NON-Neurogenic Chronic Urinary Retentionglsuna.org/LAJINESS.pdf · Treatment Algorithm. Treatment...
42
NON-Neurogenic Chronic Urinary Retention AUA White Paper Great Lakes SUNA Inside Urology March 16, 2018 Michelle J. Lajiness FNP-BC Nurse Practitioner DMC Urology
Transcript of NON-Neurogenic Chronic Urinary Retentionglsuna.org/LAJINESS.pdf · Treatment Algorithm. Treatment...
NON-Neurogenic
Chronic Urinary RetentionAUA White Paper
Great Lakes SUNA Inside Urology
March 16, 2018
Michelle J. Lajiness FNP-BC
Nurse Practitioner DMC Urology
Incidence
Really unknown
Lack consensus on definition
Unknown
Difficult to differentiate non neurogenic
from neurogenic
AUA White Paper
Based on expert opinion
Lacks evidenced base trials
Lacks consensus
No standardized criteria

Goals of White Paper
Characterize patients with CUR into clinically definable index patient populations in adult men and women(>18 years old)
Propose diagnostic and treatment alogorithms for these index populations
Identify future areas of research for CUR
CUR Definition
There is no one definition
Use of the term varies in the literature
Research tends to use atonic detrusor
Urodynamic study
No contraction during study
Recently linked with primary muscle
activity and underactive bladder

ICS definition
A contraction of reduced strength and/or
duration, resulting in prolonged
bladder emptying and/or failure to
achieve complete bladder emptying
within a normal time span
AUA Definition (clinical)
Non Neurogenic CUR is empirically
defined herein as an elevated PVR
>300 mL that has persisted for at least
six months documented on two or
more separate occasions.
Controversy
PVR as definition
PVR consensus >100- >500 mL
Cut off value based on total volume
voided vs. volume left
Sign not uniform diagnosis
Conditions Commonly
associated with CUR
Outlet obstruction
Poor bladder contractility
Outlet obstruction
Long-term use of medications
Antihistamines
Alpha adrenergic agonists
antipsychotics
Urethral or bladder neck constricture
High grade pelvic floor prolapse
Urethral diverticula in women
Outlet Obstruction
Prior anti-incontinence procedure
Prior vaginal vault prolapse procedure
Primary bladder neck obstruction in
men and women
Dysfunctional voiding
Poor bladder contractility
Long standing outlet obstruction
Long term use of medication
Anticholinergic/Antispasmotic
Tricyclic anti depressants
Beta adrenergic agonist
Calcium channel blockers
Non steroidal anti inflammatory
Opioids
Benzodiazepines
antipsychotics
Poor Bladder Contractility
Diabetes
Constipation
Frailty
idiopathic

Categories of CUR
High –risk
Subset of individuals with CUR who
are at potentially elevated risk for
organ system harm or failure from
CUR
Symptomatic CUR
Subset of individuals who are
bothered by symptoms
High risk CUR Radiology findings
Hydronephrosis
Hydroureter
Lab findings Stage III chronic kidney disease
• GFR 30-50 mL/min
Recurrent symptomatic, culture proven UTI
Culture proven systemic urosepsis
Signs and symptoms Urinary Incontinence associated with skin
breakdown
UI associated with decub

Symptomatic CUR
Having subjectively moderate to severe
urinary symptoms impacting QOL on a
validated urinary questionnaire
History of requiring catheterization for
treatment of a symptomatic episode of
inability to void within the last 6 months
Excluding acute onset or urinary retention
caused by oncologic, traumatic, or any
neurologic event.

Treatment Algorithm
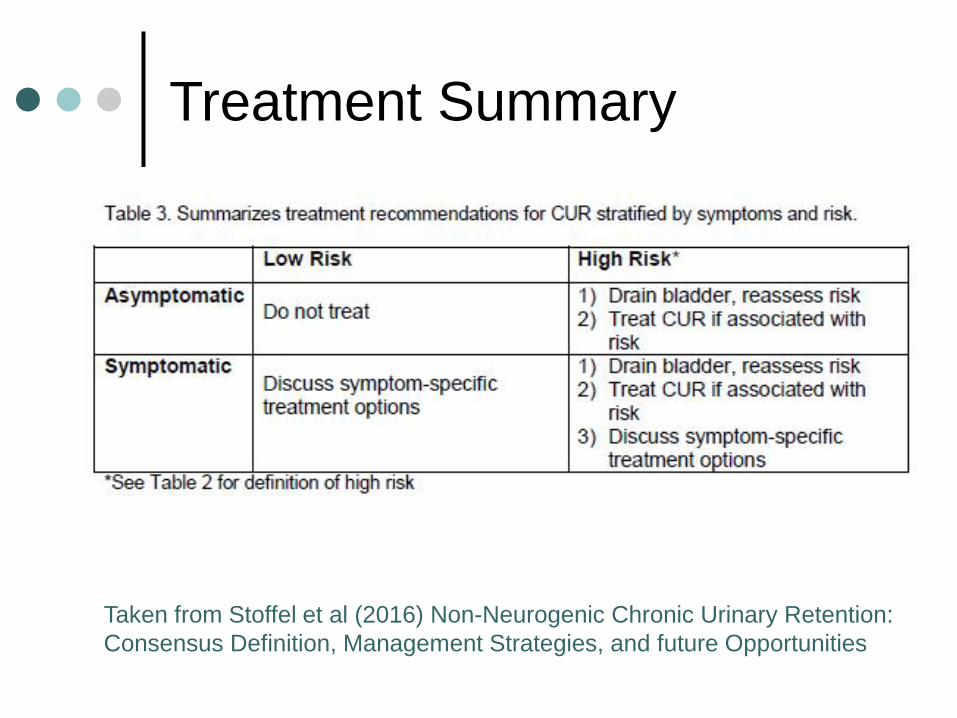
Treatment Summary
Taken from Stoffel et al (2016) Non-Neurogenic Chronic Urinary Retention:
Consensus Definition, Management Strategies, and future Opportunities
Treatment
If patient is asymptomatic and there is
no hydro---
DO NOT CATH PATIENT
Index Patient
The first medically-identified Pt in a
family or other group, with a particular
condition which triggers a line of
investigation
Medication
Outlet obstruction caused by prostate
Alpha blockers
5-alpha- reductase inhibitors
Primary bladder obstruction male and
female
Alpha blockers
Improve bladder contractility
Cholinergic agonist
• Bethanechol

Catheterization
CIC performed frequently enough to
effectively target reduction of risk and
symptoms should be tailored for the
individual treatment plan
If long term catheterization is needed
consider SP tube
Surgical Treatments
Dictated by etiology
In men obstruction secondary to
prostate several surgeries available
Chronic BOO in women secondary to
prior mid urethral sling placement
simple sling incision
Prolapse- several options

Surgical Treatment
CUR due to decreased bladder
contractility consider sacral
neuromodulation
Outcome measures
Symptom improvement , as measured by
quality questionnaires
Risk reduction, as defined by resolution of
hydronephrosis, renal failure, recurrent UTI,
urosepsis, and secondary complications
from overflow incontinence
Successful trial of voiding without
catheterization
Stability of symptoms and risk over time
WHAT’S NEXT
Define it
Determine causes
Research on interventions
Multi-institutional cohort studies
Identify molecular markers
Investigation for pharmacological and
neurological interventions.
UAB Symposium
Index Patient Examples
50 year old male
c/o urinary frequency, hesitancy, slow
stream and nocturia
Index Patient 1 work-up
AUA SI >15
50 g prostate on DRE
UA normal
PVR- 350 cc

Risk Category
Low/Risk Symptomatic
Index Patient 1 Treatments
Timed voiding
Fluid management
PVR 6 months later 450 cc
Renal Ultrasound and renal panel
negative
Treatment Index Patient 1
Offer CIC and/or
Alpha blockers and/or
5-alpha- reductase inhibitors
Formal evaluation for outlet
obstruction with a UDS
Goal improve QOL monitor with
validated questionnaires
Index Patient 2
77 year old male
HX of CHF
Four culture positve UTI’s over the
past 3 months
Long history of bothersome, irritative
LUTS
Index Patient 2 work-up
60 g prostate
2 separate PVR’s over 6 months
>500ml
UA positive for leukocyte esterase,
nitrites, and crystals
Renal US shows mild to moderate
hydronephrosis and a 3 cm bladder
stone

Risk Category
High/Risk Symptomatic
Index Patient 2 Treatment
Immediate catheterization to address
UTI and hydro
Consider evaluation for a bladder
outlet procedure and/or lithotripsy
Long term CIC or SP Tube

Index Patient 3
75 yo female
No symptoms
No prior urologic history
Presents to EC after a fall for hip pain
CT shows distended bladder no hydro
PE shows mild vaginal vault prolapse
PVRS consistently >400 mL
Risk Category
Low Risk/Asymptomatic
Index Patient 4
80 yo male
Distant history or TURP and
chronically elevated PVR
No bothersome symptoms
RUS shows bilat
hydroureteronephrosis and a PVR
1,800 mL
Risk Category
High Risk/Asymptomatic

Index Patient 4 treatment
PVR consistent with longstanding
bladder decompensation
Short term indwelling foley
CIC if able after

Conclusion
Need clinical research studies
Only treat those high risk categories
Treatment should be based on
Assessment of symptoms
Reduction of risk
Ability to void without catheterization
Stability of symptoms/risk over time