NICE works - final report - tamba.org.uk · NICE WORKS - Maternity Engagement Project final report...
84
NICE works the final report Twins and Multiple Births Association Maternity Engagement Project Final Report
Transcript of NICE works - final report - tamba.org.uk · NICE WORKS - Maternity Engagement Project final report...
NICE worksthe final report
Twins and Multiple Births AssociationMaternity Engagement ProjectFinal Report

NICE WORKS - Maternity Engagement Project final report2
AcknowledgementsAcknowledgements
Acknowledgements
Birmingham Centre forWomen's & New Born'sHealthProfessor Mark Kilby
BLISSCaroline Lee-Davey
Brighton & SussexUniversity HospitalJoanna Fitzsimons
British Association ofPerinatal MedicineCaroline Lee-Davey,Kate Dinwiddy
Care QualityCommissionProfessor James Walker
Department ofHealth & Social CareKaren Todd
FivewaysRichard Donaldson
Leeds TeachingHospitalKathryn Harper
Liverpool Women'sHospitalJennifer Robinson,Surabhi Nanda
Maternity VoicesPartnershipLisa Ramsay
MBRRACEDr Brad Manktelow
Multiple BirthsFoundationJane Denton
NHS EnglandClaire Mathews, LisaRamsay, Matt Tagney,Jacqueline Dunkley-Bent,Kath Evans, Yana Richens
NHS Fetal AnomalyScreening ProgrammeRita Phillips
NHS ImprovementMichelle Upton
NICELouise Miller
FASP

NICE WORKS - Maternity Engagement Project final report 3
Acknowledgements
Public Health EnglandAnnette Mchugh
Royal College ofMidwiferyProfessor Debbie Carrick-Sen, Mandy Forrester, LiaBrigante, Jacque Gerrard
Royal College ofNursingJane Denton,Carmel Bagness
Royal College ofObstetricians &GynaecologistsAnita Dougall,Mathew Miles
Royal College ofPaediatrics andChild HealthKate Dinwiddy
SandsClea Harmer,Mehali Patel, Laura Price,Janet Scott
Select StatisticsSarah Littler, Sally Hunton
Society & College ofRadiographersNigel Thomson
St George’sUniversity HospitalProfessor Asma Khalil(chaired the steeringcommittee)
University of LeicesterDr Brad Manktelow
West MiddlesexUniversity HospitalAlexandra Drought
Thanks to the Department of Health forfinancially supporting this quality
improvement project, enabling Tamba toadvocate on behalf of the multiple birthcommunity and improve health related
outcomes for our families.
“I feel privileged to have worked closely withthe team on this important qualityimprovement initiative where we aimed toimprove the outcomes of multiple pregnanciesby promoting the implementation of NICEguidance. The steering committee had a largenumber of key national stakeholders and theircontribution was key to the success of thisproject. The findings of this report representreal life clinical data on pregnancy outcomes,reflecting current practice in the UK and I seethis as an important step towards achievingour national target of reducing stillbirths by 50%by 2025 and in addressing the unmet needs ofmultiple pregnancies.”
Professor Asma KhalilChair of Steering Group(Professor of Obstetrics and Maternal-FetalMedicine, St George’s University Hospital)
Foreword1
NICE WORKS - Maternity Engagement Project final report 5
Foreword
Iwelcome this important report on the Tamba'Maternity Engagement Project', which wascompleted under the Government's 'Innovation,
Excellence and Strategic Development (IESD) Fund' forvoluntary sector organisations.
The Department for Health and Social Care expectsNHS services to be provided in line with NICE clinicalguidelines and quality standards. This reportdemonstrates how increased adherence to the NICEQuality Standard on Multiple pregnancy (QS46) is linkedto improved outcomes for women and their babiesincluding reduced rates of stillbirths, neonatal admissionsand emergency caesarean sections for multiples.
This research should inform the effective targeting ofresources to where they are needed and raises theawareness of key issues in the provision of care formultiple pregnancies. The finding that admissions toneonatal units could be reduced by 1,308 with a costsaving of around £8 million if all maternity units inEngland implemented similar changes should focus theminds of all commissioners and providers of maternityservices working to achieve the national ambition tohalve the rates of stillbirths and neonatal deaths by 2025.
This project also emphasises the impact that external,expert support can have on an organisation'scontinuous quality improvement (QI). The MaternityTransformation Programme's QI programme, the'Maternal and Neonatal Health Safety Collaborative'together with Maternity Safety Champions, aresupporting cultures of multidisciplinary team workingand learning in the NHS, vital for safe, high-qualitymaternity care. They also support implementation ofthe NHS Long Term Plan commitment to roll out theSaving Babies Lives Care Bundle, which recommendsusing the NICE guidance for multiple pregnancies,across every maternity unit in England this year.
I would like to thank and congratulate Tamba, theMaternity Engagement Project team and the 30maternity units that took part in this important researchfor this excellent report.
Jackie Doyle-Price MP
Parliamentary Under Secretaryof State for Mental Healthand Inequalities
Department of Healthand Social Care
ExecutiveSummary2
NICE WORKS - Maternity Engagement Project final report 7
Executive Summary
In England, multiple pregnanciesmake up around 1.5% ofpregnancies but account for 5% ofstillbirths, 10% of neonatal deathsand 15-20% of all neonataladmissions(1).
The National Institute for Care andExcellence (NICE) first publishedantenatal care guidelines formultiple pregnancies (Clinical
Guideline 129) in 2011(2) andfollowed these with eight qualitystandards (NICE QS46) in 2013(3).These aim to improve the qualityand consistency of clinical careprovided, however eight years onfrom the first guidelines there is stillan excessive variation in theirimplementation across maternityunits.
2.1 Background
2.2 The Maternity Engagement ProjectThe central hypothesis of theMaternity Engagement Project wasthat by providing support toimplement NICE QS46, maternityunits would increase their level ofadherence to NICE qualitystandards, and this could lead toreduced rates of stillbirth, neonataldeath, neonatal admissions andemergency caesarean sections aswell as considerable cost savings.
With funding from the Departmentof Health and Social Care, Tamba'sMaternity Engagement Projectsuccessfully delivered a three-yearproject which worked with 30maternity units across England to
identify and implement changes toimprove antenatal care for multiplepregnancies, in line with NICEQS46.
Units were audited and supportedto implement an agreed actionplan. Follow up re-audits werecarried out one year later to assessthe changes made and theirimpact. In total there were 40statistically significant positivefindings which clearly demonstratethat both Tamba's support and theNICE guidelines work. All trustsshould ensure they are followingNICE QS46 and Tamba can help.
2.3 Key findings■ 65% of units saw a reduction in
their neonatal admissions rate formultiples in 12 months. Across allunits there was an averagereduction of 5.8 percentagepoints. This relates to 200 feweradmissions across the 23 unitswhere data was available.
■ There was an instance ofincreased adherence to NICE
guidelines being linked to adecrease in neonatal deaths formultiples in one unit in just 12months. There is evidence tosuggest leadership support andcloser adherence to the QualityStandards results in lower stillbirthrates. There is strong evidencethat over a longer periodimplementing the Quality
NICE WORKS - Maternity Engagement Project final report8
Executive Summary
Standards can lead to aconsiderable fall in stillbirth rates.
⬥ At re-audit, one unit saw astatistically significantreduction in their neonataldeath rate (from 3.2% to 0%,p=0.0336).
⬥ At re-audit there was someevidence (p=0.0257) ofstillbirth rates being lower forsites with a maternitychampion compared tothose without (byapproximately -0.009%p; 95%CI = -0.017%p to -0.001%p).
⬥ At baseline, increasedadherence to QS46statement seven (discussionsby 24 weeks on pretermlabour and birth) and eight(discussions by 32 weeks ontiming and delivery) wascorrelated with a lowerstillbirth rate in larger units (r=-0.89, p=0.02 and r=-0.9, p=0.01respectively).
⬥ Although in the 12 monthsbetween audits there was nota significant change inmultiple stillbirth rates, theevidence from St George'sUniversity Hospital, which wasan exemplar unit and an earlyadopter of NICE QS46, saw a70% reduction (from 14 per1000 in 2012 to 4 per 1000 in2016) in stillbirths over a fiveyear period. Over a longerperiod of time (2000-2019)and with an increased cohort,comparing the preimplementation 32/2250 vs.post implementation 5/1147rates, the result becomesstatistically significant(p=0.008).
■ 60% of units saw a reduction intheir emergency caesareansection rate for multiples in 12
months. Across all units there wasan average reduction of 3.1percentage points. This relates to105 fewer emergency C-sectionsover 26 units where data wasavailable.
■ 100% of units re-auditedincreased their overalladherence to NICE QS46between the baseline andfollow-up audits. Units thatimplemented a higher proportionof the actions to improve carepractice identified by Tamba,tended to see a greater increasein their overall adherence toNICE QS46.
■ Nine out of ten professionals inunits that had completed theproject agreed that "if we hadn'tdone the Maternity EngagementProject we would not haveachieved as much positivechange".
■ If all units in England (157)implemented similar changes toincrease adherence in NICEQS46, within a year neonataladmissions could be reduced by1,308 with a cost saving of £8million. Emergency caesareansections could be reduced by634 and up to 100 stillbirthsacross the UK could beprevented.
2.3 Key findings (continued)
NICE WORKS - Maternity Engagement Project final report 9
These findings will be of interest toindividual trusts and maternityteams looking to implement NHSEngland’s Saving Babies Lives CareBundle which explicitlyrecommends using the NICEguidance for multiple pregnancies.Furthermore, the CQC’s hospitalinspection framework checkswhether units are delivering carefor multiple pregnancies inaccordance with this guidance.
Care in multiple pregnancies willbe under the spotlight like neverbefore. Various reviews are alreadyunderway including; a maternityunit level audit of care based onprofessional and patient feedbackacross the UK, an MBRRACEconfidential enquiry into twinstillbirths and neonatal deaths andupdates to NICE guidance.
Tamba would urge every healthprofessional to work with theirmaternity safety champions anduse the Tamba resources availableto ensure their trust is effectivelyimplementing NICE QS46. Weencourage all trusts that havetaken part in this project tocontinue their improvement.
We also call on NHS England toensure that Local Maternity Systems
are aware that this project canmake a considerable contributionto meeting the Department ofHealth’s Better Births ambition forcontinuity of carer, and that twinand triplet pregnancies continueto be explicitly recognised incommissioning frameworks, tariffrequirements and carebundles.
Tamba’s Maternity EngagementProject has shown that in the bestcase, after five years, the lives ofup to 100 stillborn babies could besaved every year if all maternityunits across the UK follow NICE QS46.This would result in a twin stillbirthrate of 1.85 per thousand which isbelow the 2016 singleton stillbirth
rate of 3.86(4). The evidence fromthe Netherlands is that it is possibleto reduce the twin stillbirth rate to arate lower than the singleton rate(5).
In addition, at least £8m offinancial savings would be made inEngland. Tamba can support unitsto achieve these positiveoutcomes.
2.4 Conclusion
2.5 Recommendations
Executive Summary
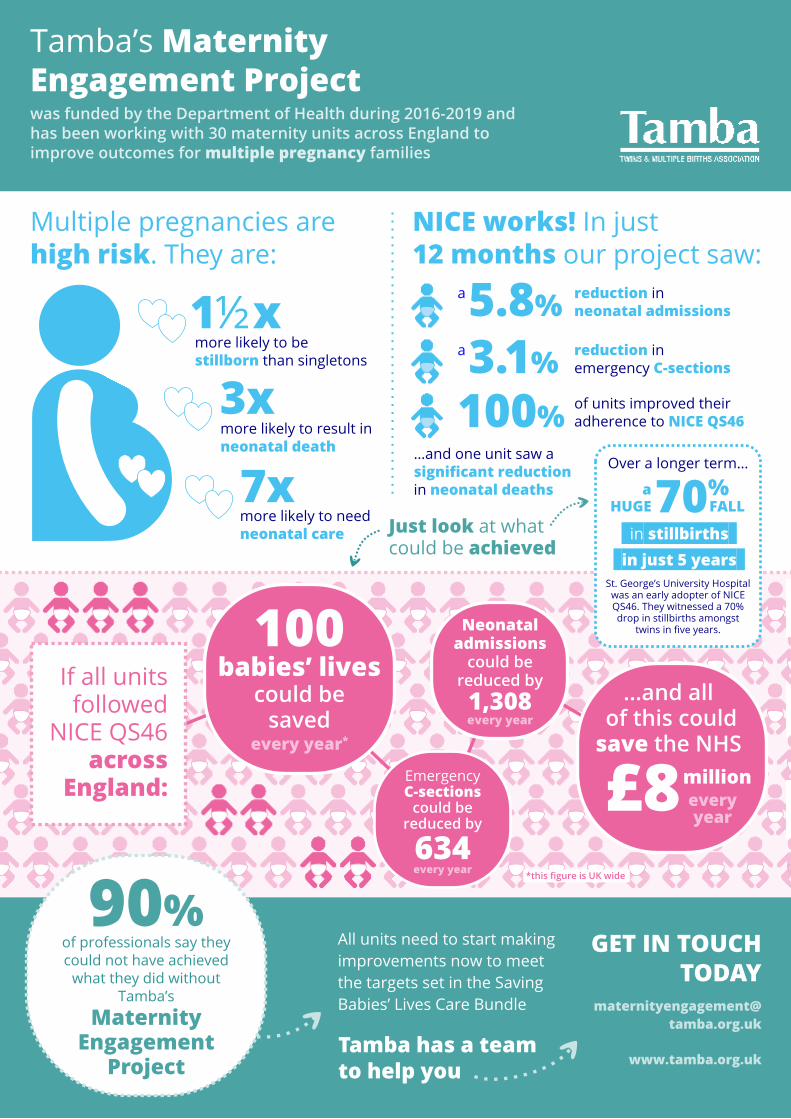
Tamba’s MaternityEngagement Projectwas funded by the Department of Health during 2016-2019 andhas been working with 30 maternity units across England toimprove outcomes for multiple pregnancy families
All units need to start makingimprovements now to meetthe targets set in the SavingBabies’ Lives Care Bundle
Tamba has a teamto help you
GET IN TOUCHTODAY
www.tamba.org.uk
If all unitsfollowed
NICE QS46across
England:
100babies’ lives
could besaved
every year*
634
EmergencyC-sections
could bereduced by
every year
every year
Neonataladmissions
could bereduced by1,308
*this figure is UK wide
…and all of this couldsave the NHS
£8millioneveryyear
MaternityEngagement
Project
of professionals say theycould not have achieved
what they did withoutTamba’s
90%
Multiple pregnancies arehigh risk. They are:
1½xmore likely to bestillborn than singletons
3xmore likely to result inneonatal death
7xmore likely to needneonatal care
NICE works! In just12 months our project saw:
5.8%a reduction inneonatal admissions
3.1%a reduction inemergency C-sections
…and one unit saw asignificant reductionin neonatal deaths
100% of units improved theiradherence to NICE QS46
Just look at whatcould be achieved
Over a longer term…
aHUGE70%
FALL
St. George’s University Hospitalwas an early adopter of NICEQS46. They witnessed a 70%drop in stillbirths amongst
twins in five years.
in stillbirthsin just 5 years
Introduction3
NICE WORKS - Maternity Engagement Project final report12
In England, multiple pregnanciesmake up around 1.5% ofpregnancies but account for 5% ofstillbirths, 10% of neonatal deathsand 15-20% of all neonataladmissions(6).
The risk of preterm birth is alsoconsiderably higher occurring in atleast 50% of twin pregnancies(7)
with twins facing six times the risk ofcerebral palsy(8). This paints aconcerning picture for the multiplebirth community, one which iscompounded by unwarrantedvariations in clinical care deliveredacross the UK.
Whilst Tamba welcomes the currentnational policy focus on qualityimprovement and patient safety inour maternity services, thereappears to be a distinct lack ofunderstanding surrounding thesophisticated and uniquechallenges faced by patients witha multiple pregnancy. The NationalInstitute for Care and Excellence(NICE) first published antenatalcare guidelines for multiplepregnancies (Clinical Guideline129) in 2011(9) and followed thesewith eight quality standards (NICEQS46) in 2013(10). These guidelines
aim to improve the quality andconsistency of clinical careprovided, however eight years onthere is still an excessive variation intheir implementation acrossdifferent providers(11).
Evidence suggests that maternityunits that follow national clinicalguidance have the potential toreduce the clinical risks associatedwith fetal compromise and patientsafety within the antenatal careperiod and improve patientoutcomes(12). This particularlyappears to be the caseconcerning multiple pregnancieswhere units have implemented amodel of care that closelymatches that set out in NICE QS46.
Furthermore, research suggeststhat external quality improvementinterventions have increasedsuccess rates within the NHS, asthey provoke practice reflectionand motivate behaviour change inways not achieved by someinternal interventions. This ispotentially due to the neutrality ofthe external body, being removedfrom the organisation's internalpolitics and culture(13).
3.1 Project Context
3.2 The Maternity Engagement Project
In 2016 Tamba securedDepartment of Health and SocialCare funding to undertake theMaternity Engagement Projectwhich aimed to improve the out-comes for twin and other multiplepregnancies across 30 targeted
maternity units in England. Theproject was conducted over athree-year period with units havingone year to implement changes.
The project aimed to achieve thisoutcome through ensuring multiplepregnancy care is delivered
3.2.1 Project background and aims
Introduction

NICE WORKS - Maternity Engagement Project final report 13
Introduction
consistently and in line withnational guidance - specificallyNICE Quality Standard 46 (NICEQS46). NICE's guideline and qualitystandards aim to improve outcomesby recommending additional carethat should be offered to womenwith twin and triplet pregnancies.Overall evidence suggests thatadherence to clinical guidelines inmaternity care saves lives andimproves outcomes for multiples
and their families, whilst promotinggood, safe quality care for all (14).
The central hypothesis of theMaternity Engagement Project wastherefore that by providing supportto maternity units to implementNICE QS46, the units wouldincrease their level of adherenceto NICE QS46, and this increasedadherence would, in turn, lead toimproved patient outcomes.
NICE Quality Standard 46
1 Women who are pregnant with twins ortriplets (referred to as a multiplepregnancy) have an ultrasound scanbetween 11 weeks and 13 weeks 6 daysof their pregnancy. This is to seewhether the babies share the sameplacenta (chorionicity) and amniotic sac(amnionicity). This information isrecorded in the woman's notes.
Women with a multiple pregnancy havean ultrasound scan between 11 weeksand 13 weeks 6 days of their pregnancyto record the positions of their babies.
Women with a multiple pregnancy arecared for by a team of healthcareprofessionals with different skills androles (for example, specialist doctors,specialist midwives and ultrasoundoperators).
Women with a multiple pregnancy havea care plan that has the dates and timesof all their antenatal care appointmentsand details of who the appointments arewith.
Women with a multiple pregnancy aremonitored to check the babies for anycomplications (for example, to check thebabies' growth and blood flow) in a waythat is appropriate for their pregnancy.
Women with a multiple pregnancy havean expert in fetal medicine involved intheir care if their pregnancy is higher riskor if there are complications.
Women with a multiple pregnancydiscuss the risks and signs of an early(preterm) labour with one or moremembers of their healthcare team. Thediscussion should take place by 24 weeksof their pregnancy and also cover thepossible problems associated with anearly birth.
Women with a multiple pregnancy have adiscussion with one or more members oftheir healthcare team about the timing ofthe birth and how they want their babiesto be delivered. This discussion needs totake place by 32 weeks of theirpregnancy and include agreement oftheir birth plan.
8
23
4
76
5The quality standard is made up of eight statements that describe high-qualitycare for patients and are summarised as follows:
NICE WORKS - Maternity Engagement Project final report14
Introduction
3.2.2 Delivery methodThe project compared practice at each participating unit against seven ofthe eight(15) NICE QS46 statements. A description of the delivery methodfollows.
2017:Baselineaudit andactionplan
12 months ofimplementation
supportfrom Tamba
2018:Re-audit
(followup)
��� ���
To capture the baseline situation,independent midwifery consultantswith extensive experience of multiplepregnancies and NICE QS46implementation were contractedby Tamba to visit units and carry outa baseline audit. The audit involved:
■ Ethical protocols being agreedby the unit and Tamba. The visitswere conducted in line withCaldicott principles(16) and thenecessary confidentialityagreements were put in placewith the units prior to the visit.
■ Reviewing a sample of multiplebirth mothers' case notes frompatients that had delivered theirbabies in the 12-month periodprior to the baseline audit(typically ten per unit to fit theresources available and to beable to conduct an audit in oneworking day). Tamba requestedthat units randomly select amixture of monochorionic,dichorionic and tripletpregnancies. In total 277 casenotes were reviewed by Tamba'smidwifery consultants at baseline.
■ The risk of three differentmidwifery consultants reviewingnotes at different units andinterpreting them differently wasmitigated by one of the TambaMaternity Engagement projectteam accompanying them onearly baseline audits, anddiscussions within the team toagree what evidenceconstituted "high-risk", "continuityof care" or whether someonewas a "specialist"(17).
■ Reviewing practice andprotocols by conductingstructured conversations withstaff that look after multiplepregnancies (in total over 140group or individual interviewswere conducted with relevanthealthcare professionalsincluding fetal medicineconsultants, obstetricians, headsof midwifery, midwives andsonographers).
■ Trusts providing statistics relatingto patient outcomes for the 12months prior to the baselineaudit and any intervention fromTamba (see 3.2.4).
NICE WORKS - Maternity Engagement Project final report 15
Introduction
The audit process offered each sitethe opportunity to reflect uponcurrent practice and provided aplatform from which to implementpractical solutions to improve careand explore barriers to change.The approach was very much "unitled", with the Tamba project teamfacilitating the process, capturinginformation and feeding back tothe unit in the form of a recom-mended bespoke action planwhich:
■ Highlighted areas where the unitcould increase NICE QS46adherence using a "traffic light"system (i.e. green - no actionrequired, amber - actionrequired and red - urgent actionrequired).
■ Suggested resources to supportimplementation of those actions.
■ Incorporated areas that linked toother national policy prioritiesand inspection frameworks.
To finalise the action plan, aconference call was held with keystaff at Tamba and the unit toreview the actions and agreedates to review progress.
The unit then took ownership ofdelivering the plan. During itsimplementation the unit couldaccess a support packageincluding the following:
■ Access to Tamba's midwiferyconsultants with specialistexperience and knowledge ofmultiple births for remote supportover 12 months, includingscheduled quarterly updatecalls.
■ Peer-support learning andnetworking opportunities(including advice and supportfrom other units of similar size thathave been shown to closelyfollow NICE guidelines).
■ Best practice tools e.g. Tamba'sMultiple Pregnancy CarePathway.
■ Signposting to innovative multiplespecific resources such asmultiple growth charts(18) andawareness of leading research inthe field.
■ Access to a free extensivespecialist health careprofessional online CPD resource(208 professionals from theparticipating units signed up tothis resource(19)) and freemultidisciplinary study day (111professionals from theparticipating units attended astudy day).
■ Access to the full range ofTamba booklets, leaflets,factsheets, webinars and courseswhich offer guidance andsupport to both healthprofessionals and parents.
■ A quarterly health professionalnewsletter.
Approximately 12 months after thebaseline audit Tamba's midwiferyconsultant returned to the unit toconduct a re-audit using the sameprocess as the baseline auditdescribed above (i.e. a review ofcase notes, a review of practice,and gathering statistics relating topatient outcomes) This wasfollowed by another conferencecall to review what had beenachieved and make suggestions asto how progress could besustained.
NICE WORKS - Maternity Engagement Project final report16
Introduction
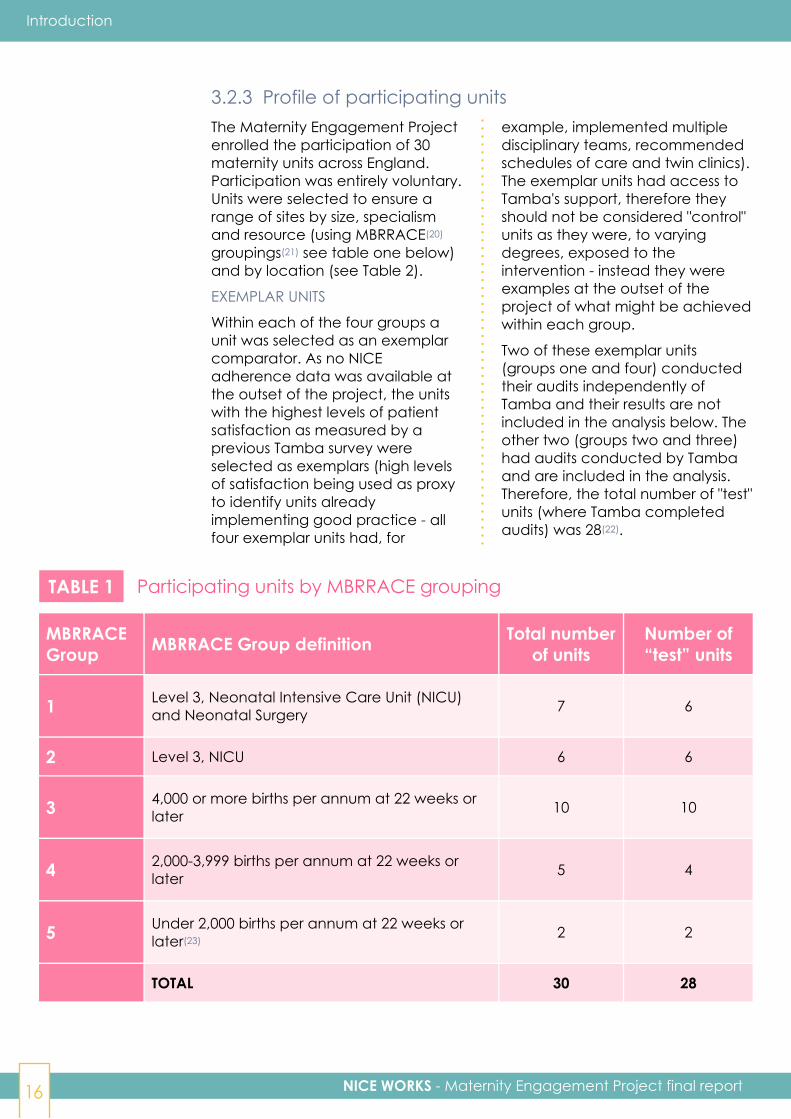
3.2.3 Profile of participating unitsThe Maternity Engagement Projectenrolled the participation of 30maternity units across England.Participation was entirely voluntary.Units were selected to ensure arange of sites by size, specialismand resource (using MBRRACE(20)
groupings(21) see table one below)and by location (see Table 2).
EXEMPLAR UNITS
Within each of the four groups aunit was selected as an exemplarcomparator. As no NICEadherence data was available atthe outset of the project, the unitswith the highest levels of patientsatisfaction as measured by aprevious Tamba survey wereselected as exemplars (high levelsof satisfaction being used as proxyto identify units alreadyimplementing good practice - allfour exemplar units had, for
example, implemented multipledisciplinary teams, recommendedschedules of care and twin clinics).The exemplar units had access toTamba's support, therefore theyshould not be considered "control"units as they were, to varyingdegrees, exposed to theintervention - instead they wereexamples at the outset of theproject of what might be achievedwithin each group.
Two of these exemplar units(groups one and four) conductedtheir audits independently ofTamba and their results are notincluded in the analysis below. Theother two (groups two and three)had audits conducted by Tambaand are included in the analysis.Therefore, the total number of "test"units (where Tamba completedaudits) was 28(22).
TABLE 1 Participating units by MBRRACE grouping
MBRRACEGroup MBRRACE Group definition Total number
of unitsNumber of“test” units
1 Level 3, Neonatal Intensive Care Unit (NICU)and Neonatal Surgery 7 6
2 Level 3, NICU 6 6
3 4,000 or more births per annum at 22 weeks orlater 10 10
4 2,000-3,999 births per annum at 22 weeks orlater 5 4
5 Under 2,000 births per annum at 22 weeks orlater(23)
2 2
TOTAL 30 28
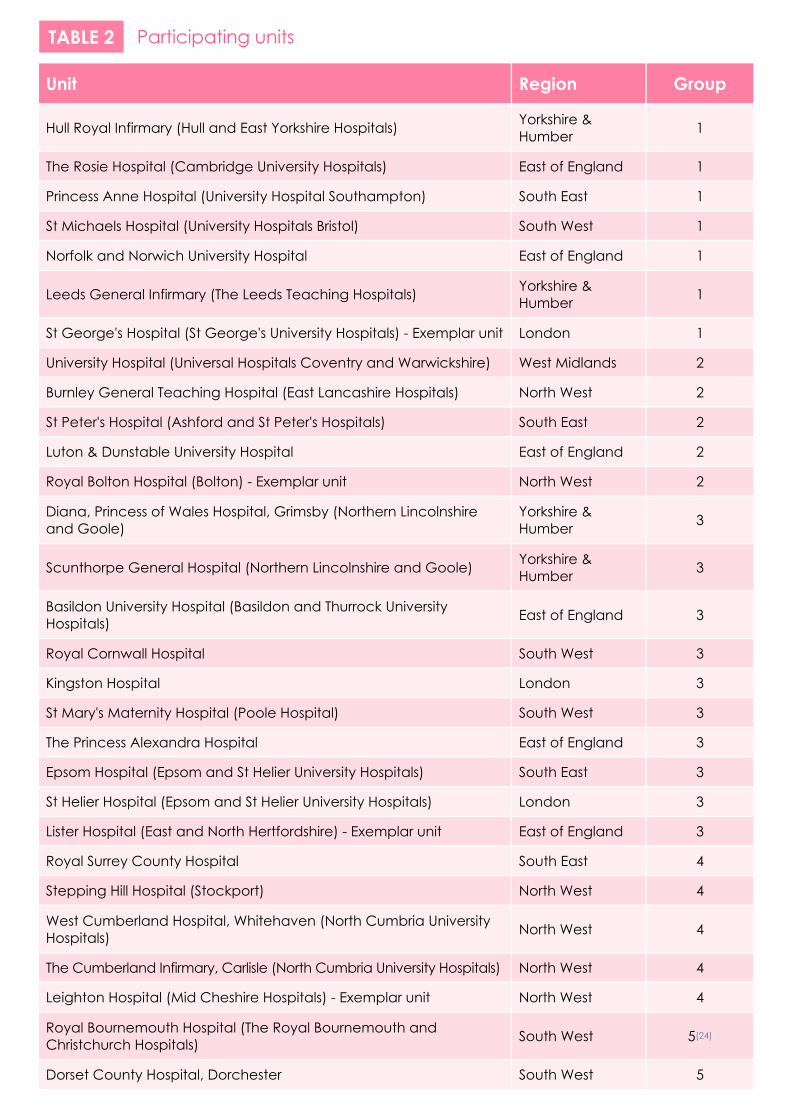
TABLE 2 Participating units
Unit Region Group
Hull Royal Infirmary (Hull and East Yorkshire Hospitals) Yorkshire &Humber 1
The Rosie Hospital (Cambridge University Hospitals) East of England 1
Princess Anne Hospital (University Hospital Southampton) South East 1
St Michaels Hospital (University Hospitals Bristol) South West 1
Norfolk and Norwich University Hospital East of England 1
Leeds General Infirmary (The Leeds Teaching Hospitals) Yorkshire &Humber 1
St George's Hospital (St George's University Hospitals) - Exemplar unit London 1
University Hospital (Universal Hospitals Coventry and Warwickshire) West Midlands 2
Burnley General Teaching Hospital (East Lancashire Hospitals) North West 2
St Peter's Hospital (Ashford and St Peter's Hospitals) South East 2
Luton & Dunstable University Hospital East of England 2
Royal Bolton Hospital (Bolton) - Exemplar unit North West 2
Diana, Princess of Wales Hospital, Grimsby (Northern Lincolnshireand Goole)
Yorkshire &Humber 3
Scunthorpe General Hospital (Northern Lincolnshire and Goole) Yorkshire &Humber 3
Basildon University Hospital (Basildon and Thurrock UniversityHospitals) East of England 3
Royal Cornwall Hospital South West 3
Kingston Hospital London 3
St Mary's Maternity Hospital (Poole Hospital) South West 3
The Princess Alexandra Hospital East of England 3
Epsom Hospital (Epsom and St Helier University Hospitals) South East 3
St Helier Hospital (Epsom and St Helier University Hospitals) London 3
Lister Hospital (East and North Hertfordshire) - Exemplar unit East of England 3
Royal Surrey County Hospital South East 4
Stepping Hill Hospital (Stockport) North West 4
West Cumberland Hospital, Whitehaven (North Cumbria UniversityHospitals) North West 4
The Cumberland Infirmary, Carlisle (North Cumbria University Hospitals) North West 4
Leighton Hospital (Mid Cheshire Hospitals) - Exemplar unit North West 4
Royal Bournemouth Hospital (The Royal Bournemouth andChristchurch Hospitals) South West 5(24)
Dorset County Hospital, Dorchester South West 5
NICE WORKS - Maternity Engagement Project final report18
Introduction
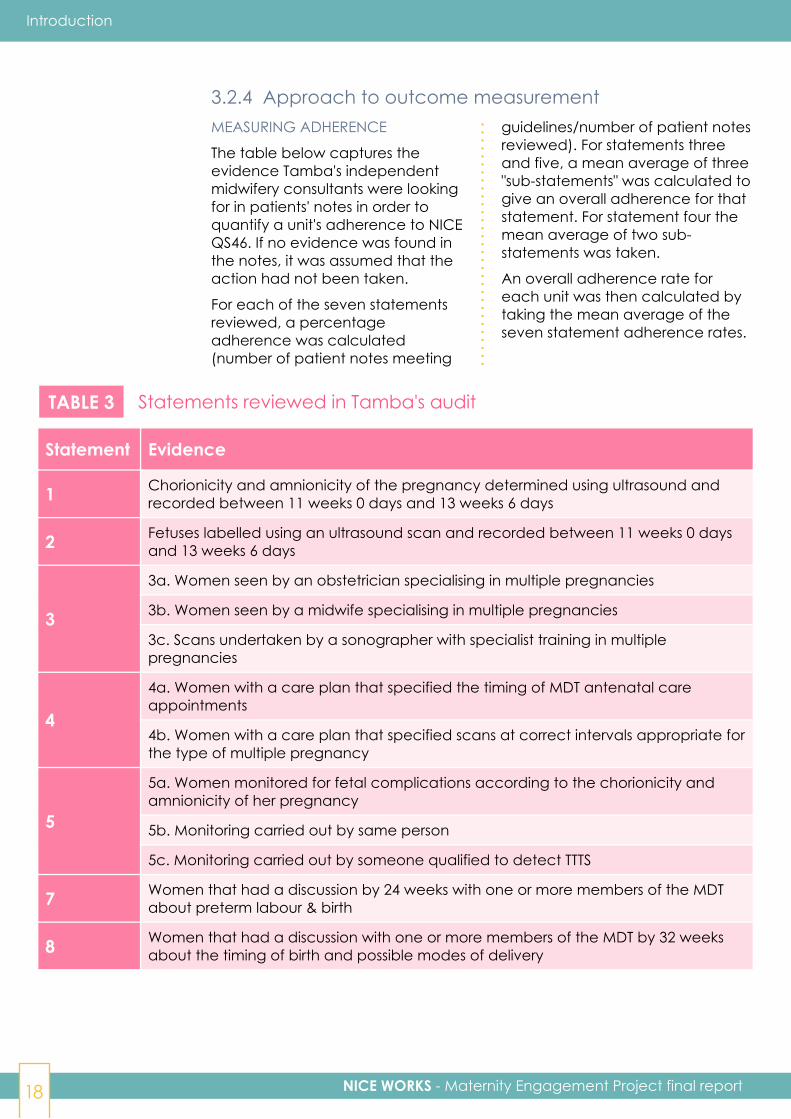
3.2.4 Approach to outcome measurementMEASURING ADHERENCE
The table below captures theevidence Tamba's independentmidwifery consultants were lookingfor in patients' notes in order toquantify a unit's adherence to NICEQS46. If no evidence was found inthe notes, it was assumed that theaction had not been taken.
For each of the seven statementsreviewed, a percentageadherence was calculated(number of patient notes meeting
guidelines/number of patient notesreviewed). For statements threeand five, a mean average of three"sub-statements" was calculated togive an overall adherence for thatstatement. For statement four themean average of two sub-statements was taken.
An overall adherence rate foreach unit was then calculated bytaking the mean average of theseven statement adherence rates.
TABLE 3 Statements reviewed in Tamba's audit
Statement Evidence
1 Chorionicity and amnionicity of the pregnancy determined using ultrasound andrecorded between 11 weeks 0 days and 13 weeks 6 days
2 Fetuses labelled using an ultrasound scan and recorded between 11 weeks 0 daysand 13 weeks 6 days
3
3a. Women seen by an obstetrician specialising in multiple pregnancies
3b. Women seen by a midwife specialising in multiple pregnancies
3c. Scans undertaken by a sonographer with specialist training in multiplepregnancies
4
4a. Women with a care plan that specified the timing of MDT antenatal careappointments
4b. Women with a care plan that specified scans at correct intervals appropriate forthe type of multiple pregnancy
5
5a. Women monitored for fetal complications according to the chorionicity andamnionicity of her pregnancy
5b. Monitoring carried out by same person
5c. Monitoring carried out by someone qualified to detect TTTS
7 Women that had a discussion by 24 weeks with one or more members of the MDTabout preterm labour & birth
8 Women that had a discussion with one or more members of the MDT by 32 weeksabout the timing of birth and possible modes of delivery
NICE WORKS - Maternity Engagement Project final report 19
MEASURING PATIENT OUTCOMES
Units supplied statistics relating tothe following patient outcomes formultiple pregnancies(25). Theserepresent key outcomes inantenatal care and are in line withthose measured in other nationalmaternity improvement initiatives.This allowed the project to establishoutcomes for comparison againstnational averages and to assesshow units were performing againstunits of a similar size and resourceon a national scale.
■ Stillbirth rates
■ Neonatal deaths
■ Neonatal admissions
■ Emergency caesarean sections
MEASURING CHANGES IN PRACTICE
In order to determine changes inworking practice, Tamba'smidwifery consultants carried outstructured conversations with keyhealth professionals as part of the
audit process. Health professionalswere also asked about changesthey have implemented during theexternal project evaluation (see3.3.1 below). The following areas ofworking practice were prioritisedfor measurement.
■ The presence of a multiplepregnancy care plan in patientnotes
■ The presence of a multiple birthsantenatal clinic
■ The presence of a multiplepregnancy specialist obstetrician
■ The presence of a multiplepregnancy specialist midwife
■ The presence of a multiplepregnancy sonographer
■ Consistent positional labelling offetuses at the dating scan andrecording positions in patientnotes using "left and right", or"upper and lower"
Introduction
The project was managed by asmall team within Tamba consistingof a Project Manager, SeniorProject Co-ordinator and ProjectCo-ordinator - supported by thecharity's senior management. Threeindependent midwifery consultants(from Liverpool Women's Hospital,Leeds General Infirmary and theBrighton and Sussex UniversityHospital Trust) were contracted byTamba to conduct the audits andsupport the units withimplementation. Statistical supportwas originally provided by anEvaluation Officer andsubsequently outsourced to astatistical services company (SelectStatistics).
The project team reported eachquarter to a steering committee.
Membership of the committeeincluded:
■ Department of Health & SocialCare - Maternity SafetyProgramme
■ NICE
■ Royal College of Obstetricians &Gynaecologists
■ Royal College of Midwives
■ Royal College of Nursing
■ British Association of PerinatalMedicine
■ Bliss
■ Sands
■ MBRRACE
■ Multiple Births Foundation
3.2.5 Project management and governance
NICE WORKS - Maternity Engagement Project final report20
3.2.5 Project management and governance (continued)
Introduction
■ NHS England - Maternity VoicesPartnership & MaternityTransformation
■ NHS Improvement - Maternityand Neonatal Transformation
■ FASP (Fetal Anomaly ScreeningProgramme)
■ Society of Radiographers
■ Care Quality Commission -Maternity
■ St George's Hospital
■ The University of Birmingham
3.3 Scope of the reportThis report explores theperformance of the MaternityEngagement Project in relation toits core hypothesis - i.e. that unitscould be encouraged andsupported to make changes to theantenatal care they provide formultiple pregnancies, that thesechanges would increase units'adherence to NICE QS46, and thatincreased adherence to the
guidelines would improve patientoutcomes.
In addition, the experiences ofTamba and the participating unitsof implementing the project areused to generaterecommendations for all thoseseeking to improve practice andoutcomes for twin and othermultiple pregnancies.
3.3.1 InputsThis report draws on the followingsources:
■ An interim report of the projectproduced in conjunction withEva Antoniou ("NICE works, whatwe have learnt so far") coveringanalysis of the baseline auditresults (July 2018)(26).
■ An external evaluation of theproject conducted by FivewaysNP Ltd (December 2018). Thisevaluation:
⬥ reviewed the implementationof the project and its methodof measurement.
⬥ identified good practice,potential improvements, keyrecommendations andlessons learned to support thedevelopment of the approachfor other maternity services.
⬥ identified outcomesgenerated by the project inaddition to those relating toNICE adherence and patientoutcomes.
■ External statistical analysis of theproject's outcomes (actionstaken, levels of NICE adherenceand patient outcomes)comparing the baseline and re-audit data, produced by SelectStatistics Ltd (February 2019).
■ Feedback provided by parentsfrom participating units via aTamba patient satisfactionsurvey conducted after thebaseline audit, and one in-depthqualitative interview (from anadditional unit). Theimplementation of the parentsurvey was problematic - unitswere distributing it at different

NICE WORKS - Maternity Engagement Project final report 21
Introduction
times and the response (97surveys from 16 units) was notsufficient to triangulate NICEadherence, patient outcomesand patient experience.(perhaps understandably as theaudience were parents of new-borns). Although not statisticallyrobust enough to be included inthe project's outcome analysis,qualitative responses fromparents have been used toillustrate points within this report.
■ Feedback from professionalsworking in the participating units(the external evaluationgenerated insight from 47professionals from 25participating units via an online
survey and conducted nine in-depth interviews. Research forthe final report included a furthereight in-depth interviews withprofessionals from the units).
■ Feedback from the Tambaproject team and steering group(the external evaluationgenerated insight from sevenmembers of the Tamba projectteam, including the threemidwifery consultants, and threesteering committee members viain-depth interviews andfacilitated discussions).
■ A review of projectdocumentation (e.g. auditreports, resources available tounits, reports to the funder).
Section 4 covers the actions takenby units (with Tamba's support) toimprove NICE Q46 adherence,outlining what changes to practiceoccurred in the 12 monthsfollowing Tamba's baseline auditand action plan. Qualitativefeedback from parents andprofessionals working in the units(including four detailed casestudies) is used to highlight theneed for those actions and theexperience of making thosechanges.
Section 5 covers the changes tothe level NICE Q46 adherence foreach statement across theparticipating units in the 12 monthsbetween the baseline audit andre-audit. It also explores thecorrelation between taking theactions described in section 4 andimproving adherence.
Section 6 explores the changes inpatient outcomes across theparticipating units in the 12 monthsbetween the baseline audit andre-audit. It explores the relationship
between changes to adherence(described in section 5) andchanges to patient outcomes. Italso postulates what the widerimpact of Tamba's project mightbe if more units were able toachieve the level of improvementin performance as achieved by theproject.
Section 7 summarises key findingsfrom an external processevaluation of the project, includinglearning for future implementation.
Sections 8 and 9 outline the keyconclusions from the project andclarify its recommendations for NHStrusts, units, and policy makers.
3.3.2 Report structure

4 Changes to unitpractice during
the project

NICE WORKS - Maternity Engagement Project final report 23
Changes to unit practice during the project
Key points
59% units introduced at least onenew working practice in the twelvemonths between baseline auditand re-audit in order to improveNICE QS46 adherence.
85% units improved at least onearea of working practice in orderto improve NICE QS46 adherence.
All but one of the 26 units thatneeded to make changes inworking practice did so.
Units in group two made the mostpositive change in the six areas ofpractice measured by the project -addressing (by introducing orimproving practice) 81% of theareas of practice requiring change.
The change most commonlyintroduced by units was theestablishment of a multiplepregnancy specialist midwife (38%units).
The area of practice in which mostunits (73%) made positive change(i.e. introduced or improved) wasthe use of a multiple pregnancycare plan. This change was
facilitated by the provision ofTamba's NICE endorsed MultiplePregnancy Care Pathway(27).
Introducing and improvingspecialist obstetricians,midwives and sonographers wasoften challenging for units asthey faced barriers includingconcerns of "deskilling" thosewho weren't in a specialist role.
Other barriers to changeexperienced by units includedstaffing and capacity issues, andresistance to alter establishedworking practices withinsonography teams.
85% of professionals in unitsthat had completed the projectsaid that the awareness of theclinical needs of multiplepregnancy families hadimproved (no-one thought it hadgot worse).
81% said the continuity of carefor women expecting multipleshad improved over the period ofthe project (no-one thought ithad got worse).
NICE WORKS - Maternity Engagement Project final report24
Changes to unit practice during the project
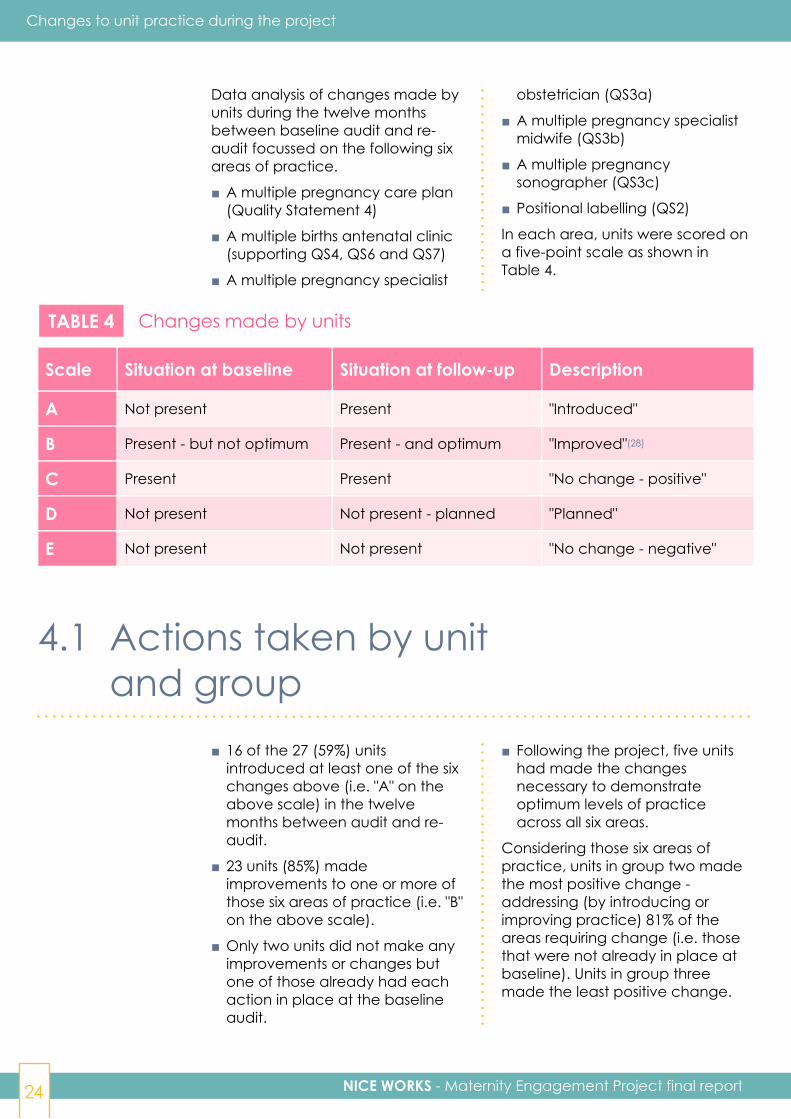
Data analysis of changes made byunits during the twelve monthsbetween baseline audit and re-audit focussed on the following sixareas of practice.
■ A multiple pregnancy care plan(Quality Statement 4)
■ A multiple births antenatal clinic(supporting QS4, QS6 and QS7)
■ A multiple pregnancy specialist
obstetrician (QS3a)
■ A multiple pregnancy specialistmidwife (QS3b)
■ A multiple pregnancysonographer (QS3c)
■ Positional labelling (QS2)
In each area, units were scored ona five-point scale as shown inTable 4.
TABLE 4 Changes made by units
Scale Situation at baseline Situation at follow-up Description
A Not present Present "Introduced"
B Present - but not optimum Present - and optimum "Improved"(28)
C Present Present "No change - positive"
D Not present Not present - planned "Planned"
E Not present Not present "No change - negative"
4.1 Actions taken by unitand group
■ 16 of the 27 (59%) unitsintroduced at least one of the sixchanges above (i.e. "A" on theabove scale) in the twelvemonths between audit and re-audit.
■ 23 units (85%) madeimprovements to one or more ofthose six areas of practice (i.e. "B"on the above scale).
■ Only two units did not make anyimprovements or changes butone of those already had eachaction in place at the baselineaudit.
■ Following the project, five unitshad made the changesnecessary to demonstrateoptimum levels of practiceacross all six areas.
Considering those six areas ofpractice, units in group two madethe most positive change -addressing (by introducing orimproving practice) 81% of theareas requiring change (i.e. thosethat were not already in place atbaseline). Units in group threemade the least positive change.
NICE WORKS - Maternity Engagement Project final report 25
Changes to unit practice during the project
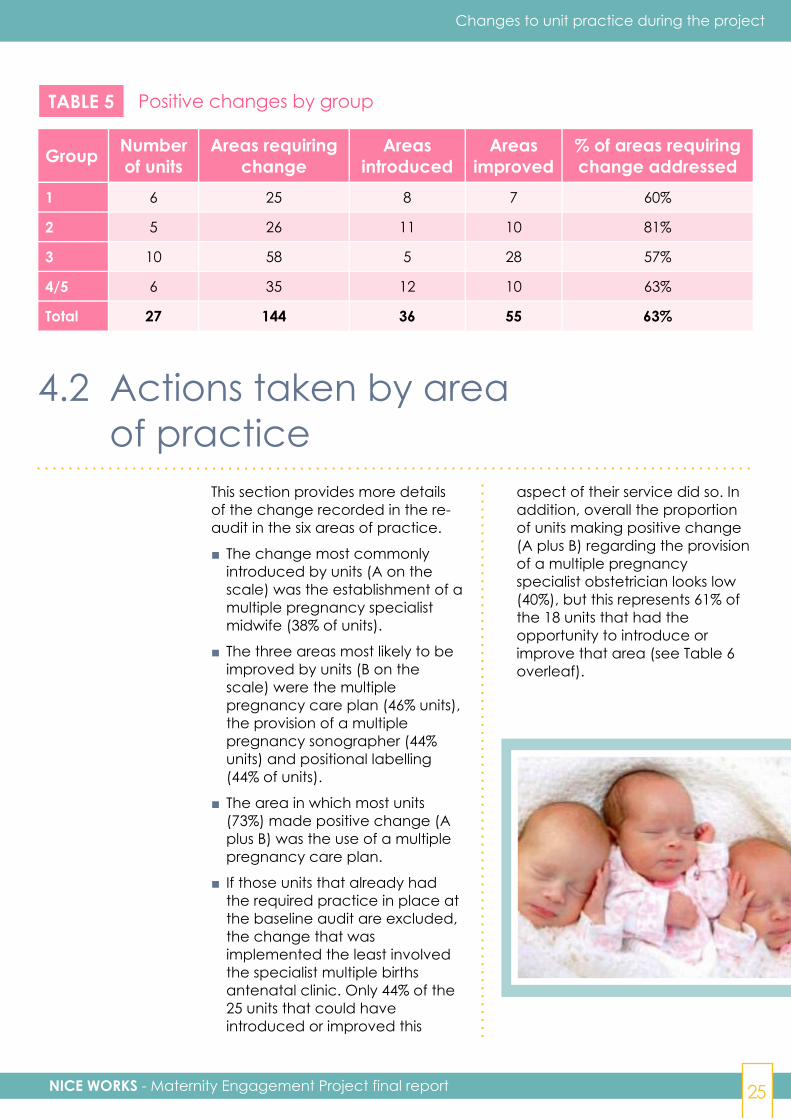
TABLE 5 Positive changes by group
Group Numberof units
Areas requiringchange
Areasintroduced
Areasimproved
% of areas requiringchange addressed
1 6 25 8 7 60%
2 5 26 11 10 81%
3 10 58 5 28 57%
4/5 6 35 12 10 63%
Total 27 144 36 55 63%
4.2 Actions taken by areaof practice
This section provides more detailsof the change recorded in the re-audit in the six areas of practice.
■ The change most commonlyintroduced by units (A on thescale) was the establishment of amultiple pregnancy specialistmidwife (38% of units).
■ The three areas most likely to beimproved by units (B on thescale) were the multiplepregnancy care plan (46% units),the provision of a multiplepregnancy sonographer (44%units) and positional labelling(44% of units).
■ The area in which most units(73%) made positive change (Aplus B) was the use of a multiplepregnancy care plan.
■ If those units that already hadthe required practice in place atthe baseline audit are excluded,the change that wasimplemented the least involvedthe specialist multiple birthsantenatal clinic. Only 44% of the25 units that could haveintroduced or improved this
aspect of their service did so. Inaddition, overall the proportionof units making positive change(A plus B) regarding the provisionof a multiple pregnancyspecialist obstetrician looks low(40%), but this represents 61% ofthe 18 units that had theopportunity to introduce orimprove that area (see Table 6overleaf).
NICE WORKS - Maternity Engagement Project final report26
Changes to unit practice during the project
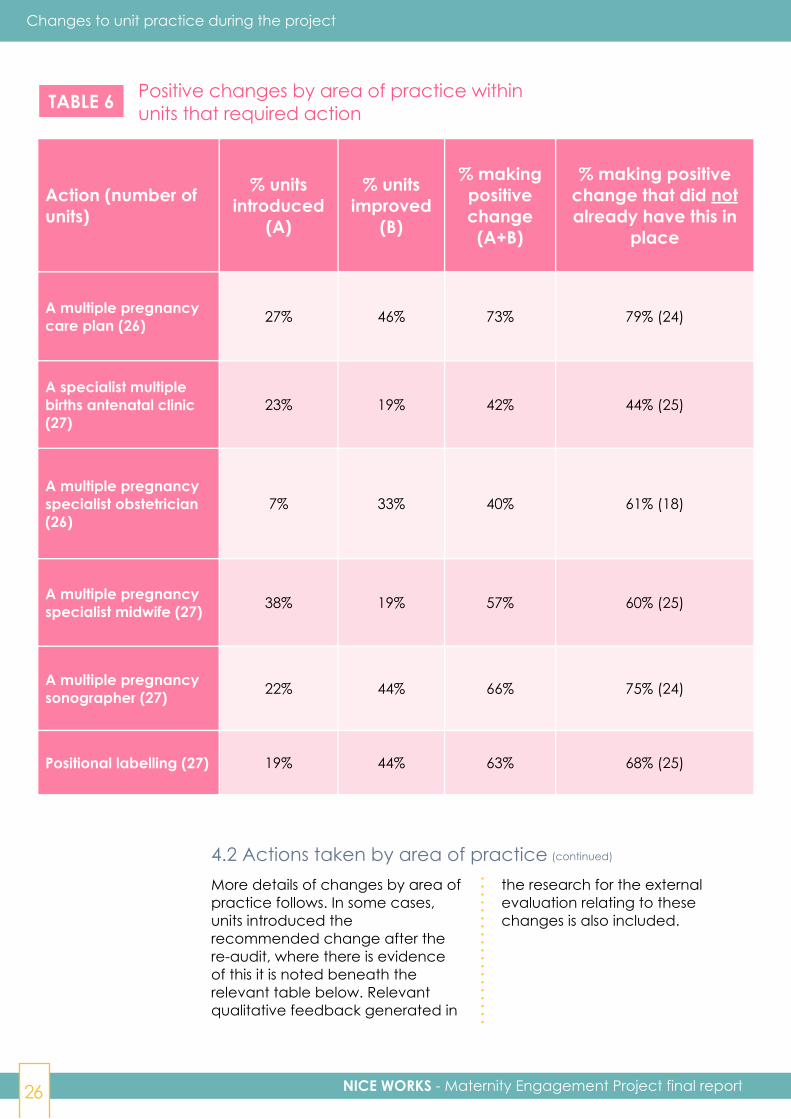
TABLE 6 Positive changes by area of practice withinunits that required action
Action (number ofunits)
% unitsintroduced
(A)
% unitsimproved
(B)
% makingpositivechange
(A+B)
% making positivechange that did notalready have this in
place
A multiple pregnancycare plan (26) 27% 46% 73% 79% (24)
A specialist multiplebirths antenatal clinic(27)
23% 19% 42% 44% (25)
A multiple pregnancyspecialist obstetrician(26)
7% 33% 40% 61% (18)
A multiple pregnancyspecialist midwife (27) 38% 19% 57% 60% (25)
A multiple pregnancysonographer (27) 22% 44% 66% 75% (24)
Positional labelling (27) 19% 44% 63% 68% (25)
More details of changes by area ofpractice follows. In some cases,units introduced therecommended change after there-audit, where there is evidenceof this it is noted beneath therelevant table below. Relevantqualitative feedback generated in
the research for the externalevaluation relating to thesechanges is also included.
4.2 Actions taken by area of practice (continued)
NICE WORKS - Maternity Engagement Project final report 27
Changes to unit practice during the project
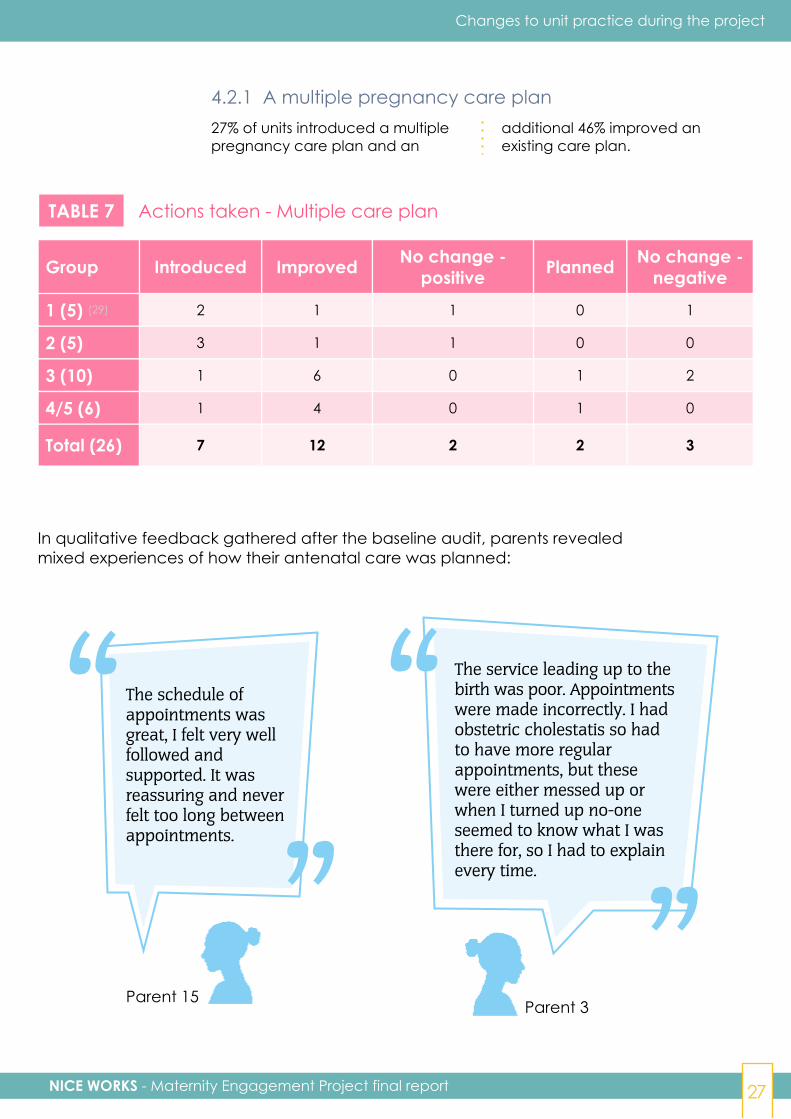
4.2.1 A multiple pregnancy care plan27% of units introduced a multiplepregnancy care plan and an
additional 46% improved anexisting care plan.
Group Introduced Improved No change -positive Planned No change -
negative
1 (5) (29) 2 1 1 0 1
2 (5) 3 1 1 0 0
3 (10) 1 6 0 1 2
4/5 (6) 1 4 0 1 0
Total (26) 7 12 2 2 3
TABLE 7 Actions taken - Multiple care plan
In qualitative feedback gathered after the baseline audit, parents revealedmixed experiences of how their antenatal care was planned:
The schedule ofappointments wasgreat, I felt very wellfollowed andsupported. It wasreassuring and neverfelt too long betweenappointments.
The service leading up to thebirth was poor. Appointmentswere made incorrectly. I hadobstetric cholestatis so hadto have more regularappointments, but thesewere either messed up orwhen I turned up no-oneseemed to know what I wasthere for, so I had to explainevery time.
Parent 15 Parent 3
“”
“
”

NICE WORKS - Maternity Engagement Project final report28
In particular, parents would welcome more detailed discussions aroundthe timing and mode of delivery as part of their plan:
Changes to unit practice during the project
Parent 12“
”It was clear from discussions prior to 36 weeksthat they would prefer a vaginal delivery - I wasn'treally asked what my preference was. I was neverreally sure of how far it would be safe for me togo and when they would consider intervening.
Parent 10“”
There were no discussions -I was told!
The provision of Tamba's Multiple Pregnancy Care Pathway proformasupported units standardise their care planning:
The care plans have been more consistently adhered to over theaudit period. Prior to the audit, our documentation did not alwaysprove that women were receiving information about the signs andsymptoms of pre-term labour, or that the delivery had beenplanned by 32 weeks. Our documentation is more robust now.
We have a high turnover of midwives and doctors - the fact theproforma is so user friendly has really helped. Some registrars haveworked in hospitals where they don't have a proforma and theirfeedback is 'this is great, this is brilliant, it makes it simple and easyto see that all these risk factors have been discussed'. Parents like tohave the facts and figures about the risk factors, the proformamakes sure people are on the right medication or supplements andhelps to identify any issues early. It also ensures discussions onrisks happen in a timely fashion - they can be as early as 14-18weeks. We have ladies who transfer - we complete the proformafor them. Often they haven't been told about the risks.
“”
Unit 1Midwife(survey)
”
“Unit 10Midwife(interview)

NICE WORKS - Maternity Engagement Project final report 29
Case study: Introducing amultiple pregnancy care plan
T amba's MultiplePregnancy CarePathway is a tool that
supports healthcareprofessionals to meet specificaspects of the multiple birthNICE guidelines. It alsosupports statements 1, 3, 4, 5,7 and 8 in NICE's qualitystandard on multiplepregnancy (QS46). Theproforma is used throughouta pregnancy and, as well asencouraging the NICEguidelines to be followed, italso captures importantinformation relating to thepregnancy at key stages. NICEendorsed use of the proformain summer 2018.
According to Mr RichardSmith, Consultant at Norfolkand Norwich UniversityHospitals Trust, Tamba'sMaternity EngagementProject encouraged his unit todevelop their own care planwhich is initially completed atthe parents' booking visit."Beforehand the approach wasnot always consistent acrossmembers of the team - withnotes being written freehandrather than in a template.Tamba helped us focus ourefforts. The fact we were goingto be audited again in twelvemonths' time gave us some
specific targets to worktowards. Tamba also offereduseful advice and guidance onthe content of the plan."
Richard has already seen thebenefits of using the careplan. "It provides a consistentapproach for parents nomatter who they are seeing,and ensures we are complyingwith the national guidance. Ithas also helped us to shareimportant information bothwith parents, who receive acopy of their plan, and withother members of the team.We are now moving towardsembedding the free textcomments made on theantenatal care record into thepatients' electronic record forintrapartum and postnatalcare - so they are very visible tothe relevant member of staffwithout them having to trawlthrough the notes."
Richard also considers thecare plan has contributed topatient safety. "Any measurethat tightens the control wehave over meeting the nationalguidance has to be a positivestep towards patient safetyboth for mothers and babies.Furthermore, we have twospecialist consultants, andother obstetricians at differentstages of their training but who
are not specialists. The careplan means that those doctorsin training are moreempowered to deal with lesscomplicated multiplepregnancies, which allows moretime for specialists to see morecomplex patients who needconsultant input at everyappointment."
One case study where theproject has improved safetyinvolved a patient with apregnancy recorded asdichorionic at booking.Complications arose whichwere suggestive of amonochorionic pregnancy.The team were able to lookback at the scan image (whichthe sonography team havebeen attaching to the recordsince Tamba's visit). Thisallowed them to reclassify thepregnancy as monochorionicand manage the pregnancyappropriately, with a goodoutcome.
In conclusion, Richard feelsthat the project has been "apositive experience for patientsand staff, I would encourageany unit consideringintroducing a multiple specificantenatal care plan to engagewith Tamba every step of theway."
Changes to unit practice during the project
NICE WORKS - Maternity Engagement Project final report30
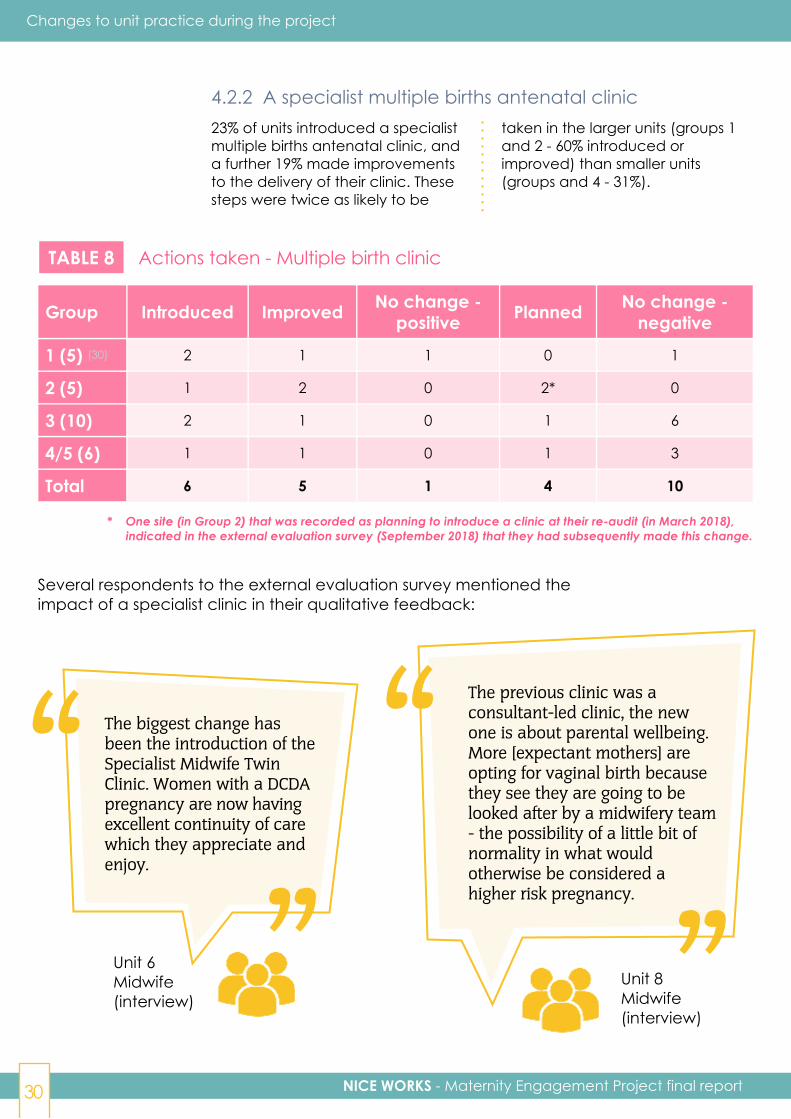
4.2.2 A specialist multiple births antenatal clinic23% of units introduced a specialistmultiple births antenatal clinic, anda further 19% made improvementsto the delivery of their clinic. Thesesteps were twice as likely to be
taken in the larger units (groups 1and 2 - 60% introduced orimproved) than smaller units(groups and 4 - 31%).
TABLE 8 Actions taken - Multiple birth clinic
Group Introduced Improved No change -positive Planned No change -
negative
1 (5) (30) 2 1 1 0 1
2 (5) 1 2 0 2* 0
3 (10) 2 1 0 1 6
4/5 (6) 1 1 0 1 3
Total 6 5 1 4 10
* One site (in Group 2) that was recorded as planning to introduce a clinic at their re-audit (in March 2018), indicated in the external evaluation survey (September 2018) that they had subsequently made this change.
Several respondents to the external evaluation survey mentioned theimpact of a specialist clinic in their qualitative feedback:
Unit 6Midwife(interview)
The biggest change hasbeen the introduction of theSpecialist Midwife TwinClinic. Women with a DCDApregnancy are now havingexcellent continuity of carewhich they appreciate andenjoy.
The previous clinic was aconsultant-led clinic, the newone is about parental wellbeing.More [expectant mothers] areopting for vaginal birth becausethey see they are going to belooked after by a midwifery team- the possibility of a little bit ofnormality in what wouldotherwise be considered ahigher risk pregnancy.
Unit 8Midwife(interview)
“”
“
”
Changes to unit practice during the project

NICE WORKS - Maternity Engagement Project final report 31
This was echoed in one parents' feedback:
Parent 7
”“ Overall the care I received was just as I hoped and
expected it would be. I liked the fact that everything wasin one place (midwife, sonographer, consultant anddiabetic clinic - as I developed gestational diabetes)and staff arranged appointments to run after theother. I was monitored more closely than in aregular pregnancy.
The midwife-led clinic builds a relationshipwith multiple pregnancy women whomare often anxious and need lots ofreassurance.
“”
Unit 10Midwife(survey)
Changes to unit practice during the project
NICE WORKS - Maternity Engagement Project final report32
Case study: Introducing a specialistmultiple births antenatal clinic
A lthough not specificallymentioned in the NICEQS46 guidance,
establishing a specialistmultiple births clinic supportsthe delivery of several of thequality statements (e.g. 4, 6and 7).
Setting up a multiples clinicwas something that KingstonHospital NHS FoundationTrust had given the greenlight for just prior to Tamba'sMaternity Engagementproject. Resources in terms ofhours and space had beenapproved for a clinic for thoseexpecting non-identical twins.
According to Sophie Linghorn,Multiple Birth Midwife atKingston Hospital NHSFoundation Trust, Tamba'ssupport proved useful in theearly days of the clinic, as apoint of reference for whatneeded to be covered at eachappointment. The on-goingsupport of Tamba's specialistmidwife was also important.In addition, Sophie feels thatthe support she received from
her fetal medicineconsultants and consultantmidwife was "invaluable".Having those relationships inplace made the introductionof the clinic verystraightforward.
The clinic has allowed Sophieto incorporate specialistmidwifery-led care into apreviously consultant-ledmodel. "I am now able to haveregular contact with all ourtwin mothers who are nowgetting specialist midwifesupport." For example, shecan "drip feed antenatalinformation at everyappointment so parents aregetting information about (forexample) feeding, getting into aroutine, safe sleeping, and theneonatal unit rather than coverit all in one 'twins talk.' "Sophie also has been giventime to do the bookingappointment for thoseexpecting twins. "Parents arealso signposted to Tamba'sresources plus they have anemail address for non-urgentadvice or questions."
The twin clinic has added toan already close workingrelationship between Sophieand the fetal medicineconsultants - for Sophie thishas meant that, for the morehigh-risk pregnancies, "thereis more of a feeling that we areall watching these women, theirscans and their appointments."This will help improve patientsafety: "I could tell you thehistory of every pregnantwoman from last year - we havemuch more surveillance andcommunication within theteam."
The benefits of offering theclinic and providing continuityof care are clear to Sophie: "asa midwife, it is the best way towork and it gives me a greatdeal of satisfaction - but themain benefit is for the women. Ihave never had so many thankyou cards from parents in mycareer! They feel more lookedafter. All mention the trust andreassurance that is built andhow anxiety levels havelessened."
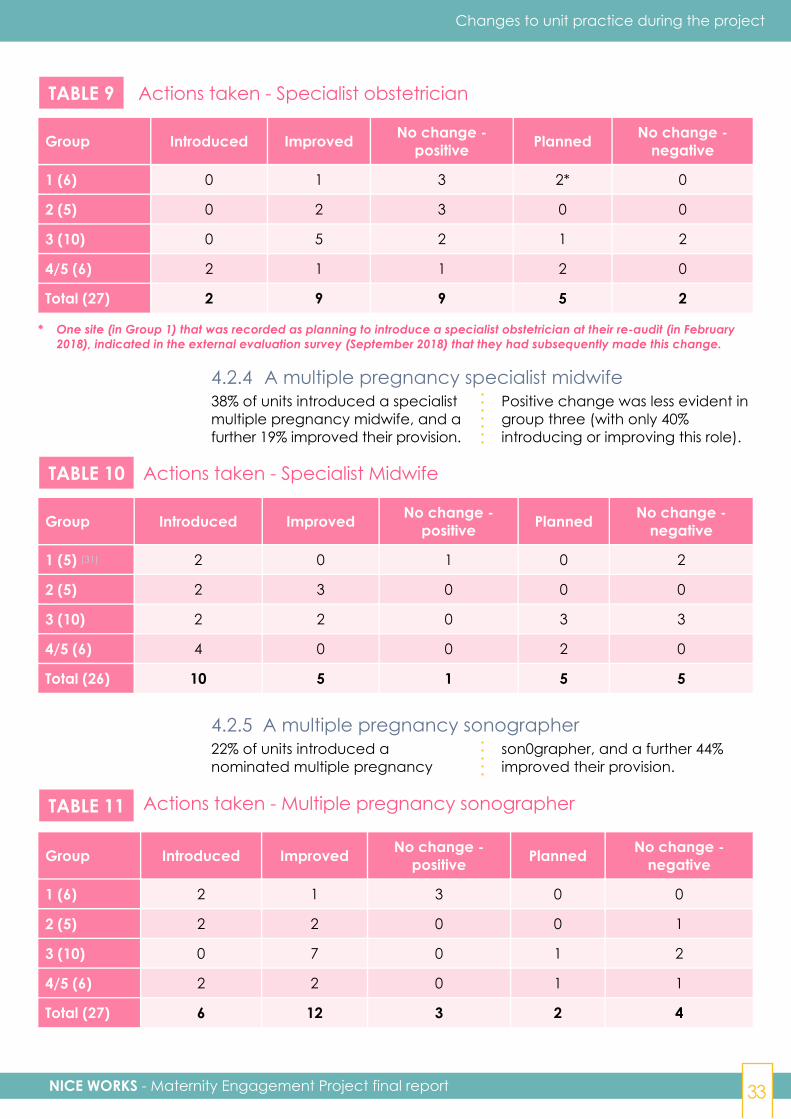
Two thirds of units already had anominated multiple pregnancyobstetrician at baseline, but half ofthese did make improvements to
their provision. Two units (both ingroup four) introduced a specialistobstetrician during the project.
4.2.3 A multiple pregnancy specialist obstetrician
Changes to unit practice during the project
NICE WORKS - Maternity Engagement Project final report 33
TABLE 9 Actions taken - Specialist obstetrician
Group Introduced Improved No change -positive Planned No change -
negative
1 (6) 0 1 3 2* 0
2 (5) 0 2 3 0 0
3 (10) 0 5 2 1 2
4/5 (6) 2 1 1 2 0
Total (27) 2 9 9 5 2
* One site (in Group 1) that was recorded as planning to introduce a specialist obstetrician at their re-audit (in February 2018), indicated in the external evaluation survey (September 2018) that they had subsequently made this change.
4.2.4 A multiple pregnancy specialist midwife38% of units introduced a specialistmultiple pregnancy midwife, and afurther 19% improved their provision.
Positive change was less evident ingroup three (with only 40%introducing or improving this role).
TABLE 10 Actions taken - Specialist Midwife
Group Introduced Improved No change -positive Planned No change -
negative
1 (5) (31) 2 0 1 0 2
2 (5) 2 3 0 0 0
3 (10) 2 2 0 3 3
4/5 (6) 4 0 0 2 0
Total (26) 10 5 1 5 5
4.2.5 A multiple pregnancy sonographer22% of units introduced anominated multiple pregnancy
son0grapher, and a further 44%improved their provision.
TABLE 11 Actions taken - Multiple pregnancy sonographer
Group Introduced Improved No change -positive Planned No change -
negative
1 (6) 2 1 3 0 0
2 (5) 2 2 0 0 1
3 (10) 0 7 0 1 2
4/5 (6) 2 2 0 1 1
Total (27) 6 12 3 2 4
Changes to unit practice during the project

NICE WORKS - Maternity Engagement Project final report34
Case study: Building aMulti-Disciplinary Team
T he third quality statementwithin NICE QS46 is that"women with a multiple
pregnancy are cared for by amultidisciplinary core team" andthat "members of this team willhave the expertise needed toprovide high-quality care forwomen with a multiple pregnancy."The guidance recommends theteam consists of a specialistobstetrician, specialist midwife andan ultrasonographer, "all of whomhave experience and knowledge ofmanaging twin and tripletpregnancies."
The situation at Basildon andThurrock University HospitalsNHS Foundation Trust before theMaternity Engagement projectwas not in line with thisguidance. Women expectingdichorionic twins were put underthe care of one of elevenconsultants and there was nodedicated multiples midwife.Women would see the midwifewho was assisting the doctor intheir clinics at the time. Theymight also see their registrar.
According to Donna Southam,Advanced Specialist Audit andResearch Midwife at Basildonand Thurrock "it was evident inthe initial audit that Tambaconducted that there was noconsistency within the consultantteam as to how to manage twinpregnancies." The audithighlighted that, althoughmonochorionic twins were seenby the same fetal medicineconsultant, those expectingdichorionic twins were neitherseen by an obstetrician or amidwife specialising in multiplepregnancies, nor scanned by asonographer with specialisttraining in multiple pregnancies.
Tamba's recommendation was to
implement a multiples clinic, runby specialist staff.
To implement this Donnaembarked on ten months of"non-stop escalation" feedingback at divisional governancemeetings, the NICE committee,and meeting with the ClinicalDirector and General Managerof the imaging department. ForDonna, implementing changewas all about raising the issuesat the right level and "makingeveryone aware we weren'toffering the best service we could."
To implement change Donnabelieves it is necessary to havesomeone leading the projectwith experience of setting upservices and projectmanagement, who is tenaciousand willing to be a leader withina change management process,and able to build the respect ofthe consultant community.
The trust now has a dedicatedmultiples clinic with a specialistmidwife and deputy (who nowsee all the women after theirscans), and a specialistobstetrician, which waschallenging as, according toDonna, "we needed to review jobplans to facilitate a consultantleading on the clinic. Job planningfor consultants is not a simpleprocess - it takes about a year toget anything changed and agreed. Itcan be difficult for Clinical Directorsand Clinical Leads to manage."
There is also a lead sonographer,although some of Tamba's otherrecommendations on screening(such as labelling and weightdiscordance) took longer tointroduce. In this case, Donnastresses the importance ofhaving the resources toconstantly monitorimplementation: "we were told
by sonography they were doinglabelling and weight discordance,but they weren't. I had to get it onthe imaging department's riskregister that they were breachingNICE guidance, once I did that itturned around within a week." Thefact that the trust was going tobe re-audited by an externalorganisation (Tamba) also helpedwith encouraging action: "whenpeople know somebody's watchingthey change their behaviour".
The benefits of the multi-disciplinary team are alreadybeing realised. "It feels like ateam, they work well together. It'sco-ordinated. The midwife canbring forward appointments withthe consultant if she has anyconcerns. Women have fewer,more streamlined appointmentsand a named contact. It's good forcontinuity of care."
Donna is full of praise forTamba's approach "it's a low-costintervention that leads to asmarter way of working."
Crucially, having the MDT mayhave already helped to improvepatient outcomes. A weightdiscordance of over 25% shouldbe referred to the fetal medicineunit. In 2018 the MDT had threecases of a discordance of over40% who were referred, seen thenext day, and delivered within 72hours because of seriousconcerns. According to Donna"we weren't doing that before,previously these parents mighthave seen a junior doctor and beensent home, and the sonographerswouldn't be writing down theweight discordance - so we mayhave had poor outcomes thatcould have been prevented. Nowwe are monitoring and followingguidance and have clear pathwaysin place."
Changes to unit practice during the project
NICE WORKS - Maternity Engagement Project final report 35
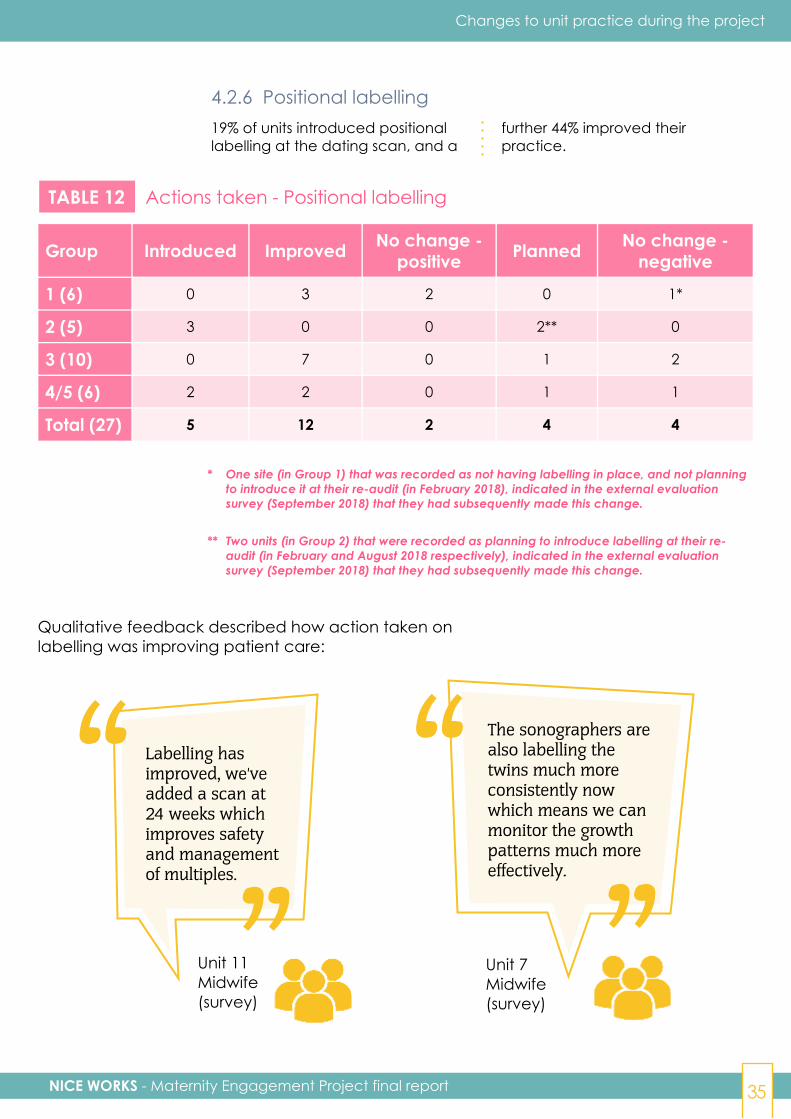
4.2.6 Positional labelling19% of units introduced positionallabelling at the dating scan, and a
further 44% improved theirpractice.
TABLE 12 Actions taken - Positional labelling
Group Introduced Improved No change -positive Planned No change -
negative
1 (6) 0 3 2 0 1*
2 (5) 3 0 0 2** 0
3 (10) 0 7 0 1 2
4/5 (6) 2 2 0 1 1
Total (27) 5 12 2 4 4
* One site (in Group 1) that was recorded as not having labelling in place, and not planning to introduce it at their re-audit (in February 2018), indicated in the external evaluation survey (September 2018) that they had subsequently made this change.
** Two units (in Group 2) that were recorded as planning to introduce labelling at their re- audit (in February and August 2018 respectively), indicated in the external evaluation survey (September 2018) that they had subsequently made this change.
Qualitative feedback described how action taken onlabelling was improving patient care:
Unit 7Midwife(survey)
The sonographers arealso labelling thetwins much moreconsistently nowwhich means we canmonitor the growthpatterns much moreeffectively.
Labelling hasimproved, we'veadded a scan at24 weeks whichimproves safetyand managementof multiples.
Unit 11Midwife(survey)
“”
“”
Changes to unit practice during the project
NICE WORKS - Maternity Engagement Project final report36
4.3 Other changes promptedby the project
The research amongst units for theexternal evaluation revealed thatinvolvement in the projectgenerated broader positive
changes in addition to thechanges specifically targeted bythe project (above).
4.3.1 Attitudinal changeAmongst staff in units that had hadboth their audit and re-audit (27):
■ 81% said that the understandingof what is required to deliver thebest possible care to multiplepregnancy families had improved(no-one thought it had got worse).
■ 85% said that the awareness of
the clinical needs of multiplepregnancy families had improved(no-one thought it had got worse).
■ 82% agreed that "the MaternityEngagement Project has helpedto raise the profile of effectivecare for women expectingmultiples within my hospital" (no-one disagreed).
This cultural or attitudinal change was also reflected in some of the qualitative feedback:
Unit 11SeniorManagement(survey) “
”The overall focus on multiples by the teamhas led to an improvement in standardsand care provided to families.
Unit 8Midwife(interview)
It has just snowballed from a simple email saying I was keento get involved in this audit! Because the audit was sopositive, news travelled to senior management. They weredumbfounded we had done so well in a service where wehadn't put any resources. I finally found people were listening.[Care for multiples] wasn't just "another" specialty inmidwifery. People finally sat up and listened. ”
“4.3.2 Increased continuity of carerHaving more specialist staff isanticipated to improve continuityof carer as parents are likely to see
the same staff members duringtheir antenatal care.
"Better Births", the report of the
Changes to unit practice during the project

NICE WORKS - Maternity Engagement Project final report 37
National Maternity Review,recommended that the NHS inEngland should roll out continuity ofcarer to a much greater number ofwomen. This reflects an aspirationthat "women should havecontinuity of the person lookingafter them during their maternity
journey, before, during and afterthe birth. This continuity of careand relationship between caregiver and receiver has been provento lead to better outcomes andsafety for the woman and baby, aswell as offering a more positive andpersonal experience"(32)
In qualitative responses to Tamba's survey, parentsexpecting multiples clearly would value thisapproach:
[I] always saw the same consultant who did most of the scansand was excellent. The care we received was second to none andwe can't sing her praises highly enough. If I could nominate herfor some kind of recognition award I would.
Parent 16 “ ”Parent 22
I only saw the specialist multiple consultant on one occasionabout 30 weeks and he was great and knowledgeable. I wasvery anxious as I had had wrong and conflictinginformation from other consultants.“
”The many consultants we saw couldn't answer our questions, itwas only on the penultimate visit when we saw the twinsspecialist that we were informed accurately of how the pregnancywas progressing. Numerous conversations with differentconsultants made my pregnancy very stressful. I saw manysonographers - some had an idea, some didn't.
“ ”Parent 20
Parent 4
As there was a different midwife covering every antenatalclinic, I had to explain my pregnancy each time.“ ”
Changes to unit practice during the project

NICE WORKS - Maternity Engagement Project final report38
Changes to unit practice during the project
4.3.3 Teamwork69% of staff in units that had hadboth their audit and re-audit (26)said the team-working betweenobstetricians, midwives andsonographers had improved. No-one felt it had got worse. Thisconfirms the qualitative comments
on more effective teamworkincluded in the case studies aboveon establishing an antenatalmultiple birth clinic (4.2.2) andbuilding a multi-disciplinary teamapproach (4.2.5).
4.3.4 Other changesThe qualitative research alsorevealed additional steps beingintroduced to improve care inother areas as a result of or, atleast, coinciding with, the MEP suchas increasing parental education
sessions, securing resources for amidwife to visit parents at homepostnatally, care plan proformasbeing developed for intrapartumand post-natal care, and changingpolicies relating to water births.
The projectmotivated andencouraged usto improve, evenin areas it wasn'tfocusing on.
Unit 1 Midwife(interview)
The project haschanged mypersonal practicein discussions Ihave with womenunder my care.
Unit 13Obstetrician(survey)
The birth suite isdeveloping a proforma for twinwomen in labour.NICU are alsoinvolved becausethey have seen whatwe're doing. Theyhave used us as aspring board.
Unit 4Midwife(interview)
“”
“
”“
”
I have seen from the changes we have made the benefits of havingcontinuity of sonographer - and how much that is improving patientexperience and their ability to build a relationship with the personcaring for them, and in terms of consistency of measurements, thescan report, and the management pathway.
Amongst staff in units that had had both their audit and re-audit (27) 81% said thecontinuity of care for women expecting multiples had improved overthe period of the project. No-one felt it had got worse:
Unit 3Midwife(interview) “
”

NICE WORKS - Maternity Engagement Project final report 39
Changes to unit practice during the project
4.4 Barriers faced and overcomeThe project revealed commonbarriers faced by units whenimplementing the changes above,
and suggestions for how they mightbe overcome.
4.4.1 "Deskilling"Changes that involved creatingspecialist roles could presentsignificant barriers to change,particularly around the issue of"deskilling" (i.e. that by placing thespecialism for multiples with onemember of the team, othermembers of the team will not haveas much contact with multiplesand, therefore, lose control or the
opportunity to develop their skills incaring for them). In general, largerunits tended to be moreaccustomed to having specialistroles. One of Tamba's midwiferyconsultant reported that makingthe case for an MDT and aspecialist clinic was morechallenging for smaller units withfewer multiple pregnancies.
For those units the focus was more on care pathways andmaking sure all midwives know where resources are. It wasbetter to use a team leader to educate a small team ratherthan put all the onus on one midwife.
TambaMidwiferyConsultant 3 “
”De-skilling is an issue with a specialist service. There wasresistance from ultra-sonographers who felt they were being de-skilled, so we introduced a deputy that rotates so others canstill be involved. IVF consultants like to see their ownpregnancies. Some didn't want to give them up. Ourcompromise was for them to work alongside a consultantlead for multiples, so they will still have an overview.
In others it was clear that some compromiseshad been found to facilitate this change inpractice:
“”
Unit 3Midwife(interview)

NICE WORKS - Maternity Engagement Project final report40
Changes to unit practice during the project
TambaMidwiferyConsultant 3
4.4.2 Influencing sonography teamsAll three of Tamba's midwiferyconsultants spoke aboutsonography being a hard area inwhich to effect this change,especially where sonographerswork for the whole hospital, notonly maternity. It was reported thatmany sonographers enjoyedvariety in their work and that thereare concerns about developingrepetitive strain injury (RSI) ifsonographers were only scanningmultiple pregnancies. This concernis compounded by the issue of
obesity in pregnant womenincreasing the physical demandson sonographers. There were alsoadditional barriers relating tostaffing and capacity issues due tothe implementation of the GrowthAssessment Protocol (GAP)national scanning initiative(33). Itmay be that having a clearprocess for all to follow, rather thanhaving a specialist scanningmultiple pregnancies all the time,would be a more effective methodof facilitating change in this area.
There needs to be practical compromise. There doesn't have tobe one consultant lead. Narrowing it down from six to two is astep in the right direction. It is less about a named role, moreabout making sure someone is taking responsibility.
“”
We have 8-10 sonographers here but not one of them iskeen to join the multiple team - they say it is stressfulscanning twins and there are also concerns about RSI.Midwives love continuity, it is a fabulous way to work -but I don't think sonographers are in that headspace,maybe if they experienced it they would understand thatit is an easier and more satisfying way to work, you feellike you can really make a difference if you have got toknow someone along the way and they trust you.
Unit 6Midwife(interview)
“”4.4.3 Resources and priority
Another barrier was ensuring theimprovements identified by theaudit were given the appropriatepriority and resources (whether thatbe time or money). This wasparticularly challenging for those
leading the project who needed toinfluence change outside of theirteam or area of control. Thequalitative feedback highlightsthese issues:

NICE WORKS - Maternity Engagement Project final report 41
Our lead midwife overseesmultiples, but it is not a specialistrole and she doesn't haveprotected hours - the barriers arefinding resource and getting allthe MDT to agree that isimportant compared with theother pulls on their resources.We want a one stop clinic - butthat needs organisation. Wewould need to release aconsultant and a midwife tojust concentrate on twins, thathas knock on effects on otherstaff - the organisationalaspects are challenging.
Unit 2Midwife Sonographer(interview)“
”
[The barriers are]personnel and finance.Our department hasmany pressures toimprove care, and otherareas are seen as higherpriority e.g. SGA screening,smoking cessation andmaternal mental health.
Unit 14Obstetrician(survey)
“”
Funding is a barrier in terms of clinic time and staff availabilityto ensure consistency of follow up, and in terms of enablingultrasound to have dedicated numbers and members ofstaff assigned to the scanning of multiples.
”“Unit 15
ConsultantRadiologist(survey)
The case study on building a multi-disciplinary team above (4.2.5)reveals the level of tenacity andpersistence needed to positivelyinfluence others.
Qualitative feedback from theexternal evaluation revealed othermethods that were deployed toensure the project was given highenough priority by others such asengaging colleagues early in theproject (especially the baselineaudit) and linking the project towider priorities or projects beingundertaken by the trust - thereforetapping into to others' motivationto achieve those other objectives.
For example, aligning the project'sobjectives to recommendationswithin "Better Births"(34) (such aspersonalised care, continuity ofcarer, multi-professional working)and "Saving Babies Lives - A carebundle for reducing stillbirth"(35) wasconsidered useful. In addition, oneproject lead used compliance withthe CQC framework to drivechange and it was also reportedthat NICE's endorsement of theproject had helped leads bring it tothe attention of others.
It should be recognised that theactions achieved, qualitativefeedback and case studies all
Changes to unit practice during the project
NICE WORKS - Maternity Engagement Project final report42
Changes to unit practice during the project
Case study: A parent's view
V icky, mother to twinsSam and Joe, describesthe antenatal care she
received in one of theparticipating hospitals as "areally positive experience."
Key to her care was regularappointments with aspecialist multiple midwife(whom she describes as"absolutely fantastic, like goingto see a friend") and aspecialist multiple consultant:"they instilled a lot ofconfidence in me, and I washappy to trust them with mycare." When it came tosonography, Vicky saw adifferent professional eachtime.
Having continuity ofmidwifery and obstetric carewas important for Vicky andallowed her to raise issuesand concerns more easily. "Ifyou see different people, theyneed time to read through yournotes to familiarise themselveswith your case. It can get quiterepetitive answering the samequestions over and over again.
You can feel like a numberrather than a patient, so youdon't open up as much. Idiscussed a whole range ofproblems with my multiplespecialist midwife that Iprobably would not haveopened up with if I had seen adifferent person each time." Atthe time Vicky attended hermidwife and consultantclinics in tandem whichmeant she had lots ofappointments. The unit hassubsequently introduced amultiples antenatal clinic toavoid this.
During her antenatal careVicky received plenty ofinformation about possiblerisks and complications. "Iwas told from the off I was ahigh-risk pregnancy and I wasvery well informed and awareof what to look out for. I hadlots of scans. The team were ontop of things, one scan was abit funny and my midwife wasstraight onto it and sent me fora glucose test to see if therewere signs of gestationaldiabetes." She also discussed
the timing of the birth anddelivery choices andwelcomed the fact that herconsultant provided"unemotional and medical"information and her midwifewas available to chat optionsthrough: "it was really good tohave both - it would also havebeen good to have a clearerexplanation of the benefits ofdelivering naturally. I was toldof how it might benefit me interms of recovery, but I wouldhave been more receptive toinformation about how it wouldbenefit the babies."
Another piece of advice fromVicky would be forsonographers to be able toprovide information about theTamba website, especially ifthere is not a dedicatedmultiple sonographer in theunit.
All in all, Vicky was "thrilled"with the care she received. "Ifelt pretty special, like I had aVIP pass to the hospital!"
demonstrate that changes inpractice that make a significantimpact on the care provided canbe made at low or zero cost. Forexample, Tamba's MultiplePregnancy Care Pathway,endorsed by NICE, is available forall units to implement at no cost.Additional resources are also
available from Tamba.Furthermore, the NHS tariffingsystem provides units withadditional funding for multiplepregnancies. A unit receives£1,693 more for the antenatal careof a multiple pregnancy than asingleton(36).
5 Changes toNICE adherence

NICE WORKS - Maternity Engagement Project final report44
Changes to unit NICE adherence
A NOTE ON STATISTICALSIGNIFICANCE
In the following analysis "p-values"help to determine the statisticalsignificance of the results. A 5%(0.05) significance level has been
applied to the calculations. If thep-value is smaller than this, theresult is said to be statisticallysignificant (i.e. it is consideredunlikely to have occurred bychance alone).
Key points
Every one of the 27 unitsmeasured increased their overallNICE QS46 adherence(37) betweenthe baseline audit and the re-audit 12 months later.
Across all 27 test units there wasa statistically significantimprovement in overalladherence of +18%p(38) (p <0.0001).
Units in group two had thelargest average increase inoverall adherence (+30%p), withan average overall adherence atre-audit of 76%.
Across all 27 test units,adherence increased in all sevenNICE QS46 statements measured- the level of increase wasstatistically significant for six ofthe seven statements.
Adherence to statement five(monitoring for fetalcomplications) increased themost from 49% to 83% (34%p)
Units that took steps tointroduce or improve therequired actions(39) saw largeincreases in adherence for therelated NICEQ46 statementcompared with units thatneeded to take action but didnot(40).
Units that implemented ahigher proportion of theirrequired actions (i.e. those notpresent at baseline) tended tosee greater increases in theiroverall adherence.
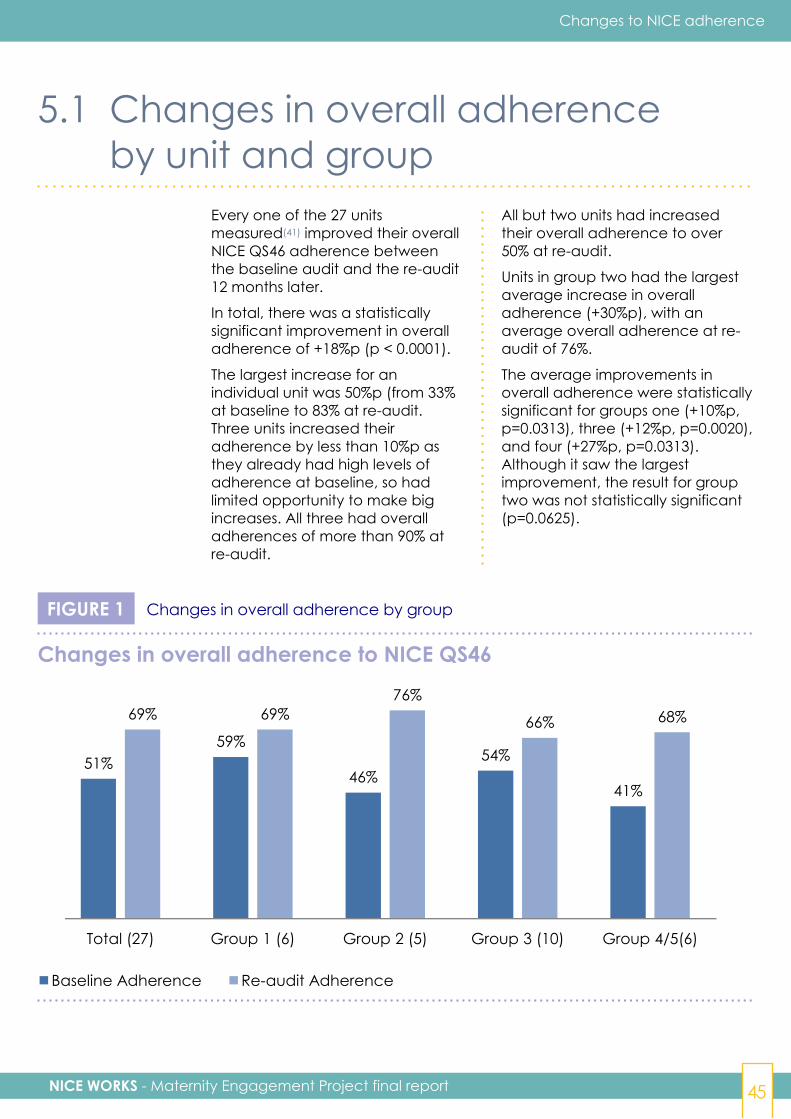
NICE WORKS - Maternity Engagement Project final report 45
Changes to NICE adherence
5.1 Changes in overall adherenceby unit and group
Every one of the 27 unitsmeasured(41) improved their overallNICE QS46 adherence betweenthe baseline audit and the re-audit12 months later.
In total, there was a statisticallysignificant improvement in overalladherence of +18%p (p < 0.0001).
The largest increase for anindividual unit was 50%p (from 33%at baseline to 83% at re-audit.Three units increased theiradherence by less than 10%p asthey already had high levels ofadherence at baseline, so hadlimited opportunity to make bigincreases. All three had overalladherences of more than 90% atre-audit.
All but two units had increasedtheir overall adherence to over50% at re-audit.
Units in group two had the largestaverage increase in overalladherence (+30%p), with anaverage overall adherence at re-audit of 76%.
The average improvements inoverall adherence were statisticallysignificant for groups one (+10%p,p=0.0313), three (+12%p, p=0.0020),and four (+27%p, p=0.0313).Although it saw the largestimprovement, the result for grouptwo was not statistically significant(p=0.0625).
FIGURE 1 Changes in overall adherence by group
51%59%
46%54%
41%
69% 69%76%
66% 68%
Total (27) Group 1 (6) Group 2 (5) Group 3 (10) Group 4/5(6)
Changes in overall adherence to NICE QS46
Baseline Adherence Re-audit AdherenceChanges in overall adherence to NICE QS46
51%59%
46%54%
41%
69% 69%76%
66% 68%
Total (27) Group 1 (6) Group 2 (5) Group 3 (10) Group 4/5(6)
Changes in overall adherence to NICE QS46
Baseline Adherence Re-audit Adherence
NICE WORKS - Maternity Engagement Project final report46
Changes to unit NICE adherence
5.2 Changes in adherence byNICE Q46 statement
5.2.1 OverviewAcross all 27 test units, adherenceincreased in all seven NICE QS46statements measured.
In six of the seven statementsadherence increased bystatistically significant levels. Onlystatement one (determining thechorionicity and amnionicity of thepregnancy by 14 weeks) did not -but adherence was already high
(90%) so there was little opportunityto reach statistical significance.
As noted above, the adherencefigure for statements three, fourand five was an average of "sub-statements". In total eight sub-statements were measured, andadherence increased by astatistically significant amount inseven of them.
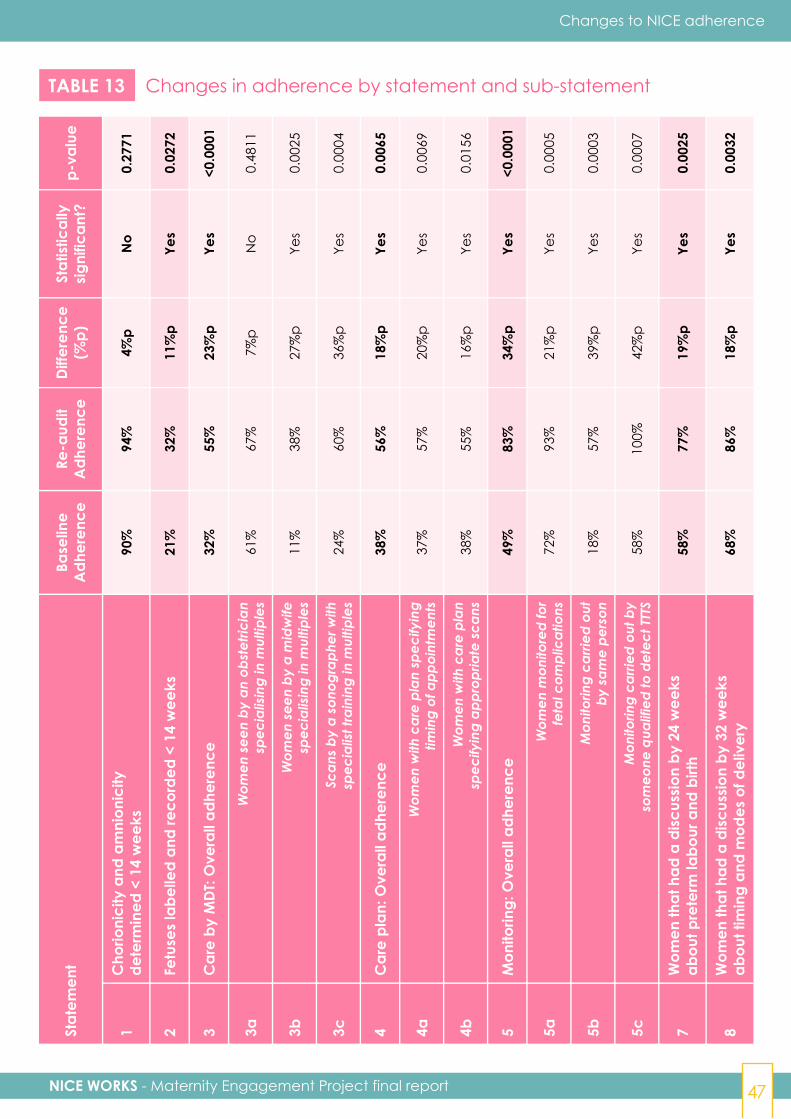
NICE WORKS - Maternity Engagement Project final report 47
Changes to NICE adherence
TABLE 13 Changes in adherence by statement and sub-statementSt
atem
ent
Base
line
Adh
eren
ceRe
-aud
itA
dher
ence
Diff
eren
ce(%
p)St
atist
ical
lysig
nific
ant?
p-va
lue
1C
horio
nici
ty a
nd a
mni
onic
ityde
term
ined
< 1
4 w
eeks
90%
94%
4%p
No
0.27
71
2Fe
tuse
s la
belle
d an
d re
cord
ed <
14
wee
ks21
%32
%11
%p
Yes
0.02
72
3C
are
by M
DT:
Ove
rall
adhe
renc
e32
%55
%23
%p
Yes
<0.0
001
3aW
omen
see
n by
an
obst
etric
ian
spec
ialis
ing
in m
ultip
les
61%
67%
7%p
No
0.48
11
3bW
omen
see
n by
a m
idw
ifesp
ecia
lisin
g in
mul
tiple
s11
%38
%27
%p
Yes
0.00
25
3cSc
ans
by a
son
ogra
pher
with
spec
ialis
t tra
inin
g in
mul
tiple
s24
%60
%36
%p
Yes
0.00
04
4C
are
plan
: Ove
rall
adhe
renc
e38
%56
%18
%p
Yes
0.00
65
4aW
omen
with
car
e pl
an s
peci
fyin
gtim
ing
of a
ppoi
ntm
ents
37%
57%
20%
pYe
s0.
0069
4bW
omen
with
car
e pl
ansp
ecify
ing
appr
opria
te s
cans
38%
55%
16%
pYe
s0.
0156
5M
onito
ring:
Ove
rall
adhe
renc
e49
%83
%34
%p
Yes
<0.0
001
5aW
omen
mon
itore
d fo
rfe
tal c
ompl
icat
ions
72%
93%
21%
pYe
s0.
0005
5bM
onito
ring
carri
ed o
utby
sam
e pe
rson
18%
57%
39%
pYe
s0.
0003
5cM
onito
ring
carri
ed o
ut b
yso
meo
ne q
ualif
ied
to d
etec
t TTT
S58
%10
0%42
%p
Yes
0.00
07
7W
omen
that
had
a d
iscus
sion
by 2
4 w
eeks
abou
t pre
term
labo
ur a
nd b
irth
58%
77%
19%
pYe
s0.
0025
8W
omen
that
had
a d
iscus
sion
by 3
2 w
eeks
abou
t tim
ing
and
mod
es o
f del
iver
y68
%86
%18
%p
Yes
0.00
32
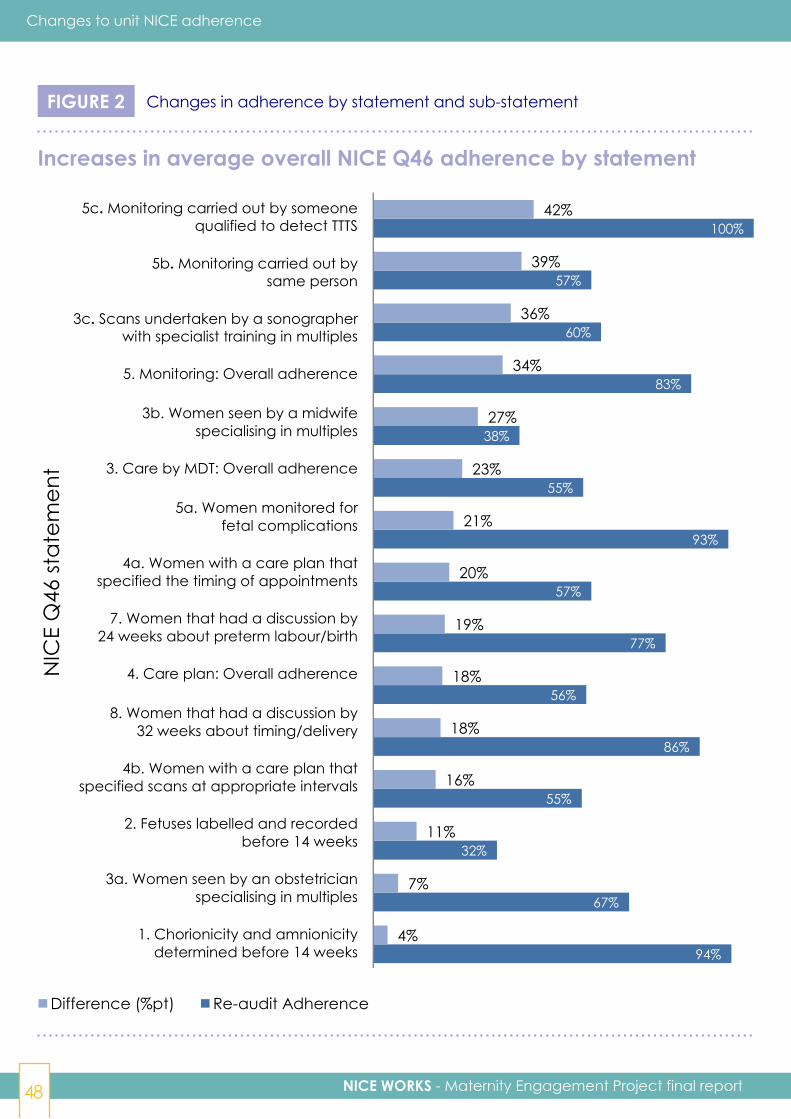
NICE WORKS - Maternity Engagement Project final report48
Changes to unit NICE adherence
FIGURE 2 Changes in adherence by statement and sub-statement
Increases in average overall NICE Q46 adherence by statement
NIC
E Q
46 st
atem
ent
94%
67%
32%
55%
86%
56%
77%
57%
93%
55%
38%
83%
60%
57%
100%
4%
7%
11%
16%
18%
18%
19%
20%
21%
23%
27%
34%
36%
39%
42%
1. Chorionicity and amnionicity determined before 14 weeks
3a. Women seen by an obstetrician specialising in multiples
2. Fetuses labelled and recorded before 14 weeks
4b. Women with a care plan that specified scans at appropriate intervals
8. Women that had a discussion by 32 weeks about timing/delivery
4. Care plan: Overall adherence
7. Women that had a discussion by 24 weeks about preterm labour/birth
4a. Women with a care plan that specified the timing of appointments
5a. Women monitored for fetal complications
3. Care by MDT: Overall adherence
3b. Women seen by a midwife specialising in multiples
5. Monitoring: Overall adherence
3c. Scans undertaken by a sonographer with specialist training in multiples
5b. Monitoring carried out by same person
5c. Monitoring carried out by someone qualified to detect TTTS
Difference (%pt) Re-audit Adherence
94%
67%
32%
55%
86%
56%
77%
57%
93%
55%
38%
83%
60%
57%
100%
4%
7%
11%
16%
18%
18%
19%
20%
21%
23%
27%
34%
36%
39%
42%
1. Chorionicity and amnionicity determined before 14 weeks
3a. Women seen by an obstetrician specialising in multiples
2. Fetuses labelled and recorded before 14 weeks
4b. Women with a care plan that specified scans at appropriate intervals
8. Women that had a discussion by 32 weeks about timing/delivery
4. Care plan: Overall adherence
7. Women that had a discussion by 24 weeks about preterm labour/birth
4a. Women with a care plan that specified the timing of appointments
5a. Women monitored for fetal complications
3. Care by MDT: Overall adherence
3b. Women seen by a midwife specialising in multiples
5. Monitoring: Overall adherence
3c. Scans undertaken by a sonographer with specialist training in multiples
5b. Monitoring carried out by same person
5c. Monitoring carried out by someone qualified to detect TTTS
Difference (%pt) Re-audit Adherence
5c. Monitoring carried out by someonequalified to detect TTTS
5b. Monitoring carried out bysame person
3c. Scans undertaken by a sonographerwith specialist training in multiples
5. Monitoring: Overall adherence
3b. Women seen by a midwifespecialising in multiples
3. Care by MDT: Overall adherence
5a. Women monitored forfetal complications
4a. Women with a care plan thatspecified the timing of appointments
7. Women that had a discussion by24 weeks about preterm labour/birth
4. Care plan: Overall adherence
8. Women that had a discussion by32 weeks about timing/delivery
4b. Women with a care plan thatspecified scans at appropriate intervals
2. Fetuses labelled and recordedbefore 14 weeks
3a. Women seen by an obstetricianspecialising in multiples
1. Chorionicity and amnionicitydetermined before 14 weeks
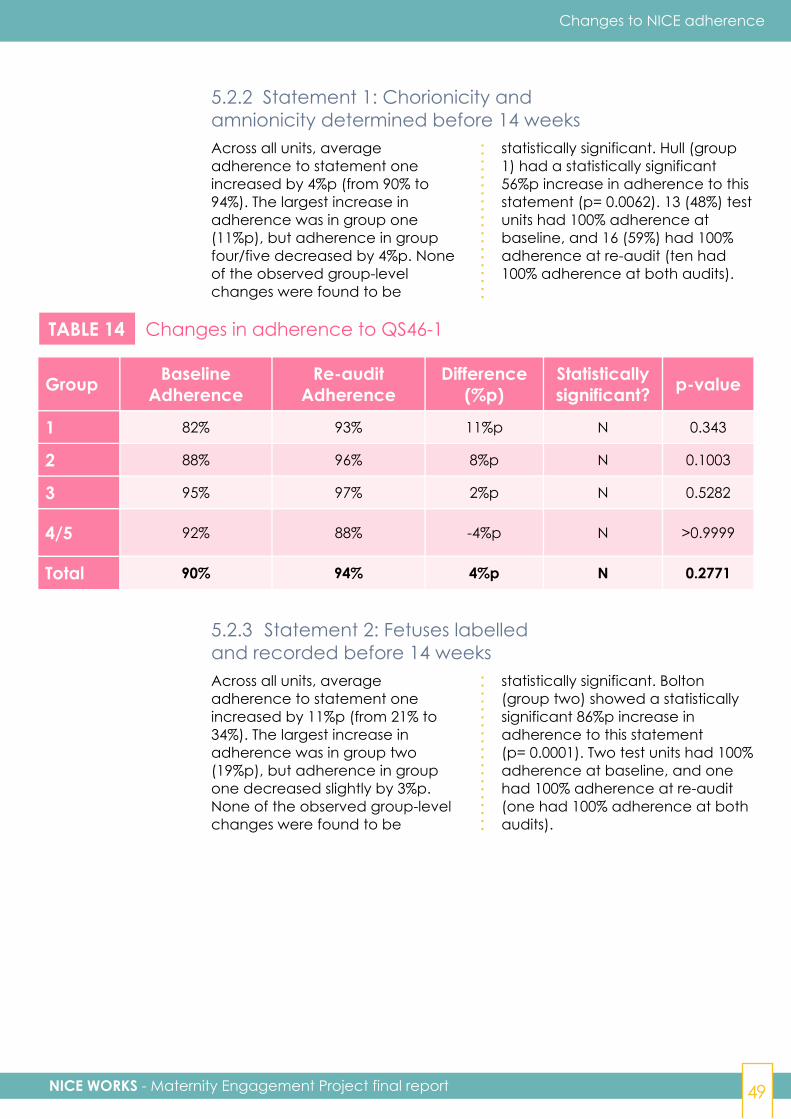
NICE WORKS - Maternity Engagement Project final report 49
Changes to NICE adherence
5.2.2 Statement 1: Chorionicity andamnionicity determined before 14 weeksAcross all units, averageadherence to statement oneincreased by 4%p (from 90% to94%). The largest increase inadherence was in group one(11%p), but adherence in groupfour/five decreased by 4%p. Noneof the observed group-levelchanges were found to be
statistically significant. Hull (group1) had a statistically significant56%p increase in adherence to thisstatement (p= 0.0062). 13 (48%) testunits had 100% adherence atbaseline, and 16 (59%) had 100%adherence at re-audit (ten had100% adherence at both audits).
TABLE 14 Changes in adherence to QS46-1
Group BaselineAdherence
Re-auditAdherence
Difference(%p)
Statisticallysignificant? p-value
1 82% 93% 11%p N 0.343
2 88% 96% 8%p N 0.1003
3 95% 97% 2%p N 0.5282
4/5 92% 88% -4%p N >0.9999
Total 90% 94% 4%p N 0.2771
5.2.3 Statement 2: Fetuses labelledand recorded before 14 weeksAcross all units, averageadherence to statement oneincreased by 11%p (from 21% to34%). The largest increase inadherence was in group two(19%p), but adherence in groupone decreased slightly by 3%p.None of the observed group-levelchanges were found to be
statistically significant. Bolton(group two) showed a statisticallysignificant 86%p increase inadherence to this statement(p= 0.0001). Two test units had 100%adherence at baseline, and onehad 100% adherence at re-audit(one had 100% adherence at bothaudits).
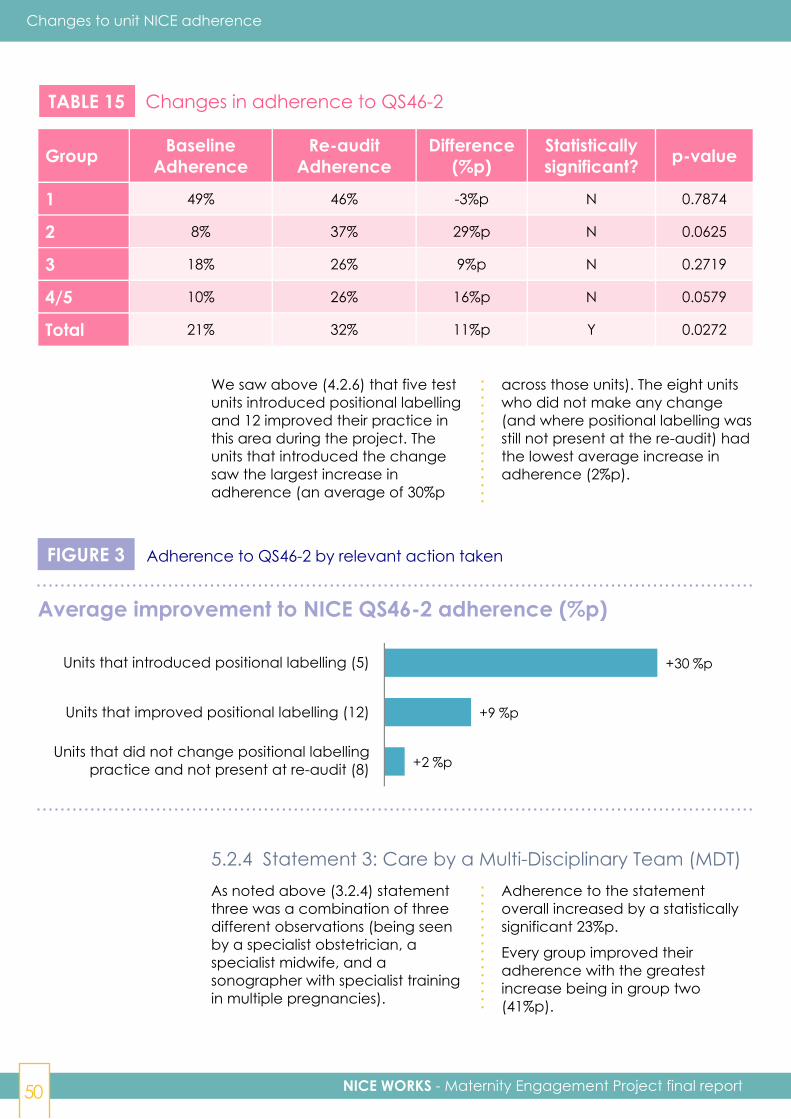
NICE WORKS - Maternity Engagement Project final report50
Changes to unit NICE adherence
TABLE 15 Changes in adherence to QS46-2
Group BaselineAdherence
Re-auditAdherence
Difference(%p)
Statisticallysignificant? p-value
1 49% 46% -3%p N 0.7874
2 8% 37% 29%p N 0.0625
3 18% 26% 9%p N 0.2719
4/5 10% 26% 16%p N 0.0579
Total 21% 32% 11%p Y 0.0272
We saw above (4.2.6) that five testunits introduced positional labellingand 12 improved their practice inthis area during the project. Theunits that introduced the changesaw the largest increase inadherence (an average of 30%p
across those units). The eight unitswho did not make any change(and where positional labelling wasstill not present at the re-audit) hadthe lowest average increase inadherence (2%p).
FIGURE 3 Adherence to QS46-2 by relevant action taken
Average improvement to NICE QS46-2 adherence (%p)
Units that introduced positional labelling (5)
Units that improved positional labelling (12)
Units that did not change positional labellingpractice and not present at re-audit (8)
+30 %p
+9 %p
+2 %p
Units that introduced positional labelling (5)
Units that improved positional labelling (12)
Units that did not change positional labelling practice and not present at re-audit (8)
Average improvement (%pts)
5.2.4 Statement 3: Care by a Multi-Disciplinary Team (MDT)As noted above (3.2.4) statementthree was a combination of threedifferent observations (being seenby a specialist obstetrician, aspecialist midwife, and asonographer with specialist trainingin multiple pregnancies).
Adherence to the statementoverall increased by a statisticallysignificant 23%p.
Every group improved theiradherence with the greatestincrease being in group two(41%p).

NICE WORKS - Maternity Engagement Project final report 51
Changes to NICE adherence
Group BaselineAdherence
Re-auditAdherence
Difference(%p)
Statisticallysignificant? p-value
1 39% 57% 18%p N 0.0739
2 34% 75% 41%p N 0.0625
3 36% 46% 10%p N 0.0801
4/5 15% 51% 36%p N 0.0591
Total 32% 55% 23%p Y <0.0001
TABLE 16 Changes in adherence to QS46-3 overall
SPECIALIST OBSTETRICIAN (3a)
Adherence to the specialistobstetrician aspect to statementthree increased by 7%p, howevermost of the increase was fromgroup four/five (31%p).
Three units showed statisticallysignificant improvements to theiradherence to this sub-statement -Hull (group one, p=0.0186),Stockport (group four, p<0.0001)and Carlisle (group four, p<0.0001).
TABLE 17 Changes in adherence to QS46-3a
Group BaselineAdherence
Re-auditAdherence
Difference(%p)
Statisticallysignificant? p-value
1 65% 68% 3%p N 0.8551
2 87% 92% 5%p N 0.5839
3 57% 52% -6%p N 0.2702
4/5 39% 70% 31%p N 0.2012
Total 61% 67% 7%p N 0.4811
FIGURE 4 Adherence to QS46-3a by relevant action taken
Average improvement to NICE QS46-3a adherence (%p)
+81 %p
+9 %p
-3 %p
Units that introduced specialist obstetrician (2)
Units that improved specialistobstetrician provision (13)
Units that did not change specialist obstetricianprovision and not present at re-audit (7)
+81 %p
+9 %p
-3 %p
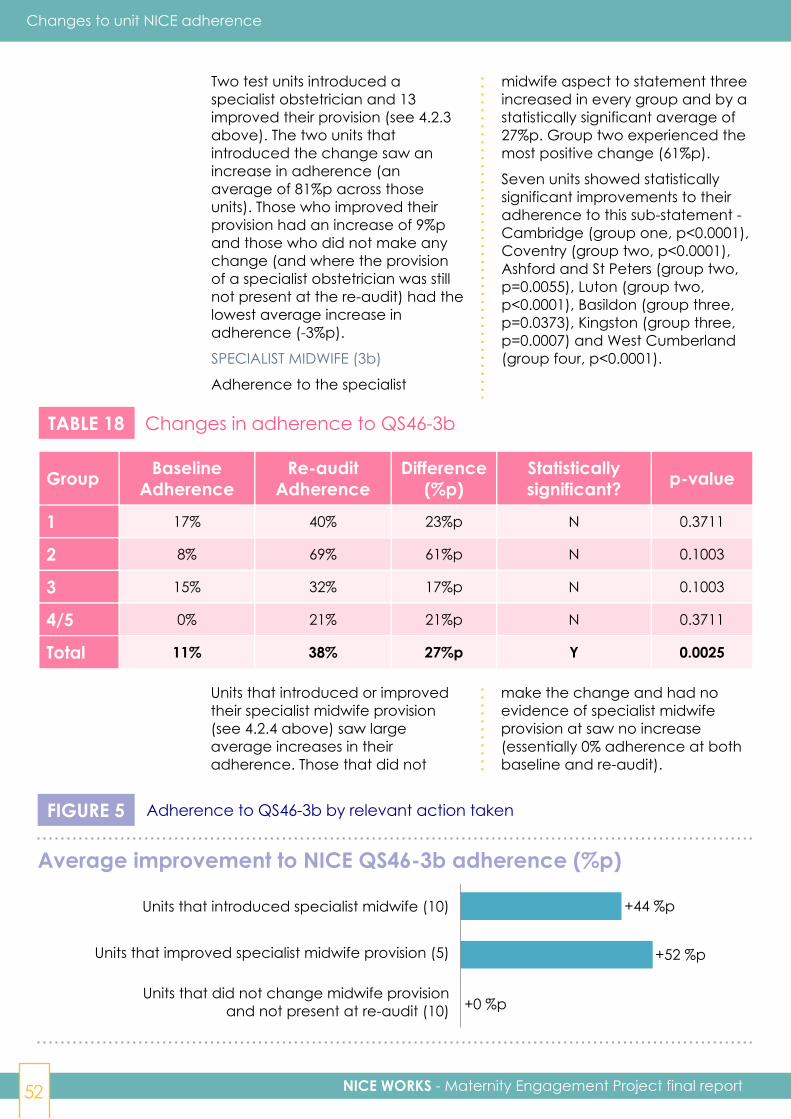
NICE WORKS - Maternity Engagement Project final report52
Changes to unit NICE adherence
Two test units introduced aspecialist obstetrician and 13improved their provision (see 4.2.3above). The two units thatintroduced the change saw anincrease in adherence (anaverage of 81%p across thoseunits). Those who improved theirprovision had an increase of 9%pand those who did not make anychange (and where the provisionof a specialist obstetrician was stillnot present at the re-audit) had thelowest average increase inadherence (-3%p).
SPECIALIST MIDWIFE (3b)
Adherence to the specialist
midwife aspect to statement threeincreased in every group and by astatistically significant average of27%p. Group two experienced themost positive change (61%p).
Seven units showed statisticallysignificant improvements to theiradherence to this sub-statement -Cambridge (group one, p<0.0001),Coventry (group two, p<0.0001),Ashford and St Peters (group two,p=0.0055), Luton (group two,p<0.0001), Basildon (group three,p=0.0373), Kingston (group three,p=0.0007) and West Cumberland(group four, p<0.0001).
TABLE 18 Changes in adherence to QS46-3b
Group BaselineAdherence
Re-auditAdherence
Difference(%p)
Statisticallysignificant? p-value
1 17% 40% 23%p N 0.3711
2 8% 69% 61%p N 0.1003
3 15% 32% 17%p N 0.1003
4/5 0% 21% 21%p N 0.3711
Total 11% 38% 27%p Y 0.0025
Units that introduced or improvedtheir specialist midwife provision(see 4.2.4 above) saw largeaverage increases in theiradherence. Those that did not
make the change and had noevidence of specialist midwifeprovision at saw no increase(essentially 0% adherence at bothbaseline and re-audit).
FIGURE 5 Adherence to QS46-3b by relevant action taken
Average improvement to NICE QS46-3b adherence (%p)
Units that introduced specialist midwife (10)
Units that improved specialist midwife provision (5)
Units that did not change midwife provisionand not present at re-audit (10)
+44 %p
+52 %p
+0 %p
Units that introduced specialist midwife (10)
Units that improved specialist midwife provision (5)
Units that did not change midwife provision and not present at re-audit (10)
+44 %p
+52 %p
+0 %p

NICE WORKS - Maternity Engagement Project final report 53
Changes to NICE adherence
SONOGRAPHER WITH SPECIALISTTRAINING (3c)
The proportion of cases wherescans were undertaken by asonographer with specialist trainingin multiples increased by astatistically significant 36%p acrossall test units. Groups two and foursaw the biggest increase (57%pand 56%p respectively).
Ten units showed statisticallysignificant improvements to their
adherence to this sub-statement -Southampton (group one,p=0.0055), Burnley (group two,p=0.0152), Ashford and St Peters(group two, p<0.0001), Bolton(group two, p<0.0001), PrincessAlexandra (group three, p=0.0108),St Helier (group three, p=0.0010),Surrey (group four, p=0.0010),Stockport (group four, p=0.0010),West Cumberland (group four,p<0.0001) and Dorchester (groupfive, p=0.0001).
TABLE 19 Changes in adherence to QS46-3c
Group BaselineAdherence
Re-auditAdherence
Difference(%p)
Statisticallysignificant? p-value
1 35% 61% 26%p N 0.1775
2 8% 65% 57%p N 0.0975
3 35% 55% 19%p N 0.0592
4/5 6% 62% 56%p N 0.0975
Total 24% 60% 36%p Y 0.0004
As with specialist midwives, unitsthat introduced or improved theirprovision of a sonographer withspecialist multiple training (see 4.2.5above) saw large averageincreases in their adherence. Those
that did not make the change andhad no evidence of provision of asonographer with specialist multipletraining at re-audit saw no increase(essentially 0% adherence at bothbaseline and re-audit).
FIGURE 6 Adherence to QS46-3c by relevant action taken
Average improvement to NICE QS46-3c (%p)
+63 %p
+47 %p
+0 %p
Units that introduced sonographer with specialist training (6)
Units that improved sonographer with specialist training provision (12)
Units that did not change sonographer with specialist training provision and not present at re-audit (6)
Series1
+63 %p
+47 %p
+0 %p
Units that introduced sonographerwith specialist training (6)
Units that improved sonographer withspecialist training provision (12)
Units that did not change sonographerwith specialist training provision and
not present at re-audit (6)

NICE WORKS - Maternity Engagement Project final report54
Changes to unit NICE adherence
5.2.5 Statement 4: Care planAcross all units, averageadherence to statement four(which is a combination to twoaspects - see below) increased by18%p (from 38% to 56%). Overall thisincrease is statistically significant.
Although every group increasedtheir adherence (with group twoincreasing it the most - 39%p), noneof these group-level changes werefound to be statistically significant.
TABLE 20 Changes in adherence to QS46-4 overall
Group BaselineAdherence
Re-auditAdherence
Difference(%p)
Statisticallysignificant? p-value
1 42% 44% 3% N 0.8551
2 34% 73% 39% N 0.0625
3 38% 50% 11% N 0.2012
4/5 36% 64% 28% N 0.0591
Total 38% 56% 18% Y 0.0065
The largest increase (32%p) inadherence was seen in the seven
units who introduced a multiplepregnancy care plan (see 4.2.1).
FIGURE 7 Adherence to QS46-4 by relevant action taken
Average improvement to NICE QS46-4 adherence (%p)
+32 %p
+18 %p
-6 %p
Units that introduced care plan (7)
Units that improved care plan (12)
Units that did not change care plan and not present at re-audit (5)
Series1
+32 %p
+18 %p
-6 %p
Units that introduced care plan (7)
Units that did not change care planand not present at re-audit (5)
Units that improved care plan (12)
MDT APPOINTMENTS (4a)
Average adherence to the careplan specifying the timing of MDTantenatal care appointmentsincreased by a statisticallysignificant 20%p from 37% to 57%.Group two saw the highestincrease (43%p).
Six units showed statistically
significant improvements to theiradherence to this sub-statement -Southampton (group one,p<0.0001), Coventry (group one,p<0.0001), Ashford and St Peters(group two, p=0.0031), Grimsby(group three, p=0.0237), Stockport(group four, p=0.0010) and Carlisle(group four, p=0.0351).

NICE WORKS - Maternity Engagement Project final report 55
Changes to NICE adherence
TABLE 21 Changes in adherence to QS46-4a
Group BaselineAdherence
Re-auditAdherence
Difference(%p)
Statisticallysignificant? p-value
1 37% 50% 13% N >0.9999
2 24% 67% 43% N 0.0625
3 39% 51% 12% N 0.1814
4/5 45% 65% 20% N 0.3613
Total 37% 57% 20% Y 0.0069
SCANS AT CORRECT INTERVALS (4b)
Average adherence to the careplan specifying scans at correctintervals appropriate for the type ofmultiple pregnancy increased by astatistically significant 16%p from38% to 55%. Groups two and foursaw the highest increase (35%p).
Six units showed statistically
significant improvements to theiradherence to this sub-statement-Ashford and St Peters (group two,p=0.0007), Luton (group two,p=0.0300), Scunthorpe (groupthree, p=0.0053), St Helier (groupthree, p=0.0351), Stockport (groupfour, p<0.0001) and Carlisle (groupfour, p=0.0351).
TABLE 22 Changes in adherence to QS46-4b
Group BaselineAdherence
Re-auditAdherence
Difference(%p)
Statisticallysignificant? p-value
1 47% 38% -8%p N 0.5839
2 43% 78% 35%p N 0.0625
3 37% 48% 10%p N 0.3613
4/5 28% 63% 35%p N 0.0591
Total 38% 55% 16%p Y 0.0156
5.2.6 Statement 5: Monitoring for fetal complicationsOf all the NICE QS46 statements,this saw the largest increase inadherence (34%p). This overallincrease was statistically significant- as were the increases for groupsone, three and four.
Three units increased their overallstatement five adherence to 100%
at re-audit (no units were 100% atbaseline) Only one test unit out of27 saw a decrease in their overallstatement five adherence.

NICE WORKS - Maternity Engagement Project final report56
TABLE 23 Changes in adherence to QS46-5 overall
Changes to unit NICE adherence
Group BaselineAdherence
Re-auditAdherence
Difference(%p)
Statisticallysignificant? p-value
1 53% 81% 28%p Y 0.0355
2 40% 88% 48%p N 0.0625
3 66% 79% 14%p Y 0.0098
4/5 26% 88% 62%p Y 0.0313
Total 49% 83% 34%p Y <0.0001
This overall result is an average ofthree measurements detailed below.
CASES MONITORED FOR FETALCOMPLICATIONS (5a)
The proportion of cases monitoredfor fetal complications increasedby 21%p - with group four/fiveseeing the largest increase (44%p).The proportion of test units with100% adherence increased from
9/27 (33%) at baseline to 17/27(63%) at re-audit.
Five units showed statisticallysignificant improvements to theiradherence to this sub-statement -Coventry (group two, p=0.0033),Luton (group two, p=0.0096),Grimsby (group three, p=0.0039),Carlisle (group four, p=0.0019) andDorchester (group five, p=0.0325).
TABLE 24 Changes in adherence to QS46-5a
Group BaselineAdherence
Re-auditAdherence
Difference(%p)
Statisticallysignificant? p-value
1 79% 87% 8% N 0.3711
2 65% 98% 33% N 0.1003
3 85% 94% 9% N 0.1362
4/5 49% 92% 44% Y 0.0313
Total 72% 93% 21% Y 0.0005
MONITORING UNDERTAKEN BY THESAME PERSON (5b)The proportion of cases monitoredfor fetal complications by the sameperson increased by 39%p - withgroup four/five again seeing thelargest increase (68%p). Theproportion of test units with 100%adherence increased from 0/27 (0%)at baseline to 4/27 (15%) at re-audit.Ten units showed statisticallysignificant improvements to their
adherence to this sub-statement -Coventry (group two, p=0.0177),Burnley (group two, p=0.0010),Ashford and St Peters (group two,p<0.0001), Bolton (group two,p=0.0049), Cornwall (group three,p=0.0108), Poole (group three,p=0.0031), Epsom (group three,p=0.0181), East and North Herts(group three, p=0.0062), Stockport(group four, p=0.0110) and WestCumberland (group four, p<0.00001).

NICE WORKS - Maternity Engagement Project final report 57
Changes to NICE adherence
TABLE 25 Changes in adherence to QS46-5b
Group BaselineAdherence
Re-auditAdherence
Difference(%p)
Statisticallysignificant? p-value
1 29% 56% 27%p N 0.1775
2 7% 67% 60%p N 0.1003
3 26% 43% 17%p N 0.1925
4/5 4% 72% 68%p Y 0.0313
Total 18% 57% 39%p Y 0.0003
MONITORING UNDERTAKEN BYSOMEONE QUALIFIED TO DETECTTWIN-TO-TWIN TRANSFUSIONSYNDROME (TTTS) (5c)
The proportion of cases wheremonitoring was carried out bysomeone qualified to detect TTTSincreased by 42%p (to 99.7%). Allbut one of the 282 cases examinedin the re-audit adhered to thiscriterion. The proportion of test unitswith 100% adherence increasedfrom 12/27 (44%) at baseline to26/27 (96%) at re-audit.
13 units showed statisticallysignificant improvements to their
adherence to this sub-statement -Hull (group one, p=0.0005),Southampton (group one,p=0.0010), Bristol (group one,p=0.0023), Coventry (group two,p=0.0028), Burnley (group two,p=0.0010), Ashford and St Peters(group two, p<0.0001), Basildon(group three, p=0.0128), Cornwall(group three, p=0.0325), Surrey(group four, p=0.0182), Stockport(group four, p=0.0o88), WestCumberland (group four,p<0.0001), Carlisle (group four,p<0.0001) and Dorchester (groupfive, p=0.0003).
TABLE 26 Changes in adherence to QS46-5c
Group BaselineAdherence
Re-auditAdherence
Difference(%p)
Statisticallysignificant? p-value
1 52% 100% 48%p N 0.0975
2 49% 98% 50%p N 0.1814
3 86% 100% 14%p N 0.1814
4/5 25% 100% 75%p N 0.0533
Total 58% 100% 42%p Y 0.0007
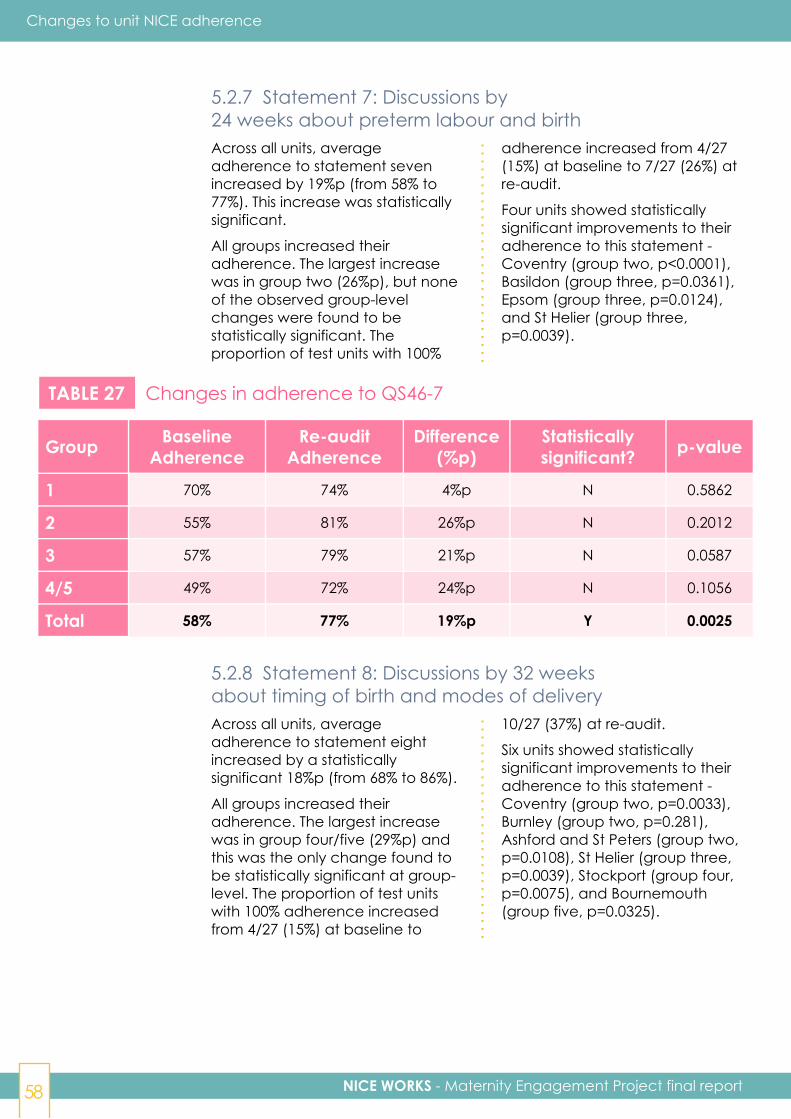
NICE WORKS - Maternity Engagement Project final report58
Changes to unit NICE adherence
5.2.7 Statement 7: Discussions by24 weeks about preterm labour and birthAcross all units, averageadherence to statement sevenincreased by 19%p (from 58% to77%). This increase was statisticallysignificant.
All groups increased theiradherence. The largest increasewas in group two (26%p), but noneof the observed group-levelchanges were found to bestatistically significant. Theproportion of test units with 100%
adherence increased from 4/27(15%) at baseline to 7/27 (26%) atre-audit.
Four units showed statisticallysignificant improvements to theiradherence to this statement -Coventry (group two, p<0.0001),Basildon (group three, p=0.0361),Epsom (group three, p=0.0124),and St Helier (group three,p=0.0039).
TABLE 27 Changes in adherence to QS46-7
Group BaselineAdherence
Re-auditAdherence
Difference(%p)
Statisticallysignificant? p-value
1 70% 74% 4%p N 0.5862
2 55% 81% 26%p N 0.2012
3 57% 79% 21%p N 0.0587
4/5 49% 72% 24%p N 0.1056
Total 58% 77% 19%p Y 0.0025
5.2.8 Statement 8: Discussions by 32 weeksabout timing of birth and modes of deliveryAcross all units, averageadherence to statement eightincreased by a statisticallysignificant 18%p (from 68% to 86%).
All groups increased theiradherence. The largest increasewas in group four/five (29%p) andthis was the only change found tobe statistically significant at group-level. The proportion of test unitswith 100% adherence increasedfrom 4/27 (15%) at baseline to
10/27 (37%) at re-audit.
Six units showed statisticallysignificant improvements to theiradherence to this statement -Coventry (group two, p=0.0033),Burnley (group two, p=0.281),Ashford and St Peters (group two,p=0.0108), St Helier (group three,p=0.0039), Stockport (group four,p=0.0075), and Bournemouth(group five, p=0.0325).
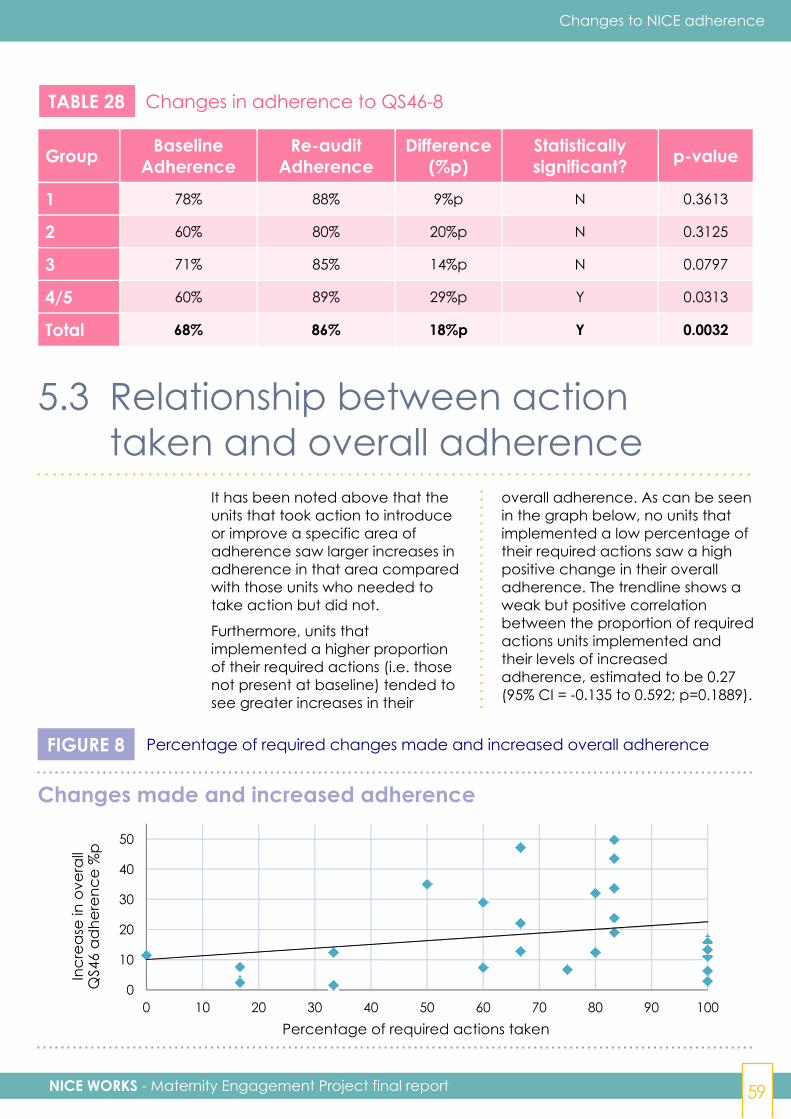
NICE WORKS - Maternity Engagement Project final report 59
Changes to NICE adherence
TABLE 28 Changes in adherence to QS46-8
Group BaselineAdherence
Re-auditAdherence
Difference(%p)
Statisticallysignificant? p-value
1 78% 88% 9%p N 0.3613
2 60% 80% 20%p N 0.3125
3 71% 85% 14%p N 0.0797
4/5 60% 89% 29%p Y 0.0313
Total 68% 86% 18%p Y 0.0032
5.3 Relationship between actiontaken and overall adherence
It has been noted above that theunits that took action to introduceor improve a specific area ofadherence saw larger increases inadherence in that area comparedwith those units who needed totake action but did not.
Furthermore, units thatimplemented a higher proportionof their required actions (i.e. thosenot present at baseline) tended tosee greater increases in their
overall adherence. As can be seenin the graph below, no units thatimplemented a low percentage oftheir required actions saw a highpositive change in their overalladherence. The trendline shows aweak but positive correlationbetween the proportion of requiredactions units implemented andtheir levels of increasedadherence, estimated to be 0.27(95% CI = -0.135 to 0.592; p=0.1889).
FIGURE 8 Percentage of required changes made and increased overall adherence
0
10
20
30
40
50
0 10 20 30 40 50 60 70 80 90 100Percentage of required actions taken
Incr
ease
in o
vera
llQ
S46
adhe
renc
e %
p
Changes made and increased adherence
6 Changes topatient outcomes
NICE WORKS - Maternity Engagement Project final report 61
Changes to patient outcomes
Key points
Six units saw statistically significantreductions in at least one patient outcome(one for emergency C-sections, four forneonatal admissions and one for neonataldeaths and neonatal admissions)
STILLBIRTHS
At baseline it was observed that increasedadherence to QS46 statements seven(discussions by 24 weeks on preterm labourand birth) and eight (discussions by 32weeks on timing and delivery) werecorrelated with a lower still birth rate ingroup one (r=-0.89(42), p=0.02 and r=-0.9,p=0.01 respectively).
At follow-up there was some weak evidence(p=0.0257) of re-audit level stillbirth ratesbeing lower for units with an engagedmaternity champion compared to thosewithout (by approximately -0.009%p; 95% CI= -0.017%p to -0.001%p).
Although in the 12 months between auditsthere was not a significant change inmultiple stillbirth rates, the evidence from StGeorge's University Hospital, which was anexemplar unit and an early adopter of NICEQS46, saw a 70% reduction (from 14 per 1000in 2012 to 4 per 1000 in 2016) in twinstillbirths over a five year period. Over alonger period of time (2000-2019) and withan increased cohort, comparing the preimplementation 32/2250 vs. postimplementation 5/1147 rates, the resultbecomes statistically significant (p=0.008).
If all units were able to replicate thisprolonged high standard of stillbirth care a70% uniform reduction would equate to savingthe lives of up to 100 stillborn babies in fiveyears. This would result in a twin stillbirthrate of 1.85 per thousand which is lower thanthe 2016 singleton stillbirth rate of 3.86(43).
NEONATAL DEATHS
There was no significant change in themultiple neonatal death rate between theaudits. Only one unit saw a statisticallysignificant reduction. The majority ofneonatal deaths are a result of prematurityand a significant proportion are
spontaneous. None of the NICE QualityStandards have focused on prevention ofspontaneous preterm births. The NICEguidance on which they are based iscurrently being updated and willpotentially address this point.
NEONATAL ADMISSIONS
In the 12 months between audits, 65% ofunits showed a reduction in theirneonatal admissions rate for multiples.This may be as a result of a reduction iniatrongenic interventions. Across all unitsthere was an average reduction of 5.8%p.This was not found to be statisticallysignificant.
There is statistically significant evidence(p=0.0011) of a greater increase in theadherence of NICE QS46-5 overall(monitoring for fetal complications)between baseline and re-audit beingassociated with a larger decrease in theneonatal admissions rate.
If all units in England (157) achievedsimilar improvements in care practice andNICE adherence that would represent1,308 fewer admissions in a year, with acost saving of £8million.
EMERGENCY CAESAREAN SECTIONS
In the 12 months between audits, 60% ofunits showed a reduction in theiremergency caesarean section rate formultiples in the 12 months betweenbaseline and re-audit. Across all unitsthere was an average reduction of 3.1%p.This was not found to be statisticallysignificant.
If all units were able to implement thechanges in care practice to achieve thisreduction that would represent 634 feweremergency caesarean sections per year.
There is statistically significant evidence(p=0.0436) of a greater increase in theadherence of NICE QS46-2 (positionallabelling) between baseline and re-auditbeing associated with a larger decrease inthe emergency C-sections rate.
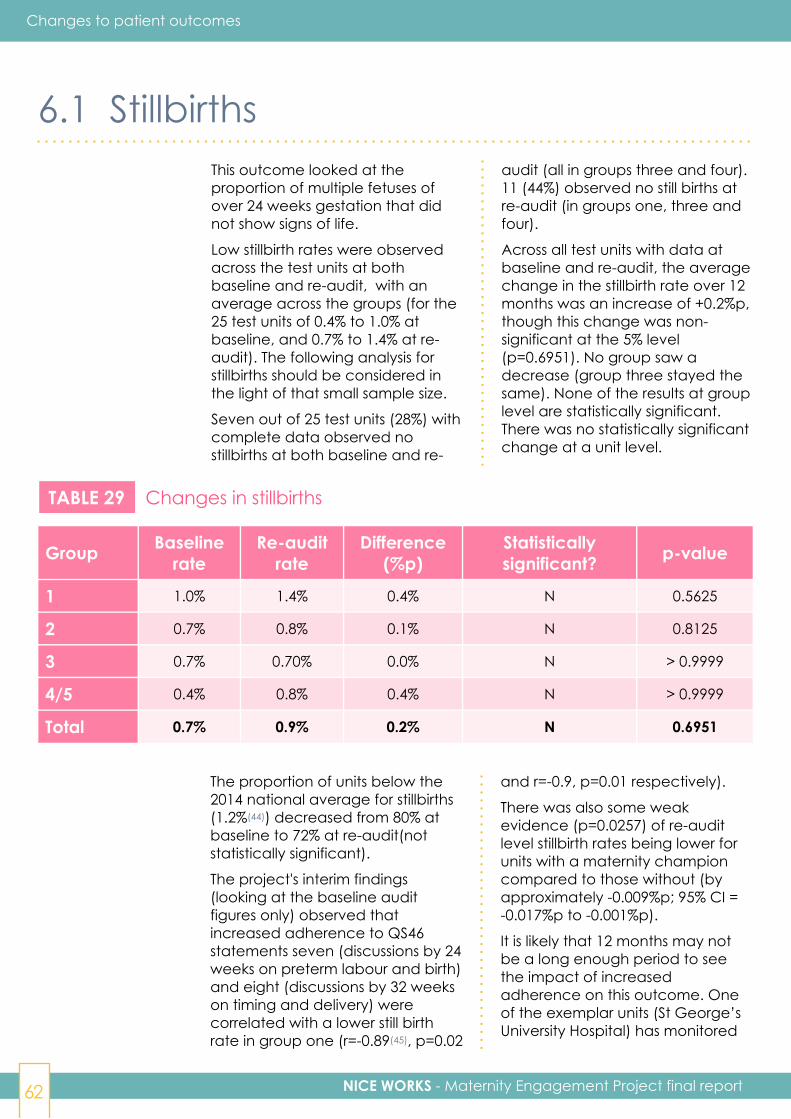
NICE WORKS - Maternity Engagement Project final report62
Changes to patient outcomes
6.1 StillbirthsThis outcome looked at theproportion of multiple fetuses ofover 24 weeks gestation that didnot show signs of life.
Low stillbirth rates were observedacross the test units at bothbaseline and re-audit, with anaverage across the groups (for the25 test units of 0.4% to 1.0% atbaseline, and 0.7% to 1.4% at re-audit). The following analysis forstillbirths should be considered inthe light of that small sample size.
Seven out of 25 test units (28%) withcomplete data observed nostillbirths at both baseline and re-
audit (all in groups three and four).11 (44%) observed no still births atre-audit (in groups one, three andfour).
Across all test units with data atbaseline and re-audit, the averagechange in the stillbirth rate over 12months was an increase of +0.2%p,though this change was non-significant at the 5% level(p=0.6951). No group saw adecrease (group three stayed thesame). None of the results at grouplevel are statistically significant.There was no statistically significantchange at a unit level.
TABLE 29 Changes in stillbirths
Group Baselinerate
Re-auditrate
Difference(%p)
Statisticallysignificant? p-value
1 1.0% 1.4% 0.4% N 0.5625
2 0.7% 0.8% 0.1% N 0.8125
3 0.7% 0.70% 0.0% N > 0.9999
4/5 0.4% 0.8% 0.4% N > 0.9999
Total 0.7% 0.9% 0.2% N 0.6951
The proportion of units below the2014 national average for stillbirths(1.2%(44)) decreased from 80% atbaseline to 72% at re-audit(notstatistically significant).
The project's interim findings(looking at the baseline auditfigures only) observed thatincreased adherence to QS46statements seven (discussions by 24weeks on preterm labour and birth)and eight (discussions by 32 weekson timing and delivery) werecorrelated with a lower still birthrate in group one (r=-0.89(45), p=0.02
and r=-0.9, p=0.01 respectively).
There was also some weakevidence (p=0.0257) of re-auditlevel stillbirth rates being lower forunits with a maternity championcompared to those without (byapproximately -0.009%p; 95% CI =-0.017%p to -0.001%p).
It is likely that 12 months may notbe a long enough period to seethe impact of increasedadherence on this outcome. Oneof the exemplar units (St George’sUniversity Hospital) has monitored

NICE WORKS - Maternity Engagement Project final report 63
Changes to patient outcomes
6.2 Neonatal deathsThis outcome looked at theproportion of multiple fetuses ofany gestation with signs of life thatdied before 28 days of age.
Low neonatal death rates wereobserved across the units at bothbaseline and re-audit, with anaverage across the groups (for the25 test units) of 0.2% to 2.1% atbaseline, and 0.5% to 2.2% at re-audit. As with stillbirths, thefollowing analysis for neonataldeaths should be considered in thelight of the small sample size.
Six of the test units (24%) withcomplete data observed noneonatal deaths at both baselineand re-audit, and therefore nochange between baseline and re-
audit (all in Groups three and four).11 (44%) observed no neonataldeaths at re-audit (across allGroups).
Across all test units with data atbaseline and re-audit, the averagechange in neonatal death ratewas an increase of +0.1%p, thoughthis change was non-significant atthe 5% level (p=0.7936). Group onewas the only group to show adecrease (-0.5%p), but none of theresults at group level are statisticallysignificant.
One unit, Norwich (group one),saw a statistically significantreduction in their neonatal deathrate (from 3.2% to 0%, p=0.0336).
the impact of adherence toguidelines on twin stillbirths over alonger period and found that ittook 18-24 months to implementthe guidelines and see theimprovement in outcomes. It saw a70% reduction (from 14 per 1000 in2012 to 4 per 1000 in 2016) in twin
stillbirths over a five year period.Over a longer period of time (2000-2019) and with an increasedcohort, comparing the preimplementation 32/2250 vs. postimplementation 5/1147 rates, theresult becomes statisticallysignificant (p=0.008).

NICE WORKS - Maternity Engagement Project final report64
Changes to patient outcomes
TABLE 30 Changes in neonatal deaths
Group Baselinerate
Re-auditrate
Difference(%p)
Statisticallysignificant? p-value
1(46) 1.90% 1.3% -0.5% N 0.6875
2 2.1% 2.2% 0.2% N 0.8125
3 0.3% 0.5% 0.2% N 0.5839
4/5 0.6% 1.1% 0.5% N 0.5839
Total 1.0% 1.2% 0.1% N 0.7936
The proportion of units below the2014 national average for neonataldeaths for multiples (1.1%)increased from 56% at baseline to64% at re-audit.
As with stillbirths, 12 months maynot be a long enough period tosee the impact of increasedadherence on neonatal deaths.The majority of neonatal deaths
are a result of prematurity and asignificant proportion arespontaneous. None of the NICEQuality Standards focus onprevention of spontaneous preterm births. The NICE guidance onwhich they are based is currentlybeing updated and is due to bepublished by the end of 2019.
6.3 Neonatal admissionsThis outcome looked at thenumbers of babies admitted toneonatal care as a proportion ofmultiple fetuses.
15 out of 23 (65%)(47) of the testunits with complete data showed areduction in their neonataladmission rate for multiples in the12 months between baseline to re-audit. Five units saw a statisticallysignificant reduction in theirneonatal admission rate.Southampton (group one, from46% to 24%, p<0.0001), Norwich(group one, from 82% to 69%,p=0.0082), Cornwall (group three,from 58% to 38%, p=0.0066), Surrey(group four, from 64% to 25%,p<0.0001) and Carlisle (group four,from 53% to 19%, p=0.0137).
Across the "test" units with
complete data, overall there wasan average -5.6%p decrease in theneonatal admission rate formultiples. This change was non-significant at the 5% level(p=0.1424). Group four/five showedthe largest decrease (14%p). Thisreduction equates to 200 feweradmissions in 12 months across the24 units with complete data.
Anecdotally this reduction may bedue to improved scanningpractices identifying risks earlier,leading to closer monitoring and areduction in early intervention iftreatment is not required - thoughthis hypothesis would need furtherinvestigation.
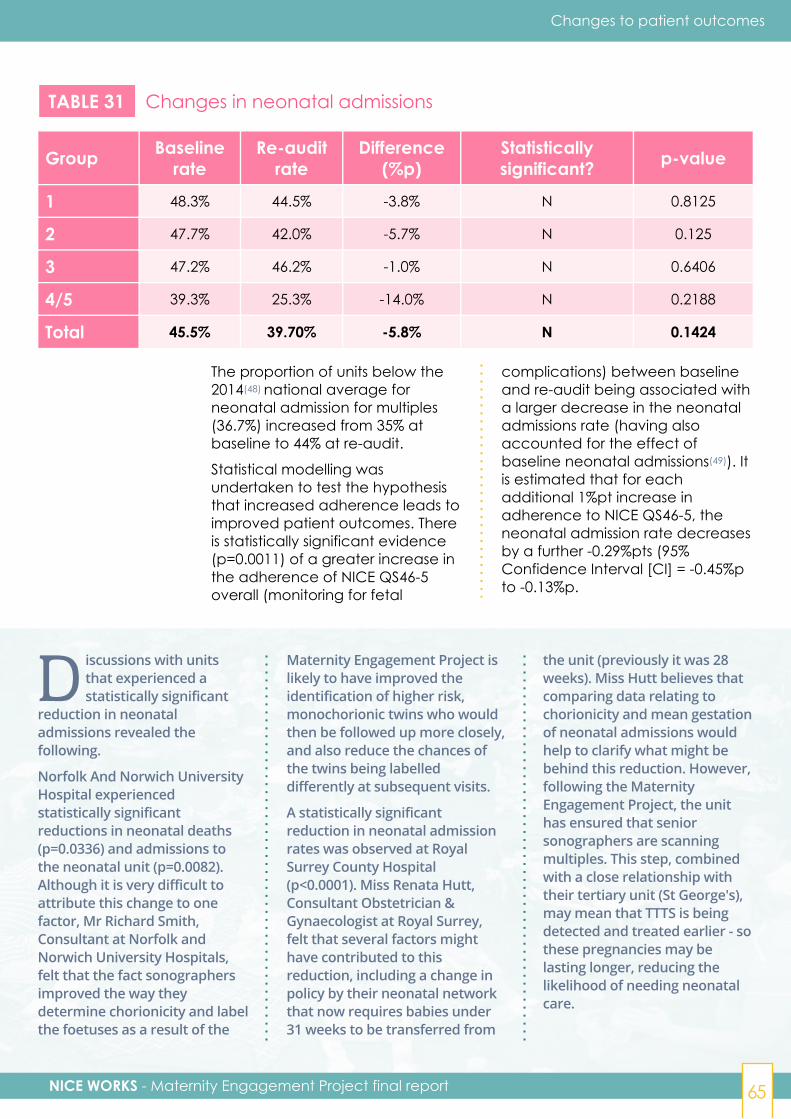
NICE WORKS - Maternity Engagement Project final report 65
Changes to patient outcomes
TABLE 31 Changes in neonatal admissions
Group Baselinerate
Re-auditrate
Difference(%p)
Statisticallysignificant? p-value
1 48.3% 44.5% -3.8% N 0.8125
2 47.7% 42.0% -5.7% N 0.125
3 47.2% 46.2% -1.0% N 0.6406
4/5 39.3% 25.3% -14.0% N 0.2188
Total 45.5% 39.70% -5.8% N 0.1424
The proportion of units below the2014(48) national average forneonatal admission for multiples(36.7%) increased from 35% atbaseline to 44% at re-audit.
Statistical modelling wasundertaken to test the hypothesisthat increased adherence leads toimproved patient outcomes. Thereis statistically significant evidence(p=0.0011) of a greater increase inthe adherence of NICE QS46-5overall (monitoring for fetal
complications) between baselineand re-audit being associated witha larger decrease in the neonataladmissions rate (having alsoaccounted for the effect ofbaseline neonatal admissions(49)). Itis estimated that for eachadditional 1%pt increase inadherence to NICE QS46-5, theneonatal admission rate decreasesby a further -0.29%pts (95%Confidence Interval [CI] = -0.45%pto -0.13%p.
D iscussions with unitsthat experienced astatistically significant
reduction in neonataladmissions revealed thefollowing.
Norfolk And Norwich UniversityHospital experiencedstatistically significantreductions in neonatal deaths(p=0.0336) and admissions tothe neonatal unit (p=0.0082).Although it is very difficult toattribute this change to onefactor, Mr Richard Smith,Consultant at Norfolk andNorwich University Hospitals,felt that the fact sonographersimproved the way theydetermine chorionicity and labelthe foetuses as a result of the
Maternity Engagement Project islikely to have improved theidentification of higher risk,monochorionic twins who wouldthen be followed up more closely,and also reduce the chances ofthe twins being labelleddifferently at subsequent visits.
A statistically significantreduction in neonatal admissionrates was observed at RoyalSurrey County Hospital(p<0.0001). Miss Renata Hutt,Consultant Obstetrician &Gynaecologist at Royal Surrey,felt that several factors mighthave contributed to thisreduction, including a change inpolicy by their neonatal networkthat now requires babies under31 weeks to be transferred from
the unit (previously it was 28weeks). Miss Hutt believes thatcomparing data relating tochorionicity and mean gestationof neonatal admissions wouldhelp to clarify what might bebehind this reduction. However,following the MaternityEngagement Project, the unithas ensured that seniorsonographers are scanningmultiples. This step, combinedwith a close relationship withtheir tertiary unit (St George's),may mean that TTTS is beingdetected and treated earlier - sothese pregnancies may belasting longer, reducing thelikelihood of needing neonatalcare.
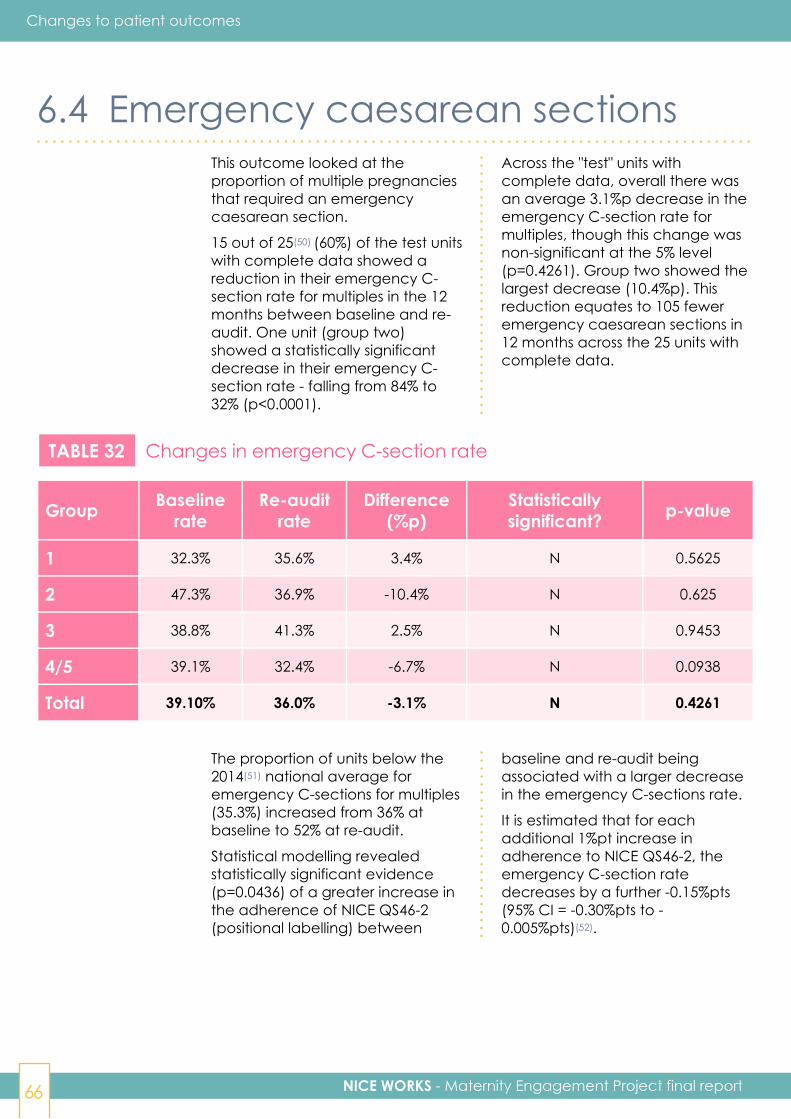
NICE WORKS - Maternity Engagement Project final report66
Changes to patient outcomes
6.4 Emergency caesarean sectionsThis outcome looked at theproportion of multiple pregnanciesthat required an emergencycaesarean section.
15 out of 25(50) (60%) of the test unitswith complete data showed areduction in their emergency C-section rate for multiples in the 12months between baseline and re-audit. One unit (group two)showed a statistically significantdecrease in their emergency C-section rate - falling from 84% to32% (p<0.0001).
Across the "test" units withcomplete data, overall there wasan average 3.1%p decrease in theemergency C-section rate formultiples, though this change wasnon-significant at the 5% level(p=0.4261). Group two showed thelargest decrease (10.4%p). Thisreduction equates to 105 feweremergency caesarean sections in12 months across the 25 units withcomplete data.
TABLE 32 Changes in emergency C-section rate
Group Baselinerate
Re-auditrate
Difference(%p)
Statisticallysignificant? p-value
1 32.3% 35.6% 3.4% N 0.5625
2 47.3% 36.9% -10.4% N 0.625
3 38.8% 41.3% 2.5% N 0.9453
4/5 39.1% 32.4% -6.7% N 0.0938
Total 39.10% 36.0% -3.1% N 0.4261
The proportion of units below the2014(51) national average foremergency C-sections for multiples(35.3%) increased from 36% atbaseline to 52% at re-audit.
Statistical modelling revealedstatistically significant evidence(p=0.0436) of a greater increase inthe adherence of NICE QS46-2(positional labelling) between
baseline and re-audit beingassociated with a larger decreasein the emergency C-sections rate.
It is estimated that for eachadditional 1%pt increase inadherence to NICE QS46-2, theemergency C-section ratedecreases by a further -0.15%pts(95% CI = -0.30%pts to -0.005%pts)(52).
NICE WORKS - Maternity Engagement Project final report 67
Changes to patient outcomes
6.5 Potential project impactAs detailed earlier in the report,overall, units saw a 5.8% reductionin neonatal admissions in the 12months of the project. If all units inEngland (157) achieved similarimprovements in care practice andNICE adherence that wouldrepresent 1,308 fewer admissions ina year, with a cost saving on£8million.
Similarly, units saw a 3.1% reductionin emergency caesarean sections.If all units were able to implementthe changes in care practice toachieve this reduction that wouldrepresent 634 fewer emergency
caesarean sections each year.
If units were able to achieve highlevels of adherence to guidelinesover a longer period than thisproject, they could anticipatereducing twin stillbirths by 70% afterfive years. If all units were able toreplicate that standard of care thiswould equate to saving the lives ofup to 100 stillborn babies each yearafter this five year period. Thiswould result in a twin stillbirth rateof 1.85 per thousand which isbelow the 2016 singleton stillbirthrate of 3.86.

7 Processlearning
NICE WORKS - Maternity Engagement Project final report 69
Key points
Units were highly satisfied withhow the project was conducted.82% of professionals in the unitswould recommend that allmaternity units get involved inthe project (no-one disagreed).
77% of professionals agree theinitial audit was a fair reflectionof the situation (7% disagreed)and 85% agreed the re-audit wasan accurate reflection of thechanges their unit had made(11% disagreed).
90% of professionals who hadcompleted the project agreedthat "if we hadn't done the
Maternity Engagement Projectwe would not have achieved asmuch positive change" (only 6%disagreed).
74% of professionals agreed"The Maternity EngagementProject was the catalyst forpositive change in care forwomen expecting multiples inour unit" (14% disagreed).
The main piece of processlearning was to conduct thefollow-up re-audit later to giveunits longer than 12 months todeliver their action plan(perhaps after 18 to 24months).
Process learning
This section summarises the keylearning from the external
evaluation of the MaternityEngagement Project (see 3.3.1).
NICE WORKS - Maternity Engagement Project final report70
Process learning
7.1 Units' experience ofparticipating in the project
Overall, units were very positiveabout their experience of workingwith Tamba on the MEP with amajority of professionals surveyed(35)(53) describing Tamba'sapproach as "professional",
"supportive" and "collaborative".The predominately positiveexperience of the units wasreflected in the qualitativefeedback.
Recommending others participatein the MEP was used as a proxy foroverall satisfaction. 82% ofprofessionals surveyed (33) would
recommend that all maternity unitsget involved in the MaternityEngagement Project (with only 6%disagreeing(54)).
7.2 Units' feedback on thesupport provided
7.2.1 The auditsThe audit process itself wasbeneficial to the units as a meansof reflecting on current practiceand what might be improved. 89%of professionals who had had both
audits at the time of the evaluationsurvey (28) agreed that the auditswere useful in helping identifyareas to improve.
The involvement from Tamba has exceededmy expectations. My contacts were alwayshelpful, efficient and professional.“
”Unit 6Midwife(interview)
NICE WORKS - Maternity Engagement Project final report 71
Process learning
The audit hashighlighted areas,such as early labellingof twins, where wehad clear guidelines,but these were notbeing followed asaccurately as theyshould have been.
Unit 9Obstetrician(survey)
The project helped toidentify the gaps - that wasreally valuable. Nothingwas provided for thesehigh-risk women who endup in hospital. We wereproviding lots of things forlots of other high-riskpregnancies but not forthese poor women - whenwe said that it was an eyeopener.
Unit 4Midwife(interview)
Most professionals felt that theaudit was measuring the rightthings and that the process ofbeing audited was"straightforward", "well planned"and "positive". 77% of allprofessionals who responded to theevaluation survey (44) agreed the
initial audit was a fair reflection ofthe situation (7% disagreed).Where dissatisfaction with themeasurement process existed, itcentred on the auditors'unfamiliarity with a specific unit'snotes or system.
Unit 9Obstetrician(interview)
Our systems seem to be marked down. The auditorshad in their head a mode of care that exists in otherhospitals. Our system is different. Some hospitals dohave consultants do the scan to assess fetal growthrestriction and feto-fetal transfusion syndrome. Wedon't, but we review the scan immediately.
“”
“
”
“”85% of all re-audited respondents
to the survey (27) agreed the re-audit was an accurate reflection of
the changes made (11%disagreed).
NICE WORKS - Maternity Engagement Project final report72
Process learning
7.2.2 The action planThe action plan generated by theinitial audit was also considered auseful tool to guide and focusimplementation. 71% of
professionals who had had bothaudits at the time of the evaluationsurvey (28) agreed that the actionsin the plan were achievable.
7.2.3 Ongoing supportThose leading the project reportedthat they had received excellent
support from the Tamba midwiferyconsultant they worked alongside.
I had wonderful support, incredibly helpful, focussed -knowledgeable, committed, non-judgemental, really,really kind and sympathetic. She [the Tamba midwiferyconsultant] understood we didn't have the sameresources as other trusts. I felt I could ask her anything.
Unit 5Midwife(interview)
7.3 Tamba’s role in facilitating changeThe external evaluation surveyrevealed that a vast majority ofrespondents attributed the positivechange they have witnessed totheir involvement with theMaternity Engagement Project.
90% of professionals that had hadboth the baseline audit and re-audit at the time of the survey (21)agreed that "if we hadn't done theMaternity Engagement Project we
would not have achieved as muchpositive change" (only 6% disagreed)and 74% agreed "The MaternityEngagement Project was thecatalyst for positive change in carefor women expecting multiples inour unit" (14% disagreed).
Feedback from the qualitativeresearch supports the overallpositive impact of the project onparticipating units.
“”
They [Tamba] didn't just tell uswhat we needed to do, theygave us advice on how to do it. Unit 3
Midwife(interview)
“”

NICE WORKS - Maternity Engagement Project final report 73
Process learning
7.4 Learning for future implementationAs we have seen above, units werehighly satisfied with the projectdelivery. However, four key
suggestions were made for howthings might be improved ordeveloped in subsequent projects.
7.4.1 A later re-auditOne theme in the qualitativefeedback was for units to havelonger than 12 months to deliver
their action plan (perhaps 18 to 24months).
Having an external organisation involved also helpedproject leads to instigate change:
Since the Tamba audit, the [multiple] service has beenbetter recognised through our trust and further fundedhours have been allocated to the specialist midwife tobegin a continuity of carer model. This is all due to thepositive feedback that we had received from Tamba. Thetrust has now invested in the multiples service as theycan clearly see the benefits to the patients, thepatient experience has improved vastly.
Unit 8Midwife(survey)
We were aware of inconsistent care provided by themedical team from a previous audit. I had tried tochallenge this before but hadn't moved forward. Butbecause this was an external project it made peoplelisten within the department. When you know you arebeing monitored externally and people are comingback a year later to measure change - that definitelyhelps move things along.
Unit 3Midwife(interview)
“”“
”
NICE WORKS - Maternity Engagement Project final report74
Process learning
The re-audit was too soon for us really. It was 12months since the initial audit but only a maximum of6 months since we had had the opportunity to startto implement changes. A bigger window between theaudits would have given a better demonstration ofthe changes we've implemented.
Unit 2Midwife Songrapher(survey)
”“
This feedback from the units wasstrongly echoed by the Tambamidwifery consultants, one felt that
the 12-month period should startfrom delivery of the action planrather than the initial audit.
“”7.4.2 Provide multi-disciplinary support
The support provided by Tamba tounits for implementation was givenby specialist midwives. Some unitssuggested that it would have been
useful to have also had obstetricianand sonographer involvement inthe support package.
Professionals listen to experts in their own profession[Involving others in the support] would add moreweight and may be better valued. It is supposed to bea multi-disciplinary approach. The review wasmidwifery lead, but the plan is an MDT plan, itaddresses MDT issues.
“”
Unit 3Midwife(interview)
We gave the units a year to make the changes, but weweren't giving them the action plan until 3-4 weeks afterwe'd been in - if we were lucky, as it took a long time toensure everyone could make the conference call.They had less than a year.
TambaMidwiferyConsultant 2

NICE WORKS - Maternity Engagement Project final report 75
Process learning
7.4.3 Provide more opportunities for sharing between unitsPeer learning is greatly valued byrespondents and several wouldhave welcomed moreopportunities to share experiences,
information and best practice -potentially building a community ofmultiple midwives.
7.4.4 Link with other bodies and initiativesSome respondents felt that Tambaneeded to align itself to influentialbodies such as Local Maternity
Systems and ClinicalCommissioning Groups in order toeffect change.
It wouldencouragematernity unitsto engage ifthe LMS andCCG aremonitoringtheir success.
Unit 3Midwife(survey)
“”
Tamba need to engage with the MaternityTransformation Programme - especially the safetyworkstream. It is important if they want to continuethis work. The main one would be Maternal andNeonatal health safety collaborative - this is inline with their work.
“”Steering Group
Member 3
Another opportunity would be towork with Maternity Champions. Aspart of Safer Maternity Care (2016)The Department of Health andSocial Care's action plan formaking NHS maternity servicessome of the safest in the world,Maternity Clinical Networks wereasked to designate a MaternitySafety Champion as the local
quality improvement adviser,coach and conduit for sharinglearning from national andinternational research and fromlocal investigations or initiatives.The role also includes fosteringrelationships between MaternityClinical Networks and NeonatalOperational Delivery Networks.(55)
7.4.5 Develop the way the project is measuredAs well as having a later re-audit(see 7.3.1), units made othersuggestions to develop theproject's measurement processfurther:
■ Consider capturing electivecaesarean sections as well asemergency ones - as reducing
the elective rate would be auseful target.
■ Focus on preventable stillbirthsand neonatal deaths as theseare where the greatest benefitswill arise from improving care.Definitions would need to beagreed as to what wouldconstitute a preventable death.
NICE WORKS - Maternity Engagement Project final report76
7.4.5 Develop the way the project is measured
Process learning
(continued)
The midwifery consultants andSteering Group members alsosuggested:
■ Auditing more than ten patientfiles - or the number of filesaudited being proportionate tothe size of the unit. This wouldrequire more audit time and,therefore, resource.
■ Having clearer definitions ofwhat competencies are requiredfrom someone to be considereda "specialist".
■ Focusing on the NationalMaternity Safety AmbitionOutcomes - a national ambitionto reduce pre-term births.(56)
■ Capturing the demographicprofile of a hospital's catchmentarea - to analyse factors such asrural or urban settings, or levels ofdeprivation.
In addition to these suggestions,Fiveways who conducted theexternal evaluation
recommended:
■ Reviewing whether it is possibleto have a control/comparisongroup that has not had a similarintervention.
■ Developing a scale that can beused to measure "distancetravelled" in terms of key actionsrequired to increase adherence.Progress along this scale can bemeasured at audit, re-audit andduring quarterly update calls. Anexample of a six-point scalemight be (1) "Not present", (2)"Present but not optimum", (3)"Changes accepted", (4)"Changes planned", (5)"Changes made - not optimum",(6) "Present".
■ Introducing metrics to captureunit engagement. This could alsobe a scale or proxies could bedeveloped such as attendanceat training, use of the CPD areaor participation in quarterlyreview calls.
8 Conclusion andrecommendations
NICE WORKS - Maternity Engagement Project final report78
Conclusion and recommendations
A s can be seen from theresults above, the MaternityEngagement Project has
successfully demonstrated thatactions taken to improve carepractice for multiple pregnancieslead to improved adherence toNICE QS46, improved patientoutcomes for neonatal admissionsand emergency caesareansections, and an associated costsaving for units.
All 27 participating units increasedtheir overall NICE QS46 adherence,and across all units this increasewas statistically significant. Unitsthat implemented a higherproportion of the actions toimprove working practiceidentified by Tamba tended to seea greater increase in their overalladherence to NICE QS46.
Six individual units (of 25 withcomplete data) saw statisticallysignificant reductions in one ormore patient outcomes.
Across all sites, statisticallysignificant links were establishedbetween increased adherence toNICE QS46 statement five(monitoring for fetal complications)and decreased neonataladmissions, and increasedadherence to NICE QS46statement two (positional labelling)and decreased emergencycaesarean sections.
If all units in England implementedsimilar changes to increaseadherence in NICE QS46, within ayear neonatal admissions could bereduced by 1,308 with a costsaving of £8 million and emergencycaesarean sections could bereduced by 634.
These results were achieved in just12 months - it is likely that theassociation between improvedadherence and improvedoutcomes will become moreapparent if measured over a
longer period, and that decreasesin stillbirths and neonatal deaths willbe noticed (as in the St George'sexperience).
Importantly, participating units feltsupported to make the changes byTamba's expert advice and thecharity's role as an "external"auditor. Many of the changesrecommended and made did notrequire increased financialresources, rather a commitment toreview care planning and ensureexisting working practices wereimplemented consistently.
In addition to changes directlyrelated to practice change - unitsreported the project had helped toraise the profile and understandingof multiple pregnancy care, andthat it had promptedimprovements in continuity of carerand teamwork within their unit.
These findings will be of interest toindividual hospitals and maternityteams looking to implement NHSEngland's Saving Babies Lives CareBundle which explicitlyrecommends using the NICEguidance for multiple pregnancies.Furthermore, the CQC's hospitalinspection framework checkswhether units are delivering carefor multiple pregnancies inaccordance with this guidance. Asa result of what this project hasachieved in just 12 months, thefollowing recommendations aremade for a range of stakeholders:
NICE WORKS - Maternity Engagement Project final report 79
Conclusion and recommendations
Health Professionals■ Work alongside the maternity safety
champions in your trust to identifychanges required to improve the care ofmultiple pregnancies.
■ Contact Tamba now for resources andpractical support. We can help developan action plan and provide practicalhelp to drive change within yourhospital.
NHS England■ Raise awareness amongst Local
Maternity Systems that this project is akey contributor to meeting theAmbition, especially improvements incontinuity of carer among a vulnerablegroup, as set out in the Long-Term Plan.
■ Ensure that Local Maternity Systems areaware that twin and triplet pregnanciescontinue to be explicitly recognised incommissioning frameworks, tariffrequirements, and care bundles.
NHS Improvement■ Share the results of this project across
maternity safety champions and ensureit is understood that this project is a keycontributor to meeting the Better Birthsambition, especially improvements incontinuity of carer among a vulnerablegroup, as set out in the Long-Term Plan.
NHS Resolution■ Check that trusts applying for the
Maternity Incentive Scheme understandthat in order to meet the twin specificrequirements of Element Two (riskassessment, prevention and
surveillance of pregnancies at risk offetal growth restriction) of the SavingBabies Lives Care Bundle (2019), theyneed to implement the standards setout in NICE QS46 or a local variation,and that Tamba can support them to dothat.
Care Quality Commission■ Ensure the inspection framework for
antenatal care continues to focus oncare for multiple pregnancies beingprovided in line with NICE QS46.
■ Check feedback to trusts highlights theTamba resources and support that areavailable to help them makeimprovements to their care practicewhere appropriate.
Health Education England■ Provide CPD opportunities for teams to
improve their skills and knowledgeavailable in the care of multiplepregnancies.
The Department of Health andSocial Care■ Ensure the Maternity Engagement
Project receives ongoing support bothto reach new units and to monitoroutcomes achieved by participatingunits over a longer period.
■ Acknowledge that the MaternityEngagement Project is a key contributorto achieving the Better Births ambition,especially improvements in continuityof carer among a vulnerable group, asset out in the Long-Term Plan.
NICE worksReferences
NICE WORKS - Maternity Engagement Project final report 81
References
1. MBRRACE-UK - UK Perinatal Deaths for Births fromJanuary to December 2016) www.npeu.ox.ac.uk/downloads/files/mbrrace-uk/reports/MBRRACE-UK%20Perinatal%20Surveillance%20Full%20Report%20for%202016%20-%20June%202018.pdf
2. Visintin, C., Mugglestone, M. A., James, D., Kilby,M. D., & Guideline Development, G. (2011).Antenatal care for twin and triplet pregnancies:summary of NICE guidance. BMJ, 343, d5714.doi:10.1136/bmj.d5714
3. NICE Excellence (2013). Multiple pregnancy:twin and triplet pregnancies. Seewww.nice.org.uk/guidance/qs46
4. See www.npeu.ox.ac.uk/downloads/files/mbrrace-uk/reports/MBRRACE-UK%20Perinatal%20Surveillance%20Full%20Report%20for%202016%20-%20June%202018.pdf
5. www.sciencedirect.com/science/article/pii/S0002937816308687
6. MBRRACE-UK - UK Perinatal Deaths for Births fromJanuary to December 2016) www.npeu.ox.ac.uk/downloads/files/mbrrace-uk/reports/MBRRACE-UK%20Perinatal%20Surveillance%20Full%20Report%20for%202016%20-%20June%202018.pdf
7. Chauhan, S. P., Scardo, J. A., Hayes, E.,Abuhamad, A. Z., & Berghella, V. (2010). Twins:prevalence, problems, and preterm births. Am JObstet Gynecol, 203(4), 305-315.doi:10.1016/j.ajog.2010.04.031
8. See www.cerebralpalsyguidance.com/cerebral-palsy/risk-factors/multiple-births/ citesresearch that found that there were 2.3incidents of cerebral palsy per 1,000 singletonbirths, 12.6 per 1,000 in twins, and 44.8 per 1,000in triplets.
9. Visintin, C., Mugglestone, M. A., James, D., Kilby,M. D., & Guideline Development, G. (2011).Antenatal care for twin and triplet pregnancies:summary of NICE guidance. BMJ, 343, d5714.doi:10.1136/bmj.d5714
10. NICE Excellence (2013). Multiple pregnancy:twin and triplet pregnancies. Seewww.nice.org.uk/guidance/qs46
11. Antoniou, E., McCarthy, A., Turier, H., Roberts, N.,& Reed, K. (2017). Twin pregnancy andneonatal care in England. Retrieved from:www.tamba.org.uk/document.doc?id=903
12. Draper E.S., Kurinczuk, J., Kenyon S, on behalf ofMBRRACE-UK (2017). Term, singleton,intrapartum stillbirth and intrapartum-relatedneonatal death. Centre for Medicine,Department of Health Sciences, University ofLeicester: Leicester.
13. See Ham, C., Berwick, D., & Dixon, J. (2016).Improving quality in the English NHS: A strategyfor action. Retrieved from www.kingsfund.org.uk/units/default/files/field/field_publication_file/Improvingquality-Kings-Fund-February-2016.pdf andLeatherman, S., & Sutherland, K. (2008). Thequest for quality in the NHS: refining the NHSreforms. Retrieved from www.nuffieldtrust.org.uk/research/the-quest-for-quality-in-the-nhs-refining-the-nhs-reforms
14. Draper E.S., Kurinczuk, J., Kenyon S, on behalf ofMBRRACE-UK (2017). Term, singleton,intrapartum stillbirth and intrapartum-relatedneonatal death. Centre for Medicine,Department of Health Sciences, University ofLeicester: Leicester.
15. Statement six which recommends referrals and /or consultation with tertiary level provider wasexcluded from the project as this referral wasoften not required.
16. The Caldicott Principles were developed in 1997following a review of how patient informationwas handled across the NHS. They set out sixPrinciples that organisations should follow toensure that information that can identify apatient is protected and only used when it isappropriate to do so.
17. NICE do not define what a "specialist" is. Forspecialist midwives the project developed a jobdescription to clarify the role however the issueof defining specialist sonographers wasproblematic. Some units stated that allsonographers were specialists in multiples -defining specialism by what you do (i.e. theysee multiple pregnancies so therefore they arespecialists) rather than any qualification orexpertise. In such cases, Tamba midwiferyconsultants needed to probe further todetermine what sonographers might do incertain situations to define their level ofspecialism. Following this some trusts were opento change their stance, but others were not.
18. The use of multiple growth charts does notappear in NICE guidance; however, they werea resource some units introduced during theproject. Previously, units may have measuredtwin babies using singleton growth charts, withclinicians using their judgement to decide howthe babies were progressing. However, twins arenormally smaller than singletons so comparingthem to singleton growth charts could meanthat decisions were made to deliver twins earlierthan necessary (assuming they weren't growingsufficiently), increasing the risk and sometimescausing harm.
NICE WORKS - Maternity Engagement Project final report82
19. From January 2017 to February 2019, 1022professionals in total (from all units) have signedup to this resource.
20. MBRRACE-UK (Mothers and Babies: ReducingRisk through Audits and Confidential Enquiries inthe UK) is a collaboration led from the NationalPerinatal Epidemiology Unit (NPEU) at theUniversity of Oxford. The aim of MBRRACE-UK isto provide robust information to support thedelivery of safe, equitable, high quality, patient-centred maternal, newborn and infant healthservices.
21. Groupings are referred to it the MBRRACEPerinatal Mortality surveillance report publishedJune 2018 www.npeu.ox.ac.uk/downloads/files/mbrrace-uk/reports/MBRRACE-UK%20Perinatal%20Surveillance%20Full%20Report%20for%202016%20-%20June%202018.pdf pages16,17.
22. One test unit in group two subsequentlywithdrew from the project. The statistics in thisreport are therefore calculated for 27 test units.
23. Results for groups four and five are combined inthe analysis below.
24. Two units from group five were included toinvolve the Dorset Local Maternity System - theirresults have been combined with the group fourunits.
25. Patient safety incidents and patient satisfactionwere originally included as measurable patientoutcomes. However, this information was nottypically broken down between multiples andsingletons, so it was subsequently excluded fromthe project's analysis.
26. See www.tamba.org.uk/document.doc?id=985
27. See www.nice.org.uk/guidance/cg129/resources/endorsed-resource-multiple-antenatal-care-pathway-4844249677
28. Areas may have been assessed as being"improved" where the existing practice wasadapted to more closely meet the NICEguidelines or was implemented moreconsistently. This might be someone whopreviously had an interest in multiples beinggiven a named specialist role or ensuring coverfor times when specialists were on leave orabsent.
29. Results for one unit that took action onmonochorionic births only have been excludedfrom this table
30. Results for one unit that took action onmonochorionic births only have been excludedfrom this table
31. Results for one unit that took action onmonochorionic births only have been excludedfrom this table
32. See www.england.nhs.uk/wp-content/uploads/2017/12/implementing-better-births.pdf
33. Identification and monitoring of fetal growthrestriction, specifically implementing the use ofthe Growth Assessment Programme (GAP) is acomponent of Saving Babies Lives, NHS England'sstillbirth "care bundle" (2016) that confirmed bestpractice to reduce stillbirth rates. However, GAPis not recommended for multiple pregnancies.See Tamba - "Reducing Stillbirths in MultiplePregnancies and the NHS Stillbirth 'Care Bundle'"www.tamba.org.uk/document.doc?id=738
34. See www.england.nhs.uk/wp-content/uploads/2017/12/implementing-better-births.pdf
35. See www.england.nhs.uk/wp-content/uploads/2016/03/saving-babies-lives-car-bundl.pdf
36. See https://improvement.nhs.uk/documents/1044/ 2017-18_and_2018-19_National_Tariff_Payment_System.pdf
37. Overall adherence is an average of the levels ofadherence to each of the seven NICEQS46statements measured.
38. The unit "%p" is used for "percentage points"
39. i.e. graded A and B (see section 4.1)
40. i.e. graded D and E (see section 4.1)
41. The two exemplar units that conducted theiraudits independently were excluded from thisanalysis (see 3.2.4)
42. The "r" value is the coefficient of correlation - thismeasures the linear relationship (correlation)between a dependent-variable and anindependent variable. It's value varies between-1 and 1 : 1 means perfect correlation, 0 meansno correlation, positive values means therelationship is positive (when one goes up sodoes the other), negative values mean therelationship is negative (when one goes up theother goes down).
43. Uniform reduction of 70% across all units is basedon the assumption that all units have the samestarting point. MBRRACE report -www.npeu.ox.ac.uk/ downloads/files/mbrrace-uk/reports/MBRRACE-UK%20Perinatal%20Surveillance%20Full%20Report%20for%202016%20-%20June%202018.pdf. Stillbirth figure forsingletons in 2016 is 3.86 and 6.16 for twins.Calculation based on 30% giving a value:6.16*0.3 = 1.848 (or 1.85 rounded)
References
NICE WORKS - Maternity Engagement Project final report 83
44. All national averages quoted in this section arefrom the National Neonatal Research Database(NRNRD) 2014
45. The "r" value is the coefficient of correlation - thismeasures the linear relationship (correlation)between a dependent-variable and anindependent variable. It's value varies between-1 and 1 : 1 means perfect correlation, 0 meansno correlation, positive values means therelationship is positive (when one goes up sodoes the other), negative values mean therelationship is negative (when one goes up theother goes down). Read more:www.businessdictionary.com/definition/coefficient-of-correlation-r.html
46. Larger tertiary units receive the most seriouscases, and this will reflect in their patientoutcomes.
47. Four test units did not supply complete data.
48. Data were only available for 2014 and 2016. Forconsistency with the national averagespreviously discussed with the units andpresented in the project's interim report, 2014data were used for comparison with the re-auditresults in the project.
49. The analysis revealed that units with a highpatient outcome figure at baseline have, onaverage, a larger decrease in that outcomefrom baseline to re-audit. This is because thoseunits with a higher baseline rate have the
greater potential for a decrease in theoutcome. The results from the statisticalmodelling have accounted for these baselineeffects.
50. Two units in group 3 did not submit patientoutcome data at re-audit.
51. Data were only available for 2014 and 2016. Forconsistency with the national averagespreviously discussed with the units andpresented in the project's interim report, 2014data were used for comparison with the re-auditresults in the project.
52. Grimsby (Group 3), and Scunthorpe (Group 3)were excluded from this model as they had nooutcome data, along with Southampton (Group1) (see note above). Luton (Group 2) was alsoexcluded from this model as it was outlying interms of its change in emergency C-sectionrate, which negatively affected the model fit.
53. The number of responses to the relevantquestion is shown in brackets. This number canalter from question to question.
54. Answer options also included "neither agree nordisagree" or "I don't know".
55. See https://improvement.nhs.uk/resources/maternity-safety-champions/
56. These were launched after the MaternityEngagement Project had started.
References
Thanks to all the Tamba staff whohave worked on the project andthe final report:■ Jane Gorringe
■ Deborah Dillon
■ Jade Buckland
■ Amy McCarthy
■ Keith Reed
■ Helen Turier
■ Nikki Roberts
■ Alyson Chorley
■ Nicky Deans
■ Tanya Darlow
Tamba, Manor House, Church Hill, Aldershot, Hants, GU12 4JUwww.tamba.org.uk
Twinline - freephone helpline0800 138 0509 (10am-1pm and 7pm-10pm seven days a week)
Registered Company Number: 3688825 | Registered Charity Numbers: 1076478 and SC041055