Nodules in Autoimmune Thyroiditis Are Associated With Increased Risk of Thyroid Cancer in Surgical...
6
Nodules in Autoimmune Thyroiditis Are Associated With Increased Risk of Thyroid Cancer in Surgical Series But Not in Cytological Series: Evidence for Selection Bias Maria Grazia Castagna, Valentina Belardini, Silvia Memmo, Fabio Maino, Andrea Di Santo, Paolo Toti, Anton Ferdinando Carli, Giuseppe Caruso, and Furio Pacini Departments of Medical, Surgical, and Neurological Sciences (M.G.C., V.B., S.M., F.M., A.F.C., G.C., F.P.) and Medical Biotechnology (A.D.S., P.T.), University of Siena, 53100 Siena, Italy Background: The association of thyroid cancer and autoimmune thyroiditis (AIT) has been widely addressed, with conflicting results in surgical and cytological series, likely affected by selection bias. Objective: The objective of the study was to evaluate the association between the cytological features suggestive or indicative of malignancy and AIT in 2504 consecutive patients (2029 females and 475 males, mean age 58.3 14.1 y) undergoing fine-needle aspiration cytology for thyroid nodules. Patients: Based on the clinical diagnosis, patients were divided into four groups: AIT with nodules (N-AIT, 14.9%); nodular Graves disease (N-GD, 2.8%); nodular goiter and negative thyroid anti- bodies (NGAb, 68.4%); and nodular goiter with positive thyroid antibodies (NGAb, 13.9%). Results: The prevalence of patients with cytological features suggestive (Thy4) or indicative of malignancy (Thy5) was 4.5 % in the N-AIT group, not different compared with the other groups (N-GD, 5.6%; NGAb, 5.0%; NGAb, 4.3%). No difference was also found in the other categories (Thy2 and Thy3). When the same analysis was performed in the subgroup of patients (14.3%) with a histological confirmation, we found that the prevalence of differentiated thyroid cancer was significantly higher (P .01) in the N-AIT group (67.8%) compared with the other groups (N-GD, 40.0%; NGAb, 37.2%; NGAb, 36.9%). Conclusions: The results of our cytological series do not support a link between N-AIT and thyroid cancer. The association between cancer and N-AIT found in the histology-based series is likely due to a selection bias represented by the fact that the prevalent indication for surgery in the N-AIT group was suspicious cytology (60.7% of patients) more frequently than in the other groups. (J Clin Endocrinol Metab 99: 3193–3198, 2014) T he association between autoimmune thyroiditis (AIT) and differentiated thyroid cancer (DTC), mainly papillary, has been largely studied. but it still remains controversial. Some studies have demonstrated a higher risk of DTC in patients with nodular AIT (1–9), whereas others did not observe such a risk (10 –15). In particular, the association between DTC and AIT is reported mainly in retrospective surgical series (1–5), which have a selection bias. As a matter of fact, in most of these studies, the indication for thyroidectomy in patients with AIT are not specified, but, considering that patients with AIT are treated by surgery ISSN Print 0021-972X ISSN Online 1945-7197 Printed in U.S.A. Copyright © 2014 by the Endocrine Society Received January 31, 2014. Accepted May 30, 2014. First Published Online June 3, 2014 Abbreviations: AIT, autoimmune thyroiditis; CI, confidence interval; DTC, differentiated thyroid cancer; FNAC, fine-needle aspiration cytology; OR, odds ratio; PTC, papillary thy- roid cancer; Q, quintile; TgAb, thyroglobulin antibody; TPOAb, thyroperoxidase antibody; US, ultrasonography. ORIGINAL ARTICLE Endocrine Care doi: 10.1210/jc.2014-1302 J Clin Endocrinol Metab, September 2014, 99(9):3193–3198 jcem.endojournals.org 3193 The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 29 September 2014. at 15:59 For personal use only. No other uses without permission. . All rights reserved.
Transcript of Nodules in Autoimmune Thyroiditis Are Associated With Increased Risk of Thyroid Cancer in Surgical...

Nodules in Autoimmune Thyroiditis Are AssociatedWith Increased Risk of Thyroid Cancer in SurgicalSeries But Not in Cytological Series: Evidence forSelection Bias
Maria Grazia Castagna, Valentina Belardini, Silvia Memmo, Fabio Maino,Andrea Di Santo, Paolo Toti, Anton Ferdinando Carli, Giuseppe Caruso,and Furio Pacini
Departments of Medical, Surgical, and Neurological Sciences (M.G.C., V.B., S.M., F.M., A.F.C., G.C.,F.P.) and Medical Biotechnology (A.D.S., P.T.), University of Siena, 53100 Siena, Italy
Background: The association of thyroid cancer and autoimmune thyroiditis (AIT) has been widelyaddressed, with conflicting results in surgical and cytological series, likely affected by selection bias.
Objective: The objective of the study was to evaluate the association between the cytologicalfeatures suggestive or indicative of malignancy and AIT in 2504 consecutive patients (2029 femalesand 475 males, mean age 58.3 � 14.1 y) undergoing fine-needle aspiration cytology for thyroidnodules.
Patients: Based on the clinical diagnosis, patients were divided into four groups: AIT with nodules(N-AIT, 14.9%); nodular Graves disease (N-GD, 2.8%); nodular goiter and negative thyroid anti-bodies (NGAb�, 68.4%); and nodular goiter with positive thyroid antibodies (NGAb�, 13.9%).
Results: The prevalence of patients with cytological features suggestive (Thy4) or indicative ofmalignancy (Thy5) was 4.5 % in the N-AIT group, not different compared with the other groups(N-GD, 5.6%; NGAb�, 5.0%; NGAb�, 4.3%). No difference was also found in the other categories(Thy2 and Thy3). When the same analysis was performed in the subgroup of patients (14.3%) witha histological confirmation, we found that the prevalence of differentiated thyroid cancer wassignificantly higher (P � .01) in the N-AIT group (67.8%) compared with the other groups (N-GD,40.0%; NGAb�, 37.2%; NGAb�, 36.9%).
Conclusions: The results of our cytological series do not support a link between N-AIT and thyroidcancer. The association between cancer and N-AIT found in the histology-based series is likely dueto a selection bias represented by the fact that the prevalent indication for surgery in the N-AITgroup was suspicious cytology (60.7% of patients) more frequently than in the other groups. (J ClinEndocrinol Metab 99: 3193–3198, 2014)
The association between autoimmune thyroiditis (AIT)and differentiated thyroid cancer (DTC), mainly
papillary, has been largely studied. but it still remainscontroversial.
Some studies have demonstrated a higher risk of DTCin patients with nodular AIT (1–9), whereas others did not
observe such a risk (10–15). In particular, the associationbetween DTC and AIT is reported mainly in retrospectivesurgical series (1–5), which have a selection bias. As amatter of fact, in most of these studies, the indication forthyroidectomy in patients with AIT are not specified, but,considering that patients with AIT are treated by surgery
ISSN Print 0021-972X ISSN Online 1945-7197Printed in U.S.A.Copyright © 2014 by the Endocrine SocietyReceived January 31, 2014. Accepted May 30, 2014.First Published Online June 3, 2014
Abbreviations: AIT, autoimmune thyroiditis; CI, confidence interval; DTC, differentiatedthyroid cancer; FNAC, fine-needle aspiration cytology; OR, odds ratio; PTC, papillary thy-roid cancer; Q, quintile; TgAb, thyroglobulin antibody; TPOAb, thyroperoxidase antibody;US, ultrasonography.
O R I G I N A L A R T I C L E
E n d o c r i n e C a r e
doi: 10.1210/jc.2014-1302 J Clin Endocrinol Metab, September 2014, 99(9):3193–3198 jcem.endojournals.org 3193
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 29 September 2014. at 15:59 For personal use only. No other uses without permission. . All rights reserved.

almost exclusively when there is a suspicion of malig-nancy, it is conceivable that the surgical series are enrichedwith malignant cases. In the last decade, the relationshipbetween AIT and thyroid cancer has been studied in cy-tological series (6–13). In such series patients are selectedfor fine-needle aspiration cytology (FNAC) just for thepresence of nodules, without the bias of suspicion of ma-lignancy. However, these studies have reported conflictingresults (6–13).
In a recent review (16), the author compared the prev-alence and the risk of papillary thyroid cancer (PTC) inAIT patients included in cytological or surgical series andfound that in cytological series the average prevalence ofPTC in AIT was 1.2% and the risk ratio was 0.69, incontrast with 27.5% and 1.59 in surgical series. Thesedata corroborate the hypothesis that the discrepant resultsbetween cytological and surgical series might derive fromselection bias.
The aim of this study was to evaluate the associationbetween cytological features suggestive or indicative ofDTC and the presence of AIT in a series of consecutivepatients submitted to FNAC and to search for this asso-ciation in the subgroup of patients of the same series sub-mitted to thyroidectomy for any indication.
Patients and Methods
PatientsWe retrospectively evaluated FNAC results of 2504
(2029 females and 475 males, mean age 58.3 � 14.1 y)consecutive patients (3990 nodules) who underwentFNAC of thyroid nodules with adequate cytology. All pa-tients were submitted to serological testing [thyroperoxi-dase antibodies (TPOAbs), thyroglobulin antibodies(TgAbs), free T4, free T3, and TSH] and neck ultrasonog-raphy (US). Based on clinical, biochemical, and ultra-sound data available at the time of FNAC, patients withthyroid nodules were classified into four groups: 1) nod-ular autoimmune thyroiditis (N-AIT) in the presence ofclearly positive antithyroid antibodies (TgAbs and/orTPOAbs � 100 IU/L) associated with the thyroiditis pat-tern on neck US, with or without hypothyroidism. Patientswith a clear thyroiditis pattern on neck US and hypothy-roidism but with modest increase of TgAbs and/or TPO-Abs (�100 IU/L) were also considered as N-AIT; 2) nod-ular Graves disease (N-GD); 3) nodular goiter withnegative antithyroid antibodies and no thyroiditis patternon US and no hypothyroidism (NGAb�); and 4) nodulargoiter with positive antithyroid antibodies (regardless oftheir titers) and no thyroiditis pattern on neck US or hy-pothyroidism [(NGAb�).
Three hundred fifty-eight of 2504 patients (14.3%)were sent to surgery. Specifically, all patients with Thy4/Thy5 cytologies were sent to surgery in every group. How-ever, a small minority of patients (10.7%) decided to havesurgery in other institutions and were considered as lost tofollow-up. In the benign nodule categories (Thy2), onlyselected patients, those with compressive symptoms, weresent to surgery (2.1% in N-AIT, 10% in N-GD, 7.2% inNGAb�, and 10.5% in NGAb�). Patients with Thy2 cy-tologies (n � 1198) not submitted to surgery were ob-served with annual follow-up consisting in clinical exam-ination, neck US, and serological testing (free T3, free T4,and TSH measurement).
Materials
Serum TSH was measured by chemiluminescent immunometricassay (Immulite 2000; Diagnostic Products Corp). Measurementof TgAbs and TPOAbs was performed with a solid-phase, en-zyme-labeled, chemiluminiscent sequential immunometric assay(Immulite 2000; Siemens Medical Solutions Diagnostics). Valuesof 40 IU/mL or less were regarded as negative for TgAbs and 35IU/mL for or less TPOAbs. For both measurements, values of 100or greater were considered clearly elevated.
TSH receptor antibodies were measured, when indicated, us-ing a third-generation ELISA kit (RSR ElisaRSR TSH receptorantibody; Third Generation). Values of 1 IU/L or less were re-garded as negative.
Neck US was performed by experienced endocrinologists(members of our staff) using a high-resolution ultrasound colorDoppler apparatus (AU 590 Asynchronous; Esaote Biomedical)with a 7.5-MHz linear transducer. Nodules were selected forFNAC according to the criteria reported in the 2009 AmericanThyroid Association guidelines (17). FNAC was performed un-der US guidance using a 23/25-gauge needle, and only nodulesclearly distinct from the surrounding parenchyma were submit-ted to FNAC. Specifically, in N-AIT we did not perform FNACin pseudonodules and we did not perform random biopsy. Thematerial was air dried, stained with May-Grunwald Giemsa, andinterpreted by an experienced cytologist. Cytological resultswere reported according to the criteria of the British ThyroidAssociation (2007) (18).
Statistical analysisFor the statistical analysis, the Thy4 and Thy5 categories were
combined and Thy1 categories were excluded from the begin-ning. Epidemiological data are presented as the mean � SD. Thet test for independent data or the Mann-Whitney U test wasperformed for normal or nonnormal variables, respectively. Toevaluate significant differences in data frequency, we analyzedcontingency tables. Tables with a size larger than 2 � 2 wereexamined by the �2 test or a numerical approximation of theFisher exact test, when all cell frequencies were greater than 4 ornot, respectively. The following variables were studied by uni-variate analysis: age at diagnosis, sex, nodule size, TSH levels,single nodule, and antithyroid antibodies (TgAbs and TPOAbs).Statistically significant variables found in univariate analysiswere entered into a multivariate analysis to identify those with
3194 Castagna et al Autoimmune Thyroiditis and Thyroid Cancer J Clin Endocrinol Metab, September 2014, 99(9):3193–3198
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 29 September 2014. at 15:59 For personal use only. No other uses without permission. . All rights reserved.

independent prognostic significance and to calculate the oddsratio (OR). Diagnostic accuracy was calculated according to Ga-len (19) and was based on true positive, true negative, false-positive, and false negative results. The 95% confidence interval(CI) of all estimates was also evaluated. Thy3 categories wereexcluded from uni- and multivariate logistic regression analysisand for the diagnostic accuracy of FNAC.
Statistical analysis was performed using the software Stat-View for Windows version 5.0.1 (SAS Institute).
Results
Results of cytological seriesBased on clinical, biochemical, and ultrasound data
available at the time of FNAC, 373 of 2504 patients(14.9%) were classified as having N-AIT, 71 of 2504 pa-tients (2.8%) as having N-GD, 1713 of 2504 patients(68.4%) as having NGAb�, and finally, 347 of 2504 pa-tients (13.9%) as affected by NGAb�. Of 2504 patients(3990 nodules), FNAC was performed in one single nod-ule in 1426 patients (57%) and in more than one nodulein 1078 of 2054 (43%) patients. In multinodular glands,varying cytological diagnoses among different noduleswere observed in 111 of 1078 patients (10.3%). In thesecases, the patient was classified according to the most con-cerning level of cytology (Thy2 � Thy3 � Thy4/5). FNACwas benign (Thy2) in 85.8% of the patients (2148 of
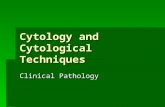
2504), suspicious or malignant(Thy4/Thy5) in 4.8% (121 of 2504),and indeterminate (Thy3) in 9.4%(235 of 2504). The prevalence ofThy4/Thy5 nodules was not differ-ent in the four groups (P � .80):4.5% in N-AIT, 5.6% in N-GD,5.0% in NGAb�, and 4.3% inNGAb� (Figure 1).
In addition, we correlated theprevalence of Thy4/Thy5 accordingto the presence/absence of TPOAbs.The rate of Thy4/Thy5 was 4.97% inTPOAb-positive and 5.4% inTPOAb-negative patients (P � .80).
Results of surgical seriesSurgery was performed in 28 of 373 patients (7.5%)
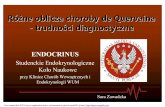
from the N-AIT group, 10 of 71 patients (14.1%) from theN-GD group, 255 of 1731 patients (14.7%) from theNGAb� group, and 65 of 347 patients (18.7%) from theNGAb� group. As shown in Table 1, 358 of 2504 patients(14.3%) were selected for surgery: the indication for sur-gical therapy was the presence of suspicious cytology ormalignant nodule (Thy4–5) (108 patients; 30.2%), inde-terminate nodules (Thy3) (100 patients, 28.0%), or be-nign nodules (Thy2) with large nodular goiter and/or com-pressive symptoms (150 of 358 patients; 41.8%). Asuspicion of malignancy (Thy 4/5 cytology) was the indi-cation for surgery more frequently in N-AIT patients thanin the other groups (P � .009). As a consequence of thisselection bias, not surprisingly, the prevalence of DTC atfinal histology was significantly higher (67.8%) in the N-AIT group (P � .01) (Figure 2).
Risk factors for suspicious/malignant cytology(univariate and multivariate analysis)
As shown in Table 2, univariate analysis risk factors forcytological diagnosis of suspicious/malignant cytology(Thy4/5) were younger age, higher TSH levels, and singlenodules but not sex, nodule size, and antithyroid antibod-
Figure 1. Cytological diagnosis [benign (Thy2), indeterminate (Thy3), suspicious or malignant(Thy4/5)] according to the clinical diagnosis (N-AIT, N-GD, NGAb�, NGAb�). The y-axisrepresents the percentage of cytological results in each group of patients.
Table 1. Reason for Surgery in Each Patient Group
Presurgical Clinical Diagnosis
Nodular Autoimmune Disease Nodular GoiterPValueN-AIT N-GD NGAb� NGAb�
Reason for surgerySuspicious nodules (Thy4/5) (n � 108) 17 (60.7%) 3 (30.0%) 74 (29.0%) 14 (21.5%) .009Indeterminate nodules (Thy3) (n � 100) 4 (14.3%) 1 (10.0%) 75 (29.4%) 20 (30.7%)Large nodular goiter (Thy2) (n � 150) 7 (25.0%) 6 (60.0%) 106 (41.6%) 31 (47.8%)Total (n � 358) 28 10 255 65
doi: 10.1210/jc.2014-1302 jcem.endojournals.org 3195
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 29 September 2014. at 15:59 For personal use only. No other uses without permission. . All rights reserved.

ies. With multivariate analysis, only TSH levels and singlenodules were significantly and independently associatedwith Thy4/5 cytologies. (Table 3).
Mean (�SD) TSH levels were 1.7 � 1.7 mIU/L in pa-tients with suspicious/malignant (Thy4/5) thyroid nod-ules, significantly higher (P � .0001) compared with pa-tients with benign cytologies (1.43 � 3.5 mU/L). WhenTSH levels were divided into quintiles (Q1, � 0.4 mIU/L;Q2, 0.4–0.8 mIU/L; Q3, 0.9–1.4 mIU/L; Q4, 1.5–3.9mIU/L; and Q5, � 4.0 mIU/L), the prevalence of malig-nancy (Thy4/Thy5) increased significantly (P � .001) withincreasing TSH levels (3.5%, 2.8%, 7.3%, 7.3%, and10%, respectively) (Table 2). The highest rate of suspi-cious/malignant (Thy4/5) cytologies was observed in thenodules with serum TSH levels of 4.0 mU/L or greater (OR3.86; 95% CI 1.458–10.025) (Table 3).
When we correlated the TSH parameter with theTPOAb status, we found that the rate of Thy4/5 cytologies
in TPOAb-positive patients (�100 IU/L) was higher(7.2%) in the presence of serum TSH levels of 4.0 mU/L orgreater compared with 3.2% in the presence of serum TSHlevels less than 4.0 mU/L; similarly, in TPOAb-negativepatients, the rate of Tyr4/5 cytologies was higher (10.2%)in the presence of serum TSH levels of 4.0 mU/L or greatercompared with 3.6% in the presence of serum TSH levelsless than 4.0 mU/L. This analysis demonstrates that TSHelevations (�4.0 mU/L) were significantly associated withan increased rate of suspicious or malignant cytologies,regardless of the TPOAb status.
Suspicious/malignant (Thy4/5) cytologies were signif-icantly (P � .0001) more frequent in solitary nodules (43of 443, 9.7%) than in multinodular goiter (78 of 1826,4.2%) (OR 2.40; 95% CI 1.605–3.610) (Table 3).
Validation of FNACBecause a possible bias of our or similar studies might
be related to the skill of the cytologist, we tried to validatehis performance by comparing the cytological and the his-tological diagnosis in the subset of patients submitted tosurgery (358 patients, 496 nodules). A histological diag-nosis of DTC was observed in 79.3% of the Thy4, 100%of the Thy5, and 3.7% of the Thy2 nodules submitted tosurgery, which is a diagnostic performance similar to thatreported in the literature. As shown in Table 4, the pres-ence of AIT did not affect the diagnostic accuracy. Thepositive predictive value (PPV) and the negative predictivevalue (NPV) in AIT nodules was 100% and 95.4% re-spectively, similar to that observed in nodular goiter (94%and 96.5%, respectively).
Figure 2. Prevalence of benign or malignant histologies (percentagein the y-axis) according to the clinical diagnosis (N-AIT, N-GD, NGAb�,NGAb�).
Table 2. Univariate Analysis for Risk Factors Predicting Suspicious/Malignant Cytology (Thy 3 Excluded)
Thy2(n � 2148)
Thy4/Thy5(n � 121)
P ValueUnivariate
Sex, n (% males) 393 (18.3%) 28 (23.1%) .39Age, y
Group 1 (� 30 y) 43 (68.3%) 20 (31.7%)Group 2 (30–49 y) 480 (82.1%) 41 (7.9%) <.0001Group 3 (50–69 y) 1156 (96.4%) 44 (3.6%)Group 4 (� 70 y) 469 (96.7%) 16 (3.3%)
TSH mIU/La
Q1 (�0.4) 245 (96.5%) 9 (3.5%)Q2 (0.4–0.8) 557 (97.2%) 16 (2.8%)Q3 (0.9–1.4) 380 (92.7%) 30 (7.3%) .001Q4 (1.5–3.9) 354 (92.7%) 28 (7.3%)Q5 (�4.0) 72 (90%) 8 (10%)
Size, cm 2.3 � 1.2 2.1 � 1.5 .08Single nodule 400 (18.6%) 43 (35.5%) <.0001TgAb positive, � 100 IU/mL 279 (13.0%) 13 (10.7%) .57TPOAb positive, � 100 IU/mL 363 (16.9%) 19 (15.7%) .80
Bold indicates significant values.a A total of 1699 patients without therapy.
3196 Castagna et al Autoimmune Thyroiditis and Thyroid Cancer J Clin Endocrinol Metab, September 2014, 99(9):3193–3198
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 29 September 2014. at 15:59 For personal use only. No other uses without permission. . All rights reserved.

Discussion
The association between AIT and thyroid cancer has beenextensively studied, but it still remains controversial. Moststudies are retrospective and analyze patients submitted tothyroidectomy, allowing for a selection bias (1–5, 14, 15).More recently, to overcome these limitations, cytologicalseries have been published (6–13). Some of these studiesreported a higher risk of DTC in patients with AIT (6–9),whereas others did not observe such an association (10–13). In a comprehensive review (16), the prevalence andthe relative risk of PTC in AIT patients according to cy-tological or surgical series were compared. In cytologicalseries the average prevalence of PTC in patients with AITwas lower than that observed in the histological series(1.2% and 27.56%, respectively) (16). In agreement withthe results of this meta-analysis, we have not found anassociation between N-AIT and thyroid cancer in our cy-tological series, but we did find an association in the subsetof patients sent to surgery (surgical series). It is apparentfrom our data that the discrepancy between the cytologicaland the surgical series is due to selection bias in the latter.Considering that the vast majority of patients with N-AITare not treated by surgery, it is clear that the surgical in-dication for surgery in these patients is a high suspicion ofmalignancy, and thus, the category of N-AIT is artificiallyenriched of thyroid cancer. On the contrary, because nod-ular goiters were sent to surgery for suspicious cytologiesbut also for compressive symptoms and large goiter, evenif benign, the relative proportion of patients with Thy4/Thy5 cytologies in this group were diluted, thus creatingthe bias of fewer cancers in the surgical series comparedwith N-AIT. Indeed, the criterion for surgery in the N-AIT
group was the presence of suspicious/malignant nodules atFNAC (60.7%) much more frequently than in the otherthree groups.
Our results are at variance with the cytological series byBoi et al (6, 7) and Fiore et al (8), who found an associationbetween AIT and DTC. This discrepancy deserves com-ments. As far as the two Sardinian series (6, 7) are con-cerned, a particular genetic background (Sardinia is anisland), the inclusion of patients with only single nodules,and the lack of US assessment may explain the difference.
Fiore et al (8) used the same diagnostic criteria of AITas in our study (positive antithyroid antibodies and USfeatures) and their patient population should have verysimilar genetic background of our patients (our two cen-ters are located in the same region, 140 km apart). Thus,it is difficult to explain the discrepant results between thetwo studies. However, it is intriguing that the same group,in a previous retrospective cytological series of 13 738patients (11) published in 2009, did not find any associ-ation between AIT and thyroid cancer, at variance withtheir second series published in 2011 (8). In addition, thesame group did not find any association between DTC andAIT (clinical and histological) in a series of patients sub-mitted to thyroid surgery for nodules with an indetermi-nate (Thy3) cytology (20).
We confirmed that DTC is more frequent in single nod-ules than in multinodular goiter. Our results are in agree-ment with some studies (13, 21), whereas others reportedno difference in thyroid cancer prevalence between singlenodules and multinodular goiter (22–24). A recent meta-analysis reported that thyroid cancer is less frequent inmultinodular goiter than in a single nodule, particularlyoutside the United States and perhaps in iodine deficientareas (25).
Increased levels of serum TSH are a risk factor for DTC(8, 9, 26–29), independently from the presence or absenceof AIT. With serum TSH values of 4 mU/L or greater, theprevalence of thyroid cancer in our series was as high as10% and TSH elevations were associated with increasedrate of suspicious or malignant cytologies both in patientswith positive (�100 IU/L) TPOAbs or negative TPOAbs.
In conclusion, our analysis of a large cytological seriesof thyroid nodules provides no evidence in favor of a re-lationship between AIT and thyroid cancer and suggests
Table 3. Multivariate Logistic Regression PredictingSuspicious/Malignant Cytology (Thy 3 Excluded)
Variables OR (95% CI)PValue
Single nodule 2.40 (1.605–3.610) �.0001TSH, mIU/L
Q2 (0.4–0.8) 1Q1 (�0.4) 2.17 (0.515–3.116) .66Q3 (0.9–1.4) 2.74 (1.4.23–5.353) .001Q4 (1.5–3.9) 2.75 (1.413–5.410) .001Q5 (�4.0) 3.86 (1.458–10.025) .004
Table 4. Diagnostic Accuracy of FNAC in Patients With Histological Confirmation (Thy3 Excluded)
Sensitivity Specificity PPV NPVFalsePositive
FalseNegative
Total nodules (n � 496) 89.2% 98.4% 95% 96.2% 1.6% 10.7%Nodules in AIT (n � 44 ) 95.6% 100% 100% 95.4% 0% 4.4%Nodular goiter (n � 441 ) 88.3% 98.2% 94% 96.5% 1.7% 11.6%
Abbreviations: NPV, negative predictive value; PPV, positive predictive value.
doi: 10.1210/jc.2014-1302 jcem.endojournals.org 3197
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 29 September 2014. at 15:59 For personal use only. No other uses without permission. . All rights reserved.

that the apparent association reported in surgical series isthe result of selection bias in patients’ referral for surgery.
Acknowledgments
Address all correspondence and requests for reprints to: FurioPacini, MD, Section of Endocrinology and Metabolism, Depart-ment of Medical, Surgical, and Neurological Sciences, Universityof Siena, Policlinico Santa Maria alle Scotte, Viale Bracci 1,53100 Siena, Italy. E-mail: [email protected].
This work was supported by Grant 2012Z3F7HE from theMinistero Italiano dell’Università e Ricerca.
Disclosure Summary: The authors have nothing to declare.
References
1. Bradly DP, Reddy V, Prinz RA, Gattuso P. Incidental papillary car-cinoma in patients treated surgically for benign thyroid diseases.Surgery. 2009;146:1099–1104.
2. Cipolla C, Sandonato L, Graceffa G, et al. Hashimoto thyroiditiscoexistent with papillary thyroid carcinoma. Am Surg. 2005;71:874–878.
3. Larson SD, Jackson LN, Riall TS, et al. Increased incidence of well-differentiated thyroid cancer associated with Hashimoto thyroiditisand the role of the PI3k/Akt pathway. J Am Coll Surg. 2007;204:764–773.
4. Kurukahvecioglu O, Taneri F, Yüksel O, Aydin A, Tezel E, Onuk E.Total thyroidectomy for the treatment of Hashimoto’s thyroiditiscoexisting with papillary thyroid carcinoma. Adv Ther. 2007; 24:510–516.
5. Consorti F, Loponte M, Milazzo F, Potasso L, Antonaci A. Risk ofmalignancy from thyroid nodular disease as an element of clinicalmanagement of patients with Hashimoto’s thyroiditis. Eur Surg Res.2010;45:333–337.
6. Boi F, Minerba L, Lai ML, et al. Both thyroid autoimmunity andincreased serum TSH are independent risk factors for malignancy inpatients with thyroid nodules. J Endocrinol Invest. 2013;36:313–320.
7. Boi F, Lai ML, Marziani B, Minerba L, Faa G, Mariotti S. Highprevalence of suspicious cytology in thyroid nodules associated withpositive thyroid autoantibodies. Eur J Endocrinol. 2005;153:637–642.
8. Fiore E, Rago T, Latrofa F, et al. Hashimoto’s thyroiditis is associ-ated with papillary thyroid carcinoma: role of TSH and of treatmentwith L-thyroxine. Endocr Relat Cancer. 2011;18:429–437.
9. Kim ES, Lim DJ, Baek KH, et al. Thyroglobulin antibody is associ-ated with increased cancer risk in thyroid nodules. Thyroid. 2010;20:885–891.
10. Matesa-Anic D, Matesa N, Dabelic N, Kusic Z. Coexistence of pap-illary carcinoma and Hashimoto’s thyroiditis. Acta Clin Croat.2009;48:9–12.
11. Fiore E, Rago T, Scutari M, et al. Papillary thyroid cancer, althoughstrongly associated with lymphocytic infiltration on histology, isonly weakly predicted by serum thyroid auto-antibodies in patientswith nodular thyroid diseases. J Endocrinol Invest. 2009;32:344–351.
12. Anil C, Goksel S, Gursoy A. Hashimoto’s thyroiditis is not associ-ated with increased risk of thyroid cancer in patients with thyroid
nodules: a single-center prospective study. Thyroid. 2010;20:601–606.
13. Grani G, Calvanese A, Carbotta G, et al. Thyroid autoimmunity andrisk of malignancy in thyroid nodules submitted to fine-needle as-piration cytology [published online April 2, 2014]. Head Neck. doi:10.1002/hed.23587.
14. Mazokopakis EE, Tzortzinis AA, Dalieraki-Ott EI, et al. Coexis-tence of Hashimoto’s thyroiditis with papillary thyroid carcinoma.A retrospective study. Hormones. 2010;9:312–317.
15. Repplinger D, Bargren A, Zhang YW, Adler JT, Haymart M, ChenH. Is Hashimoto’s thyroiditis a risk factor for papillary thyroid can-cer? J Surg Res. 2008;150:49–52.
16. Jankovic B, Le KT, Hershman JM. Clinical review: Hashimoto’sthyroiditis and papillary thyroid carcinoma: is there a correlation?J Clin Endocrinol Metab. 2013;98:474–482.
17. American Thyroid Association (ATA) Guidelines Taskforce onThyroid Nodules and Differentiated Thyroid Cancer, Cooper DS,Doherty GM, et al. Revised American Thyroid Association man-agement guidelines for patients with thyroid nodules and differen-tiated thyroid cancer. Thyroid. 2009;19(11):1167–1214.
18. British Thyroid Association and Royal College of Physicians.Guidelines for the Management of Thyroid Cancer. 2nd ed. 2007www.british-thyroid-association.org.
19. Galen RS. Application of the predictive value model in the analysisof test effectiveness. Clin Lab Med. 1982;2:685–699.
20. Rago T, Di Coscio G, Ugolini C, et al. Clinical features of thyroidautoimmunity are associated with thyroiditis on histology and arenot predictive of malignancy in 570 patients with indeterminatenodules on cytology who had a thyroidectomy. Clin Endocrinol(Oxf). 2007;67:363–369.
21. Rago T, Fiore E, Scutari M, et al. Male sex, single nodularity, andyoung age are associated with the risk of finding a papillary thyroidcancer on fine-needle aspiration cytology in a large series of patientswith nodular thyroid disease. Eur J Endocrinol. 2010;162:763–770.
22. Sachmechi I, Miller E, Varatharajah R, et al. Thyroid carcinoma insingle cold nodules and in cold nodules of multinodular goiters.Endocr Pract. 2000;6:5–7.
23. Belfiore A, La Rosa GL, La Porta GA, et al. Cancer risk in patientswith cold thyroid nodules: relevance of iodine intake, sex, age, andmultinodularity. Am J Med. 1992;93:363–369.
24. Frates MC, Benson CB, Doubilet PM, et al. Prevalence and distri-bution of carcinoma in patients with solitary and multiple thyroidnodules on sonography. J Clin Endocrinol Metab. 2006;91:3411–3417.
25. Brito JP, Yarur AJ, Prokop LJ, McIver B, Murad MH, Montori VM.Prevalence of thyroid cancer in multinodular goiter versus singlenodule: a systematic review and meta-analysis. Thyroid. 2013 23:449–455.
26. Boelaert K, Horacek J, Holder RL, Watkinson JC, Sheppard MC,Franklyn JA. Serum thyrotropin concentration as a novel predictorof malignancy in thyroid nodules investigated by fine-needle aspi-ration. J Clin Endocrinol Metab. 2006;91:4295–4301.
27. Haymart MR, Glinberg SL, Liu J, Sippel RS, Jaume JC, Chen H.Higher serum TSH in thyroid cancer patients occurs independent ofage and correlates with extrathyroidal extension. Clin Endocrinol(Oxf). 2009;71:434–439.
28. Fiore E, Rago T, Provenzale MA, et al. Lower levels of TSH areassociated with a lower risk of papillary thyroid cancer in patientswith thyroid nodular disease: thyroid autonomy may play a protec-tive role. Endocr Relat Cancer. 2009;16:1251–1260.
29. Fiore E, Rago T, Provenzale MA, et al. L-thyroxine-treated patientswith nodular goiter have lower serum TSH and lower frequency ofpapillary thyroid cancer: results of a cross-sectional study on 27 914patients. Endocr Relat Cancer. 2010;17:231–239.
3198 Castagna et al Autoimmune Thyroiditis and Thyroid Cancer J Clin Endocrinol Metab, September 2014, 99(9):3193–3198
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 29 September 2014. at 15:59 For personal use only. No other uses without permission. . All rights reserved.