages, myeloablative and reduced intensity conditioning regimens, PBSC and marrow, AML/ALL/CML/MDS from 1988 to 2009. The multivariate analyses included comparing the presence of these AAS vs. the
16

Not for publication or presentation Attachment 1
absence of these AAS within the 7/8 pairs. (These analyses were restricted to each HLA Class I locus [HLA‐A, ‐B and –C.]) The multivariate analyses also included evaluating the AAS residue combinations with a frequency greater than 30. The single AAS frequencies were shown, with AAS 116 having the largest frequency of the five at N=137 (34% of single frequencies.) The total AAS frequencies show that these specific AAS usually come in combination with at least one other of these specific AAS. The significant multivariate results were then shown. The presence of AAS 116 has a significant effect on Grades III‐IV acute GvHD when mismatching at HLA‐C (RR=1.45, 95% CI=[1.15,1.82], p=0.0016). The presence of AAS 116 also has a potentially significant effect on overall survival when mismatching at HLA‐C (RR=1.20, 95% CI=[1.01, 1.41], p=0.03). The presence of AAS 99 has a significant effect on TRM when mismatching at HLA‐C (RR=1.37, 95% CI=[1.11,1.69], p=0.004). Also shown for AAS 99 in HLA‐C, the presence of the residue pair Cys – Tyr has significantly higher TRM (RR=1.78, 95% CI=[1.27,2.51], p=0.0009), and the change in charge is 0, while the change in hydrophobicity is 3.8 and the Risler score is 83. The multivariate analysis also showed that the presence of AAS 9 has a significant effect on chronic GvHD when mismatching at HLA‐B (RR=2.28, 95% CI=[1.36,3.82], p=0.0018). The analyses could not demonstrate association of AAS at KIR binding position 77 with studied outcomes, nor could they confirm previously reported findings from JMDP. A question was raised as to what the hypothesis of this study was. Dr. Pidala explained that the hypothesis is that these selected AAS would have an effect on outcome, due to their peptide binding nature. Another question was raised about the adjustment to the p‐value for multiple comparisons. Dr. Pidala stated that for most of the analyses, a p<0.01 was considered significant. However, a Bonferroni adjustment was used for the AAS residue analysis, which was p<0.00125. The goal of this study is to be able to state that AAS with relevant peptide binding have impact on outcome. IB11‐06 Evaluation of the impact of potentially non‐immunogenic HLA‐C allele level mismatches (M Fernandez‐Vina/M Setterholm) – Dr. Fernandez‐Vina presented this study update, which evaluates the HLA disparity of HLA‐C alleles and antigens in Caucasians, and compares them to the other 7/8 and 8/8 populations from the Dr. Lee and Dr. Anasetti study (R04‐97). One specific HLA‐C mismatch evaluated was the C*03:03 vs. C*03:04 mismatch. This mismatch is the most common HLA‐C allele mismatch in 69% of the Lee/Anasetti study population. These two alleles differ by one AAS residue (AAS 91). Multivariate analysis evaluating the C*03:03/C*03:04 mismatch against other 7/8 groups and the 8/8 group showed no significant difference in overall survival between the C*03:03/C*03:04 mismatch group and the 8/8 group. The 7/8 HLA‐C allele mismatch group (outside of the C*03:03/C*03:04 mismatch group) was borderline significantly worse than the 8/8 group, but that may have been due to lack of power. The 7/8 HLA‐C antigen mismatch group and the 7/8 HLA‐other mismatches group were both significantly worse than the 8/8 group, when considering overall survival. This held true for Disease‐free Survival (DFS) as well. Similar results were found in Grades III‐IV acute GvHD, except that the HLA‐C allele mismatch group (outside of the C*03:03/C*03:04 mismatch group) was not significantly different than the 8/8 group and appears different than the other 7/8 groups. No associations with relapse or cGvHD in any of the 7/8 groups compared with 8/8 were found. Analyses of 7/8 transplants other than those including C*03:03/C*03:04 and different 6/8 transplants were done, and 6/8 transplants including C*03:03/C*03:04 paired with other mismatches did not show statistically significant differences; however hazard ratios (HR) were higher than 1.10 in each outcome. Dr. Fernandez‐Vina would like to caution against concluding that
17

Not for publication or presentation Attachment 1
the mismatch C*03:03/C*03:04 is not relevant in transplantation, although it does appear that the C*03:03/C*03:04 mismatch could be considered a permissible mismatch, but it is not equivalent to an 8/8 match. The 7/8 groups are small, but most are HLA‐C mismatches. This study was done on Caucasians only. IB12‐03 Effect of genetic ancestry matching on HCT outcomes (A Madbouly/M Maiers/N Majhail)– Dr. Abeer Madbouly presented this update, which looks at genetic ancestry where race and ethnicity are defined genetically. One objective is to study the effect of differences in genetic ancestry, as detected by ancestry informative Single Nucleotide Polymorphisms (SNPs) for HLA matched unrelated donors and recipients, on HCT transplantation outcomes. Another objective is to evaluate the correlation of self‐identified race with information derived from genetic ancestry typing. The study started with a pilot study of 300 HLA‐matched donor/recipient pairs, and 578 samples have been typed so far, leading to 280 pairs typed for the pilot study. The current analysis is focused on development of a genetic ancestry match distance model and evaluation of self‐identified race/ethnicity (SIRE) concordance with genetic defined race. A question was raised about analyzing the self identified race and ethnicity, wondering if that analysis has been performed before. Mr. Spellman mentioned the Baker study a couple of years ago showing that African Americans had worse outcome. This analysis is different because it uses genetic information, not self‐reported race, to look for correlation with outcomes. IB06‐02 Mismatching for low expression HLA loci in matched unrelated donor transplants (M Fernandez‐Vina) – This study has been submitted to Blood. IB09‐02 Non‐permissive HLA‐DPB1 disparities based on T cell alloreactivity (K Fleischhauer) – No update was given. IB12‐01 Impact of unrelated donor HLA‐mismatch in reduced‐intensity conditioning allogeneic hematopoietic stem cell transplantation outcomes (J Koreth) – No update was given. IB12‐02 Impact of unrelated donor HLA‐mismatch in myeloablative conditioning allogeneic hematopoietic stem cell transplantation outcomes (J Pidala/C Anasetti) – No update was given.
CYTOKINE/CHEMOKINE
18
Not for publication or presentation Attachment 1
IB08‐04s Immune response gene polymorphisms in unrelated donor stem cell transplantation in children (K Müller) – No update was given.
NK/KIR
R02‐40s/R03‐63s KIR Program Project/NK receptor acquisition (J Miller/E Trachtenberg/S Cooley)– Dr. Sarah Cooley presented the update of this ongoing study. Previous publications have specified the importance of a KIR B/x haplotype in the donor, especially with AML patients. Data that will soon be published showed no interaction between the KIR B/x haplotype and Bw4/Bw6. It also shows that all KIR B/x haplotype defining genes contribute to benefit for the patient. Dr. Cooley showed that leukemia‐free survival (LFS) is lower for C2/C2 patients when the donor KIR haplotype is KIR B/x, whether you are looking at all patients or just the ones that are less than 10/10, although it doesn’t reach significance in the less than 10/10 group. It has also been shown that B/x with C1/x is associated with less TRM in HLA Matched HSCT (C1/C2 same in Donor/Recipient pair.) The NK P01 Program Project grant has done two separate analyses on data provided by the NMDP/CIBMTR; the first cohort was 1920 cases with a mixture of AML, ALL, CML and MDS; and the second cohort was 660 AML cases only. All of these cases included donor/recipient paired samples. There are also new cohorts of 1326 AML and 603 ALL cases that have been KIR genotyped, either by Dr. Elizabeth Trachtenberg’s laboratory or by the NMDP consortium laboratories. Dr. Cooley then provided an update on the KIR donor selection trial. There are currently 139 patients enrolled with 41 transplanted. Sixteen centers are actively participating with Washington University (N=57), Ohio (N=12) and Mayo Scottsdale (N=10) the top three accruing transplant centers. She discussed barriers to accrual and following the study procedures. She clarified that a patient may start the donor search prior to consent. IB11‐05s KIR genotyping and immune function in MDS patients prior to unrelated donor transplantation (E Warlick/J Miller) – Dr. Jeffrey Miller presented the update for this study, in the absence of Dr. Erica Warlick. The hypothesis of this study is that progression of MDS is a result of clone‐induced immune dysfunction. The group wants to study CD33 expression, which is a committed myeloid lineage marker. It is found on myeloid leukemia blasts and mature monocytes. They are not expressed on normal pluripotent HSCs, but they have high expression in AML and MDS. Another marker that they would like to evaluate is CD16 because natural killer (NK) cells express activating Fc receptor CD16, and they potently induce resting NK cell degranulation and cytokine secretion via ADCC. The CD16‐directed recombinant reagent with CD33 (called “Bispecific Killer Cell Engager (BiKE)”) will be evaluated. It lacks an Fc domain. It has both effector and target cell specificity. It involves a fusion of single chain variable fragment (scFv) to a specific tumor associated antigen, and it is small in size (~60kD). The hypothesis is that CD16/CD33 BiKEs enhance NK cell targeting of CD33+ cells in patients with MDS. It
19

Not for publication or presentation Attachment 1
has been shown that CD16/CD33 BiKE activates PBNK Cells from MDS patients and targets CD33+ cells. This group will continue with the pilot study of 100 samples where the recipient had MDS. They will correlate function with the clinical data, and the plan is to get more samples after completion of the pilot study and summary review by the Immunobiology working committee. There will be a request of approximately 971 MDS cases with special plans for pediatric MDS. The goal is to get a MDS P01 or SPORE grant in 2014. The current funding is coming from the University of Minnesota and the Mayo Clinic. IB07‐03 Analysis of Killer Immunoglobulin‐like Receptor (KIR) ligands in reduced intensity conditioning (RIC) allogeneic hematopoietic stem cell transplantation (HSCT) (R Sobecks/K Hsu/M Askar) – No update was given. IB12‐04 Determining the Effects of HLA‐C KIR Ligand Expression on Outcomes of Unrelated Hematopoietic Stem Cell Transplantation (J Venstrom) –
Dr. Jeffrey Venstrom presented his study update. The background for this study is that HLA‐C2/C2 is associated with higher AML relapse, and the hypothesis is that C2/C2 AML patients have high HLA‐C2 expression, inducing broad donor NK cell inhibition and less GvL. The study design is based on known and predicted linkage disequilibrium between HLA‐C alleles and the miR148 binding site. This study looks at HLA‐C expression as low/low vs. low/high vs. high/high, based on the alleles at HLA‐C. A second hypothesis is that the presence of a miR148 binding site is a marker of HLA‐C2 expression. The current data set is 8497 patients with high resolution HLA typing, consisting of 3148 AML as well as ALL, CML and MDS patients from 1988‐2009. There are 2421 “7/8” cases where 1072 are HLA‐C mismatches, and 758 “6/8” cases. Preliminary results show that HLA‐C2 ligands are enriched with high expression HLA‐C alleles, based on linkage disequilibrium with the miR148 binding site. Low expression alleles (N=25) in C2/C2 patients are associated with a 10% lower risk of relapse in matched HSCT. No donor KIR genotyping will be performed. HLA‐C2/C2 AML patients with low expressing alleles may uniquely benefit from an HLA‐C mismatched HSCT, but again, this preliminary information is from small numbers and no donor KIR genotyping. This data was just looking at the HLA alleles, not genotypic frequencies. This is hypothesis generating. There may be a chance to add patients to the cohort. A question was raised about considering different conditioning regimens. R04‐74s KIR functional significance (IHWG) (K Hsu/J Venstrom) – No update was given. IB08‐06 Analysis of Killer Immunoglobulin‐Like Receptor (KIR) ligands in umbilical cord blood transplantation (R Sobecks/V Rocha/M Eapen) – No update was given.
20
Not for publication or presentation Attachment 1
IB12‐06s Natural killer cell genomics and outcomes after allogeneic transplantation for lymphoma (V Bachanova/J Miller/D Weisdorf/L Burns) – No update was given.
OTHER GENES R04‐76s Identification of functional SNPs (IHWG) (E Petersdorf) – Dr. Effie Petersdorf presented this ongoing study update. The goals of this study were to identify novel MHC region variants that affect transplant outcome. The methods include retrospective mapping of the MHC using Illumina SNP mapping panel, sequencing and haplotypes. The study population consists of HLA matched (N = 5147), HLA‐mismatched (N = 4597) and cord blood transplants (N = 1007), which includes clinical outcome data as well as data acquired from typing samples. An analysis of single locus mismatched (9/10) transplants for HLA‐A, ‐B, ‐C, ‐DRB1 and –DQB1has shown that twelve SNPs are of significant interest. Each SNP affected one endpoint, but not multiple endpoints. Three models were evaluated: the donor genotype model, the patient genotype model and the donor/recipient mismatch model. Each SNP position only affected one of the three models. Dr. Petersdorf presented a slide showing the impact of the total number of unfavorable SNPs on transplant outcome. The outcomes evaluated were Grades III‐IV acute GvHD, chronic GvHD, relapse, TRM and survival. As the number of bad SNPs increase from 1 to 7 or more, HR mortality for mortality increases 1.28, 1.43, 1.68, 1.86, 1.63 and 2.40. It was also shown that HLA and SNPs affect outcome independently. Relative to HLA‐C antigen mismatches, all other mismatches may have similar risks with the exception of DQB1 which, as a group, is associated with lower III‐IV aGVHD and TRM, and better survival. For future studies, validation is in progress for unrelated donor transplants and CBT. Fine mapping is also in progress for unrelated donor transplants and CBT. They hope to determine the role of SNPs in the definition of permissible HLA mismatches and to determine haplotype riskiness and catalogue haplotypes based on their SNP content. They also would like to prospectively integrate SNP genotyping and assessment in patients and donors. IB10‐01 Donor and Recipient Telomere Length as Predictors of Outcomes after Hematopoietic Stem Cell Transplant in Patients with Acquired Severe Aplastic Anemia (S Gadalla/S Savage) – Dr. Sharon Savage presented this study update in Dr. Shahinaz Gadalla’s absence. The specific aims of this study is to compare pre‐HSCT telomere length in HSCT recipients with SAA with age‐matched controls and patients with dyskeratosis congenital, to assess the relationships between pre‐HSCT telomere length and post‐HSCT outcomes (e. g. ‐ survival, count recovery, GVHD, post‐HSCT malignancy, organ fibrosis), and to identify factors that modify the association between recipient and/or donor telomere length, and post‐HSCT outcomes in patients with SAA. This group received 344 SAA cases from the NMDP out of 381 NMDP donor samples. They also added in thirty mutation positive cases from NCI, fifty DC relatives that are mutation negative and fifty NIH children free of disease. They adjusted for age because telomere length changes by age. The analytic plan is to first look at SAA telomere length (TL) vs. all controls, then SAA vs. DC, then SAA TL vs. outcome, and finally genetic factors. They should have some exciting analysis in about six months. The outcomes have not been looked at yet.
21
Not for publication or presentation Attachment 1
IB12‐05/RT10‐01 Plasma YKL‐40 and CHI3L1 genotype to predict mortality after allogeneic hematopoietic cell transplantation (HCT) (B Kornblit) – Mr. Spellman gave an update on this study in Dr. Brian Kornblit’s absence. Dr. Kornblit is looking at YKL‐40 which is an inflammatory marker. He is evaluating donors and recipients pre‐transplant. This study is in combination with Dr. Artz study in the Regimen Related Toxicity (RRT) working committee. Once Dr. Artz has finished with his testing, the analysis will be completed, and the results will be distributed. IB08‐08 Genome‐Wide Association in Unrelated Donor Transplant Recipients and Donors: A Pilot Study (R Goyal) – No update was given. IB09‐04s Association of donor and recipient gene polymorphisms of drug metabolisms [GSTP, GSTT, GSTM and UGT (2B17, 2B7, 2B28)] and innate immune response [CD14, TIRAP, and NALPs (1 and 3)] with outcomes after allele matched unrelated hematopoietic stem cell transplantation (V Rocha) – No update was given. IB09‐06s/RT09‐04s Genetic polymorphisms and HCT related mortality Re: Pre‐HCT conditioning in matched unrelated donor HCT (T Hahn) – No update was given. IB10‐03 TLR and HMGB1 gene polymorphisms in unrelated haematopoietic stem cell transplantation (K Müller/B Kornblit) – No update was given. IB10‐04s A validation study of the role of base excision repair pathway as a predictor of outcome after hematopoietic stem cell transplant (B Thyagrajan /M Arora) – No update was given. IB11‐02s Impact of CTLA4 single nucleotide polymorphisms on outcome after unrelated donor transplant (M Jagasia/W Clark/B Savani/S Sengsayadeth) – No update was given.
SENSITIZATION/TOLERANCE IB11‐01 Analysis of the NIMA effect on the outcome of unrelated PBSC/BM transplantation (G Ehninger/JJ van Rood/ A Schmidt) – Mr. Spellman presented this study update in Dr. Gerhard Ehninger’s absence. The background and rationale of this study is that HLA mismatches to non‐inherited maternal antigen (NIMA) mismatches appear to be better tolerated. This was shown by Dr. Jon van Rood in haplo‐identical
22

Not for publication or presentation Attachment 1
transplants in 2001 as well as in cord blood by Dr. van Rood in 2009 and by Dr. Vanderson Rocha in 2012. This study will investigate the impact of NIMA mismatches in adult URD HSCT. The study design includes 9/10 matched URD HSCT utilizing a DKMS donor from the CIBMTR or EBMT. DKMS contacts the donor and mother to obtain a maternal DNA sample, and they will perform HLA typing on maternal samples and assign NIMA matches and mismatches. So far, from the pilot study 150 donors were contacted and 80 were enrolled. Of these, only five were NIMA matches. From CIBMTR, 368 donors were contacted, of which 173 were enrolled, and only eight NIMA matches were found. From EBMT, 786 donors were contacted, of which 368 were enrolled, and fifteen were NIMA matches. This leaves the total of 28 NIMA matches to evaluate for this study, and an approximate 4.5% NIMA match rate. A feasibility analysis will have to be performed. IB11‐07 Effect of Pretransplant Rituximab upon ABO Mismatch Hematopoietic Cell Transplantation (D Miklos/A Logan) – Dr. Aaron Logan presented this study update. Previous analyses at Stanford showed that recipients of ABO minor mismatched grafts (i.e. ‐ donor has anti‐recipient ABO B cells and antibodies) experienced decreased OS and increased Non‐Relapse Mortality (NRM). Survival impairment with ABO minor mismatches was observed in patients with leukemias but not with lymphomas. The group then hypothesized that pre‐HCT Rituximab in lymphoma patients may ameliorate the ABO minor mismatch effect by in vivo depletion of adoptively transferred anti‐recipient ABO B cells. They evaluated a data set from a previous study of 435 B‐cell NHL cases that were PBSC grafts led by Dr. Ratanatharathorn, which did not evaluate ABO mismatch in the analysis. The worse outcome appeared to be true for ABO minor mismatches in this data set. However, a second attempt was done on a larger data set from a study led by Dr. Luger, which contained 5179 AML or MDS patients. The results showed that ABO major mismatch led to worse TRM and overall survival. ABO minor mismatch was not significant. ABO matching remains an important consideration in donor selection, but mismatch directionality may not have consistent effects across different centers, diagnoses, conditioning regimens and graft types. Possible explanations for different outcomes include 1) heterogeneity amongst centers with respect to RBC depletion and management of hemolytic events or red cell aplasia in recipients of ABO major mismatched grafts; 2) heterogeneity with respect to plasma depletion in setting of ABO minor mismatched grafts; and 3) possible interactions between ABO, conditioning regimen, graft type, and transplant center. R03‐65s HY antigen (D Miklos) – No update was given. IB06‐09s Detection of HLA antibody to the mismatched antigen in single antigen HLA‐mismatched unrelated donor transplants: Is it a predictor of graft‐versus‐host disease outcome? (S Arai/D Miklos)– No update was given.
MINOR HISTOCOMPATIBILITY ANTIGENS No update was given.
23
Not for publication or presentation Attachment 1
6. Deferred studies pending accrual/funding
IB06‐10 Evaluation of the impact of the exposure to NIMA during fetal life and breast feeding and to the IPA during pregnancy on the clinical outcome of HSCT from haploidentical family members (J van Rood) – No update was given. IB12‐07 Telomeres and incidence of leukemia recurrence and survival after hematopoietic stem cell transplantation (M Eapen) – No update was given.
7. Closing remarks
Dr. Miklos thanked the committee for being able to serve on the committee. He adjourned the meeting at 4:25 pm.
8. Working Committee Overview Plan for 2013 ‐ 2014
Notes:
- Please note that projects primarily conducted under the IHWG, NK‐KIR PO1, and other investigator‐initiated grants are not included below)
- Other studies that are ongoing are not detailed below. Please refer to the Master List for more details
STUDIES IN PROGRESS
IB12‐01 Impact of unrelated donor HLA‐mismatch in reduced‐intensity conditioning allogeneic hematopoietic stem cell transplantation outcomes (J Koreth). This is a high impact study. Data file preparation is in process, but will be slowed because chimerism data need to be hand‐cleaned by physicians in this large dataset. The goal for this study is to submit an ASH abstract.
IB12‐02 Impact of unrelated donor HLA‐mismatch in myeloablative conditioning allogeneic hematopoietic stem cell transplantation outcomes (J Pidala/C Anasetti) – This is a high impact study, and the dataset is needed for several other derivative studies. Data file preparation is in progress. The goal for this study is to submit an ASH abstract.
IB07‐03 Analysis of Killer Immunoglobulin‐like Receptor (KIR) ligands in reduced intensity conditioning (RIC) allogeneic hematopoietic stem cell transplantation (HSCT) (R Sobecks/K Hsu/M Askar) – This is a high impact study. Analysis is in progress and the goal is a Tandem abstract.
IB12‐04 Determining the Effects of HLA‐C KIR Ligand Expression on Outcomes of Unrelated Hematopoietic Stem Cell Transplantation (J Venstrom) – This study is in protocol development now, but the goal is a Tandem abstract.
24
Not for publication or presentation Attachment 1
STUDIES AT THE MANUSCRIPT PHASE – THE GOAL OF THESE STUDIES IS PUBLICATION.
IB06‐13/R04‐80s HLA matching in unrelated cord blood transplants (S Rodriguez‐Marino/LA Baxter‐Lowe/V Rocha/M Eapen) – IB11‐03 Evaluation of the impact of allele homozygosity at HLA loci on outcome (C Hurley/A Woolfrey/M Maiers) – IB11‐04 Impact of amino acid substitutions at peptide binding pockets of HLA class I molecules on hematopoietic cell transplantation (HCT) outcomes (J Pidala/C Anasetti) – IB11‐06 Evaluation of the impact of potentially non‐immunogenic HLA‐C allele level mismatches (M Fernandez‐Vina/M Setterholm) – IB06‐02 Mismatching for low expression HLA loci in matched unrelated donor transplants (M Fernandez‐Vina) – IB09‐02 Non‐permissive HLA‐DPB1 disparities based on T cell alloreactivity (K Fleischhauer) – IB11‐07 Effect of Pretransplant Rituximab upon ABO Mismatch Hematopoietic Cell Transplantation (D Miklos/A Logan) –
NEW PROPOSALS
PROP 0212‐01/0712‐01 Interaction between SNPs and clinical data using predictive modeling on a Bayesian network framework/ Short and long term survival assessment of post HSCT transplantation using predictive modeling on a Bayesian network framework. (R Abdi/G Alterovitz/D McDermott) –The goals are to complete a formal protocol and transfer the data to the investigators, who will perform their own analysis. PROP 0712‐02/IB13‐01 The Impact Of MHC Class I Chain‐Related Gene A (MICA) Donor‐Recipient Mismatches and MICA‐129 Polymorphism On Unrelated Donor Hematopoietic Stem Cell Transplants (HSCT) For Hematological Malignancies (M Askar/R Sobecks) – The goals are to formalize the protocol, identify and transfer samples for testing, complete the analysis and submit a Tandem abstract. PROP 0712‐03 The development of Machine Learning based classifiers to define the alloreactivity of HLA mismatches in unrelated donor hematopoietic stem cell transplantation (Y Louzoun) ‐ The goals are to complete a formal protocol and transfer the data to the investigators, who will perform their own analysis. PROP 1112‐68 The effect of allele‐level HLA‐matching on survival after umbilical cord blood transplantation for non‐malignant diseases in children. (P Veys/M Eapen) – The goal of this study is to formalize the protocol and create the dataset.
25

Not for publication or presentation Attachment 1
PROP 1112‐27 Impact of donor signal‐regulatory protein alpha (SIRPα) polymorphism on outcome of allogeneic hematopoietic stem cell transplantation (allo‐HCT) (A Gassas/J Danska/S Rajakumar) – The goals are to formalize the protocol and identify and transfer samples for testing.. PROP 1212‐04 Effects of HLA Class I Amino Acid Mismatches on Stem Cell Transplant Outcomes (SR Marino/SM Lee/T Karrison/TA Binkowski/A Artz) – The goal of this study is to create a final protocol and complete the analysis. It will use a dataset already being prepared for another study. Goal: submit Tandem abstract
NEW PROPOSALS ON HOLD OR OTHERWISE DEFERRED PROP 0312‐01 Role of the complement system in graft‐versus‐host disease (V Afshar‐Kharghan /J Belmont/C Amos) – awaiting funding PROP 1112‐16 Effect of HLA‐C allele matching in the context of recipient HLA‐C‐encoded KIR ligand grouping (C1 or C2) on the outcome of unrelated hematopoietic stem cell transplantation (HCT) (J Fischer/M Uhrberg) – This study will be combined with IB12‐04 (J Venstrom). IB12‐07 Telomeres and incidence of leukemia recurrence and survival after hematopoietic stem cell transplantation (M Eapen) – awaiting funding IB06‐10 Evaluation of the impact of the exposure to NIMA during fetal life and breast feeding and to the IPA during pregnancy on the clinical outcome of HSCT from haploidentical family members (J van Rood) – awaiting more cases
PROTOCOLS SUBMITTED BUT NOT DISCUSSED Haplo‐identical transplants – not enough cases
WORK ASSIGNMENTS FOR WORKING COMMITTEE LEADERSHIP Participate in monthly conference calls – review materials, contribute to discussion, contact investigators or provide study‐specific support as requested by the Scientific Directors
26
Not for publication or presentation Attachment 2
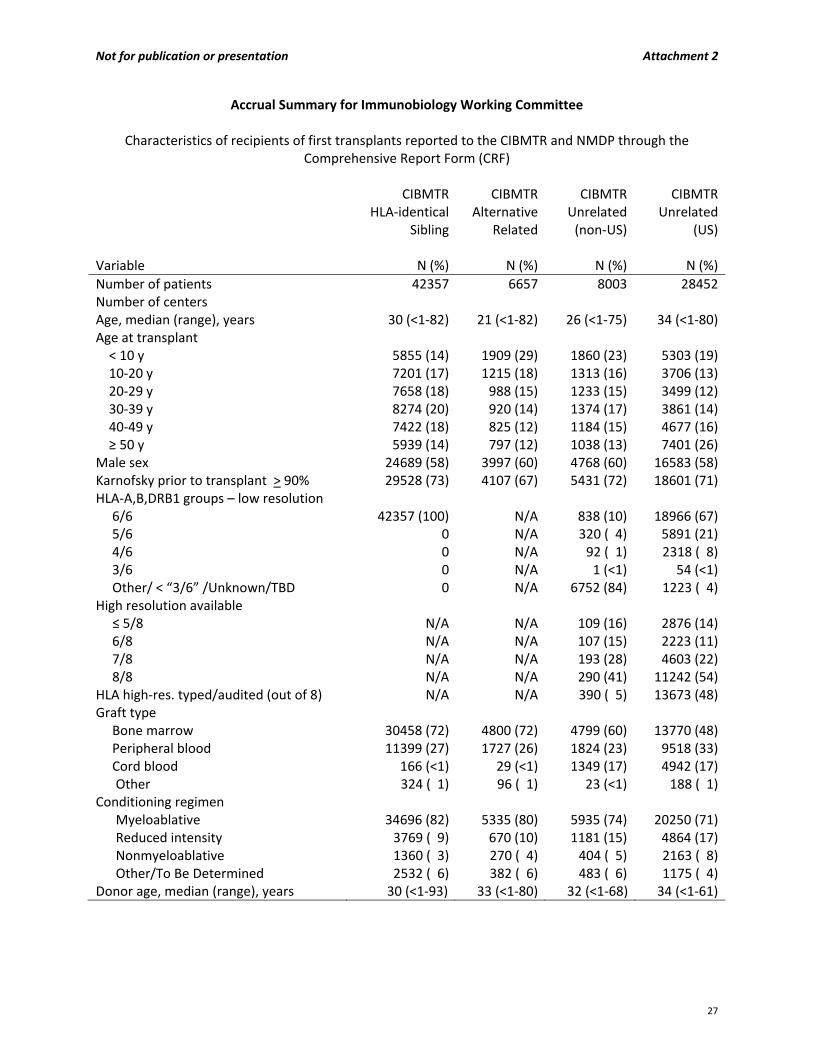
Accrual Summary for Immunobiology Working Committee
Characteristics of recipients of first transplants reported to the CIBMTR and NMDP through the Comprehensive Report Form (CRF)
CIBMTR
HLA‐identical Sibling
CIBMTRAlternative
Related
CIBMTR Unrelated (non‐US)
CIBMTRUnrelated
(US)
Variable N (%) N (%) N (%) N (%)
Number of patients 42357 6657 8003 28452Number of centers Age, median (range), years 30 (<1‐82) 21 (<1‐82) 26 (<1‐75) 34 (<1‐80)Age at transplant < 10 y 5855 (14) 1909 (29) 1860 (23) 5303 (19) 10‐20 y 7201 (17) 1215 (18) 1313 (16) 3706 (13) 20‐29 y 7658 (18) 988 (15) 1233 (15) 3499 (12) 30‐39 y 8274 (20) 920 (14) 1374 (17) 3861 (14) 40‐49 y 7422 (18) 825 (12) 1184 (15) 4677 (16) ≥ 50 y 5939 (14) 797 (12) 1038 (13) 7401 (26)Male sex 24689 (58) 3997 (60) 4768 (60) 16583 (58)Karnofsky prior to transplant > 90% 29528 (73) 4107 (67) 5431 (72) 18601 (71)HLA‐A,B,DRB1 groups – low resolution 6/6 42357 (100) N/A 838 (10) 18966 (67) 5/6 0 N/A 320 ( 4) 5891 (21) 4/6 0 N/A 92 ( 1) 2318 ( 8) 3/6 0 N/A 1 (<1) 54 (<1) Other/ < “3/6” /Unknown/TBD 0 N/A 6752 (84) 1223 ( 4)High resolution available ≤ 5/8 N/A N/A 109 (16) 2876 (14) 6/8 N/A N/A 107 (15) 2223 (11) 7/8 N/A N/A 193 (28) 4603 (22) 8/8 N/A N/A 290 (41) 11242 (54)HLA high‐res. typed/audited (out of 8) N/A N/A 390 ( 5) 13673 (48)Graft type Bone marrow 30458 (72) 4800 (72) 4799 (60) 13770 (48) Peripheral blood 11399 (27) 1727 (26) 1824 (23) 9518 (33) Cord blood 166 (<1) 29 (<1) 1349 (17) 4942 (17)
Other 324 ( 1) 96 ( 1) 23 (<1) 188 ( 1)Conditioning regimen
Myeloablative 34696 (82) 5335 (80) 5935 (74) 20250 (71)Reduced intensity 3769 ( 9) 670 (10) 1181 (15) 4864 (17)Nonmyeloablative 1360 ( 3) 270 ( 4) 404 ( 5) 2163 ( 8)Other/To Be Determined 2532 ( 6) 382 ( 6) 483 ( 6) 1175 ( 4)
Donor age, median (range), years 30 (<1‐93) 33 (<1‐80) 32 (<1‐68) 34 (<1‐61)
27
Not for publication or presentation Attachment 2
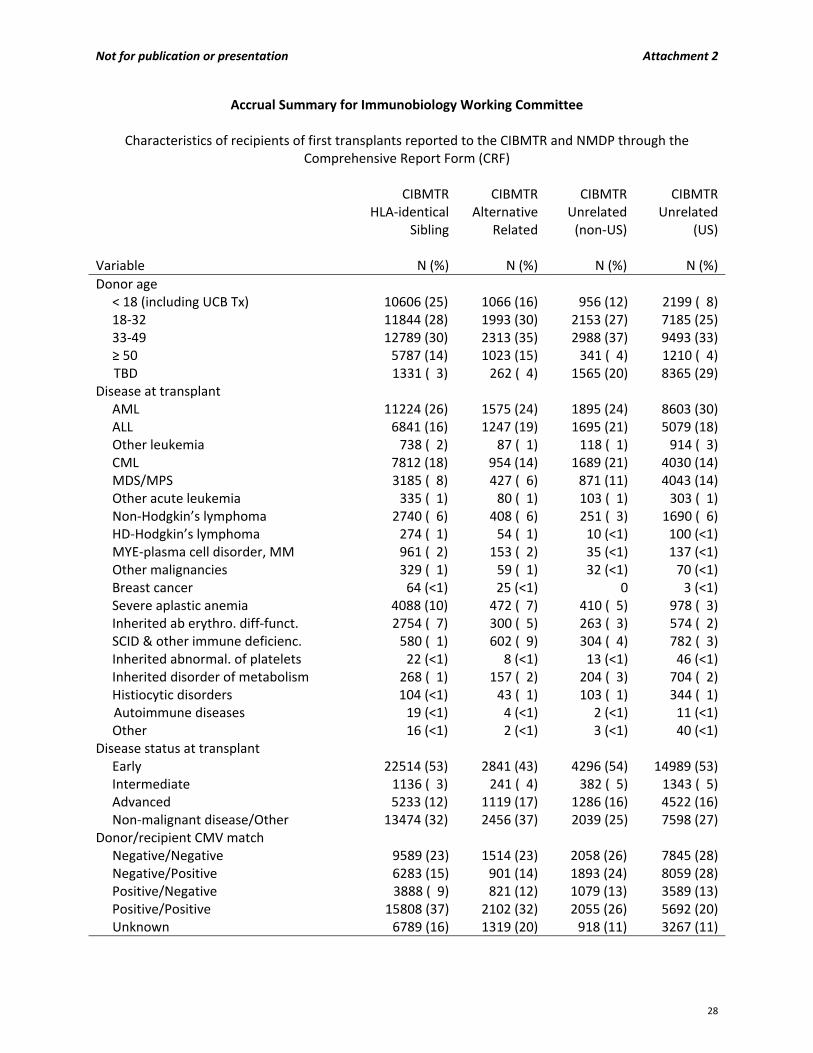
Accrual Summary for Immunobiology Working Committee
Characteristics of recipients of first transplants reported to the CIBMTR and NMDP through the Comprehensive Report Form (CRF)
CIBMTR
HLA‐identical Sibling
CIBMTRAlternative
Related
CIBMTR Unrelated (non‐US)
CIBMTRUnrelated
(US)
Variable N (%) N (%) N (%) N (%)
Donor age < 18 (including UCB Tx) 10606 (25) 1066 (16) 956 (12) 2199 ( 8) 18‐32 11844 (28) 1993 (30) 2153 (27) 7185 (25) 33‐49 12789 (30) 2313 (35) 2988 (37) 9493 (33) ≥ 50 5787 (14) 1023 (15) 341 ( 4) 1210 ( 4)
TBD 1331 ( 3) 262 ( 4) 1565 (20) 8365 (29)Disease at transplant AML 11224 (26) 1575 (24) 1895 (24) 8603 (30) ALL 6841 (16) 1247 (19) 1695 (21) 5079 (18) Other leukemia 738 ( 2) 87 ( 1) 118 ( 1) 914 ( 3) CML 7812 (18) 954 (14) 1689 (21) 4030 (14) MDS/MPS 3185 ( 8) 427 ( 6) 871 (11) 4043 (14) Other acute leukemia 335 ( 1) 80 ( 1) 103 ( 1) 303 ( 1) Non‐Hodgkin’s lymphoma 2740 ( 6) 408 ( 6) 251 ( 3) 1690 ( 6) HD‐Hodgkin’s lymphoma 274 ( 1) 54 ( 1) 10 (<1) 100 (<1) MYE‐plasma cell disorder, MM 961 ( 2) 153 ( 2) 35 (<1) 137 (<1) Other malignancies 329 ( 1) 59 ( 1) 32 (<1) 70 (<1) Breast cancer 64 (<1) 25 (<1) 0 3 (<1) Severe aplastic anemia 4088 (10) 472 ( 7) 410 ( 5) 978 ( 3) Inherited ab erythro. diff‐funct. 2754 ( 7) 300 ( 5) 263 ( 3) 574 ( 2) SCID & other immune deficienc. 580 ( 1) 602 ( 9) 304 ( 4) 782 ( 3) Inherited abnormal. of platelets 22 (<1) 8 (<1) 13 (<1) 46 (<1) Inherited disorder of metabolism 268 ( 1) 157 ( 2) 204 ( 3) 704 ( 2) Histiocytic disorders 104 (<1) 43 ( 1) 103 ( 1) 344 ( 1)
Autoimmune diseases 19 (<1) 4 (<1) 2 (<1) 11 (<1) Other 16 (<1) 2 (<1) 3 (<1) 40 (<1)Disease status at transplant Early 22514 (53) 2841 (43) 4296 (54) 14989 (53) Intermediate 1136 ( 3) 241 ( 4) 382 ( 5) 1343 ( 5) Advanced 5233 (12) 1119 (17) 1286 (16) 4522 (16) Non‐malignant disease/Other 13474 (32) 2456 (37) 2039 (25) 7598 (27)Donor/recipient CMV match Negative/Negative 9589 (23) 1514 (23) 2058 (26) 7845 (28) Negative/Positive 6283 (15) 901 (14) 1893 (24) 8059 (28) Positive/Negative 3888 ( 9) 821 (12) 1079 (13) 3589 (13) Positive/Positive 15808 (37) 2102 (32) 2055 (26) 5692 (20) Unknown 6789 (16) 1319 (20) 918 (11) 3267 (11)
28

Not for publication or presentation Attachment 2
Accrual Summary for Immunobiology Working Committee
Characteristics of recipients of first transplants reported to the CIBMTR and NMDP through the Comprehensive Report Form (CRF)
CIBMTR
HLA‐identical Sibling
CIBMTRAlternative
Related
CIBMTR Unrelated (non‐US)
CIBMTRUnrelated
(US)
Variable N (%) N (%) N (%) N (%)
GVHD prophylaxis Ex vivo T‐cell depletion alone 1591 ( 4) 752 (11) 223 ( 3) 1053 ( 4)Ex vivo T‐cell depletion + post‐tx immune suppression
1484 ( 4)
711 (11)
241 ( 3)
1882 ( 7)
CD34 selection alone 155 (<1) 135 ( 2) 32 (<1) 156 ( 1)CD34 selection + post‐tx immune suppression
280 ( 1)
120 ( 2)
37 (<1)
329 ( 1)
Cyclophosphamide alone 38 (<1) 3 (<1) 0 58 (<1)Cyclophosphamide + others 387 ( 1) 120 ( 2) 34 (<1) 83 (<1)FK506 + MMF +‐ others 706 ( 2) 123 ( 2) 77 ( 1) 3012 (11)FK506 + MTX +‐ others (except MMF) 2878 ( 7) 240 ( 4) 462 ( 6) 7194 (25)FK506 + others (except MTX, MMF) 449 ( 1) 33 (<1) 59 ( 1) 1062 ( 4)FK506 alone 260 ( 1) 40 ( 1) 20 (<1) 521 ( 2)CSA + MMF +‐ others (except FK506) 1016 ( 2) 70 ( 1) 606 ( 8) 2824 (10)CSA + MTX +‐ others (except FK506,MMF) 20294 (48) 1986 (30) 4486 (56) 6996 (25)CSA + others (except FK506, MTX, MMF) 3645 ( 9) 445 ( 7) 931 (12) 1763 ( 6)CSA alone 5062 (12) 481 ( 7) 404 ( 5) 319 ( 1)Other GVHD prophylaxis 4112 (10) 1398 (21) 391 ( 5) 1200 ( 4)
Donor/recipient sex match Male/Male 12408 (32) 2058 (35) 2328 (39) 588 (32) Male/Female 8384 (22) 971 (17) 1331 (22) 368 (20) Female/Male 9904 (26) 1440 (25) 1254 (21) 514 (28) Female/Female 7502 (20) 1352 (23) 1125 (19) 367 (20)
29
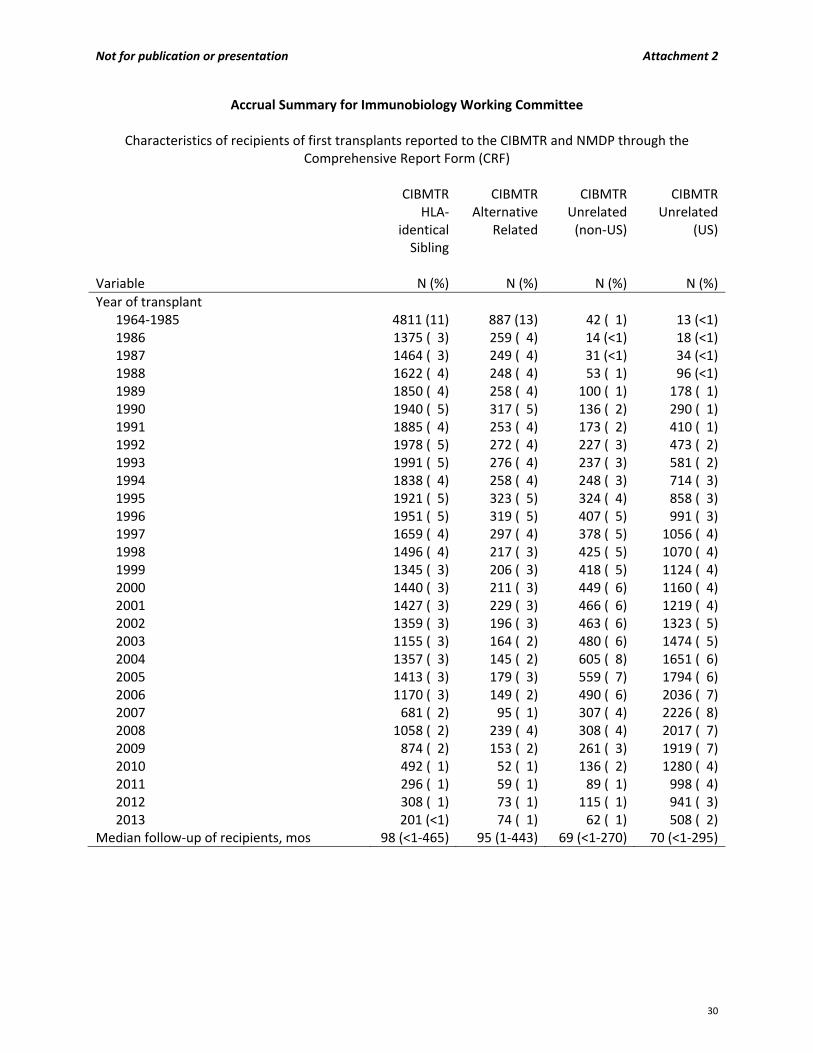
Not for publication or presentation Attachment 2
Accrual Summary for Immunobiology Working Committee
Characteristics of recipients of first transplants reported to the CIBMTR and NMDP through the Comprehensive Report Form (CRF)
CIBMTR
HLA‐identical Sibling
CIBMTRAlternative
Related
CIBMTR Unrelated (non‐US)
CIBMTRUnrelated
(US)
Variable N (%) N (%) N (%) N (%)
Year of transplant 1964‐1985 4811 (11) 887 (13) 42 ( 1) 13 (<1)1986 1375 ( 3) 259 ( 4) 14 (<1) 18 (<1)1987 1464 ( 3) 249 ( 4) 31 (<1) 34 (<1)1988 1622 ( 4) 248 ( 4) 53 ( 1) 96 (<1)1989 1850 ( 4) 258 ( 4) 100 ( 1) 178 ( 1)1990 1940 ( 5) 317 ( 5) 136 ( 2) 290 ( 1)1991 1885 ( 4) 253 ( 4) 173 ( 2) 410 ( 1)1992 1978 ( 5) 272 ( 4) 227 ( 3) 473 ( 2)1993 1991 ( 5) 276 ( 4) 237 ( 3) 581 ( 2)1994 1838 ( 4) 258 ( 4) 248 ( 3) 714 ( 3)1995 1921 ( 5) 323 ( 5) 324 ( 4) 858 ( 3)1996 1951 ( 5) 319 ( 5) 407 ( 5) 991 ( 3)1997 1659 ( 4) 297 ( 4) 378 ( 5) 1056 ( 4)1998 1496 ( 4) 217 ( 3) 425 ( 5) 1070 ( 4)1999 1345 ( 3) 206 ( 3) 418 ( 5) 1124 ( 4)2000 1440 ( 3) 211 ( 3) 449 ( 6) 1160 ( 4)2001 1427 ( 3) 229 ( 3) 466 ( 6) 1219 ( 4)2002 1359 ( 3) 196 ( 3) 463 ( 6) 1323 ( 5)2003 1155 ( 3) 164 ( 2) 480 ( 6) 1474 ( 5)2004 1357 ( 3) 145 ( 2) 605 ( 8) 1651 ( 6)2005 1413 ( 3) 179 ( 3) 559 ( 7) 1794 ( 6)2006 1170 ( 3) 149 ( 2) 490 ( 6) 2036 ( 7)2007 681 ( 2) 95 ( 1) 307 ( 4) 2226 ( 8)2008 1058 ( 2) 239 ( 4) 308 ( 4) 2017 ( 7)2009 874 ( 2) 153 ( 2) 261 ( 3) 1919 ( 7)2010 492 ( 1) 52 ( 1) 136 ( 2) 1280 ( 4)2011 296 ( 1) 59 ( 1) 89 ( 1) 998 ( 4)2012 308 ( 1) 73 ( 1) 115 ( 1) 941 ( 3)2013 201 (<1) 74 ( 1) 62 ( 1) 508 ( 2)
Median follow‐up of recipients, mos 98 (<1‐465) 95 (1‐443) 69 (<1‐270) 70 (<1‐295)
30

Not for publication or presentation Attachment 2
Accrual Summary for First Transplants with Samples Available for Recipient and/or Donor through the NMDP for Adult Unrelated Donor Transplants
Samples Available
for Recipient and Donor
Samples Available for Recipient Only
Samples Available for Donor Only
Variable N Eval N (%) N Eval N (%) N Eval N (%)
Number of cases 18291 3816 3249Number of centers 206 178 221Age, median (range), years 18291 39 (<1‐83) 3816 38 (<1‐79) 3249 34 (<1‐75)Age at transplant 18291 3816 3249 < 10 y 2091 (11) 454 (12) 534 (16) 10‐20 y 2152 (12) 473 (12) 428 (13) 20‐29 y 2363 (13) 482 (13) 441 (14) 30‐39 y 2699 (15) 571 (15) 468 (14) 40‐49 y 3277 (18) 728 (19) 549 (17) ≥ 50 y 5709 (31) 1108 (29) 829 (26)Male sex 18291 10594 (58) 3816 2272 (60) 3249 1953 (60)Karnofsky prior to transplant > 90% 14488 10206 (70) 3128 2164 (69) 2465 1753 (71)HLA‐A,B,C,DRB1 groups – high‐res 16259 1488 1201 0/8 ‐ 3/8 64 (<1) 0 2 (<1) 4/8 180 ( 1) 5 (<1) 4 (<1) 5/8 515 ( 3) 11 ( 1) 18 ( 1) 6/8 1393 ( 9) 42 ( 3) 78 ( 6) 7/8 3954 (24) 352 (24) 279 (23) 8/8 10153 (62) 1078 (72) 820 (68)HLA high‐res. typed and audited 13031 12940 (99) 69 63 (91) 170 168 (99)Disease status at transplant 18291 3816 3249 Early 8320 (45) 1842 (48) 1359 (42) Intermediate 767 ( 4) 150 ( 4) 135 ( 4) Advanced 2677 (15) 570 (15) 506 (16) Non‐malignant disease/Other 6527 (36) 1254 (33) 1249 (38)Graft type 18291 3816 3249
Bone marrow 9794 (54) 2362 (62) 1946 (60)Peripheral blood 8410 (46) 1439 (38) 1292 (40)Bone marrow + PBSC 87 (<1) 15 (<1) 11 (<1)
Conditioning regimen 18291 3816 3249 Myeloablative 11714 (64) 2590 (68) 2031 (63)Reduced intensity 2858 (16) 550 (14) 453 (14)Nonmyeloablative 1288 ( 7) 198 ( 5) 199 ( 6)Other/To be determined 2431 (13) 478 (13) 566 (17)
31
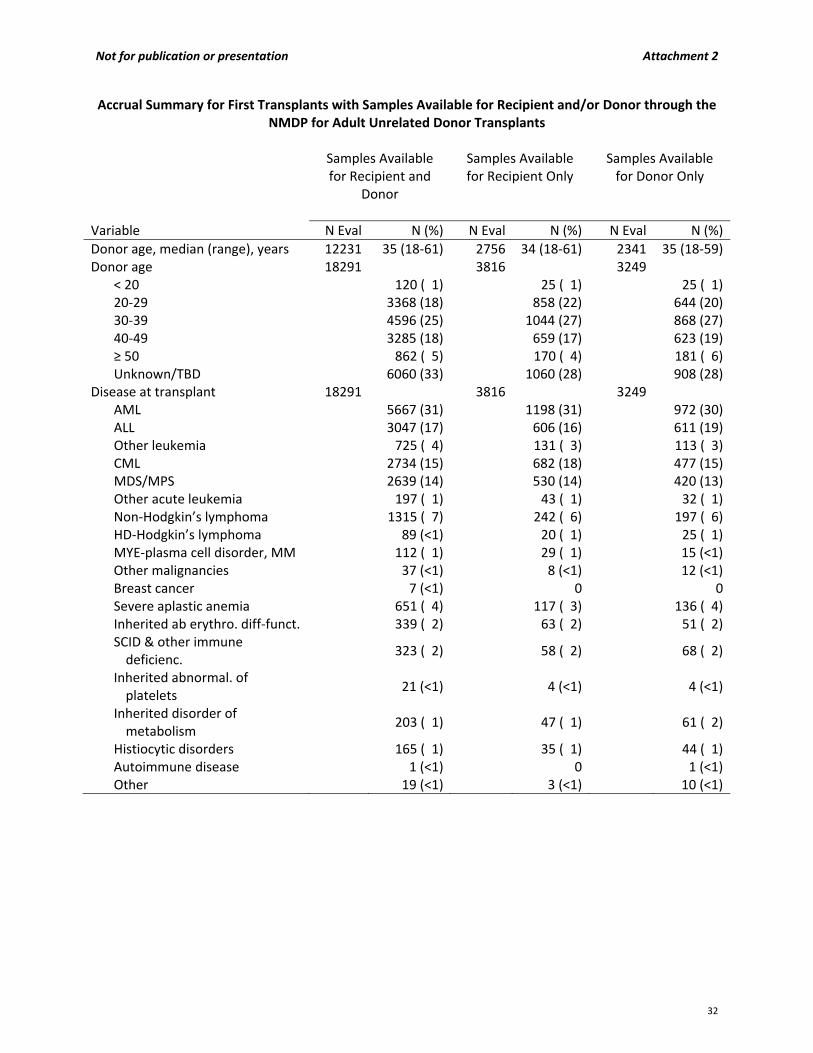
Not for publication or presentation Attachment 2
Accrual Summary for First Transplants with Samples Available for Recipient and/or Donor through the NMDP for Adult Unrelated Donor Transplants
Samples Available
for Recipient and Donor
Samples Available for Recipient Only
Samples Available for Donor Only
Variable N Eval N (%) N Eval N (%) N Eval N (%)
Donor age, median (range), years 12231 35 (18‐61) 2756 34 (18‐61) 2341 35 (18‐59)Donor age 18291 3816 3249
< 20 120 ( 1) 25 ( 1) 25 ( 1)20‐29 3368 (18) 858 (22) 644 (20)30‐39 4596 (25) 1044 (27) 868 (27)40‐49 3285 (18) 659 (17) 623 (19)≥ 50 862 ( 5) 170 ( 4) 181 ( 6)Unknown/TBD 6060 (33) 1060 (28) 908 (28)
Disease at transplant 18291 3816 3249 AML 5667 (31) 1198 (31) 972 (30)ALL 3047 (17) 606 (16) 611 (19)Other leukemia 725 ( 4) 131 ( 3) 113 ( 3)CML 2734 (15) 682 (18) 477 (15)MDS/MPS 2639 (14) 530 (14) 420 (13)Other acute leukemia 197 ( 1) 43 ( 1) 32 ( 1)Non‐Hodgkin’s lymphoma 1315 ( 7) 242 ( 6) 197 ( 6)HD‐Hodgkin’s lymphoma 89 (<1) 20 ( 1) 25 ( 1)MYE‐plasma cell disorder, MM 112 ( 1) 29 ( 1) 15 (<1)Other malignancies 37 (<1) 8 (<1) 12 (<1)Breast cancer 7 (<1) 0 0Severe aplastic anemia 651 ( 4) 117 ( 3) 136 ( 4)Inherited ab erythro. diff‐funct. 339 ( 2) 63 ( 2) 51 ( 2)SCID & other immune deficienc.
323 ( 2) 58 ( 2) 68 ( 2)
Inherited abnormal. of platelets
21 (<1) 4 (<1) 4 (<1)
Inherited disorder of metabolism
203 ( 1) 47 ( 1) 61 ( 2)
Histiocytic disorders 165 ( 1) 35 ( 1) 44 ( 1)Autoimmune disease 1 (<1) 0 1 (<1)Other 19 (<1) 3 (<1) 10 (<1)
32
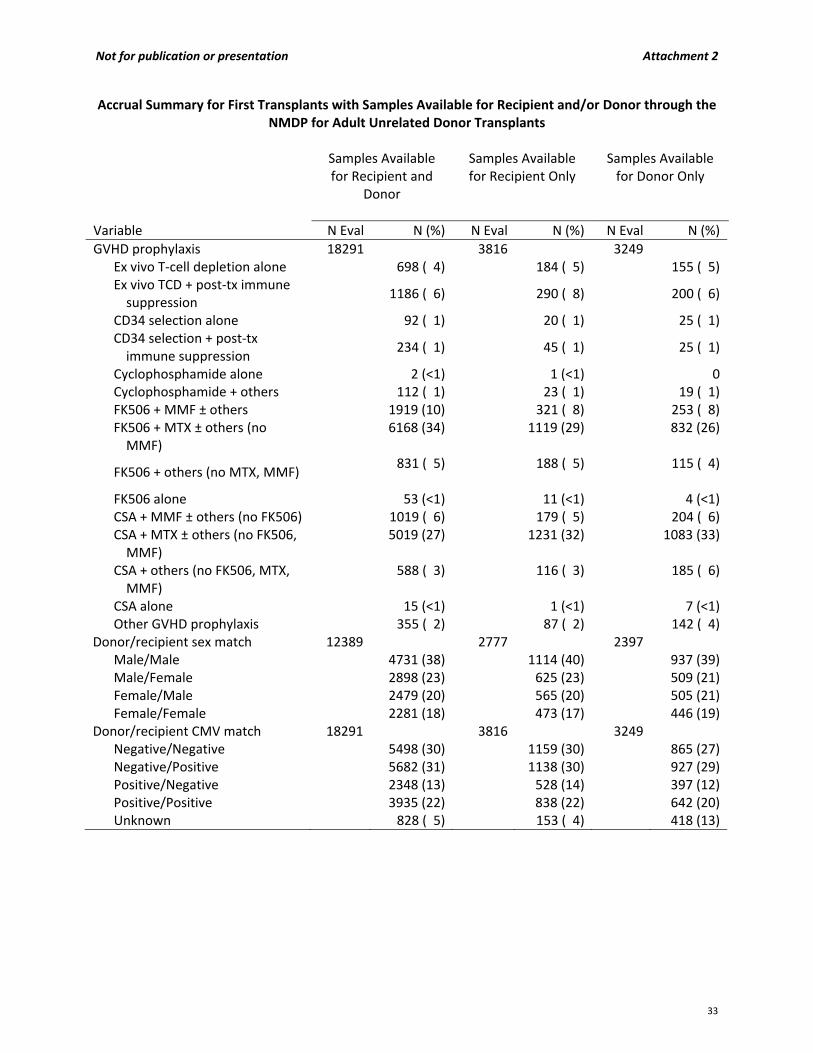
Not for publication or presentation Attachment 2
Accrual Summary for First Transplants with Samples Available for Recipient and/or Donor through the NMDP for Adult Unrelated Donor Transplants
Samples Available
for Recipient and Donor
Samples Available for Recipient Only
Samples Available for Donor Only
Variable N Eval N (%) N Eval N (%) N Eval N (%)
GVHD prophylaxis 18291 3816 3249 Ex vivo T‐cell depletion alone 698 ( 4) 184 ( 5) 155 ( 5) Ex vivo TCD + post‐tx immune suppression
1186 ( 6) 290 ( 8) 200 ( 6)
CD34 selection alone 92 ( 1) 20 ( 1) 25 ( 1) CD34 selection + post‐tx immune suppression
234 ( 1) 45 ( 1) 25 ( 1)
Cyclophosphamide alone 2 (<1) 1 (<1) 0 Cyclophosphamide + others 112 ( 1) 23 ( 1) 19 ( 1) FK506 + MMF ± others 1919 (10) 321 ( 8) 253 ( 8) FK506 + MTX ± others (no MMF)
6168 (34)
1119 (29)
832 (26)
FK506 + others (no MTX, MMF) 831 ( 5)
188 ( 5)
115 ( 4)
FK506 alone 53 (<1) 11 (<1) 4 (<1) CSA + MMF ± others (no FK506) 1019 ( 6) 179 ( 5) 204 ( 6) CSA + MTX ± others (no FK506, MMF)
5019 (27)
1231 (32)
1083 (33)
CSA + others (no FK506, MTX, MMF)
588 ( 3)
116 ( 3)
185 ( 6)
CSA alone 15 (<1) 1 (<1) 7 (<1) Other GVHD prophylaxis 355 ( 2) 87 ( 2) 142 ( 4)
Donor/recipient sex match 12389 2777 2397 Male/Male 4731 (38) 1114 (40) 937 (39) Male/Female 2898 (23) 625 (23) 509 (21) Female/Male 2479 (20) 565 (20) 505 (21) Female/Female 2281 (18) 473 (17) 446 (19)
Donor/recipient CMV match 18291 3816 3249 Negative/Negative 5498 (30) 1159 (30) 865 (27) Negative/Positive 5682 (31) 1138 (30) 927 (29) Positive/Negative 2348 (13) 528 (14) 397 (12) Positive/Positive 3935 (22) 838 (22) 642 (20) Unknown 828 ( 5) 153 ( 4) 418 (13)
33
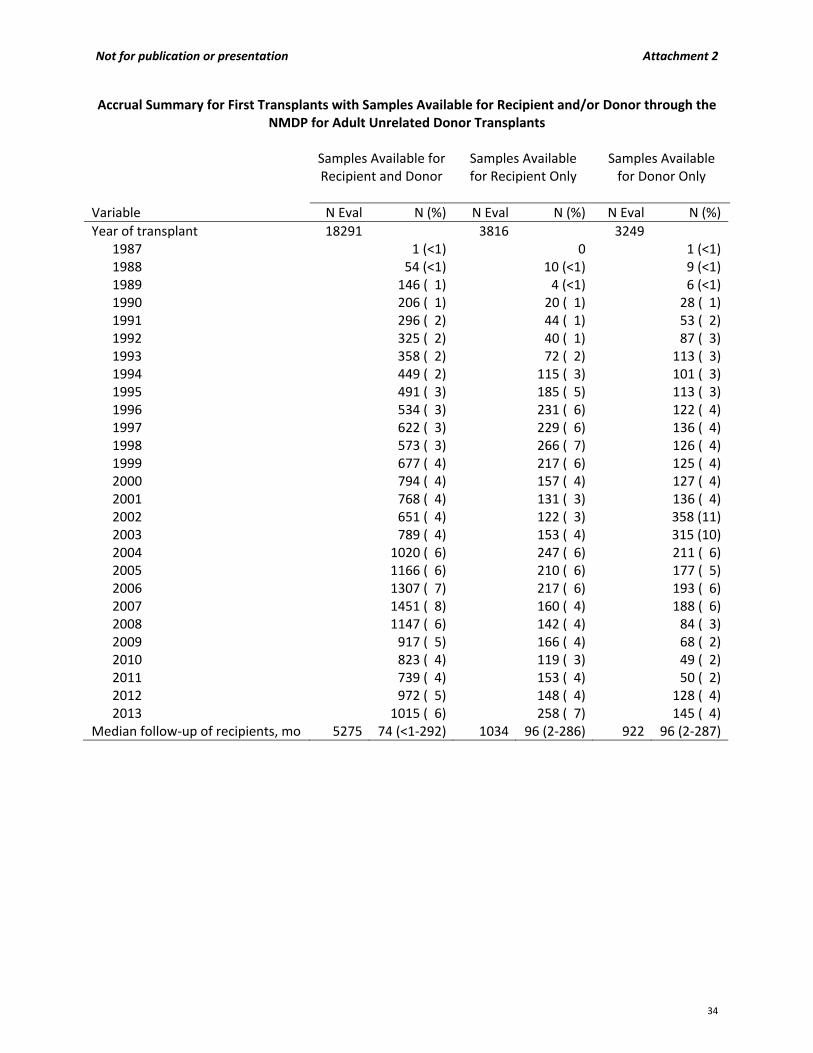
Not for publication or presentation Attachment 2
Accrual Summary for First Transplants with Samples Available for Recipient and/or Donor through the NMDP for Adult Unrelated Donor Transplants
Samples Available for
Recipient and Donor
Samples Available for Recipient Only
Samples Available for Donor Only
Variable N Eval N (%) N Eval N (%) N Eval N (%)
Year of transplant 18291 3816 3249 1987 1 (<1) 0 1 (<1)1988 54 (<1) 10 (<1) 9 (<1)1989 146 ( 1) 4 (<1) 6 (<1)1990 206 ( 1) 20 ( 1) 28 ( 1)1991 296 ( 2) 44 ( 1) 53 ( 2)1992 325 ( 2) 40 ( 1) 87 ( 3)1993 358 ( 2) 72 ( 2) 113 ( 3)1994 449 ( 2) 115 ( 3) 101 ( 3)1995 491 ( 3) 185 ( 5) 113 ( 3)1996 534 ( 3) 231 ( 6) 122 ( 4)1997 622 ( 3) 229 ( 6) 136 ( 4)1998 573 ( 3) 266 ( 7) 126 ( 4)1999 677 ( 4) 217 ( 6) 125 ( 4)2000 794 ( 4) 157 ( 4) 127 ( 4)2001 768 ( 4) 131 ( 3) 136 ( 4)2002 651 ( 4) 122 ( 3) 358 (11)2003 789 ( 4) 153 ( 4) 315 (10)2004 1020 ( 6) 247 ( 6) 211 ( 6)2005 1166 ( 6) 210 ( 6) 177 ( 5)2006 1307 ( 7) 217 ( 6) 193 ( 6)2007 1451 ( 8) 160 ( 4) 188 ( 6)2008 1147 ( 6) 142 ( 4) 84 ( 3)2009 917 ( 5) 166 ( 4) 68 ( 2)2010 823 ( 4) 119 ( 3) 49 ( 2)2011 739 ( 4) 153 ( 4) 50 ( 2)2012 972 ( 5) 148 ( 4) 128 ( 4)2013 1015 ( 6) 258 ( 7) 145 ( 4)
Median follow‐up of recipients, mo 5275 74 (<1‐292) 1034 96 (2‐286) 922 96 (2‐287)
34
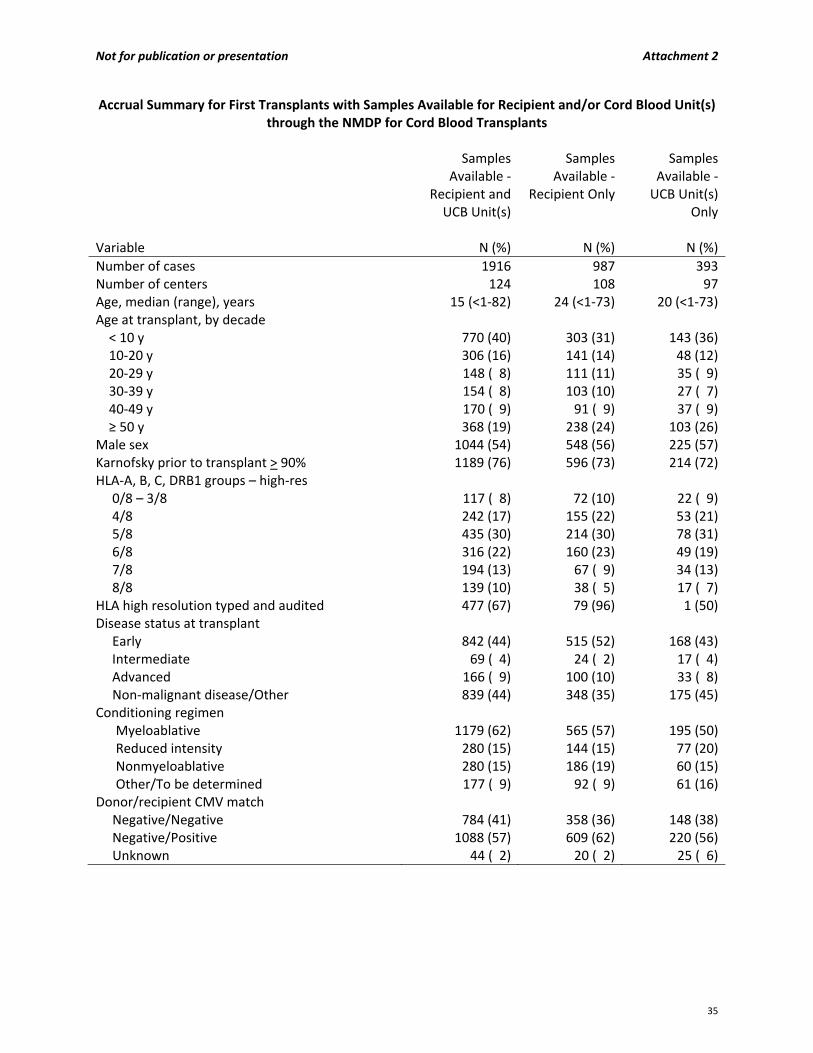
Not for publication or presentation Attachment 2
Accrual Summary for First Transplants with Samples Available for Recipient and/or Cord Blood Unit(s) through the NMDP for Cord Blood Transplants
Samples
Available ‐ Recipient and UCB Unit(s)
Samples Available ‐
Recipient Only
Samples Available ‐ UCB Unit(s)
Only
Variable N (%) N (%) N (%)
Number of cases 1916 987 393Number of centers 124 108 97Age, median (range), years 15 (<1‐82) 24 (<1‐73) 20 (<1‐73)Age at transplant, by decade < 10 y 770 (40) 303 (31) 143 (36) 10‐20 y 306 (16) 141 (14) 48 (12) 20‐29 y 148 ( 8) 111 (11) 35 ( 9) 30‐39 y 154 ( 8) 103 (10) 27 ( 7) 40‐49 y 170 ( 9) 91 ( 9) 37 ( 9) ≥ 50 y 368 (19) 238 (24) 103 (26)Male sex 1044 (54) 548 (56) 225 (57)Karnofsky prior to transplant > 90% 1189 (76) 596 (73) 214 (72)HLA‐A, B, C, DRB1 groups – high‐res 0/8 – 3/8 117 ( 8) 72 (10) 22 ( 9) 4/8 242 (17) 155 (22) 53 (21) 5/8 435 (30) 214 (30) 78 (31) 6/8 316 (22) 160 (23) 49 (19) 7/8 194 (13) 67 ( 9) 34 (13) 8/8 139 (10) 38 ( 5) 17 ( 7)HLA high resolution typed and audited 477 (67) 79 (96) 1 (50)Disease status at transplant Early 842 (44) 515 (52) 168 (43) Intermediate 69 ( 4) 24 ( 2) 17 ( 4) Advanced 166 ( 9) 100 (10) 33 ( 8) Non‐malignant disease/Other 839 (44) 348 (35) 175 (45)Conditioning regimen
Myeloablative 1179 (62) 565 (57) 195 (50)Reduced intensity 280 (15) 144 (15) 77 (20)Nonmyeloablative 280 (15) 186 (19) 60 (15)Other/To be determined 177 ( 9) 92 ( 9) 61 (16)
Donor/recipient CMV match Negative/Negative 784 (41) 358 (36) 148 (38) Negative/Positive 1088 (57) 609 (62) 220 (56) Unknown 44 ( 2) 20 ( 2) 25 ( 6)
35

Not for publication or presentation Attachment 2
Accrual Summary for First Transplants with Samples Available for Recipient and/or Cord Blood Unit(s)
through the NMDP for Cord Blood Transplants Samples
Available ‐ Recipient and UCB Unit(s)
Samples Available ‐
Recipient Only
Samples Available ‐ UCB Unit(s)
Only
Variable N (%) N (%) N (%)
Disease at transplant AML 608 (32) 373 (38) 131 (33) ALL 410 (21) 234 (24) 83 (21) Other leukemia 56 ( 3) 26 ( 3) 6 ( 2) CML 60 ( 3) 16 ( 2) 11 ( 3) MDS/MPS 198 (10) 132 (13) 45 (11) Other acute leukemia 44 ( 2) 9 ( 1) 7 ( 2) Non‐Hodgkin’s lymphoma 99 ( 5) 40 ( 4) 19 ( 5) HD‐Hodgkin’s lymphoma 6 (<1) 1 (<1) 1 (<1)
Plasma cell disorders, Multiple Myeloma 0 2 (<1) 2 ( 1) Other malignancies 6 (<1) 0 0 Severe aplastic anemia 39 ( 2) 22 ( 2) 6 ( 2) Inherited ab erythro. diff‐funct. 62 ( 3) 29 ( 3) 13 ( 3) SCID & other immune deficienc. 119 ( 6) 35 ( 4) 19 ( 5) Inherited abnormal. of platelets 7 (<1) 3 (<1) 1 (<1) Inherited disorder of metabolism 129 ( 7) 44 ( 4) 32 ( 8) Histiocytic disorders 64 ( 3) 17 ( 2) 15 ( 4) Autoimmune diseases 2 (<1) 2 (<1) 0 Other 7 (<1) 2 (<1) 2 ( 1)GVHD prophylaxis
Ex vivo T‐cell depletion alone 0 2 (<1) 0Ex vivo T‐cell depletion + post‐tx immune suppression
2 (<1)
0
0
CD34 selection alone 4 (<1) 1 (<1) 2 ( 1)CD34 selection + post‐tx immune suppression 0 1 (<1) 0FK506 + MMF +‐ others 501 (26) 292 (30) 79 (20)FK506 + MTX +‐ others (except MMF) 106 ( 6) 47 ( 5) 11 ( 3)FK506 + others (except MTX, MMF) 130 ( 7) 58 ( 6) 42 (11)FK506 alone 1 (<1) 0 0CSA + MMF +‐ others (except FK506) 876 (46) 448 (45) 180 (46)CSA + MTX +‐ others (except FK506, MMF) 51 ( 3) 31 ( 3) 14 ( 4)CSA + others (except FK506, MTX, MMF) 214 (11) 100 (10) 52 (13)CSA alone 1 (<1) 1 (<1) 1 (<1)Other GVHD prophylaxis 30 ( 2) 6 ( 1) 12 ( 3)
36
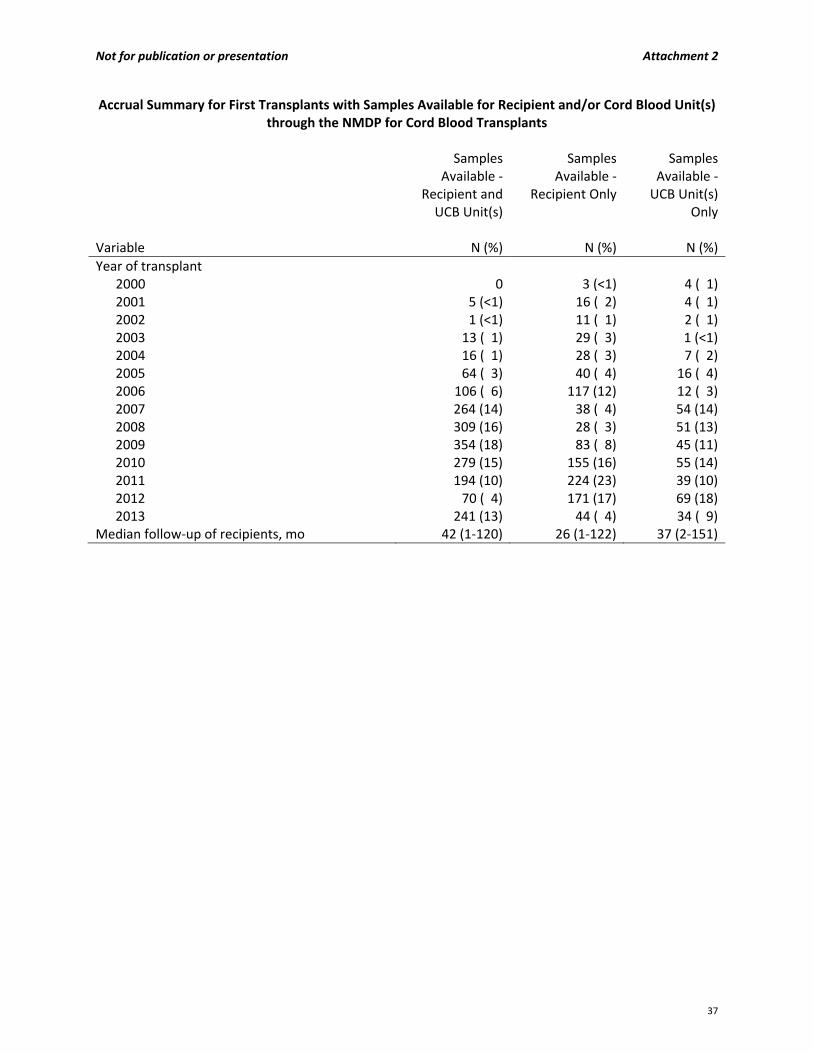
Not for publication or presentation Attachment 2
Accrual Summary for First Transplants with Samples Available for Recipient and/or Cord Blood Unit(s) through the NMDP for Cord Blood Transplants
Samples
Available ‐ Recipient and UCB Unit(s)
Samples Available ‐
Recipient Only
Samples Available ‐ UCB Unit(s)
Only
Variable N (%) N (%) N (%)
Year of transplant 2000 0 3 (<1) 4 ( 1)2001 5 (<1) 16 ( 2) 4 ( 1)2002 1 (<1) 11 ( 1) 2 ( 1)2003 13 ( 1) 29 ( 3) 1 (<1)2004 16 ( 1) 28 ( 3) 7 ( 2)2005 64 ( 3) 40 ( 4) 16 ( 4)2006 106 ( 6) 117 (12) 12 ( 3)2007 264 (14) 38 ( 4) 54 (14)2008 309 (16) 28 ( 3) 51 (13)2009 354 (18) 83 ( 8) 45 (11)2010 279 (15) 155 (16) 55 (14)2011 194 (10) 224 (23) 39 (10)2012 70 ( 4) 171 (17) 69 (18)2013 241 (13) 44 ( 4) 34 ( 9)
Median follow‐up of recipients, mo 42 (1‐120) 26 (1‐122) 37 (2‐151)
37
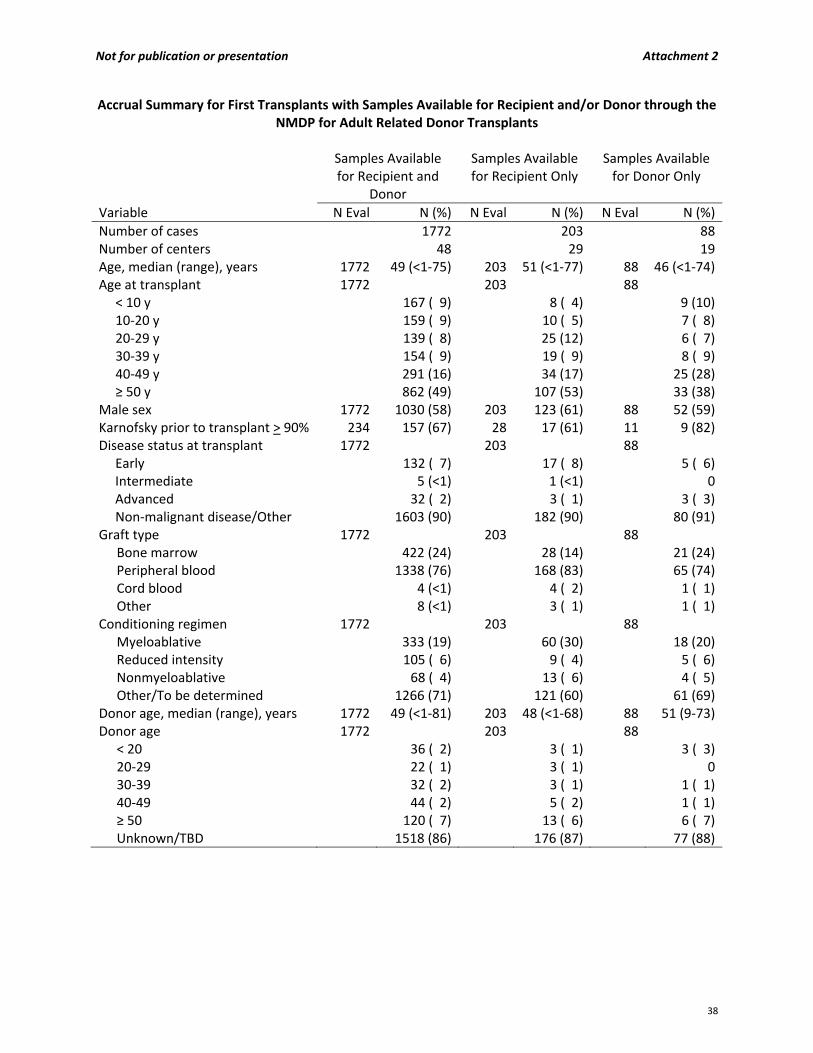
Not for publication or presentation Attachment 2
Accrual Summary for First Transplants with Samples Available for Recipient and/or Donor through the NMDP for Adult Related Donor Transplants
Samples Available
for Recipient and Donor
Samples Available for Recipient Only
Samples Available for Donor Only
Variable N Eval N (%) N Eval N (%) N Eval N (%)
Number of cases 1772 203 88Number of centers 48 29 19Age, median (range), years 1772 49 (<1‐75) 203 51 (<1‐77) 88 46 (<1‐74)Age at transplant 1772 203 88
< 10 y 167 ( 9) 8 ( 4) 9 (10)10‐20 y 159 ( 9) 10 ( 5) 7 ( 8)20‐29 y 139 ( 8) 25 (12) 6 ( 7)30‐39 y 154 ( 9) 19 ( 9) 8 ( 9)40‐49 y 291 (16) 34 (17) 25 (28)≥ 50 y 862 (49) 107 (53) 33 (38)
Male sex 1772 1030 (58) 203 123 (61) 88 52 (59)Karnofsky prior to transplant > 90% 234 157 (67) 28 17 (61) 11 9 (82)Disease status at transplant 1772 203 88 Early 132 ( 7) 17 ( 8) 5 ( 6) Intermediate 5 (<1) 1 (<1) 0 Advanced 32 ( 2) 3 ( 1) 3 ( 3) Non‐malignant disease/Other 1603 (90) 182 (90) 80 (91)Graft type 1772 203 88
Bone marrow 422 (24) 28 (14) 21 (24)Peripheral blood 1338 (76) 168 (83) 65 (74)Cord blood 4 (<1) 4 ( 2) 1 ( 1)Other 8 (<1) 3 ( 1) 1 ( 1)
Conditioning regimen 1772 203 88 Myeloablative 333 (19) 60 (30) 18 (20)Reduced intensity 105 ( 6) 9 ( 4) 5 ( 6)Nonmyeloablative 68 ( 4) 13 ( 6) 4 ( 5)Other/To be determined 1266 (71) 121 (60) 61 (69)
Donor age, median (range), years 1772 49 (<1‐81) 203 48 (<1‐68) 88 51 (9‐73)Donor age 1772 203 88
< 20 36 ( 2) 3 ( 1) 3 ( 3)20‐29 22 ( 1) 3 ( 1) 030‐39 32 ( 2) 3 ( 1) 1 ( 1)40‐49 44 ( 2) 5 ( 2) 1 ( 1)≥ 50 120 ( 7) 13 ( 6) 6 ( 7)Unknown/TBD 1518 (86) 176 (87) 77 (88)
38
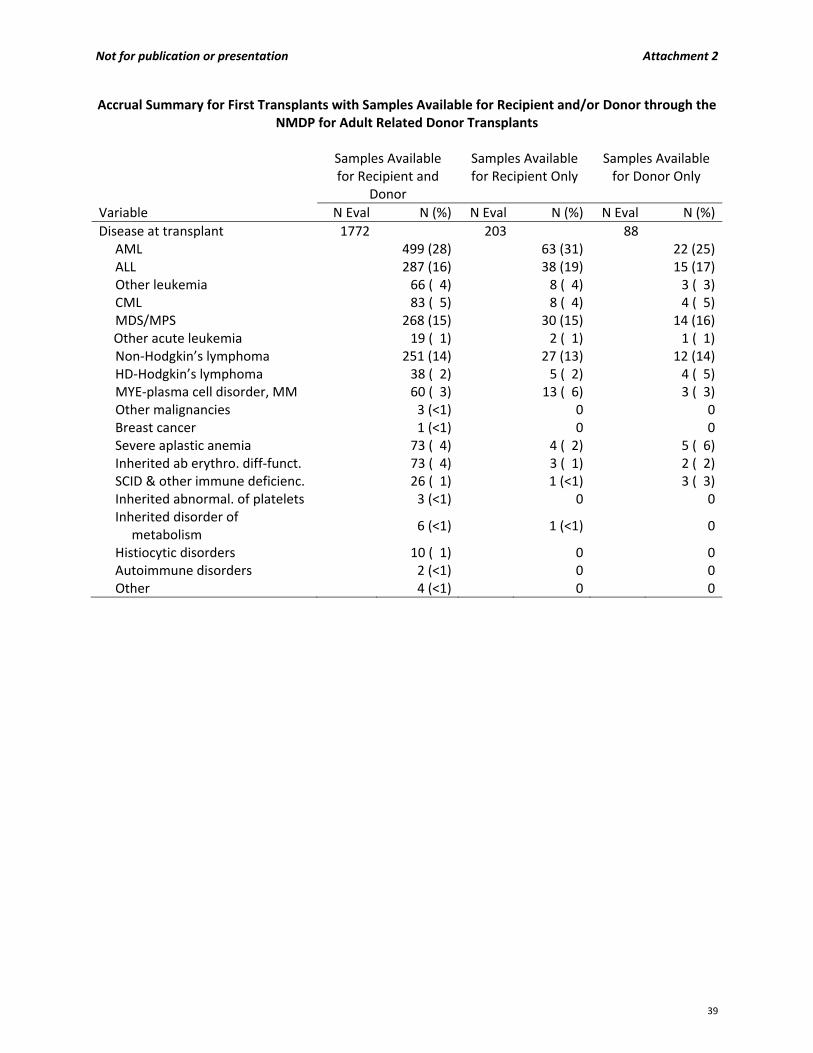
Not for publication or presentation Attachment 2
Accrual Summary for First Transplants with Samples Available for Recipient and/or Donor through the NMDP for Adult Related Donor Transplants
Samples Available
for Recipient and Donor
Samples Available for Recipient Only
Samples Available for Donor Only
Variable N Eval N (%) N Eval N (%) N Eval N (%)
Disease at transplant 1772 203 88 AML 499 (28) 63 (31) 22 (25) ALL 287 (16) 38 (19) 15 (17) Other leukemia 66 ( 4) 8 ( 4) 3 ( 3) CML 83 ( 5) 8 ( 4) 4 ( 5) MDS/MPS 268 (15) 30 (15) 14 (16)
Other acute leukemia 19 ( 1) 2 ( 1) 1 ( 1) Non‐Hodgkin’s lymphoma 251 (14) 27 (13) 12 (14) HD‐Hodgkin’s lymphoma 38 ( 2) 5 ( 2) 4 ( 5) MYE‐plasma cell disorder, MM 60 ( 3) 13 ( 6) 3 ( 3) Other malignancies 3 (<1) 0 0 Breast cancer 1 (<1) 0 0 Severe aplastic anemia 73 ( 4) 4 ( 2) 5 ( 6) Inherited ab erythro. diff‐funct. 73 ( 4) 3 ( 1) 2 ( 2) SCID & other immune deficienc. 26 ( 1) 1 (<1) 3 ( 3) Inherited abnormal. of platelets 3 (<1) 0 0 Inherited disorder of
metabolism 6 (<1) 1 (<1) 0
Histiocytic disorders 10 ( 1) 0 0 Autoimmune disorders 2 (<1) 0 0 Other 4 (<1) 0 0
39

Not for publication or presentation Attachment 2
Accrual Summary for First Transplants with Samples Available for Recipient and/or Donor through the NMDP for Adult Related Donor Transplants
Samples Available for
Recipient and Donor Samples Available for
Recipient Only Samples Available for
Donor Only
Variable N Eval N (%) N Eval N (%) N Eval N (%)
GVHD prophylaxis 1772 203 88 Ex vivo T‐cell depletion alone 7 (<1) 2 ( 1) 1 ( 1)Ex vivo T‐cell depletion + post‐tx immune suppression
2 (<1)
1 (<1)
0
CD34 selection alone 7 (<1) 0 0CD34 selection + post‐tx immune suppression
3 (<1)
0
1 ( 1)
Cyclophosphamide alone 1 (<1) 0 0Cyclophosphamide + others 36 ( 2) 3 ( 1) 3 ( 3)FK506 + MMF +‐ others 231 (13) 9 ( 4) 5 ( 6)FK506 + MTX +‐ others (except MMF)
866 (49)
69 (34)
37 (42)
FK506 + others (except MTX, MMF)
203 (11)
68 (33)
18 (20)
FK506 alone 12 ( 1) 0 0CSA + MMF +‐ others (except FK506)
45 ( 3)
7 ( 3)
2 ( 2)
CSA + MTX +‐ others (except FK506, MMF)
125 ( 7)
10 ( 5)
10 (11)
CSA + others (except FK506, MTX, MMF)
24 ( 1)
3 ( 1)
1 ( 1)
CSA alone 21 ( 1) 1 (<1) 1 ( 1)Other GVHD prophylaxis 189 (11) 30 (15) 9 (10)
Donor/recipient sex match 249 27 11 Male/Male 86 (35) 13 (48) 3 (27)Male/Female 52 (21) 4 (15) 4 (36)Female/Male 63 (25) 4 (15) 3 (27)Female/Female 48 (19) 6 (22) 1 ( 9)
Donor/recipient CMV match 1772 203 88 Negative/Negative 317 (18) 31 (15) 9 (10)Negative/Positive 366 (21) 34 (17) 18 (20)Positive/Negative 173 (10) 21 (10) 7 ( 8)Positive/Positive 719 (41) 90 (44) 44 (50)Unknown 197 (11) 27 (13) 10 (11)
Year of transplant 1735 198 87 2007 17 ( 1) 1 (<1) 02008 120 ( 7) 8 ( 4) 5 ( 6)2009 174 (10) 15 ( 7) 8 ( 9)2010 225 (13) 27 (13) 11 (13)2011 335 (19) 43 (21) 20 (23)2012 466 (26) 51 (25) 26 (30)2013 398 (22) 53 (26) 17 (19)
Median follow‐up of recipients, mo 670 16 (2‐85) 77 12 (3‐54) 38 12 (6‐24)
40
Not for publication or presentation Attachment 3
Study Proposal 1303‐04/1312‐08 Study Title: The prognostic impact of somatic point mutations and CXC chemokine ligand expression in patients with myelodysplastic syndromes (MDS) undergoing allogeneic hematopoietic stem cell transplantation (HSCT). PI Information: R. Coleman Lindsley, MD, PhD, Dana‐Farber Cancer Institute, Boston, Massachusetts Benjamin L. Ebert, MD, PhD, Brigham and Women’s Hospital, Boston, Massachusetts Wael Saber, MD, MS, Medical College of Wisconsin, Milwaukee, WI Specific Aims: 1. Determine the spectrum and clinical effect of acquired genetic abnormalities in a cohort of 1393
adult and pediatric MDS patients who have undergone allogeneic HSCT.
Identify mutations in a panel of 120 genes, including 70 genes that are recurrently mutated in myeloid malignancies and 50 genes that are mutated in inherited and acquired bone marrow failure syndromes.
Identify associations between point mutations and clinicopathologic features, including IPSS score, bone marrow blast percentage, peripheral blood cytopenias, karyotype, age, prior exposure to leukemogenic therapy, and disease status at time of transplantation.
Identify associations between point mutations and post‐transplant clinical outcomes, including disease progression or relapse, progression‐free survival, non‐relapse mortality, and overall survival.
Completion of Specific Aim 1 will achieve two central goals. First, MDS samples from the CIBMTR will be annotated with mutation status for the full spectrum of point mutations in MDS, enabling current and future investigators to explore the relationship between genetic lesions and clinical phenotype. Second, the association of mutations with clinical outcomes can validate and extend our previous analysis, potentially culminating in practice‐changing findings with regard to the use of genetics to guide clinical transplant decisions.
2. Determine the level and prognostic value of CXCL4 and CXCL7 expression in pre‐HCT serum from 500
adult MDS patients.
Determine the level of CXCL4 or CXCL7 in pre‐transplant serum samples from 500 adults MDS patients who have undergone allogeneic‐HCT.
Identify associations between pre‐HCT chemokine (CXCL4 or CXCL7) expression and post‐HCT clinical outcomes, including disease progression or relapse, progression‐free survival, non‐relapse mortality, and overall survival.
Exploratory Aim ‐ Identify associations between pre‐HCT chemokine (CXCL4 or CXCL7) expression and genetically‐defined risk groups defined in Aim 1.
Scientific Justification: Myelodysplastic syndrome (MDS) is a heterogeneous collection of clonal stem cell disorders unified by an inexorable progression to overt bone marrow failure or acute myeloid leukemia (AML). Without therapy, MDS is uniformly progressive and the prognosis of higher risk patients is poor. Despite recent advances in medical management of MDS, allogeneic HSCT remains the only therapeutic intervention
41

Not for publication or presentation Attachment 3
with curative potential. However, cumulative mortality after HSCT is high, approaching 60‐70% at five years, with most deaths attributable to relapsed disease or transplant‐related complications.1,2 Predicting which patients are likely to benefit from HSCT is thus a central challenge in clinical transplantation. Decision analyses suggest that there is an inflection point in the natural history of MDS where the benefits of transplantation outweigh its risks.3‐6 Even so, clinical decisions regarding the timing of HSCT remain complex and are influenced by a variety of factors related to the disease, the patient, and the transplant itself. Disease‐intrinsic risk is estimated based on existing prognostic risk models such as the International Prognostic Scoring System (IPSS) and the WHO Classification‐Based Prognostic Scoring System (WPSS).4,7 Disease‐extrinsic risk is influenced by a range of variables, including age,8‐10 serum ferritin level,11 donor cell source,12 and comorbidity score.13,14 Despite the development of finely wrought diagnostic and prognostic schema, however, substantial clinical heterogeneity remains within current MDS classification systems. Now, with the extensive characterization of the landscape of recurrent somatic alterations in MDS, a central role has been revealed for specific mutations in driving diverse clinical and hematologic phenotypes.15 For example, we demonstrated that mutations in ASXL1, TP53, ETV6, EZH2, and RUNX1 are powerful predictors of survival, independent of IPSS and other clinical risk variables.16,17 However, MDS patients who undergo HSCT are poorly represented in this and other MDS genetic analyses and it is not know whether these results are generalizable to the transplant context. Indeed, based on the immunologic mechanism of HSCT, we hypothesize that there is a distinctive spectrum of mutations that predict outcomes after HSCT. The bone marrow niche is an important regulator of normal and neoplastic hematopoiesis, perhaps independently of disease‐intrinsic genetics.18‐20 This complex microenvironment is comprised of varied constituents, including specialized cellular compartments, secreted factors, and autonomic nervous system innervation. In the context of MDS, the dynamic relationship between disease clone and its microenvironmental context is poorly understood, particularly as it relates to clinical outcomes with different treatment strategies. Several recent studies have evaluated the MDS proteome in specific clinicopathologic contexts. 21‐24 Using surface‐enhanced laser desorption/ionization (SELDI)‐TOF‐MS, Aivado et al. identified an MDS‐specific proteome profile capable of differentiating MDS patients from normal individuals and individuals with non‐MDS cytopenias.25 Further analysis using peptide mass fingerprinting and quadrupole time‐of‐flight MS demonstrated an MDS‐specific reduction in levels of the chemokines CXCL4 and CXCL7. This reduction was especially pronounced in patients with refractory anemia with excess blasts (RAEB) and refractory anemia with excess blasts in transformation (RAEB‐T), indicating that these biomarkers could be used as markers of severity of the underlying MDS. Indeed, recent findings have implicated specific chemokine interactions, including CXCL4, in regulating stem cell quiescence,26 suggesting that reduced chemokine expression may be an important step in the pathobiology of MDS disease progression. We hypothesize that identification patients with aberrant reduction of chemokine levels will highlight a group of MDS patients with adverse post‐HCT outcomes. Preliminary Data: To test the hypothesis that specific point mutations can predict outcomes after allogeneic HSCT for MDS, we surveyed for mutations in 40 recurrently affected MDS genes in pre‐transplant samples collected from 72 patients (Bejar, Lindsley, and Ebert; JCO in revision). We identified mutations in 35 of
42

Not for publication or presentation Attachment 3
the 40 genes, one or more of which were present in 85% of samples (Figure 1A). Mutations in several genes associated with higher risk MDS were more prevalent in this cohort than in previously reported MDS patient populations, including ASXL1 (29%), TP53 (19%), DNMT3A (19%), and RUNX1 (17%), while mutations in TET2 (8%) and SF3B1 (10%) were relatively underrepresented. In multivariable analysis of overall survival including clinical variables, mutations of TP53 (HR=3.29, p = 0.002) and DNMT3A (HR=2.59, p = 0.026) were each independently associated with shorter overall survival and mutations in one of these two genes were identified in 36% of patients. Three‐year overall survival in patients with TP53 or DNMT3A mutations was 19% [95% CI 7‐36%] vs. 67% [95% CI 51‐78%] in those without these mutations (Figure 1B).
Clinical Relevance: The proposed studies will provide a comprehensive CIBMTR resource that will facilitate a range of retrospective studies and drive clinical investigation aimed at improving HSCT outcomes in MDS patients. Specifically, we expect the results to enable development of a transplant‐specific MDS genetic prognostic model that may be integrated into clinical decision‐making regarding HSCT timing and patient selection. Further, identification of a cohort of high‐risk MDS patients may provoke development of alternative approaches to conditioning (novel regimens, altered intensity, genotype‐directed therapies, etc.), post‐transplant relapse prevention, or stratification to “minimize toxicity” versus “maximize efficacy” transplantation strategies. Patient Eligibility Population: We propose to perform a comprehensive analysis of all MDS patients with appropriate samples available in the NMDP Research Sample Repository, without restriction by age or specific transplant variables. To ensure adequate clinical follow‐up and to focus on patients treated with contemporary transplant approaches, we will limit the years of transplant to 2005‐2011. With the assistance of CIBMTR biostatisticians, we have identified a large cohort of patients meeting these basic criteria (Table 1). Data Requirements: No supplemental data collection is required for this study.
D. Other&muta*on&(n&=&46)&DNMT3A'&or&TP53&muta*on&present&(n=26)'
Months'
Probab
ility&of&Overall&Survival&
A. B.
Figure 1: Spectrum and clinical significance of point mutations in MDS patients undergoing allogeneic HSCT. (A) Distribution of mutations in selected MDS associated genes. Each column represents an individual patient sample and each colored cell represents a mutation of the gene or gene group listed to left of that row. The number of mutations for each row is indicated in the column to the right. (B) Overall survival of patients with either TP53 or DNMT3A mutation compared with patients having neither abnormality.
43

Not for publication or presentation Attachment 3
Sample Requirements: Overview of sample processing and handling: This study relies on two distinctive features of MDS. First, at the time of transplantation, patients with MDS typically have active disease, as reflected by the presence of detectable myeloid driver mutations in at least 85% of pre‐conditioning samples (Bejar, Lindsley, and Ebert, JCO in revision). Second, we and others have demonstrated that there is high concordance between molecular genetic alterations detected in bone marrow and those detected in peripheral blood.27,28 As such, we request pre‐HSCT whole peripheral blood samples, in the form of cell pellets or viably frozen cells. Study samples will be submitted to the Biological Samples Platform (BSP) at the Broad Institute, where DNA will be extracted, quantitated using PicoGreen, 2D barcoded, and stored at ‐80C for subsequent, on‐demand plating using automated retrieval technology. For large sample sets, this approach is critical for ensuring accurate sample tracking and database management. Overview of genetic analysis: For the proposed studies, we will utilize a next‐generation sequencing platform designed and validated by the PIs, and a robust analysis pipeline developed in collaboration with the Sequencing Platform at the Broad Institute. Development of a hybrid capture sequencing panel for myeloid malignancies: Since there are a large number of genes that are recurrently mutated in myeloid malignancies, we sought to develop a cost‐ and time‐effective method to examine large numbers of patients for a focused, yet comprehensive panel of relevant disease genes. Systematic screening for by PCR and Sanger sequencing is prohibitively expensive and labor intensive. We have therefore developed a custom DNA capture panel specifically targeting all known and candidate myeloid disease genes based on our survey of existing, publicly available data from unbiased sequencing studies. The most recent version of our panel evaluates the relevant exons and splice junctions of a total of 120 genes, including 70 genes implicated in myeloid malignancies as well as 50 additional genes associated with inherited and acquired bone marrow failure syndromes (Table 2). Importantly, this platform is dynamic and we maintain the flexibility to modify the gene list based on emerging data or to suit the evolving needs of specific projects and hypotheses. To increase throughput and reduce cost, we tested whether up to 48 samples could be molecularly barcoded, mixed together, and then captured as one pool. In multiple previous studies, data obtained from a single Illumina HiSeq2000 lane generated deep sequence coverage for all samples with a mean coverage >200x. Over 95.8% of targeted bases had greater than 40x sequence coverage, which is sufficient for identification of heterozygous mutant alleles with high sensitivity and specificity. More importantly, the levels of coverage of each of the samples are very similar, indicating uniformity of library preparation and capture in all samples of the pool. We have used this specific platform to analyze more than 1000 samples from patients with myeloid malignancies, including MDS, AML, myeloproliferative neoplasms, and bone marrow failure syndromes. Hybrid Capture using the Agilent Custom SureSelect platform: We will prepare pooled, barcoded libraries from tumor samples, perform liquid phase capture using probes designed against all known MDS and bone marrow failure genes, and perform deep sequencing on the Illumina platform. All sequencing will be performed at the Broad Institute of MIT and Harvard University. Initial data processing will be performed at the Broad Institute, with subsequent analysis by the PIs in the Ebert laboratory using algorithms developed by colleagues at the Broad Institute. Data analysis: We will utilize the sequencing data processing pipeline developed by the Sequencing Platform at the Broad Institute. This platform analyzes reads and quality scores produced by the Illumina
44
Not for publication or presentation Attachment 3
software for each sample and produces, at the end of the pipeline, a single BAM file representing the sample. The final BAM file stores all reads with well‐calibrated qualities together with their alignments to the genome. Using the Broad Cancer Genome Analysis pipeline (Firehose), BAM files are subjected to various analyses, including quality control, local realignment, mutation calling (MuTect), small insertion and deletion identification (Indelocator), coverage calculations, tandem duplication detection (Pindel), and others. Passing single nucleotide variants found within coding areas of the genome are annotated for the chromosomal location, the type of variant, the codon change, and the change in the amino acid sequence (Annovar). The details of these sequencing data processing techniques have been described previously.29‐31 Determining significance of individual variants: In the absence of germline tissue, ascertainment of the somatic status of some variants can be challenging. In prior studies where germline control tissue is unavailable, we have utilized strict filtering criteria aimed at efficiently stratifying variants based on known or suspected somatic status. We will annotate samples as oncogenic if they meet any of the following criteria: (1) Known oncogenic variants, confirmed as somatic in the literature, (2) recurrent variants, not present in SNP databases, that are detected in well‐characterized myeloid disease genes, and (3) truncating mutations (nonsense, splice site, frameshift insertion/deletions) in myeloid tumor suppressor genes. All other variants will be annotated and included in supplementary materials for independent validation and subsequent re‐analysis as additional genetic data are reported in the literature. Previous experience with the proposed sequencing methodology: The principal investigators (Lindsley and Ebert) have extensive experience in the field of myeloid genomics. We have designed and implemented clinical and research‐based sequencing platforms at the Dana‐Farber Cancer Institute and the Broad Institute. Using the proposed sequencing platform and other related sequencing platforms, we have analyzed more than 1500 samples from patients with myeloid malignancies (Lindsley and Ebert, in preparation; Bejar, Lindsley, and Ebert, JCO in revision; Bejar and Ebert, NEJM 2011, Bejar and Ebert, JCO 2012). The PIs (Lindsley and Ebert) are both members of the International Working Group for Prognosis of MDS (IWG‐PM) molecular subcommittee (chaired by Dr. Ebert). The IWG‐PM recently established the refined consensus system for estimating prognosis in MDS (IPSS‐R), based on aggregation of data from more than 7000 patients in 18 databases.32 The IWG‐PM molecular subcommittee was formed in recognition of the importance of molecular genetic alterations in driving clinical phenotypes in MDS and will generate a novel prognostic model that incorporates molecular genetic alterations, based on comprehensive sequencing of 4000‐5000 MDS patients who have not received disease modifying therapy, including HSCT. The PIs (Lindsley and Ebert) as well as key collaborators (Bejar and Neuberg) are integral to this international effort and will contribute to the aggregation and analysis of existing and new sequencing data. Of note, the proposed CIBMTR analysis will be conducted outside the auspices of the IWG‐PM. Overview of proteome analysis: Using commercially available ELISA kits (http://www.abcam.com/PF4‐Human‐ELISA‐Kit‐1‐x‐96‐Well‐Plate‐ab100628; http://www.abcam.com/CXCL7‐Human‐ELISA‐Kit‐1‐x‐96‐Well‐Plate‐ab100613.html), will measure the plasma levels of CXCL4 and CXCL7. Abcam’s Human CXCL4 and CXCL7 ELISA (Enzyme‐Linked Immunosorbent Assay) kits are the in vitro enzyme‐linked immunosorbent assay for the quantitative measurement of Human CXCL4 and CXCL7 in serum, plasma, and cell culture supernatants. The assay employs an antibody specific for Human CXCL4
45
Not for publication or presentation Attachment 3
or CXCL7 coated on a 96‐well plate. Standards and samples are pipetted into the wells and CXCL4 or CXCL7 present in a sample is bound to the wells by the immobilized antibody. The wells are washed and biotinylated anti‐Human CXCL4 or CXCL7 antibody is added. After washing away unbound biotinylated antibody, HRP‐conjugated streptavidin is pipetted to the wells. The wells are again washed, a TMB substrate solution is added to the wells and color develops in proportion to the amount of CXCL4 or CXCL7 bound. The Stop Solution changes the color from blue to yellow, and the intensity of the color is measured at 450 nm. To determine CXCL4 or CXCL7 concentrations, mean absorbance for each set of duplicate standards, controls and samples is calculated, and the average zero standard optical density is subtracted. Plot the standard curve using the Prism program and the concentrations of CXCL4 or CXCL7 will be determined based on the standard curve. Sample size estimate: In a study of 250 patients, CXCL4 and CXCL7 levels were found to be suppressed in patients with advanced MDS (RAEB and RAEB‐T).25 The WPSS, which was developed in a cohort of 426 cases, depends on the WHO morphologic classification.33 In this system (the only validated time‐dependent system for MDS), advanced stages were at significantly higher risk for death or leukemic transformation. Therefore, we propose that we analyze samples from 500 MDS cases to evaluate whether low chemokines levels are associated with worse post allogeneic HCT survival. Previous experience with the proposed proteomics methodology: This work will be undertaken in collaboration with Dr. Carolyn Taylor, Ph.D. Link to Dr. Taylor’s website: http://www.mcw.edu/Hemonc/faculty/carolynkeevertaylor.htm Outcomes: Primary outcome:
Overall‐survival (OS) ‐ OS will be calculated from the date of transplant to the date of death, and surviving patients will be censored at the date on which the patient was last known to be alive.
Secondary outcomes:
Relapse and Disease Progression
Progression‐free Survival
Non‐Relapse Mortality All secondary outcomes will be calculated from the time of transplantation, and will be censored at the last date known alive and progression‐free. Statistical analyses: Curves will be constructed for OS and PFS using the method of Kaplan and Meier and compared using a log rank test. Cox models will be constructed to adjust for clinical and transplant characteristics. Factors to be included in the Cox models include:
Donor and Recipient Age
Donor and Recipient Gender
HLA Match
Donor Type: Related, Unrelated
IPSS score (or individual components)
WPSS score at HCT (in the model evaluating chemokine levels)
46
Not for publication or presentation Attachment 3
Conditioning intensity (Myeloablative / Reduced Intensity / Nonmyeloablative)
T cell Depletion and GVHD Prophylaxis
Prior exposure to leukemogenic therapy
Others A time‐dependent variable for the interaction between mutation status and the natural log of time will also be included in these models to test the proportional hazard assumption. Associations of continuous measures between groups will be assessed using a Wilcoxon rank‐sum test and for categorical variables will be assessed using a Fisher exact test. References:
1. Sockel K, Platzbecker U. When to Transplant MDS, and What to Do When Transplant Fails. Curr Hematol Malig Rep 2013.
2. Vaughn JE, Scott BL, Deeg HJ. Transplantation for myelodysplastic syndromes 2013. Curr Opin Hematol 2013;20(6):494–500.
3. Cutler CS, Lee SJ, Greenberg P et al. A decision analysis of allogeneic bone marrow transplantation for the myelodysplastic syndromes: delayed transplantation for low‐risk myelodysplasia is associated with improved outcome. Blood 2004;104(2):579–585.
4. Alessandrino EP, Porta MGD, Malcovati L et al. Optimal timing of allogeneic hematopoietic stem cell transplantation in patients with myelodysplastic syndrome. Am J Hematol 2013.
5. Abel GA, Koreth J. Optimal positioning of hematopoietic stem cell transplantation for older patients with myelodysplastic syndromes. Curr Opin Hematol 2013.
6. Alessandrino EP, Porta Della MG, Bacigalupo A et al. WHO classification and WPSS predict posttransplantation outcome in patients with myelodysplastic syndrome: a study from the Gruppo Italiano Trapianto di Midollo Osseo (GITMO). Blood 2008;112(3):895–902.
7. Deeg HJ, Storer B, Slattery JT et al. Conditioning with targeted busulfan and cyclophosphamide for hemopoietic stem cell transplantation from related and unrelated donors in patients with myelodysplastic syndrome. Blood 2002;100(4):1201–1207.
8. Gómez‐Núñez M, Martino R, Caballero MD et al. Elderly age and prior autologous transplantation have a deleterious effect on survival following allogeneic peripheral blood stem cell transplantation with reduced‐intensity conditioning: results from the Spanish multicenter prospective trial. Bone Marrow Transplant 2004;33(5):477–482.
9. Anderson JE, Appelbaum FR, Schoch G et al. Allogeneic marrow transplantation for refractory anemia: a comparison of two preparative regimens and analysis of prognostic factors. Blood 1996;87(1):51–58.
10. Ringdén O, Horowitz MM, Gale RP et al. Outcome after allogeneic bone marrow transplant for leukemia in older adults. JAMA: The Journal of the American Medical Association 1993;270(1):57–60.
11. Armand P, Kim HT, Cutler CS et al. Prognostic impact of elevated pretransplantation serum ferritin in patients undergoing myeloablative stem cell transplantation. Blood 2007;109(10):4586–4588.
12. Saber W, Cutler CS, Nakamura R et al. Impact of donor source on hematopoietic cell transplantation outcomes for patients with myelodysplastic syndromes (MDS). Blood 2013;122(11):1974–1982.
13. Sorror ML, Sandmaier BM, Storer BE et al. Comorbidity and disease status based risk stratification of outcomes among patients with acute myeloid leukemia or myelodysplasia receiving allogeneic hematopoietic cell transplantation. J Clin Oncol 2007;25(27):4246–4254.
14. Sorror ML. How I assess comorbidities prior to hematopoietic cell transplantation. Blood. 2013.
47

Not for publication or presentation Attachment 3
15. Lindsley RC, Ebert BL. Molecular pathophysiology of myelodysplastic syndromes. Annu Rev Pathol 2013;8:21–47.
16. Bejar R, Stevenson K, Abdel‐Wahab O et al. Clinical effect of point mutations in myelodysplastic syndromes. N Engl J Med 2011;364(26):2496–2506.
17. Bejar R, Stevenson KE, Caughey BA et al. Validation of a prognostic model and the impact of mutations in patients with lower‐risk myelodysplastic syndromes. J Clin Oncol 2012;30(27):3376–3382.
18. Yusuf RZ, Wang Y‐H, Scadden DT. The secrets of the bone marrow niche: Metabolic priming for AML. Nat Med 2012;18(6):865–867.
19. Krause DS, Fulzele K, Catic A et al. Differential regulation of myeloid leukemias by the bone marrow microenvironment. Nat Med 2013;19(11):1513–1517.
20. Fujisaki J, Wu J, Carlson AL et al. In vivo imaging of Treg cells providing immune privilege to the haematopoietic stem‐cell niche. Nature 2011;474(7350):216–219.
21. Májek P, Riedelová‐Reicheltová Z, Suttnar J et al. Plasma proteome changes associated with refractory anemia and refractory anemia with ringed sideroblasts in patients with myelodysplastic syndrome. Proteome Sci 2013;11(1):14.
22. Májek P, Reicheltová Z, Suttnar J et al. Plasma proteome changes associated with refractory cytopenia with multilineage dysplasia. Proteome Sci 2011;9:64.
23. Chen C, Bowen DT, Giagounidis AAN et al. Identification of disease‐ and therapy‐associated proteome changes in the sera of patients with myelodysplastic syndromes and del(5q). Leukemia 2010;24(11):1875–1884.
24. Braoudaki M, Tzortzatou‐Stathopoulou F, Anagnostopoulos AK et al. Proteomic analysis of childhood de novo acute myeloid leukemia and myelodysplastic syndrome/AML: correlation to molecular and cytogenetic analyses. Amino Acids 2011;40(3):943–951.
25. Aivado M, Spentzos D, Germing U et al. Serum proteome profiling detects myelodysplastic syndromes and identifies CXC chemokine ligands 4 and 7 as markers for advanced disease. Proc. Natl Acad Sci USA 2007;104(4):1307–1312.
26. Lucas D, Pinho S, Ahmed J et al. Megakaryocytes Regulate Hematopoietic Stem Cell Quiescence Via PF4 Secretion. Blood 2013;122(21):3–3.
27. Papaemmanuil E, Gerstung M, Malcovati L et al. Clinical and biological implications of driver mutations in myelodysplastic syndromes. Blood 2013.
28. Mohamedali AM, Alkhatabi H, Kulasekararaj A et al. Utility of peripheral blood for cytogenetic and mutation analysis in myelodysplastic syndrome. Blood 2013;122(4):567–570.
29. Ye K, Schulz MH, Long Q, Apweiler R et al. Pindel: a pattern growth approach to detect break points of large deletions and medium sized insertions from paired‐end short reads. Bioinformatics 2009;25(21):2865–2871.
30. Carter SL, Cibulskis K, Helman E et al. Absolute quantification of somatic DNA alterations in human cancer. Nat Biotechnol 2012;30(5):413–421.
31. Wang L, Lawrence MS, Wan Y et al. SF3B1 and other novel cancer genes in chronic lymphocytic leukemia. N Engl J Med 2011;365(26):2497–2506.
32. Greenberg PL, Tuechler H, Schanz J et al. Revised international prognostic scoring system for myelodysplastic syndromes. Blood 2012;120(12):2454–2465.
33. Malcovati L, Germing U, Kuendgen A et al. Time‐dependent prognostic scoring system for predicting survival and leukemic evolution in myelodysplastic syndromes. J Clin Oncol 2007;25(23):3503–3510.
48
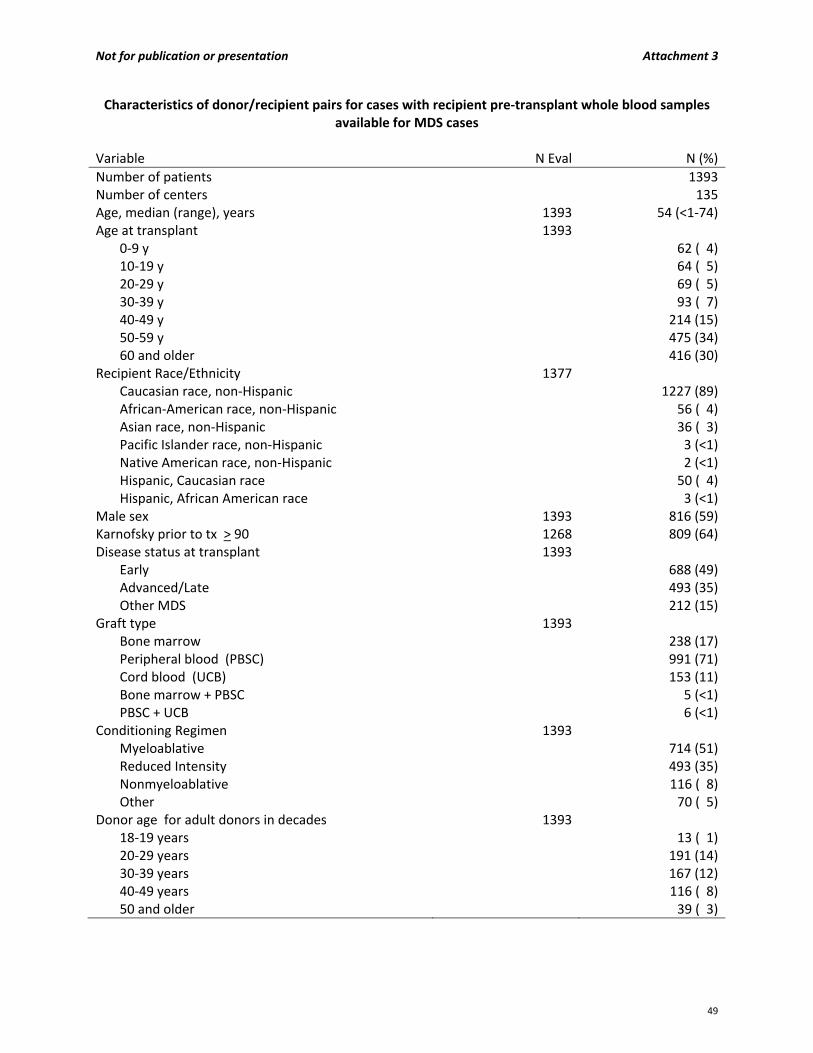
Not for publication or presentation Attachment 3
Characteristics of donor/recipient pairs for cases with recipient pre‐transplant whole blood samples available for MDS cases
Variable N Eval N (%)
Number of patients 1393Number of centers 135Age, median (range), years 1393 54 (<1‐74)Age at transplant 1393
0‐9 y 62 ( 4)10‐19 y 64 ( 5)20‐29 y 69 ( 5)30‐39 y 93 ( 7)40‐49 y 214 (15)50‐59 y 475 (34)60 and older 416 (30)
Recipient Race/Ethnicity 1377 Caucasian race, non‐Hispanic 1227 (89)African‐American race, non‐Hispanic 56 ( 4)Asian race, non‐Hispanic 36 ( 3)Pacific Islander race, non‐Hispanic 3 (<1)Native American race, non‐Hispanic 2 (<1)Hispanic, Caucasian race 50 ( 4)Hispanic, African American race 3 (<1)
Male sex 1393 816 (59)Karnofsky prior to tx > 90 1268 809 (64)Disease status at transplant 1393
Early 688 (49)Advanced/Late 493 (35)Other MDS 212 (15)
Graft type 1393 Bone marrow 238 (17)Peripheral blood (PBSC) 991 (71)Cord blood (UCB) 153 (11)Bone marrow + PBSC 5 (<1)PBSC + UCB 6 (<1)
Conditioning Regimen 1393 Myeloablative 714 (51)Reduced Intensity 493 (35)Nonmyeloablative 116 ( 8)Other 70 ( 5)
Donor age for adult donors in decades 1393 18‐19 years 13 ( 1)20‐29 years 191 (14)30‐39 years 167 (12)40‐49 years 116 ( 8)50 and older 39 ( 3)
49
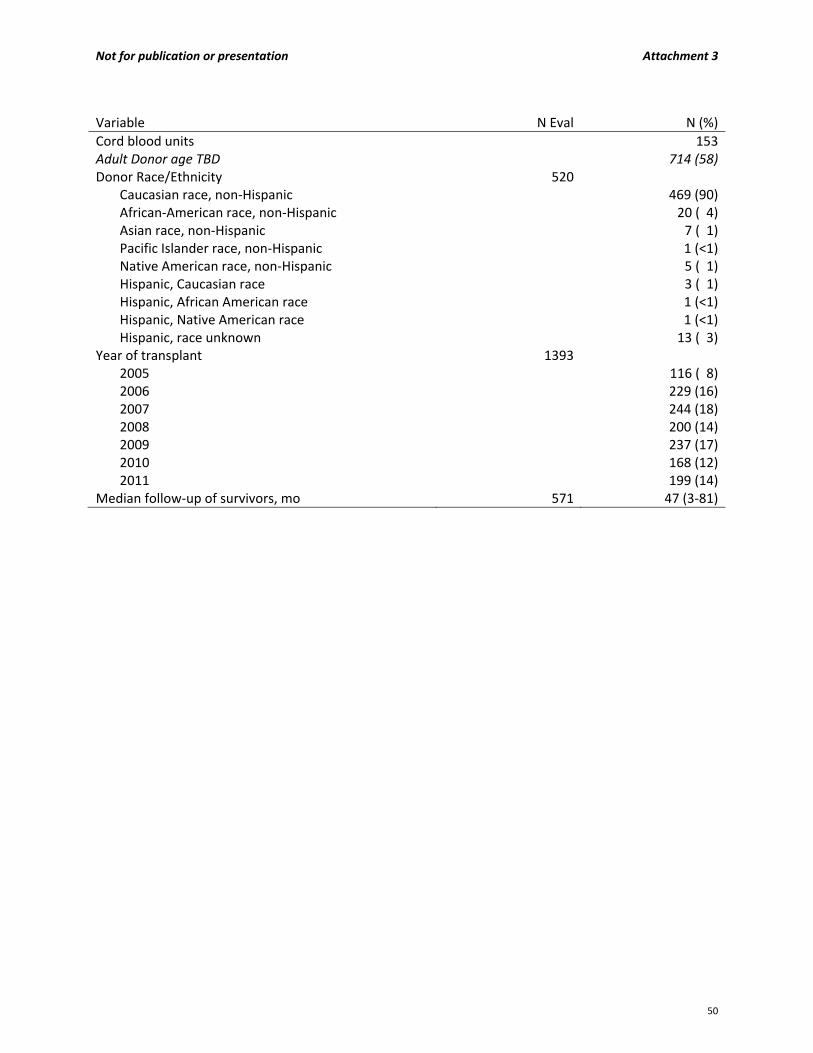
Not for publication or presentation Attachment 3
Variable N Eval N (%)
Cord blood units 153Adult Donor age TBD 714 (58)Donor Race/Ethnicity 520
Caucasian race, non‐Hispanic 469 (90)African‐American race, non‐Hispanic 20 ( 4)Asian race, non‐Hispanic 7 ( 1)Pacific Islander race, non‐Hispanic 1 (<1)Native American race, non‐Hispanic 5 ( 1)Hispanic, Caucasian race 3 ( 1)Hispanic, African American race 1 (<1)Hispanic, Native American race 1 (<1)Hispanic, race unknown 13 ( 3)
Year of transplant 1393 2005 116 ( 8)2006 229 (16)2007 244 (18)2008 200 (14)2009 237 (17)2010 168 (12)2011 199 (14)
Median follow‐up of survivors, mo 571 47 (3‐81)
50
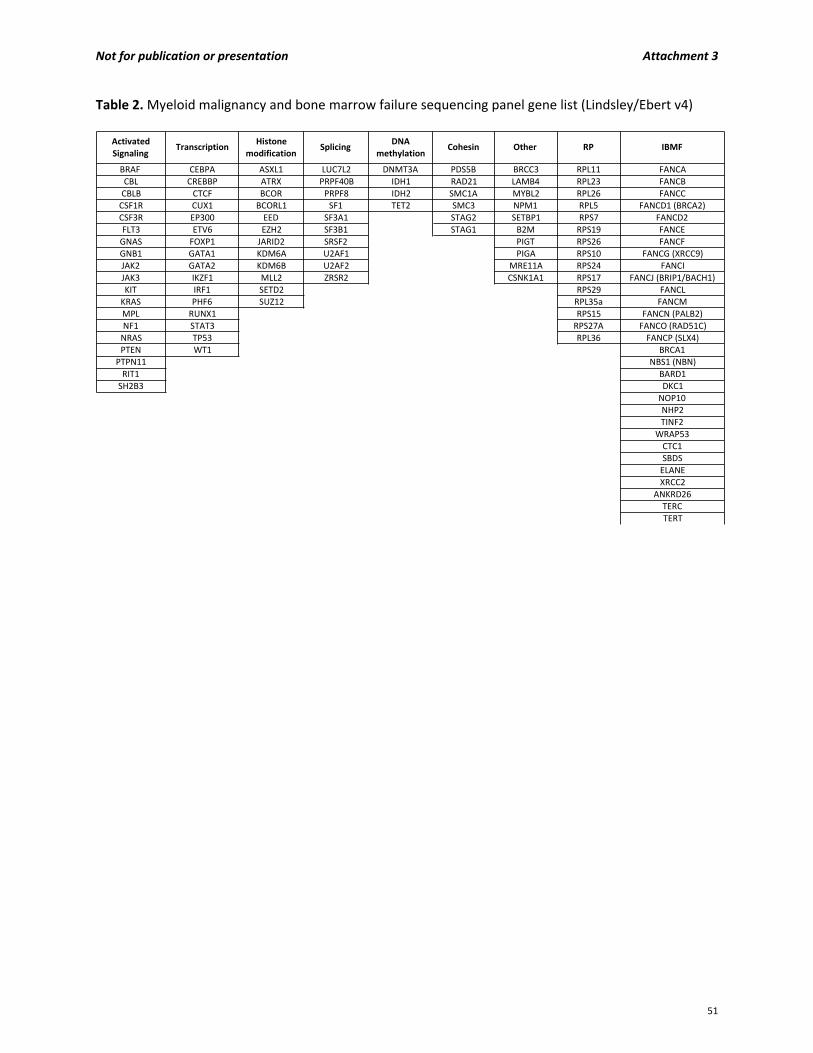
Not for publication or presentation Attachment 3
Table 2. Myeloid malignancy and bone marrow failure sequencing panel gene list (Lindsley/Ebert v4)
Activated Signaling
TranscriptionHistone
modificationSplicing
DNA methylation
Cohesin Other RP IBMF
BRAF CEBPA ASXL1 LUC7L2 DNMT3A PDS5B BRCC3 RPL11 FANCA
CBL CREBBP ATRX PRPF40B IDH1 RAD21 LAMB4 RPL23 FANCB
CBLB CTCF BCOR PRPF8 IDH2 SMC1A MYBL2 RPL26 FANCCCSF1R CUX1 BCORL1 SF1 TET2 SMC3 NPM1 RPL5 FANCD1 (BRCA2)CSF3R EP300 EED SF3A1 STAG2 SETBP1 RPS7 FANCD2
FLT3 ETV6 EZH2 SF3B1 STAG1 B2M RPS19 FANCE
GNAS FOXP1 JARID2 SRSF2 PIGT RPS26 FANCFGNB1 GATA1 KDM6A U2AF1 PIGA RPS10 FANCG (XRCC9)JAK2 GATA2 KDM6B U2AF2 MRE11A RPS24 FANCI
JAK3 IKZF1 MLL2 ZRSR2 CSNK1A1 RPS17 FANCJ (BRIP1/BACH1)KIT IRF1 SETD2 RPS29 FANCLKRAS PHF6 SUZ12 RPL35a FANCM
MPL RUNX1 RPS15 FANCN (PALB2)NF1 STAT3 RPS27A FANCO (RAD51C)NRAS TP53 RPL36 FANCP (SLX4)PTEN WT1 BRCA1
PTPN11 NBS1 (NBN)RIT1 BARD1
SH2B3 DKC1
NOP10NHP2
TINF2
WRAP53
CTC1SBDS
ELANE
XRCC2
ANKRD26TERC
TERT
51

Not for publication or presentation Attachment 4
Study Proposal 1309‐02 Study Title: Donor‐Specific anti HLA antibodies, Allele and Antigen level HLA mismatches in the outcomes of Transplantation of Non‐Malignant Diseases with Unrelated Donors PI Information: Marcelo A. Fernandez‐Vina, PhD, D(ABHI), Department of Pathology, Stanford University School of Medicine, Stanford, California Dolly B. Tyan, PhD, D(ABHI), Department of Pathology, Stanford University School of Medicine, Stanford, California Ann E. Woolfrey, MD, Fred Hutchinson Center Research Center, Seattle, Washington Specific Aims:
To investigate the impact of the presence of Donor Specific anti‐HLA Antibodies (DSA) in the patient's pre‐transplant serum specimens in the outcomes of nonmalignant disease transplants utilizing unrelated donors. Primary graft failure, graft failure and overall survival as end points
To determine is the impact of pre‐formed donor‐directed HLA‐specific depends on strength of the reactivity against donor antigens, on the number of HLA mismatched allo‐antibodies and in the ability of the DSA to fix complement
To evaluate if antigen and allele level mismatches associate differently in the outcomes of non‐malignant disease transplants utilizing unrelated donors. Primary graft failure, graft failure and overall survival as end points.
Scientific Justification: In a recent study conducted by Horan and colleagues the differences in the HLA alleles of patients and unrelated donors in hematopoietic stem cell transplantation (HSCT) for nonmalignant diseases result in increased risk for adverse treatment outcome.1 The nonmalignant disease cohort1 differs significantly from those examining HSCT for hematologic malignancies2 in age, conditioning regimens, and graft composition. In the nonmalignant disease study the incidence of graft failure was at least 2 to 3 times higher than in the cohorts of malignant diseases. In nonmalignant disease transplantation, many patient deaths (29.8%) were associated with graft failure. The multivariate analyses showed that the occurrence of a single or a double mismatch in HLA‐A, ‐B, ‐C, or DRB1 loci associated with graft failure2; HLA mismatches were also associated with mortality. The increased incidence of graft failure in nonmalignant disease transplantation may be caused by preserved or enhanced patient immune competence as they have not received chemotherapy prior to the preparative regimen. In the study by Horan et al the impact of preformed allo‐antibodies in the patients' serum that could react with the mismatched donor antigens (DSAs) was not evaluated. Other studies of HSCT in malignant diseases showed an association between DSA and primary graft failure (PGF).3,4 Typically, many nonmalignant disease patients have preserved or enhanced immune function and often receive blood transfusions; it is likely that in nonmalignant diseases the incidence of humoral HLA allo‐immunization may be even higher than in patients with hematologic malignancies. Therefore, in the nonmalignant disease HSCT setting, the presence of anti‐HLA donor antigens may be more significant in outcome by increasing the risk of PGF.
52

Not for publication or presentation Attachment 4
Previous studies5, 6 have shown that antigen level mismatches at HLA‐A and C associated with a significant delay in neutrophil engraftment; in contrast allele level mismatches at HLA‐A, B or C loci or mismatches in DRB1 did not associate significantly with this outcome. We propose to evaluate if antigen and allele level mismatches associate differently in NMD transplantation. Although humoral sensitization plays a significant role in graft rejection, the patient's T‐cell HLA allo‐reactivity may also cause graft failure. In HSCT for malignant diseases, 30% to 40% of PGFs present anti‐HLA antibodies reactive with the mismatched donor antigens.3,4 It can be argued that a significant proportion of the remaining PGF cases may have resulted from rejection mediated by patients' T‐cell lymphocytes. We propose to evaluate the impact of the different types of HLA mismatches in the full cohort of patients and in a subset of patient which serum was available for evaluation of anti‐HLA antibodies stratified according to the presence or absence of DSA. Study Population: Here we propose to investigate the impact of DSA in the outcome nonmalignant disease transplants utilizing unrelated donors. We propose to investigate the presence of anti HLA allo‐antibodies in the serum of all patients by solid phase assays utilizing single antigen bead preparations; the proposed assays include detection of IgG antibodies7 or complement fixing antibodies detected by the C1q8 binding assay. DSA will be assessed on the basis of reactivity against the donor's HLA mismatched antigens at all classical HLA antigens (A, B, C, DRB1, DRB3/4/5, DQA1, DQB1, DPA1 and DPB1). Anti MICA antibodies will also be evaluated; anti‐MICA DSA9 will be evaluated after typing MICA alleles in transplant pairs in which the patient's serum shows anti‐MICA reactivity. We propose to evaluate the effects of humoral sensitization, donor‐specific antibodies and HLA mismatches with primary graft failure, graft failure and overall survival as end points. Intensity of and of DSA by the IgG assay will be evaluated as a continuous variable and as a discontinuous variable classified as Negative (MFI<1,000), Weak Positive (MFI ranging 1,000‐5,000) and Strong Positive (MFI>5,000). Number of Positive DSA will also be scored in each patient. DSA by IgG and C1q assays will be scored in four categories: 1) Positive with both assays; 2) Positive by IgG and Negative by C1q assays; 3) Negative by IgG and Positive by C1q assays; 4) Negative by both assays. The effect of mismatch type in HLA‐A, B, C and DRB1 loci will be evaluated in the full cohort of patients. The frequencies of mismatch type HLA‐A, B, C and DRB1 loci will be evaluated in patients with and without DSA; similarly the frequencies of mismatches in DR and DP loci will be examined in patient groups stratified according to DSA. Variables to be Analyzed: Main effect:
Presence or absence of DSA
DSA determined by C1q and IgG assays; intensity, type and number of DSA
Type of HLA mismatches in HLA‐A, B, C, DRB1 loci
Confounding effect of HLA‐DP and DQ will be considered if numbers permit Patient related:
Age: continuous or in decades (0‐9, 10‐19, 20‐29, 30‐39, 40‐49, ≥ 50)
53
Not for publication or presentation Attachment 4
Race (White vs. Hispanic vs. Black vs. Other)
Karnofsky/Lansky score at transplant: < 90 vs. 90‐100 Disease related:
Disease at transplant: aplastic anemia, T cell immune deficiency (including SCID), hemoglobinopathies, metabolic disorder, other nonmalignant disorder (for the engraftment endpoints, patients will be categorized into 3 groups: T cell immune deficiency/SCID; aplastic anemia/hemoglobinopathy; other)
Time from diagnosis to transplant Transplant related:
Donor age: continuous or in 5 year increments
Year of transplant: in 3‐year increments
Gender match: M‐M vs. M‐F vs. F‐M vs. F‐F
Donor/recipient CMV status: ‐/‐ vs. ‐/+ vs. +/‐ vs. +/+ vs. Unknown
Conditioning regimen: TBI‐based vs. chemotherapy only, myeloablative vs. non‐myeloablative/reduced intensity
GvHD prophylaxis: (Ex‐vivo T cell depletion vs. non‐T cell depleted)
Transplant center
Type of graft (BM vs. PBSC)
In vivo T cell depletion (ATG, Campath)
Graft characteristics (number of mononucleated cells, CD34+ cells, CD3+ cells per kg recipient weight)
Study Design: To summarize the characteristics of the dataset, descriptive tables of patient‐, disease‐ and transplant‐related factors will be reported.
For discrete factors, the number of cases and their respective percentages will be calculated. Chi‐Square tests will be used to compare discrete factors between the HLA matched vs. mismatched groups.
For continuous factors, the median and ranges will be calculated. The Kruskal‐Wallis test will be used to compare the continuous factors between the HLA matched vs. mismatched groups.
Univariate probabilities for overall survival will be calculated using the Kaplan‐Meier estimator with variance estimated by Greenwood's formula. Comparison of survival curves will be done using the log‐rank test. For engraftment/graft loss by day 28, logistic regression will be used. Center effect will be tested. Multivariate analyses will be performed using the proportional hazards model to compare the DSA positive and DSA negative groups. Models will be fit to determine which risk factors may be related to a given outcome. All variables will be tested for the affirmation of the proportional hazards assumption. Factors violating the proportional hazards assumption will be adjusted for first before the stepwise model building approach will be used in developing models for the primary and secondary outcomes.
54
Not for publication or presentation Attachment 4
References: 1. Horan J, Wang T, Haagenson M et al. Evaluation of HLA matching in unrelated hematopoietic
stem cell transplantation for nonmalignant disorders. Blood 2012;120(14):2918‐2924. 2. Lee SJ, Klein J, Haagenson M et al. High‐resolution donor‐recipient HLA matching contributes to
the success of unrelated donor marrow transplantation. Blood 2007;110(13):4576‐4583. 3. Spellman S, Bray R, Rosen‐Bronson S et al. The detection of donor directed, HLA‐specific
alloantibodies in recipients of unrelated hematopoietic cell transplantation is predictive of graft failure. Blood 2010;115(13):2704‐2708.
4. Ciurea SO, Thall PF, Wang X et al. Donor‐specific anti‐HLA Abs and graft failure in matched unrelated donor hematopoietic stem cell transplantation. Blood 2011;118(22):5957‐5964.
5. Petersdorf EW, Hansen JA, Martin PJ etal. Major‐histocompatibility‐complex class I alleles and antigens in hematopoietic‐cell transplantation. N Engl J Med 2001;345(25):1794‐800.
6. Flomenberg N, Baxter‐Lowe LA, Confer D et al. Impact of HLA class I and class II high‐resolution matching on outcomes of unrelated donor bone marrow transplantation: HLA‐C mismatching is associated with a strong adverse effect on transplantation outcome. Blood 2004;104(7):1923‐1930.
7. Pei R, Lee JH, Shih NJ et al. Single human leukocyte antigen flow cytometry beads for accurate identification of HLA antibody specificities. Transplantation 2003;75:43.
8. Chen G, Sequeira F, Tyan DB. Novel C1q assay reveals a clinically relevant subset of human leukocyte antigen antibodies independent of immunoglobulin G strength on single antigen beads. Hum Immunol 2011 Oct;72(10):849‐58.
9. Zhang Q, Cecka JM, Gjertson DW, Ge P, Rose ML, Patel JK, Ardehali A, Kobashigawa JA, Fishbein MC, Reed EF. HLA and MICA: targets of antibody‐mediated rejection in heart transplantation. Transplantation 2011 May;91(10):1153‐8.
55
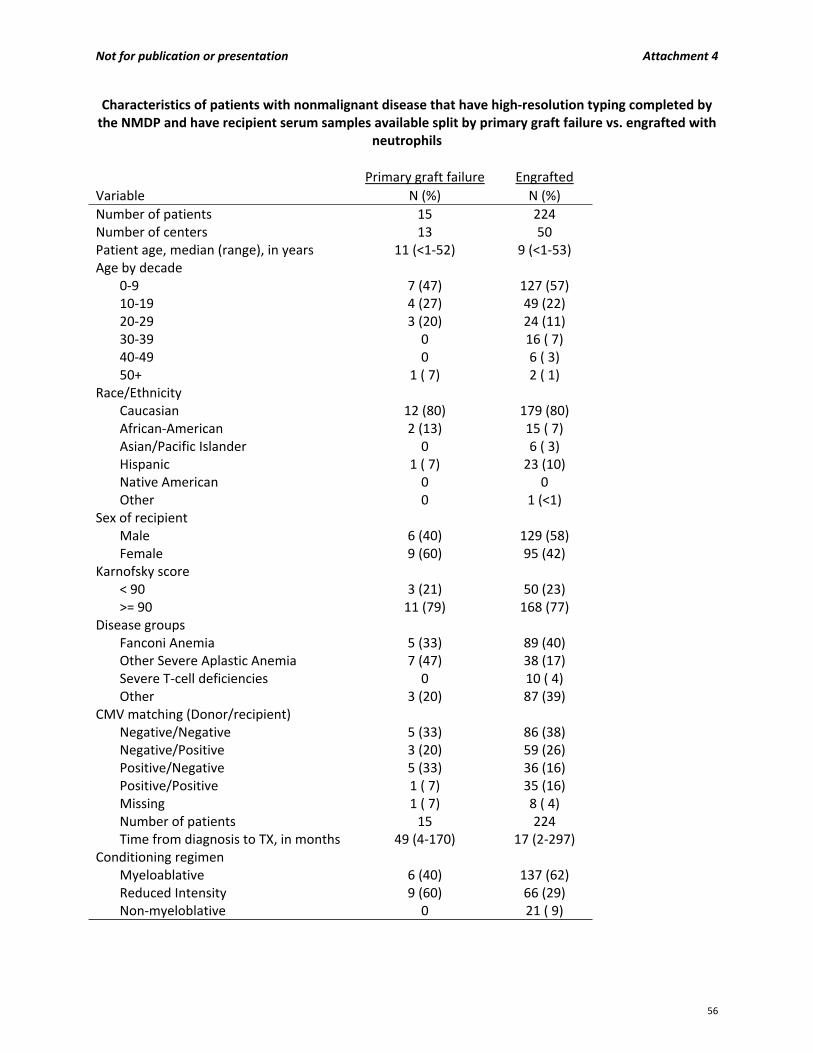
Not for publication or presentation Attachment 4
Characteristics of patients with nonmalignant disease that have high‐resolution typing completed by the NMDP and have recipient serum samples available split by primary graft failure vs. engrafted with
neutrophils
Primary graft failure Engrafted Variable N (%) N (%)
Number of patients 15 224Number of centers 13 50Patient age, median (range), in years 11 (<1‐52) 9 (<1‐53) Age by decade
0‐9 7 (47) 127 (57)10‐19 4 (27) 49 (22)20‐29 3 (20) 24 (11)30‐39 0 16 ( 7)40‐49 0 6 ( 3)50+ 1 ( 7) 2 ( 1)
Race/Ethnicity Caucasian 12 (80) 179 (80)African‐American 2 (13) 15 ( 7)Asian/Pacific Islander 0 6 ( 3)Hispanic 1 ( 7) 23 (10)Native American 0 0Other 0 1 (<1)
Sex of recipient Male 6 (40) 129 (58)Female 9 (60) 95 (42)
Karnofsky score < 90 3 (21) 50 (23)>= 90 11 (79) 168 (77)
Disease groups Fanconi Anemia 5 (33) 89 (40)Other Severe Aplastic Anemia 7 (47) 38 (17)Severe T‐cell deficiencies 0 10 ( 4)Other 3 (20) 87 (39)
CMV matching (Donor/recipient) Negative/Negative 5 (33) 86 (38)Negative/Positive 3 (20) 59 (26)Positive/Negative 5 (33) 36 (16)Positive/Positive 1 ( 7) 35 (16)Missing 1 ( 7) 8 ( 4)Number of patients 15 224Time from diagnosis to TX, in months 49 (4‐170) 17 (2‐297)
Conditioning regimen Myeloablative 6 (40) 137 (62)Reduced Intensity 9 (60) 66 (29)Non‐myeloblative 0 21 ( 9)
56
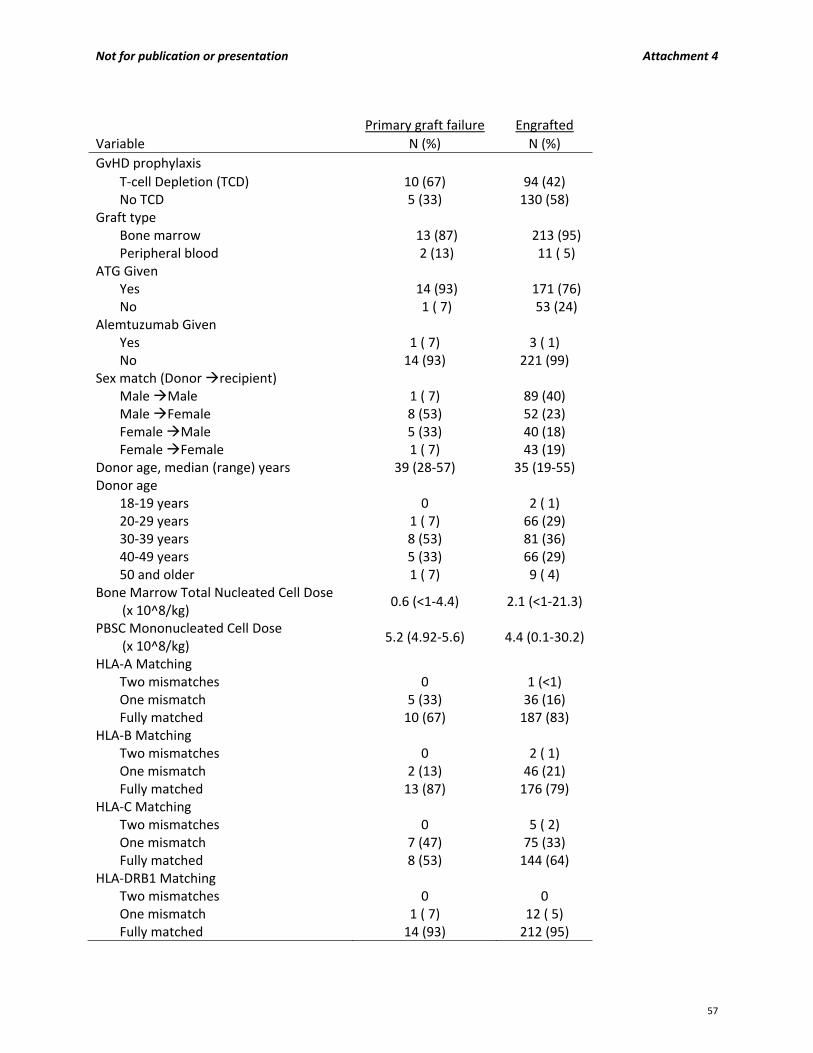
Not for publication or presentation Attachment 4
Primary graft failure Engrafted
Variable N (%) N (%)
GvHD prophylaxis T‐cell Depletion (TCD) 10 (67) 94 (42)No TCD 5 (33) 130 (58)
Graft type Bone marrow 13 (87) 213 (95) Peripheral blood 2 (13) 11 ( 5)
ATG Given Yes 14 (93) 171 (76) No 1 ( 7) 53 (24)
Alemtuzumab Given Yes 1 ( 7) 3 ( 1)No 14 (93) 221 (99)
Sex match (Donor recipient) Male Male 1 ( 7) 89 (40)Male Female 8 (53) 52 (23)Female Male 5 (33) 40 (18)Female Female 1 ( 7) 43 (19)
Donor age, median (range) years 39 (28‐57) 35 (19‐55) Donor age
18‐19 years 0 2 ( 1)20‐29 years 1 ( 7) 66 (29)30‐39 years 8 (53) 81 (36)40‐49 years 5 (33) 66 (29)50 and older 1 ( 7) 9 ( 4)
Bone Marrow Total Nucleated Cell Dose (x 10^8/kg)
0.6 (<1‐4.4) 2.1 (<1‐21.3)
PBSC Mononucleated Cell Dose (x 10^8/kg)
5.2 (4.92‐5.6) 4.4 (0.1‐30.2)
HLA‐A Matching Two mismatches 0 1 (<1)One mismatch 5 (33) 36 (16)Fully matched 10 (67) 187 (83)
HLA‐B Matching Two mismatches 0 2 ( 1)One mismatch 2 (13) 46 (21)Fully matched 13 (87) 176 (79)
HLA‐C Matching Two mismatches 0 5 ( 2)One mismatch 7 (47) 75 (33)Fully matched 8 (53) 144 (64)
HLA‐DRB1 Matching Two mismatches 0 0One mismatch 1 ( 7) 12 ( 5)Fully matched 14 (93) 212 (95)
57
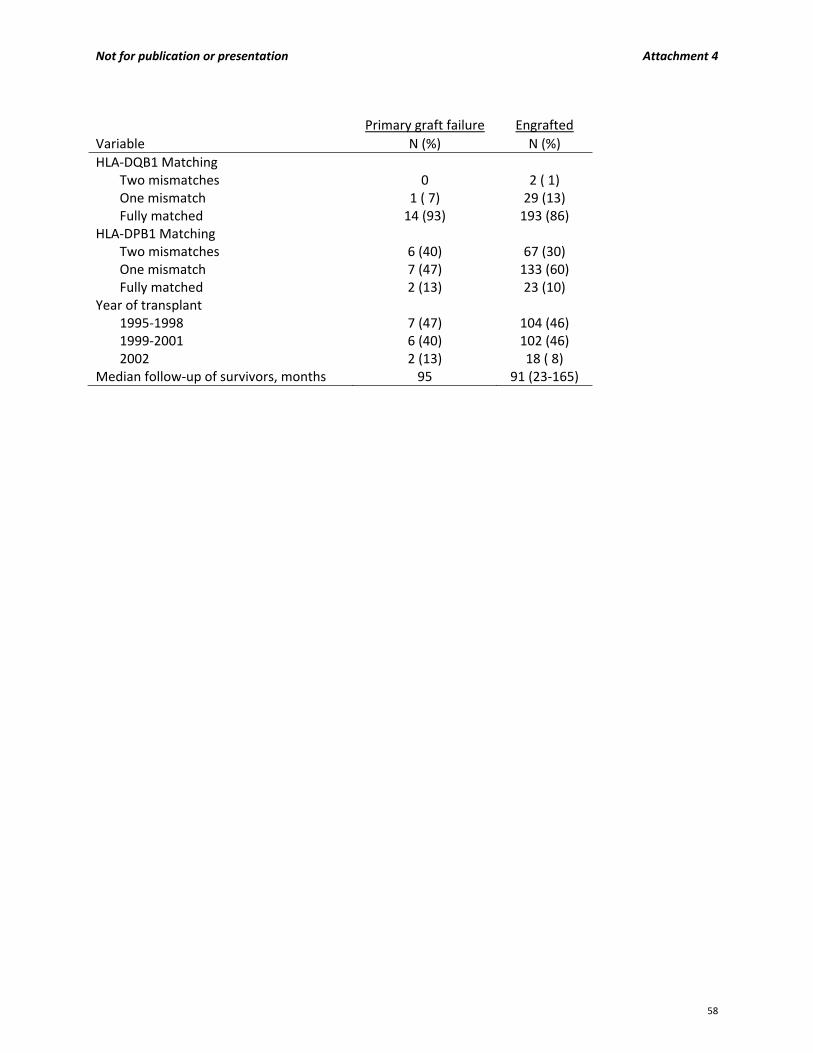
Not for publication or presentation Attachment 4
Primary graft failure Engrafted
Variable N (%) N (%)
HLA‐DQB1 Matching Two mismatches 0 2 ( 1)One mismatch 1 ( 7) 29 (13)Fully matched 14 (93) 193 (86)
HLA‐DPB1 Matching Two mismatches 6 (40) 67 (30)One mismatch 7 (47) 133 (60)Fully matched 2 (13) 23 (10)
Year of transplant 1995‐1998 7 (47) 104 (46)1999‐2001 6 (40) 102 (46)2002 2 (13) 18 ( 8)
Median follow‐up of survivors, months 95 91 (23‐165)
58
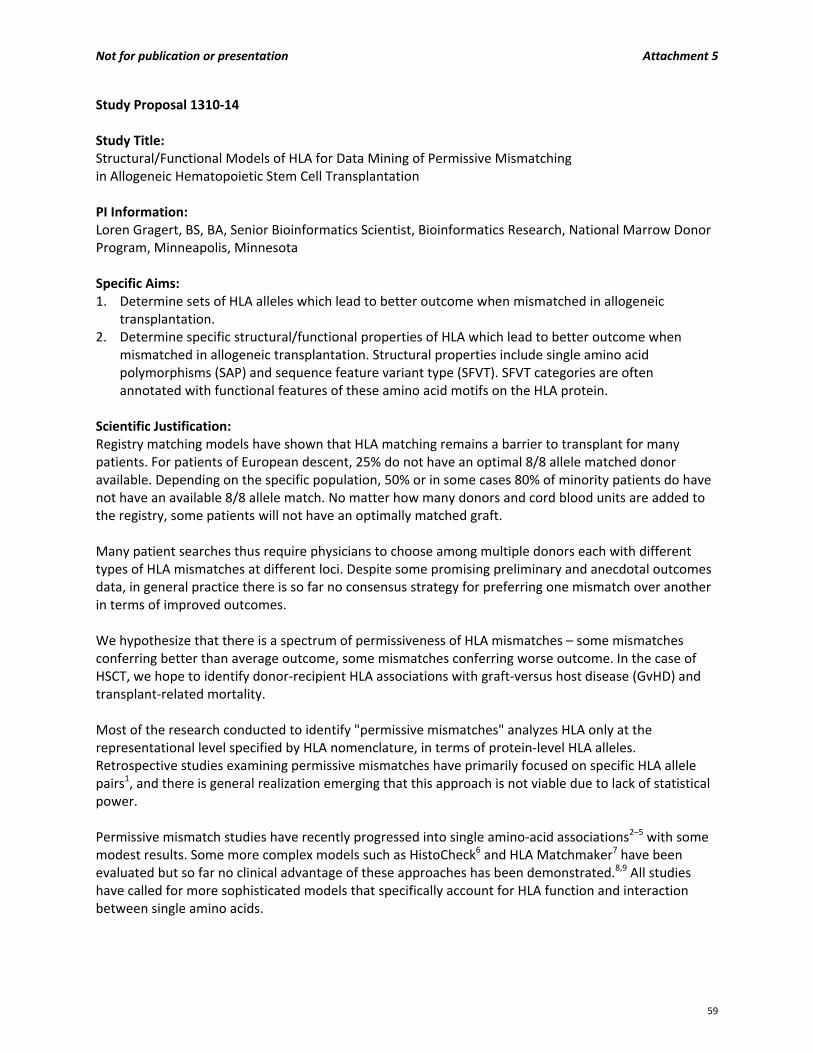
Not for publication or presentation Attachment 5
Study Proposal 1310‐14 Study Title: Structural/Functional Models of HLA for Data Mining of Permissive Mismatching in Allogeneic Hematopoietic Stem Cell Transplantation PI Information: Loren Gragert, BS, BA, Senior Bioinformatics Scientist, Bioinformatics Research, National Marrow Donor Program, Minneapolis, Minnesota Specific Aims: 1. Determine sets of HLA alleles which lead to better outcome when mismatched in allogeneic
transplantation. 2. Determine specific structural/functional properties of HLA which lead to better outcome when
mismatched in allogeneic transplantation. Structural properties include single amino acid polymorphisms (SAP) and sequence feature variant type (SFVT). SFVT categories are often annotated with functional features of these amino acid motifs on the HLA protein.
Scientific Justification: Registry matching models have shown that HLA matching remains a barrier to transplant for many patients. For patients of European descent, 25% do not have an optimal 8/8 allele matched donor available. Depending on the specific population, 50% or in some cases 80% of minority patients do have not have an available 8/8 allele match. No matter how many donors and cord blood units are added to the registry, some patients will not have an optimally matched graft. Many patient searches thus require physicians to choose among multiple donors each with different types of HLA mismatches at different loci. Despite some promising preliminary and anecdotal outcomes data, in general practice there is so far no consensus strategy for preferring one mismatch over another in terms of improved outcomes. We hypothesize that there is a spectrum of permissiveness of HLA mismatches – some mismatches conferring better than average outcome, some mismatches conferring worse outcome. In the case of HSCT, we hope to identify donor‐recipient HLA associations with graft‐versus host disease (GvHD) and transplant‐related mortality. Most of the research conducted to identify "permissive mismatches" analyzes HLA only at the representational level specified by HLA nomenclature, in terms of protein‐level HLA alleles. Retrospective studies examining permissive mismatches have primarily focused on specific HLA allele pairs1, and there is general realization emerging that this approach is not viable due to lack of statistical power. Permissive mismatch studies have recently progressed into single amino‐acid associations2–5 with some modest results. Some more complex models such as HistoCheck6 and HLA Matchmaker7 have been evaluated but so far no clinical advantage of these approaches has been demonstrated.8,9 All studies have called for more sophisticated models that specifically account for HLA function and interaction between single amino acids.
59

We propose a case/control study design using multivariate logistic regression to attack the permissive mismatch problem. We will develop a coding system for different types of HLA mismatches at the structural/functional level. At the structural level, we are able to not only examine single amino acid associations, but have also implemented sequence feature variant type (SFVT) analysis that can examine sets of amino acids on the HLA protein.10 The ImmPort database defines HLA sequence features and often provides annotation that indicates the role of the amino acid motif in functional categories such as peptide binding, T‐cell binding, and structural features of the HLA molecule. SFVT analysis also allows for more complete examination of protein structure than provided by HLA Matchmaker or HistoCheck. With SFVT annotation, we can group similar types of mismatches together, such as amino acids surrounding a particular pocket in the peptide binding groove or those likely to be in contact with T‐cell receptor. These SFVT annotation category groupings can increase statistical power substantially because many pairs of HLA alleles would be mismatched over a specific region. Most mismatched allele pairs differ at more than one amino acid, and SFVT analysis removes the criticism made by Baxter‐Lowe that SAP aren't considered in the context of other SAP mismatches.1 The theory that minor differences in HLA structure leads to less alloreactivity has not been supported, so unlike HistoCheck, we will not be use amino acid scoring matrices. While there is evidence that amino acid changes that perturb peptide binding specificity lead to worse outcome,11 results from Heemskerk indicate that highly disparate mismatches may actually be more permissive.12 This permissiveness could be related to the fact that during the course of T cell maturation, T cells die from neglect if they don't bind at all to the self‐MHC peptide complex in the thymus.13 The T cells that are weak binders to self‐MHC complexes mature through positive selection, and therefore T cells should be most sensitive to more subtle differences.13 Promising permissive mismatch results for T cell epitope groupings at the DPB1 locus indicate that an approach considering HLA structure in the area of interaction with the T cell receptor could be successful when applied to other HLA loci.14 Success with our more comprehensive structural/functional approach to examining HLA could lead to development of a set of guidelines for selecting mismatched donors and lead to better overall outcome for HSCT. Study Population: All patients who were transplanted for allo‐HSCT recorded in the CIBMTR database where HLA typing is available. We specifically request the patients included in the dataset for the HistoCheck permissive mismatch study.9 Data Requirements: The CIBMTR Immunobiology Working Committee has defined a standard dataset that can be provided for the discovery and validation phases of permissive mismatch algorithm assessment.9 Data required include: Patient and donor HLA typing for unrelated adult transplant pairs, outcomes variables of acute GvHD and overall survival at 1 year. Sample Requirements: There are no sample requirements for this study.
60

Study Design: We will apply a case/control design with multivariate logistic regression to the permissive mismatch problem. For the primary analysis, controls will be transplant pairs where the patient survived at one year and cases will be transplant pairs with patient deaths before one year. A secondary analysis will segregate cases and controls by incidence of acute GVHD of grades III‐IV at one year. We have developed a coding system for mismatches based on amino acid differences, SFVTs, SFVT annotation category. Directionality of differences is also encoded. We will also examine associations of donor and patient factors, independent of each other, with outcome. The concept of sequence feature variant type (SFVT) requires a detailed example: Sequence Feature 247 (SF247), defined in the ImmPORT database (http://immport.niaid.nih.gov/), consists of 3 amino acids at positions 70, 73, and 74 on the HLA protein. Variant Type 1 (VT1) of sequence feature SF247 has a HTD motif at these 3 amino acids, while Variant Type 2 (VT2) has a QTH motif, and VT3 has a HTH motif. VT1 includes hundreds of HLA‐A alleles including A*01:01, A*23:01, A*24:04, while VT2 includes A*03:01, A*11:01, A*29:01, and VT3 includes A*02:01 and other A*02 alleles. These 3 variant types comprise the vast majority of HLA‐A allele frequency. SF247 has a structural‐functional annotation of “alpha‐helix 2” and “peptide antigen binding pocket C”. We propose a semi‐hierarchical mismatch coding system where we first examine broadest categories of mismatches and goes into more detail as statistical power allows. For SF247, we will first examine where any differences in variant type at SF247 are associated with outcome, where all mismatched cases are put into one category and matched cases are put into another. Considering all types of VT mismatches would give maximal statistical power, and give a result that indicate if mismatches in the “peptide antigen binding pocket C” annotation category is associated with better or worse than average outcome. Variant type differences can also be subdivided by the number of amino acid differences. SF247 has 3 amino acids, and variant types within this sequence feature can differ at between 1 and 3 amino acids. VT1 and VT2 differ at 2 amino acids, VT1 and VT3 at 1 amino acid, while VT2 and VT3 different also at 1 amino acid. We will next group all variant type mismatches by the number of amino acids mismatched, so VT1‐VT3 and VT2‐VT3 mismatch types would be grouped together. Results from this analysis would indicate if greater divergence in amino acids at a particular sequence motif is associated with better or worse than average outcome. Other amino acid properties could also be considered as ways to group different sorts of variant type mismatches. For an additional round of statistical analysis, each pair of mismatched SFVTs would be tested as independent categories (SF247 would have 3 types of mismatched pairs: VT1‐VT2, VT1‐VT3, VT2‐VT3). This analysis would give the highest specificity for an association, but the least statistical power. Finally, Further subdivision of SFVT mismatches could consider donor‐recipient directionality (here the notation VT1>VT2 would denote a donor with VT1 is transplanted into a patient with VT2, which would be different than VT2>VT1). Statistical power to examine specific pairs of SFVTs may be limited, as seen in other studies. Factor analysis will be applied to eliminate redundancy between linked amino acid and SFVT variants commonly found together on the same sets of the HLA alleles. We will apply False Discovery Rate (FDR) to adjust P‐values for multiple testing.15
61

We will also apply statistical methods to distinguish transplant pairs that are likely to be single haplotype matches compared to those that are likely to have both haplotypes mismatched. We will assign HLA haplotype phase across 5 loci (A~C~B~DRB1~DQB1) using imputation based on the population haplotype frequencies.16 Another statistical method named multiple imputation17 maintains the phase ambiguity in the statistical models to allow for examination of associations with phased haplotype matching even though phase is not determined experimentally. References
1. Baxter‐Lowe LA, Maiers M, Spellman SR et al. HLA‐A disparities illustrate challenges for ranking the impact of HLA mismatches on bone marrow transplant outcomes in the United States. Biology of Blood and Marrow Transplantation 2009;15(8):971–81.
2. Ferrara GB. Bone marrow transplantation from unrelated donors: the impact of mismatches with substitutions at position 116 of the human leukocyte antigen class I heavy chain. Blood 2001;98(10):3150–3155.
3. Morishima Y, Kawase T, Malkki M et al. Effect of HLA‐A2 allele disparity on clinical outcome in hematopoietic cell transplantation from unrelated donors. Tissue antigens 2007;69 Suppl 1:31–5.
4. Kawase T, Matsuo K, Kashiwase K et al. HLA mismatch combinations associated with decreased risk of relapse: implications for the molecular mechanism. Blood 2009;113(12):2851–8.
5. Marino SR, Lin S, Maiers M et al. Identification by random forest method of HLA class I amino acid substitutions associated with lower survival at day 100 in unrelated donor hematopoietic cell transplantation. Bone marrow transplantation 2011; January:1–10.
6. Elsner H, DeLuca D, Strub J et al. HistoCheck: rating of HLA class I and II mismatches by an internet‐based software tool. Bone marrow transplantation 2004;33(2):165–9.
7. Duquesnoy RJ. HLAMatchmaker: a molecularly based algorithm for histocompatibility determination. I. Description of the algorithm. Human immunology 2002;63(5):339–52.
8. Duquesnoy R, Spellman S, Haagenson M, et al. HLAMatchmaker‐defined triplet matching is not associated with better survival rates of patients with class I HLA allele mismatched hematopoietic cell transplants from unrelated donors. Biology of blood and marrow transplantation: journal of the American Society for Blood and Marrow Transplantation 2008;14(9):1064–71.
9. Spellman S, Klein J, Haagenson M et al. Scoring HLA class I mismatches by HistoCheck does not predict clinical outcome in unrelated hematopoietic stem cell transplantation. Biology of blood and marrow transplantation: journal of the American Society for Blood and Marrow Transplantation 2012;18(5):739–46.
10. Karp DR, Marthandan N, Marsh SGE et al. Novel sequence feature variant type analysis of the HLA genetic association in systemic sclerosis. Human molecular genetics 2010;19(4):707–19.
11. Yanover C, Petersdorf EW, Malkki M et al. HLA mismatches and hematopoietic cell transplantation: Structural simulations assess the impact of changes in peptide binding specificity on transplant outcome. Immunome research 2011;7(2):4.
12. Heemskerk MB, Cornelissen JJ, Roelen DL et al. Highly diverged MHC class I mismatches are acceptable for haematopoietic stem cell transplantation. Bone marrow transplantation 2007;40(3):193–200.
13. Archbold JK, Ely LK, Kjer‐Nielsen L et al. T cell allorecognition and MHC restriction‐‐A case of Jekyll and Hyde? Molecular immunology 2008;45(3):583–98.
14. Fleischhauer K, Shaw BE, Gooley T et al. Effect of T‐cell‐epitope matching at HLA‐DPB1 in recipients of unrelated‐donor haemopoietic‐cell transplantation: a retrospective study. The lancet oncology 2012;13(4):366–374.
62
15. Benjamini Y, Hochberg Y. Controlling the False Disovery Rate ‐ A Practical and Powerful Approach to Multiple Testing. Journal of the Royal Statistical Society. Series B (Methodological) 1995;57(1):289–300.
16. Gourraud P‐A, Lamiraux P, El‐Kadhi N et al. Inferred HLA haplotype information for donors from hematopoietic stem cells donor registries. Human Immunology 2005;66(5):563–70.
17. Rubin DB. Multiple Imputation for Nonresponse in Surveys. New York: Wiley and Sons; 1987.
63
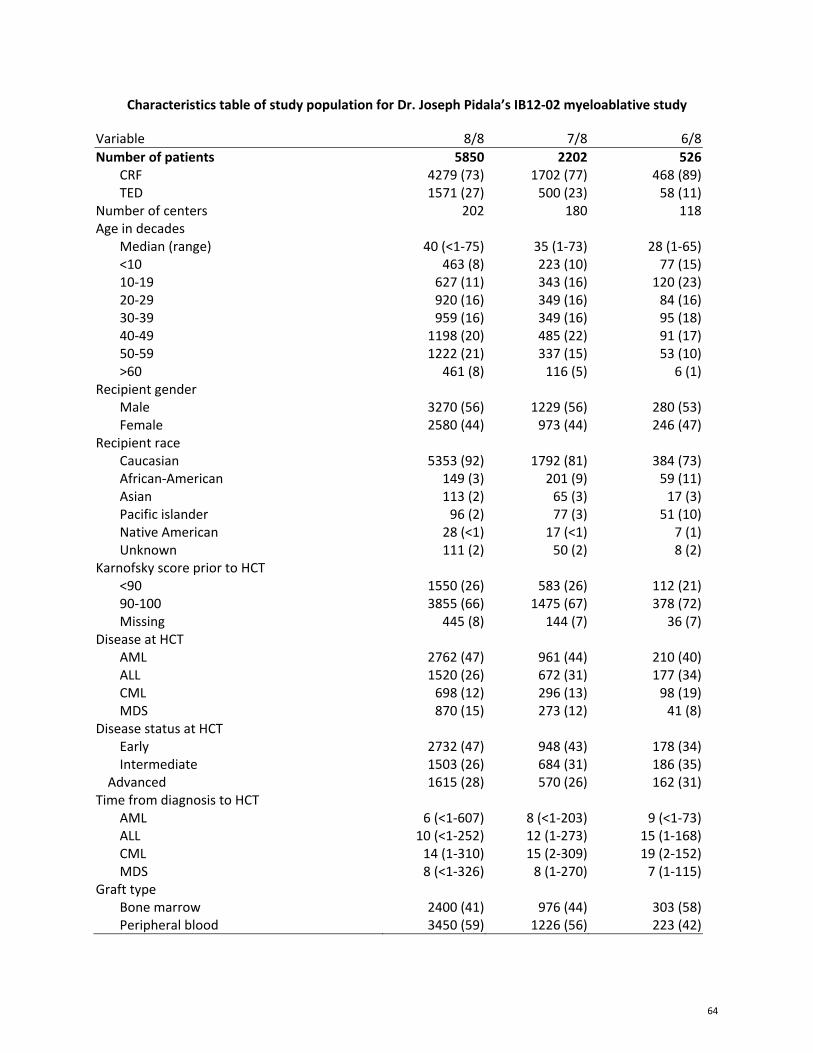
Characteristics table of study population for Dr. Joseph Pidala’s IB12‐02 myeloablative study
Variable 8/8 7/8 6/8
Number of patients 5850 2202 526CRF 4279 (73) 1702 (77) 468 (89)TED 1571 (27) 500 (23) 58 (11)
Number of centers 202 180 118Age in decades
Median (range) 40 (<1‐75) 35 (1‐73) 28 (1‐65)<10 463 (8) 223 (10) 77 (15)10‐19 627 (11) 343 (16) 120 (23)20‐29 920 (16) 349 (16) 84 (16)30‐39 959 (16) 349 (16) 95 (18)40‐49 1198 (20) 485 (22) 91 (17)50‐59 1222 (21) 337 (15) 53 (10)>60 461 (8) 116 (5) 6 (1)
Recipient gender Male 3270 (56) 1229 (56) 280 (53)Female 2580 (44) 973 (44) 246 (47)
Recipient race Caucasian 5353 (92) 1792 (81) 384 (73)African‐American 149 (3) 201 (9) 59 (11)Asian 113 (2) 65 (3) 17 (3)Pacific islander 96 (2) 77 (3) 51 (10)Native American 28 (<1) 17 (<1) 7 (1)Unknown 111 (2) 50 (2) 8 (2)
Karnofsky score prior to HCT <90 1550 (26) 583 (26) 112 (21)90‐100 3855 (66) 1475 (67) 378 (72)Missing 445 (8) 144 (7) 36 (7)
Disease at HCT AML 2762 (47) 961 (44) 210 (40)ALL 1520 (26) 672 (31) 177 (34)CML 698 (12) 296 (13) 98 (19)MDS 870 (15) 273 (12) 41 (8)
Disease status at HCT Early 2732 (47) 948 (43) 178 (34)Intermediate 1503 (26) 684 (31) 186 (35)
Advanced 1615 (28) 570 (26) 162 (31)Time from diagnosis to HCT
AML 6 (<1‐607) 8 (<1‐203) 9 (<1‐73)ALL 10 (<1‐252) 12 (1‐273) 15 (1‐168)CML 14 (1‐310) 15 (2‐309) 19 (2‐152)MDS 8 (<1‐326) 8 (1‐270) 7 (1‐115)
Graft type Bone marrow 2400 (41) 976 (44) 303 (58)Peripheral blood 3450 (59) 1226 (56) 223 (42)
64
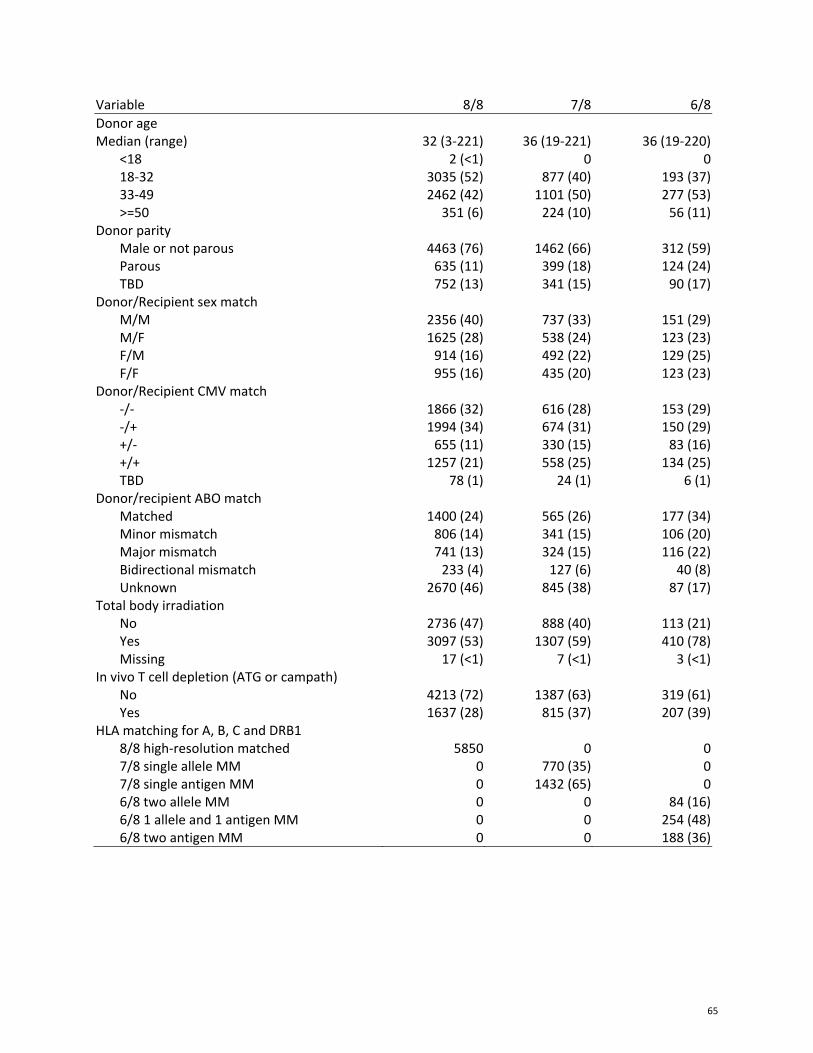
Variable 8/8 7/8 6/8
Donor age Median (range) 32 (3‐221) 36 (19‐221) 36 (19‐220)
<18 2 (<1) 0 018‐32 3035 (52) 877 (40) 193 (37)33‐49 2462 (42) 1101 (50) 277 (53)>=50 351 (6) 224 (10) 56 (11)
Donor parity Male or not parous 4463 (76) 1462 (66) 312 (59)Parous 635 (11) 399 (18) 124 (24)TBD 752 (13) 341 (15) 90 (17)
Donor/Recipient sex match M/M 2356 (40) 737 (33) 151 (29)M/F 1625 (28) 538 (24) 123 (23)F/M 914 (16) 492 (22) 129 (25)F/F 955 (16) 435 (20) 123 (23)
Donor/Recipient CMV match ‐/‐ 1866 (32) 616 (28) 153 (29)‐/+ 1994 (34) 674 (31) 150 (29)+/‐ 655 (11) 330 (15) 83 (16)+/+ 1257 (21) 558 (25) 134 (25)TBD 78 (1) 24 (1) 6 (1)
Donor/recipient ABO match Matched 1400 (24) 565 (26) 177 (34)Minor mismatch 806 (14) 341 (15) 106 (20)Major mismatch 741 (13) 324 (15) 116 (22)Bidirectional mismatch 233 (4) 127 (6) 40 (8)Unknown 2670 (46) 845 (38) 87 (17)
Total body irradiation No 2736 (47) 888 (40) 113 (21)Yes 3097 (53) 1307 (59) 410 (78)Missing 17 (<1) 7 (<1) 3 (<1)
In vivo T cell depletion (ATG or campath) No 4213 (72) 1387 (63) 319 (61)Yes 1637 (28) 815 (37) 207 (39)
HLA matching for A, B, C and DRB1 8/8 high‐resolution matched 5850 0 07/8 single allele MM 0 770 (35) 07/8 single antigen MM 0 1432 (65) 06/8 two allele MM 0 0 84 (16)6/8 1 allele and 1 antigen MM 0 0 254 (48)6/8 two antigen MM 0 0 188 (36)
65
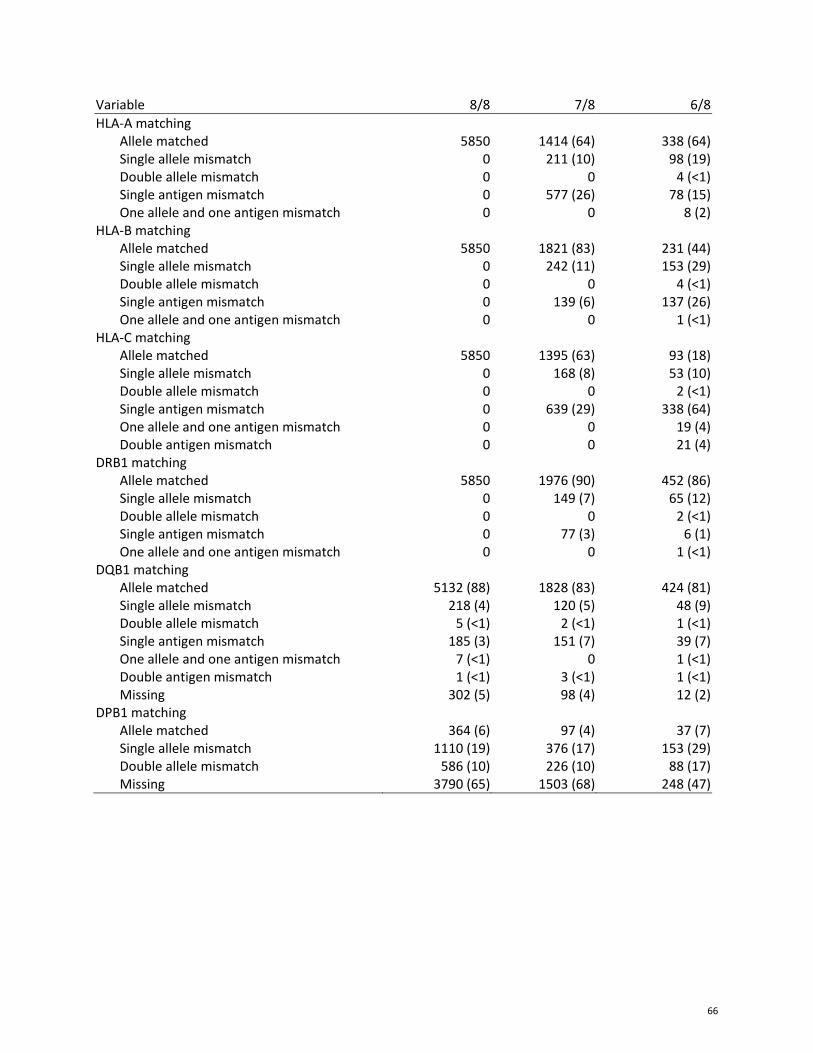
Variable 8/8 7/8 6/8
HLA‐A matching Allele matched 5850 1414 (64) 338 (64) Single allele mismatch 0 211 (10) 98 (19) Double allele mismatch 0 0 4 (<1) Single antigen mismatch 0 577 (26) 78 (15) One allele and one antigen mismatch 0 0 8 (2)HLA‐B matching Allele matched 5850 1821 (83) 231 (44) Single allele mismatch 0 242 (11) 153 (29) Double allele mismatch 0 0 4 (<1) Single antigen mismatch 0 139 (6) 137 (26) One allele and one antigen mismatch 0 0 1 (<1)HLA‐C matching Allele matched 5850 1395 (63) 93 (18) Single allele mismatch 0 168 (8) 53 (10) Double allele mismatch 0 0 2 (<1) Single antigen mismatch 0 639 (29) 338 (64) One allele and one antigen mismatch 0 0 19 (4) Double antigen mismatch 0 0 21 (4)DRB1 matching Allele matched 5850 1976 (90) 452 (86) Single allele mismatch 0 149 (7) 65 (12) Double allele mismatch 0 0 2 (<1) Single antigen mismatch 0 77 (3) 6 (1) One allele and one antigen mismatch 0 0 1 (<1)DQB1 matching Allele matched 5132 (88) 1828 (83) 424 (81) Single allele mismatch 218 (4) 120 (5) 48 (9) Double allele mismatch 5 (<1) 2 (<1) 1 (<1) Single antigen mismatch 185 (3) 151 (7) 39 (7) One allele and one antigen mismatch 7 (<1) 0 1 (<1) Double antigen mismatch 1 (<1) 3 (<1) 1 (<1) Missing 302 (5) 98 (4) 12 (2)DPB1 matching Allele matched 364 (6) 97 (4) 37 (7) Single allele mismatch 1110 (19) 376 (17) 153 (29) Double allele mismatch 586 (10) 226 (10) 88 (17) Missing 3790 (65) 1503 (68) 248 (47)
66
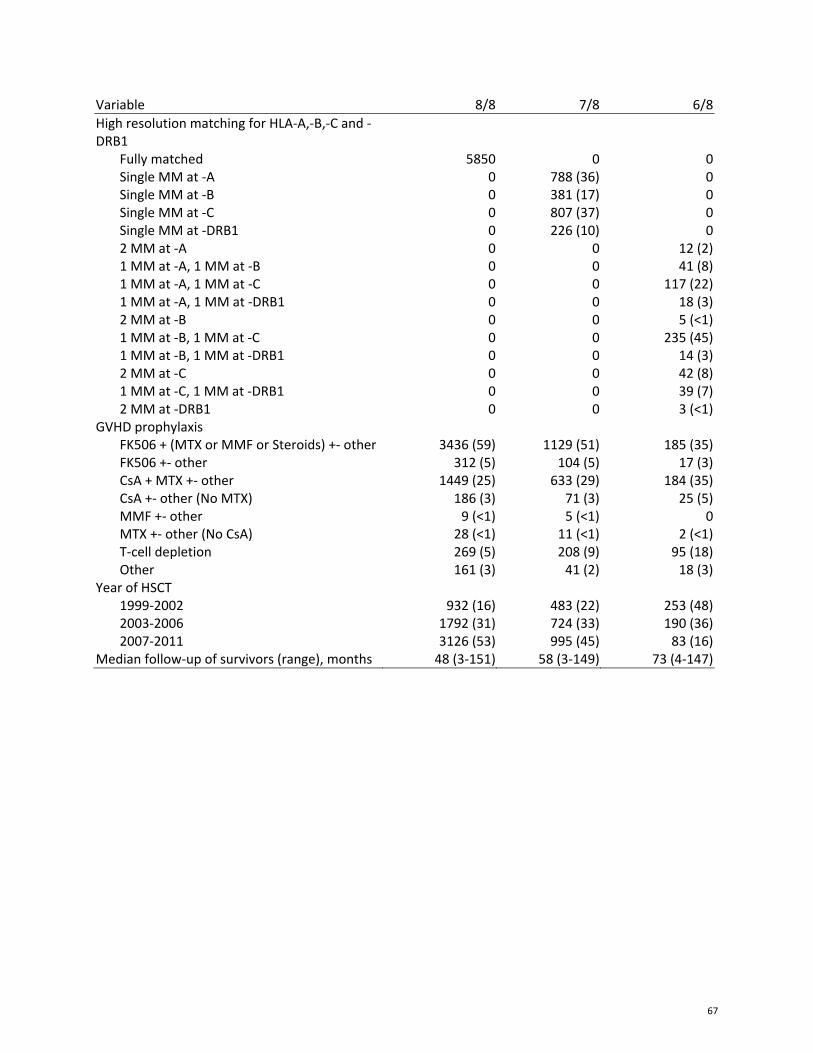
Variable 8/8 7/8 6/8
High resolution matching for HLA‐A,‐B,‐C and ‐DRB1
Fully matched 5850 0 0 Single MM at ‐A 0 788 (36) 0 Single MM at ‐B 0 381 (17) 0 Single MM at ‐C 0 807 (37) 0 Single MM at ‐DRB1 0 226 (10) 0 2 MM at ‐A 0 0 12 (2) 1 MM at ‐A, 1 MM at ‐B 0 0 41 (8) 1 MM at ‐A, 1 MM at ‐C 0 0 117 (22) 1 MM at ‐A, 1 MM at ‐DRB1 0 0 18 (3) 2 MM at ‐B 0 0 5 (<1) 1 MM at ‐B, 1 MM at ‐C 0 0 235 (45) 1 MM at ‐B, 1 MM at ‐DRB1 0 0 14 (3) 2 MM at ‐C 0 0 42 (8) 1 MM at ‐C, 1 MM at ‐DRB1 0 0 39 (7) 2 MM at ‐DRB1 0 0 3 (<1)GVHD prophylaxis FK506 + (MTX or MMF or Steroids) +‐ other 3436 (59) 1129 (51) 185 (35) FK506 +‐ other 312 (5) 104 (5) 17 (3) CsA + MTX +‐ other 1449 (25) 633 (29) 184 (35) CsA +‐ other (No MTX) 186 (3) 71 (3) 25 (5) MMF +‐ other 9 (<1) 5 (<1) 0 MTX +‐ other (No CsA) 28 (<1) 11 (<1) 2 (<1) T‐cell depletion 269 (5) 208 (9) 95 (18) Other 161 (3) 41 (2) 18 (3)Year of HSCT 1999‐2002 932 (16) 483 (22) 253 (48) 2003‐2006 1792 (31) 724 (33) 190 (36) 2007‐2011 3126 (53) 995 (45) 83 (16)Median follow‐up of survivors (range), months 48 (3‐151) 58 (3‐149) 73 (4‐147)
67
Not for publication or presentation Attachment 6
Study Proposal 1310‐24 Study Title: Indirectly recognizable HLA epitopes (PIRCHES): a retrospective validation study on the role of indirect recognition of mismatched HLA in hematopoietic stem‐cell transplantation outcome. PI Information: Eric Spierings, PhD, University Medical Center Utrecht, The Netherlands Specific Aims: We hypothesize that indirect recognition of HLA disparities is important for the occurrence of alloreactivity after HLA mismatched hematopoietic stem‐cell transplantation (HSCT). This hypothesis has been derived from a previous analysis on a small local cohort (n=48) and was confirmed in a larger multicenter cohort (n=909). In these studies, we determined the number of predicted indirectly recognizable HLA Epitopes (PIRCHES) in silico. The number of PIRCHES appeared to correlate with an increased clinical alloreactivity and a poorer outcome. The aim of this current project is to improve the value of the algorithm by externally validating our results and determining the strength of the effect in relation to other factors that can be important in the development of alloreactivity (e.g. conditioning regimen, gender‐mismatches, high‐risk malignancies). Furthermore, we aim at improving our algorithm by defining more specifically which peptides lead to alloreactivity. The results will be published in a peer reviewed journal and thereby they might improve current donor selection strategies. Scientific Justification: HSCT with an HLA‐mismatched donor is an established risk factor for acute GVHD.1;2 Some of the HLA mismatches are more prone to evoke alloreactivity than others.3;4 As such, HLA mismatches can be characterized as being either permissive or non‐permissive. Until recent the mechanism behind these non‐permissive mismatches was poorly understood. We recently developed an in silico method that predicts indirect recognition of the mismatched HLA‐molecule by determining the numbers of PIRCHES. PIRCHES are peptides that are exclusively present in the mismatched HLA‐molecule of the recipient and are predicted to be presented on the cell surface by shared HLA. In a pilot study on a small local cohort of 48 patients that were transplanted with a 9/10 matched unrelated donor after having received a non‐myeloablative conditioning regimen we showed that high numbers of these PIRCHES increased the risk for acute GVHD (Thus et al. unpublished). In a collaboration with Dr. J. Mytilineos, we multivariately confirmed these observations in an extended study on a German cohort of 909 patients transplanted with a 9/10 MUD (Thus et al. manuscript in preparation and abstract #3544). The latter study additionally showed a clear correlation between numbers of PIRCHES and 1) transplant‐related mortality and 2) overall survival. Importantly, 2 patients transplanted with donors with low numbers of PIRCHES had similar 5 year survival probabilities as patients transplanted with HLA‐identical (10/10; n=1847) donors. The latter observation suggests that PIRCHE matching may be useful in donor selection. The aim of the proposed study is to validate the PIRCHE cut‐off values as defined in the initial studies. Furthermore, we hypothesize that the current PIRCHE determination can be improved. Validation and
68
Not for publication or presentation Attachment 6
fine‐tuning of the algorithm may facilitate implementation of this concept in the current donor selection process, thus improving the outcome of HLA‐mismatched HSCT. Study Population: Patients eligible for this study are those who have undergone unrelated HSCT for the treatment of hematological malignancy or non‐malignant bone marrow diseases and for which high resolution molecular typing for HLA‐A, ‐B, ‐C, ‐DRB1, ‐DQB1, and ‐DPB1 is available. All patients should have at least a single mismatch with their donor for either one the HLA‐A, ‐B, ‐C, ‐DRB1, ‐DQB1, and ‐DPB1alleles. When HLA‐DRB3,4,5 typing is available, these data will be included. There are no limitations concerning age, disease stage, year of transplant, graft type, prior treatment, or transplant regimens. Data Requirements: High resolution (4‐digit) typing of HLA‐A, ‐B, ‐C, ‐DRB1, ‐DQB1, and ‐DPB1 is essential for determining PIRCHES. Main outcomes are overall survival and cumulative incidence of transplant related mortality. Secondary outcomes are severity of acute and chronic graft‐versus‐host disease, disease free survival, relapse, and graft rejection. For the multivariate analyses the standard risk factors described to impact on the risk of graft‐versus‐host disease and relapse (age and gender of patient and donor, type and stage of disease, conditioning regimen, graft‐manipulation, GVHD prophylaxis, donor parity if available, CMV and EBV status of donor and recipient, donor and recipient blood group) are required. Sample Requirements: The study does not require biological samples from the NMDP repository. Study Design: This study is a retrospective analysis. For every donor‐recipient combination the number of PIRCHES that can evoke alloreactivity will be determined with the current and the newly constructed algorithms. Main outcomes are overall survival and cumulative incidence of transplant related mortality. Secondary outcomes are severity of acute and chronic graft‐versus‐host disease, disease free survival, relapse, and graft rejection. Competing risk analyses will be performed when longitudinal data are available to test the correlation of PIRCHES with clinical outcomes. Cox regression analyses will be performed for multivariate testing. When longitudinal data are not available, logistic regression analyses will be performed to test the magnitude of the association of PIRCHES with clinical outcomes. The analyses will test whether higher numbers of PIRCHES are associated with an increase in donor‐versus‐recipient alloreactivity, as measured by an increase in overall mortality, acute and chronic graft‐versus‐host disease, an increase in transplant‐related mortality, and a decrease in relapse incidence. In order to test the improvement in predictive value of newly constructed algorithms with respect to the clinical outcomes, Receiver Operating Curves will be constructed for the various models. The areas under the curves will be compared in order to select the most optimal model. Abstract #3544: Background:
69

Not for publication or presentation Attachment 6
HLA mismatches in hematopoietic stem‐cell transplantation (HSCT) correlate with adverse outcome due to increased alloreactivity. Identification of permissible HLA‐mismatches might be beneficial for donor selection when a 10/10 matched donor cannot be found. Methods: We developed an algorithm based upon the concept of indirect recognition of HLA mismatches to identify permissible mismatches. We subsequently analysed whether in silico prediction of the numbers of peptides derived from the recipients’ mismatched‐HLA molecules that can be presented by donorrecipient shared HLA, designated as Predicted Indirectly ReCognizable HLA‐Epitopes (PIRCHES), correlate with HSCT outcome. The numbers of PIRCHES presented on HLA class‐I (PIRCHE‐I) and ‐II (PIRCHE‐II) were calculated for 909 recipients of a single HLA mismatched unrelated donor (9/10) using the high resolution HLA‐A, ‐B, ‐C, ‐DRB1 and ‐DQB1 typings. Recipients were subsequently divided into tertiles according to their PIRCHE score (PIRCHE‐I low: 0‐1, mid: 2‐4, high 5‐31 and PIRCHE‐II low: 0‐3, mid 4‐13, high 14‐79). The clinical outcome of these groups was evaluated and compared to a reference patient group transplanted with completely HLA‐A, ‐B, ‐C, ‐DRB1 and ‐DQB1 matched donors (10/10, n=1847). Results: Patients in the low PIRCHE tertiles had a significantly lower risk for overall mortality, DFS, TRM, and acute and chronic GvHD, when compared to patients in the mid and high tertiles. Moreover, these risk in the low PIRCHE tertiles were similar to those in 10/10 HLA‐matched transplantations. Conclusions: In this study, we demonstrate that PIRCHES correlate with clinical alloreactivity. In particular, patients presenting low PIRCHE‐I have similar clinical outcomes as patients transplanted with a 10/10 HLAmatched donor. Our data thus suggest that indirect recognition of mismatched HLA by T cells is an important mechanism in clinical alloreactivity after HLA‐mismatched HSCT. Determining the number of PIRCHES for potential donors prior to HSCT may allow reducing complications after HLA‐mismatched HSCT by avoiding donors that can recognize higher numbers of PIRCHE. The present observations indicate that selection of HLA‐mismatched donors with low numbers of PIRCHES may lead to 5‐year survival probabilities similar to 10/10 matched unrelated donors. These observations require, however, confirmation in other cohorts. Moreover, the PIRCHES concept may also be valuable in other HSCT settings, such as CB transplantation and HSCT with a 10/10 matched unrelated donor that is mismatched for HLA‐DPB1. References:
1. Flomenberg N, Baxter‐Lowe LA, Confer D et al. Impact of HLA class I and class II high‐resolution matching on outcomes of unrelated donor bone marrow transplantation: HLA‐C mismatching is associated with a strong adverse effect on transplantation outcome. Blood 2004;104(7):1923‐30.
2. Morishima Y, Sasazuki T, Inoko H et al. The clinical significance of human leukocyte antigen (HLA) allele compatibility in patients receiving a marrow transplant from serologically HLA‐A, HLA‐B, and HLA‐DR matched unrelated donors. Blood 2002;99(11):4200‐6.
3. Maruya E, Takemoto S, Terasaki PI. HLA matching: identification of permissible HLA mismatches. Clin Transpl 1993:511‐20.
70
Not for publication or presentation Attachment 6
4. Kawase T, Morishima Y, Matsuo K, et al. High‐risk HLA allele mismatch combinations responsible for severe acute graft‐versus‐host disease and implication for its molecular mechanism. Blood 2007;110(7):2235‐41.
71
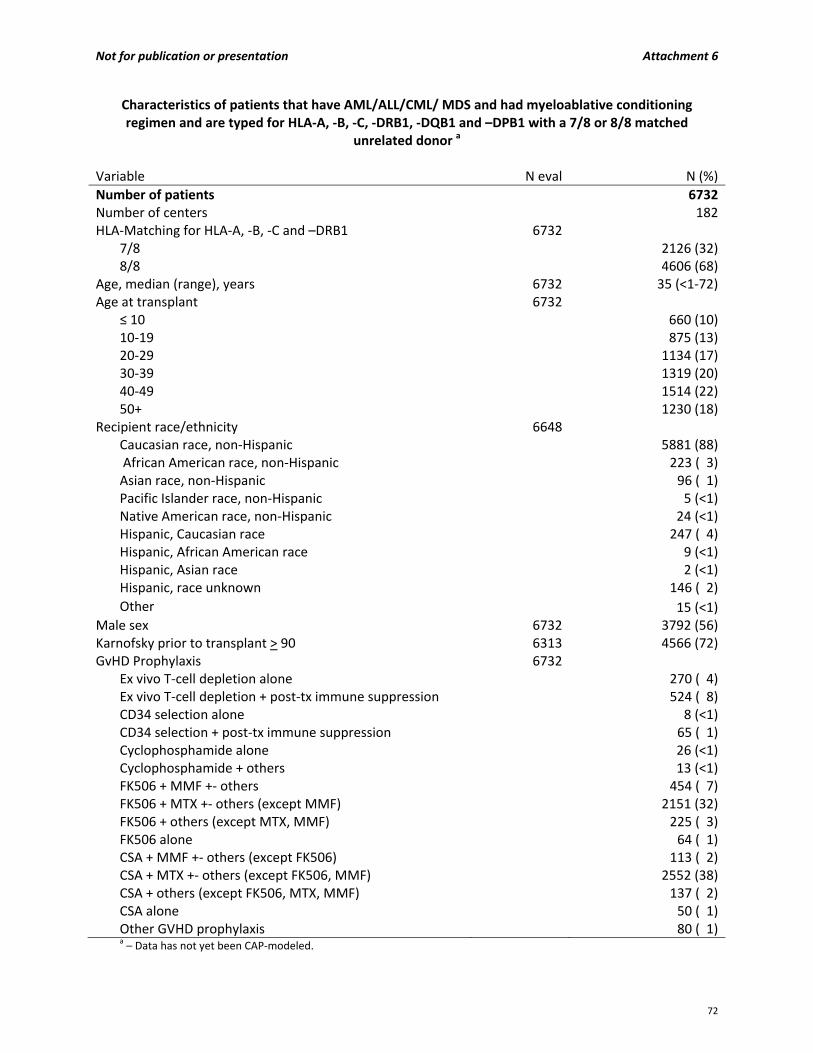
Not for publication or presentation Attachment 6
Characteristics of patients that have AML/ALL/CML/ MDS and had myeloablative conditioning regimen and are typed for HLA‐A, ‐B, ‐C, ‐DRB1, ‐DQB1 and –DPB1 with a 7/8 or 8/8 matched
unrelated donor a
Variable N eval N (%)
Number of patients 6732Number of centers 182HLA‐Matching for HLA‐A, ‐B, ‐C and –DRB1 6732
7/8 2126 (32)8/8 4606 (68)
Age, median (range), years 6732 35 (<1‐72)Age at transplant 6732
≤ 10 660 (10)10‐19 875 (13)20‐29 1134 (17)30‐39 1319 (20)40‐49 1514 (22)50+ 1230 (18)
Recipient race/ethnicity 6648 Caucasian race, non‐Hispanic 5881 (88) African American race, non‐Hispanic 223 ( 3)Asian race, non‐Hispanic 96 ( 1)Pacific Islander race, non‐Hispanic 5 (<1)Native American race, non‐Hispanic 24 (<1)Hispanic, Caucasian race 247 ( 4)Hispanic, African American race 9 (<1)Hispanic, Asian race 2 (<1)Hispanic, race unknown 146 ( 2)
Other 15 (<1)Male sex 6732 3792 (56)Karnofsky prior to transplant > 90 6313 4566 (72)GvHD Prophylaxis 6732
Ex vivo T‐cell depletion alone 270 ( 4)Ex vivo T‐cell depletion + post‐tx immune suppression 524 ( 8)CD34 selection alone 8 (<1)CD34 selection + post‐tx immune suppression 65 ( 1)Cyclophosphamide alone 26 (<1)Cyclophosphamide + others 13 (<1)FK506 + MMF +‐ others 454 ( 7)FK506 + MTX +‐ others (except MMF) 2151 (32)FK506 + others (except MTX, MMF) 225 ( 3)FK506 alone 64 ( 1)CSA + MMF +‐ others (except FK506) 113 ( 2)CSA + MTX +‐ others (except FK506, MMF) 2552 (38)CSA + others (except FK506, MTX, MMF) 137 ( 2)CSA alone 50 ( 1)Other GVHD prophylaxis 80 ( 1)a – Data has not yet been CAP‐modeled.
72
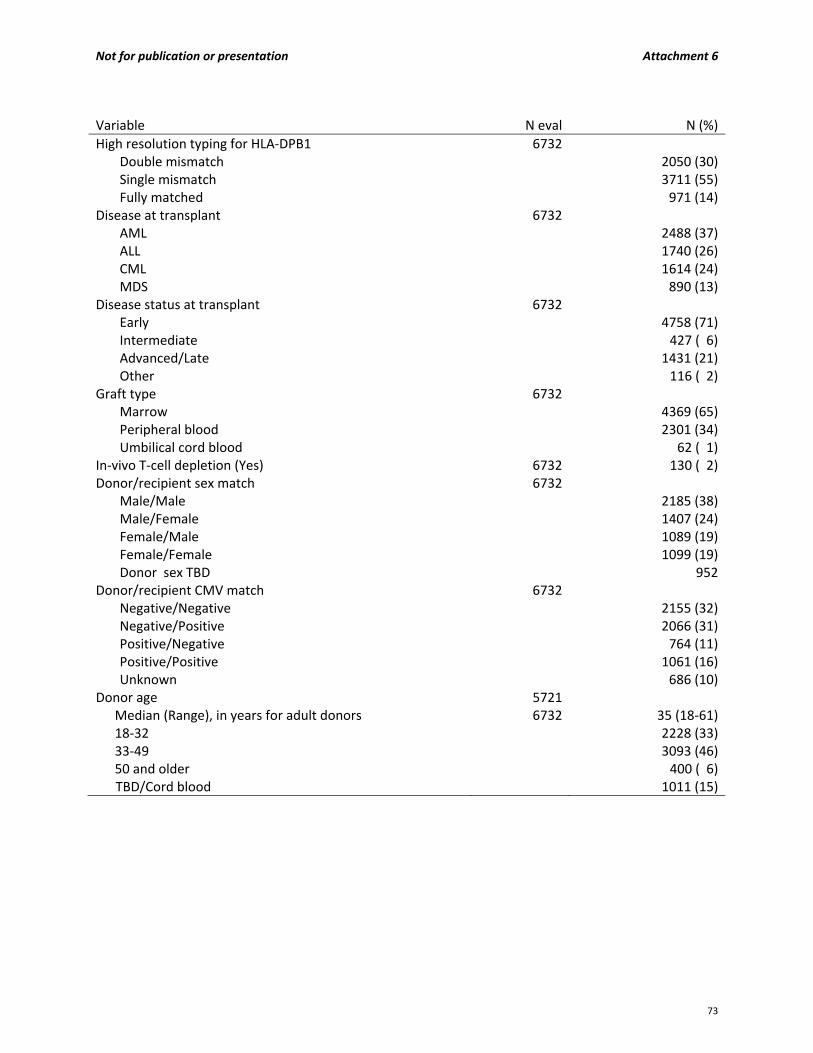
Not for publication or presentation Attachment 6
Variable N eval N (%)
High resolution typing for HLA‐DPB1 6732 Double mismatch 2050 (30)Single mismatch 3711 (55)Fully matched 971 (14)
Disease at transplant 6732 AML 2488 (37)ALL 1740 (26)CML 1614 (24)MDS 890 (13)
Disease status at transplant 6732 Early 4758 (71)Intermediate 427 ( 6)Advanced/Late 1431 (21)Other 116 ( 2)
Graft type 6732 Marrow 4369 (65)Peripheral blood 2301 (34)Umbilical cord blood 62 ( 1)
In‐vivo T‐cell depletion (Yes) 6732 130 ( 2)Donor/recipient sex match 6732
Male/Male 2185 (38)Male/Female 1407 (24)Female/Male 1089 (19)Female/Female 1099 (19)Donor sex TBD 952
Donor/recipient CMV match 6732 Negative/Negative 2155 (32)Negative/Positive 2066 (31)Positive/Negative 764 (11)Positive/Positive 1061 (16)Unknown 686 (10)
Donor age 5721 Median (Range), in years for adult donors 6732 35 (18‐61)18‐32 2228 (33)33‐49 3093 (46)50 and older 400 ( 6)
TBD/Cord blood 1011 (15)
73

Not for publication or presentation Attachment 6
Variable N eval N (%)
Donor race/ethnicity 5351 Caucasian race, non‐Hispanic 4757 (89)African American race, non‐Hispanic 175 ( 3)Asian race, non‐Hispanic 57 ( 1)Pacific Islander race, non‐Hispanic 2 (<1)Native American race, non‐Hispanic 80 ( 1)Hispanic, Caucasian race 43 ( 1)Hispanic, African American race 1 (<1)Hispanic, Native American race 2 (<1)Hispanic, race unknown 218 ( 4)Other 16 (<1)
Year of transplant 6732 1988 19 (<1)1989 57 ( 1)1990 86 ( 1)1991 122 ( 2)1992 156 ( 2)1993 173 ( 3)1994 241 ( 4)1995 269 ( 4)1996 272 ( 4)1997 312 ( 5)1998 312 ( 5)1999 352 ( 5)2000 386 ( 6)2001 378 ( 6)2002 317 ( 5)2003 310 ( 5)2004 450 ( 7)2005 504 ( 7)2006 563 ( 8)2007 555 ( 8)2008 422 ( 6)2009 336 ( 5)2010 62 ( 1)2011 35 ( 1)2012 21 (<1)2013 22 (<1)
Median follow‐up of survivors 2255 95 (2.7‐289)
74

Not for publication or presentation Attachment 7
Study Proposal 1311‐20/1311‐37 Study Title: Impact of human leukocyte antigen (HLA) haplotypes on outcomes of allogeneic transplantation for B‐cell non‐Hodgkin lymphomas (B‐NHL) PI Information: Basem M. William, MD, Case Western Reserve University, Cleveland, Ohio Brian T. Hill, MD, PhD, Cleveland Clinic, Cleveland, Ohio Marcos de Lima, MD, Case Western Reserve University, Cleveland, Ohio Marcelo A. Fernandez‐Vina, PhD, Stanford University School of Medicine, Stanford, California Specific Aims: This study will determine the impact of common human leukocyte antigen (HLA) alleles on the outcomes of B‐cell non‐Hodgkin’s lymphomas (B‐NHL) after allogeneic stem cell transplantation (alloSCT). Primary endpoints to be examined include:
Time to relapse, progression free (PFS), event free (EFS) and overall survival (OS)
Transplant related mortality at 100 days and 1, 3, and 5 years
Incidence and severity of acute and chronic graft versus host disease (GVHD)
Secondary endpoints will include:
Time to neutrophil or platelet engraftment
Incidence of organ toxicity
Incidence of secondary malignancies
Cause of death Scientific Justification: Non‐Hodgkin lymphoma (NHL) is a heterogeneous group of hematologic malignancies with varied aggressiveness and many therapeutic options. An estimated 66,360 new cases of NHL were diagnosed in the United States in 2011. B‐cell non‐Hodgkin (B‐NHL) lymphoma comprises approximately 85% of these cases. Transplantation, both autologous and allogeneic, has a role in the management of B‐cell lymphoma, and more than 5,000 hematopoietic cell transplantations (HCTs) are performed annually in North America for this indication. Diffuse large B‐cell lymphoma (DLBCL) is the most common type of lymphoma seen in developed countries, accounting for 30% of all newly diagnosed NHL. It is an aggressive lymphoma, and when treated with anthracycline and rituximab‐based chemotherapy, only half of the patients are cured with upfront therapy. (1) High‐dose therapy followed by autologous stem cell transplantation (autoSCT) has been the standard of care for patients with relapsed B‐NHL. The efficacy of autoSCT as salvage for such patients, in the post‐rituximab era, was recently questioned by the CORAL trial which demonstrated a dismal 23% PFS at 2 years.(2) Historically, allogeneic transplantation (alloSCT) was considered an option after failure of autoSCT but some centers have transplanted higher risk B‐NHL at first relapse or second complete remission (CR2). No prospective comparative studies have been completed in this setting.(1) The effectiveness of alloSCT in B‐NHL has been attributed to a graft‐versus‐leukemia (GVL) effect because of elimination of tumor cells by alloimmune effector lymphocytes. Durable responses were demonstrated
75

Not for publication or presentation Attachment 7
after alloSCT in follicular lymphomas (FL) however a higher transplant related mortality (TRM), related to myeloablative conditioning regimens, limited the widespread use of alloSCT for FL.(1) Earlier studies, including a large analysis from the Center for International Blood and Marrow Transplant Research (CIBMTR), (3) have demonstrated a differential GVL among B‐NHL with low/intermediate grade histologies like FL and mantle cell lymphomas (MCL) being more sensitive to GVL compared to their aggressive counterparts (DLBCL and Burkitt’s). The advent of reduced‐intensity conditioning (RIC) regimens has renewed interest in alloSCT, which reduces TRM while maintaining a GVL effect and therefore allows the treatment of elderly patients and/or patients with comorbidities.(4) A more recent analysis from the CIBMTR has shown that disease state was the main determining factor for outcomes after alloSCT regardless of the intensity of conditioning regimen in DLBCL.(5) Given the limited efficacy of autoSCT in the post‐rituximab era and the decreased TRM with RIC, it is more likely that the use of alloSCT in B‐NHL would be expanding. Further understanding of the factors likely to predict a more robust GVL response, and potentially better clinical outcomes, would be very useful in selecting patients with B‐NHL who are likely to benefit from alloSCT. Human leukocyte antigen (HLA) class I molecules are involved in the presentation of antigenic peptides to CD8+ cytotoxic T lymphocytes (CTLs), which is important for the development of cellular immunity during viral infections and in cancers.(6) Inherited variations within the HLA genes as well as variations in host immune responses have long been recognized to be associated with susceptibility to disease. CD8+ cytotoxic T lymphocytes (CTLs), which kill target cells presenting specific endogenous peptides on major histocompatibility complex (MHC) class I molecules, are recognized as the main effector cells in antitumour immunity and are the main mediators of GVL responses.(7) The presentation of certain tumor epitopes to CD8+ CTLs is restricted to specific HLA haplotypes. For instance, Zhang and colleagues have identified the myeloid azurophil granule protease cathepsin G (CG): an HLA‐A*0201‐restricted antigen on acute myeloid leukemia (AML) cells. They showed killing of primary AML by CG‐CTL, but not normal bone marrow. Blocking HLA‐A*0201 abrogated CG1‐CTL‐mediated cytotoxicity, further confirming HLA‐A*0201‐dependent killing. Finally, they showed functional CG‐CTLs in peripheral blood from AML patients following alloSCT.(8) HLA‐A2 is one of the most frequent HLA class I specificities and thus is extensively studied structurally and functionally. Many well characterized HLA‐A2 restricted epitopes have been tested for their therapeutic effects for viral infection or tumor formation in the HLA‐A2 transgenic mouse models.(9) Many tumor antigens are HLA‐A2 restricted and some cancer cells evade CD8+ CTLs by downregulating surface HLA‐A2 expression.(10) In HLA‐A2‐positive individuals, a major component of the CMV‐specific CD8+ T‐cell response is specific for CMV peptides presented by the HLA‐A2 allele.(11) A retrospective study by Nachbaur and colleagues analyzed the outcomes of 103 HLA‐identical sibling alloSCT recipients in relation to the CMV serostatus of their donors, and observed that both overall and disease‐free survival were significantly improved in HLA‐A2‐positive alloSCT recipients whose donors were CMV seropositive suggesting that HLA‐A2‐restricted CMV‐specific CD8+ CTLs might cross‐react with leukemia‐associated minor H antigens and contribute to a GVL effect.(12) Weng and colleagues have demonstrated that T‐cell leukemia/lymphoma (TCL1), an oncoprotein that is hyperexpressed on a myriad of malignant B‐cell including DLBCL, FL, and MCL, elicits HLA‐A2 restricted CD8+ CTL responses and CD8+ CTLs generated from patients with B‐NHL were capable of killing B‐NHL cells in vitro in an HLA‐A2 restricted fashion.(13) This data suggests a potential immunologic advantage from inheritance of HLA‐A2 haplotype however this has never been proven. In contrast, Khouri and colleagues have retrospectively analyzed 86 patients with chronic lymphocytic leukemia (CLL) and showed that RIC alloSCT produced an estimated 5‐year current PFS rate of 68.2% in HLA‐A1+/A2‐/B44‐ patients versus 15% for patients with none of the HLA factors described (p=0.02).(14) The etiology for that is unclear but it is possible that HLA‐
76
Not for publication or presentation Attachment 7
A2 subjects with CLL who progressed to require an alloSCT may have unfavorable biology that might have outweighed any potential immunologic advantage attributable to the HLA‐A2 haplotype. Study CK12‐02: A Retrospective Assessment of Outcomes of Patients who have Undergone Allogeneic Stem Cell Transplant for Chronic Lymphocytic Leukemia (CLL) Based on Histocompatibility Leukocyte Antigen (HLA) Type currently ongoing under the Chronic Leukemia Committee of the CIBMTR will attempt to validate these findings. There are limited reports on the relationship between HLA status and follicular lymphoma and its effect on transplant outcomes has never been explored. Wang, et al. reported an increased risk of follicular lymphoma with HLA‐DRB1*0101 [odds ratio (OR) 2.14, 95% confidence interval (CI) 1.40‐3.26, P < 0.001] and an inverse association with HLA‐DRB1*13 (OR = 0.48, 95% CI = 0.28‐0.82).(15) A recent secondary analysis of 204 follicular lymphoma (FL) patients participating in the Eastern Cooperative Oncology Group (ECOG) RESORT trial (E4402) treated with rituximab showed that patients homozygous for HLA‐C1 (C1C1) showed a trend towards a longer duration of response (p=0.06) as compared to those that were heterozygous (C1C2) or homozygous for HLA‐C2 (C2C2). Further analyses revealed that the influence of these HLA C specificities on clinical outcome could be related to the presence or absence of inhibitory and/or activating KIR genes(16) . In the case of diffuse large B‐cell lymphoma (DLBCL), in those patients treated with curative intention using cyclophosphamide, doxorubicin, vincristine, and prednisolone (CHOP)‐like regimen, DLBCL patients were found to have a higher phenotypic frequency of HLA‐DRB1*01 (29% vs 19.5%, P=.0008) and a lower frequency of HLA‐C*03 (6.4% vs 17.9%, P < .0005, Pc 5 .007) compared with healthy individuals.(17) Irrespective of the age‐adjusted International Prognostic Index, patients treated with CHOP‐like regimen plus rituximab and carrying the HLA‐B44 supertype had inferior 5‐year progression‐free (54% vs 71%, P5.019) and 5‐year overall (71% vs 92%, P=.001) survival compared with patients without this haplotype. The authors conclude that some HLA polymorphisms influence the development and outcome of DLBCL. This study will investigate the impact of the HLA combination HLA‐A1+, HLA‐A2‐ and HLA‐B44‐ on outcomes of alloSCT for B‐NHL. We plan to restrict our analysis to fully matched donor/recipient pairs as we are interested in examining the impact of the presence of specific HLA haplotypes, rather than HLA mismatches, on transplant outcomes. We elected to study B‐NHL preferentially as they are biologically less heterogeneous than T‐cell NHL(18) which, again, is more likely to yield statistically significant associations. It would be of particular interest to examine the impact of this HLA combination on the outcomes of common lymphomas specifically FL and DLBCL. Study Population: The study will include patients with the following:
Diagnosis of B‐NHL including FL grade I, II, DLBCL to include FL grade III, MCL, marginal zone lymphoma, small lymphocytic lymphomas, Burkitt’s lymphoma, B‐cell lymphoblastic lymphomas, and other B‐cell NHL
Age of 18 years or older
Allogeneic stem cell transplant for non‐Hodgkin lymphoma from fully matched (at HLA‐A, B, C, and DR) related (MRD) or matched unrelated donors (MUD)
Excluded are:
Patients with the diagnosis of T‐cell lymphomas or CLL
Any allele or antigen mismatches in HLA‐A, B, C, or DR
Umbilical cord transplants
Patients who have undergone more than one alloSCT
77

Not for publication or presentation Attachment 7
Graft purging, CD34+ selection, or any ex vivo graft manipulation Outcome Definitions:
Time to engraftment: Defined as time between day of transplantation and recovery of neutrophils and/or platelets.
Time to progression: Defined as time between day of transplantation and documentation of disease recurrence/progression. Patients alive and disease free will be censored at last follow up.
Event free survival: an event is defined as progression/recurrence or death.
Transplant Related Mortality: Defined as death within 28 days of transplantation or time to death without recurrence of disease.
Overall survival: time to death. Patients are censored at last follow‐up.
Causes of death: as defined by Copeland et al(19) Variables to be Analyzed: Patient Related:
Age at transplantation (≤60 vs. >60)
Karnofsky performance status (<70 vs. ≥70)
Gender (male vs. female)
CMV status in donor and recipient Disease related at diagnosis:
Histology (DLBCL, FL, MCL, MZL, other B‐NHL)
Stage at diagnosis (I/II vs. III/IV)
Age adjusted IPI
B‐symptoms (yes/no)
Bone marrow involvement (yes/no)
Extranodal/splenic involvement (yes/no) Disease related at transplant:
Type of lymphoma (relapsed or refractory)
B‐symptoms (yes/no)
Extranodal/splenic involvement (yes/no)
Bone marrow involvement (yes/no)
Time from diagnosis to transplant
Number of lines of therapy
Prior autologous transplant (yes/no)
Disease status o 2nd vs. 3rd or greater CR/PR o Duration of 1st CR
Disease sensitivity (sensitive vs. resistant vs. untreated) Peri‐transplant therapy:
Pre‐transplant o Rituximab exposure (yes/no) o Prior involved field radiotherapy (yes/no) Lung shielding (yes/no)
o Other prior radiotherapy
Post‐ transplant o Involved field radiotherapy (yes/no)
78
Not for publication or presentation Attachment 7
o Rituximab (yes/no) o Chemotherapy (yes/no) o Other
Post‐transplant outcomes:
Peri‐transplant performance status o Pre‐transplant organ dysfunction o Post‐transplant organ dysfunction (pneumonitis, VOD)
Post‐transplant outcomes o PFS o OS o Cumulative incidence of relapse o Sites of relapse
Graft versus host disease (GVHD) o Acute (site, grade) o Chronic (site, grade)
CMV reactivation o CMV viremia o Invasive CMV disease
Long term outcomes o Secondary malignancies o Organ dysfunction
Transplant related:
HLA combination HLA‐A1+, HLA‐A2‐ and HLA‐B44‐
Conditioning regimen o Myeloablative vs reduced‐intensity conditioning o Type of conditioning regimen o Dose of TBI and number of fractions o T‐cell depletion (antithymocyte globulin or alemtuzumab) o MRD vs MUD o Mismatches at HLA‐DQ and DP
Year of transplant
Stem cell source (bone marrow vs peripheral blood stem cells)
Time to neutrophil/platelet engraftment Data Requirements: Patients, disease and transplant related characteristics will be obtained from the CIBMTR database. No additional supplemental data collection is anticipated. Patient HLA type should be available in 100% of patients. Additional clinical details will include baseline characteristics including basic demographics and stage at diagnosis and relapse, and number of prior therapies including autologous stem cell transplant. Allo‐SCT outcomes including progression‐free survival, relapse, and overall survival will be collected. We will also collect data on the source of stem cells: whether they are from a related donor, unrelated donor or cord blood. HLA matching data will be collected. Study Design: Outcomes of patients who have undergone fully matched transplants (from matched sibling donor or 8 out of 8 matched unrelated donors) calculated relative to the date of transplant, until the event of interest, or until the date of last follow‐up. Relapse will be estimated using the cumulative incidence
79
Not for publication or presentation Attachment 7
method. Cox proportional hazards analysis will be used to identify prognostic factors. Survival will be estimated using the Kaplan–Meier. Comparison of baseline characteristics between the groups with and without the HLA combination HLA‐A1+, HLA‐A2‐ and HLA‐B44‐ will be made to other groups using the log‐rank test. Cox proportional hazard analysis will be used to identify univariable and multivariable risk factors for relapse and mortality. For the multivariable analysis, stepwise analysis will be used with a variable entry criterion of P<0.10 and a variable retention criterion of P<0.05. Cox analyses will be summarized as the hazard ratio (HR), 95% confidence interval for the HR and the corresponding P‐value. All statistical tests will be two‐sided, and P<0.05 was used to indicate statistical significance. Factors to be considered in multivariable analysis include HLA status (A1+, HLA‐A2‐ and HLA‐B4‐ or not), histology (FL, DLBCL, MCL, MZL, other B‐NHL), presence of absence of predisposing/protective alleles HLA‐DRB1*01:01 and HLA‐DRB1*13, disease status at the time of transplant (complete/partial remission vs. refractory disease), and type of preparative regimen (myeloablative vs. non‐myeloablative). Comparisons between the groups will be performed using a Cox proportional hazard model. Because there may be a selection or institutional bias in patients who receive a TBI based regimen vs. a non‐TBI based regimen, a propensity score will be used to refine the Cox model. The propensity score will be calculated using a logistic‐regression model using the following factors: age, gender, Karnofsky performance status pre‐transplant, disease stage, B‐symptoms, extranodal involvement, bone marrow involvement at diagnosis, number of regimens prior to transplant, prior autologous transplant, disease sensitivity prior to transplant, time from diagnosis to transplant, graft source, year of transplant, and transplant center. Finally, if time and resources permit, it may of interest to examine the impact of other alleles, beyond the HLA‐A1+, HLA‐A2‐ and HLA‐B44‐ combination, that are common on most world populations including HLA‐A1, A2, A3, A24, B7, B8, B35, B44, B60, B62, BW4, BW6, and CW7 on outcomes of alloSCT. We propose analyzing the impact of each haplotype separately and then common HLA‐A/B/C haplotype combinations. References:
1. Ayala E. Hematopoietic cell transplantation for B‐cell lymphoma: an update. Cancer control: Journal of the Moffitt Cancer Center 2012 Jul;19(3):175‐86.
2. Gisselbrecht C, Schmitz N, Mounier N et al. Rituximab maintenance therapy after autologous stem‐cell transplantation in patients with relapsed CD20(+) diffuse large B‐cell lymphoma: final analysis of the collaborative trial in relapsed aggressive lymphoma. J Clin Oncol 2012 Dec 20;30(36):4462‐9.
3. Bierman PJ, Sweetenham JW, Loberiza FR, Jr et al. Syngeneic hematopoietic stem‐cell transplantation for non‐Hodgkin's lymphoma: a comparison with allogeneic and autologous transplantation‐‐The Lymphoma Working Committee of the International Bone Marrow Transplant Registry and the European Group for Blood and Marrow Transplantation. J Clin Oncol 2003 Oct 15;21(20):3744‐53.
4. William BM, de Lima M. Advances in conditioning regimens for older adults undergoing allogeneic stem cell transplantation to treat hematologic malignancies. Drugs & Aging. 2013 Jun;30(6):373‐81.
5. Hamadani M, Saber W, Ahn KW et al. Impact of pretransplantation conditioning regimens on outcomes of allogeneic transplantation for chemotherapy‐unresponsive diffuse large B cell lymphoma and grade III follicular lymphoma. Biology of blood and marrow transplantation: journal of the American Society for Blood and Marrow Transplantation 2013 May;19(5):746‐53.
80
Not for publication or presentation Attachment 7
6. Chen KY, Liu J, Ren EC. Structural and functional distinctiveness of HLA‐A2 allelic variants. Immunologic Research 2012 Sep;53(1‐3):182‐90.
7. Banchereau J, Palucka AK. Dendritic cells as therapeutic vaccines against cancer. Nature Reviews Immunology 2005 Apr;5(4):296‐306.
8. Zhang M, Sukhumalchandra P, Enyenihi AA et al. A novel HLA‐A*0201 restricted peptide derived from cathepsin G is an effective immunotherapeutic target in acute myeloid leukemia. Clinical Cancer Research: an official journal of the American Association for Cancer Research 2013 Jan 1;19(1):247‐57.
9. Epstein H, Hardy R, May JS et al. Expression and function of HLA‐A2.1 in transgenic mice. Eur journal Immunol 1989 Sep;19(9):1575‐83.
10. Pandolfi F, Boyle LA, Trentin L et al. Expression of HLA‐A2 antigen in human melanoma cell lines and its role in T‐cell recognition. Cancer Research 1991 Jun 15;51(12):3164‐70.
11. Kuzushima K, Hayashi N, Kimura H et al. Efficient identification of HLA‐A*2402‐restricted cytomegalovirus‐specific CD8(+) T‐cell epitopes by a computer algorithm and an enzyme‐linked immunospot assay. Blood 2001 Sep 15;98(6):1872‐81.
12. Nachbaur D, Bonatti H, Oberaigner W et al. Survival after bone marrow transplantation from cytomegalovirus seropositive sibling donors. Lancet 2001;Oct 6;358(9288):1157‐9.
13. Weng J, Rawal S, Chu F et al. TCL1: a shared tumor‐associated antigen for immunotherapy against B‐cell lymphomas. Blood 2012 Aug 23;120(8):1613‐23.
14. Khouri IF, Bassett R, Poindexter N et al. Nonmyeloablative allogeneic stem cell transplantation in relapsed/refractory chronic lymphocytic leukemia: long‐term follow‐up, prognostic factors, and effect of human leukocyte histocompatibility antigen subtype on outcome. Cancer 2011 Oct 15;117(20):4679‐88.
15. Wang SS, Abdou AM, Morton LM et al. Human leukocyte antigen class I and II alleles in non‐Hodgkin lymphoma etiology. Blood 2010 Jun 10;115(23):4820‐3.
16. Erbe AK, Wang W, Ranheim EA et al. Specific KIR and HLA Genotypes Affect Outcomes Of Single‐Agent Anti‐CD20 Immunotherapy Of Follicular Lymphoma. Blood 2013 Oct 21, 2013;122(21):507.
17. Alcoceba M, Sebastian E, Marin L et al. HLA specificities are related to development and prognosis of diffuse large B‐cell lymphoma. Blood 2013 Aug 22;122(8):1448‐54.
18. William BM, Vose JM. T‐Cell Lymphomas. In: Younes A, Coiffier B, editors. Lymphoma Diagnosis and Treatment. 43. New York: Springer; 2012.
19. Copelan E, Casper JT, Carter SL et al. A scheme for defining cause of death and its application in the T cell depletion trial. Biology of blood and marrow transplantation: journal of the American Society for Blood and Marrow Transplantation. 2007 Dec;13(12):1469‐76.
81
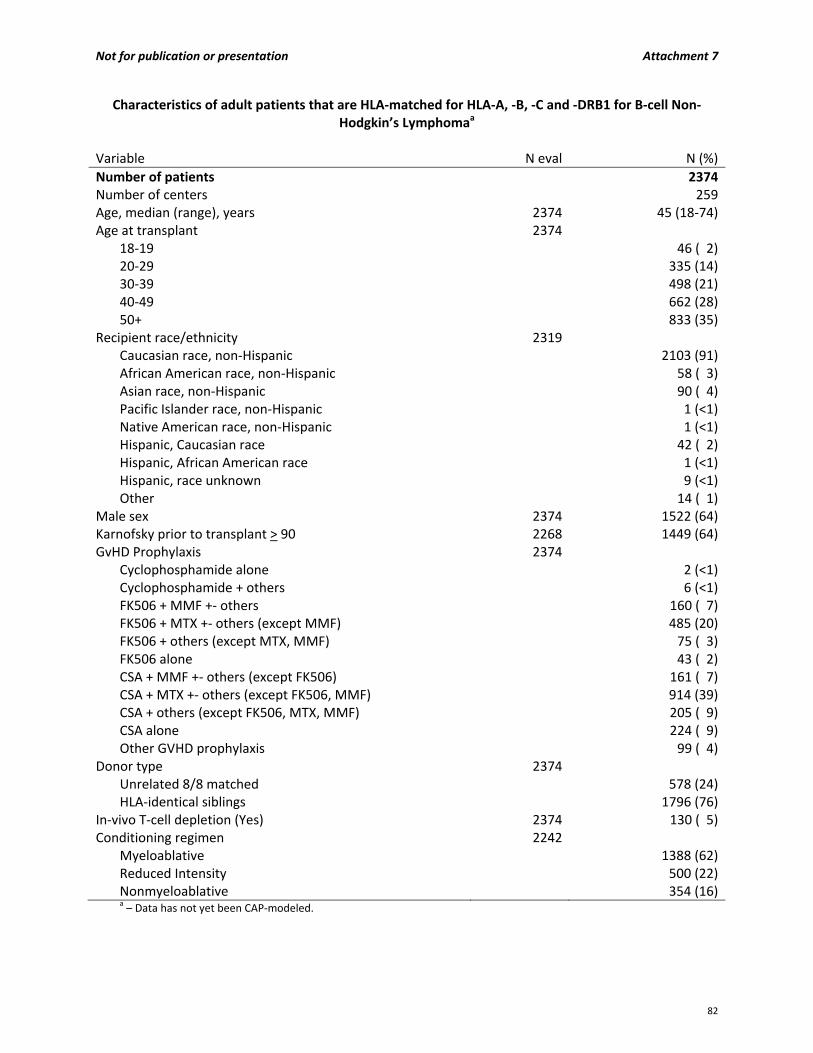
Not for publication or presentation Attachment 7
Characteristics of adult patients that are HLA‐matched for HLA‐A, ‐B, ‐C and ‐DRB1 for B‐cell Non‐Hodgkin’s Lymphomaa
Variable N eval N (%)
Number of patients 2374Number of centers 259Age, median (range), years 2374 45 (18‐74)Age at transplant 2374
18‐19 46 ( 2)20‐29 335 (14)30‐39 498 (21)40‐49 662 (28)50+ 833 (35)
Recipient race/ethnicity 2319Caucasian race, non‐Hispanic 2103 (91)African American race, non‐Hispanic 58 ( 3)Asian race, non‐Hispanic 90 ( 4)Pacific Islander race, non‐Hispanic 1 (<1)Native American race, non‐Hispanic 1 (<1)Hispanic, Caucasian race 42 ( 2)Hispanic, African American race 1 (<1)Hispanic, race unknown 9 (<1)Other 14 ( 1)
Male sex 2374 1522 (64)Karnofsky prior to transplant > 90 2268 1449 (64)GvHD Prophylaxis 2374
Cyclophosphamide alone 2 (<1)Cyclophosphamide + others 6 (<1)FK506 + MMF +‐ others 160 ( 7)FK506 + MTX +‐ others (except MMF) 485 (20)FK506 + others (except MTX, MMF) 75 ( 3)FK506 alone 43 ( 2)CSA + MMF +‐ others (except FK506) 161 ( 7)CSA + MTX +‐ others (except FK506, MMF) 914 (39)CSA + others (except FK506, MTX, MMF) 205 ( 9)CSA alone 224 ( 9)Other GVHD prophylaxis 99 ( 4)
Donor type 2374 Unrelated 8/8 matched 578 (24)HLA‐identical siblings 1796 (76)
In‐vivo T‐cell depletion (Yes) 2374 130 ( 5)Conditioning regimen 2242
Myeloablative 1388 (62)Reduced Intensity 500 (22)Nonmyeloablative 354 (16)a – Data has not yet been CAP‐modeled.
82
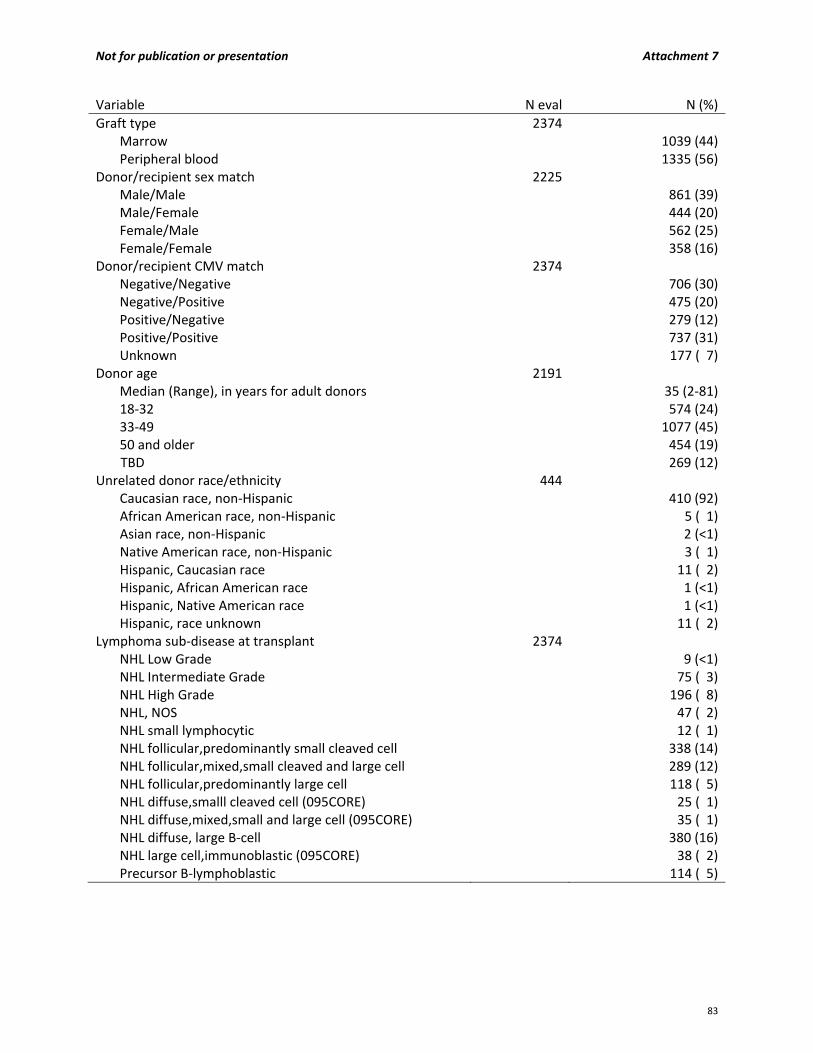
Not for publication or presentation Attachment 7
Variable N eval N (%)
Graft type 2374Marrow 1039 (44)Peripheral blood 1335 (56)
Donor/recipient sex match 2225Male/Male 861 (39)Male/Female 444 (20)Female/Male 562 (25)Female/Female 358 (16)
Donor/recipient CMV match 2374Negative/Negative 706 (30)Negative/Positive 475 (20)Positive/Negative 279 (12)Positive/Positive 737 (31)Unknown 177 ( 7)
Donor age 2191Median (Range), in years for adult donors 35 (2‐81)18‐32 574 (24)33‐49 1077 (45)50 and older 454 (19)
TBD 269 (12)Unrelated donor race/ethnicity 444
Caucasian race, non‐Hispanic 410 (92)African American race, non‐Hispanic 5 ( 1)Asian race, non‐Hispanic 2 (<1)Native American race, non‐Hispanic 3 ( 1)Hispanic, Caucasian race 11 ( 2)Hispanic, African American race 1 (<1)Hispanic, Native American race 1 (<1)Hispanic, race unknown 11 ( 2)
Lymphoma sub‐disease at transplant 2374NHL Low Grade 9 (<1)NHL Intermediate Grade 75 ( 3)NHL High Grade 196 ( 8)NHL, NOS 47 ( 2)NHL small lymphocytic 12 ( 1)NHL follicular,predominantly small cleaved cell 338 (14)NHL follicular,mixed,small cleaved and large cell 289 (12)NHL follicular,predominantly large cell 118 ( 5)NHL diffuse,smalll cleaved cell (095CORE) 25 ( 1)NHL diffuse,mixed,small and large cell (095CORE) 35 ( 1)NHL diffuse, large B‐cell 380 (16)NHL large cell,immunoblastic (095CORE) 38 ( 2)Precursor B‐lymphoblastic 114 ( 5)
83

Not for publication or presentation Attachment 7
Variable N eval N (%)
NHL snc,unclassified (095CORE) 2 (<1)Burkitt lym/Burkitt cell leukemia 65 ( 3)NHL snc,non‐burkitt (095CORE) 9 (<1)NHL mycosis fungoides 24 ( 1)NHL histiocytic (095CORE) 1 (<1)NHL mantle cell 329 (14)NHL composite,specify (095CORE) 16 ( 1)NHL large cell anaplastic,Ki 1+ (095CORE) 21 ( 1)Primary CNS lymphoma 2 (<1)NHL other, specify (095CORE) 102 ( 4)NHL small lymphoplasmacytic 18 ( 1)Extranodal marginal zone B‐cell of MALT 5 (<1)Nodal marginal zone B‐cell 14 ( 1)Splenic marginal zone B‐cell 10 (<1)Large granular lymphocytic leukemia 3 (<1)Tranformed low grade lymphoma (095CORE) 26 ( 1)Other B‐cell, spec 46 ( 2)Angiocentric lymphoma (095CORE) 1 (<1)High‐grade B‐cell lymphoma 4 (<1)
Year of transplant 23741975 1 (<1)1978 1 (<1)1979 2 (<1)1980 3 (<1)1981 3 (<1)1982 6 (<1)1983 10 (<1)1984 6 (<1)1985 17 ( 1)1986 32 ( 1)1987 32 ( 1)1988 31 ( 1)1989 55 ( 2)1990 70 ( 3)1991 75 ( 3)1992 86 ( 4)1993 59 ( 2)1994 62 ( 3)1995 88 ( 4)1996 95 ( 4)1997 128 ( 5)1998 91 ( 4)1999 120 ( 5)
84

Not for publication or presentation Attachment 7
Variable N eval N (%)
2000 127 ( 5)2001 130 ( 5)2002 138 ( 6)2003 146 ( 6)2004 126 ( 5)2005 161 ( 7)2006 163 ( 7)2007 130 ( 5)2008 77 ( 3)2009 55 ( 2)2010 10 (<1)2011 19 ( 1)2012 10 (<1)2013 9 (<1)
Median follow‐up of survivors 939 94 (<1‐363)
85

Not for publication or presentation Attachment 8
Study Proposal 1311‐72 Study Title: Assessing the similarity of the T cell receptor repertoire in allogeneic hematopoietic stem cell recipients with the same single human leukocyte mismatches PI Information: Everett Hurteau Meyer, MD, PhD, Stanford University, Stanford, California Specific Aims: Mismatch of human leukocyte antigens T cell allorecognition of mismatched human leukeocyte antigen is a significant risk factor in blood and marrow transplantation. Donor derived alloreactive T cells recognize HLA mismatches as an immune target, but the exact mechanics of T cell alloreactivity remains murky.1 Given the large diversity of HLA alleles, most mismatched antigen transplants are unique, however, we have surveyed data from the CIBMTR tissue collection and our own Stanford biobank repository and identified multiple instances of specific HLA allele mismatches for which post‐transplant recipient blood or PBMCs are available. We propose: 1. Extract the genomic DNA and sequence the post‐transplant V CDR3 T cell receptor repertoires of
four groups of HCT recipient with replicated HLA antigen mismatched. 2. Use biostatistical approaches to identify any shared T cell receptor among recipients that share HLA
mismatches. Determine if the incidence of shared clones is above that expected. 3. If shared TCR clones occur at high frequency in recipient blood, attempt single cell sorting and
identification of paired TCR V� sequence. Scientific Justification: The central question we hope to investigate is the reproducibility of allorecognition in hematopoietic cell transplantation. We hypothesize that individual HCT recipients with the same donor to recipient mismatch antigen will show a conserved TCR repertoire attributable to reproducible patterns of alloreactive to defined major mismatch antigens. Patient Eligibility Population: Any allogeneic HLA mismatched antigen transplant recipient with a mismatch that occurs multiple times. Study Design: We propose to obtain post‐recipient transplant samples of the identified HLA mismatches in Table 1. Ideally, these samples would be at day +30 post‐transplant, however we anticipate for this pilot that 30 +/‐ 30 days post‐transplant would be sufficient. We will require at genomic DNA from at least 1x106 cells which will provide a sampling of at least 1.5 x 105. The ideal cell count for analysis would be 1x107 cells. For Stanford samples, we bank 5x107 total PBMCs and will DNA extract from 1x107 cells. We will sequence at a depth of 1.5‐15 x 105 T cells per sample. We will PCR amplify the T cell receptor V� CDR3 region as described and perform analysis of sequence similarity between samples using a custom R script.
86

Not for publication or presentation Attachment 8
Methods:
We will use genomic DNA extraction and V TCR sequencing as described.2 References:
1. Archbold JK, Macdonald WA, Burrows SR et al. T‐cell allorecognition: a case of mistaken identity or déjà vu? Trends Immunol 2008; 29(5):220‐226.
2. Meyer EH, Hsu AR, Liliental J et al. A distinct evolution of the T‐cell repertoire categorizes treatment refractory gastrointestinal acute graft‐versus‐host disease Blood 2013; 121(24): 4955‐4962
HLA Mismatch (Donor/Recipient) Frequency
A*01:01/A*03:01 2A*02:01/A*03:01 2A*03:01/A*68:01 2 A*30:02/A*30:01 2 B*14:02/B*14:01 2 B*35:01/B*35:02 2 Cw*01:02/Cw*15:02 2 Cw*03:03/Cw*03:04 3 Cw*03:04:01/Cw*03:03:01 2 Cw*04:01:01/Cw*16:01 2 Cw*05:01/Cw*07:ET 2Cw*06:02/Cw*07:AG 3 Cw*07:02/Cw*07:AG 2Cw*07:AG/Cw*06:02 2Cw*15:02/Cw*02:02:02 2 DQB1*03:02/DQB1*03:01 5 DQB1*03:03/DQB1*02:02 2 DQB1*06:02/DQB1*06:03 3 DQB1*06:03/DQB1*06:02 2
Table 1. Frequency refers to occurrences of HCT with specific allelic mismatch identified as having recipient post-transplant blood samples in the Stanford and CIBMTR biobanks. Boxed mismatches occur at a frequency of 3 or greater and would be the target of initial investigation (n=4). Frequency of 2 (n=15).
87
Not for publication or presentation Attachment 9
Study Proposal 1312‐10 Study Title: mtDNA haplotypes and unrelated donor transplant outcomes PI Information: Michael R. Verneris, MD, University of Minnesota, Minneapolis, MN, [email protected] Julie A. Ross, PhD, University of Minnesota, Minneapolis, MN, [email protected]
Specific Aims: 1. To determine whether recipient mtDNA haplotypes are associated with unrelated donor (URD)
transplant outcomes (TRM, relapse, GVHD, DFS and OS). 2. To determine whether donor mtDNA haplotypes are associated with URD transplant outcomes
(TRM, relapse, GVHD, DFS and OS). 3. To determine whether mismatching between donor and recipient mtDNA haplotypes in the URD
setting are associated with transplant outcomes (TRM, relapse, GVHD, DFS and OS). Scientific Justification: Mitochondria are essential organelles of bacterial origin that are estimated to be captured by eukaryotic cells through endosymbiosis around 2‐3 billion years ago. Now, mitochondria play an essential role in cell biology by providing the biosynthetic cellular energy through oxidative phosphorylation and electron transport. Mitochondria contain ~16,600 base pairs of circular, double stranded DNA that encodes 37 genes. Unlike nuclear DNA, which is inherited from both maternal and paternal sources, paternal mitochondrial DNA (mtDNA) is degraded (by ubiquitination) during fertilization; thus mtDNA inheritance is almost exclusively maternal1. Like nuclear DNA, mtDNA undergoes deletions and mutations, leading to heterogeneity across individuals. Numerous studies have linked mtDNA mutations to a mitochondrial function as well as to a variety of diseases; most notably neurodegenerative diseases such as dystonia, mitochondrial myopathies, myoclonic epilepsy and raged red fibers (MERRF), mitochondrial myopathy, encephalomyopathy, lactic acidosis, stroke‐like symptoms (MELAS), Pearson syndrome (sideroblastic anemia, exocrine and pancreas dysfunction) and a host of other disorders. Of particular interest are more subtle changes in mtDNA that lead to mtDNA haplogroups that can be further divided into haplotypes based on restriction fragment length polymorphism. These haplotypes can be identified using standard PCR techniques2. There are approximately 30 mitochondrial haplotypes identified worldwide, with additional subdivisions among them. Importantly, mtDNA haplotypes are found in indigenous populations within specific regions of the world, suggesting either climatic selection or genetic drift3. There is increasing evidence of functional differences among specific mtDNA haplotypes4, and some studies have correlated mtDNA haplotypes with longevity. There have also been a number of association studies that have linked mtDNA haplotype to disease severity and/or response to therapy including: progression from HIV to AIDs 5, 6, survival after sepsis 7, progression to heart failure 8, cancer risk and progression (reviewed in9). Clearly, allogeneic hematopoietic cell transplantation (allo‐HCT) is a time of high metabolic demand, including the need for restoration of hematopoiesis, response to febrile episodes and septic events, as well the ongoing metabolic demands of graft vs. host disease and perhaps, graft vs. leukemia reactions. If genetic differences in mtDNA are associated with cellular energetics, then donor or recipient mtDNA
88

Not for publication or presentation Attachment 9
Figure 1: Multivariate Analysis of Transplant Outcomes For Matched Sibling Donors
and Recipients Based on m tDNA Haplotype. All outcomes were normalized to
haplotype K which was the most common (~40% of population). Outcomes are shown
for disease free survival (DSF), non‐relapse mortality (NRM), Relapse, and GVHD.
haplotypes may be important in transplant outcomes. As well, DNA sequence variations that result in amino acid changes can also serve as minor histocompatibility antigens. Thus, the details of mtDNA haplotype and matching/mismatching between donor and recipient may be important in transplantation. To date, no study has examined mtDNA haplotypes in the donor and recipient and whether they are associated with transplant outcomes. Given the important role for mitochondria in a number of biological processes related to allo‐HCT, we explored associations between mtDNA haplotypes of donors and recipients on outcomes following allo‐HCT. In preliminary work, we performed mtDNA typing on 198 sibling transplant recipients who were transplanted from 1995‐2005. The majority of patients received myeloablative conditioning (75.2%) for a variety of malignant hematological diseases. Most received peripheral blood stem cells (73%). GVHD prophylaxis was mainly with CSA/MTX (75%). Donor and recipient DNA was tested for the following 11 mtDNA haplotypes: H, I, J, K, K2, T, U, V, W, X, Z and a group that could not be further characterized using the primer set (referred to as “other”). As predicted, the vast majority of donor‐recipient pairs matched at mtDNA. There was no clear association between mtDNA haplotype and recipient race or HLA type. More than 80% of the mtDNA haplotypes occurred in non‐Hispanic Caucasians. To test associations between haplotype and transplant outcomes, multivariable Cox models were constructed, controlling for relevant variables. Given that haplotype H was the most common (41%), we adjusted all relative risks to haplotype H. As shown in figure 1, compared to the most common haplotype (H, 43/83), recipient siblings with haplotypes I (5/6) and V (5/5) were significantly more likely to die within 5 years (RR=3.01; CI=1.15‐7.86 and 4.63; 1.75‐12.25, respectively). Haplotypes W (3/4) and the ‘other’ (6/8) group experienced significantly higher aGVHD II‐IV events (RR=2.1, 1.1‐2.4; and 4.3, 1.5‐11.7, respectively). For aGVHD III‐IV, patients with U (n=5/19) and V (2/5) experienced significantly higher events than H (9/83); there were no events for K and K2.
89
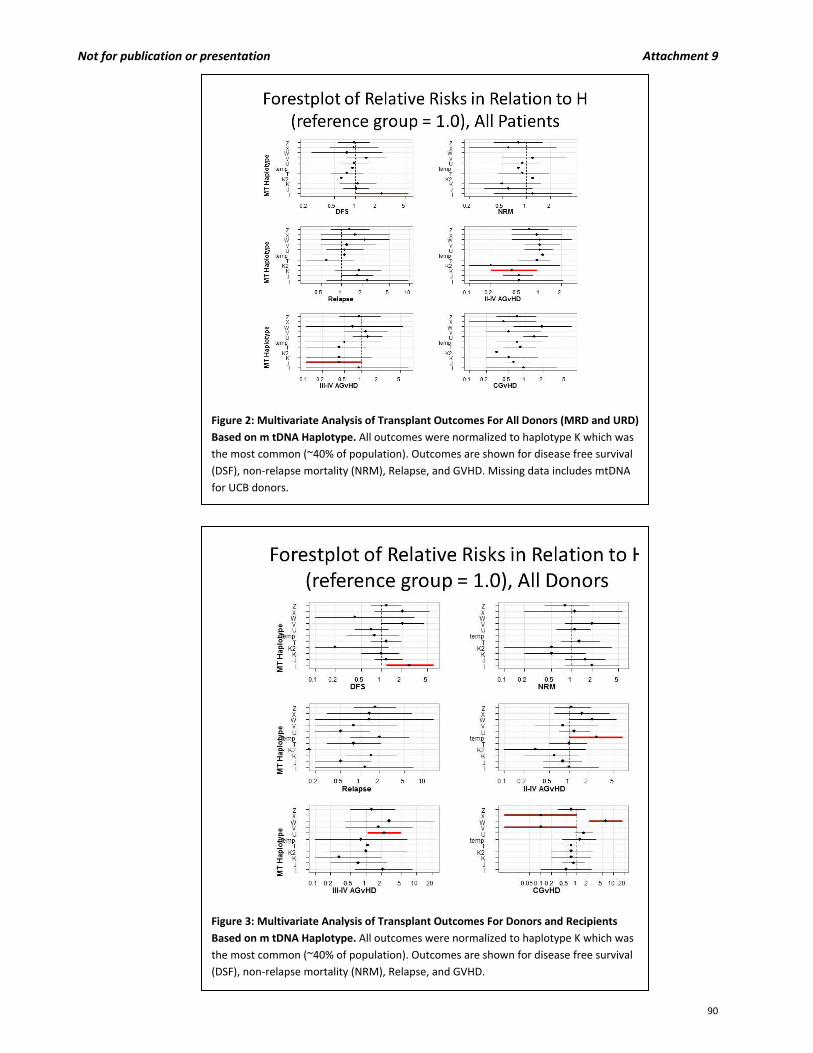
Not for publication or presentation Attachment 9
Figure 2: Multivariate Analysis of Transplant Outcomes For All Donors (MRD and URD)
Based on m tDNA Haplotype. All outcomes were normalized to haplotype K which was
the most common (~40% of population). Outcomes are shown for disease free survival
(DSF), non‐relapse mortality (NRM), Relapse, and GVHD. Missing data includes mtDNA
for UCB donors.
Figure 3: Multivariate Analysis of Transplant Outcomes For Donors and Recipients
Based on m tDNA Haplotype. All outcomes were normalized to haplotype K which was
the most common (~40% of population). Outcomes are shown for disease free survival
(DSF), non‐relapse mortality (NRM), Relapse, and GVHD.
90

Not for publication or presentation Attachment 9
The above analysis which used siblings (that have identical mtDNA haplotype) could not distinguish between whether mtDNA of the donor or recipient played differing roles in transplant outcomes. We then combined the sibling cohort with a group of URD transplants (UCB, BM and PBSC) to address this question. In this analysis, we were able to obtain mtDNA from an additional 116 donors and 223 recipients (cord DNA was not available for study). Combining the siblings and the URDs, we performed a larger analysis based on donor and recipient mtDNA haplotype (Figure 2 and 3, respectively). When considering outcomes for all recipients: compared to H (78/156), fewer aGVHD II‐IV events were observed for J (17/59) and K (6/22) (RR=0.47, 0.28‐0.78; RR=0.40, 0.17‐0.93, respectively). Considering all donors, I (6/7) donors were associated with a 2.68 fold increased risk of death in recipients in five years (CI=1.15‐6.24) compared to H donors (68/127), while only 1/7 and 1/4 patients receiving a transplant from a K2 or W donor, respectively, died. Moreover, no patients who received a transplant from a K2 donor (n=7) relapsed compared to 27/127 H donors. Patients who received transplants from U donors (n=4/34) were also less likely to relapse. In conclusion, while small in number for any particular haplotype, these data suggest that donor and recipient haplotype may be associated with increased risk for a variety of transplant associated outcomes. Study Population: We would like to request DNA from an existing large CIBMTR data set (n=~5,000) in URDs, where donor and recipient DNA is available. Ideally, additional inclusion criteria would include similarity at the following:
Disease (hematological malignancies)
Time of transplant (2000‐2010)
Patient related factors (age, KPS, CMV, gender, CR status)
Conditioning (TBI‐based myeloablative conditioning)
A uniform stem cell source (either PBSC or BM) with no graft manipulation (including in vivo TCD), matched at HLA‐A, ‐B, ‐C and –DRB1 (? DQ)
Similar GVHD prophylaxis (Calcineurin inhibitor based therapy)
Methods and Study Design: mtDNA haplotype would be determined as above. Multivariate models would be constructed controlling for relevant factors (depending on the final data set). Comparisons would be made across mtDNA haplotype grouping for the various transplant outcomes (NRM, aGVHD, relapse and DFS) to determine whether any of these haplotypes in either the donor or the recipient are associated with transplant outcomes. Lastly, donors and recipients would be grouped into either mtDNA “matched” or “mismatched” groups and we will determine whether mtDNA (mis)matching impacts the above stated transplant outcomes. References:
1. Sutovsky, P., Moreno, R. D., Ramalho‐Santos, J. et al. Ubiquitin tag for sperm mitochondria. Nature 1999; 402, 371‐372.
2. Raby, B. A., Klanderman, B., Murphy, A. et al. A common mitochondrial haplogroup is associated with elevated total serum IgE levels. J Allergy Clin Immunol 2007;120, 351‐358.
3. Wallace, D. C. Mitochondria, bioenergetics, and the epigenome in eukaryotic and human evolution. Cold Spring Harbor symposia on quantitative biology 2009;74, 383‐393.
4. Kenney, M. C., Chwa, M., Atilano, S. R. et al. Molecular and bioenergetic differences between cells with African versus European inherited mitochondrial DNA haplogroups: Implications for population susceptibility to diseases. Biochimica et biophysica acta 2014;1842, 208‐219.
91
Not for publication or presentation Attachment 9
5. Guzman‐Fulgencio, M., Jimenez, J. L., Garcia‐Alvarez, M. et al. Mitochondrial haplogroups are associated with clinical pattern of AIDS progression in HIV‐infected patients. J Acquir Immune Defic Syndr 2013;63, 178‐183.
6. Micheloud, D., Berenguer, J., Guzman‐Fulgencio, M. et al. European mitochondrial DNA haplogroups and metabolic disorders in HIV/HCV‐coinfected patients on highly active antiretroviral therapy. J Acquir Immune Defic Syndr 2011;58, 371‐378.
7. Baudouin, S. V., Saunders, D., Tiangyou, W. et al. Mitochondrial DNA and survival after sepsis: a prospective study. Lancet 2005;366, 2118‐2121
8. Gallardo, M. E., Garcia‐Pavia, P., Chamorro, R. et al. Mitochondrial haplogroups associated with end‐stage heart failure and coronary allograft vasculopathy in heart transplant patients. European heart journal 2012;33,346‐353
9. Theodoratou, E., Din, F. V., Farrington, S. M. et al. Association between common mtDNA variants and all‐cause or colorectal cancer mortality. Carcinogenesis 2010;31, 296‐301
92

Not for publication or presentation Attachment 9
Characteristics of patients that are high‐resolution matched for HLA‐A, ‐B, ‐C and ‐DRB1, have diseases of AML/ALL/CML/MDS and have donor/recipient paired samples available a
Variable N eval N (%)
Number of patients 4207Number of centers 166Age, median (range), years 4207 44 (<1‐74)Age at transplant 4207
≤ 10 247 ( 6)10‐19 356 ( 8)20‐29 571 (14)30‐39 593 (14)40‐49 856 (20)50+ 1584 (38)
Recipient race/ethnicity 4139Caucasian race, non‐Hispanic 3771 (91) African American race, non‐Hispanic 103 ( 2)Asian race, non‐Hispanic 53 ( 1)Pacific Islander race, non‐Hispanic 3 (<1)Native American race, non‐Hispanic 9 (<1)Hispanic, Caucasian race 156 ( 4)Hispanic, African American race 3 (<1)Hispanic, Asian race 1 (<1)Hispanic, race unknown 33 ( 1)Other 7 (<1)
Male sex 4207 2348 (56)Karnofsky prior to transplant > 90 3798 2582 (68)GvHD Prophylaxis 4207
FK506 + MMF +‐ others 674 (16)FK506 + MTX +‐ others (except MMF) 2009 (48)FK506 + others (except MTX, MMF) 208 ( 5)CSA + MMF +‐ others (except FK506) 308 ( 7)CSA + MTX +‐ others (except FK506, MMF) 936 (22)CSA + others (except FK506, MTX, MMF) 72 ( 2)
Disease at transplant 4207AML 2011 (48)ALL 798 (19)CML 523 (12)MDS 875 (21)
Disease status at transplant 4207Early 2973 (71)Intermediate 157 ( 4)Advanced/Late 912 (22)Other 165 ( 4)
Graft type 4207Marrow 1522 (36)Peripheral blood 2685 (64)a – Data has not yet been CAP‐modeled.
93

Not for publication or presentation Attachment 9
Variable N eval N (%)
HLA typing for HLA‐DQB1 at high‐resolution Double Mismatch 988 (29)Single Mismatch 1892 (55)Fully matched 535 (16)
Conditioning regimen 4207Myeloablative 3015 (72)Reduced Intensity 887 (21)Nonmyeloablative 210 ( 5)Other 95 ( 2)
Donor/recipient sex match 4207Male/Male 1214 (40)Male/Female 806 (26)Female/Male 506 (17)Female/Female 520 (17)TBD Donor sex 1161
Donor/recipient CMV match 4207Negative/Negative 1290 (31)Negative/Positive 1406 (33)Positive/Negative 465 (11)Positive/Positive 822 (20)Unknown 224 ( 5)
Donor age 4207Median (Range), in years 34 (18‐61)18‐32 1385 (33)33‐49 1412 (34)50 and older 174 ( 4)TBD 1236 (29)
Donor race/ethnicity 2802Caucasian race, non‐Hispanic 2545 (91)African American race, non‐Hispanic 69 ( 2)Asian race, non‐Hispanic 32 ( 1)Pacific Islander race, non‐Hispanic 2 (<1)Native American race, non‐Hispanic 37 ( 1)Hispanic, Caucasian race 27 ( 1)Hispanic, Native American race 1 (<1)Hispanic, race unknown 84 ( 3)Other 5 (<1)
94
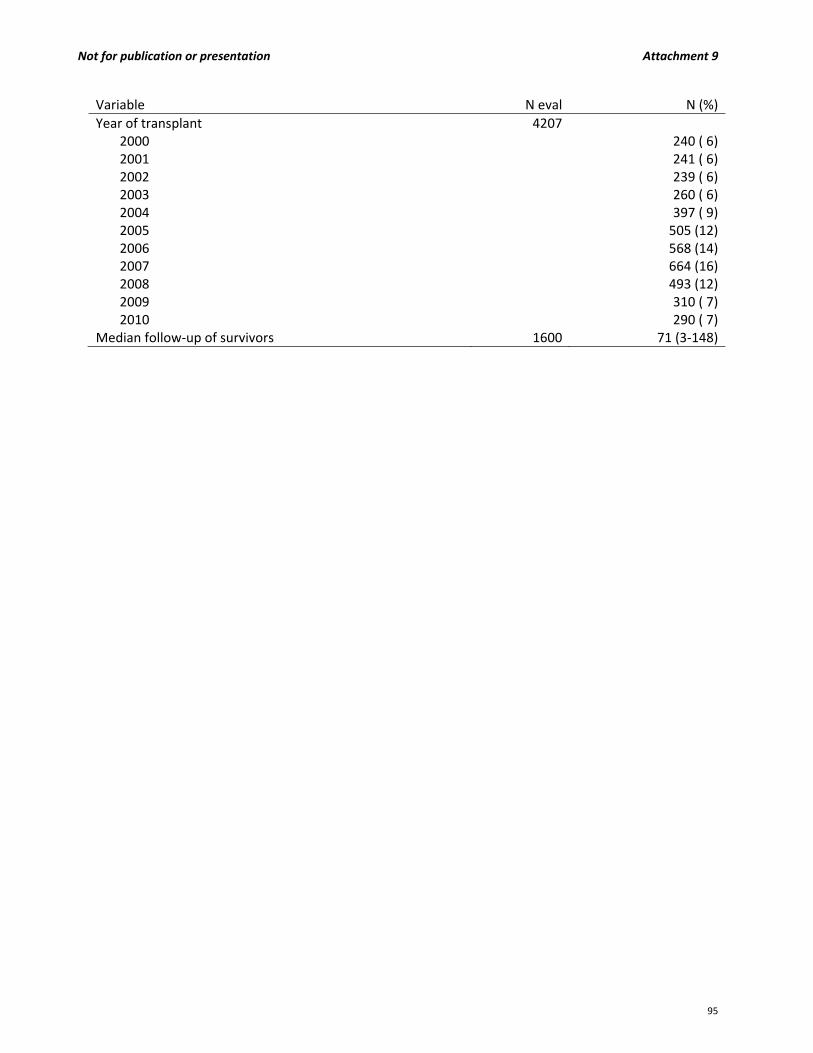
Not for publication or presentation Attachment 9
Variable N eval N (%)
Year of transplant 42072000 240 ( 6)2001 241 ( 6)2002 239 ( 6)2003 260 ( 6)2004 397 ( 9)2005 505 (12)2006 568 (14)2007 664 (16)2008 493 (12)2009 310 ( 7)2010 290 ( 7)
Median follow‐up of survivors 1600 71 (3‐148)
95
Not for publication or presentation Attachment 10
TO: Immunobiology Working Committee Members FROM: Stephen Spellman, MBS; Co‐Scientific Director for the Immunobiology WC Stephanie Lee, MD, MPH; Co‐Scientific Director for the Immunobiology WC RE: Studies in Progress Summary
HLA GENES IB12‐01: Impact of unrelated donor HLA‐mismatch in reduced‐intensity conditioning allogeneic hematopoietic stem cell transplantation outcomes (J Koreth): The goal of this study is to evaluate the impact of HLA mismatching in the reduced intensity conditioning setting. The analysis was presented at the 2013 ASH annual meeting and a draft manuscript is in progress. IB12‐02: Impact of unrelated donor HLA‐mismatch in myeloablative conditioning allogeneic hematopoietic stem cell transplantation outcomes (J Pidala/C Anasetti): The primary objective of the study is to re‐evaluate the impact of HLA mismatching described in the Lee et al. Blood manuscript from 2007 in larger more modern cohort. The analysis received a best abstract award at the 2014 BMT Tandem meetings and a draft manuscript is in progress. IB12‐03: Effect of genetic ancestry matching on HSCT outcomes (A Madbouly/M Maiers/N Majhail): The goal of the study is to evaluate the genetic ancestry disparity between donor‐recipient pairs and analyze the impact of the disparity on transplant outcome. A pilot cohort of transplant pairs was typed and study approved for release of the full cohort. IB13‐01: The effect of allele‐level HLA‐matching on survival after umbilical cord blood transplantation for non‐malignant diseases in children. (P Veys/M Eapen) : The primary objective of the study is to evaluate the impact of allele‐level HLA matching at HLA‐A, B, C and DRB1 on umbilical cord blood transplantation for non‐malignant disease in children. This is a collaborative study between the CIBMTR, UK and Eurocord. A draft protocol is under development. IB13‐02: Effects of HLA Class I Amino Acid Mismatches on Stem Cell Transplant Outcomes (SR Marino/SM Lee/T Karrison/TA Binkowski/A Artz): The main goal of the study is to validate the results of Dr. Marino’s prior discovery analysis that identified a select group of HLA Class I amino acid substitutions that are associated with poor transplant outcomes. The analysis is in progress. IB13‐03: Significance of HLA Class I and II Allelic Mismatching Within and Outside of HLA Supertypes among Recipients of Single‐Allele Mismatched Unrelated Allogeneic Hematopoietic Stem Cell Transplantation: A CIBMTR and NMDP Research Study (A Lazaryan/D Weisdorf/M Arora) : The primary objective of the study is to determine the impact of HLA mismatches that occur within or outside of HLA supertype clusters. The protocol and datafile are under development.
96
Not for publication or presentation Attachment 10
IB13‐08: Short and long term survival assessment of post HSCT transplantation using predictive modeling on a Bayesian network framework. (R Abdi/G Alterovitz/D McDermott): The primary objective of the study is to evaluate 100 day, 1 year and 5 year survival following related or unrelated donor HCT for hematological malignancies using a Bayesian network framework. The protocol and datafile are under development. IB13‐09: The development of Machine Learning based classifiers to define the alloreactivity of HLA mismatches in unrelated donor hematopoietic stem cell transplantation (Y Louzoun): The main goal of this study is to classify alloreactivity of HLA Class I mismatches based on peptide repetoire differences and apply Machine Learning based classifiers to evaluate the impact on HCT outcome. The protocol and datafile are under development. CYTOKINE/CHEMOKINE None. NK/KIR R02‐40/R03‐63: Choosing donors with favorable KIR B genotypes for unrelated hematopoietic cell transplantation (HCT) results in superior relapse protection and better relapse‐free survival for patients with acute myeloid leukemia (AML) (J Miller): This is an ongoing study in support of Dr. Miller’s NK Biology program project grant. R04‐74: Functional significance of Killer‐IG‐ligand genes in HLA‐matched and mismatched unrelated hematopoietic cell transplantation (HCT) (K Hsu / B DuPont): The purpose of this study is to determine the influence of donor KIR genotypes and haplotypes on HCT for leukemia. This is a collaborative study with the IHWG and is an ongoing effort. IB07‐03: Analysis of KIR ligands in reduced intensity conditioning allogeneic hematopoietic stem cell transplantation (HCT) (R Sobecks): The objectives of this study are to evaluate the clinical effects of KIR ligand absence in recipients of HLA matched and mismatched unrelated donor RIC HCT for myeloid malignancies. The analysis was presented at the 2013 ASH annual meeting and a draft manuscript is in progress. IB08‐06: KIR ligands in umbilical cord blood hematopoietic cell transplantation (HCT) (R Sobecks/V Rocha/M Eapen): The goal of the study is evaluate the role of HLA‐defined KIR ligands on the outcome of umbilical cord blood transplantation for acute leukemia. The study is a collaborative effort between the CIBMTR and Eurocord. The analysis is in progress. IB11‐05: KIR genotyping and Immune function in MDS patients prior to unrelated donor transplantation (E Warlick/J Miller): The goal of this study is assess the correlation of NK cell function with disease progression in MDS and potentially develop therapeutic immune strategies to control MDS progression. The retrospective cohort provided by the CIBMTR will be compared to a prospective cohort of newly diagnosed MDS patients from the University of Minnesota. The results of the pilot cohort analysis were presented at the 2013 ASH annual meeting. The study is proceeding with the full cohort. IB12‐04: Determining the Effects of HLA‐C KIR Ligand Expression on Outcomes of Unrelated Hematopoietic Stem Cell Transplantation (J Venstrom): The objective of the study is to determine the influence of high and low expression HLA‐C encoded KIR ligands on the transplant outcome and define a donor selection strategy that will optimize NK cell alloreactivity. The analysis is in progress.
97
Not for publication or presentation Attachment 10
IB12‐04B: Effect of HLA‐C allele matching in the context of recipient HLA‐C‐encoded KIR ligand grouping (C1 or C2) on the outcome of unrelated hematopoietic stem cell transplantation (HSCT) (J Fischer/M Uhrberg): The main goal of the study is to evaluate the effect of HLA‐C mismatches on HCT outcome based on KIR ligand group assignments. The protocol and datafile are under development. IB12‐06: Natural killer cell genomics and outcomes after allogeneic transplantation for lymphoma (V Bachanova/J Miller/D Weisdorf/L Burns): The goal of the study is to evaluate the influence of KIR genotype and ligands on the outcome of allogeneic transplantation for Non‐Hodgkin lymphoma. The study will KIR genotype a cohort of unrelated and related donor recipient pairs and test for correlation with relapse and survival. The analysis is in progress. IB13‐05: The Impact Of MHC Class I Chain‐Related Gene A (MICA) Donor‐Recipient Mismatches and MICA‐129 Polymorphism On Unrelated Donor Hematopoietic Stem Cell Transplants (HSCT) For Hematological Malignancies (M Askar/R Sobecks): The primary objective of the study is to evaluate the impact of MICA allele and MICA‐129 SNP mismatches on HCT outcomes. A draft manuscript is in progress. OTHER GENES R04‐76: Identification of functional single nucleotide polymorphisms (SNPs) in unrelated hematopoietic cell transplantation (HCT) (E Petersdorf): This study proposes to identify novel major histocompatibility complex resident SNPs of clinical importance. HLA matched pairs were genotyped for 1120 MHC SNPs and correlated with outcomes. This is a collaborative study with the IHWG. The study was published in Blood. IB08‐08: Genome‐wide association in unrelated donor hematopoietic cell transplant (HCT) recipients and donors (R Goyal): This study hypothesizes that an unbiased recipient‐donor genome‐wide association (GWA) study will identify genes associated with risk of acute graft versus host disease (aGvHD) after HLA‐matched unrelated donor HCT. Preliminary results suggested an association with specific HLA‐DPB1 alleles and aGVHD. A validation analysis is in progress to confirm the preliminary results. IB09‐04: Donor/recipient gene polymorphisms of drug metabolism and in innate immune response post allele‐matched unrelated donor hematopoietic stem cell transplantation (HCT) (V Rocha): This study is designed to validate associations between polymorphisms in drug metabolism and innate immune response genes and outcomes previously identified in matched sibling donor HCT in the HLA‐matched unrelated donor HCT setting. Analysis is underway. IB09‐05: Identification of functional single nucleotide polymorphisms (SNPs) in umbilical cord blood transplant (E Petersdorf): The primary hypothesis of the study is that umbilical cord blood units and recipients differ for genome‐wide single nucleotide polymorphism and gene copy number variation and that these differences may define putative transplant outcome determinants. Testing is underway. IB09‐06/RT09‐04: Genetic susceptibility to transplant‐related mortality after matched unrelated stem cell transplant (T Hahn): This is a joint study with the Regimen Related Toxicity working committee and is supported by an R01 grant to Drs. Hahn and Sucheston. This study will test for a genetic association with transplant‐related and overall mortality in recipients of myeloablative and reduced intensity
98
Not for publication or presentation Attachment 10
conditioning matched unrelated donor HCT. Sample testing has been completed and the analysis is in progress. IB09‐07: Clinical significance of genome‐wide variation in unrelated donor hematopoietic stem cell transplantation (HCT) (E Petersdorf): This study is designed to assess the impact of genome‐wide variation between donors and recepients in HLA matched unrelated donor HCT. This is a collaborative study with the IHWG. IB10‐01: Donor and recipient telomere length as predictors of outcomes after hematopoietic stem cell transplant in patients with acquired severe aplastic anemia (S Gadalla): This study will explore the role that telomere length plays in outcomes after HCT for SAA and other bone marrow failure disorders. The analysis will be presented at the 2014 BMT Tandem meetings and a draft manuscript is in progress. IB10‐03: TLR and HMGB1 gene polymorphisms in unrelated haematopoietic stem cell transplantation (K Müller/ B Kornblit): The objective of this study is to validate single center findings of a correlation between High Mobility Group Box 1 (HMGB1) polymorphism in the recipient and relapse rates following HLA matched unrelated donor HCT. A draft manuscript is in progress. IB10‐04: A validation study of the role of base excision repair pathway as a predictor of outcome after hematopoietic stem cell transplant (M Arora): This study is designed to validate findings from a single center that noted a correlation between SNPs in the DNA repair genes and relapse and TRM after HLA matched unrelated donor HCT. A draft manuscript is in progress. IB11‐02: Impact of CTLA4 single nucleotide polymorphisms on outcome after unrelated donor transplant (M Jagasia/W Clark/B Savani/S Sengsayadeth): The aim of the study is to validate findings from a single center analysis that found an association between CTLA4 single nucleotide polymorphisms and relapse, acute and chronic GVHD in unrelated donor HCT for hematological malignancies. The analysis was presented at the 2013 ASH annual meeting and manuscript submitted to BBMT. IB12‐05/RT10‐01: Plasma YKL‐40 and CHI3L1 genotype to predict mortality after allogeneic hematopoietic cell transplantation (HCT) (B Kornblit): The goals of the study are to describe the variation in YKL‐40 (inflammatory marker) plasma levels in recipients pre‐transplant and donors pre‐donation and assess the prognostic value in predicting transplantation outcomes. In addition, the plasma levels will be correlated to polymorphisms in the CHI3L1 promoter genotype. Plasma testing is complete and data analysis is underway. IB13‐04: Discrepancy analysis of microsatellite loci as a proxy measure for ancestral differentiation between donors and recipients: correlation between high scores and poorer overall survival in high resolution matched unrelated donor transplantation (J Harvey/C Steward/ V Rocha): The primary objective of the study is to validate a single center study noting a correlation between microsatellite variation in donors and recipients and HCT outcome. The protocol is complete and testing is in progress. SENSITIZATION and TOLERANCE R03‐65s: Detection of H‐Y antibodies in healthy female donors: Does H‐Y presensitization predict male hematopoietic stem cell transplantation (HCT) outcome (D Miklos): The goal of the study is to analyze the transfer of HY sensitization in sex mismatched HCT. The results will be presented at the 2014 BMT Tandem meetings and a draft manuscript is in progress.
99
Not for publication or presentation Attachment 10
IB06‐09s: Detection of HLA antibody to the mismatched antigen in single antigen HLA‐mismatched unrelated donor transplantation (HCT): Is it associated with GVHD outcome? (S Arai): Draft manuscript is underway and expected to be submitted in 2014. IB11‐01: Analysis of the NIMA effect on the outcome of unrelated PBSC/BM transplantation (G Ehninger/J van Rood/A Schmidt): The goal of this study is to determine whether matching for NIMA in the selection of unrelated donors can lead to better outcomes. The study was restricted to transplants where the donors were supplied by the DKMS. The DKMS team will attempt to collect samples from each donor’s mother for HLA typing and assignment of NIMA matching but too few NIMA matches were identified for analysis. Additional recent cases were identified to attempt to increase the sample size. This is a collaborative study with the EBMT Immunobiology Working Party. IB11‐07: Effect of Rituximab and ABO mismatch (D Miklos/A Logan): The aim of the study is to validate the finding of a single center analysis that found an association between ABO minor mismatch and increased acute GVHD. A draft manuscript is underway. MINOR HISTOCOMPATIBILITY ANTIGENS IB11‐08: Synergism between minor and major histocompatibility antigens (E Spierings): The goal of the study is to evaluate the interaction between HLA‐DPB1 mismatching and female into male (HY mismatched) transplantation to determine whether there is a synergistic effect on transplant outcome. Multivariate analysis revealed a synergistic interaction between HLA‐DP mismatching and H‐Y mismatching on acute GVHD grades III‐IV. A draft manuscript is underway. Approved studies not yet initiated: HLA GENES CYTOKINE/CHEMOKINE IB08‐04: Immune response gene polymorphisms in unrelated donor hematopoietic cell transplantation (HCT) in children (K Muller): Study deferred pending completion of an EBMT preliminary analysis. NK/KIR OTHER GENES IB13‐06: Role of the complement system in graft‐versus‐host disease (V Afshar‐Kharghan /J Belmont/C Amos). Study deferred pending receipt of grant funding. IB13‐07: Impact of donor signal‐regulatory protein alpha (SIRPα) polymorphism on outcome of allogeneic hematopoietic stem cell transplantation (allo‐HSCT) (A Gassas/J Danska/S Rajakumar): Study deferred pending receipt of grant funding. SENSITIZATION AND TOLERANCE IB06‐10: Evaluation of the impact of exposure to non‐inherited maternal antigens (NIMA) during fetal life and breast feeding and to the inherited paternal antigens during pregnancy on the clinical outcome of hematopoietic cell transplantation (HCT) from haploidentical family members (J Van Rood): The study is deferred pending activation in the EBMT Immunobiology Working Party.
100
Not for publication or presentation Attachment 10
MINOR HISTOCOMPATIBILITY ANTIGENS IB12‐07: Telomeres and incidence of leukemia recurrence and survival after hematopoietic stem cell transplantation (M Eapen): Study deferred pending receipt of grant funding.
101

Not for publication or presentation Attachment 11
2013 AMERICAN SOCIETY OF HEMATOLOGY (ASH) MEETINGS ABSTRACT HLA‐mismatch is Associated with Worse Outcomes after Unrelated Donor Reduced Intensity Conditioning Hematopoietic Cell Transplantation: A CIBMTR Analysis John Koreth, Kwang Woo Ahn, Joseph Pidala, James Gajewski, Hailin Wang, Marcelo Fernandez‐Vina, Stephen Spellman, Stephanie Lee In myeloablative unrelated donor allogeneic hematopoietic cell transplantation (HCT) a 1‐locus HLA‐mismatch (‐A, ‐B, ‐C, ‐DRB1) is associated with lower survival compared to fully matched pairs. However data in reduced‐intensity and non‐myeloablative conditioning (together called RIC) HCT are limited. We analyzed adult AML/ALL/CML/MDS recipients of first 8/8 HLA‐matched or 1‐locus mismatched unrelated donor (MUD, MMUD) RIC HCT performed in the period 1999‐2011 and registered in the CIBMTR. HLA‐A, ‐B, ‐C and ‐DRB1 loci were typed in all pairs at high resolution; ‐DQB1 and ‐DPB1 loci could not be evaluated in all pairs. Transplants involving ex‐vivo T‐cell depletion, CD34+ selection, or post‐transplant cyclophosphamide were excluded. Overall survival (OS) was the primary outcome. Secondary outcomes included non‐relapse mortality (NRM), relapse, disease‐free survival (DFS) and acute and chronic GVHD. Individual locus mismatch was also assessed. Apart from HLA matching, variables related to patient (age, race, sex, KPS, diagnosis, disease‐risk), donor (age, parity), both (sex match/ABO match/CMV match) treatment (conditioning intensity, TBI use, in‐vivo T‐cell depletion (ATG), graft source (PB, BM) and GVHD prophylaxis (CyA‐, Tac‐based)) were considered. 2588 RIC HCT (8/8 MUD: 2025; 7/8 MMUD: 563) from 144 centers and 12 countries were analyzed. Median follow up in 8/8 MUD and 7/8 MMUD was 38 and 48 months respectively. Diagnoses were AML (65%), ALL (8%), CML (7%), MDS (20%). Conditioning intensity was RIC (79%), NMA (21%). 58% received in‐vivo T‐cell depletion. Graft source was PBSC (85%), BM (15%). GVHD prophylaxis was Tac‐based (70%), CyA‐based (27%). Mismatches involved HLA‐A (188), ‐B (81), ‐C (219), and ‐DRB1 (75); with ‐DPB1 and ‐DQB1 typing available in 1382 and 2502 cases respectively. Compared to 8/8 MUD, 7/8 MMUD recipients were more likely to be younger and ethnic minorities and to have older and parous donors. In univariate analyses DQB1‐ and ‐DPB1 mismatch was not associated with worse OS, DFS, or NRM and was not further evaluated. There was a trend toward more grade II‐IV acute GVHD in ‐DPB1 double (p=0.02) but not single mismatches. In multivariate models 7/8 MMUD RIC HCT had worse grade II‐IV and III‐IV acute GVHD, NRM, DFS and OS, but not relapse or chronic GVHD (Table). No significant interactions were identified between degree of HLA matching and other clinical variables. Adjusted 1‐ and 3‐year NRM for 8/8 MUD vs. 7/8 MMUD was 20.4% vs. 28.9% (p<0.0001) and 29.2% vs. 38.1% (p<0.0007) respectively. Adjusted 1‐ and 3‐year OS was 54.7% vs. 48.8% (p=0.01) and 37.4% vs. 30.9% (p=0.005) respectively (Figure). There was no difference between allele and antigen
102

Not for publication or presentation Attachment 11
mismatches. HLA‐A, ‐B, ‐C, and ‐DRB1 locus mismatches were each associated with 1 or more impaired outcomes (acute GVHD, NRM, DFS, and/or OS). Compared to 8/8 MUD, both 7/8 allele and antigen MMUD RIC HCT have greater treatment toxicity and worse survival, of a magnitude similar to that seen in myeloablative transplantation. An isolated mismatch at HLA‐A, ‐B, ‐C, or ‐DRB1 was associated with 1 or more adverse outcomes. In unrelated donor RIC HCT, matching for all alleles of HLA‐A, ‐B, ‐C and ‐DRB1 loci results in superior outcomes.
7/8 vs. 8/8 HLA HR (95% CI) p‐value
Acute GVHD II‐IV 1.29 (1.09‐1.53) 0.003
Acute GVHD III‐IV 1.69 (1.00‐3.36) 0.05
Chronic GVHD 1.11 (0.96‐1.28) 0.15
Relapse 1.01 (0.87‐1.17) 0.92
NRM 1.52 (1.29‐1.79) <0.0001
DFS 1.20 (1.07‐1.34) 0.0015
OS 1.25 (1.11‐1.40) 0.0001
103

Not for publication or presentation Attachment 12
2014 TANDEM MEETINGS ABSTRACT
HLA‐Mismatch Is Associated With Worse Outcomes after Myeloablative Conditioning and Unrelated Donor Hematopoietic Cell Transplantation: A CIBMTR Analysis
Joseph Pidala MD, MS; Stephanie J. Lee, MD, MPH; Stephen Spellman, MBS; Hai‐Lin Wang, MPH; Kwang Woo Ahn, PhD; Mahmoud Aljurf, MD, MPH; Medhat Askar, MD, MPH; Jason Dehn, MPH; Marcelo Fernandez Viña, PhD; Alois Gratwohl, MD; Vikas Gupta, MD; Rabi Hanna, MD; Carolyn K. Hurley, PhD; Yoshihiro Inamoto, MD; Adetola A. Kassim, MD, MS; Taiga Nishihori, MD; Machteld Oudshoorn, PhD; Effie W. Petersdorf, MD; Vinod Prasad, MD Wael Saber, MD, MS; Kirk R. Schultz, MD; Jan Storek, MD, PhD; William A. Wood, MD, MPH; Ann E. Woofrey, MD; Claudio Anasetti, MD Background: Previous studies have demonstrated the adverse impact of HLA mismatch on the outcome of myeloablative conditioning and unrelated donor allogeneic hematopoietic cell transplantation (HCT). These have had limited power in certain sub‐groups, and do not reflect changes in HCT utilization and technology. Methods: Included were adult and pediatric patients who had undergone first myeloablative unrelated bone marrow or peripheral blood HCT for AML, ALL, CML, or MDS between 1999 and 2011. Patient and donor had high resolution typing for HLA‐A, B, C, DRB1, DQB1, and DPB1. Study outcomes included overall survival (OS), disease‐free survival (DFS), treatment‐related mortality (TRM), malignancy relapse, acute graft vs. host disease (GVHD), and chronic GVHD. The primary analysis tested the impact of mismatch at HLA‐A, B, C and DRB1. Secondary analyses examined HLA locus‐specific effects, allele vs. antigen mismatch, and the impact of DPB1 and DQB1 mismatch. Additional patient, disease, and HCT variables were considered in multivariate analyses. A p value < 0.01 was considered significant. Results: Of the study population (n=8,003), cases were 8/8 (n=5,449), 7/8 (n=2,071), or 6/8 (n=483) matched. Median follow up for surviving patients was 49 (3‐151) months. The study population was 88% Caucasian, 67% KPS 90‐100, 77% acute leukemia and only 14% CML, 56% peripheral blood, and 43% non‐TBI myeloablative conditioning. Of the total, 20% were from 1999‐2002, 32% 2003‐2006, and 49% from 2007‐2011. In the primary analysis, HLA mismatch (6‐7/8) conferred significantly increased risk for grade II‐IV and III‐IV acute GVHD, chronic GVHD, and TRM, and worsened DFS and OS compared to HLA matched cases (8/8). Malignancy relapse was not affected by HLA mismatch at A, B, C, or DRB1. The 6/8 cases had significantly worse TRM than 7/8 cases. The adverse impact of HLA mismatch on OS was greatest among those with early or intermediate stage disease. Single mismatch at HLA‐A, B, and C increased the risk for acute GVHD, TRM, and worsened OS. While single antigen mismatch at HLA‐B increased risk for grade II‐IV acute GVHD over single allele mismatch at –B, no other differences were detected between allele or antigen mismatch. Among 8/8 matched cases, DPB1 mismatch was associated with increased grade II‐IV and III‐IV acute GVHD and decreased relapse, and DQB1 mismatch was associated with increased grade II‐IV acute GVHD; these effects were not observed among 7/8 cases. DPB1 and DQB1 mismatch among 7/8 or 8/8 cases had no effect on OS or DFS. Conclusion: Despite improvements in survival after unrelated donor HCT over time, donor‐recipient HLA disparity remains a major source of GVHD and mortality.
104
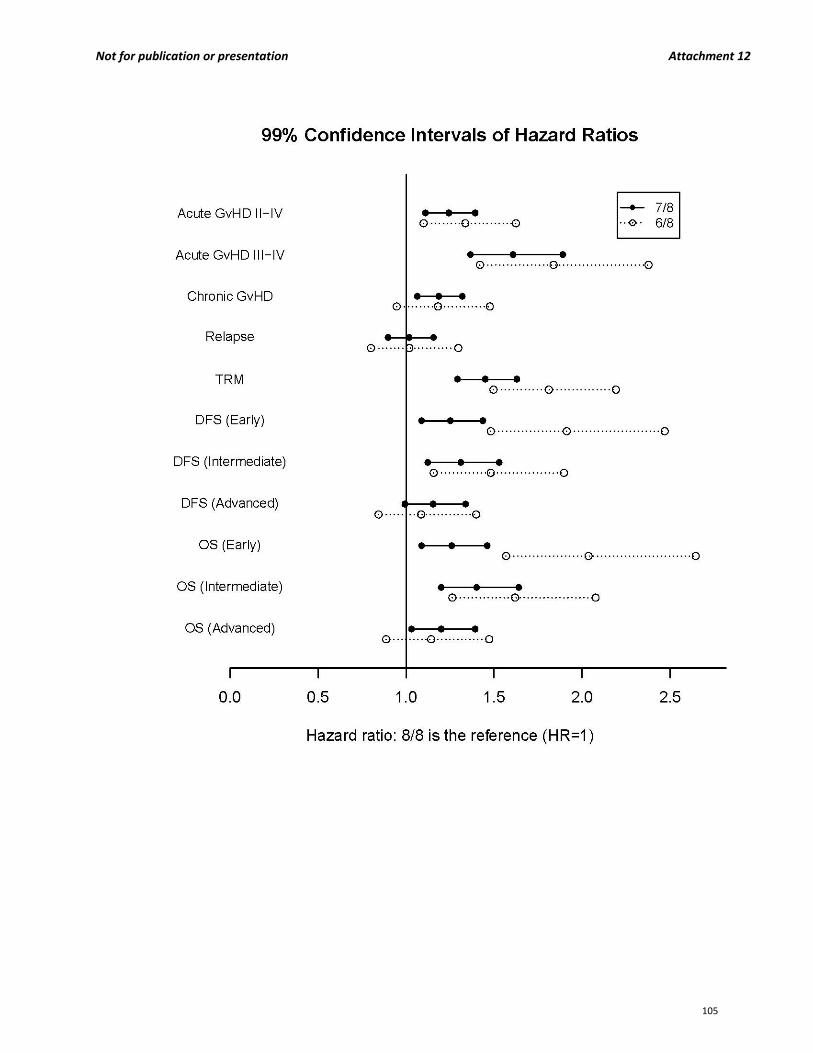
Not for publication or presentation Attachment 12
105

Not for publication or presentation Attachment 13
2013 AMERICAN SOCIETY OF HEMATOLOGY (ASH) MEETINGS ABSTRACT A Novel CD16xCD33 Bispecific Killer Cell Engager (BiKE) Mediates a Double Hit For Natural Killer (NK) Cells To Target CD33+ Myelodysplastic Syndrome (MDS) Cells and Myeloid Derived Suppressor Cells (MDSCs) At All Disease Stages Michelle K. Gleason, PhD1*, Julie A. Ross, PhD1, Troy C. Lund, MD/PhD2, Michael R. Verneris, MD2, Andres Wiernik, MD3, Erica D. Warlick, MD3, Stephen Spellman, MBS4*, Michael D. Haagenson, MS4*, Alexander J. Lenvik3*, Mark R. Litzow, MD5, Daniel J. Weisdorf, MD6, Daniel A. Vallera, PhD7* and Jeffrey S. Miller, MD3
1Department of Pediatrics, University of Minnesota, Minneapolis, MN; 2Pediatric Blood and Marrow Transplantation, University of Minnesota, Minneapolis, MN; 3Hematology, Oncology and Transplantation, University of Minnesota, Minneapolis, MN; 4CIBMTR, National Marrow Donor Program, Minneapolis, MN; 5Division of Hematology, Mayo Clinic, Rochester, MN; 6Center for International Blood & Marrow Transplantation Research, University of Minnesota Medical Center, Fairview, Minneapolis, MN; 7Therapeutic Radiology‐Radiation Oncology, University of Minnesota, Minneapolis, MN MDS is a clonal heterogeneous stem cell disorder identified by pancytopenia that frequently progresses to acute myeloid leukemia (AML). The only curative treatment is hematopoietic cell transplantation (HCT), but many patients are ineligible due to advanced age and comorbidities. New therapeutic strategies are urgently needed to reduce disease burden and improve overall survival. Studies of NK cell function from MDS patients have shown diminished natural cytotoxicity against K562 targets. These NK cell defects have been ascribed to abnormalities in expression and function of the NK cell activating receptors NKG2D, NKp30, NKp46 and DNAM‐1.
However, the properties of the potent activating receptor CD16 (FcRIII) and its potential for mediating targeted immunotherapy remain unexplored in MDS. Frozen pre‐transplant samples from 67 MDS patients (age 19‐74 years, Median=47) receiving unrelated HCT were obtained from the research sample repository of the National Marrow Donor Program and were compared to normal volunteers. NK cell degranulation, cytotoxicity and cytokine production were evaluated using published methods. We focused on CD16‐induced NK cell function using a bispecific killer cell engager generated to target CD16 along with the myeloid differentiation antigen CD33 (CD16xCD33 BiKE). CD16 expression on total CD56+ MDS‐NK cells was significantly lower compared to normal donors (MDS vs. normal: 63 ± 3% (n=67) vs. 89 ± 2% (n=20); p < 0.0001). However, reverse‐antibody dependent cell‐mediated cytotoxicity (R‐ADCC) assays revealed no significant differences in CD107a (46 ± 5%
(n=16) vs. 46 ± 3% (n=12)), IFN‐ (6 ± 1% vs. 10 ± 2%) or TNF‐ (9 ± 2% vs. 6% ± 1%) production when resting MDS‐NK cells were triggered with an agonistic CD16 mAb, indicating MDS‐NK cell function triggered through CD16 is intact. To evaluate the therapeutic potential of targeting CD16 in MDS patients, resting
MDS‐mononuclear cells were coated with 10g/mL of the CD16xCD33 BiKE and co‐cultured for 4 hours with the CD33+ target cell line HL‐60. MDS‐NK cell CD107a (CD16xCD33 BiKE vs. no reagent: 42 ± 2% (n=62) vs. 22 ±
1% (n=20); p < 0.0001), IFN‐ (15 ± 1% vs. 3 ± 1%; p < 0.0001) and TNF‐ (13 ± 1% vs. 3 ± 1%; p < 0.0001) production was significantly increased compared to the no reagent and scFv CD16 controls. Moreover, in the absence of HL‐60 targets, MDS‐NK cells treated with the CD16xCD33 BiKE targeted endogenous CD33+ targets,
significantly enhancing degranulation (37 ± 2% vs. 17 ± 1%; p < 0.0001), IFN‐ (4 ± 1% vs. 2% ± 1%; p < 0.01) and TNF‐ (5 ± 1% vs. 2 ± 1%; p < 0.01) production. Recent data have shown an increase in the frequency of MDSCs, phenotypically defined as CD33+/CD11b+/CD14‐/HLA‐DRlo/‐, during oncogenesis and in the presence of inflammatory cytokines. Indeed, in our MDS patient cohort, the frequency of MDSCs was significantly higher compared to normal donors (63 ± 3% (n=64) vs. 6 ± 2% (n=18), respectively; p < 0.0001) (figure). Furthermore, CD16xCD33 BiKE‐treated resting NK cells from normal donors co‐cultured with cytokine‐induced MDSCs generated from normal PBMCs in a 51Cr‐release cytotoxicity assay successfully targeted and lysed MDSCs
106
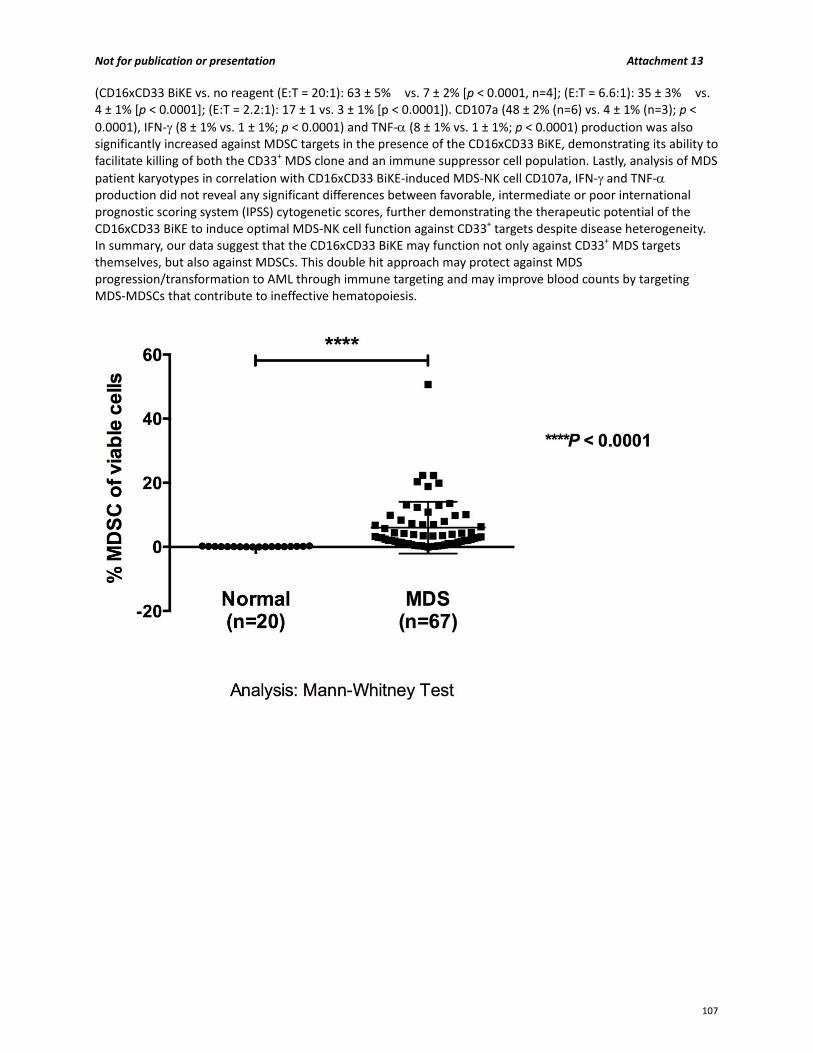
Not for publication or presentation Attachment 13
(CD16xCD33 BiKE vs. no reagent (E:T = 20:1): 63 ± 5% vs. 7 ± 2% [p < 0.0001, n=4]; (E:T = 6.6:1): 35 ± 3% vs. 4 ± 1% [p < 0.0001]; (E:T = 2.2:1): 17 ± 1 vs. 3 ± 1% [p < 0.0001]). CD107a (48 ± 2% (n=6) vs. 4 ± 1% (n=3); p <
0.0001), IFN‐ (8 ± 1% vs. 1 ± 1%; p < 0.0001) and TNF‐ (8 ± 1% vs. 1 ± 1%; p < 0.0001) production was also significantly increased against MDSC targets in the presence of the CD16xCD33 BiKE, demonstrating its ability to facilitate killing of both the CD33+ MDS clone and an immune suppressor cell population. Lastly, analysis of MDS
patient karyotypes in correlation with CD16xCD33 BiKE‐induced MDS‐NK cell CD107a, IFN‐ and TNF‐ production did not reveal any significant differences between favorable, intermediate or poor international prognostic scoring system (IPSS) cytogenetic scores, further demonstrating the therapeutic potential of the CD16xCD33 BiKE to induce optimal MDS‐NK cell function against CD33+ targets despite disease heterogeneity. In summary, our data suggest that the CD16xCD33 BiKE may function not only against CD33+ MDS targets themselves, but also against MDSCs. This double hit approach may protect against MDS progression/transformation to AML through immune targeting and may improve blood counts by targeting MDS‐MDSCs that contribute to ineffective hematopoiesis.
107
Not for publication or presentation Attachment 14
2013 AMERICAN SOCIETY OF HEMATOLOGY (ASH) MEETINGS ABSTRACT
Influence of Killer Immunoglobulin‐like Receptor (KIR) and HLA Genotypes on Outcomes after
Reduced‐Intensity Conditioning Allogeneic Hematopoietic Stem Cell Transplantation for Patients with
AML and MDS: A Report from the CIBMTR Immunobiology Working Committee
Ronald M. Sobecks, MD1, Meighan M. Gallagher, BA2*, Medhat Askar, MD, PhD1*, Michael D. Haagenson, MS3*, Tao Wang, PhD4*, Stephen Spellman, MBS3*, Stephanie J. Lee, MD, MPH5, Marcelo A. Fernandez Viña, PhD, D(ABHI)6*, Carlheinz R. Muller, MD, PhD7*, Michael R. Verneris, MD8, Ann E. Woolfrey, MD9, Peter J. Shaw, MD10, Daniel J. Weisdorf, MD11, Sarah Cooley, MD12, Jeffrey S. Miller, MD12 and Katharine C. Hsu, MD, PhD13*
1Cleveland Clinic Foundation, Cleveland, OH; 2Memorial Sloan Kettering Cancer Center, New York, NY; 3Center for International Blood & Marrow Transplant Research, National Marrow Donor Program, Minneapolis, MN; 4Division of Biostatistics, Medical College of Wisconisn, Milwaukee, WI; 5Clinical Research Division, Fred Hutchinson Cancer Research Center, Seattle, WA;6Stanford Hospital & Clinics, Stanford, CA; 7Zentrales Knochenmarkspender‐Register Deutschland, Ulm, Germany; 8Blood and Marrow Transplant Program, University of Minnesota, Minneapolis, MN; 9Pediatric Hematologic Cell Transplant, Fred Hutchinson Cancer Research Center, Seattle, WA; 10The Children's Hospital at Westmead, Westmead, Australia; 11Center for International Blood & Marrow Transplant Research, University of Minnesota Medical Center, Fairview, Minneapolis, MN; 12University of Minnesota Medical Center, Fairview, Minneapolis, MN; 13Memorial Sloan Kettering Cancer Center, New York, NY
Disease relapse is a significant cause of treatment failure after allogeneic hematopoietic stem cell
transplantation (HCT). In the setting of reduced‐intensity conditioning (RIC), a graft‐versus‐leukemia
(GVL) effect is critical for successful outcomes in patients with advanced myeloid malignancies. A GVL
effect has been attributed in part to donor‐derived alloreactive natural killer (NK) cells, which are
regulated by interaction of KIRs with their HLA‐class I ligands. Several models of NK reactivity (missing
KIR ligand, centromeric haplotype‐B content, non‐tolerized KIR2DS1) have been associated with
improved outcomes following HLA‐matched, HLA‐mismatched, related, and unrelated donor HCT,
particularly for AML patients given myeloablative conditioning. The effect of KIR‐HLA combinations on
outcomes after RIC HCT, however, is not known. We retrospectively analyzed donor‐recipient KIR/HLA
genotypes from 929 URD HCTs facilitated by the National Marrow Donor Program for patients with AML
(n=624) or MDS (n=305) treated with RIC between 1990 and 2007. 664 donor‐recipient pairs were 10/10
HLA‐matched and 265 were 9/10 HLA‐matched. 332 (37%) patients received ATG and 73 (8%) received
alemtuzumab. P‐values less than 0.01 were considered significant. We hypothesized that donor‐
recipient KIR‐HLA interactions may be associated with improved post‐transplant outcomes following RIC
HCT for AML and MDS. Patients lacking the HLA‐Bw4 ligand for donor inhibitory KIR3DL1 experienced
lower relapse following HCT at 1 year (27 vs 36%, p=0.002) and 5 years (31 vs 42%, p=0.003) compared
108

Not for publication or presentation Attachment 14
to patients with the Bw4 ligand (Figure). The lower risk for relapse was confirmed in multivariate
analysis (HR 0.71, p=0.005). However, there was no significant association of Bw4 ligand with disease‐
free survival (HR 0.84, p=0.05) and overall survival (HR=0.97, p=0.70). Risk for acute GVHD was higher
among patients lacking KIR ligands after adjusting for other clinical factors. In particular, patients lacking
HLA‐C2 for donor KIR2DL1 experienced higher grade 2‐4 (HR 1.3, p=0.005) and 3‐4 acute GVHD (HR 1.5,
p=0.002), and patients lacking multiple KIR ligands experienced higher grade 3‐4 acute GVHD (HR 1.5,
p=0.007). The analysis was then restricted to AML patients, the patient population with greatest
reported KIR‐HLA effects. Patients whose donors were KIR2DS1+ and HLA‐C2C2 (n=33) had higher
transplant‐related mortality (TRM) (HR, 2.4, p=0.002) compared to all other patients. There was no
significant effect of KIR2DS1 with HLA on relapse. In a multivariate analysis, lack of HLA‐C2 in AML
patients was associated with higher grade 2‐4 (HR 1.4, p=0.002) and 3‐4 acute GVHD (HR 1.5, p=0.01),
and risk for grade 3‐4 acute GVHD was higher in patients lacking multiple KIR ligands (HR 1.6, p=0.005).
There were no significant associations between donor homozygosity for the centromeric B‐haplotype
(cenBB) or overall B‐haplotype KIR content and RIC HCT outcomes.
Overall, these results suggest that in the RIC HCT setting, lack of Bw4 ligand for KIR3DL1 is associated
with a lower risk of relapse for AML/MDS. This observation corroborates previous findings in
myeloablative HCT transplants. Furthermore, tolerance of donor KIR2DS1 by HLA‐C2C2 was associated
with worse outcome, as manifested by higher TRM, in AML patients. In contrast, it appears that in RIC
HCT homozygosity for the centromeric B‐haplotype does not have a significant role in leukemia relapse.
The associations of KIR ligands with acute GVHD were not previously observed suggesting that NK cell
alloreactivity depends on multiple variables, including RIC. Further elucidation of the biology of NK cell
alloreactivity in the RIC setting may provide guidance for future approaches to help optimize conditions
for generating GVL reactions without GVHD and less TRM in this transplant population.
109
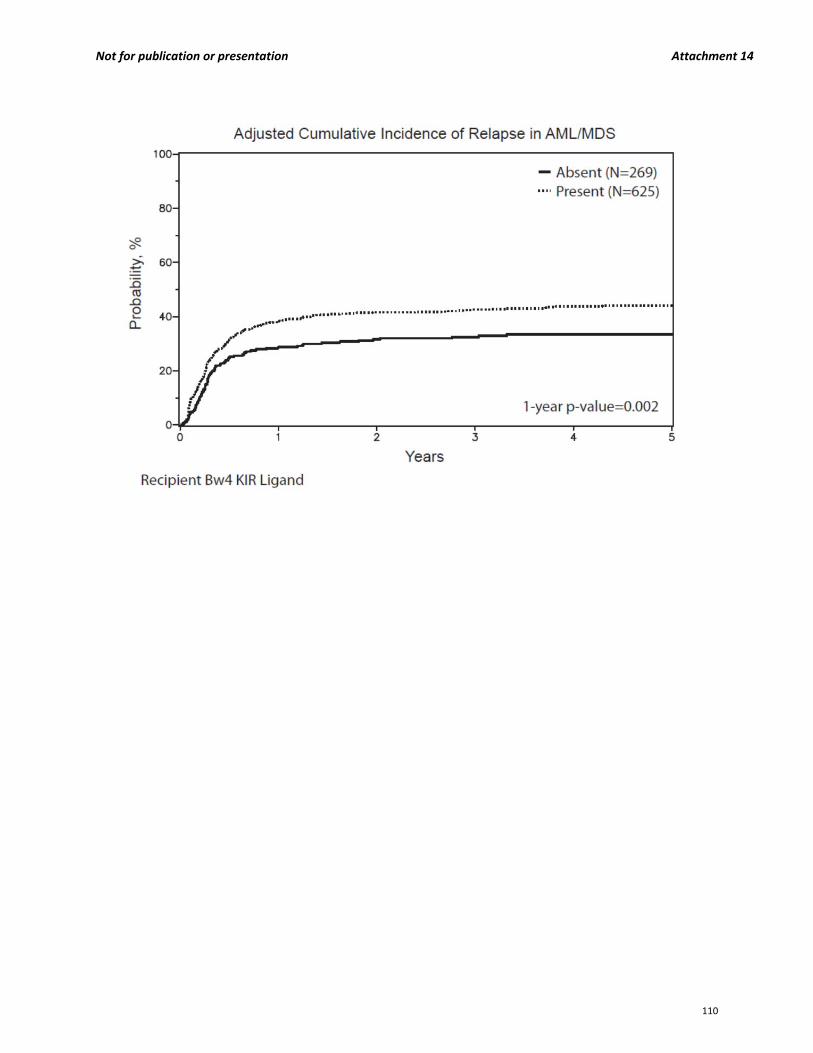
Not for publication or presentation Attachment 14
110
Not for publication or presentation Attachment 15
2014 TANDEM MEETINGS ABSTRACT Donor Telomere Length Predicts Recipient Survival After Allogeneic Hematopoietic Cell Transplantation In Patients With Bone Marrow Failure Syndromes Shahinaz M. Gadalla1, Tao Wang2, Michael Haagenson3, Stephen Spellman3, Stephanie Lee4, Jason Wong5, Kirsten M Williams6, Immaculata De Vivo5, Sharon A. Savage1 1Clinical Genetics Branch, Division of Cancer Epidemiology and Genetics, National Cancer Institute, Bethesda, MD, 2Center for International Blood and Marrow Transplant Research and Division of Biostatistics, Medical College of Wisconsin, Milwaukee, WI, 3Center for International Blood and Marrow Transplant Research, Minneapolis, MN, 4Center for International Blood and Marrow Transplant Research and Fred Hutchinson Cancer Research Institute, Seattle, WA, 5Harvard School of Public Health, Boston, MA, 6Division of Blood and Marrow Transplantation, Center for Cancer and Blood Disorders, Children’s National Medical Center, George Washington University Medical Center; Washington, DC Background: Telomeres are long nucleotide repeats and an associated protein complex at chromosome ends essential for chromosomal stability. They shorten with every cell division and thus are a marker of cellular replicative capacity. We hypothesized that telomere length may be a predictive marker for outcomes after hematopoietic cell transplantation (HCT). Method: We used quantitative PCR (qPCR) to measure pre‐transplant relative telomere length (RTL) in blood DNA of 342 young recipients (median age=14 yr; range=0.5–39), and their matched unrelated donors (median age=36 yr; range=19‐61). HCTs were performed for marrow failure syndromes between 1989 and 2007 and reported to the Center for International Blood and Marrow Transplant Research (CIBMTR), and the National Marrow Donor program (NMDP). The log‐rank test was used to compare survival across RTL categories. For multivariable models, we used Cox proportional hazard models and calculated hazard ratios (HR) and 95% confidence intervals (CI) comparing outcome across RTL categories. Results: Patients were followed for up to 20 years (median=6.3 years; range=0.5–20.7), with an overall survival (OS) probability at 3 years of 49% (44‐55). There were 243 (71%) with severe aplastic anemia, 87 (25%) with Fanconi anemia, and 12 (4%) with Diamond Blackfan anemia. Pre‐transplant RTL in the recipients was not associated with post‐transplant outcomes, including OS (3‐year survival probability=51% and 46%, in RTL ≥25% percentile and <25th percentile‐for age, respectively; p=0.76); acute (p=0.53 at 100 days) or chronic GVHD (p=0.99 at 1 year) and neutrophil engraftment (p=0.48). Pre‐transplant donor RTL was a significant predictor for OS after HCT, with longer donor telomere length associated with improved survival (3 year OS 59%, 49%, and 38%, in the longest, intermediate, and shortest tertiles, respectively; p=0.006). No association between donor RTL and either acute or chronic GVHD or engraftment was observed. Donor RTL was correlated with age (R2=0.12, p<0.0001), but after adjusting for donor age and factors known to influence patient survival after HCT (such as prior treatment and time between diagnosis and transplant), donor RTL remained a statistically significant predictor for recipient survival (HR=0.59, 95% CI=0.41‐0.86, p=0.006 for longest tertile; HR=0.92, p=0.61 for intermediate tertile, compared to the shortest tertile). There was no significant interaction between donor RTL and the patient’s underlying disease. Results were similar when the analysis was limited to
111
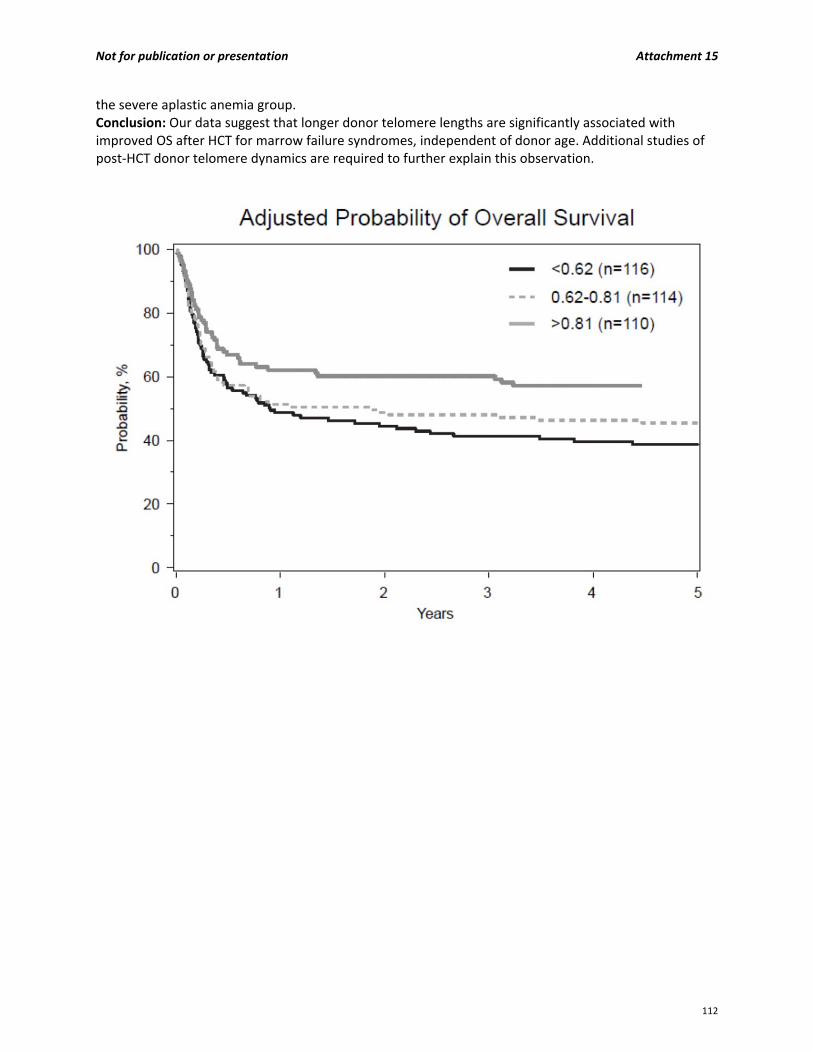
Not for publication or presentation Attachment 15
the severe aplastic anemia group. Conclusion: Our data suggest that longer donor telomere lengths are significantly associated with improved OS after HCT for marrow failure syndromes, independent of donor age. Additional studies of post‐HCT donor telomere dynamics are required to further explain this observation.
112

Not for publication or presentation Attachment 16
Study Proposal 1302‐01 Study Title: Discrepancy analysis of microsatellite loci as a proxy measure for ancestral differentiation between donors and recipients: correlation between high scores and poorer overall survival in high resolution matched unrelated donor transplantation. PI Information: John Harvey, BSc, MSc, DBMS, National Health Service Blood and Transplant, United Kingdom Colin Steward, MA, BM, BCh, PhD, FRCPCH, FRCP, Department of Pediatric Oncology/BMT, Bristol Royal Hospital for Sick Children, Bristol, United Kingdom Vanderson Rocha, MD, PhD, National Health Service Blood and Transplant, United Kingdom Specific Aims: The specific aims of this study are: 1. To calculate the Weighted Average Allelic Size Difference (WAASD) values for informative short
tandem repeats in a large cohort of HLA ‐ high resolution matched unrelated donors/recipient pairs. 2. To evaluate the WAASD scores generated in the North American genetic admixture populations and
compare to a relatively homogeneous European population (South West of England population). 3. From the WAASD numeric continuum, to see if there is an increasing trend of significance when
correlating post‐transplant outcome with WAASD score in the patient cohort tested. 4. To see if the higher scores in the WAASD continuum correlate with increased levels of non‐relapse
mortality.
Scientific Justification: The following text is from the first draft of a brief report we are currently preparing for publication. We also have preliminary results from a larger cohort of adult and pediatric patients which shows the same significant correlation between the calculated WAASD values (based upon donor recipients STR allele length differences) and transplant survival. We have previously reported on improved overall survival following the introduction of high resolution HLA typing in consecutive pediatric ALL patients undergoing matched unrelated stem cell transplantation at a single transplant centre1. We wish to report a novel measure of genetic disparity between donor and recipient that appears to impact transplant outcome within this patient cohort. Inter and intra population STR size differences have been used to calculate genetic distance in anthropology studies 2;3. Genetic distance has been shown to correlate with genetic differentiation and geographic distance between populations 3‐5. This genetic differentiation is reflected in differences in protein polymorphisms, which could potentially include those with effects on transplant outcome. Alcoceba, et.al. has reported a higher severity of acute GvHD and shorter 5‐year overall survival in patients displaying more than 10 (from 15) STR loci mismatches in a series HLA matched sibling transplants; Kim et.al. has reported STR disparities linked to increased non‐relapse mortality 6;7.
STR mutations have been studied and shown to be predominately single unit stepwise alteration in length due to strand‐slippage replication2;3;8 generating alleles of differing lengths. In a stepwise mutation model (SMM) the repeat number increases or decreases by one repeat at each mutation step. In an evolutionary mutation models for STR alleles, increasing size difference between alleles is seen to emerge from increasingly segregated phylogenic branches consistent with increasing numbers of single step mutations (figure 1).
113
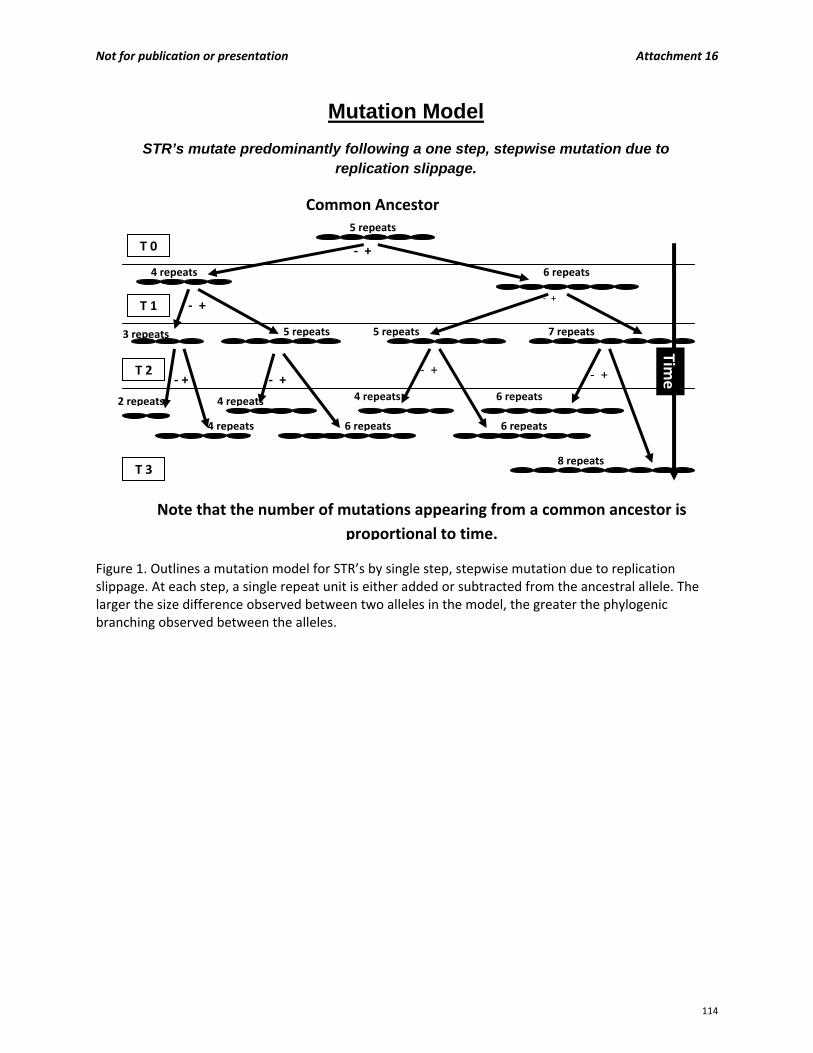
Not for publication or presentation Attachment 16
Figure 1. Outlines a mutation model for STR’s by single step, stepwise mutation due to replication slippage. At each step, a single repeat unit is either added or subtracted from the ancestral allele. The larger the size difference observed between two alleles in the model, the greater the phylogenic branching observed between the alleles.
T 0
T 1
T 2
T 3
‐ +
‐ +
‐ +
‐ +
‐ + ‐ + ‐ +
Common Ancestor
5 repeats
5 repeats5 repeats
4 repeats
4 repeats
4 repeats
4 repeats
6 repeats
6 repeats
6 repeats
6 repeats
7 repeats
8 repeats
2 repeats
Time
3 repeats
Mutation Model
STR’s mutate predominantly following a one step, stepwise mutation due to replication slippage.
Note that the number of mutations appearing from a common ancestor is
proportional to time.
114
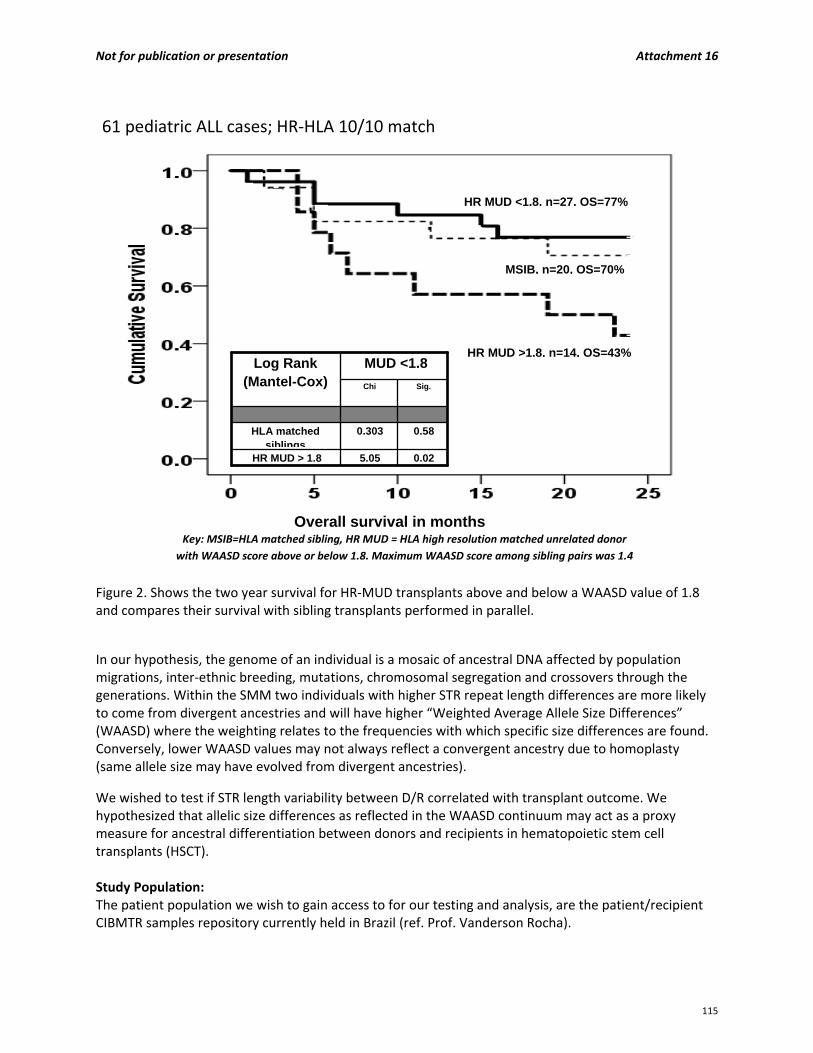
Not for publication or presentation Attachment 16
Figure 2. Shows the two year survival for HR‐MUD transplants above and below a WAASD value of 1.8 and compares their survival with sibling transplants performed in parallel.
In our hypothesis, the genome of an individual is a mosaic of ancestral DNA affected by population migrations, inter‐ethnic breeding, mutations, chromosomal segregation and crossovers through the generations. Within the SMM two individuals with higher STR repeat length differences are more likely to come from divergent ancestries and will have higher “Weighted Average Allele Size Differences” (WAASD) where the weighting relates to the frequencies with which specific size differences are found. Conversely, lower WAASD values may not always reflect a convergent ancestry due to homoplasty (same allele size may have evolved from divergent ancestries).
We wished to test if STR length variability between D/R correlated with transplant outcome. We hypothesized that allelic size differences as reflected in the WAASD continuum may act as a proxy measure for ancestral differentiation between donors and recipients in hematopoietic stem cell transplants (HSCT). Study Population: The patient population we wish to gain access to for our testing and analysis, are the patient/recipient CIBMTR samples repository currently held in Brazil (ref. Prof. Vanderson Rocha).
HR MUD <1.8, n=27, OS=77%
MSIB, n=20, OS=70%
HR MUD >1.8, n=14, OS=43%
0.025.05 HR MUD > 1.8
0.58 0.303 HLA matched siblings
Sig.Chi
MUD <1.8 Log Rank (Mantel-Cox)
Overall survival in months Key: MSIB=HLA matched sibling, HR MUD = HLA high resolution matched unrelated donor
with WAASD score above or below 1.8. Maximum WAASD score among sibling pairs was 1.4
61 pediatric ALL cases; HR‐HLA 10/10 match
115
Not for publication or presentation Attachment 16
Data was obtained from 61 consecutive HLA matched, ALL patients under the age of 18, who received a stem cell transplant at the Bristol Royal Hospital for Children between 2004 and 2010 and were analyzed for post transplant chimerism using STRs. This research was approved to meet NHS Blood and Transplant research group governance requirements. Data Requirements: The transplant outcome data relating to the patient/ donor DNA repository would be needed at the analysis phase of the study.
Sample Requirements: 1. The testing methodology is as described for the Promega PowerPlex 16® test system
(www.promega.com).
PCR amplification: The PCR programs used were as recommended by the PP16® manual (www.promega.com). PCR reactions using the PP16 kit were set up and carried out according to the instructions provided. PCR reactions were performed in a total volume of 25 �l containing 400 µM dNTPs, 2 mM MgCl2, 10 x PCR‐buffer II (Applied Biosystems (AB), Foster City, USA) 1 U AmpliTaq Gold® (AB) and 10 ng DNA template.
o Capillary electrophoresis: PCR amplicons generated from PP16 primers were analyzed on the ABI 3100xl genetic analyzer system in our studies. The instruments were initialized according to the manufacturer’s instructions, and the PCR products were loaded using standard injection parameters (5 kv, 15 sec). The time and voltage of injection was appropriately adjusted in the presence of low peak heights (< 500 relative fluorescence units [RFU]) or peak heights exceeding the limit of linear quantification (> 6‐7.000 RFU).
The allele size of the amplicons was determined using ABI genemapper software and tabulated for donor recipient comparisons and calculation of allele size differences. These results were then interpreted for WAASD calculations and analysed for correlation with transplant outcome data.
2. Experience: Dr. Colin Steward was a pioneer in early evaluation of chimerism for the post transplant monitoring of chimerism using STR microsatellites. Dr. John Harvey took developments from the research bench to develop an active routine service for the Bristol Royal Hospital for Children and the University Hospital Bristol adult and paediatric stem cell transplant programs.
Both Dr Harvey and Dr Steward participated in a collaborative study by leading laboratories from ten European countries supported by a grant from the European Commission, the EuroChimerism Concerted Action. The aim of this Concerted Action was the development of a standardized diagnostic methodology for the detection and monitoring of chimerism in patients undergoing allogeneic stem cell transplantation. They have several publications from their work in post transplant monitoring of chimerism and the analysis of STR’s.
Hancock JP, Goulden NJ, Oakhill A et al. Quantitative analysis of chimerism after allogeneic bone marrow transplantation using immunomagnetic selection and fluorescent microsatellite PCR. Leukemia. 2003; 17: 247‐251.
Watzinger F, Lion T, Steward C. The RSD code: proposal for a nomenclature of allelic configurations in STR‐PCR‐based chimerism testing after allogeneic stem cell transplantation. Leukemia. 2006; 20: 1448‐1452.
116
Not for publication or presentation Attachment 16
Lion T, Watzinger F, Preuner S et al. On behalf of the EuroChimerism Consortium (EU‐Project number: QLG1‐CT‐2002‐01485). The EuroChimerism concept for a standardized approach to chimerism analysis after allogeneic stem cell transplantation. Leukemia. 2012;26:1821‐1828.
van der Burg M, Kreyenberg H, Willasch A et al. On behalf of the EU‐supported EuroChimerism Consortium (project QLRT‐2001‐01485). Standardization of DNA isolation from low cell numbers for chimerism analysis by PCR of short tandem repeats. Leukemia. 25, 1467‐1470 (September 2011).
Study Design: STR profiling: We selected the PROMEGA PowerPlex®16 system which permits co‐amplification and three‐color detection of fifteen STR loci in a single PCR amplification, a system widely used in forensic science and post transplant monitoring for chimerism. The system contains fifteen STR loci, Penta E, D18S51, D21S11, TH01, D3S1358, FGA, TPOX, D8S1179, vWA, Penta D, CSF1PO, D16S539, D7S820, D13S317 D5S818 and the Amelogenin gene. Methodology was as described by the Eurochimera Consortium9. Calculation of WAASD scores for donor and recipient pairs: The donor and recipient STR alleles are identified and their base pair size tabulated. For each locus, alleles of identical length shared between donor and recipient are paired giving a size difference of zero. For other alleles the smallest sized allele of the donor is paired with the smallest allele for the recipient and the size difference is determined. This was similarly determined for the larger alleles. The STR repeat unit difference for each paired allele was calculated. Where the base pair difference was not an exact multiple of the repeat unit size, the value obtained was rounded down to the nearest whole number. When this was completed for all 30 allele pairs, the weighted average STR repeat unit size difference between donor and recipient was calculated. The number generated was the WAASD score for the transplant pair and correlates with the absolute number of single step, stepwise STR mutations observed to separate the D/R ancestries. Conditioning regime: The conditioning regime for this patient cohort has been previously reported 1. Data analysis: We have previously reported single and multivariate analysis on the co‐variates; disease status, patient/donor cytomegalovirus serology combinations, patient/donor age, patient/donor relationship and HLA match grade, stem cell source, days to engraftment, patient/donor sex combinations, graft versus host disease and changes to pre‐transplant conditioning protocol using logistic regression and the Cox proportional hazards models in this patient cohort of pediatric ALL transplants1. The only significant factors were disease status at time of transplant and HLA matching criteria were found to significantly influence two year OS in this patient cohort. As all transplants reported in this study were 10/10 high resolution HLA matches (HLA‐A, B, C, DRB1, DQB1), only disease status at the time of transplantation as a possible confounder for further analysis was considered. Stage one of the study is laboratory based. The STR profiles of the 740 donor and recipients in the DNA( require 50ng DNAper donor and recipient) repository currently held in Brazil would be analyzed and tabulated for analysis (I am informed that there may be a possible further 500 donor recipient pairs made available). The company Promega has intimated that they would be willing to supply reagents for the study. With access to all required equipment and reagents this could be completed in one month for 750 donor recipient pairs and two months if extended to 1250 transplant pairs. Stage two of the study is to calculate the weighted average allelic size difference of the donor recipient pairs. The differing profiles likely to emerge for the differing ethnic groups found in the North American population should be analyzed for . This could be completed in two to three months.
117

Not for publication or presentation Attachment 16
Stage three of the study would be to analyze the WAASD values for each transplant pair and see if the higher values correlate with increased mortality and other transplant outcomes that may be analyzed using a larger patient cohort. We have access to statisticians at the NHS blood and transplant organ donor registry in the UK however I assume the analysis will be performed by the statisticians working with the CIBMTR.
118
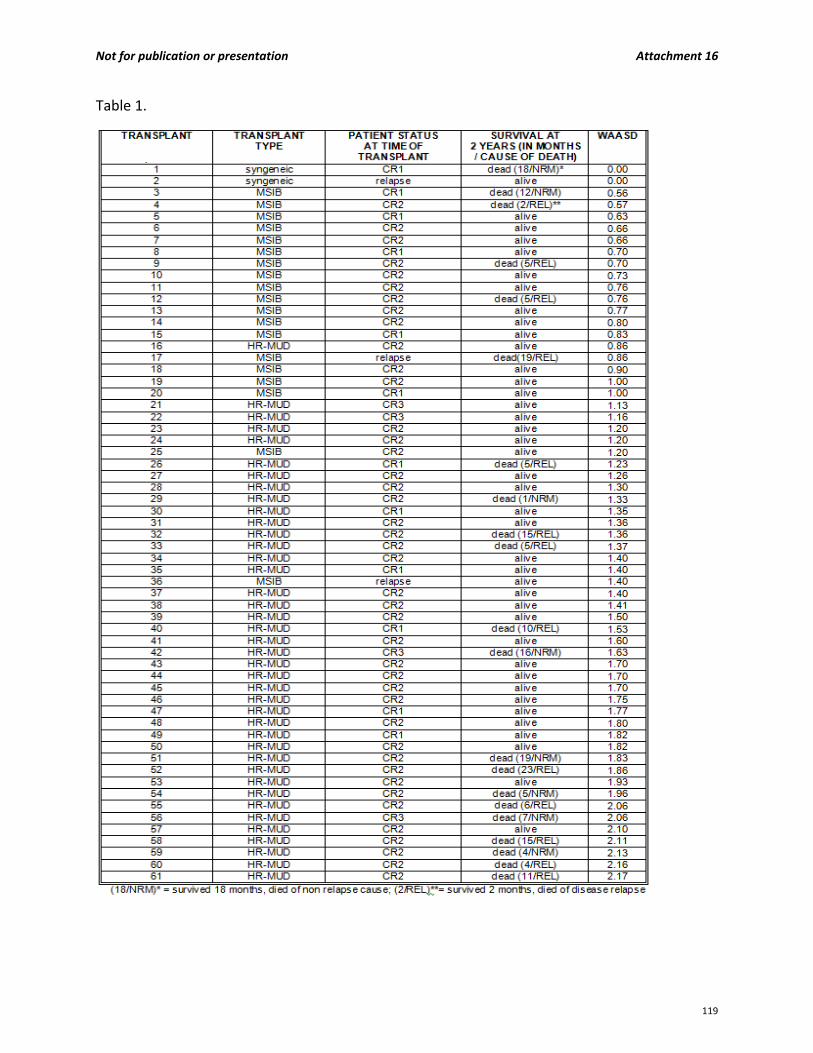
Not for publication or presentation Attachment 16
Table 1.
119

Not for publication or presentation Attachment 16
Results and Discussion: STR allelic length differences have been shown to correlate with genetic distance in ancestral populations including European admixtures10. Agrawal and Khan have shown that five selected forensic STR loci were sufficiently discriminating to differentiate 21 world populations and construct recent human phylogenic trees of their evolution based upon STR allelic length variability within and between populations11. In a study of genetic drift and the evolution of microsatellites, a series of paired randomly selected individuals (from within and between populations) was studied for STR absolute allele length differences at 145 loci12. They concluded that the values obtained were consistent with estimates of genetic distance between populations and the theory of African origin for modern humans. Between 2004 and 2010, consecutive stem cell transplants for 61 pediatric ALL patients consisting of 20 HLA matched sibling transplants (MSIB) and 41 high resolution HLA matched unrelated donor transplants (HR‐MUD) were analyzed. Donor and recipient STR profiles used in post transplant monitoring of chimerism were available. We calculated the average STR repeat unit size difference between the donor and recipient using 15 highly informative forensic STR’s (Promega, Powerplex 16TM). When the average allelic size differences for transplants in the study were listed the values formed a numeric continuum from zero to a highest observed value of 2.2 (Table 1). We have named this continuum the weighted average allelic size difference (WAASD). In our hypothesis, higher WAASD scores are indicative of increased ancestral differentiation between donor and recipient. There was an increasing trend of significance when correlating post‐transplant outcome with WAASD score reaching statistical significance at the WAASD value of 1.8 in this patient cohort; 2 year OS was 77% in MUD patients with a score of <1.8 (n=27) and 70% in matched siblings (n=20) compared to 43% in those with a score of >1.8 (n=14, p=0.02) (figure 2). (Further analysis of this data is ongoing and awaited from NHSBT organ donor transplant statistics department UK. i.e. competing risk analysis between relapse and NRM)
References: 1. Harvey J, Green A, Cornish J et al. Improved survival in matched unrelated donor transplant for
childhood ALL since the introduction of high‐resolution matching at HLA class I and II. Bone Marrow Transplant 2012;47:1294‐1300.
2. Slatkin M. A measure of population subdivision based on microsatellite allele frequencies. Genetics 1995;139:457‐462.
3. Liu H, Prugnolle F, Manica A, Balloux F. A geographically explicit genetic model of worldwide human‐settlement history. Am J Hum Genet 2006;79:230‐237.
4. Ramachandran S, Deshpande O, Roseman CC et al. Support from the relationship of genetic and geographic distance in human populations for a serial founder effect originating in Africa. Proc Natl Acad Sci U S A 2005;102:15942‐15947.
5. Rosenberg NA, Pritchard JK, Weber JL et al. Genetic Structure of Human Populations. Science 2002;298:2381‐2385.
6. Alcoceba M, Balanzategui A, Díez‐Campelo M et al. Clinical and Prognostic Value of Discrepancies in Microsatellite DNA Regions Between Recipient and Donor in Human Leukocyte Antigen‐Identical Allogeneic Transplantation Setting. Transplantation 2008;86:893‐900.
7. Kim DW, Jung WD, Kwack DH et al. Predicting outcomes of HLA‐identical allogeneic stem cell transplants from variable number of tandem repeat disparity between donors and recipients. Haematologica 2006;91:71‐77.
120

Not for publication or presentation Attachment 16
8. Schriver M, Jin L, Boerwinkle E et al. A novel Measure of Genetic Distance for Highly Polymorphic Tandem Repeat loci. Mol Biol Evol 1995;12:914‐920.
9. Lion T, Watzinger F, Preuner S et al. The EuroChimerism concept for a standardized approach to chimerism analysis after allogeneic stem cell transplantation. Leukemia 2012;26:1821‐1828.
10. Belle EMS, Landry PA, Barbujani G. Origins and evolution of Europeans genome: evidence from multiple microsatellite loci. Proc.of the Royal Society B, Biological Sciences 2006;B2006:1595‐1602.
11. Agrawal S, Khan F. Reconstructing recent human phylogenies with forensic STR loci:a statistical approach. BMC Genetics 2005;6:1‐7.
12. Takezaki N, Nei M. Genomic drift and evolution of microsatellite DNAs in human populations. Mol Biol Evol 2009;26:1835‐1840.
121
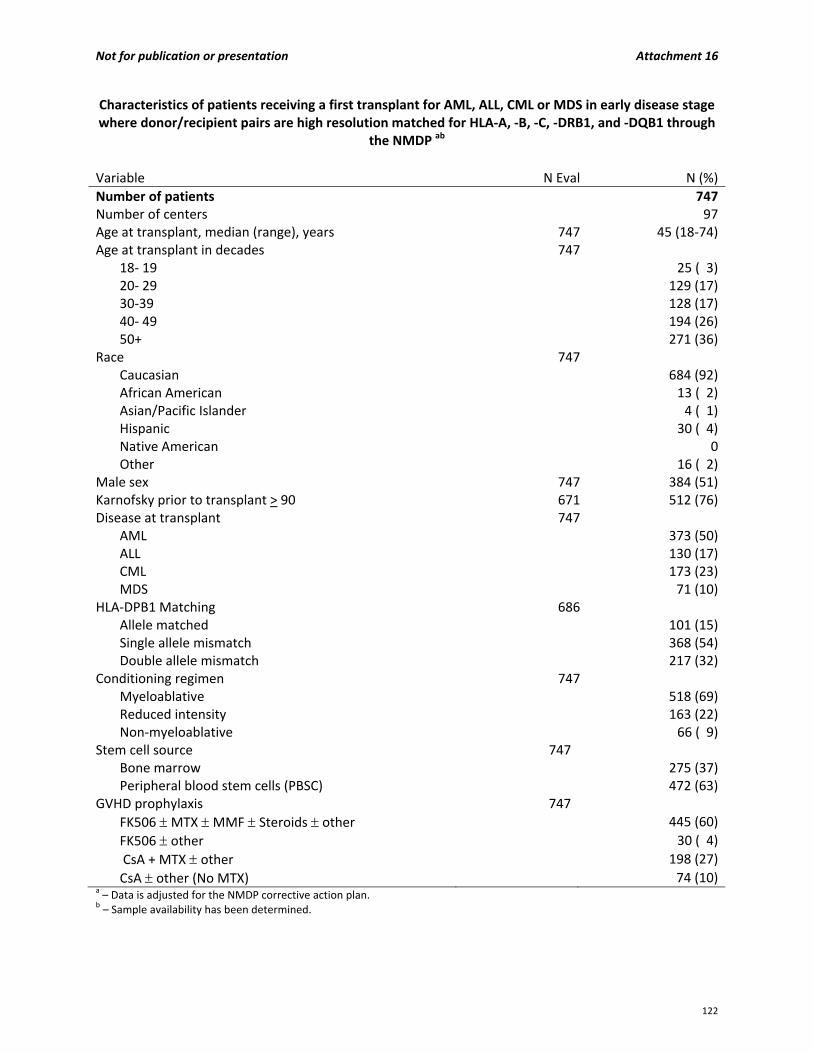
Not for publication or presentation Attachment 16
Characteristics of patients receiving a first transplant for AML, ALL, CML or MDS in early disease stage where donor/recipient pairs are high resolution matched for HLA‐A, ‐B, ‐C, ‐DRB1, and ‐DQB1 through
the NMDP ab
Variable N Eval N (%)
Number of patients 747Number of centers 97Age at transplant, median (range), years 747 45 (18‐74)Age at transplant in decades 747
18‐ 19 25 ( 3)20‐ 29 129 (17)30‐39 128 (17)40‐ 49 194 (26)50+ 271 (36)
Race 747 Caucasian 684 (92)African American 13 ( 2)Asian/Pacific Islander 4 ( 1)Hispanic 30 ( 4)Native American 0Other 16 ( 2)
Male sex 747 384 (51)Karnofsky prior to transplant > 90 671 512 (76)Disease at transplant 747
AML 373 (50)ALL 130 (17)CML 173 (23)MDS 71 (10)
HLA‐DPB1 Matching 686 Allele matched 101 (15)Single allele mismatch 368 (54)Double allele mismatch 217 (32)
Conditioning regimen 747 Myeloablative 518 (69)Reduced intensity 163 (22)Non‐myeloablative 66 ( 9)
Stem cell source 747 Bone marrow 275 (37)Peripheral blood stem cells (PBSC) 472 (63)
GVHD prophylaxis 747
FK506 MTX MMF Steroids other 445 (60)
FK506 other 30 ( 4)
CsA + MTX other 198 (27)
CsA other (No MTX) 74 (10)a – Data is adjusted for the NMDP corrective action plan. b – Sample availability has been determined.
122
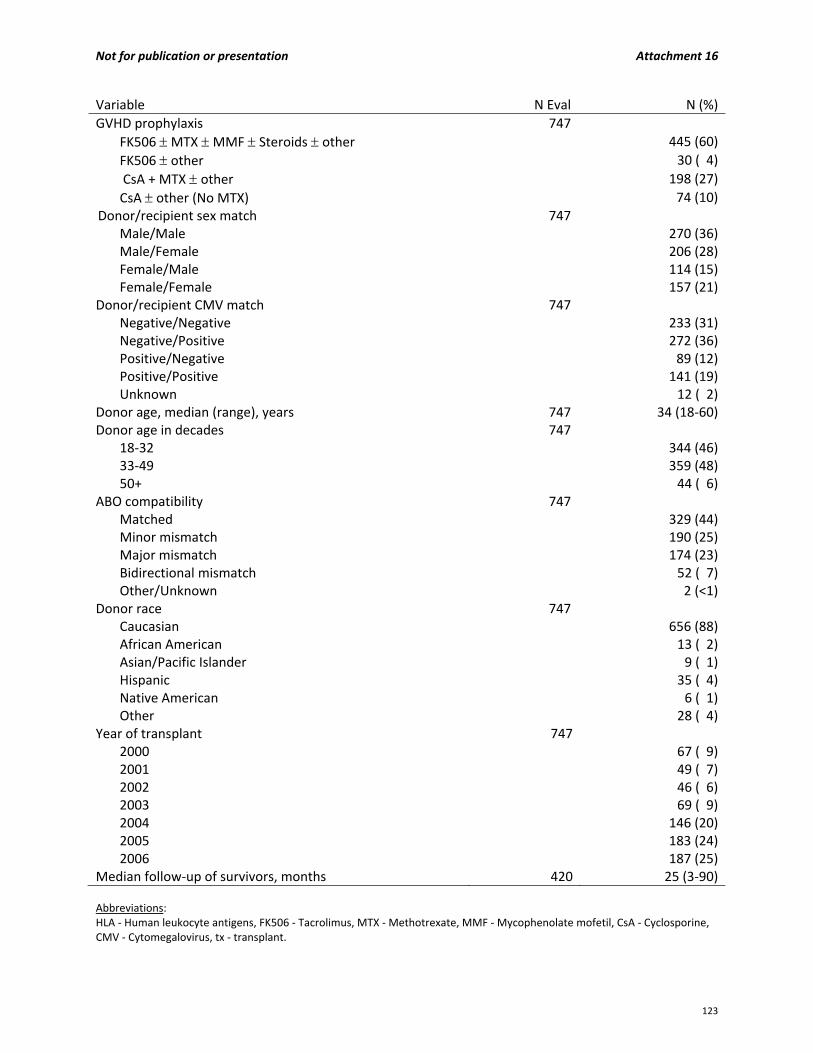
Not for publication or presentation Attachment 16
Variable N Eval N (%)
GVHD prophylaxis 747
FK506 MTX MMF Steroids other 445 (60)
FK506 other 30 ( 4)
CsA + MTX other 198 (27)
CsA other (No MTX) 74 (10)
Donor/recipient sex match 747 Male/Male 270 (36)Male/Female 206 (28)Female/Male 114 (15)Female/Female 157 (21)
Donor/recipient CMV match 747 Negative/Negative 233 (31)Negative/Positive 272 (36)Positive/Negative 89 (12)Positive/Positive 141 (19)Unknown 12 ( 2)
Donor age, median (range), years 747 34 (18‐60)Donor age in decades 747
18‐32 344 (46)33‐49 359 (48)50+ 44 ( 6)
ABO compatibility 747 Matched 329 (44)Minor mismatch 190 (25)Major mismatch 174 (23)Bidirectional mismatch 52 ( 7)Other/Unknown 2 (<1)
Donor race 747 Caucasian 656 (88)African American 13 ( 2)Asian/Pacific Islander 9 ( 1)Hispanic 35 ( 4)Native American 6 ( 1)Other 28 ( 4)
Year of transplant 747 2000 67 ( 9)2001 49 ( 7)2002 46 ( 6)2003 69 ( 9)2004 146 (20)2005 183 (24)2006 187 (25)
Median follow‐up of survivors, months 420 25 (3‐90) Abbreviations: HLA ‐ Human leukocyte antigens, FK506 ‐ Tacrolimus, MTX ‐ Methotrexate, MMF ‐ Mycophenolate mofetil, CsA ‐ Cyclosporine, CMV ‐ Cytomegalovirus, tx ‐ transplant.
123
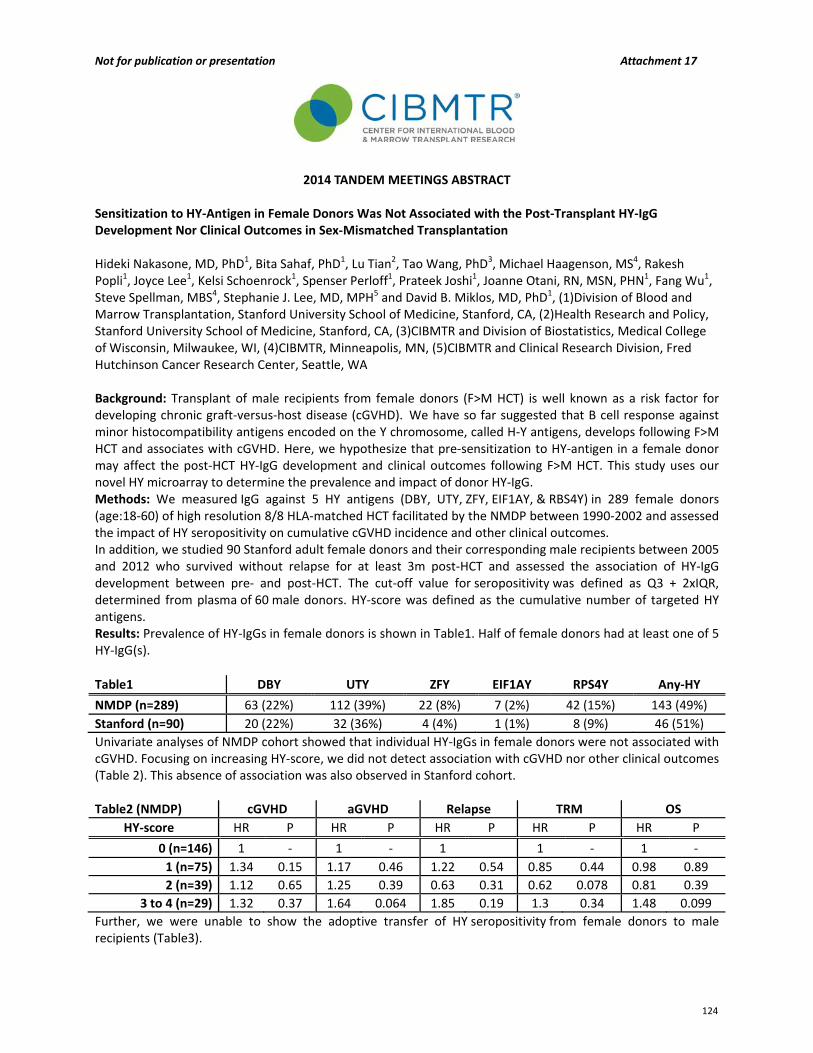
Not for publication or presentation Attachment 17
2014 TANDEM MEETINGS ABSTRACT Sensitization to HY‐Antigen in Female Donors Was Not Associated with the Post‐Transplant HY‐IgG Development Nor Clinical Outcomes in Sex‐Mismatched Transplantation Hideki Nakasone, MD, PhD1, Bita Sahaf, PhD1, Lu Tian2, Tao Wang, PhD3, Michael Haagenson, MS4, Rakesh Popli1, Joyce Lee1, Kelsi Schoenrock1, Spenser Perloff1, Prateek Joshi1, Joanne Otani, RN, MSN, PHN1, Fang Wu1, Steve Spellman, MBS4, Stephanie J. Lee, MD, MPH5 and David B. Miklos, MD, PhD1, (1)Division of Blood and Marrow Transplantation, Stanford University School of Medicine, Stanford, CA, (2)Health Research and Policy, Stanford University School of Medicine, Stanford, CA, (3)CIBMTR and Division of Biostatistics, Medical College of Wisconsin, Milwaukee, WI, (4)CIBMTR, Minneapolis, MN, (5)CIBMTR and Clinical Research Division, Fred Hutchinson Cancer Research Center, Seattle, WA Background: Transplant of male recipients from female donors (F>M HCT) is well known as a risk factor for developing chronic graft‐versus‐host disease (cGVHD). We have so far suggested that B cell response against minor histocompatibility antigens encoded on the Y chromosome, called H‐Y antigens, develops following F>M HCT and associates with cGVHD. Here, we hypothesize that pre‐sensitization to HY‐antigen in a female donor may affect the post‐HCT HY‐IgG development and clinical outcomes following F>M HCT. This study uses our novel HY microarray to determine the prevalence and impact of donor HY‐IgG. Methods: We measured IgG against 5 HY antigens (DBY, UTY, ZFY, EIF1AY, & RBS4Y) in 289 female donors (age:18‐60) of high resolution 8/8 HLA‐matched HCT facilitated by the NMDP between 1990‐2002 and assessed the impact of HY seropositivity on cumulative cGVHD incidence and other clinical outcomes. In addition, we studied 90 Stanford adult female donors and their corresponding male recipients between 2005 and 2012 who survived without relapse for at least 3m post‐HCT and assessed the association of HY‐IgG development between pre‐ and post‐HCT. The cut‐off value for seropositivity was defined as Q3 + 2xIQR, determined from plasma of 60 male donors. HY‐score was defined as the cumulative number of targeted HY antigens. Results: Prevalence of HY‐IgGs in female donors is shown in Table1. Half of female donors had at least one of 5 HY‐IgG(s).
Table1 DBY UTY ZFY EIF1AY RPS4Y Any‐HY
NMDP (n=289) 63 (22%) 112 (39%) 22 (8%) 7 (2%) 42 (15%) 143 (49%)
Stanford (n=90) 20 (22%) 32 (36%) 4 (4%) 1 (1%) 8 (9%) 46 (51%)
Univariate analyses of NMDP cohort showed that individual HY‐IgGs in female donors were not associated with cGVHD. Focusing on increasing HY‐score, we did not detect association with cGVHD nor other clinical outcomes (Table 2). This absence of association was also observed in Stanford cohort. Table2 (NMDP) cGVHD aGVHD Relapse TRM OS
HY‐score HR P HR P HR P HR P HR P
0 (n=146) 1 ‐ 1 ‐ 1 1 ‐ 1 ‐
1 (n=75) 1.34 0.15 1.17 0.46 1.22 0.54 0.85 0.44 0.98 0.89
2 (n=39) 1.12 0.65 1.25 0.39 0.63 0.31 0.62 0.078 0.81 0.39
3 to 4 (n=29) 1.32 0.37 1.64 0.064 1.85 0.19 1.3 0.34 1.48 0.099
Further, we were unable to show the adoptive transfer of HY seropositivity from female donors to male recipients (Table3).
124
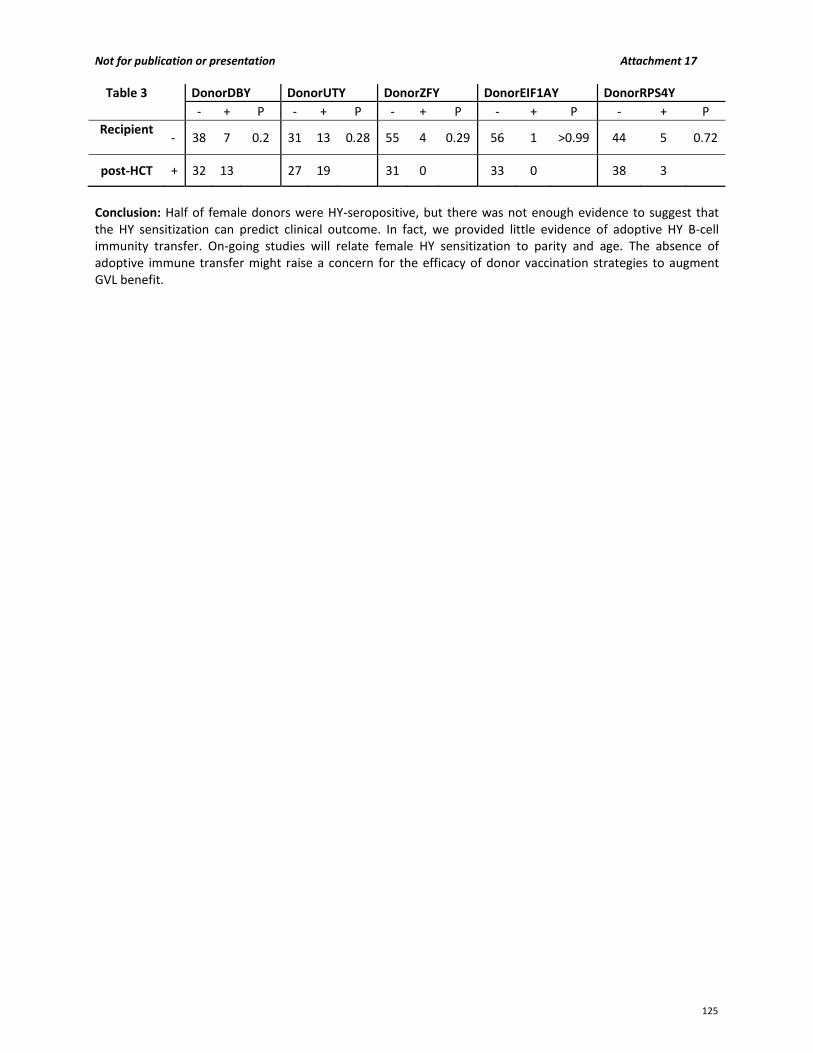
Not for publication or presentation Attachment 17
Table 3 DonorDBY DonorUTY DonorZFY DonorEIF1AY DonorRPS4Y
‐ + P ‐ + P ‐ + P ‐ + P ‐ + P
Recipient
‐ 38 7 0.2 31 13 0.28 55 4 0.29 56 1 >0.99 44 5 0.72
post‐HCT + 32 13 27 19 31 0 33 0 38 3
Conclusion: Half of female donors were HY‐seropositive, but there was not enough evidence to suggest that the HY sensitization can predict clinical outcome. In fact, we provided little evidence of adoptive HY B‐cell immunity transfer. On‐going studies will relate female HY sensitization to parity and age. The absence of adoptive immune transfer might raise a concern for the efficacy of donor vaccination strategies to augment GVL benefit.
125