non-ulcer dyspepsia lily fd
8
J Clin Pathol 1'986;39:863-870 Local immune response to gastnic pyoacter in non-ulcer dyspepsia .1J WYATT,* RJ RATHBONE, RY IRVHEATLEY'f Frm tdie University DL-parmemnts of *PatIwI(,y andljtMedliee, St James's University Hospital, Leeds SUMMARY C fC 'Ioiwter pyk*i4lwereiditiiedhistolo¢caflyisgastric biopsy speci- mem; fom WY8 83 patimns with non-uke and chGromi gastriis,. bta nott in 58 dys- pcFplt- swth 1 IlA l llSI The Flle ad l p densit ofo was associ- wg1ob b- was investilgted by, suinm ofigA, IG, and IgM 54 btopsy gA coated b r wr se ial case of ative aiis, ad of biopsy Withu iCoating wi-th igG or IgM,. or both,, was rielitited with,ativit of p s and was rardy senm n theabsm ofa rto. Dl'ace theipr vmegmti~~bo Wae adMahli W311i the of m goaL¶p i camnplo- bactarflme ofrm fowud imndroi * ~~~~~~malli 2- 46 p,gms-, bMter py in aatra1 PsMlb ((qtpe 3 Mo- ant t1Cymoirtcdbis) is r to be around!9e°i.. beThe can be on in pre RMC .MfshaN 3imf M a aWln of'rDr Cpyfmiwidi and dwk sy r onmi iIIwr lkam ci#d!withmcu ooiXl deby KocWs; tliinrd and' fih pt Cpy ae Ofe' pmt in wi^s th thi s ii may be due to 1 as mast acdthbat lid ukars. with thec notaWi acepq,,- tim oft I bal Mt 1w e a e th C'yw& S -<dS. Zb_t ¢ beftwe Cpyiand gaaridis canncr be duibtd9' and must rival that i is i* 1bo its 'aD acde°' and a tlid SIIs oIgA, .tS ¢ w. I th lieu u&ibami w iise intlmmiy Imii shos, Gries W o1&SA tope wi bsoy3"" for. FmiDR'o .6 Fduiry1 and ibei16ar4- Tbe I i rpysical or", imsuts, woddl be well saied to combat a bacterial patkgam. Evidne of a lra specifim rmespose, to) C(I1C@U5U C r&uridJa woWol triomref . i vowr a cauatinve, ir We bave pzeviou*iy shown am&CPY&ddb inin- patIimtsD (W. aims in the stvdy was to, t_ X thle1 ill viivo op o1 cf host m- onto o CpyJini gastiri biopsy, tics of antibody catiiup the bactera.r Paired fioim ess loescopke bipsy of anra and body! uucosa om 11411 patients. wi nac uk= ysepi were studiied.. The prfesecew and sever- lily fd mi was ow dbloiF- gust (W)) on fixed pwaffmi am 5 e.^ scdfious staimed with tolin and eosii, ac¢¢dL mg to the crtea of Wuiteled. ' Co CpQ&Iis ware dntikdl by, the W stain. The distirutin of Cpykwd&s and the paresure ofi sG,. IgA,iamd 1gM coatimg the ware Stud- idin dmainm 30 case Inth e biopsy, te OJSiif' in tht siS; te. sr,. ~th upp9almd th d eepe poew og' the gastie ptse wiiich wrer sepaately td o M ao s*af to ***++ = icnsTb" fom_I afklE sg + + = epCrst in mw s D 863
Transcript of non-ulcer dyspepsia lily fd

J Clin Pathol 1'986;39:863-870
Local immune response to gastnic pyoacter innon-ulcer dyspepsia.1J WYATT,* RJ RATHBONE, RYIRVHEATLEY'fFrm tdie University DL-parmemnts of*PatIwI(,y andljtMedliee, St James's University Hospital, Leeds
SUMMARY C fC 'Ioiwter pyk*i4lwereiditiiedhistolo¢caflyisgastric biopsy speci-mem; fom WY8 83 patimns with non-uke and chGromi gastriis,. bta nott in 58 dys-
pcFplt- swth 1 IlA l llSITheFlle ad lp densit ofo was associ-
wg1ob b- was investilgted by, suinm ofigA, IG, and IgM 54 btopsygA coated b r wr se ial case of ative aiis,ad of biopsy
Withu iCoating wi-th igG or IgM,. or both,, was rielititedwith,ativit ofp s andwasrardy senmntheabsm ofa rto.
Dl'ace theiprvmegmti~~bo Wae adMahliW311i the of m goaL¶p i camnplo-
bactarflme ofrm fowud imndroi* ~~~~~~malli 2- 46 p,gms-,
bMter py in aatra1 PsMlb ((qtpe 3 Mo-ant t1Cymoirtcdbis)is r to bearound!9e°i..beThe can be on in pre
RMC .MfshaN 3imf M a aWln of'rDrCpyfmiwidi anddwk sy ronmiiIIwr lkamci#d!withmcu ooiXl debyKocWs; tliinrd and' fihpt Cpy aeOfe' pmt in wi^sththi s ii may be due to 1 as
mast acdthbat lid ukars. with thec notaWi acepq,,-tim oft I balMt 1w e a eth C'yw& S -<dS. Zb_t¢
beftwe Cpyiand gaaridis canncr be duibtd9'and must rival that i is
i* 1bo its 'aDacde°' and a tlidSIIs oIgA,.tS¢ w.Ith
lieu u&ibami wiiseintlmmiyImii
shos, GriesW o1&SA tope wi bsoy3""
for. FmiDR'o .6 Fduiry1
and ibei16ar4- Tbe I irpysical or", imsuts, woddl be well
saied to combat a bacterial patkgam. Evidne of alra specifim rmespose, to) C(I1C@U5UC r&uridJa woWol triomref . ivowr a cauatinve, ir
We bave pzeviou*iy shown am&CPY&ddb inin-
patIimtsD (W. aims in the stvdy was to,t_X thle1 ill viivo op o1cf host m-
onto o CpyJini gastiri biopsy,
tics of antibody catiiup the bactera.r
Paired fioim ess loescopke bipsy ofanra and body! uucosa om 11411 patients. wi nacuk= ysepi were studiied.. The prfesecew and sever-lily fd mi was ow dbloiF-
gust (W)) on fixed pwaffmi am 5e.^scdfious staimed with tolin and eosii, ac¢¢dLmg to the crtea of Wuiteled. ' CoCpQ&Iis ware dntikdl by, the Wstain.The distirutin of Cpykwd&s and the paresure ofi
sG,. IgA,iamd 1gM coatimg the ware Stud-idindmainm30case Inth e biopsy, te
OJSiif' intht siS; te.sr,. ~th upp9almd th deepe poew og'
the gastie ptse wiiich wrer sepaately td oMaos*af to ***++ = icnsTb"fom_I afklE sg + + = epCrst inmws D
863

Wyatt, Rathbone, Heatlev
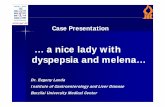
Fig. 1 Antral biopsy specimen stained by Warthin-Starry technique, showing colonising Cpyloridis. Organisms are presenton surface (arrow) and in upper and deep sections ofpits. Both pits contain organisms, although of varying population density.Dense colonies ofbacteria (open arrow) present in upper pit (score 4 + ). This specimen scored 9 + for density ofcolonisingCpyloridis (surface 2 +; upper pits 4 +; deep pits 3+ ). Original magnification x 130.
power fields of surface and gastric pits; + + + =Cpyloridis in all high power fields of surface and pits;+ + + + = Cpyloridis particularly numerous in allfields) (Fig. 1) and these values were added to quan-tify the density of bacterial colonisation, giving a pos-sible range of I to 12+.
Paired biopsy specimens were stained by the indi-rect immunoperoxidase method, with rabbit poly-clonal antiserum to human IgA, IgM, and IgG(Dako) at a dilution of l in 500, haematoxylin beingused as a counterstain. The presence of labelledCpyloridis on the surface and in the upper and deeppits of each specimen was recorded. Negative controlsconsisted of sections of normal non-colonisedmucosa, colonised mucosa with omission of rabbitantiserum, and sections from an adhesion study, inwhich Cpyloridis from broth culture adhered in vitroto normal antral mucosa maintained in tissue culturefor two hours. All immunoperoxidase sections wereexamined without knowledge of the histological diag-nosis and graded as follows: no immunoperoxidaselabelling of bacteria present (-); one or two weaklypositive bacteria present (±); high incidence ofweakly positive bacteria (+); high incidence ofstrongly positive bacteria (+ +).
Patterns of immunoperoxidase labelling of
Cpyloridis on actively inflamed gastric mucosa werecompared with those of normal body mucosa andmucosa from antrum and body showing inactivechronic gastritis (Figs. 2 and 3).
Statistical analysis was performed using the Mann-Whitney U test for comparing population densities ofCpyloridis, and elsewhere by Fisher's exact test.
Results
Table 1 shows the prevalence of chronic gastritis andcolonising Cpyloridis in one or both biopsy specimensfrom 141 patients with non-ulcer dyspepsia.Cpyloridis were present in 74 of 83 (89%) patientswith chronic gastritis and in none of the 58 patients inwhom both antral and body mucosa were normal.Cpyloridis were detected on the morphologicallynormal body mucosa in 20 of 22 patients in whomgastritis affected only the antrum. There was no cor-relation between the severity of chronic gastritis(superficial or atrophic) and detection of Cpyloridis,except that organisms were never present on areas ofintestinal metaplasia. The association between theactivity of gastritis and Cpyloridis on individual biop-sies was, however, significant (Table 2). In active gas-tritis the neutrophils were predominantly between
864

Local immune response to gastric Campylobacter in non-ulcer dyspepsia 865
M
4%~~~~~~~~~~4
L~~~~~~~~~~~~~~~~~~~~~4.cAJ~~~"
a~~~~~t4~~4
ir~~~~
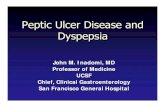
Fig. 2 Mucosal biopsyfrom gastric body stained by indrectibmmunoperoxedase techniquefor IgA. (a) (b) Cpyloridis ofcharacteristic morphology are present on and above surface; these score + + for IgA labelling. (c) A gastric pit in same case;IgA positive Cpyloridis are present on surface and in upper pit; unlabelled organisms are present in deep pit (open arrow).Original magnification (a) x 80: (b) and (c) x 320.

Wyatt, Rathbone, Heatley
S.
::t ~
*:
:b
I}* *
AI4
.4.
A _..w~~~~~~~~~~~~A
_
_L_"S
._>.E.
_ez=_^ ...-
Fig. 3 Antral mucosa stainedfor IgA and IgG. (a) Cpyloridis strongly positivefor IgA (+ +) are present on surface, whilethose in gastric pit are weakly positive ( + ) (arrow). (b) IgG+ + organisms are present on surface and IgG + in upper pit.Unlabelled Cpyloridis are present in deeper part ofpit (open arrow). Original magnificazion x 320.)
.4
Air
Il::/ 11
I -~
.:1:
-f^ NA
r0-*.Al
t:,
0
i
866

Local immune response to gastric Campylobacter in non-ulcer dyspepsia
Table 1 Prevalence ofchronic gastritis and Cpyloridis in 141 patients with non-ulcer dyspepsia
Age Total Normal gastric mucosa Chronic gastritis Chronic gastritisCpylori&s absent Cpyloridis absent Cpyloridis present
<20 11 6 0 521-30 29 18 1 1031-40 22 13 2 741-50 24 4 1 195140 25 12 1 1261-70 20 5 2 1371-80 10 0 2 8
Table 2 Presence ofCpyloridis related to activity in 144biopsy specimens showing chronic gastritis
Gastritis Cpyloridis
Active 95 14Inactive 22 13 p < 0 001
epithelial cells rather than in the lumen of gastricglands (a pattern reminiscent of infective colitis'6),and were most numerous in the deep portion of thepits.
Table 3 shows the histological diagnoses in the 30pairs of biopsy specimens studied in detail. The speci-mens were of full thickness mucosa, with a meannumber of 31-44 (SD 11-63) gastric pits per biopsy.The 30 cases included three with normal antral andbody mucosae with no bacteria, included as negativecontrols. All of the remaining 54 biopsy specimensshowed Cpyloridis colonisation; those of activelyinflamed mucosa, however, carried a significantlygreater population density ofcolonising bacteria thanthose showing inactive gastritis or normal mucosa
(p = 010022) (Fig. 4).Cpyloridis labelled by anti-IgA and anti-IgM were
easily identified; background staining of gastricmucus in active gastritis occurred with anti-IgG, butlabelled Cpyloridis could still be confidently detected.Unlabelled organisms were apparent due to theirfaint haematoxyphilia in areas of mucosa in whichimmunoperoxidase positive Cpyloridis were sparse or
absent. The anti-Ig labelled Cpyloridis were alwaysless numerous than those apparent on the Warthin-Starry stain, suggesting that only a proportion of theorganisms were coated by host immunoglobulin. In
all sections examined immunoperoxidase negativeCpyloridis could be seen at the depths of the gastricpits.The pattern of immunoperoxidase positivity of
Cpyloridis for the three antibody classes in activegastritis was different to that in inactive gastritis andnormal mucosa (Fig. 5). Numerous Cpyloridis, whichwere positive for IgG or IgM, or both, were presenton the surface of 25 of 29 active gastritis biopsy speci-mens, but rarely seen on the others (6 of 25,p < 0O001). IgA positive Cpyloridis were alwayspresent on the mucosal surface in active gastritis andwere usually seen within pits. In the inactive and nor-mal groups IgA positive Cpyloridis were found on thesurface in 60% of cases, but were less commonlyfound within the gastric pits.No immunoperoxidase stained organisms were
seen on the three pairs of biopsy specimens from nor-mal patients, or in the negative control slides. Sec-tions from the adhesion study provided a usefulnegative control; Cpyloridis were also unstained byimmunoperoxidase for IgA, IgG, and IgM.
Dicsson
We propose that the immunoperoxidase labelling ofmucosal Cpyloridis by anti-IgA, IgG, and IgM is dueto the in vivo adsorption of specific host antibodies onto the bacteria. Other workers have used similar tech-niques to detect in vivo adsorbed antibody on oralbacterial7 and on Legionella pneumophila.'8 We havepreviously shown the presence of anti-Cpyloridis IgAand IgM in the gastric juice ofcolonised subjects. Thecharacteristic morphology, position, and populationdensity of Cpyloridis on the mucosal surface in tissuesections' allowed the immunoperoxidase positiveorganisms to be identified with confidence. This posi-
Table 3 Histological diagnoses in 30paired biopsy specimensfor inmtnoperoxidase study
Active chronic Inactive chronic Normal (inchldes threegastritis gastritis negative control cases)
Antral mucosa 22 5 3Body mucosa 7 6 17
867

86810
9-
8-
0d
CD.X6-0
o.
.= 5-
4
3
0
0
0@@
I
Active gastritis(n =29)
__
Inactive gastritis
and normal mucosa
(n=25)
Fig. 4 Density ofcolonising Cpyloridis in biopsy specimensshowing active gastritis compared with that of inactivegastritis and normal mucosa (p = 0 0022).
tivity is unlikely to be due to a non-specific cross
reaction as some unlabelled Cpyloridis were alsopresent in each section.
Lymphocytes and plasma cells are sparse in thelamina propria of the normal stomach, and an
increase in their number is the principal criterion forthe histological diagnosis of chronic gastritis.12 Inter-estingly, the intestinal mucosa of neonates and germfree animals is similarly devoid of mononuclear cellsbefore contact with luminal antigens. 9 The mainclass of antibody present in mucosal secretions isdimeric IgA, which is produced locally by plasmacells in the lamina propria and transported from theinterstitium to the lumen by secretory component, a
protein synthesised by the epithelial cells.20 Thissecretory mechanism, which is apparently inactive inthe normal stomach, has been shown in inflamedgastric mucosa, together with the secretion oflysozyme 3 and lactoferrin. 4 The mucosal plasmacells throughout the gastrointestinal tract are pre-dominantly of IgA class,19 although an increase in theIgG and IgM plasma cell population occurs during
Wyatt, Rathbone, Heatleythe active phase in various inflammatory condi-tions,21-23 including chronic gastritis.24 The IgGappears in secretions during active inflammation bymeans of a non-specific increase in transudation ofserum proteins across the inflamed epithelium."We detected coating of Cpyloridis by host IgA in
all cases with active gastritis and in many with inac-tive gastritis, a finding in accordance with the prepon-derance of IgA in mucosal secretions. IgA protectsthe mucosa by interfering with the adhesion oforganisms to the epithelial surface.26 It has alsorecently been shown to be capable of inducing anti-body dependent cell mediated activity against entero-pathogenic bacteria.27 IgA does not, however,opsonise or fix complement and therefore does notenhance neutrophil phagocytosis of coatedorganisms. This is in keeping with our observation ofIgA coated Cpyloridis, irrespective of the presence ofa neutrophil infiltrate in the mucosa. IgG and IgMcoated Cpyloridis were observed almost exclusivelyon actively inflamed mucosae. Both these antibodiesfix complement, with IgG also opsonising bacteria;thus both would be expected to enhance neutrophilactivity against Cpyloridis. Other authors haveobserved phagocytosed Cpyloridis in neutrophils onthe mucosal surface.4 This association of active gas-tritis with the presence of IgM and IgG coatedCpyloridis is therefore corroborative evidence thatthe inflammatory response may, indeed, be elicited bythis organism.The consistent observation of unlabelled
Cpyloridis deep in the gastric pits is of considerableinterest. Although the self induced Campylobactergastritis of Marshall resolved spontaneously by thefourteenth day,7 colonisation by organisms has beenshown to persist for at least four months in asymp-tomatic subjects.28 Indeed, the prevalence ofCpyloridis in patients of all ages and with all grades ofchronic gastritis suggests that colonisation, onceestablished, may persist indefinitely. The host'simmune response is therefore not effective in eradi-cating the organism. In their ecological niche deep inthe gastric pits, Cpyloridis may evade contact withhost immunoglobulin, at least in a concentrationsufficient to be detected by our immunoperoxidasetechnique. The alternative explanation for theirpersistence-that Cpyloridis are merely commensalsin the inflamed stomach-seems unlikely in view ofthe systemic antibody response in colonisedsubjects2 15 and their association with activity of gas-tritis, an observation recently confirmed by electronmicroscopy.29We do not yet know the clinical importance of
Cpyloridis in the pathogenesis of chronic gastritis.The immune mechanisms of the stomach areequipped to combat a luminal antigen, and the histo-

Local immune response to gastric Campylobacter in non-ulcer dyspepsia
Active gastritis(n-29)
Inactive gastritisor normal
I (n=25)IgM Active gastritis Inactive/normal
(n=29) (n=25)
Surface
Upper pit
Deep pit
Inactive /normalI (n= 25)
+
Lii-Fig. 5 Immunoperoxidase labelling of Cpyloridis present on surface and in upper and deep gastric pits by anti-IgA, IgG,and IgM.
logical features of chronic gastritis are consistent withthose of a response to chronic infection. We havepresented evidence for the in vivo coating ofCpyloridis by host antibody, the class of which varieswith the activity of the gastritis. A chronic infectionby Cpyloridis, therefore, offers a plausible expla-nation for the histological and immunopathologicalfeatures observed in type B chronic gastritis.
We thank Miss Sally Grey and Mr Declen Lunny fortechnical help, Dr MF Dixon for his helpful sug-gestions, and Mrs C Mann and Mrs J Fearnley forsecretarial help.
Referenmes
'Warren JR, Marshall B. Unidentified curved bacilli on gastricepithelium in active chronic gastritis. Lancet 1983;i: 1273-5.
2Jones DM, Lessells AM, Eldridge J. Campylobacter-like organismson the gastric mucosa: culture, histological and serological stud-ies. J Clin Pathol 1984;37:1002-6.
3Langenberg ML, Tytgat GNJ, Schipper MEI, Reitra PJGM,Zanen HC. Campylobacter-like organisms in the stomach ofpatients and healthy individuals. Lancet 1984;i:1348.
'Lee WK, Gourley WK, Buck GE, Subramanyam K. A light andelectron microscopic study of a campylobacter-like bacteriainhabiting the human stomach. Gastroenterology 1985;88:1470.
'Anonymous. Validation of the publication of new names and new
combinations previously effectively published outside the IJSB.Int J Syst Bacteriol 1985;35:223-5.
'Marshall BJ, Warren JR. Unidentified curved bacilli in the stomachof patients with gastritis and peptic ulceration. Lancet1984;i:131 1-4.
7Marshall BJ, Armstrong JA, McGechie DB, Glancy RJ. Attemptto fulfil Koch's postulates for pyloric campylobacter. Med JAust 1985;142:436-9.
8Lambert JR, Hansky J, Davidson A, Pinkard K, Stockman K.Campylobacter-like organisms (CLO)-in vivo and in vitro sus-
ceptibility to antimicrobial and antiulcer therapy. Gastro-enterology 1985;88:1462.
9Thomas JM. Campylobacter-like organisms in gastritis. Lancet1984;ii: 1217.
t0Giannella RA, Broitman SA, Zamcheck N. Gastric acid barrier toingested micro-organisms in man: studies in vivo and in vitro.Gut 1972;13:251-6.
"Gibbons RJ. Review and discussion of the role of mucus inmucosal defence. In: Strober W, Hanson LA, Sell KW, eds.Recent advances in mucosal immunity. New York: Raven Press,1982:343-51.
'2Whitehead R. Mucosal biopsy of the gastrointestinal tract. 3rd ed.Philadelphia: WB Saunders, 1984.
'3Isaacson P. Immunoperoxidase study of the secretory immu-noglobulin system and lysozyme in normal and diseased gastricmucosa. Gut 1982;23:578-88.
"Valnes K, Brandtzaeg P, Elgjo K, Stave R. Specific and non-
specific humoral defence factors in the epithelium of normal andinflamed gastric mucosa. Gastroenterology 1984;86:402-12.
Rathbone BJ, Wyatt JI, Worsley BW, et al. Systemic and localantibody responses to gastric Campylobacter pyloridis in non-
ulcer dyspepsia. Gut 1986:27:642-7.1"6Price AB, Day DW. Pseudomembranous and infective colitis. In:
Recent advances in histopathology. Vol 11. Edinburgh: ChurchillLivingstone, 1981:99-117.
'7 Brandtzaeg P, Fjellanger I, Gjeruldsen ST. Adsorption of immu-noglobulin A on to oral bacteria in vivo. J Bac-teriol 1968;
Surface
Upper pit
Deep pit
IgG Active gastritis(n= 29)
Surface
Upper pit
Deep pit
a i
i
869

87096:242-9.
18 Boyd JF, McWilliams E. Immunoperoxidase staining of Legion-ella pneumophila. Histopathology 1982;6:191-6.
19Tomasi TB, Grey HM. Structure and function of immunoglobulinA. Progress in Allergy 1972;16:81-213.
2"Solari R, Kraehenbuhl JP. The biosynthesis of secretory com-ponent and its role in the transepithelial transport of IgA dimer.Immunology Today 1985;6:17-20.
21Rosekrans PCM, Meijer CJLM, Van Der Wal AM, Comelisse CJ,Lindeman J. Immunoglobulin containing cells in inflammatorybowel disease of the colon: a morphometric and immu-nohistochenical study. Gut 1980;21:941-7.
22 Brandtzaeg P, Baklien K, Fausa 0, Hoel PS. Immuno-histochemical characterisation of local immunoglobulinformation in ulcerative colitis. Gastroenterology1974;66:1 123-36.
23Keren DF, Appelman HD, Dobbins WO, et al. Correlation of his-topathologic evidence of disease activity with the presence ofimmunoglobulin-containing cells in the colons of patients withinflammatory bowel disease. Hum Pathol 1984;15:757-63.
24Van Spreeuwel JP, Lindeman J, Van Maanen J, Meyer CJLM.
Wyatt, Rathbone, HeatleyIncreased numbers of IgE containing cells in gastric and duo-denal biopsies. An expression of food allergy secondary tochronic inflammation? J Clin Pathol 1984;37:601-6.
25Jonard PP, Rambaud JC, Dive C, Vaerman JP, Galian A,Delacroix DL. Secretion of immunoglobulins and plasma pro-teins from the jejunal mucosa. J Clin Invest 1984;74:525-35.
26Williams RC, Gibbons RJ. Inhibition of bacterial adherence bysecretory immunoglobulin A: a mechanism of antigen disposal.Science 1972;177:697-9.
27Tagliabue A, Boraschi D, Villa L, etal. IgA-dependent cell-mediated activity against enteropathogenic bacteria: distribu-tion, specificity and characterisation of the effector cells.J Immunol 1984;133:988-92.
28Tytgat GNJ, Langenberg ML, Rauws E, Rietra PJGM.Campylobacter-like organisms in the human stomach. Gastro-enterology 1985;88:1620.
29Steer HW. The gastro-duodenal epithelium in peptic ulceration.J Pathol 1985;146:355-62.
Requests for reprints to: Dr JI Wyatt, Department ofPathology, University of Leeds, L=eds LS2 9JT.