
NMDC221 Session 17: Nervous System Disease Part IV · NMDC221 Session 17: Nervous System Disease...
52
© Endeavour College of Natural Health endeavour.edu.au 1 NMDC221 Session 17: Nervous System Disease Part IV
Transcript of NMDC221 Session 17: Nervous System Disease Part IV · NMDC221 Session 17: Nervous System Disease...
© Endeavour College of Natural Health endeavour.edu.au 1
NMDC221 Session 17:
Nervous System Disease
Part IV
© Endeavour College of Natural Health endeavour.edu.au 2
Recommended Reading
Mahan, LK, & Raymond, JL (14th ed) 2016, Krause’s food & the
nutrition care process, 14th ed, Elsevier, St. Louis, MO.
pp.835-8, 852-63
© Endeavour College of Natural Health endeavour.edu.au 3
Topic Summary
Nervous System Disease: Part IV
o Nutritional treatment and consideration of drug-nutrient
interactions for:
• Dementia
• Alzheimer’s disease
• Parkinson’s disease
© Endeavour College of Natural Health endeavour.edu.au 4
Dementia
© Endeavour College of Natural Health endeavour.edu.au 5
DementiaWhat is Dementia?
o Dementia is a clinical syndrome characterised by a cluster of
symptoms and signs manifested by difficulties in memory,
disturbances in language, psychological and psychiatric changes,
and impairments in activities of daily living. Alzheimer’s disease is a
specific disease entity and is the commonest cause of dementia.’
(Burns, A 2009)
o Common in the elderly (affecting > 15% of persons > 65 yr old and
as many as 40% of persons > 80 yr old).
o May occur at any age and can affect young people as the result of
injury or hypoxia. (Kumar & Clark, 2009)
o Burden of disease - About 12 million people worldwide have
dementia, and this total is likely to increase to 25 million by 2040
(Burns A, 2009).
© Endeavour College of Natural Health endeavour.edu.au 6
DementiaDementia is categorized into a few subtypes.:-
Alzheimer’s disease (AD) accounts for about half of the affected population
Vascular dementia (VaD) (20–25%)
Mixed dementia (5–10%),
Parkinson’s disease,
Dementia with Lewy bodies
Physical brain injury
Huntington’s disease
Creutzfeldt–Jacob disease
Frontotemporal dementia/Pick’s disease
Normal pressure hydrocephalus
(Chen, Lin, Chen 2009)
AD is also the most common neurodegenerative disorder and affects 20–30
million individuals worldwide. AD has been further categorized into two forms
according to its onset: sporadic cases (> 95%) with late-onset disease; and
autosomal-dominant mutation cases (< 5%) with early onset.
© Endeavour College of Natural Health endeavour.edu.au 7
Dementia
Risks Factors:
o Several factors are related to dementia, e.g. age, ethnicity, sex,
genetic factors (APOE gene for late onset AD & for early-onset
cases, APP, preselin (PS)-1, and PS-2 genes appear most relevant)
o Physical activity, smoking, drug use, education level, alcohol
consumption, body mass index, comorbidity, and environmental
factors (Chen, Lin, Chen 2009)
Signs & symptoms:
o Poor memory and disorientation
o Cognitive impairment (aphasia, apraxia, agnosia, or a loss of
executive functioning).
Unfortunately, the appearance of clinical features suggest there is a
substantial progression of the disease process.
(Kumar & Clark, 2009)
© Endeavour College of Natural Health endeavour.edu.au 8
DementiaCauses of Dementia:o Cerebral atrophy - Alzheimer's disease accounts for over 65%.
Other diseases implicated include Parkinson’s disease, Huntington’s disease
o Diffuse vascular disease
o Metabolic insufficiencies – uraemia, liver failure
o Nutritional deficiencies - vitamins B1, B3, B6 & Folate or B12
o Toxic damage – alcohol, solvents, heavy metals
o Head trauma & lesions
o Infections – HIV, neurosyphilis
o Hypothyroidism, hypoparathyroidism
(Kumar & Clark, 2009)
© Endeavour College of Natural Health endeavour.edu.au 9
DementiaNutritional Treatment Aims
Support Digestion:
o Address nutritional deficiencies
o Increase absorption (digestive enzymes or lemon water)
o Maintain adequate protein, fibre, fluid intakes (assess hydration)
o Maintain consistent blood glucose levels (eat every 3 hours)
o Assess EFA and saturated fat intake
o Correct any gut dysbiosis: prebiotics, probiotics, anti-microbials,
repairing nutrients
(Sarris & Wardle, 2010)
© Endeavour College of Natural Health endeavour.edu.au 10
Dementia
Nutritional Treatment Aims
Support anti-oxidant status
o Increased consumption of antioxidant foods
o Minimise environmental chemical & toxin contact
o Assess homocysteine levels – support B12 & folate
Support neuronal activity
o Support phospholipid maintenance – lecithin, EPA/DHA
o Support the endogenous production of Dopamine, Serotonin, GABA
and Acetylcholine
(Sarris & Wardle, 2010)
© Endeavour College of Natural Health endeavour.edu.au 11
Dementia
Nutritional Treatment Aims
Support liver detoxification & heavy metal chelation
o Assess heavy metal exposure: lead, mercury, aluminum
o Green leafy vegetables, cruciferous vegetables, soluble fiber,
dandelion and other bitter vegetables
o Glycine, cysteine and glutamine for glutathione production
Support cellular metabolism & energy
Improve circulation
(Sarris & Wardle, 2010)
© Endeavour College of Natural Health endeavour.edu.au 12
Alzheimer's Disease
© Endeavour College of Natural Health endeavour.edu.au 13
Alzheimer's Disease
o A common, progressive form of Dementia (50% - 70% of all cases)
that usually occurs during middle age or later.
o Exact cause of Alzheimer’s Disease has not yet been determined
and is difficult to diagnose. However, there is a strong genetic link (
o On autopsy a progressive, loss of cognitive function associated with
an excessive number of senile plaques in the cerebral cortex and
subcortical grey matter, which also contains beta-amyloid and
neurofibrillary tangles.
Signs & Symptoms
o Dementia, poor memory, mood, depression, language impairment,
seizures – later in disease.
(Bryant & Knights, 2011; Kumar & Clark, 2009)

© Endeavour College of Natural Health endeavour.edu.au 14
Alzheimer's DiseaseRisk factors :
o Age. Also some studies on parental age at birth, but still inconclusive.
o Sex - AD higher in women compared with men at ages >85 years (Chen,
Lin, Chen 2009)
o Positive family history
o Presence of APO-E4 gene – significant (later AD). A Swedish twin study has
reported that 60–80% of AD is
attributable to genetic effects (Gatz M,
Fratiglioni L, Johansson B, et al 2005)
o Inflammation - recent studies have shown that polymorphisms of one of the
inflammatory genes alone or in combination have comparable effects on AD
risk to those for the APOEe4 allele (Chen, Lin, Chen 2009).
© Endeavour College of Natural Health endeavour.edu.au 15
AD Risk Factors Continued:
• Smoking
• Trisomy 21 (Down’s syndrome) – can develop pathological brain changes
after 30-40 yrs age, indistinguishable from Alzheimer’s
• Low Physical Activity (PA) - physical
activity is associated positively with
cognitive function among older
people. Other studies have found that
physical activity is associated with
a reduction of 30–50% in cognitive
decline (Chen, Lin, Chen 2009)
• Trauma to the head
• Heavy metal toxicity – particularly Aluminium
• Oxidative damage to brain tissue – low antioxidants, vascular issues
• Hyper-inflammation
• Circulation disorders – due to impaired vascular integrity
(Kumar & Clark, 2009)
© Endeavour College of Natural Health endeavour.edu.au 16
AD – Risk Factors cont.
o Drugs
Benzodiazepine's increase the risk of AD.
However - the following appeared to
reduce the risk:
Statins
HRT
antihypertensive drugs
NDAID’s (Chen. Lin, Chen 2009)
o Alcohol
Alcohol drinking may be protective for AD and dementia, but not for VaD and cognitive decline
(Peters R, Peters J, Warner J, et al. 2008)

© Endeavour College of Natural Health endeavour.edu.au 17
Alzheimer's Disease
Therapeutic Actions
Homocysteine
o Recently, a few studies have linked increased levels of
plasma Homocysteine with increased risk of AD and
increased rate of progression.
(Paulionis, Kane, & Meckling, 2005)
o Malouf & Evans (2008) found that “…group of healthy
elderly people with high homocysteine levels, 800
mcg/day folic acid supplementation over three years was
associated with significant benefit in terms of global
functioning…memory storage…and information-
processing speed.”
© Endeavour College of Natural Health endeavour.edu.au 18
Alzheimer’s Disease
Therapeutic Actions
Vitamin B3
o Mild to severe Alzheimer’s patients were given 10mg of
NADH. There was a 240% increase in NADH activity
within 2 weeks. This improved mental function, alertness
& memory with increases in dopamine & norepinephrine.
o Global deterioration scale ratings conducted before and
after NADH treatment confirmed significant
improvement. (Demarin et.al 2004)
o Green et.al. (2008) found that nicotinamide was
indicated for early or mild stages of Alzheimer’s disease.
© Endeavour College of Natural Health endeavour.edu.au 19
Alzheimer’s DiseaseTherapeutic Actions
Turmeric
o The incidence of Alzheimer disease has been found to be lower
in India and areas with a high traditional consumption of
turmeric.
o The therapeutic effect of turmeric is thought to be associated
with decreased beta-amyloid plaques, delayed degradation of
neurons, metal-chelation, anti-inflammatory, antioxidant and
decreased microglia formation.
o Rodent study found turmeric significantly reduced levels of
soluble and insoluble beta amyloid as well as phosphorylated
Tau protein. Extract 82% curcuminoids dosage 5mg/mouse/day.
(Mishra, S, & Palanivelu, K, 2008, Potter, 2010, Shytle RD et al, 2012)
© Endeavour College of Natural Health endeavour.edu.au 20
Dementia & Alzheimer’s
Nutritional Treatment Aims
Support Digestion:
o Address nutritional deficiencies
o Increase absorption (digestive enzymes or lemon water)
o Maintain adequate protein, fibre, fluid intakes (assess
hydration)
o Maintain consistent blood glucose levels (eat every 3 hours)
o Assess EFA and saturated fat intake
o Correct any gut dysbiosis: prebiotics, probiotics, anti-
microbials, repairing nutrients
(Sarris & Wardle, 2010)
© Endeavour College of Natural Health endeavour.edu.au 21
Dementia & Alzheimer’s
Nutritional Treatment Aims
Support anti-oxidant status
o Increased consumption of antioxidant foods
o Minimise environmental chemical & toxin contact
o Assess homocysteine levels: elevated in brain tissue of
Alzheimer’s. Support with B12 & folate
Support neuronal activity
o Support phospholipid maintenance – lecithin, EPA/DHA
o Support the endogenous production of Dopamine,
Serotonin, GABA and Acetylcholine.
(Sarris & Wardle, 2010)

© Endeavour College of Natural Health endeavour.edu.au 22
Dementia & Alzheimer’s
Nutritional Treatment Aims
Support liver detoxification & heavy metal chelation
o Assess heavy metal exposure: lead, mercury, aluminum
o Green leafy vegetables, cruciferous vegetables, soluble
fiber, dandelion and other bitter vegetables
o Glycine, cysteine and glutamine for glutathione
production
Support cellular metabolism & energy
Improve circulation
(Sarris & Wardle, 2010)
© Endeavour College of Natural Health endeavour.edu.au 23
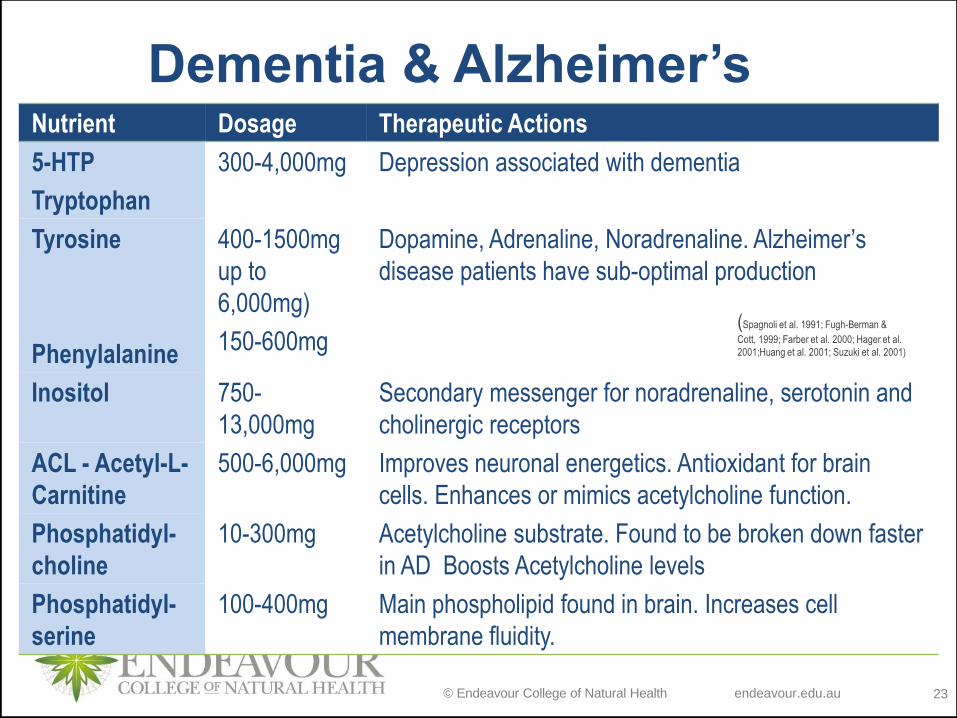
Dementia & Alzheimer’sNutrient Dosage Therapeutic Actions
5-HTP
Tryptophan
300-4,000mg Depression associated with dementia
Tyrosine
Phenylalanine
400-1500mg
up to
6,000mg)
150-600mg
Dopamine, Adrenaline, Noradrenaline. Alzheimer’s
disease patients have sub-optimal production
Inositol 750-
13,000mg
Secondary messenger for noradrenaline, serotonin and
cholinergic receptors
ACL - Acetyl-L-
Carnitine
500-6,000mg Improves neuronal energetics. Antioxidant for brain
cells. Enhances or mimics acetylcholine function.
Phosphatidyl-
choline
10-300mg Acetylcholine substrate. Found to be broken down faster
in AD Boosts Acetylcholine levels
Phosphatidyl-
serine
100-400mg Main phospholipid found in brain. Increases cell
membrane fluidity.
(Spagnoli et al. 1991; Fugh-Berman &
Cott, 1999; Farber et al. 2000; Hager et al.
2001;Huang et al. 2001; Suzuki et al. 2001)
© Endeavour College of Natural Health endeavour.edu.au 24
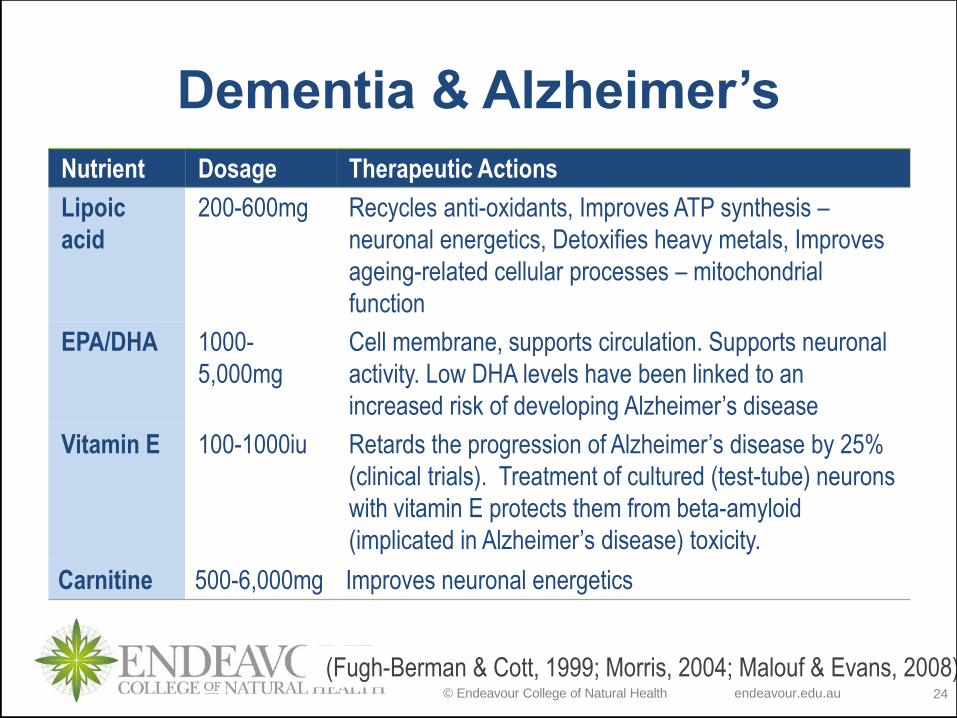
Dementia & Alzheimer’s
Nutrient Dosage Therapeutic Actions
Lipoic
acid
200-600mg Recycles anti-oxidants, Improves ATP synthesis –
neuronal energetics, Detoxifies heavy metals, Improves
ageing-related cellular processes – mitochondrial
function
EPA/DHA 1000-
5,000mg
Cell membrane, supports circulation. Supports neuronal
activity. Low DHA levels have been linked to an
increased risk of developing Alzheimer’s disease
Vitamin E 100-1000iu Retards the progression of Alzheimer’s disease by 25%
(clinical trials). Treatment of cultured (test-tube) neurons
with vitamin E protects them from beta-amyloid
(implicated in Alzheimer’s disease) toxicity.
Carnitine 500-6,000mg Improves neuronal energetics
(Fugh-Berman & Cott, 1999; Morris, 2004; Malouf & Evans, 2008)
© Endeavour College of Natural Health endeavour.edu.au 25
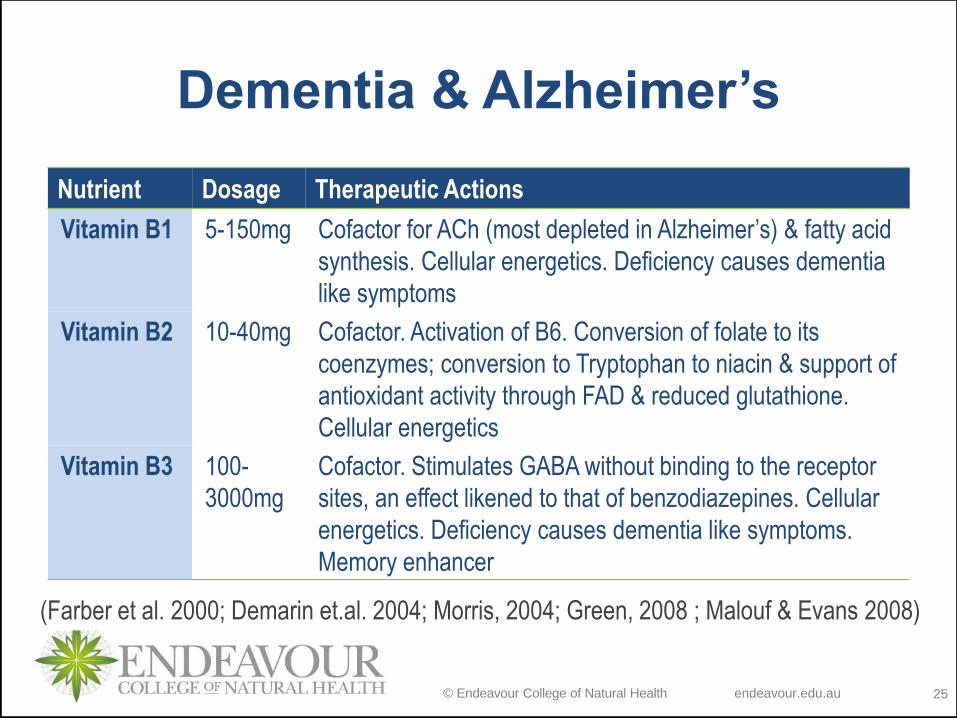
Dementia & Alzheimer’s
Nutrient Dosage Therapeutic Actions
Vitamin B1 5-150mg Cofactor for ACh (most depleted in Alzheimer’s) & fatty acid
synthesis. Cellular energetics. Deficiency causes dementia
like symptoms
Vitamin B2 10-40mg Cofactor. Activation of B6. Conversion of folate to its
coenzymes; conversion to Tryptophan to niacin & support of
antioxidant activity through FAD & reduced glutathione.
Cellular energetics
Vitamin B3 100-
3000mg
Cofactor. Stimulates GABA without binding to the receptor
sites, an effect likened to that of benzodiazepines. Cellular
energetics. Deficiency causes dementia like symptoms.
Memory enhancer
(Farber et al. 2000; Demarin et.al. 2004; Morris, 2004; Green, 2008 ; Malouf & Evans 2008)
© Endeavour College of Natural Health endeavour.edu.au 26
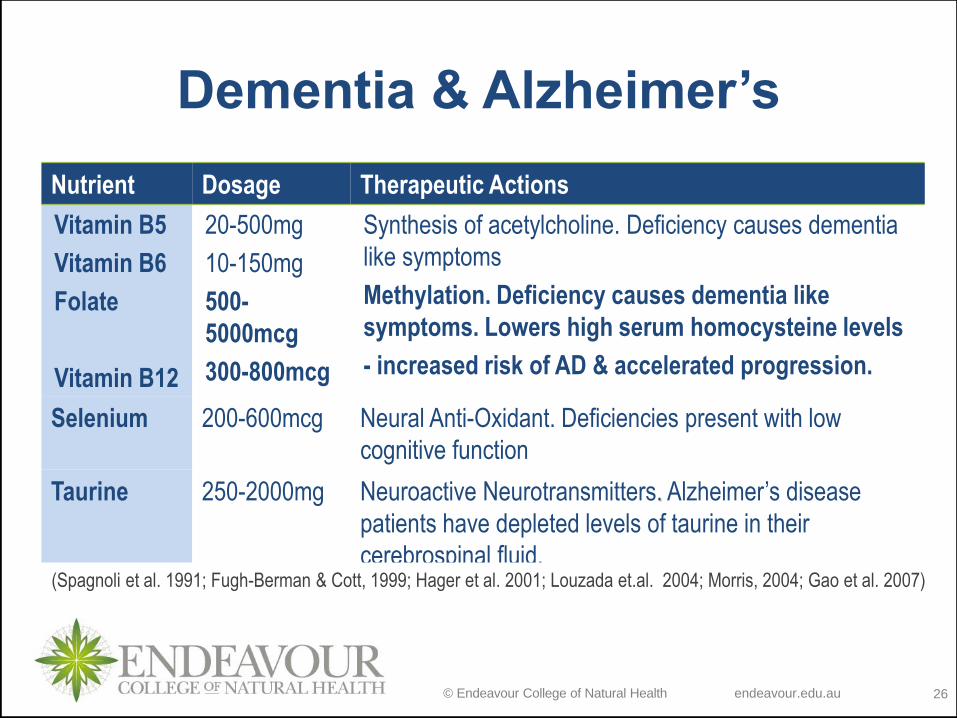
Dementia & Alzheimer’s
Nutrient Dosage Therapeutic Actions
Vitamin B5
Vitamin B6
Folate
Vitamin B12
20-500mg
10-150mg
500-
5000mcg
300-800mcg
Synthesis of acetylcholine. Deficiency causes dementia
like symptoms
Methylation. Deficiency causes dementia like
symptoms. Lowers high serum homocysteine levels
- increased risk of AD & accelerated progression.
Selenium 200-600mcg Neural Anti-Oxidant. Deficiencies present with low
cognitive function
Taurine 250-2000mg Neuroactive Neurotransmitters. Alzheimer’s disease
patients have depleted levels of taurine in their
cerebrospinal fluid. (Spagnoli et al. 1991; Fugh-Berman & Cott, 1999; Hager et al. 2001; Louzada et.al. 2004; Morris, 2004; Gao et al. 2007)
© Endeavour College of Natural Health endeavour.edu.au 27
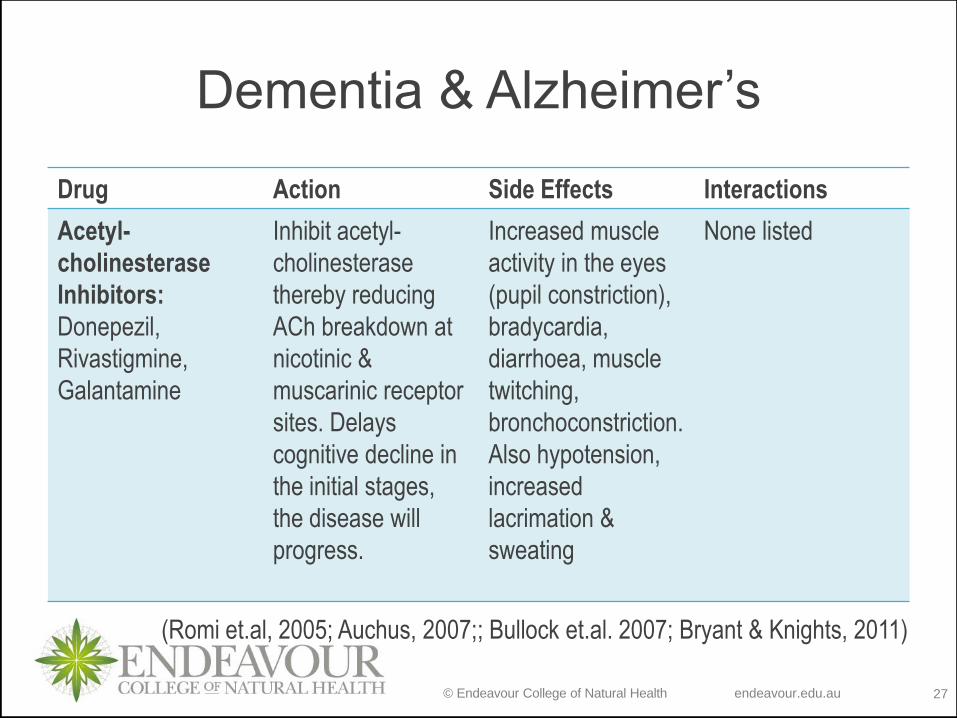
Dementia & Alzheimer’s
Drug Action Side Effects Interactions
Acetyl-
cholinesterase
Inhibitors:
Donepezil,
Rivastigmine,
Galantamine
Inhibit acetyl-
cholinesterase
thereby reducing
ACh breakdown at
nicotinic &
muscarinic receptor
sites. Delays
cognitive decline in
the initial stages,
the disease will
progress.
Increased muscle
activity in the eyes
(pupil constriction),
bradycardia,
diarrhoea, muscle
twitching,
bronchoconstriction.
Also hypotension,
increased
lacrimation &
sweating
None listed
(Romi et.al, 2005; Auchus, 2007;; Bullock et.al. 2007; Bryant & Knights, 2011)
© Endeavour College of Natural Health endeavour.edu.au 28
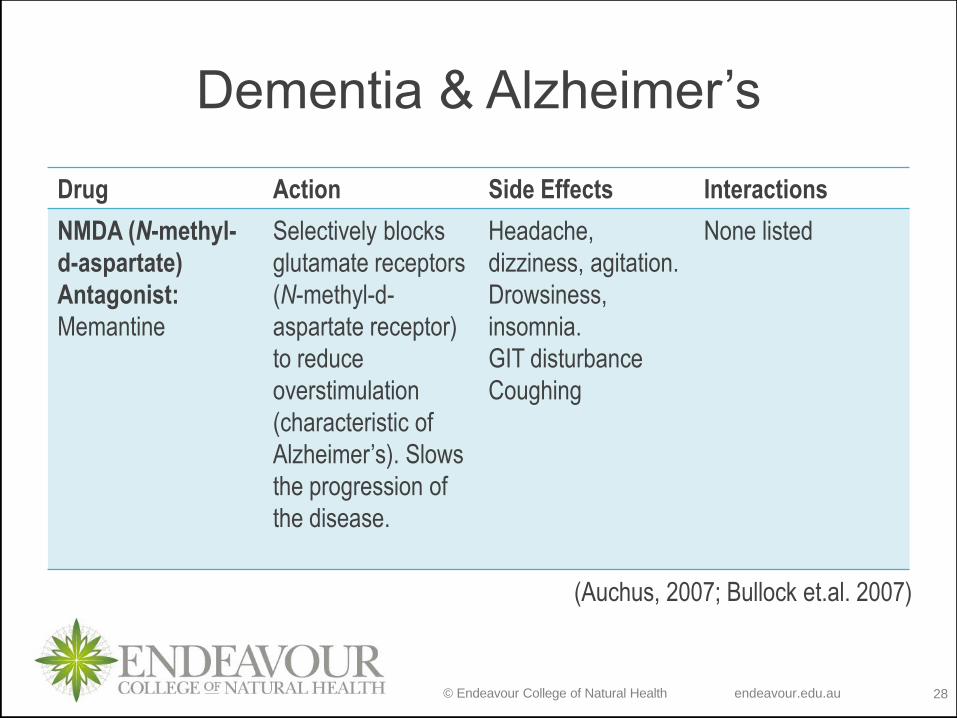
Dementia & Alzheimer’s
Drug Action Side Effects Interactions
NMDA (N-methyl-
d-aspartate)
Antagonist:
Memantine
Selectively blocks
glutamate receptors
(N-methyl-d-
aspartate receptor)
to reduce
overstimulation
(characteristic of
Alzheimer’s). Slows
the progression of
the disease.
Headache,
dizziness, agitation.
Drowsiness,
insomnia.
GIT disturbance
Coughing
None listed
(Auchus, 2007; Bullock et.al. 2007)
© Endeavour College of Natural Health endeavour.edu.au 29
Parkinson’s Disease

© Endeavour College of Natural Health endeavour.edu.au 30
Parkinson’s Disease
Chronic disease affecting the basal ganglia of the brain,
with degeneration of dopaminergic receptors in the
substantia nigra. Age is usually 40 yrs+ (can be earlier).
Risk Factors include:
o Neurotoxins
o Poor antioxidant status and high free radical production
oxidising myelin sheaths
o Impaired function of the mitochondria is closely
associated with the progression of Parkinson’s Disease
as seen with significant damage to the mitochondrial
DNA.
(Kumar & Clark, 2009)
© Endeavour College of Natural Health endeavour.edu.au 31
Parkinson’s Disease
Signs & symptoms:
o Loss of smell (early warning sign)
o Restlessness and tremors of the hands mainly at rest. Movement
reduced symptoms.
o Feeling of sluggishness
o Gait is shuffling and stumbling due to loss of centre of gravity.
o Rigidity of skeletal muscles and facial muscles (mask-like
appearance)
(Kumar & Clark, 2009)
© Endeavour College of Natural Health endeavour.edu.au 32
Parkinson’s Disease
Therapeutic Nutritional Considerations:
Folate
o Folate deficiency and hyperhomocysteinemia may contribute to
Parkinson’s disease pathogenesis, decrease dopaminergic neurons
and induced profound motor dysfunctions…” (Chen et. al, 2004, p.
373)
Vitamin B3
o “NADH administration (1.4 mg/Kg) has been useful in PD patients.
An antioxidant, that can stimulate the production of L-dopa in vivo
and dopamine in PC-12 cells, a dopaminergic cell line as well as
ATP.”
(Prasad et.al. 1999)
© Endeavour College of Natural Health endeavour.edu.au 33
Parkinson’s Disease
Therapeutic Actions
Vitamin C & Vitamin E
o Prasad et.al. (1999) found that “…a large community-based study in
the Netherlands has reported that vitamin E consumption was
significantly lower among patients with PD than among controls.” (p.
414)
o Also “…supplemental vitamin E (3,000IU/day) and vitamin C (3,000
mg/day) increased the time interval for requiring L-dopa therapy by
about 2 to 4 years in 75% of patients when compared to historical
controls.” (Prasad et.al. 1999, p. 418)
© Endeavour College of Natural Health endeavour.edu.au 34
Parkinson’s Disease
Nutritional Treatment Aims
o Support Digestive system
o Support the Liver and heavy metal chelation – increase sulphur
containing foods (e.g. garlic, onions, eggs) to aid in phase II
sulphation pathways. Sulphate conjugation has been implicated in
disease pathogenesis
o Support anti-oxidant status
o Support cellular energetics
o Support circulation
o Assess hydration levels
(Pizzorno & Murray 2006; Sarris & Wardle, 2010)
© Endeavour College of Natural Health endeavour.edu.au 35
Parkinson’s Disease
Nutritional Treatment Aims
Support neurotransmitter synthesis
o Maintain a protein status of 0.8g/kg to aid in dopamine production.
o Note: high amino acid levels can compete with levodopa across the
blood brain barrier, reducing efficacy.
o Fava (Broad) beans have been shown to be high in natural
levodopa – 100g serving = 250mg levodopa)
(Pizzorno & Murray 2006; Sarris & Wardle, 2010)
© Endeavour College of Natural Health endeavour.edu.au 36
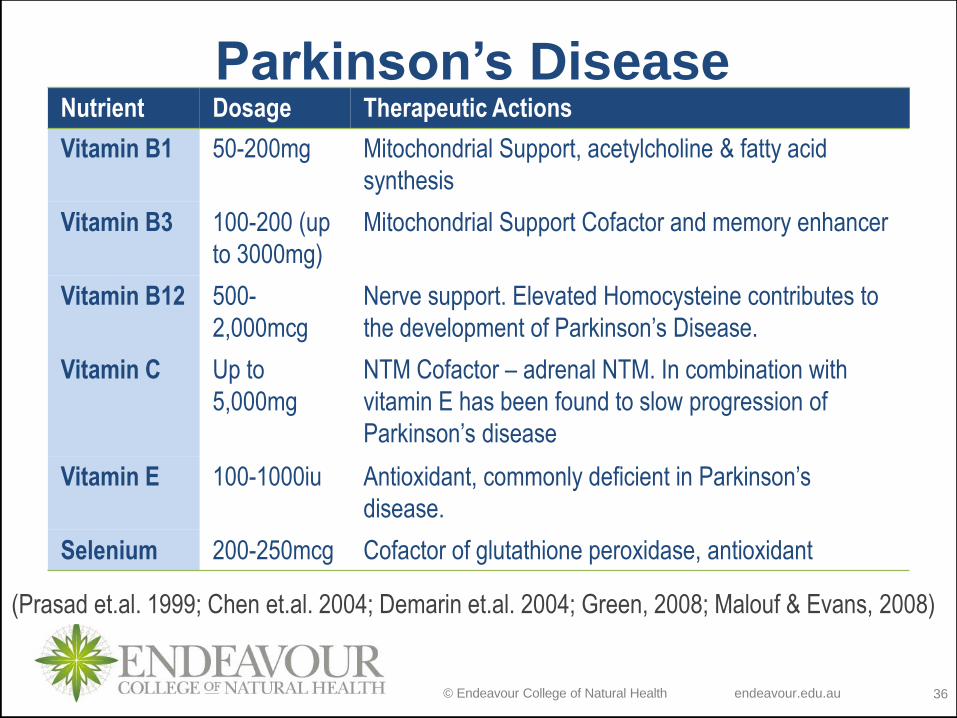
Parkinson’s DiseaseNutrient Dosage Therapeutic Actions
Vitamin B1 50-200mg Mitochondrial Support, acetylcholine & fatty acid
synthesis
Vitamin B3 100-200 (up
to 3000mg)
Mitochondrial Support Cofactor and memory enhancer
Vitamin B12 500-
2,000mcg
Nerve support. Elevated Homocysteine contributes to
the development of Parkinson’s Disease.
Vitamin C Up to
5,000mg
NTM Cofactor – adrenal NTM. In combination with
vitamin E has been found to slow progression of
Parkinson’s disease
Vitamin E 100-1000iu Antioxidant, commonly deficient in Parkinson’s
disease.
Selenium 200-250mcg Cofactor of glutathione peroxidase, antioxidant
(Prasad et.al. 1999; Chen et.al. 2004; Demarin et.al. 2004; Green, 2008; Malouf & Evans, 2008)
© Endeavour College of Natural Health endeavour.edu.au 37
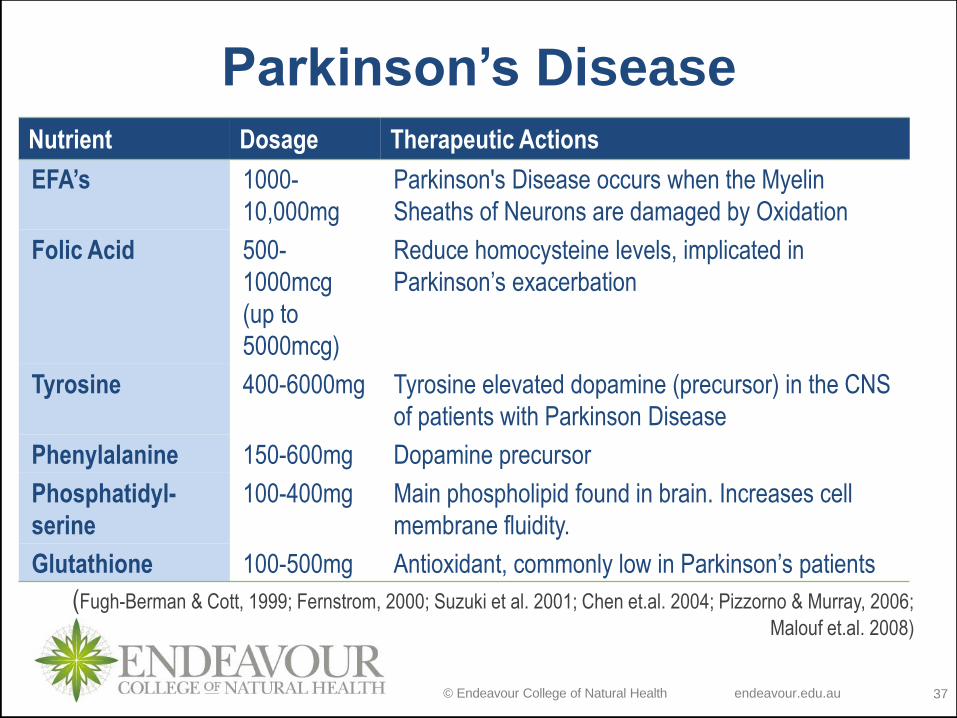
Parkinson’s Disease
Nutrient Dosage Therapeutic Actions
EFA’s 1000-
10,000mg
Parkinson's Disease occurs when the Myelin
Sheaths of Neurons are damaged by Oxidation
Folic Acid 500-
1000mcg
(up to
5000mcg)
Reduce homocysteine levels, implicated in
Parkinson’s exacerbation
Tyrosine 400-6000mg Tyrosine elevated dopamine (precursor) in the CNS
of patients with Parkinson Disease
Phenylalanine 150-600mg Dopamine precursor
Phosphatidyl-
serine
100-400mg Main phospholipid found in brain. Increases cell
membrane fluidity.
Glutathione 100-500mg Antioxidant, commonly low in Parkinson’s patients
(Fugh-Berman & Cott, 1999; Fernstrom, 2000; Suzuki et al. 2001; Chen et.al. 2004; Pizzorno & Murray, 2006;
Malouf et.al. 2008)
© Endeavour College of Natural Health endeavour.edu.au 38
Parkinson’s DiseaseDrug Management
o Parkinson’s Disease symptoms present as a depletion of
dopamine. This NT works in equilibrium with
acetylcholine to maintain proper motor function
o Goal of drug therapy is to restore the balance between
dopaminergic and cholinergic function
o This can be accomplished in different ways, including:
• Increasing dopamine levels
• Augmenting dopamine levels with drugs that mimic
dopamine activity
• Suppression of cholinergic activity (reduced ACh).
(Bullock et.al. 2007; Bryant & Knights, 2011)
© Endeavour College of Natural Health endeavour.edu.au 39
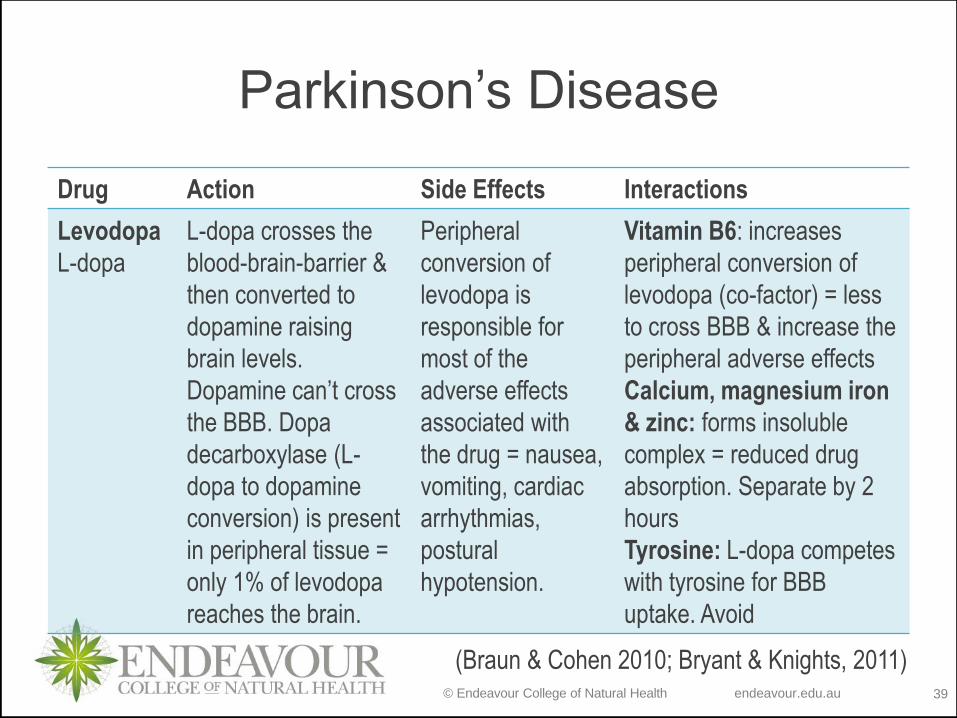
Parkinson’s Disease
Drug Action Side Effects Interactions
Levodopa
L-dopa
L-dopa crosses the
blood-brain-barrier &
then converted to
dopamine raising
brain levels.
Dopamine can’t cross
the BBB. Dopa
decarboxylase (L-
dopa to dopamine
conversion) is present
in peripheral tissue =
only 1% of levodopa
reaches the brain.
Peripheral
conversion of
levodopa is
responsible for
most of the
adverse effects
associated with
the drug = nausea,
vomiting, cardiac
arrhythmias,
postural
hypotension.
Vitamin B6: increases
peripheral conversion of
levodopa (co-factor) = less
to cross BBB & increase the
peripheral adverse effects
Calcium, magnesium iron
& zinc: forms insoluble
complex = reduced drug
absorption. Separate by 2
hours
Tyrosine: L-dopa competes
with tyrosine for BBB
uptake. Avoid
(Braun & Cohen 2010; Bryant & Knights, 2011)
© Endeavour College of Natural Health endeavour.edu.au 40
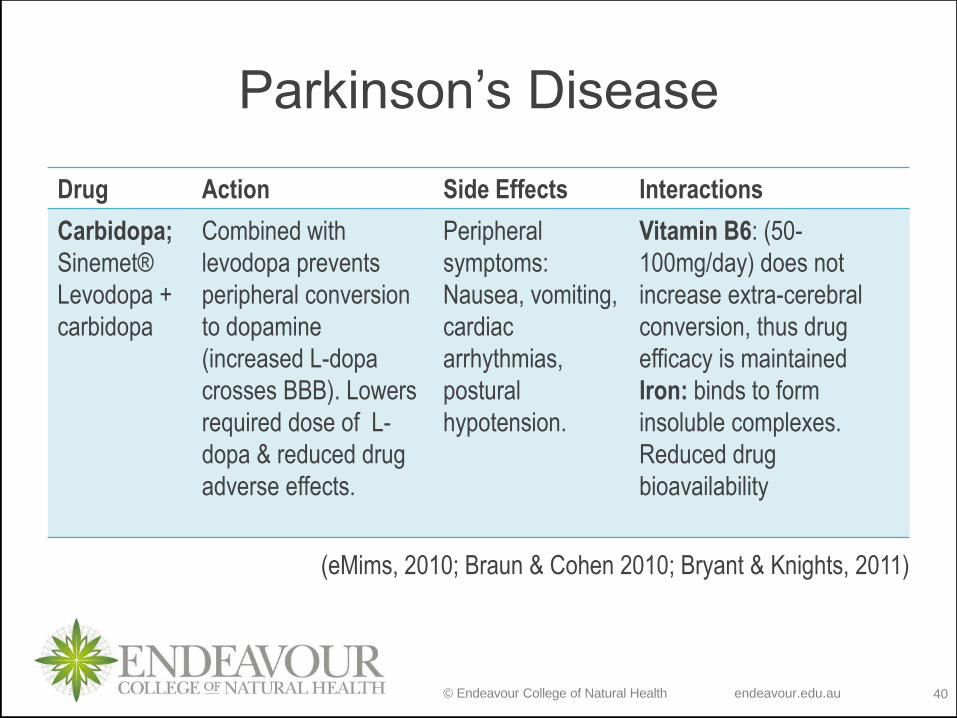
Parkinson’s Disease
Drug Action Side Effects Interactions
Carbidopa;
Sinemet®
Levodopa +
carbidopa
Combined with
levodopa prevents
peripheral conversion
to dopamine
(increased L-dopa
crosses BBB). Lowers
required dose of L-
dopa & reduced drug
adverse effects.
Peripheral
symptoms:
Nausea, vomiting,
cardiac
arrhythmias,
postural
hypotension.
Vitamin B6: (50-
100mg/day) does not
increase extra-cerebral
conversion, thus drug
efficacy is maintained
Iron: binds to form
insoluble complexes.
Reduced drug
bioavailability
(eMims, 2010; Braun & Cohen 2010; Bryant & Knights, 2011)
© Endeavour College of Natural Health endeavour.edu.au 41
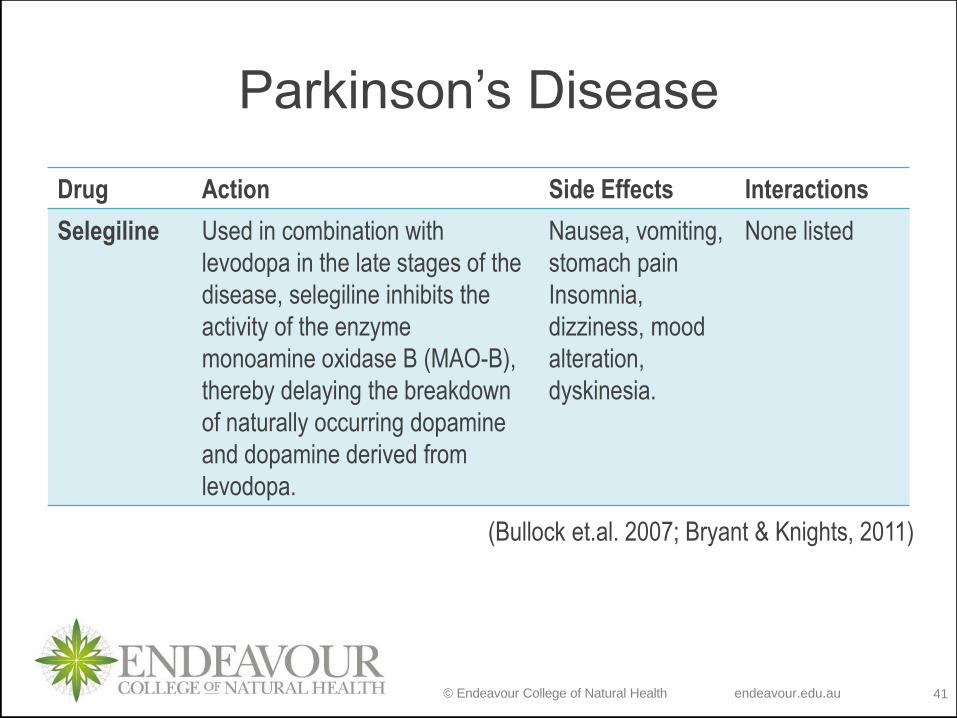
Parkinson’s Disease
Drug Action Side Effects Interactions
Selegiline Used in combination with
levodopa in the late stages of the
disease, selegiline inhibits the
activity of the enzyme
monoamine oxidase B (MAO-B),
thereby delaying the breakdown
of naturally occurring dopamine
and dopamine derived from
levodopa.
Nausea, vomiting,
stomach pain
Insomnia,
dizziness, mood
alteration,
dyskinesia.
None listed
(Bullock et.al. 2007; Bryant & Knights, 2011)
© Endeavour College of Natural Health endeavour.edu.au 42
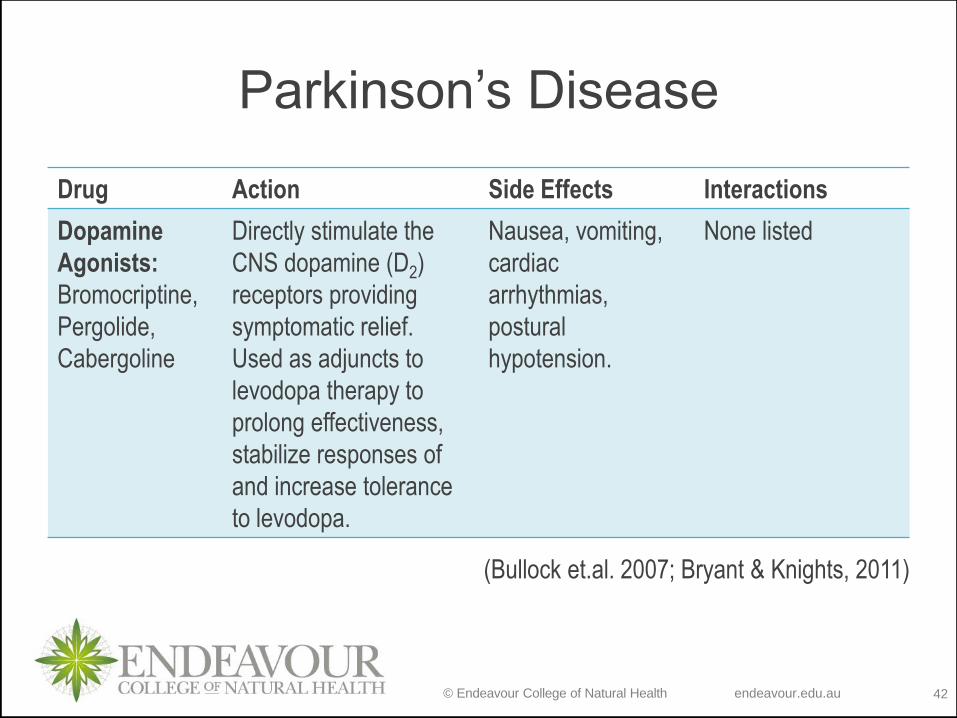
Parkinson’s Disease
Drug Action Side Effects Interactions
Dopamine
Agonists:
Bromocriptine,
Pergolide,
Cabergoline
Directly stimulate the
CNS dopamine (D2)
receptors providing
symptomatic relief.
Used as adjuncts to
levodopa therapy to
prolong effectiveness,
stabilize responses of
and increase tolerance
to levodopa.
Nausea, vomiting,
cardiac
arrhythmias,
postural
hypotension.
None listed
(Bullock et.al. 2007; Bryant & Knights, 2011)
© Endeavour College of Natural Health endeavour.edu.au 43
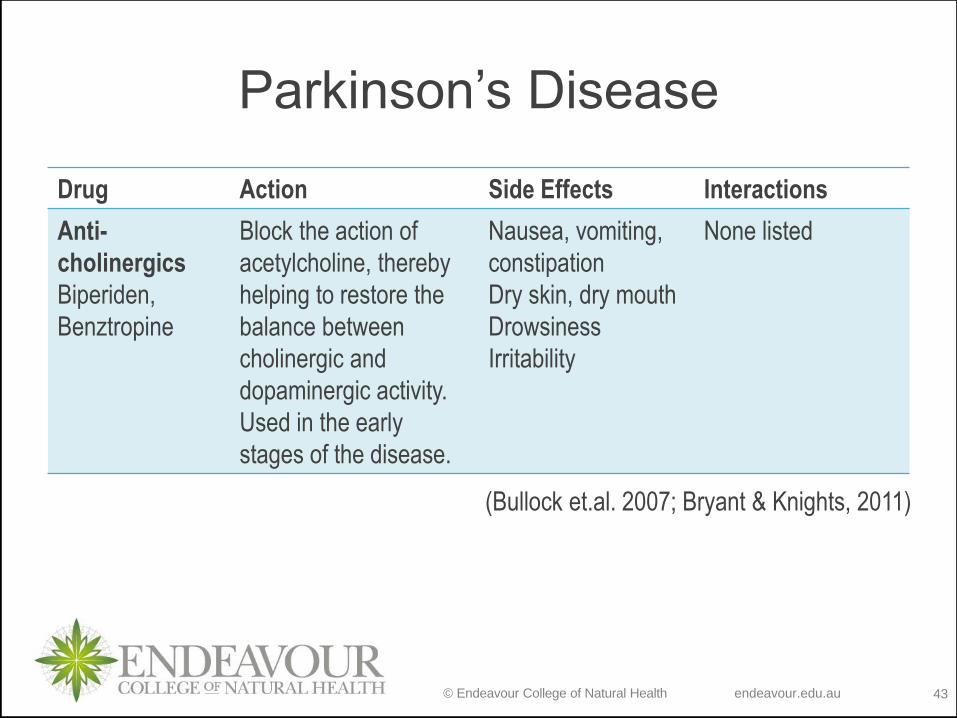
Parkinson’s Disease
Drug Action Side Effects Interactions
Anti-
cholinergics
Biperiden,
Benztropine
Block the action of
acetylcholine, thereby
helping to restore the
balance between
cholinergic and
dopaminergic activity.
Used in the early
stages of the disease.
Nausea, vomiting,
constipation
Dry skin, dry mouth
Drowsiness
Irritability
None listed
(Bullock et.al. 2007; Bryant & Knights, 2011)
© Endeavour College of Natural Health endeavour.edu.au 44
Parkinson’s Disease
Drug Interaction Considerations
o Natural therapies may be supportive in Parkinson’s
disease, but are not indicated as stand-alone therapies,
given the nature of the disease
o Currently, the only reported integrative interactions relate
to L-dopa, however care should be taken when
prescribing any natural therapies in Parkinson’s disease.
o All nutritional therapies that act on catecholamines,
especially dopamine or acetylcholine pathways, may
theoretically lead to an interaction with the anti-
Parkinson’s drug therapies
© Endeavour College of Natural Health endeavour.edu.au 45
References
o Auchus A. (2007). Dementia. Merk manual online for healthcare professionals. Retrieved 13 January 2011 from: 1http://www.merckmanuals.com/professional/sec16/ch213/ch213c.html#sec16-ch213-ch213c-99
o Burns, Alistair. (2009). Dementia. Brit Med J, 2009; 338.
o Braun, L., & Cohen, M. (2015). Herbs & natural supplements: An evidence-based guide (4th ed.). Chatswood, NSW: Elsevier.
o Bryant, B. J., & Knights, K. M. (2015). Pharmacology for health professionals (4th ed.). Chatswood, NSW: Elsevier.
o Bullock, S., Manias, E. & Galbraith, A. (2007). Fundamentals of pharmacology. 5th ed. Pearson, NSW.
o Chen, J., Lin, K., & Chen, Y. (2009). Review Article: Risk Factors for Dementia. Journal Of The Formosan Medical Association, 108754-764. doi:10.1016/S0929-6646(09)60402-2
o Chen, H., Zhang, S. M., Schwarzschild, M. A., Hernán, M. A., Logroscino, G., Willett, W. C., & Ascherio, A. (2004). Folate intake and risk of Parkinson's disease. American Journal Of Epidemiology, 160(4), 368-375.
© Endeavour College of Natural Health endeavour.edu.au 46
Referenceso Demarin, V., Podobnik, S.S., Storga-Tomic, D. & Kay, G. (2004). Treatment
of Alzheimer's disease with stabilized oral nicotinamide adenine dinucleotide: a randomized, double-blind study.’ Drugs under experimental and clinical research. Vol. 30, 1, p. 27-33. Retrieved 24 January 20122 from: http://www.ncbi.nlm.nih.gov/pubmed/15134388
o Douglas Shytle, R., Tan, J., Bickford, P. C., Rezai-zadeh, K., Hou, L., Zeng, J., Roschek, B. (2012). Optimized Turmeric Extract Reduces β-Amyloid and Phosphorylated Tau Protein Burden in Alzheimer’s Transgenic Mice. Current Alzheimer Research, 9(4), 500–506.
o Farber, S.A., Slack, B.E. & Blusztajn, J.K. (2000). Acceleration of phosphatidylcholine synthesis and breakdown by inhibitors of mitochondrial function in neuronal cells: a model of the membrane defect of Alzheimer’s disease.’ Journal of the federation of American societies for experimental biology. Vol. 14, p. 2198 – 2206. Retrieved 24 January 2011 from: http://www.fasebj.org/content/14/14/2198.abstract
o Fernstrom, J.D. (2000). Can nutrient supplements modify brain function?’ American journal of clinical nutrition. 71, 6, 1669s-1673s.
o Fugh-Berman , A & Cott, JM 1(999). Dietary supplements and natural
products as psychotherapeutic agents. Psychosomatic medicine, Vol.
61, No. 5, pp.712-28.
© Endeavour College of Natural Health endeavour.edu.au 47
References
o Gao, S., Jin, Y., Hall, K.S., Liang, C., Unverzagt, F.W., Ji, R., Murrell et al. (2007).
Selenium Level and Cognitive Function in Rural Elderly Chinese. American
journal of epidemiology. Vol. 165. Iss. 8, p. 955-965. Viewed 29 March 2018
from: http://aje.oxfordjournals.org/content/165/8/955.abstract
o Gatz, M., Fratiglioni, L., Johansson, B., Berg, S., Mortimer, J. A., Reynolds, C. A., &
Pedersen, N. L. (2005). Complete ascertainment of dementia in the Swedish
Twin Registry: the HARMONY study. Neurobiology Of Aging, 26(4), 439-
447.
o Green, K. N., Steffan, J. S., Martinez-Coria, H., Sun, X., Schreiber, S. S., Thompson,
L. M., & LaFerla, F. M. (2008). Nicotinamide restores cognition in Alzheimer's
disease transgenic mice via a mechanism involving sirtuin inhibition and
selective reduction of Thr231-phosphotau. The Journal Of Neuroscience: The
Official Journal Of The Society For Neuroscience, 28(45), 11500-11510.
doi:10.1523/JNEUROSCI.3203-08.2008
o Hager, K., Kenklies, M., & McAfoose, J. (2008). Alpha-lipoic acid as a new treatment
option for Alzheimer's disease--a 48 months follow-up analysis. Alternative
Medicine Review, (1), 74.
© Endeavour College of Natural Health endeavour.edu.au 48
Referenceso Huang, W., Alexander, G.E., Chang, L., Shetty, H.U., Krasuski, J.S.,
Rapoport, S.I. & Schapiro, M.B. (2001). Brain metabolite concentration
and dementia severity in Alzheimer’s disease. Neurology. 57, 4, 626-
634.
o Kumar, P. & Clark, M. (2009). Clinical medicine (7th ed). Edinburgh,
Scotland: Saunders Elsevier.
o Healthnotes Releases A -Z Guide to Drug-Herb-Vitamin Interactions, A
Comprehensive Reference for Consumers. (2000) PR Newswire.
o Lininger SW (1999). A-Z Guide to Drug-Herb-Vitamin Interactions. Healthnotes. Three Rivers Press. New York
o Louzada, P. R., Paula Lima, A. C., Mendonca-Silva, D. L., Noël, F., De Mello, F. G., & Ferreira, S. T. (2004). Taurine prevents the neurotoxicity of beta-amyloid and glutamate receptor agonists: activation of GABA receptors and possible implications for Alzheimer's disease and other neurological disorders. FASEB Journal: Official Publication Of The Federation Of American Societies For Experimental Biology, 18(3), 511-518.
o Luchsinger JA, Tang MX, Siddiqui M, et al (2004). Alcohol intake and risk of
dementia. J Am Geriatr Soc, vol 52:540–6.
© Endeavour College of Natural Health endeavour.edu.au 49
Referenceso Malouf, R. & Grimley Evans, J. (2008). Folic acid with or without vitamin B12 for the
prevention and treatment of healthy elderly and demented people.’ Cochrane database of systemic reviews. Retrieved 24 January 2011 from:
http://www2.cochrane.org/reviews/en/ab004514.html
o Mishra, S., & Palanivelu, K. (2008). The effect of curcumin (turmeric) on Alzheimer's disease: An overview. Annals Of Indian Academy Of Neurology, (1).
o Morris, M.C. (2004). Diet & Alzheimer’s disease: what the evidence shows.’ Medscape general medicine. Vol. 6, No. 1. Retrieved 24 January 2011 from: http://www.medscape.com/viewarticle/466037
o Mukamal KJ, Kuller LH, Fitzpatrick AL (2003). Prospective study of alcohol
consumption and risk of dementia in older adults. 2003;289:1405–13.
o Osiecki, H. (2014). The Nutrient Bible (7th ed.). Eagle Farm, QLD: Bioconcepts
Publishing.
o Peters R, Peters J, Warner J (2008). Alcohol, dementia and cognitive decline in the
elderly: a systematic review. Age Ageing. 37:505–12.
o Pizzorno, J., & Murray, M. (2006). Textbook of Natural Medicine (3rd ed). St. Louis,
MO: Churchill Livingstone.
© Endeavour College of Natural Health endeavour.edu.au 50
References
o Potter, P.E. (2010). Investigational medications for treatment of patients with Alzheimer disease.’ Journal of the American osteopathic association. Vol. 110, Iss. 9, Suppl. 8, p 27-36. Retrieved 11 January 2011 from:file:///C:/Users/staff/Desktop/Working/Research/Alzeimers%20Parkinsons/Investigations%20in%20AD.htm
o Prasad, K.N., Cole, W.C. & Kumar, B. (1999). Multiple antioxidants in the prevention
and treatment of Parkinson's disease.’ Journal of the American college of
nutrition, Vol. 18, No. 5, p. 413–423 viewed 26/01/11:
http://www.jacn.org/cgi/reprint/18/5/413
o Romi, F., Gilhus, N. E., & Aarli, J. A. (2005). Myasthenia gravis: clinical,
immunological, and therapeutic advances. Acta Neurologica Scandinavica,
111(2), 134-141.
o Reuben, D. B., Judd-Hamilton, L., Harris, T. B., & Seeman, T. E. (2003). The
associations between physical activity and inflammatory markers in high-
functioning older persons: MacArthur Studies of Successful Aging. Journal
Of The American Geriatrics Society, 51(8), 1125-1130.
o Sarris, J & Wardle, J (2010) Clinical naturopathy. Churchill Livingstone Elsevier,
Chatswood, NSW.
© Endeavour College of Natural Health endeavour.edu.au 51
References
o Spagnoli, A., Lucca, U., Menasce, G., Bandera, L., Cizza, G., Forloni et al.
(1999). Long‐term acetyl‐L‐carnitine treatment in Alzheimer's disease’
Neurology. Vol. 41, Iss. 11, p. 1726. Retrieved from:
http://www.neurology.org/content/41/11/1726.short
o Suzuki, S., Yamatoya, H., Sakai, H., Kataoka, A., Furushiro, M. & Kudo, S.
(2001). Oral administration of soybean lecithin transphosphatidylated
phosphatidylserine improves memory impairment in aged rats.’
Journal of nutrition. Vol. 131, p. 12951-2956. Viewed 24/01/11:
http://jn.nutrition.org/content/131/11/2951.full
© Endeavour College of Natural Health endeavour.edu.au 52
COMMONWEALTH OF AUSTRALIA
Copyright Regulations 1969
WARNING
This material has been reproduced and communicated to you by or on behalf of the Australian College of Natural Medicine Pty Ltd (ACNM) trading as Endeavour College of Natural Health, FIAFitnation, College of Natural Beauty, Wellnation - Pursuant Part VB of the Copyright Act 1968 (the Act).
The material in this communication may be subject to copyright under the Act. Any further reproduction or communication of this material by you may be the subject of copyright protection under the Act.
Do not remove this notice.








![Cholera, a disease of the nervous system. [Also:] … a Disease of the Nervous System. During my stay of one week at Southampton in 1865 I treated seven patients: five of these recovered,](https://static.fdocuments.net/doc/165x107/5b250b6c7f8b9a90368b4600/cholera-a-disease-of-the-nervous-system-also-a-disease-of-the-nervous-system.jpg)









