Nonalcoholic fatty liver diseases Alcoholic liver diseases Acute liver failure Yasar Kucukardali MD...
105
nonalcoholic fatty liver diseases Alcoholic liver diseases Acute liver failure Yasar Kucukardali MD Professor / Internal Medicine
-
Upload
corey-kelley -
Category
Documents
-
view
220 -
download
1
Transcript of Nonalcoholic fatty liver diseases Alcoholic liver diseases Acute liver failure Yasar Kucukardali MD...
nonalcoholic fatty liver diseases Alcoholic liver diseases
Acute liver failure Yasar Kucukardali MD
Professor / Internal Medicine

Non-Alcoholic Steatohepatitis
• Represents only a part of wide spectrum of non alcoholic fatty liver
• Prevalence – 2 to 3 % • NASH – 3rd most common cause of CLD in
North America after alcoholic liver disease & Hepatitis C
• The most common cause of raised transaminases more than 6 months.
• NASH was coined by Ludwig et al while describing a series of patients of non-alcoholic, diabetic patients, mostly females, in whom liver histology was consistent with alcoholic liver disease but did not have a history of alcohol consumption.

Prevalence
• Steatosis is the most common cause of raised transaminases & affects 10-24 % of gen.population while only 2-3 % of gen.population have steatohepatitis.
• In pts undergoing liver biopsy, the prevalence of NAFLD & steatohepatitis ranges from 15-39% &1.2-4.8% respectively.
Risk Factors for NAFLD
• Obesity• Diabetes • Hyperlipidemia• Female sex
etiology• Drugs / Toxins Metals – Antimony Barium salts Carbon disulfide Thallium compounds Cytotoxic/cytostatic drugs Antibiotics – Bleomycin Tetracycline Others – Amiodarone Estrogen Glucocorticoids
etiology• Inborn errors of metabolism – Abetalipoproteinemia Galactosemia Glycogen storage disease Weber-Christian syndrome Wilson’s Disease• Nutritional – Obesity Rapid weight loss Kwashiorkor
etiology
• Surgical –Jejuno colic bypassJejuno ileal bypassGastroplastyExtensive bowel resection
Pathogenesis• Increased delivery of fatty acids to liver Obesity Starvation• Increased synthesis of fatty acids in liver excess carbohydrate ( TPN )• Decreased mitochondrial beta oxidation of fatty acids Carnitine deficiency Mitochondrial dysfunction• Decreased incorporation of triglycerides into functional VLDL Impaired apolipoprotein synthesis

Pathogenesis
• Impaired cholesterol esterification Choline deficiency Protein malnutrition• Impaired export of VLDL from hepatocyte• Insulin resistance increased lipolysis hyperinsulinemia
Pathology
• Diagnosis of NASH depends on histopathological features & exclusion of alcohol as the cause of disease.
• Liver biopsy features : steatosis polymorphonuclear and / mononuclear hepatocyte ballooning and necrosi, mallory hyaline,glycogenated nuclei,metamitochondria and fibrosis indistinguishable from alcoholic liver disease
Pathology• Steatosis in NASH – macrovesicular• Inflammation of steatohepatitis is predominantly lobular,
whereas intense portal inflammation with interface activity is seen in chronic viral, autoimmune & drug indued hepatitis
• But in children , NASH may have portal infiltrate.• Neutrophilic cells in lobular inflammatory infiltrate • Balloon degeneration – recognized form & characteristic
finding in NASH.• Mallory hyaline may be +/- . It is characteristic of alcoholic
hepatitis
Pathology
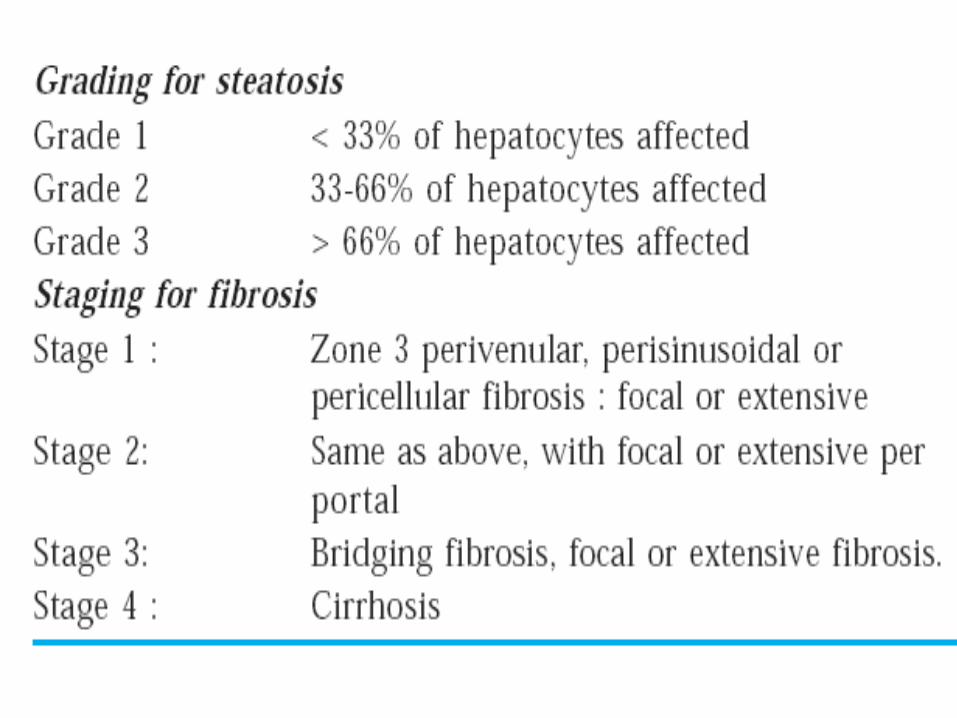
• Pattern of fibrosis is initial collagen deposition in perivenular & peri sinusoidal spaces of Zone 3 .
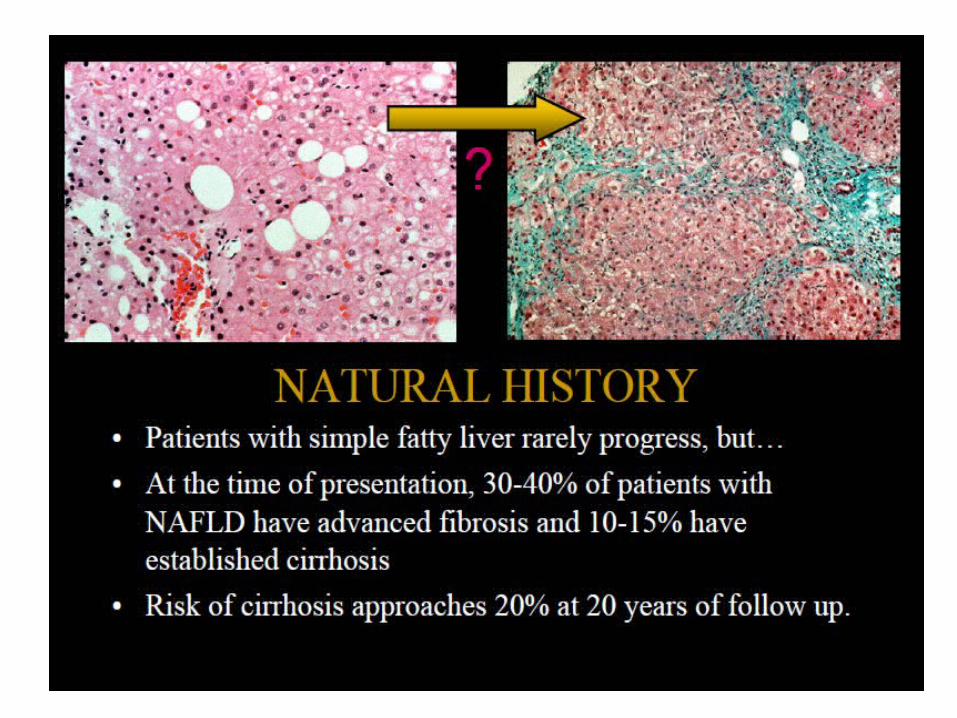
• Chicken wire fibrosis• Fibrosis – in 66% pts• While 25% have severe fibrosis• And 14% have well established cirrhosis
Histological Differential Diagnosis
• Hepatitis C• Primary Biliary Cirrhosis• Autoimmune hepatitis• Alpha 1 anti trypsin deficiency• Hemochromatosis
Clinical features Symptoms & Signs
• Most of the patients are asymptomatic • 1/3rd present with nonspecific constitutional
symptoms like weakness, fatigue & malaise.• Rapid onset of Fulminant hepatic failure – NASH d//t
drugs like nucleoside analogues, tetracyclines• Hepatomegaly , splenomegaly• Presence of ascites, spider angiomata – indicate
development of cirrhosis

Clinical featuresLaboratory findings
• Mild – moderate elevations of S.Transaminases, typically less than 4 times the upper normal limit.
• ALT level greater than AST in absence of cirrhosis.
• Liver biopsy
Diagnosis
• Clinical history• Exclusion of significant alcohol intake• Pursue dietary history, medication, occupational
exposure to organic solvents• Family history of liver disease• Other causes of CLD – infections, metabolic
heriditary & autoimmune causes to be ruled out• Liver biopsy – confirm diagnosis & for prognostic
information
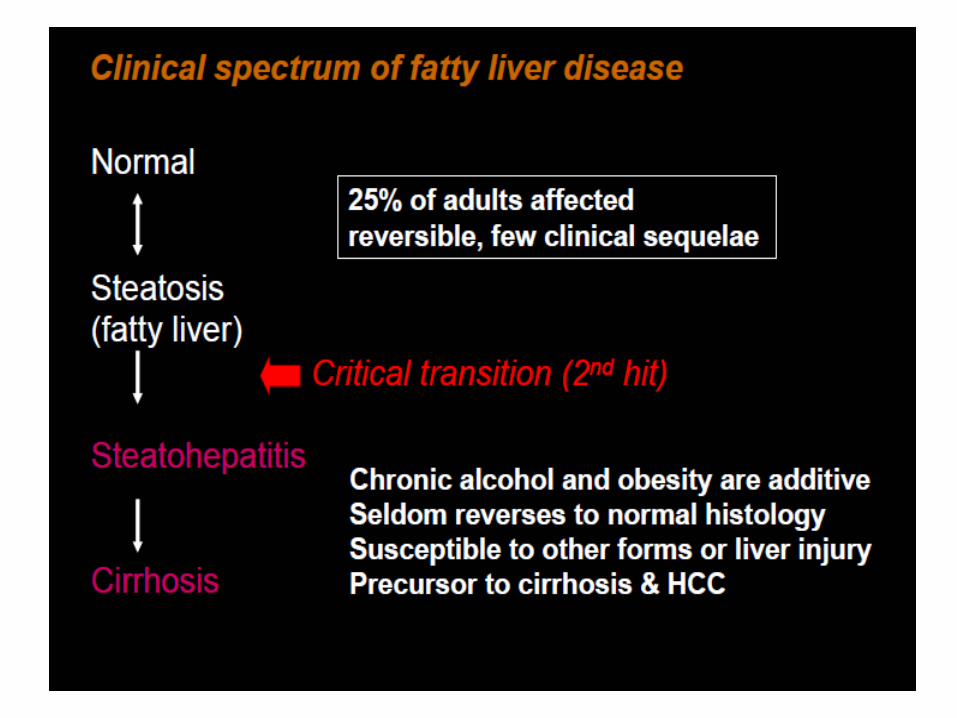
Natural course
• Steatosis• Steatohepatitis• Cirrhosis• Steatosis – good prognosis• Steatohepatitis , cirrhosis – bad prognosis

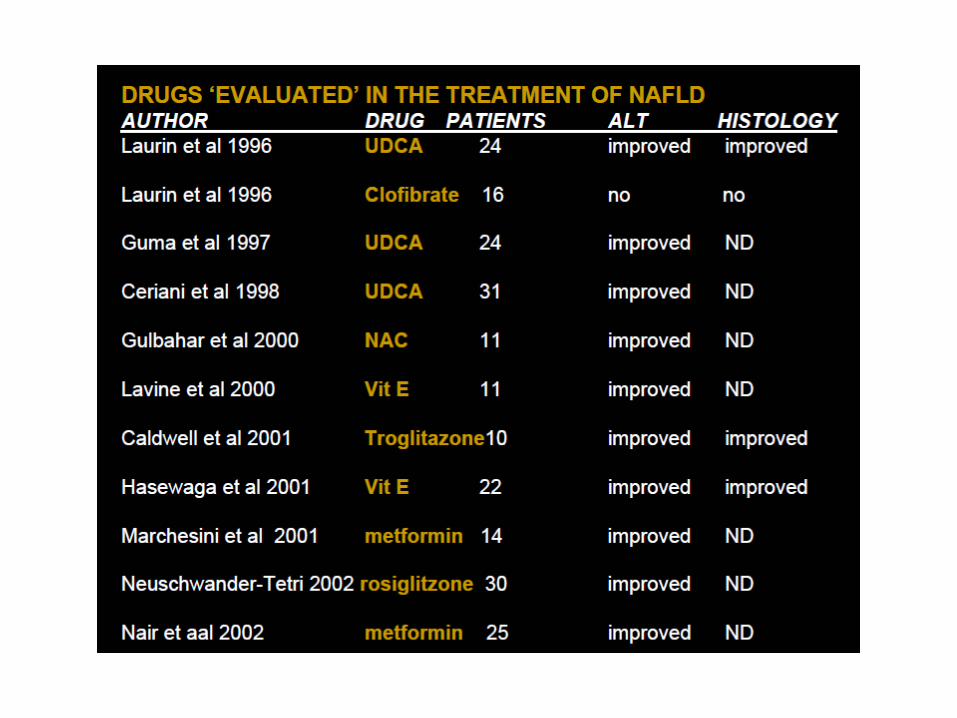
Treatment• Treatment options are limited• Weight Reduction: • wt loss – normalization of s.aminotransferases.• Means of wt loss is important not the amount of wt loss• Recommended wt loss – 230 g/day or 1.6 kg/week• Diet : 45 -100 g high quality animal protein less than 100g carbohydrates less than 10 g fat per day providing 600 -800 kcal
Treatment
• Ursodeoxycholic acid : • Has membrane stabilizing / cytoprotective /
immunological effect• 10-15 mg/kg/day for 6-12 months – significant
improvement in transaminases levels and degree of steatohepatitis
Treatment
• Liver Transplantation :• NASH – A relative contraindication• Many of pts with NASH with CLD who
underwent Liver Transplant – redeveloped NASH in the new donor liver ( 2/3 cases ) &
• 1/3rd cases – liver transplantation is unsuccessful.
Newer treatment modalities
• Inhibition of macrophage activation:
Anti oxidant ( Vit E ) glutathione prodrugsAntibiotics, preprobioticsAnti cytokines ( anti TNF alpha antibodies,
pentoxiphylline )
• Protect hepatocyte ATP storesPARP inhibitors• Minimize CYP2F activityDietary modification ( avoid fats )• Insulin sensitizers : pioglitazone• Antiobesity drugs : sibutramine, orlistat• Antilipid drugs : Simvastatin, Procusol
Alcoholic liver diseases
INTRODUCTION
• There is a spectrum of clinical and laboratory findings in patients with alcoholic liver disease, ranging from asymptomatic fatty liver to alcoholic hepatitis to end-stage liver failure with jaundice, coagulopathy, and encephalopathy
• Unfortunately, many alcoholics first become symptomatic only when severe, life threatening liver disease is already present.
• Even at this stage, abstinence can result in significant reversal in some patients.
• Patients with alcoholic liver disease often have coexisting dysfunction in other organs.
cardiomyopathy, skeletal muscle wasting, neuropathies, pancreatic dysfunction. • The presence of fever and abdominal pain should not be
taken lightly in a patient with alcoholic hepatitis with cirrhosis and ascites, and can mimic the presentation of spontaneous bacterial peritonitis.
• The distinction between these disorders should be made by ascitic fluid analysis. A polymorphonuclear leukocyte count that is ≥250/mm3 is presumptive evidence of spontaneous bacterial peritonitis since it does not occur with alcoholic hepatitis alone.
• Excessive alcohol consumption is the leading cause of liver disease.
• Alcoholic liver disease comprises of three main stages
1. Hepatic steatosis2. Alcoholic hepatitis3. Cirrhosis
Hepatic steatosis• Pathogenesis :• Fatty change is an acute, reversible manifestation of ethanol
ingestion.• Ethanol causes
– Increased fatty acid synthesis by causing catabolism of fat in the peripheral tissues
– Acetaldehyde which is metabolite of ethanol converts NAD+ to NADH. An excess NADH stimulates lipid biosynthesis.
– Oxidation of fatty acid by mitochondria is decreased– Acetaldehyde impairs the function of microtubules, resulting in
decreased transport of lipoproteins from liver• Collectively these metabolic consequences produce fatty liver.
• Pathology:• Gross:
– The liver becomes yellow, greasy and is enlarged (up to 4 to 6 kg)
– The increase in weight is because of accumulation of fat, protein and water

• Microscopy:• Following even moderate intake of alcohol,
small (microvesicular) lipid droplets accumulates in the liver
• With chronic intake of alcohol, more lipid accumulates, creating a large macrovesicular globules, compressing the nucleus the periphery.
Steatosis in Alcoholism
• Clinical features of alcoholic steatosis– Hepatomegaly – Mild elevation of serum bilirubin, alkaline
phasphatase and gamma GT
Alcoholic hepatitis
• Is characterized by1. Hepatocyte swelling and necrosis2. Mallory bodies3. Neutrophilic inflammatory response4. Perivenular fibrosis
• Hepatocyte swelling and necrosis:– Single or scattered foci of cells undergo swelling
(ballooning degeneration) and necrosis
• Mallory bodies:– Scattered hepatocytes accumulate cytokeratin
intermediate filaments and other proteins– Visible as eosinophilic cytoplasmic inclusions in
degenerating hepatocytes
• Neutrophilic reaction:– Neutrophils accumulate around the degenerating
hepatocytes, particularly those having Mallory bodies.
– Lymphocytes and macrophages also enter portal tracts and spill into parenchyma
• Fibrosis :– Commonly seen in the form of sinusoidal and
perivenular fibrosis– Occasionaly periportal fibrosis may predominate– Fibrosis mainly occurs because of the activation of
sinusoidal stellate cells and portal tract fibroblasts
• Clinical features:– Malaise, anorexia, weight loss, upper abdominal
discomfort, tender hepatomegaly.– Laboratory findings:
• Hyperbilirubinemia• Elevated ALP,GGT, moderate elevation of AST • Neutrophilic leucocytosis
• Alcoholic cirrhosis:– The final and irreversible form of alcoholic liver
disease– Usually evolves slowly– Gross:
• Initially the liver is yellow-tan, fatty and enlarged.• Later it is transformed into brown, shrunken, nonfatty
organ with multiple nodules.• Sometimes nodularity becomes very prominent with
scattred lager nodules creating a “hobnail” appearance on the surface of liver
• Microscopy:– Initially fibrous septae are very delicate and
extend through sinusoids from central to portal regions as well as from portal tract to portal tract.
– As the fibrous septae dissect and surround nodules, the liver becomes more fibrotic, loses fat, and shrinks in size. (Laennec cirrhosis)
– Bile stasis may be seen.
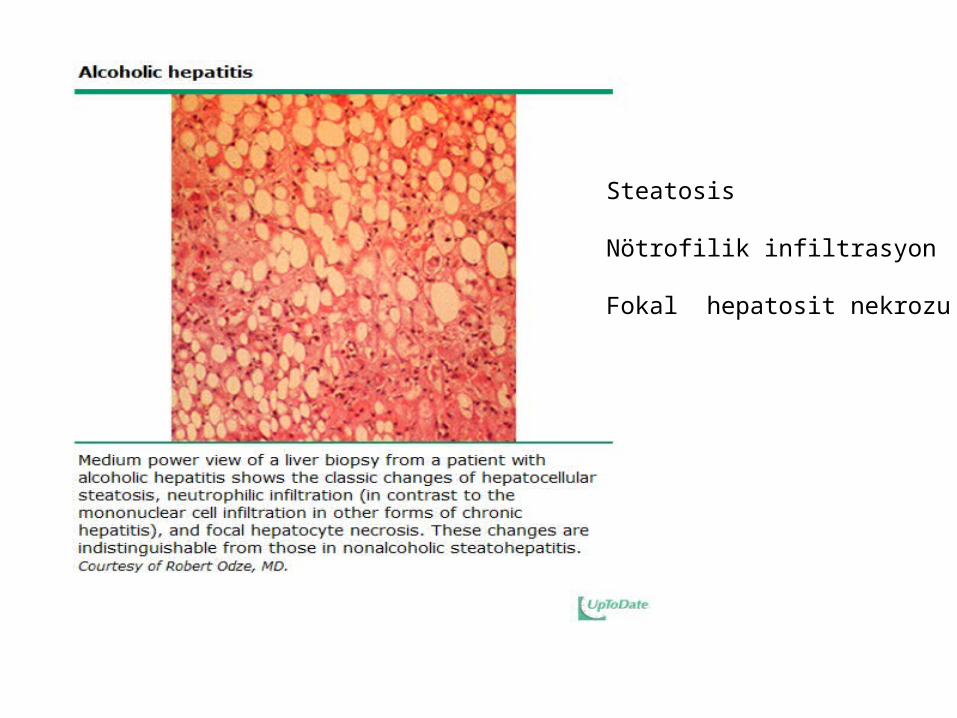
Steatosis
Nötrofilik infiltrasyon
Fokal hepatosit nekrozu
ROLE OF LIVER BIOPSY
the diagnosis of alcoholic liver disease is often made without a liver biopsy when the clinical presentation is classic. However, a liver biopsy can be used to establish the diagnosis, exclude coexisting, unsuspected liver diseases, and establish the severity of liver disease.
It is difficult to predict the presence of cirrhosis based upon clinical and laboratory features, and documentation of cirrhosis may have therapeutic and prognostic implications.
TanıAyırıcı tanıHastalık şiddeti
Tedavi ve prognoz Tayini
• Clinical features:– Features are similar to other forms of cirrhosis.– Malaise, weakness, weight loss, loss of appetite– Jaundice, ascites, and peripheral edema– Features of portal hypertension
• Laboratory findings:– Hyperbilirubinemia, elevated serum aminotransferase,
alkaline phasphatase, hypoproteinemia and anaemia
DIFFERENTIAL DIAGNOSIS
Patients with alcoholism can have concurrent forms of liver disease, or have liver disease unrelated to alcohol.
• A high prevalence (25 to 65 percent) of hepatitis C virus infection has been recognized in alcoholics . Such patients tend to have more severe disease, decreased survival, and an increased risk of hepatocellular carcinoma
• A liver biopsy may be helpful since the presence of lymphocytes rather than neutrophils suggests the presence of chronic viral hepatitis.
• Hemochromatosis and nonalcoholic steatohepatitis (NASH) may have similar clinical or histological features as alcoholic liver disease.
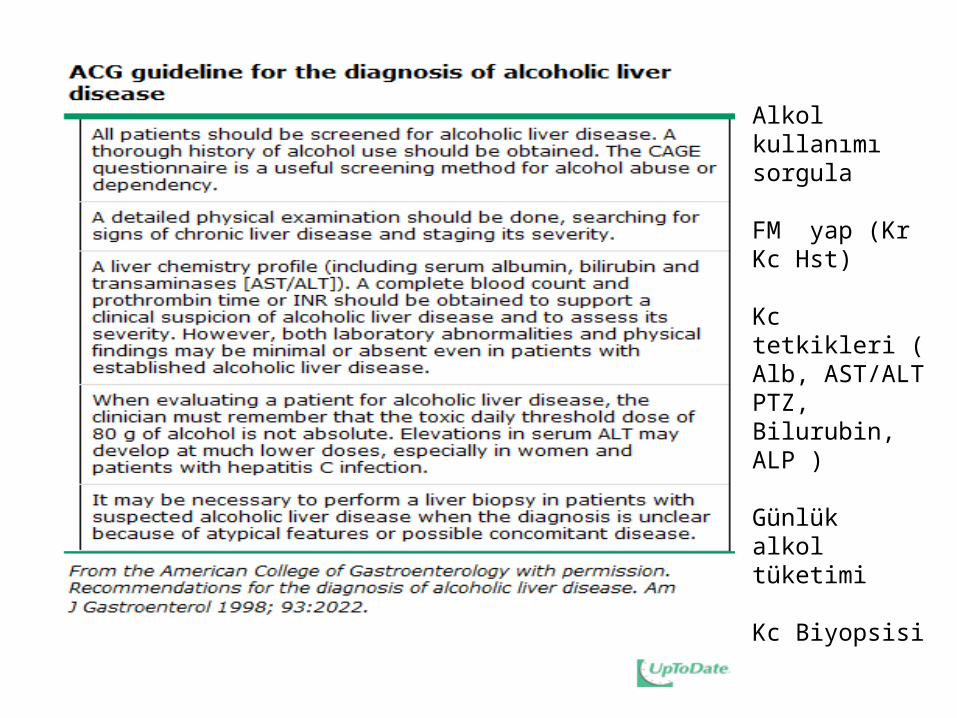
Alkol kullanımı sorgula
FM yap (Kr Kc Hst)
Kc tetkikleri ( Alb, AST/ALTPTZ, Bilurubin, ALP )
Günlük alkol tüketimi
Kc Biyopsisi
Acute liver failure
DEFINITION
Acute liver failure, impaired synthetic function and encephalopathy in a person who previously had a normal liver or had well-compensated liver disease.
The development of encephalopathy within eight weeks of the onset of symptoms in a patient with a previously healthy liver
The appearance of encephalopathy within two weeks of developing jaundice, even in a patient with previous underlying liver dysfunction
Sentez fonksiyonu bzkEnsefalopati
Semptom başlangıcı – Ensefalopati 8 hft : sağlıklı kc
Sarılık gelişen hastada İki hft da ensefalopati : Disfonksiyone kc
DEFINITION
Patients who have rapid deterioration of liver function with the development of encephalopathy within six months are considered to have "subfulminant" hepatic failure.
Cerebral edema is common in fulminant disease and rare in subfulminant disease. In contrast, renal failure and portal hypertension are more frequently observed in patients with subacute liver failure
6 aySubfulminant
Serebral ödem / fulminant
Renal ytm, portal hpt / subakut kc ytm
Definition
• The development of prolonged prothrombin time and encephalopathy within 8 weeks of symptom onset in patient with no previous liver disease
• U.S. annual incidence about 2,000 cases per year (1)
• High mortality
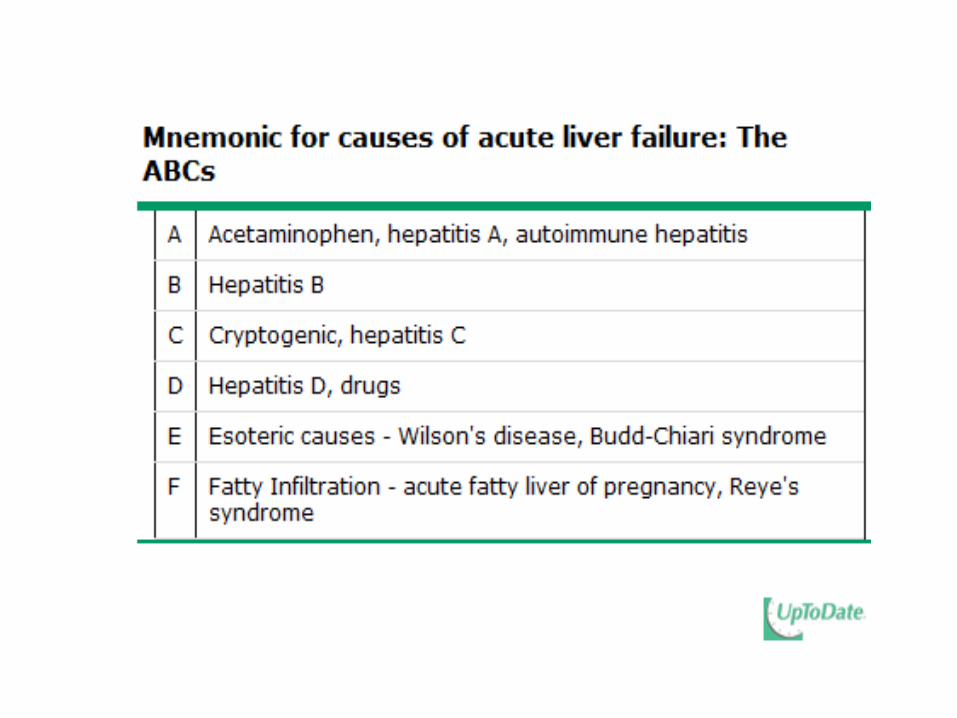
Causes of Acute Liver Failure
• Varies by geographic region• In the U.S., acetaminophen hepatotoxicity
most common• Indeterminate cause• Idiosyncratic drug reactions – Isoniazid most
common
Causes of ALF
• Hepatitis B – U.S. 4th most common cause; world wide # 1 cause
• Hepatitis A – endemic areas• Autoimmune hepatitis• Ischemia• Wilson’s Disease
Causes of ALF
• Budd Chiari Syndrome• Pregnancy – acute fatty liver of pregnancy and
the HELP syndrome (hemolysis, elevated liver chemistries, low platelets)
Transplant-free Survival
• Highest in acetaminophen hepatotoxicity • Followed by drug reaction• Followed by indeterminate cause• Best when ALF develops hyper acutely i.e.,
within seven days
The Phenomenon
• Highly unpredictable• Dramatic• Requires aggressive intensive care
management, anticipation of complications, and evaluation/listing for liver transplantation
Survival
• Correlates with degree of encephalopathy and coagulopathy
• Encephalopathy may be abrupt and rapidly progressive– Subtle mood change - > seizures - > obtunded - >
decorticate posture– Associated with cerebral edema rather than
portosystemic shunting of toxins seen in cirrhosis
Acetaminophen Overdose
• Accidental• Suicide gesture/attempt• Emergency Room administration of antidote:
p.o. NAC or I.V. Acetadote (contraindicated in sulfa allergy)
Accidental Overdose
• High dose APAP for an extended period• Inadvertent simultaneous administration of
APAP w/ combination drugs:– OTC Sinus and cold preparations– OTC Narcotic pain relievers– OTC Sleep preparations– In combination w/ alcohol
Pathophysiology
• Dose dependent; known liver toxin• Also influenced by the presence of
malnutrition, concomitant ethanol, co-administered drugs, and CYP 384 polymorphisms
• Centrilobular necrosis without inflammation
Signs and Symptoms
• Anorexia, nausea, vomiting, malaise, right upper quadrant discomfort
• Dark urine, pale stool, icterus• Transaminases rise within 10 – 12 hours, often
to dramatic levels AST > ALT, peak at day three and rapidly improve
• Jaundice develops quickly, total bilirubin not as high as that seen in other causes of ALF
Cirrhosis and Portal Hypertension
The Final Stage of Chronic Liver Disease Due to Any Cause
Cirrhosis• Excess extracellular matrix/fibrosis in liver• Fibrosis spans portal-central areas
– portal-portal or central-central also seen• Fibrosis encases groups of hepatocytes• Results in distorted architecture and
vasculature

CirrhosisCirrhosisNormalNormal
Nodules surrounded by fibrous tissue
Nodules surrounded by fibrous tissue
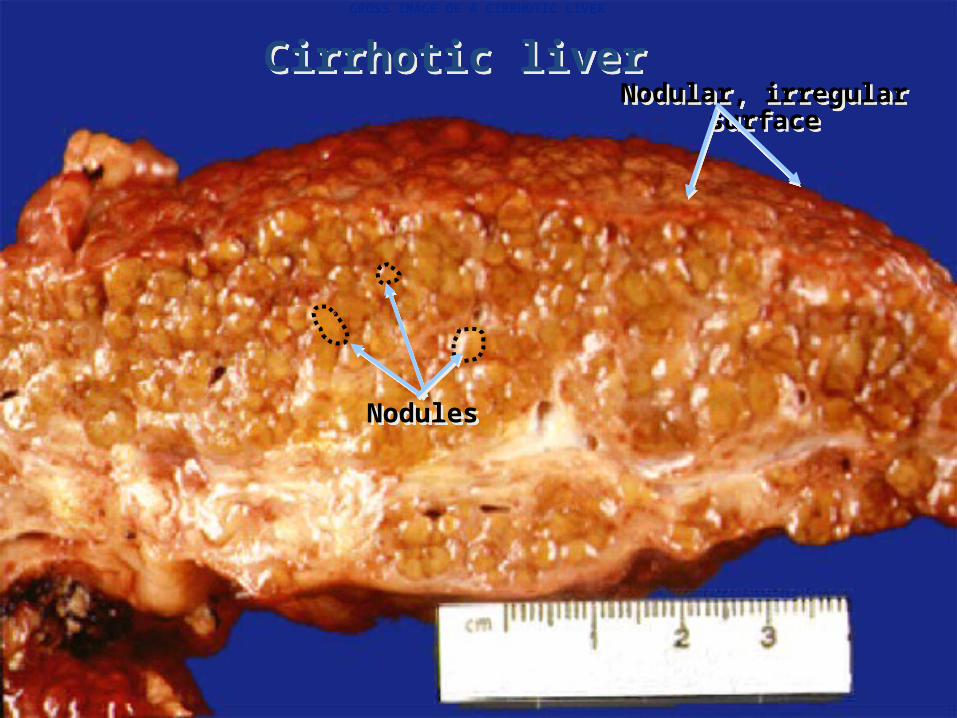
Cirrhotic liverCirrhotic liverNodular, irregular surfaceNodular, irregular surface
NodulesNodules
GROSS IMAGE OF A CIRRHOTIC LIVER
Portal Hypertension
• Cirrhosis - > increased resistance to flow of blood in sinuosoids and in liver
• Increased resistance = increased portal pressure = portal hypertension
• Pressure in PV causes release of vasodilators, i.e., nitric oxide (NO)
• NO causes splanchnic arteriolar vasodilation and increased splanchnic inflow of blood
• This increased flow maintains portal hypertension in spite of development of low resistance collaterals
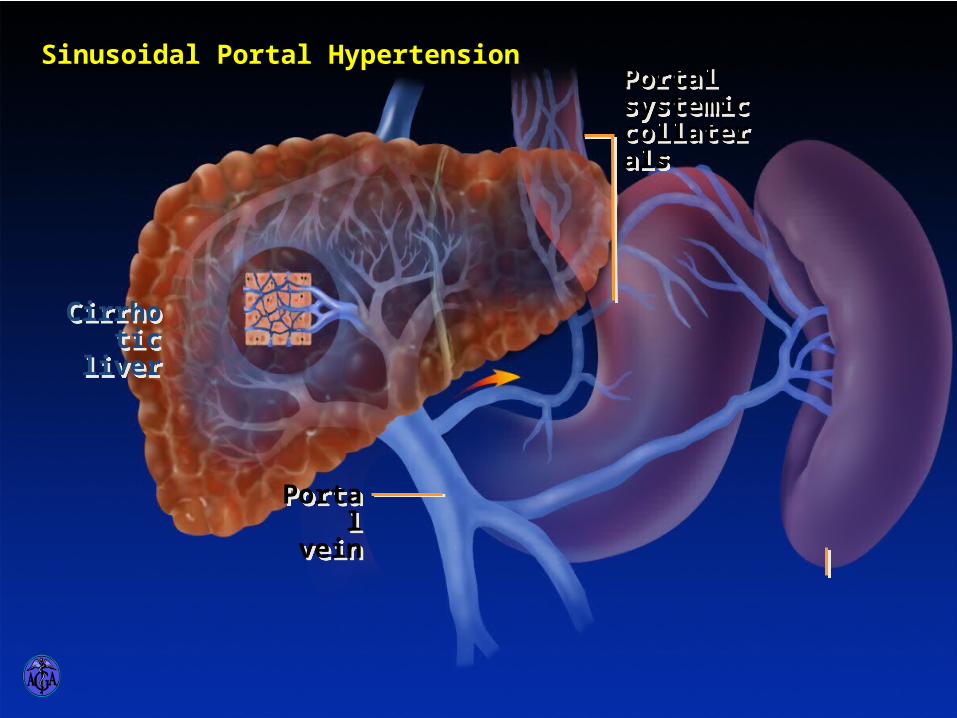
SINUSOIDAL PORTAL HYPERTENSION
Cirrhotic liver
Cirrhotic liver
Portal vein
Portal vein
Sinusoidal Portal HypertensionPortal systemic collaterals
Portal systemic collaterals
Consequences ofPortal Hypertension
• Splenomegaly– Thrombocytopenia– Palpable spleen; splenectomy harmful
• Varices– On imaging may be peri-gastric, esophageal, or splenic– On gastroscopy of variable size– Risk for bleed increases w/ advancing liver failure– Treat w/ nonselective beta blocker, banding
Consequences ofPortal Hypertension
• Ascites: The accumulation of fluid in the peritoneal cavity– An important clue to the presence of advanced
cirrhosis– Result of sinusoidal HTN caused by blocked
hepatic venous outflow 2/2 regenerative nodules and fibrosis
– Result of plasma volume expansion, sodium, and water retention
Serum to Ascites Albumin Gradient“SAAG”
• The concentration of ascitic fluid protein is much lower than the concentration of serum protein
• This is due to sinusoidal capillarization, decreased permeability to plasma proteins
• Protein concentration in ascitic fluid in cirrhosis correlates inversely w/ the degree of portal hypertension
Ascites
• Associated conditions:– Hyponatremia– Umbilical hernia– Hepatic hydrothorax
• Complication of ascites:– Spontaneous bacterial peritonitis– Pneumococus common etiology– Gram negative bacteria
Ascites• Treatment:
– Sodium restriction, diuretics, paracentesis– Transjugular intrahepatic portosystemic shunt
• TIPS often worsens encephalopathy
• Prognosis: continuum of uncomplicated ascites - > refractory ascites - > hepatorenal syndrome
• Mortality approximately 20%/year
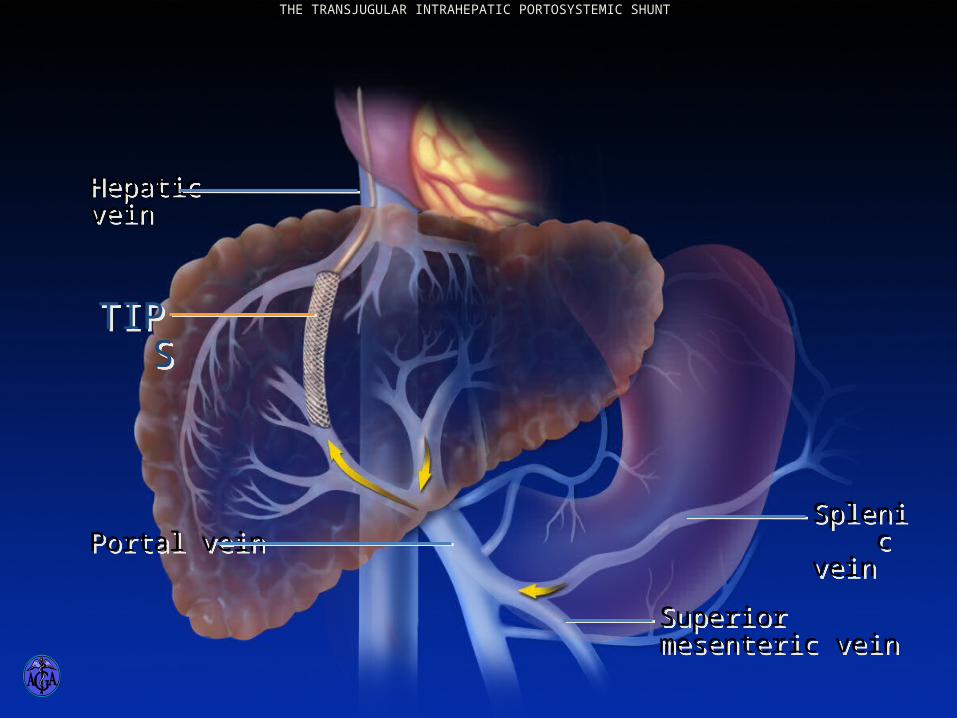
Hepatic veinHepatic vein
Portal veinPortal veinSplenic veinSplenic vein
Superior mesenteric veinSuperior mesenteric vein
TIPSTIPS
THE TRANSJUGULAR INTRAHEPATIC PORTOSYSTEMIC SHUNT
Consequences ofPortal Hypertension
• Hepatic encephalopathy• Episodic vs persistent• Usually precipitated by events such as:
– Bleeding– Infection– Use of sedatives or hypnotics– Dehydration
Hepatic Encephalopathy
• Pathogenesis: failure of the liver to detoxify portal blood toxins in the setting of decreased hepatic function and/or diminished hepatic perfusion by portal blood. Cerebral edema, ammonia, and disturbances in cell function, esp. astrocytes
• Diagnosis: don’t assume it is HE until other potential causes of altered mental status have been considered
EncephalopathyAlternative Explanations
• Metabolic: hypoxia, hypoglycemia, hypo/hypernatremia, thyroid disease, hypercalcemia
• Central Nervous System: CVA, Subdural hematoma, post ictal state, metastatic cancer
• Toxins: alcohol, CNS depressants• Infection: sepsis, meningitis, encephalitis,
delerium tremens
StagingWest Haven Criteria
• Stage 0: No abnormality• Stage 1: Trivial lack of awareness
– Shortened attention span– Euphoria or anxiety– Impairment of addition and subtraction
• Stage 2: Lethargy– Time disorientation– Personality change– Inappropriate behavior
Staging Hepatic Encephalopathy West Haven Criteria
• Stage 3: Somnolence to semistupor– Response to stimuli– Confusion– Disorientation – Bizarre behavior
• Stage 4: Coma • Generalized motor abnormalities common:
hyperreflexia, asterixis, Babinski +
Hepatic Encephalopathy• Blood ammonia testing has little role in the
diagnosis of HE• Clinical suspicion is the main guide• Treatment:
– Supportive care for altered mental state– Identify and treat the precipitating cause– Exclude and/or treat other medical illnesses– Begin empirical therapy: lactulose, nonabsorbable
antibiotics, metronidazole
Complications of Cirrhosis
• Osteoporosis• Increased risk of infections• Muscle cramps• Increased risk for hepatocellular carcinoma• Malnutrition• Depression• Pruritis
Standard Recommendationsfor All Cirrhotics
• Vaccinate against viral hepatitis, pneumococcal pneumonia, influenza
• Baseline bone density test – treat osteopenia or osteoporosis as indicated
• Baseline ultrasound and AFP and repeat semi-annually for HCC surveillance if cirrhotic
• Esophageal varix surveillance – treat as indicated
Standard Recommendationsfor All Cirrhotics
• Refer for liver transplantation• Monitor for signs of advancing liver failure• Avoid alcohol• Avoid NSAIDs• Acetaminophen is analgesic of choice• If significant ascites, cane, walker • If Grade II or higher encephalopathy take the
car keys, protect from harm
PROGNOSIS
Patients with ALF are susceptible to a wide variety of complications in addition to encephalopathy These include cerebral edema, renal failure, hypoglycemia, metabolic acidosis, sepsis, coagulopathy, and multiorgan failure.
All patients with ALF should be managed in an intensive care unit at a facility capable of performing liver transplantation.
The only therapy proven to improve patient outcome in ALF is orthotopic liver transplantation,
PROGNOSIS
An illustrative study from the United States included 308 patients with ALF of whom 67 percent survived.
As a general rule, the most important variables for predicting the outcome in ALF are the degree of encephalopathy , the patient's age, prothrombin time, and the cause of ALF. Spontaneous recovery is more likely with lower grades of encephalopathy.
Grade I to II — 65 to 70 percent Grade III — 40 to 50 percent Grade IV — <20 percent
PROGNOSIS
• Patients older than 40 or less than 10 years of age may have a lower spontaneous recovery compared to patients between these ages.
• Patients with ALF secondary to acetaminophen (with the exception of those with severe metabolic acidosis 24 hours after ingestion or progressive coagulopathy), hepatitis A, or hepatitis B have a better prognosis than those with idiosyncratic drug reactions and Wilson's disease
PROGNOSIS
Several other variables have been used to predict the probability of recovery:
• The prothrombin time, serum bilirubin concentration and arterial pH.
• The presence of a systemic inflammatory response syndrome and, in patients that receive plasma exchange, the ratio of total to direct bilirubin
• High arterial ammonia levels (>200 g/dL) have been associated with cerebral herniation
Newer approaches
• A number of approaches for delaying or obviating the need for liver transplantation in patients with ALF continue to be studied.
artificial hepatic assist devices, auxiliary liver transplantation, a liver dialysis system, xenotransplantation.
Artificial hepatic assist devices
• There has been a strong interest in developing an artificial hepatic assist device for ALF that would operate on the same basic principles as hemodialysis for renal failure.
• The major difference between the two is that the liver performs an incredibly large number of diverse and vital synthetic functions compared to the kidneys.
• As a result, developing a machine that performs the functions of the liver is inherently more difficult than developing one that performs the excretory functions of the kidneys.
• Extracorporeal assist devices currently under development use hepatocytes from human or nonhuman cell lines to provide synthetic capability.
Auxiliary liver transplantation
• Auxiliary liver transplantation involves placement of a graft adjacent to the patient's native liver (auxiliary heterotopic liver transplantation) or in the hepatic bed after a portion of the native liver (auxiliary orthotopic liver transplantation) has been removed.
• There are also reports of auxiliary liver grafts being reused in second recipients with chronic liver disease
Xenotransplantation
• The role of xenotransplantation (transplantation of a nonhuman organ) in the treatment of ALF is currently being reexamined. Prior to 1992, only 33 xenotransplants had been performed in humans .
• The longest graft survival was only nine months. Despite the initial disappointing results, this approach is being reevaluated because of advances in immunosuppression and the ability to manipulate donor antigen expression