Nobel Biocare NEWS...Information for the Osseointegration Specialist Issue 2/2012 Nobel Biocare NEWS...
16
Information for the Osseointegration Specialist Issue 2/2012 N obel B iocare NEWS 2 Traditional full-arch Dependable, well-proven and better than ever! 4 TiUnite® Engineered for performance. 6 All-on-4 ™ treatment The efficient treatment concept for immediate loading. More than a decade of experience, and only from Nobel Biocare! 8 Select options A new way to look at the matter of quality of life. 10 Advanced overdentures Fixed-removable solutions: pros and cons. 12 Zygoma expands the candidate base for maxillary treatment. 14 Micromotion Truth and consequences about micromotion and the associated interfacial strains. 15 Intra-oral radiography Seven simple rules for using IOR with implant- based restorations. In this Issue treatment option, it should be noted, was pioneered by Nobel Biocare. The humble overdenture—still a good alternative to the removable denture according to the long-term data that Nobel Biocare solutions have accumulated over the years—has gone high-tech with the advent of the NobelProcera Implant Bar Overden- ture. (Read all about it on page .) There are many options to consid- er when you meet dissatisfied re- movable denture users—including zygomatic solutions for the long- time denture wearer with severely re- sorbed maxillary bone. Nobel Bio- care covers all the bases. The challenge of longevity Despite reports from the WHO that indicate that oral health is improving in all age groups globally, edentulism is still on the upswing as we’re surviving into old age in greater dividual people—potential patients— who can be helped to a better life, one at a time. In this context, the well- proven implant-based options de- picted in the column to the right rep- resent Nobel Biocare’s offerings to the dental professional in a nut shell. All of Per-Ingvar Brånemark’s first patients were edentulous cases that he treated with full-arch restorations. Consequently, no other form of oral implant treatment has more or lon- ger favorable follow-up than these traditional bone-anchored solutions. The data set extends well back into the post-war era. Nobel Biocare is proud to continue to develop new solutions based on this experience. If you’re looking for an efficient full-arch treatment concept for im- mediate loading—one that’s both af- fordable and well-proven—All-on- treatment is supported with almost fifteen years of clinical success. This Tell removable denture wearers that there is a well proven, scientifically validated, bone-anchored alternative to the countless social, emotional and even nutritional disappointments they’ve faced since losing their teeth—and they will be eager to know more. By Frederic Love I f edentulism were an infectious disease, it would be classified as a pandemic. According to the United Nations’ World Health Or- ganization (WHO), somewhere be- tween and percent of the world’s population is toothless, which is both a tragic problem for people suffering such loss, and an epic op- portunity for professionals prepared to provide oral rehabilitation with the support of Nobel Biocare. The dramatic WHO statistics are presented in the centerfold spread. As daunting as these figures are, it’s important to remember that these vast numbers do indeed represent in- Dentures are Not the Answer Millions of despondent denture wearers yearn for renewed quality of life. Don’t Miss the Next Big Thing! New York City, New York P lanning to attend only one profes- sional meeting next year? Then make it the Nobel Biocare Global Sym- posium at the Waldorf Astoria! On June –, the field’s foremost speakers will be presenting the best sci- ence to the greatest audience in the world of implant dentistry. Think that’s hyperbole? Well, that’s the way we talk in New York: an exciting city full of at- tractions that include world-class the- ater, music, sightseeing, and sports. < More to explore: Read the full article on page 14. “No one should have to die with their teeth in a glass of water beside their bed.” — Per-Ingvar Brånemark continued on page 2
Transcript of Nobel Biocare NEWS...Information for the Osseointegration Specialist Issue 2/2012 Nobel Biocare NEWS...

Information for the Osseointegration Specialist Issue 2/2012
NobelBiocareNEWS2 Traditional full-archDependable, well-provenand better than ever!
4 TiUnite® Engineeredfor performance.
6 All-on-4™ treatmentThe efficient treatmentconcept for immediateloading. More than adecade of experience, andonly from Nobel Biocare!
8 Select optionsA new way to look at thematter of quality of life.
10 Advanced overdenturesFixed-removablesolutions: pros and cons.
12 Zygoma expands thecandidate base formaxillary treatment.
14 MicromotionTruth and consequencesabout micromotion andthe associated interfacialstrains.
15 Intra-oral radiographySeven simple rules forusing IOR with implant-based restorations.
In this Issue
treatment option, it should be noted,was pioneered by Nobel Biocare.The humble overdenture—still a
good alternative to the removabledenture according to the long-termdata that Nobel Biocare solutions haveaccumulated over the years—has gone
high-tech with the advent of theNobelProcera Implant Bar Overden-ture. (Read all about it on page .)
There are many options to consid-er when you meet dissatisfied re-movable denture users—includingzygomatic solutions for the long-time denture wearer with severely re-sorbed maxillary bone. Nobel Bio-care covers all the bases.
The challenge of longevityDespite reports from the WHO thatindicate that oral health is improvingin all age groups globally, edentulismis still on the upswing as we’resurviving into old age in greater
dividual people—potential patients—who can be helped to a better life, oneat a time. In this context, the well-proven implant-based options de-picted in the column to the right rep-resent Nobel Biocare’s offerings to thedental professional in a nut shell.
All of Per-Ingvar Brånemark’s firstpatients were edentulous cases thathe treated with full-arch restorations.Consequently, no other form of oralimplant treatment has more or lon-ger favorable follow-up than thesetraditional bone-anchored solutions.The data set extends well back into
the post-war era. Nobel Biocare isproud to continue to develop newsolutions based on this experience.If you’re looking for an efficient
full-arch treatment concept for im-mediate loading—one that’s both af-fordable and well-proven—All-on-treatment is supported with almostfifteen years of clinical success. This
Tell removable denturewearers that there is a wellproven, scientificallyvalidated, bone-anchoredalternative to the countlesssocial, emotional and evennutritional disappointmentsthey’ve faced since losingtheir teeth—and they will beeager to know more.
By Frederic Love
If edentulism were an infectiousdisease, it would be classified asa pandemic. According to the
United Nations’ World Health Or-ganization (WHO), somewhere be-tween and percent of the world’spopulation is toothless, which isboth a tragic problem for peoplesuffering such loss, and an epic op-portunity for professionals preparedto provide oral rehabilitation withthe support of Nobel Biocare.The dramatic WHO statistics are
presented in the centerfold spread.As daunting as these figures are, it’simportant to remember that thesevast numbers do indeed represent in-
Dentures are Not the AnswerMillions of despondent denture wearers yearn for renewed quality of life.
Don’t Miss the Next Big Thing!
New York City, New York
Planning to attend only one profes-sional meeting next year? Then
make it the Nobel Biocare Global Sym-posium at the Waldorf Astoria!On June –, the field’s foremost
speakers will be presenting the best sci-
ence to the greatest audience in theworld of implant dentistry. Think that’shyperbole? Well, that’s the way we talkin New York: an exciting city full of at-tractions that include world-class the-ater, music, sightseeing, and sports.<
More to explore:
Read the full article on page 14.
“No one should have to die with their teethin a glass of water beside their bed.”
—Per-Ingvar Brånemark
continued on page 2
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 1NB_NEWS_2-2012_master_for_publication_Switzerland.indd 1 08.10.12 14:0908.10.12 14:09

Richard Laube, CEO
Everyone deserves a healthy smile.Based on that simple premise, we atNobel Biocare follow our mission:“Designing for Life”. We provide supe-rior product and treatment solutions,including training and services, tohelp you reach more patients, withbetter treatment, than ever before.Decades ago, Per-Ingvar Bråne-
mark started a revolution by treatingedentulous patients first, and that’swhere we still have our greatest im-pact on patient quality of life today.You do your part and we do ours:
You and your fellow customers pro-vide the skills, and we at Nobel Bio-care provide the most attractive rangeof products and solutions for all indi-cations. Together, there isn’t a patientwe cannot help.Our company has a long and sto-
ried past that is reflected in the devel-opment of our well-proven edentu-lous arch solutions and—for thatmatter—our entire product portfolio.No one else builds on such extensiveexpertise and clinical data; and ourinnovative solutions and comprehen-sive product portfolio prove the point.We pride ourselves for keeping our
customers at the forefront of moderndentistry. Side-by-side, we havehelped millions of edentulous pa-tients regain their quality of life. Thisis what keeps us moving forward to-gether. <
Nobel Biocare NEWSPublished regularly by
Nobel Biocare Services AG
Vol.14, No.2, 2012
Editor-in-chief Nicolas Weidmann
Managing Editor Frederic Love
Assistant Editor Jim Mack
Editorial offices
Nobel Biocare News
Herdevägen 11
702 17 Örebro, Sweden
Telephone: +46 19-330680
Telefax: +46 19-330681
e-mail: [email protected]
web: nobelbiocare.com/newsletter
The contents of contributor’s articles do
not necessarily express the opinions
of Nobel Biocare.
© Nobel Biocare Services AG, 2012.
All rights reserved.
Nobel Biocare NEWS Issue 2/2012
From the CEO
2
NobelActive satisfies boththe surgical and restorativeclinicians’ needs.
By Jim Mack
NobelActive provides clinicianswith maximum flexibility, both
in placement and restorability, andits unique design expands treatmentoptions.With its innovative tip and thread
design, NobelActive slices throughbone, unlike conventional self-tap-ping implants, which cut the bone asthey tap. With NobelActive, bonecondensing increases progressivelywith each turn as the threads widen.This action, together with reverse-
cutting flutes and apical drillingblades, enables clinicians to makefine adjustments to implant orienta-tion during insertion in order to op-
NobelActive™High initial stability in all indications
numbers than ever before. Living afull life—rather than just surviving—requires teeth that work; and for theedentulous patient that means im-plant-based prosthetics. (See the Mc-Gill consensus report reference onpage , for example.)Implant innovations, such as
NobelSpeedy and NobelActive, de-
liver the high initial stability neces-sary to turn immediate loading intoroutine procedure today, but are onlypart of the treatment equation.You have to trust every aspect of
the treatment protocol, the associat-ed surgical and prosthetic compo-nents, and the time-proven reliabilityof the entire treatment concept, ifyou are going to recommend im-plants to the removable denturewearer. Nobel Biocare delivers on allthese points.To effectively present the good
news of implant-based alternatives todenture wearers, one has to be aware
of their worries and concerns andmake them aware of the long-termdetrimental effects of edentulism.Bone resorption leads to facial
changes, accelerated superficialsigns of aging, and masticatory diffi-culties. Even the best fitting remov-able dentures could cause additionalproblems such as difficulty speak-
ing, reluctance to laugh, and thewidely heard complaint: sore spotsand painful blisters.According to a scientific finding
published by J. Fisk et al, in , themost common complaints frompeople wearing dentures are seriousindeed. They include a sense of pre-mature aging, less self-confidenceand more frequent embarrassment.People who wear removable den-
tures report that they enjoy food anddrinks less, no longer laugh freelyand find social networking moredifficult. A poorly fitting dentureworsens the situation while an im-
plant-anchored or retained solutionimproves it.It may be difficult to get remov-
able denture wearers to meet the os-seointegration specialist—many ofthem don’t visit the dentist, exceptwhen they are having problems,after all. Still, it’s well worth the ef-fort to make the connection.
Patient seminarsNobel Biocare will help you prepareseminars for potential patients thatdescribe the differences between re-movable dentures and the implant-based alternative.Host such a seminar—so you can
meet removable denture users whoare looking for something better—and you’ll find that the functional,esthetic and (by extension) socialadvantages provided by implantstrumps the loose denture in everycategory.
Really?Conventional dentures (even withan adhesive) generally restore only% of chewing function, while abone-anchored prosthesis restores–% in similar evaluations.What about facial structure? Re-
movable dentures do provide somesupport for the lip and cheeks, ofcourse, but implant-based prosthet-ics provide even greater, morenatural-looking support.
continued from page 1
Dentures are Not the Answer
“The loss of teeth may prove painful in anumber of different ways, as one is deprived ofappearance, function and self-esteem.”
—Professor Björn Klinge
Then there is the issue of resorp-tion. Denture use may actually ac-celerate the shrinkage of jaw bone,while load-bearing implants preventresorption.Removable denture wearers often
complain of chronic problems dueto bad fit. For understandable rea-sons, implant patients rarely do.Add to these comparisons the fact
that patients with implant-support-ed prostheses never need adhesivesor a denture relining, and it’s easy tounderstand the attraction of thebone-anchored alternative.So here’s the message, we’d like to
help you deliver: A dental implantmimics the root of a tooth. Patientsget that.Let them know that a fixed solu-
tion will feel like their own teeth,that oral hygiene will require a fewnew skills and take some practice—and that treatment is possible inmost cases—and we’re sure you’llfind the response gratifying.<
Please note:
Some countries may have
restrictions for active marketing
towards patients other than your
own. Please ensure compliance
with local laws and all applicable
professional codes.
Article references available at:
nobelbiocare.com/newsletter
The patient first. Patient seminars offer removable denture wearers anopportunity to hear about the relative advantages of different Nobel Biocareimplant-based options in a relaxed, informative environment.
timize the final position of the pros-thetic connection—and all withoutjeopardizing this implant’s provenhigh initial stability.With a strong, sealed, internal
conical connection for abutment-supported restorations, and an exter-nal platform for implant-level bridgerestorations, the dual-function pros-thetic connection has been designedto maximize soft tissue volume aswell as restorative flexibility.<
More to explore:
nobelbiocare.com/nobelactive
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 2NB_NEWS_2-2012_master_for_publication_Switzerland.indd 2 08.10.12 16:5808.10.12 16:58

Nobel Biocare NEWSIssue 2/2012 3
Tried and TrueFull-mouth rehabilitation with high comfort, stability and esthetics
In this case of moderate boneresorption, a patient whowas dissatisfied with herdentures received an entirelynew, bone-anchored, thirddentition.
By Dr. Peter S. Wöhrle andDental Technician Aki Ogata
The patient in this case was a-year-old woman who had
been wearing upper and lower re-movable dentures for approximatelyone year when she first came in for aconsultation concerning bone-an-chored alternatives.Her chief complaint was about
the discomfort of her dentures, butas we discussed the matter, it be-came clear that changes in herspeech and worries that the den-tures might fall out were also con-tributing to her well-articulated
sense of insecurity. She told us thatin addition to these overriding con-cerns, her removable dentures felt“foreign” to her, and that she waslooking for a more estheticallypleasing solution.
Promising statusAn excellent candidate for implant-supported, full-arch restoration, thepatient’s overall health was verygood. She had no medical issues.At the oral examination, she pre-
sented an edentulous maxilla andmandible, both with moderate boneresorption. The top of the edentu-lous ridge was outside the estheticzone.After further discussion with the
patient, we decided upon fixed im-plant-supported bridges for the sakeof high comfort, stability and esthet-ics.We carried out implant treatment
planning in NobelClinician Soft-
The classic fixed solution
Indications: Edentulous mandible or maxilla
Principle: Multiple implants supporting a fixed full-arch prosthesis
Benefits: Looks, feels and works like natural teeth • Helps prevent
further bone loss • Preserves facial structure • Restores oral
functionality, both in terms of chewing and speaking • Greater
comfort than removable dentures • Longest history – most proven
implant-supported edentulous solution • Increases the patient’s
self-confidence and quality of life.
Surgical considerations: Can be combined with the computer-
aided guided surgery concept NobelGuide • Open flap, or recom-
mended with NobelGuide: flapless, mini-flap and flap.
Prosthetic considerations: Final restoration is possible with a wide
variety of prosthetic solutions, including NobelProcera Implant
Bridge in zirconia or titanium with acrylic veneering, or individual
NobelProcera Crowns cemented to the bridge framework.
Available implant systems: All Nobel Biocare platforms and other
major implant systems with multi-unit abutments.
NobelGuide: Prosthetic-driven diagnostics, treatment planning and
guided surgery system • Powered by NobelClinician Software,
NobelGuide is a complete treatment concept for diagnostics,
prosthetic-driven planning and guided implant surgery. Nobel-
Clinician functionalities work both individually or as part of a full
planning and guided surgery process. 1. Pre-op radiographic analysisshowed adequate bone height inthe mandible and anterior maxillafor implant placement. The pos-terior maxilla showed enlargedmaxillary sinuses.
7. Fixed implant-supported,screw-retained restorations.Porcelain veneering with gingivaland tooth shades creates a harmo-nious replacement for the missingteeth and soft tissue.
4. After verification of adequatestability of the implants, a provi-sional bridge was placed. Prior totaking the final impression, maturestable soft tissue topography isdesired.
2. New dentures, incorporatingthe prosthetic dimensions of archform, vertical dimension andocclusal plane, were fabricated andused as the radiographic guide andprovisional restoration.
8. Post-op radiograph withzirconia restorations in place.Tilting of posterior implants alonganterior walls of maxillary sinusallows posterior support withoutsinus grafts.
5. Six months after initial im-plant placement, the soft tissuesin the mandible and maxilla hadfully matured and final impressionswere made.
3. NobelClinician Software usesdigital diagnostics and planning toidentify the optimal position ofimplants within the available boneto best support the replacementteeth. We use this software rou-tinely today.
9. The patient was extremelypleased with the outcome of thetreatment. Her smile speaksvolumes about the successfulintra-oral integration of the implant-supported restorations.
6. NobelProcera Implant BridgeA zirconia implant bridge frame-work was produced, based on theprovisional restorations, andevaluated in the patient’s mouth forproper passive fit.
ware and chose flapless implantplacement using NobelGuide. At thetime of implant placement, we usedfixed temporary restorations.As can be seen in the photos
below, the final restorations werebuilt on NobelProcera ImplantBridge frameworks.Great care was taken with the
porcelain veneering, with natural-looking restorations for the missingteeth and gingival tissue as a result.Although healing times can vary
from case to case, the total elapsedtime for total treatment with thispatient was six months. <
More to explore:
For more extensive reading about
the products and solutions that
Nobel Biocare has to offer for
full-arch restoration, visit the
company website at:
nobelbiocare.com/edentulous
Removable dentures dimin-ished the quality of life of awidely respected swimmingcoach, but a Nobel Biocareimplant-based solution savedthe day.
By Richard Soh
Ilost all my teeth years ago and livedwith dentures much too long. I
love fruit, especially apples, but Icouldn’t eat them for years.Worst of all, my dentures inter-
ferred with my work. I’m a swim-ming instructor, and the water dis-solved the adhesive on my denturesso they fell out. Now that I have im-plants, I can swim for hours and I re-ally enjoy food again. And best of all:I no longer feel handicapped! <
“I no longer feel handicapped!”Meet Richard Soh, 58, from Singapore.
There’s more to this story!
If you or your patients would like
to view a video of Richard Soh
explaining how implants from
Nobel Biocare have changed his
life, visit: nobelbiocare.com/patient-
stories
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 3NB_NEWS_2-2012_master_for_publication_Switzerland.indd 3 08.10.12 14:0908.10.12 14:09

Nobel Biocare NEWS Issue 2/20124
TiUnite®– In Harmony with Mother NatureA Swiss research team presents their findings – and some striking scanning electron microscopic images.
Bone smear layer (BSL) on a NobelSpeedy Groovy implant. The BSL is covering the TiUnite surface immediately following experimental in vivo implant insertion (2/3 of its length) and retrieval.Note the presence of bone debris (BD) in the apical geometry (red arrow, left image). Both the bone smear and the bone debris may serve as a depot of enzymes and growth factors attracting boneforming cells. TiUnite, due to its porous surface, has an excellent texture for preserving the bone smear layer in the orifices of the pores (red arrow, right frame). (Schüpbach and Glauser, in prep.)
Blood clot, composed by blood cells, activated platelets and fibrin, attached to a TiUnite surface exposed to blood for 10 minutes in an in vitro experimentcarried out by the authors.
Implant surface propertiesare considered key when itcomes to advanced osseo-integration – in particularwhen healing times arereduced or implants areplaced under demandingbone conditions.In the most recent edition ofthis newsletter, the authorsdescribed how TiUniteinteracts with blood cells andtissues during early woundhealing, and how osteocon-ductive bone formation issupported. Building on thatfoundation, they discuss newfindings, which furtherexplain how additionalsurface parameters, such astexture and design, maypositively influence fast boneformation and osseointe-gration.
By Drs. Peter Schüpbachand Roland Glauser
Just prior to the turn of the cen-tury, implants with a moder-ately rough surface were intro-
duced by Nobel Biocare to enhanceosseointegration. Over the ensuingyears, an enormous number of invitro studies have been performed toreport upon and evaluate such vari-able conditions as surface energy;surface texture modification (downto the nano level); increased wetta-bility; and surface chemical modifi-cations.Despite the great cumulative vol-
ume of these in vitro reports, pivotalquestions about the biological ratio-
nale behind the faster bone forma-tion, higher bone-to-implant con-tact, and greater removal torquevalues of these implants—whencompared to smooth surface im-plants—remain to be definitively re-solved.Latest research reveals that in vivo
reality may be substantially differentfrom the in vitro situation. Duringthe installation of a TiUnite implant,the moderately rough surface tex-ture acts like a micro-grained sand-paper: It scratches along the walls ofthe cortical and trabecular bone ofthe osteotomy and emerizes thebone surface.
Interesting smear layerThis results in a several-microns-thick smear layer composed of bonedebris and blood, covering the im-plant surface.This smear layer provides osteo-
inductive potential due to the pres-ence of growth factors needed for
bone formation (Tabassum et al,).Consequently—because the bone
smear layer masks them—suchproperties of modified surfaces asincreased wettability, high surfaceenergy and chemical alteration maynot decisively influence either theinitial wound healing or subsequentbone formation.
Decisive differences existMoreover, not all so-called “rough”implant surfaces are the same re-garding their potential for establish-ing such a bone smear layer. In par-ticular, implant design, surfacetexture—as well as the preparationprotocol for the osteotomy—will in-fluence the presence and amount ofbone smear.Following implant insertion, only
the outer tips of the threads are oftenin direct contact with the adjacentbone: and implants placed in extrac-tion sockets may not generate a bone
smear layer at all in coronal areaswhere the osteotomy is wider thanthe diameter of the implant.In the absence of a bone smear
layer, TiUnite shows its full-strengthversatility by speeding up the osse-
ous healing process. Due to thepresence of free phosphate groups atthe surface (Schüpbach et al, ),TiUnite has a negative surfacecharge, attracting and activatingthrombocytes immediately.Subsequently, thrombocytes re-
lease enzymes and growth factors,thereby attracting osteogenic cells.TiUnite is highly osteoconductiveand new bone formation occursrapidly and directly on and alongthe implant surface.
Therefore, it’s not surprising thatseveral animal and human studieshave demonstrated enhanced osseo-integration—both in terms of speedand amount of bone-to-implantcontact on par with that of hydroxy-apatite surfaces—which many stillconsider the gold standard for os-teoconductivity.
The role of bone fragmentsIn the pursuit of fast and reliable os-seointegration, another factor mustbe considered. When drilling—andeven more pronounced when usingself-cutting implants—bone frag-ments will be generated and accu-mulate in the osteotomy, especiallyin the apical region. In this area, theyserve as nuclei for bone formationby guiding osteogenic cells throughthe wound and towards the TiUnitesurface.This effect is similar to that of a
graft material—but here on an os-teoinductive level. In conjunction
BSLBSL
BSLBSL
BD
S&ESafety and Efficacy
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 4NB_NEWS_2-2012_master_for_publication_Switzerland.indd 4 08.10.12 14:1008.10.12 14:10
Nobel Biocare NEWSIssue 2/2012 5
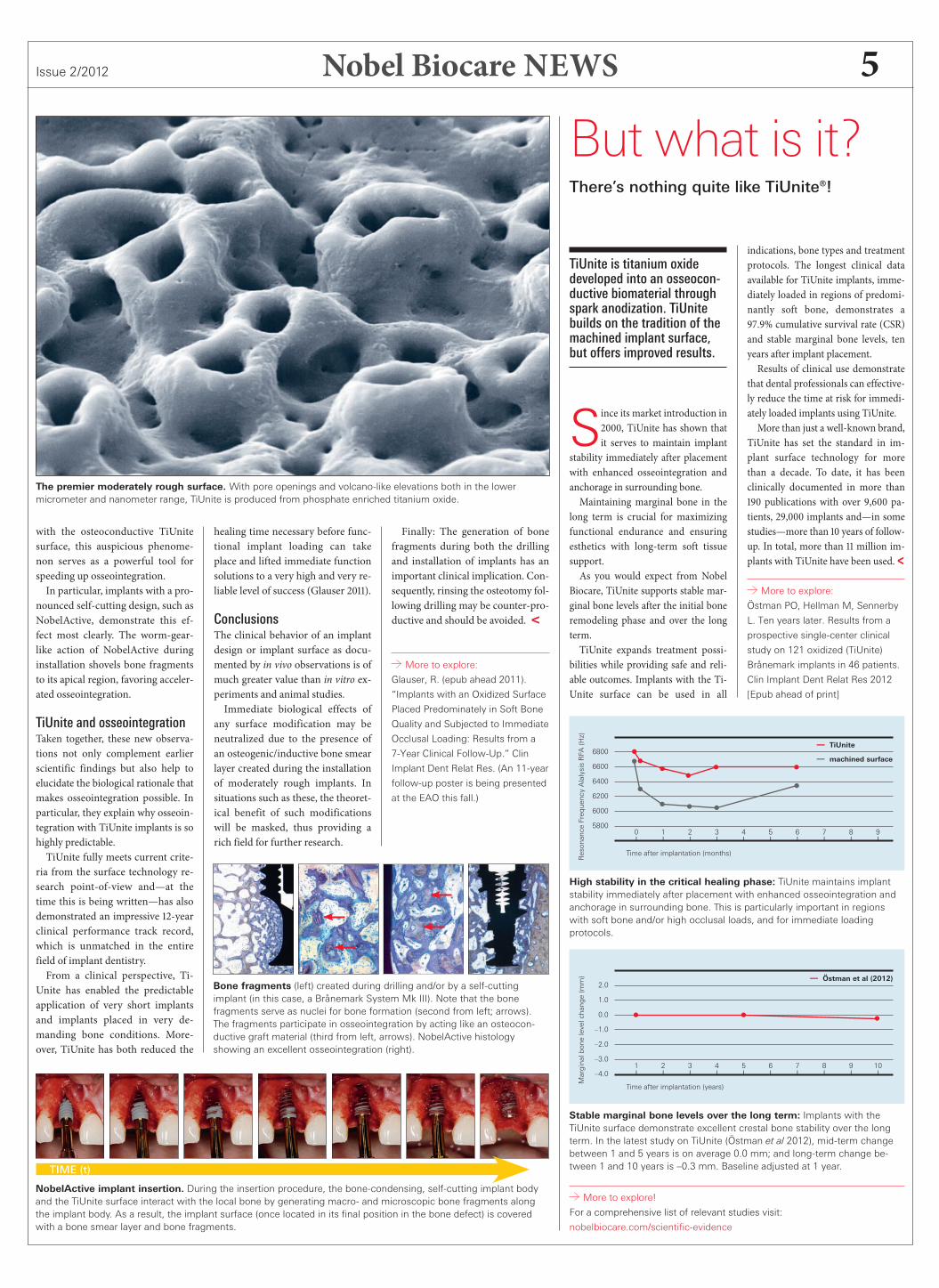
The premier moderately rough surface. With pore openings and volcano-like elevations both in the lowermicrometer and nanometer range, TiUnite is produced from phosphate enriched titanium oxide.
with the osteoconductive TiUnitesurface, this auspicious phenome-non serves as a powerful tool forspeeding up osseointegration.In particular, implants with a pro-
nounced self-cutting design, such asNobelActive, demonstrate this ef-fect most clearly. The worm-gear-like action of NobelActive duringinstallation shovels bone fragmentsto its apical region, favoring acceler-ated osseointegration.
TiUnite and osseointegrationTaken together, these new observa-tions not only complement earlierscientific findings but also help toelucidate the biological rationale thatmakes osseointegration possible. Inparticular, they explain why osseoin-tegration with TiUnite implants is sohighly predictable.TiUnite fully meets current crite-
ria from the surface technology re-search point-of-view and—at thetime this is being written—has alsodemonstrated an impressive -yearclinical performance track record,which is unmatched in the entirefield of implant dentistry.From a clinical perspective, Ti-
Unite has enabled the predictableapplication of very short implantsand implants placed in very de-manding bone conditions. More-over, TiUnite has both reduced the
healing time necessary before func-tional implant loading can takeplace and lifted immediate functionsolutions to a very high and very re-liable level of success (Glauser ).
ConclusionsThe clinical behavior of an implantdesign or implant surface as docu-mented by in vivo observations is ofmuch greater value than in vitro ex-periments and animal studies.Immediate biological effects of
any surface modification may beneutralized due to the presence ofan osteogenic/inductive bone smearlayer created during the installationof moderately rough implants. Insituations such as these, the theoret-ical benefit of such modificationswill be masked, thus providing arich field for further research.
NobelActive implant insertion. During the insertion procedure, the bone-condensing, self-cutting implant bodyand the TiUnite surface interact with the local bone by generating macro- and microscopic bone fragments alongthe implant body. As a result, the implant surface (once located in its final position in the bone defect) is coveredwith a bone smear layer and bone fragments.
TIME (t)
Finally: The generation of bonefragments during both the drillingand installation of implants has animportant clinical implication. Con-sequently, rinsing the osteotomy fol-lowing drilling may be counter-pro-ductive and should be avoided. <
More to explore:
Glauser, R. (epub ahead 2011).
“Implants with an Oxidized Surface
Placed Predominately in Soft Bone
Quality and Subjected to Immediate
Occlusal Loading: Results from a
7-Year Clinical Follow-Up.” Clin
Implant Dent Relat Res. (An 11-year
follow-up poster is being presented
at the EAO this fall.)
Bone fragments (left) created during drilling and/or by a self-cuttingimplant (in this case, a Brånemark System Mk III). Note that the bonefragments serve as nuclei for bone formation (second from left; arrows).The fragments participate in osseointegration by acting like an osteocon-ductive graft material (third from left, arrows). NobelActive histologyshowing an excellent osseointegration (right).
But what is it?There’s nothing quite like TiUnite®!
TiUnite is titanium oxidedeveloped into an osseocon-ductive biomaterial throughspark anodization. TiUnitebuilds on the tradition of themachined implant surface,but offers improved results.
Since its market introduction in, TiUnite has shown thatit serves to maintain implant
stability immediately after placementwith enhanced osseointegration andanchorage in surrounding bone.Maintaining marginal bone in the
long term is crucial for maximizingfunctional endurance and ensuringesthetics with long-term soft tissuesupport.As you would expect from Nobel
Biocare, TiUnite supports stable mar-ginal bone levels after the initial boneremodeling phase and over the longterm.TiUnite expands treatment possi-
bilities while providing safe and reli-able outcomes. Implants with the Ti-Unite surface can be used in all
More to explore!
For a comprehensive list of relevant studies visit:
nobelbiocare.com/scientific-evidence
indications, bone types and treatmentprotocols. The longest clinical dataavailable for TiUnite implants, imme-diately loaded in regions of predomi-nantly soft bone, demonstrates a.% cumulative survival rate (CSR)and stable marginal bone levels, tenyears after implant placement.Results of clinical use demonstrate
that dental professionals can effective-ly reduce the time at risk for immedi-ately loaded implants using TiUnite.More than just a well-known brand,
TiUnite has set the standard in im-plant surface technology for morethan a decade. To date, it has beenclinically documented in more than publications with over , pa-tients, , implants and—in somestudies—more than years of follow-up. In total, more than million im-plants with TiUnite have been used. <
More to explore:
Östman PO, Hellman M, Sennerby
L. Ten years later. Results from a
prospective single-center clinical
study on 121 oxidized (TiUnite)
Brånemark implants in 46 patients.
Clin Implant Dent Relat Res 2012
[Epub ahead of print]
Stable marginal bone levels over the long term: Implants with theTiUnite surface demonstrate excellent crestal bone stability over the longterm. In the latest study on TiUnite (Östman et al 2012), mid-term changebetween 1 and 5 years is on average 0.0 mm; and long-term change be-tween 1 and 10 years is –0.3 mm. Baseline adjusted at 1 year.
High stability in the critical healing phase: TiUnite maintains implantstability immediately after placement with enhanced osseointegration andanchorage in surrounding bone. This is particularly important in regionswith soft bone and/or high occlusal loads, and for immediate loadingprotocols.
6800
6600
6400
6200
6000
5800
ResonanceFrequencyAlalysisRFA(Hz)
0 1 2 3 4 5 6 7 8 9| | | | | | | | | |
Time after implantation (months)
— TiUnite
— machined surface
2.0
1.0
0.0
–1.0
–2.0
–3.0
–4.0
Marginalbonelevelchange(mm)
1 2 3 4 5 6 7 8 9 10| | | | | | | | | |
Time after implantation (years)
— Östman et al (2012)
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 5NB_NEWS_2-2012_master_for_publication_Switzerland.indd 5 08.10.12 14:1008.10.12 14:10
Nobel Biocare NEWS Issue 2/20126
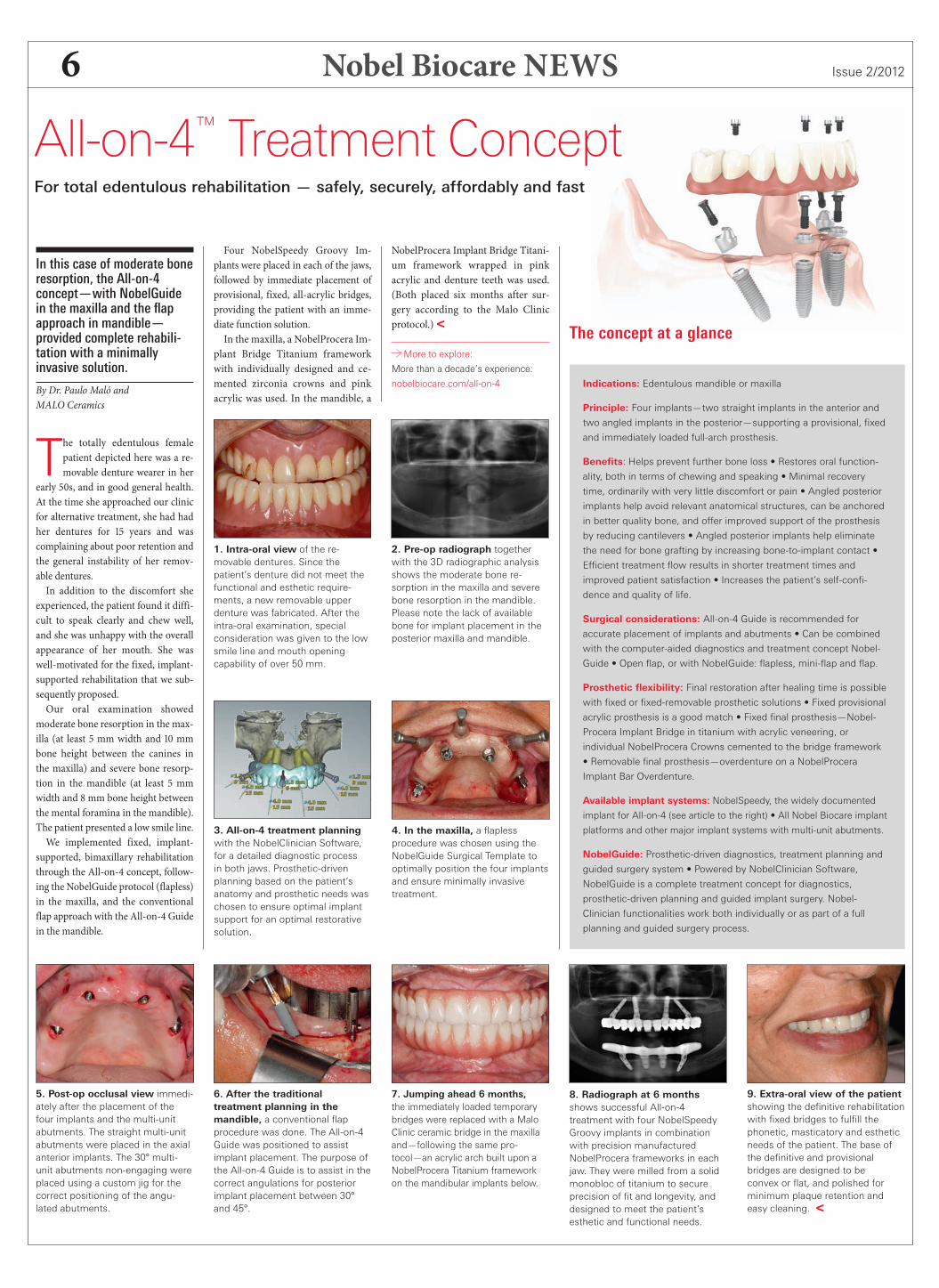
1. Intra-oral view of the re-movable dentures. Since thepatient’s denture did not meet thefunctional and esthetic require-ments, a new removable upperdenture was fabricated. After theintra-oral examination, specialconsideration was given to the lowsmile line and mouth openingcapability of over 50 mm.
2. Pre-op radiograph togetherwith the 3D radiographic analysisshows the moderate bone re-sorption in the maxilla and severebone resorption in the mandible.Please note the lack of availablebone for implant placement in theposterior maxilla and mandible.
3. All-on-4 treatment planningwith the NobelClinician Software,for a detailed diagnostic processin both jaws. Prosthetic-drivenplanning based on the patient’sanatomy and prosthetic needs waschosen to ensure optimal implantsupport for an optimal restorativesolution.
4. In the maxilla, a flaplessprocedure was chosen using theNobelGuide Surgical Template tooptimally position the four implantsand ensure minimally invasivetreatment.
5. Post-op occlusal view immedi-ately after the placement of thefour implants and the multi-unitabutments. The straight multi-unitabutments were placed in the axialanterior implants. The 30° multi-unit abutments non-engaging wereplaced using a custom jig for thecorrect positioning of the angu-lated abutments.
6. After the traditionaltreatment planning in themandible, a conventional flapprocedure was done. The All-on-4Guide was positioned to assistimplant placement. The purpose ofthe All-on-4 Guide is to assist in thecorrect angulations for posteriorimplant placement between 30°and 45°.
7. Jumping ahead 6 months,the immediately loaded temporarybridges were replaced with a MaloClinic ceramic bridge in the maxillaand—following the same pro-tocol—an acrylic arch built upon aNobelProcera Titanium frameworkon the mandibular implants below.
8. Radiograph at 6 monthsshows successful All-on-4treatment with four NobelSpeedyGroovy implants in combinationwith precision manufacturedNobelProcera frameworks in eachjaw. They were milled from a solidmonobloc of titanium to secureprecision of fit and longevity, anddesigned to meet the patient’sesthetic and functional needs.
9. Extra-oral view of the patientshowing the definitive rehabilitationwith fixed bridges to fulfill thephonetic, masticatory and estheticneeds of the patient. The base ofthe definitive and provisionalbridges are designed to beconvex or flat, and polished forminimum plaque retention andeasy cleaning. <
In this case of moderate boneresorption, the All-on-4concept—with NobelGuidein the maxilla and the flapapproach in mandible—provided complete rehabili-tation with a minimallyinvasive solution.
By Dr. Paulo Maló andMALO Ceramics
The totally edentulous femalepatient depicted here was a re-movable denture wearer in her
early s, and in good general health.At the time she approached our clinicfor alternative treatment, she had hadher dentures for years and wascomplaining about poor retention andthe general instability of her remov-able dentures.In addition to the discomfort she
experienced, the patient found it diffi-cult to speak clearly and chew well,and she was unhappy with the overallappearance of her mouth. She waswell-motivated for the fixed, implant-supported rehabilitation that we sub-sequently proposed.Our oral examination showed
moderate bone resorption in the max-illa (at least mm width and mmbone height between the canines inthe maxilla) and severe bone resorp-tion in the mandible (at least mmwidth and mm bone height betweenthe mental foramina in the mandible).The patient presented a low smile line.We implemented fixed, implant-
supported, bimaxillary rehabilitationthrough the All-on- concept, follow-ing the NobelGuide protocol (flapless)in the maxilla, and the conventionalflap approach with the All-on-Guidein the mandible.
Four NobelSpeedy Groovy Im-plants were placed in each of the jaws,followed by immediate placement ofprovisional, fixed, all-acrylic bridges,providing the patient with an imme-diate function solution.In the maxilla, a NobelProcera Im-
plant Bridge Titanium frameworkwith individually designed and ce-mented zirconia crowns and pinkacrylic was used. In the mandible, a
NobelProcera Implant Bridge Titani-um framework wrapped in pinkacrylic and denture teeth was used.(Both placed six months after sur-gery according to the Malo Clinicprotocol.)<
More to explore:
More than a decade’s experience:
nobelbiocare.com/all-on-4
All-on-4™ Treatment ConceptFor total edentulous rehabilitation — safely, securely, affordably and fast
The concept at a glance
Indications: Edentulous mandible or maxilla
Principle: Four implants—two straight implants in the anterior and
two angled implants in the posterior—supporting a provisional, fixed
and immediately loaded full-arch prosthesis.
Benefits: Helps prevent further bone loss • Restores oral function-
ality, both in terms of chewing and speaking • Minimal recovery
time, ordinarily with very little discomfort or pain • Angled posterior
implants help avoid relevant anatomical structures, can be anchored
in better quality bone, and offer improved support of the prosthesis
by reducing cantilevers • Angled posterior implants help eliminate
the need for bone grafting by increasing bone-to-implant contact •
Efficient treatment flow results in shorter treatment times and
improved patient satisfaction • Increases the patient’s self-confi-
dence and quality of life.
Surgical considerations: All-on-4 Guide is recommended for
accurate placement of implants and abutments • Can be combined
with the computer-aided diagnostics and treatment concept Nobel-
Guide • Open flap, or with NobelGuide: flapless, mini-flap and flap.
Prosthetic flexibility: Final restoration after healing time is possible
with fixed or fixed-removable prosthetic solutions • Fixed provisional
acrylic prosthesis is a good match • Fixed final prosthesis—Nobel-
Procera Implant Bridge in titanium with acrylic veneering, or
individual NobelProcera Crowns cemented to the bridge framework
• Removable final prosthesis—overdenture on a NobelProcera
Implant Bar Overdenture.
Available implant systems: NobelSpeedy, the widely documented
implant for All-on-4 (see article to the right) • All Nobel Biocare implant
platforms and other major implant systems with multi-unit abutments.
NobelGuide: Prosthetic-driven diagnostics, treatment planning and
guided surgery system • Powered by NobelClinician Software,
NobelGuide is a complete treatment concept for diagnostics,
prosthetic-driven planning and guided implant surgery. Nobel-
Clinician functionalities work both individually or as part of a full
planning and guided surgery process.
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 6NB_NEWS_2-2012_master_for_publication_Switzerland.indd 6 08.10.12 14:1008.10.12 14:10

Nobel Biocare NEWSIssue 2/2012 7
By Carole Lane
For much of my life, I sufferedfrom gum disease, bone loss and
unstable teeth. I was very self-con-scious about my situation andthought that there was no solution tomy problem.My dentist had told me that I
wasn’t a suitable patient for dentalimplants because of the bone loss.Then I read an article in the pressabout a new procedure called theAll-on- treatment concept and re-gained hope. After an Internet searchof local dentists, I found out thatQueensway Dental Clinic in Billing-ham (UK) offered the procedure,and made an appointment.From my first consultation with
Dr. Ian Lane (no relation), I felt total-ly at ease and confident. After givingthe recommendation for All-on-
treatment proper consideration, Idecided to go ahead and made an ap-pointment for a few weeks later tobegin the design of my new teeth.Not long afterwards, the proce-
dure was carried out in a single dayby a consultant surgeon, Rob Banks,and the final prosthesis was pro-duced onsite by the Queensway Lab-oratory. Throughout the treatment Ihad conscious sedation and it was to-
tally pain-free. Even afterwards therewas no bruising, just some slightswelling the next day.I cannot believe the difference
All-on- has made in my life, and Ihave been astonished by all the com-pliments I have received. My teethlook totally natural, and my hus-band says that my teeth and smileare back to what they once were.Life is good! <
Designed for immediatefunction, NobelSpeedy is theoriginal implant for theAll-on-4 treatment concept.
By Frederic Love
Well-documented, the Nobel-Speedy product line is de-
signed for immediate function andencompasses a versatile assortmentof implants.This ingenious implant has a drill-
ing protocol that varies dependingon bone quality. The resulting reduc-tion of chair time is beneficial for thepatient and dentist alike.Developed to cut through locally
dense bone and facilitate bicorticalanchorage, Nobel Biocare intro-duced this implant to ensure highinitial stability in soft to mediumbone, thus enabling the immediate
function protocol. In addition to itssurgical advantages, prosthetic flexi-bility is also a hallmark of Nobel-Speedy, as it provides a choice of ei-ther external or internal connections.Efficient surgical procedures and
prosthetic flexibility make Nobel-Speedy the cost-effective choice forAll-on- treatment. <
NobelSpeedy™ ImplantsA classic choice for the All-on-4™ concept
NobelSpeedyGroovy
NobelSpeedyReplace
One implant design,two prostheticconnections.
The Challenge of a LifetimeA predicament in need of a solution
Years ago, a young dentistwas confronted with theissue of total edentulism in apoignant situation that was,at the time, all too commonin the dental profession.
By Dr. Paulo Maló
Iwas meeting with a patientwhose quality of life would haveimproved enormously, had I
only been able to provide him with acomplete bone-anchored solution.Unfortunately, I had to tell him thatplacing implants in his maxilla wasvirtually impossible due to the lackof viable bone tissue there.Back in the nineties, in his situa-
tion, the only practicable implantsolution involved preparatory bonegrafting, also known as bone aug-mentation, but such a costly proce-dure was out of my patient’s reach fi-nancially, and his history of heartproblems indicated that it would notbe wise to proceed with such an in-vasive course of action in any case.Unfortunately, cases like his
were—and continue to be—com-monplace among seniors.Under the best of circumstances,
bone grafting can provide an effec-
tive foundation for implant-basedprostheses. Unfortunately, the ag-gregate need among the totallyedentulous population for perma-nent solutions (and thus genuineoral rehabilitation) far outstrips thenumber of best-of-circumstancescases.Looking at the big picture, it be-
came obvious to me that the optimalgeneral solution to the problem oftotal edentulism was not going tocomprise bone augmentation.
Unacceptable status quoToo many patients either could notbe recommended for such proce-dures as a result of physiologicallimitations, or would not be able tofinance such complex, multi-stagetreatment.Even if these obstacles could be
overcome, there was still the ques-tion of the availability of surgeonsskilled in the procedures of bonegrafting.When an estimated % of the
population over in North Ameri-ca and Europe is in need of completeoral rehabilitation (see page formore figures), it is self-evident that amore time-efficient and reliable pro-cedure than bone grafting is neededto meet burgeoning demand.
I decided to tackle the problem.My objective was simple: to providefixed, long-lasting teeth on a reliablebasis for my totally edentulous pa-tients, who were a large and growingpart of my practice. In order to meetthis goal, I devised the followingstrategy.First, I would determine the mini-
mum amount of bone volume thatwas required for the routinely suc-cessful use of existing implant tech-nology in connection with fixedprosthetics.Second, in the pursuit of alterna-
tive solutions, I would retroactivelyevaluate all the totally edentulouscases that had been treated at myclinic for which the generally ac-cepted implant procedures of thetime could not be recommended. Ispent a great deal of time exploringtreatment alternatives through thereview of scientific literature. In theprocess, an intriguing questionarose.How many teeth do we really
need to assure pleasant esthetics andgood masticatory function? No oneseemed to be posing this question inthe dental journals, yet without ananswer, it would be impossible tooptimize the bone-anchored reha-bilitation I was pursuing.
New thinkingThink of it this way: As the numberof teeth in a full-arch restoration in-creases, so does the amount of boneneeded to support the underlyingimplants that support it.In order to determine the mini-
mum number of teeth needed toguarantee good mastication and es-thetics, we devised something wecalled the “nut test.” We gave ourtest subjects a standardized portionof almonds, asked them to chew for
ten seconds, and then we aspiratedthe crushed nuts in order to subse-quently measure the size of the par-ticles; the idea being that the smallerthe particles, the greater the masti-catory efficiency.We compared the results from sub-
jects with arches comprising teeth(nd premolar to nd premolar) to
Dr. Paulo Maló of Lisbon, Portugal, has spent most of his professional lifedeveloping protocols devised to make oral rehabilitation possible—not tomention affordable—for patients who were previously not considered goodcandidates for implant-based rehabilitation.
continued on page 14
“I cannot believe the differenceAll-on-4™ has made in my life!”
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 7NB_NEWS_2-2012_master_for_publication_Switzerland.indd 7 08.10.12 14:1008.10.12 14:10
Nobel Biocare NEWS Issue 2/20128
If a picture is worth athousand words, then what’sthe value of a healthy smile?For many people sufferingwith edentulism, gettingtheir smile back could bepriceless.
By Jim Mack
Not everyone was gifted witha straight jaw line and a pic-ture-perfect smile. As the
world’s population continues togrow, there are ever larger numbersof people who don’t even have theprimary components of such a smile:teeth.Professor Brånemark has often
stated that losing even one tooth canbe considered a major defect, result-ing in a significant blow to a person’sidentity. The World Health Organi-zation (WHO) has even gone as faras to classify the edentulous as physi-cally impaired.Losing one or more teeth leads to
cascading repercussions that culmi-nate in a pool of complex conse-quences that include both functionaland emotional side-effects.
One true solutionModern implant-based dentistry hasdelivered something to the edentu-lous patient that conventional den-tures have never quite managed bycomparison—substantially increasedquality of life.A prosthesis held solidly in place
by dental implants not only providesthe comfort and security a patient islikely to be missing with removabledentures, it also preserves bone. Addto the equation emotional benefits—such as improved self-image, in-creased self-confidence and a re-newed social life—and an im-plant-based restoration becomes theclear choice.At Nobel Biocare we offer the
widest range of advanced treatmentsolutions available for treating eden-tulous patients. Combining diagnos-tics, treatment planning and guidedsurgery with implants for every situ-ation and versatile prosthetics, wehave scientifically proven options tomeet every patient’s need.<
More to explore
For details on all the solutions
Nobel Biocare provides for
edentulism, please go to
nobelbiocare.com/edentulous
Conventional dentures areNOT the answer
Lose more than confidence
• Severe bone resorption mayoccur without implant treatment.
• Conventional dentures can fallout at any time.
• Avoiding food can lead tonutritional deficiencies.
• Altered self-image.
• Avoiding social situations.
• Restores only 10% of thechewing function.
• Poorly fitting dentures may leadto sore spots or painful blisters.
• Dentures may need occasionalrelining.
• Adhesives must often be addedfor comfort.
• Can limit lip and cheek support.
A limited alternative
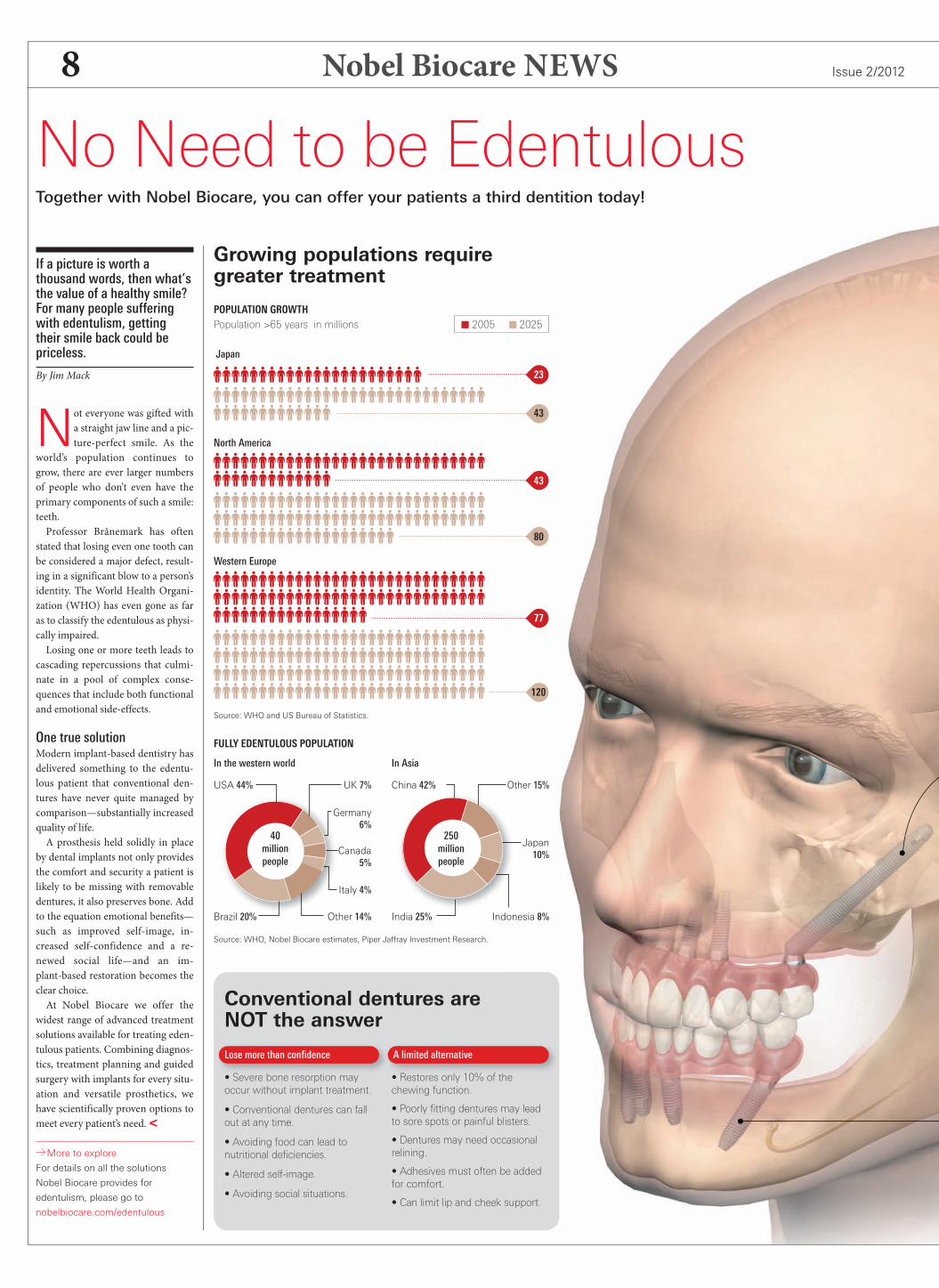
Growing populations requiregreater treatment
POPULATION GROWTH
23
43
77
43
80
120
FULLY EDENTULOUS POPULATION
Population >65 years in millions 2005 2025
In the western world In Asia
Japan
North America
Western Europe
China 42%
Source: WHO, Nobel Biocare estimates, Piper Jaffray Investment Research.
Source: WHO and US Bureau of Statistics.
India 25%Other 14% Indonesia 8%
Italy 4%
Canada5%
Japan10%
Germany6%
UK 7% Other 15%
40millionpeople
250millionpeople
No Need to be EdentulousTogether with Nobel Biocare, you can offer your patients a third dentition today!
USA 44%
Brazil 20%
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 8NB_NEWS_2-2012_master_for_publication_Switzerland.indd 8 08.10.12 14:1008.10.12 14:10
Nobel Biocare NEWSIssue 2/2012 9
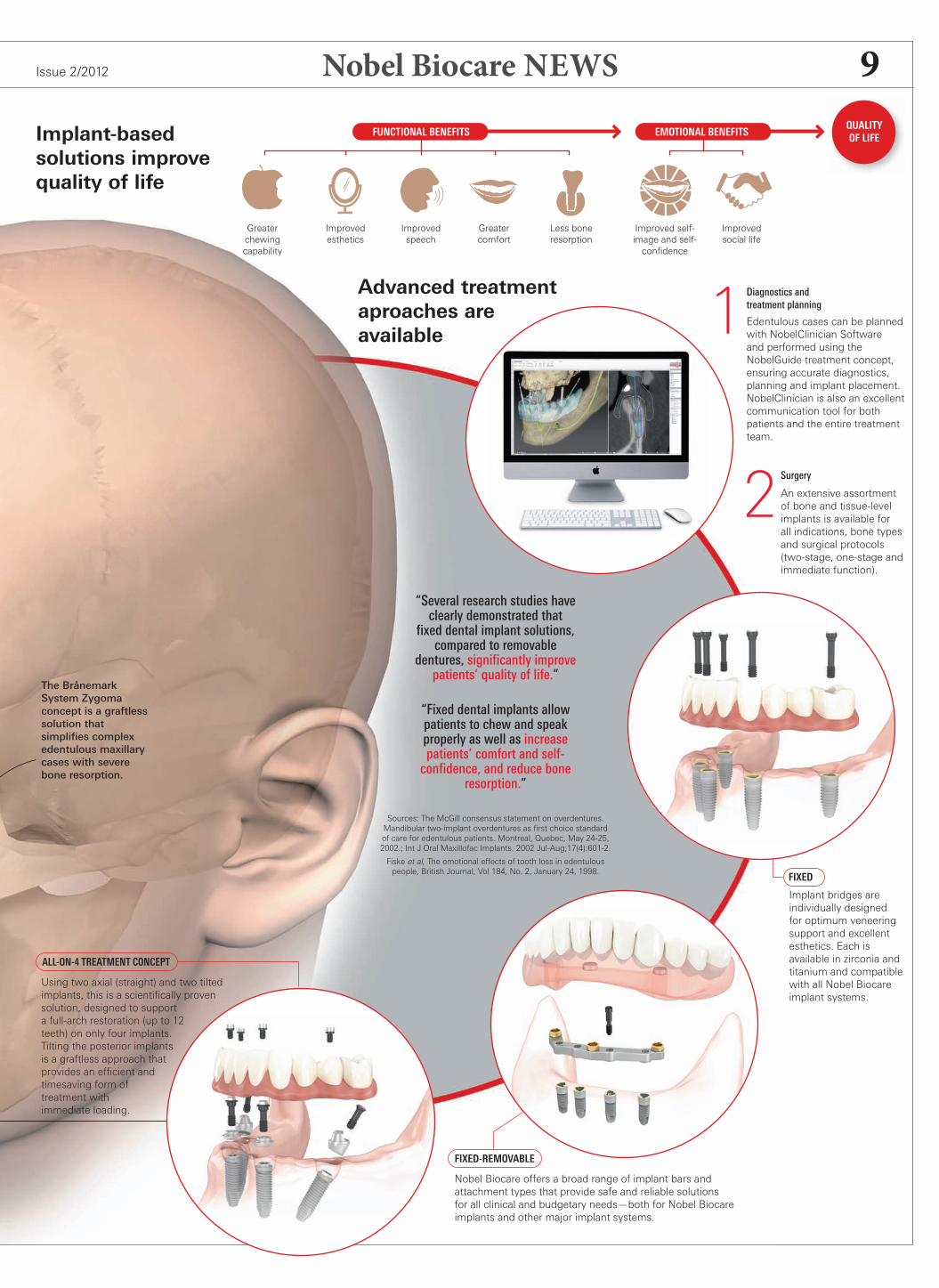
Implant-basedsolutions improvequality of life
FIXED-REMOVABLE
FIXED
ALL-ON-4 TREATMENT CONCEPT
Diagnostics andtreatment planning
Edentulous cases can be plannedwith NobelClinician Softwareand performed using theNobelGuide treatment concept,ensuring accurate diagnostics,planning and implant placement.NobelClinician is also an excellentcommunication tool for bothpatients and the entire treatmentteam.
1
Surgery
An extensive assortmentof bone and tissue-levelimplants is available forall indications, bone typesand surgical protocols(two-stage, one-stage andimmediate function).
2“Several research studies haveclearly demonstrated thatfixed dental implant solutions,compared to removable
dentures, significantly improvepatients’ quality of life.”
“Fixed dental implants allowpatients to chew and speakproperly as well as increasepatients’ comfort and self-confidence, and reduce bone
resorption.”
Sources: The McGill consensus statement on overdentures.Mandibular two-implant overdentures as first choice standardof care for edentulous patients. Montreal, Quebec, May 24-25,2002.; Int J Oral Maxillofac Implants. 2002 Jul-Aug;17(4):601-2.
Fiske et al, The emotional effects of tooth loss in edentulouspeople, British Journal, Vol 184, No. 2, January 24, 1998.
Implant bridges areindividually designedfor optimum veneeringsupport and excellentesthetics. Each isavailable in zirconia andtitanium and compatiblewith all Nobel Biocareimplant systems.
Nobel Biocare offers a broad range of implant bars andattachment types that provide safe and reliable solutionsfor all clinical and budgetary needs—both for Nobel Biocareimplants and other major implant systems.
Using two axial (straight) and two tiltedimplants, this is a scientifically provensolution, designed to supporta full-arch restoration (up to 12teeth) on only four implants.Tilting the posterior implantsis a graftless approach thatprovides an efficient andtimesaving form oftreatment withimmediate loading.
QUALITYOF LIFE
Greaterchewingcapability
Improvedspeech
Improvedesthetics
Greatercomfort
Less boneresorption
Improved self-image and self-confidence
Improvedsocial life
Advanced treatmentaproaches areavailable
The BrånemarkSystem Zygomaconcept is a graftlesssolution thatsimplifies complexedentulous maxillarycases with severebone resorption.
FUNCTIONAL BENEFITS EMOTIONAL BENEFITS
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 9NB_NEWS_2-2012_master_for_publication_Switzerland.indd 9 08.10.12 14:1008.10.12 14:10
Nobel Biocare NEWS Issue 2/201210
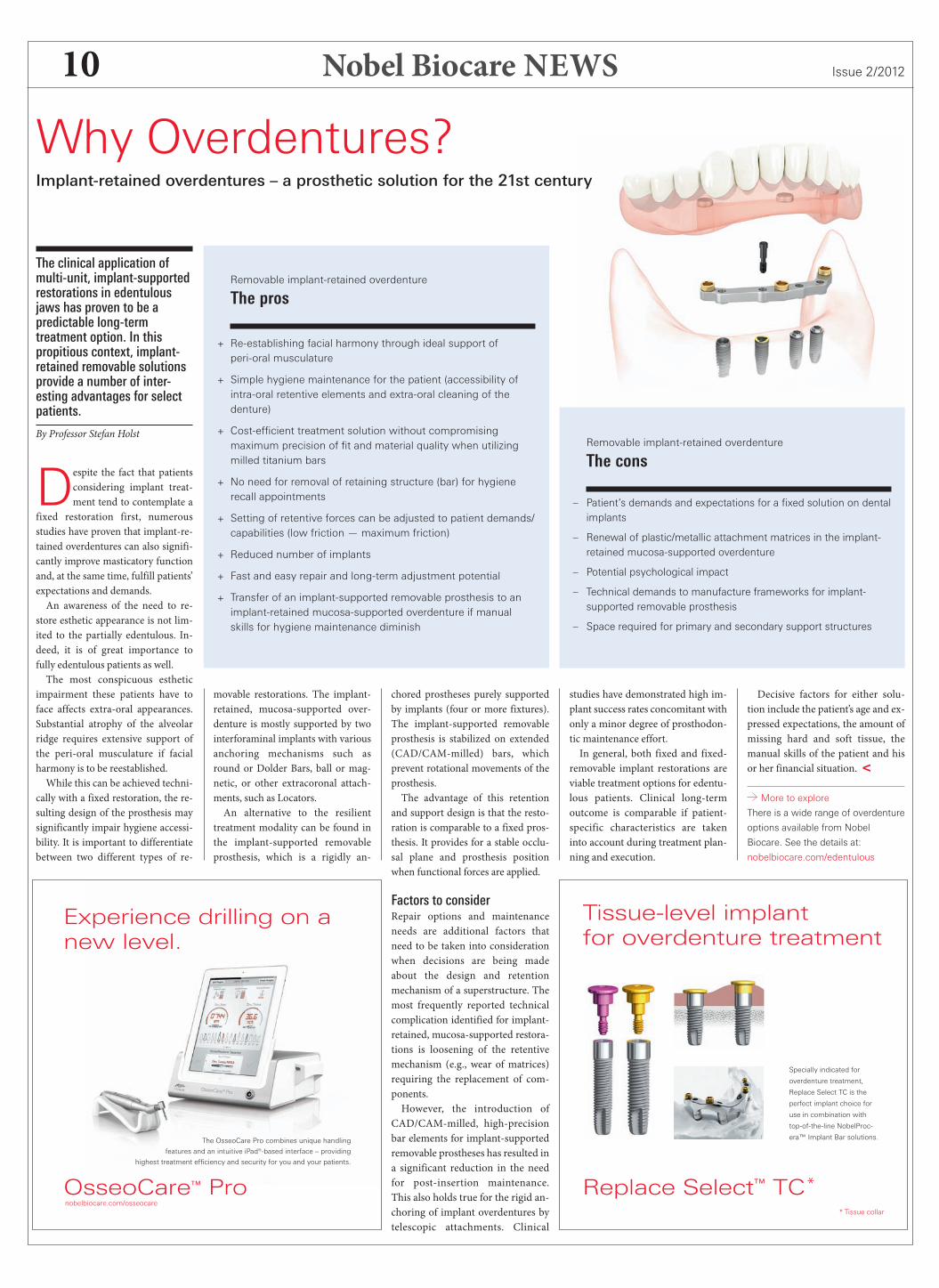
The clinical application ofmulti-unit, implant-supportedrestorations in edentulousjaws has proven to be apredictable long-termtreatment option. In thispropitious context, implant-retained removable solutionsprovide a number of inter-esting advantages for selectpatients.
By Professor Stefan Holst
Despite the fact that patientsconsidering implant treat-ment tend to contemplate a
fixed restoration first, numerousstudies have proven that implant-re-tained overdentures can also signifi-cantly improve masticatory functionand, at the same time, fulfill patients’expectations and demands.An awareness of the need to re-
store esthetic appearance is not lim-ited to the partially edentulous. In-deed, it is of great importance tofully edentulous patients as well.The most conspicuous esthetic
impairment these patients have toface affects extra-oral appearances.Substantial atrophy of the alveolarridge requires extensive support ofthe peri-oral musculature if facialharmony is to be reestablished.While this can be achieved techni-
cally with a fixed restoration, the re-sulting design of the prosthesis maysignificantly impair hygiene accessi-bility. It is important to differentiatebetween two different types of re-
movable restorations. The implant-retained, mucosa-supported over-denture is mostly supported by twointerforaminal implants with variousanchoring mechanisms such asround or Dolder Bars, ball or mag-netic, or other extracoronal attach-ments, such as Locators.An alternative to the resilient
treatment modality can be found inthe implant-supported removableprosthesis, which is a rigidly an-
Why Overdentures?Implant-retained overdentures – a prosthetic solution for the 21st century
chored prostheses purely supportedby implants (four or more fixtures).The implant-supported removableprosthesis is stabilized on extended(CAD/CAM-milled) bars, whichprevent rotational movements of theprosthesis.The advantage of this retention
and support design is that the resto-ration is comparable to a fixed pros-thesis. It provides for a stable occlu-sal plane and prosthesis positionwhen functional forces are applied.
Factors to considerRepair options and maintenanceneeds are additional factors thatneed to be taken into considerationwhen decisions are being madeabout the design and retentionmechanism of a superstructure. Themost frequently reported technicalcomplication identified for implant-retained, mucosa-supported restora-tions is loosening of the retentivemechanism (e.g., wear of matrices)requiring the replacement of com-ponents.However, the introduction of
CAD/CAM-milled, high-precisionbar elements for implant-supportedremovable prostheses has resulted ina significant reduction in the needfor post-insertion maintenance.This also holds true for the rigid an-choring of implant overdentures bytelescopic attachments. Clinical
Removable implant-retained overdenture
The pros
+ Re-establishing facial harmony through ideal support ofperi-oral musculature
+ Simple hygiene maintenance for the patient (accessibility ofintra-oral retentive elements and extra-oral cleaning of thedenture)
+ Cost-efficient treatment solution without compromisingmaximum precision of fit and material quality when utilizingmilled titanium bars
+ No need for removal of retaining structure (bar) for hygienerecall appointments
+ Setting of retentive forces can be adjusted to patient demands/capabilities (low friction — maximum friction)
+ Reduced number of implants
+ Fast and easy repair and long-term adjustment potential
+ Transfer of an implant-supported removable prosthesis to animplant-retained mucosa-supported overdenture if manualskills for hygiene maintenance diminish
Removable implant-retained overdenture
The cons
– Patient’s demands and expectations for a fixed solution on dentalimplants
– Renewal of plastic/metallic attachment matrices in the implant-retained mucosa-supported overdenture
– Potential psychological impact
– Technical demands to manufacture frameworks for implant-supported removable prosthesis
– Space required for primary and secondary support structures
studies have demonstrated high im-plant success rates concomitant withonly a minor degree of prosthodon-tic maintenance effort.In general, both fixed and fixed-
removable implant restorations areviable treatment options for edentu-lous patients. Clinical long-termoutcome is comparable if patient-specific characteristics are takeninto account during treatment plan-ning and execution.
Decisive factors for either solu-tion include the patient’s age and ex-pressed expectations, the amount ofmissing hard and soft tissue, themanual skills of the patient and hisor her financial situation. <
More to explore
There is a wide range of overdenture
options available from Nobel
Biocare. See the details at:
nobelbiocare.com/edentulous
Experience drilling on anew level.
OsseoCare™ Pro
The OsseoCare Pro combines unique handling
features and an intuitive iPad®-based interface – providing
highest treatment efficiency and security for you and your patients.
nobelbiocare.com/osseocare
Replace Select™ TC*
Specially indicated for
overdenture treatment,
Replace Select TC is the
perfect implant choice for
use in combination with
top-of-the-line NobelProc-
era™ Implant Bar solutions.
* Tissue collar
Tissue-level implantfor overdenture treatment
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 10NB_NEWS_2-2012_master_for_publication_Switzerland.indd 10 08.10.12 14:1008.10.12 14:10

Nobel Biocare NEWSIssue 2/2012 11
Visit Nobel Biocare at eventsaround the world. They providea great opportunity for observingthe latest innovations andscientific research, but also formeeting and interacting with thedental community and withindustry experts.Nobel Biocare participates ina number of key industry eventsand symposia across the globeeach year, and hosts its ownleading scientific congresses tobetter gauge and meet the needsof customers and their patients.
2012
ACP Annual Session
31 October – 3 November
Baltimore, Maryland, USA
SADA Conference
1–3 November
Cape Town, South Africa
Osteology Foundation Symposium
8–10 November
São Paulo, Brazil
OMD Congress
8–10 November
Porto, Portugal
Swedental
15–17 November
Gothenburg, Sweden
GNYD Congress
23–28 November
New York City, New York, USA
ADF Annual Meeting
27 November – 1 December
Paris, France
SGI, DGI, ÖGI Congress
29 November – 1 December
Bern, Switzerland
AAOMS DIC Congress
29 November – 1 December
Chicago, Illinois, USA
2013
CDS Midwinter Meeting
21–23 February
Chicago, Illinois, USA
LMT Lab Day
22–23 February
Chicago, Illinois, USA
AO Annual Meeting
7–9 March
Tampa, Florida, USA
IDS
12–16 March
Cologne, Germany
IADR General Session
20–23 March
Seattle, Washington, USA
Nobel Biocare Global Symposium 2013
20–23 June
New York City, New York, USA
To find out more, visit |
nobelbiocare.com/events
UpcomingEvents
NobelProcera™ Implant BridgesWhen only the best is good enough
Reporting from Japan, one ofthe country’s leading dentaltechnicians writes about whyhe prefers to provide Nobel-Procera Implant Bridges forthe treatment of discerningpatients.
By Mr. Atsushi Sogo
Given the increase in implanttreatment in recent years, itis not surprising that a
greater number of problems havealso been reported.Besides a greater absolute number
of implant failures due to impropertreatment, patients complain in in-creasing numbers about the designand shape of the final restoration. Inmy experience, failing to meet pa-tient expectations is most likely dueto a lack of communication.Discerning patients have high ex-
pectations for their implant treat-ment. They anticipate a high level ofsurgical and prosthetic performanceand may not be willing to accept a
compromised superstructure even ifthe doctor had no choice due to thestatus of the patient’s oral cavity.The doctor must always under-
stand the patient’s expectations andprovide an adequate explanation ofthe treatment.One way for the doctor and the
patient to come to agreement ami-cably is for them to come to termsduring the consultation phase on
what should be expected of the finalimplant-based restoration.
The ideal restoration can be char-acterized by good functionality, fit,strength, ease of cleaning, biocom-patibility and esthetics. A good bal-ance between these factors is impor-tant and no one factor should besignificantly compromised for anyother. This is the kind of funda-mental information that must bediscussed openly.
Nobel Biocare at the forefrontCurrent state-of-the-art diagnosticand implant treatment tools includenot only D radiographic examina-tion but also D simulation soft-ware, i.e. NobelClinician, throughwhich the patient’s CT data can beused for computer-based implanttreatment planning.
NobelClinician provides a solu-tion to support implant treatmentwith a surgical template that makesguided surgery possible. It is alsouseful as a communication tool be-tween the doctor and the dentaltechnician in prosthetic-driven im-plant treatment, and furthermore asa patient consultation tool.Laboratory work must keep up
with the rapid progress of implanttreatment, of course. Particularly inedentulous cases where large-scalerestorations are under consider-ation, we dental technicians con-stantly have concerns over the fitand strength of the framework.In the production of large restora-
tions for edentulous cases in thepast, we often felt the limitations ofanalog/manual techniques, which
were the conventional methods, atthat time.NobelProcera dental CAD/CAM
was a savior. It resolved our con-cerns, and it is no exaggeration tosay that this systemmade for a para-digm shift in dental technology forimplant treatment.In the production of NobelProc-
era Implant Bridges, NobelProceratechnology continues to be an excel-lent choice as it ensures: ) consis-tent quality, based on computer-ized management; ) precision fit,backed by CAD/CAM technology;) high strength, due to one-piecestructure; and ) superior biocom-patibility, based on erudite materialscience. Without question, Nobel-Procera Implant Bridges represent agreat leap forward from the frame-work produced by conventional an-alog/manual methods.
Early adoptersWe quickly adopted this systemwhen it was first released and havesince used it in our dental laborato-ry. As long as proper procedures arefollowed, we have not encounteredany problems with fit or strength,and work-time management has be-come much easier than ever before.As Nobel Biocare is a well-estab-
lished global manufacturer of im-plants—and an experienced provid-er of CAD/CAM-based prostheticsystems—the company routinelymeets the quality and safety expec-tations of users. Thus, the companyhas become our preferred partner.Needless to say, we will continue touse the NobelProcera system. <
Mr. Atsushi Sogo, Presidentof DenTech International, Japan
Figure 3. The NobelProceraImplant Bridge Zirconia is availablein four shades for optimal es-thetics.
Figure 1. The NobelProceraImplant Bridge Titanium is a pre-cision-milled CAD/CAM product.
Figure 4. In this image, one cansee how the NobelProcera ImplantBridge Zirconia framework hasbeen veneered with porcelain.
Figure 2. As seen here, theviewer can better appreciate thatthe titanium has been veneeredwith hybrid type composite resin.
In Brief
Very satisfied patientsIn the June issue of the Journal of Oral Implantology,Dr. Charles A. Babbush published a paper entitled, “Post-treatment Quantification of Patient Experiences withFull-Arch Implant Treatment.“
Improving quality of life is an essential aspect of successful full-arch rehabil-
itation. In this study, using a modification of the OHIP-14 questionnaire, 250
patients with Nobel Biocare implants responded. 95% of the respondents
described themselves as being either satisfied or extremely satisfied with
their new teeth, and 98% said they would definitely recommend similar
treatment or consider recommending it to a friend or colleague.
nobelbiocare.com/patientsurvey-babbush
Download the app today!A new version of the Nobel Biocare News App is now avail-able in the Apple App Store and the Google Play online store.
Free of charge, it offers many improvements, including late-
breaking news from Nobel Biocare. Whichever mobile device
you choose—using iOS or Android—the new app makes it
easier than ever to read Nobel Biocare News on the go.
nobelbiocare.com/newsletter
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 11NB_NEWS_2-2012_master_for_publication_Switzerland.indd 11 08.10.12 14:1008.10.12 14:10
Nobel Biocare NEWS Issue 2/201212
The following is the con-clusion of a research updatethat began in the most recentissue of Nobel Biocare News.
By Professor John B. Brunski
We’ve been tes t ingthe mechano-biologicalquestion inherent in the
headline above in a series of experi-ments in a mouse model (e.g., Leucht,Kim, Wazen et al. ; Leucht, Kim,Currey et al. ; Brunski et al. ).Our methodology allows us to con-trol implant micromotion and the re-sulting interfacial strain fields in vivo,while also permitting molecular andhistological studies of the bone-im-plant interface.As one aspect of our research, our
mouse model has a custom-designedmicromotion device (Fig. ) that canbe implanted on the mouse’s tibia topermit us to deliver known axial mi-cromotion to a special implant.We can design the implant to have
various tip geometries—such as a pinwith circumferential ridges, or ascrew shape (Fig. ) and use both inorder to produce certain interfacialstrain states in vivo when each im-plant is subjected to certain values ofaxial micromotion in a transcorticalhole in the tibia.For example, as seen in the finite
element modeling of a pin-shapedimplant subjected to µm of mi-
cromotion (Fig. ), large (e.g., greaterthan %) principal tensile and com-pressive strains develop near the baseand ridges of the implant, while atthe same time smaller strains (e.g.,less than %) develop along thesmooth sides of the implant.
This demonstrates that for the sameimplant micromotion, the interfacialstrains can differ quite a lot fromplace to place, depending on the ge-ometry of the implant.As it turns out, micromotion alone
may not be the key to interfacial re-actions; one also has to consider thestrain produced by the micromotion,which will depend on the implant’sgeometry and the fit of the implantin the surgical site, to name just twokey factors.In examining the biological results
of our experiments on micromotion,consider an experiment done in onesort of initial interface that we call a“bone-implant-gap interface” (BIGI);this is an interface formed by im-planting the . mm diameter pin-shaped implant (made of % L-lac-tide/% D,L-lactide, grade LR,Midwest Plastics, MN; machined byMedical Micro Machining, Inc., WA)into a . mm hole drilled in onecortex of the mouse tibia.The rationale for testing an im-
plant in this type of initial interface isthat an implant subjected to micro-motion in this “gap” interface allowsus to study the influence of certainstrain fields on the disposition of theearly fibrin clot and granulation tis-sue of the interface (along the linesdepicted in our first article in NobelBiocare News)—which should go onto form bone if the mechanical con-ditions permit this healing to occur!
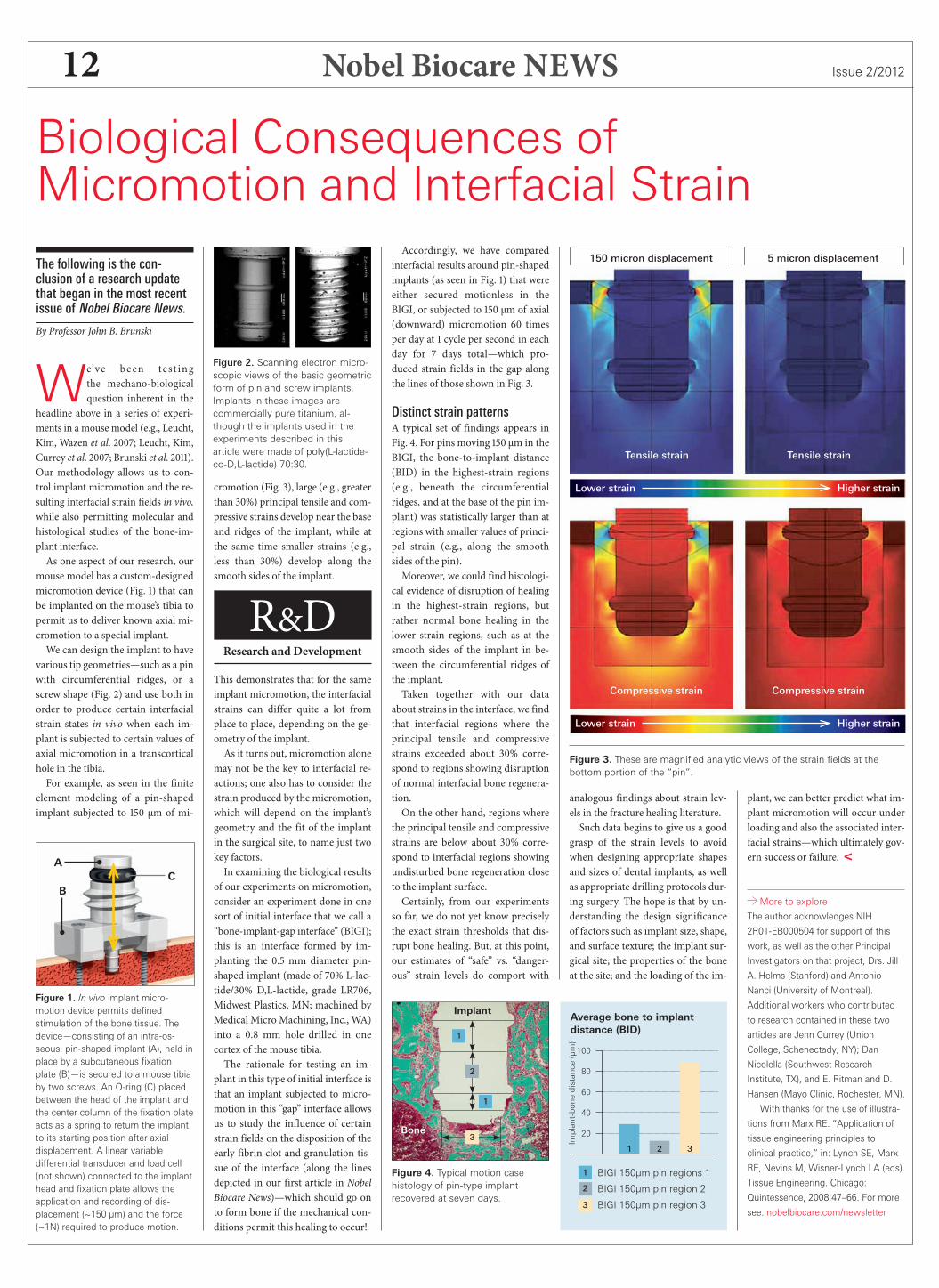
Accordingly, we have comparedinterfacial results around pin-shapedimplants (as seen in Fig. ) that wereeither secured motionless in theBIGI, or subjected to µm of axial(downward) micromotion timesper day at cycle per second in eachday for days total—which pro-duced strain fields in the gap alongthe lines of those shown in Fig. .
Distinct strain patternsA typical set of findings appears inFig. . For pins moving μm in theBIGI, the bone-to-implant distance(BID) in the highest-strain regions(e.g., beneath the circumferentialridges, and at the base of the pin im-plant) was statistically larger than atregions with smaller values of princi-pal strain (e.g., along the smoothsides of the pin).Moreover, we could find histologi-
cal evidence of disruption of healingin the highest-strain regions, butrather normal bone healing in thelower strain regions, such as at thesmooth sides of the implant in be-tween the circumferential ridges ofthe implant.Taken together with our data
about strains in the interface, we findthat interfacial regions where theprincipal tensile and compressivestrains exceeded about % corre-spond to regions showing disruptionof normal interfacial bone regenera-tion.On the other hand, regions where
the principal tensile and compressivestrains are below about % corre-spond to interfacial regions showingundisturbed bone regeneration closeto the implant surface.Certainly, from our experiments
so far, we do not yet know preciselythe exact strain thresholds that dis-rupt bone healing. But, at this point,our estimates of “safe” vs. “danger-ous” strain levels do comport with
analogous findings about strain lev-els in the fracture healing literature.Such data begins to give us a good
grasp of the strain levels to avoidwhen designing appropriate shapesand sizes of dental implants, as wellas appropriate drilling protocols dur-ing surgery. The hope is that by un-derstanding the design significanceof factors such as implant size, shape,and surface texture; the implant sur-gical site; the properties of the boneat the site; and the loading of the im-
plant, we can better predict what im-plant micromotion will occur underloading and also the associated inter-facial strains—which ultimately gov-ern success or failure. <
More to explore
The author acknowledges NIH
2R01-EB000504 for support of this
work, as well as the other Principal
Investigators on that project, Drs. Jill
A. Helms (Stanford) and Antonio
Nanci (University of Montreal).
Additional workers who contributed
to research contained in these two
articles are Jenn Currey (Union
College, Schenectady, NY); Dan
Nicolella (Southwest Research
Institute, TX), and E. Ritman and D.
Hansen (Mayo Clinic, Rochester, MN).
With thanks for the use of illustra-
tions from Marx RE. “Application of
tissue engineering principles to
clinical practice,” in: Lynch SE, Marx
RE, Nevins M, Wisner-Lynch LA (eds).
Tissue Engineering. Chicago:
Quintessence, 2008:47–66. For more
see: nobelbiocare.com/newsletter
Biological Consequences ofMicromotion and Interfacial Strain
R&DResearch and Development
Figure 2. Scanning electron micro-scopic views of the basic geometricform of pin and screw implants.Implants in these images arecommercially pure titanium, al-though the implants used in theexperiments described in thisarticle were made of poly(L-lactide-co-D,L-lactide) 70:30.
Figure 1. In vivo implant micro-motion device permits definedstimulation of the bone tissue. Thedevice—consisting of an intra-os-seous, pin-shaped implant (A), held inplace by a subcutaneous fixationplate (B)—is secured to a mouse tibiaby two screws. An O-ring (C) placedbetween the head of the implant andthe center column of the fixation plateacts as a spring to return the implantto its starting position after axialdisplacement. A linear variabledifferential transducer and load cell(not shown) connected to the implanthead and fixation plate allows theapplication and recording of dis-placement (~150 µm) and the force(~1N) required to produce motion.
Figure 3. These are magnified analytic views of the strain fields at thebottom portion of the “pin”.
100
80
60
40
20
Implant-bonedistance(µm)
Average bone to implantdistance (BID)
321
BIGI 150µm pin regions 1
BIGI 150µm pin region 2
BIGI 150µm pin region 3
1
2
3
Figure 4. Typical motion casehistology of pin-type implantrecovered at seven days.
1
2
1
3
Implant
Bone
CA
B
Tensile strain Tensile strain
Compressive strain Compressive strain
150 micron displacement 5 micron displacement
Lower strain Higher strain
Lower strain Higher strain
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 12NB_NEWS_2-2012_master_for_publication_Switzerland.indd 12 08.10.12 14:1008.10.12 14:10

Nobel Biocare NEWSIssue 2/2012 13
Patients with chronicperiodontal disease (a.k.a.“terminal dentition patients”)are often advised to removetheir remaining teeth in orderto improve their oral andoverall health, but time aftertime, they do not follow thisrecommendation. One mightask, “How can this infor-mation be so plain to see, yetat the same time so hard toconvey?”
By Dr. Edmond Bedrossian
Ithink the answer to the questionposed above is obvious. The ideaof losing all one’s teeth is devastat-
ing to most people. Even more objec-tionable is the idea of wearing a den-ture.If this is true, we as dental profes-
sionals have an obligation to formu-late and execute treatment plans thataddress the social, psychological, cos-metic—as well as the biologic—needsof this patient group.Implant dentistry is the best option
for existing edentulous patients or forpatients with terminal dentition forone major reason: Implant-supportedprostheses internally load the edentu-lous alveolus and therefore maintainthe residual volume of the alveolarbone.
But what about the maxilla?Treatment planning for a fixed, im-plant-supported prostheses is restrict-ed by unique anatomical limitationsin the maxilla.The pneumatization of the maxil-
lary sinuses bilaterally does not readi-
ly allow for the placement of implantsin the posterior maxilla for the fabri-cation of implant-supported prosthe-ses. Therefore, implants are usuallyplaced in the os incisivum (Zone I),between the cuspid teeth. The place-ment of the implants in the os incisi-vum does not allow for adequate AP(anterior-posterior) distribution ofthe implants, and results in the fabri-cation of a tissue-supported implantoverdenture that does not internallyload the residual bone.To physiologically load the residual
alveolar bone with biomechanicallystable implant-supported prostheses,grafting techniques such as the sinuslift procedure are often proposed. Al-though sinus grafting is a stable andpredictable procedure, the multiplesurgical interventions needed, as wellas the inability to immediately loadthe implants, limit the number of pa-tients who choose to proceed with thistreatment option.
Zygomatic advantagesTo address this objection, the use of zy-gomatic implants in the posterior max-illa in conjunction with two to fourpremaxillary implants has solved thevarious issues associated with estab-lishing a predictable posterior supportfor implant-supported prostheses.The use of zygomatic implants has
many advantages over grafting theposterior maxilla; this surgical proto-col allows for a graftless approach, asingle surgical procedure and imme-diate loading. These advantages resultin an increased rate of patient accep-tance of the proposed treatment.The zygomatic implant protocol
addresses the needs of patients whoare missing residual alveolar bone in
their premolar and molar regions;lack of bone in Zone II (the premolarregion) and Zone III (the molar re-gion), respectively. These groups ofpatients are sometimes referred to ashaving moderate to advanced re-sorbed maxillae.The use of the zygomatic implant
also addresses the “extremely” re-sorbed maxilla, patients lacking bonein Zones I, II and III; otherwiseknown as the “untreatable” maxilla.By placement of four zygomatic im-plants, even this group of patients canbe treated with fixed implant-sup-ported prostheses.The zygomatic implant is some-
times called the “Rescue Implant.”Many patients have had multiplegrafting procedures to establish ade-quate boney volume for the placementof conventional implants. For various
reasons, however, such as resorptionof the bone graft or infection of thegrafted bone, the residual boney vol-ume remains inadequate for the place-ment of implants. The BrånemarkSystem Zygoma implant addressesthe needs of this group, too. The zygo-matic concept encompasses proce-dures that complete the implant sur-geon’s repertoire of surgical skills intreatment of the edentulous maxilla.Consider the following possibilities:
Two scenariosIn scenario one, the surgeon is plac-ing tilted implants for the All-on-procedure. During installation ofone or both of the posterior tiltedimplants, – Ncm of insertiontorque is not reached. What shouldthe surgeon do if immediate loadingwas the treatment plan proposed tothe patient?Scenario two: the All-on- proce-
dure has been performed; the patienthas been immediately loaded. Afterthree months, the patient returns witha loose immediately loaded provision-al prosthesis. After removal of theprosthesis, one of the tilted implants isdiagnosed as mobile and is removed.After its removal, the surgeon notesthe lack of buccal bone in the areawhere the failed tilted implant was re-moved. What options does the sur-geon have?In scenario one, the surgeon may
decide to leave the implant, which hasan insertion torque of less than –Ncm, and not immediately load thepatient; but if this is not acceptable tothe patient, the surgeon may removethe tilted implant and place a Bråne-mark System Zygoma implant in its
place and continue with immediateloading.In scenario two, the surgeon may
debride the failed implant site andimmediately place a zygoma implant,rescuing the case and reattaching theprovisional, immediately loadedprosthesis.In conclusion, the Brånemark Sys-
tem Zygoma surgical protocol allowsfor the treatment as well as rescue ofevery possible maxillary defect. It is apredictable protocol for either delayedor immediate loading for the patientwith a fully edentulous maxillary arch.Without question, the contemporarysurgeon should incorporate this surgi-cal protocol into his or her practice.<
More to explore:
The author’s Implant Treatment
Planning for the Edentulous Patient –
A Graftless Approach to Immediate
Loading, with a foreword by Profes-
sor Per-Ingvar Brånemark.
The Nobel Biocare website is also a
goldmine of information:
nobelbiocare.com/edentulous
The Zygomatic AngleWhen grafting is not an option, consider the advantages of implant anchorage in the zygoma.
Precision and stability are key words in all full-arch restoration work, but especially when working with zygomaticimplants. One should incorporate appropriate rigidity and precision in the restoration in order to decrease bendingmoments and to accommodate functional, esthetic, phonetic and hygiene requirements. Stability in the bridgeframework and precision in the connecting screw joints bode well for achieving long-term success.
Precision
Stability
For Smarter, Easier, More Personal Choices
More to explore:
Visit the Nobel Biocare Store today!
store.nobelbiocare.com
Nobel Biocare has launchedan online store based onmore than eight years ofonline sales experience.The US has been first in line;selected markets will haveaccess to the store this fall.
At the new Nobel Biocare Store,customers can choose from the
full range of high-quality NobelBiocare products hours a day. In-
telligent filtering helps you find theproduct you’re looking for fast, andsearch results show related productsto make comparisons easy. Shoppingcan take place on virtually any de-vice, and with the “quick buy” func-tion, you can order regular supplieswith ease.What’s more, you can buy items di-
rectly from your previous purchasehistory or even build up your ownpractice-specific product catalog—complete with product information.At the Nobel Biocare Store, you
can shop with confidence. All Nobel
Biocare products are covered by gen-erous warranties and the company’sconvenient return policy is literally,“just what the doctor ordered!” <
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 13NB_NEWS_2-2012_master_for_publication_Switzerland.indd 13 08.10.12 14:1108.10.12 14:11
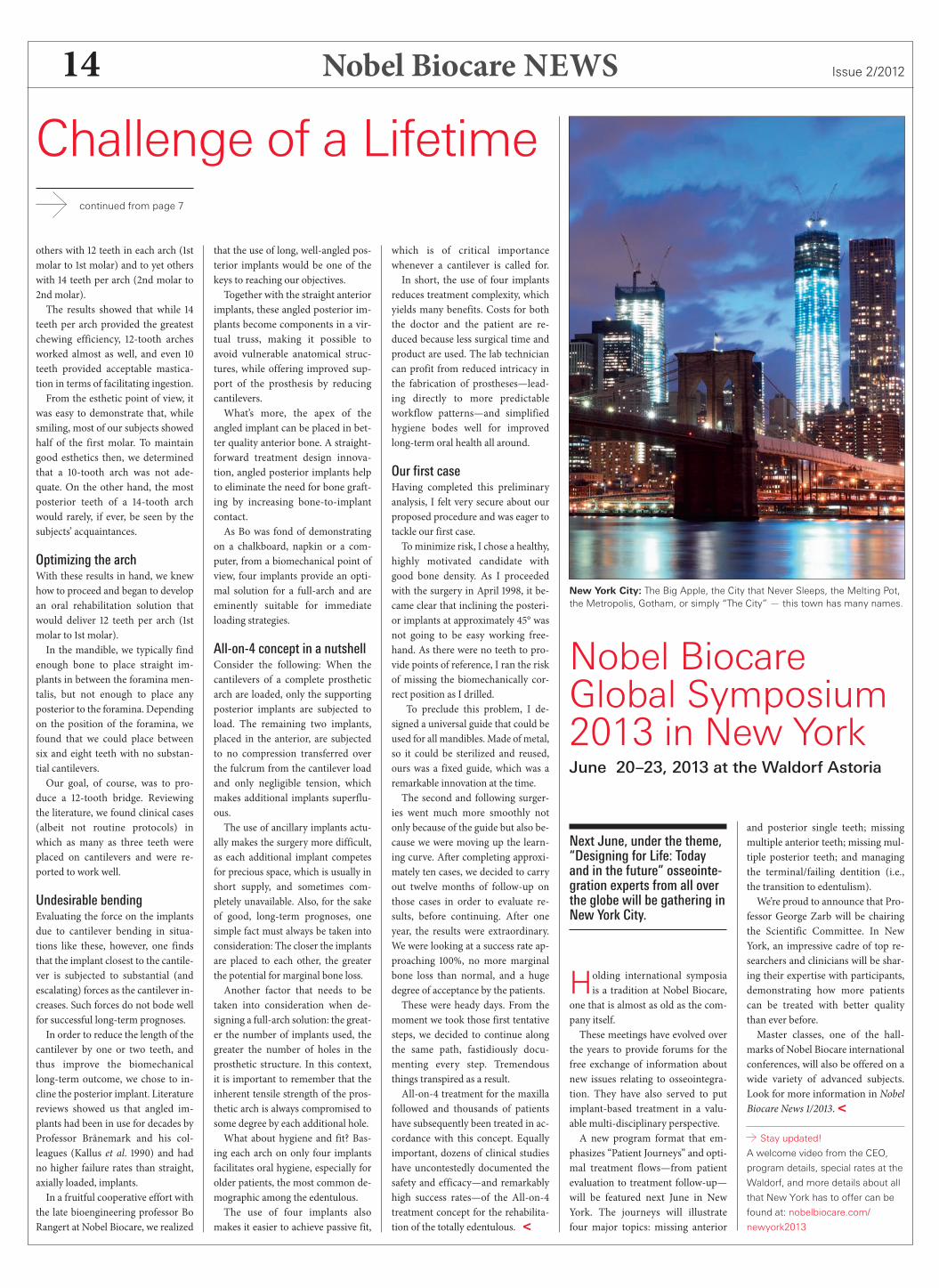
Nobel Biocare NEWS Issue 2/201214
others with teeth in each arch (stmolar to st molar) and to yet otherswith teeth per arch (nd molar tond molar).The results showed that while
teeth per arch provided the greatestchewing efficiency, -tooth archesworked almost as well, and even teeth provided acceptable mastica-tion in terms of facilitating ingestion.From the esthetic point of view, it
was easy to demonstrate that, whilesmiling, most of our subjects showedhalf of the first molar. To maintaingood esthetics then, we determinedthat a -tooth arch was not ade-quate. On the other hand, the mostposterior teeth of a -tooth archwould rarely, if ever, be seen by thesubjects’ acquaintances.
Optimizing the archWith these results in hand, we knewhow to proceed and began to developan oral rehabilitation solution thatwould deliver teeth per arch (stmolar to st molar).In the mandible, we typically find
enough bone to place straight im-plants in between the foramina men-talis, but not enough to place anyposterior to the foramina. Dependingon the position of the foramina, wefound that we could place betweensix and eight teeth with no substan-tial cantilevers.Our goal, of course, was to pro-
duce a -tooth bridge. Reviewingthe literature, we found clinical cases(albeit not routine protocols) inwhich as many as three teeth wereplaced on cantilevers and were re-ported to work well.
Undesirable bendingEvaluating the force on the implantsdue to cantilever bending in situa-tions like these, however, one findsthat the implant closest to the cantile-ver is subjected to substantial (andescalating) forces as the cantilever in-creases. Such forces do not bode wellfor successful long-term prognoses.In order to reduce the length of the
cantilever by one or two teeth, andthus improve the biomechanicallong-term outcome, we chose to in-cline the posterior implant. Literaturereviews showed us that angled im-plants had been in use for decades byProfessor Brånemark and his col-leagues (Kallus et al. ) and hadno higher failure rates than straight,axially loaded, implants.In a fruitful cooperative effort with
the late bioengineering professor BoRangert at Nobel Biocare, we realized
that the use of long, well-angled pos-terior implants would be one of thekeys to reaching our objectives.Together with the straight anterior
implants, these angled posterior im-plants become components in a vir-tual truss, making it possible toavoid vulnerable anatomical struc-tures, while offering improved sup-port of the prosthesis by reducingcantilevers.What’s more, the apex of the
angled implant can be placed in bet-ter quality anterior bone. A straight-forward treatment design innova-tion, angled posterior implants helpto eliminate the need for bone graft-ing by increasing bone-to-implantcontact.As Bo was fond of demonstrating
on a chalkboard, napkin or a com-puter, from a biomechanical point ofview, four implants provide an opti-mal solution for a full-arch and areeminently suitable for immediateloading strategies.
All-on-4 concept in a nutshellConsider the following: When thecantilevers of a complete prostheticarch are loaded, only the supportingposterior implants are subjected toload. The remaining two implants,placed in the anterior, are subjectedto no compression transferred overthe fulcrum from the cantilever loadand only negligible tension, whichmakes additional implants superflu-ous.The use of ancillary implants actu-
ally makes the surgery more difficult,as each additional implant competesfor precious space, which is usually inshort supply, and sometimes com-pletely unavailable. Also, for the sakeof good, long-term prognoses, onesimple fact must always be taken intoconsideration: The closer the implantsare placed to each other, the greaterthe potential for marginal bone loss.Another factor that needs to be
taken into consideration when de-signing a full-arch solution: the great-er the number of implants used, thegreater the number of holes in theprosthetic structure. In this context,it is important to remember that theinherent tensile strength of the pros-thetic arch is always compromised tosome degree by each additional hole.What about hygiene and fit? Bas-
ing each arch on only four implantsfacilitates oral hygiene, especially forolder patients, the most common de-mographic among the edentulous.The use of four implants also
makes it easier to achieve passive fit,
which is of critical importancewhenever a cantilever is called for.In short, the use of four implants
reduces treatment complexity, whichyields many benefits. Costs for boththe doctor and the patient are re-duced because less surgical time andproduct are used. The lab techniciancan profit from reduced intricacy inthe fabrication of prostheses—lead-ing directly to more predictableworkflow patterns—and simplifiedhygiene bodes well for improvedlong-term oral health all around.
Our first caseHaving completed this preliminaryanalysis, I felt very secure about ourproposed procedure and was eager totackle our first case.To minimize risk, I chose a healthy,
highly motivated candidate withgood bone density. As I proceededwith the surgery in April , it be-came clear that inclining the posteri-or implants at approximately ° wasnot going to be easy working free-hand. As there were no teeth to pro-vide points of reference, I ran the riskof missing the biomechanically cor-rect position as I drilled.
To preclude this problem, I de-signed a universal guide that could beused for all mandibles. Made of metal,so it could be sterilized and reused,ours was a fixed guide, which was aremarkable innovation at the time.The second and following surger-
ies went much more smoothly notonly because of the guide but also be-cause we were moving up the learn-ing curve. After completing approxi-mately ten cases, we decided to carryout twelve months of follow-up onthose cases in order to evaluate re-sults, before continuing. After oneyear, the results were extraordinary.We were looking at a success rate ap-proaching %, no more marginalbone loss than normal, and a hugedegree of acceptance by the patients.These were heady days. From the
moment we took those first tentativesteps, we decided to continue alongthe same path, fastidiously docu-menting every step. Tremendousthings transpired as a result.All-on- treatment for the maxilla
followed and thousands of patientshave subsequently been treated in ac-cordance with this concept. Equallyimportant, dozens of clinical studieshave uncontestedly documented thesafety and efficacy—and remarkablyhigh success rates—of the All-on-treatment concept for the rehabilita-tion of the totally edentulous. <
continued from page 7
Challenge of a Lifetime
Nobel BiocareGlobal Symposium2013 in New YorkJune 20–23, 2013 at the Waldorf Astoria
Next June, under the theme,“Designing for Life: Todayand in the future” osseointe-gration experts from all overthe globe will be gathering inNew York City.
Holding international symposiais a tradition at Nobel Biocare,
one that is almost as old as the com-pany itself.These meetings have evolved over
the years to provide forums for thefree exchange of information aboutnew issues relating to osseointegra-tion. They have also served to putimplant-based treatment in a valu-able multi-disciplinary perspective.A new program format that em-
phasizes “Patient Journeys” and opti-mal treatment flows—from patientevaluation to treatment follow-up—will be featured next June in NewYork. The journeys will illustratefour major topics: missing anterior
and posterior single teeth; missingmultiple anterior teeth; missing mul-tiple posterior teeth; and managingthe terminal/failing dentition (i.e.,the transition to edentulism).We’re proud to announce that Pro-
fessor George Zarb will be chairingthe Scientific Committee. In NewYork, an impressive cadre of top re-searchers and clinicians will be shar-ing their expertise with participants,demonstrating how more patientscan be treated with better qualitythan ever before.Master classes, one of the hall-
marks of Nobel Biocare internationalconferences, will also be offered on awide variety of advanced subjects.Look for more information in NobelBiocare News /.<
Stay updated!
A welcome video from the CEO,
program details, special rates at the
Waldorf, and more details about all
that New York has to offer can be
found at: nobelbiocare.com/
newyork2013
New York City: The Big Apple, the City that Never Sleeps, the Melting Pot,the Metropolis, Gotham, or simply “The City” — this town has many names.
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 14NB_NEWS_2-2012_master_for_publication_Switzerland.indd 14 08.10.12 14:1108.10.12 14:11

Nobel Biocare NEWSIssue 2/2012 15
Intra-oral RadiographySeven rules for the successful use of IOR with implant-based restorations
This article focuses on therestoration and subsequentmonitoring of dental implantswith the intra-oral radiog-raphy (IOR) equipment mostcommonly used in dentaloffices.
By Dr. Chandur Wadhwani
Radiography plays an integralrole in the planning, surgicaland restorative phases of
dental implant therapy. It has alsobeen used to follow the “health” andmeasure long-term success of thesemedical devices.A well-made radiographic image
(film or sensor) can give lots of in-formation about what is occurring,but as with any diagnostic tool, it isnot without limitations. Theseshould be clearly understood by theclinician so that information re-ceived can be properly acted upon.Here are my suggestions:
Rule number 1Osseointegration can only be con-firmed with light microscopy sections(see image below) and cannot be con-firmed by radiographs alone.Radiography simply gives an indi-
cation of bone-to-implant contact,which for most offices is restricted to-dimensional imaging even thoughthe site is -dimensional.As a guide, it should be under-
stood that limitations exist when re-viewing bone-to-implant contact ona radiograph. Studies report that uni-form gaps of up to microns be-tween the implant and surroundingbone sometimes go undetected, evenwhen experienced clinicians are re-viewing the images.
Rule number 2Radiographic site information prior torestoration is extremely useful.The implant and the adjacent sites
can be evaluated for any pathosis, theimplant position, the angulation and
the path of restoration insertion,among other things. Radiographscan reveal bone quality and quantityand various bone patters can behighlighted by IOR images.This is important as implants are
commonly placed in alveolar bone,which may have large marrow spacesthat could impact the way we restorethe implant. This is well understood
in other areas of dentistry (e.g., end-odontics). Marrow spaces provide aneasy escape route for cement, whichcan sometimes be observed aroundimplants when cementing a crown.
Rule number 3X-ray angulation is everything.When confirming how compo-
nents fit, IOR can be indispensable,especially for sites that cannot be di-rectly visualized or accessed with ex-plorers. With the implant more than degrees off the incident X-raybeam, the mismatch of componentsbecomes almost impossible to detect.When the angulation error is closer to degrees or less, the components canbe confirmed to fit to within mi-crons or less. As a general rule, whenreviewing radiographic images, theclearer the screw thread pattern seen,the closer the incident X-ray beam isto perpendicular to the implant body.
Rule number 4Serial radiographs intended to moni-tor marginal bone levels must be stan-dardized.Standardized positioning requires
establishing a consistent method ofholding the radiographic sensor (orfilm) and the incident beam at de-grees to the implant’s long axis, eachand every time the image is pro-duced. Remember, when a -dimen-sional image is made of a -dimen-
sional site, angulation grossly affectswhat is identified in the image due tobeam projection.Interestingly, most studies on bone
loss around implants fail to achievestandard, reproducible images, mak-ing comparisons between serial im-ages just about meaningless.Note that sites adjacent to the im-
plant offer clues to angulation errors.Radiopaque crown margins thatchange shape on nearby teeth are fre-quently a giveaway of angle shift.
Rule number 5Understand your implant system andhow the mechanical union of the partsyou are working with appear on a ra-diograph.Because NobelReplace and Bråne-
mark System components have flatmatching surfaces, errors in attach-ments can be easily detected whenthe radiographs have been taken degrees to the incident X-ray beam.Non-flat, internal tapered systems
may appear very different to theirflat-top counterparts. For instance,the Nobel Biocare conical connec-tion fit is very distinct. By assessingthe screw dimensions carefully, theclinician will readily understand ifthe components match well and areseated correctly.
Rule number 6When making a cement-retained im-plant restoration with inaccessiblemargins, use IOR to locate possible re-sidual excess cement that may causefuture problems.Use a cement that can be clearly
identified on a radiographic film.Many cements show up poorly, thusremaining undetected (see images tothe right, above), which could im-pact the future health of the tissuessupporting the implant. As a generalrule, choose a cement with mini-mum radiopacity equivalent to mmof aluminum (which is the sameminimum required by the ADA forendodontic sealer cements).
Rule number 7Use radiographic imaging as one ofseveral diagnostic tools.A variety of clinical criteria need to
The implant abutment is not seated correctly in the images to the left.Note the orientation and gap size, compared to the images to the right,where the seating is correct. A radiograph taken at a right angle to theimplant is invaluable.
The images to the left show failure of the abutment to seat fully:The gap is larger than 1 mm. Compare this to the images to the right,which show correct seating. Again, the value of a correctly angled radio-graph is essential for appropriate interpretation of these effects.
These four radiographs showhow angulation affects the abilityto detect component misfit. Notehow the screw thread changeswith angle. If it is clearly visible, theradiograph will more likely show anerror.
30°20°
10°0°
be taken into account before treat-ment decisions are made. For exam-ple, probing-depths correlate verywell with radiographic bone changes,especially within the first few yearsfollowing implant placement. Usingmore than one test to determinewhat, if any, therapy is required is al-ways a good idea. Remember no testis perfect or absolute!And do remember: All radio-
graphic procedures require that themost appropriate and best practicesbe used to minimize patient expo-sure to radiation.<
More to explore!
”Intra-oral radiography and dental
implant restoration.” August 2012,
Dentistry Today : Vol. 31 No.8. For a
full list of other references, visit:
nobelbiocare.com/newsletter
Osseointegration can only beconfirmed with light microscopysections like this. Radiographysimply gives an indication ofbone-to-implant contact.
These two radiographs show the same site at different times. It appearsthat there is a difference between the bone levels on the mesial aspect ofthe implant but—because these two images were not taken from the sameangle on identical or parallel planes—they provide very little clinicallyrelevant comparative information concerning bone status.
Here are eight commonly usedcements for implant restorationsin the form of uniform disks, nextto an aluminum step wedge forcomparison. When radiographed,at 1 mm thick, only 3 of the 8 diskscan be clearly seen. Note: If allthese disks were fabricated fromendodontic sealer materials, theywould all be clearly visible.
Marrow spaces can allow endo-dontic sealer to flow into them.Alveolar bone (from the latin for“little cavities”) consists of manysuch spaces, highlighted by thisendodontic case.T&T
Tips and Techniques
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 15NB_NEWS_2-2012_master_for_publication_Switzerland.indd 15 08.10.12 14:1108.10.12 14:11

Nobel Biocare NEWS Issue 2/201216
Nobel Biocare NEWSPrinted on non-chlorine bleached
FSC-certified paper.
Design and printing: www.linkgroup.ch
Prefer e-mail delivery? Then visit:
nobelbiocare.com/enews
Europe and Russia
AustriaNobel Biocare AustriaPhone: +43 1 892 89 90
BelgiumNobel Biocare BelgiumPhone: +32 2 467 41 70
DenmarkNobel Biocare DenmarkPhone: +45 39 40 48 46
FinlandNobel Biocare FinlandPhone: +358 9 343 69 70
FranceNobel Biocare FrancePhone: +33 1 49 20 00 30
GermanyNobel Biocare GermanyPhone: +49 221 500 85 590
HungaryNobel Biocare HungaryPhone: +36 1 279 33 79
IrelandNobel Biocare IrelandPhone: toll free 1 800 677 306
ItalyNobel Biocare ItalyPhone: +39 039 683 61Cust. support: toll free 800 53 93 28
LithuaniaNobel Biocare LithuaniaPhone: +370 5 268 3448
NetherlandsNobel Biocare NetherlandsPhone: +31 30 635 4949
NorwayNobel Biocare NorwayPhone: +47 64 95 75 55
PolandNobel Biocare PolandPhone: +48 22 549 93 50Cust. support: +48 22 549 93 52
PortugalNobel Biocare PortugalPhone: +351 22 374 73 50Cust. support: toll free 800 300 100
RussiaNobel Biocare RussiaPhone: +7 495 974 77 55Cust. support: toll free 8 800 250 77 55
SpainNobel Biocare SpainPhone: +34 93 508 8800Cust. support: toll free 900 850 008
SwedenNobel Biocare SwedenPhone: +46 31 335 49 00Cust. support: +46 31 335 49 10
SwitzerlandNobel Biocare SwitzerlandPhone: +41 43 211 53 20
United KingdomNobel Biocare UKPhone: +44 208 756 3300
North America
CanadaNobel Biocare CanadaPhone: +1 905 762 3500Cust. support: +1 800 939 9394
USANobel Biocare USAPhone: +1 714 282 4800Cust. support: +1 800 322 5001
Central/South America
BrazilNobel Biocare BrazilPhone: +55 11 5102 7000Cust. support: 0800 169 996
ChileECM Ingeniera S.A.Phone: +56 2 655 5500Cust. support: +56 2 655 5502
ColombiaHospimedics S.A.Phone: +57 1 620 9410Cust. support: +57 1 620 9410
MexicoNobel Biocare MexicoPhone: +52 55 524 974 60
Asia/Pacific
AustraliaNobel Biocare AustraliaPhone: +61 2 8064 5100Cust. support: toll free 1800 804 597
ChinaNobel Biocare ChinaPhone: +86 21 5206 6655Cust. support: +86 21 5206 0974
Hong KongNobel Biocare Hong KongPhone: +852 2845 1266Cust. support: +852 2823 8926
IndiaNobel Biocare IndiaPhone: +91 22 6751 9999Cust. support: toll free 1 800 22 9998
JapanNobel Biocare JapanPhone: +81 3 6717 6191
New ZealandNobel Biocare New ZealandPhone: +61 2 8064 5100Cust. support: toll free 0800 441 657
SingaporeNobel Biocare SingaporePhone: +65 6737 7967Cust. support: +65 6737 7967
TaiwanNobel Biocare TaiwanPhone: +886 2 2793 9933
Africa
South AfricaNobel Biocare South AfricaPhone: +27 11 802 0112
Europe and Middle East
Distributor Markets
Bahrain, Bulgaria, Croatia,Cyprus, Czech Republic, Greece,Iran, Iraq, Israel, Jordan, Kuwait,Lebanon, Malta, Oman, Romania,Saudi Arabia, Serbia, Slovakia,Slovenia, Turkey, United ArabEmirates and Qatar
Phone: +48 22 549 93 56Cust. support: +48 22 549 93 55
Headquarters
Nobel Biocare Services AGP.O. Box8058 Zürich-Flughafen, Switzerland
Offices:Balsberg-Balz Zimmermann-Strasse 78302 Kloten, SwitzerlandPhone +41 43 211 42 00Fax +41 43 211 42 42
Web contact: nobelbiocare.com/contact
GMT29501GB1210PrintedinSwitzerland©NobelBiocareServicesAG,2012.Allrightsreserved.NobelBiocare,theNobelBiocarelogotypeandallothertrademarksare,ifnothingelseisstated
orisevidentfromthecontextinacertaincase,trademarksofNobelBiocare.Productimagesarenotnecessarilytoscale.Disclaimer:Someproductsmaynotberegulatorycleared/releasedforsaleinallmarkets.PleasecontactthelocalNobelBiocaresalesofficeforcurrentproductassortmentandavailability.
An independent multidisci-plinary working group tacklesthe issue and calls for greaterscientific enquiry into bonemanagement.
By Prof. Daniel van Steenberghe
The long-term survival of en-dosseous intra-oral implantshas become a public health
issue in recent years inasmuch astens of millions of patients now haveone or more of these implants.To ensure implant survival and re-
storative longevity, the maintenanceof marginal bone around these im-plants is a significant element oftreatment and consequently shouldbe the subject of conscientious scien-tific follow-up. Progressive bone lossmay lead to insufficient anchorage,significant infections and even theloss of the implant, after all.In order to address the issue of
bone maintenance in a scientific andclinically documented manner,Nobel Biocare proposed that an in-ternational group of experts be as-sembled last year, and asked me tomoderate the group. Our brief: tothoroughly review the current stateof knowledge in this area, and to pro-pose how to proceed in the future.Thus the Working Group on “Treat-ment options for the maintenance of
marginal bone around endosseousoral implants” was born.Eight independent scientists and
clinicians joined the Working Groupfrom the very beginning and havemade valuable contributions eversince: Marco Esposito (IT), BjörnKlinge (SE), Jörg Meyle (DE), An-drea Mombelli (CH), Eric Rompen(BE), Tom Van Dyke (US), Hom-LayWang (US), and Arie-Jan van Win-kelhoff (NL).
All of these renowned authoritiesjoined the group under the provisothat they would be willing to partici-pate on an independent, pro bonobasis. For several months last year,they reviewed the literature on mar-ginal bone from the perspective oftheir own fields of study, which in-clude investigational methodology,oral and maxillofacial surgery, peri-odontology, immunology, biomateri-als, oral physiopathology, oral reha-bilitation, and microbiology.After exchanging their review pa-
pers, the members of the group metin September for two days at the Kar-olinska Institut in Stockholm, wherethe Nobel Assembly chooses the
Experts Seek Keys toMarginal Bone MaintenanceSome of the best minds in the field reach consensus, reporting their findings at Europerio 7.
prestigious Nobel Prize laureate inPhysiology or Medicine each year.Björn Klinge served as host.Nobel Biocare has very generously
covered the Working Group’s travelexpenses in good faith since its in-ception, and done so without inter-vening in any way in the discussionsor demanding a quid pro quo of anysort. The company also provided asubsequent public discussion forumfor the group at the Europerio meetings in Vienna this June.Revised review papers, consensus
statements and clinical guidelineswere published in their entirety inthe interim between these two meet-ings in a single-topic supplementto the “European Journal of Oral Im-plantology” (, supplement:–).
Key causes of marginal boneloss addressedThe group identified a series of pos-sible causes of marginal bone loss.These can be divided into twogroups: those playing a role soonafter implant insertion and those oc-curring at a (much) later stage.Among the causes leading to mar-
ginal bone resorption soon afterimplant placement, surgical trauma(either by overheating or unduecompression of the surroundingbone) is well documented. As Per-Ingvar Brånemark learned in his
Prof. Daniel van Steenberghechaired the Working Group.
early studies of osseointegration, inorder to prevent such unintendedtrauma, it is of the utmost impor-tance to treat bone as a living tissue.Other causes of resorption are less
well documented, but are represent-ed in the scientific literature never-theless, and hardly in doubt. To givethree examples: When implants areplaced in jawbone with very limitedbone volume, dehiscences often re-sult, which leads to proximal boneresorption; although reluctantly re-ported, subgingival cement rem-nants generally result in substantialbone resorption; and too-deep place-ment of an implant can also provokemarginal bone loss.At a later stage, several weeks or
months after prosthesis installation,
occlusal overload has been recog-nized as another potential cause ofmarginal bone loss. In situations likethese, occlusal adjustments or otherbiomechanical interventions arecalled for to stabilize the bone.Nowadays, a proclivity for opti-
mizing esthetics—or even cosmet-ics—sometimes leads to repeated re-moval of the abutment. These dis-ruptions of the connective tissue sealcan result in bone loss.The same applies to insufficient
biological width. The colonization ofthe implant surfaces by bacterial bio-films has been associated withchronic inflammation of the margin-al tissues and subsequent bone loss.A proper oral hygiene regimen is theappropriate response in circum-stances such as these. <
M&RMyths and Realities
There’s more to this story!
Because Nobel Biocare implants
have proven their exceptional
performance for safety and efficacy
over many years, the company
welcomes both the effort of the
working group and their findings. In
our enhanced digital edition,
Professor van Steenberghe
discusses the importance of
establishing a common baseline in
continued research and appropriate
forms of prophylactic and follow-up
treatment in clinical practice. See:
nobelbiocare.com/newsletter
NB_NEWS_2-2012_master_for_publication_Switzerland.indd 16NB_NEWS_2-2012_master_for_publication_Switzerland.indd 16 08.10.12 14:1108.10.12 14:11