NICU AUDIT February 2014. JPB Born on February 14, 2014 Live preterm baby girl Delivered via...
26
NICU AUDIT February 2014
-
Upload
merry-stephens -
Category
Documents
-
view
216 -
download
0
description
Maternal History Chronic hypertensive for 24 years, usual BP systolic Feb 11, admitted at IMU for increase in BP given Methyldopa and Dexamethasone 10 mg every 12 hrs for 2 doses
Transcript of NICU AUDIT February 2014. JPB Born on February 14, 2014 Live preterm baby girl Delivered via...
NICU AUDIT
February 2014
JPB
• Born on February 14, 2014
• Live preterm baby girl• Delivered via Scheduled
Primary Cesarean Section for Maternal Condition (Breast Cancer)
• 41 y/o• G2P2 (1102) • 28 5/7 weeks AOG
• BW 1250 g• BL 38 cm• HC 26 cm• CC 23 cm• AC 21 cm• MT 30, AGA• AS 9,9

Maternal History
• Chronic hypertensive for 24 years, usual BP 140-150 systolic
• Feb 11, 2014- admitted at IMU for increase in BP given Methyldopa and Dexamethasone 10 mg every 12 hrs for 2 doses

Past Medical History• Feb. 2013
– noted to have a 2x3 cm mass on the left breast. – Mammography done showing “malignancy” but was lost to ff-
up• Feb. 3, 2014
– Breast mass was increasing in size w/ engorgement of the breast– Biopsy done w/c showed Intraductal Carcinoma of the Left
Breast, BIRADS 4• Feb 12, 2014
– Ultrasound done: BPS 8/8, EFW 1305 g, Placenta anterior, grade 2, high lying, normohydramnios, Myoma 2.5X2.6 cm

Family History• DM• HTN
Personal/ Social History• unremarkable
OB History•G1- 2008, NSD, Full Term, male, BW 8lbs•G2- present pregnancy
Delivery
• Apgar 1 min: HR >120’s, acrocyanotic, good cry and activity, spontaneous breathing
• Apgar 5 min: HR >120’s, acrocyanotic, good cry and activity, spontaneous breathing
• Immediately placed in a food grade plastic bag• O2 saturation: >85%• Newborn care was rendered
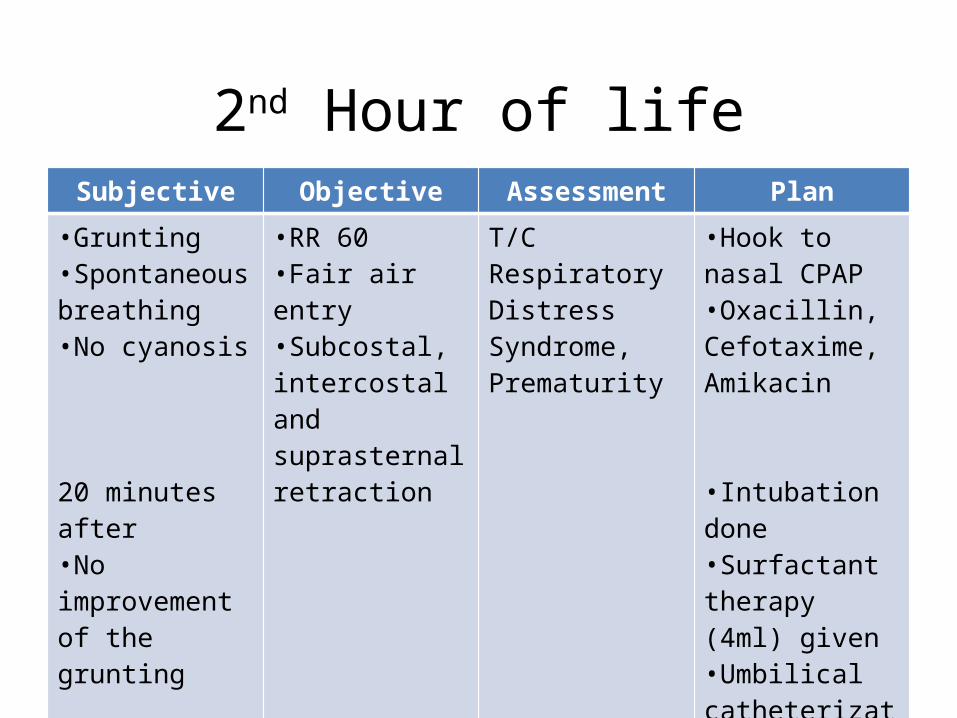
2nd Hour of lifeSubjective Objective Assessment Plan
•Grunting•Spontaneous breathing•No cyanosis
20 minutes after•No improvement of the grunting
•RR 60•Fair air entry•Subcostal, intercostal and suprasternal retraction
T/C Respiratory Distress Syndrome, Prematurity
•Hook to nasal CPAP•Oxacillin, Cefotaxime, Amikacin
•Intubation done•Surfactant therapy (4ml) given•Umbilical catheterization

VBG
pH pCO2 PO2 HCO3 O2 BE
7.328 61.7 45.1 32.3 76.3 5.3 Compensated Respiratory Acidosis
Chest Xray Consider Hyaline Membrane Disease, cannot totally rule out Neonatal Pnemonia
Blood Culture
No Growth (7 days)
CBC
Hgb Hct WBC Band Neu Lymp Mon Eos Plt
151 45 7.9 4 48 42 5 1 239 4nRBC/100 WBC
HGT 82


1st day of lifeSubjective Objective Assessment Plan
•Intubated•FiO2 40%•RR 35•PIP 14•PEEP 3.8•s/p surfactant therapy•Mother had a would culture: Heavy growth of S. aureus: sensitive to all except Penicillin
•VS: HR 144, RR 65, T 36.9 O2 sat 98%•Jaundice to upper chest•Good air entry, subcostal, intercostal, suprasternal retractions •Good cardiac tone•Soft abdomen•Full pulses
Respiratory Distress Syndrome vs Neonatal Pneumonia, Sepsis, unspecified, Hyperbilirubinemia, unspecified
•Labs: Bilirubin Levels, CRP, Chest Xray, Hgt
•Single Overhead Phototherapy
•Oxacillin, Cefotaxime, Amikacin

Bilirubin Levels
Total Direct Indirect
5.21 0.38 4.92
Chest Xray Consider Hyaline Membrane Disease, with interval improvement in the Lung Status
CRP 0.21 mg/dl
HGT 152
VBG
pH pCO2 PO2 HCO3 O2 BE
7.354 59.8 28.4 33.2 50.3 6.6 Compensated Respiratory Acidosis


4th day of lifeSubjective Objective Assessment Plan
•Extubated•Shifted to nasal IPPVFiO2 30%PIP 12/4RR 15iT 0.4FR 8
•VS: HR 178, RR 68, T 36.8 O2 sat 100%•Jaundice to face•Good air entry, subcostal, retractions •Good cardiac tone•Soft abdomen•Full pulses
Mild Respiratory Distress Syndrome, Sepsis, unspecified, Hyperbilirubinemia, unspecified
•Labs: Hgt (119)
•Single Overhead Phototherapy
•Epinephrine 0.1 ml + 1.5 ml NSS every 30 mins for 2 doses•Aminophylline 6 mg loading dose (4.8mg/kg), 1 mg every 12 hrs (0.8 mg/kg)•Oxacillin,Cefotaxime, Amikacin

5th day of lifeSubjective Objective Assessment Plan
•No desaturations•No cyanosis
•VS: HR 177, RR 50, T 36.8 O2 sat 100%•Jaundice to abdomen•Good air entry, subcostal, retractions •Good cardiac tone•Soft abdomen•Full pulses
Mild Respiratory Distress Syndrome, Sepsis, unspecified, Hyperbilirubinemia, unspecified
•Labs: Hgt, Bilirubin level, Na, K
•Single Overhead Phototherapy
•Shifted to nasal cannula at 0.5 lpm, then discontinued
•Oxacillin, Cefotaxime, Amikacin
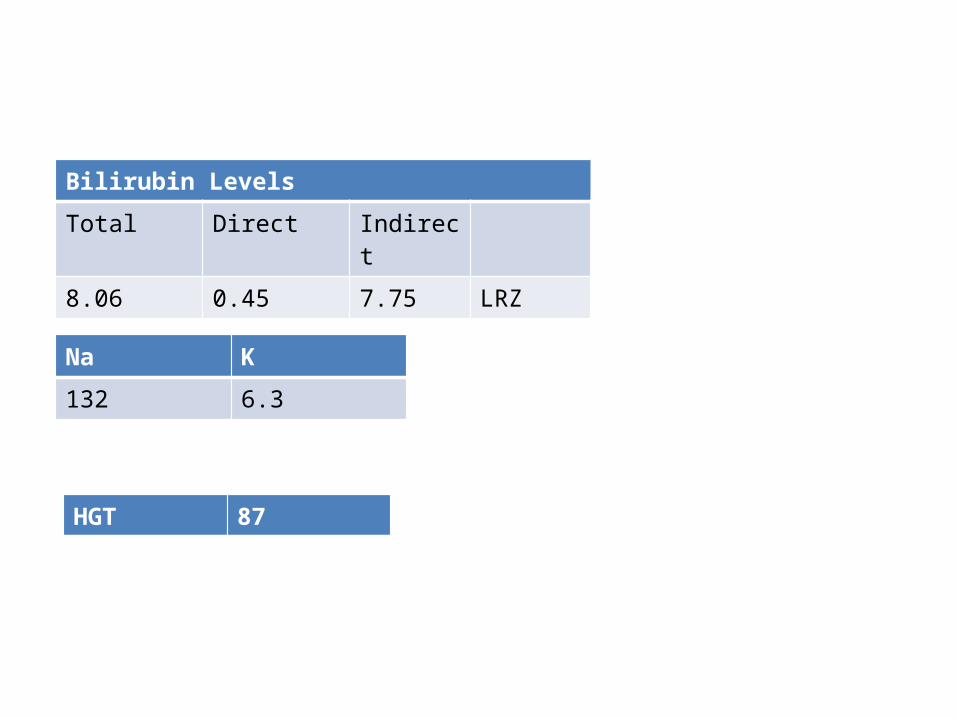
Bilirubin Levels
Total Direct Indirect
8.06 0.45 7.75 LRZ
Na K
132 6.3
HGT 87

7th day of lifeSubjective Objective Assessment Plan
•No desaturations•No cyanosis•apnea 5-10 seconds, HR 90’s, O2 sats 64-69%
•VS: HR 152, RR 67, T 36.6 O2 sat 98%•Jaundice to abdomen•Good air entry, no retractions•Good cardiac tone•Soft abdomen•Full pulses
Apnea, Mild Respiratory Distress Syndrome, Sepsis, unspecified, Hyperbilirubinemia, unspecified
•Labs: CBC, hgt, Chest Xray
•Single Overhead Phototherapy (intermittent)
•O2 support discontined•Aminophylline increased to 2 mg IV (1.6 mg/kg)•Antibiotics shifted to Piperacillin- Tazobactam 60 mg IV (53 mg/kg/dose)

• CBC, hgt, chest xray
Chest Xray Hyaline Membrane Disease with further improvement in lung status
CBC
Hgb Hct WBC Band Neu Lymp Mon Eos Plt
150 45 22 9 61 22 7 1 370 Slight toxic granules
HGT 68


14th day of lifeSubjective Objective Assessment Plan
•Episodes of desaturations•Episodes of apnea (5-10 seconds, HR 80’s-90’s, O2 saturation 70%) w/c responds to tactile stimulation
•VS: HR 150, RR 49, T 36.6 O2 sat 95%•pink•Good air entry, shallow subcostal retractions•Good cardiac tone•Soft abdomen•Full pulses
Apnea, Mild Respiratory Distress Syndrome, Sepsis, unspecified, Hyperbilirubinemia, unspecified, resolved
•Labs: CBC, hgt
•O2 support •Aminophylline resumed•Piperacillin- Tazobactam increased to 120 mg (100 mg/kg/dose)

• CBC, hgt, chest xray
CBC
Hgb Hct WBC Band Neu Lymp Mon Eos Plt
143 43 14.4 20 47 16 10 7 522 Slight toxic granules
HGT 92

15th day of lifeSubjective Objective Assessment Plan
•Episodes of desaturations •Episodes of apnea (10-20 seconds, HR 60’s-70’s, O2 saturation 70%) w/c responds to tactile stimulation
•VS: HR 150, RR 49, T 36.6 O2 sat 95%•Pink, mottled skin•Good air entry, shallow subcostal retractions•Good cardiac tone•Soft abdomen•Full pulses
Apnea, Mild Respiratory Distress Syndrome, Sepsis, unspecified, Hyperbilirubinemia, unspecified, resolved
•Labs: blood culture, urinalysis, Chest xray, Na, K, Bilirubin levels, Hgt, blood gas•Nasal CPAP intubation •Aminophylline increased to every 8 hours•Pip-Taz discontinued shifted to Meropenem 24 mg IV every 12 hrs (20 mkdose)

VBG
pH pCO2 PO2 HCO3 O2 BE
7.24 55.7 33 24 26 -3.0 Respiratory Acidosis
Chest Xray unchanged bilateral lung opacities consistent with resolving hyaline membrane disease
Blood Culture
No growth for 24 hrs
Hgb Hct
126 37HGT 92
Urinalysis
RBC WBC Epithelial Cast Bacteria
2 5 61 0 14
Na K iCal139 4.9 139
Bilirubin Levels
Total Direct Indirect
4.54 0.38 4.22 LRZ


16th day of lifeSubjective Objective Assessment Plan
•Intubated•FR 8•FiO2 20•RR 20•PIP 10•PEEP 4• iT 0.5•No desaturations
•VS: HR 141, RR 52, T 37 O2 sat 100%•Pink•Good air entry, shallow subcostal retractions•Good cardiac tone•Soft abdomen•Full pulses
Apnea, Mild Respiratory Distress Syndrome, Sepsis, unspecified, Hyperbilirubinemia, unspecified, resolved
•Labs: Blood gas
•Nasal CPAP intubation
•Aminophylline decreased to every 12 hours
•Meropenem 24 mg IV every 12 hrs (20 mg/kg/dose)

VBG
pH pCO2 PO2 HCO3 O2 BE
7.261 63.4 35.7 28.4 57.9 -0.2 Respiratory Acidosis
Current Diagnosis
Prematurity, Very Low Birth Weight, Apnea of Prematurity, Sepsis, Mild
Respiratory Distress Syndrome, Hyperbilirubinemia, unspecified,
Resolved