Treatment of Multidrug-resistant and Extensively Drug-Resistant Tuberculosis - Prof. G.B. Migliori
Upload
bushra-hasan-khanCategory
view
35download
0
PULMONARY TUBERCULOSIS
Dr. Bushra Hasan Khan
Department of Pharmacology
JNMC, AMU, Aligarh.
• Tuberculosis is a global pandemic
• TB is second leading cause of death from
a single infectious agent, after HIV.
• INCIDENCE : 9 million new cases in 2013
• MORTALITY : A total of 1.5 million people died
from TB in 2013 (including 360 000 people with HIV)
• TB is a leading killer of HIV-positive people
causing one fourth of all HIV-related deaths.
• 480 000 people developed MDR-TB in 2013.
• In 2012, out of the estimated global annual incidence
of 8.6 million TB cases, 2.3 million were estimated
to have occurred in India.
• The TB mortality rate has decreased 45% since 1990.
• About 37 million lives were saved worldwide between 2000
and 2013 through TB diagnosis and treatment
• The world is on track to achieve the global TB target
set for 2015 in the Millennium Development Goals
• The target for TB in the MDGs is to halt and
reverse global incidence.
• 86% of people who developed TB and were
put on treatment in 2012 were successfully treated.
(http://www.tbcindia.nic.in/rntcp.html)
ETIOLOGY
• TB is caused by Mycobacterium tuberculosis, a slow-growing
obligate aerobe and a facultative intracellular
parasite.
• Non-spore-forming, rod-shaped, 0.5μm × 3μm
• Neutral on Gram's staining
• The organism grows in parallel groups called cords
in which acid-fast bacilli are arranged in parallel chains .
• Cord formation is correlated with virulence.
• Mycobacteria are rich in lipids
– Mycolic acid prevent attack of cationic proteins,
lysozyme, and oxygen radicals in the phagocytic granule
– Waxes
– Phosphatides
• Lipids are bound to proteins and polysaccharides.
• Muramyl dipeptide + mycolic acids granuloma formation;
phospholipids caseous necrosis.

• Once stained, the bacilli cannot be decolorized by
acid alcohol acid-fast bacilli (AFB)
• Acid fastness is due mainly to the organisms'
– High content of mycolic acids,
– Long-chain cross-linked fatty acids ,
– Other cell-wall lipids.
• Mycolic acids + Arabinogalactan and Peptidoglycan
results in very low permeability of the cell wall
effectiveness of most antibiotics is reduced.
• Lipoarabinomannan
involved in the pathogen-host interaction
facilitates the survival of M. tuberculosis within macrophages.
PHARMACOLOGICAL BARRIER:
Cell wall Mainly contains Lipids (Mycolic acid)
Efflux pumps pump out harmful chemicals
Propensity to hide inside the host cells
CLINICAL FEATURES
• Fever
• Weight loss / anorexia
• Cough
• Hemoptysis
• Chest pain
• Night sweats
• Fatigue

DIAGNOSIS
• History
• Physical examination
• Radiology
• Sputum microscopy
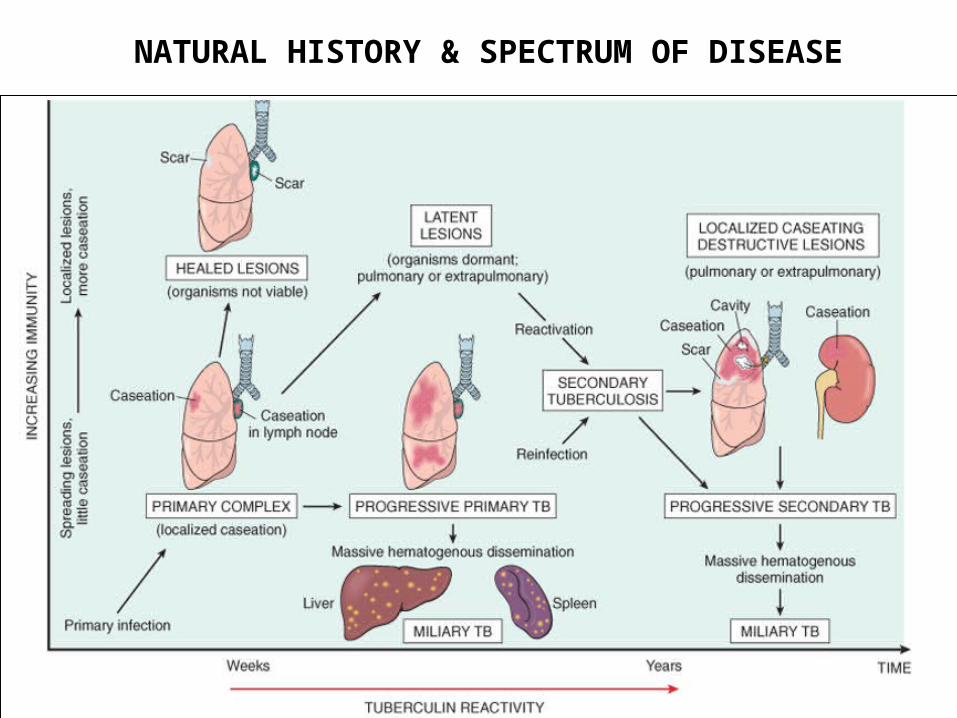
NATURAL HISTORY & SPECTRUM OF DISEASE
AIMS OF TREATMENT
• To cure the patient ; restore quality of life & productivity
• To prevent death from active TB or its late effects
• To prevent relapse of TB
• To reduce transmission of TB to others
• To prevent the development & transmission of drug resistance
RNTCP
• RNTCP ( Revised National Tuberculosis Control Programme)
is an application of WHO recommended strategy of DOTS in
India.
• Objectives:
1- Detecting at least 70% of sputum positive TB patients in
the community.
2- Curing at least 85% of the newly detected sputum positive
cases.
Five components of DOTS:
1. Political commitment with increased & sustained financing
2. Case detection through quality-assured bacteriology
3. Standardized treatment with supervision & patient support
4. Regular, uninterrupted supply of Anti-TB drugs
5. Monitoring & evaluation system & impact measurement
Stop TB Strategy (WHO, 2006)
1. Pursue high-quality DOTS expansion & enhancement
2. Address TB-HIV, MDR-TB, & the needs of poor &
vulnerable populations
3. Contribute to health system strengthening based on
primary health care
4. Engage all health care providers
5. Empower people with TB, & communities through partnership
6. Enable & promote research
• Based on the nature/severity of the disease & the
patient's exposure to previous ATTs, RNTCP classifies
TB patients into 2 t/t categories
– NEW
– PREVIOUSLY TREATED
NEW PATIENT CATEGORY
• New sputum smear-positive,
• New sputum smear-negative,
• New extrapulmonary tuberculosis,
PREVIOUSLY TREATED
• Sputum smear-positive relapse,
• Sputum smear-positive failure,
• Sputum smear-positive treatment after default,
• Others (patients who are Sputum Smear-Negative
or who have Extra-pulmonary disease who can have
recurrence)
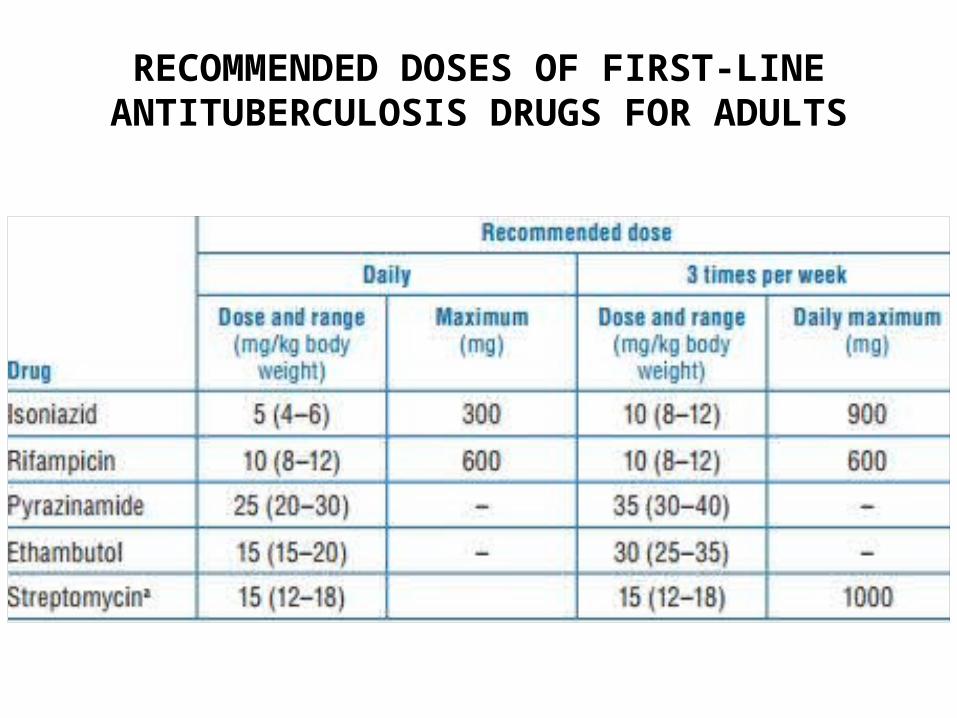
RECOMMENDED DOSES OF FIRST-LINE ANTITUBERCULOSIS DRUGS FOR ADULTS
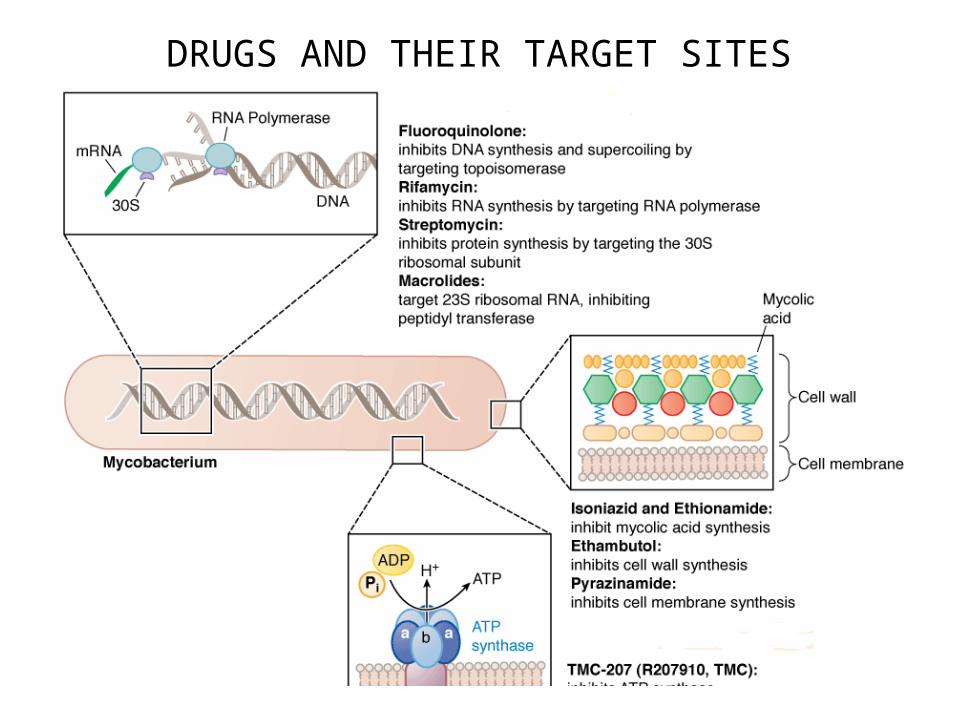
DRUGS AND THEIR TARGET SITES
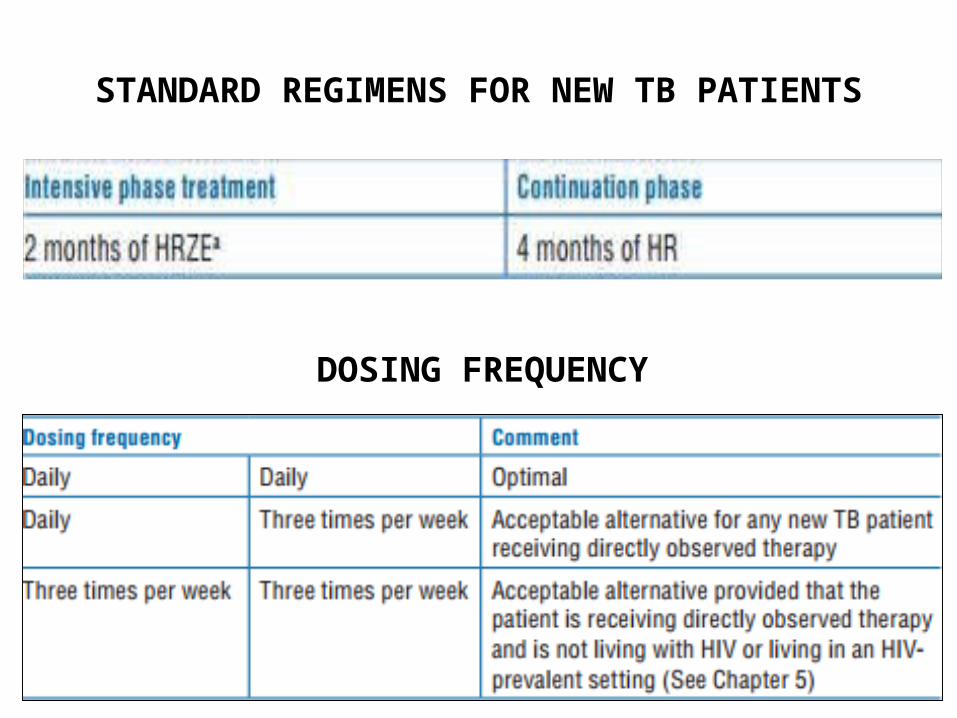
STANDARD REGIMENS FOR NEW TB PATIENTS
DOSING FREQUENCY
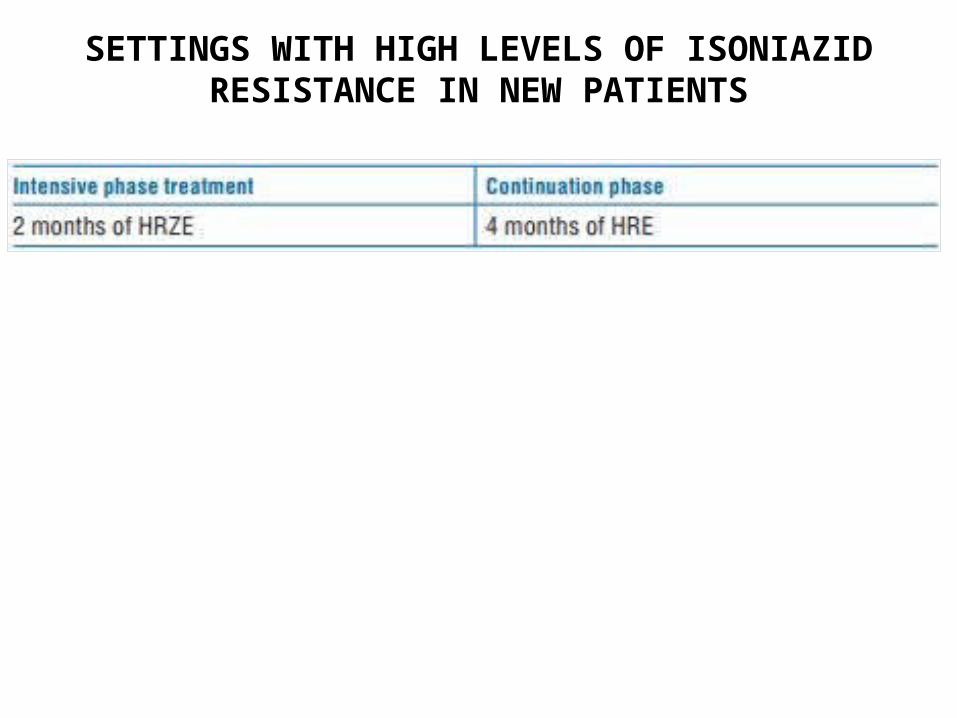
SETTINGS WITH HIGH LEVELS OF ISONIAZID RESISTANCE IN NEW PATIENTS
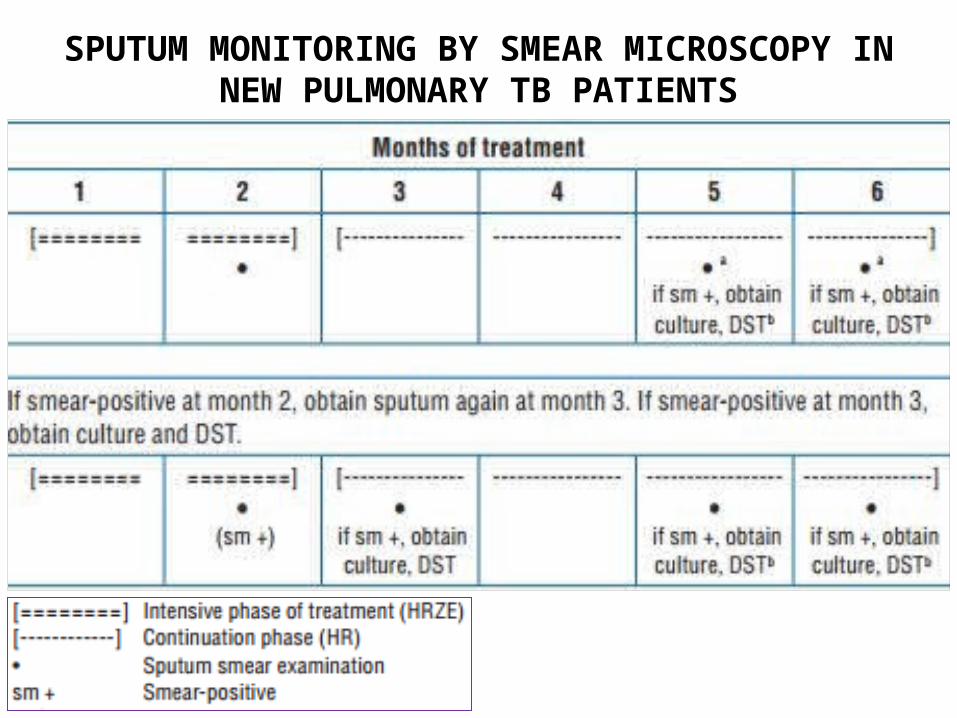
SPUTUM MONITORING BY SMEAR MICROSCOPY IN NEW PULMONARY TB PATIENTS

STANDARD REGIMENS FOR PREVIOUSLY TREATED PATIENTS
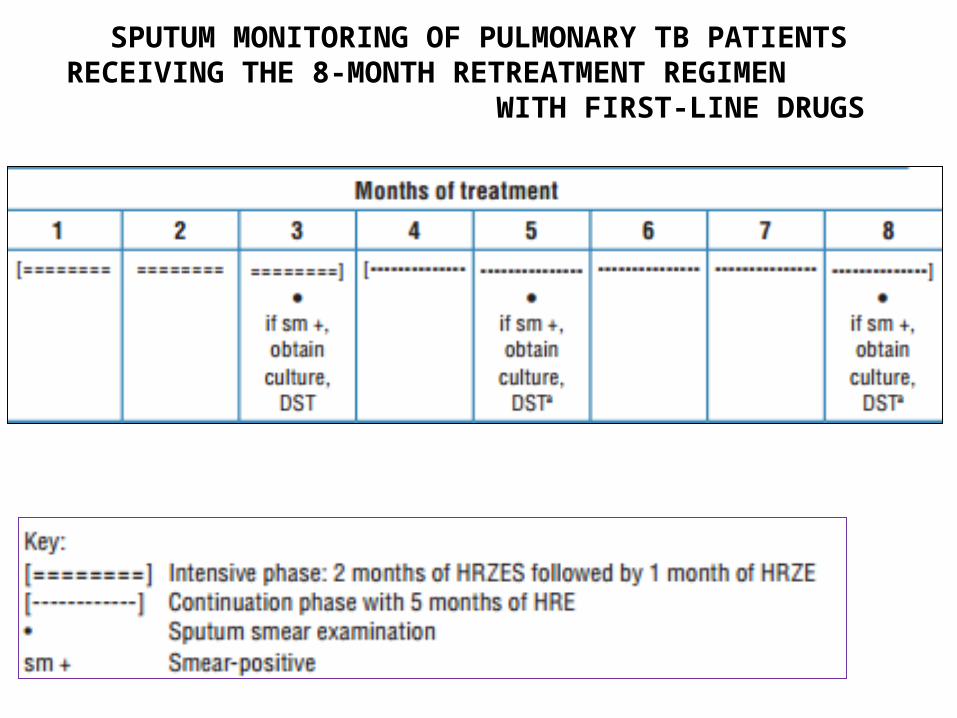
SPUTUM MONITORING OF PULMONARY TB PATIENTS RECEIVING THE 8-MONTH RETREATMENT REGIMEN
WITH FIRST-LINE DRUGS

A POSITIVE SPUTUM SMEAR AT THE END
OF THE INTENSIVE PHASE
• Poorly supervised initial phase of t/t & poor patient adherence
• Poor quality of anti-TB drugs
• Doses of anti-TB drugs below the recommended range
• Slow resolution extensive cavitation & a heavy initial
bacillary load
• Co-morbid conditions
• MDR-TB that is not responding to first-line treatment
• Non-viable bacteria remain visible by microscopy
COHORT ANALYSIS OF TREATMENT OUTCOMES
• COHORT a group of patients diagnosed & registered
for t/t during one-quarter of a year
• Evaluation of t/t outcome in new pulmonary smear-positive
patients major indicator of programme quality.
• Outcomes in other patients
(retreatment, pulmonary smear-negative, extrapulmonary)
are analysed in separate cohorts.

• Outcomes are routinely evaluated at the beginning
of the quarter following the completion of treatment
by the last patient in that cohort.
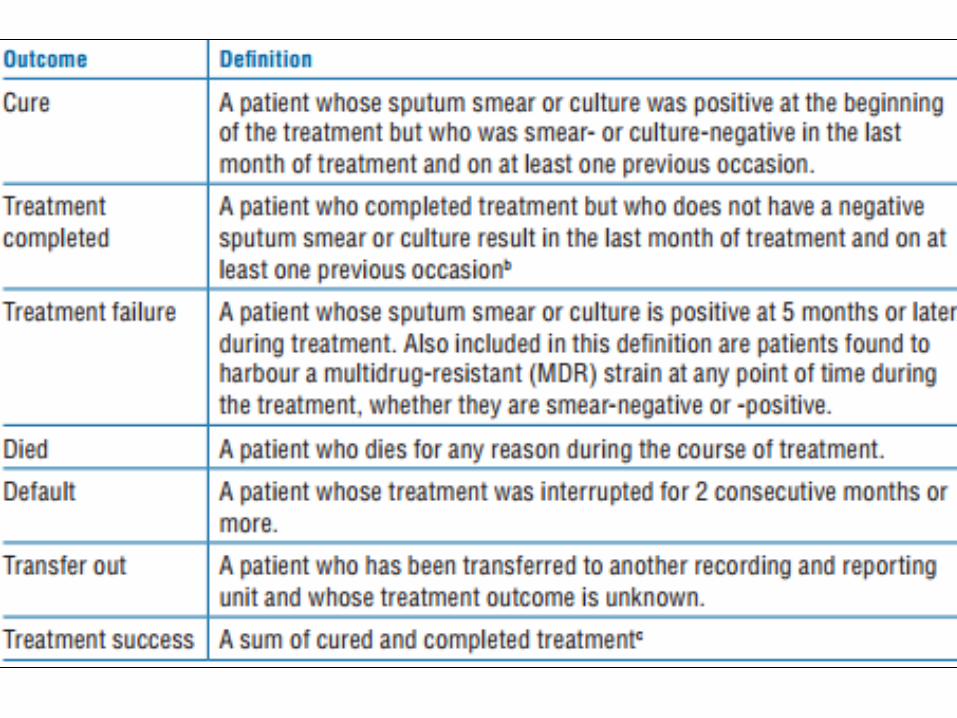
TREATMENT OUTCOMES
• CURED
• TREATMENT COMPLETED
• TREATMENT FAILURE
• DIED
• DEFAULT
• TRANSFER OUT
• TREATMENT SUCCESS
MANAGEMENT OF TREATMENT INTERRUPTION
• If a patient misses an arranged appointment to receive
treatment the NTP should ensure that the patient is
contacted within a day after missing treatment during the
initial phase, & within a week during the continuation phase.
• Culture and DST should be performed upon return of patients
who meet the definition for default
MAJOR ADVERSE EFFECTS OF ATT
• The most common ADR is Hepatitis.
• Cutaneous reactions
• Shock, purpura
• Visual impairment
• Deafness, dizziness
• Acute renal failure
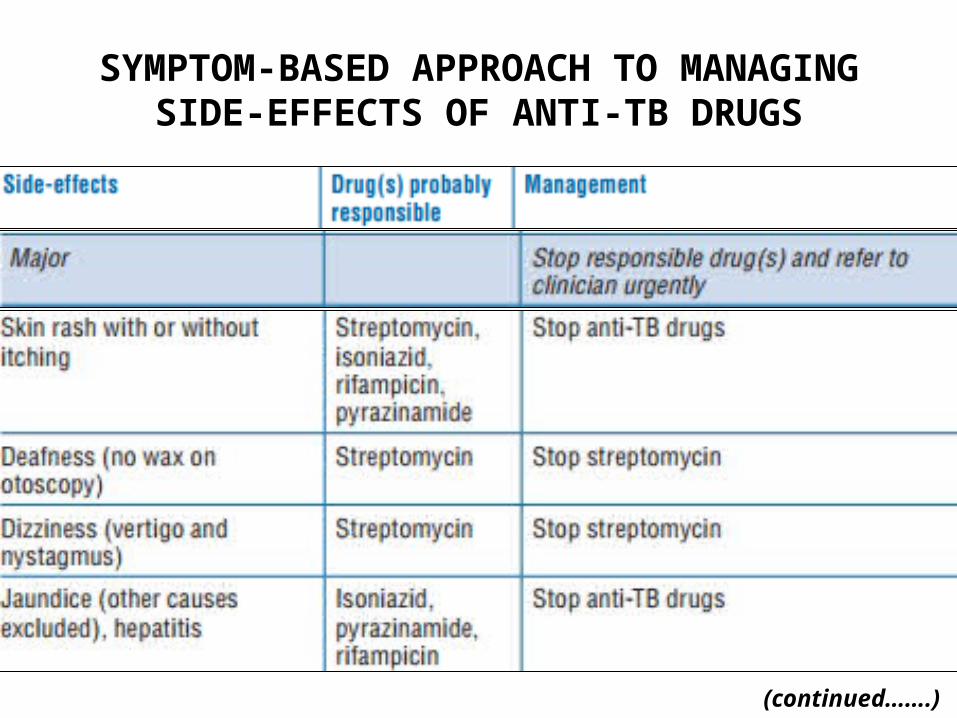
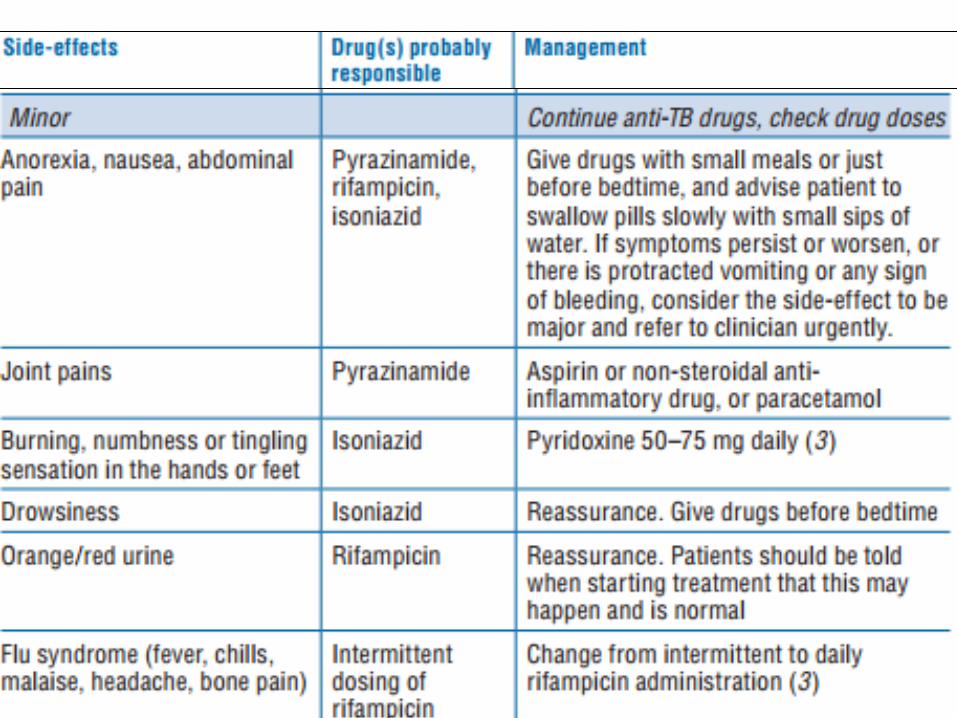
SYMPTOM-BASED APPROACH TO MANAGING SIDE-EFFECTS OF ANTI-TB DRUGS
(continued…….)
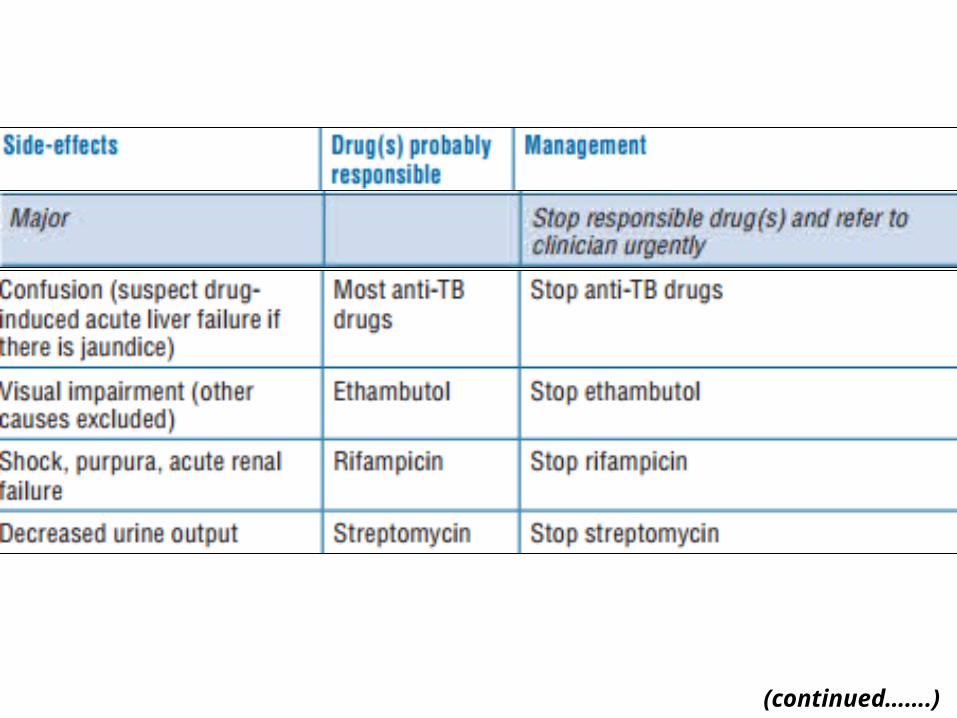
(continued…….)
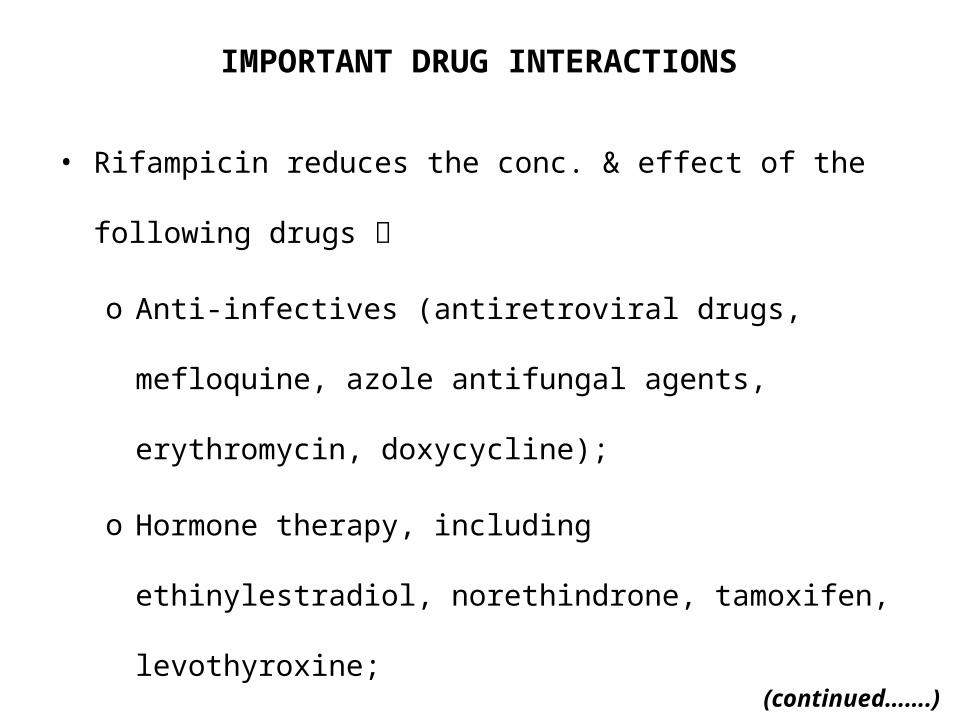
IMPORTANT DRUG INTERACTIONS
• Rifampicin reduces the conc. & effect of the following drugs
o Anti-infectives (antiretroviral drugs, mefloquine, azole
antifungal agents, erythromycin, doxycycline);
o Hormone therapy, including ethinylestradiol, norethindrone,
tamoxifen, levothyroxine;
o CVS drugs including digoxin, digitoxin, verapamil,
nifedipine, diltiazem, propranolol, metoprorol, enalapril,
losartan;(continued…….)

o Anticonvulsants (including phenytoin);
o Haloperidol, quetiapine, benzodiazepines (including
diazepam, triazolam), zolpidem, buspirone;
o Warfarin;
o Cyclosporin;
o Corticosteroids;
o Theophylline;
o Sulfonylurea hypoglycaemics;
o Hypolipidaemics including simvastatin and fluvastatin;
T/T REGIMENS IN SPECIAL SITUATIONS
• Pregnancy & Lactation
• Liver disorders
• Renal failure
PREGNANCY AND BREASTFEEDING
• Streptomycin ototoxic to the fetus ; must not be used
• Lactation is not a C/I to ATT
• After active TB in the baby is ruled out, the baby should be
given 6 months of Isoniazid preventive therapy, followed by
BCG vaccination
• Pyridoxine supplementation is recommended for all pregnant
or breastfeeding women taking Isoniazid
LIVER DISORDERS
• Patients with the following conditions can receive the usual
TB regimens provided that there is no clinical evidence of
chronic liver disease:
Hepatitis virus carriage,
A past history of acute hepatitis,
Current excessive alcohol consumption
• Hepatotoxic reactions to anti-TB drugs more common
among these patients & should therefore be anticipated

• In patients with unstable or advanced liver disease, LFTs
should be done at the start of treatment, if possible.
• The more unstable or severe the liver disease is,
the fewer hepatotoxic drugs should be used.
• If the serum ALT level is more than 3 times normal before the
initiation of treatment, the following regimens should be
considered.
(continued…….)
POSSIBLE REGIMENS INCLUDE:
• Two hepatotoxic drugs
9 months of Isoniazid and Rifampicin, plus Ethambutol (until
or unless Isoniazid susceptibility is documented);
2 months of Isoniazid, Rifampicin, Streptomycin &
Ethambutol, followed by 6 months of Isoniazid & Rifampicin;
6–9 months of Rifampicin, Pyrazinamide and Ethambutol.
• One hepatotoxic drug:
2 months of Isoniazid, Ethambutol & Streptomycin,
followed by 10 months of Isoniazid & Ethambutol.
• No hepatotoxic drugs:
18–24 months of Streptomycin, Ethambutol &
a Fluoroquinolone.

RENAL FAILURE
• The recommended initial TB t/t regimen :
– 2 months of Isoniazid, Rifampicin, Pyrazinamide &
Ethambutol, followed by 4 months of Isoniazid & Rifampicin.
• There is significant renal excretion of Ethambutol and
metabolites of Pyrazinamide, & doses should therefore be
adjusted.
• Three times/week administration of Pyrazinamide (25 mg/kg),
& Ethambutol (15 mg/kg) is recommended
• While receiving Isoniazid, patients with severe renal
insufficiency or failure should also be given Pyridoxine in
order to prevent peripheral neuropathy.
• Because of an increased risk of nephrotoxicity & ototoxicity,
Streptomycin should be avoided in patients with renal failure.
• If Streptomycin must be used, the dosage is 15 mg/kg,
two or three times/week, to a maximum of 1 gram per dose, &
serum levels of the drug should be monitored.


• MAIN FIRST LINE ANTITUBERCULAR DRUGS
– ISONIAZID
– RIFAMPICIN
– ETHAMBUTOL
– PYRAZINAMIDE
• OTHER FIRST LINE ANTITUBERCULAR DRUGS
– RIFABUTIN
– RIFAPENTINE
– STREPTOMYCIN

SECOND-LlNE ANTI-TB DRUGS
• Fluoroquinolones– Levofloxacin– Moxifloxacin– Gatifloxacin
• Injectable Agents– Capreomycin– Amikacin– Kanamycin
• Others– Cyclosrine– PAS – Ethionamide– clofazimine
NEWER ANTl-TB DRUGS
• Oxazolidinones Linezolid
• Amoxicillin-Clavulanate
• Carbapenems
• Diarylquinolines Bedaquiline
• Nitroimidazoles Delamanid
• Diamines SQ109 (an Ethambutol analogue)
• Pyrroles LL3858
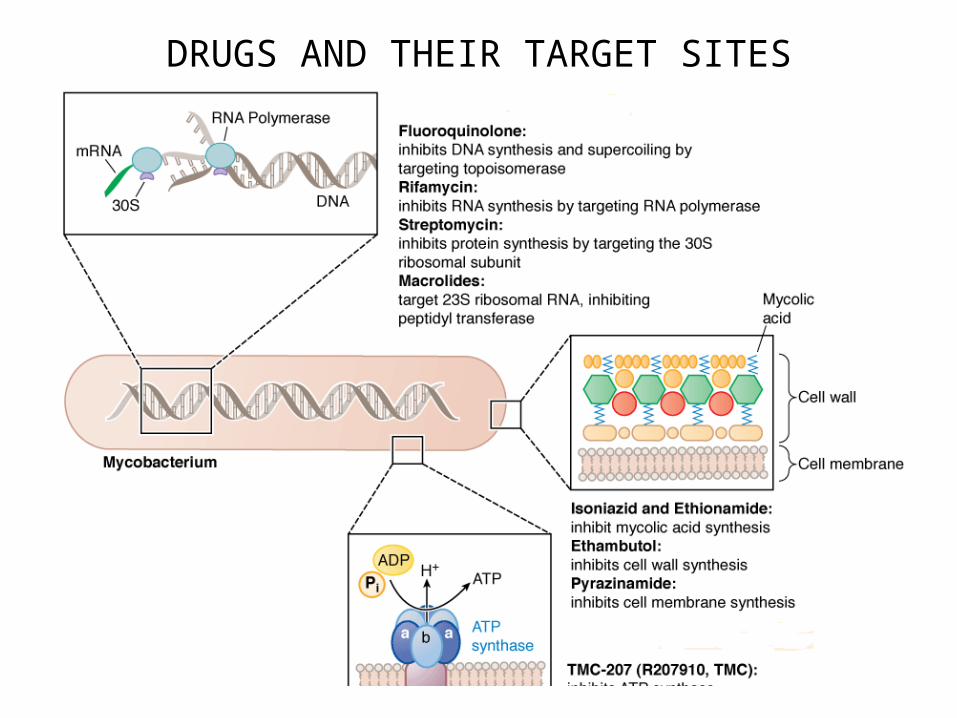
DRUGS AND THEIR TARGET SITES
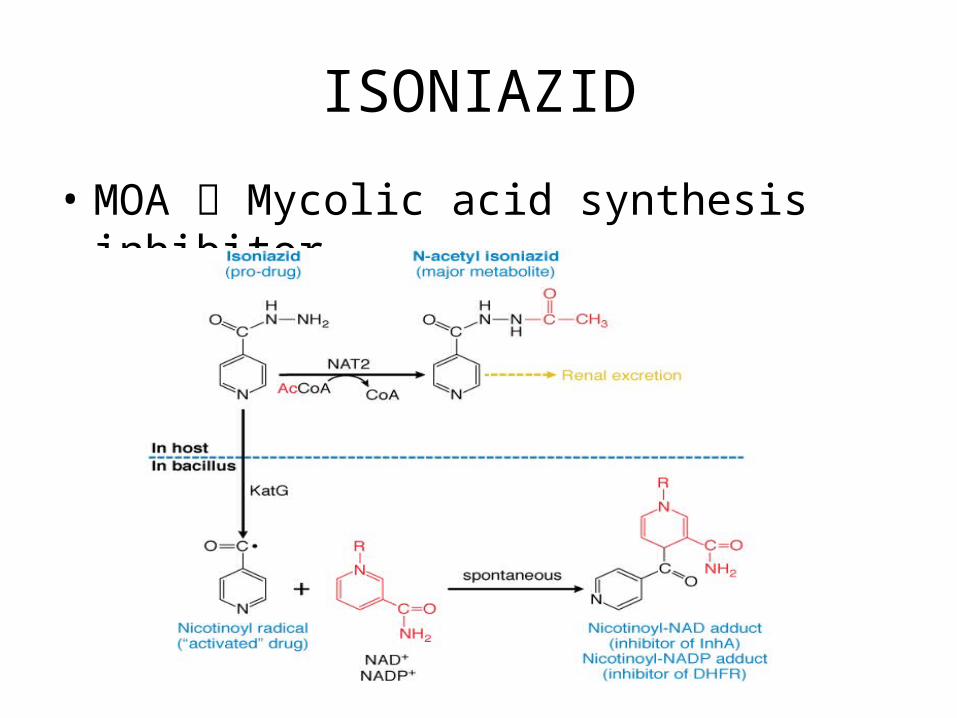
ISONIAZID
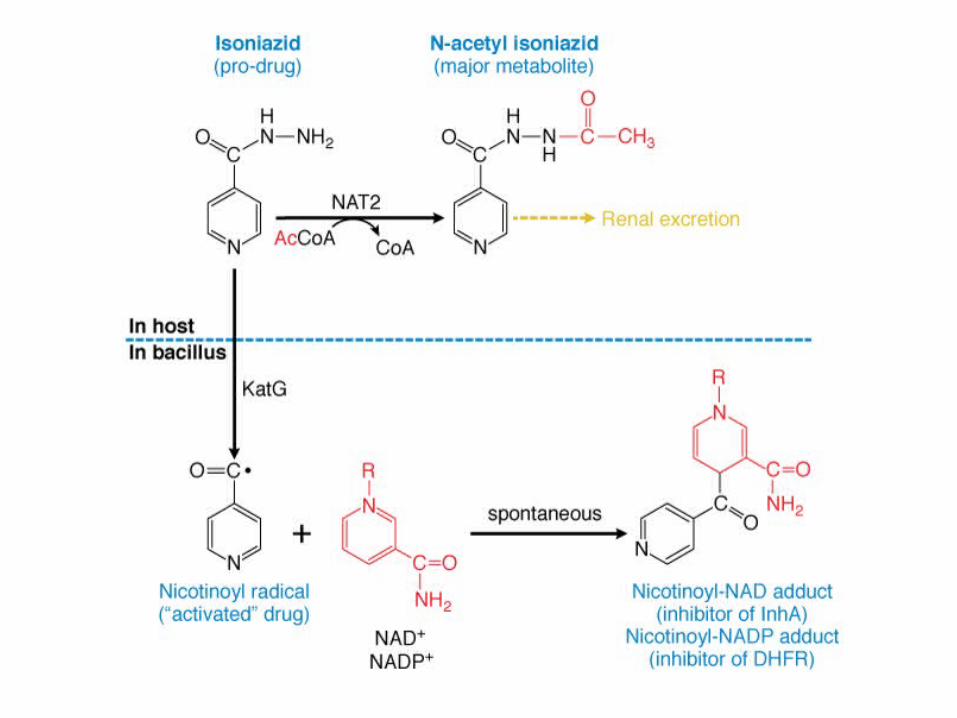
• MOA Mycolic acid synthesis inhibitor
Nicotinoyl-NAD adduct→
inhibits the activities of enoyl-ACP reductase (inhA) &
β-ketoacyl acyl carrier protein synthase (KasA)→
interfere with mycolic acid synthesis.
Nicotinoyl-NADP adduct→ inhibit mycobacterial dihydrofolate
reductase (DHFRase)→ interfere with
nucleic acid synthesis.
MECHANISM OF RESISTANCE:
• Mutation or deletion of katG gene (MC).
• Mutation in kasA gene.
• Over-expression of the inhA & aphC gene (detoxify organic
peroxide)
PHARMACOKINETICS:
• Oral BA ~ 100%.
• Only ~10% is protein bound.
• Metabolised in liver by Arylamine N-acetyltransferase2 (NAT2).
• Excreted in urine as Acetylisoniazid & Isonicotinic acid.
DOSE:
• 5mg/kg (4-6 mg/kg) daily, maximum 300 mg
• 10 mg/kg (8-12 mg/kg) three times/week; maximum 900 mg
• Oral / im / iv
ADRs:
• Peripheral neuritis : INH binds with Pyridoxal 5-phosphate →
decreased neuronal Pyridoxal 5-phosphate
• Liver damage : Acetylisoniazid→ Acetylhydralazine Liver
damage
• Others : Optic neuritis, Convulsions, Hypersensitivity reactions
DRUG INTERACTIONS:
• Al(OH)3 inhibit INH absorption.
• With Acetaminophen → Hepatotoxicity
• With Carbamazepine, Diazepam, Ethosuximide
Neurological & Psychiatric toxicities by inhibiting CYP3A
• With Isoflurane, Enflurane decrease their effectiveness by
inducing CYPE1
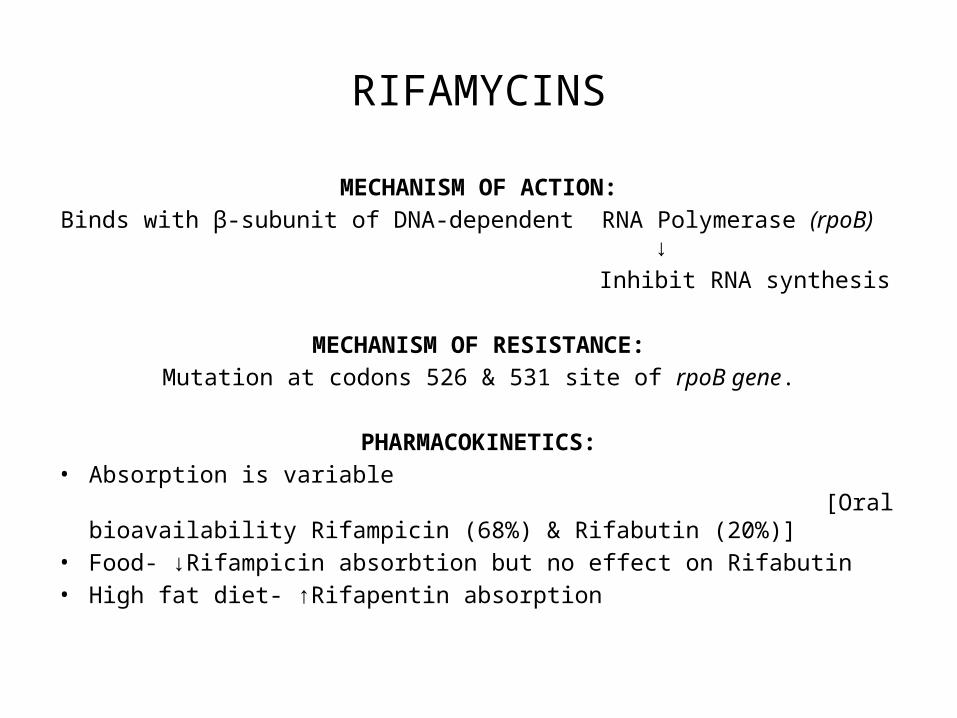
RIFAMYCINS
MECHANISM OF ACTION:
Binds with β-subunit of DNA-dependent RNA Polymerase (rpoB) ↓
Inhibit RNA synthesis
MECHANISM OF RESISTANCE:
Mutation at codons 526 & 531 site of rpoB gene.
PHARMACOKINETICS:• Absorption is variable
[Oral bioavailability Rifampicin (68%) & Rifabutin (20%)]• Food- ↓Rifampicin absorbtion but no effect on Rifabutin• High fat diet- ↑Rifapentin absorption
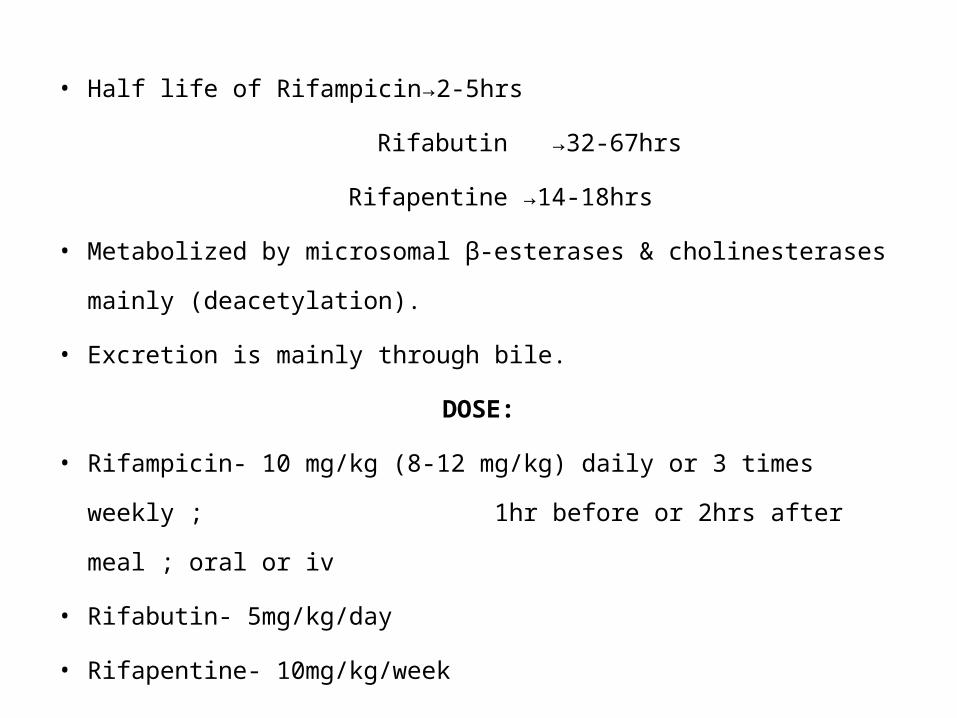
• Half life of Rifampicin→2-5hrs
Rifabutin →32-67hrs
Rifapentine →14-18hrs
• Metabolized by microsomal β-esterases & cholinesterases mainly
(deacetylation).
• Excretion is mainly through bile.
DOSE:
• Rifampicin- 10 mg/kg (8-12 mg/kg) daily or 3 times weekly ;
1hr before or 2hrs after meal ; oral or iv
• Rifabutin- 5mg/kg/day
• Rifapentine- 10mg/kg/week
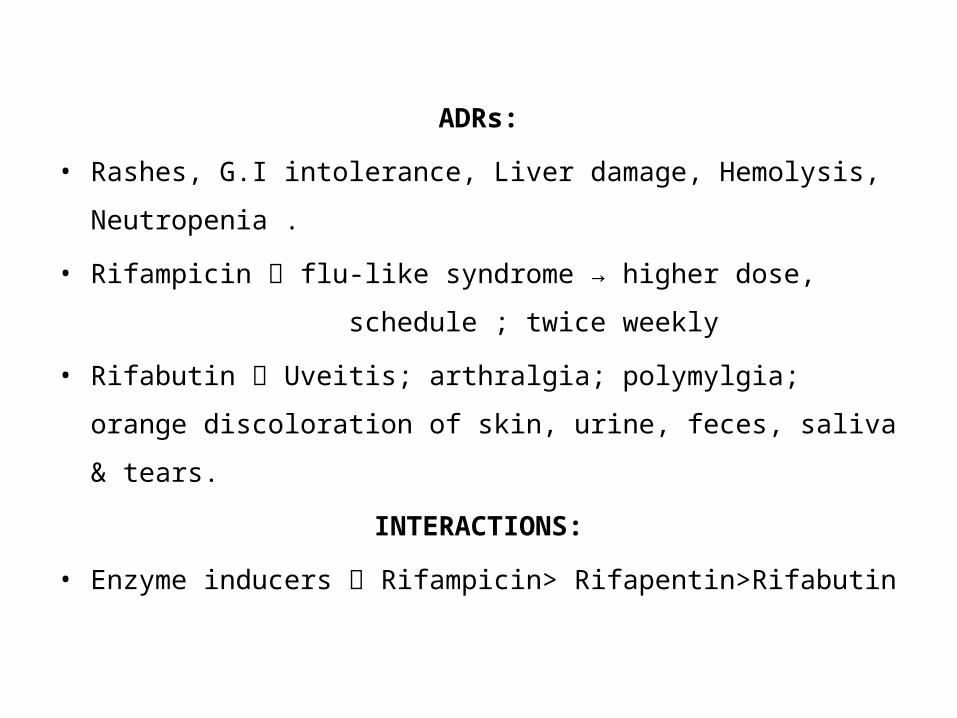
ADRs:
• Rashes, G.I intolerance, Liver damage, Hemolysis,
Neutropenia .
• Rifampicin flu-like syndrome → higher dose,
schedule ; twice weekly
• Rifabutin Uveitis; arthralgia; polymylgia; orange
discoloration of skin, urine, feces, saliva & tears.
INTERACTIONS:
• Enzyme inducers Rifampicin> Rifapentin>Rifabutin
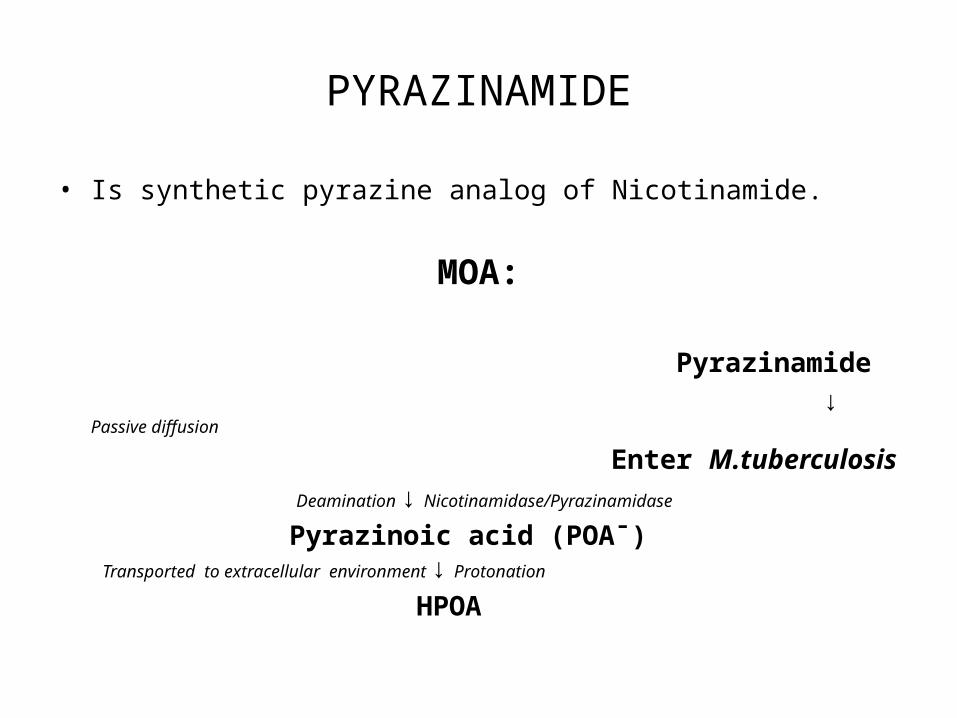
PYRAZINAMIDE
• Is synthetic pyrazine analog of Nicotinamide.
MOA:
Pyrazinamide
↓ Passive diffusion
Enter M.tuberculosis
Deamination ↓ Nicotinamidase/Pyrazinamidase
Pyrazinoic acid (POAˉ) Transported to extracellular environment ↓ Protonation
HPOA
• HPOA → Inhibit fatty acid synthase-1→ interfere with
mycolic acid synthesis.
→ disruption of membrane transport
MECHANISM OF RESISTANCE:• Point mutation in pncA gene (encodes Pyrazinamidase).
PHARMACOKINETICS:• Oral bioavailability >90%.• Highly concentrated in lung lining fluid.• T1/2 variable depends upon weight.• Metabolised by microsomal deaminidase.• Excreted in urine.
DOSE:• Orally• 25 mg/kg (20-30 mg/kg) daily• 35 mg/kg (30-40 mg/kg) three times weekly
ADRs:• Hepatic damage• Hyperuricemia- inhibit excretion of urate• Others- arthralgia, rashes, g.i upset, dysuria
ETHAMBUTOL
• Tuberculostatic drug.
MOA: Inhibit Arabinosyl transferase-Ш enzyme
↓ Disrupt the transport of Arabinose sugar
↓ Arbinogalactan biosynthesis impaired
↓ Disruption in mycobacterial cell wall formation

MECHANISM OF RESISTANCE:
• Mainly by mutation in codon 306 of embB gene.
• KatG 315 mutation Co-occurance of Ethambutol & Isoniazid
resistance.
PHARMACOKINETICS:
• Oral bioavailability ~80%.
• ~10-40% bound to plasma proteins.
• Half life: 3hrs (1st 12hrs) & 9hrs (next 12hrs) → redistribution.
• Rest of drug excreted unchanged in urine.
DOSE:• 15 mg/kg (15-20 mg/kg) daily• 30 mg/kg (25-35 mg/kg) three times weekly
ADRs:• Optic neuritis (dose related & daily schedule for >9mnths)• Colour blindness• Hyperuriceamia• Rashes, drug fever, joint pain
C/I:• Children <5 years
STREPTOMYCIN
MOA:
Binds with 30s ribosomal subunit
↓
Misreading of genetic code
↓
Inhibit protein synthesis
MECHANISM OF RESISTANCE:
• Mutation in rpsL gene
• Mutation in GidB gene
PHRAMACOKINETICS:
• Very poor oral bioavailability hence given in injectable form.
• Distributed extracellularly mainly
• Excreted unchanged in urine
DOSE:
• 15mg/kg (12-18 mg/kg) daily, or 2 or 3 times weekly; im.
ADRs:
• Nephrotoxicity
• Ototoxicity
• Neuromuscular blockade- ↓release of Ach by inhibiting
fusion of vesicles with terminal membrane
THANKYOU


ISONIAZID
•
For treatment of TB disease , isoniazid is used in combination withother agents to ensure killing of both actively dividing M. tuberculosisand slowlygrowing "persister" organisms. Unless the organism is resistant , the standard regimen includes isoniazid , rifampin , ethambutol ,and pyrazinamide (Table 20 元 -2). 1soniazid is often given togetherwith 25-50 mg of pyridoxine daily to prevent drug-related peripheralneuropathy.
PHARMACOLOGY• 1soniazid is 出 e hydrazide of isonicotinic ac 此 a small ,
water-soluble molecule. The usual adult oral daily dose of 300 mgresults in peak serum levels of 3-5 吨 /mL within 30 min to 2 h afteringestion-well in excess ofthe M1Cs for most susceptible strains ofM.tubercu/osis. Both oral and 1M preparations of isoniazid reach effectivelevels in the body , although antacids and high-carbohydrate meals mayinterfere with oral absorption. 1soniazid diffuses well throughout thebody , reaching therapeutic concentrations in body cavities and fluids ,with concentrations in cerebrospinal fluid (CSF) comparable to thosem serum.1soniazid is metabolized in the liver via acetylation byN-acetyltransferase 2 (NAT2) and hydrolysis. Both fast- and slowacetylation phenotypes occur; patients who are "fast acetylators" mayhave lower serum levels of ison 阳 id , whereas "slow acetylators" mayhave higher levels and experience more toxicity. Satisfactory isoniazidlevels are attained in the majority of homozygous fast NAT2 acetylators given a dose of 6 mg/kg and in the majority of homozygous slowacetylators given only 3 mg/kg. Genotyping is increasingly being usedto charaιterize isoniazid-related pharmacogenomic responses.
1soniazid's interactions with other drugs
• are due primarily to itsinhibition of the cytochrome P450 system. Among the drugs withsignificant isoniazid interactions are warfarin , carbamazepine , benzodiazepines , acetaminophen , clopidogrel , maraviroc , dronedarone ,salmeterol , tamoxifen , eplerenone , and phenytoin.
DOSING
• The recommended daily dose for the treatment of TB in theUnited States is 5 mg/kg for adults and 10-20 mg/kg for children , witha maximal daily dose of 300 mg for both. For intermittent therapy inadults (usually twice per week) , the dose is 15 mg/kg , with a maximaldaily dose of 900 mg. 1soniazid does not require dosage adjustment inpatients with renal disease.
RESISTANCE• Five separate pa 出 ways for isoniazid
resistance have been elucidated. • Most strains have amino acid changes
in either the catalase-peroxidase gene (katG) or the mycobacterial ketoenoylreductase gene (inhA).
• Less frequently , alterations in kasA ,the gene for an enzyme involved in mycolic acid elongation , and loss of NADH dehydrogenase 2 activity confer isoniazid resistance.
• 1n 20-30% of isoniazid-resistant M. tuberculosis isolates, increased expression of efflux pump genes , such as efpA , mmpL7 , mmr , p55 , and the Tap-like gene Rv1258c , has been implicated as the underlyingmechanism of resistance.

ADVERSE EFFECTS • Although isoniazid is generally well tolerated , druginduced liver injury
and peripheral neuropathy are signi 且 cant adverseeffects associated with this agent. 1soniazid may cause as 严 nptomatictransient elevation of aminotransferase levels (often termed hepaticadaptation) in up to 20% of recipients. Other adverse reactions includerash (2%) , fever (1.2%) , anemia , acne , arthritic s 严nptoms , a systemiclupus erythematosus-like syndrome , optic atrophy , seizures , and psychiatric symptoms. Symptomatic hepatitis occurs in fewer than 0.1% ofpersons treated with isoniazid alone for LTB1 , and fulminant hepatitiswith hepatic failure occurs in fewer than 0.01%. 1soniazid-associatedhepatitis is idiosyncratic , but its incidence increases with age , withdaily alcohol consumption , and in women who are within 3 monthspostpartum.
• Guidelines recommend that isoniazid be discontinued in the presence of hepatitisS 严 nptoms or jaundice and an ALT level three times the upper limit ofnormal or in the absence of symptoms with an ALT level five times theupper limit ofnormal

• Peripheral neuropathy associated with isoniazid occurs in up to2% of patients given 5 mg/kg. 1soniazid appears to interfere withP 严 idoxine (vitamin B6) metabolism. The risk of isoniazid-relatedneurotoxicity is greatest for patients with preexisting disorders thatalso pose a risk of neuropathy , such as H1V infection; for those withdiabetes mellitus , alcohol abuse , or malnutrition; and for those simultaneously receiving other potentially neuropathiι medications , suchas sta 叽 ldine. These patients should be given prophylactic pyridoxine(25-50 mg/d)
RIFAMPIN
• Rifampin is a semisynthetic derivative of Amycolatopsisrifamycinica (formerly known as Streptomyces mediterranei). The mostactive antimycobacterial agent available , rifampin is the keystone offirst-line treatment for TB. 1ntroduced in 1968 , this drug eventuallypermitted dramatic shortening of the TB treatment course. Rifampinhas both sterilizing and bactericidal activity against dividing andnondividing M. tuberculosis.

MOA
• Rifampin exerts both intracellular and extracellular bactericidal activity. Like other rifamycins , rifampin specificallybinds to and inhibits mycobacterial DNA-dependent RNA polymerase , blocking RNA synthesis.
PHARMACOLOGY
• Rifampin is a fat-soluble , complex macrocyclic molecule readily absorbed after oral administration. Serum levels of10-20 Ilg/mL are achieved 2.5 h after the usual adult oral dose of 10mg/kg (given without food). Rifampin has a half-life of 1.5-5 h. Thedrug distributes well throughout most body tissues , includi 吨 CSF.Rifampin turns body tluids such as urine , saliva , sputum , and tears areddish-orange color-an effect that offers a simple means of assessingpatients' adherence to this medication. Rifampin is excreted primarilythrough the bile and enters the enterohepatic circulation; <30% of adose is renally excreted.As a potent inducer of the hepatic cytochrome P450 system ,rifampin can decrease the half-life of some drugs , such as digoxin ,warfarin , phenytoin , prednisone , cyclosporine , methadone , oral contraceptives , clarithromycin , azole antifungal agents , quinidine , antiretroviral protease inhibitors , and non-nucleoside reverse transcriptaseinhibitors.

DOSING
• The daily dosage ofrifampin is 10 mg/kg for adults and 10-20mg/kg for children , with a maximum of600 mg/d forboth. The drug isgiven once daily , twice weekly , or three times weekly. No adjustmentsof dose or frequency are necessary in patients with renal insufficiency
RESISTANCE
• Resistance to rifampin in M. tuberculosis , Mycobacteriumleprae , and other organisms is the consequence ofspontaneous , mostlymissense point mutations in a core region of the bacterial gene codingfor the BETA subunit of RNA polymerase (rpoB). RNA polymerase alteredin this manner is no longer subject to inhibition by rifampin
ADVERSE EFFECTS
• Adverse events associated with rifampin are infrequent and generally mild.
• Hepatotoxicity due to rifampin alone isuncommon in the absence of preexisting liver disease and often consists of isolated hyperbilirubinemia rather than aminotransferase elevation.
• Other adverse reactions include rash , pruritus , gastrointestinal symptoms , and pancytopenia.
• Rarely , a hypersensitivity reaction mayoccur with intermittent therapy , manifesting as fever , chills , malaise , rash , and-in some instances-renal and hepatic failure.
ETHAMBUTOL
• ME(HANISM OF AaJON Ethambutol is bacteriostatiι against M. tuberculosis. Its prima 巧 mechanism ofaction is the inhibition of tlle arabinosyltransferases involved in cell wall s 严 lthesis , which probably inhibitsthe formation of arabinogalactan and lipoarabinomannan.
PHARMACOLOGYAND DOSING
• From a single dose of etllambutol , 75-80% isabsorbedwitllin 2-4 h ofadministration. Serum levels peak at 2-4 Ilg/mLafter tlle standard adult da 让 y dose of 15 mg/kg. Ethambutol is well dis-tributed tllroughout the body except in tlle CSF; a dosage of 25 mg/kgis necessary for attainment of a CSF level half of that in serum. Forintermittent tllerapy , tlle dosage is 50 mg/kg twice weekly. To prevent toxicity , tlle dosage must be lowered and the frequency ofadministrationreduced for patients with renal insufficiency.
ADVERSE EFFECTS
• Ethambutol is usually well tolerated and has nosignificant interactions with other drugs. Optic neuritis , the mostserious adverse effect reported , typically presents as reduced visualacuity , central scotoma , and loss of the ability to see green (or , lesscommonly , red). The cause of this neuritis is unknown , but it may bedue to an effect of ethambutol on the amacrine and bipolar cells ofthe retina. Symptoms typically develop several months after initiationof therapy , but ocular toxicity soon after initiation of ethambutol hasbeen described. The risk of ocular toxicity is dose dependent , occurring in 1-5% of patients , and can be increased by renal insufficiency.The routine use of ethambutol in younger children is not recommended because monitoring for visual complications can be difficult.Ifdrug-resistant TB is suspected , ethambutol can be used for treatmentof children
• All patients starting therapywith ethambutol should have a baselinetest for visual acuity , visual fields , and color vision and should undergoan examination of the optic fundus. Visual acuity and color visionshould be monitored monthly or less often as needed. Cessation ofethambutol in response to early symptoms of ocular toxicity usuallyresults in reversal of the deficit within several months. Recovery of all叽 sual function may take up to 1 year. In the elderly and in patientswhose symptoms are not recognized 巳 a 由, defic 山 may be permanentSome experts think that supplementation with hydroxocobalamin(vitamin B12) is beneficial for patients with etllambutol-related oculartoxicity. Other adverse effects of ethambutol are rare. Peripheral sensory neuropathy occurs in rare instances
RESISTANCE
• Ethambutol resistance in M. tuberculosis and NTM isassociated primarily with missense mutations in the embB gene thatencodes for arabinosyltransferase. Mutations have been found in resistant strains at codon 306 in 50-70% of cases. Mutations at embB306can cause slgm 且 cantly increased MICs of ethambutol , resulting inclinical resistance.
PYRAZINAMIDE
• A nicotinamide analog , pyrazinamide is an importantbactericidal drug used in the initial phase of TB treatment. Its administration for the first 2 months of therapy with rifampin and isoniazidallows treatment duration to be shortened from 9 months to 6 monthsand decreases rates of relapse
MOA
• Pyrazinamide's antimycobaιterial activity isessentially limited to M. tuberculosis. The drug is more active againstslowly replicating organisms than against actively replicating organisms. Pyrazinamide is a prodrug that is converted by the mycobacterial pyrimidase to the active form , pyrazinoic acid (POA). This agentis active only in acidic environments (pH <6.0) , as are found withinphagocytes or granulomas. The exact mechanism of action of POAis unclear , but fatty acid synthetase 1 may be the primary target inM. tuberculosis. Susceptible strains of M. tuberculosis are inhibited bypyrazinamide concentrations of 16-50 Ilg/mL at pH 5.5.
PHARMACOLOGY AND DOSING
• Pyrazinamide is well absorbed after oraladministration , with peak serum concentrations of 20-60 Ilg/mL at1-2 h after ingestion of the recommended adult daily dose of 15-30mg/kg (maximum , 2 g/d). It distributes well to various body compartments , including CSF , and is an important component oftreatment fortuberculous meningitis. The serum half-life of the drug is 9-1 1 h withnormal renal and hepatic function. Pyrazinamide is metabolized in theliver to POA , 5-hydroxypyrazinamide , and 5-hydroxy-POA. A highproportion of pyrazinamide and its metabolites (-70%) is excreted inthe urine. The dosage must be adjusted according to the level of renalfunction in patients with reduced creatinine clearance
ADVERSE EFFECTS • At the higher dosages used previously , hepatotoxic
ity was seen in as many as 15% of patients treated with pyrazinamideHowever , at the currently recommended dosages , hepatotoxic 盯 nowoccurs less commonly when this drug is administered with isoniazidand rifampin during the treatment of TB. Older age , active liver disease , HIV infection , and low albumin levels may increase the risk of hepatotoxicity. The use of pyrazinamide with rifampin for the treatment of LTBI is no longer recommended because of unacceptablerates of hepatotoxicity and death in this setting. Hyperuricemia is acommon adverse effect of pyrazinamide therapy that usually can bemanaged conservatively. Clinical gout is rareAlthough pyrazinamide is recommended by international TBorganizations for routine use in PI 吨 nancy , it is not recommended in the United States because of inadequate teratogenicity data.
RESISTANCE
• The basis of pyrazinamide resistance in M. tuberculosis isa mutation in the pncA gene coding for pyrazinamidase , the enzymethat converts the prodrug to active POA. Resistance to pyrazinamideis associated with loss of pyrazinamidase activity , which preventsconversion of pyrazinamide to POA. Of pyrazinamide-resistant M.tuberculosis isolates , 72-98% have mutations in pncA. Conventionalmethods of testing for susceptibility to p 严 azinamide may produceboth false-negative and false-positive results because the high-acidityenvironment required for the drug's activation also inhibits the growthofM. tuberculosis. There is some controversy as to the clinical significance of in vitro pyrazinamide resistance
Rifabutin
• Rifabutin , a semisynthetic derivative of rifamycin S , inhibits mycobacterial DNA-dependent RNA polymerase. Rifabutin is recommended in place of rifampin for the treatment of HIV-co-infectedindividuals who are taking protease inhibitors or non-nucleosidereverse transcriptase inhibitors , particularly nevirapine. Rifabutin'seffect on hepatic enzyme induction is less pronounced than that ofrifampin. Protease inhibitors may cause sign 凶 cant increases in rifabutin levels through inhibition of hepatic metabolism
PHARMACOLOGY
• Like rifampin , rifabutin is lipophilic and is absorbedrapidly after oral administration , reaching peak serum levels 2-4 hafter ingestion. Rifabutin distributes best to tissues , reaching levels5 一 10 times higher than those in plasma. Unlike rifampin , rifabutin andits metabolites are partially cleared by the hepatic microsomal system.Rifabutin's slow clearance results in a mean serum half-life of 45 hmuch longer than the 3- to 5-h half-life of rifampin. Clarithromycin(but not azithromycin) and fluconazole appear to increase rifabutinlevels by inhibiting hepatic metabolism
ADVERSE EFFECTS
• Rifabutin is generallywell tolerated , with adverse effectsoιcurring at higher doses. The most common adverse events are gastrointestinal; other reactions include rash , headache , asthenia , chest pain ,myalgia , and insomnia. Less common adverse reactions include fever ,chills , a flulike syndrome , anterior uveitis , 1 叩 atitis , Clostridium d 伊 cileassociated diarrhea , a diffuse polymyalgia syndrome , and yellow skindiscoloration ("pseudo-jaundice"). Laboratory abnormalities includeneutropenia , leukopenia , 出 rombocytopenia , and increased levels ofliverenzymes. Approximately 80% of patients who develop rifampin-relatedadverse events are able to complete TB treatment with rifabutin

• RESISTANCE Similar to rifampin resistance , resistance to rifabutin ismediated by some mutations in rpoB
Rifapentine • Rifapentine is a semisynthetic cyclopentyl rifamycin ,
sharing a mechanism of action with rifampin. Rifapentine is lipophilicand has a prolonged half-life that permits weekly or twice-weekly dosing. Therefore , this drug is the subjeιt ofintensive clinical investigationaimed at determining optimal dosing and frequency ofadministrationCurrently , rifapentine is an alternative to rifampin in the continuationphase of treatment for noncavitary drug-susceptible pulmonary TB inHIV-seronegative patients who have negative sputum smears at completion of the initial phase of treatment. When administered in thesespecific circumstances , rifapentine (10 mg/ 峙, up to 600 mg) is givenonce weekly with isoniazid. Because of higher rates of relapse , thisregimen is not recommended for patients with TB disease and HIV coinfection. The regimen is not recommended for pregnant women , for persons with hypersensitivity reactions to isoniazidor rifampin , or for HIV-infected individuals taking ART.
• PHARMACOLOGY Rifapentine's absorption is improved when the drug is taken with food. After oral administration , rifapentine reaches peak serum concentrations in 5-6 h and achieves a steady state in 10 days.The half-life of rifapentine and its active metabolite , 25-desacetyl rifapentine , is -13 h. The administered dose is excreted via the liver (70%).
• ADVERSE EFFECTS The adverse-effects profile of rifapentine is similar to that of other rifamycins. Rifapentine is teratogenic in animal models and is relatively contraindicated in pregnancy.
• RESISTANCE Rifapentine resistance is mediated by mutations in rpoB Mutations that cause resistance to rifampin also cause resistance to rifapentine
Streptomycin
• Streptomycin was the first antimycobacterialagent used for the treatment ofTB. Derived from Streptomycesgriseus , streptomycin is bactericidal against dividing M. tuberculosis organisms but has onlylow-level early bactericidal activity. Thisdrug is administered only by the 1M and IV routes. In developednations , streptomycin is used infrequently because of its toxicity , theinconvenience of injections , and drug resistance. In developing countries , however , streptomycin is used because of its low cost.
•MECHANISM OF ACTlON Streptomycin inhibits protein synthesis by binding at a site on the 30S mycobacterial ribosome
Pharmacology and dosing
• Serum levels of Streptomycin peak at 25-45 microgram/mL a 丘 er a l-g dose. This agent penetrates poorly into the CSF ,reaching levels that are only 20% ofserum levels. The usual daily doseof streptomycin (given 1M either daily or 5 days per week) is 15 mg/kgfor adults and 20-40 mg/kg for children , with a maximum of 1 g/dfor both. For patients 60 years of age� , 10 mg/kg is the recommendeddaily dose , with a maximum of 750 mg/d. Because streptomycin iseliminated almost exclu 盯 ely by the kidneys , 出 use in patients withrenal impairment should be avoided or implemented with caution ,with lower doses and less frequent administration
ADVERSE EFFECTS
• Adverse reactions occur frequently with streptomycin (10-20% of patients). Ototoxicity (primarily vestibulotoxicity) ,neuropathy , and renal toxicity are the most common and the mostserious. Renal toxicity , usually manifested as nonoliguric renal failure ,is less common with streptomycin than with other frequently usedaminoglycosides , such as gentamicin. Manifestations of vestibulartoxicity include loss of balance , vertigo , and tinnitus. Patients receiving streptomycin must be monitored carefully for these adverse effects ,undergoing audiometry at baseline and monthly thereafter.

RESISTANCE
• Spontaneous mutations conferring resistance to streptomycin are relatively common , occurring in 1 in 106 organisms. In thetwo-thirds of streptomycin-resistant M. tuberculosís strains exhibitinghigh -level resistanιe , mutations have been identified in one of twogenes: a 16S rRNA gene (rrs) or the gene encoding ribosomal proteinS12 (rpsL). Both targets are believed to be involved in streptomycinribosomal binding. However , low-level resistance , which is seen inabout one-third of resistant isolates , has no associated resistancemutation. A gene (gídB) that confers low-level resistance to streptomycin has recently been identified. Strains ofM. tuberculosis resistantto streptomycin generally are not cross-resistant to capreomycin oramikacin. Streptomycin is not used for the treatment of MDR-TB orXDR-TB because of (1) the high prevalence of streptomycin resistanceamong strains resistant to isoniazid and (2) the unreliability of drugsusceptibility testing







![New Multidrug-resistant tuberculosis outbreak associated with poor … · 2019. 5. 7. · drug-resistant TB globally, including rifampicin-resistant-tuberculosis [6]. This represents](https://static.fdocuments.net/doc/165x107/600d77f9f2a2e24066677183/new-multidrug-resistant-tuberculosis-outbreak-associated-with-poor-2019-5-7.jpg)