NONSPECIFIC DEFENSES OF THE HOST. Innate Immunity (Non-Adaptive Immunity) (Pre-existing immunity)...
129
NONSPECIFIC DEFENSES OF THE HOST
-
Upload
claude-patterson -
Category
Documents
-
view
226 -
download
4
Transcript of NONSPECIFIC DEFENSES OF THE HOST. Innate Immunity (Non-Adaptive Immunity) (Pre-existing immunity)...
NONSPECIFIC DEFENSES
OF THE HOST
Innate Immunity (Non-Adaptive Immunity)
(Pre-existing immunity)
Immunity you are born with
Does not change/adapt
during life in response to infection
There are over 400 known pathogens of man and each of us is likely to come into contact with at least 150 of them within our life span
HOST IMMUNE SYSTEM
Viruses (10-20 nm)
Bacteria (1-2 um)
Protozoa (50-100um)
Fungi (10um-10cm)
Parasites (Worms & Flukes) (>10cm)
Include:
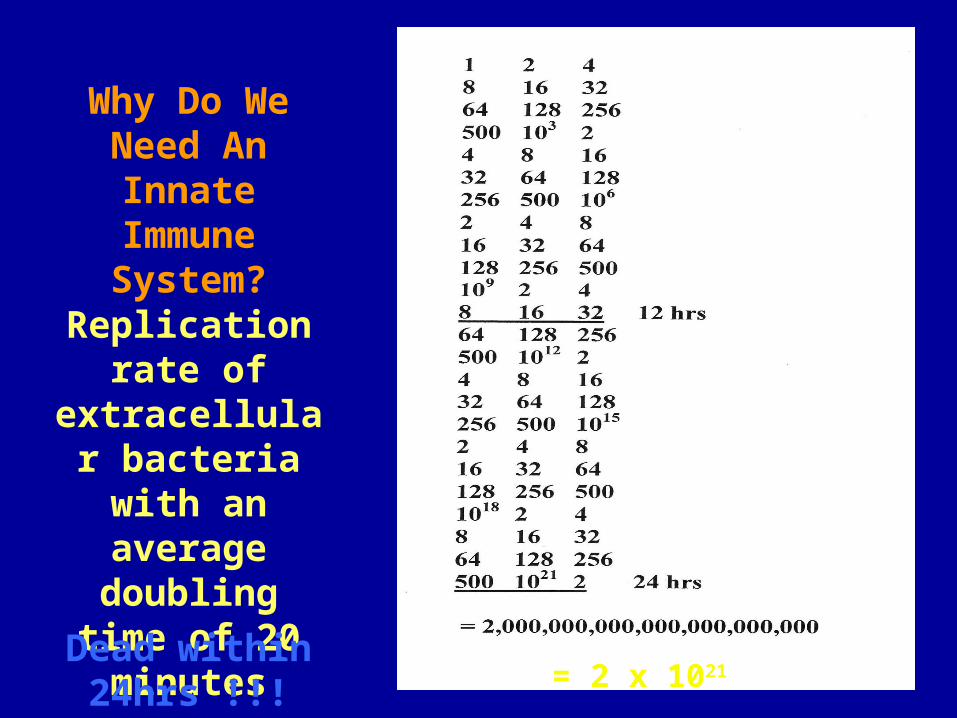
Replication rate of extracellular bacteria with an
average doubling time of 20 minutes
Why Do We Need An Innate
Immune System?
Dead within 24hrs !!! = 2 x 1021
Innate Immune System comprises
of a
Cellular arm (cells)
and
a
Humoral arm (soluble factors)
IMMUNOLOGYStudy of how the body limits invasion by non-self andrecognises and eliminates altered self - damaged cells and cancer cells
HAEMATOLOGYStudy of blood cells and their origins andthe homeostatic mechanisms that control coagulation
Most types of blood cell are components of the immune system
INFECTIONDifferences between infectious agents andtheir sites of replication necessitatedifferent immune mechanisms for their control
•VIRUSES (DNA & RNA, intracellular replication)
•BACTERIA (intracellular / extracellular replication)
•FUNGI
•PROTOZOA
•WORMS
DEFENCE AGAINST INFECTION
•Physical barriers
•Non-adaptive (Innate) immunity
•Adaptive immunity
NONSPECIFIC RESISTANCE
• Defenses that protect the host against ANY pathogen– Mechanical factors
– Chemical factors
Specific Resistance
Specific Resistance, or immunity is based on antibody production
It is a defense against a particular microorganism
Mechanical Factors
The intact skin consists of the dermis, an inner thicker portion composed of connective tissue, and the epidermis, an outer, thinner portion consisting of several layers of epithelial cells
The top layer of epidermal cells contains the protein keratin (remember—fungi produce keratinase)
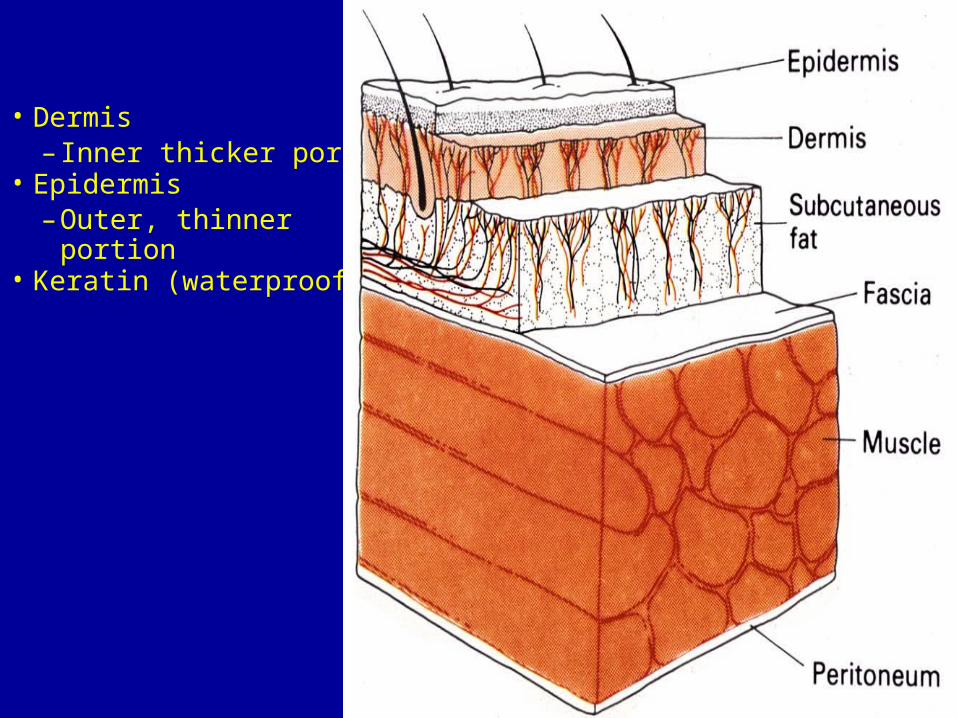
SKIN• Dermis
– Inner thicker portion• Epidermis
– Outer, thinner portion• Keratin (waterproofing)
SKIN INFECTIONS• Rare in unbroken skin• Sweat washes microbes off• Cuts and burns may get infected
–Subcutaneous infections–Staphylococcus spp.
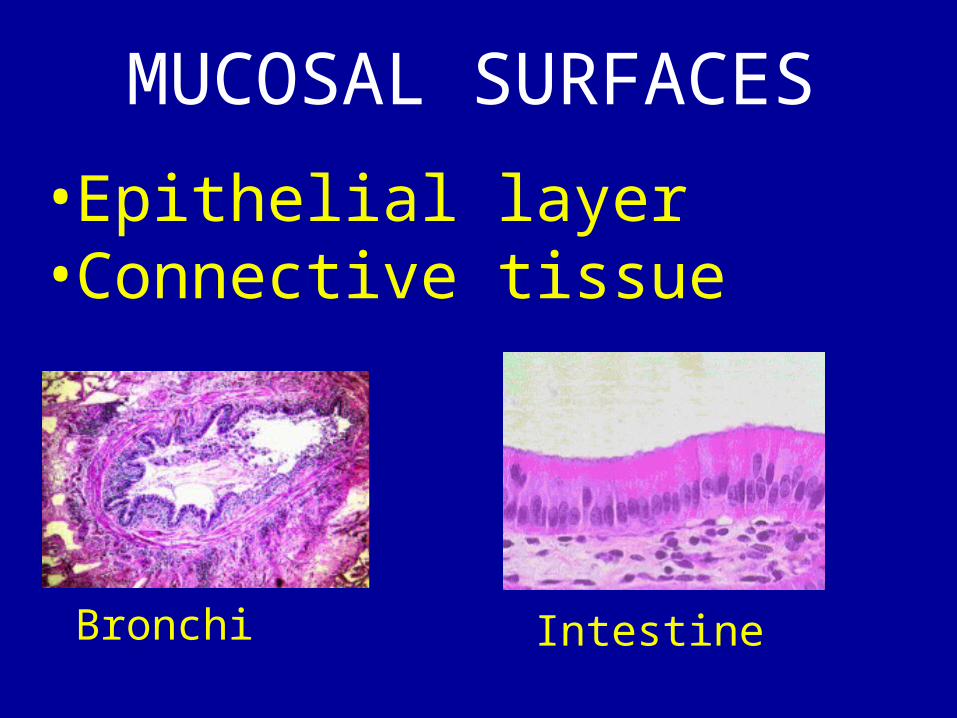
MUCOSAL SURFACES
• Epithelial layer• Connective tissue
Bronchi Intestine
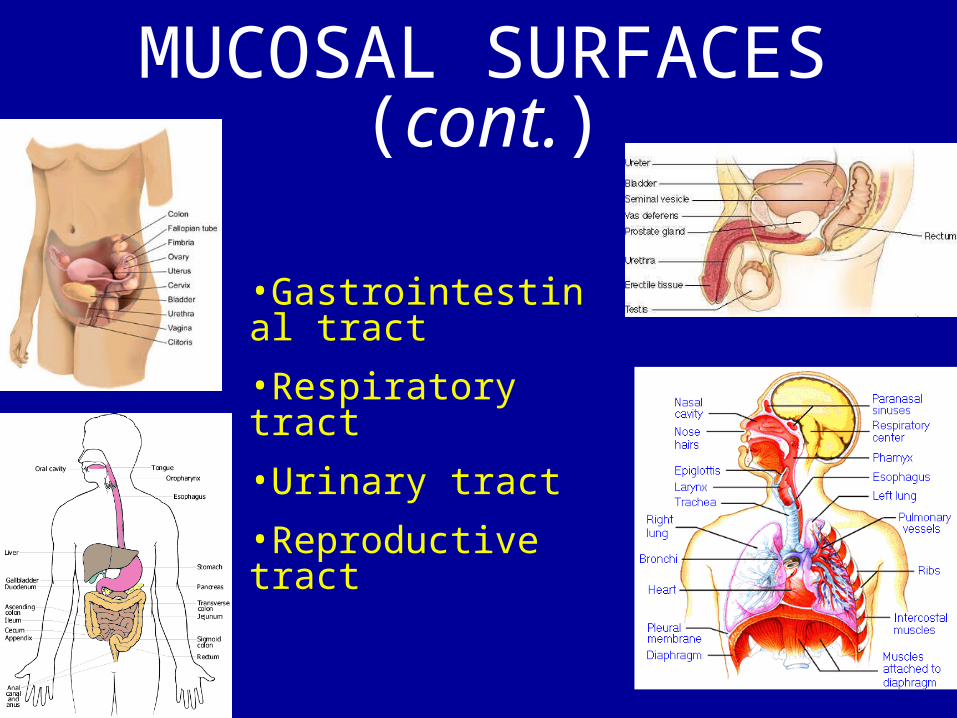
MUCOSAL SURFACES (cont.)
•Gastrointestinal tract
•Respiratory tract
•Urinary tract
•Reproductive tract
MUCOSAL SURFACES (cont.)
• Mucus traps microorganisms
• Physical barrier• Cilia lower respiratory
tract• Washing (sweat)
MUCOSAL SURFACES (cont.)
• Mucosal irritation or damage facilitates infection (smoking)
• Substances produced by pathogens–Treponema pallidum
Flushing of Cavities• Prevents colonization–Tears (lysozyme—breaks down NAG/NAM)
–Saliva–Urine–Feces–Sebum (unsaturated fatty acids of
sebum inhibit growth of certain pathogens)
CHEMICAL FACTORS
• Skin–Sebaceous glands
•Unsaturated fatty acids
•pH 3-5
LYSOZYME
• Enzyme that degrades peptidoglycans–Gram positives more susceptible than Gram negatives
LYSOZYME (cont.)
• Sweat• Saliva• Tears• Nasal
secretions
GASTRIC JUICE
• Hydrochloric acid (pH 1.2 to 3)–Helicobacter pylori
•Neutralizes acidic pH• Enzymes• Mucus
BLOOD
• Iron-binding proteins–Lactoferrins
–Transferrins
• Iron unavilable for pathogens
DEAD TISSUE leads to INFECTION
Mechanical, chemical or thermal injuryDebride wounds
Interruption of blood supply – infarction
DEFENCE AGAINST INFECTION•Physical barriers•Non-adaptive (Innate) immunity•Adaptive immunity
A variety of immune mechanisms utilisingproteins and cells that act in concertto control and eradicate infection
Immune mechanisms are targeted bymolecular recognition of micro-organisms
INNATE IMMUNITY
•Mast cellsincrease blood flow and vascular permeabilitybring components of immunity to site of infection
•Phagocytesengulf (phagocytose) and destroy micro-organisms
•Complementactivate mast cells, attract phagocytes, opsonizeand lyze micro-organisms
•Acute phase proteinsactivate complement and opsonise
SPECIFIC IMMUNITY
For each different antigen there is a specific receptor
1011 different antigens
1
2
3
4
1011 different receptors
4
31
2
Exposure to infection Resistance to infection
•Climate•Vectors•Population•Housing•Water / sewage•Public health•Mutation
•Age•Previous exposure•Vaccination•Nutrition•Disease•immunodeficiency

PHAGOCYTOSIS is the body’s second line of
defense
• Ingestion of particulated matter by a cell–Phagocytes (white blood cells)
–Phagocytosis derived from the Greek work “to eat” and “cell”
Formed Elements in Blood--Blood fluid is called plasma
--Cells and cell fragments of the blood are the formed elements
--Most important ones in Immunology are the leukocytes (WBC)
--Decreased leukocyte counts are called leukopenia (I.e.Thrombocytopenia)
A differential white blood count detects leukocyte number changes
Leukocytes are subdivided into three categoriesGRANULOCYTES---have granules in their cytoplasm (neutrophils, basophils, eosinophils)
LYMPHOCYTES (are note phagocytic—occur in lymphoid tissue)
MONOCYTES (lack granules & are phagocytic only after maturing into MQ)
PHAGOCYTES• Neutrophils (60-70%)
–Initial phagocytic cells• Monocytes/Macrophages (3-
8%)–Final phagocytic cells
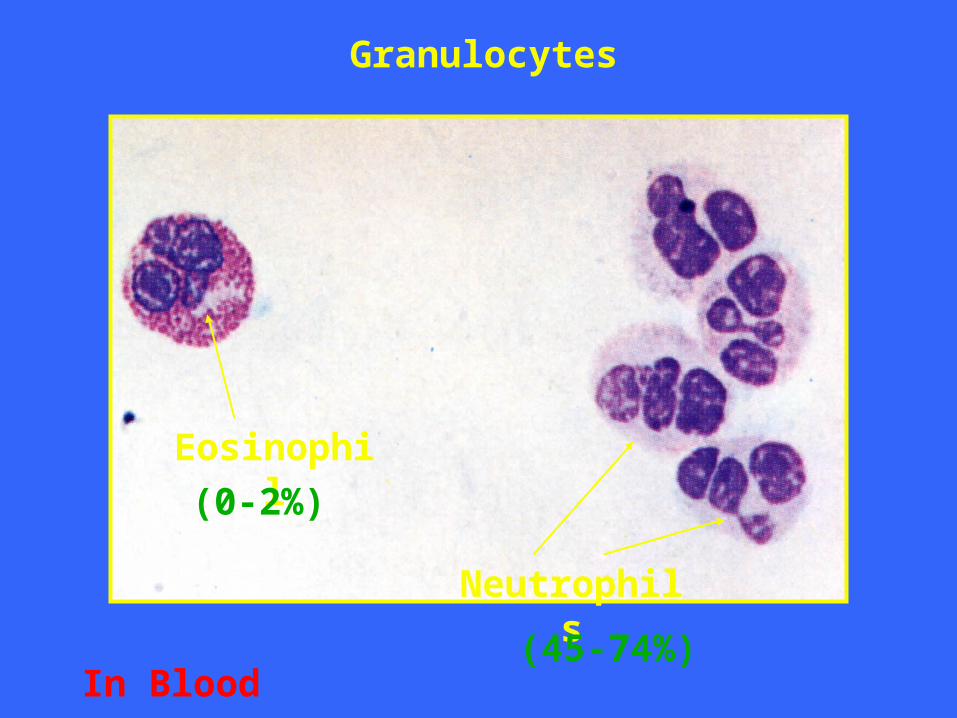
Eosinophil
Neutrophils
Granulocytes
In Blood
(0-2%)
(45-74%)
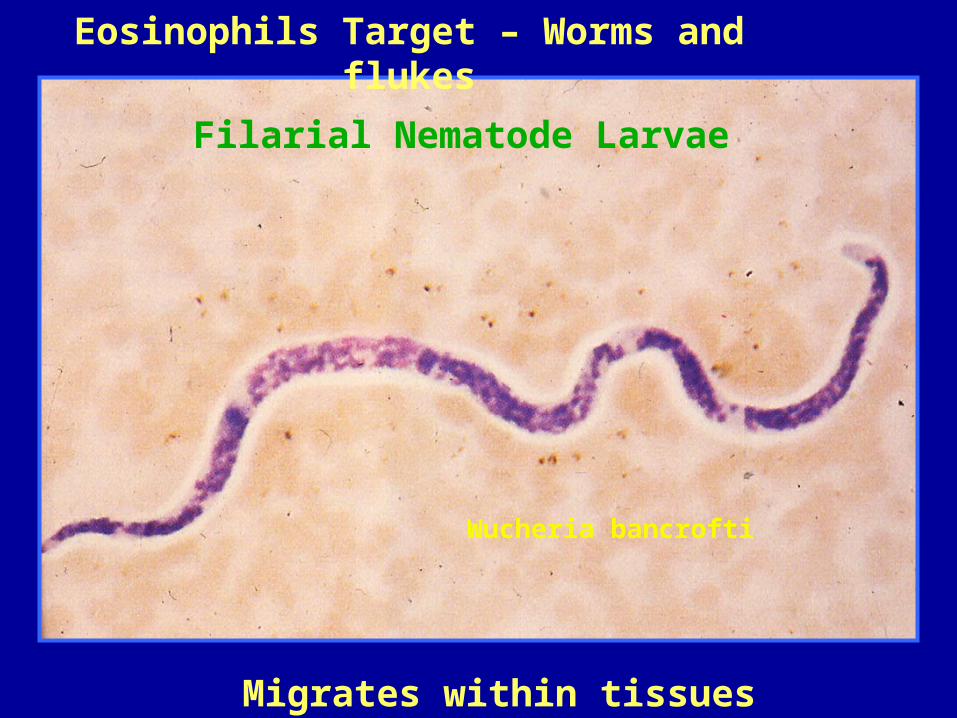
Filarial Nematode Larvae
Migrates within tissues
Wucheria bancrofti
Eosinophils Target – Worms and flukes
Granulocytes are mostly neutrophils that wander in the blood and can pass through capillary walls to reach trauma sites
MQ are highly phagocytic cells called wandering MQ’s b/c of their ability to migrate
Fixed MQ’s (histiocytes) enter tissue/organs and remain there (I.e. Kupffer cells in the liver)
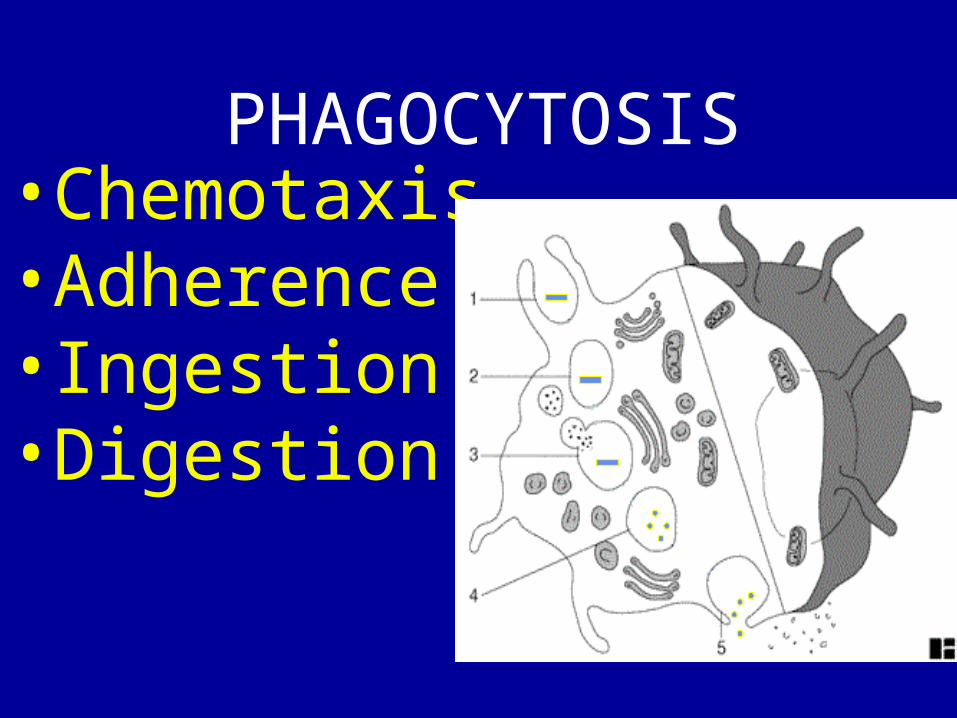
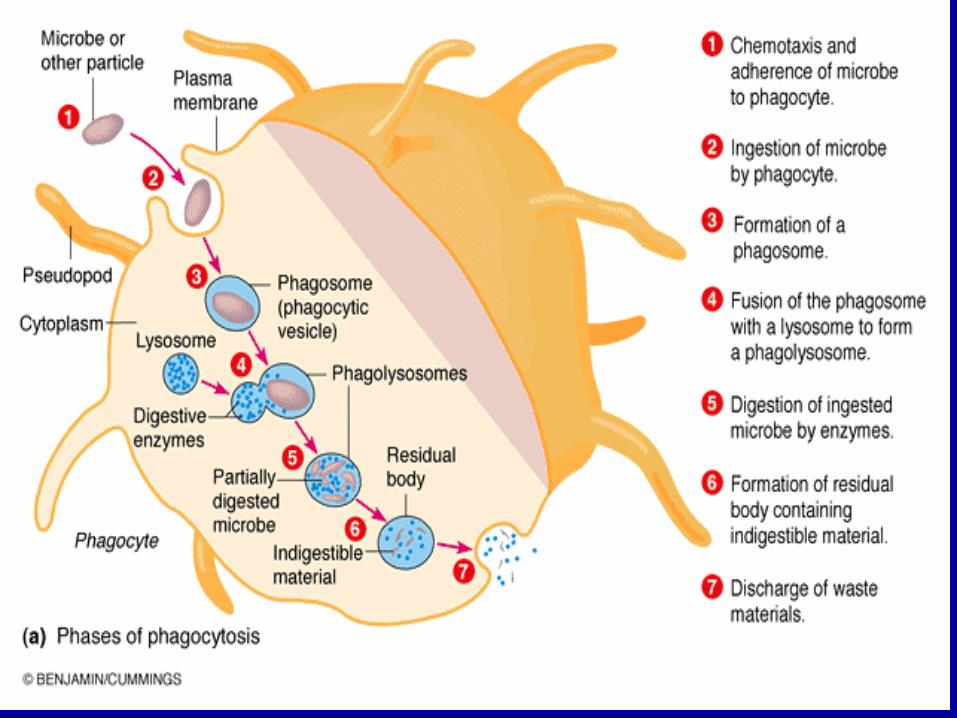
PHAGOCYTOSIS• Chemotaxis• Adherence• Ingestion• Digestion
Avoiding Contact with Phagocytes
• Bacteria can avoid the attention of phagocytes in a number of ways
• Pathogens may invade or remain confined in regions inaccessible to phagocytes. Certain internal tissues (e.g. the lumens of glands, the urinary bladder) and surface tissues (e.g. the skin) are not patrolled by phagocytes.
• Some pathogens are able to avoid provoking an overwhelming inflammatory response. Without inflammation the host is unable to focus the phagocytic defenses.
Some bacteria or their products inhibit phagocyte chemotaxis
For example, Streptococcal streptolysin suppresses neutrophil chemotaxis, even in very low concentrations
Fractions of Mycobacterium tuberculosis are known to inhibit leukocyte migration.
• Some pathogens can cover the surface of the bacterial cell with a component which is seen as "self" by the host phagocytes and immune system. Such a strategy hides the antigenic surface of the bacterial cell.
• Phagocytes cannot recognize bacteria upon contact and the possibility of opsonization by antibodies to enhance phagocytosis is minimized.
• Staphylococcus aureus produces cell-bound coagulase which clots fibrin on the bacterial surface
• Treponema pallidum, the agent of syphilis, binds fibronectin to its surface.
• Group A streptococci are able to synthesize a capsule composed of hyaluronic acid. Hyaluronic acid is the ground substance (tissue cement) in connective tissue.
CHEMOTAXIS
• Chemical attraction of phagocyte to microorganism–Microbial products–Damaged tissue–White blood cell components
ADHERENCE & ENGULFMENT (INGESTION)
• Attachment of phagocyte plasma membrane to microorganism
INGESTION
• Pseudopods extend from phagocyte plasma membrane and engulf the microorganism forming the phagosome
A pathogen is only a pathogen if it “tricks” the immune
system’s defense missiles (phagocytes)
Inhibition of Phagocytic Engulfment
• Some bacteria employ strategies to avoid engulfment (ingestion) if phagocytes do make contact with them
• Many important pathogenic bacteria bear on their surfaces substances that inhibit phagocytic adsorption or engulfment
• Clearly it is the bacterial surface that matters• Resistance to phagocytic ingestion is usually
due to a component of the bacterial cell surface (cell wall, or fimbriae, or a capsule).
Classical examples of antiphagocytic substances on the bacterial surface
include• Polysaccharide capsules of S. pneumoniae,
Haemophilus influenzae, Treponema pallidum and Klebsiella pneumoniae
• M protein and fimbriae of Group A streptococci • Surface slime (polysaccharide) produced as a
biofilm by Pseudomonas aeruginosa • O polysaccharide associated with LPS of E. coli • K antigen (acidic polysaccharides) of E. coli or
the analogous Vi antigen of Salmonella typhi
DIGESTION
• Within cytoplasma the phagosome fuses with lysosome (digestive enzymes) forming the phagolysosome
• Lysozyme• Lipases• Proteases
• Hypochlorous acid• Toxic O2
• Nucleases
LYSOSOME CONTENTS
Survival Inside of Phagocytes• Some bacteria survive inside of phagocytic
cells, in either neutrophils or macrophages• Bacteria that can resist killing and survive or
multiply inside of phagocytes are considered intracellular parasites
• In this case, the environment of the phagocyte may be a protective one, protecting the bacteria during the early stages of infection or until they develop a full complement of virulence factors
• The intracellular environment guards the bacteria against the activities of extracellular bactericides, antibodies, drugs, etc.
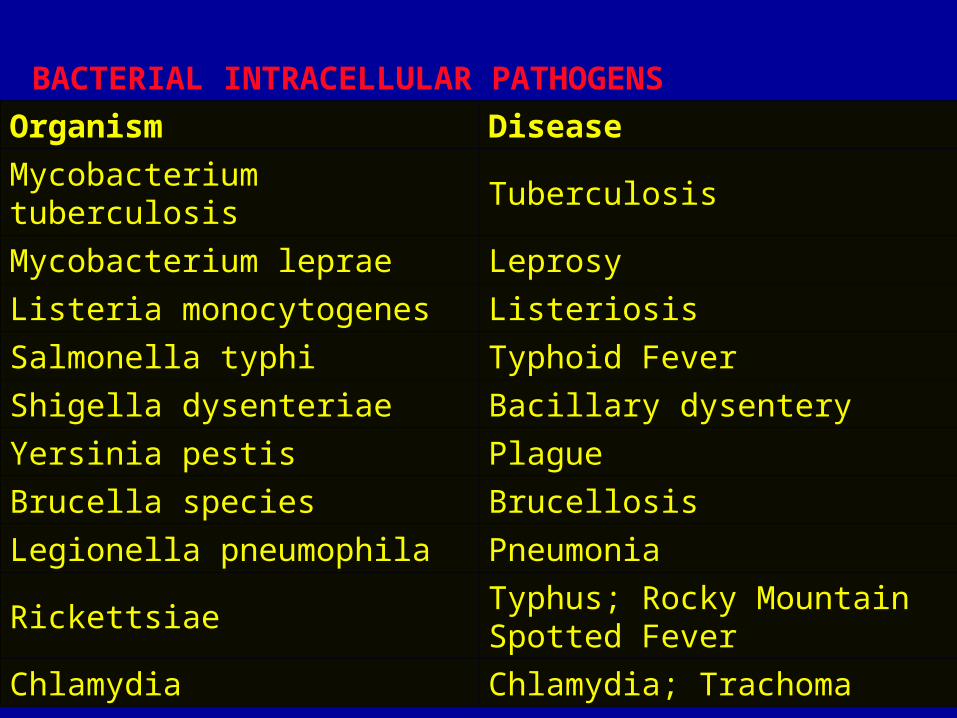
BACTERIAL INTRACELLULAR PATHOGENS
Organism Disease
Mycobacterium tuberculosis Tuberculosis
Mycobacterium leprae Leprosy
Listeria monocytogenes Listeriosis
Salmonella typhi Typhoid Fever
Shigella dysenteriae Bacillary dysentery
Yersinia pestis Plague
Brucella species Brucellosis
Legionella pneumophila Pneumonia
RickettsiaeTyphus; Rocky Mountain Spotted Fever
Chlamydia Chlamydia; Trachoma
• Many intracellular parasites have special (genetically-encoded) mechanisms to get themselves into host cells that are nonphagocytic
• Intracellular pathogens such as Yersinia, Listeria, Salmonella, Shigella and Legionella possess complex machinery for cellular invasion and intracellular survival
• These systems involve various types of non-toxin virulence factors
• Sometimes these factors are referred to as bacterial invasins
• Still other bacteria such as Bordetella pertussis and Streptococcus pyogenes, have recently been discovered in the intracellular habitat of epithelial cells
• Intracellular parasites survive inside of phagocytes by virtue of mechanisms which interfere with the bactericidal activities of the host cell.
PREVENTION OF PHAGOSOME AND
LYSOSOME
• Replicate inside phagocyte• Shigella• Mycobacterium
• Mycobacteria (including M. tuberculosis) have waxy, hydrophobic cell wall and capsule components (mycolic acids), which are not easily attacked by lysosomal enzymes
• In Salmonella typhimurium, the pH that develops in the phagosome after engulfment actually induces bacterial gene products that are essential for their survival in macrophages.
KILLING OF PHAGOCYTE
• Toxins• Staphylococcus
–Actinobacillus
• B. abortus and Staphylococcus aureus are vigorous catalase and superoxide dismutase producers, which might neutralize the toxic oxygen radicals that are generated by systems in phagocytes
• S. aureus produces cell-bound pigments (carotenoids) that "quench" singlet oxygen produced in the phagocytic vacuole
• Escape from the phagosome
• Early escape from the phagosome vacuole is essential for growth and virulence of some intracellular pathogens
• This is a clever strategy employed by the Rickettsiae
• Rickettsia enter host cells in membrane-bound vacuoles (phagosomes) but are free in the cytoplasm a short time later, perhaps in as little as 30 seconds
• A bacterial enzyme, phospholipase A, may be responsible for dissolution of the phagosome membrane.
• Listeria monocytogenes relies on several molecules for early lysis of the phagosome to ensure their release into the cytoplasm
• These include a pore-forming hemolysin (listeriolysin O) and two forms of phospholipase C
• Once in the cytoplasm, Listeria induces its own movement through a remarkable process of host cell actin polymerization and formation of microfilaments within a comet-like tail
Killing Phagocytes Before Ingestion
• Many Gram-positive pathogens, particularly the pyogenic cocci, secrete extracellular enzymes that kill phagocytes
• Many of these enzymes are called hemolysins because their activity in the presence of red blood cells results in the lysis of the RBC
• Extracellular proteins that inhibit phagocytosis include the Exotoxin A of Pseudomonas aeruginosa which kills macrophages
• bacterial exotoxins (Bacillus anthrax toxin EF & Bordatella pertussis toxin AC) which decrease phagocytic activity
INFLAMMATION• A localized protective response
of the body to tissue injury–Pain–Heat–Redness–Swelling–Loss of function
INFLAMMATION FUNCTIONS
• To destroy invading agents• Walling off invading agents• Repair or replace damaged
tissue
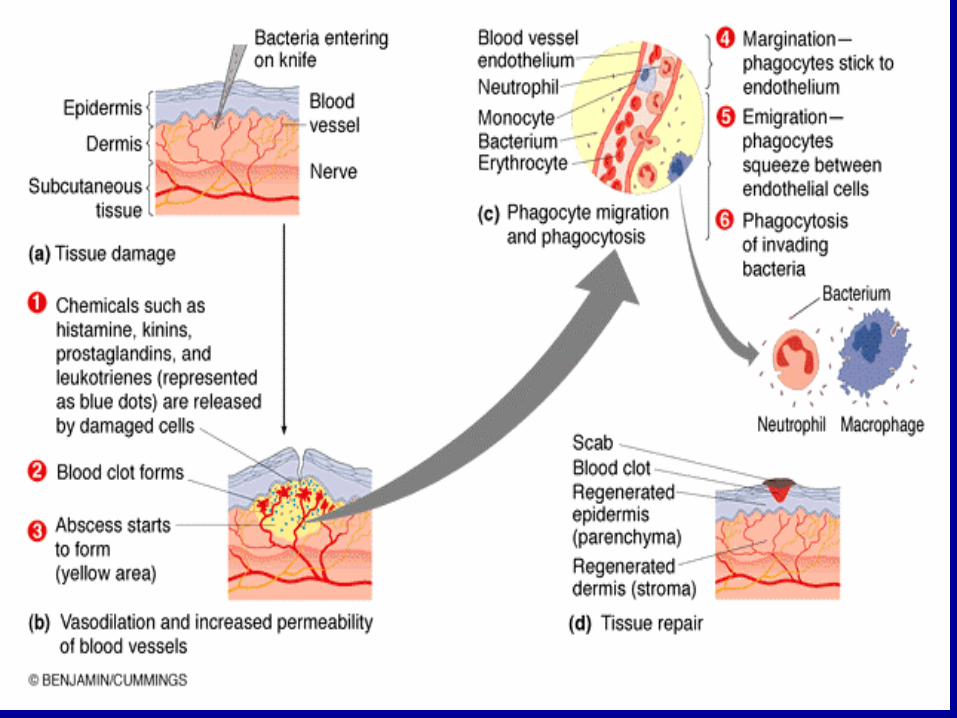
Vasodilatation & Increased Permeability of Blood Vessels
-Vasodilatation is the 1st stage of inflammation
-It involves an increase in blood vessel diameters more blood flow to the injured area
-Responsible for the redness, heat, edema (swelling), & pain of inflammation
-Histamine is released by injured cells & increases permeability of immune system cells to the site of injury
THE COMPLEMENT SYSTEM
part II
COMPLEMENT SYSTEM• 30 different serum proteins
involved in:–Lysis (destruction) of foreign
cells
–Inflammation
–Phagocytosis
Blood
SerumBlood clot
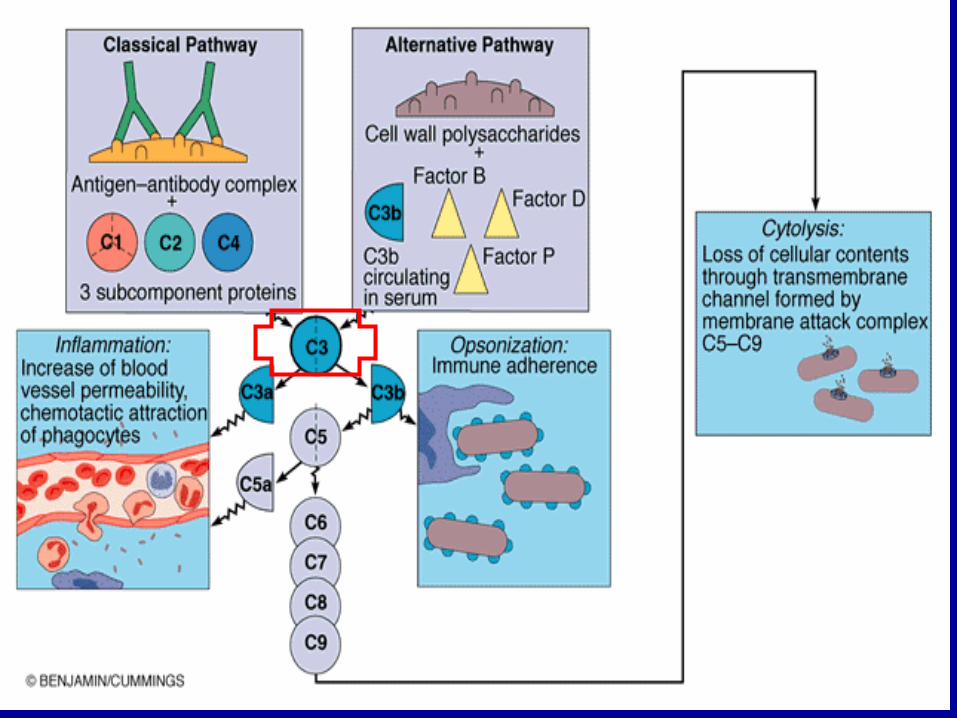
COMPLEMENT SYSTEM• Two cascade activation paths:
–Classical (immune system)
•Antibodies
–Alternative
•Interaction with Polysaccharides (mostly bacterial)
•Protein C3 activates both the alternative & the classical pathway
•Major components of the classical pathway are C1 and C9
Classical pathway is initiated by the binding of AB’s to Ag
Alternative pathway is initiated by the interaction of foreign particle with the protein factors (important in combating enteric G- MO)
Classical pathway
Alternative pathway
•Endotoxin (Lipid A) trigger the alternative pathway
•The alternative pathway is often known as the lectin pathway
•MQ interacting w/ the foreign particle stimulate the liver to secrete lectin, which assists in the opsonization of MO
• Increases the susceptibility of microorganisms to ingestion by phagocytes
What is opsonization?
Complement system & inflammation
•C5a is the most potent complement protein triggering inflammation
•It causes mast cells to release vasodilators such as histamine so that blood vessels become more permeable
•it increases the expression of adhesion molecules on leukocytes and the vascular endothelium so that leukocytes can squeeze out of the blood vessels and enter the tissue (diapedesis)
•it causes neutrophils to release toxic oxygen radicals for extracellular killing; and it induces fever
COMPLEMENT SYSTEM FUNCTIONS
• Cytolysis–Formation of membrane attack
complexes by the complement proteins
–Damage of plasma membrane
•leakage and death of the cell
COMPLEMENT SYSTEM FUNCTIONS
• Inflammation–Triggers histamine release
•Increased blood vessel permeability
•Promotes migration of cells to site of inflammation
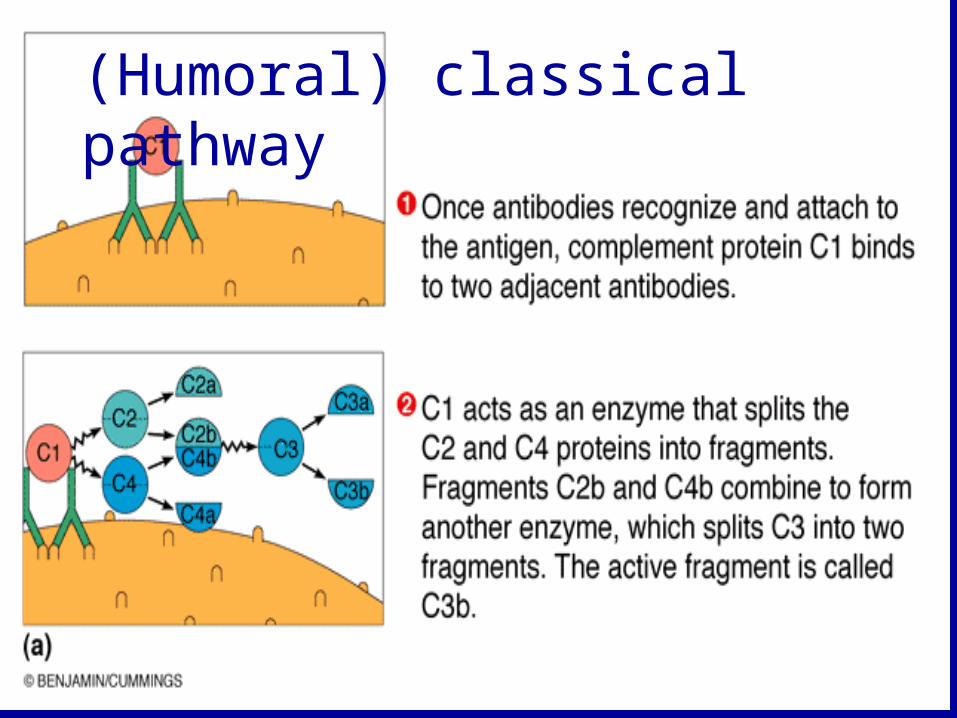
(Humoral) classical pathway
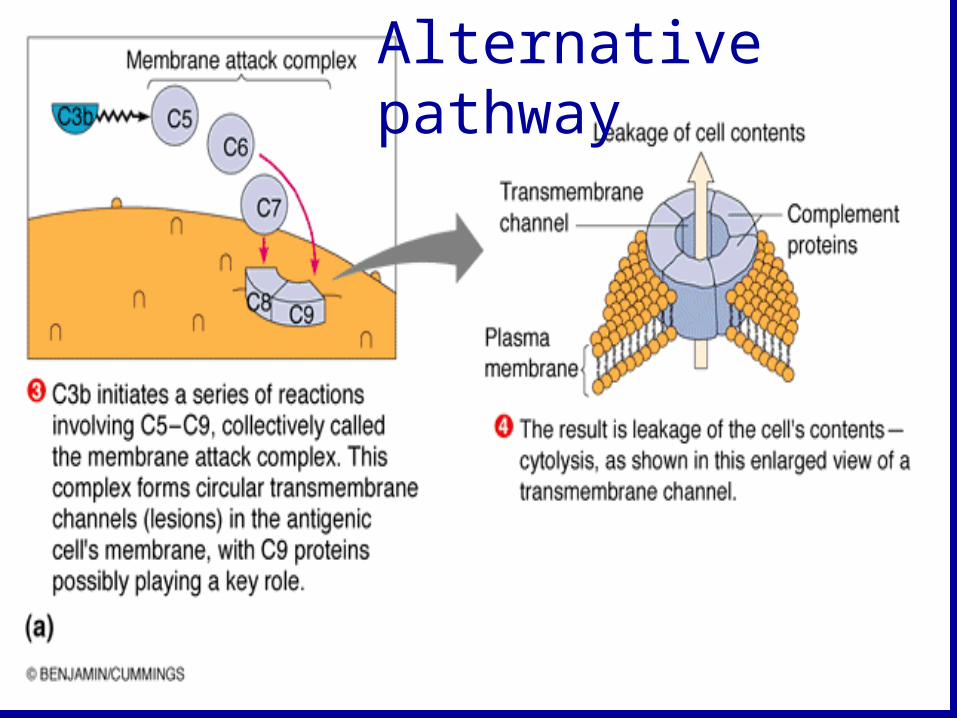
Alternative pathway
SPECIFIC DEFENSES OF THE HOST: THE IMMUNE
RESPONSE
IMMUNITY• Specific response to foreign
microorganisms or substances–Antibodies
–Specialized lymphocytes (B and T)

ANTIGENS
• Foreign substances or microorganisms that provoke an immune response
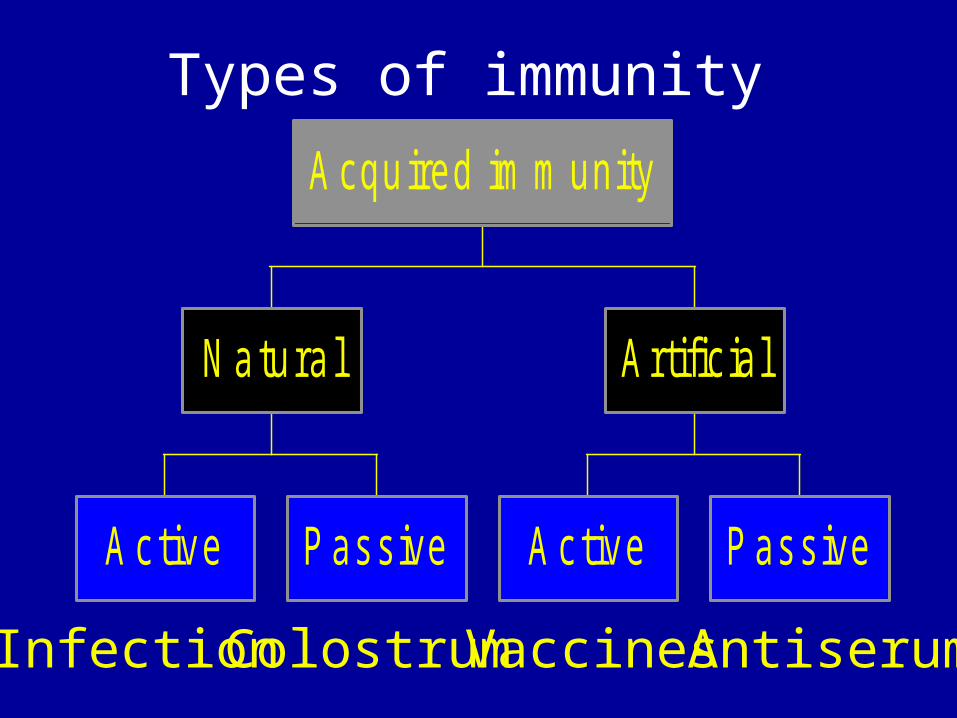
A ctive Passive
N atura l
A c tive Passive
Artificial
A cquired im m unity
Infection Colostrum Vaccines Antiserum
Types of immunity
COLOSTRUM
• Fluid rich in protein and immune factors, secreted by the mammary glands during the first few days of lactation

SERUM• Fluid remaining after
blood has clotted• Fluid where most
antibodies are found–Antiserum
Blood
SerumBlood clot
SEROLOGY
• The study of antibodies and antigens
IMMUNE SYSTEM
• Humoral or antibody-mediated–B lymphocytes
• Cell-mediated
–T lymphocytes (TH & TC)
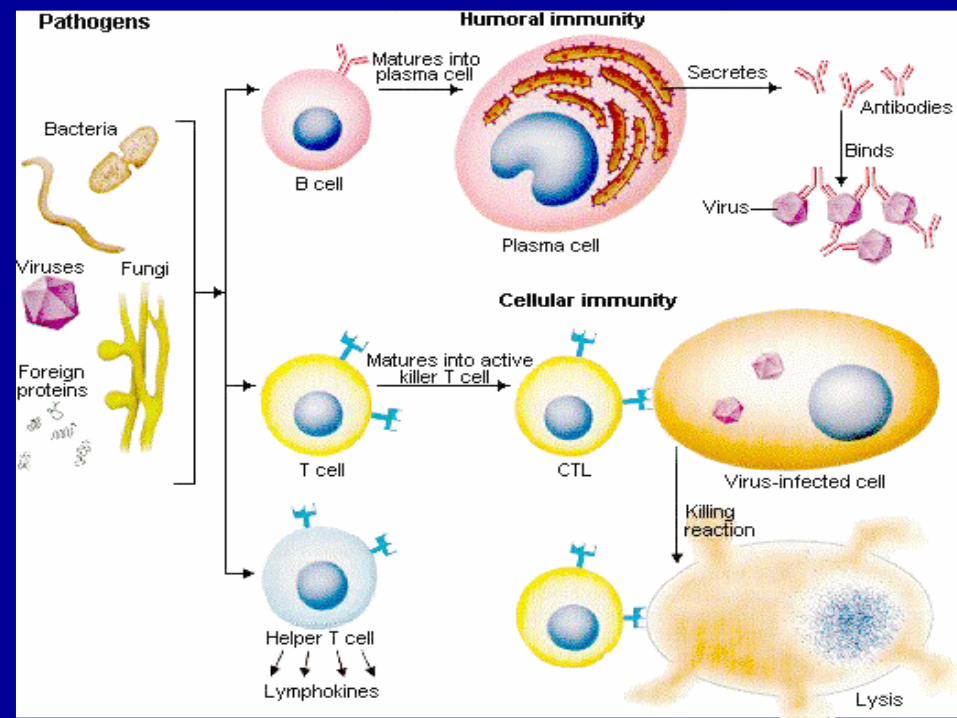
HUMORAL IMMUNE RESPONSE
• Against:–Bacteria
–Bacterial toxins
–Viruses outside of cells
CELLULAR IMMUNE RESPONSE
• Against:–Intracellular agents–Fungi–Protozoa–Helminths–Viruses inside cells
ANTIGENS
• Proteins• Polysaccharides• Lipids and nucleic acids
only if combined with proteins or polysaccharides
EPITOPES OR ANTIGENIC DETERMINANTS
• Antibodies specifically combine with a small segment of the antigen called the antigenic determinant or epitope to form an antigen-antibody complex
• The antigen-antibody reaction is characterized by specificity
HAPTEN• Small molecule that needs a large molecule carrier
to behave as an antigen• Drugs and pesticides are low molecular weight
molecules and can be treated as haptens• By conjugation to larger carrier molecules
(albumin), low molecular weight drugs and pesticides can be made antigenic
• Not antigenic unless attached to a carrier molecule– Penicillin – Penicillin binding to certain blood proteins
(albumin) can become antigenic Penicillin allergy
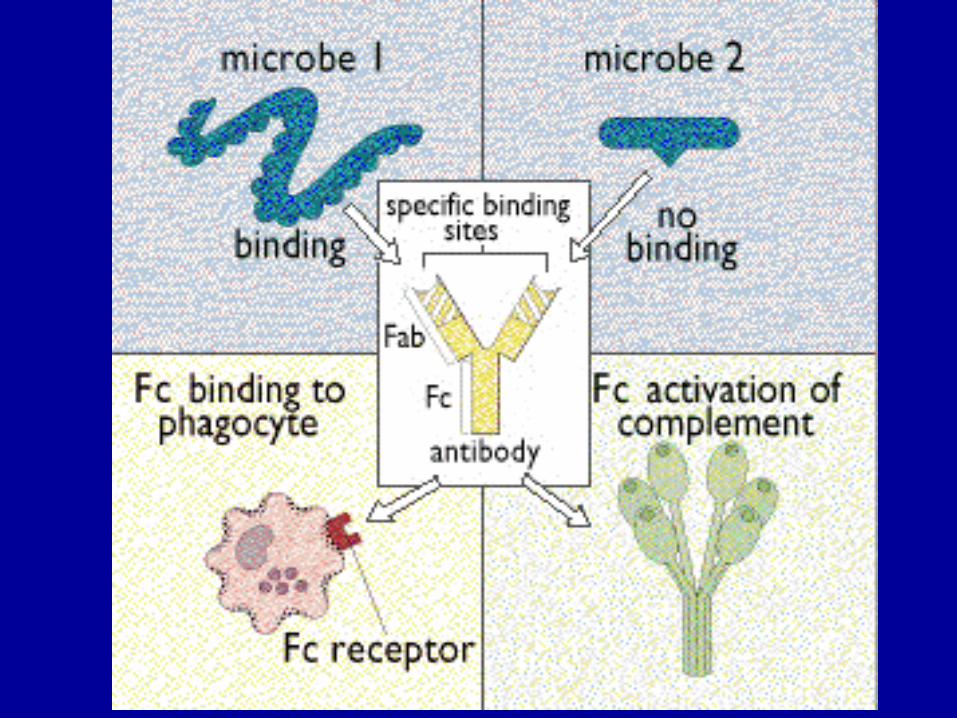
ANTIBODIES OR IMMUNOGLOBULINS
(Igs)• Y-shaped proteins made
in response to an antigen• Antibodies specifically
bind to that antigen by two antigen-binding sites
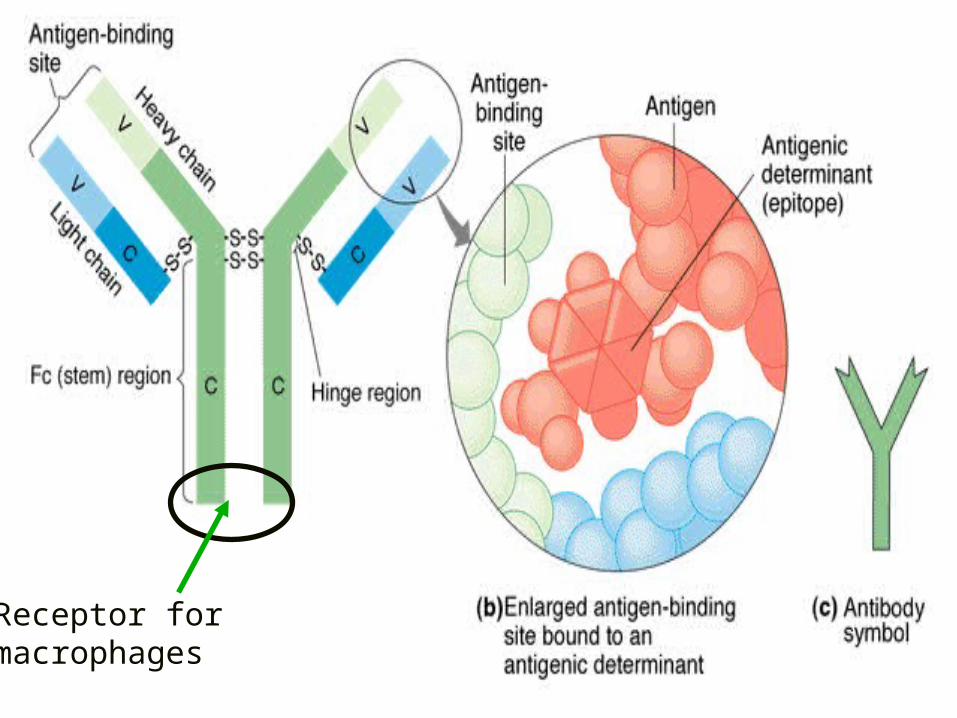
Receptor formacrophages
CLASSES OF IMMUNOGLOBULINS
• IgG• IgM• IgA• IgD• IgE
IMMUNOGLOBULIN G (IgG)
–80% of all Igs
–Cross blood vessels and enter tissue fluids
–Cross human placenta
IMMUNOGLOBULIN G (IgG) (cont.)
• Protects against circulating bacteria and viruses
• Neutralizes bacterial toxins• Trigger the complement
system• Facilitates phagocytosis
IMMUNOGLOBULIN M (IgM)
• 1st AB that appears in response to an AG—however their conc. declines rapidly–Used for diagnosis
• 5-10% of all Igs• Pentamer (5 “Y”s) joined by a j chain• Do not cross placenta b/c too big
IMMUNOGLOBULIN M (IgM) (cont.)
• Predominant AB in the blood typing process rx
• Hi IgM conc. Represents an active disease
• Aggregates antigens• Triggers the complement system• Facilitates phagocytosis• Antigen receptor of B cell
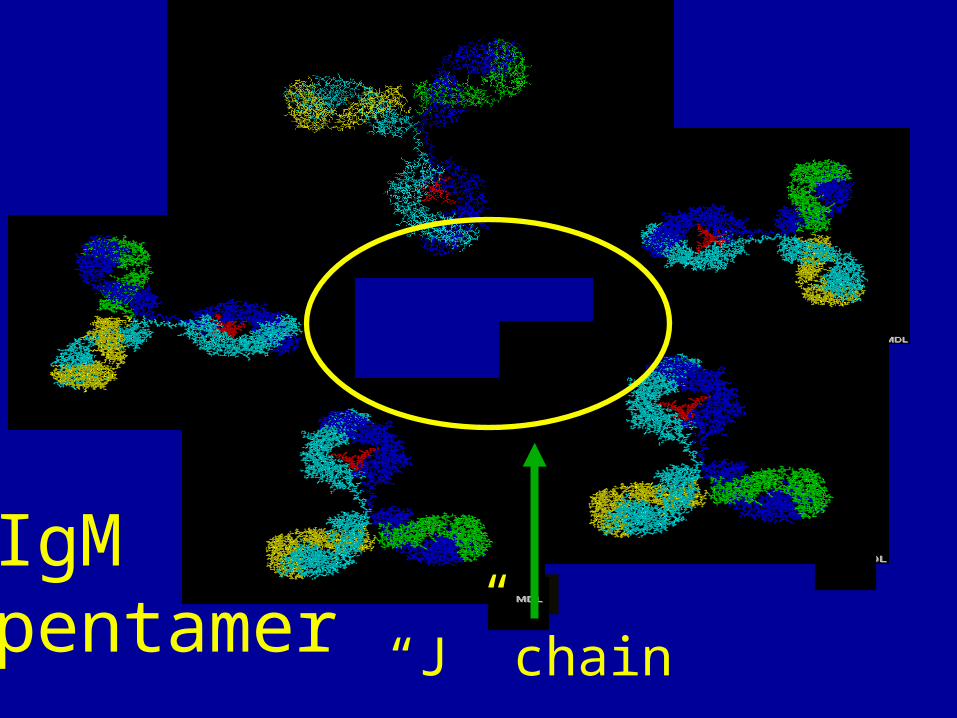
IgM pentamer “J” chain
IMMUNOGLOBULIN A (IgA)
• 10 - 15% of all Igs• Most common in mucous
membranes and body secretions–Mucus, saliva, tears and milk
IMMUNOGLOBULIN A (IgA) (cont.)
• Dimer (2 “Y”s) joined by a j chain
• Prevents attachment (adherence) of pathogens to mucosal surfaces
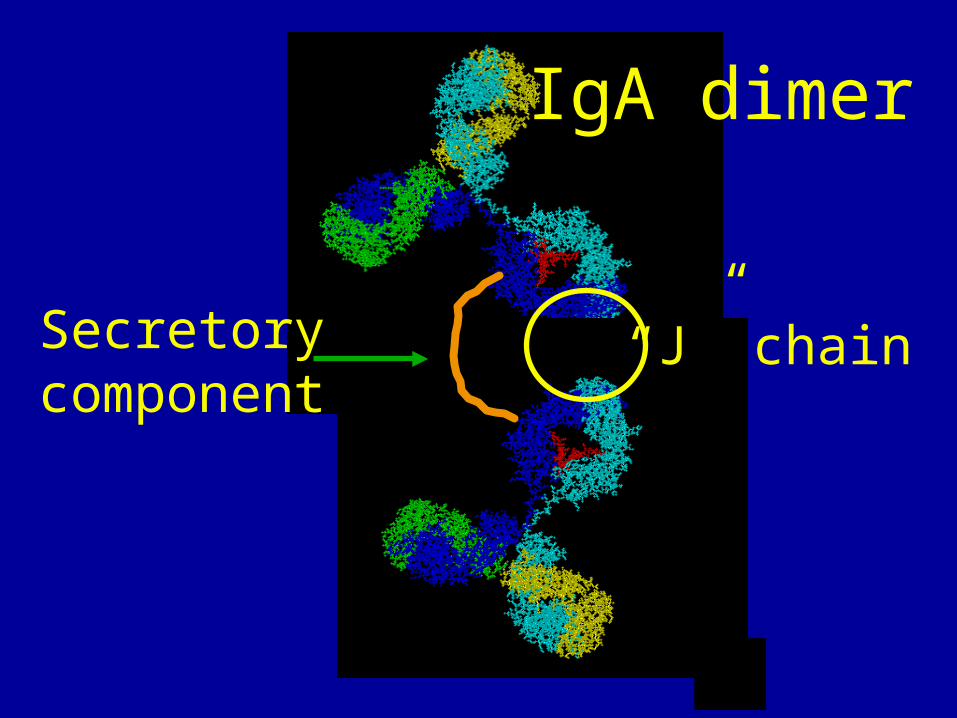
IgA dimer
“J” chainSecretorycomponent
IMMUNOGLOBULIN E (IgE)
• 0.002% of all Igs• Bind to mast cells and basophils
• Involved in allergies• Effective against parasitic worms
IMMUNOGLOBULIN D (IgD)
• Structurally similar to IgG
• Unknown function in serum
• Antigen receptor on B cell surfaces
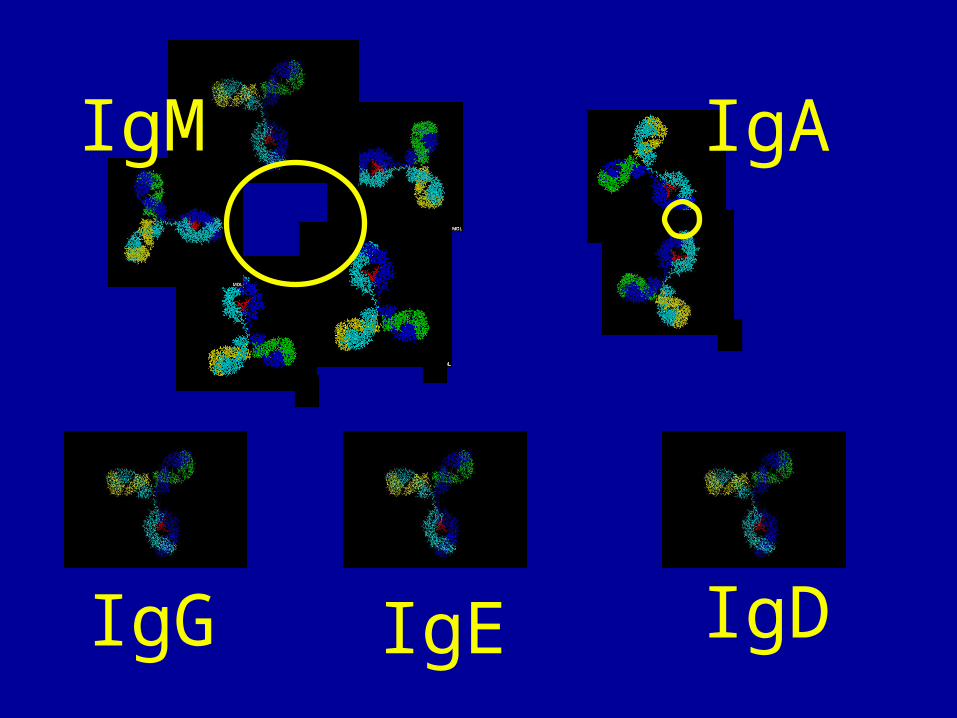
IgM IgA
IgG IgE IgD
ANTIGEN-ANTIBODY REACTION
• Neutralization–Viruses and toxins
• Agglutination (clumping of AG &AB so phagocytes can ingest them better)–Bacterial cells
• Precipitation–Soluble antigens
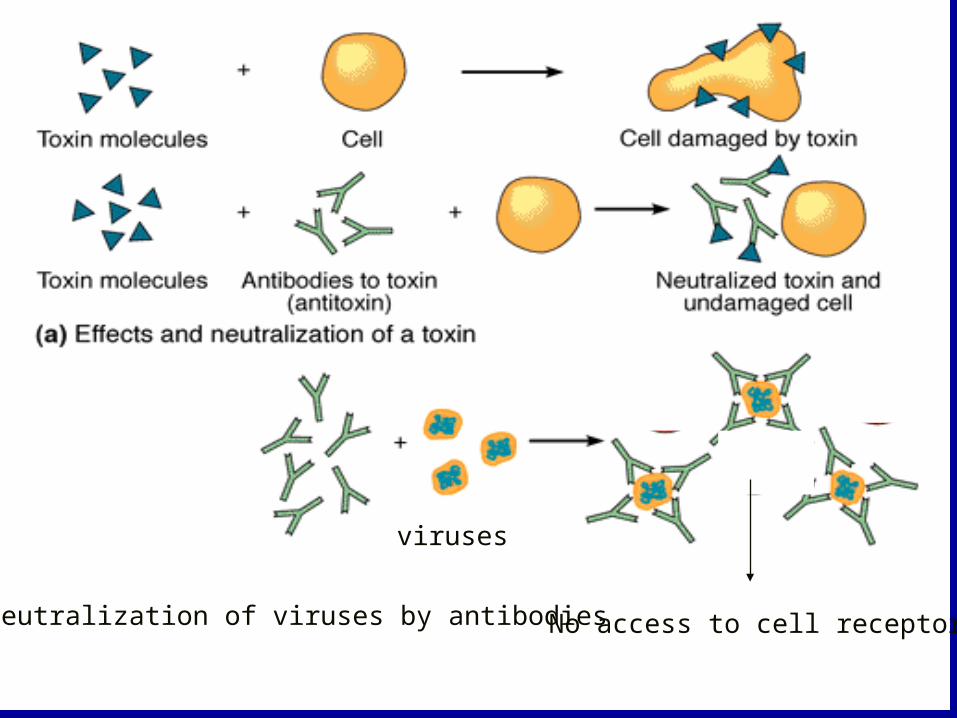
(b) Neutralization of viruses by antibodies
viruses
No access to cell receptors
IMMUNE SYSTEM
• Humoral or antibody-mediated–B lymphocytes
• Cell-mediated–T lymphocytes
B CELLS AND HUMORAL IMMUNITY• Stem cells in bone
marrow–Adults
• Liver–Fetuses
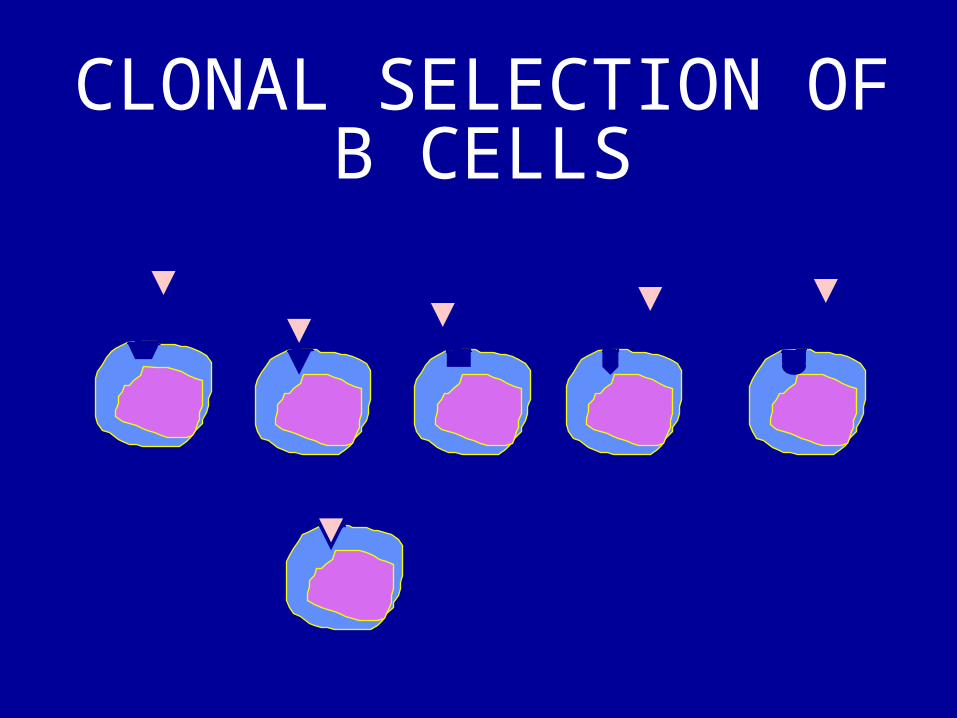
CLONAL SELECTION OF B CELLS
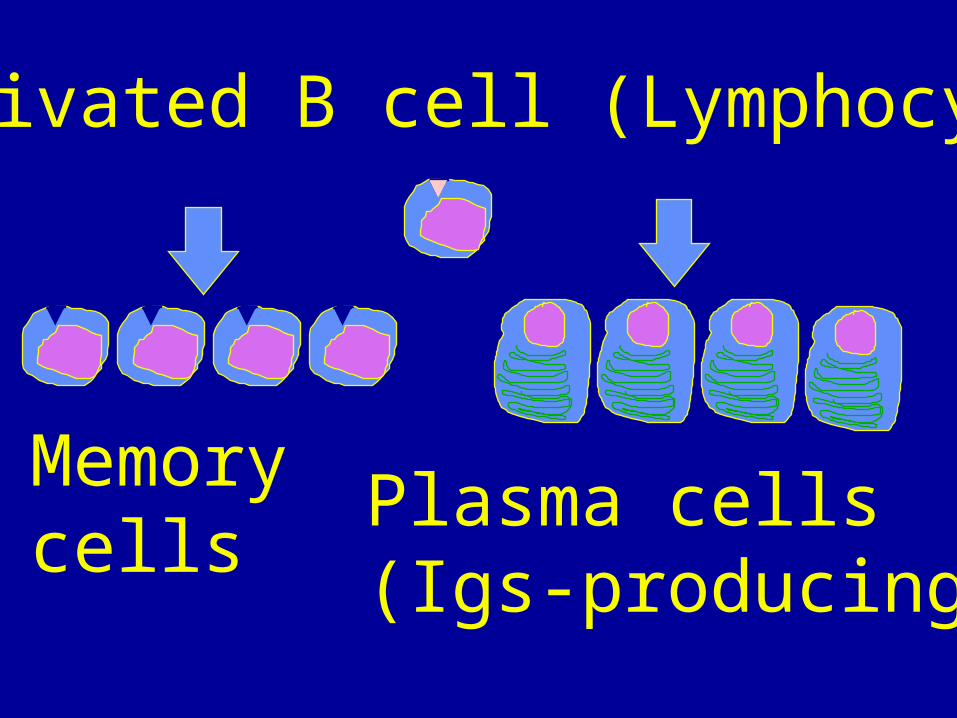
Activated B cell (Lymphocyte)
Memory cells
Plasma cells(Igs-producing)
CLONAL DELETION
• During fetal development, clones of lymphocytes that react with self antigens are eliminated (self-tolerance)
PLASMA CELLS
• Secrete antibodies (Igs) against specific antigens
• Short lived • Produce 2000 antibodies
per second
T-CELL MEDIATED IMMUNITY
• Derived from stem cells –Adults
•Bone marrow–Fetuses
•Liver
T-CELL MEDIATED IMMUNITY (cont.)
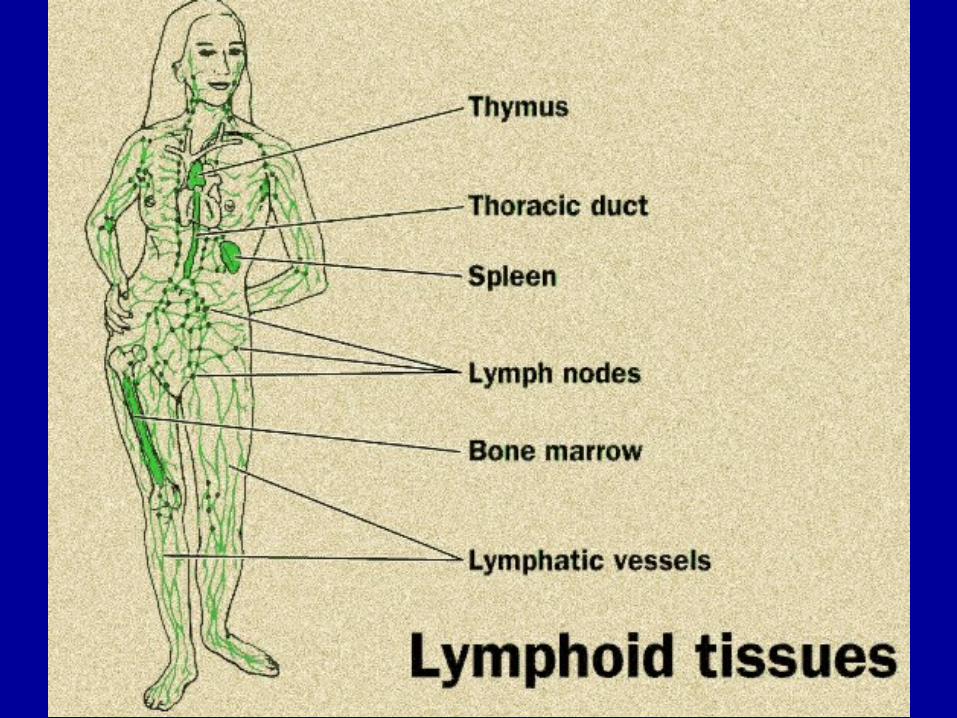
• Mature and differentiate in thymus
• Mature T cells migrate to lymphoid organs
T-CELL MEDIATED IMMUNITY (cont.)
• Clonal selection determines proliferation of T cells that carry out cell-mediated immunity
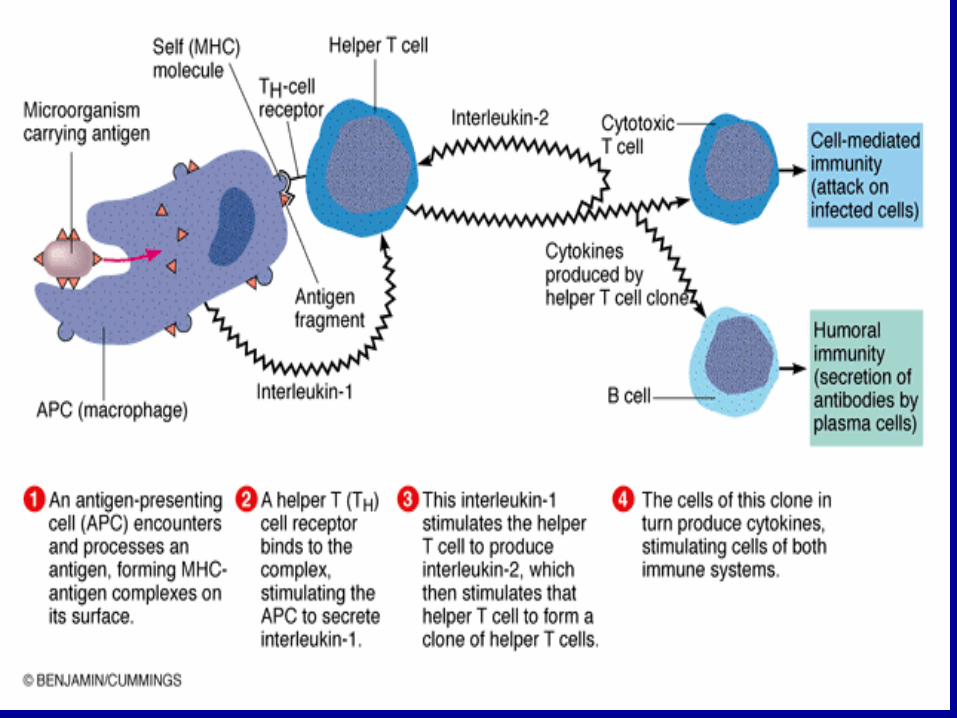
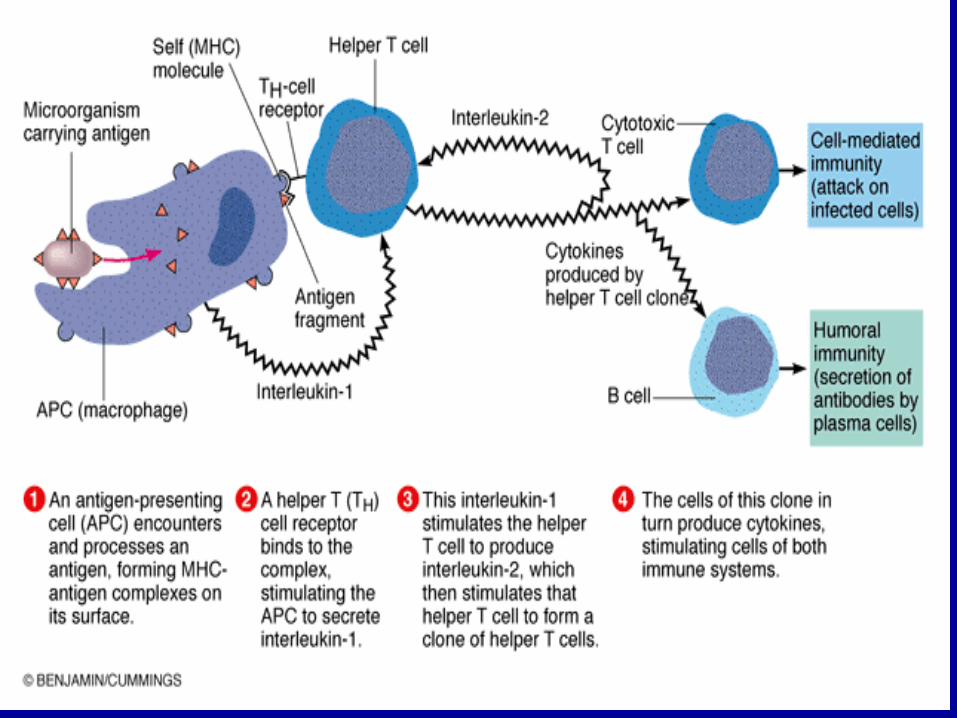
• Respond only to antigens presented by macrophages
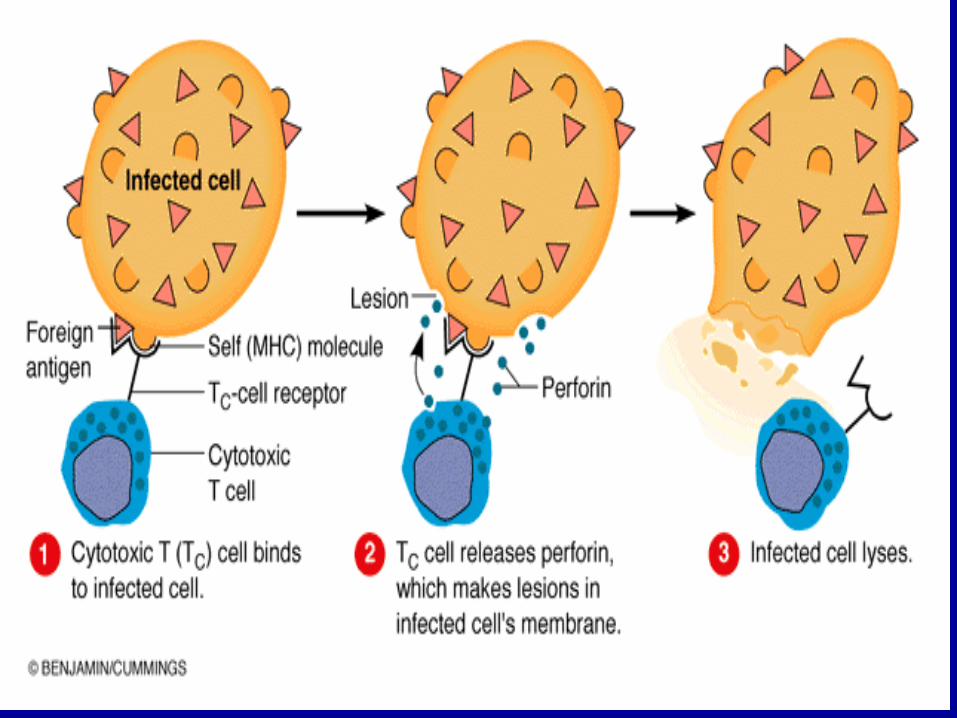
TYPES OF T CELLS
• Cytotoxic (TC) CD8
–Kill altered cells• Helper (TH) CD4
–Activate B, TH, and TC
cells
TYPES OF T CELLS (cont.)• Delayed Hypersensitivity (TD)
CD4 and CD8–Anti-cancer, allergies
• Suppressor (TS) CD4 and CD8– Suppress immune response
NATURAL KILLER (NK) CELLS
• Non-T lymphocytes• Not specific• Kill altered cells
CYTOKINES (INTERLEUKINS)
• Chemical messengers of the immune system–Interleukin-1
•Stimulates TH cells–Interleukin-2
•Proliferation of TH cells