Nonlinear Dynamic Analysis of the EEG in Patients.10

of 10
-
Upload
dvm22029719 -
Category
Documents
-
view
216 -
download
0
Transcript of Nonlinear Dynamic Analysis of the EEG in Patients.10
-
7/28/2019 Nonlinear Dynamic Analysis of the EEG in Patients.10
1/10
Nonlinear Dynamic Analysis of the EEG in Patients with
Alzheimers Disease and Vascular Dementia
*Jaeseung Jeong, JeongHo Chae, Soo Yong Kim, and SeolHeui Han
*Department of Diagnostic Radiology, School of Medicine, Yale University, New Haven, Connecticut, U.S.A.; Department of
Psychiatry, College of Medicine, The Catholic University of Korea, Seoul, Korea; Department of Physics, Korea Advanced
Institute of Science and Technology, Taejon, Korea; andDepartment of Neurology, Chungbuk National University
Hospital, Korea
Summary: To assess nonlinear EEG activity in patients with Alzheimers disease(AD) and vascular dementia (VaD), the authors estimated the correlation dimension(D2) and the first positive Lyapunov exponent (L1) of the EEGs in both patients andage-matched healthy control subjects. EEGs were recorded in 15 electrodes from 12AD patients, 12 VaD patients, and 14 healthy subjects. The AD patients had signifi-cantly lower D2 values than the normal control subjects, (P H 0.05), except at theF7 and the O1 electrodes, and the VaD patients, except at the C3 and the C4 electrodes.The VaD patients had relatively increased values of D2 and L1 compared with the ADpatients, and rather higher values of D2 than the normal control subjects at the F7, F4,F8, Fp2, O1, and O2 electrodes. The L1 values of the EEGs were also lower for theAD patients than for the normal control subjects, except in the O1 and the O2 channels,and for the VaD patients at all electrodes. The L1 values were higher for the VaDpatients than for the normal control subjects (F3, F4, F8, O1, and O2). In addition, theauthors detected that the VaD patients had an uneven distribution of D2 values over theregions than the AD patients and the normal control subjects, although the statistics do
not confirm this. By contrast, AD patients had uniformly lower D2 values in mostregions, indicating that AD patients have less complex temporal characteristics of theEEG in entire regions. These nonlinear analyses of the EEG may be helpful inunderstanding the nonlinear EEG activity in AD and VaD. Key Words: AlzheimersdiseaseVascular dementiaEEGCorrelation dimensionLyapunov exponent.
Two of the most common kinds of dementia in the
elderly are Alzheimers disease (AD) and vascular de-
mentia (VaD). Although AD is a leading cause of de-
mentia in the Western world, VaD prevails in Asian
countries (Jorm, 1991; Kase, 1991). It is important todiagnose AD and VaD accurately, because this enables
the clinician to provide demented patients and their
families with a more reliable prediction of the diseases
course, and it facilitates planning for necessary social
resources. However, the differential diagnosis is compli-
cated by the fact that a co-occurrence of AD and stroke
is common. There have been substantial efforts to dif-
ferentiate AD from VaD using various diagnostic mo-
dalities, including neuropsychological tests (Bowler et
al., 1997; Sultzer et al., 1993; Swanwick et al., 1996),neuroimaging techniques (Mielke et al., 1994; OBrien et
al., 1997), quantitative EEG (Dunkin et al., 1994; Si-
gnorino et al., 1995; Szelies et al., 1994), and transcranial
Doppler sonography (Ries et al., 1993).
Quantitative EEG analyses have been used in attempts
at differential diagnosis in dementia studies. A higher
incidence of focal abnormalities in VaD has been ob-
served repeatedly (Erkinjuntti et al., 1988; Soininen et
al., 1982). Progressive deterioration of the background
Address correspondence and reprint requests to Dr. Jaeseung Jeong,P.O. Box 208042, 333 Cedar Street, Department of Diagnostic Radiology,School of Medicine, Yale University, New Haven, CT 06520.
Journal of Clinical Neurophysiology18(1):5867, Lippincott Williams & Wilkins, Inc., Philadelphia 2001 American Clinical Neurophysiology Society
58
-
7/28/2019 Nonlinear Dynamic Analysis of the EEG in Patients.10
2/10
rhythms and sequential changes in serial studies are usually
helpful in confirming the existence of a progressive degen-
erative dementia (Markand, 1984). Spectral analysis of the
EEG has shown an increased power of the lower frequency
bands and a decrease of high frequencies in AD patients
(Brenner et al., 1988; Coben et al., 1985, 1990; Hooijer etal., 1990; Penttil et al. 1985; SchreiterGasser et al., 1993;
Soininen et al., 1991). A positive linear relationship be-
tween slowing of the average EEG frequency and the
degree of cognitive impairment has been reported in AD
patients (Coben et al., 1985). Signorino et al. (1995, 1996a,
b) and others (Pucci et al., 1998) showed that EEG spectral
parameters can offer enough data to discriminate between
the subtypes of AD and VaD. EEG coherence studies
demonstrated that long-distance coherence seems to be
more affected than local coherence in AD patients, whereas
the opposite occurs in VaD patients (Comi et al., 1998;
Leuchter et al., 1992). In AD patients, local changes of
coherence of the band have been reported to affect
selectively the left temporoparietaloccipital areas
(Leuchter et al., 1992; Locatelli et al., 1998) or the anterior
areas (Besthorn et al., 1994).
Recent progress in the theory of nonlinear dynamics
has provided new methods for the study of time-series
data from human brain activities. Babloyantz et al.
(1985) first reported that EEG data from the human brain
had chaotic attractors for sleep stages II and IV. Much
research using nonlinear methods revealed that the EEG
is generated by a deterministic neural process (Babloy-
antz, 1988; Rapp et al., 1985; Rochke and Basar, 1988;
Soong and Stuart, 1989). According to these reports, theEEG has a finite correlation dimension (D2) and a
positive Lyapunov exponent (L1). Furthermore, distinct
states of brain activity produce different chaotic proper-
ties quantified by nonlinear invariant measures such as
D2 and L1 (Babloyantz, 1988; Babloyantz and Destexhe,
1987; Fell et al., 1993; Pijn et al., 1991; Rochke and
Aldenhoff, 1991; Wackermann et al., 1993).
By contrast, there is some evidence that an EEG is not
a chaotic signal of low dimension (Osborne and Proven-
zale, 1989; Palus, 1996; Pritchard et al., 1995; Rapp et
al., 1993; Theiler and Rapp, 1996; Theiler et al., 1992).
Research has shown that the normal resting human EEGis nonlinear but does not represent low-dimensional
chaos, and it may be generated from 1/f-like linear
stochastic systems. Our previous study also failed to
detect any determinism in the EEG with the smoothness
method (Jeong et al., 1999).
Although no compelling evidence for a deterministic
nature of the EEG has been adduced, nonlinear dynamic
analyses of the EEG to estimate D2 and L1 have proved to
be useful in differentiating normal and pathologic brain
states (Rapp, 1993). Many studies using nonlinear methods
presented possible medications (Lehnertz and Elger, 1998)
for nonlinear analysis and the possibility that nonlinear
analysis of the EEG may be a useful tool in differentiating
physiologic brain states (Babloyantz and Destexhe, 1986,
1987; Fell et al., 1995; Frank et al., 1990; Jeong et al.,1998a, b; Kim et al., 2000; Lehnertz and Elger, 1998;
Pritchard et al., 1994).
There are several studies of the EEG in AD patients
using nonlinear methods. D2 and L1 from EEG data
were estimated (Besthorn et al., 1995; Jelles et al., 1999;
Jeong et al., 1998a; Pritchard et al., 1991, 1993, 1994;
Stam et al., 1995, 1996). Their results indicated that AD
patients had significantly lower values in D2 and L1 than
age-matched normal subjects, indicating that the dy-
namic processes underlying the EEG recording are less
complex for AD patients than for normal subjects.
The aim of the current study was to examine nonlinear
EEG activity in AD and VaD, and to compare the
nonlinear properties of the EEGs in AD and VaD. D2
and L1 were estimated from the EEGs with the optimal
embedding dimension. We regarded these nonlinear pa-
rameters as operationally defined measures of complex-
ity. They may not be appropriate measures for differen-
tiating between periodic, chaotic, or stochastic dynamics
in the formal sense. Because this study focuses on
comparing nonlinear EEG activity in AD and VaD, we
do not use the surrogate-data method to detect nonlin-
earity and determinism of the EEG.
METHODS
One-dimensional EEG data were transformed into
multidimensional phase space. The concept of phase
space is central to the analysis of nonlinear dynamics. In
a hypothetical system governed by n variables, the phase
space is n-dimensional. Each state of the system corre-
sponds to a point in phase space with n coordinates that
are the values assumed by the governing variables for
this specific state. If the system is observed for a period
of time, the sequence of points in phase space forms a
trajectory. This trajectory fills a subspace of the phase
space, called the systems attractor.Reconstruction of the attractor in phase space was
carried out through the technique of delay coordinates.
To unfold the projection back to a multivariate state
space that is a representation of the original system, we
use the delay coordinates y(t) [xj(t), xj(t T), . . . , xj(t [d 1]T)] from a single time series xj and perform
an embedding procedure, where y(t) is one point of the
trajectory in the phase space at time t, x(t iT) are the
coordinates in the phase space corresponding to the
59NONLINEAR DYNAMIC ANALYSIS OF EEG IN AD AND VAD
J Clin Neurophysiol, Vol. 18, No. 1, 2001
-
7/28/2019 Nonlinear Dynamic Analysis of the EEG in Patients.10
3/10
time-delayed values of the time series, T is the time delay
between the points of the time series considered, and dis
the embedding dimension (Eckmann and Ruelle, 1985;
Takens, 1981).
The choice of an appropriate time delay T and embed-
ding dimension d are important to the success of recon-
struction with finite data. For the time delay T, we used the
first local minimum of the average mutual information
between the set of measurements v(t) and v(t T) in the
current study. Mutual information measures the general
dependence of two variables (Fraser and Swinney, 1986).We used the minimum (optimal) embedding dimension
in the reconstruction procedure (Kennel et al., 1992). The
algorithm is based on the idea that in the passage from
dimension d to dimension d 1, one can differentiate
between points on the orbit that are true neighbors and those
that are false. A false neighbor is a point in the dataset that
is a neighbor solely because we are viewing the orbit (the
attractor) in too small an embedding space (d dmin).
When we have achieved a large enough embedding space
(d dmin), all neighbors of every orbit point in the multi-
variate phase space will be true neighbors.
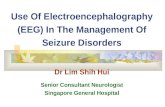
We defined the embedding rate as the ratio of trueneighbors to neighbors in the embedding dimension.
Figure 1 shows a typical example of the embedding rate
as a function of the embedding dimension for 16,384
EEG data points in a normal control subject. The proper
minimum embedding dimension was selected as 11 in
this case. The detailed algorithm was reported in our
previous paper (Jeong et al., 1998a). We also showed the
increase in the efficiency and accuracy of our method
relative to the old one.
One of the important mathematical quantities charac-
terizing an attractor is its correlation dimension (D2),
which is a metric property of the attractor that estimates
the degree of freedom. It determines the number of
independent variables that are necessary to describe the
dynamics of the original system. For instance, in the case
of steady-state behavior, D2 of the attractor is zero and
D2 of the periodic attractor is one. In chaotic states, D2
usually takes on noninteger values. The larger the D2
value of the attractor, the more complicated the behavior
of the nonlinear system. D2 is thus a measure of thecomplexity of the process being investigated, and it
characterizes the distribution of points in phase space
(Hornero et al., 1999).
We evaluate the D2 values of the attractors from the
EEG using the GrassbergerProcaccia algorithm (Grass-
berger and Procaccia, 1983). With this algorithm, D2 is
based on determining the relative number of pairs of
points in the phase-space set that are separated by a
distance less than r. It is computed from the following
D2 limr3O
limN3
log C(r, N)
log r
(1)
where the correlation integral C(N, r) is defined by the
C(r)1
N2 i,j1ij
N
(r x3
i x3
j ) (2)
where xi and xj are the points of the trajectory in the
phase space, N is the number of data points in the phase
space, the distance r is a radius around each reference
FIG. 1. The embedding rate as afunction of embedding dimension for16,384 EEG data points at T4 in anormal control subject. The optimalminimum embedding dimension forcalculating D2 and L1 was 11 in thiscase.
60 J. JEONG ET AL.
J Clin Neurophysiol, Vol. 18, No. 1, 2001
-
7/28/2019 Nonlinear Dynamic Analysis of the EEG in Patients.10
4/10
-
7/28/2019 Nonlinear Dynamic Analysis of the EEG in Patients.10
5/10
dynamics. This more detailed algorithm is also reported
in a previous paper (Jeong et al., 1998a).
A consecutive series of patients with AD and VaD
who attended the Department of Neurology, Chungbuk
National University Hospital, Korea, were screened for
inclusion in this study. All patients had undergone athorough clinical evaluation that included clinical his-
tory, physical and neurologic examinations, routine lab-
oratory tests, electrocardiogram, EEG, and brain MRI.
Twelve AD patients (four men and eight women;
mean age, 68.7 5.1 years) met the criteria for AD as
mandated in the Diagnostic and Statistical Manual of
Mental Disorders, 4th edition (American Psychiatric
Association, 1994), and probable AD established by the
National Institute of Neurologic Disorders and Stroke
Association and Alzheimers Disease and Related Dis-
orders Association (McKhann et al., 1984). The probable
AD patients had a Mini-Mental State ExaminationKo-
rean version (MMSE-K) score (Kwon and Park, 1989) of
less than 12 points (mean MMSE-K score, 9.2 3.5
points), indicating a severe degree of dementia. The
average age at onset of dementia was approximately 64.9
3.1 years, and the average length of illness was
approximately 46.0 7.3 months.
Twelve VaD patients (four men and eight women;
mean age, 67.9 4.9 years) met the National Institute of
Neurologic Disorders and Stroke AssociationInternatio-
nale pour la Recherche et lEnseignement en Neuro-
sciences criteria (Roman et al., 1993). The patients with
VaD also had MMSE-K scores less than 12 points (mean
MMSE-K score, 9.9 4.2 points). Additionally, theyeither had experienced the onset of cognitive impairment
after a clinical stroke or had shown clear focal neurologic
signs on examination. They had a Hachinski ischemic
score of more than 7 points. MRI revealed large-vessel
stroke, multiple subcortical lacunar infarcts, and/or ex-
tensive white matter lesions in each VaD patient. Al-
though it is impossible to be certain that no patients had
coexisting AD and VaD, patients with evidence of both
disorders were excluded.
Fourteen age-matched, healthy, elderly control sub-
jects (five men and nine women; mean age, 66.9 5.0
years) were recruited from a senior community club inTaejon, South Korea. The control subjects had a mean
score of 27.1 0.7 points on the MMSE-K.
All subjects were excluded from each group if there
was a history of psychotic disorder unrelated to demen-
tia, a history of head trauma with loss of consciousness,
a psychoactive substance use disorder, a systemic illness,
or other neurologic illness that could account for the
cognitive impairment. The local ethics committee ap-
proved the study. All subjects and all caregivers of the
demented patients gave informed consent for participa-
tion in the current study.
EEGs were recorded from the 15 scalp loci of the
International 1020 System. The EEG reading from the
T5 channel was not recorded because of a hardware
problem. With the subjects in a relaxed state with theireyes closed, 32,768 seconds of data (16,384 data points)
were recorded with a sampling frequency of 500 Hz,
digitized by a 12-bit analogdigital converter in an IBM
personal computer. Recordings were made under the
eyes-closed condition to obtain as many stationary EEG
data as possible. Potentials from 15 electrodes (F7, T3,
Fp1, F3, C3, P3, O1, F8, T4, T6, Fp2, F4, C4, P4, and
O2) against linked earlobes were amplified on a Nihon
Kohden EEG-4421K using a time constant of 0.1 second.
All data were filtered digitally to remove residual elec-
tromyographic activity at 1 to 35 Hz. Each EEG record
was judged by inspection to be free from electro-oculo-
graphic and movement artifacts, and to contain minimal
electromyographic activity.
All analyses were carried out using the Statistical
Package for the Social Sciences (SPSS version 7.0;
SPSS, Inc., Cary, NC USA) for Windows. One-way of
analyses of variance (SPSS General Linear Models mod-
ule) were used to test group-specific effect. If significant
effects between groups were found, the effects were
analyzed additionally using Duncans post hoc test. The
results of group data are expressed as mean standard
deviation. A two-tailed probability of less than 0.05 was
considered to be significant.
RESULTS
During the reconstruction procedure, time delays of 34
to 50 msec and embedding dimensions of 11 to 18 were
used for the AD patients, and time delays of 26 to 46
msec and embedding dimensions of 13 to 19 were used
for the VaD patients. The normal control subjects had
time delays of 28 to 34 msec and embedding dimensions
of 11 to 19.
The average D2 values and standard deviations for the
AD patients, VaD patients, and normal control subjects
for the 15 electrodes identified earlier are summarized inTable 1, which shows that each group had distinctly
different D2 values in all electrodes. The AD patients
had significantly lower D2 values than the normal sub-
jects except at the F7 and O1 electrodes, and lower than
the VaD patients except at the C3 and C4 electrodes. The
differences between the D2 values in the F4, F8, Fp1,
Fp2, O1, and O2 channels were approximately 1.5 to 2.2
U. The VaD patients had significantly higher D2 values
than the normal control subjects in six channels (F7, F4,
62 J. JEONG ET AL.
J Clin Neurophysiol, Vol. 18, No. 1, 2001
-
7/28/2019 Nonlinear Dynamic Analysis of the EEG in Patients.10
6/10
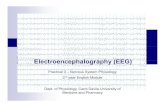
F8, Fp2, O1, and O2). In addition, the VaD patients had
a less uniform distribution of D2 values over the regions
than the AD patients and the normal control subjects,
although statistics do not confirm this (Fig. 3).
Another nonlinear measure, L1, was calculated for all
subjects at all electrodes. The evolving time was selected
using the 1/e spectral frequency, and was approximately180 to 240 msec. The calculation of L1 depended on the
time over which the trajectory was evaluated. After 200
propagation steps, the values converged in an interval of
0.92% around the final value of L1.
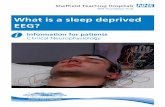
The average L1 values and standard deviations for all
subjects at all electrodes are summarized in Table 2. It
shows that the average L1 values were higher for the
normal control subjects than for the AD patients (F7, T3,
Fp1, P3, F8, T4, T6, Fp2, C4, P4, P 0.01; F3, C3, F4,
P 0.01), just as the D2s were. The L1s of the AD
patients in channels O1 and O2 were not significantly
different from those of the normal control subjects.
The differences between the values of L1 in the F7,
T3, Fp1, P3, F8, T4, T6, Fp2, C4, and P4 channels
were very significantapproximately 1.0 to 1.8 U.
The results for L1 were consistent with those for D2,
except in the F7 and O2 channels. AD patients had
significantly lower L1 values than VaD patients (P
0.001) in all channels. The L1 values for the VaD
patients were higher than for the normal control sub-
jects (F3, F4, F8, O1, O2, P 0.01).
DISCUSSION
Our results indicate that AD patients have signifi-
cantly lower D2 and L1 values than VaD patients and the
age-matched healthy control subjects over all regions
except at a few electrodes. By contrast, VaD patients
have relatively higher D2 and L1 values than AD pa-
tients. VaD patients have an uneven distribution of D2
values over the channels than other groups, whereas AD
patients have uniformly lower values of D2 and L1,
indicating that EEGs in AD patients are less complex
than those in other groups.
Our findings of a decreased dimensional complexity
and flexibility of EEGs in AD patients supports a number
of previous findings (Besthorn et al., 1995; Jelles et al.,
1999; Pritchard et al., 1991, 1993, 1994; Pucci et al.,
1998; Stam et al., 1995; Woyshville and Calabrese,
1994; Woyshville et al., 1987; Yagyu et al., 1997). If
dynamic properties of the EEG reflect differential infor-
mation processing in the brain, the states of information
processing could be estimated by nonlinear measures
(Rochke, 1992). Lutzenberger et al. (1992) demon-
strated that human intellectual ability may be reflected
in a higher complexity of the electrical dynamics of
the brain. Accordingly, we may interpret our results to
mean that a decrease of D2 and L1 in AD may be
associated with deficient information processing in the
brain injured by AD.
TABLE 1. The average estimates of D2 in patients with AD and VaD and normal subjects
Leadposition
AD patients(n 12)
VaD patients(n 12)
Normal control subjects(n 14)
Analysis
F value(df 2, 35) P value
F7 8.90 0.35 10.32 0.38 9.13 0.46 6.21 0.01F3* 8.92 0.58 10.29 0.54 10.09 0.65 5.23 0.05F4* 8.71 0.42 11.03 0.43 9.67 0.37 6.96 0.01F8* 8.27 0.55 10.79 0.48 8.82 0.44 5.29 0.01Fp1* 8.41 0.52 10.21 0.38 9.57 0.46 6.86 0.01Fp2* 8.03 0.43 10.25 0.49 9.25 0.41 6.74 0.01C3* 9.06 0.55 9.67 0.48 9.97 0.36 4.98 0.05C4* 8.62 0.63 9.14 0.55 9.85 0.53 5.02 0.05T3* 8.40 0.38 9.56 0.51 9.75 0.32 5.46 0.01T4* 8.25 0.35 9.21 0.48 9.38 0.45 5.26 0.05T6* 8.09 0.39 9.89 0.49 9.54 0.48 6.12 0.01P3* 9.01 0.52 10.12 0.47 9.94 0.39 6.81 0.01P4* 8.63 0.48 9.54 0.46 9.67 0.28 5.47 0.01O1 8.16 0.33 10.24 0.41 8.25 0.45 5.54 0.01O2* 8.15 0.39 10.89 0.49 8.77 0.46 6.21 0.01
* AD control (P 0.05, analysis of variance [ANOVA] with posthoc Duncan). AD VaD (P 0.05, ANOVA with posthoc Duncan). Control VaD (P 0.05, ANOVA with posthoc Duncan).AD, Alzheimers disease; VaD, vascular dementia.
63NONLINEAR DYNAMIC ANALYSIS OF EEG IN AD AND VAD
J Clin Neurophysiol, Vol. 18, No. 1, 2001
-
7/28/2019 Nonlinear Dynamic Analysis of the EEG in Patients.10
7/10
FIG. 4. Graphical representation of the mean L1 values in patients with(A) (AD) and (B) VaD, and in (C) normal subjects.
FIG. 3. Graphical representation of the mean D2 values in patients with(A) Alzheimers disease (AD) and (B) vascular dementia (VaD), and(C) in normal subjects.
64 J. JEONG ET AL.
J Clin Neurophysiol, Vol. 18, No. 1, 2001
-
7/28/2019 Nonlinear Dynamic Analysis of the EEG in Patients.10
8/10
The finding that VaD patients have relatively higher
values of D2 and L1 than AD patients and even normal
control subjects, and have an uneven distribution of D2
values, may be in accord with previous findings (Johan-
nesson et al., 1979; Saletu et al., 1991). Saletu et al.
(1991) demonstrated the uneven distribution of EEG
abnormality in multi-infarct dementia by multichannel
EEG mapping. In mild cerebrovascular dementia, the
EEG was often normal or slightly abnormal (Johannes-son et al., 1979).
An uneven distribution of D2 values in VaD compared
with those in AD may be the result of uneven neuronal
pathology in VaD. VaD is a heterogeneous syndrome
with various subtypes, including multi-infarct dementia,
strategic single infarct dementia, small-vessel disease
with dementia, hypoperfusion, and hemorrhagic demen-
tia (Roman et al., 1993). VaD may exhibit cortical and/or
subcortical involvement (Weiner et al., 1991). Several
lines of studies using topographic EEG analysis showed
the VaD group had more asymmetric findings than the
AD group (Ding, 1990). Diffuse abnormality of EEGwas found to increase in AD (Erkinjuntti et al., 1988).
Conversely, clinical studies have linked signs and symp-
toms of VaD to patchy and irregular brain damage.
Radiologic studies showed that VaD patients had central
brain atrophy more often than AD patients or normal
control subjects, indicating multiple small infarcts in the
thalamus and other basal brain structures (Cumming and
Beson, 1992). Fenton (1986) showed that VaD patients
had the lowest coherence between the different cortical
areas, indicating asymmetry of functioning, whereas pa-
tients with non-VaD had the greatest EEG coherence
between the centroparietal and temporal regions within
each hemisphere. The current study suggested that the
distributions of lesions were more scattered in VaD than
in AD. Therefore, an uneven distribution in the nonlinear
measures in VaD patients may, to some extent, result
from underlying etiologic heterogeneity.
Similar disturbances in electrical activity may becaused by a variety of disease processes involving either
damage to nerve cells or potentially reversible distur-
bances in cell metabolism resulting from metabolic in-
sults. Hence, electrical patterns associated with brain
dysfunction cannot be used to predict the exact nature of
the underlying disease process (Fenton, 1986). Our re-
sults from the nonlinear analysis of the EEG suggest that
the estimation of nonlinear measures like D2 and L1 may
be helpful in diagnosing AD and VaD more accurately.
Pritchard et al. (1994) found that the addition of nonlin-
ear EEG measures improved the classification accuracy
of the subjects as either AD patients or control subjects.Several limitations of these findings merit consider-
ation. The sample size was small, and the severity of
cognitive dysfunction was not strictly controlled. The
results obtained seem to depend on the clinical degree of
dementia studied. The stage of dementia must affect the
ability of the EEG to distinguish one type of dementia
from the other or from control subjects. The relationship
of EEG alterations to the severity of dementia raises an
issue concerning the strict psychometric or neuropsycho-
TABLE 2. The average estimates of the L1 in patients with AD and VaD and normal subjects
Leadposition
AD patients(n 12)
VaD patients(n 12)
Normal control subjects(n 14)
Analysis
F value(df 2, 35) P value
F7* 4.92 0.22 5.45 0.28 5.32 0.23 5.58 0.01F3* 4.72 0.34 5.54 0.23 5.17 0.22 6.23 0.05F4* 4.93 0.31 5.78 0.25 5.34 0.24 6.36 0.01F8* 4.75 0.21 5.63 0.27 5.12 0.23 6.42 0.01Fp1* 4.94 0.20 5.51 0.35 5.47 0.27 5.26 0.05Fp2* 5.09 0.21 5.47 0.29 5.56 0.20 6.74 0.01C3* 5.24 0.30 5.57 0.36 5.62 0.23 5.25 0.05C4* 4.93 0.21 5.47 0.31 5.53 0.24 5.01 0.05T3* 4.56 0.15 5.31 0.22 5.69 0.29 5.76 0.01T4* 4.71 0.19 5.39 0.28 5.67 0.29 5.72 0.05T6* 4.46 0.21 5.24 0.36 5.41 0.22 6.17 0.01P3* 5.00 0.21 5.45 0.30 5.50 0.21 5.11 0.05P4* 5.22 0.20 5.78 0.34 5.80 0.27 5.17 0.05O1 4.76 0.22 5.73 0.36 4.93 0.17 5.74 0.01O2 4.90 0.13 5.74 0.29 4.91 0.15 5.10 0.05
* AD control (P 0.05, analysis of variance [ANOVA] with posthoc Duncan). AD VaD (P 0.05, ANOVA with posthoc Duncan). Control VaD (P 0.05, ANOVA with posthoc Duncan).AD, Alzheimers disease; VaD, vascular dementia.
65NONLINEAR DYNAMIC ANALYSIS OF EEG IN AD AND VAD
J Clin Neurophysiol, Vol. 18, No. 1, 2001
-
7/28/2019 Nonlinear Dynamic Analysis of the EEG in Patients.10
9/10
logical evaluation in the nonlinear analysis of EEG.
Additionally, we cannot explain why the VaD patients
had higher D2 and L1 values in some channels than
normal subjects. Our results, however, encourage further
investigation of the complexity of electrocortical re-
sponses in brains injured by dementia, although thecurrent study is quite preliminary.
REFERENCES
American Psychiatric Association. Diagnostic and statistical manual ofmental disorders. 4th ed. Washington, DC: American PsychiatricPress, 1994.
Babloyantz A. Chaotic dynamics in brain activity. In: Basar E, ed.Dynamics of sensory and cognitive processing by the brain.Berlin: Springer, 1988:196202.
Babloyantz A, Destexhe A. The CreutzfeldtJacob disease in thehierarchy of chaotic attractor. In: Markus M, Muller S, Nicolis G,eds. From chemical to biological organization. Berlin: Springer,
1987:30716.Babloyantz A, Destexhe A. Low dimensional chaos in an instance ofepilepsy. Proc Natl Acad Sci U S A 1986;83:35157.
Babloyantz A, Salazar JM, Nicolls C. Evidence of chaotic dynamics ofbrain activity during the sleep cycle. Phys Lett A 1985;111:152 6.
Besthorn C, Frstl H, GeigerKabisch C, Sattel H, Gasser T, SchreiterGasser U. EEG coherence in Alzheimer disease. Electroencepha-logr Clin Neurophysiol 1994;90:2425.
Besthorn C, Sattel H, GeigerKabisch C, Zerfass R, Forstl H. Param-eters of EEG dimensional complexity in Alzheimers disease.
Electroencephalogr Clin Neurophysiol 1995;95:849.Bowler JV, Eliasziw M, Steenhuis R, et al. Comparative evolution of
Alzheimers disease, vascular dementia, and mixed dementia.Arch Neurol 1997;54:697703.
Brenner RP, Reynolds CF, Ulrich RF. Diagnostic efficacy of comput-erized spectral versus visual EEG analysis in elderly normal,demented and depressed subjects. Electroencephalogr Clin Neu-
rophysiol 1988;69:1107.Coben LA, Chi D, Snyder AZ, Storandt M. Replication of a study of
frequency analysis of the resting awake EEG in mild probableAlzheimers disease. Electroencephalogr Clin Neurophysiol1990;75:148 54.
Coben LA, Danziger W, Storandt M. A longitudinal EEG study of mildsenile dementia of Alzheimer type: changes at 1 year and at 2.5year. Electroencephalogr Clin Neurophysiol 1985;61:10112.
Comi GC, Fornara C, Locatelli T, et al. EEG coherence in Alzheimerand multi-infarct dementia. Arch Gerontol Geriatr 1998;6(suppl6):918.
Cummings JL, Benson DF. Dementia: a clinical approach. Stoneham,MA: ButterworthHeinemann, 1992:15376.
Ding M. EEG topographic study of Alzheimers disease and multi-infarction dementia. Chin Med J (Engl) 1990;70:4347.
Dunkin JJ, Leuchter AF, Newton TF, Cook IA. Reduced EEG coher-
ence in dementia: state or trait marker? Biol Psychiatry 1994;35:8709.Eckmann JP, Ruelle D. Ergodic theory of chaos and strange attractors.
Rev Mod Phys 1985;57:61756.Erkinjuntti T, Larsen T, Sulkava R, Ketonen L, Laaksonen R, Palo J.
EEG in differential diagnosis between Alzheimers disease andvascular dementia. Acta Neurol Scand 1988;77:3643.
Fell J, Rochke J, Beckmann P. Nonlinear analysis of sleep EEG data inschizophrenia: calculation of the principal Lyapunov exponent.Psychiatry Res 1995;56:25769.
Fell J, Rochke J, Beckmann P. The calculation of the first positiveLyapunov exponent in sleep EEG data. Electroencephalogr Clin
Neurophysiol 1993;86:34852.
Fenton GW. Electrophysiology of Alzheimers disease. Br Med Bull1986;42:2933.
Frank GW, Lookman T, Nerenberg MAH, Essex C. Chaotic time seriesanalysis of epileptic seizures. Physica D 1990;46:42738.
Fraser AM, Swinney HL. Independent coordinates for strange attrac-tors from mutual information. Phys Rev A 1986;33:113440.
Grassberger P, Procaccia I. Measuring the strangeness of strange
attractors. Physica D 1983;9:189208.Hooijer C, Jonker C, Posthuma J, Visser SL. Reliability, validity and
follow-up of the EEG in senile dementia: sequelae of sequentialmeasurement. Electroencephalogr Clin Neurophysiol 1990;76:40012.
Hornero R, Alonso A, Jimero N, Jimero A, Lopez M. Nonlinearanalysis of time series generated by schizophrenic patients. IEEE
Eng Med Biol 1999;18:8490.Jelles B, van Birgelen JH, Slaets JPJ, Hekster REM, Jonkman EJ, Stam
CJ. Decrease of nonlinear structure in the EEG of Alzheimerspatients compared to healthy control subjects. Clin Neurophysiol1999;110:115967.
Jeong J, Joung MK, Kim SY. Quantification of emotion by nonlinearanalysis of the chaotic dynamics of EEGs during perception of 1/fmusic. Biol Cybern 1998a;78:21725.
Jeong J, Kim SY, Han SH. Nonlinear analysis of chaotic dynamicsunderlying EEGs in patients with Alzheimers disease. Electro-encephalogr Clin Neurophysiol 1998b;106:2208.
Jeong J, Kim M, Kim SY. Detecting low-dimensional determinism inelectroencephalogram. Phys Rev E 1999;60:8317.
Johannesson G, Hagberg B, Gustafson L, Ingvar D. EEG and cognitiveimpairment in presenile dementia. Acta Neurol Scand 1979;59:22540.
Jorm AF. Cross-national comparisons of the occurrence of Alzheimersand vascular dementia. Eur Arch Psychiatry Clin Neurosci 1991;240:21822.
Kase CS. Epidemiology of multi-infarct dementia. Alzheimer Dis AssocDisord 1991;5:716.
Kennel MB, Brown R, Abarbanel HDI. Determining embedding di-mension for phase-space reconstruction using a geometrical con-struction. Phys Rev A 1992;45:340311.
Kim DJ, Jeong J, Chae J-H, Kim SY, Go HJ, Paik H-I. The estimationof the first positive Lyapunov exponent of the EEG in patients
with schizophrenia. Psychiatry Res 2000;98:177 89.Kwon YC, Park JH. Korean version of Mini-Mental State Examination
(MMSE-K). Part I: development of the test for the elderly.J Korean Neuropsychiatry Assoc 1989;28:12535.
Lehnertz K, Elger C. Can epileptic seizures be predicted? Evidencefrom nonlinear time series analysis of brain electrical activity.Phys Rev Lett 1998;80:5019 22.
Leuchter AF, Newton TF, Cook IA, Walter DO, RosenbergThomsonS, Lachenbruch PA. Changes in brain functional connectivity inAlzheimer-type and multi-infarct dementia. Brain 1992;115:154361.
Locatelli T, Cursi M, Liberati D, Franceschi M, Comi G. EEG coher-ence in Alzheimers disease. Electroencephalogr Clin Neuro-
physiol 1998;106:22937.Lutzenberger W, Birbaumer N, Flor H, Rockstroh B, Elbert T. Dimen-
sional analysis of the human EEG and intelligence. Neurosci Lett
1992;143:104.Markand ON. Electroencephalography in diffuse encephalopathies.J Clin Neurophysiol 1984;1:357407.
McKhann G, Drachman D, Folstein M, Katzman R, Price D, StadlanEM. Clinical diagnosis of Alzheimers disease. Report of theNINDS-ADRDA Work Group under the auspices of Departmentof Health and Human Services Task Force on Alzheimers dis-ease. Neurology 1984;34:93944.
Mielke R, Pietrzyk U, Jacobs A, et al. HMPAO SPECT and FDG PETin Alzheimers disease and vascular dementia: comparison ofperfusion and metabolic pattern. Eur J Nucl Med 1994;21:105260.
OBrien JT, Desmond P, Ames D, Schweitzer I, Chiu E, Tress B.
66 J. JEONG ET AL.
J Clin Neurophysiol, Vol. 18, No. 1, 2001
-
7/28/2019 Nonlinear Dynamic Analysis of the EEG in Patients.10
10/10
Temporal lobe magnetic resonance imaging can differentiate Alz-heimers disease from normal ageing, depression, vascular demen-tia and other causes of cognitive impairment. Psychol Med 1997;27:126775.
Osborne AR, Provenzale A. Finite correlation dimension for stochasticsystems with power-law spectra. Physica D 1989;35:357 81.
Palus M. Nonlinearity in normal human EEG: cycles, temporal asym-
metry, nonstationarity and randomness, not chaos. Biol Cybern1996;75:389 96.
Penttil M, Partanen JV, Soininen H, Riekkinen PJ. Quantitativeanalysis of occipital EEG in different stages of Alzheimers dis-ease. Electroencephalogr Clin Neurophysiol 1985;60:16.
Pijn JP, Van Neerven J, Noest A, Lopes da Silva FH. Chaos or noisein EEG signals: dependence on state and brain site. Electroen-cephalogr Clin Neurophysiol 1991;79:37181.
Principe JC, Lo PC. Towards the determination of the largest Lyapunovexponent of EEG segments. In: Duke DW, Pritchard WS, eds.Proceedings of the Conference on Measuring Chaos in the Human
Brain. Singapore: World Scientific, 1991:15666.Pritchard WS, Duke DW, Coburn KL. Altered EEG dynamical respon-
sivity associated with normal aging and probable Alzheimersdisease. Dementia 1991;2:1025.
Pritchard WS, Duke DW, Coburn KL, Moore NC, Tucker KA. AlteredEEG dynamical responsivity associated with Alzheimers disease:replication and extension. In: Jansen BH, Brandt ME, eds. Pro-ceedings of the Second Annual Conference on Nonlinear Dynam-
ical Analysis of the EEG. Singapore: World Scientific, 1993:1658.
Pritchard WS, Duke DW, Coburn KL, et al. EEG-based, neural-netpredictive classification of Alzheimers disease versus controlsubjects is augmented by non-linear EEG measures. Electroen-cephalogr Clin Neurophysiol 1994;91:11830.
Pritchard WS, Duke DW, Krieble KK. Dimensional analysis of restinghuman EEG II: surrogate data testing indicates nonlinearity butnot low-dimensional chaos. Psychophysiology 1995;32:48691.
Pucci E, Cacchio G, Angeloni R, et al. EEG spectral analysis inAlzheimers disease and different degenerative dementias. ArchGerontol Geriatr 1998;26:28397.
Rapp PE. Chaos in the neurosciences: cautionary tales from thefrontier. Biologist 1993;40:8994.
Rapp PE, Albano AM, Schmah TI, Farwell LA. Filtered noise canmimic low-dimensional chaotic attractors. Phys Rev E 1993;47:228997.
Rapp PE, Zimmerman ID, Albano AM, deGuzman GC, GreenbaunNN, Bashore TR. Experimental studies of chaotic neural behavior:cellular activity and electroencephalographic signals. In: OthmerHG, ed. Nonlinear oscillations in biology and chemistry: lecturenotes in biomathematics. Berlin: SpringerVerlag, 1985:175205.
Ries F, Horn R, Hillekamp J, Honisch C, Konig M, Solymosi L.Differentiation of multi-infarct and Alzheimer dementia by intra-cranial hemodynamic parameters. Stroke 1993;24:228 35.
Rochke J. Strange attractors, chaotic behavior and informational as-pects of sleep EEG data. Neuropsychobiology 1992;25:172 6.
Rochke J, Aldenhoff J. The dimensionality of the humans electroen-cephalogram during sleep. Biol Cybern 1991;64:30713.
Rochke J, Basar E. The EEG is not a simple noise: strange attractors inintracranial structures. In: Basar E, ed. Dynamics of sensory andcognitive processing by the brain. Berlin: Springer, 1988:20316.
Roman GC, Tatemichi TK, Erkinjuntti T, et al. Vascular dementia:diagnostic criteria for research studiesreport of the NINDS-AIREN International Workshop. Neurology 1993;43:25060.
Saletu B, Anderer P, Paulus E. EEG brain mapping in diagnostic andtherapeutic assessment of dementia. Alzheimer Dis Assoc Disord1991;5:S5775.
SchreiterGasser U, Gasser T, Ziegler P. Quantitative EEG analysis inearly onset Alzheimers disease and control subjects. Electroen-cephalogr Clin Neurophysiol 1993;86:1522.
Signorino M, Brizioli E, Amadio L, Belardinelli N, Pucci E, Angeleri
F. An EEG power index (eyes open vs. eyes closed) to differen-
tiate Alzheimers from vascular dementia and healthy ageing.
Arch Gerontol Geriatr 1996a;22:24560.
Signorino M, Pucci E, Belardinelli N, Nolfe G, Angeleri F. EEG
spectral analysis in vascular and Alzheimer dementia. Electroen-
cephalogr Clin Neurophysiol 1995;94:31325.
Signorino M, Pucci E, Brizioli E, Cacchio G, Nolfe G, Angeleri F. EEGpower spectrum typical of vascular dementia in a subgroup of
Alzheimer patients. Arch Gerontol Geriatr 1996b;23:13951.
Soininen H, Partanen VJ, Helkala EL, Riekkinen PJ. EEG findings in
senile dementia and normal aging. Acta Neurol Scand 1982;65:
5970.
Soininen H, Partanen J, Laulumaa V, Helkala EL, Laakso M, Riekki-
nen PJ. Longitudinal EEG spectral analysis in early stage of
Alzheimers disease. Electroencephalogr Clin Neurophysiol 1991;
72:2907.
Soong ACK, Stuart CIJM. Evidence of chaotic dynamics underlying
the human alpha-rhythm electroencephalogram. Biol Cybern
1989;62:5562.
Stam CJ, Jelles B, Achtereekte HAM, Rombouts SARB, Slaets JPJ,
Keunen RWM. Investigation of EEG nonlinearity in dementia and
Parkinsons disease. Electroencephalogr Clin Neurophysiol 1995;
95:30917.Stam CJ, Jelles B, Achtereekte HAM, van Birgelen JH, Slaets JPJ.
Diagnostic usefulness of linear and nonlinear quantitative EEG
analysis in Alzheimers disease. Clin Electroencephalogr 1996;
27:6977.
Sultzer DL, Levin HS, Mahler ME, High WM, Cummings JL. A
comparison of psychiatric symptoms in vascular dementia and
Alzheimers disease. Am J Psychiatry 1993;150:1806 12.
Swanwick GR, Cohen RF, Lawlor BA, OMahony D, Walsh JB,
Coaklely D. Utility of ischemic scores in the differential diagnosis
of Alzheimers disease and ischemic vascular dementia. Int Psy-
chogeriatr 1996;8:41324.
Szelies B, Mielke R, Herholz K, Heiss WD. Quantitative topographical
EEG compared to FDG PET for classification of vascular and
degenerative dementia. Electroencephalogr Clin Neurophysiol
1994;91:1319.
Takens F. Detecting strange attractors in turbulence in dynamicalsystems and turbulence. Lecture Notes Math 1981;898:36681.
Theiler J, Eubank S, Longtin A, Galdrikian B, Farmer JD. Testing for
nonlinearity in times series: the method of surrogate data. Physica
D 1992;58:7794.
Theiler J, Rapp P. Re-examination of the evidence for low-dimen-
sional, nonstructure in the human electroencephalogram. Electro-
encephalogr Clin Neurophysiol 1996;98:21322.
Wackermann J, Lehmann D, Dvorak I, Michel CM. Global dimen-
sional complexity of multi-channels EEG indicates change of
human brain functional state after a single dose of a nootropic
drug. Electroencephalogr Clin Neurophysiol 1993;86:1938.
Weiner MF, Tintner RJ, Goodkin K. Differential diagnosis. In. Weiner
MF, ed. Dementia: diagnosis & management. Washington, DC:
American Psychiatric Press, 1991:77106.
Wolf A, Swift JB, Swinney HL, Vastano JA. Deterministic Lyapunov
exponents from a time series. Physica D 1985;16:285317.Woyshville MJ, Calabrese JR. Quantification of occipital EEG changes
in Alzheimers disease utilising a new metric: the fractal dimen-
sion. Biol Psychiatry 1994;35:3817.
Woyshville MJ, Zemlan F, Koellike D. The fractal dimension as a
quantifier of occipital EEG change in Alzheimers dementia. Clin
Res 1987;5:812.
Yagyu T, Wackermann J, Shigeta M, et al. Global dimensional com-
plexity of multichannel EEG in mild Alzheimers disease and
age-matched control subjects. Dementia 1997;8:3437.
67NONLINEAR DYNAMIC ANALYSIS OF EEG IN AD AND VAD
J Clin Neurophysiol, Vol. 18, No. 1, 2001