Not All That Flattens is Celiac Disease: Mimics of Celiac Enteropathy in Contemporary Clinical...
2
R1 showed increased RAS activity compared to IEC18 cells which have no RAS activity. Infection with PY4-PUMA induced a marked inhibition of cell growth (40-50%), and induc- tion of apoptosis, in all cells exhibiting high levels of RAS activity whereas IEC18 were unaffected. The vector control SV40-PUMA had no effect. Selective and high expression of PUMA protein was detected in PY4-PUMA infected cells (Fig. 2). In xenograft models of PC in nude mice, PY4-PUMA injected i.p twice during a period of 3 weeks, inhibited by ~35% the growth of established tumors compared to the control virus. The histopathological analysis revealed prominent apoptotic features in the PY4-PUMA-treated tumors, and increased expression level of the PUMA protein. Conclusions: Selective overexpression of the pro-apoptotic PUMA gene inhibits the growth of RAS-transformed but not normal cells. This treatment modality may become a useful, effective and safe approach to selectively target RAS-mutated tumor cells. 144 Analysis of the Role of JNK and Therapeutic Effect of JNK Inhibition in Pancreatic Cancer Ryota Takahashi, Wachiko Nakata, Hiroto Kinoshita, Yoku Hayakawa, Hayato Nakagawa, Hideaki Ijichi, Yoshihiro Hirata, Shin Maeda, Kazuhiko Koike Introduction: c-Jun NH2-terminal kinase (JNK) is a member of mitogen-activated protein kinase (MAPK) family, and its signaling pathway is known to regulate a variety of cellular activities including apoptosis, survival, differentiation, and proliferation. Recently, it has been suggested that JNK pathway is involved in tumorigenesis in several cancers, but the role of JNK in developing pancreatic cancer is not fully elucidated. In this study, we examined the role of JNK in tumorigenesis and proliferation of pancreatic cancer. We also evaluated the effect of JNK inhibition on the growth of pancreatic cancer. Methods: The status of JNK pathway was examined by immunohistochemical staining of human pancreatic cancers and murine pancreatic cancers developed in the pancreas-specific Kras G12D and type II TGFβ receptor knockout mice (Kras G12D +Tgfbr2 KO mice). The activity of JNK in pancreatic cancer cell lines was determined by western blotting and kinase assay. The effect of JNK inhibition by JNK inhibitor (SP600125) or by siRNA on the growth of cancer cell lines was determined by Cell Counting Kit-8. The effect of JNK inhibitor was also evaluated In Vivo by IP injection of SP600125 to Kras G12D +Tgfbr2 KO mice. Results: In the immunohistochemical staining, JNK activation was observed in almost half of human pancreatic cancer specimens. Pancreatic tissue from Kras G12D +Tgfbr2 KO mice showed higher activation of JNK than pancreatic tissue from Kras G12D mice or WT mice. In Kras G12D +Tgfbr2 KO mice, JNK activity was increased in accordance with histological change. Growth inhibition was observed in pancreatic cancer cell lines treated with JNK inhibitor in a dose dependent manner. The growth was also inhibited by knockdown of JNK1. Treating Kras G12D +Tgfbr2 KO mice with JNK inhibitor for 4 weeks lead to less proliferation of cancer and mesenchymal tissues, and immunohistochemical staining showed reduced phospho-JNK, c-jun and cyclin D1 in the pancreatic cancer tissues compared to Kras G12D +Tgfbr2 KO mice treated with vehicle. Conclusion: These data indicate that JNK is involved in the tumorigenesis and proliferation of pancreatic cancer, and inhibiting JNK may be a potential therapy of pancreatic cancer. 145 Ngal in Pancreatic Juice Helps to Discriminate Chronic Pancreatitis and Pancreatic Cancer Patients From Healthy Controls Michael Baine, Nobuo Ochi, Michael B. Wallace, Timothy A. Woodward, Colleen S. Thomas, Sushovan Guha, Massimo Raimondo Background: The dismal 5-year survival rate for pancreatic cancer (PC) of 5% is related to its late diagnosis. To aid in improving ability to diagnose PC, surrogate biomarker testing that can differentiate PC from both healthy controls (HC) and those with chronic pancreatitis (CP) will be vital. Prospectively, we analyzed 3 potential biomarkers: NGAL, MIC-1, and CA19-9 in pancreatic juice (PJ) from PC, CP and HC patients. Materials & Methods: One hundred fifty-six patients diagnosed as HC, CP, or PC were recruited from Mayo Clinic. Of these, 6 and 45 pts were excluded due to screening failure and diagnoses not related to HC, CP & PC, respectively. Thus, the final group consisted of 105 pts: HC=23, CP=24 and PC=58. PJ was collected for biomarker analysis during endoscopy after IV secretin. Concentrations of MIC-1 and CA 19-9 were measured at University of Nebraska Medical Center (UNMC). NGAL was measured at both MD Anderson Cancer Center (MDACC) using commercially available assay (NGAL-MDACC) and UNMC utilizing a lab-developed assay (NGAL-UNMC). To assess the ability of each biomarker to discriminate among groups, ROC curves were constructed and AUCs were estimated along with 95% CIs. Statistical analyses were performed using SAS and S-Plus. Results: All markers showed significantly higher concentrations in CP when compared to HC (p<0.035). NGAL was most effective in discrim- inating between HC and CP, with estimated AUCs of 0.88 and 0.87 (for analysis at UNMC and MDACC, respectively). Between these groups, NGAL provided a sensitivity of 75-79% and a specificity of 74-78%. Comparing HC and PC samples, all markers were significantly higher in the disease group (p<0.036). As evidenced by AUC estimates, NGAL-MDACC (AUC 0.90), NGAL-UNMC (AUC 0.91), and MIC-1 (AUC 0.83) were best able to discriminate S-35 AGA Abstracts between HC and PC with sensitivities of 81%, 79% and 78% and specificities of 83%, 83% and 78%, respectively. By comparison, AUC estimates for CA19-9 was only 0.76. The only marker which showed a statistically significant difference between PC and CP was MIC-1 (p=0.043). However, the estimated AUC for MIC-1 was only 0.63, indicating that this marker is unlikely to be effective in discriminating between CP and PC. High correlation between UNMC and MDACC and NGAL assays was found. Conclusions: This study provides evidence of differences in PJ biomarker expression between HC, CP and PC. These results suggest that some of the differences may be strong enough to be effective diagnostically. Specifically, MIC-1 and NGAL were fairly effective in discriminating between HC and PC, while NGAL alone was fairly effective in discriminating between HC and CP. No markers helped discrimin- ating between CP and PC, though further study with an expanded sample set may allow significant differences to be observed. 146 Increased Incidence of Non-Hodgkin Lymphoma Subtypes in Patients With Celiac Disease Lori A. Leslie, Benjamin Lebwohl, Alfred I. Neugut, John Gregory Mears, Govind Bhagat, Peter H. Green PURPOSE: Prior studies have described an increased incidence of lymphoma in patients with celiac disease. However, few studies differentiated among the various types of lymphop- roliferative disorders (LPD). Additionally, identification of patients at high risk of developing LPD remains unclear. Our aims were to (1) determine the incidence of LPD subtypes in celiac disease patients compared to the general population and (2) describe the pattern of celiac disease presentation in those who develop concurrent LPD compared to those who do not. METHODS: We conducted a single-center retrospective cohort study of patients with biopsy-proven celiac disease seen at Columbia University Medical Center between 1981 and 2010 to identify patients with LPDs (defined as any non-Hodgkin lymphoma, Hodgkin lymphoma, or chronic lymphocytic leukemia). We calculated standardized incidence ratios (SIR) and correlating 95% confidence intervals (95%CI) using the Surveillance, Epidemiology, and End Result database to estimate the expected incidence of LPD subtypes. SIR was not calculated for a LPD subtype if the observed incidence was less than 2 or expected incidence was zero. RESULTS: Our cohort included 1,281 celiac patients with a total of 13,459 person- years of observation. We identified 35 case of LPD (SIR 5.7, 95%CI 3.9-7.7); 29 non- Hodgkin lymphomas (SIR 3.4, 95%CI 1.9-5.0), one Hodgkin lymphoma, and 5 chronic lymphocytic leukemias (SIR 4.1, 95%CI 1.2-8.3). Of the 29 non-Hodgkin lymphomas, there were 11 enteropathy-associated T-cell (expected rate of 0), 4 peripheral T-cell (SIR 18.0, 95%CI 4.6-39.9), and 14 B-cell lymphomas (SIR 3.0, 95%CI 1.6-4.7). Of the 14 B-cell non- Hodgkin lymphomas, there were 4 diffuse large B-cell (SIR 3.6, 95%CI 0.9-7.9), 3 mantle cell (SIR 32.3, 95%CI 6.0-79.1), 4 marginal zone (SIR 29.8, 95%CI 7.7-66.2), one follicular, one primary effusion, and one post-transplant LPD. The incidence of non-Hodgkin lymphoma in both genders was similar (SIR women 6.0, 95%CI 3.7-8.9; SIR men 5.3, 95%CI 2.9- 8.4). Twenty patients were diagnosed with celiac disease prior to LPD (mean 7.8±8.2 years), 5 concurrently, and 10 after LPD (mean 6.6±5.0 years). Patients who developed LPD were diagnosed with celiac disease at a later age (mean 55±16 versus 43±17 years old, p<0.0001) and were more likely to present with diarrhea (69% versus 40% p=0.0068) and/or abdominal pain (12% versus 3% p=0.041) than those who did not develop LPD. CONCLUSIONS: The incidence of LPD is increased in celiac disease compared to the general population; particularly enteropathy-associated T-cell lymphoma as well as peripheral T-cell, mantle cell, and marginal zone lymphomas. Patients diagnosed with celiac disease after age 50 who initially present with diarrhea and/or abdominal pain are at increased risk and may benefit from routine follow-up and surveillance. 147 Not All That Flattens is Celiac Disease: Mimics of Celiac Enteropathy in Contemporary Clinical Practice Kumar Pallav, Daniel A. Leffler, Sohaib Tariq, Jeffrey D. Goldsmith, Robert M. Najarian, Joshua Hansen, Melinda Dennis, Detlef Schuppan, Ciaran P. Kelly Background The diagnosis of celiac disease (CD) is based on histologic changes including villous blunting on duodenal biopsies and positive serum antibodies. However, while celiac disease is the most common cause of duodenal villous atrophy, there is a broad differential diagnosis for villous atrophy, especially in patients with negative celiac serologies. Our aim was to identify the spectrum of conditions causing non celiac enteropathy (NCE) and to assess methods of differentiating between CD and NCE in clinical practice. Methods Through record review we identified patients with duodenal villous atrophy due to causes other than CD. Inclusion criteria for NCE were villous atrophy and either negative CD HLA testing or the combination of negative CD serology and lack of histological improvement on a gluten free diet (GFD). Investigations that lead to a correct diagnosis of NCE were noted. Findings were also compared to our overall CD population. Results The underlying etiologies of the 30 NCE patients identified are listed in Table1. The male to female ratio was 1:2 and the median age at diagnosis was 55 years (range 20-76), compared to 42 (range 0-89) for CD (p=.01). All classic symptoms of CD occurred at a higher frequency in NCE patients (Table 2). 19 (86%) of the 22 NCE patients who underwent celiac genetic testing were HLA DQ2 & DQ8 negative. 4 (13%) NCE patients had a positive tissue transglutaminase antibody, (mean 37 U, nl < 20, range 20 to 67) as compared to 97% of CD patients (p=.0001). 21 (70%) of the NCE patients were initially diagnosed with CD, 8 of whom reported some symptom improvement on a gluten free diet, however none showed histological recovery. Anti enterocyte antibodies were positive in 1 of 7 patients tested. The frequencies of abnormal LFTs and inflammatory markers were similar in both groups. Conclusion Most patients (70%) with villous atrophy caused by NCE are initially misdiagnosed as having CD and NCE is easily further misdiagnosed as refractory celiac disease. In patients with villous blunting, a normal initial tTG (87%) should alert clinicians to possible NCE. The diagnosis can often be confirmed (86%) by negative HLA-DQ2/DQ8 genetic test. While CD often presents with extraintestinal manifestations, NCE symptoms are nearly always gastrointesti- nal. A subjective response to GFD is not an accurate indicator of CD vs NCE. Repeat biopsy and review of initial biopsies by a skilled GI pathologist may help when findings other than AGA Abstracts
-
Upload
kumar-pallav -
Category
Documents
-
view
212 -
download
0
Transcript of Not All That Flattens is Celiac Disease: Mimics of Celiac Enteropathy in Contemporary Clinical...

R1 showed increased RAS activity compared to IEC18 cells which have no RAS activity.Infection with PY4-PUMA induced a marked inhibition of cell growth (40-50%), and induc-tion of apoptosis, in all cells exhibiting high levels of RAS activity whereas IEC18 wereunaffected. The vector control SV40-PUMA had no effect. Selective and high expression ofPUMA protein was detected in PY4-PUMA infected cells (Fig. 2). In xenograft models ofPC in nude mice, PY4-PUMA injected i.p twice during a period of 3 weeks, inhibited by~35% the growth of established tumors compared to the control virus. The histopathologicalanalysis revealed prominent apoptotic features in the PY4-PUMA-treated tumors, andincreased expression level of the PUMA protein. Conclusions: Selective overexpression ofthe pro-apoptotic PUMA gene inhibits the growth of RAS-transformed but not normal cells.This treatment modality may become a useful, effective and safe approach to selectivelytarget RAS-mutated tumor cells.
144
Analysis of the Role of JNK and Therapeutic Effect of JNK Inhibition inPancreatic CancerRyota Takahashi, Wachiko Nakata, Hiroto Kinoshita, Yoku Hayakawa, Hayato Nakagawa,Hideaki Ijichi, Yoshihiro Hirata, Shin Maeda, Kazuhiko Koike
Introduction: c-Jun NH2-terminal kinase (JNK) is a member of mitogen-activated proteinkinase (MAPK) family, and its signaling pathway is known to regulate a variety of cellularactivities including apoptosis, survival, differentiation, and proliferation. Recently, it hasbeen suggested that JNK pathway is involved in tumorigenesis in several cancers, but therole of JNK in developing pancreatic cancer is not fully elucidated. In this study, we examinedthe role of JNK in tumorigenesis and proliferation of pancreatic cancer. We also evaluatedthe effect of JNK inhibition on the growth of pancreatic cancer. Methods: The status ofJNK pathway was examined by immunohistochemical staining of human pancreatic cancersand murine pancreatic cancers developed in the pancreas-specific KrasG12D and type II TGFβreceptor knockout mice (KrasG12D+Tgfbr2KO mice). The activity of JNK in pancreatic cancercell lines was determined by western blotting and kinase assay. The effect of JNK inhibitionby JNK inhibitor (SP600125) or by siRNA on the growth of cancer cell lines was determinedby Cell Counting Kit-8. The effect of JNK inhibitor was also evaluated In Vivo by IP injectionof SP600125 to KrasG12D+Tgfbr2KO mice. Results: In the immunohistochemical staining,JNK activation was observed in almost half of human pancreatic cancer specimens. Pancreatictissue from KrasG12D+Tgfbr2KO mice showed higher activation of JNK than pancreatic tissuefrom KrasG12D mice or WT mice. In KrasG12D+Tgfbr2KO mice, JNK activity was increasedin accordance with histological change. Growth inhibition was observed in pancreatic cancercell lines treated with JNK inhibitor in a dose dependent manner. The growth was alsoinhibited by knockdown of JNK1. Treating KrasG12D+Tgfbr2KO mice with JNK inhibitor for 4weeks lead to less proliferation of cancer andmesenchymal tissues, and immunohistochemicalstaining showed reduced phospho-JNK, c-jun and cyclin D1 in the pancreatic cancer tissuescompared to KrasG12D+Tgfbr2KO mice treated with vehicle. Conclusion: These data indicatethat JNK is involved in the tumorigenesis and proliferation of pancreatic cancer, and inhibitingJNK may be a potential therapy of pancreatic cancer.
145
Ngal in Pancreatic Juice Helps to Discriminate Chronic Pancreatitis andPancreatic Cancer Patients From Healthy ControlsMichael Baine, Nobuo Ochi, Michael B. Wallace, Timothy A. Woodward, Colleen S.Thomas, Sushovan Guha, Massimo Raimondo
Background: The dismal 5-year survival rate for pancreatic cancer (PC) of 5% is related toits late diagnosis. To aid in improving ability to diagnose PC, surrogate biomarker testingthat can differentiate PC from both healthy controls (HC) and those with chronic pancreatitis(CP) will be vital. Prospectively, we analyzed 3 potential biomarkers: NGAL, MIC-1, andCA19-9 in pancreatic juice (PJ) from PC, CP and HC patients. Materials & Methods: Onehundred fifty-six patients diagnosed as HC, CP, or PC were recruited from Mayo Clinic. Ofthese, 6 and 45 pts were excluded due to screening failure and diagnoses not related toHC, CP & PC, respectively. Thus, the final group consisted of 105 pts: HC=23, CP=24and PC=58. PJ was collected for biomarker analysis during endoscopy after IV secretin.Concentrations of MIC-1 and CA 19-9 were measured at University of Nebraska MedicalCenter (UNMC). NGAL was measured at both MD Anderson Cancer Center (MDACC) usingcommercially available assay (NGAL-MDACC) and UNMC utilizing a lab-developed assay(NGAL-UNMC). To assess the ability of each biomarker to discriminate among groups, ROCcurves were constructed and AUCs were estimated along with 95% CIs. Statistical analyseswere performed using SAS and S-Plus. Results: All markers showed significantly higherconcentrations in CP when compared to HC (p<0.035). NGAL was most effective in discrim-inating between HC and CP, with estimated AUCs of 0.88 and 0.87 (for analysis at UNMCand MDACC, respectively). Between these groups, NGAL provided a sensitivity of 75-79%and a specificity of 74-78%. Comparing HC and PC samples, all markers were significantlyhigher in the disease group (p<0.036). As evidenced by AUC estimates, NGAL-MDACC(AUC 0.90), NGAL-UNMC (AUC0.91), andMIC-1 (AUC 0.83) were best able to discriminate
S-35 AGA Abstracts
between HC and PC with sensitivities of 81%, 79% and 78% and specificities of 83%, 83%and 78%, respectively. By comparison, AUC estimates for CA19-9 was only 0.76. The onlymarker which showed a statistically significant difference between PC and CP was MIC-1(p=0.043). However, the estimated AUC for MIC-1 was only 0.63, indicating that this markeris unlikely to be effective in discriminating between CP and PC. High correlation betweenUNMC and MDACC and NGAL assays was found. Conclusions: This study provides evidenceof differences in PJ biomarker expression between HC, CP and PC. These results suggestthat some of the differences may be strong enough to be effective diagnostically. Specifically,MIC-1 and NGAL were fairly effective in discriminating between HC and PC, while NGALalone was fairly effective in discriminating between HC and CP. Nomarkers helped discrimin-ating between CP and PC, though further study with an expanded sample set may allowsignificant differences to be observed.
146
Increased Incidence of Non-Hodgkin Lymphoma Subtypes in Patients WithCeliac DiseaseLori A. Leslie, Benjamin Lebwohl, Alfred I. Neugut, John Gregory Mears, Govind Bhagat,Peter H. Green
PURPOSE: Prior studies have described an increased incidence of lymphoma in patientswith celiac disease. However, few studies differentiated among the various types of lymphop-roliferative disorders (LPD). Additionally, identification of patients at high risk of developingLPD remains unclear. Our aims were to (1) determine the incidence of LPD subtypes inceliac disease patients compared to the general population and (2) describe the pattern ofceliac disease presentation in those who develop concurrent LPD compared to those whodo not. METHODS: We conducted a single-center retrospective cohort study of patientswith biopsy-proven celiac disease seen at Columbia University Medical Center between 1981and 2010 to identify patients with LPDs (defined as any non-Hodgkin lymphoma, Hodgkinlymphoma, or chronic lymphocytic leukemia). We calculated standardized incidence ratios(SIR) and correlating 95% confidence intervals (95%CI) using the Surveillance, Epidemiology,and End Result database to estimate the expected incidence of LPD subtypes. SIR was notcalculated for a LPD subtype if the observed incidence was less than 2 or expected incidencewas zero. RESULTS: Our cohort included 1,281 celiac patients with a total of 13,459 person-years of observation. We identified 35 case of LPD (SIR 5.7, 95%CI 3.9-7.7); 29 non-Hodgkin lymphomas (SIR 3.4, 95%CI 1.9-5.0), one Hodgkin lymphoma, and 5 chroniclymphocytic leukemias (SIR 4.1, 95%CI 1.2-8.3). Of the 29 non-Hodgkin lymphomas, therewere 11 enteropathy-associated T-cell (expected rate of 0), 4 peripheral T-cell (SIR 18.0,95%CI 4.6-39.9), and 14 B-cell lymphomas (SIR 3.0, 95%CI 1.6-4.7). Of the 14 B-cell non-Hodgkin lymphomas, there were 4 diffuse large B-cell (SIR 3.6, 95%CI 0.9-7.9), 3 mantlecell (SIR 32.3, 95%CI 6.0-79.1), 4 marginal zone (SIR 29.8, 95%CI 7.7-66.2), one follicular,one primary effusion, and one post-transplant LPD. The incidence of non-Hodgkin lymphomain both genders was similar (SIR women 6.0, 95%CI 3.7-8.9; SIR men 5.3, 95%CI 2.9-8.4). Twenty patients were diagnosed with celiac disease prior to LPD (mean 7.8±8.2 years),5 concurrently, and 10 after LPD (mean 6.6±5.0 years). Patients who developed LPD werediagnosed with celiac disease at a later age (mean 55±16 versus 43±17 years old, p<0.0001)and were more likely to present with diarrhea (69% versus 40% p=0.0068) and/or abdominalpain (12% versus 3% p=0.041) than those who did not develop LPD. CONCLUSIONS: Theincidence of LPD is increased in celiac disease compared to the general population; particularlyenteropathy-associated T-cell lymphoma aswell as peripheral T-cell, mantle cell, andmarginalzone lymphomas. Patients diagnosed with celiac disease after age 50 who initially presentwith diarrhea and/or abdominal pain are at increased risk and may benefit from routinefollow-up and surveillance.
147
Not All That Flattens is Celiac Disease: Mimics of Celiac Enteropathy inContemporary Clinical PracticeKumar Pallav, Daniel A. Leffler, Sohaib Tariq, Jeffrey D. Goldsmith, Robert M. Najarian,Joshua Hansen, Melinda Dennis, Detlef Schuppan, Ciaran P. Kelly
Background The diagnosis of celiac disease (CD) is based on histologic changes includingvillous blunting on duodenal biopsies and positive serum antibodies. However, while celiacdisease is the most common cause of duodenal villous atrophy, there is a broad differentialdiagnosis for villous atrophy, especially in patients with negative celiac serologies. Our aimwas to identify the spectrum of conditions causing non celiac enteropathy (NCE) and toassess methods of differentiating between CD and NCE in clinical practice. Methods Throughrecord review we identified patients with duodenal villous atrophy due to causes other thanCD. Inclusion criteria for NCE were villous atrophy and either negative CD HLA testing orthe combination of negative CD serology and lack of histological improvement on a glutenfree diet (GFD). Investigations that lead to a correct diagnosis of NCE were noted. Findingswere also compared to our overall CD population. Results The underlying etiologies of the30 NCE patients identified are listed in Table1. The male to female ratio was 1:2 and themedian age at diagnosis was 55 years (range 20-76), compared to 42 (range 0-89) for CD(p=.01). All classic symptoms of CD occurred at a higher frequency in NCE patients (Table2). 19 (86%) of the 22 NCE patients who underwent celiac genetic testing were HLA DQ2& DQ8 negative. 4 (13%) NCE patients had a positive tissue transglutaminase antibody,(mean 37 U, nl < 20, range 20 to 67) as compared to 97% of CD patients (p=.0001). 21(70%) of the NCE patients were initially diagnosed with CD, 8 of whom reported somesymptom improvement on a gluten free diet, however none showed histological recovery.Anti enterocyte antibodies were positive in 1 of 7 patients tested. The frequencies of abnormalLFTs and inflammatory markers were similar in both groups. Conclusion Most patients(70%) with villous atrophy caused by NCE are initially misdiagnosed as having CD andNCE is easily further misdiagnosed as refractory celiac disease. In patients with villousblunting, a normal initial tTG (87%) should alert clinicians to possible NCE. The diagnosiscan often be confirmed (86%) by negative HLA-DQ2/DQ8 genetic test. While CD oftenpresents with extraintestinal manifestations, NCE symptoms are nearly always gastrointesti-nal. A subjective response to GFD is not an accurate indicator of CD vs NCE. Repeat biopsyand review of initial biopsies by a skilled GI pathologist may help when findings other than
AG
AA
bst
ract
s
AG
AA
bst
ract
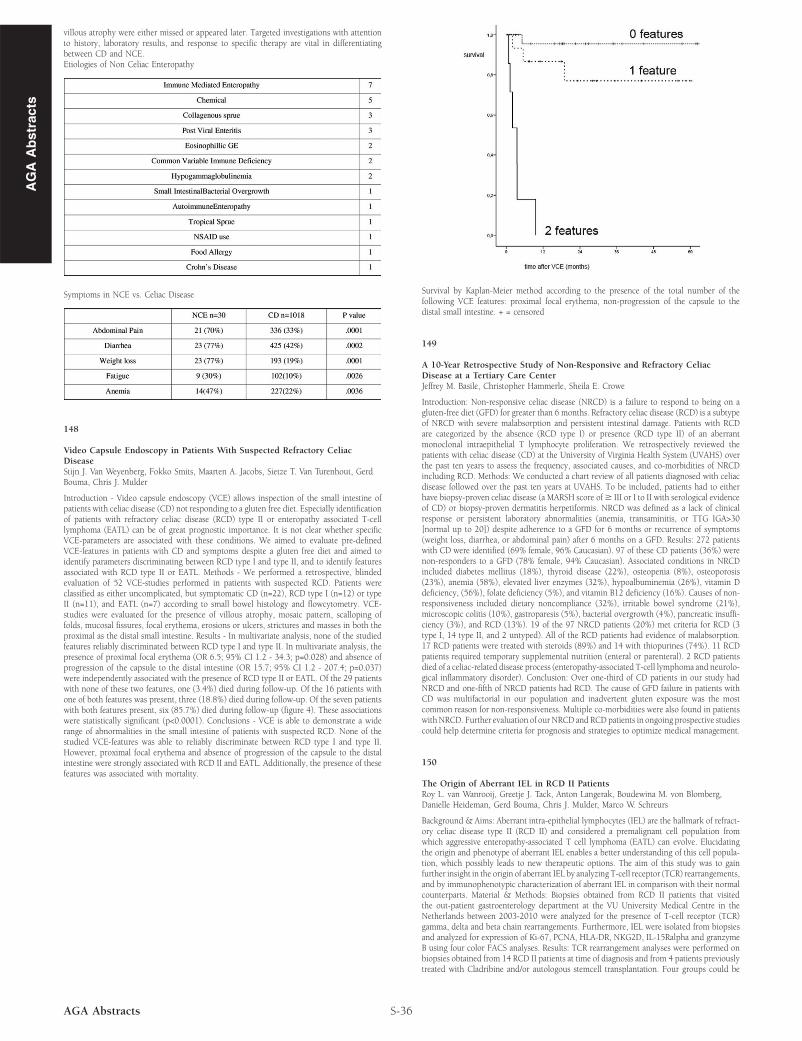
svillous atrophy were either missed or appeared later. Targeted investigations with attentionto history, laboratory results, and response to specific therapy are vital in differentiatingbetween CD and NCE.Etiologies of Non Celiac Enteropathy
Symptoms in NCE vs. Celiac Disease
148
Video Capsule Endoscopy in Patients With Suspected Refractory CeliacDiseaseStijn J. Van Weyenberg, Fokko Smits, Maarten A. Jacobs, Sietze T. Van Turenhout, GerdBouma, Chris J. Mulder
Introduction - Video capsule endoscopy (VCE) allows inspection of the small intestine ofpatients with celiac disease (CD) not responding to a gluten free diet. Especially identificationof patients with refractory celiac disease (RCD) type II or enteropathy associated T-celllymphoma (EATL) can be of great prognostic importance. It is not clear whether specificVCE-parameters are associated with these conditions. We aimed to evaluate pre-definedVCE-features in patients with CD and symptoms despite a gluten free diet and aimed toidentify parameters discriminating between RCD type I and type II, and to identify featuresassociated with RCD type II or EATL. Methods - We performed a retrospective, blindedevaluation of 52 VCE-studies performed in patients with suspected RCD. Patients wereclassified as either uncomplicated, but symptomatic CD (n=22), RCD type I (n=12) or typeII (n=11), and EATL (n=7) according to small bowel histology and flowcytometry. VCE-studies were evaluated for the presence of villous atrophy, mosaic pattern, scalloping offolds, mucosal fissures, focal erythema, erosions or ulcers, strictures and masses in both theproximal as the distal small intestine. Results - In multivariate analysis, none of the studiedfeatures reliably discriminated between RCD type I and type II. In multivariate analysis, thepresence of proximal focal erythema (OR 6.5; 95% CI 1.2 - 34.3; p=0.028) and absence ofprogression of the capsule to the distal intestine (OR 15.7; 95% CI 1.2 - 207.4; p=0.037)were independently associated with the presence of RCD type II or EATL. Of the 29 patientswith none of these two features, one (3.4%) died during follow-up. Of the 16 patients withone of both features was present, three (18.8%) died during follow-up. Of the seven patientswith both features present, six (85.7%) died during follow-up (figure 4). These associationswere statistically significant (p<0.0001). Conclusions - VCE is able to demonstrate a widerange of abnormalities in the small intestine of patients with suspected RCD. None of thestudied VCE-features was able to reliably discriminate between RCD type I and type II.However, proximal focal erythema and absence of progression of the capsule to the distalintestine were strongly associated with RCD II and EATL. Additionally, the presence of thesefeatures was associated with mortality.
S-36AGA Abstracts
Survival by Kaplan-Meier method according to the presence of the total number of thefollowing VCE features: proximal focal erythema, non-progression of the capsule to thedistal small intestine. + = censored
149
A 10-Year Retrospective Study of Non-Responsive and Refractory CeliacDisease at a Tertiary Care CenterJeffrey M. Basile, Christopher Hammerle, Sheila E. Crowe
Introduction: Non-responsive celiac disease (NRCD) is a failure to respond to being on agluten-free diet (GFD) for greater than 6 months. Refractory celiac disease (RCD) is a subtypeof NRCD with severe malabsorption and persistent intestinal damage. Patients with RCDare categorized by the absence (RCD type I) or presence (RCD type II) of an aberrantmonoclonal intraepithelial T lymphocyte proliferation. We retrospectively reviewed thepatients with celiac disease (CD) at the University of Virginia Health System (UVAHS) overthe past ten years to assess the frequency, associated causes, and co-morbidities of NRCDincluding RCD. Methods: We conducted a chart review of all patients diagnosed with celiacdisease followed over the past ten years at UVAHS. To be included, patients had to eitherhave biopsy-proven celiac disease (a MARSH score of≥ III or I to II with serological evidenceof CD) or biopsy-proven dermatitis herpetiformis. NRCD was defined as a lack of clinicalresponse or persistent laboratory abnormalities (anemia, transaminitis, or TTG IGA>30[normal up to 20]) despite adherence to a GFD for 6 months or recurrence of symptoms(weight loss, diarrhea, or abdominal pain) after 6 months on a GFD. Results: 272 patientswith CD were identified (69% female, 96% Caucasian). 97 of these CD patients (36%) werenon-responders to a GFD (78% female, 94% Caucasian). Associated conditions in NRCDincluded diabetes mellitus (18%), thyroid disease (22%), osteopenia (8%), osteoporosis(23%), anemia (58%), elevated liver enzymes (32%), hypoalbuminemia (26%), vitamin Ddeficiency, (56%), folate deficiency (5%), and vitamin B12 deficiency (16%). Causes of non-responsiveness included dietary noncompliance (32%), irritable bowel syndrome (21%),microscopic colitis (10%), gastroparesis (5%), bacterial overgrowth (4%), pancreatic insuffi-ciency (3%), and RCD (13%). 19 of the 97 NRCD patients (20%) met criteria for RCD (3type I, 14 type II, and 2 untyped). All of the RCD patients had evidence of malabsorption.17 RCD patients were treated with steroids (89%) and 14 with thiopurines (74%). 11 RCDpatients required temporary supplemental nutrition (enteral or parenteral). 2 RCD patientsdied of a celiac-related disease process (enteropathy-associated T-cell lymphoma and neurolo-gical inflammatory disorder). Conclusion: Over one-third of CD patients in our study hadNRCD and one-fifth of NRCD patients had RCD. The cause of GFD failure in patients withCD was multifactorial in our population and inadvertent gluten exposure was the mostcommon reason for non-responsiveness. Multiple co-morbidities were also found in patientswithNRCD. Further evaluation of our NRCD and RCDpatients in ongoing prospective studiescould help determine criteria for prognosis and strategies to optimize medical management.
150
The Origin of Aberrant IEL in RCD II PatientsRoy L. van Wanrooij, Greetje J. Tack, Anton Langerak, Boudewina M. von Blomberg,Danielle Heideman, Gerd Bouma, Chris J. Mulder, Marco W. Schreurs
Background & Aims: Aberrant intra-epithelial lymphocytes (IEL) are the hallmark of refract-ory celiac disease type II (RCD II) and considered a premalignant cell population fromwhich aggressive enteropathy-associated T cell lymphoma (EATL) can evolve. Elucidatingthe origin and phenotype of aberrant IEL enables a better understanding of this cell popula-tion, which possibly leads to new therapeutic options. The aim of this study was to gainfurther insight in the origin of aberrant IEL by analyzing T-cell receptor (TCR) rearrangements,and by immunophenotypic characterization of aberrant IEL in comparison with their normalcounterparts. Material & Methods: Biopsies obtained from RCD II patients that visitedthe out-patient gastroenterology department at the VU University Medical Centre in theNetherlands between 2003-2010 were analyzed for the presence of T-cell receptor (TCR)gamma, delta and beta chain rearrangements. Furthermore, IEL were isolated from biopsiesand analyzed for expression of Ki-67, PCNA, HLA-DR, NKG2D, IL-15Ralpha and granzymeB using four color FACS analyses. Results: TCR rearrangement analyses were performed onbiopsies obtained from 14 RCD II patients at time of diagnosis and from 4 patients previouslytreated with Cladribine and/or autologous stemcell transplantation. Four groups could be