Nicotinamide Mononucleotide in the Context of Elevated ...€¦ · Wheeler, and Dr. Pausova for...
147
Nicotinamide Mononucleotide in the Context of Elevated Plasma Levels of Free Fatty Acids Improves Glucose Tolerance by Decreasing Insulin Clearance By Ashraf Nahle A thesis submitted in conformity with the requirements for the degree of Master of Science Department of Physiology University of Toronto © Copyright by Ashraf Nahle (2016)
Transcript of Nicotinamide Mononucleotide in the Context of Elevated ...€¦ · Wheeler, and Dr. Pausova for...

Nicotinamide Mononucleotide in the Context
of Elevated Plasma Levels of Free Fatty Acids
Improves Glucose Tolerance by Decreasing
Insulin Clearance
By
Ashraf Nahle
A thesis submitted in conformity with the requirements
for the degree of Master of Science
Department of Physiology
University of Toronto
© Copyright by Ashraf Nahle (2016)

ii
Nicotinamide Mononucleotide in the Context of Elevated
Plasma Levels of Free Fatty Acids Improves Glucose
Tolerance by Decreasing Insulin Clearance
Ashraf Nahle
Master of Science
Department of Physiology
University of Toronto
2016
Abstract
The NAD-dependent deacetylase SIRT1 has been shown to be beneficial to beta cell function.
Nicotinamide Mononucleotide (NMN), the product of the rate-limiting enzyme in NAD synthesis,
has recently been shown to have positive effects on glucose tolerance in mice fed a high fat diet.
This is the first study to examine the effects of NMN on insulin clearance and FFA-induced beta
cell dysfunction. NMN was i.v. infused, with or without oleate, in C57BL/6 mice over 48h in
order to elevate intracellular NAD levels and consequently increase SIRT1 activity. We
demonstrated that administration of NMN in the context of elevated plasma FFA levels results in
a significant decrease in insulin clearance as well as partial protection against FFA-induced beta
cell dysfunction in vivo. This culminated in a large improvement in glucose tolerance. In
summary, NMN may have a therapeutic potential to improve glucose tolerance in conditions of
increased plasma FFA levels, which is typical in patients with type 2 diabetes mellitus.

iii
Acknowledgements
I am very grateful to Dr. Adria Giacca for providing me with the opportunity to contribute
to the front-line of research in type 2 diabetes mellitus, a disease that afflicts many millions
globally. Almost always available, Dr. Giacca has been a beacon of wisdom, guidance, and
patience. I am also incredibly grateful to my supervisory committee, Dr. I. George Fantus, Dr.
Carolyn Cummins, and Dr. Jonathan Rocheleau for their wise guidance, encouragement, and
understanding throughout the years. I would like to thank Dr. Zdenka Pausova for introducing me
to research during my undergraduate degree, as well as Dr. Denise Belsham, Dr. Michael
Wheeler, and Dr. Pausova for their enlightening courses on presentation skills and on the critical
analysis of studies.
In the beginning, I found leading basic science research projects to be challenging;
however, through perseverance, dedication to researching this important illness, and generous
support from friends and colleagues, we have discovered a potentially therapeutic biochemical
pathway. I have also matured both educationally and personally.
I would like to thank my friends and colleagues, Dr. Prasad Dalvi, Dr. Yusaku Mori, Alex
Ivovic, Frankie Poon, Loretta Lam, Lucy Yeung, Alex Orazietti, Tiffany Yu, Tejas Desai, Dr.
Khajag Koulajian, Dr. June Guo, Sammy Cai, and Cynthia Putra for helping make my experience
enjoyable and memorable. I trust that we will stay in touch. I am especially grateful to Loretta
Lam and Frankie Poon for their considerable experimental assistance, and to Dr. Prasad Dalvi,
Dr. Yusaku Mori, and Alex Ivovic for their generous advice, support, and encouragement during
my tough times doing research. Thank you, as well, to Dr. Sonia M. Najjar and her lab, especially
Hilda Ghadieh, for their collaboration in our research and their valuable scientific advice. Of
course, thank you to Ms. Rosalie Pang for her indispensable administrative advice.
I am extremely grateful to my mother, father, and sister for their unwavering support, love,
and frequent phone calls while they were overseas for years. I am very grateful to my close
friends, especially my significant other Lindsay Kuipers and her family, for their kind support,
wise advice, and positivity.
It feels very rewarding to have worked with highly motivated and skilled researchers and to
have contributed to the development of therapeutic and preventive healthcare for patients with
type 2 diabetes. I will always be grateful to everyone involved in our research. Best wishes to
your life and career!

iv
Table of Contents
Abstract………………………………………………………………………………………..ii
Acknowledgements…………………………………………………………………………...iii
Table of Contents……………………………………………………………………………..iv
List of Abbreviations………………………………………………………………………….vi
List of Figures……………………………………………………………………………….viii
List of Tables………………………………………………………………………………….ix
Chapter 1: Introduction ..................................................................................................... 1 1.1 Glucose Homeostasis .......................................................................................................... 1 1.2 Diabetes Mellitus ................................................................................................................ 3 1.3 Complications ..................................................................................................................... 5 1.4 Risk Factors ........................................................................................................................ 7
1.5 Epidemiology ...................................................................................................................... 9 1.6 Insulin Secretion ............................................................................................................... 10
1.7 Insulin Clearance .............................................................................................................. 13 1.8 Fat-Induced Beta Cell Dysfunction .................................................................................. 19
1.8.1 .... Methods of Assessing FFA-Induced Beta Cell Dysfunction ............................................ 20 1.8.2 .... Effects of Different Lipid Treatments on Beta Cell Dysfunction ..................................... 22 1.8.3 .... Genetic Predisposition to Lipid-Induced Beta Cell Dysfunction ..................................... 23 1.8.4 .... Beta Cell Replenishment .................................................................................................. 24 1.8.5 .... Effect of FFAs on Beta Cell Mass .................................................................................... 25
1.9 Glucotoxicity and Glucolipotoxicity ................................................................................ 26 1.10 Mechanisms of FFA-Induced Beta Cell Dysfunction ...................................................... 28
1.10.1 .. The Role of Oxidative Stress ............................................................................................ 28 1.10.2 .. The Role of Endoplasmic Reticulum Stress ..................................................................... 32 1.10.3 .. The Role of Inflammation ................................................................................................ 34 1.10.4 .. The Role of Protein Kinase C ........................................................................................... 35 1.10.5 .. The Role of Ceramides ..................................................................................................... 38
1.11 Sirtuins .............................................................................................................................. 38 1.11.1 .. Sirtuin-1 ............................................................................................................................ 41 1.11.2 .. Role of SIRT1 in Beta Cells ............................................................................................. 42 1.11.3 .. Roles of SIRT1 in the Liver, Skeletal Muscle, and Brain ................................................ 44 1.11.4 .. Roles of FOXO Proteins ................................................................................................... 45 1.11.5 .. Regulation of SIRT1 ......................................................................................................... 46 1.11.6 .. Nicotinamide Mononucleotide ......................................................................................... 50 1.11.7 .. Potential Role of SIRT3.................................................................................................... 54
1.12 Potential Treatments for Lipid-Induced Beta Cell Dysfunction ....................................... 55
Chapter 2: Rationale ........................................................................................................ 59 2.1 Previous Results from the Giacca Lab .............................................................................. 59 2.2 My Experimental Design ................................................................................................... 63
Chapter 3: Materials and Methods ................................................................................. 65 3.1 Animal Models .................................................................................................................. 65 3.2 Mouse Cannulation Surgery .............................................................................................. 65

v
3.3 Treatment Infusion in Mice ............................................................................................... 66 3.4 One-Step Hyperglycemic Clamp ....................................................................................... 66
3.5 Glycemia ............................................................................................................................ 67
3.6 Plasma Insulin Levels ........................................................................................................ 68 3.7 Plasma C-Peptide Levels ................................................................................................... 69 3.8 Plasma FFA Levels ............................................................................................................ 69 3.9 Western Blotting ................................................................................................................ 70 3.10 Insulin Sensitivity Index .................................................................................................... 70
3.11 Disposition Index ............................................................................................................... 71 3.12 Insulin Clearance Index ..................................................................................................... 71 3.13 Statistics ............................................................................................................................. 72
Chapter 4: Results ............................................................................................................ 73 4.1 Glycemia ............................................................................................................................. 74 4.2 Glucose Infusion Rate ......................................................................................................... 75
4.3 Plasma Insulin Levels ......................................................................................................... 76 4.4 Plasma C-Peptide Levels .................................................................................................... 77
4.5 Insulin Clearance Index ...................................................................................................... 78 4.6 Insulin Sensitivity Index ..................................................................................................... 79
4.7 Disposition Index ................................................................................................................ 81
4.8 Plasma Free Fatty Acids Levels ......................................................................................... 82 4.9 CEACAM1 Western Blots ................................................................................................. 84
Chapter 5: Discussion ....................................................................................................... 85 5.1 Potential Mechanisms Behind NMN’s Effects on Insulin Clearance ................................. 87
5.1.1 Synergistic Effects of SIRT1 and FFA on PPARα-Mediated Decrease in CEACAM1
Expression .............................................................................................................................. 87 5.1.2 NMN Accentuates the FFA–Akt–FOXO1–PGC-1α–PPARα–Mediated Decrease in
CEACAM Expression............................................................................................................ 89 5.1.3 Potentially Opposing Effects of FFA and SIRT1 on PKCδ/ε-Mediated Decrease in Insulin
Clearance ............................................................................................................................... 91
5.2 Potential Mechanisms Behind NMN’s Effects on Beta Cell Function ............................... 92 5.2.1 SIRT1-FOXO1/3-Mediated Reduction of Oxidative Stress Ameliorated FFA-Induced Beta
Cell Dysfunction .................................................................................................................... 92 5.2.2 Decreased Plasma FFA Levels Resulted in the Amelioration of FFA-Induced Beta Cell
Dysfunction ............................................................................................................................ 94 5.2.3 Excess Antioxidants During Normal Plasma FFA and Intracellular ROS Levels Resulted in
Sub-Optimal ROS Levels and Decreased GSIS .................................................................... 94 5.2.4 SIRT1-FOXO1-Mediated Nuclear Exclusion of Pdx-1, Resulting in Decreased Insulin
Secretion ................................................................................................................................ 95 5.2.5 NAD-Mediated Increase in PARP Activity Decreases ATP for Insulin Secretion ............... 95
5.3 Limitations ........................................................................................................................... 97 5.4 Future Directions ................................................................................................................. 98 5.5 Conclusions ....................................................................................................................... 103
References ........................................................................................................................ 105

vi
List of Abbreviations
8-OHdG – 8-hydroxy-2’-deoxyguanosine
ACS – Acyl-CoA Synthetase
ANOVA – One-way non-parametric analysis
of Variance
AROS – Active Regulator of SIRT1
ATM – Ataxia Telangiectasia Mutated
ATP - Adenosine triphosphate
BAT – Brown Adipose Tissue
BIM – Bisindolylmaleimide
BMI – Body Mass Index
BSA – Bovine Serum Albumin
CDA – Canadian Diabetes Association
Cdk-1 – Cyclin-dependent kinase-1
CEACAM1 – Carcinoembryonic Antigen-
related Cell Adhesion Molecule-1
ChIP – Chromatin Immunoprecipitation
CHOP – CCAAT-enhancer-binding protein
homologous protein
CPT1B – Carnitine palmitoyltransferase 1B
CV – Coefficient of Variation
DAG – Diacylglycerol
DBC-1 – Deleted in Breast Cancer-1
DCF – Dichlorodihydrofluorescein
DI – Disposition Index
DKA – Diabetic Ketoacidosis
DPP-4 – Dipeptidyl Peptidase-4
ER – Endoplasmic Reticulum
ETC – Electron Transport Chain
FFA – Free Fatty Acid
FPG – Fasting Plasma Glucose
FFAR – Free Fatty Acid Receptor
FOXO – Forkhead box-O
FRD – Fructose-Rich Diet
GAPDH – Glyceraldehyde-3-phosphate
dehydrogenase
GDH – Glucose dehydrogenase
GDM – Gestational Diabetes Mellitus
GINF – Glucose Infusion Rate
GIP – Gastric Inhibitory Polypeptide
GIP-R – Gastric Inhibitory Polypeptide
Receptor
GLP-1 – Glucagon-like Peptide-1
GLP1R – Glucagon-like Peptide 1 Receptor
GLUT1/2 – Glucose transporter 1/2
GPCR – G-protein-coupled receptor
GPR40/41/43/119 – G-protein-coupled
receptor 40/41/43/119
GPx4 – Glutathione Peroxidase-4
GSIS – Glucose-Stimulated Insulin
Secretion
H2DCF-DA - 2',7'-dichlorodihydrofluorescein
diacetate
HFD – High Fat Diet
HLA – Human Leukocyte Antigens
HRP – Horseradish peroxidase
IDE – Insulin Degrading Enzyme
IH – Intralipid + Heparin
IKKB – Inhibitor of nuclear factor kappa-B
kinase subunit beta
IPGTT – Intraperitoneal Glucose Tolerance
Test
IR – Insulin Receptor
IRS – Insulin Receptor Substrate
IκBα – Nuclear factor of kappa light
polypeptide gene enhancer in B-cells
inhibitor, alpha
JNK – c-Jun-N-terminal Kinase
KM – Michaelis constant
LC-CoA – Long-Chain Coenzyme A
LDCV – Large Dense Core Vesicles
LPL – Lipoprotein Lipase
L-SACC1 - Liver-specific dominant-negative
phosphorylation-defective S503A CEACAM1
LXR – Liver X Receptor
M/I – Glucose metabolism value/[insulin]
(Index of insulin sensitivity)
MCAD – Medium-chain acyl-CoA
dehydrogenase
MDA – Malondialdehyde

vii
MEHA – 3-methyl-N-ethyl-N-(B-
hydroxyethyl)-aniline
MnSOD – Manganese superoxide dismutase
MUFA – Monounsaturated Fatty Acid
NAC – N-acetylcysteine
NAD – Nicotinamide Adenosine
Dinucleotide
NADPH oxidase – Nicotinamide Adenine
Dinucleotide Phosphate oxidase
NAMPT – Nicotinamide
phosphoribosyltransferase
NCLX – Na+/Ca2+ exchanger
NCoR – Nuclear receptor co-repressor
NFκB – Nuclear factor kappa-light-chain-
enhancer of activated B cells
NMN – Nicotinamide mononucleotide
NMNAT – Nicotinamide mononucleotide
adenylyltransferase-1
OGTT – Oral Glucose Tolerance Test
OLE – Oleate
PARP – Poly (ADP-Ribose) Polymerase
PBA – Phenylbutyrate
PC – Proprotein Convertase
PCOS – Polycystic Ovary Syndrome
PDK4 – Pyruvate Dehydrogenase Kinase 4
Pdx-1 – Pancreas duodenum homeobox-1
PGC-1α - Peroxisome proliferator-activated
receptor gamma coactivator 1-alpha
PI3K – Phosphoinositide 3-kinase
PKA – Protein Kinase-C Activator
PKC – Protein Kinase C
PML - Promyelocytic leukemia
POD – Peroxidase
POMC – Proopiomelanocortin
PP Cells – Pancreatic Polypeptide Cells
PTP1B – Protein-tyrosine phosphatase 1B
PUFA – Polyunsaturated Fatty Acid
PVDF – Polyvinylidene fluoride
RER – Rough Endoplasmic Reticulum
ROS – Reactive Oxygen Species
RPMI media – Roswell Park Memorial
Institute media
RPTPs – Receptor-like Protein Tyrosine
Phosphatases
RPTPs – Receptor-like Protein Tyrosine
Phosphatases
SAL – Saline
SAS – Statistical Analysis System
SDS-PAGE – Sodium dodecyl sulfate
polyacrylamide gel electrophoresis
SE – Standard Error
SF-1 – Steroidogenic Factor-1
SFA – Saturated Fatty Acid
SIR genes – Silent Information Regulator
genes
siRNA – Small interfering ribonucleic acid
SIRT – Silent mating type information
regulation 2 homolog
SMRT – Silencing Mediator of Retinoid and
Thyroid hormone receptors
SPT – Serine palmitoyltransferase
STZ – Streptozotocin
T1DM – Type 1 Diabetes Mellitus
T2DM – Type 2 Diabetes Mellitus
TCA Cycle – Tricarboxylic Acid Cycle
TGN – Trans-Golgi Network
TLR-4 – Toll-like receptor-4
TMB – 3,3',5,5'-tetramethylbenzidine
TZDs – Thiazolidinediones
UCP1/2 – Uncoupling protein 1/2
UPR – Unfolded Protein Response
VDCC – Voltage-Dependent Ca2+ Channels
WAT – White Adipose Tissue
WHO – World Health Organization
ZDF rats – Zucker Diabetic Fatty rats

viii
List of Figures
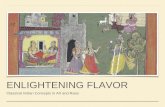
Figure 1. Anatomy of the Islets of Langerhans in the Human Pancreas. ................................................. 2
Figure 2. Mechanisms of glucose-stimulated insulin secretion (GSIS) in the beta cell. ....................... 12
Figure 3. Summary of the process of insulin clearance in the hepatocyte. ............................................ 16
Figure 4. The Disposition Index (DI) is the product constant of insulin secretion and insulin
sensitivity ............................................................................................................................................... 21
Figure 5. Illustrations of the three-dimensional protein structure and catalytic activity of the NAD-
dependent protein deacetylase Sirtuin-1 (SIRT1). ................................................................................. 41
Figure 6. Chemical structure of nicotinamide mononucleotide (NMN). ............................................... 50
Figure 7. Summary of the Nampt-mediated NAD synthesis. ................................................................ 54
Figure 8. Resveratrol, a SIRT1 activator, partially protects against FFA-induced beta cell
dysfunction in rats in vivo ...................................................................................................................... 60
Figure 9. Beta cell-specific SIRT1 overexpressing (BESTO) mice were partially protected against
FFA-induced beta cell dysfunction in vivo ............................................................................................ 60
Figure 10. Islets of Wistar rats i.v. infused with oleate did not demonstrate decreased NAD
bioavailability, compared with the saline-infused control ..................................................................... 62
Figure 11. Glucose tolerance and plasma levels of insulin, cholesterol, triglycerides, and free fatty
acids of mice fed a high-fat-diet and treated with nicotinamide mononucleotide.. ............................... 63
Figure 12. Gradual elevation in glycemia of wildtype mice i.v. infused with 37.5% glucose during
the hyperglycemic clamp.. ..................................................................................................................... 74
Figure 13. Glucose infusion rate (GINF) required for obtaining and maintaining hyperglycemia in
mice. ....................................................................................................................................................... 75
Figure 14. Plasma insulin levels prior to i.v. glucose infusion (basal glycemia) and after the
maintenance of hyperglycemia (clamp) for ~30 minutes in C57BL/6 mice.. ........................................ 76
Figure 15. Plasma C-peptide levels prior to i.v. glucose infusion (basal glycemia) and after the
maintenance of hyperglycemia (clamp) for ~30 minutes in C57BL/6 mice. ......................................... 77
Figure 16. Insulin Clearance Indices prior to i.v. glucose infusion (basal glycemia) and after the
maintenance of hyperglycemia (clamp) for ~30 minutes in C57BL/6 mice.. ........................................ 78
Figure 17. Insulin Sensitivity Indices (M/I) obtained after the maintenance of hyperglycemia
(clamp) in C57BL/6 mice for ~30 minutes ............................................................................................ 79
Figure 18. The Disposition Indices obtained after the maintenance of hyperglycemia (clamp) in
C57BL/6 mice for ~30 minutes ............................................................................................................. 81
Figure 19. Plasma FFA levels of mice during basal glycemia (after 4 h of fasting and prior to
glucose infusion) and during hyperglycemia (after ~30 minutes at steady-state) ................................. 82
Figure 20. Western blots of CEACAM1 (Cc1) performed on livers of mice infused with SAL,
OLE, NMN+OLE, or NMN for 48h ...................................................................................................... 84

ix
List of Tables
Table 1. Summary of the seven mammalian sirtuins SIRT1-7 ....................................................... 40

1
Chapter 1: Introduction
1.1 Glucose Homeostasis
Glucose homeostasis is mainly regulated by the secretion of hormones from the islets of
Langerhans (hereinafter referred to as “islets”), which are sphere-like tissues that make up the
endocrine portion of the pancreas1,2. These islets were discovered in 1869 by Paul Langerhans in
Germany3. The islets contain hormone-secreting cells, which include alpha, beta, delta, epsilon,
and pancreatic polypeptide (PP) cells (Figure 1).
While the islets are crucial for glucose homeostasis, they only make up ~2% (1-2 g) of the
total pancreatic mass (60-100 g) in adult humans1,2. There is an estimated one million islets
scattered throughout the pancreas, together containing about one billion beta cells. In humans, the
islets consist of approximately 54.6% beta cells, 33.6% alpha cells, 12% delta cells, 1.6% PP
cells, and < 1% epsilon cells. The proportion of cells in islets is known to slightly vary between
different species1,2. In addition, islets are highly vascularized (10 - 15% of pancreatic blood flow)
and are innervated by sympathetic and parasympathetic nervous fibres. These allow the islets to
be quick and precise at regulating glucose homeostasis1,2.

2
Figure 1. Anatomy of the Islets of Langerhans in the Human Pancreas. Reprinted courtesy of
Encyclopaedia Britannica, Inc., copyright 2003; used with permission.
In response to elevated blood glucose levels, insulin is secreted from beta cells located in
the islets. Insulin travels through the blood stream and binds to insulin receptors, which are
located mainly on hepatocytes, skeletal myocytes, and white adipocytes2. Via an insulin-signaling
cascade, hepatocytes increase their uptake of glucose from the blood and decrease their output of
glucose via gluconeogenesis and glycogenolysis. In response to insulin, skeletal myocytes and
adipocytes increase their rate of glucose transport, resulting in increased glucose uptake2. Overall,
these effects result in decreased blood glucose levels.
In the case of hypoglycemia, glucagon is secreted from alpha cells, located in the islets.
Glucagon is transported in the blood and mainly binds to the glucagon receptors (GR) on
hepatocytes. Via a signaling cascade, this results in an increased output of glucose from the liver
to the blood via glycogenolysis and gluconeogenesis, consequently increasing circulating glucose
levels2.

3
As beta cells and alpha cells are crucial in glucose homeostasis, it is no surprise that they
comprise the majority of cells in the islets, at ~54.6% and ~33.6%, respectively. Delta cells
secrete the hormone somatostatin, which inhibits the secretion of both insulin and glucagon1. PP
cells and epsilon cells secrete the hormones pancreatic polypeptide, and ghrelin, respectively1.
1.2 Diabetes Mellitus
Diabetes mellitus, commonly known as “diabetes”, is characterized by chronically elevated
blood glucose levels due to insufficient insulin production in relation to the body’s need2.
Diabetes seems to have been first described in Egyptian manuscripts dating back to 1500 BC4.
The term “diabetes” is originally Greek for “siphon” or “to pass through”. It was probably coined
by Apollonius of Memphis approximately 250 BC. The word “mellitus” originates from Latin,
meaning “honey” or “sweet”. This term was added to form “diabetes mellitus” by the English
physician Thomas Willis in 16755. The disease was named as such because of the copious amount
of sweet urine produced from its afflicted individuals5,6.
According to the International Diabetes Federation, the global prevalence of diabetes is
estimated to be at least 415 million adults (~9% of adults)7,8. Diabetes has increased in incidence
by ~50% over the past decade. It is expected that, by 2040, the incidence of diabetes will have
risen to 642 million7–9. Although diabetes occurs worldwide, a majority of people with diabetes
live in developing countries. Furthermore, the number of cases of diabetes in developing countries
is increasing, and unfortunately, due to inferior healthcare systems, sufferers of diabetes tend to
have worse outcomes in developing countries, compared with developed countries10–12.
There are three main types of diabetes: type 1 diabetes mellitus, type 2 diabetes mellitus,
and gestational diabetes mellitus. Type 1 Diabetes Mellitus (T1DM) is a disease caused by the
autoimmune-mediated destruction of the insulin-producing beta cells in the pancreas. This

4
eventually results in the inability to produce insulin, causing hyperglycemia to ensue. Although
T1DM can occur at any age, it is typically manifested before the age of 30. As such, it is also
termed juvenile-onset diabetes. T1DM accounts for ~5-10% of all diabetes cases13.
Type 2 Diabetes Mellitus (T2DM) makes up ~85-90% of diabetes cases. T2DM occurs
mainly due to decreased insulin sensitivity (termed “insulin resistance”) in skeletal muscle, liver,
and adipose tissue, in combination with decreased beta cell function (the ability of beta cells to
secrete insulin). The decrease in insulin sensitivity is typically caused by relatively high levels of
free fatty acids (FFA; also called nonesterified fatty acids) and cytokines in plasma. This is
common in overweight and obese individuals, who happen to be ~90% of T2DM patients14. In
response to insulin resistance, beta cells increase their insulin secretion in order to maintain
normal glycemia1. This is termed compensatory hyperinsulinemia since insulin levels must be
elevated above normal levels.
Although hyperinsulinemia can prevent hyperglycemia in the context of moderate insulin
resistance, this does not remain the case after prolonged periods of high plasma FFA levels. This
is because prolonged periods of elevated FFA decrease beta cell function (termed “beta cell
dysfunction”), consequently impairing their ability to compensate for insulin resistance. When
compensation for insulin resistance is no longer sufficient, hyperglycemia ensues. The diagnostic
criteria for prediabetes are: 1) fasting plasma glucose (FPG) levels between 6.1 – 6.9 mmol/L; 2)
plasma glucose between 7.8 – 11.0 mmol/L two hours following a 75g oral glucose tolerance test
(OGTT); and 3) Hb A1c levels between 6.0% to 6.4%15. If hyperglycemia is above these
diagnostic criteria, it is termed T2DM. About one third of cases of prediabetes eventually
progress to T2DM16–18. In T2DM, approximately 4% of the capacity of the beta cell to secrete
insulin is decreased per year19.

5
The third type of diabetes is Gestational Diabetes Mellitus (GDM). Over the past 20 years,
the prevalence of GDM has increased by ~10-100% in several race/ethnicity groups in USA20,21.
GDM occurs to varied degrees in ~7-14% of pregnancies in USA, depending on demographics
and ethnicities21. It is characterized by hyperglycemia, which is caused by increased insulin
resistance during pregnancy, typically during the third trimester. Women who experience GDM
have an elevated risk of acquiring T2DM later in life21–23.
All three types of diabetes share hyperglycemia as an outcome. Accordingly, the most
common symptoms of diabetes are polyuria (frequent urination), polydipsia (frequent thirst), and
polyphagia (excessive hunger)13,14,21. Polyuria and polydipsia are caused by the excessive loss of
water and salts in the form of urine (due to the osmotic effect of glycosuria), and polyphagia is
caused by the calorie loss caused by glycosuria21.
1.3 Complications
Diabetes is associated with a variety of complications. Acute life-threatening complications
include coma, as a result of hypoglycemia (caused by an overdose of exogenous insulin), and
diabetic ketoacidosis (DKA), which occurs during severe hyperglycemia24.
Besides the potentially fatal acute complications, diabetes can have devastating and life-
threatening chronic complications. These typically involve blood vessels, which are damaged
over time by high blood glucose levels (angiopathy)24. Depending on the size of the vessels
damaged, angiopathy is categorized as “microvascular disease” (damaged small blood vessels) or
“macrovascular disease” (damaged arteries)24.
As blood vessels are vital to the function of all organs, angiopathy can result in a variety of
complications. For example, microvascular disease can result in damage to the retina of the eye
(retinopathy), possibly causing blindness after many years. In fact, diabetic retinopathy is the

6
leading cause of blindness among adults aged 20 – 74 years25,26. Diabetic retinopathy can include
capillary microaneurysms and/or degeneration (causing hypoxia, ischemia, and/or macular
edema), altered vascular permeability, and excessive blood vessel growth on the retina
(neovascularization-- which can cause retinal detachment or vitreal hemorrhage)25. Microvascular
disease can also result in kidney damage (nephropathy) and contribute to neural damage
(neuropathy) and limb amputations24.
Diabetic nephropathy can lead to end-stage renal failure. This often occurs gradually over a
period of 10 – 20 years27, and can result in fatal uremia if left untreated28. Furthermore,
nephropathy can amplify the risk for cardiovascular disease due to the resulting increase in
hypertension29, 30.
More than half of all people with diabetes will eventually develop a form of neuropathy31.
Diabetic neuropathy is a progressive disease known to affect the nervous system at both its
somatic and autonomic divisions, in particular the parasympathetic division24. As a result of
microvascular damage, blood flow to nerve fibers can be compromised. After prolonged periods,
hypoxia or ischemia would cause nerve fiber deterioration32. Far more common, however, is a
condition known as “metabolic neuropathy” whereby nerve cells slowly degenerate due to
hyperglycemia. Symptoms may vary depending on which nerves are damaged and the severity of
the damage. Typically, sensitivities to vibrations and/or thermal thresholds are significantly
reduced or lost. However, some individuals may suffer from paresthesia (tingling), hyperalgesia
(increased sensitivity to pain), and/or neuropathic pain32. The lack of pain can be very dangerous
as it places patients at a high risk of unknowingly injuring themselves. Combined with impaired
wound healing due to angiopathy and susceptibility to infection because of hyperglycemia,
neuropathy often leads to amputations24.

7
Due to the acceleration of atherosclerosis in T1DM and T2DM33, people with diabetes have
a six-fold increased risk for myocardial infarction (heart attack), compared with the general
population34. This risk is as high as that of an individual who has previously experienced a
myocardial infarction35. Cardiovascular disease, including myocardial infarction and stroke,
accounts for more than half of the mortality of diabetic populations35,36. Associated with diabetes
is myocardial dysfunction. However, the etiology of myocardial dysfunction is currently unclear
and controversial. It seems to occur independently of atherosclerosis and have a metabolic
causation24,37,38. Lastly, many of the previously mentioned complications tend to be reported as
the cause of death of many diabetic patients. This results in the under-reporting of the mortality of
diabetes per se.
1.4 Risk Factors
T1DM, T2DM, and GDM are caused by different mechanisms. As previously described,
T1DM is caused by the autoimmune-mediated destruction of the insulin-producing beta cells. On
the other hand, T2DM is mainly caused by insulin resistance and beta cell dysfunction, both
typically induced by high plasma levels of FFA. The mechanisms of GDM, though very unclear,
likely involve human placental lactogen39,40. As such, the risk factors for these main forms of
diabetes are different. According to the World Health Organization (WHO), a “risk factor” is
defined as “any attribute, characteristic, or exposure of an individual that increases the likelihood
of developing a disease or injury”41.
The risk factors for T1DM include family history, race, the expression patterns of T1DM-
associated genes (the most important of which are certain Human Leukocyte Antigens (HLA)),
and some viral infections42–45. There is currently no cure for T1DM; however, it can be relatively
well-managed mainly by insulin therapy (exogenous insulin injections due to lack of endogenous

8
insulin production), healthy diet, and exercise43. The risk factors for GDM include age, family
history of GDM, prediabetes, or T2DM, adiposity, and race. While there is also no cure for GDM,
patients tend to recover within weeks after the end of their pregnancy22,46,47. Management of
GDM is focused on the mother and child. It includes monitoring blood glucose levels and the
development of the child, adopting a healthy diet, exercise, and, in some cases, insulin therapy22.
The risk factors for T2DM are many. Similar to the other forms of diabetes, T2DM seems to
be caused by the combination of genetic susceptibility and environmental trigger(s). As such, the
risk factors for T2DM include: overweight/obesity; visceral adiposity (abdominal fat); a family
history of T2DM; inactivity; age; race; prediabetes; GDM; and polycystic ovary syndrome
(PCOS)48. PCOS is a common endocrine disorder among women, where the ovaries are enlarged
and contain small collections of fluid, and features insulin resistance49.
The major predisposing factor for T2DM is obesity, particularly the presence of a large
amount of visceral adipose tissue50–52. Obesity is clinically defined as having a body mass index
(BMI) of at least 30 kg/m2. Visceral adipose tissue has a significantly higher lipolytic activity
than subcutaneous adipose tissue does53. Consequently, visceral adipose tissue is a more potent
elevator of plasma FFA levels, which are the main inducers of insulin resistance and beta cell
dysfunction, compared with subcutaneous adipose tissue16,54–56.
Similar to the other forms of diabetes, there is currently no cure for T2DM. However,
T2DM can be reversible in many cases, particularly in cases caused by obesity57,58. T2DM is
usually reversed by weight loss. This can be achieved through a healthy diet and exercise57,58. In
some cases of severe obesity, bariatric surgery may be performed to induce long-term weight
loss59–64. Nevertheless, it should be noted that ~10% of patients with T2DM are not obese and
require treatments besides weight loss65.

9
Bariatric surgery is considered to be the most effective treatment for obesity59. It can be
performed by: 1) reducing the size of the stomach by using a gastric band; 2) dividing the
stomach into a small “pouch” and a larger part, then resecting and re-routing the small intestine to
the small “pouch” in order to bypass a large portion of the stomach (roux-en-Y gastric bypass); or
3) removing a portion of the stomach (sleeve gastrectomy)59–64. Roux-en-Y gastric bypass, which
is the most common form of bariatric surgery in the United States of America, has a T2DM-
reversal rate of 83%. Gastric band surgery confers a reversal rate of 62%64.
In the cases where weight loss fails to reverse fat-induced T2DM, weight loss remains
beneficial in that it improves insulin sensitivity and beta cell function61,62. This decreases the
severity of the patient’s T2DM, consequently improving blood glucose control. Building on that
point, weight loss, whether by healthy diet and exercise or by bariatric surgery, is a treatment for
T2DM. Other treatments include adopting a healthy diet, exercise (independent of weight loss),
insulin-sensitizing medication (such as metformin, which is the first-line antidiabetic medication,
and thiazolidinediones (TZDs)), insulin secretagogues (such as sulphonylureas and analogues),
incretin-based therapies (such as glucagon-like peptide-1 (GLP-1) and dipeptidyl peptidase-4
(DPP-4)-inhibitors), and insulin therapy in severe cases of T2DM66–68. Some advances in current
research of potential treatments for T2DM are described in the section “Potential Treatments for
Lipid-Induced Beta Cell Dysfunction”.
1.5 Epidemiology
As mentioned earlier, over 415 million adults, from both developed and developing
countries, suffer from diabetes7. In Canada, over 9 million people (~31% of the population) are
estimated to have diabetes or pre-diabetes (Canadian Diabetes Association (CDA), May 201569).
In 2012, over 29 million people in USA were estimated to have diabetes (~9% of the US

10
population)70. While these figures are already staggering, we must remember that the actual
prevalence of diabetes is probably greater than estimated due to the numerous cases of diabetes
that go undiagnosed71–73. Lastly, the incidence of diabetes, especially T2DM, has been increasing
dramatically and steadily over the past decades. As stated previously, it is expected that the
number of adults with diabetes worldwide will have will have risen to 642 million (an increase of
over 50%) by 20407.
Since obesity is the major risk factor for T2DM, it is not surprising that the incidence of
T2DM has been following the substantial increase in incidence of obesity65. Besides the obvious
negative effects of T2DM on health, this rise in prevalence of T2DM will put huge strains on
healthcare systems and economies. T2DM already costs the Canadian healthcare system ~$13
billion annually; however, this is expected to rise to ~$17 billion by 2020 (CDA, December
200974). This is due to the high cost of treating chronic diseases, including the expenses for
hospitals, drugs, and treatments for T2DM-associated complications, such as amputations. In
addition, T2DM can cause personal disability, potentially weakening the workforce and economy.
Thus, T2DM is significantly increasing in prevalence and represents a serious and considerable
threat to the health and economies of Canada and the rest of the world. As such, it must be
researched vigorously in order to arrive at potential ways of preventing and treating T2DM with
reliable effectiveness.
1.6 Insulin Secretion
Insulin is a peptide hormone consisting of two polypeptide chains: the A- and B-chains,
which are linked by disulfide bonds75. It is produced and secreted by beta cells in response to
elevated blood glucose levels. Insulin is secreted in a biphasic pattern consisting of an acute
(lasting ~10 min) and prolonged secretion of insulin76. Insulin that had already been synthesized

11
is stored in large dense core vesicles (LDCV; termed secretory granules) near the membrane in
the beta cells. When glucose enters the beta cell via the glucose transporters GLUT1 (in
humans77,78) and GLUT2, it is metabolized, ultimately causing a signaling cascade which induces
the exocytosis of the insulin granules79,80,77,81. This is the acute phase of insulin secretion, which
responds quickly to increases in glycemia76.
In detail, the mechanism by which glucose metabolism induces insulin secretion is as
follows (Figure 2): after entering the beta cell, glucose is metabolized to produce adenosine
triphosphate (ATP) via glycolysis and the tricarboxylic acid (TCA) cycle. The rise in cellular
ATP levels causes the closure of KATP channels, which results in the build-up of K+ and
depolarization of the cell membrane. This depolarization causes voltage-dependent Ca2+ channels
(VDCC) to open, allowing an influx of Ca2+ into the beta cell. The rise in cytosolic Ca2+ levels
then induces the exocytosis of insulin granules76. While glucose is the primary stimulant of
insulin secretion, insulin secretion can also be induced by other means. These include a number of
amino acids, acetylcholine (secreted by the peripheral nervous system), gastric inhibitory
polypeptide (GIP), and glucagon-like peptide (GLP), the latter two being incretin hormones
secreted by the gut following food ingestion82.
Acetylcholine binds to the M3 muscarinic acetylcholine receptor, and GIP and GLP bind to
the gastric inhibitory polypeptide receptor (GIP-R) and glucagon-like peptide 1 receptor
(GLP1R), respectively. The M3 muscarinic acetylcholine receptor, GIP-R, and GLP1R, the three
of which are expressed on beta cells, enhance insulin secretion82,83. Interestingly, FFAs, such as
oleate, have specific receptors on a wide variety of cells in the body, including beta cells. These
receptors, known as Free Fatty Acid Receptors (FFARs), are G-protein-coupled receptors
(GPCRs) which act as signaling molecules in many physiological processes related to energy
metabolism84–87. FFARs are classified according to the chain-length of their FFA ligands. With

12
regards to FFARs found on beta cells, medium- and long-chain FFAs, such as oleate, are known
to activate G-protein-coupled receptor 40 (GPR40), whereas short-chain FFAs activate GPR41
and GPR4385,88. Derivatives of FFAs have a specific FFAR on beta cells, namely GPR11989.
GPR40 and GPR119 have positive effects on insulin secretion, and thus may explain the acute
stimulatory effect of FFAs on insulin secretion84,87,89. Although the roles of GPR41 and GPR43 in
beta cells are at present not completely clarified, GPR41 appears to be mainly inhibitory and
GPR43 appears to be mainly stimulatory90.
Figure 2. Summary of the mechanism of glucose-stimulated insulin secretion (GSIS) in the beta cell.
Glucose enters the cell via GLUT2 transporters. Glucose is then metabolized via glycolysis and the
tricarboxylic acid (TCA) cycle, resulting in the production of ATP. The rise in intracellular ATP levels
results in the closure of KATP channels, which leads to the depolarization of the cell membrane. This
depolarization then stimulates voltage-dependent Ca2+ channels (VDCC), resulting in an influx of Ca2+ into
the cytosol. The increase in intracellular Ca+ concentration induces the exocytosis of insulin secretory
granules located at the membrane. Figure adapted from Desai T., M.Sc. Thesis, Dept. of Physiology,
University of Toronto, 2013.
Once the store of insulin granules is secreted, the beta cells must synthesize and secrete
additional insulin. This is a relatively slow process which is rate-limited by the synthesis of

13
insulin91. This is the second phase of insulin secretion. Insulin is first translated in the form of a
single polypeptide termed preproinsulin. Preproinsulin contains a 24-residue signal peptide that
directs the polypeptide to the rough endoplasmic reticulum (RER). In the RER, preproinsulin is
cleaved to form proinsulin, which is then folded into the correct conformation. This includes the
formation of disulfide bonds. Subsequently, proinsulin is transported to the Trans-Golgi Network
(TGN), where it is cleaved by Proprotein Convertase (PC) 1 and 2 to release the two chains of
insulin along with C-peptide. At this point, insulin and C-peptide are ready to be secreted from
the beta cells upon proper stimulation91. As C-peptide is always co-secreted with insulin, the
concentration of C-peptide in plasma is correlated with that of insulin. As such, it is often
assessed as an index of insulin secretion92–95.
The autocrine effects of insulin on beta cells have been a controversial topic for over a
decade96,97. Although insulin signaling in beta cells was first suggested to negatively regulate
insulin secretion98–100, recent evidence depicts a positive effect on insulin transcription,
translation, and secretion, as well as beta cell survival101–104.
1.7 Insulin Clearance
While insulin action is vital for glucose homeostasis, excess insulin action can result in
hypoglycemia and possibly death. As such, besides regulating the secretion of insulin, the body
modulates insulin levels by removing insulin from the blood plasma. This is termed insulin
clearance. It is mainly performed by the liver and to a lesser extent by the kidneys105.
While increases in insulin secretion elevate circulating insulin levels, decreases in insulin
clearance can also produce this effect106. This is evident in certain liver diseases where impaired
insulin clearance results in hyperinsulinemia, which, after chronic periods, can induce peripheral
insulin resistance107. Insulin resistance can be induced by chronic hyperinsulinemia via the

14
downregulation of insulin receptors in the cell membrane as a result of the internalization of the
insulin-insulin receptor complex as well as the impairment of synthesis of the insulin receptor.
Hence, insulin clearance plays an important role in the regulation of insulin action and, in turn,
glucose homeostasis108.
Insulin clearance occurs through receptor-mediated insulin endocytosis followed by
degradation108–110. Approximately 50% of circulating insulin is removed during its first passage
through the liver111. This takes place via the endocytosis and degradation of the insulin-insulin
receptor complex in hepatocytes. While insulin clearance mainly occurs via the liver, insulin in
the systemic circulation is removed to a significant extent by the kidneys.
The insulin clearance rate by the liver is known to be proportional to portal insulin
concentrations112,113 and inversely proportional to portal FFA concentrations in rats114–116.
Elevated levels of plasma FFA are well-known to decrease insulin clearance114–117. FFAs are
known to impair insulin clearance at two main levels. First, by inducing hepatic insulin resistance,
insulin signaling is decreased, resulting in decreased activation of carcinoembryonic antigen-
related cell adhesion molecule 1 (CEACAM1; formerly known as pp120) by the insulin-insulin
receptor complex activity118. CEACAM1 is a transmembrane glycoprotein that is responsible for
the endocytosis of the insulin-insulin receptor complex (described below)118–120. Second, as
insulin action is known to increase CEACAM1 transcription, decreased insulin signaling may
reduce CEACAM1 levels121. In addition, FFAs taken up by the liver are mainly esterified to form
triglycerides. Afterwards, this pool of triglycerides is used in several metabolic processes,
including fatty acid oxidation122. Hepatic triglyceride levels have been shown to be inversely
proportional to insulin clearance123.

15
1.7.1 Mechanisms of Insulin Clearance
Hepatic insulin clearance occurs via the internalization of the insulin-insulin receptor
complex, which is mediated by the tyrosine autophosphorylation of the insulin receptor upon
insulin binding. The tyrosine-phosphorylated insulin receptor subsequently phosphorylates
CEACAM1124,125. Via clathrin-coated pits, the insulin-insulin receptor complex is internalized
into a clathrin-coated vesicle and subsequently an endosome. Insulin degradation begins in the
acidic environment of the endosome by the action of Insulin Degrading Enzyme (IDE; also
known as insulysin). The endosome is then processed into the late endosome where insulin is
further degraded. Eventually, the late endosome returns to the plasma membrane by diacytosis in
order to recycle the insulin receptor and exocytose the degradation products of insulin126.
Alternatively, the late endosome may transition to a lysosome, where insulin and the insulin
receptor are both degraded127. A basic illustration of the process of insulin clearance by the
hepatocyte is summarized below in Figure 3.

16
Figure 3. Summary of the process of insulin clearance in the hepatocyte. After insulin binds
to the insulin receptor, it triggers the tyrosine autophosphorylation of the insulin receptor. The
insulin receptor, in turn, tyrosine phosphorylates carcinoembryonic antigen-related cell adhesion
molecule-1 (CEACAM1; also known as pp120), resulting in its activation. CEACAM1 then
induces the internalization of the insulin-insulin receptor complex into an endosome. In the acidic
endosome, IDE begins degrading insulin. The endosome is then processed into a lysosome, where
insulin and the insulin receptor are completely degraded. Alternatively, the late endosome fuses
with the plasma membrane, resulting in the recycling of the insulin receptor and the exocytosis of
the degradation products of insulin. Figure modified from Duckworth W.C. et al. 1998. Endocr
Rev. 19(5), 608–624.
In kidneys, insulin clearance occurs via two mechanisms: 1) glomerular filtration followed
by proximal tubular reabsorption and degradation, and 2) diffusion of insulin from peritubular
capillaries followed by the binding of insulin to contraluminal membranes of tubular cells and the
endocytosis of insulin128–131. Glomerular filtration of insulin occurs by nonspecific diffusion and
by specific-receptor-mediated transport. More than 99% of insulin that enters the renal tubule is
reabsorbed by proximal tubule cells, mainly via endocytosis132. Hence, almost no insulin is
excreted in the urine of healthy individuals. However, insulin that is endocytosed by the proximal
tubule cells is processed for degradation in a manner similar to that in the hepatocyte, which is
described above129. Nevertheless, while insulin in the proximal tubule cell proceeds through the

17
endosomal complex, it is transferred to lysosomes much earlier than in hepatocytes128. In
addition, some insulin is released intact into the circulation via retroendocytosis131.
CEACAM1 was originally discovered as a substrate of the insulin receptor tyrosine kinase
in rat hepatocytes124. While CEACAM1 protein is ubiquitously produced, it is predominantly
expressed in the liver and has limited expression in skeletal muscle and white adipose tissue
(WAT)108,133. CEACAM2, a less expressed isoform of CEACAM1, plays a role in the regulation
of metabolic rate and insulin sensitivity and is mainly expressed in the brain, spleen, kidneys, and
testes134,135. CEACAM2 is not expressed in peripheral insulin-targeted tissues, such as the liver,
skeletal muscles, and WAT134,135. In addition, only CEACAM1 is expressed in humans and
rats134. Although CEACAM1 is significantly expressed in beta cells, CEACAM1-null mice
exhibited normal beta cell area and insulin secretion in response to glucose in vivo and in isolated
islets111.
CEACAM1 is known to be highly conserved among different species108. It has been
suggested that tyrosine-phosphorylated CEACAM1 reduces the mitogenic effects of insulin by
binding with Shc, which is another substrate of the insulin receptor. This results in the
sequestration of Shc, preventing it from coupling Grb2 to the insulin receptor and thus results in
the downregulation of the Ras/MAP kinase mitogenesis pathway136,137. In addition, CEACAM1 is
known to act as a cell adhesion molecule, mediating Ca2+-dependent and Ca2+-independent cell
adhesion138. CEACAM1 has also been reported to suppress tumor growth139 and to mediate
angiogenesis140. Phosphorylation of CEACAM1 is necessary for its activation, with the exception
of its role in cell adhesion16,141–143.
IDE is a highly conserved Zn2+-dependent endopeptidase that plays a key role in the
degradation of insulin in endosomes144,145. IDE was first described as “insulinase” by Mirsky and
Broh-Kahn in 1949146. The expression of IDE is highest in the cytosol followed by the

18
peroxisomes of cells144,147–149. Yet, in regards to concentration, one study, using immunoelectron
microscopy, reports that IDE is ~3.5 times more concentrated in peroxisomes than it is in the
cytosol of rat hepatocytes (due to the relatively large volume of the cytosol), suggesting that
peroxisomes contain 10-20% of total IDE147. However, the precise difference of IDE
concentration between the two subcellular compartments is unclear because, using immunoblot
analysis, the same study found similar concentrations of IDE in the peroxisomal and cytosolic
fractions147. This difference may have been in part due to leakage of protein from the fragile
peroxisomes during homogenization147,150.
Overexpression of IDE has been shown to increase the rate of insulin degradation by cells,
supporting the significance of IDE in insulin degradation151. However, while IDE is important for
insulin proteolysis, a 2015 study published in the Journal of Biological Chemistry suggests that
IDE may not be necessary for the clearance of insulin from blood plasma152. Utilizing novel IDE
inhibitors which do not bind with IDE’s catalytic Zn domain (and hence do not need to compete
with IDE’s substrates), the authors of this study performed insulin tolerance tests and euglycemic
clamps on High Fat Diet (HFD)-fed obese mice152. The authors found that plasma insulin levels
and insulin action were not significantly altered, compared with control mice in vivo.
It is possible that insulin clearance during inhibited IDE activity was not affected because of
the internalization of insulin by CEACAM1, which effectively removes insulin from the blood
plasma even if the downstream IDE action is impaired. Alternatively, it is possible that, in the
HFD model, insulin clearance was already impaired by the elevated plasma FFA levels. A study
by the lab of Dr. Malcolm A. Leissring (University of California, Irvine) reported that whole-
body IDE-null mice exhibited ~3-fold higher fasting levels of insulin in plasma and improved
glycemic control at 2 months of age, compared with wildtype mice; however, at 6 months of age,
IDE-null mice exhibited severe insulin resistance and glucose intolerance due to their chronic

19
exposure to extremely high plasma levels of insulin (caused by the complete genetic deletion of
IDE)153.
Unpublished data from Dr. Leissring’s lab show that liver-specific IDE-KO mice do not
exhibit a significant difference in insulin clearance, compared with wildtype mice. This may have
been due to a compensatory increase in insulin clearance by the kidneys or due to the extent of
IDE knockout in the liver. Thus, the magnitude of the effect of IDE on insulin clearance is
currently controversial.
In addition to degrading insulin, studies based on pharmacological inhibition of IDE show
that IDE degrades amylin (also known as islet amyloid polypeptide)154–157. Amylin is a 37-residue
peptide hormone that is co-secreted with insulin by beta cells. Pharmacological levels of amylin
help suppress glucagon secretion, delay gastric emptying, and induce satiety158–160. Physiological
levels of amylin have been shown to contribute to the regulation of glucagon release and gastric
emptying161–164.
In conclusion, insulin clearance is an important process in the regulation of the levels and
action of insulin in the body. It occurs mainly by the liver and kidneys, primarily by CEACAM1-
mediated endocytosis followed by degradation in peroxisomes by the action of IDE.
1.8 Fat-Induced Beta Cell Dysfunction
Many studies have shown that acute exposure of beta cells to elevated FFA levels results in
increased glucose and non-glucose-stimulated insulin secretion in vitro165,166 and in vivo in
animals167 and humans168–171. The responsible mechanisms (which include the interactions of
FFAs with FFARs) have been extensively reviewed84,86,87,89,172,173. In contrast, prolonged
exposure of beta cells to elevated FFA levels impairs glucose-stimulated insulin secretion (GSIS)
in vitro. There are comprehensive reviews outlining the molecular mechanisms of fat-induced

20
beta cell dysfunction172,173. In vivo studies assessing absolute GSIS after prolonged i.v. infusion of
fat showed inconsistent results, namely increased174,175, unchanged168,176–184, or decreased170,185
absolute GSIS in humans and rats.
There are several explanations for the differences observed in these in vivo studies. First, the
assessment of absolute GSIS does not account for insulin resistance induced by elevated plasma
levels of FFA. Second, the compositions of triglyceride or fatty acid infusates administered in
each study were not necessarily similar. Third, a number of human studies have demonstrated that
genetic predispositions to diabetes greatly influence the effect of FFA on beta cell function. The
detrimental effects of FFA on beta cell function and/or viability fall under the category of beta
cell lipotoxicity186–188. In addition, chronic hyperglycemia is also known to cause beta cell
dysfunction. This is termed glucotoxicity189–191.
1.8.1 Methods of Assessing FFA-Induced Beta Cell Dysfunction
As explained earlier, beta cells increase insulin secretion during insulin resistance
(compensatory hyperinsulinemia) in order to maintain proper glucose homeostasis1. As insulin
sensitivity decreases, insulin secretion increases, and as insulin sensitivity increases, lower plasma
levels of insulin are required, resulting in decreased insulin secretion. Since chronically high FFA
levels induce insulin resistance as well as beta cell dysfunction, absolute GSIS is not a reliable
assessment of beta cell function. This is because compensatory hyperinsulinemia induced in
response to insulin resistance could mask a decrease in beta cell function.
As the relationship between insulin secretion and insulin sensitivity is hyperbolic, their
product is a constant. This constant, first published by Toffolo G., Bergman R.N., and Cobelli C.
in Diabetes192, is termed the Disposition Index (DI; Figure 4). The DI is the current reliable index
of beta cell function in vivo193. This is because the DI expresses beta cell function while
controlling for potential changes in insulin sensitivity.

21
Figure 4. The Disposition Index (DI) is the product constant of insulin secretion and insulin
sensitivity. The arrow depicts a decrease in the DI as beta cell function is decreased. This is demonstrated
by the fact that for the same insulin sensitivity, insulin secretion is decreased. Figure modified from
Stumvoll M. et al.194.
In all of Dr. Giacca’s collaborative studies on humans, aside from one185, 48-h intravenous
fat infusions did not affect absolute GSIS. However, lipid infusions for 16- to 48-h impaired DI,
indicating that the ability of beta cells to compensate for insulin resistance had been
diminished168,176,177,180,181,183–185. During hyperglycemic clamp studies, these collaborative studies
found that the glucose infusion rate (GINF) required for maintaining hyperglycemia (an index of
glucose tolerance) was lower in humans infused with lipids for 48h, compared with saline
controls. In another study, a graded i.v. glucose infusion, rather than a hyperglycemic clamp, was
performed following prolonged fat infusion. This resulted in slightly elevated blood glucose
levels, further demonstrating that prolonged fat infusion causes beta cell dysfunction16. Beta cell
dysfunction usually increases in severity with the duration that beta cells are exposed to high
levels of FFA187. After very long periods of beta cell lipotoxicity, such as high-fat feeding in
rodents or T2DM, beta cell death via apoptosis can occur195,196.
In summary, acute elevation of plasma FFA levels results in increased beta cell function,
whereas chronic elevation of plasma FFA levels results in decreased beta cell function. If beta cell

22
dysfunction is severe enough to prevent insulin secretion from compensating for FFA-induced
insulin resistance, T2DM would manifest.
1.8.2 Effects of Different Lipid Treatments on Beta Cell Dysfunction
Several FFA and lipids are used to model FFA-induced beta cell dysfunction. In humans
and rodents, the two most abundant fatty acids present in blood plasma are oleate and
palmitate197. Oleate is a monounsaturated fatty acid (MUFA) whereas palmitate is a saturated
fatty acid (SFA). Compared with non-obese individuals, obese individuals have 1.5 – 2 fold
greater levels of both fatty acids and a higher ratio of SFA to MUFA198,199. The chronic elevation
of either of those fatty acids has been shown to result in beta cell
dysfunction168,176,177,180,181,183,185,200.
Our studies suggest that the in vivo elevation of MUFA in rats is most effective in causing
beta cell dysfunction, compared with SFA and polyunsaturated fatty acid (PUFA) infusion201,202.
There is currently no convincing evidence that this is true in humans203.
Models of FFA-induced beta cell dysfunction have included the elevation of oleate and/or
palmitate plasma levels in animals in vivo. This is often done by i.v. infusion of albumin-bound
oleate, as has been done in a number of our studies56,201,204,205. This is not feasible with palmitate
due to its toxicity and low solubility. More recently, it has been possible to non-toxically elevate
plasma palmitate concentrations in vivo. This method consists of i.v. infusing ethyl palmitate
instead of palmitate200. The ethyl moiety which is esterified to the carboxylic end of the fatty acid
abolishes the fatty acid’s detergent action, and thus its toxicity. Plasma esterase present in the
blood plasma act on ethyl palmitate to release palmitate and ethanol into the circulation.
Another method of elevating plasma FFA levels is by i.v. infusion of a fat emulsion with
heparin. Conventional fat emulsions that can be infused in humans include Intralipid and Liposyn,

23
which mainly contain unsaturated triglycerides206–208. Heparin is co-infused in order to release
lipoprotein lipase (LPL) into the blood stream in order to hydrolyze the triglycerides into FFA.
A third common model of FFA-induced beta cell dysfunction is the chronic administration
of a HFD (typically > 45% of energy by fat) to rodents, as opposed to a standard diet (typically <
20% fat209–211. Although this model of diet-induced obesity is common and convenient, it has
several limitations. A HFD model is non-selective in regards to circulating FFA and involves the
expansion of cytokine-releasing adipose tissue and the secretion of gut hormones, both of which
affect glucose metabolism82.
Lastly, numerous studies have assessed beta cell function in vitro by exposing beta cell
models or isolated islets to cell culture media containing specific fatty acids205,212–217. Fatty acids,
such as oleate or palmitate, are complexed with Bovine Serum Albumin (BSA) in the culture
media in order to simulate in vivo conditions and to prevent the toxic effect of excess unbound
FFA. These in vitro models facilitate mechanistic studies.
1.8.3 Genetic Predisposition to Lipid-Induced Beta Cell Dysfunction
A study found that having a positive family history of T2DM was correlated with increased
susceptibility to lipid-induced beta cell dysfunction218. This was also found to be the case for
glucose-intolerant first-degree relatives of patients with T2DM182.
A collaborative study by our lab examined genetic susceptibility to lipid-induced beta cell
dysfunction in the Sandy Lake Oji-Cree community of Ontario, Canada176, which has the third
highest prevalence of T2DM in the world219. Counter-intuitively, our lab found that nondiabetic
subjects with a family history of T2DM experienced a lower decrease in beta cell function
following a 2-day lipid infusion, compared with non-Oji-Cree subjects. This was assessed using
the DI. Although the Oji-Cree subjects exhibited a lower decrease in beta cell function, their
overall beta cell function was less than that of non-Oji-Cree subjects. Thus, Oji-Cree subjects

24
seemed to have had impaired beta cell function prior to the infusion of lipid. Some of the
genetically susceptible individuals may normally have relatively high plasma levels of FFA, as
decreasing FFA levels improved insulin secretion in the Oji-Cree population220–222.
Further collaborative work by our lab demonstrated that Caucasians with a family history of
T2DM tend to have higher levels of FFA during i.v. Intralipid + Heparin (IH) infusion due to
enhanced FFA spillover into the plasma223. Physiologically, triglycerides infused into blood
plasma are broken down by LPL primarily in the capillaries of muscles and adipose tissue,
releasing FFA and glycerol224. The released FFA are normally taken up and esterified
immediately within the organs, resulting in very little amounts of FFA remaining in the plasma. In
conditions where FFA esterification is impaired, plasma FFA levels are elevated above
physiological levels. This is termed spillover225. FFA spillover is considered a measure of
inefficiency in dietary fat storage.
Given the recent discovery of many genetic variants associated with T2DM226, it may be
worth investigating which genetic variants increase susceptibility to lipotoxicity. For instance, it
has been shown that some genetic variants of the KATP channel increase susceptibility to T2DM
by having a greater sensitivity to opening in response to FFA in vitro227. The opening of the KATP
channel allows K+ to flow out of the beta cell, causing a shift towards hyperpolarization of the cell
membrane. This increases the barrier that must be overcome for the cell membrane to depolarize
and induce insulin secretion227.
1.8.4 Beta Cell Replenishment
Beta cell populations are mainly regulated by cell proliferation and cell death. In adult
humans, the rate of proliferation of beta cells is very low228,142. Beta cells arise from pre-existing
beta cells, pancreatic cells, and extra-pancreatic cells. In rodents, the main source of new beta
cells seems to be replication from pre-existing beta cells. Secondary sources of new beta cells in

25
rodents are pancreatic cells (mainly duct cells), whereas extra-pancreatic cells including
stem/progenitor cells, although capable of generating beta cells, do not normally contribute to
beta cell replenishment. In humans, beta cells appear to mainly originate from non-beta cells in
the pancreatic duct due to limited beta cell replication, particularly in adulthood229.
In metabolic states of increased insulin demand, beta cells may adapt by increasing in size
and/or number1. However, after chronic periods of T2DM, beta cell mass is decreased, further
exacerbating hyperglycemia. Beta cell mass is reduced mainly through apoptosis, although
necrosis, autophagy, and ferroptosis may also cause cell death1.
The discovery that lipid-induced apoptosis occurs in vivo is important since in vitro
experiments involving beta cell incubation in media containing albumin-bound FFA can simulate
in vivo FFA effects to a limited extent. This is because beta cell death in vitro may be due to the
toxic effect of excess unbound fatty acids, which does not occur in vivo. Fatty acids released from
adipose tissues are immediately buffered by the great amount of albumin in plasma.
1.8.5 Effect of FFAs on Beta Cell Mass
Although a 16-20 week HFD diet administration has been shown to increase insulin
resistance and absolute GSIS in rodents230,231, a chronic HFD ultimately results in glucose
intolerance. The increased GSIS is attributed to increased beta cell function and/or mass230,231.
Nevertheless, the final outcome of glucose intolerance demonstrates the failure of beta cells to
compensate for insulin resistance following a chronic HFD.
Fat-induced beta cell failure is typically due to beta cell dysfunction and/or beta cell
death231,232. Beta cell dysfunction typically precedes the decrease in beta cell mass174,233. This
decrease in beta cell mass tends to occur because of beta cell apoptosis230,231,234–237 and beta cell
senescence237. Thus, although absolute GSIS and beta cell mass are increased after a chronic

26
HFD, the effects of lipotoxicity on beta cells result in beta cell failure. Consequently, glucose
intolerance ensues.
1.9 Glucotoxicity and Glucolipotoxicity
In addition to having elevated plasma levels of FFA, individuals with prediabetes or T2DM
have high levels of blood glucose. Chronic hyperglycemia is known to lead to beta cell
dysfunction through a process termed glucotoxicity190,238. A recent study in our lab suggests that
high-glucose-induced beta cell dysfunction in vivo mainly occurs through oxidative stress,
endoplasmic reticulum (ER) stress, and the stress-activated enzyme c-Jun-N-terminal kinase
(JNK)239. This study utilized a pharmacological model and a genetic model: 1) inhibition of JNK
by administering SP600125 to rats, and 2) JNK1-null mice i.v. infused with glucose or saline.
SP600125 protected against high-glucose-induced beta cell dysfunction without significantly
decreasing total and mitochondrial superoxide levels. The administration of the antioxidant
tempol with the chemical chaperone sodium phenylbutyrate (which reduces ER stress) prevented
the activation of JNK by high glucose.
There are many studies, including one done by our lab240, which implicate oxidative stress
in high-glucose-induced beta cell dysfunction both in vitro241–244 and in vivo240,245,246. According
to one study, high-glucose-induced beta cell dysfunction stems from decreased insulin gene
expression caused by a defect in the mRNA maturation of pancreas duodenum homeobox-1 (Pdx-
1), which is an important insulin transcription factor238. The study discovered an absence of Pdx-1
in glucotoxic beta cells, and demonstrated an increase in insulin promoter activity after Pdx-1
transfection into glucotoxic beta cells238.
The combined toxicity of elevated plasma fatty acid and glucose levels on beta cells is
termed glucolipotoxicity. Glucolipotoxicity has been demonstrated in many in vitro studies and is

27
thought to be more detrimental to beta cell function than lipotoxicity and glucotoxicity are
alone247,248. Glucolipotoxicity has been extensively documented in vitro173; however, in vivo
studies of glucolipotoxicity are far less common.
In one in vivo study, 48h i.v. co-infusion of Intralipid + Heparin (IH) and glucose in
dexamethasone-treated rats induced greater beta cell dysfunction than when IH or glucose were
each infused alone248. In another study, the co-infusion of IH and glucose in normal rats resulted
in a synergistic effect, i.e., a significant decrease in insulin gene transcription which was not
observed after infusion of IH or glucose alone249. This supports the theory that glucolipotoxicity
tends to be a more potent cause of beta cell dysfunction, compared with glucotoxicity or
lipotoxicity.
In humans, prolonged hyperglycemia has been shown to result in beta cell dysfunction250.
However, experimentally inducing prolonged hyperglycemia is usually not performed on humans
due to inflammation of the i.v. site, swelling, nausea, and electrolyte imbalance. Nevertheless,
there have been a few studies investigating glucolipotoxicity in humans. In a collaborative study
by our lab, IH was co-infused with glucose (achieving 7.5 mM glycemia) in humans for 24h180.
Although this resulted in beta cell dysfunction, its severity was not greater than that induced by
IH infusion alone. Thus, this did not manifest the effects of true glucolipotoxicity. Interestingly,
the 24h infusion of glucose alone (achieving 7.5 mM glycemia) enhanced beta cell function.
However, it is important to note that 7.5 mM glycemia is a mild elevation of blood glucose, and
that a greater degree of hyperglycemia, when prolonged, is known to cause beta cell
dysfunction251,252,190.
In summary, although glucolipotoxicity has been clearly demonstrated in vitro173 and in
animal models in vivo249, it has not been sufficiently demonstrated in humans likely due to the
limitations in experimentally elevating glycemia.

28
1.10 Mechanisms of FFA-Induced Beta Cell
Dysfunction
FFA-induced beta cell dysfunction has been widely studied in vitro; however, it has been
far less studied in vivo173. As a result, many of the mechanisms discovered in in vitro studies have
not been tested in vivo, especially in humans. Mechanisms for beta cell dysfunction and death
which are supported by in vitro and in vivo studies include FFA-induced oxidative stress177,212,253,
ER stress184, and inflammation230,254,255.
1.10.1 The Role of Oxidative Stress
In beta cells, Reactive Oxygen Species (ROS) are mainly produced in mitochondria via
the oxidation of glucose and, to a lesser extent, via oxidation of FFA. More specifically, ROS are
produced downstream of glucose and fatty acid oxidation as a product of the electron transport
chain (ETC). This form of ROS is mainly superoxide (O2•-)256,257. FFA lead to increased ROS
production by directly disrupting the mitochondrial membrane composition, resulting in
decreased efficiency of oxidative phosphorylation and an increase in ROS production258.
In addition, oxidation of FFA in the peroxisome plays a role in ROS production via the
generation of H2O2256. While mitochondria primarily oxidize small- to long-chain fatty acids,
peroxisomes tend to oxidize very long-chain fatty acids187,256. High levels of plasma FFA are
known to induce the shifting of the energy pathway towards the oxidation of FFA and away from
glucose oxidation and glycolysis259.
Recently, ROS has been shown to be produced in beta cells via plasma membrane
Nicotinamide Adenine Dinucleotide Phosphate (NADPH) oxidase187,260. NADPH oxidase is a
membrane-bound enzyme complex that is found on the plasma membrane and on membranes of
phagosomes in neutrophils. It is responsible for the generation of superoxide during phagocytosis
of microorganisms187. A study done by our lab demonstrated that NADPH-oxidase-derived

29
cytosolic superoxide is increased following 48h of oleate i.v. infusion in mice56. This study also
made the valuable finding that pharmacological and genetic whole-body inhibition of NADPH
oxidase decreases superoxide levels and prevents oleate-induced beta cell dysfunction. In
addition, studies have shown increased concentrations of components of NADPH oxidase in islets
of animal models of T2DM126 and in beta cell lines treated with palmitate for 24h261. As NADPH
oxidase is activated by elevated levels of Protein Kinase C (PKC), cytokines, and increased
activity of toll-like receptor-4 (TLR-4; which is activated by saturated FFA200,262), NADPH
oxidase can be a significant source of ROS production in beta cells exposed to high levels of
FFA56,263.
Oxidative stress is defined as an elevation in levels of intracellular ROS to a level that
begins to cause damage to the cell242,264,265. This typically occurs when the production of ROS is
beyond the cell’s ability to decrease ROS levels. Being highly reactive, ROS can cause damage to
DNA, enzymes, and membranes in cells, resulting in dysfunction of the cells, and in some cases,
cell death266. Patients with T2DM have been shown to exhibit 5-fold higher levels of markers of
ROS in their beta cells, compared with healthy controls267. Markers of oxidative stress include
malondialdehyde (MDA) and 8-hydroxy-2'-deoxyguanosine (8-OHdG), which are indicators of
lipid peroxidation and oxidative DNA damage, respectively268.
Beta cells are particularly susceptible to dysfunction via oxidative stress. Normally, cells
use antioxidants in order to control their levels of ROS. These include manganese superoxide
dismutase (MnSOD), glutathione, and catalase, to name a few257. However, beta cells have
significantly lower levels of antioxidants, compared with most cells, and are therefore very
susceptible to damage caused by increased ROS141,269.
Since beta cells have a limited capacity to store triglycerides189,143,188, exposure to high
levels of FFA tends to result in the metabolism of excess FFA in beta cells including their

30
conversion into toxic FFA esterification products, such as diacylglycerol (DAG) and ceramides.
This leads to increased ROS production188. As the very low rate of beta cell proliferation renders
beta cells susceptible to significant loss of beta cell mass, chronic oxidative stress could lead to
the inability of beta cells to compensate for insulin resistance, thus resulting in T2DM. Overall, it
is clear that the intrinsic physiology of beta cells renders them very vulnerable to FFA-induced
oxidative stress.
In beta cells, oxidative stress has been consistently shown to be causal in beta cell
dysfunction, which is the impairment of the ability of the beta cell to synthesize or secrete
insulin242,264,265. In collaboration with Dr. Michael B. Wheeler’s lab, our studies have shown that
the antioxidant taurine protects GSIS of both rat islets and MIN6 beta cells exposed to FFA for
48h270. Our lab found that the antioxidants N-acetylcysteine (NAC), taurine, and tempol
prevented beta cell dysfunction in oleate-infused rats in vivo, in vitro, and ex vivo212. The in vivo
assessments of beta cell function utilized hyperglycemic clamps, whereas the ex vivo experiments
measured insulin secretion from isolated islets of i.v. infused rats. Our lab’s results are consistent
with another study, which showed that NAC administration prevented beta cell dysfunction in rats
infused with IH over 96h253.
As mentioned earlier, inhibition of NADPH oxidase with apocynin as well as its deletion
in NADPH oxidase-null mice prevented oleate-induced beta cell dysfunction56. In addition, a
recent study in our lab has shown that elevated levels of lipid peroxides are causal to FFA-
induced beta cell dysfunction in vivo and ex vivo (isolated islets obtained from mice i.v. infused
with treatments)205. Our study utilized mice overexpressing Glutathione Peroxidase-4 (GPx4),
which is an enzyme that specifically reduces lipid peroxides, and wildtype control mice. After i.v.
infusion with saline or oleate for 48h, dichlorodihydrofluorescein diacetate was used to image
levels of ROS in isolated islets. Alternatively, beta cell function was assessed in vivo using the

31
hyperglycemic clamp method or ex vivo via an insulin secretion assay (measurement of insulin
secretion after incubating islets in glucose-containing media for 2h).
A potential mechanism by which ROS can decrease insulin synthesis is by decreasing the
levels and activities of the transcription factors Pdx-1 and MafA264,271. This was suggested by
studies which showed that the antioxidant NAC prevented the ROS-induced decrease of Pdx-1
and MafA expression in HIT-T15 cells (beta cell line) or human islets incubated in high glucose
concentrations in vitro244–246,264. One of these studies also found that NAC protected against a
ROS-induced decrease in insulin expression and secretion in vivo246. Pdx-1 is important for the
transcription of insulin, whereas MafA plays a role in beta cell growth and maturation as well as
insulin transcription272. Oxidative stress can decrease insulin transcription by activating the
general stress-related enzymes JNK and NFκB (nuclear factor kappa-light-chain-enhancer of
activated B cells)273. This is known to disrupt the process of insulin secretion. The responsible
mechanisms will be discussed later in my thesis. This can occur via inflammatory pathways,
eventually implicating forkhead box-O (FOXO) proteins in insulin signaling265.
In pancreatic beta cells, ROS can also decrease GSIS via mitochondrial dysfunction, which
can consist of the inhibition of the Na+/Ca2+ exchanger (NCLX) directly by ROS in vitro274,275.
This prevents the transport of Ca2+ in mitochondria, causing a decrease in ATP production. As
insulin secretion depends on ATP, it may also be decreased as a consequence.
A decrease in ATP levels can also occur via the ROS-mediated activation of uncoupling
protein 2 (UCP2). Uncoupling protein 1 (UCP1; also known as thermogenin) has been clearly
shown to be responsible for the uncoupling of the ETC and ATP synthesis, resulting in decreased
ATP synthesis and increased thermogenesis257,276,276,277. However, the role of UCP2 in beta cells
is not clear. Studies regarding the role of UCP2 in beta cells will be described in section “Role of
SIRT1 in Beta Cells”.

32
Severe ROS damage can result in the death of the beta cell via apoptosis. ROS-induced
apoptosis is usually the result of mitochondrial damage that allows the release of proapoptotic
factors such as cytochrome c278. In sufficiently high levels, these proapoptotic factors activate a
signaling cascade that leads to apoptosis256,278.
While high levels of ROS have been shown to cause beta cell dysfunction and beta cell
death in some cases, it is important to keep in mind that a certain level of ROS is necessary for the
proper functioning of all cells, including beta cells266. Depending on the type of cell, there is a
level of ROS that is optimal to its function. It has been shown that exposure of beta cells to high
levels of antioxidants results in a decrease in GSIS266. Furthermore, some studies have found that
ROS can serve as important signaling molecules in insulin secretion257,266. For instance, a
transient increase in intracellular ROS levels has been shown to promote insulin signaling via the
oxidation and inhibition of Receptor-like Protein Tyrosine Phosphatases (RPTPs), which would
normally impair the tyrosine-phosphorylation-mediated activation of the insulin receptor279,280.
While the mechanisms behind the beneficial effects of ROS are currently not clear, the
aforementioned findings certainly shed a new light on the role of ROS in the beta cell.
1.10.2 The Role of Endoplasmic Reticulum Stress
As mentioned earlier, the synthesis of insulin involves the cleavage and folding of
preproinsulin within the RER. When the beta cell must produce excessive amounts of insulin,
such as during compensatory hyperinsulinemia in response to FFA-induced insulin resistance, the
RER can become congested with preproinsulin272,281,282. This leads to disruption of the RER,
which manifests itself as ER stress. This has been demonstrated by elevated ER stress markers in
islets and beta cell lines exposed to elevated FFA levels272,281,282. As 50% of the protein
synthesized by beta cells is insulin283, an increase in insulin synthesis can cause significant ER
stress. This can result in beta cell dysfunction, and in some cases, beta cell apoptosis284.

33
Prolonged ER stress is known to activate the unfolded protein response (UPR), which is a
common cellular response that reduces ER stress. This occurs by degrading misfolded proteins,
halting protein translation, and increasing the levels of molecular chaperones involved in protein
folding. However, if the UPR is prolonged or is initiated too late, it progresses towards
apoptosis281,282. Studies have shown that markers of apoptosis, such as CHOP (CCAAT-enhancer-
binding protein homologous protein), are increased in the beta cells of T2DM patients, and in beta
cells exposed to FFA in vitro272,283.
In addition to increasing the load of insulin synthesis on beta cells, there is evidence that
FFA can decrease the capacity of the ER to process proteins284. This is in part due to the FFA-
induced depletion of ER Ca2+ stores, which are necessary for ER function282. By decreasing ER
capacity, FFA also increase the susceptibility to ER stress.
In contrast to in vitro studies, few in vivo studies have investigated the role of ER stress in
FFA-induced beta cell dysfunction. A recent study done by our lab found that ER stress plays a
causal role in high-glucose-induced beta cell dysfunction in vivo239. This was shown to occur via
the positive feedback relationship between ER stress and oxidative stress, particularly
mitochondrial superoxide. In the context of FFA-induced beta cell dysfunction, recent data in our
lab suggest that neither the administration of IH nor oleate affect ER stress markers in rodent beta
cells in vivo (unpublished data). As i.v. infusion of palmitate in vivo has very recently become
feasible, our lab aims to investigate the role of ER stress in palmitate-induced beta cell
dysfunction in vivo in the future. Nevertheless, a collaborative study by our lab has shown that
oral administration of sodium phenylbutyrate (PBA), which reduces ER stress, in humans
ameliorates beta cell dysfunction and insulin resistance induced by IH i.v. infusion184. Hence, it is
also possible that the positive effect of PBA on FFA-induced beta cell dysfunction is not mediated

34
by ER stress reduction due to the multiple effects of PBA. Thus, additional studies are needed in
order to elucidate the role of ER stress in FFA-induced beta cell dysfunction in vivo.
1.10.3 The Role of Inflammation
There is a reciprocal relationship between oxidative stress, ER stress, and inflammation as
they are known to induce each other. Oxidative stress is known to activate IKKB (inhibitor of
nuclear factor kappa-B kinase subunit beta)285, which subsequently phosphorylates the inhibitor
IκBα (nuclear factor of kappa light polypeptide gene enhancer in B-cells inhibitor, alpha),
resulting in the activation of the proinflammatory NFκB. In addition, IKKB has been shown to
prevent the tyrosine phosphorylation of insulin receptor substrate (IRS) by serine phosphorylating
IRS286,287. This prevents the activation of IRS, consequently impairing insulin signaling.
A study performed by our lab suggests that IKKB is causal to FFA-induced beta cell
dysfunction in vitro, ex vivo, and in vivo (unpublished data). This study utilized the IKKB-
inhibitor salicylate as well as beta cell-specific IKKB-null mice. Nevertheless, as with ROS, some
studies have found that a certain degree of activation of the IKKB/NFκB pathway may be
beneficial to beta cell function288–290. A collaborative study by our lab and the lab of Dr. Gary F.
Lewis found that oral administration of the anti-inflammatory sodium salicylate at a high dose in
men did not prevent insulin resistance and beta cell dysfunction induced by i.v. infusion of IH183.
However, the majority of studies have reported positive results in the treatment of FFA-induced
beta cell dysfunction using salicylate in humans291–293.
IKKB can be activated by FFA through multiple mechanisms. These include oxidative
stress induced by FFA, ER stress294, inflammatory cytokines, PKC295–298, and TLRs which are
directly activated by saturated FFA299.
Another mechanism by which inflammation can cause beta cell dysfunction is the
activation of JNK. Similar to IKKB, JNK is known to serine phosphorylate IRS, consequently

35
impairing insulin signaling300. JNK has also been implicated in FFA-induced beta cell
dysfunction300. In addition, JNK is at least partially responsible for retention of FOXO1 in the
nucleus, which results in the exclusion of Pdx-1 from the nucleus and the consequent decrease in
insulin transcription301,302. Based on in vivo and in vitro experiments, a recent study suggests that
nuclear translocation of FOXO1 results in decreased transcription of peroxisome proliferator-
activated receptor-γ (PPARγ), which is an important transcription factor for Pdx-1303. As a stress-
activated enzyme, JNK can also be activated by inflammatory cytokines, ceramides, ER stress,
and PKC16.
Recent results in our lab have shown that FFA-induced beta cell dysfunction is mediated
by JNK in the context of palmitate, but not in the context of oleate, in vitro. Isolated islets
obtained from JNK1-null mice and wildtype controls were cultured for 48h in Roswell Park
Memorial Institute (RPMI)-based media with or without palmitate or oleate (0.4 mM in 0.5%
BSA). Afterwards, the islets underwent an insulin secretion assay followed by the measuring of
their intracellular insulin content. As mentioned above, other data in our lab have demonstrated
that JNK plays a causal role in high-glucose-induced beta cell dysfunction downstream of
superoxide generation and ER stress in vivo.
1.10.4 The Role of Protein Kinase C
PKC is a family of protein kinase enzymes that play a significant role in regulating
signaling cascades by phosphorylating other proteins. There are many isoforms of PKC304.
Activated PKC is thought to induce beta cell dysfunction and, in some cases, apoptosis partly by
impeding insulin signaling in beta cells305. During excess energy conditions, lipid-derived by-
products can begin to accumulate. These include Long-Chain Coenzyme A (LC-CoA), DAG, and
ceramides306. LC-CoA and DAG are known to activate classical and novel isoforms of PKC,

36
which subsequently lead to beta cell dysfunction307–309. Ceramides are also known to induce beta
cell dysfunction310,311, as described below.
Activated PKC, particularly its novel isoforms (δ, ε, η, and θ isoforms), serine/threonine
phosphorylate the insulin receptor (IR) and IRS. This prevents the tyrosine-phosphorylation-
mediated activation of the IR and IRS, and consequently impairs insulin signaling. This
mechanism of preventing tyrosine-phosphorylation of IRS was evidenced using human IRS-1 in
vitro312. Another study found that HFD-fed mice overexpressing dominant-negative Akt exhibit
decreased GSIS, suggesting that impaired insulin signaling may be involved in FFA-induced beta
cell dysfunction313. Thus it is possible that PKC mediates FFA-induced beta cell dysfunction by
impairing insulin signaling.
FFA-induced activation of PKCε results in decreased transcription of insulin249, 314. It has
been shown that PKCε whole-body knockout mice are protected against glucose intolerance
induced by a HFD, compared with wildtype controls314. In addition, deletion of PKCε in mice
treated with high levels of FFA resulted in improved GSIS and modestly decreased whole-body
and hepatic insulin clearance314. The most likely mechanism by which PKCε inhibition improves
GSIS is the restoration of the efficiency of FFA esterification via glucose-stimulated flux through
the TCA cycle314,315. The study reported that deletion of PKCε did not alter hepatic insulin
signaling or the number of insulin receptors on hepatocytes or their affinity to insulin, but rather
resulted in decreased insulin internalization by hepatocytes (assessed using [125I]insulin). The
mechanism responsible for the decrease in hepatic insulin internalization following PKCε-
deletion was not investigated in that study. The article concluded that a modest reduction in
insulin internalization by hepatocytes can be accomplished without necessarily impairing insulin
signaling.

37
In a study done by our lab using the PKC inhibitor bisindolylmaleimide (BIM), oleate was
found to induce the translocation of PKCδ from the cytosol to membrane fractions, mediating the
FFA-induced decrease in hepatocyte insulin binding316. Although the mechanism by which PKCδ
in membrane fractions affects hepatocyte insulin binding requires further research, it has been
reported that PKC increases the internalization of membrane receptors, including the IR, via a
non-specific and ligand-independent process of coated-pits internalization317. This may be
mediated by the phosphorylation of internalization motifs on the cytoplasmic juxtamembrane
domain of the membrane receptors317,318. Thus, PKCδ may mediate the oleate-induced decrease in
hepatocyte insulin binding by increasing the internalization of the IR, resulting in a deficiency of
IRs on the plasma membrane.
As CEACAM1 is a key mediator in the internalization of the insulin receptor, it is possible
that it is implicated in the PKC-mediated internalization of the insulin receptor. CEACAM1 can
be activated via serine/threonine phosphorylation by PKC120,319. Indeed, a study found that
Protein Kinase-C Activator (PKA) increased the Ser503 phosphorylation of CEACAM1 in
hepatocytes, resulting in its activation319. However, since the administration of a PKC inhibitor
(calphostin C) in colon carcinoma cells did not alter the phosphorylation of CEACAM1319, it is
currently unclear whether or not PKC had mediated the PKA-induced Ser503 phosphorylation of
CEACAM1 in hepatocytes.
Acute overexpression of kinase-negative PKCδ specifically in beta cells of mice on a HFD
was found to improve glucose tolerance and increase plasma insulin levels, compared with
wildtype controls235. Although the mechanism is unknown, this seems to have been caused by
PKCδ’s effect of preventing the translocation of FOXO1 into the nucleus where it would cause
the nuclear exclusion of Pdx-1235. Thus, Pdx-1 was uninhibited and insulin transcription was not
impaired. In addition, kinase-negative PKCδ overexpression in beta cells was found to prevent

38
apoptosis and mitochondrial dysfunction235. Thus, PKC, in particular its novel isoforms, are
known to be causal to FFA-induced beta cell dysfunction. Nevertheless, the responsible
mechanisms are currently unclear.
1.10.5 The Role of Ceramides
Ceramides are a family of waxy lipids that are found in cell membranes and can act as
signaling molecules in apoptosis. Ceramides are endogenously formed in highest amounts by the
metabolism of saturated fatty acids, such as palmitate. Studies have shown that ceramides can
decrease insulin transcription by impairing the nuclear translocation of Pdx-1 and by preventing
the glucose-induced expression of MafA, though the mechanisms are unknown320,138. Many
studies have shown that ceramides can cause apoptosis in beta cells196,321,195. Furthermore, other
studies have demonstrated that inhibition of serine palmitoyltransferase (SPT), which catalyzes
the first step in ceramide production, prevents apoptosis in human and rat islets exposed to high
levels of palmitate in vitro322. Inhibition of ceramide production also protected beta cells from
apoptosis in Zucker Diabetic Fatty (ZDF) rats311. In summary, oxidative stress, ER stress,
inflammation, PKC, and ceramides all play important roles in the development of beta cell
dysfunction in the context of exposure to elevated FFA levels.
1.11 Sirtuins
In the past decade, sirtuins were discovered in yeast and were named Silent Information
Regulator (SIR) genes323. Members of the SIR gene family were later discovered in other species,
eventually indicating that the SIR genes are expressed in all kingdoms of life. The proteins
encoded by the SIR genes were found to be Nicotinamide Adenosine Dinucleotide (NAD)-
dependent deacetylases324,325. Importantly, SIR genes were found to extend the lifetime of
yeast326,327. As a result, research into the role of SIR genes in human aging skyrocketed. Many

39
years of research in this area have revealed that animals contain seven members of the SIR
family. They are named SIRT (silent mating type information regulation 2 homolog) 1 - 7. While
most mammalian SIRT enzymes are deacetylases, their tissue-specific expression, intracellular
localization, and specific roles in physiological processes vary328. SIRT1 is the most studied
sirtuin in mammals. It is also the closest mammalian homologue to the first yeast sirtuin. The
similarities and differences between the mammalian sirtuins are briefly summarized in Table 1.

40
Table 1. Summary of the seven mammalian sirtuins SIRT1-7.
Sirtuin Associated
Diseases Main Processes
Enzymatic
Activity
Main
Substrates
Subcellular
Localization
SIRT1
Metabolic,
neurological,
renal,
cardiovascular,
cancer,
mitochondrial
Glucose
production, β-
oxidation,
insulin
secretion,
neuroprotection,
cell stress
response
Deacetylase
FOXO1/3/4,
p53, NF-κB,
PGC-1α,
eNOS,
Histone
H1/4, LXR,
DBC-1
AROS
Nuclear,
cytoplasmic
SIRT2
Neurological,
metabolic,
cancer
Cell cycle
control, tubulin
deacetylation
Deacetylase
Tubulin,
FOXO,
Histone H4
Nuclear,
cytoplasmic
SIRT3 Metabolic,
mitochondrial
ATP production,
mitochondrial
protein
deacetylation, β-
oxidation
Deacetylase ACS2 Mitochondrial
SIRT4 Metabolic,
mitochondrial
Amino acid-
stimulated
insulin secretion
ADP-
ribosyltransferase
GDH, IDE,
ANT2/3 Mitochondrial
SIRT5 Neurological Urea cycle
regulation Deacetylase CPS1 Mitochondrial
SIRT6 Cancer
NF-κB
regulation, base
excision repair
Deacetylase,
ADP-
ribosyltransferase
Histone H3 Nuclear
SIRT7 Cardiovascular RNA Pol I
transcription Deacetylase
RNA Pol I,
p53 Nucleolar
Abbreviations and definitions (in alphabetical order): ACS2, acetyl-CoA-synthetase 2; ANT2/3, adenine
nucleotide translocator – transports ATP into mitochondria; AROS, active regulator of SIRT1 – an
activator of SIRT1 and a suppressor of p53 activity; CPS1, carbamoyl phosphate synthetase 1 - a
mitochondrial ligase involved in the production of urea; DBC-1, deleted in breast cancer 1 - an inhibitor of
SIRT1; eNOS, endothelial nitric oxide synthase; FOXO, forkhead box O - a family of transcription factors
that regulate cell growth and cell differentiation; GDH, glutamate dehydrogenase - a mitochondrial enzyme
involved in urea synthesis; Histone H1/4, two of five main histone components of chromatin in eukaryotes;
IDE, insulin degrading enzyme; LXR, liver X receptor - a member of a family of transcription factors that
regulate cholesterol levels, fatty acids and glucose homeostasis; NF-κB, nuclear factor kappa B; p53, also
known as TP53 is a protein that suppresses tumor growth; PGC-1α, peroxisome proliferator-activated
receptor gamma co-activator 1 alpha; RNA Pol I, RNA polymerase I; Tubulin, a major component of the
eukaryotic cytoskeleton. Table adapted from references 323,329–332.

41
1.11.1 Sirtuin-1
Figure 5. Illustrations of the three-dimensional protein structure and catalytic activity of the NAD-
dependent protein deacetylase Sirtuin-1 (SIRT1). Protein structure adapted from J. Mol. Biol. 426: 526-
541, 2014.
SIRT1 is an NAD-dependent protein deacetylase that has been shown to have beneficial
effects, such as improving beta cell function by increasing insulin secretion333. The three-
dimensional structure of the SIRT1 protein is depicted above in Figure 5. Modest transgenic
overexpression of SIRT1 in C57BL/6 mice was reported to protect against HFD-induced glucose
intolerance in vivo334. Although SIRT1 has been found in almost all tissues of the body, it plays a
different role depending on the tissue in which it is expressed. In most tissues, SIRT1 has been
shown to be important in the regulation of nutrient metabolism. SIRT1 has been involved in
various diseases, including diabetes, neurodegenerative diseases, and cancer. As was shown in
Table 1, SIRT1 affects many molecules and physiological processes. Significant regulators of
energy metabolism which are influenced by SIRT1 activity include PGC-1α (peroxisome
proliferator-activated receptor gamma coactivator 1-alpha), PPARγ332, and UCP2335,336. PGC-1α
is activated by direct deacetylation by SIRT1 at specific lysine residues333,337. In adipocytes,
SIRT1 was shown to repress PPARγ by binding to PPARγ’s cofactors NCoR (nuclear receptor

42
co-repressor) and SMRT (silencing mediator of retinoid and thyroid hormone receptors)332.
SIRT1 represses the transcription of UCP2 by directly binding to its promoter336.
According to the aforementioned study, unpublished results obtained by its authors
demonstrate that the inhibition of SIRT1 by nicotinamide (a SIRT1 inhibitor) restores UCP2
transcription, suggesting that deacetylation may be involved in the suppression of UCP2
expression by SIRT1336. Nevertheless, although deacetylation has been shown to be involved in
most of the effects of SIRT1, it is not clear whether deacetylation is involved in all of SIRT1’s
effects338–340. In summary, deacetylation can increase or decrease function depending on the target
protein.
1.11.2 The Role of SIRT1 in Beta Cells
While SIRT1 has been most studied in the liver, there are relatively few studies focused on
SIRT1 in beta cells. In beta cells, SIRT1 is primarily found in the nucleus341, although it is also
present in the cytosol342,343. Overall, these studies support the role of SIRT1 as an enhancer or
protector of beta cell function in response to glucose, as described below.
One of the studies utilized a potent SIRT1-activator, resveratrol, to activate SIRT1 in INS-
1E insulinoma cells in vitro344. Resveratrol is a natural polyphenol that has been widely used as an
activator of SIRT1. Resveratrol is typically found in grapes and red wine. The study found that
exposure to 1 µM resveratrol significantly increased insulin secretion by the insulinoma cells
acutely and over 24h of exposure344. Furthermore, this improvement in beta cell function
remained after removing the cells from the resveratrol-containing culture following 24h of
resveratrol exposure. The same study also assessed the effects of resveratrol on islets obtained
from a type 2 diabetic human donor. It found that resveratrol partially enhanced insulin secretion
in response to glucose.

43
Another study found that Beta Cell-Specific Sirtuin 1-Overexpressing (BESTO) transgenic
mice exhibited improved glucose tolerance and glucose-stimulated insulin secretion in vivo,
compared with wildtype mice335. SIRT1 has been shown to positively regulate insulin secretion
in beta cells335. As described earlier, SIRT1 accomplishes this effect by suppressing the
transcription of UCP2 via directly binding with the UCP2 promoter336. As UCP2 is involved in
dissipating the H+ electrochemical gradient in mitochondria, its decreased expression increases
the efficiency of oxidative phosphorylation, leading to greater ATP production345. As insulin
secretion depends on ATP, it is also increased346. The lack of dissipation of the electrochemical
gradient also results in increased ROS production257,347. However, net ROS levels do not increase
since SIRT1 also activates FOXO proteins, which increase the transcription of antioxidant
enzymes. This ultimately leads to decreased oxidative stress348, as will be explained in the section
“Role of FOXO Proteins”.
Levels of UCP2 have been shown to decrease when SIRT1 levels are increased, and to
increase when SIRT1 levels are decreased335,336. As mentioned earlier in my thesis, studies
regarding the effects of UCP2 on beta cell function have been controversial. However, it is
possible that this is due to the dual effect of UCP2 resulting in decreased levels of ATP as well as
ROS. Thus, in the absence of an increase in ROS (because SIRT1 decreases ROS levels), the
decrease in UCP2 levels by SIRT1 results in increased beta cell function.
Some studies have demonstrated that knockdown or knockout of UCP2 expression
improves GSIS due to elevated ATP levels within beta cells231,336,347,349. While some studies state
that activation of UCP2 in beta cells decreases ATP levels and insulin secretion231,345,350, other
studies report contradicting results276,350,351. Nevertheless, UCP2 seems to be involved in some
way in ROS-induced beta cell dysfunction345.

44
Some studies showed that increased UCP2 levels decrease ATP production and insulin
secretion346,352. There is evidence that decreased UCP2 expression protects mice against a HFD-
induced decrease in beta cell function, although the responsible mechanism is currently
unclear231,334,353. On the other hand, a number of studies did not find a link between UCP2 and
FFA-induced beta cell dysfunction. For instance, a study utilizing UCP2-null mice have reported
decreased GSIS and no changes in islet insulin content, compared with controls350. Other studies
which involved the overexpression of UCP2 did not find any significant changes in GSIS or ATP
levels within beta cells, compared with wildtype controls277,354. Thus, although most studies
support the hypothesis that UCP2 plays a role in FFA-induced beta cell dysfunction, some
confounding studies render the evidence unclear. It is possible that the contradictory studies are
due to the dual effects of UCP2 in increasing the production of ATP as well as ROS.
1.11.3 Roles of SIRT1 in the Liver, Skeletal Muscle, and Brain
In hepatocytes, SIRT1 deacetylates FOXO1, PGC-1α, and Liver X Receptor (LXR),
resulting in their activation. Although FOXO1, PGC-1α, and LXR have different roles in the
liver, they collectively regulate beta oxidation and gluconeogenesis340,355,356. Although the
upregulation of gluconeogenesis seems to portray SIRT1 as an antagonist to insulin action in the
liver, SIRT1’s effect of decreasing intrahepatic fat content ultimately results in increased hepatic
insulin sensitivity357. It has been shown that although liver-specific SIRT1-knockdown mice had
improved glucose tolerance, they had greater hepatic steatosis and steatohepatitis after being fed a
HFD, compared with controls358. Since SIRT1 activates PGC-1α, and PGC-1α upregulates
mitochondrial biogenesis, it is thought that SIRT1 increases energy expenditure in hepatocytes358.
In WAT, SIRT1 has been shown to exert significant effects via PPARγ and FOXO1.
SIRT1’s direct repression of PPARγ was shown to result in an increase in FFA mobilization355.
SIRT1’s deacetylation and activation of FOXO1 results in increased transcription and production

45
of adiponectin since FOXO1 is a transcription factor for adiponectin359. In a study, mice
overexpressing SIRT1 exhibited an ~30% increase in adiponectin concentration in blood
plasma360.
In skeletal muscle, one of SIRT1’s main roles is the upregulation of mitochondrial
biogenesis, resulting in an increase in beta oxidation and energy production358. As explained
above, this occurs via the direct deacetylation and activation of PGC-1α by SIRT1. In addition,
SIRT1 in skeletal muscle is known to increase insulin sensitivity via histone H3 deacetylation,
resulting in the repression of the expression of PTP1B (protein-tyrosine phosphatase 1B), which
is a negative regulator of insulin signaling361,362. This was evident from two studies: the first
utilized muscle-specific PTP1B-null mice363, and the second used whole-body PTP1B-null
mice364. Thus, SIRT1 increases insulin sensitivity in skeletal muscle.
In the brain, SIRT1 is found in the hypothalamus, particularly in the proopiomelanocortin
(POMC) and steroidogenic factor-1 (SF-1) neurons365,366. The effects of SIRT1 in the brain are
less clear, compared with its effects in the liver, skeletal muscles, and WAT. Studies involving
transgenic mouse models have shown that SIRT1 in the brain may increase energy expenditure
and prevent obesity367,368. In addition, neuronal SIRT1 has been found to protect against oxidative
stress, ameliorate inflammation and apoptosis, and regulate neuronal and stem cell
differentiation369,370. Studies suggest that the protective effects of SIRT1 on neurons are based on
the SIRT1-mediated decrease in inflammation and apoptosis. These are likely caused by SIRT1’s
deacetylation of NFκB, resulting in the suppression of the inflammatory pathway and
apoptosis323,371.
1.11.4 Roles of FOXO Proteins
FOXO proteins are transcription factors, and consist of FOXO 1, 3, 4, and 6 in mammals.
These transcription factors are inhibited by the insulin/PI3K (phosphoinositide 3-kinase)/Akt

46
pathway and are involved in oxidative stress, metabolism, and organismal longevity372,373.
FOXO2 is a pseudogene of FOXO3, and FOXO5 is the fish orthologue of FOXO3373. Acetylated
FOXO4 has been shown to promote podocyte apoptosis374. FOXO6, mainly found in the brain
and liver, has been recently shown to have negative effects on glucose metabolism, where
overexpressing FOXO6 in livers of mice gradually resulted in glucose intolerance, fasting
hyperglycemia, and insulin resistance375,376.
FOXO1 is the most common FOXO protein in beta cells377. FOXO1 and 3 are known to
decrease oxidative stress by upregulating antioxidant genes, such as MnSOD348,378. In addition, a
study has reported that FOXO1 may form a complex with the promyelocytic leukemia protein
(Pml) and SIRT1. This complex subsequently increases the expression of the transcription factors
NeuroD and MafA379. In addition to Pdx-1, MafA and NeuroD are transcription factors that
regulate insulin. Moreover, NeuroD and MafA are involved in the regulation of beta cell
maturation380. FOXO1 has also been shown to directly activate the SIRT1 promoter, increasing
SIRT1 mRNA and protein levels381. Similarly, FOXO3 is a transcription factor for SIRT1372,382.
Thus, FOXO1 or FOXO3 activation may upregulate SIRT1 via a feed-forward mechanism.
With that said about the protective role of FOXOs against oxidative stress and the effects
of FOXOs on NeuroD and MafA, it must be noted that FOXO1 can also indirectly decrease
insulin transcription. Active FOXO1 is localized in the nucleus, where it induces the nuclear
exclusion of Pdx-1, which is a major transcription factor for insulin300. In summary, although
activation of FOXO proteins seems to ultimately attenuate ROS, the overall effect of FOXO1 on
beta cell function in particular is not very clear.
1.11.5 Regulation of SIRT1
As mentioned earlier, SIRT1 is a deacetylase that is NAD-dependent. Hence, one of the
main regulators of SIRT1 activity is the availability of intracellular NAD. During fasting, reduced

47
energy production results in an increase in the NAD/NADH ratio in cells323. Thus, provided that
the sum of NAD and NADH levels are not significantly altered, this results in a relative increase
in intracellular NAD levels. As a result, SIRT1 activity is upregulated383,384. Consistently, the
activity of SIRT1 is known to be increased during fasting385–387. A decrease in NAD levels
reduces SIRT1 activity388–390. This can be caused by a number of factors, ranging from decreased
NAD/NADH ratio due to energy excess to depletion of NAD levels by enzymes other than
SIRT1391.
Calorie restriction has been shown to increase lifespan in several organisms, including
primates, via increased SIRT1 activity391–393 and levels394–396. While this may be caused by
increased NAD availability, a 2004 study published in Science suggests that p53 can also
upregulate SIRT1 activity382. A transcription factor, p53, can function as either an activator or a
repressor. Normally, p53 directly decreases SIRT1 transcription; however, under caloric
restriction, p53 has been shown to play a complex role in which it is required for the FOXO3-
mediated increase in SIRT1 expression382. Activated FOXO3a subsequently increases SIRT1
transcription by directly interacting with p53 and two p53-binding sites at the SIRT1 promoter.
The same study found that FOXO3a-knockdown mice did not exhibit an increase in SIRT1
expression after chronic caloric restriction, compared with wildtype controls. Hence, FOXO3a
seems to be important in the caloric restriction-mediated increase in SIRT1 expression.
While caloric restriction increases SIRT1 activity in many tissues, such as skeletal muscle
and WAT, caloric restriction was found to decrease SIRT1 activity in the liver by reducing the
NAD/NADH ratio in hepatocytes397. Interestingly, a high-caloric diet was shown to increase
SIRT1 activity in hepatocytes. The reason for the opposite effect of caloric restriction on SIRT1
in the liver, compared with the other tissues, is thought to be because the liver plays a large role in
the synthesis of triglycerides and cholesterol. As these processes are usually in proportion to

48
caloric intake and are highly reductive, the highly-fed liver should have an oxidized redox state
(increased NAD/NADH ratio) in order to perform these processes397,398. Hence, the effects of
caloric restriction on SIRT1 may depend on the tissues in which SIRT1 is expressed.
Incubation of rat islets in palmitate-containing media or intravenous infusion of IH in rats
decreased SIRT1 mRNA and protein levels in beta cells399, 400. The mechanisms responsible for
the FFA-induced decrease in SIRT1 are unclear. However, one known mechanism is that FFA-
induced ROS damages DNA, leading to the activation of the DNA repair enzyme Poly (ADP-
Ribose) Polymerase (PARP). PARP consumes NAD to repair DNA, resulting in decreased NAD
availability401. As SIRT1 is dependent on the bioavailability of NAD, a decrease in SIRT1
activity may ensue384,402,403. Accordingly, studies using whole-body PARP-knockout mice (PARP
decreases NAD availability) have demonstrated increased SIRT1 activity404,405; however, this
effect has not been assessed in beta cells. Decreased SIRT1 activity may reduce the activity of the
SIRT1-transcription factors FOXO1 and FOXO3 via a feed-forward mechanism372, and thus
result in decreased SIRT1 expression.
As explained above, FFA-induced ROS can attenuate SIRT1 activity by decreasing NAD
bioavailability. Nevertheless, ROS can alter SIRT1 activity independently of NAD. For instance,
the oxidative stress-activated enzyme JNK1 has been shown to serine-phosphorylate SIRT1406,
transiently activating it. However, this serine-phosphorylation of SIRT1 has additional effects on
SIRT1. It induces SIRT1’s ubiquitination, resulting in SIRT1’s gradual degradation and decreased
activity over time. This form of SIRT1 ubiquitination was demonstrated using a model of HFD-
fed mice in vivo407. ROS have also been shown to directly induce the alkylation of cysteine
residues on SIRT1. This results in increased SIRT1 proteosomal degradation, ultimately leading
to decreased SIRT1 protein levels408.

49
In addition to being serine-phosphorylated by JNK1, SIRT1 can be serine- and threonine-
phosphorylated by cyclin-dependent kinase-1 (Cdk-1), independently of JNK, resulting in
decreased SIRT1 activity409. Cdk-1 is a highly conserved kinase that plays a regulatory role in the
G2/M phase of mitosis. SIRT1 activity can be positively regulated by the nuclear protein AROS
(Active Regulator of SIRT1). This takes place by AROS directly binding to SIRT1, inducing a
conformational change in SIRT1410. As a result of this conformational change, SIRT1’s
deacetylation activity is enhanced.
A negative regulator of SIRT1 is the nuclear protein Deleted in Breast Cancer-1 (DBC-
1)411,412. DBC-1 directly binds to the catalytic site of SIRT1, consequently inhibiting SIRT1’s
activity412. It has recently been shown that DBC-1 is phosphorylated and activated by the kinase
Ataxia Telangiectasia Mutated (ATM) following DNA damage and oxidative stress413,414.
Interestingly, DBC-1 can also act as a switch for SIRT1 activity. For example, activated AMPK
induces the dissociation of the DBC-1-SIRT1 complex, resulting in activated SIRT1415. As the
regulation of SIRT1 by DBC-1 seems to occur independently of intracellular changes in NAD
levels415–417, DBC-1 might have been involved in the decrease of SIRT1 activity in our lab’s
previous experiments since we did not observe decreased NAD levels in rat islets treated with
FFA. While AROS and DBC-1 do regulate SIRT1 function, their mechanisms are not quite clear
yet since their effects on SIRT1 have only recently been discovered.
Lastly, it should be mentioned that over 3,500 activators of SIRT1 have been
developed329. These small-molecule compounds are structurally unrelated to resveratrol, yet are
1,000 fold more potent than resveratrol at activating SIRT1. These activators bind to the SIRT1
enzyme-peptide substrate complex at an allosteric site near the catalytic domain, lowering the
Michaelis constant (KM) for SIRT1’s deacetylation activity418. The KM is a widely used index of

50
enzyme activity. It is defined as the concentration of substrate required for a chemical reaction to
occur at half of its maximum velocity419.
1.11.6 Nicotinamide Mononucleotide
As described earlier, SIRT1 being an NAD-dependent enzyme is affected by NAD
availability. As such, altering intracellular levels of NAD is a viable method of regulating SIRT1
activity. A number of studies have demonstrated that altering NAD levels by altering NAD
synthesis affects SIRT1 activity420–424. NAD is derived from nicotinamide by the action of several
enzymes. A key intermediate of NAD synthesis is nicotinamide mononucleotide (NMN), which is
produced from nicotinamide and 5-phosphoribosyl-pyrophosphate using nicotinamide
phosphoribosyltransferase (NAMPT). NMN is a water-soluble ribonucleotide consisting of a
ribose backbone, a nitrogenous base (nicotinamide), and a phosphate group425. The structural
formula of NMN is depicted in Figure 6. NAMPT represents the rate-limiting enzyme in
mammalian NAD biosynthesis. NMN is then converted to NAD by nicotinamide mononucleotide
adenylyltransferase-1 (NMNAT)426.
Figure 6. Chemical structure of nicotinamide mononucleotide (NMN), which consists of a ribose
backbone, a nitrogenous base (nicotinamide), and a phosphate group. Adapted from Cell. 129(3): 453–454,
2007425.
There are two forms of NAMPT: intracellular NAMPT (iNAMPT) and extracellular
NAMPT (eNAMPT). iNAMPT is found in high levels in brown adipose tissue (BAT), liver, and

51
kidneys, and in intermediate levels in WAT, skeletal muscle, lung, testes, and spleen. No
iNAMPT has been detected in the pancreas or brain423. eNAMPT, thought to be produced by
post-translational modification of iNAMPT, is secreted from adipose tissue and promotes insulin
secretion427. While iNAMPT is essential to the NAD biosynthetic pathway, eNAMPT is vital to
NAD synthesis in beta cells due to the absence of iNAMPT in the pancreas. A study found that an
eNAMPT-knockdown (haplodeficient) mouse model and chemical inhibition of NAMPT in
wildtype mice exhibited impaired NAD biosynthesis and GSIS in vivo and in vitro423.
A study published in Cell Metabolism showed that wildtype B6 mice fed a HFD
demonstrated impaired NAMPT-mediated NAD biosynthesis, resulting in decreased SIRT1
activity and exacerbated T2DM (the study did not assess which form of NAMPT was
decreased)424. The same study found that administration of the rate-limiting intermediate in NAD
biosynthesis, NMN, restored normal NAD levels and synthesis in the liver, WAT, and skeletal
muscles. Interestingly, NMN treatment also protected against T2DM induced by HFD. NMN was
administered intraperitoneally to male diabetic mice at 500 mg/kg body weight/day for 10
consecutive days. No noticeable abnormalities or significant changes in body weight were
reported.
Another study, published in Diabetologia, found that mice on a fructose-rich diet (FRD)
exhibited markedly lower eNAMPT levels in blood plasma, increased iNAMPT levels in WAT,
and decreased insulin secretion, compared with controls427. This suggests that excess energy
consumption, metabolic dyslipidemia, and chronic inflammation impair NAD biosynthesis and
insulin secretion. Furthermore, administration of NMN restored normal insulin secretion in FRD-
fed mice in vivo. The protective effect of NMN was also observed in isolated islets cultured with
pro-inflammatory cytokines427.

52
The mechanism of transport of NMN into eukaryotic cells is currently unknown424;
however, the very few studies performed to date suggest that NMN transport in Salmonella
typhimurium occurs via PnuC and NadI428,429. One study found that PnuC is a membrane-
associated protein which is a major component of the NMN transport system. NadI is a protein
that depends on pyridine levels (presumably NAD) in order to serve two functions: 1) increase the
transcription of the nadA and nadB biosynthetic genes, and 2) positively regulate the activity of
NMN permease, which is part of the NMN transport system428. Another study found that pnuC of
Haemophilus influenzae, which is distally related to S. typhimurium, was able to uptake only
nicotinamide riboside and not NMN429. Thus, while few studies on NMN’s mechanism of
transport have been done, specifically in prokaryotic cells, and are unclear, it is possible that a
transporter mediates the uptake of NMN in eukaryotic cells.
There is evidence suggesting that SIRT1 may be one of the mediators of NMN’s
protective effects against T2DM427. Transcription factors expressed during HFD treatment and
during NMN administration were analyzed. The transcription factors that exhibited greatest
changes in expression particularly during the HFD and NMN treatments were all targets of SIRT1
deacetylation: NF-κB, PPARγ, p53, and c-Myc427. Moreover, assessment of the acetylation status
of NF-κB in the liver indicated increased acetylation during HFD feeding (suggesting reduced
SIRT1 deacetylation), and considerably decreased acetylation during NMN administration (likely
reflecting increased SIRT1 activity).
NAMPT-mediated NAD synthesis is involved in many physiological processes, including
metabolism, energy balance, stress responses, circadian rhythm, and cell differentiation430,431.
Based on several studies, NAMPT-mediated NAD synthesis seems to be impaired during
oxidative stress and/or inflammation. This consequently contributes to decreased SIRT1 activity
and to the progression of T2DM420–424. Nevertheless, it remains unclear how changes in the

53
environment and nutritional context affect the network of NAMPT/NAD/SIRT1 pathways
(referred to as the “NAD World”431).
NAD affects several metabolic pathways which involve SIRT1. In addition, NAD levels
can affect the SIRT2-7 and PARP enzymes (Figure 7). For instance, increases in NAD levels
have been shown to increase the activities of mitochondrial sirtuins SIRT3–5. As impaired
mitochondrial sirtuin activity can lead to mitochondrial dysfunction, this seems to protect against
mitochondrial dysfunction and ROS generation432. PARPs, which are DNA repairing enzymes,
are also stimulated by NAD. With regard to beta cell function, PARP stimulation may not be
beneficial. This is because PARP-1-deficient mice were shown to be protected against cytokine-
induced islet cell death, which, however, may be due to increased NAD. However, PARP-1-
deficiency did not protect against cytokine-induced inhibition of insulin secretion433.
The importance of NAD in cell metabolism is demonstrated by the model of diabetes
which is induced by streptozotocin (STZ) administration in rodents434. STZ in blood plasma is
transported into beta cells via the GLUT2 glucose transporter. In the beta cell, STZ results in
significant DNA damage, leading to the excessive activation of the DNA-repair enzyme PARP.
As PARP consumes NAD during its DNA repair action, excessive PARP activity leads to a
depletion of NAD, which due to its necessary role in the TCA cycle, subsequently leads to a
deficiency in ATP. Consequently, the beta cells undergo necrosis434. Interestingly, the co-
administration of nicotinamide with STZ is known to produce a milder form of diabetes,
compared with STZ-only administration435,436. In this context, nicotinamide partially protects beta
cells by inhibiting PARP1 activity, consequently preventing the depletion of NAD and ATP in
STZ-exposed cells. In addition, as nicotinamide is a precursor to NAD, its administration also
results in increased intracellular NAD levels434,435.

54
Figure 7. Summary of the Nampt-mediated NAD synthesis, where the rate-limiting enzyme is Nampt. The
effects of NAD on enzymes other than SIRT1 are also depicted.
1.11.7 Potential Role of SIRT3
SIRT3 is an important mitochondrial protein deacetylase that regulates enzymes involved in
beta oxidation as well as ATP production437. SIRT3 is also known to regulate ROS production
and to exert anti-inflammatory effects438. As with SIRT1, caloric restriction has been shown to
increase SIRT3 protein levels in mice439, and a chronic HFD is associated with decreased SIRT3
mRNA levels440. Intriguingly, an acute HFD was shown to increase SIRT3 mRNA levels440. Very
interestingly, SIRT3 is known to be upregulated by a substrate of SIRT1: PGC-1α. A moderate
overexpression (~2.5 fold) of SIRT1 in skeletal muscle of rats was associated with an increase in
SIRT3 and PGC-1α expression441. Thus, it seems very possible that SIRT1 may upregulate SIRT3
expression via PGC-1α.
In fact, recent studies have been investigating the role of SIRT3 in metabolic disorders. A
study published in Diabetologia in 2013 assessed changes in SIRT3 expression in mouse islets
and INS1 cells incubated in IL1β and TNFα, and in islets isolated from patients with T2DM438.
The study found significantly decreased SIRT3 expression in mouse islets and INS1 cells, and in

55
the islets of type 2 diabetic patients. In addition, the study assessed the effects of SIRT3-
knockdown in INS1 cells. The authors reported a significant decrease in GSIS and in the
expression of beta cell genes, as well as a significant increase in beta cell apoptosis and
intracellular ROS and IL1β levels. Interestingly, the above study also revealed that SIRT3-
knockdown blocked the protective effects of NMN on beta cell function in INS1 cells incubated
in the proinflammatory cytokines. In addition, another study found that SIRT3-knockout mice
exhibited impaired glucose tolerance at 3 and 12 months of age when fed a HFD, and at 12
months of age when fed a standard diet439.
The above evidence suggests that an NMN-mediated increase in NAD levels may prevent
beta cell dysfunction by enhancing the activity of SIRT3 in addition to SIRT1. Nevertheless, there
are few studies regarding the role of SIRT3 in FFA-induced beta cell dysfunction per se,
compared with studies assessing SIRT1’s role. Thus, additional research is needed in order to
determine whether or not SIRT3 plays a complementary role to SIRT1 in mediating the protective
effects of NMN.
1.12 Potential Treatments for Lipid-Induced
Beta Cell Dysfunction
Dr. Adria Giacca’s laboratories and others have shown that therapies aimed at reducing
oxidative stress, ER stress, and inflammation have the potential to alleviate lipid-induced beta cell
dysfunction in animals and humans16.
As mentioned earlier, glucotoxicity in the presence of lipotoxicity accentuates beta cell
dysfunction. Nevertheless, this glucotoxicity-induced accentuation of FFA-induced beta cell
dysfunction seems to be reversible. A collaborative study by our lab showed that diabetic subjects
who undergo biliopancreatic diversion, which normalizes glycemia, exhibited similar beta cell

56
dysfunction, compared with IH-infused controls181. Thus, the diabetic subjects which were
chronically exposed to hyperglycemia did not demonstrate accentuated beta cell dysfunction after
their glycemia was normalized.
It is known that nonpharmacological weight-loss improves beta cell function and insulin
sensitivity via reducing plasma FFA levels442–444. Some studies have shown that the lowering of
plasma FFA improved GSIS only in diabetic patients with very low levels of Hb A1c, suggesting
that in diabetes which is not well-controlled, the damage to beta cell function may not be
reversible445. A collaborative study by our lab showed that increasing plasma FFA levels resulted
in a greater impairment of GSIS in obese, non-diabetic patients, compared with diabetic patients
with already impaired beta cell function185. However, obese humans185 and obese prediabetic rats
were found to be more susceptible to the effect of FFA on decreasing beta cell function, compared
with non-obese, non-diabetic humans or rats446.
It seems that the reduction of plasma FFA levels, such as by pharmacological intervention,
is beneficial in preventing and treating FFA-induced beta cell dysfunction. However, current
antilipolytic treatments, such as Acipimox447, are not very effective mainly due to their short half-
life and the common post-treatment rebound in FFA levels in overweight individuals.
Furthermore, current antilipolytic treatments have been known to sometimes cause adverse side
effects, such as insulin resistance16. Lastly, pharmacologically decreasing plasma FFA levels by
increasing net FFA uptake by adipocytes may not be beneficial in the long-run. This would be due
to the resulting increase in adiposity, which may exacerbate the negative effects of obesity, such
as complications from inflammation and metabolic disorders.
Based on many studies, including some done by our lab, focusing on the reduction of
oxidative stress, ER stress, and inflammation seems to be a more promising approach, compared
with decreasing FFA mobilization16,141,187,212,239,241,242,265,271,282,284,294,350,448,449. Previous research

57
done in our lab has shown that administration of the IKKβ inhibitor salicylate to rats i.v. infused
with oleate or 20% olive oil + heparin (50 U/ml) for 48h prevented FFA-induced beta cell
dysfunction (unpublished data). Beta cell function was assessed using hyperglycemic clamps (in
vivo). We had also observed this protective effect of salicylate ex vivo in islets isolated from rats
which had been i.v. infused with oleate or olive oil + heparin for 48h (unpublished data).
Another study found that pioglitazone (an anti-inflammatory TZD drug) and sodium
salicylate prevented an increase in apoptosis and partially protected against beta cell dysfunction
in human islets exposed to IL-1β or 33.3 mM of glucose (glucotoxicity)287. This was shown to
occur via pioglitazone and salicylate blocking the activation of NFκB by cytokines or
glucotoxicity287. Furthermore, a recent clinical trial suggests that preventing the activation of the
IL-1 receptor by using a synthetic antagonist (Anakinra) results in an improvement in beta cell
function, however, the largest improvement was observed in HbA1C levels450. Since Anakinra has
a short half-life of 4-6h and is a relatively weak antagonist, it is thought that using a stronger
antagonist with a longer half-life or inhibiting multiple targets in the inflammatory pathway may
yield a more therapeutic effect, compared with the use of Anakinra alone450. These results suggest
that oxidative stress and inflammation both play a role in FFA-induced beta cell dysfunction.
Currently, several insulin-sensitizing drugs seem to have beneficial side effects in treating
FFA-induced beta cell dysfunction. For example, besides improving insulin sensitivity, metformin
and TZDs decrease oxidative stress and islet inflammation. Metformin and TZDs also activate
AMP kinase, resulting in the depletion of triglycerides stored in islets451. The combination of the
aforementioned effects results in increased beta cell function in FFA-exposed rats452,453 and in
humans454,455. Thus, although metformin and TZDs are beneficial for treating insulin resistance
and beta cell dysfunction, their inhibitory effects are not specific to oxidative, ER, or
inflammatory stress. Elucidating the mechanisms of FFA-induced beta cell dysfunction may

58
allow for the development of more specific drugs for the prevention and/or treatment of beta cell
dysfunction.

59
Chapter 2
Rationale 2.1 Previous Results from the Giacca Lab
Small interfering ribonucleic acid (siRNA)-mediated and pharmacological inhibition of
SIRT1 activity were both found to decrease insulin transcription in INS-1 cells (rat beta cell
model456). This mimicked the effect of palmitate in vitro399. While SIRT1 activity may decrease
insulin transcription via the FOXO1-induced nuclear exclusion of Pdx-1, inhibition of SIRT1 may
decrease the FOXO1-mediated transcription of antioxidant enzymes, and thus increase
vulnerability to ROS-induced decrease in insulin gene transcription. This study reflected the dual
effects of FOXO1. The study also showed that SIRT1 activation by resveratrol administration
protected INS-1 cells from palmitate-induced beta cell dysfunction in vitro. Thus, decreased
SIRT1 activity may be causal to palmitate-induced beta cell dysfunction. Furthermore, another
study found that rats fed a HFD or FRD for 12 weeks exhibited a decrease in SIRT1 protein
expression in the pancreas and liver, whereas rats treated with caloric restriction showed an
increase in SIRT1 expression457.
Our laboratory aimed to investigate the potentially protective effect of SIRT1 on beta cells
in vivo in the context of high plasma levels of FFA. In hyperglycemic clamps in Wistar rats,
previous lab members found that i.v. co-infusion of resveratrol with oleate for 48h partially
protected against beta cell dysfunction induced by oleate in vivo (Figure 8). In hyperglycemic
clamps in mice, they found that BESTO mice are partially protected from oleate-induced beta cell
dysfunction in vivo (Figure 9).

60
Figure 8. Resveratrol, a SIRT1 activator, partially protects against FFA-induced beta cell
dysfunction in rats in vivo. Disposition index as assessed by two-step hyperglycemic clamps following
48h treatments. Rats were i.v. infused with saline (SAL; 0.5 μmol/min), oleate (OLE; 1.3 μmol/min), OLE
+ resveratrol (RSV; 0.025 mg/kg/min), or RSV only. Data are means ± SE. ¶ p vs. SAL and RSV < 0.05; ‡
p<0.01 vs. SAL. Adapted from Desai T., M.Sc. Thesis, Dr. Giacca Lab, Department of Physiology, 2013.
Figure 9. Beta cell-specific SIRT1 overexpressing (BESTO) mice were partially protected against
FFA-induced beta cell dysfunction in vivo, compared with wildtype mice. Disposition index as
assessed by one-step hyperglycemic clamps after 48h treatment. BESTO mice (TG) and C57BL/6 controls
(WT) were i.v. infused with saline (SAL) or oleate (OLE; 0.4 μmol/min). Data are means ± SE. ‡ p vs. WT
SAL and TG SAL < 0.01. Adapted from Desai T., M.Sc. Thesis, Dr. Giacca Lab, Department of
Physiology, 2013.
As SIRT1 activation prevented oleate-induced beta cell dysfunction, our lab hypothesized
that decreased SIRT1 activity was present in islets and was responsible for the oleate-induced
beta cell dysfunction. Thus, previous lab members performed an ex vivo study in which rats were

61
i.v. infused with treatments for 48h. Since SIRT1 is NAD-dependent, our lab investigated whether
or not NAD deficiency may be responsible for the oleate-induced decrease in SIRT1 activity. This
was done in collaboration with Dr. Jamie Joseph’s lab, based at the University of Waterloo. No
significant difference in NAD and NADH levels or ratios between any of the treatment groups
was observed (Figure 10A & B). As a previous study had reported that palmitate decreases
SIRT1 mRNA levels399, our lab measured SIRT1 mRNA levels using RT-PCR. This was done in
collaboration with Dr. Michael Wheeler’s lab. Preliminary experiments suggest that oleate might
not affect SIRT1 mRNA levels in rats (Figure 10C). Our lab’s current hypothesis is that SIRT1
activity or protein level in the beta cell is affected by FFA independently of NAD levels;
however, this remains to be investigated.

62
Figure 10. Islets of Wistar rats i.v. infused with oleate did not demonstrate decreased NAD
bioavailability, compared with the saline-infused control. (A & B) Unaltered NAD and NADH levels
and ratios in rat islets indicate that the oleate-induced decrease in SIRT1 activity does not seem to be
mediated by decreased NAD bioavailability. (C) Preliminary qRT-PCR-measured mRNA expression of
SIRT1 (relative to Histone H3a mRNA) in rat islets suggest that oleate does not decrease SIRT1
transcription. Data are means ± SE. Data in A and B were obtained by Dr. Jamie Joseph’s lab, University
of Waterloo. Data in C were obtained by Desai T. in our lab.
C
A
. B
.

63
2.2 My Experimental Design
It has been shown that administration of NMN, which is a key intermediate of NAD
biosynthesis, restores NAD levels and increases GSIS and glucose tolerance in HFD-fed C57BL/6
mice in vivo424 (Figure 11). NMN was administered to C57BL/6 mice via intraperitoneal
injection at 500 mg/kg/day for 10 days.
Figure 11. Glucose tolerance and plasma levels of insulin, cholesterol, triglycerides, and free fatty
acids of mice fed a high-fat-diet (HFD) and treated with nicotinamide mononucleotide (NMN). (A)
Glucose tolerance in high fat diet (HFD)-fed male mice before and after NMN treatment. Intraperitoneal
glucose tolerance tests (IPGTT) were conducted on mice before and after treatment with NMN for 10
consecutive days (500 mg/kg body weight/day). The Area Under the Curve (AUC) is presented next to the
graph. (B) Plasma insulin levels during IPGTT before and after NMN treatment. (C) Cholesterol (Chol),
triglycerides (TG), and FFA levels in aged, HFD-fed female mice before and after NMN infusion. Data are
means ± SEM. ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001. Adapted from Yoshino J et al. 2011. Cell Metab 14:
528-536.
A
.
B C

64
Mainly based on the previous results of our lab, this thesis will test the hypothesis that
NMN administration would counteract oleate-induced beta cell dysfunction in vivo in mice.
Although NAD levels were shown to have not been decreased in a previous study of ours,
increasing NAD levels should still stimulate SIRT1 activity if SIRT1’s activity is low. Therefore,
I investigated the effects of NMN infusion on oleate-induced beta cell dysfunction in C57BL/6
mice in vivo. Male, 11 – 13 wk old mice, cannulated at the jugular vein, were i.v. infused with
saline (SAL), oleate (OLE), NMN + OLE, or NMN only, for 48h. The mice then underwent a
hyperglycemic clamp assessing beta cell function in vivo.
NMN administration is an alternative method of SIRT1 activation that does not have the
same drawbacks as resveratrol infusion, which has non-specific antioxidant effects, and the
BESTO mouse model, which has a high, non-physiological level of SIRT1 expression (~50 fold).
In addition, as NMN is produced endogenously, the administration of NMN may be considered a
nutriceutical approach of treating T2DM424. A caveat of this approach is that NAD, the levels of
which are elevated by NMN administration, is involved in many physiological processes, and
therefore would have non-specific effects besides increasing SIRT1 activity.
In Summary:
My Hypothesis: NMN administration would counteract oleate-induced beta cell dysfunction
in mice in vivo.
o Aim 1: To investigate the role of SIRT1 in FFA-induced beta cell dysfunction in vivo
without the non-specific effects of resveratrol and the excessive overexpression of SIRT1.
o Aim 2: To investigate the potential effects of NMN (not necessarily specific to SIRT1) on
the metabolism of glucose and plasma FFA in vivo.

65
Chapter 3
Materials and Methods
Note: The following procedures were performed in the same manner performed by previous lab
members56.
3.1 Animal Models
Wildtype, male, C57BL/6 mice at 11 – 13 weeks of age were utilized. The mice were
housed in the Department of Comparative Medicine at the University of Toronto, under a 12h
light/dark cycle. All mice were fed a rodent diet which consisted of 25% protein (percent of
energy), 58% carbohydrate, and 17% fat (LM-485, Harland Teklad Global Diets, Madison, WI,
USA). Mice were allowed to reach 11 – 13 weeks of age before being utilized in our studies.
Littermates of experimental groups were used as controls.
3.2 Mouse Cannulation Surgery
All procedures were performed in accordance with the Canadian Council of Animal Care
Standards and were approved by the Animal Care Committee of the University of Toronto. Under
isoflurane anesthesia and sterile conditions, 11 - 13 wk old, male, C57BL/6 mice underwent
jugular vein cannulation surgery. The left jugular vein was cannulated with a catheter consisting
of two parts: a long polyethylene tubing (PE-10; Cay Adams, Boston, MA, USA) and a shorter
silastic tubing (length of 1.5 cm; Dow Corning, Midland, MI, USA). Only the silastic tubing
portion (which was soft and elastic to minimize vessel damage) was inserted inside the jugular
vein. The catheter was exteriorized by running through a subcutaneous tunnel (created using a
16G needle) and emerging at the back of the neck. This was done to protect the catheter from
being bitten by the mouse. The catheter was filled with heparinized saline (40 units/ml) in order to
prevent blood clots. The catheter was subsequently tied at its free end and wrapped with tape for

66
additional protection. Post-surgery, every cannulated mouse was housed individually and
provided with a recovery period of 3 – 5 days before i.v. infusion.
3.3 Treatment Infusion in Mice
Prior to i.v. infusion, each cannulated mouse was fitted with a polyethylene harness that
allowed the mouse’s catheter to pass through a metal, protective tether and attach to a swivel
placed above the cage. This allowed the mice freedom of movement without risking damage to
the cannula. Mice were i.v. infused via their catheters with SAL, OLE (0.4 μmol/min),
NMN+OLE (0.025 mg/kg body weight/min of NMN, as performed in previous studies424,458–460),
or NMN alone, using syringe infusion pumps for 48h. Oleate was infused while bound to BSA
(according to the Bezman-Tarcher method461) at a dose that elevates plasma FFA levels by 1.5 – 2
fold, simulating the pathophysiological levels present in obesity56,201,205,212,462. The binding of
BSA to oleate simulates physiological conditions and protects the mice from the detergent effects
of oleate. This allows the i.v. infusion of the oleate FFA into animals461. The OLE and NMN
infusates were freshly prepared and were protected from light, as had been performed in our
previous studies56,205,463,464. The pH of infusates was adjusted to 7.4 ± 0.05 prior to i.v. infusion.
Mice had ad libitum access to standard rodent chow and water. Whole blood samples were
taken at 0h and 46h of infusion via the tail vein (immediately prior to commencing the
hyperglycemic clamp, which is described below). Immediately after collection, the whole-blood
samples were centrifuged in order to obtain the plasma samples of FFA, insulin, and C-peptide.
3.4 One-Step Hyperglycemic Clamp
Mice were fasted (but had access to water) for 4 hours prior to beginning the two-hour-
long hyperglycemic clamp at 46h of i.v. infusion. Twenty minutes before initiating the
hyperglycemic clamp, a sample of blood was taken from each mouse in order to establish basal

67
plasma levels of glucose, FFA, insulin, and C-peptide. Beta cell function was assessed in
conscious mice using a one-step hyperglycemic clamp without interrupting the i.v. infusion of
treatments. This method mainly analyzes the rise in insulin and C-peptide levels in response to
elevated plasma glucose levels. Glucose was i.v. infused via a Y-shaped connector at the catheter
at 37.5% (g/ml) concentration in order to gradually elevate plasma glucose levels to ~22 mmol/L
(which is the maximum stimulatory level).
Glycemia was assessed every 5-10 minutes by measuring a drop of blood from the tail
using a HemoCue Glucose 201+ System (HemoCue, Lake Forest, CA, USA). Minimal blood
volume was collected in order to reduce the risk of anemia. By the end of the experiment, a
maximum total of 0.3 ml of blood was collected from each mouse. Once glycemia was
approximately 22 mmol/L, the plasma glucose levels were maintained, i.e. “clamped”, for ~30
minutes. This was done by varying the infusion rate of glucose according to the glycemia
readings obtained every 5-10 minutes. After maintaining glycemia at an equilibrium of ~22
mmol/L, a blood sample was obtained for plasma levels of FFA, insulin, and C-peptide.
At the end of the experiments, mice were anesthetized via an i.v. infusion of
ketamine:xylazine:acepromazine (87:1.7:0.4 mg/ml, 1 ul/g of body weight). The liver and soleus
muscles were collected, snap-frozen in liquid nitrogen, and stored at -80°C for future analyses. In
addition, the mouse pancreases were immediately fixed in formalin over 24h, and then transferred
to a 70% ethanol solution. The samples were embedded in paraffin within 7 days of collection.
Measurements
3.5 Glycemia
The concentration of glucose in plasma samples of mice were measured using the HemoCue
Glucose 201+ System. A very small volume of blood (~5 µL) per sample was required by the
machine. Upon placing a blood sample in the HemoCue microcuvette, saponin hemolyzes the

68
erythrocytes, and the mutarotase enzyme converts α-D-glucose to β-D-glucose. Glucose
dehydrogenase (GDH) then catalyzes the oxidation of β-D-glucose in the presence of NAD,
resulting in the formation of NADH. This production of β-D-glucose and NADH has a molar
relationship to the glucose concentration of the sample. Subsequently, diaphorase catalyzes the
oxidation of NADH in the presence of a specific tetrazolium salt (MTT chromogen). This results
in a redox reaction by which the tetrazolium salt is converted to a colored formazan. The
concentration of the formazan is then quantified photometrically at 660 nm and 840 nm in order
to determine the plasma glucose concentration of the sample.
3.6 Plasma Insulin Levels
Plasma insulin levels were measured using an ELISA kit (Antibody and Immunoassay
Services, Li Ka Shing Faculty of Medicine, University of Hong Kong, Hong Kong). A 96-well
microplate was pre-coated with a monoclonal antibody against insulin. Insulin standards of
known concentrations (0, 34.5, 86, 172, 345, 603, and 1210 pM) and the plasma samples were
added to wells in duplicates. Next, an insulin-specific monoclonal antibody conjugated to
horseradish peroxidase (HRP) was added to each well, and the plate was incubated at room
temperature with shaking at 600 rpm for 90 minutes. The HRP-conjugated antibody binds to
insulin that was already bound by the antibody which was anchored to the wells. This effectively
anchors a certain amount of HRP-conjugated antibody to the wells. Subsequently, the wells were
washed with washing buffer in order to remove all substances that were unbound to the wells. A
chromogenic substrate of HRP, 3,3',5,5'-tetramethylbenzidine (TMB), was added, and the mixture
was protected from light. After 15 minutes of incubation at room temperature, a solution which
stops the reaction between TMB and HRP was added. Immediately afterwards, the concentration
of HRP-antibody was visualized at 450 nm using a microplate reader.

69
During every assay, a new standard curve was generated using the insulin standards that
were pipetted in the microplate in duplicate. As the increase in light absorbance from each well is
directly proportional to the concentration of insulin, the levels of insulin in the plasma samples
were determined using the standard curve. The sensitivity of the assay is 34.5 pM, and the
interassay coefficient of variation (CV) determined on reference plasma is less than 10%.
3.7 Plasma C-Peptide Levels
Plasma C-peptide levels were measured using an ELISA kit (ALPCO Diagnostics, Salem,
NH, USA). The kit’s protocol was identical to that of the insulin ELISA kit described above, with
exception that the antibodies used were specific to C-peptide instead of insulin. The sensitivity of
the assay is 7.6 pM, and the interassay CV is less than 10%.
3.8 Plasma FFA Levels
Plasma FFA levels were measured using a colorimetric kit (Wako and Boehringer
Chemicals, Neuss, Germany). Catalyzed by acyl-CoA synthetase (ACS), plasma FFAs acylate
coenzyme A, resulting in the formation of acyl-CoA. Acyl-CoA is then oxidized by the action of
acyl-CoA oxidase, producing H2O2. Subsequently, H2O2 is used by the enzyme peroxidase (POD)
to drive the oxidative condensation of 3-methyl-N-ethyl-N-(B-hydroxyethyl)-aniline (MEHA)
with 4-aminophenazone. This reaction results in the production of a purple coloured adduct, the
concentration of which is then measured colorimetrically at 550 nm with a variability of 1.1%.
The above reactions are summarized below:
𝐹𝐹𝐴 + 𝐴𝑇𝑃 + 𝐶𝑜𝐴𝐴𝐶𝑆→ Acyl-CoA + 𝐴𝑀𝑃 + 𝑃𝑃𝑖
Acyl-CoA + 𝑂2Acyl-CoA oxidase→ 2,3-trans-Enoly-CoA + 𝐻2𝑂2
2 𝐻2𝑂2 + 4-aminoantipyrine + MEHA 𝑃𝑂𝐷→ Purple adduct + 3 𝐻2𝑂

70
3.9 Western Blotting
Mouse liver samples were lysed in RIPA buffer containing protease and phosphatase
inhibitors (Roche). 7 µg of protein lysate from the liver samples were separated across a 7% SDS-
PAGE (sodium dodecyl sulfate polyacrylamide gel electrophoresis) gel. The proteins were
transferred to a polyvinylidene fluoride (PVDF) membrane, and then immunoblotted with a
custom-made rabbit polyclonal primary antibody specific to α-CEACAM1 (1:500; Ab-2457,
Abcam). After washing the membranes, a secondary antibody specific to the primary antibody
was applied (1:5,000; LiCOR Biosciences, Lincoln, NE, USA). After washing, bands of light
produced from the secondary antibodies were visualized. In order to assess the levels of the
loading control tubulin, the membranes were stripped of antibodies, washed, and then reprobed
with a monoclonal antibody against tubulin (1:500; Santa Cruz Biotechnology). The membranes
were then washed and probed with secondary antibody as performed previously. The different
band densities were quantified using the ImageJ software and normalized to total protein content.
The western blotting procedure was performed by Ms. Hilda Ghadieh in Dr. Sonia Najjar’s lab
(University of Toledo, Toledo, OH, USA).
3.10 Insulin Sensitivity Index
The insulin sensitivity index (glucose metabolism value/[insulin]; abbreviated as M/I
where M is GINF + change in plasma glucose pool during an imperfect clamp) was first defined
by Dr. Ralph A. DeFronzo in 1979 at Yale University (New Haven, CT, USA)465. In the condition
that hyperglycemia is at a steady-state and is similar between all experimental groups (which is
our case), the sensitivity index can be calculated by dividing the average glucose infusion rate
(GINF; normalized for body weight) by the plasma insulin concentration during the
hyperglycemic clamp465. This is summarized by the following formula:

71
M/I =Steady-Stat𝒆 𝑮𝑰𝑵𝑭
[𝑰𝒏𝒔𝒖𝒍𝒊𝒏]
M/I is expressed as deciliter per kilogram per minute per microunit per milliliter. This
equation assumes that the insulin-induced change in glucose uptake is proportional to the plasma
concentration of insulin, which is not always the case466.
3.11 Disposition Index
Beta cell function was assessed during the hyperglycemic clamp by using the established
index of relative insulin secretion, the Disposition Index (DI). The DI was used instead of
absolute insulin secretion because the DI accounts for compensatory hyperinsulinemia induced by
changes in insulin sensitivity whereas absolute insulin secretion does not.
The DI was calculated as the product of the index of insulin sensitivity (M/I) and the
concentration of C-peptide in plasma. Plasma levels of C-peptide, as opposed to the insulin
secretion rate, were used since the kinetics of C-peptide (which are necessary for calculation of
insulin secretion rate) are unknown in rodents because C-peptide (species-specific) is not
available for injection and C-peptide kinetics have only been studied in humans and dogs467,468.
The DI has been used in many of our previous studies168,177,180,181,183,184,205,240,449,469,470. The
formula used in the calculation of the DI is depicted below:
𝑫𝑰 = 𝑴/𝑰 ∗ [C-peptide]
3.12 Insulin Clearance Index
The index of endogenous insulin clearance was calculated as the ratio of C-peptide to
insulin plasma levels during basal glycemia and during the hyperglycemic clamp. The ratio of C-
peptide to insulin plasma levels is an established index of the insulin clearance rate465. In cases of
increased insulin clearance rate, the ratio of plasma C-peptide to insulin would be increased as

72
insulin is removed at a higher rate, compared with that of C-peptide (which is cleared via a
different mechanism at a constant rate). By the same logic, a reduction in the insulin clearance
rate would result in a decrease in the ratio of plasma C-peptide to insulin levels. The equation
used to calculate the insulin clearance index is:
𝑰𝒏𝒔𝒖𝒍𝒊𝒏 𝑪𝒍𝒆𝒂𝒓𝒂𝒏𝒄𝒆 𝑰𝒏𝒅𝒆𝒙 =[C-peptide]
[𝑰𝒏𝒔𝒖𝒍𝒊𝒏]
3.13 Statistics
One-way non-parametric analysis of variance (ANOVA) followed by Tukey’s t-test was
used to assess statistical significance between different groups. Data are presented as means ±
standard error (SE). Calculations were performed using the Statistical Analysis System software
(SAS; Cary, NC, USA).

73
Chapter 4
Results
Glucose was i.v. infused into the mice in order to measure the DIs of the beta cells at a
similar degree of hyperglycemia. Prior to the beginning of i.v. glucose infusion, glycemia (basal)
was slightly lower in the NMN+OLE group, compared with the SAL (p < 0.04) and NMN (p <
0.001) groups (Figure 12, below). The OLE group exhibited mildly lower basal glycemia,
compared with the NMN group (p < 0.02). The blood glucose levels were elevated by the 37.5%
glucose infusion to a steady state that was similar between all groups (~22 mM). There was no
significant difference in glycemia between any two groups during the last 30 minutes of the clamp
(Figure 12). The elevation of glycemia during the entire clamp in the NMN+OLE group was
slower than those of the OLE (p < 0.04) and NMN (p < 0.01) groups even though the NMN+OLE
group was i.v. infused with glucose at a significantly higher rate compared with all other groups
(Figure 13). Thus, the NMN+OLE group’s resistance to hyperglycemia, coupled with its
relatively high GINF, compared with the other groups, reflects improved glucose tolerance. This
is consistent with our hypothesis.

74
Figure 12. Gradual elevation in glycemia of wildtype mice i.v. infused with 37.5% glucose during the
hyperglycemic clamp. Male, 11-13 week old, C57BL/6 mice were i.v. infused for 48h with SAL, OLE
(0.4 µmol/min), NMN+OLE (0.025 mg/kg body weight/min of NMN), or NMN alone. After 4h of fasting
at 42h of infusion, the hyperglycemic clamp was initiated at 46h without interrupting the administration of
treatments. Hyperglycemia was maintained during the last 30 minutes of the clamp. ¶ p SAL vs
NMN+OLE during basal < 0.04; ‡ p NMN+OLE vs NMN during basal < 0.001 and during glucose
infusion < 0.01; ¥ p OLE vs NMN during basal < 0.02; † p OLE vs NMN+OLE during glucose infusion
< 0.04. Data are means ± SE.
The glucose infusion rate (GINF) required for maintaining hyperglycemia is a reflection
of glucose tolerance. As expected, the average GINF required for maintaining a steady-state of
hyperglycemia for 30 minutes was significantly lower in the OLE group, compared with the SAL
group (Figure 13 A&B, below). Remarkably, mice co-infused with NMN+OLE had a substantial
increase in GINF, compared with the OLE (p < 0.001) or SAL group (p < 0.03). Interestingly, the
infusion of NMN in the absence of elevated FFA resulted in a significant decrease in GINF,
compared with SAL. The average GINF for the groups over the entire period of i.v. glucose
infusion (Figure 13 C) had a very similar pattern to the average GINF over the last 30 minutes of
the clamp (Figure 13 B).

75
Figure 13. Glucose infusion rate (GINF) required for obtaining and maintaining hyperglycemia in
mice. Co-infusion of NMN + OLE in C57BL/6 mice for 48h substantially improved glucose tolerance,
compared with infusion of OLE or SAL. C57BL/6 mice were i.v. infused for 48h with SAL, OLE (0.4
µmol/min), NMN+OLE (0.025 mg/kg body weight/min of NMN), or NMN alone. (A) Glucose tolerance
was reflected by the GINF required for obtaining and maintaining hyperglycemia. Comparison of the
average GINF required for maintaining hyperglycemia for (B) the last 30 minutes of the clamp and for (C)
the entire i.v. glucose infusion period. * p SAL vs OLE < 0.04; † p OLE vs NMN+OLE < 0.001 (for B
& C); ‡ p NMN+OLE vs NMN < 0.001 (for B & C); ¶ p SAL vs NMN+OLE < 0.03 (for B & C); # p
SAL vs NMN < 0.001 (for B) and < 0.01 (for C). Data are means ± SE.
A.
B. C.

76
The plasma concentration of insulin was measured in order to calculate the Insulin
Sensitivity Index (M/I = Steady-State GINF/[Insulin]), the DI (which is M/I * [C-peptide]), and
the Insulin Clearance Index (which is [C-peptide]/[Insulin]). Plasma insulin levels were similar
between the SAL and OLE groups prior to i.v. glucose infusion (basal glycemia, which was after
4 hours of fasting) and during the hyperglycemic clamp (Figure 14). While insulin levels were
similar between the SAL and OLE groups during hyperglycemia, the GINF required by the OLE
group was lowered due to oleate-induced insulin resistance, as will be shown in Figure 17.
During basal glycemia, the plasma concentration of insulin was significantly higher in the
NMN+OLE group, compared with the SAL group. During hyperglycemia, plasma insulin levels
in the NMN+OLE group were more than twice as high as those in the other groups. The insulin
concentration of the NMN group was not significantly different from that of the SAL or OLE
groups during both basal glycemia and hyperglycemia.
Figure 14. Plasma insulin levels prior to i.v. glucose infusion (basal glycemia) and after the
maintenance of hyperglycemia (clamp) for ~30 minutes in C57BL/6 mice. Mice were i.v. infused for
48h with SAL, OLE (0.4 µmol/min), NMN+OLE (0.025 mg/kg body weight/min of NMN), or NMN
alone. Administration of treatment was maintained during the hyperglycemic clamp experiments. † p OLE
vs NMN+OLE < 0.01; ‡ p NMN+OLE vs NMN <0.001; ¶ p SAL vs NMN+OLE < 0.04 during basal
and < 0.001 during clamp. Data are means ± SE.

77
The plasma concentration of C-peptide was measured in order to determine absolute insulin
secretion (not controlling for insulin resistance), the DI (which is M/I * [C-peptide]), and the
Insulin Clearance Index (which is [C-peptide]/[Insulin]). During basal glycemia, plasma C-
peptide levels tended to be lower in the OLE and NMN+OLE groups, compared with the SAL
group, although they were not statistically significant (Figure 15). During the hyperglycemic
clamp, the NMN+OLE group had a significantly greater C-peptide level, compared with the OLE
and NMN groups. However, this increase in C-peptide level was not proportional to the increase
in insulin levels in the NMN+OLE group, compared with the other groups.
Figure 15. Plasma C-peptide levels prior to i.v. glucose infusion (basal glycemia) and after the
maintenance of hyperglycemia (clamp) for ~30 minutes in C57BL/6 mice. Mice were i.v. infused for
48h with SAL, OLE (0.4 µmol/min), NMN+OLE (0.025 mg/kg body weight/min of NMN), or NMN
alone. Administration of treatment was maintained during the hyperglycemic clamp experiments. † p OLE
vs NMN+OLE < 0.01; ‡ p NMN+OLE vs NMN < 0.04. Data are means ± SE.

78
During the hyperglycemic clamp, OLE infusion resulted in a significant decrease in the
Insulin Clearance Index (which is [C-peptide]/[Insulin]), compared with SAL infusion (Figure
16). However, during basal glycemia, OLE infusion did not significantly decrease insulin
clearance, compared with SAL infusion. Interestingly, the co-infusion of NMN+OLE resulted in a
significant decrease in insulin clearance during basal glycemia and hyperglycemia, compared with
SAL infusion. Thus, NMN accentuated the oleate-induced decrease in insulin clearance in the
context of elevated FFA levels, although both the OLE and NMN+OLE groups significantly
decreased insulin clearance during hyperglycemia. As NMN infusion on its own did not
significantly alter insulin clearance, the effect of NMN on insulin clearance seems to be specific
to the context of elevated plasma levels of FFA.
Figure 16. Insulin Clearance Indices prior to i.v. glucose infusion (basal glycemia) and after the
maintenance of hyperglycemia (clamp) for ~30 minutes in C57BL/6 mice. Mice were i.v. infused for
48h with SAL, OLE (0.4 µmol/min), NMN+OLE (0.025 mg/kg body weight/min of NMN), or NMN
alone. Administration of treatment was maintained during the hyperglycemic clamp experiments. * p SAL
vs OLE < 0.05; ‡ p NMN+OLE vs NMN < 0.05 during basal and < 0.001 during clamp; ¶ p SAL vs
NMN+OLE < 0.04 during basal and < 0.001 during clamp. Data are means ± SE.

79
As expected, oleate infusion resulted in a significant decrease in the Insulin Sensitivity
Index (M/I = Steady-State GINF/[Insulin]), compared with SAL infusion (Figure 17). NMN
infusion with or without OLE did not significantly alter insulin sensitivity, compared with the
SAL and OLE groups. Thus, NMN in the context of elevated plasma FFA levels seems to have
overcome insulin resistance through hyperinsulinemia, evidently resulting in a substantial
improvement in glucose tolerance (Figure 13).
Figure 17. Insulin Sensitivity Indices (M/I) obtained after the maintenance of hyperglycemia (clamp)
in C57BL/6 mice for ~30 minutes. Mice were i.v. infused for 48h with SAL, OLE (0.4 µmol/min),
NMN+OLE (0.025 mg/kg body weight/min of NMN), or NMN alone. Administration of treatment was
maintained during the hyperglycemic clamp experiments. * p SAL vs OLE < 0.04; ¶ p SAL vs
NMN+OLE < 0.01. Data are means ± SE.

80
To assess beta cell function in vivo, the DI is typically evaluated as it controls for potential
changes in insulin sensitivity and thus more accurately represents beta cell function, compared
with absolute insulin secretion471. Consistent with our expectations, OLE infusion decreased beta
cell function in mice, compared with SAL infusion (Figure 18, below). NMN+OLE co-infusion
resulted in a DI that was not significantly different, compared with both SAL and OLE groups.
Hence, NMN+OLE co-infusion resulted in an intermediate DI, suggesting partial protection from
FFA-induced beta cell dysfunction.
It is worth noting that, had insulin clearance not changed, the improvement in DI of the
NMN+OLE group relative to that of the OLE group could have been higher because of the
suppressive effects of hyperinsulinemia on insulin secretion in the NMN+OLE group, compared
with the OLE group472. The hypothesis that beta cell function was improved by NMN in the
context of elevated plasma levels of FFA is supported by the significantly higher C-peptide levels
(indicator of insulin secretion) in the NMN+OLE group, compared with the OLE group. Indeed,
the improvement in DI was less than that in C-peptide because of the slightly lower insulin
sensitivity in the NMN+OLE group, compared with the OLE group. Mice infused with NMN in
the absence of elevated FFA levels exhibited a significantly lower DI, compared with the SAL
group.

81
Figure 18. Disposition Indices obtained after the maintenance of hyperglycemia (clamp) in C57BL/6
mice for ~30 minutes. Mice were i.v. infused for 48h with SAL, OLE (0.4 µmol/min), NMN+OLE (0.025
mg/kg body weight/min of NMN), or NMN alone. Administration of treatment was maintained during the
hyperglycemic clamp experiments. * p SAL vs OLE < 0.01; # p SAL vs NMN < 0.04. Data are means ±
SE.

82
The plasma concentration of FFA was measured in order to verify the intended plasma
FFA levels in each group as well as to assess the potential effects of NMN on plasma FFA levels.
48h i.v. infusion of OLE resulted in a 1.5 – 2 fold elevation of FFA levels, compared with SAL
infusion (Figure 19). Interestingly, co-infusion of NMN resulted in a significant decrease in
plasma FFA levels, compared with the OLE group, and NMN alone had a similar trend compared
with the SAL group. These results are consistent with previous findings published in Cell
Metabolism424. Thus, it seems that NMN has a significant FFA-lowering effect in the context of
elevated FFA levels.
At the end of the hyperglycemic clamps, plasma FFA levels in all groups had moderately
decreased, compared with their levels prior to the commencement of the clamp (basal glycemia).
This decrease in FFA levels is expected and is due to hyperinsulinemia increasing FFA uptake and
decreasing lipolysis by adipocytes473. As the NMN+OLE group exhibited higher plasma levels of
insulin, compared with the other groups, its relatively greater decrease in FFA levels is logical.
Figure 19. Plasma FFA levels of mice during basal glycemia (after 4 h of fasting and prior to glucose
infusion) and during hyperglycemia (after ~30 minutes at steady-state). Wildtype mice were i.v.
infused for 48h with SAL, OLE (0.4 µmol/min), NMN+OLE (0.025 mg/kg body weight/min of NMN), or
NMN alone. * p SAL vs OLE < 0.001; † p OLE vs NMN+OLE < 0.04; ‡ p NMN+OLE vs NMN <
0.001; ¶ p SAL vs NMN+OLE < 0.01; ¥ p OLE vs NMN < 0.02. Data are means ± SE.

83
Since we unexpectedly found a decrease in insulin clearance in the NMN + OLE group
versus the OLE group alone, we collaborated with a renowned expert in CEACAM biology, Dr.
Sonia Najjar (University of Toledo), in order to measure CEACAM1 protein levels in livers of
mice belonging to our treatment groups. As shown in Figure 20 (below), CEACAM1 protein
expression was significantly decreased in the NMN+OLE group, compared with controls.

84
Figure 20. Western blots of CEACAM1 (Cc1) performed on livers of mice infused with SAL, OLE,
NMN+OLE, or NMN for 48h. 7 µg of protein lysates from each liver were separated using 7% SDS-
PAGE gel. Proteins were immunoblotted (Ib) with polyclonal antibodies against α-CEACAM1 (1:500, Ab-
2457) and reimmunoblotted (reIb) with monoclonal antibodies against Tubulin (loading control; Santa
Cruz Biotech). Proteins were visualized using LiCOR secondary antibodies according to manufacturer’s
instructions (LiCOR Biosciences, Lincoln, BE). Protein band density was quantified using Image J.
Analysis was performed using one-way ANOVA. Mouse treatment and liver collection were performed by
A.N.; western blotting for CEACAM1 was carried out by Ms. Hilda Ghadieh, at Dr. Sonia Najjar’s lab,
University of Toledo. * p SAL vs NMN+OLE < 0.05; ¶ p NMN+OLE vs NMN < 0.05. Data are means ±
SE.

85
Chapter 5
Discussion
In C57BL/6 mice, we have obtained sufficient evidence supporting the notion that NMN
administration in the context of elevated plasma FFA levels substantially improves glucose
tolerance. Interestingly, NMN administration in the context of normal plasma levels of FFA had
an opposite effect on glucose tolerance. As NMN is metabolized into NAD, which is involved in
numerous physiological processes, the mechanisms behind the dual effects of NMN
administration are not clear. Nevertheless, there are a several possibilities that may explain these
results. These possibilities are described in the next few pages.
Our hyperglycemic clamps have demonstrated that NMN administration in the context of
elevated plasma FFA levels accentuated the FFA-induced decrease in insulin clearance. This was
evident by the co-infusion of NMN with OLE resulting in a significant difference in insulin
clearance, compared with the SAL group. This was in contrast to the OLE group not being
significantly different in insulin clearance, compared with the SAL group during basal glycemia.
In addition to substantially improving glucose tolerance, decreased insulin clearance may relieve
beta cell overload by helping overcome insulin resistance, thus slowing the deterioration of beta
cell function.
The substantial decrease in insulin clearance in the NMN+OLE group, compared with the
OLE group, may have been due to decreased CEACAM1 expression in the NMN+OLE group.
Indeed, Western blots of CEACAM1 which were produced in collaboration with Dr. Najjar’s lab
support our hypothesis that NMN administration decreased CEACAM1 expression in the liver in
the context of elevated plasma FFA levels (Figure 20); however, NMN resulted in no significant
difference in the context of normal FFA levels, compared with controls. NMN administration

86
results in increased NAD availability, which consequently increases SIRT1 activity. Thus, the
NMN+OLE-induced decrease in CEACAM1 expression may be due to increased SIRT1 activity
and/or other pathways affected by NAD.
Since OLE infusion decreased beta cell function, and since NMN+OLE co-infusion did
not result in a significant decrease in DI, compared with SAL infusion, NMN+OLE co-infusion
partially rescued beta cell function. As mentioned earlier, the DI of the NMN+OLE group could
have been higher than reported had insulin secretion not been suppressed by hyperinsulinemia
(due to decreased insulin clearance) or had insulin sensitivity (M/I) not been slightly (although
not significantly) lower, compared with the OLE group (since DI = M/I * [C-peptide]).
Intriguingly, NMN infusion in the presence of normal plasma FFA levels significantly decreased
DI, compared with the SAL group. Consistent with our results, a 2008 study has reported a
decrease in glucose tolerance and insulin secretion (assessed using an IPGTT) after NMN
administration in 20-month-old male mice fed a normal diet, compared with saline
administration458.
After 4h of fasting and before the hyperglycemic clamp, the insulin concentration in the
NMN+OLE group tended to be higher than those of the other groups due to decreased insulin
clearance. The aforementioned three parameters: decreased insulin clearance, increased beta cell
function, and elevated basal insulin levels seem to have collectively resulted in high levels of
plasma insulin during the hyperglycemic clamps. Although oleate-induced insulin resistance was
not ameliorated, the over-two-fold elevation of plasma insulin concentration in the NMN+OLE
group resulted in a considerable improvement in glucose tolerance.
Interestingly, NMN infusion in the context of normal FFA levels decreased beta cell
function, compared with the SAL group. Consistently, the NMN-only group tended to have lower
plasma levels of insulin, compared with the SAL and OLE groups. Although NMN did not

87
significantly alter insulin sensitivity, the decrease in beta cell function seems to have significantly
decreased glucose tolerance, compared with the SAL group.
5.1 Potential Mechanisms Behind NMN’s Effects on
Insulin Clearance
With regards to insulin clearance, the mechanisms are relatively challenging to explore as
insulin uptake and degradation are complex, are not well-understood, and involve multiple
tissues. As described earlier, insulin clearance occurs mainly in hepatocytes via CEACAM1-
mediated insulin-insulin-receptor complex endocytosis followed by IDE-mediated endosomal
degradation. Currently, there is very little research available connecting NMN metabolism with
CEACAM1 regulation.
As described earlier, insulin clearance is known to be decreased by elevated plasma FFA
levels and liver fat content462,474. Nevertheless, in our study, the accentuation of the decrease in
insulin clearance in the NMN+OLE group occurred despite a significant decrease in FFA levels,
compared with the OLE group. This finding indicates that the accentuation of the FFA-induced
decrease in insulin clearance in the NMN+OLE group was not caused by the change in FFA
levels, but by the co-infusion of NMN.
5.1.1 Synergistic Effects of SIRT1 and FFA on PPARα-Mediated Decrease in
CEACAM1 Expression
Long-chain FFA, such as oleate, are activating ligands for PPARα475–479, which is highly
expressed in the liver and directly decreases CEACAM1 transcription, as will be explained below.
A study found that treatment of cultured hepatoma cells with a PPARα agonist (Wy14,643)
resulted in decreased promoter activity of rat and mouse Ceacam1, compared with controls480. In
the same study, treatment of hepatoma cells with Wy14,643 also resulted in a rapid decrease in

88
CEACAM1 mRNA and protein levels. In Pparα+/+ mice, but not Pparα-/- mice, supplementing a
chow diet with Wy14,643 resulted in a decrease in hepatic CEACAM1 mRNA and protein levels,
and revealed that ligated PPARα was bound to the Ceacam1 promoter in liver lysates480.
As described earlier in my thesis, one of the main targets of deacetylation by SIRT1 is
PGC-1α333,337,481,482. PGC-1α is activated via direct deacetylation by SIRT1 at specific lysine
residues333,337. Moreover, as FOXO1 serves as a transcription factor for both PGC-1α and SIRT1
in hepatocytes, and SIRT1 activates FOXO1, FOXO1 could amplify the effects of SIRT1 on
PGC-1α via a feedforward mechanism483,484. PGC-1α, in addition to being a co-activator for
PPARγ, interacts with and co-activates PPARα482,485,486. Hence, FFA and NMN may play a
synergistic role in the activation of PPARα and consequent decrease in CEACAM1 expression.
This would explain the accentuated decrease in insulin clearance observed in our NMN+OLE
group, compared with the OLE group.
Further research is required to identify the co-activators and co-repressors involved in the
binding of PPARα to the CEACAM1 promoter in murine hepatocytes; however, chromatin
immunoprecipitation (ChIP) analysis suggests that liganded PPARα directly regulates
CEACAM1 expression480. Consistently, mice treated with potent PPARα-selective agonists
exhibited decreased CEACAM1 mRNA in the liver in vivo487. Thus, current evidence supports the
hypothesis that an NMN-mediated increase in hepatic NAD levels resulted in increased SIRT1
activity, which led to the deacetylation of PGC-1α and the subsequent activation of PPARα,
which directly silenced the Ceacam1 promoter. This ultimately resulted in decreased hepatic
insulin clearance in vivo.
In addition to inhibiting CEACAM1 transcription, PPARα increases the transcription of
many genes (such as carnitine palmitoyltransferase 1, Acadl, and Acadv1) which shift hepatic fuel
metabolism towards mitochondrial fatty acid oxidation and away from glucose oxidation488–497.

89
This results in the conservation of glucose for the central nervous system488–497. This increased
beta oxidation could also account for the decrease in plasma FFA levels in groups infused with
NMN, compared with their controls.
5.1.2 NMN Accentuates the FFA–Akt–FOXO1–PGC-1α–PPARα–Mediated Decrease
in CEACAM Expression
PGC-1α can act as a co-activator for FOXO1 by directly interacting with FOXO1, resulting
in the formation of a PGC-1α-FOXO1 complex483. Specifically, the carboxy-terminal of PGC-1α
binds with the amino-terminal of FOXO1483. Using a constitutively active form of Akt, it has been
shown that the direct phosphorylation of FOXO1 by Akt strongly impedes the physical interaction
between FOXO1 and PGC-1α483. Furthermore, phosphorylation of FOXO1 by Akt is known to
result in the nuclear exclusion of FOXO1498,499. Hence, the insulin signaling pathway regulates the
co-activation of FOXO1 by PGC-1α as well as the subcellular localization of FOXO1499,500.
Insulin action has been shown to increase CEACAM1 transcription and insulin clearance501.
Since FOXO1 functions as a transcription factor for PGC-1α in hepatocytes483,484, the Akt-
mediated nuclear exclusion of FOXO1 results in decreased PGC-1α expression and activity, and
consequently decreased co-activation of PPARα by PGC-1α482,485,486. As activated PPARα
decreases CEACAM1 transcription by directly binding to its promoter480, decreased PPARα
activity results in increased CEACAM1 expression and insulin clearance487. Thus, the Akt-
mediated decrease in FOXO1 transcriptional activity results in reduced PGC-1α expression,
which leads to decreased co-activation of PPARα. By this indirect pathway and/or perhaps by
direct action of FOXO1 on the CEACAM1 promoter, CEACAM1 expression is upregulated502.
Moreover, since FOXO1 is also a transcription factor for SIRT1381, the Akt-mediated
nuclear exclusion of FOXO1 results in decreased SIRT1 expression and activity. As SIRT1

90
directly activates both PGC-1α and FOXO1 by deacetylation333,337, this leads to the decreased
activation of FOXO1 by SIRT1 and thus a further reduction in CEACAM1 expression.
In our study, the elevation of plasma FFA levels resulted in the development of insulin
resistance in the OLE and NMN+OLE groups. Elevated plasma FFA levels can induce insulin
resistance as follows: as insulin resistance involves the serine-phosphorylation of IRS286,287,300,
this leads to decreased Akt activation by IRS, which consequently leads to decreased FOXO1
inhibition and nuclear exclusion by Akt. As a result, FOXO1’s upregulation of PGC-1α
transcription is less impaired by Akt, leading to increased co-activation of PPARα by PGC-
1α482,485,486. Activated PPARα decreases CEACAM1 transcription by directly binding to its
promoter480, resulting in decreased insulin clearance487. Thus, decreased insulin action also results
in decreased insulin clearance. Conversely, insulin increases its own clearance by upregulating
CEACAM1 expression118.
In our study, administration of NMN accentuated the reduction in insulin clearance caused
by elevated plasma FFA levels in vivo. In addition to a synergistic effect on PPARα due to FFA
activation of PPARα and PGC-1α activation by NMN-induced SIRT1 activity, as described
previously, a synergistic effect between FFA and NMN may have occurred at the level of
FOXO1. FOXO1 may have been activated by FFA-induced insulin resistance as well as by the
increase in NAD levels and consequently SIRT1 activity following NMN administration. Hence,
NMN and FFAs may have synergistically activated FOXO1 in the group treated with both NMN
and OLE, resulting in further stimulation of the PGC-1α – PPARα pathway, which decreases
CEACAM1 expression and insulin clearance. Moreover, since the administration of NMN on its
own did not decrease CEACAM1 expression in our study, the activation of FOXO1 and/or PGC-
1α by the administration of NMN alone may not be sufficient. It would be insightful to conduct a

91
study in which the activities of FOXO1 and PPARα are assessed in the mouse liver samples
collected in our study.
5.1.3 Potentially Opposing Effects of FFA and SIRT1 on PKCδ/ε-Mediated Decrease
in Insulin Clearance
As described earlier in my thesis, our lab had demonstrated that oleate induces the
translocation of PKCδ from the cytosol to the membrane fractions of hepatocytes316. PKCδ
increases the internalization of membrane receptors, including the insulin receptor, via a non-
specific and ligand-independent process of coated-pits internalization317. This may be mediated
by the phosphorylation of internalization motifs on the cytoplasmic juxtamembrane domain of the
membrane receptors317,318. By decreasing the number of insulin receptors available on
hepatocytes, PKCδ mediates the FFA-induced decrease in insulin binding316. Since insulin
clearance requires the binding of insulin to its receptor, and is predominantly performed by
hepatocytes, PKCδ may mediate the FFA-induced decrease in insulin clearance.
In insulin-targeted cells, FFAs are known to also activate PKCε503–505, and both PKCδ and
ε lead to decreased insulin sensitivity506,507. Since the insulin signaling pathway is in part required
for insulin clearance in addition to insulin action, this would be expected to also lead to reduced
insulin clearance.
However, surprisingly, PKCε-null mice were shown to exhibit reduced hepatic insulin
clearance, compared with wildtype controls314. Furthermore, PKCε-null mice exhibited higher
circulating insulin levels during an intraperitoneal glucose tolerance test (IPGTT) despite having
similar rates of C-peptide secretion, compared with controls314. This finding would be consistent
with a study in human endometrial carcinoma cells, which has shown that pharmacological
activation of several PKC isoforms, including PKCδ and ε, results in increased CEACAM1

92
expression508. However, treatment with PKC inhibitor (calphostin C) did not alter CEACAM1
phosphorylation in colon carcinoma cells319. Thus, the effect of PKC isoforms on insulin
clearance and CEACAM1 expression remains unclear.
In contrast to the effects of FFA on activating PKCδ and ε, a recent study has shown that
adenoviral-mediated SIRT1 overexpression in an immortalized mouse hepatocyte cell line509,510
inhibits PKC activity (isoforms were not specified)511. The mechanism by which SIRT1 may have
decreased PKC activity is not known511. No other studies suggesting that SIRT1 activity inhibits
PKC have been found. If increased SIRT1 activity does in fact inhibit PKCδ and ε activities, then
SIRT1 would have an effect on insulin clearance and sensitivity opposite to that of FFA.
However, in our study, the combination of NMN and elevated FFA levels resulted in a synergistic
effect on insulin clearance and no significant effect on insulin sensitivity, compared with elevated
plasma levels of FFA alone.
5.2 Potential Mechanisms Behind NMN’s Effects on
Beta Cell Function
A number of mechanisms could explain our results regarding the effects of NMN on beta
cell function in the context of normal and elevated plasma FFA levels. These mechanisms are
explained below.
5.2.1 SIRT1-FOXO1/3-Mediated Reduction of Oxidative Stress Ameliorated FFA-
Induced Beta Cell Dysfunction
Although we have shown, in collaboration with Dr. Jamie Joseph’s lab, that OLE does not
decrease NAD or NADH levels or ratios in islets (Figure 10), the increase in NAD levels by
NMN administration seems to have increased SIRT1 activity enough to partially counter-act
FFA-induced beta cell dysfunction in vivo.

93
As described earlier in my thesis, FOXO1/3, which are activated by SIRT1, are known to
decrease oxidative stress by upregulating antioxidant genes, such as MnSOD, glutathione, and
catalase348,378. Thus, it is possible that the NMN-induced increase in SIRT1 activity reduced the
FFA-induced oxidative stress by increasing the levels of antioxidants via FOXO1/3. This would
have culminated in ameliorated FFA-induced beta cell dysfunction.
It is also possible that increased SIRT1 activity resulted in the repression of UCP2
transcription by directly binding to the UCP2 promoter336. Since UCP2 is involved in dissipating
the H+ electrochemical gradient in the mitochondrial membranes, decreased UCP2 expression
results in improved efficiency of oxidative phosphorylation and thus increased ATP levels257,347.
As insulin secretion depends on the availability of ATP, it is also increased346. However, using a
novel beta cell-specific UCP2-knockout model, a recent study has demonstrated that UCP2 does
not play a large role as a metabolic uncoupler in beta cells, but rather is important in the
regulation of ROS levels276. Furthermore, preliminary measurements of UCP2 mRNA levels in
our lab have shown no significant differences between any of the SAL, OLE, OLE + resveratrol
(RSV), and RSV groups (unpublished data). Thus, NMN’s partial protection against FFA-induced
beta cell dysfunction is likely due to a decrease in oxidative stress caused by increased antioxidant
expression, and not caused by decreased UCP2 expression.
Our results regarding the effects of NMN on beta cell dysfunction in the context of
elevated plasma FFA levels complement our previous studies which demonstrated SIRT1’s
protective effects on FFA-induced beta cell dysfunction using the SIRT1 activator RSV and the
BESTO (beta cell-specific SIRT1-overexpression) genetic model (Figure 8 &Figure 9).

94
5.2.2 Decreased Plasma FFA Levels Resulted in the Amelioration of FFA-Induced
Beta Cell Dysfunction
With regards to plasma FFA levels, NMN+OLE co-infusion resulted in an intermediate
elevation of FFA levels, compared with the SAL and OLE groups (p < 0.01 vs SAL and p < 0.04
vs OLE). Thus, NMN administration in the context of oleate infusion seems to decrease plasma
FFA levels. It is possible that the NMN-induced decrease in FFA levels in the NMN+OLE group,
compared with the OLE group, had reduced the amplitude of beta cell dysfunction induced by
FFAs. The decrease in plasma FFA levels could be due to increased beta oxidation mediated by
SIRT1 and PPARα in the skeletal muscles512.
In many cells, NMN is converted to NAD by NMNAT513. In skeletal muscles, increased
NAD levels increase SIRT1 activity. SIRT1 then directly activates the transcriptional co-activator
PGC-1α, which, through PPARα, increases mitochondrial biogenesis and the expression of
mitochondrial fatty acid oxidation genes514. These genes include pyruvate dehydrogenase kinase 4
(PDK4), carnitine palmitoyltransferase 1B (CPT1B), and medium-chain acyl-CoA dehydrogenase
(MCAD). Increased beta oxidation would reduce the levels of FFA in plasma515.
5.2.3 Excess Antioxidants During Normal Plasma FFA and Intracellular ROS Levels
Resulted in Sub-Optimal ROS Levels and Decreased GSIS
Unlike the positive effect on beta cell function caused by NMN administration in the
context of elevated plasma FFA levels, NMN in the presence of normal plasma FFA levels
resulted in a significant decrease in beta cell function. There is a mechanism that can explain the
dual effects of NMN on beta cell function. This mechanism depends on the intracellular levels of
ROS (i.e. presence or absence of FFA-induced oxidative stress). As the dose of NMN
administered was relatively high (0.025 mg/kg body weight/min), it may have resulted in excess

95
expression of antioxidant enzymes, which in the presence of normal levels of plasma FFA, led to
sub-optimal levels of ROS. Sub-optimal levels of ROS are known to result in impaired insulin
secretion257,266,279,280.
As described earlier in my thesis, it has been shown that exposure of beta cells to high
levels of antioxidants in the absence of oxidative stress negatively affects GSIS266. Some studies
have found that ROS can be important signaling molecules in insulin secretion257,266. For instance,
a transient increase in ROS levels has been shown to promote insulin signaling via the oxidation
and inhibition of RPTPs (receptor-like protein tyrosine phosphatases), which normally impair the
tyrosine-phosphorylation-mediated activation of the insulin receptor279,280. This mechanism can
be tested by measuring ROS as well as intracellular markers of oxidative stress, such as MDA and
8-OHdG, as described earlier268.
5.2.4 SIRT1-FOXO1-Mediated Nuclear Exclusion of Pdx-1, Resulting in Decreased
Insulin Secretion
There is another mechanism that can potentially explain the NMN-induced decrease in
beta cell function in the context of normal plasma levels of FFA. It is possible that the NAD-
SIRT1-FOXO1 pathway resulted in the nuclear exclusion of the key insulin transcription factor
Pdx-1348. This would have resulted in a decrease in beta cell function during normal plasma FFA
levels and absence of oxidative stress, whereas in the presence of FFA-induced oxidative stress,
the increased transcription of antioxidant genes induced by FOXO1/3 would have resulted in
overall beneficial effects on beta cell function.
5.2.5 NAD-Mediated Increase in PARP Activity Decreases ATP for Insulin Secretion
There is a third potential mechanism by which NMN in the context of normal plasma
levels of FFA results in decreased beta cell function. As described earlier, since PARP consumes

96
NAD during its DNA repair action401, an increase in NAD levels can increase PARP activity. In a
normal physiological context, excessive PARP activity can lead to NAD depletion and a
consequent impairment of the TCA cycle and ATP production. However, in our experiments,
PARP is very unlikely to have depleted NAD levels due to the supplementation of NMN.
Nevertheless, PARP may have been involved in decreased beta cell function. In cells of
the proximal tubule of the kidney subjected to ischemic renal injury, PARP1 has been reported to
directly inhibit glyceraldehyde-3-phosphate dehydrogenase (GAPDH) activity via poly(ADP-
ribosyl)ation in vivo and in vitro516. As GAPDH catalyzes the sixth step in glycolysis, this results
in decreased glycolysis and thus decreased ATP production516,517. The effects of GAPDH on ATP
production were confirmed by the inhibition of GAPDH activity using a GAPDH inhibitor
(iodoacetamide) in a pig kidney epithelial cell line (LLCPK1)516. Iodoacetamide inhibits GAPDH
activity by directly modifying cysteine residues in the GAPDH active site518,519. Iodoacetamide
treatment was found to dose-dependently inhibit GAPDH activity and thus decrease glycolysis
and ATP production. Since ATP is required for insulin secretion, this results in decreased beta
cell function. This mechanism can be assessed by measuring the levels of ATP and D-glycerate
1,3-bisphosphate (product of GAPDH) in islets or beta cell lines. In addition, it would be
informative to measure PARP activity in islets or beta cell lines520.
Similar to the case of nuclear exclusion of Pdx-1, it is possible that the beneficial effect of
increased expression of antioxidant enzymes in the presence of significant FFA-induced oxidative
stress outweighed the negative effect of decreased ATP production in beta cells. This would
explain the partially protective effect of NMN on beta cell function observed in the NMN+OLE
group, compared with the OLE group.

97
5.3 Limitations
The utilization of the ratio of C-peptide to insulin plasma levels obtained during
hyperglycemic clamps has its limitation as an index of endogenous whole-body insulin clearance
as it requires a relatively steady-state of glycemia and insulin secretion. In addition, the
hyperglycemic clamp is not the gold-standard method of assessing insulin sensitivity due to the
potential differences in plasma levels of insulin across different groups and due to the non-
linearity of insulin action with respect to plasma levels of insulin. The hyperglycemic clamp was
used in this study since, based on our previous studies involving the activation of SIRT1 by
resveratrol and genetic overexpression, we expected to observe changes mainly in beta cell
function (for which the hyperglycemic clamp is the gold standard), and not in insulin clearance. It
would have not been feasible to perform both hyperglycemic and hyperinsulinemic-euglycemic
clamps on the same mice due to the limited blood volume in mice and the excessive stress which
would have been caused by their experience of both clamps.
Hyperinsulinemia caused by decreased insulin clearance has been reported to result in
secondary insulin resistance by the downregulation of insulin receptors on hepatocytes111. Global
CEACAM1-null mice and liver-specific dominant-negative phosphorylation-defective S503A
CEACAM1 (L-SACC1) mutants have been known to develop secondary insulin resistance due to
chronic hyperinsulinemia111,120,521. Hyperinsulinemia can also upregulate hepatic lipogenesis via
the insulin-mTORC2-AKT signaling pathway, which can contribute towards hepatic steatosis and
a further decrease in insulin clearance522.
As we did not find secondary insulin resistance in our studies, it appears that the
chronicity and degree of inhibition of CEACAM1 activity determine whether or not secondary
insulin resistance will develop from hyperinsulinemia. In the context of decreased CEACAM1

98
expression via PPARα activation, other studies have shown improved insulin sensitivity and
reduced dyslipidemia480,523–525. Thus, it seems that the effect of PPARα activation to increase
insulin sensitivity prevails over the effect of decreased CEACAM1 expression to decrease it.
In our study, insulin sensitivity was not improved by NMN, and in fact, it was slightly but
not significantly decreased (Figure 17). It is also possible that the two effects of NMN to
decrease CEACAM1 expression and activate PPARα resulted in a balance between the opposite
effects of CEACAM1 and PPARα on insulin sensitivity. Hence, although CEACAM1 activity
tended to induce a decrease in insulin sensitivity, the activation of PPARα prevented that from
happening480,523–525.
5.4 Future Directions
As mentioned above, the hyperglycemic clamp method is the gold-standard for the
assessment of beta cell function, but not of insulin clearance and sensitivity, in vivo. As the
hyperinsulinemic-euglycemic clamp is a more accurate and direct assessment of insulin clearance
and sensitivity (because the plasma insulin levels in all groups would be equalized), compared
with the hyperglycemic clamp method, future experiments should include performing
hyperinsulinemic-euglycemic clamps. In addition, insulin labeled with radioactive iodine (I125)
could be administered during the hyperinsulinemic-euglycemic clamps in order to more
accurately measure insulin clearance (independent of the plasma levels of insulin) and to follow
up on the insulin uptake by hepatocytes in tissue studies. Insulin uptake by hepatocytes may also
be examined in vitro. In order to study the effects of NMN on beta cell function independent of
the effects of changes in insulin clearance, it would be informative to assess beta cell function of
islets ex vivo (after i.v. administration of NMN to animals) or in vitro (after direct administration
of NMN to isolated islets).

99
Regarding the SIRT1-PGC-1α-PPARα-mediated mechanism by which NMN may have
decreased CEACAM1 expression, the activity of PPARα in liver samples could be assessed by
measuring mRNA levels of Cyp4A10 and Cyp4A14, which are targets genes of PPARα and
extremely sensitive markers of its activity in mouse hepatocytes497. In addition, the activity and
expression of SIRT1 and PGC-1α in our mouse livers may be worth measuring in order to assess
their potential roles in the effects of NMN on hepatocytes. In response to elevated plasma FFA
levels, we expect the activity and expression of SIRT1 and PPARα to be decreased and increased,
respectively.
Since FFA and NMN both lead to increased PPARα activity, they may have had
synergistic effects on PPARα activation. Hence, we would expect PPARα activity to be greatest
in the NMN+OLE group, compared with the other groups. If this turns out to be the case, it would
indicate that both NMN and FFA are required to sufficiently activate PPARα in order to decrease
CEACAM1 expression, compared with the NMN group and OLE group. On the other hand, since
SIRT1 activity is decreased by FFA but increased by NMN administration, we would expect to
see an intermediate degree of SIRT1 activity in the NMN+OLE group, compared with the OLE
and NMN groups. Since FOXO1 may amplify the effects of SIRT1 on the activation of PGC-1α
and consequently PPARα, as described earlier, it would be informative to examine the activity
and expression of FOXO1, particularly in the nucleus. The potentially opposing effects of FFA
and SIRT1 on PKCδ and ε and consequently on insulin clearance can be assessed by measuring
the activities of PKCδ and ε in our liver samples.
In order to discern the effects of NMN on hepatic insulin clearance without the potentially
confounding effects of unequal plasma levels of insulin (which can affect the rate of insulin
clearance) between groups in vivo, our collaborator Dr. Sonia Najjar will be performing a similar
study using rat hepatoma cells and human HepG2 cells in vitro. Hepatocytes will be exposed to

100
NMN in culture media with or without elevated FFA levels, and the insulin uptake of hepatocytes
will be measured using radioactive insulin. The effects of an increase in SIRT1 activity on
CEACAM expression in hepatocytes will also be assessed.
Preliminary results suggest that NMN and SIRT1 affect CEACAM1 expression differently
in rat, compared with human, hepatocytes in vitro. Specifically, an adenoviral-mediated increase
in SIRT1 activity resulted in decreased CEACAM1 expression in rat hepatoma cells, but
increased CEACAM1 expression in human HepG2 cells, where NMN also increased CEACAM1
expression. Since these data are still preliminary, additional experiments are currently being
conducted by the lab of Dr. Najjar. If the results of the additional experiments are consistent with
the preliminary results, an important question would be raised about the potential differences
between the effects of NMN and SIRT1 on hepatic insulin clearance in rats and in humans, and
whether or not their effects in the HepG2 cells were specific to the cell line and not representative
of human hepatocytes. Thus, it may be important to examine the effects of NMN and SIRT1 on
insulin clearance in humans526. It is worth noting that a very recently launched clinical trial
(March 3rd, 2016) at the Keio University School of Medicine in Japan will be assessing the safety
of oral consumption of NMN in healthy adult men527. New clinical trials regarding NMN will be
described in the “Conclusions” section of my thesis.
It may be worth performing a similar study ex vivo in which animal models would be
treated with NMN in vivo and then the rate of insulin uptake by hepatocytes would be examined
in vitro. This would simulate the physiological conversion of NMN to NAD by eNAMPT in
blood plasma in vivo yet avoid the potential interference of different plasma levels of insulin
between groups by assessing insulin uptake by hepatocytes in vitro. Radioactive insulin could be
used in order to measure the uptake of insulin by hepatocytes.

101
Lastly, in both in vitro and ex vivo studies, the expected increase in SIRT1 activity in
hepatocytes following NMN administration can be confirmed since the in vitro system is better
suited to measuring the enzymatic activity of SIRT1. As described earlier, it has been confirmed
in other studies that administration of NMN results in elevated NAD levels and SIRT1 activity in
hepatocytes and beta cells in vivo and in vitro424,427,528,529.
As described earlier, studies regarding the effects of FFA on IDE gave contrasting results.
Nevertheless, it may be useful to gain insight into the levels and activity of IDE in the livers of
our mice. In a study published in Diabetologia in 2012, FFA were shown to decrease hepatic
insulin clearance as well as protein and mRNA levels of high-activity and low-activity IDE in
mouse livers530. We are collaborating with renowned IDE expert Dr. Malcolm A. Leissring, based
at the University of California, Irvine. His lab will be assaying the liver samples of all four of our
mouse treatment groups for IDE expression and activity.
To investigate whether or not sub-optimal levels of ROS were responsible for NMN’s
negative effect on beta cell function in the context of normal plasma FFA levels, and to confirm
the increase in ROS after OLE treatment, the levels of intracellular ROS in our mouse pancreatic
islet cells can be measured. This can be done using the method of dichlorodihydrofluorescein
(DCF) fluorescence531,532, the principle of which is as follows: pancreatic islet cells are incubated
in buffer containing the non-fluorescent chemical 2',7'-dichlorodihydrofluorescein diacetate
(H2DCF-DA). After entering the cells, H2DCF-DA is hydrolyzed by intracellular esterases and
oxidized by ROS to form the highly fluorescent molecule DCF. Fluorescence intensity is then
measured at the excitation and emission wavelengths of 485 and 535 nm, respectively. We would
expect the levels of ROS to be highest in the OLE group and lowest in the NMN group, compared
with the other groups.

102
Since the dose of NMN administered in our study (as well as in several other
studies423,424,427,533) was relatively high, it is possible that excess levels of NMN were responsible
for the adverse effects observed in the context of normal plasma FFA levels. It would be
insightful to conduct a study with the aim of determining the effects of different doses of NMN on
beta cell function. It is possible that a dose of NMN that is lower than the dose utilized in our
study would not result in a decrease in beta cell function in the presence of normal FFA levels,
compared with controls.
In beta cells, the proposed mechanism involving Pdx-1 exclusion via the SIRT1-FOXO1
pathway can be assessed in our mouse pancreas samples. Using immunohistochemistry, Pdx-1
expression and its nucleocytoplasmic localization will be determined in the mouse pancreases
which were fixed in formalin and then embedded in paraffin. The procedure would involve
deparaffinizing the pancreas sections, performing Pdx-1-antigen retrieval, and staining with anti-
Pdx-1 antibodies534.
As described earlier, the NMN-mediated activation of PARP may have been involved in
the decreased beta cell function observed in the absence of oxidative stress by directly inhibiting
GAPDH, consequently impairing glycolysis and ATP production516. This mechanism can be
tested by measuring the activities and expression of PARP and GAPDH in islets or beta cells.
Using immunohistochemistry, the expression of PARP535–537 and GAPDH538–540 in our fixed
pancreas samples can be assessed.

103
5.5 Conclusions
Overall, our study provides evidence that NMN administration in the presence of elevated
plasma FFA levels (which simulates obesity) results in substantially improved glucose tolerance
by significantly decreasing insulin clearance and partially protecting against FFA-induced beta
cell dysfunction in vivo. However, in the presence of normal FFA levels, NMN administration
does not affect insulin clearance and significantly reduces beta cell function. NMN resulted in
decreased plasma FFA levels in the context of either elevated or normal plasma FFA levels.
Although the decrease in plasma FFA levels is not responsible for many of the effects induced by
NMN (as explained earlier), the NMN-induced decrease in plasma FFA levels would be
beneficial in increasing the chance of reversing the progression of T2DM60,62,541 and in reducing
the risk of developing fat-related diseases other than T2DM, such as metabolic syndrome and
cardiovascular disease34,36,65,115,198,443,524,542,543.
A very recent clinical trial (initiated on March 3rd, 2016) at the Keio University School of
Medicine in Japan is investigating the safety of oral consumption of NMN in healthy adult
men527. This trial will also evaluate parameters related to metabolic syndrome in order to assess
the potential benefits of NMN as an orally administered drug527. The few studies which have
utilized the administration of NMN in human cells are encouraging regarding the safety of NMN
administration in humans544–546. In addition, based on an email exchange between me and Dr.
David Sinclair, Professor at Harvard University, Dr. Sinclair may begin a clinical trial within a
year in order to investigate the potential ability of NMN to slow the aging process in humans, as it
had done in mice547. Thus, depending on the results of the clinical trials, it may be safe to begin
clinical trials assessing the effects of NMN on glucose tolerance, insulin clearance, and FFA-
induced beta cell dysfunction.

104
Due to Dr. Najjar’s preliminary results showing that adenoviral- and NMN-mediated
activation of SIRT1 induced an increase in CEACAM1 expression in human HepG2 cells, it is
not clear whether or not the administration of NMN in humans will have effects similar to those
observed in our mouse study. If the effects are similar, NMN administration in humans with
elevated plasma levels of FFA (such as patients with T2DM) would significantly improve glucose
tolerance. This would occur via decreased insulin clearance and partial protection against FFA-
induced beta cell dysfunction. However, NMN administration in humans with normal plasma
levels of FFA may have negative effects on beta cell function.
Thus, if clinical trials regarding the effects of NMN on glucose tolerance, insulin
clearance, and FFA-induced beta cell dysfunction end up being consistent with our results, NMN
would be a beneficial treatment for individuals with elevated plasma FFA levels and impaired
glucose tolerance. If individuals no longer have elevated plasma levels of FFA (such as through
weight loss), their treatment with NMN might need to be ceased in order to avoid the net negative
effect of NMN on glucose tolerance in the absence of oxidative stress.

105
References
1. Cerf, M. E. Beta cell dynamics: beta cell replenishment, beta cell compensation and
diabetes. Endocrine 44, 303–311 (2013).
2. Olokoba, A. B., Obateru, O. A. & Olokoba, L. B. Type 2 diabetes mellitus: a review of
current trends. Oman Med J 27, 269–273 (2012).
3. Haubrich, W. S. Langerhans of the islets of Langerhans. Gastroenterology 129, 783 (2005).
4. MacCracken, J. & Hoel, D. From ants to analogues. Puzzles and promises in diabetes
management. Postgrad. Med. 101, 138–140, 143–145, 149–150 (1997).
5. Ahmed, A. M. History of diabetes mellitus. Saudi Med. J. 23, 373–378 (2002).
6. Lakhtakia, R. The history of diabetes mellitus. Sultan Qaboos Univ. Med. J. 13, 368–370
(2013).
7. International Diabetes Federation. IDF Diabetes Atlas, 7th Ed. (2015).
8. Statistics About Diabetes: American Diabetes Association®. Available at:
http://www.diabetes.org/diabetes-basics/statistics/. (Accessed: 18th January 2016)
9. Danaei, G. et al. National, regional, and global trends in fasting plasma glucose and diabetes
prevalence since 1980: systematic analysis of health examination surveys and
epidemiological studies with 370 country-years and 2·7 million participants. Lancet Lond.
Engl. 378, 31–40 (2011).
10. Shaw, J. E., Sicree, R. A. & Zimmet, P. Z. Global estimates of the prevalence of diabetes for
2010 and 2030. Diabetes Res. Clin. Pract. 87, 4–14 (2010).
11. Rawal, L. B. et al. Prevention of Type 2 Diabetes and Its Complications in Developing
Countries: A Review. Int. J. Behav. Med. 19, 121–133 (2012).
12. On the up. Nature 482, 276 (2012).
13. Van Belle, T. L., Coppieters, K. T. & Von Herrath, M. G. Type 1 Diabetes: Etiology,
Immunology, and Therapeutic Strategies. Physiol. Rev. 91, 79–118 (2011).
14. Whitmore, C. Type 2 diabetes and obesity in adults. Br. J. Nurs. Mark Allen Publ. 19, 880,
882–886 (2010).
15. American Diabetes Association. (2) Classification and diagnosis of diabetes. Diabetes Care
38 Suppl, S8–S16 (2015).
16. Giacca, A., Xiao, C., Oprescu, A. I., Carpentier, A. C. & Lewis, G. F. Lipid-induced
pancreatic β-cell dysfunction: focus on in vivo studies. AJP Endocrinol. Metab. 300, E255–
E262 (2011).
17. Kahn, S. E., Cooper, M. E. & Del Prato, S. Pathophysiology and treatment of type 2
diabetes: perspectives on the past, present, and future. The Lancet 383, 1068–1083 (2014).
18. Weir, G. C. & Bonner-Weir, S. Five stages of evolving beta-cell dysfunction during
progression to diabetes. Diabetes 53, S16–S21 (2004).

106
19. Weyer, C., Tataranni, P. A., Bogardus, C. & Pratley, R. E. Insulin resistance and insulin
secretory dysfunction are independent predictors of worsening of glucose tolerance during
each stage of type 2 diabetes development. Diabetes Care 24, 89–94 (2001).
20. Ferrara, A. Increasing prevalence of gestational diabetes mellitus: a public health
perspective. Diabetes Care 30 Suppl 2, S141-146 (2007).
21. Chen, P. et al. Risk Factors and Management of Gestational Diabetes. Cell Biochem.
Biophys. 71, 689–694 (2015).
22. Gestational diabetes: what it means for you and your baby. Am. Fam. Physician 60, 1009–
1010 (1999).
23. Hawryluk, J., Grafka, A., Gęca, T. & Łopucki, M. [Gestational diabetes in the light of
current literature]. Pol. Merkur. Lek. Organ Pol. Tow. Lek. 38, 344–347 (2015).
24. Forbes, J. M. & Cooper, M. E. Mechanisms of Diabetic Complications. Physiol. Rev. 93,
137–188 (2013).
25. Frank, R. N. Diabetic retinopathy. N. Engl. J. Med. 350, 48–58 (2004).
26. Hirai, F. E., Tielsch, J. M., Klein, B. E. K. & Klein, R. Ten-year change in vision-related
quality of life in type 1 diabetes: Wisconsin epidemiologic study of diabetic retinopathy.
Ophthalmology 118, 353–358 (2011).
27. Gilbertson, D. T. et al. Projecting the number of patients with end-stage renal disease in the
United States to the year 2015. J. Am. Soc. Nephrol. JASN 16, 3736–3741 (2005).
28. Mogensen, C. E., Christensen, C. K. & Vittinghus, E. The stages in diabetic renal disease.
With emphasis on the stage of incipient diabetic nephropathy. Diabetes 32 Suppl 2, 64–78
(1983).
29. Tight blood pressure control and risk of macrovascular and microvascular complications in
type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. BMJ 317, 703–713
(1998).
30. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional
treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK
Prospective Diabetes Study (UKPDS) Group. Lancet Lond. Engl. 352, 837–853 (1998).
31. Abbott, C. A., Malik, R. A., van Ross, E. R. E., Kulkarni, J. & Boulton, A. J. M. Prevalence
and characteristics of painful diabetic neuropathy in a large community-based diabetic
population in the U.K. Diabetes Care 34, 2220–2224 (2011).
32. Obrosova, I. G. Diabetic painful and insensate neuropathy: pathogenesis and potential
treatments. Neurother. J. Am. Soc. Exp. Neurother. 6, 638–647 (2009).
33. Chait, A. & Bornfeldt, K. E. Diabetes and atherosclerosis: is there a role for hyperglycemia?
J. Lipid Res. 50 Suppl, S335-339 (2009).
34. Haffner, S. M., Lehto, S., Rönnemaa, T., Pyörälä, K. & Laakso, M. Mortality from coronary
heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without
prior myocardial infarction. N. Engl. J. Med. 339, 229–234 (1998).

107
35. Haffner, S. M., Lehto, S., Rönnemaa, T., Pyörälä, K. & Laakso, M. Mortality from coronary
heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without
prior myocardial infarction. N. Engl. J. Med. 339, 229–234 (1998).
36. Laing, S. P. et al. Mortality from heart disease in a cohort of 23,000 patients with insulin-
treated diabetes. Diabetologia 46, 760–765 (2003).
37. Guo, R. et al. Myocardial dysfunction in early diabetes patients with microalbuminuria: a 2-
dimensional speckle tracking strain study. Cell Biochem. Biophys. 70, 573–578 (2014).
38. Patel, S. S. & Goyal, R. K. Prevention of diabetes-induced myocardial dysfunction in rats
using the juice of the Emblica officinalis fruit. Exp. Clin. Cardiol. 16, 87–91 (2011).
39. Ramos-Román, M. Prolactin and Lactation as Modifiers of Diabetes Risk in Gestational
Diabetes. Horm. Metab. Res. 43, 593–600 (2011).
40. Männik, J., Vaas, P., Rull, K., Teesalu, P. & Laan, M. Differential placental expression
profile of human Growth Hormone/Chorionic Somatomammotropin genes in pregnancies
with pre-eclampsia and gestational diabetes mellitus. Mol. Cell. Endocrinol. 355, 180–187
(2012).
41. World Health Organization. Risk Factors. Available at:
http://www.who.int/topics/risk_factors/en/. (Accessed: 28th December 2015)
42. Wu, Y.-L., Ding, Y.-P., Gao, J., Tanaka, Y. & Zhang, W. Risk Factors and Primary
Prevention Trials for Type 1 Diabetes. Int. J. Biol. Sci. 9, 666–679 (2013).
43. Leroux, C. et al. Lifestyle and cardiometabolic risk in adults with type 1 diabetes: a review.
Can. J. Diabetes 38, 62–69 (2014).
44. Xie, Z., Chang, C. & Zhou, Z. Molecular Mechanisms in Autoimmune Type 1 Diabetes: a
Critical Review. Clin. Rev. Allergy Immunol. 47, 174–192 (2014).
45. Filippi, C. M. & von Herrath, M. G. Viral Trigger for Type 1 Diabetes: Pros and Cons.
Diabetes 57, 2863–2871 (2008).
46. Olagbuji, B. N. et al. Prevalence of and risk factors for gestational diabetes using 1999, 2013
WHO and IADPSG criteria upon implementation of a universal one-step screening and
diagnostic strategy in a sub-Saharan African population. Eur. J. Obstet. Gynecol. Reprod.
Biol. 189, 27–32 (2015).
47. Mohan, M. A. & Chandrakumar, A. Evaluation of prevalence and risk factors of gestational
diabetes in a tertiary care hospital in Kerala. Diabetes Metab. Syndr. (2015).
doi:10.1016/j.dsx.2015.09.002
48. Stevens, J. W. et al. Preventing the progression to type 2 diabetes mellitus in adults at high
risk: a systematic review and network meta-analysis of lifestyle, pharmacological and
surgical interventions. Diabetes Res. Clin. Pract. 107, 320–331 (2015).
49. Teede, H., Deeks, A. & Moran, L. Polycystic ovary syndrome: a complex condition with
psychological, reproductive and metabolic manifestations that impacts on health across the
lifespan. BMC Med. 8, 41 (2010).
50. Lebovitz, H. E. & Banerji, M. A. Point: visceral adiposity is causally related to insulin
resistance. Diabetes Care 28, 2322–2325 (2005).

108
51. Gastaldelli, A. Abdominal fat: does it predict the development of type 2 diabetes? Am. J.
Clin. Nutr. 87, 1118–1119 (2008).
52. Hanley, A. J. G. et al. Insulin resistance, beta cell dysfunction and visceral adiposity as
predictors of incident diabetes: the Insulin Resistance Atherosclerosis Study (IRAS) Family
study. Diabetologia 52, 2079–2086 (2009).
53. Arner, P. Differences in lipolysis between human subcutaneous and omental adipose tissues.
Ann. Med. 27, 435–438 (1995).
54. Pereira, S. et al. In vivo effects of polyunsaturated, monounsaturated, and saturated fatty
acids on hepatic and peripheral insulin sensitivity. Metabolism 64, 315–322 (2015).
55. Koulajian, K. et al. Overexpression of glutathione peroxidase 4 prevents β-cell dysfunction
induced by prolonged elevation of lipids in vivo. Am. J. Physiol. Endocrinol. Metab. 305,
E254-262 (2013).
56. Koulajian, K. et al. NADPH oxidase inhibition prevents beta cell dysfunction induced by
prolonged elevation of oleate in rodents. Diabetologia 56, 1078–1087 (2013).
57. Petersen, K. F. et al. Reversal of muscle insulin resistance by weight reduction in young,
lean, insulin-resistant offspring of parents with type 2 diabetes. Proc. Natl. Acad. Sci. U. S.
A. 109, 8236–8240 (2012).
58. Petersen, K. F. et al. Reversal of nonalcoholic hepatic steatosis, hepatic insulin resistance,
and hyperglycemia by moderate weight reduction in patients with type 2 diabetes. Diabetes
54, 603–608 (2005).
59. Benaiges, D. et al. Bariatric surgery: to whom and when? Minerva Endocrinol. 40, 119–128
(2015).
60. Parikh, M. et al. Randomized pilot trial of bariatric surgery versus intensive medical weight
management on diabetes remission in type 2 diabetic patients who do NOT meet NIH
criteria for surgery and the role of soluble RAGE as a novel biomarker of success. Ann.
Surg. 260, 617-622-624 (2014).
61. Lee, W.-J. & Almulaifi, A. Recent advances in bariatric/metabolic surgery: appraisal of
clinical evidence. J. Biomed. Res. 29, 98–104 (2015).
62. Perugini, R. A. & Malkani, S. Remission of type 2 diabetes mellitus following bariatric
surgery: review of mechanisms and presentation of the concept of ‘reversibility’. Curr.
Opin. Endocrinol. Diabetes Obes. 18, 119–128 (2011).
63. Scopinaro, N. Bariatric metabolic surgery. Rozhl. V Chir. Měsíč. Českoslov. Chir. Spol. 93,
404–415 (2014).
64. Meijer, R. I. et al. Bariatric surgery as a novel treatment for type 2 diabetes mellitus: a
systematic review. Arch. Surg. Chic. Ill 1960 146, 744–750 (2011).
65. Daousi, C. et al. Prevalence of obesity in type 2 diabetes in secondary care: association with
cardiovascular risk factors. Postgrad. Med. J. 82, 280–284 (2006).
66. Bennett, W. L. et al. Comparative effectiveness and safety of medications for type 2
diabetes: an update including new drugs and 2-drug combinations. Ann. Intern. Med. 154,
602–613 (2011).

109
67. American Diabetes Association. Standards of medical care in diabetes--2009. Diabetes Care
32 Suppl 1, S13-61 (2009).
68. Inzucchi, S. E. et al. Management of hyperglycemia in type 2 diabetes: a patient-centered
approach: position statement of the American Diabetes Association (ADA) and the
European Association for the Study of Diabetes (EASD). Diabetes Care 35, 1364–1379
(2012).
69. Estimated diabetes statistics in Canada are generated by the Canadian Diabetes Cost Model.
70. Atlanta, GA: US Department of Health and Human Services. Centers for Disease Control
and Prevention. National Diabetes Statistics Report: Estimates of Diabetes and Its Burden in
the United States. (2014).
71. Demmer, R. T., Zuk, A. M., Rosenbaum, M. & Desvarieux, M. Prevalence of diagnosed and
undiagnosed type 2 diabetes mellitus among US adolescents: results from the continuous
NHANES, 1999-2010. Am. J. Epidemiol. 178, 1106–1113 (2013).
72. Hoang, Q. N., Pisani, M. A., Inzucchi, S., Hu, B. & Honiden, S. The prevalence of
undiagnosed diabetes mellitus and the association of baseline glycemic control on mortality
in the intensive care unit: a prospective observational study. J. Crit. Care 29, 1052–1056
(2014).
73. Leahy, S. et al. Prevalence and correlates of diagnosed and undiagnosed type 2 diabetes
mellitus and pre-diabetes in older adults: Findings from the Irish Longitudinal Study on
Ageing (TILDA). Diabetes Res. Clin. Pract. 110, 241–249 (2015).
74. Canadian Diabetes Association. An economic tsunami - the cost of diabetes in Canada.
(2009).
75. Blundell, T. L. et al. Atomic positions in rhombohedral 2-zinc insulin crystals. Nature 231,
506–511 (1971).
76. Gerich, J. E. Is reduced first-phase insulin release the earliest detectable abnormality in
individuals destined to develop type 2 diabetes? Diabetes 51 Suppl 1, S117-121 (2002).
77. De Vos, A. et al. Human and rat beta cells differ in glucose transporter but not in
glucokinase gene expression. J. Clin. Invest. 96, 2489–2495 (1995).
78. Gurgul-Convey, E., Kaminski, M. T. & Lenzen, S. Physiological characterization of the
human EndoC-βH1 β-cell line. Biochem. Biophys. Res. Commun. 464, 13–19 (2015).
79. Liang, Y., Cushman, S. M., Whitesell, R. R. & Matschinsky, F. M. GLUT1 is adequate for
glucose uptake in GLUT2-deficient insulin-releasing beta-cells. Horm. Metab. Res. Horm.
Stoffwechselforschung Horm. Métabolisme 29, 255–260 (1997).
80. Thorens, B., Guillam, M. T., Beermann, F., Burcelin, R. & Jaquet, M. Transgenic
reexpression of GLUT1 or GLUT2 in pancreatic beta cells rescues GLUT2-null mice from
early death and restores normal glucose-stimulated insulin secretion. J. Biol. Chem. 275,
23751–23758 (2000).
81. van de Bunt, M. & Gloyn, A. L. A tale of two glucose transporters: how GLUT2 re-emerged
as a contender for glucose transport into the human beta cell. Diabetologia 55, 2312–2315
(2012).

110
82. Yabe, D. & Seino, Y. Two incretin hormones GLP-1 and GIP: comparison of their actions in
insulin secretion and β cell preservation. Prog. Biophys. Mol. Biol. 107, 248–256 (2011).
83. Gautam, D. et al. Role of the M3 muscarinic acetylcholine receptor in beta-cell function and
glucose homeostasis. Diabetes Obes. Metab. 9 Suppl 2, 158–169 (2007).
84. Burant, C. F. Activation of GPR40 as a therapeutic target for the treatment of type 2
diabetes. Diabetes Care 36 Suppl 2, S175-179 (2013).
85. Hirasawa, A., Hara, T., Katsuma, S., Adachi, T. & Tsujimoto, G. Free fatty acid receptors
and drug discovery. Biol. Pharm. Bull. 31, 1847–1851 (2008).
86. Hara, T., Kimura, I., Inoue, D., Ichimura, A. & Hirasawa, A. Free fatty acid receptors and
their role in regulation of energy metabolism. Rev. Physiol. Biochem. Pharmacol. 164, 77–
116 (2013).
87. McNelis, J. C. et al. GPR43 Potentiates β-Cell Function in Obesity. Diabetes 64, 3203–3217
(2015).
88. Bahar Halpern, K., Veprik, A., Rubins, N., Naaman, O. & Walker, M. D. GPR41 gene
expression is mediated by internal ribosome entry site (IRES)-dependent translation of
bicistronic mRNA encoding GPR40 and GPR41 proteins. J. Biol. Chem. 287, 20154–20163
(2012).
89. Ohishi, T. & Yoshida, S. The therapeutic potential of GPR119 agonists for type 2 diabetes.
Expert Opin. Investig. Drugs 21, 321–328 (2012).
90. Priyadarshini, M., Wicksteed, B., Schiltz, G. E., Gilchrist, A. & Layden, B. T. SCFA
Receptors in Pancreatic β Cells: Novel Diabetes Targets? Trends Endocrinol. Metab. TEM
(2016). doi:10.1016/j.tem.2016.03.011
91. Hoang Do, O. & Thorn, P. Insulin secretion from beta cells within intact islets: location
matters. Clin. Exp. Pharmacol. Physiol. 42, 406–414 (2015).
92. Thibault, V. et al. The increase in serum 25-hydroxyvitamin D following weight loss does
not contribute to the improvement in insulin sensitivity, insulin secretion and β-cell function.
Br. J. Nutr. 114, 161–168 (2015).
93. Sanke, T. [Serum and urine C-peptide and proinsulin to insulin ratio as an index for insulin
secretion]. Nihon Rinsho Jpn. J. Clin. Med. 70 Suppl 3, 465–470 (2012).
94. Morisset, A.-S. et al. Associations Between Serum 25-Hydroxyvitamin D, Insulin
Sensitivity, Insulin Secretion, and β-Cell Function According to Glucose Tolerance Status.
Metab. Syndr. Relat. Disord. 13, 208–213 (2015).
95. Gagnon, C. et al. Effects of combined calcium and vitamin D supplementation on insulin
secretion, insulin sensitivity and β-cell function in multi-ethnic vitamin D-deficient adults at
risk for type 2 diabetes: a pilot randomized, placebo-controlled trial. PloS One 9, e109607
(2014).
96. Rhodes, C. J., White, M. F., Leahy, J. L. & Kahn, S. E. Direct autocrine action of insulin on
β-cells: does it make physiological sense? Diabetes 62, 2157–2163 (2013).
97. Leibiger, I. B., Leibiger, B. & Berggren, P.-O. Insulin feedback action on pancreatic beta-
cell function. FEBS Lett. 532, 1–6 (2002).

111
98. Best, C. H. & Haist, R. E. The effect of insulin administration on the insulin content of the
pancreas. J. Physiol. 100, 142–146 (1941).
99. Elahi, D. et al. Feedback inhibition of insulin secretion by insulin: relation to the
hyperinsulinemia of obesity. N. Engl. J. Med. 306, 1196–1202 (1982).
100. Khan, F. A., Goforth, P. B., Zhang, M. & Satin, L. S. Insulin activates ATP-sensitive K(+)
channels in pancreatic beta-cells through a phosphatidylinositol 3-kinase-dependent
pathway. Diabetes 50, 2192–2198 (2001).
101. Leibiger, I. B., Leibiger, B., Moede, T. & Berggren, P. O. Exocytosis of insulin promotes
insulin gene transcription via the insulin receptor/PI-3 kinase/p70 s6 kinase and CaM kinase
pathways. Mol. Cell 1, 933–938 (1998).
102. Xu, G. G. & Rothenberg, P. L. Insulin receptor signaling in the beta-cell influences insulin
gene expression and insulin content: evidence for autocrine beta-cell regulation. Diabetes
47, 1243–1252 (1998).
103. Aspinwall, C. A. et al. Roles of insulin receptor substrate-1, phosphatidylinositol 3-kinase,
and release of intracellular Ca2+ stores in insulin-stimulated insulin secretion in beta -cells.
J. Biol. Chem. 275, 22331–22338 (2000).
104. Aspinwall, C. A., Lakey, J. R. & Kennedy, R. T. Insulin-stimulated insulin secretion in
single pancreatic beta cells. J. Biol. Chem. 274, 6360–6365 (1999).
105. Duckworth, W. C., Bennett, R. G. & Hamel, F. G. Insulin degradation: progress and
potential. Endocr. Rev. 19, 608–624 (1998).
106. Bergman, R. N. Non-esterified fatty acids and the liver: why is insulin secreted into the
portal vein? Diabetologia 43, 946–952 (2000).
107. Bril, F. et al. Relationship between disease severity, hyperinsulinemia, and impaired insulin
clearance in patients with nonalcoholic steatohepatitis. Hepatol. Baltim. Md 59, 2178–2187
(2014).
108. Najjar, S. M. Regulation of insulin action by CEACAM1. Trends Endocrinol. Metab. 13,
240–245 (2002).
109. Sato, H., Terasaki, T., Mizuguchi, H., Okumura, K. & Tsuji, A. Receptor-recycling model of
clearance and distribution of insulin in the perfused mouse liver. Diabetologia 34, 613–621
(1991).
110. Duckworth, W. C., Hamel, F. G. & Peavy, D. E. Hepatic metabolism of insulin. Am. J. Med.
85, 71–76 (1988).
111. DeAngelis, A. M. et al. Carcinoembryonic Antigen-Related Cell Adhesion Molecule 1: A
Link Between Insulin and Lipid Metabolism. Diabetes 57, 2296–2303 (2008).
112. Mortimore, G. E., Tietze, F. & Stetten, D. Metabolism of insulin-I 131; studies in isolated,
perfused rat liver and hindlimb preparations. Diabetes 8, 307–314 (1959).
113. Wirth, A., Holm, G. & Björntorp, P. Effect of physical training on insulin uptake by the
perfused rat liver. Metabolism. 31, 457–462 (1982).
114. Svedberg, J., Strömblad, G., Wirth, A., Smith, U. & Björntorp, P. Fatty acids in the portal
vein of the rat regulate hepatic insulin clearance. J. Clin. Invest. 88, 2054–2058 (1991).

112
115. Ebbert, J. O. & Jensen, M. D. Fat depots, free fatty acids, and dyslipidemia. Nutrients 5,
498–508 (2013).
116. Boden, G. Free fatty acids and insulin secretion in humans. Curr. Diab. Rep. 5, 167–170
(2005).
117. Hennes, M. M., Shrago, E. & Kissebah, A. H. Receptor and postreceptor effects of free fatty
acids (FFA) on hepatocyte insulin dynamics. Int. J. Obes. 14, 831–841 (1990).
118. Pereira, S. et al. FFA-induced hepatic insulin resistance in vivo is mediated by PKC ,
NADPH oxidase, and oxidative stress. AJP Endocrinol. Metab. 307, E34–E46 (2014).
119. Choice, C. V., Howard, M. J., Poy, M. N., Hankin, M. H. & Najjar, S. M. Insulin stimulates
pp120 endocytosis in cells co-expressing insulin receptors. J. Biol. Chem. 273, 22194–22200
(1998).
120. Poy, M. N. et al. CEACAM1 regulates insulin clearance in liver. Nat. Genet. 30, 270–276
(2002).
121. Huang, J. et al. Targeted Deletion of Murine CEACAM 1 Activates PI3K-Akt Signaling and
Contributes to the Expression of (Pro) Renin Receptor via CREB Family and NF-κB
Transcription Factors. Hypertension 62, 317–323 (2013).
122. Ontko, J. A. Metabolism of free fatty acids in isolated liver cells. Factors affecting the
partition between esterification and oxidation. J. Biol. Chem. 247, 1788–1800 (1972).
123. Strömblad, G. & Björntorp, P. Reduced hepatic insulin clearance in rats with dietary-induced
obesity. Metabolism. 35, 323–327 (1986).
124. Rees-Jones, R. W. & Taylor, S. I. An endogenous substrate for the insulin receptor-
associated tyrosine kinase. J. Biol. Chem. 260, 4461–4467 (1985).
125. Najjar, S. M. et al. Insulin-stimulated phosphorylation of recombinant pp120/HA4, an
endogenous substrate of the insulin receptor tyrosine kinase. Biochemistry (Mosc.) 34, 9341–
9349 (1995).
126. Nakayama, M. et al. Increased expression of NAD(P)H oxidase in islets of animal models of
Type 2 diabetes and its improvement by an AT1 receptor antagonist. Biochem. Biophys. Res.
Commun. 332, 927–933 (2005).
127. Duckworth, W. C., Bennett, R. G. & Hamel, F. G. Insulin degradation: progress and
potential. Endocr. Rev. 19, 608–624 (1998).
128. Fawcett, J. & Rabkin, R. Sequential processing of insulin by cultured kidney cells.
Endocrinology 136, 39–45 (1995).
129. Rabkin, R., Ryan, M. P. & Duckworth, W. C. The renal metabolism of insulin. Diabetologia
27, 351–357 (1984).
130. Hysing, J., Tolleshaug, H. & Kindberg, G. M. Renal uptake and degradation of trapped-label
insulin. Ren. Physiol. Biochem. 12, 228–237 (1989).
131. Dahl, D. C., Tsao, T., Duckworth, W. C., Mahoney, M. J. & Rabkin, R. Retroendocytosis of
insulin in a cultured kidney epithelial cell line. Am. J. Physiol. 257, C190-196 (1989).
132. Nielsen, S. Time course and kinetics of proximal tubular processing of insulin. Am. J.
Physiol. 262, F813-822 (1992).

113
133. Accili, D., Perrotti, N., Rees-Jones, R. & Taylor, S. I. Tissue distribution and subcellular
localization of an endogenous substrate (pp 120) for the insulin receptor-associated tyrosine
kinase. Endocrinology 119, 1274–1280 (1986).
134. Han, E. et al. Differences in tissue-specific and embryonic expression of mouse Ceacam1
and Ceacam2 genes. Biochem. J. 355, 417–423 (2001).
135. Patel, P. R. et al. Increased metabolic rate and insulin sensitivity in male mice lacking the
carcino-embryonic antigen-related cell adhesion molecule 2. Diabetologia 55, 763–772
(2012).
136. Poy, M. N., Ruch, R. J., Fernstrom, M. A., Okabayashi, Y. & Najjar, S. M. Shc and
CEACAM1 interact to regulate the mitogenic action of insulin. J. Biol. Chem. 277, 1076–
1084 (2002).
137. Soni, P., Lakkis, M., Poy, M. N., Fernström, M. A. & Najjar, S. M. The differential effects
of pp120 (Ceacam 1) on the mitogenic action of insulin and insulin-like growth factor 1 are
regulated by the nonconserved tyrosine 1316 in the insulin receptor. Mol. Cell. Biol. 20,
3896–3905 (2000).
138. Kelpe, C. L. et al. Palmitate inhibition of insulin gene expression is mediated at the
transcriptional level via ceramide synthesis. J. Biol. Chem. 278, 30015–30021 (2003).
139. Luo, W. et al. Association of an 80 kDa protein with C-CAM1 cytoplasmic domain
correlates with C-CAM1-mediated growth inhibition. Oncogene 16, 1141–1147 (1998).
140. Ergün, S. et al. CEA-related cell adhesion molecule 1: a potent angiogenic factor and a
major effector of vascular endothelial growth factor. Mol. Cell 5, 311–320 (2000).
141. Tiedge, M., Lortz, S., Drinkgern, J. & Lenzen, S. Relation between antioxidant enzyme gene
expression and antioxidative defense status of insulin-producing cells. Diabetes 46, 1733–
1742 (1997).
142. Meier, J. J. Beta cell mass in diabetes: a realistic therapeutic target? Diabetologia 51, 703–
713 (2008).
143. Unger, R. H. & Zhou, Y. T. Lipotoxicity of beta-cells in obesity and in other causes of fatty
acid spillover. Diabetes 50 Suppl 1, S118-121 (2001).
144. Hamel, F. G., Mahoney, M. J. & Duckworth, W. C. Degradation of intraendosomal insulin
by insulin-degrading enzyme without acidification. Diabetes 40, 436–443 (1991).
145. Hamel, F. G., Posner, B. I., Bergeron, J. J., Frank, B. H. & Duckworth, W. C. Isolation of
insulin degradation products from endosomes derived from intact rat liver. J. Biol. Chem.
263, 6703–6708 (1988).
146. Mirsky, I. A. & Broh-Kahn, R. H. The inactivation of insulin by tissue extracts; the
distribution and properties of insulin inactivating extracts. Arch. Biochem. 20, 1–9 (1949).
147. Morita, M. et al. Insulin-degrading enzyme exists inside of rat liver peroxisomes and
degrades oxidized proteins. Cell Struct. Funct. 25, 309–315 (2000).
148. Authier, F. et al. Degradation of the cleaved leader peptide of thiolase by a peroxisomal
proteinase. Proc. Natl. Acad. Sci. U. S. A. 92, 3859–3863 (1995).

114
149. Duckworth, W. C. Insulin and glucagon binding and degradation by kidney cell membranes.
Endocrinology 102, 1766–1774 (1978).
150. Amar-Costesec, A., Wibo, M., Thinès-Sempoux, D., Beaufay, H. & Berthet, J. Analytical
study of microsomes and isolated subcellular membranes from rat liver. IV. Biochemical,
physical, and morphological modifications of microsomal components induced by digitonin,
EDTA, and pyrophosphate. J. Cell Biol. 62, 717–745 (1974).
151. Kuo, W. L., Gehm, B. D. & Rosner, M. R. Regulation of insulin degradation: expression of
an evolutionarily conserved insulin-degrading enzyme increases degradation via an
intracellular pathway. Mol. Endocrinol. Baltim. Md 5, 1467–1476 (1991).
152. Durham, T. B. et al. Dual Exosite-binding Inhibitors of Insulin-degrading Enzyme
Challenge Its Role as the Primary Mediator of Insulin Clearance in Vivo. J. Biol. Chem. 290,
20044–20059 (2015).
153. Abdul-Hay, S. O. et al. Deletion of insulin-degrading enzyme elicits antipodal, age-
dependent effects on glucose and insulin tolerance. PloS One 6, e20818 (2011).
154. Maianti, J. P. et al. Anti-diabetic activity of insulin-degrading enzyme inhibitors mediated
by multiple hormones. Nature 511, 94–98 (2014).
155. Bennett, R. G., Duckworth, W. C. & Hamel, F. G. Degradation of amylin by insulin-
degrading enzyme. J. Biol. Chem. 275, 36621–36625 (2000).
156. Bennett, R. G., Hamel, F. G. & Duckworth, W. C. An insulin-degrading enzyme inhibitor
decreases amylin degradation, increases amylin-induced cytotoxicity, and increases amyloid
formation in insulinoma cell cultures. Diabetes 52, 2315–2320 (2003).
157. Farris, W. et al. Insulin-degrading enzyme regulates the levels of insulin, amyloid beta-
protein, and the beta-amyloid precursor protein intracellular domain in vivo. Proc. Natl.
Acad. Sci. U. S. A. 100, 4162–4167 (2003).
158. Scherbaum, W. A. The role of amylin in the physiology of glycemic control. Exp. Clin.
Endocrinol. Diabetes Off. J. Ger. Soc. Endocrinol. Ger. Diabetes Assoc. 106, 97–102
(1998).
159. Young, A. & Denaro, M. Roles of amylin in diabetes and in regulation of nutrient load. Nutr.
Burbank Los Angel. Cty. Calif 14, 524–527 (1998).
160. Schmitz, O., Brock, B. & Rungby, J. Amylin agonists: a novel approach in the treatment of
diabetes. Diabetes 53 Suppl 3, S233-238 (2004).
161. Shen, Y., Joachimiak, A., Rosner, M. R. & Tang, W.-J. Structures of human insulin-
degrading enzyme reveal a new substrate recognition mechanism. Nature 443, 870–874
(2006).
162. Bronský, J., Chada, M., Kotaska, K. & Průsa, R. [Amylin--its physiological role in humans].
Ceskoslovenská Fysiol. Ústrední Úst. Biol. 51, 176–180 (2002).
163. Martin, C. The physiology of amylin and insulin: maintaining the balance between glucose
secretion and glucose uptake. Diabetes Educ. 32 Suppl 3, 101S–104S (2006).
164. Duckworth, W. C. Insulin and glucagon degradation by the kidney. II. Characterization of
the mechanisms at neutral pH. Biochim. Biophys. Acta 437, 531–542 (1976).

115
165. Stein, D. T. et al. Essentiality of circulating fatty acids for glucose-stimulated insulin
secretion in the fasted rat. J. Clin. Invest. 97, 2728–2735 (1996).
166. Warnotte, C., Gilon, P., Nenquin, M. & Henquin, J. C. Mechanisms of the stimulation of
insulin release by saturated fatty acids. A study of palmitate effects in mouse beta-cells.
Diabetes 43, 703–711 (1994).
167. Crespin, S. R., Greenough, W. B. & Steinberg, D. Stimulation of insulin secretion by long-
chain free fatty acids. A direct pancreatic effect. J. Clin. Invest. 52, 1979–1984 (1973).
168. Carpentier, A. et al. Acute enhancement of insulin secretion by FFA in humans is lost with
prolonged FFA elevation. Am. J. Physiol.-Endocrinol. Metab. 276, E1055–E1066 (1999).
169. Dobbins, R. L., Chester, M. W., Daniels, M. B., McGarry, J. D. & Stein, D. T. Circulating
fatty acids are essential for efficient glucose-stimulated insulin secretion after prolonged
fasting in humans. Diabetes 47, 1613–1618 (1998).
170. Paolisso, G. et al. Opposite effects of short-and long-term fatty acid infusion on insulin
secretion in healthy subjects. Diabetologia 38, 1295–1299 (1995).
171. Hennes, M. M., Dua, A. & Kissebah, A. H. Effects of free fatty acids and glucose on
splanchnic insulin dynamics. Diabetes 46, 57–62 (1997).
172. Nolan, C. J., Madiraju, M. S. R., Delghingaro-Augusto, V., Peyot, M.-L. & Prentki, M. Fatty
Acid Signaling in the -Cell and Insulin Secretion. Diabetes 55, S16–S23 (2006).
173. Poitout, V. & Robertson, R. P. Glucolipotoxicity: Fuel Excess and β-Cell Dysfunction.
Endocr. Rev. 29, 351–366 (2008).
174. Magnan, C. et al. Lipid infusion lowers sympathetic nervous activity and leads to increased
β-cell responsiveness to glucose. J. Clin. Invest. 103, 413 (1999).
175. Magnan, C. et al. Glucose-induced insulin hypersecretion in lipid-infused healthy subjects is
associated with a decrease in plasma norepinephrine concentration and urinary excretion. J.
Clin. Endocrinol. Metab. 86, 4901–4907 (2001).
176. Carpentier, A. et al. Free fatty acid-mediated impairment of glucose-stimulated insulin
secretion in nondiabetic Oji-Cree individuals from the Sandy Lake community of Ontario,
Canada a population at very high risk for developing type 2 diabetes. Diabetes 52, 1485–
1495 (2003).
177. Xiao, C., Giacca, A. & Lewis, G. F. Oral taurine but not N-acetylcysteine ameliorates
NEFA-induced impairment in insulin sensitivity and beta cell function in obese and
overweight, non-diabetic men. Diabetologia 51, 139–146 (2007).
178. Stefan, N., Wahl, H. G., Fritsche, A., Häring, H. & Stumvoll, M. Effect of the pattern of
elevated free fatty acids on insulin sensitivity and insulin secretion in healthy humans.
Horm. Metab. Res. Horm. Stoffwechselforschung Horm. Metab. 33, 432–438 (2001).
179. Kahn, S. E. et al. Quantification of the relationship between insulin sensitivity and β-cell
function in human subjects: evidence for a hyperbolic function. Diabetes 42, 1663–1672
(1993).
180. Leung, N. et al. Prolonged increase of plasma non-esterified fatty acids fully abolishes the
stimulatory effect of 24 hours of moderate hyperglycaemia on insulin sensitivity and
pancreatic beta-cell function in obese men. Diabetologia 47, 204–213 (2004).

116
181. Carpentier, A. C., Bourbonnais, A., Frisch, F., Giacca, A. & Lewis, G. F. Plasma
Nonesterified Fatty Acid Intolerance and Hyperglycemia Are Associated with Intravenous
Lipid-Induced Impairment of Insulin Sensitivity and Disposition Index. J. Clin. Endocrinol.
Metab. 95, 1256–1264 (2010).
182. Storgaard, H., Jensen, C. B., Vaag, A. A., Vølund, A. & Madsbad, S. Insulin secretion after
short- and long-term low-grade free fatty acid infusion in men with increased risk of
developing type 2 diabetes. Metabolism 52, 885–894 (2003).
183. Xiao, C., Giacca, A. & Lewis, G. F. The effect of high-dose sodium salicylate on chronically
elevated plasma nonesterified fatty acid-induced insulin resistance and -cell dysfunction in
overweight and obese nondiabetic men. AJP Endocrinol. Metab. 297, E1205–E1211 (2009).
184. Xiao, C., Giacca, A. & Lewis, G. F. Sodium Phenylbutyrate, a Drug With Known Capacity
to Reduce Endoplasmic Reticulum Stress, Partially Alleviates Lipid-Induced Insulin
Resistance and -Cell Dysfunction in Humans. Diabetes 60, 918–924 (2011).
185. Carpentier, A., Mittelman, S. D., Bergman, R. N., Giacca, A. & Lewis, G. F. Prolonged
elevation of plasma free fatty acids impairs pancreatic beta-cell function in obese
nondiabetic humans but not in individuals with type 2 diabetes. Diabetes 49, 399–408
(2000).
186. Pang, J., Xi, C., Jin, J., Han, Y. & Zhang, T. Relative quantitative comparison between
lipotoxicity and glucotoxicity affecting the PARP-NAD-SIRT1 pathway in hepatocytes.
Cell. Physiol. Biochem. Int. J. Exp. Cell. Physiol. Biochem. Pharmacol. 32, 719–727 (2013).
187. Li, N., Frigerio, F. & Maechler, P. The sensitivity of pancreatic beta-cells to mitochondrial
injuries triggered by lipotoxicity and oxidative stress. Biochem. Soc. Trans. 36, 930–934
(2008).
188. Cusi, K. The role of adipose tissue and lipotoxicity in the pathogenesis of type 2 diabetes.
Curr. Diab. Rep. 10, 306–315 (2010).
189. Poitout, V. & Robertson, R. P. Glucolipotoxicity: fuel excess and beta-cell dysfunction.
Endocr. Rev. 29, 351–366 (2008).
190. Kaiser, N., Leibowitz, G. & Nesher, R. Glucotoxicity and beta-cell failure in type 2 diabetes
mellitus. J. Pediatr. Endocrinol. Metab. JPEM 16, 5–22 (2003).
191. Rabuazzo, A. M., Piro, S., Anello, M., Patanè, G. & Purrello, F. Glucotoxicity and
lipotoxicity in the beta cell. Int. Congr. Ser. 1253, 115–121 (2003).
192. Toffolo, G., Bergman, R. N., Finegood, D. T., Bowden, C. R. & Cobelli, C. Quantitative
estimation of beta cell sensitivity to glucose in the intact organism: a minimal model of
insulin kinetics in the dog. Diabetes 29, 979–990 (1980).
193. Bergman, R. N., Ader, M., Huecking, K. & Van Citters, G. Accurate assessment of beta-cell
function: the hyperbolic correction. Diabetes 51 Suppl 1, S212-220 (2002).
194. Stumvoll, M., Goldstein, B. J. & van Haeften, T. W. Pathogenesis of Type 2 Diabetes.
Endocr. Res. 32, 19–37 (2007).
195. Lupi, R. et al. Prolonged exposure to free fatty acids has cytostatic and pro-apoptotic effects
on human pancreatic islets: evidence that beta-cell death is caspase mediated, partially
dependent on ceramide pathway, and Bcl-2 regulated. Diabetes 51, 1437–1442 (2002).

117
196. Shimabukuro, M., Zhou, Y. T., Levi, M. & Unger, R. H. Fatty acid-induced beta cell
apoptosis: a link between obesity and diabetes. Proc. Natl. Acad. Sci. U. S. A. 95, 2498–2502
(1998).
197. Carpentier, A. C. et al. On the suppression of plasma nonesterified fatty acids by insulin
during enhanced intravascular lipolysis in humans. Am. J. Physiol. Endocrinol. Metab. 289,
E849-856 (2005).
198. Boden, G. Obesity and free fatty acids. Endocrinol. Metab. Clin. North Am. 37, 635–646,
viii–ix (2008).
199. Boden, G. Free fatty acids-the link between obesity and insulin resistance. Endocr. Pract.
Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 7, 44–51 (2001).
200. Eguchi, K. et al. Saturated fatty acid and TLR signaling link β cell dysfunction and islet
inflammation. Cell Metab. 15, 518–533 (2012).
201. Mason, T. M. et al. Prolonged elevation of plasma free fatty acids desensitizes the insulin
secretory response to glucose in vivo in rats. Diabetes 48, 524–530 (1999).
202. Dobbins, R. L. et al. The composition of dietary fat directly influences glucose-stimulated
insulin secretion in rats. Diabetes 51, 1825–1833 (2002).
203. Xiao, C., Giacca, A., Carpentier, A. & Lewis, G. F. Differential effects of monounsaturated,
polyunsaturated and saturated fat ingestion on glucose-stimulated insulin secretion,
sensitivity and clearance in overweight and obese, non-diabetic humans. Diabetologia 49,
1371–1379 (2006).
204. Oprescu, A. I. et al. Free fatty acid-induced reduction in glucose-stimulated insulin
secretion: evidence for a role of oxidative stress in vitro and in vivo. Diabetes 56, 2927–
2937 (2007).
205. Koulajian, K. et al. Overexpression of glutathione peroxidase 4 prevents β-cell dysfunction
induced by prolonged elevation of lipids in vivo. AJP Endocrinol. Metab. 305, E254–E262
(2013).
206. Ji, Y. et al. Activation of rat intestinal mucosal mast cells by fat absorption. Am. J. Physiol.
Gastrointest. Liver Physiol. 302, G1292-1300 (2012).
207. Ji, Y. et al. Lymphatic diamine oxidase secretion stimulated by fat absorption is linked with
histamine release. Am. J. Physiol. Gastrointest. Liver Physiol. 304, G732-740 (2013).
208. Byrne, W. J. Intralipid or Liposyn--comparable products? J. Pediatr. Gastroenterol. Nutr. 1,
7–8 (1982).
209. Winzell, M. S. & Ahrén, B. The high-fat diet-fed mouse: a model for studying mechanisms
and treatment of impaired glucose tolerance and type 2 diabetes. Diabetes 53 Suppl 3, S215-
219 (2004).
210. Wang, C.-Y. & Liao, J. K. A mouse model of diet-induced obesity and insulin resistance.
Methods Mol. Biol. Clifton NJ 821, 421–433 (2012).
211. Hong, E.-G. et al. Interleukin-10 prevents diet-induced insulin resistance by attenuating
macrophage and cytokine response in skeletal muscle. Diabetes 58, 2525–2535 (2009).

118
212. Oprescu, A. I. et al. Free Fatty Acid Induced Reduction in Glucose-Stimulated Insulin
Secretion: Evidence for a Role of Oxidative Stress In Vitro and In Vivo. Diabetes 56, 2927–
2937 (2007).
213. Frigerio, F. et al. Peroxisome proliferator-activated receptor alpha (PPARalpha) protects
against oleate-induced INS-1E beta cell dysfunction by preserving carbohydrate metabolism.
Diabetologia 53, 331–340 (2010).
214. Tuo, Y. et al. Long-term in vitro treatment of INS-1 rat pancreatic β-cells by unsaturated
free fatty acids protects cells against gluco- and lipotoxicities via activation of GPR40
receptors. Clin. Exp. Pharmacol. Physiol. 39, 423–428 (2012).
215. Manukyan, L., Ubhayasekera, S. J. K. A., Bergquist, J., Sargsyan, E. & Bergsten, P.
Palmitate-induced impairments of β-cell function are linked with generation of specific
ceramide species via acylation of sphingosine. Endocrinology 156, 802–812 (2015).
216. Erion, K. A., Berdan, C. A., Burritt, N. E., Corkey, B. E. & Deeney, J. T. Chronic Exposure
to Excess Nutrients Left-shifts the Concentration Dependence of Glucose-stimulated Insulin
Secretion in Pancreatic β-Cells. J. Biol. Chem. 290, 16191–16201 (2015).
217. Hovsepyan, M., Sargsyan, E. & Bergsten, P. Palmitate-induced changes in protein
expression of insulin secreting INS-1E cells. J. Proteomics 73, 1148–1155 (2010).
218. Kashyap, S. et al. A sustained increase in plasma free fatty acids impairs insulin secretion in
nondiabetic subjects genetically predisposed to develop type 2 diabetes. Diabetes 52, 2461–
2474 (2003).
219. Kakekagumick, K. E. et al. Sandy lake health and diabetes project: a community-based
intervention targeting type 2 diabetes and its risk factors in a first nations community. Front.
Endocrinol. 4, 170 (2013).
220. Bajaj, M. et al. Sustained Reduction in Plasma Free Fatty Acid Concentration Improves
Insulin Action without Altering Plasma Adipocytokine Levels in Subjects with Strong
Family History of Type 2 Diabetes. J. Clin. Endocrinol. Metab. 89, 4649–4655 (2004).
221. Cusi, K., Kashyap, S., Gastaldelli, A., Bajaj, M. & Cersosimo, E. Effects on insulin secretion
and insulin action of a 48-h reduction of plasma free fatty acids with acipimox in
nondiabetic subjects genetically predisposed to type 2 diabetes. AJP Endocrinol. Metab.
292, E1775–E1781 (2007).
222. Paolisso, G. et al. Lowering fatty acids potentiates acute insulin response in first degree
relatives of people with type II diabetes. Diabetologia 41, 1127–1132 (1998).
223. Brassard, P. et al. Impaired Plasma Nonesterified Fatty Acid Tolerance Is an Early Defect in
the Natural History of Type 2 Diabetes. J. Clin. Endocrinol. Metab. 93, 837–844 (2008).
224. Mead, J. R., Irvine, S. A. & Ramji, D. P. Lipoprotein lipase: structure, function, regulation,
and role in disease. J. Mol. Med. Berl. Ger. 80, 753–769 (2002).
225. Almandoz, J. P. et al. Spillover of Fatty acids during dietary fat storage in type 2 diabetes:
relationship to body fat depots and effects of weight loss. Diabetes 62, 1897–1903 (2013).
226. Staiger, H., Machicao, F., Fritsche, A. & Häring, H.-U. Pathomechanisms of Type 2
Diabetes Genes. Endocr. Rev. 30, 557–585 (2009).

119
227. Riedel, M. J. & Light, P. E. Saturated and cis/trans unsaturated acyl CoA esters differentially
regulate wild-type and polymorphic beta-cell ATP-sensitive K+ channels. Diabetes 54,
2070–2079 (2005).
228. Butler, A. E. et al. Beta-cell deficit and increased beta-cell apoptosis in humans with type 2
diabetes. Diabetes 52, 102–110 (2003).
229. Wang, P. et al. Diabetes mellitus--advances and challenges in human β-cell proliferation.
Nat. Rev. Endocrinol. 11, 201–212 (2015).
230. Sauter, N. S., Schulthess, F. T., Galasso, R., Castellani, L. W. & Maedler, K. The
antiinflammatory cytokine interleukin-1 receptor antagonist protects from high-fat diet-
induced hyperglycemia. Endocrinology 149, 2208–2218 (2008).
231. Joseph, J. W. et al. Uncoupling protein 2 knockout mice have enhanced insulin secretory
capacity after a high-fat diet. Diabetes 51, 3211–3219 (2002).
232. Ahrén, B. et al. Islet perturbations in rats fed a high-fat diet. Pancreas 18, 75–83 (1999).
233. Steil, G. M. et al. Adaptation of beta-cell mass to substrate oversupply: enhanced function
with normal gene expression. Am. J. Physiol. Endocrinol. Metab. 280, E788-796 (2001).
234. Butler, A. E. et al. Beta-cell deficit and increased beta-cell apoptosis in humans with type 2
diabetes. Diabetes 52, 102–110 (2003).
235. Hennige, A. M. et al. Overexpression of kinase-negative protein kinase Cdelta in pancreatic
beta-cells protects mice from diet-induced glucose intolerance and beta-cell dysfunction.
Diabetes 59, 119–127 (2010).
236. Matveyenko, A. V. & Butler, P. C. Relationship between beta-cell mass and diabetes onset.
Diabetes Obes. Metab. 10 Suppl 4, 23–31 (2008).
237. Sone, H. & Kagawa, Y. Pancreatic beta cell senescence contributes to the pathogenesis of
type 2 diabetes in high-fat diet-induced diabetic mice. Diabetologia 48, 58–67 (2005).
238. Robertson, R. P., Harmon, J., Tran, P. O., Tanaka, Y. & Takahashi, H. Glucose toxicity in
beta-cells: type 2 diabetes, good radicals gone bad, and the glutathione connection. Diabetes
52, 581–587 (2003).
239. Tang, C. et al. Glucose-induced beta cell dysfunction in vivo in rats: link between oxidative
stress and endoplasmic reticulum stress. Diabetologia 55, 1366–1379 (2012).
240. Tang, C. et al. Evidence for a role of superoxide generation in glucose-induced beta-cell
dysfunction in vivo. Diabetes 56, 2722–2731 (2007).
241. Harmon, J. S., Stein, R. & Robertson, R. P. Oxidative stress-mediated, post-translational loss
of MafA protein as a contributing mechanism to loss of insulin gene expression in
glucotoxic beta cells. J. Biol. Chem. 280, 11107–11113 (2005).
242. Robertson, R. P., Tanaka, Y., Takahashi, H., Tran, P. O. T. & Harmon, J. S. Prevention of
oxidative stress by adenoviral overexpression of glutathione-related enzymes in pancreatic
islets. Ann. N. Y. Acad. Sci. 1043, 513–520 (2005).
243. Kaneto, H. et al. Activation of the hexosamine pathway leads to deterioration of pancreatic
beta-cell function through the induction of oxidative stress. J. Biol. Chem. 276, 31099–
31104 (2001).

120
244. Tanaka, Y., Tran, P. O. T., Harmon, J. & Robertson, R. P. A role for glutathione peroxidase
in protecting pancreatic beta cells against oxidative stress in a model of glucose toxicity.
Proc. Natl. Acad. Sci. U. S. A. 99, 12363–12368 (2002).
245. Tanaka, Y., Gleason, C. E., Tran, P. O., Harmon, J. S. & Robertson, R. P. Prevention of
glucose toxicity in HIT-T15 cells and Zucker diabetic fatty rats by antioxidants. Proc. Natl.
Acad. Sci. U. S. A. 96, 10857–10862 (1999).
246. Kaneto, H. et al. Beneficial effects of antioxidants in diabetes: possible protection of
pancreatic beta-cells against glucose toxicity. Diabetes 48, 2398–2406 (1999).
247. Gwiazda, K. S., Yang, T.-L. B., Lin, Y. & Johnson, J. D. Effects of palmitate on ER and
cytosolic Ca2+ homeostasis in -cells. AJP Endocrinol. Metab. 296, E690–E701 (2009).
248. Sako, Y. & Grill, V. E. A 48-hour lipid infusion in the rat time-dependently inhibits glucose-
induced insulin secretion and B cell oxidation through a process likely coupled to fatty acid
oxidation. Endocrinology 127, 1580–1589 (1990).
249. Hagman, D. K. et al. Cyclical and alternating infusions of glucose and intralipid in rats
inhibit insulin gene expression and Pdx-1 binding in islets. Diabetes 57, 424–431 (2008).
250. Boden, G., Ruiz, J., Kim, C. J. & Chen, X. Effects of prolonged glucose infusion on insulin
secretion, clearance, and action in normal subjects. Am. J. Physiol. 270, E251-258 (1996).
251. Chen, F. et al. Transcription factor Ets-1 links glucotoxicity to pancreatic beta cell
dysfunction through inhibiting PDX-1 expression in rodent models. Diabetologia (2015).
doi:10.1007/s00125-015-3805-3
252. Robertson, R. P., Harmon, J., Tran, P. O., Tanaka, Y. & Takahashi, H. Glucose toxicity in
beta-cells: type 2 diabetes, good radicals gone bad, and the glutathione connection. Diabetes
52, 581–587 (2003).
253. Zhang, X., Bao, Y., Ke, L. & Yu, Y. Elevated circulating free fatty acids levels causing
pancreatic islet cell dysfunction through oxidative stress. J. Endocrinol. Invest. 33, 388–394
(2010).
254. Ehses, J. A. et al. Toll-like receptor 2-deficient mice are protected from insulin resistance
and beta cell dysfunction induced by a high-fat diet. Diabetologia 53, 1795–1806 (2010).
255. Owyang, A. M. et al. XOMA 052, an anti-IL-1{beta} monoclonal antibody, improves
glucose control and {beta}-cell function in the diet-induced obesity mouse model.
Endocrinology 151, 2515–2527 (2010).
256. Gehrmann, W., Elsner, M. & Lenzen, S. Role of metabolically generated reactive oxygen
species for lipotoxicity in pancreatic β-cells. Diabetes Obes. Metab. 12 Suppl 2, 149–158
(2010).
257. Pi, J. & Collins, S. Reactive oxygen species and uncoupling protein 2 in pancreatic β-cell
function. Diabetes Obes. Metab. 12 Suppl 2, 141–148 (2010).
258. Li, N., Frigerio, F. & Maechler, P. The sensitivity of pancreatic β-cells to mitochondrial
injuries triggered by lipotoxicity and oxidative stress. Biochem. Soc. Trans. 36, 930–934
(2008).
259. Muoio, D. M. & Newgard, C. B. Fatty acid oxidation and insulin action: when less is more.
Diabetes 57, 1455–1456 (2008).

121
260. Newsholme, P. et al. Insights into the critical role of NADPH oxidase(s) in the normal and
dysregulated pancreatic beta cell. Diabetologia 52, 2489–2498 (2009).
261. Morgan, D. et al. Glucose, palmitate and pro-inflammatory cytokines modulate production
and activity of a phagocyte-like NADPH oxidase in rat pancreatic islets and a clonal beta
cell line. Diabetologia 50, 359–369 (2007).
262. Mamedova, L. K. et al. Toll-like receptor 4 signaling is required for induction of
gluconeogenic gene expression by palmitate in human hepatic carcinoma cells. J. Nutr.
Biochem. 24, 1499–1507 (2013).
263. Inoguchi, T. et al. High glucose level and free fatty acid stimulate reactive oxygen species
production through protein kinase C–dependent activation of NAD (P) H oxidase in cultured
vascular cells. Diabetes 49, 1939–1945 (2000).
264. Robertson, R. P. Oxidative stress and impaired insulin secretion in type 2 diabetes. Curr.
Opin. Pharmacol. 6, 615–619 (2006).
265. Evans, J. L., Goldfine, I. D., Maddux, B. A. & Grodsky, G. M. Oxidative Stress and Stress-
Activated Signaling Pathways: A Unifying Hypothesis of Type 2 Diabetes. Endocr. Rev. 23,
599–622 (2002).
266. Pi, J. et al. Reactive oxygen species as a signal in glucose-stimulated insulin secretion.
Diabetes 56, 1783–1791 (2007).
267. Brunner, Y., Schvartz, D., Priego-Capote, F., Couté, Y. & Sanchez, J.-C. Glucotoxicity and
pancreatic proteomics. J. Proteomics 71, 576–591 (2009).
268. Noh, S. R. et al. Oxidative stress biomarkers in long-term participants in clean-up work after
the Hebei Spirit oil spill. Sci. Total Environ. 515–516, 207–214 (2015).
269. Lenzen, S., Drinkgern, J. & Tiedge, M. Low antioxidant enzyme gene expression in
pancreatic islets compared with various other mouse tissues. Free Radic. Biol. Med. 20,
463–466 (1996).
270. Wang, X. et al. Gene and protein kinase expression profiling of reactive oxygen species-
associated lipotoxicity in the pancreatic beta-cell line MIN6. Diabetes 53, 129–140 (2004).
271. Robertson, R. P. & Harmon, J. S. Diabetes, glucose toxicity, and oxidative stress: A case of
double jeopardy for the pancreatic islet beta cell. Free Radic. Biol. Med. 41, 177–184
(2006).
272. Poitout, V. et al. Glucolipotoxicity of the pancreatic beta cell. Biochim. Biophys. Acta 1801,
289–298 (2010).
273. Evans, J. L., Goldfine, I. D., Maddux, B. A. & Grodsky, G. M. Are oxidative stress-activated
signaling pathways mediators of insulin resistance and beta-cell dysfunction? Diabetes 52,
1–8 (2003).
274. Maechler, P., Jornot, L. & Wollheim, C. B. Hydrogen peroxide alters mitochondrial
activation and insulin secretion in pancreatic beta cells. J. Biol. Chem. 274, 27905–27913
(1999).
275. Nita, I. I. et al. Pancreatic β-cell Na+ channels control global Ca2+ signaling and oxidative
metabolism by inducing Na+ and Ca2+ responses that are propagated into mitochondria.
FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 28, 3301–3312 (2014).

122
276. Robson-Doucette, C. A. et al. Beta-cell uncoupling protein 2 regulates reactive oxygen
species production, which influences both insulin and glucagon secretion. Diabetes 60,
2710–2719 (2011).
277. Produit-Zengaffinen, N. et al. Increasing uncoupling protein-2 in pancreatic beta cells does
not alter glucose-induced insulin secretion but decreases production of reactive oxygen
species. Diabetologia 50, 84–93 (2007).
278. Rial, E. et al. Lipotoxicity, fatty acid uncoupling and mitochondrial carrier function.
Biochim. Biophys. Acta 1797, 800–806 (2010).
279. Frijhoff, J. et al. The mitochondrial reactive oxygen species regulator p66Shc controls
PDGF-induced signaling and migration through protein tyrosine phosphatase oxidation. Free
Radic. Biol. Med. 68, 268–277 (2014).
280. Shintani, T. et al. The R3 receptor-like protein tyrosine phosphatase subfamily inhibits
insulin signalling by dephosphorylating the insulin receptor at specific sites. J. Biochem.
(Tokyo) 158, 235–243 (2015).
281. Karaskov, E. et al. Chronic palmitate but not oleate exposure induces endoplasmic reticulum
stress, which may contribute to INS-1 pancreatic beta-cell apoptosis. Endocrinology 147,
3398–3407 (2006).
282. Cunha, D. A. et al. Initiation and execution of lipotoxic ER stress in pancreatic beta-cells. J.
Cell Sci. 121, 2308–2318 (2008).
283. Cnop, M., Ladrière, L., Igoillo-Esteve, M., Moura, R. F. & Cunha, D. A. Causes and cures
for endoplasmic reticulum stress in lipotoxic β-cell dysfunction. Diabetes Obes. Metab. 12
Suppl 2, 76–82 (2010).
284. Cnop, M., Igoillo-Esteve, M., Cunha, D. A., Ladrière, L. & Eizirik, D. L. An update on
lipotoxic endoplasmic reticulum stress in pancreatic beta-cells. Biochem. Soc. Trans. 36,
909–915 (2008).
285. Azevedo-Martins, A. K. et al. Improvement of the mitochondrial antioxidant defense status
prevents cytokine-induced nuclear factor-kappaB activation in insulin-producing cells.
Diabetes 52, 93–101 (2003).
286. Rehman, K. K. et al. Protection of islets by in situ peptide-mediated transduction of the
Ikappa B kinase inhibitor Nemo-binding domain peptide. J. Biol. Chem. 278, 9862–9868
(2003).
287. Zeender, E. et al. Pioglitazone and sodium salicylate protect human beta-cells against
apoptosis and impaired function induced by glucose and interleukin-1beta. J. Clin.
Endocrinol. Metab. 89, 5059–5066 (2004).
288. Kharroubi, I. et al. Free fatty acids and cytokines induce pancreatic beta-cell apoptosis by
different mechanisms: role of nuclear factor-kappaB and endoplasmic reticulum stress.
Endocrinology 145, 5087–5096 (2004).
289. Hammar, E. B. et al. Activation of NF-kappaB by extracellular matrix is involved in
spreading and glucose-stimulated insulin secretion of pancreatic beta cells. J. Biol. Chem.
280, 30630–30637 (2005).

123
290. Norlin, S., Ahlgren, U. & Edlund, H. Nuclear factor-{kappa}B activity in {beta}-cells is
required for glucose-stimulated insulin secretion. Diabetes 54, 125–132 (2005).
291. Fernández-Real, J.-M. et al. Salicylates increase insulin secretion in healthy obese subjects.
J. Clin. Endocrinol. Metab. 93, 2523–2530 (2008).
292. Chen, M. & Robertson, R. P. Restoration of the acute insulin response by sodium salicylate.
A glucose dose-related phenomenon. Diabetes 27, 750–756 (1978).
293. Giugliano, D. et al. Studies on the mechanism of salicylate-induced increase of insulin
secretion in man. Diabète Métabolisme 14, 431–436 (1988).
294. Kaneto, H. et al. Oxidative stress, ER stress, and the JNK pathway in type 2 diabetes. J. Mol.
Med. Berl. Ger. 83, 429–439 (2005).
295. Karin, M. How NF-kappaB is activated: the role of the IkappaB kinase (IKK) complex.
Oncogene 18, 6867–6874 (1999).
296. Tam, A. B., Mercado, E. L., Hoffmann, A. & Niwa, M. ER stress activates NF-κB by
integrating functions of basal IKK activity, IRE1 and PERK. PloS One 7, e45078 (2012).
297. Jiao, P. et al. FFA-induced adipocyte inflammation and insulin resistance: involvement of
ER stress and IKKβ pathways. Obes. Silver Spring Md 19, 483–491 (2011).
298. Ma, X.-F. et al. IKKβ/NF-κB mediated the low doses of bisphenol A induced migration of
cervical cancer cells. Arch. Biochem. Biophys. 573, 52–58 (2015).
299. Kiely, A., Robinson, A., McClenaghan, N. H., Flatt, P. R. & Newsholme, P. Toll-like
receptor agonist induced changes in clonal rat BRIN-BD11 beta-cell insulin secretion and
signal transduction. J. Endocrinol. 202, 365–373 (2009).
300. Solinas, G., Naugler, W., Galimi, F., Lee, M.-S. & Karin, M. Saturated fatty acids inhibit
induction of insulin gene transcription by JNK-mediated phosphorylation of insulin-receptor
substrates. Proc. Natl. Acad. Sci. U. S. A. 103, 16454–16459 (2006).
301. Essers, M. A. G. et al. FOXO transcription factor activation by oxidative stress mediated by
the small GTPase Ral and JNK. EMBO J. 23, 4802–4812 (2004).
302. Kitamura, T. et al. The forkhead transcription factor Foxo1 links insulin signaling to Pdx1
regulation of pancreatic beta cell growth. J. Clin. Invest. 110, 1839–1847 (2002).
303. Gupta, D. et al. Peroxisome proliferator-activated receptor γ (PPARγ) and its target genes
are downstream effectors of FoxO1 protein in islet β-cells: mechanism of β-cell
compensation and failure. J. Biol. Chem. 288, 25440–25449 (2013).
304. Mellor, H. & Parker, P. J. The extended protein kinase C superfamily. Biochem. J. 332 ( Pt
2), 281–292 (1998).
305. Kulkarni, R. N. Receptors for insulin and insulin-like growth factor-1 and insulin receptor
substrate-1 mediate pathways that regulate islet function. Biochem. Soc. Trans. 30, 317–322
(2002).
306. Nolan, C. J., Madiraju, M. S. R., Delghingaro-Augusto, V., Peyot, M.-L. & Prentki, M. Fatty
acid signaling in the beta-cell and insulin secretion. Diabetes 55 Suppl 2, S16-23 (2006).
307. Koya, D. & King, G. L. Protein kinase C activation and the development of diabetic
complications. Diabetes 47, 859–866 (1998).

124
308. Geraldes, P. & King, G. L. Activation of protein kinase C isoforms and its impact on
diabetic complications. Circ. Res. 106, 1319–1331 (2010).
309. Idris, I., Gray, S. & Donnelly, R. Protein kinase C activation: isozyme-specific effects on
metabolism and cardiovascular complications in diabetes. Diabetologia 44, 659–673 (2001).
310. Boslem, E., Meikle, P. J. & Biden, T. J. Roles of ceramide and sphingolipids in pancreatic β-
cell function and dysfunction. Islets 4, 177–187 (2012).
311. Lang, F., Ullrich, S. & Gulbins, E. Ceramide formation as a target in beta-cell survival and
function. Expert Opin. Ther. Targets 15, 1061–1071 (2011).
312. Greene, M. W., Morrice, N., Garofalo, R. S. & Roth, R. A. Modulation of human insulin
receptor substrate-1 tyrosine phosphorylation by protein kinase Cdelta. Biochem. J. 378,
105–116 (2004).
313. Bernal-Mizrachi, E. et al. Defective insulin secretion and increased susceptibility to
experimental diabetes are induced by reduced Akt activity in pancreatic islet beta cells. J.
Clin. Invest. 114, 928–936 (2004).
314. Schmitz-Peiffer, C. et al. Inhibition of PKCepsilon improves glucose-stimulated insulin
secretion and reduces insulin clearance. Cell Metab. 6, 320–328 (2007).
315. Prentki, M. & Nolan, C. J. Islet beta cell failure in type 2 diabetes. J. Clin. Invest. 116,
1802–1812 (2006).
316. Chen, S. et al. Oleate-induced decrease in hepatocyte insulin binding is mediated by PKC-
delta. Biochem. Biophys. Res. Commun. 346, 931–937 (2006).
317. Carpentier, J. L. Robert Feulgen Prize Lecture 1993. The journey of the insulin receptor into
the cell: from cellular biology to pathophysiology. Histochemistry 100, 169–184 (1993).
318. Carpentier, J. L. Insulin receptor internalization: molecular mechanisms and
physiopathological implications. Diabetologia 37 Suppl 2, S117-124 (1994).
319. Fournès, B., Sadekova, S., Turbide, C., Létourneau, S. & Beauchemin, N. The CEACAM1-
L Ser503 residue is crucial for inhibition of colon cancer cell tumorigenicity. Oncogene 20,
219–230 (2001).
320. Hagman, D. K., Hays, L. B., Parazzoli, S. D. & Poitout, V. Palmitate inhibits insulin gene
expression by altering PDX-1 nuclear localization and reducing MafA expression in isolated
rat islets of Langerhans. J. Biol. Chem. 280, 32413–32418 (2005).
321. Maedler, K., Oberholzer, J., Bucher, P., Spinas, G. A. & Donath, M. Y. Monounsaturated
fatty acids prevent the deleterious effects of palmitate and high glucose on human pancreatic
beta-cell turnover and function. Diabetes 52, 726–733 (2003).
322. Shimabukuro, M. et al. Lipoapoptosis in beta-cells of obese prediabetic fa/fa rats. Role of
serine palmitoyltransferase overexpression. J. Biol. Chem. 273, 32487–32490 (1998).
323. Haigis, M. C. & Sinclair, D. A. Mammalian sirtuins: biological insights and disease
relevance. Annu. Rev. Pathol. 5, 253–295 (2010).
324. Sinclair, D. A. & Guarente, L. Unlocking the secrets of longevity genes. Sci. Am. 294, 48–
51, 54–57 (2006).

125
325. Imai, S., Armstrong, C. M., Kaeberlein, M. & Guarente, L. Transcriptional silencing and
longevity protein Sir2 is an NAD-dependent histone deacetylase. Nature 403, 795–800
(2000).
326. Kaeberlein, M., McVey, M. & Guarente, L. The SIR2/3/4 complex and SIR2 alone promote
longevity in Saccharomyces cerevisiae by two different mechanisms. Genes Dev. 13, 2570–
2580 (1999).
327. Sinclair, D. A. & Guarente, L. Extrachromosomal rDNA circles--a cause of aging in yeast.
Cell 91, 1033–1042 (1997).
328. Sanders, B. D., Jackson, B. & Marmorstein, R. Structural basis for sirtuin function: what we
know and what we don’t. Biochim. Biophys. Acta 1804, 1604–1616 (2010).
329. Lavu, S., Boss, O., Elliott, P. J. & Lambert, P. D. Sirtuins--novel therapeutic targets to treat
age-associated diseases. Nat. Rev. Drug Discov. 7, 841–853 (2008).
330. Kong, X.-X. et al. Function of SIRT1 in physiology. Biochem. Biokhimii︠ a︡ 74, 703–708
(2009).
331. Imai, S. & Guarente, L. Ten years of NAD-dependent SIR2 family deacetylases:
implications for metabolic diseases. Trends Pharmacol. Sci. 31, 212–220 (2010).
332. Picard, F. et al. Sirt1 promotes fat mobilization in white adipocytes by repressing PPAR-
gamma. Nature 429, 771–776 (2004).
333. Rodgers, J. T. et al. Nutrient control of glucose homeostasis through a complex of PGC-
1alpha and SIRT1. Nature 434, 113–118 (2005).
334. Pfluger, P. T., Herranz, D., Velasco-Miguel, S., Serrano, M. & Tschöp, M. H. Sirt1 protects
against high-fat diet-induced metabolic damage. Proc. Natl. Acad. Sci. 105, 9793–9798
(2008).
335. Moynihan, K. A. et al. Increased dosage of mammalian Sir2 in pancreatic β cells enhances
glucose-stimulated insulin secretion in mice. Cell Metab. 2, 105–117 (2005).
336. Bordone, L. et al. Sirt1 regulates insulin secretion by repressing UCP2 in pancreatic beta
cells. PLoS Biol. 4, e31 (2006).
337. Erion, D. M. et al. SirT1 knockdown in liver decreases basal hepatic glucose production and
increases hepatic insulin responsiveness in diabetic rats. Proc. Natl. Acad. Sci. U. S. A. 106,
11288–11293 (2009).
338. Monteiro, J. P. & Cano, M. I. N. SIRT1 deacetylase activity and the maintenance of protein
homeostasis in response to stress: an overview. Protein Pept. Lett. 18, 167–173 (2011).
339. Shao, S., Yang, Y., Yuan, G., Zhang, M. & Yu, X. Signaling molecules involved in lipid-
induced pancreatic beta-cell dysfunction. DNA Cell Biol. 32, 41–49 (2013).
340. Vetterli, L. & Maechler, P. Resveratrol-activated SIRT1 in liver and pancreatic β-cells: a
Janus head looking to the same direction of metabolic homeostasis. Aging 3, 444–449
(2011).
341. Michishita, E., Park, J. Y., Burneskis, J. M., Barrett, J. C. & Horikawa, I. Evolutionarily
conserved and nonconserved cellular localizations and functions of human SIRT proteins.
Mol. Biol. Cell 16, 4623–4635 (2005).

126
342. Jin, Q. et al. Cytoplasm-localized SIRT1 enhances apoptosis. J. Cell. Physiol. 213, 88–97
(2007).
343. Tanno, M., Sakamoto, J., Miura, T., Shimamoto, K. & Horio, Y. Nucleocytoplasmic
shuttling of the NAD+-dependent histone deacetylase SIRT1. J. Biol. Chem. 282, 6823–
6832 (2007).
344. Vetterli, L., Brun, T., Giovannoni, L., Bosco, D. & Maechler, P. Resveratrol potentiates
glucose-stimulated insulin secretion in INS-1E beta-cells and human islets through a SIRT1-
dependent mechanism. J. Biol. Chem. 286, 6049–6060 (2011).
345. Affourtit, C. & Brand, M. D. On the role of uncoupling protein-2 in pancreatic beta cells.
Biochim. Biophys. Acta BBA - Bioenerg. 1777, 973–979 (2008).
346. Chan, C. B. et al. Increased uncoupling protein-2 levels in beta-cells are associated with
impaired glucose-stimulated insulin secretion: mechanism of action. Diabetes 50, 1302–
1310 (2001).
347. Lee, S. C., Robson-Doucette, C. A. & Wheeler, M. B. Uncoupling protein 2 regulates
reactive oxygen species formation in islets and influences susceptibility to diabetogenic
action of streptozotocin. J. Endocrinol. 203, 33–43 (2009).
348. Hsu, C.-P. et al. Silent information regulator 1 protects the heart from ischemia/reperfusion.
Circulation 122, 2170–2182 (2010).
349. Zhang, C. Y. et al. Uncoupling protein-2 negatively regulates insulin secretion and is a
major link between obesity, beta cell dysfunction, and type 2 diabetes. Cell 105, 745–755
(2001).
350. Pi, J. et al. Persistent oxidative stress due to absence of uncoupling protein 2 associated with
impaired pancreatic beta-cell function. Endocrinology 150, 3040–3048 (2009).
351. Ježek, P. et al. Antioxidant and regulatory role of mitochondrial uncoupling protein UCP2 in
pancreatic beta-cells. Physiol Res 63, S73–S91 (2014).
352. Saleh, M. C., Wheeler, M. B. & Chan, C. B. Endogenous islet uncoupling protein-2
expression and loss of glucose homeostasis in ob/ob mice. J. Endocrinol. 190, 659–667
(2006).
353. Ramsey, K. M., Mills, K. F., Satoh, A. & Imai, S. Age-associated loss of Sirt1-mediated
enhancement of glucose-stimulated insulin secretion in beta cell-specific Sirt1-
overexpressing (BESTO) mice. Aging Cell 7, 78–88 (2008).
354. Galetti, S. et al. Fatty acids do not activate UCP2 in pancreatic beta cells: comparison with
UCP1. Pflüg. Arch. Eur. J. Physiol. 457, 931–940 (2009).
355. Schug, T. T. & Li, X. Sirtuin 1 in lipid metabolism and obesity. Ann. Med. 43, 198–211
(2011).
356. Bovenga, F., Sabbà, C. & Moschetta, A. Uncoupling nuclear receptor LXR and cholesterol
metabolism in cancer. Cell Metab. 21, 517–526 (2015).
357. González-Rodríguez, Á. et al. Resveratrol treatment restores peripheral insulin sensitivity in
diabetic mice in a sirt1-independent manner. Mol. Nutr. Food Res. 59, 1431–1442 (2015).

127
358. Imai, S. & Guarente, L. Ten years of NAD-dependent SIR2 family deacetylases:
implications for metabolic diseases. Trends Pharmacol. Sci. 31, 212–220 (2010).
359. Qiao, L. & Shao, J. SIRT1 regulates adiponectin gene expression through Foxo1-
C/enhancer-binding protein alpha transcriptional complex. J. Biol. Chem. 281, 39915–39924
(2006).
360. Banks, A. S. et al. SirT1 gain of function increases energy efficiency and prevents diabetes
in mice. Cell Metab. 8, 333–341 (2008).
361. Sun, C. et al. SIRT1 Improves Insulin Sensitivity under Insulin-Resistant Conditions by
Repressing PTP1B. Cell Metab. 6, 307–319 (2007).
362. Combs, A. P. Recent advances in the discovery of competitive protein tyrosine phosphatase
1B inhibitors for the treatment of diabetes, obesity, and cancer. J. Med. Chem. 53, 2333–
2344 (2010).
363. Delibegovic, M. et al. Improved glucose homeostasis in mice with muscle-specific deletion
of protein-tyrosine phosphatase 1B. Mol. Cell. Biol. 27, 7727–7734 (2007).
364. Elchebly, M. et al. Increased insulin sensitivity and obesity resistance in mice lacking the
protein tyrosine phosphatase-1B gene. Science 283, 1544–1548 (1999).
365. Coppari, R. Metabolic actions of hypothalamic SIRT1. Trends Endocrinol. Metab. TEM 23,
179–185 (2012).
366. Ramadori, G. et al. Brain SIRT1: anatomical distribution and regulation by energy
availability. J. Neurosci. Off. J. Soc. Neurosci. 28, 9989–9996 (2008).
367. Ramadori, G. et al. SIRT1 deacetylase in SF1 neurons protects against metabolic imbalance.
Cell Metab. 14, 301–312 (2011).
368. Ramadori, G. et al. SIRT1 deacetylase in POMC neurons is required for homeostatic
defenses against diet-induced obesity. Cell Metab. 12, 78–87 (2010).
369. Torres, G., Dileo, J. N., Hallas, B. H., Horowitz, J. M. & Leheste, J. R. Silent information
regulator 1 mediates hippocampal plasticity through presenilin1. Neuroscience 179, 32–40
(2011).
370. Guo, W. et al. Sirt1 overexpression in neurons promotes neurite outgrowth and cell survival
through inhibition of the mTOR signaling. J. Neurosci. Res. 89, 1723–1736 (2011).
371. Finkel, T., Deng, C.-X. & Mostoslavsky, R. Recent progress in the biology and physiology
of sirtuins. Nature 460, 587–591 (2009).
372. Brunet, A. et al. Stress-dependent regulation of FOXO transcription factors by the SIRT1
deacetylase. Science 303, 2011–2015 (2004).
373. Tao, R. et al. Hepatic FoxOs regulate lipid metabolism via modulation of expression of the
nicotinamide phosphoribosyltransferase gene. J. Biol. Chem. 286, 14681–14690 (2011).
374. Chuang, P. Y. et al. Alteration of Forkhead Box O (Foxo4) Acetylation Mediates Apoptosis
of Podocytes in Diabetes Mellitus. PLoS ONE 6, e23566 (2011).
375. Kim, D. H., Zhang, T., Lee, S. & Dong, H. H. FoxO6 in glucose metabolism (FoxO6). J.
Diabetes 5, 233–240 (2013).

128
376. Calabuig-Navarro, V. et al. Forkhead Box O6 (FoxO6) Depletion Attenuates Hepatic
Gluconeogenesis and Protects against Fat-induced Glucose Disorder in Mice. J. Biol. Chem.
290, 15581–15594 (2015).
377. Glauser, D. A. & Schlegel, W. The emerging role of FOXO transcription factors in
pancreatic beta cells. J. Endocrinol. 193, 195–207 (2007).
378. Marinkovic, D. et al. Foxo3 is required for the regulation of oxidative stress in
erythropoiesis. J. Clin. Invest. 117, 2133–2144 (2007).
379. Kitamura, Y. I. et al. FoxO1 protects against pancreatic beta cell failure through NeuroD and
MafA induction. Cell Metab. 2, 153–163 (2005).
380. Kitamura, Y. I. et al. FoxO1 protects against pancreatic β cell failure through NeuroD and
MafA induction. Cell Metab. 2, 153–163 (2005).
381. Xiong, S., Salazar, G., Patrushev, N. & Alexander, R. W. FoxO1 mediates an autofeedback
loop regulating SIRT1 expression. J. Biol. Chem. 286, 5289–5299 (2011).
382. Nemoto, S., Fergusson, M. M. & Finkel, T. Nutrient availability regulates SIRT1 through a
forkhead-dependent pathway. Science 306, 2105–2108 (2004).
383. Ho, C., van der Veer, E., Akawi, O. & Pickering, J. G. SIRT1 markedly extends replicative
lifespan if the NAD+ salvage pathway is enhanced. FEBS Lett. 583, 3081–3085 (2009).
384. Zhang, T. et al. Enzymes in the NAD+ salvage pathway regulate SIRT1 activity at target
gene promoters. J. Biol. Chem. 284, 20408–20417 (2009).
385. Kulkarni, S. R. et al. Fasting induces nuclear factor E2-related factor 2 and ATP-binding
Cassette transporters via protein kinase A and Sirtuin-1 in mouse and human. Antioxid.
Redox Signal. 20, 15–30 (2014).
386. Rickenbacher, A. et al. Fasting protects liver from ischemic injury through Sirt1-mediated
downregulation of circulating HMGB1 in mice. J. Hepatol. 61, 301–308 (2014).
387. Yamamoto, M. et al. SIRT1 regulates adaptive response of the growth hormone--insulin-like
growth factor-I axis under fasting conditions in liver. Proc. Natl. Acad. Sci. U. S. A. 110,
14948–14953 (2013).
388. Imai, S. & Yoshino, J. The importance of NAMPT/NAD/SIRT1 in the systemic regulation
of metabolism and ageing. Diabetes Obes. Metab. 15 Suppl 3, 26–33 (2013).
389. Fang, M., Guo, W.-R., Park, Y., Kang, H.-G. & Zarbl, H. Enhancement of NAD+-dependent
SIRT1 deacetylase activity by methylselenocysteine resets the circadian clock in carcinogen-
treated mammary epithelial cells. Oncotarget 6, 42879–42891 (2015).
390. Cerutti, R. et al. NAD(+)-dependent activation of Sirt1 corrects the phenotype in a mouse
model of mitochondrial disease. Cell Metab. 19, 1042–1049 (2014).
391. Chung, S. et al. Regulation of SIRT1 in cellular functions: role of polyphenols. Arch.
Biochem. Biophys. 501, 79–90 (2010).
392. Rogina, B. & Helfand, S. L. Sir2 mediates longevity in the fly through a pathway related to
calorie restriction. Proc. Natl. Acad. Sci. U. S. A. 101, 15998–16003 (2004).
393. Weindruch, R. The retardation of aging by caloric restriction: studies in rodents and
primates. Toxicol. Pathol. 24, 742–745 (1996).

129
394. Cohen, H. Y. et al. Calorie restriction promotes mammalian cell survival by inducing the
SIRT1 deacetylase. Science 305, 390–392 (2004).
395. Guarente, L. & Picard, F. Calorie restriction--the SIR2 connection. Cell 120, 473–482
(2005).
396. Boily, G. et al. SirT1 regulates energy metabolism and response to caloric restriction in
mice. PloS One 3, e1759 (2008).
397. Chen, D. et al. Tissue-specific regulation of SIRT1 by calorie restriction. Genes Dev. 22,
1753–1757 (2008).
398. Canbay, A., Bechmann, L. & Gerken, G. Lipid metabolism in the liver. Z. Für
Gastroenterol. 45, 35–41 (2007).
399. Wu, L. et al. Activation of SIRT1 protects pancreatic β-cells against palmitate-induced
dysfunction. Biochim. Biophys. Acta BBA - Mol. Basis Dis. 1822, 1815–1825 (2012).
400. Garcia-Lorda, P., Nash, W., Roche, A., Pi-Sunyer, F.-X. & Laferrere, B. Intralipid/heparin
infusion suppresses serum leptin in humans. Eur. J. Endocrinol. Eur. Fed. Endocr. Soc. 148,
669–676 (2003).
401. Chung, S. et al. Regulation of SIRT1 in cellular functions: Role of polyphenols. Arch.
Biochem. Biophys. 501, 79–90 (2010).
402. Ho, C., van der Veer, E., Akawi, O. & Pickering, J. G. SIRT1 markedly extends replicative
lifespan if the NAD+ salvage pathway is enhanced. FEBS Lett. 583, 3081–3085 (2009).
403. Furukawa, A., Tada-Oikawa, S., Kawanishi, S. & Oikawa, S. H2O2 accelerates cellular
senescence by accumulation of acetylated p53 via decrease in the function of SIRT1 by
NAD+ depletion. Cell. Physiol. Biochem. Int. J. Exp. Cell. Physiol. Biochem. Pharmacol.
20, 45–54 (2007).
404. Bai, P. et al. PARP-1 inhibition increases mitochondrial metabolism through SIRT1
activation. Cell Metab. 13, 461–468 (2011).
405. Bai, P. et al. PARP-2 regulates SIRT1 expression and whole-body energy expenditure. Cell
Metab. 13, 450–460 (2011).
406. Nasrin, N. et al. JNK1 Phosphorylates SIRT1 and Promotes Its Enzymatic Activity. PLoS
ONE 4, e8414 (2009).
407. Gao, Z. et al. Sirtuin 1 (SIRT1) Protein Degradation in Response to Persistent c-Jun N-
terminal Kinase 1 (JNK1) Activation Contributes to Hepatic Steatosis in Obesity. J. Biol.
Chem. 286, 22227–22234 (2011).
408. Caito, S. et al. SIRT1 is a redox-sensitive deacetylase that is post-translationally modified by
oxidants and carbonyl stress. FASEB J. 24, 3145–3159 (2010).
409. Sasaki, T. et al. Phosphorylation regulates SIRT1 function. PloS One 3, (2008).
410. Kim, E.-J., Kho, J.-H., Kang, M.-R. & Um, S.-J. Active regulator of SIRT1 cooperates with
SIRT1 and facilitates suppression of p53 activity. Mol. Cell 28, 277–290 (2007).
411. Zschoernig, B. & Mahlknecht, U. SIRTUIN 1: regulating the regulator. Biochem. Biophys.
Res. Commun. 376, 251–255 (2008).

130
412. Escande, C. et al. Deleted in breast cancer-1 regulates SIRT1 activity and contributes to
high-fat diet-induced liver steatosis in mice. J. Clin. Invest. 120, 545–558 (2010).
413. Zannini, L., Buscemi, G., Kim, J.-E., Fontanella, E. & Delia, D. DBC1 phosphorylation by
ATM/ATR inhibits SIRT1 deacetylase in response to DNA damage. J. Mol. Cell Biol. 4,
294–303 (2012).
414. Yuan, J., Luo, K., Liu, T. & Lou, Z. Regulation of SIRT1 activity by genotoxic stress. Genes
Dev. 26, 791–796 (2012).
415. Nin, V. et al. Role of deleted in breast cancer 1 (DBC1) protein in SIRT1 deacetylase
activation induced by protein kinase A and AMP-activated protein kinase. J. Biol. Chem.
287, 23489–23501 (2012).
416. Gerhart-Hines, Z. et al. The cAMP/PKA pathway rapidly activates SIRT1 to promote fatty
acid oxidation independently of changes in NAD(+). Mol. Cell 44, 851–863 (2011).
417. Escande, C. et al. Deleted in breast cancer-1 regulates SIRT1 activity and contributes to
high-fat diet-induced liver steatosis in mice. J. Clin. Invest. 120, 545–558 (2010).
418. Milne, J. C. et al. Small molecule activators of SIRT1 as therapeutics for the treatment of
type 2 diabetes. Nature 450, 712–716 (2007).
419. Chen, W. W., Niepel, M. & Sorger, P. K. Classic and contemporary approaches to modeling
biochemical reactions. Genes Dev. 24, 1861–1875 (2010).
420. Cantó, C. et al. Interdependence of AMPK and SIRT1 for metabolic adaptation to fasting
and exercise in skeletal muscle. Cell Metab. 11, 213–219 (2010).
421. Fulco, M. et al. Glucose restriction inhibits skeletal myoblast differentiation by activating
SIRT1 through AMPK-mediated regulation of Nampt. Dev. Cell 14, 661–673 (2008).
422. Moynihan, K. A. et al. Increased dosage of mammalian Sir2 in pancreatic beta cells
enhances glucose-stimulated insulin secretion in mice. Cell Metab. 2, 105–117 (2005).
423. Revollo, J. R. et al. Nampt/PBEF/Visfatin regulates insulin secretion in beta cells as a
systemic NAD biosynthetic enzyme. Cell Metab. 6, 363–375 (2007).
424. Yoshino, J., Mills, K. F., Yoon, M. J. & Imai, S. Nicotinamide Mononucleotide, a Key
NAD+ Intermediate, Treats the Pathophysiology of Diet- and Age-Induced Diabetes in
Mice. Cell Metab. 14, 528–536 (2011).
425. Denu, J. M. Vitamins and aging: pathways to NAD+ synthesis. Cell 129, 453–454 (2007).
426. Imai, S.-I. Nicotinamide phosphoribosyltransferase (Nampt): a link between NAD biology,
metabolism, and diseases. Curr. Pharm. Des. 15, 20–28 (2009).
427. Caton, P. W., Kieswich, J., Yaqoob, M. M., Holness, M. J. & Sugden, M. C. Nicotinamide
mononucleotide protects against pro-inflammatory cytokine-mediated impairment of mouse
islet function. Diabetologia 54, 3083–3092 (2011).
428. Zhu, N., Olivera, B. M. & Roth, J. R. Activity of the nicotinamide mononucleotide transport
system is regulated in Salmonella typhimurium. J. Bacteriol. 173, 1311–1320 (1991).
429. Sauer, E., Merdanovic, M., Mortimer, A. P., Bringmann, G. & Reidl, J. PnuC and the
utilization of the nicotinamide riboside analog 3-aminopyridine in Haemophilus influenzae.
Antimicrob. Agents Chemother. 48, 4532–4541 (2004).

131
430. Imai, S. & Guarente, L. Ten years of NAD-dependent SIR2 family deacetylases:
implications for metabolic diseases. Trends Pharmacol. Sci. 31, 212–220 (2010).
431. Imai, S.-I. ‘Clocks’ in the NAD World: NAD as a metabolic oscillator for the regulation of
metabolism and aging. Biochim. Biophys. Acta 1804, 1584–1590 (2010).
432. Lowell, B. B. & Shulman, G. I. Mitochondrial dysfunction and type 2 diabetes. Science 307,
384–387 (2005).
433. Andreone, T., Meares, G. P., Hughes, K. J., Hansen, P. A. & Corbett, J. A. Cytokine-
mediated -cell damage in PARP-1-deficient islets. AJP Endocrinol. Metab. 303, E172–E179
(2012).
434. Szkudelski, T. Streptozotocin-nicotinamide-induced diabetes in the rat. Characteristics of the
experimental model. Exp. Biol. Med. Maywood NJ 237, 481–490 (2012).
435. Fukaya, M. et al. Protective effects of a nicotinamide derivative, isonicotinamide, against
streptozotocin-induced β-cell damage and diabetes in mice. Biochem. Biophys. Res.
Commun. 442, 92–98 (2013).
436. Szkudelska, K., Nogowski, L. & Szkudelski, T. Adipocyte dysfunction in rats with
streptozotocin-nicotinamide-induced diabetes. Int. J. Exp. Pathol. 95, 86–94 (2014).
437. Green, M. F. & Hirschey, M. D. SIRT3 weighs heavily in the metabolic balance: a new role
for SIRT3 in metabolic syndrome. J. Gerontol. A. Biol. Sci. Med. Sci. 68, 105–107 (2013).
438. Caton, P. W. et al. Sirtuin 3 regulates mouse pancreatic beta cell function and is suppressed
in pancreatic islets isolated from human type 2 diabetic patients. Diabetologia 56, 1068–
1077 (2013).
439. Yoshino, J. & Imai, S. Mitochondrial SIRT3: a new potential therapeutic target for
metabolic syndrome. Mol. Cell 44, 170–171 (2011).
440. Hirschey, M. D. et al. SIRT3 deficiency and mitochondrial protein hyperacetylation
accelerate the development of the metabolic syndrome. Mol. Cell 44, 177–190 (2011).
441. Zhang, H.-H. et al. SIRT1 overexpression in skeletal muscle in vivo induces increased
insulin sensitivity and enhanced complex I but not complex II-V functions in individual
subsarcolemmal and intermyofibrillar mitochondria. J. Physiol. Biochem. 71, 177–190
(2015).
442. McLaughlin, T., Abbasi, F., Lamendola, C., Kim, H. S. & Reaven, G. M. Metabolic changes
following sibutramine-assisted weight loss in obese individuals: role of plasma free fatty
acids in the insulin resistance of obesity. Metabolism. 50, 819–824 (2001).
443. Varady, K. A. et al. Effects of weight loss via high fat vs. low fat alternate day fasting diets
on free fatty acid profiles. Sci. Rep. 5, 7561 (2015).
444. Blaha, V. et al. Effects of body fat reduction on plasma adipocyte fatty acid-binding protein
concentration in obese patients with type 1 diabetes mellitus. Neuro Endocrinol. Lett. 33
Suppl 2, 6–12 (2012).
445. Qvigstad, E., Mostad, I. L., Bjerve, K. S. & Grill, V. E. Acute lowering of circulating fatty
acids improves insulin secretion in a subset of type 2 diabetes subjects. Am. J. Physiol.
Endocrinol. Metab. 284, E129-137 (2003).

132
446. Goh, T. T. et al. Lipid-induced beta-cell dysfunction in vivo in models of progressive beta-
cell failure. Am. J. Physiol. Endocrinol. Metab. 292, E549-560 (2007).
447. Worm, D. et al. Pronounced blood glucose-lowering effect of the antilipolytic drug acipimox
in noninsulin-dependent diabetes mellitus patients during a 3-day intensified treatment
period. J. Clin. Endocrinol. Metab. 78, 717–721 (1994).
448. Novials, A., Montane, J. & Cadavez-Trigo, L. Stress and the inflammatory process: a major
cause of pancreatic cell death in type 2 diabetes. Diabetes Metab. Syndr. Obes. Targets Ther.
25 (2014). doi:10.2147/DMSO.S37649
449. Tang, C. et al. Susceptibility to Fatty Acid-Induced β-Cell Dysfunction Is Enhanced in
Prediabetic Diabetes-Prone BioBreeding Rats: A Potential Link Between β-Cell Lipotoxicity
and Islet Inflammation. Endocrinology 154, 89–101 (2013).
450. Donath, M. Y. & Mandrup-Poulsen, T. The use of interleukin-1-receptor antagonists in the
treatment of diabetes mellitus. Nat. Clin. Pract. Endocrinol. Metab. 4, 240–241 (2008).
451. Diraison, F. et al. Over-expression of sterol-regulatory-element-binding protein-1c
(SREBP1c) in rat pancreatic islets induces lipogenesis and decreases glucose-stimulated
insulin release: modulation by 5-aminoimidazole-4-carboxamide ribonucleoside (AICAR).
Biochem. J. 378, 769–778 (2004).
452. Patanè, G. et al. Metformin restores insulin secretion altered by chronic exposure to free
fatty acids or high glucose: a direct metformin effect on pancreatic beta-cells. Diabetes 49,
735–740 (2000).
453. Shimabukuro, M., Zhou, Y. T., Lee, Y. & Unger, R. H. Troglitazone lowers islet fat and
restores beta cell function of Zucker diabetic fatty rats. J. Biol. Chem. 273, 3547–3550
(1998).
454. Lupi, R. et al. Lipotoxicity in human pancreatic islets and the protective effect of metformin.
Diabetes 51 Suppl 1, S134-137 (2002).
455. Vandewalle, B. et al. PPARgamma-dependent and -independent effects of rosiglitazone on
lipotoxic human pancreatic islets. Biochem. Biophys. Res. Commun. 366, 1096–1101 (2008).
456. Skelin, M., Rupnik, M. & Cencic, A. Pancreatic beta cell lines and their applications in
diabetes mellitus research. ALTEX 27, 105–113 (2010).
457. Chen, Y.-R. et al. Calorie restriction on insulin resistance and expression of SIRT1 and
SIRT4 in rats. Biochem. Cell Biol. Biochim. Biol. Cell. 88, 715–722 (2010).
458. Ramsey, K. M., Mills, K. F., Satoh, A. & Imai, S.-I. Age-associated loss of Sirt1-mediated
enhancement of glucose-stimulated insulin secretion in beta cell-specific Sirt1-
overexpressing (BESTO) mice. Aging Cell 7, 78–88 (2008).
459. Yoon, M. J. et al. SIRT1-Mediated eNAMPT Secretion from Adipose Tissue Regulates
Hypothalamic NAD+ and Function in Mice. Cell Metab. 21, 706–717 (2015).
460. Gomes, A. P. et al. Declining NAD(+) induces a pseudohypoxic state disrupting nuclear-
mitochondrial communication during aging. Cell 155, 1624–1638 (2013).
461. Bezman-Tarcher, A. Method for continuous intravenous infusion of large amounts of oleic
acid into rats. J. Lipid Res. 10, 197–206 (1969).

133
462. Yoshii, H. Effects of portal free fatty acid elevation on insulin clearance and hepatic glucose
flux. AJP Endocrinol. Metab. 290, E1089–E1097 (2006).
463. Dobbins, R. L. et al. The composition of dietary fat directly influences glucose-stimulated
insulin secretion in rats. Diabetes 51, 1825–1833 (2002).
464. Stein, D. T. et al. Essentiality of circulating fatty acids for glucose-stimulated insulin
secretion in the fasted rat. J. Clin. Invest. 97, 2728–2735 (1996).
465. DeFronzo, R. A., Tobin, J. D. & Andres, R. Glucose clamp technique: a method for
quantifying insulin secretion and resistance. Am. J. Physiol. 237, E214-223 (1979).
466. Cersosimo, E., Solis-Herrera, C., Trautmann, M. E., Malloy, J. & Triplitt, C. L. Assessment
of pancreatic β-cell function: review of methods and clinical applications. Curr. Diabetes
Rev. 10, 2–42 (2014).
467. Kawamori, R., Morishima, T. & Kamada, T. [Insulin, its kinetics and metabolism]. Nihon
Rinsho Jpn. J. Clin. Med. 48 Suppl, 90–98 (1990).
468. Radziuk, J. & Morishima, T. New methods for the analysis of insulin kinetics in vivo:
insulin secretion, degradation, systemic dynamics and hepatic extraction. Adv. Exp. Med.
Biol. 189, 247–276 (1985).
469. Hahn, M. K. et al. Acute effects of single-dose olanzapine on metabolic, endocrine, and
inflammatory markers in healthy controls. J. Clin. Psychopharmacol. 33, 740–746 (2013).
470. Guenette, M. D. et al. Atypical antipsychotics and effects of adrenergic and serotonergic
receptor binding on insulin secretion in-vivo: an animal model. Schizophr. Res. 146, 162–
169 (2013).
471. Faerch, K., Brøns, C., Alibegovic, A. C. & Vaag, A. The disposition index: adjustment for
peripheral vs. hepatic insulin sensitivity?: The disposition index. J. Physiol. 588, 759–764
(2010).
472. Mari, A. et al. Influence of hyperinsulinemia and insulin resistance on in vivo β-cell
function: their role in human β-cell dysfunction. Diabetes 60, 3141–3147 (2011).
473. Dimitriadis, G., Mitrou, P., Lambadiari, V., Maratou, E. & Raptis, S. A. Insulin effects in
muscle and adipose tissue. Diabetes Res. Clin. Pract. 93 Suppl 1, S52-59 (2011).
474. Kotronen, A., Vehkavaara, S., Seppala-Lindroos, A., Bergholm, R. & Yki-Jarvinen, H.
Effect of liver fat on insulin clearance. AJP Endocrinol. Metab. 293, E1709–E1715 (2007).
475. Gilde, A. J. et al. Peroxisome proliferator-activated receptor (PPAR) alpha and
PPARbeta/delta, but not PPARgamma, modulate the expression of genes involved in cardiac
lipid metabolism. Circ. Res. 92, 518–524 (2003).
476. van Bilsen, M., van der Vusse, G. J., Gilde, A. J., Lindhout, M. & van der Lee, K. A. J. M.
Peroxisome proliferator-activated receptors: lipid binding proteins controling gene
expression. Mol. Cell. Biochem. 239, 131–138 (2002).
477. Forman, B. M., Chen, J. & Evans, R. M. Hypolipidemic drugs, polyunsaturated fatty acids,
and eicosanoids are ligands for peroxisome proliferator-activated receptors alpha and delta.
Proc. Natl. Acad. Sci. U. S. A. 94, 4312–4317 (1997).

134
478. Li, X. et al. Non-esterified fatty acids activate the AMP-activated protein kinase signaling
pathway to regulate lipid metabolism in bovine hepatocytes. Cell Biochem. Biophys. 67,
1157–1169 (2013).
479. Murray, A. J., Panagia, M., Hauton, D., Gibbons, G. F. & Clarke, K. Plasma free fatty acids
and peroxisome proliferator-activated receptor alpha in the control of myocardial uncoupling
protein levels. Diabetes 54, 3496–3502 (2005).
480. Ramakrishnan, S. K. et al. PPAR alpha Activation Reduces Hepatic CEACAM1 Expression
to Regulate Fatty Acid Oxidation during Fasting-refeeding Transition. J. Biol. Chem. 291,
8121–9 (2016).
481. Tan, M. et al. SIRT1/PGC-1α signaling protects hepatocytes against mitochondrial oxidative
stress induced by bile acids. Free Radic. Res. 49, 935–945 (2015).
482. Liang, H. & Ward, W. F. PGC-1alpha: a key regulator of energy metabolism. Adv. Physiol.
Educ. 30, 145–151 (2006).
483. Puigserver, P. et al. Insulin-regulated hepatic gluconeogenesis through FOXO1-PGC-1alpha
interaction. Nature 423, 550–555 (2003).
484. Wuescher, L. et al. Insulin regulates menin expression, cytoplasmic localization, and
interaction with FOXO1. Am. J. Physiol. Endocrinol. Metab. 301, E474-483 (2011).
485. van Raalte, D. H., Li, M., Pritchard, P. H. & Wasan, K. M. Peroxisome proliferator-activated
receptor (PPAR)-alpha: a pharmacological target with a promising future. Pharm. Res. 21,
1531–1538 (2004).
486. Vega, R. B., Huss, J. M. & Kelly, D. P. The coactivator PGC-1 cooperates with peroxisome
proliferator-activated receptor alpha in transcriptional control of nuclear genes encoding
mitochondrial fatty acid oxidation enzymes. Mol. Cell. Biol. 20, 1868–1876 (2000).
487. Kane, C. D. et al. Molecular characterization of novel and selective peroxisome proliferator-
activated receptor alpha agonists with robust hypolipidemic activity in vivo. Mol.
Pharmacol. 75, 296–306 (2009).
488. Herzig, S. et al. CREB regulates hepatic gluconeogenesis through the coactivator PGC-1.
Nature 413, 179–183 (2001).
489. Yoon, J. C. et al. Control of hepatic gluconeogenesis through the transcriptional coactivator
PGC-1. Nature 413, 131–138 (2001).
490. Brandt, J. M., Djouadi, F. & Kelly, D. P. Fatty acids activate transcription of the muscle
carnitine palmitoyltransferase I gene in cardiac myocytes via the peroxisome proliferator-
activated receptor alpha. J. Biol. Chem. 273, 23786–23792 (1998).
491. Gulick, T., Cresci, S., Caira, T., Moore, D. D. & Kelly, D. P. The peroxisome proliferator-
activated receptor regulates mitochondrial fatty acid oxidative enzyme gene expression.
Proc. Natl. Acad. Sci. U. S. A. 91, 11012–11016 (1994).
492. Lee, S. S. et al. Targeted disruption of the alpha isoform of the peroxisome proliferator-
activated receptor gene in mice results in abolishment of the pleiotropic effects of
peroxisome proliferators. Mol. Cell. Biol. 15, 3012–3022 (1995).

135
493. Göttlicher, M., Widmark, E., Li, Q. & Gustafsson, J. A. Fatty acids activate a chimera of the
clofibric acid-activated receptor and the glucocorticoid receptor. Proc. Natl. Acad. Sci. U. S.
A. 89, 4653–4657 (1992).
494. Kersten, S. et al. Peroxisome proliferator-activated receptor alpha mediates the adaptive
response to fasting. J. Clin. Invest. 103, 1489–1498 (1999).
495. Leone, T. C., Weinheimer, C. J. & Kelly, D. P. A critical role for the peroxisome
proliferator-activated receptor alpha (PPARalpha) in the cellular fasting response: the
PPARalpha-null mouse as a model of fatty acid oxidation disorders. Proc. Natl. Acad. Sci.
U. S. A. 96, 7473–7478 (1999).
496. Evans, R. M., Barish, G. D. & Wang, Y.-X. PPARs and the complex journey to obesity. Nat.
Med. 10, 355–361 (2004).
497. Patsouris, D., Reddy, J. K., Müller, M. & Kersten, S. Peroxisome proliferator-activated
receptor alpha mediates the effects of high-fat diet on hepatic gene expression.
Endocrinology 147, 1508–1516 (2006).
498. Brunet, A. et al. Akt promotes cell survival by phosphorylating and inhibiting a Forkhead
transcription factor. Cell 96, 857–868 (1999).
499. Nakae, J., Park, B. C. & Accili, D. Insulin stimulates phosphorylation of the forkhead
transcription factor FKHR on serine 253 through a Wortmannin-sensitive pathway. J. Biol.
Chem. 274, 15982–15985 (1999).
500. Rena, G., Guo, S., Cichy, S. C., Unterman, T. G. & Cohen, P. Phosphorylation of the
transcription factor forkhead family member FKHR by protein kinase B. J. Biol. Chem. 274,
17179–17183 (1999).
501. Najjar, S. M. et al. Cloning and characterization of a functional promoter of the rat pp120
gene, encoding a substrate of the insulin receptor tyrosine kinase. J. Biol. Chem. 271, 8809–
8817 (1996).
502. Buteau, J., Shlien, A., Foisy, S. & Accili, D. Metabolic diapause in pancreatic beta-cells
expressing a gain-of-function mutant of the forkhead protein Foxo1 (Supplemental Data). J.
Biol. Chem. 282, 287–293 (2007).
503. Dasgupta, S. et al. Mechanism of lipid induced insulin resistance: activated PKCε is a key
regulator. Biochim. Biophys. Acta 1812, 495–506 (2011).
504. Yaguchi, T. et al. Effects of cis-unsaturated free fatty acids on PKC-epsilon activation and
nicotinic ACh receptor responses. Brain Res. Mol. Brain Res. 133, 320–324 (2005).
505. Dey, D., Bhattacharya, A., Roy, S. & Bhattacharya, S. Fatty acid represses insulin receptor
gene expression by impairing HMGA1 through protein kinase Cepsilon. Biochem. Biophys.
Res. Commun. 357, 474–479 (2007).
506. Samuel, V. T. et al. Inhibition of protein kinase Cepsilon prevents hepatic insulin resistance
in nonalcoholic fatty liver disease. J. Clin. Invest. 117, 739–745 (2007).
507. Bezy, O. et al. PKCδ regulates hepatic insulin sensitivity and hepatosteatosis in mice and
humans. J. Clin. Invest. 121, 2504–2517 (2011).

136
508. Bamberger, A.-M. et al. Stimulation of CEACAM1 expression by 12-O-
tetradecanoylphorbol-13-acetate (TPA) and calcium ionophore A23187 in endometrial
carcinoma cells. Carcinogenesis 27, 483–490 (2006).
509. Kanda, H. et al. Hepatocyte growth factor transforms immortalized mouse liver epithelial
cells. Oncogene 8, 3047–3053 (1993).
510. Ramboer, E. et al. Strategies for immortalization of primary hepatocytes. J. Hepatol. 61,
925–943 (2014).
511. Park, G.-J. et al. Effects of sirtuin 1 activation on nicotine and lipopolysaccharide-induced
cytotoxicity and inflammatory cytokine production in human gingival fibroblasts. J.
Periodontal Res. 48, 483–492 (2013).
512. Imai, S. & Guarente, L. Ten years of NAD-dependent SIR2 family deacetylases:
implications for metabolic diseases. Trends Pharmacol. Sci. 31, 212–220 (2010).
513. Jayaram, H. N., Kusumanchi, P. & Yalowitz, J. A. NMNAT expression and its relation to
NAD metabolism. Curr. Med. Chem. 18, 1962–1972 (2011).
514. Gerhart-Hines, Z. et al. Metabolic control of muscle mitochondrial function and fatty acid
oxidation through SIRT1/PGC-1alpha. EMBO J. 26, 1913–1923 (2007).
515. Lin, J., Handschin, C. & Spiegelman, B. M. Metabolic control through the PGC-1 family of
transcription coactivators. Cell Metab. 1, 361–370 (2005).
516. Devalaraja-Narashimha, K. & Padanilam, B. J. PARP-1 Inhibits Glycolysis in Ischemic
Kidneys. J. Am. Soc. Nephrol. 20, 95–103 (2009).
517. Du, X. et al. Inhibition of GAPDH activity by poly(ADP-ribose) polymerase activates three
major pathways of hyperglycemic damage in endothelial cells. J. Clin. Invest. 112, 1049–
1057 (2003).
518. Lash, L. H., Tokarz, J. J., Chen, Z., Pedrosi, B. M. & Woods, E. B. ATP depletion by
iodoacetate and cyanide in renal distal tubular cells. J. Pharmacol. Exp. Ther. 276, 194–205
(1996).
519. Lemasters, J. J., DiGuiseppi, J., Nieminen, A. L. & Herman, B. Blebbing, free Ca2+ and
mitochondrial membrane potential preceding cell death in hepatocytes. Nature 325, 78–81
(1987).
520. Grdović, N. et al. CXC chemokine ligand 12 protects pancreatic β-cells from necrosis
through Akt kinase-mediated modulation of poly(ADP-ribose) polymerase-1 activity. PloS
One 9, e101172 (2014).
521. Xu, E. et al. Targeted disruption of carcinoembryonic antigen-related cell adhesion molecule
1 promotes diet-induced hepatic steatosis and insulin resistance. Endocrinology 150, 3503–
3512 (2009).
522. Zhang, D. et al. Liver Clock Protein BMAL1 Promotes de Novo Lipogenesis through
Insulin-mTORC2-AKT Signaling. J. Biol. Chem. 289, 25925–25935 (2014).
523. Shiomi, Y. et al. A Novel Peroxisome Proliferator-activated Receptor (PPAR)α Agonist and
PPARγ Antagonist, Z-551, Ameliorates High-fat Diet-induced Obesity and Metabolic
Disorders in Mice. J. Biol. Chem. 290, 14567–14581 (2015).

137
524. Liu, Z.-M., Hu, M., Chan, P. & Tomlinson, B. Early investigational drugs targeting PPAR-α
for the treatment of metabolic disease. Expert Opin. Investig. Drugs 24, 611–621 (2015).
525. Soares, F. L. P. et al. Gluten-free diet reduces adiposity, inflammation and insulin resistance
associated with the induction of PPAR-alpha and PPAR-gamma expression. J. Nutr.
Biochem. 24, 1105–1111 (2013).
526. Lannin, S. Scientists reverse ageing process in mice; early human trials showing ‘promising
results’. Australian Broadcasting Corporation (2014).
527. Itoh, H. Assessment of the safety of nicotinamide mononucleotide (NMN) in healthy subjects;
phase I study. (Keio University School of Medicine, University Hospital Medical
Information Network, Japan, 2016).
528. Yu, A. et al. Resistin impairs SIRT1 function and induces senescence-associated phenotype
in hepatocytes. Mol. Cell. Endocrinol. 377, 23–32 (2013).
529. Spinnler, R. et al. The Adipocytokine Nampt and Its Product NMN Have No Effect on Beta-
Cell Survival but Potentiate Glucose Stimulated Insulin Secretion. PLoS ONE 8, e54106
(2013).
530. Rezende, L. F., Santos, G. J., Santos-Silva, J. C., Carneiro, E. M. & Boschero, A. C. Ciliary
neurotrophic factor (CNTF) protects non-obese Swiss mice against type 2 diabetes by
increasing beta cell mass and reducing insulin clearance. Diabetologia 55, 1495–1504
(2012).
531. Wang, X. & Roper, M. G. Measurement of DCF fluorescence as a measure of reactive
oxygen species in murine islets of Langerhans. Anal. Methods Adv. Methods Appl. 6, 3019–
3024 (2014).
532. Ferrer, E., Juan-García, A., Font, G. & Ruiz, M. J. Reactive oxygen species induced by
beauvericin, patulin and zearalenone in CHO-K1 cells. Toxicol. Vitro Int. J. Publ. Assoc.
BIBRA 23, 1504–1509 (2009).
533. Yamamoto, T. et al. Nicotinamide Mononucleotide, an Intermediate of NAD+ Synthesis,
Protects the Heart from Ischemia and Reperfusion. PLoS ONE 9, e98972 (2014).
534. Zhang, Y. et al. Regeneration of Pancreatic Non-β Endocrine Cells in Adult Mice following
a Single Diabetes-Inducing Dose of Streptozotocin. PLoS ONE 7, e36675 (2012).
535. Klauschen, F. et al. High nuclear poly-(ADP-ribose)-polymerase expression is prognostic of
improved survival in pancreatic cancer. Histopathology 61, 409–416 (2012).
536. Jiang, H. et al. Oral administration of soybean peptide Vglycin normalizes fasting glucose
and restores impaired pancreatic function in Type 2 diabetic Wistar rats. J. Nutr. Biochem.
25, 954–963 (2014).
537. Kato, H., Duarte, S., Liu, D., Busuttil, R. W. & Coito, A. J. Matrix Metalloproteinase-2
(MMP-2) Gene Deletion Enhances MMP-9 Activity, Impairs PARP-1 Degradation, and
Exacerbates Hepatic Ischemia and Reperfusion Injury in Mice. PloS One 10, e0137642
(2015).
538. Leisner, T. M., Moran, C., Holly, S. P. & Parise, L. V. CIB1 prevents nuclear GAPDH
accumulation and non-apoptotic tumor cell death via AKT and ERK signaling. Oncogene
32, 4017–4027 (2013).

138
539. Hao, L. et al. Elevated GAPDH expression is associated with the proliferation and invasion
of lung and esophageal squamous cell carcinomas. Proteomics 15, 3087–3100 (2015).
540. Steinritz, D., Weber, J., Balszuweit, F., Thiermann, H. & Schmidt, A. Sulfur mustard
induced nuclear translocation of glyceraldehyde-3-phosphate-dehydrogenase (GAPDH).
Chem. Biol. Interact. 206, 529–535 (2013).
541. Wilson, V. Reversing type 2 diabetes with lifestyle change. Nurs. Times 111, 17–19 (2015).
542. Kvasnicka, T., Kvasnicka, J., Ceska, R. & Vrablik, M. Increase of inflammatory state in
overweight adults with combined hyperlipidemia. Nutr. Metab. Cardiovasc. Dis. NMCD 13,
227–231 (2003).
543. Bermudez, J. A. & Velásquez, C. M. [Profile of free fatty acids (FFA) in serum of young
Colombians with obesity and metabolic syndrome]. Arch. Latinoam. Nutr. 64, 248–257
(2014).
544. Grozio, A. et al. CD73 protein as a source of extracellular precursors for sustained NAD+
biosynthesis in FK866-treated tumor cells. J. Biol. Chem. 288, 25938–25949 (2013).
545. Sociali, G. et al. Antitumor effect of combined NAMPT and CD73 inhibition in an ovarian
cancer model. Oncotarget 7, 2968–2984 (2016).
546. Spinnler, R. et al. The adipocytokine Nampt and its product NMN have no effect on beta-
cell survival but potentiate glucose stimulated insulin secretion. PloS One 8, e54106 (2013).
547. North, B. J. et al. SIRT2 induces the checkpoint kinase BubR1 to increase lifespan. EMBO
J. 33, 1438–1453 (2014).