
Noninferiority Trials Presentation
20
Noninferiority Trials An Overview Hollie Sturgeon, PharmD
Transcript of Noninferiority Trials Presentation

Noninferiority TrialsAn Overview
Hollie Sturgeon, PharmD

What is a noninferiority trial?A clinical trial wherein the objective is to establish that
the experimental treatment is not clinically worse than
the active comparison treatment by more than a
small, predetermined margin.

Treatment A$35/Month
Treatment B$50/Month
Similar to classically designed head-to-head superiority trials, noninferiority trials provide comparison
data for evaluating treatment alternatives.
CONCEPT: If Treatment A is similar enough in efficacy to Treatment B that the
difference between them is clinically negligible, then my patient can use the less
expensive alternative.
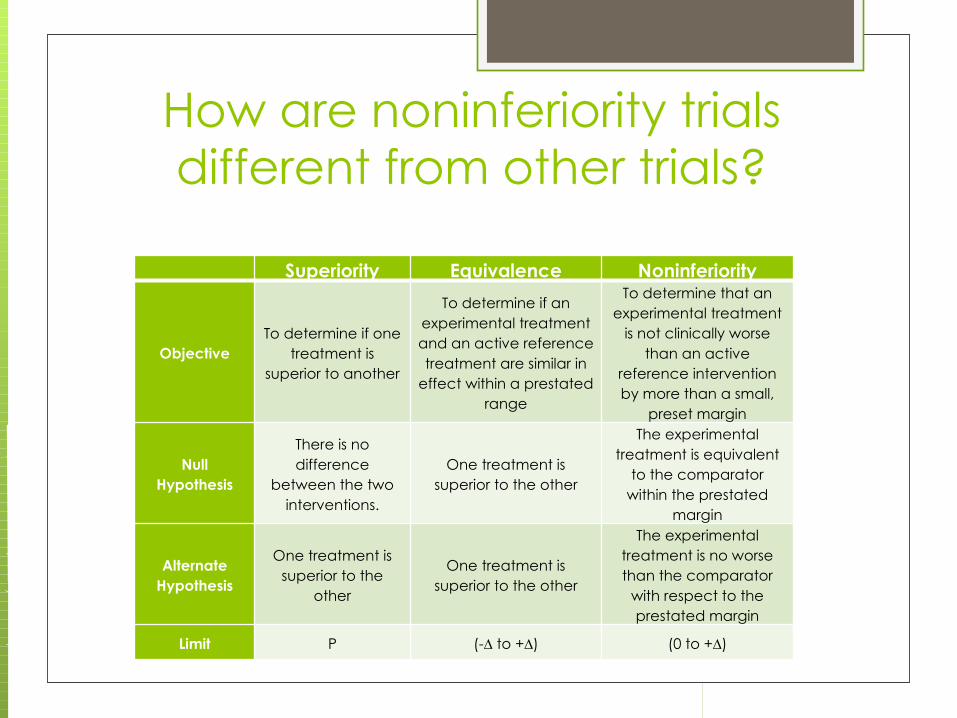
How are noninferiority trials different from other trials?
Superiority Equivalence Noninferiority
ObjectiveTo determine if one
treatment is superior to another
To determine if an experimental treatment and an active reference treatment are similar in
effect within a prestated range
To determine that an experimental treatment
is not clinically worse than an active
reference intervention by more than a small,
preset margin
Null Hypothesis
There is no difference
between the two interventions.
One treatment is superior to the other
The experimental treatment is equivalent
to the comparator within the prestated
margin
Alternate Hypothesis
One treatment is superior to the
other
One treatment is superior to the other
The experimental treatment is no worse than the comparator
with respect to the prestated margin
Limit P (-∆ to +∆) (0 to +∆)

How common are noninferiority trials?
During the 10-year period between 1999 & 2009,
582 noninferiority trials were published.
Between 1989 and 1999, there was one.
Of the 43 New Drug Applications approved by
the FDA between 2002 and 2009, 2/3 cited
evidence obtained from noninferiority trials
“Our study identified a clear trend of increasing frequency of publication of noninferiority trials”[5]

Advantages of noninferiority trials
Useful when placebo control is inappropriate.
Not limited to pharmaceutical therapy
Can be used for risk-benefit analyses
Appropriate for comparing a specific intervention to
itself (dose vs. dose or formulation vs. formulation)
Provides evidence for inferiority, noninferiority OR
superiority claims
Disadvantages of noninferiority trials Must meet specific design and analysis parameters
to be useful.
These requirements appear to be poorly understood
by investigators and their readers.
Not recommended when the reference treatment
is not well established, or is inconsistent when
compared with placebo
An appropriate sample size for noninferiority trials is
usually larger than that required for superiority trials

Noninferiority Trial DesignTo correctly interpret the results of a noninferiority
trial, we must first understand its specific
methodology and design requirements.

The hypothesis is the opposite of classically designed superiority studies.
Null hypothesis: One treatment is superior to the
other.
Alternate hypothesis: The experimental
treatment is no worse than the comparator with
respect to the prestated noninferiority margin.
Noninferiority Trial Design
Typical trial procedures such as randomization and blinding
apply; however, stricter limitations are placed on the active
control.
Comparator must be a well-established intervention with at least
one superiority trial establishing its clinical advantage over
placebo.
Overall study design is structured as closely as possible to that
superiority trial (inclusion/exclusion criteria, outcome measures,
trial conduct, etc.)
A noninferiority margin must be determined prior to trial
initiation.
Justification for the margin is provided, stating both statistical
and clinical validation.
Noninferiority Trial Design

The noninferiority margin should be no larger than the
“smallest value representing a clinically meaningful
difference” between the two interventions.
Ideally a value smaller than the minimum difference
between the active comparator and a placebo.
For example, if the referenced superiority trial showed the
comparator to be 12% better than placebo, a researcher
might set the noninferiority margin at 7%
In other words, 5% worse than the comparator, but still 7%
better than placebo
Noninferiority margin, Confidence Interval and desired
Power all influence sample size.
Noninferiority Trial Design

Intention-To-Treat (ITT) analysis can shift bias towards a
finding of noninferiority when dropouts & protocol violations
occur
The bias introduced by Per-Protocol analysis is less
predictable, especially when the rates & reasons for patient
loss differ between treatment groups.
Noninferiority trials should employ & report both methods of
analysis.
Balanced conclusions may be derived when both
methods are treated with equal importance.
A more conservative approach would be to base
conclusions on the more pessimistic of the analyses.
Noninferiority Trial Design
Noninferiority Trial Design

The tinted area represents the zone of inferiority.
•When the entire CI is less than zero, the treatment is clearly superior•When the upper limit of the CI is less than ∆, the treatment is noninferior•When the upper limit of the CI is greater than ∆, the result is inconclusive•When the entire CI is greater than ∆, the treatment is clearly inferior
Noninferiority Trial Interpretation
Superior
Noninferior
Noninferior
Inconclusive
Inconclusive
Inferior

Common ErrorsReviewers have found examples of repeated design
and reporting flaws. Becoming familiar with the
more typical faults will make it easier to evaluate
quality studies & draw appropriate conclusion.

Improper or misleading terminology
Quality reporting uses proper vocabulary, such as “Treatment
A is not inferior to (or is equivalent to) Treatment B with regard
to the margin predetermined as ____.”
Inappropriate noninferiority margin Must be defined prior to trial onset.
Justification must include be statistically & clinically relevant
Confused error types Type I error = an inferior treatment is accepted as noninferior
Type II error = a noninferior treatment is mistakenly rejected
Common errors to watch for
Incomplete analysis of results
Quality articles include both Intention-To-Treat and Per-
Protocol analyses, enabling the reader to correctly interpret
the evidence and form appropriate conclusions.
Noninferiority claims from a superiority trial
When articles omit pertinent information about the
noninferiority margin, or the sample size is calculated without
reference to that margin, clinicians should treat the
subsequent information with some skepticism
Common errors to watch for

The publication of noninferiority trials is gaining in
frequency. Evidence from these trials influence
current treatment policies, and play a role in the
decision making process for new drug acceptance.
Healthcare providers involved in the
recommendation or selection of evidenced-based
interventions should have a clear understanding of
how to evaluate the quality of these studies and
interpret their results.
Summary

The quality of noninferiority studies depends on their adherence
to basic design requisites and reporting obligations.
Standard trial procedures (randomization, blinding, etc)Active comparator that is well-established backed by at least one superiority trial Overall study design mirrors reference superiority trialA prestated noninferiority margin that is statistically and clinically justifiedSample size based on noninferiority margin, Confidence Interval size and desired study PowerBoth Intention-To-Treat and Per-Protocol analyses used and reportedResults reported as Confidence IntervalsConclusions drawn from comparison of Confidence Intervals with the noninferiority marginClaims of noninferiority correspond to the results provided and are written in precise, standardized vocabulary
Summary
1. Henanff AL, Giraudeau B, Baron G, Ravaud P. Quality of reporting of noninferiority and equivalence randomized trials. JAMA. 2006;295(10):1147-51
2. Dasgupta A, Lawson KA, Wilson JP. Evaluating equivalence and noninferiority trials. Am J Health-Syst Pharm. 2010;67:1337-43
3. Gotzsche PC. Lessons from and cautions about noninferiority and equivalence randomized trials. JAMA. 2006;295(10):1172-74
4. Piaggio G, Elbourne DR, Altman DG, Pocock SJ, Evans SJW. Reporting of noninferiority and equivalence randomized trials: an extension of the CONSORT statement. JAMA. 2006;295(10):1152-60
5. Suda KJ, Hurley AM, McKibbin T, Motl Moroney SE. Publication of noninferiority clinical trials: changes over a 20-year interval. Pharmacotherapy. 2011;31(9):833-839
6. Greene WL, Concato J, Feinstein AR. Claims of equivalence in medical research: are they supported by the evidence? Ann Intern Med. 2000;132:715-722
References


















