NHSCT/18/1210 National Early Warning Score (NEWS)
37
National Early Warning Score (NEWS) Version 3_0 Page 1 of 11 This is an official Northern Trust policy and should not be edited in any way Please note that the policy library on Staffnet will contain the most up to date version of Trust policies Reference No: NHSCT/18/1210 Title: National Early Warning Score (NEWS) Key words within policy (max 10 words): National early warning scores, NEWS, charts, observations, SBAR communication tool Policy Author(s): Padraig Dougan, Resuscitation Officer; and Suzanne Pullins, Assistant Director of Nursing Safety, Quality and User Experience Responsible Director: Mr Seamus O’Reilly, Executive Director of Medicine Policy Type: Trust Wide Division Specific Clinical and/or social care Policy Replacement: Yes No National Early Warning Score (NEWS) to include Obstetric Early Warning Score (OEWS) NHSCT/14/782 Directors/Divisions policy to be issued to: Nursing Medicine Finance Medicine and Emergency Medicine Human Resources, Organisational Development and Corporate Communications Community Care Surgical and Clinical Services Mental Health, Learning Disability and Community Wellbeing Women, Children and Families Strategic Development and Business Services Target Audience, ie, specific staff groups: Health care professionals in Acute clinical facilities Approved by: Dr Kate Scott and Mrs Suzanne Pullins Co-chairs, Clinical and Social Care Policy and Guidelines Committee 9 July 2018 Operational Date: 1 August 2018 Review Date: January 2019 (or sooner if required due to regional implementation of NEWS2 by March 2019) Policy Library Categories: (Please tick as appropriate) No more than 3 categories to be selected Clinical and Social Care - Hospital (incl Comm Hosp) Clinical and Social Care - Children’s Hospital & Community Clinical and Social Care - Community Clinical and Social Care - Mental Health and/or Learning Disability Children’s Nursing Estates Maternity & Gynae Human Resources Health & Safety Major Incident Plan Palliative Care Information Management Infection Control Allied Health Professions Family Planning Trust Wide Finance Safeguarding Children NHSCT Vision To deliver excellent integrated services in partnership with our community.
Transcript of NHSCT/18/1210 National Early Warning Score (NEWS)
National Early Warning Score (NEWS) Version 3_0 Page 1 of 11
This is an official Northern Trust policy and should not be edited in any way
Please note that the policy library on Staffnet will contain the most up to date version of Trust policies
Reference No: NHSCT/18/1210 Title: National Early Warning Score (NEWS) Key words within
policy (max 10 words):
National early warning scores, NEWS, charts, observations, SBAR
communication tool
Policy Author(s): Padraig Dougan, Resuscitation Officer; and Suzanne Pullins, Assistant Director of Nursing Safety, Quality and User Experience
Responsible Director: Mr Seamus O’Reilly, Executive Director of Medicine
Policy Type: Trust Wide ☒ Division Specific ☐ Clinical and/or social care ☒
Policy Replacement: Yes ☒ No ☐ National Early Warning Score (NEWS) to include Obstetric Early
Warning Score (OEWS) NHSCT/14/782
Directors/Divisions
policy to be issued to:
Nursing ☒
Medicine ☒
Finance ☐
Medicine and Emergency Medicine ☒
Human Resources, Organisational Development and Corporate
Communications
☐
Community Care ☒
Surgical and Clinical Services ☒
Mental Health, Learning Disability and Community Wellbeing ☒
Women, Children and Families ☒
Strategic Development and Business Services ☐
Target Audience, ie,
specific staff groups:
Health care professionals in Acute clinical facilities
Approved by: Dr Kate Scott and Mrs Suzanne Pullins Co-chairs, Clinical and Social Care Policy and
Guidelines Committee
9 July 2018
Operational Date: 1 August 2018 Review
Date:
January 2019 (or sooner if required due to
regional implementation of NEWS2 by March 2019)
Policy Library
Categories:
(Please tick as
appropriate)
No more than 3
categories to be
selected
Clinical and Social Care - Hospital (incl Comm Hosp) ☒
Clinical and Social Care - Children’s Hospital & Community ☐
Clinical and Social Care - Community ☐
Clinical and Social Care - Mental Health and/or Learning Disability ☒
Children’s Nursing ☐ Estates ☐
Maternity & Gynae ☐ Human Resources ☐
Health & Safety ☐ Major Incident Plan ☐
Palliative Care ☐ Information Management ☐
Infection Control ☐ Allied Health Professions ☐
Family Planning ☐ Trust Wide ☒
Finance ☐
Safeguarding Children ☐
NHSCT Vision
To deliver excellent integrated services in partnership with our community.
National Early Warning Score (NEWS) Version 3_0 Page 2 of 11
National Early Warning Score (NEWS)
Contents
1.0 Summary of Policy …………………………………………………………….. 3
2.0 Responsibilities ………………………………………………………………… 4
3.0 Policy Statement ……………………………………………………………….. 5
4.0 Monitoring ……………………………………………………………………….. 6
5.0 Evidence Base/References …………………………………………………… 7
6.0 Personal & Public Involvement (PPI)/Consultation Process …………… 7
7.0 Equality, Human Rights & DDA ……………………………………………… 7
8.0 Alternative Formats ……………………………………………………………. 7
9.0 Sources of advice in relation to this document …………………………... 8
10.0 Policy Sign Off …………………………………………………………………... 8
11.0 Appendix 1 Protocol for Senior Nursing Assistants………………… 9-10
Appendix 2 SBAR Communication Tool .……………………………. 11
National Early Warning Score (NEWS) Version 3_0 Page 3 of 11
1.0 Summary of Policy / Background
1.1 In Northern Ireland, the use of Physiological Early Warning Scoring
Systems (PEWS) in the Health and Personal Social Services (HPSS)
was recommended following the Regulation and Quality Improvement
Authority (RQIA) Report “Review of the Lessons Arising from the Death
of the Late Mrs Janine Murtagh”, October 2005. The Report
recommended that PEWS is used for every patient in all acute
hospitals, as there was a need to provide clinical teams with
formalised protocols and guidance to support critically ill patients.
1.2 The NHSCT on recommendation of the HSC Safety Forum adopted
the National Early Warning Score (NEWS) in August 2013, which was
to replace PEWS observation charts for Adults.
1.3 The NHSCT on recommendation of the HSC Safety Forum adopted
the Regional Obstetric Early Warning Score Chart (OEWS) in
November 2013. The Trust’s OEWS Policy is available in the Trust
Policy Library on Staffnet. OEWS are to be completed on all pregnant
women from 12+0 weeks gestation.
1.4 The NHSCT on recommendation of the HSC Safety Forum has from
September 2015 introduced the Paediatric Early Warning Score which
covers all age groups of children up to and including the age of 16
which is addressed in the Paediatric Early Warning Score (PEWS)
and Paediatric Inpatient Observation Policy (available in the Trust
Policy Library on Staffnet).
1.5 NEWS should be used for all patients in hospital from their 16th
birthday (except for all pregnant women from 12+0 weeks gestation) to
assist in tracking their clinical condition and to ensure that the clinical
team can be appropriately alerted to any clinical deterioration so that a
timely clinical response can be triggered.
1.6 NEWS is based on a simple scoring system in which a score is
allocated to physiological measurements already undertaken when
patients present to, or are being monitored in hospital.
Six simple physiological parameters form the basis of the scoring
system.
1. Respiratory Rate
2. Oxygen Saturations
3. Temperature
National Early Warning Score (NEWS) Version 3_0 Page 4 of 11
4. Systolic Blood Pressure
5. Pulse rate
6. Level of Consciousness (AVPU)
A score is allocated to each as they are measured , the magnitude of
the score reflecting how extreme the parameter varies from the norm.
The score is then aggregated, and uplifted for people requiring oxygen.
It is important to emphasize that all parameters must be routinely
measured in hospitals and recorded on the NEWS Observation chart.
2.0 Responsibilities
2.1 Directors are accountable for ensuring that NEWS is implemented and
used effectively in conjunction with Clinical Response Triggers/Action
Protocols within inpatient areas across their Division.
2.1.1 Directors are responsible for ensuring that systems are in place
to provide training for staff on NEWS as appropriate.
2.1.2 Each Division must ensure that a minimum of 10 NEWS charts
are audited per adult inpatient ward per month. The expected
Standard to be achieved is 100% compliance on the identified
parameters in the use of NEWS.
2.2 Healthcare staff are individually accountable for their practice and for
the provision of appropriate care. The Registered Nurse responsible for
the patient remains responsible for the appropriate delegation of NEWS
observations to Health Care Assistants and must adhere to the NMC
guidance on the delegation of care (NMC,2015).
2.2.1 Education and Training on the use of the NEWS system must
be completed annually by all staff using the e-learning
programme found at the web-site below:
https://tfinews.ocbmedia.com/
2.2.2 Bank staff working in the Trust will access mandatory training
through the Trust, in the same way as substantive staff, and
contract agency staff are required to be trained as well but that
at an operational level it is the shift coordinators responsibility
to ensure all staff have the skill set required to care for patients.
National Early Warning Score (NEWS) Version 3_0 Page 5 of 11
2.2.3 Health Care Assistants (Band 3) who have been nominated
and authorized to undertake NEWS observations must prove
that they have successfully undertaken the Vital Signs-
Undertaking and Recording (CEC) course and successfully
completed their record of supervision sessions (see Appendix
1). In addition they must also complete the NEWS e-learning
programme before undertaking the recording of Clinical
observations. Note e-learning web site above.
2.2.4 Health Care Assistants must submit their certificate of
completion and record of supervised sessions to the Ward
Sister/Charge Nurse and the date completed recorded in the
Health Care Assistants’ training records.
3.0 Policy Statement
3.1 This policy sets out the standards for recording and scoring clinical
observations for adult inpatients from their 16th birthday in clinical
facilities (except within maternity) across the Northern Health and
Social Care Trust.
3.2 Only NEWS charts approved by the Trust should be used.
3.3 All healthcare professionals using NEWS must ensure compliance with
the following actions:
• All adult inpatients in the Acute setting MUST have as a minimum
one set of NEWS observations carried out in each 12 hour period.
• All 6 scored observations MUST be accurately measured and
recorded on the chart at each intervention, dated and signed
• The score for each set of observations MUST be calculated and
charted and review time stipulated on the chart.
• Act on the observations and scores based on the Clinical Response
Triggers/Action Protocols, which may include contacting Medical
staff or the Hospital at Night Team as appropriate.
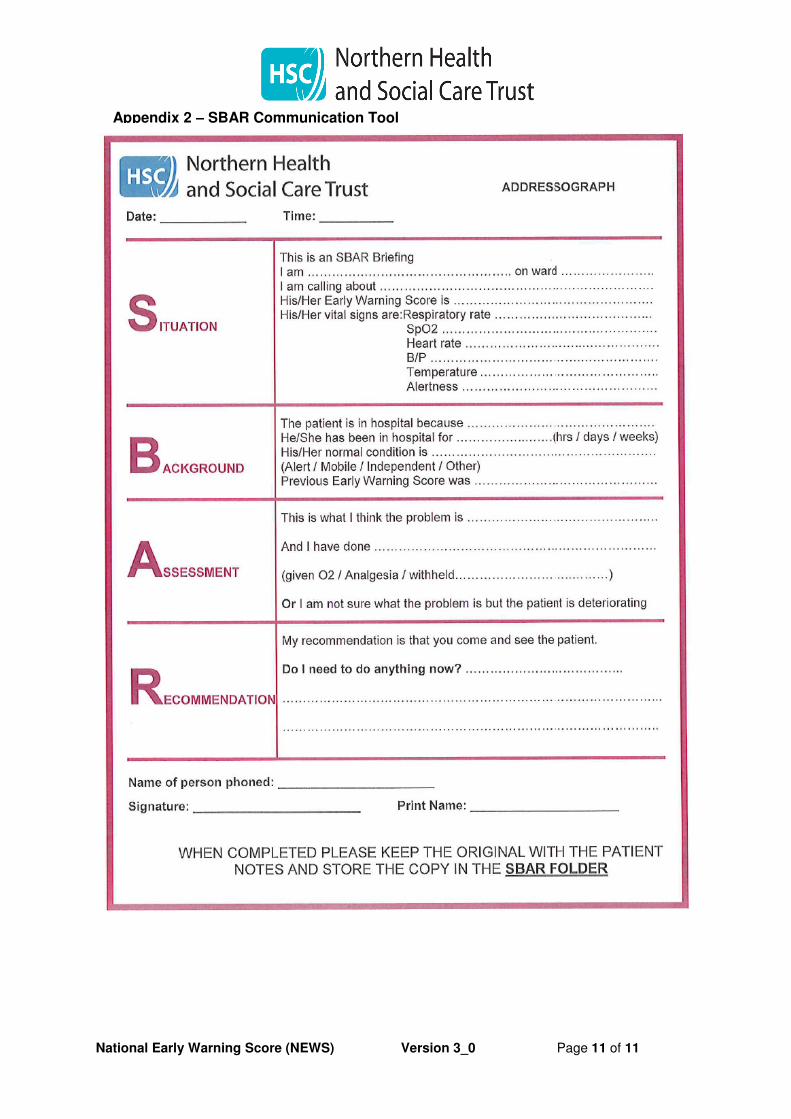
• The Situation, Background, Assessment, Recommendation (SBAR)
communication tool should be used as per clinical response action
protocol
• Frequency of observations will be determined by current NEWS
score, patient diagnosis, current condition, previous scores or any
agreed clinical decision to change frequency made by (ST3 level
Doctor or above) which has been documented in patients’ clinical
notes

National Early Warning Score (NEWS) Version 3_0 Page 6 of 11
• Concern about a patient’s clinical condition should always override
the NEWS if the attending healthcare professional considers it
necessary to escalate care
• Any decision to deviate from the Trust escalation protocol must be
documented alongside the patient response and rationale
• When clinical teams (ST3 and above) decide that the routine
recording of data for NEWS is inappropriate, such decisions should
be discussed with the patient and recorded in the clinical notes
3.4 Settings outside the Acute Hospital
• All adult inpatients in the Mental Health setting will have a full set of
NEWS observations carried out on admission or following transfer
to be discussed at the earliest multidisciplinary meeting re:
continuation of NEWS observations
• All adult inpatients in the Community Hospital setting MUST have at
least one set of NEWS observations carried out in each 24 hour
period.
• When the decision is made to delegate the task of carrying out
NEWS observations the registrant must retain accountability.
4.0 Monitoring
4.1 Clinical Services Managers/General Managers/Heads of Service in
each Division will be responsible for ensuring that there is a plan to
audit the use of the NEWS systems in their area of responsibility on a
monthly basis. The plan should be approved by the Divisional
Governance Team.
4.2 Local audits of the use of NEWS will be undertaken on a monthly
basis on all ward areas.
4.3 The findings of these audits are reported to the Governance
Department and recorded on the Nursing Dashboard.
4.4 An annual NEWS audit is carried regionally in all Trusts, and the
findings reported to the Director of Nursing within the Trust and to the
Quality and Safety Forum.
4.5 Further Trust and regional audits will be carried out as agreed.
National Early Warning Score (NEWS) Version 3_0 Page 7 of 11
5.0 Evidence Base/References
5.1 National Early Warning Score (NEWS)
Standardising the assessment of acute-illness severity in the NHS
www.rcplondon.ac.uk/national-early-warning-score
5.2 “Review of the Lessons Arising from the Death of the Late Mrs Janine
Murtagh”, RQIA, October 2005.
https://rqia.org.uk/RQIA/files/4c/4caa7dda-4a33-4913-bea3-
c025824ae4e2.pdf
5.3 Nursing & Midwifery Council (2015) The Code Professional Standards
of Practice and Behaviour for Nurses and Midwives
5.4 Acutely ill adults in hospital recognising and responding to deterioration
NICE Clinical Guideline (CG 50)
https://www.nice.org.uk/guidance/CG50
6.0 Personal & Public Involvement (PPI)/Consultation Process
6.1 The Trust’s Resuscitation Officers, Assistant Director of Nursing and
User Experience, Medical Director and Clinical and Social Care
Governance Managers were involved in the creation of this document
following regional input from the Patient Safety Forum.
7.0 Equality, Human Rights & DDA
7.1 This policy has been drawn up and reviewed in the light of Section 75
of the Northern Ireland Act (1998) which requires the Trust to have due
regard to the need to promote equality of opportunity. It has been
screened to identify any adverse impact on the 9 equality categories.
7.2 The policy has been ‘screened out’ without mitigation or an alternative policy proposed to be adopted.
8.0 Alternative Formats
8.1 This document can be made available on request on disc, larger font,
Braille, audio-cassette and in other minority languages to meet the
needs of those who are not fluent in English.
National Early Warning Score (NEWS) Version 3_0 Page 8 of 11
9.0 Sources of advice in relation to this document
9.1 The Policy Author, responsible Assistant Director or Director as
detailed on the policy title page should be contacted with regard to any
queries on the content of this policy.
10.0 Policy Sign Off (Typed name/scanned signature sufficient)
Padraig Dougan
Resuscitation Officer
Lead Policy Author Date: 5 February 2018
Mr Seamus O’Reilly
Executive Director of Medicine Date: 16 February 2018
National Early Warning Score (NEWS) Version 3_0 Page 9 of 11
11.0 Appendix 1
Protocol for the Measurement and Recording of Physiological
Observations by nominated Health Care Assistants (Band 3)
This Appendix forms part of the NHSCT’s policy on National Early Warning Score
(NEWS) and specifically outline the delegated task undertaking the measurement,
recording and escalation of NEWS observations by nominated Health Care
Assistants (Band 3).
Each Division must ensure that the nominated and authorized Health Care
Assistants (Band 3) have received the specific training provided by CEC, supervision
and assessment regarding measurement and recording of NEWS observations.
Competence
All Health Care Assistants (Band 3) who undertake NEWS observations must prove
that they have successfully undertaken the Vital Signs – Undertaking and Recording
(CEC) course and successfully completed their record of supervision sessions and
complete the NEWS e-learning tool before undertaking and recording clinical
observations. The e-learning tool can be accessed at https://tfinews.ocbmedia.com/
When completed the certificate of completion and record of supervised sessions
must be submitted to the Ward/Department Manager and the date completed
recorded in the Health Care Assistant’s training records.
Reporting
The Registered Nurse responsible for the patient remains responsible for the
appropriate delegation of NEWS observations to Health Care Assistants and must
adhere to the NMC guidance on the delegation of care (NMC, 2015). Health Care
Assistants must follow Trust procedure regarding reporting and records of NEWS
observations.
Specific attention should be noted as follows:
• Health Care Assistants must be aware of their responsibilities in response to
any change in the patient’s condition and/or an abnormal earning warning
score. They must adhere to the processes for escalation in order to provide
safe and effective care for the patient.
• Health Care Assistants must document and inform the registered nurse who is
responsible for the patient of any NEWS 1-4.
National Early Warning Score (NEWS) Version 3_0 Page 10 of 11
• Health Care Assistants must document and immediately inform the
registered nurse who is responsible for the patient of any NEWS of 5 or above
or 3 in any single parameter.
Exclusions regarding the delegation of NEWS observations to Health Care
Assistants (band 3)
Health Care Assistants must not be delegated to record physiological observations
for the following patients:
• Patients on admission
• Patients requiring central neurological (CNS) observations
• Patients receiving any blood transfusions/products
• Patients who are unstable/clinically deteriorating
• Immediate post-operative patients. On-going assessment of the patient must
be carried out by the Registered Nurse. NEWS observations are only
delegated to the Health Care Assistant when the patient is assessed as stable
post operatively.
It should be noted that the Registered Nurse should not delegated the recording of
NEWS observations to a Health Care Assistant if the RN has any concerns
regarding the clinical status of the patient.
References
Nursing and Midwifery Council (2015). The Code. Professional Standards of
Practice and Behaviour for Nurses and Midwives.
Northern Health and Social Care Trust (2018). National Early Warning Score
(NEWS) available within the Policy Library on Staffnet
National Early Warning Score (NEWS) Version 3_0 Page 11 of 11
Appendix 2 – SBAR Communication Tool
This is an official Northern Trust policy and should not be edited in any way Please note that the policy library on Staffnet will contain the most up to date version of Trust policies Reference No: NHSCT/19/1335 Title: Rapid Tranquilisation Guidelines
Key words within policy (max 10 words):
Options for disturbed, violent behaviour in adult patients.
Policy Author(s): Dr U Huda, Divisional Medical Director Richard Bakasa, Acting Head of Acute Services (Mental Health) Dr A Collins, Consultant Psychiatrist Dr S McCann and Dr J McIlvenna, Psychiatrist of Old Age/Dementia Dr C O’Lynn, Speciality Doctor, PICU Joby Joseph, Charge Nurse Ms N Gribben, Clinical Pharmacist Dr M Bell & Dr M Jenkins, Antrim Area Hospital Emergency Department
Responsible Director: Mr Oscar Donnelly, Divisional Director of Mental Health, Learning Disability and Community Wellbeing Division
Policy Type: Trust Wide ☒ Division Specific ☐ Clinical and/or social care ☒
Policy Replacement: Yes ☒ No ☐ Replaces policy NHSCT/16/981- reviewed due to new clinical guidance and inclusion of other trust areas.
Directors/Divisions policy to be issued to:
Nursing and User Experience ☐ Medicine and Pharmacy ☒
Finance and Estate Services ☐
Medicine and Emergency Medicine ☒
Human Resources, Organisational Development & Corporate Comms ☐
Community Care ☐
Surgical and Clinical Services ☒
Mental Health, Learning Disability and Community Wellbeing ☒
Women, Children and Families ☒
Strategic Development and Business Services ☐
Target Audience, ie, specific staff groups:
This policy is directed to all staff within the Mental Health Division, the acute hospital setting including Emergency Departments and CAMHS medical staff
Approved by: Dr Kate Scott & Mrs Suzanne Pullins Co-chairs, Clinical and Social Care Policy and Guidelines Committee
30 September 2019
Operational Date: 31 October 2019 Review Date: December 2021 Policy Library Categories: (Please tick as appropriate) No more than 3 categories to be selected
Clinical and Social Care - Hospital (incl Comm Hosp) ☐
Clinical and Social Care - Children’s Hospital & Community ☐
Clinical and Social Care - Community ☐
Clinical and Social Care - Mental Health and/or Learning Disability ☒
Children’s Nursing ☐
Maternity & Gynae ☐ Estates ☐
Health & Safety ☐ Human Resources ☐
Palliative Care ☐ Major Incident Plan ☐
Infection Control ☐ Information Management ☐
Family Planning ☐ Allied Health Professions ☐
Finance ☐ Trust Wide ☒
Safeguarding Children ☐
Rapid Tranquilisation Guidelines Version 3_0 Page 1 of 25
Rapid Tranquilisation Guidelines Contents Page
1 Summary 2
2 Responsibilities 2
3 Policy Statement 3
3.1 The Definition and Background of the Policy 4 3.2 Medication in Acute Psychiatric Emergencies 5
General Prescribing Principles 3.3 Maximum Doses 6
3.4 Precautions to Rapid Tranquilisation 7 3.5 Cardiovascular Disease 7
3.6 Cardiovascular Safety 8 3.7 Drug Selection 9-12
- Adults over 18 years - Older People over 65 years - People with Dementia - Children and Young people under 18 years
3.8 Monitoring after Use of Intramuscular medication 12 3.9 Drugs not recommended Rapid Tranquillisation 12 3.10 Actions after Rapid Tranquillisation 13
4 Guidelines for the Acute Hospital Emergency Departments 13
5 Monitoring of policy 14
6 Evidence Base/References 14
7 Personal & Public Involvement(PPI)/Consultation Process 15
8 Equality, Human Rights and DDA 16
9 Alternative Formats 16
10 Sources of Advice in Relation to this Document 16
11 Policy Sign Off 16
12 Appendices/Attachments 17-25
NHSCT Vision To deliver excellent integrated services in partnership with our community.
Rapid Tranquilisation Guidelines Version 3_0 Page 2 of 25
Northern Trust and Social Care Trust Rapid Tranquilisation Guidelines
1.0 Summary of Policy
This Guideline document describes the recommended pharmacological
management options that may be used to manage disturbed and violent
behaviour in adult patients cared for in the Northern Health and Social Care
Trust. The physical observations and monitoring required after the use of
injectable medication are described.
It is expected that this Guideline will be used primarily in Mental Health settings
but it will be applicable for the acute management of known or apparently
disturbed mental states in other settings. In these situations, clinicians may
wish to seek further advice on management from a psychiatrist.
However, it is important to recognise that this is NOT applicable for the primary
management of acute alcohol withdrawal.
1.1 Purpose
To ensure a consistent approach to the Rapid Tranquillisation for violent and
aggressive behaviour in order to minimise risk.
1.2 Objectives
• To effectively manage violent and aggressive behaviour whilst
maintaining patient safety and minimising risk.
2.0 Responsibilities
Senior Management
• All Trust Directors, Assistant Directors, Service Heads and Senior
Managers have responsibility for the effective implementation of this
policy. They will ensure that actions are implemented and monitored
and that information required in relation to affecting this policy is
provided promptly and completely. Compliance with these guidelines
will be monitored by relevant senior and first line managers.
Rapid Tranquilisation Guidelines Version 3_0 Page 3 of 25
Clinical Team
• Junior doctors must not prescribe rapid tranquilisation to young
people under 18 years of age without advance consultation with a
senior doctor/consultant.
• All practitioners are responsible for ensuring that they have a working
knowledge of and adhere to the guidance of this policy. All Staff should
read and sign that they have understood the policy.
• Ensure adherence to appropriate policies and procedures throughout
the decision making process.
• To ensure a full explanation is given to the patient and appropriate carer
as to why the policy interventions are necessary. In line with The Quality
Standards for The Health and Personal Social Services (NI) the Trust
must provide effective leadership and clear direction to make the most
of its people, skills, time and money as to deliver safe, sustainable and
high quality services. The ability of the organisation to reach and
maintain this requirement will be dependent on effective supervision for
all grades of staff.
• Supervision is a shared responsibility between operational manager /
supervisor and staff member.
• All staff involved in the Rapid Tranquillisation of patients with disturbed
and violent behaviour must follow this guidance.
• Clinicians should use their own clinical judgement in each case and if
they decide that a different management approach is clinically indicated
then the reasons for this should be clearly documented.
3.0 Policy Statement
• Rapid Tranquillisation should be part of an overall management plan
that includes appropriate nursing care and de-escalation techniques
and should only be considered when de-escalation approaches have
failed.
• Patients should only be treated with the medicines described in this
guideline only after it is established that the risk of not doing so is
greater than the risk of rapid tranquillisation.
• This guideline applies to the management of acutely disturbed
behaviour and not to the management of delirium.
• Staff should be trained, to a level appropriate to their role, in how to
assess and manage potential and actual violence using de-escalation
Rapid Tranquilisation Guidelines Version 3_0 Page 4 of 25
techniques, restraint and the pharmacological treatment. Staff should
also be trained to use Intermediate Life Support.
• Staff should be trained to understand and apply the Mental Health
Order of Northern Ireland 1986 and have awareness of Human Rights
Act 1998 and Common Law.
• If the patient has expressed a preference for a particular antipsychotic in
an Advance Directive consider prescribing this, if appropriate to the
clinical circumstances.
• Before an intramuscular medication is administered, the patient must be
given the opportunity to take oral medication if it is thought this would be
effective and appropriate in the clinical circumstances.
• In all cases the likely minimum effective dose of medication should be
used.
• All staff need to be aware of the legal framework that authorises the use
of these interventions.
• Staff involved in rapid tranquillisation should be aware of the licensed
indications and maximum doses of medicines (see BNF or Summary of
Product Characteristics, SPC) and should endeavour to keep within
these limits. In some cases current BNF and SPC dose may be
knowingly exceeded (e.g. Lorazepam >4mg/day), bearing in mind the
overall risks. This decision should not be taken lightly or the risks
underestimated. Record a risk-benefit decision and rationale in the case
notes. Junior doctors must consult a more senior colleague in these
cases.
3.1 The Definition and Background of the Policy
The use of psychotropic medication in acute psychiatric emergencies is with
the aim of controlling agitation, aggression or excitement. As there are no
drugs that produce an immediate antipsychotic effect, the principal aim is
immediate sedation and tranquillisation – hence, this is often known as ‘rapid
tranquillisation’. Antipsychotic (neuroleptic) drugs can be used for this purpose
and may then be continued for their antipsychotic effect, which may take two
or three weeks to develop.
Rapid Tranquilisation Guidelines Version 3_0 Page 5 of 25
The use of antipsychotics in acute psychiatric emergencies has been linked to
sudden death, the cause of which is not entirely clear. During violent struggles
an injection may be inadvertently injected intravascularly or the normally
clinically insignificant prolongation of QTc interval associated with some
antipsychotics might be potentiated by the arrhythmogenic effect of
catecholamines released during violent struggles. Monitor closely when IM
antipsychotics have to be used in patients prescribed other medicines that
might prolong QTc interval.
3.2 Medication in Acute Psychiatric Emergencies
General Prescribing Principles
The aim of rapid tranquillisation is to achieve a state of calm sufficient to
minimise the risk posed to the patient and others. Patients should be able to
respond throughout. With this in mind, it is important to individualise the dose
and type of medication for each service user. This will depend on several
factors including previous response to medication, age, physical problems
(renal, hepatic, cardiovascular or neurological disease) other prescribed
medication and possible use of drugs of abuse.
• Check that the patient has not had previous allergy or severe
idiosyncratic reaction to the drugs to be used.
• Check there is no recent history of Neuroleptic Malignant Syndrome or
hyperthermia.
• Simultaneous administration of IM antipsychotics and IM
benzodiazepines (Lorazepam) may be associated with excessive
sedation and cardio respiratory depression. If this combination is
deemed necessary then patients must be monitored for excessive
sedation and for postural hypotension.
• Patients taking Clozapine or Olanzapine require care when giving
benzodiazepines especially via IM route as potentially fatal orthostatic
and cardio-respiratory dysregulation have been reported. If this
combination is considered necessary it is essential to undertake
frequent monitoring of the patient.
• If the patient has expressed a preference for a particular antipsychotic in
an Advance Decision consider prescribing this if warranted by clinical
circumstances.
Rapid Tranquilisation Guidelines Version 3_0 Page 6 of 25
• Avoid unnecessary polypharmacy. This may necessitate careful choice
of drug in relation to either current treatment or expected maintenance
treatment.
• Carefully consider the number of active PRN prescriptions operative at
any one time in relation to the risk of inadvertent overdose.
• The Multidisciplinary Team in Mental Health Settings should review
PRN medication at least once a week and if PRN medication is to be
continued the rationale for its continuation should be included in the
review. If psychotropic PRN medication has not been used since the
last review, consider stopping it.
• Be mindful that parenteral doses generally have a greater bioavailability
than oral doses.
• Don’t mix medications in the same syringe.
• Patients entering LEVEL 2 on the protocol (See Appendix 1+2) must
have details of all medicines administered, rationale of use and an
assessment of effectiveness recorded in the clinical notes. All current
psychotropic PRN prescriptions on the Kardex should be reviewed in 6-
12 hours.
3.3 Maximum Doses
Staff involved in rapid tranquillisation should be aware of the licensed
indications and maximum doses of medicines (see BNF or Summary of
Product Characteristics, SPC) and should endeavour to keep within these
limits. In some cases current BNF and SPC dose may be knowingly
exceeded (e.g. Lorazepam >4mg/day), bearing in mind the overall risks.
This decision should not be taken lightly or the risks underestimated.
Record a risk-benefit decision and rationale in the case notes. Junior
doctors must consult a more senior colleague in these cases. If BNF doses
are exceeded, it is particularly important to undertake frequent and
intensive monitoring of a calmed patient. Pay particular attention to regular
check of airway and intensive monitoring of level of consciousness, pulse,
blood pressure, respiratory effort, temperature and hydration. (Appendix 4).
Rapid Tranquilisation Guidelines Version 3_0 Page 7 of 25
3.4 Precautions to Rapid Tranquilisation
• Patients never previously prescribed antipsychotic medication
Use lower doses, (Appendix 1+2)
Avoid haloperidol if possible.
• Patients with no evidence of psychotic symptoms
Consideration should be given to dependency potential or potential for
misuse of PRN medication
Use lorazepam initially however promethazine may be preferable in
Benzodiazepine - tolerant patients (see below)
• Co-morbid Substance Misuse
In patients who are benzodiazepine-tolerant consider use of IM
promethazine 25-50mg (up to a maximum of 100mg/24hours). Wait 1-2
hours after injection to assess response. Note this is an unlicensed use.
Care should be exercised if methadone prescribed due to increased
potential for QTc prolongation.
• Frail/Elderly and patients with Dementia
Use lower doses. (Appendix 2)
Only use oral route except in very extreme emergencies.
• Organic Disease
Use lower doses.
In patients with suspected or confirmed Lewy Body Dementia or
Disease; avoid the use of antipsychotics.
3.5 Cardiovascular Disease
Avoid antipsychotics (or use of IM haloperidol with IM promethazine).
Use lorazepam alone.
Consider any concomitant medication, which may prolong QTc interval.
NB: Haloperidol is contra-indicated in clinically significant cardiac
disorders. A clinical risk assessment must be carried out before
prescribing haloperidol. The Summary of Product Characteristics
(SPC) for haloperidol recommends that a baseline ECG is performed
prior to treatment for all patients and also avoiding the use of
concomitant antipsychotics. This will not always be possible in an
acutely disturbed, psychotic patient. In such a situation, the
prescribing doctor will have to balance the cardiac risks against
those arising from the patient’s behaviour.
Rapid Tranquilisation Guidelines Version 3_0 Page 8 of 25
• Compromised respiratory function
Avoid benzodiazepines.
• Alcohol Withdrawal / Risk of Seizures
Caution when using antipsychotics – lowering of seizure threshold.
• Hepatic or renal impairment
Use lower doses – risk of accumulation due to reduced clearance.
• Pregnancy
Specialist advice must be sought on the management of pregnant
women requiring emergency sedation. The risks and benefits of
treatment should be considered on a case by case basis.
3.6 Cardiovascular Safety
Antipsychotics as a group are probably associated with an increased risk
of QTc prolongation. Normal limits of QTc are less than 440 ms in men and
less than 470 ms in women. The risk of arrhythmia increases exponentially
beyond normal limits, with strong evidence that QTc greater than 500 ms is
clearly linked to an increased risk of arrhythmia. The risk is dose related
and the risk for individual drugs is probably additive when they are used in
combination.
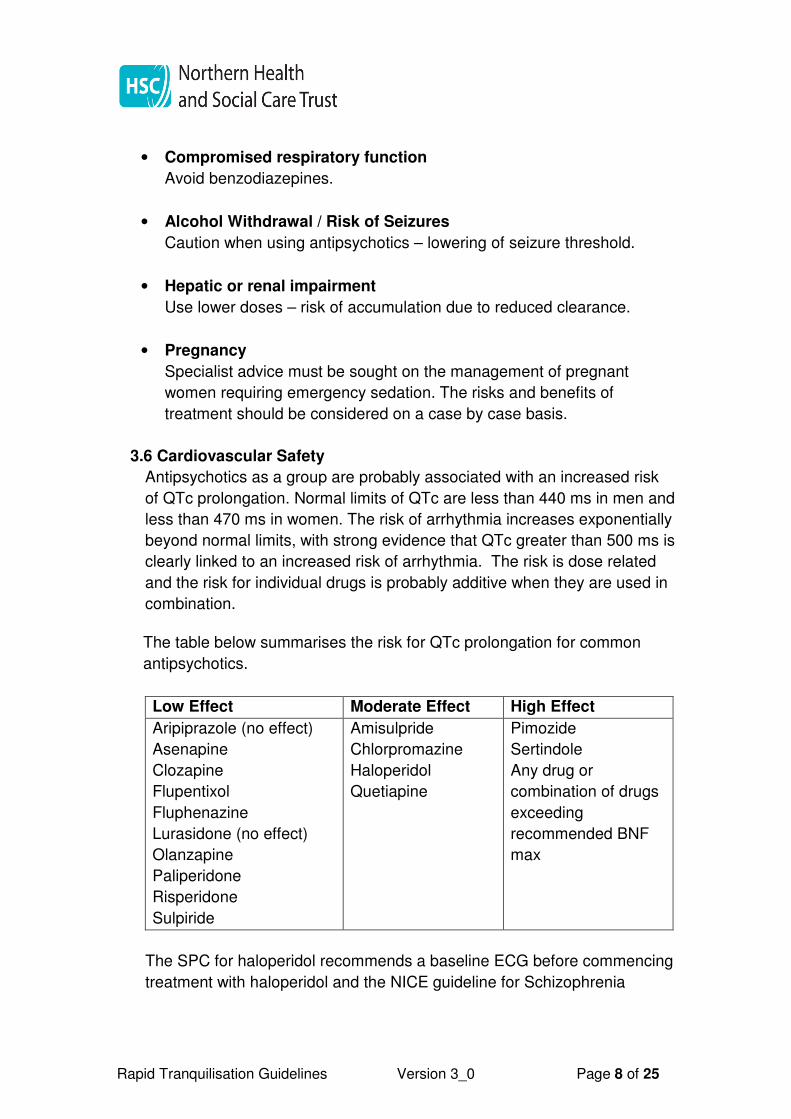
The table below summarises the risk for QTc prolongation for common
antipsychotics.
Low Effect Moderate Effect High Effect
Aripiprazole (no effect)
Asenapine
Clozapine
Flupentixol
Fluphenazine
Lurasidone (no effect)
Olanzapine
Paliperidone
Risperidone
Sulpiride
Amisulpride
Chlorpromazine
Haloperidol
Quetiapine
Pimozide
Sertindole
Any drug or
combination of drugs
exceeding
recommended BNF
max
The SPC for haloperidol recommends a baseline ECG before commencing
treatment with haloperidol and the NICE guideline for Schizophrenia
Rapid Tranquilisation Guidelines Version 3_0 Page 9 of 25
(CG82) recommends an ECG before starting an antipsychotic if a patient is
admitted as an inpatient.
A number of medications are associated with prolonged QTc including
amiodarone, erythromycin, clarithromycin, quinine, ciclosporin,
diphendyramine, methadone and tamoxifen. Diuretics can cause
electrolyte disturbance which is also a risk factor. Consult the BNF for
further examples of drugs that prolong QTc.
3.7 Drug Selection (See Appendix 7)
Appendix 7 contains a summary of recommended drugs, their onset of
action and doses for different age groups.
Olanzapine IM injection is not available to the UK market via UK licensing
process however products are available, centrally approved for use in EU
countries with an EU license number.
A benzodiazepine may be the safest and best tolerated drug with which to
effect ‘rapid tranquillisation’ of the patient. Once the patient has been
calmed, either by de-escalation techniques or by a benzodiazepine, an
antipsychotic drug may be best for maintenance of the situation.
Remember that repeated use of a benzodiazepine may result in tolerance
to the effect and this will probably become evident by 7 to 10 days.
For Adults Over 18 years (see Appendix 1)
The flow chart in Appendix 1 outlines a stepped approach to rapid
tranquillisation for Adults over 18 years of age.
If you are unsure about initial pharmacological management then always
call a more senior doctor. If you are a junior doctor and your initial drug
treatment does not work then you should consider discussion with
someone more senior. If you are a Consultant and have tried two or three
approaches without success then it may be wise to seek a second opinion
from a colleague. If the incident is outside a mental health unit, clinicians
may wish to consult a psychiatrist for further advice.
For Older People Over 65 years (see Appendix 2)
This guideline applies to the management of acutely disturbed behaviour
and not to the management of delirium.
Rapid Tranquilisation Guidelines Version 3_0 Page 10 of 25
There is evidence that antipsychotics are associated with increased
mortality (probably by increasing the risk of cerebrovascular adverse
events) even in people without dementia. A cautious approach is
recommended.
• Oral medication should always be offered whenever possible.
• Lorazepam, starting at a low dose, is the preferred first line treatment.
• If there is confirmed history of previous antipsychotic use then oral
Haloperidol or Olanzapine may be considered.
• If a patient requires IM medication, Lorazepam should be used first
line.
• IM Haloperidol may be used if there is confirmed history of previous
antipsychotic use.
• If previous use of antipsychotics can’t be confirmed and Lorazepam
fails to control the situation, low dose of oral Olanzapine may be
considered. In such cases it may be appropriate to consult a doctor
experienced in the management of older people.
For People with Dementia (see Appendix 2)
• People with Alzheimer's disease, vascular dementia or mixed
dementias with mild-to-moderate non-cognitive symptoms should not
be prescribed antipsychotic drugs because of the possible increased
risk of cerebrovascular adverse events and death.
• People with Dementia with Lewy Bodies (DLB) with mild-to-moderate
non-cognitive symptoms, should not be prescribed antipsychotic drugs,
because those with DLB are at particular risk of severe adverse
reactions.
• Non-pharmacological options should be considered as first line
management. If this is ineffective, then Lorazepam may be
considered. Risperidone is licensed for short-term use for persistent
aggression in people with moderate to severe Alzheimer’s dementia.
The starting dose is 0.25mg twice daily increased to 0.5mg twice daily.
If ongoing use of Risperidone is considered necessary then the advice
of a doctor experienced in the management of dementia should be
sought.
• The use of Olanzapine is unlicensed but may be justified in some
cases as per Maudsley Guidelines (12th edition). Consider a dose of
2.5- 5mg PO/IM. (Max 5mg/24hrs)
Rapid Tranquilisation Guidelines Version 3_0 Page 11 of 25
• In very exceptional circumstances, when oral treatment is impossible,
low dose haloperidol IM may be used. In these cases, consider
consulting a doctor with experience in managing disturbed behaviour
in people with dementia.
For Children and Young people under 18 years (see Appendix 3)
• The NICE Guideline on Violence and Aggression NG10 states that
restrictive interventions (which includes Rapid Tranquilisation) should
only be used if all attempts to defuse the situation have failed and the
child or young person becomes aggressive or violent. Staff must be
familiar with and use the de-escalation techniques outlined in the
NICE guideline to avoid having a restrictive intervention.
• A multidisciplinary approach is required and junior doctors e.g.F1s
must seek advice from a senior doctor or consultant before carrying
out rapid tranquilisation
• The general prescribing principles for adults outlined in Point 3.2-3.7
apply when prescribing for children and young people.
• Medication can be given against a child’s will with parental consent
i.e. permission from a person with Parental Responsibility under The
Children’s Act NI and or common law. If repeated medication is
required, the Mental Health Order NI (1986) should be considered.
Children and young people should be informed that a medication is
going to be given and always given the opportunity to accept oral
medication.
• The flow chart in Appendix 3 outlines a stepped approach to rapid
tranquilisation for Children and Young People aged between 6 and
18 years of age. In the following circumstances contact someone
more senior with experience in psychiatry: (a) if you are a junior
doctor and your initial drug treatment does not work, (b) if you are a
Consultant and have tried two or three approaches without success
then it may be wise to seek a second opinion from a colleague or
consult with a psychiatrist who works within the Child and Adolescent
Mental Health Service (CAMHS) within office hours
• The CAMHS Consultant on call hours are as follows:
Monday –Friday 9am - 9pm
Saturday and Bank Holidays 10am - 2pm
Rapid Tranquilisation Guidelines Version 3_0 Page 12 of 25
Sunday 9am - 5pm.
Outside these times, there is no CAMHS consultant on call and any
queries would need to go through the on–call arrangements for Mental
Health Liaison Service. This team offers an assessment service for our
young people outside the CAMHS Crisis working hours
3.8 Monitoring after Use of Intramuscular medication
• Appendix 4 outlines the monitoring required after the use of
intramuscular medication.
• If patients refuse monitoring of vital signs or of they remain too
behaviourally disturbed to be approached, this must be documented in
the patients notes at each time monitoring would have been due. The
patient should be observed for sign/symptoms of pyrexia, hypotension,
over sedation and general physical well-being and documented
accordingly.
3.9 Drugs NOT recommended for rapid tranquillisation
The following drugs are NOT recommended for rapid tranquillisation:
• Oral and IM Chlorpromazine – IM Chlorpromazine is painful and can
cause severe hypotension. Chlorpromazine must never be given
intravenously
• IM Diazepam – absorption is erratic
• IM depot antipsychotics
• Zuclopenthixol acetate is not recommended for routine use in rapid
tranquillisation due to its slow onset of action. It may however be
recommended by a senior doctor or consultant when:
� The patient is disturbed/violent over an extended time period
� Past history of good/timely response
� Past history of repeated parenteral administration required
� Cited in an advance decision.
Rapid Tranquilisation Guidelines Version 3_0 Page 13 of 25
3.10 Actions after Rapid Tranquillisation
• When Rapid Tranquillisation has been implemented, the Duty Doctor
must be called to attend the ward to ensure the treatment has been
effective and that undue adverse effects are no longer likely to occur.
• The Duty Doctor must assess the patient’s mental state and record
same.
• After IM Rapid Tranquilisation administered , or where clinically
necessary with oral medications, a Registered Nurse must observe the
patient for 1 hour and record NEWS (National Early Warning Score) at
10 minute intervals if possible. If patient is secluded or unwilling to have
NEWS recorded the Registered Nurse must observe the patient directly
at their side or through the viewing window and assess the patients
level of consciousness continually and record at 10 minute intervals
positive interaction with the patient, such as:
- The patient talking to the nurse
- The patient sitting or standing and being alert.
• These interactions must be recorded on the Seclusion Care Plan or
Nursing Notes.
• Any concern regarding the patient’s physical wellbeing such as reduced
respiration or change in level of consciousness a group of staff who are
MAPA trained must enter the room and check the patient’s physiological
observations and summon medical assistance as per policy.
• A report of use of IM Rapid Tranquillisation should be made on a
Trust Incident Form/Datix web for review within Mental Health for
learning purposes.
• The ward manager will discuss the service user’s experience after the
use of restrictive interventions and record their views in the relevant
patient notes. A referral to advocacy services will be offered in all cases.
4.0 Rapid Tranquilisation Guidelines for Emergency Departments
As per The Royal College of Emergency Medicine (RCEM) guidelines 05/16 –
Management of Excited Delirium/Acute Behavioural Disturbance
Acute Behavioural Disturbance (ABD) is a medical emergency in the
Emergency Department (ED). As per College Guidelines, in the ED setting
Rapid Tranquilisation Guidelines Version 3_0 Page 14 of 25
sedation should be with intravenous benzodiazepines, ketamine or
antipsychotics. Individuals displaying ABD may need much higher doses of
sedative agents than typically required or recommended.
Pharmacological management should be part of an overall management plan
that includes appropriate nursing care and de-escalation techniques
• Buccal olanzapine (zyprexia velotabs) 10mgs can be used where a
patient is compliant and parenteral route avoided.
• Where there is actual or clear risk of violence or aggression. De-
escalation including oral PRN (olanzapine 10mg buccal melt) not
possible or appropriate due to Risk of harm to self or others.
• In The Emergency Department Setting:
- 1 – Lorazepam IM (4mg) / IV (2-4mg)
- 2 - Ketamine IM (2-4mg/kg) / IV (1-2mg/kg)
- 3 – Haloperidol IM (10-20mg) / IV (5-10mg)
- (doses as suggested by RCEM for Rapid Tranquilisation)
Full patient monitoring in line with the RCEM guidance on safe procedural
sedation, including ETCO2 monitoring, must be used in all cases in which
sedation is administered if possible.
5.0 Monitoring
This policy will be reviewed in 3 years or less if changes to Regional Guidance,
post SAI or if a review is required.
6.0 Evidence Base/References
NHSCT National Early Warning Score (NEWS) Policy
NHSCT Resuscitation Policy includes Do Not Attempt Cardiopulmonary
Resuscitation Policy (DNACPR)
Royal College of Psychiatrists Consensus Statement on High Dose
Antipsychotic Medication CR190, 2014
BNF for Children 74th edition. bnf.org
Rapid Tranquilisation Guidelines Version 3_0 Page 15 of 25
Maudsley Prescribing Guidelines 12th Edition, Taylor, D, Paton C, Kapur S,
Informa Healthcare London 2010
Violence and Aggression: Short term management in Mental Health, Health
and Community Settings. National Institute for Health and Clinical Excellence
NG10, May 2015.
The Royal College of Emergency Medicine Best practice Guideline: Guidelines
for the Management of Excited Delirium/Acute Behavioural Disturbance (ABD),
May 2016
SPc Haloperidol tablets and Injection, Electronic Medicines Compendium,
www.medicines.org.uk accessed 30/10/2015
SPc Aripiprazole Tablets and Injection, Electronic Medicines Compendium,
www.medicines.org.uk accessed 30/10/2015
SPc Olanzapine tablets and Injection, Electronic Medicines Compendium,
www.medicines.org.uk accessed 30/10/2015
SPc Risperidone tablets, Electronic Medicines Compendium,
www.medicines.org.uk accessed 30/10/2015
SPc Lorazepam Tablets and Injection Electronic Medicines Compendium,
www.medicines.org.uk accessed 30/10/2015
7.0 Personal and Public Involvement (PPI)/Consultation Process
Dr A Collins Consultant Psychiatrist
Dr Catherine O’Lynn Speciality Doctor
Dr J McIlvenna Old Age Psychiatrist
Dr S McCann Old Age Psychiatrist
Mr Richard Bakasa Acting Head of Service & Acute Mental Health Services
Joby Joseph Charge Nurse
Ms N Gribben Clinical Pharmacist
Divisional Governance Team subgroup
Medical Staff Committee
Dr Mark A Bell & Dr M Jenkins Antrim Hospital Emergency Department
Dr F McCartan Child & Adolescent Mental Health Services
Dr Uzma Huda Divisional Medical Director, Mental Health Services
Dr Dave Watkins Consultant Paediatrician and Divisional Medical Director,
Women, Children and Families Division
Rapid Tranquilisation Guidelines Version 3_0 Page 16 of 25
8.0 Equality, Human Rights and DDA
This policy has been drawn up and reviewed in the light of Section 75 of the
Northern Ireland Act (1998) which requires the Trust to have due regard to the
need to promote equality of opportunity. It has been screened to identify any
adverse impact on the 9 equality categories.
The policy has been ‘screened out’ without mitigation or an alternative policy
proposed to be adopted
9.0 Alternative formats
This document can be made available on request on disc, larger font, Braille,
audio-cassette and in other minority languages to meet the needs of those
who are not fluent in English.
10.0 Sources of Advice in relation to this document
The Policy Author, responsible Assistant Director or Director as detailed on the
policy title page should be contacted with regard to any queries on the content
of this policy.
11.0 Policy Sign off.
Dr Uzma Huda ___________________________
Date: 2 September 2019
Lead Policy Author
Oscar Donnelly ____________________________ Date: 2 September 2019 Director
Rapid Tranquilisation Guidelines Version 3_0 Page 17 of 25
12.0 Appendices/Attachments
(1) Pharmacological management of violent and aggressive behaviour (for adults over 18 years) (2) Pharmacological management of violent and aggressive behaviour For over 65 years + dementia patients
(3) Pharmacological management of violent and aggressive behaviour For Children and Young people aged under 18 years (4) Rapid Tranquillisation - Monitoring Guidelines (5) Guidelines for the use of Flumazenil (6) The Neuroleptic Malignant Syndrome (NMS) (7) Dose Information (8) Medication Notes
Rapid Tranquilisation Guidelines Version 3_0 Page 18 of 24
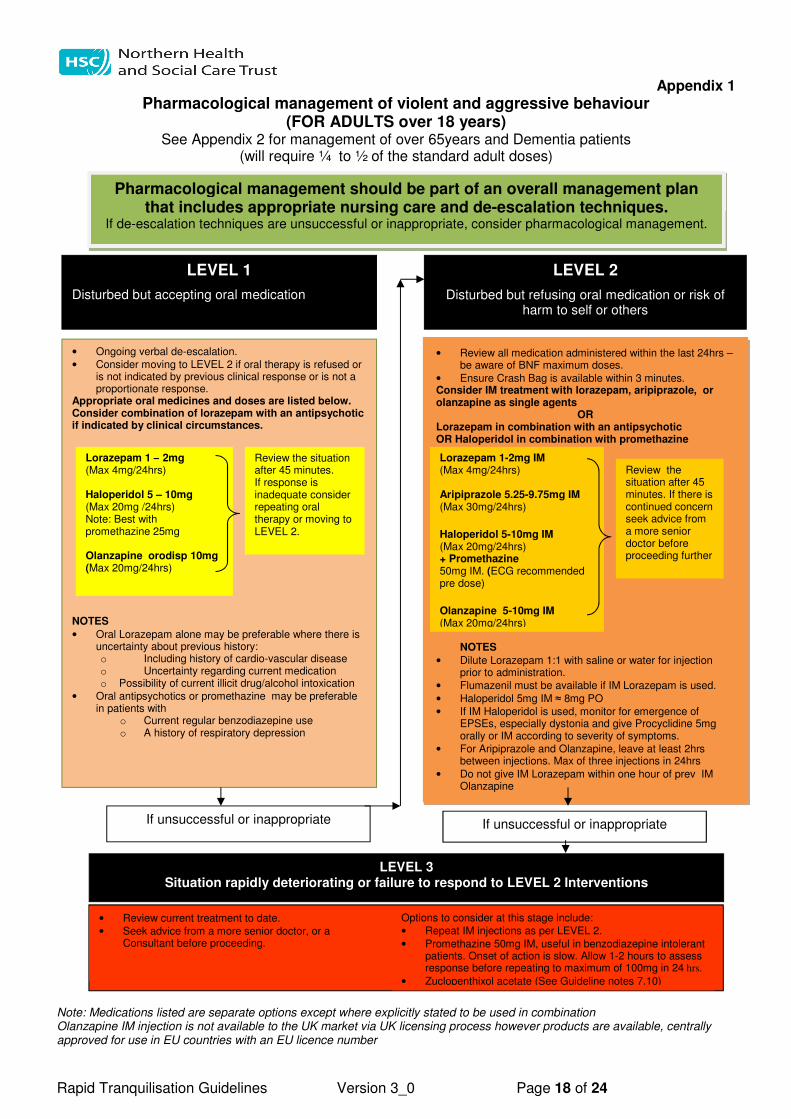
Appendix 1
Pharmacological management of violent and aggressive behaviour (FOR ADULTS over 18 years)
See Appendix 2 for management of over 65years and Dementia patients (will require ¼ to ½ of the standard adult doses)
Note: Medications listed are separate options except where explicitly stated to be used in combination Olanzapine IM injection is not available to the UK market via UK licensing process however products are available, centrally approved for use in EU countries with an EU licence number
Pharmacological management should be part of an overall management plan that includes appropriate nursing care and de-escalation techniques.
If de-escalation techniques are unsuccessful or inappropriate, consider pharmacological management.
LEVEL 1
Disturbed but accepting oral medication
LEVEL 2
Disturbed but refusing oral medication or risk of harm to self or others
• Ongoing verbal de-escalation.
• Consider moving to LEVEL 2 if oral therapy is refused or is not indicated by previous clinical response or is not a proportionate response.
Appropriate oral medicines and doses are listed below. Consider combination of lorazepam with an antipsychotic if indicated by clinical circumstances. NOTES
• Oral Lorazepam alone may be preferable where there is uncertainty about previous history: o Including history of cardio-vascular disease o Uncertainty regarding current medication o Possibility of current illicit drug/alcohol intoxication
• Oral antipsychotics or promethazine may be preferable in patients with
o Current regular benzodiazepine use o A history of respiratory depression
• Review all medication administered within the last 24hrs – be aware of BNF maximum doses.
• Ensure Crash Bag is available within 3 minutes. Consider IM treatment with lorazepam, aripiprazole, or olanzapine as single agents
OR Lorazepam in combination with an antipsychotic OR Haloperidol in combination with promethazine NNOTES
NOTES
• Dilute Lorazepam 1:1 with saline or water for injection prior to administration.
• Flumazenil must be available if IM Lorazepam is used.
• Haloperidol 5mg IM ≈ 8mg PO
• If IM Haloperidol is used, monitor for emergence of EPSEs, especially dystonia and give Procyclidine 5mg orally or IM according to severity of symptoms.
• For Aripiprazole and Olanzapine, leave at least 2hrs between injections. Max of three injections in 24hrs
• Do not give IM Lorazepam within one hour of prev IM Olanzapine
Lorazepam 1 – 2mg (Max 4mg/24hrs) Haloperidol 5 – 10mg (Max 20mg /24hrs) Note: Best with promethazine 25mg Olanzapine orodisp 10mg (Max 20mg/24hrs)
If unsuccessful or inappropriate If unsuccessful or inappropriate
LEVEL 3 Situation rapidly deteriorating or failure to respond to LEVEL 2 Interventions
• Review current treatment to date.
• Seek advice from a more senior doctor, or a Consultant before proceeding.
Options to consider at this stage include:
• Repeat IM injections as per LEVEL 2.
• Promethazine 50mg IM, useful in benzodiazepine intolerant patients. Onset of action is slow. Allow 1-2 hours to assess response before repeating to maximum of 100mg in 24 hrs.
• Zuclopenthixol acetate (See Guideline notes 7.10)
Review the situation after 45 minutes. If response is inadequate consider repeating oral therapy or moving to LEVEL 2.
Review the situation after 45 minutes. If there is continued concern seek advice from a more senior doctor before proceeding further
Lorazepam 1-2mg IM (Max 4mg/24hrs) Aripiprazole 5.25-9.75mg IM (Max 30mg/24hrs)
Haloperidol 5-10mg IM (Max 20mg/24hrs) + Promethazine 50mg IM. (ECG recommended pre dose)
Olanzapine 5-10mg IM (Max 20mg/24hrs)
Rapid Tranquilisation Guidelines Version 3_0 Page 19 of 24
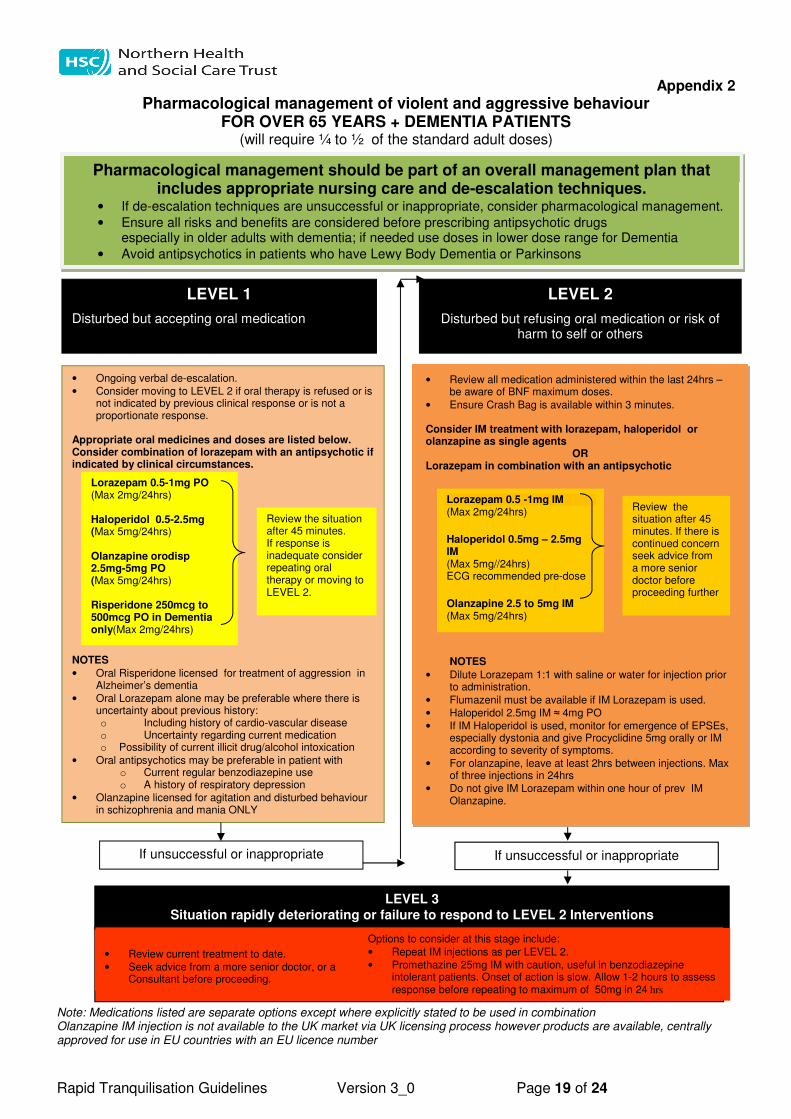
Appendix 2
Pharmacological management of violent and aggressive behaviour FOR OVER 65 YEARS + DEMENTIA PATIENTS
(will require ¼ to ½ of the standard adult doses) Note: Medications listed are separate options except where explicitly stated to be used in combination Olanzapine IM injection is not available to the UK market via UK licensing process however products are available, centrally approved for use in EU countries with an EU licence number
Pharmacological management should be part of an overall management plan that includes appropriate nursing care and de-escalation techniques.
• If de-escalation techniques are unsuccessful or inappropriate, consider pharmacological management.
• Ensure all risks and benefits are considered before prescribing antipsychotic drugs especially in older adults with dementia; if needed use doses in lower dose range for Dementia
• Avoid antipsychotics in patients who have Lewy Body Dementia or Parkinsons
LEVEL 1
Disturbed but accepting oral medication
LEVEL 2
Disturbed but refusing oral medication or risk of harm to self or others
• Ongoing verbal de-escalation.
• Consider moving to LEVEL 2 if oral therapy is refused or is not indicated by previous clinical response or is not a proportionate response.
Appropriate oral medicines and doses are listed below. Consider combination of lorazepam with an antipsychotic if indicated by clinical circumstances. NOTES
• Oral Risperidone licensed for treatment of aggression in Alzheimer’s dementia
• Oral Lorazepam alone may be preferable where there is uncertainty about previous history: o Including history of cardio-vascular disease o Uncertainty regarding current medication o Possibility of current illicit drug/alcohol intoxication
• Oral antipsychotics may be preferable in patient with o Current regular benzodiazepine use o A history of respiratory depression
• Olanzapine licensed for agitation and disturbed behaviour in schizophrenia and mania ONLY
• Review all medication administered within the last 24hrs – be aware of BNF maximum doses.
• Ensure Crash Bag is available within 3 minutes. Consider IM treatment with lorazepam, haloperidol or olanzapine as single agents
OR Lorazepam in combination with an antipsychotic
NOTES
• Dilute Lorazepam 1:1 with saline or water for injection prior to administration.
• Flumazenil must be available if IM Lorazepam is used.
• Haloperidol 2.5mg IM ≈ 4mg PO
• If IM Haloperidol is used, monitor for emergence of EPSEs, especially dystonia and give Procyclidine 5mg orally or IM according to severity of symptoms.
• For olanzapine, leave at least 2hrs between injections. Max of three injections in 24hrs
• Do not give IM Lorazepam within one hour of prev IM Olanzapine.
Lorazepam 0.5-1mg PO (Max 2mg/24hrs) Haloperidol 0.5-2.5mg (Max 5mg/24hrs)
Olanzapine orodisp 2.5mg-5mg PO (Max 5mg/24hrs) Risperidone 250mcg to 500mcg PO in Dementia only(Max 2mg/24hrs)
If unsuccessful or inappropriate If unsuccessful or inappropriate
LEVEL 3 Situation rapidly deteriorating or failure to respond to LEVEL 2 Interventions
• Review current treatment to date.
• Seek advice from a more senior doctor, or a Consultant before proceeding.
Options to consider at this stage include:
• Repeat IM injections as per LEVEL 2.
• Promethazine 25mg IM with caution, useful in benzodiazepine intolerant patients. Onset of action is slow. Allow 1-2 hours to assess response before repeating to maximum of 50mg in 24 hrs
Review the situation after 45 minutes. If response is inadequate consider repeating oral therapy or moving to LEVEL 2.
Review the situation after 45 minutes. If there is continued concern seek advice from a more senior doctor before proceeding further
Lorazepam 0.5 -1mg IM (Max 2mg/24hrs)
Haloperidol 0.5mg – 2.5mg IM (Max 5mg//24hrs) ECG recommended pre-dose
Olanzapine 2.5 to 5mg IM (Max 5mg/24hrs)
Rapid Tranquilisation Guidelines Version 3_0 Page 20 of 24
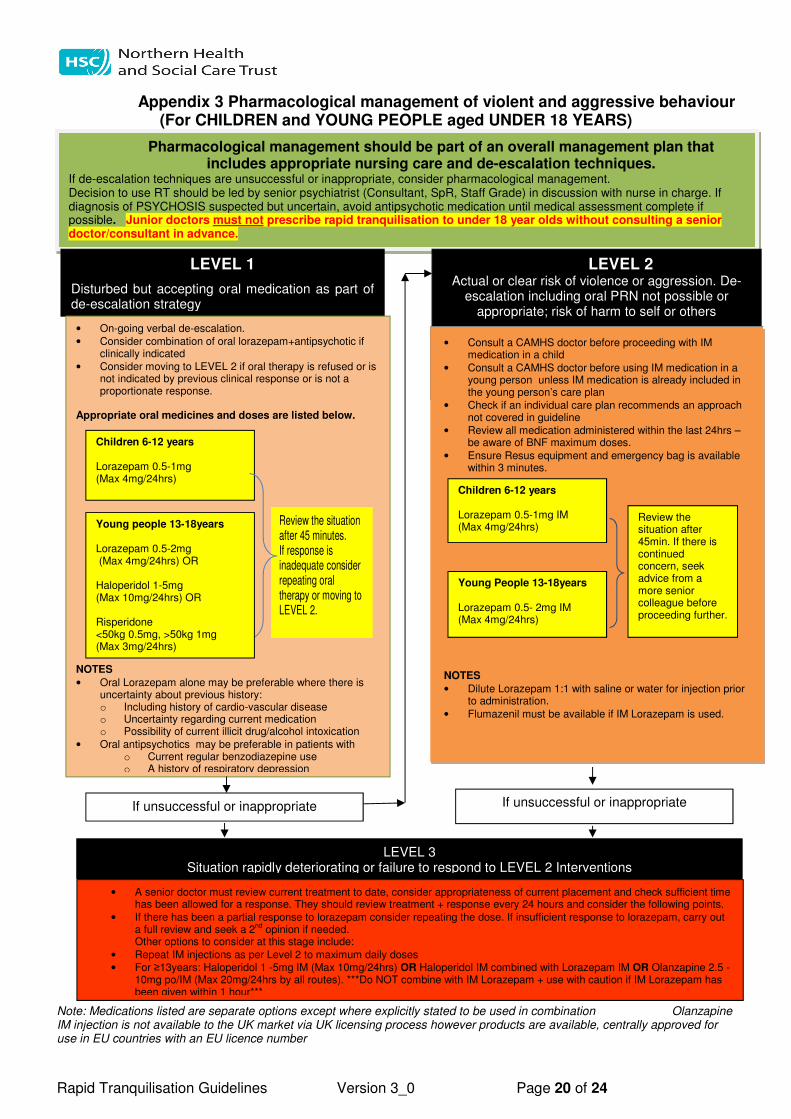
Appendix 3 Pharmacological management of violent and aggressive behaviour
(For CHILDREN and YOUNG PEOPLE aged UNDER 18 YEARS)
Note: Medications listed are separate options except where explicitly stated to be used in combination Olanzapine IM injection is not available to the UK market via UK licensing process however products are available, centrally approved for use in EU countries with an EU licence number
Pharmacological management should be part of an overall management plan that includes appropriate nursing care and de-escalation techniques.
If de-escalation techniques are unsuccessful or inappropriate, consider pharmacological management. Decision to use RT should be led by senior psychiatrist (Consultant, SpR, Staff Grade) in discussion with nurse in charge. If diagnosis of PSYCHOSIS suspected but uncertain, avoid antipsychotic medication until medical assessment complete if possible. Junior doctors must not prescribe rapid tranquilisation to under 18 year olds without consulting a senior doctor/consultant in advance.
LEVEL 1
Disturbed but accepting oral medication as part of de-escalation strategy
LEVEL 2 Actual or clear risk of violence or aggression. De-
escalation including oral PRN not possible or appropriate; risk of harm to self or others
• On-going verbal de-escalation.
• Consider combination of oral lorazepam+antipsychotic if clinically indicated
• Consider moving to LEVEL 2 if oral therapy is refused or is not indicated by previous clinical response or is not a proportionate response.
Appropriate oral medicines and doses are listed below.
NOTES
• Oral Lorazepam alone may be preferable where there is uncertainty about previous history: o Including history of cardio-vascular disease o Uncertainty regarding current medication o Possibility of current illicit drug/alcohol intoxication
• Oral antipsychotics may be preferable in patients with o Current regular benzodiazepine use o A history of respiratory depression
Review the situation after 45 minutes. If response is inadequate consider repeating oral therapy or moving to LEVEL 2.
• Consult a CAMHS doctor before proceeding with IM medication in a child
• Consult a CAMHS doctor before using IM medication in a young person unless IM medication is already included in the young person’s care plan
• Check if an individual care plan recommends an approach not covered in guideline
• Review all medication administered within the last 24hrs – be aware of BNF maximum doses.
• Ensure Resus equipment and emergency bag is available within 3 minutes.
NOTES
• Dilute Lorazepam 1:1 with saline or water for injection prior to administration.
• Flumazenil must be available if IM Lorazepam is used.
Children 6-12 years Lorazepam 0.5-1mg IM (Max 4mg/24hrs)
Children 6-12 years Lorazepam 0.5-1mg (Max 4mg/24hrs)
Review the situation after 45min. If there is continued concern, seek advice from a more senior colleague before proceeding further.
If unsuccessful or inappropriate If unsuccessful or inappropriate
LEVEL 3 Situation rapidly deteriorating or failure to respond to LEVEL 2 Interventions
• A senior doctor must review current treatment to date, consider appropriateness of current placement and check sufficient time has been allowed for a response. They should review treatment + response every 24 hours and consider the following points.
• If there has been a partial response to lorazepam consider repeating the dose. If insufficient response to lorazepam, carry out a full review and seek a 2
nd opinion if needed.
Other options to consider at this stage include:
• Repeat IM injections as per Level 2 to maximum daily doses • For ≥13years: Haloperidol 1 -5mg IM (Max 10mg/24hrs) OR Haloperidol IM combined with Lorazepam IM OR Olanzapine 2.5 -
10mg po/IM (Max 20mg/24hrs by all routes). ***Do NOT combine with IM Lorazepam + use with caution if IM Lorazepam has been given within 1 hour***
Young people 13-18years Lorazepam 0.5-2mg (Max 4mg/24hrs) OR Haloperidol 1-5mg (Max 10mg/24hrs) OR Risperidone <50kg 0.5mg, >50kg 1mg (Max 3mg/24hrs)
Young People 13-18years Lorazepam 0.5- 2mg IM (Max 4mg/24hrs)
Rapid Tranquilisation Guidelines Version 3_0 Page 21 of 24
Rapid Tranquillisation - Monitoring Guidelines Appendix 4
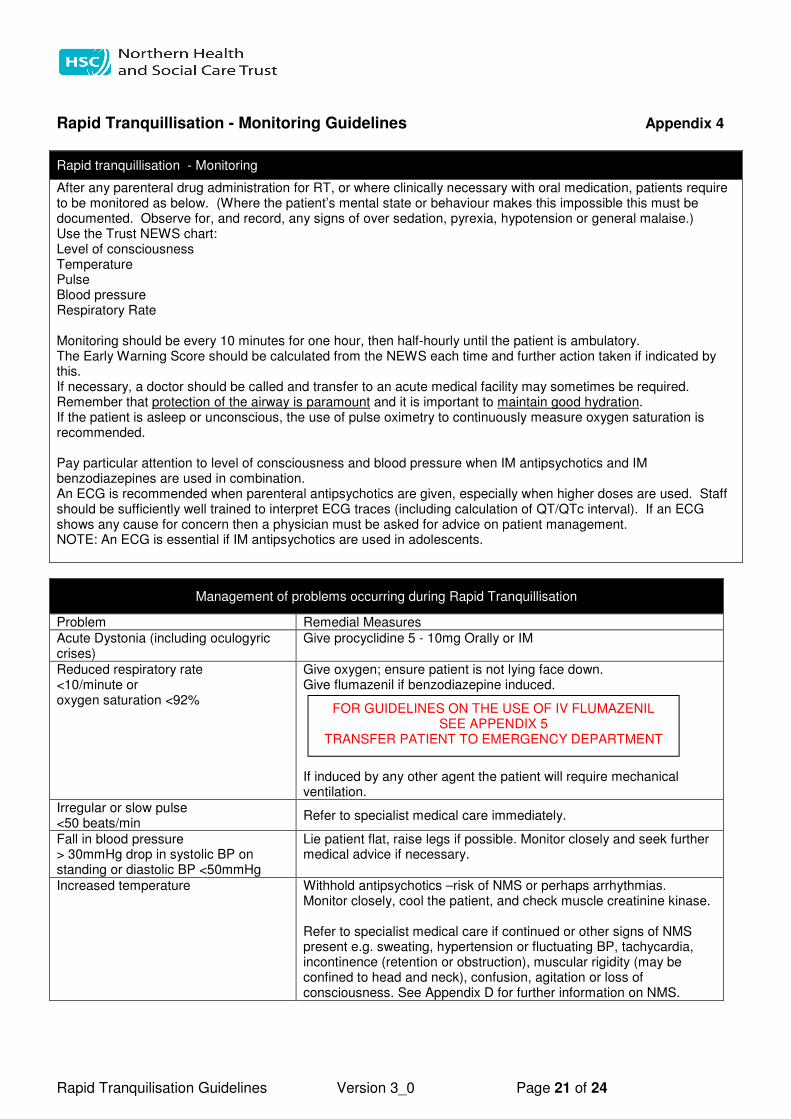
Rapid tranquillisation - Monitoring
After any parenteral drug administration for RT, or where clinically necessary with oral medication, patients require to be monitored as below. (Where the patient’s mental state or behaviour makes this impossible this must be documented. Observe for, and record, any signs of over sedation, pyrexia, hypotension or general malaise.) Use the Trust NEWS chart: Level of consciousness Temperature Pulse Blood pressure Respiratory Rate Monitoring should be every 10 minutes for one hour, then half-hourly until the patient is ambulatory. The Early Warning Score should be calculated from the NEWS each time and further action taken if indicated by this. If necessary, a doctor should be called and transfer to an acute medical facility may sometimes be required. Remember that protection of the airway is paramount and it is important to maintain good hydration. If the patient is asleep or unconscious, the use of pulse oximetry to continuously measure oxygen saturation is recommended. Pay particular attention to level of consciousness and blood pressure when IM antipsychotics and IM benzodiazepines are used in combination. An ECG is recommended when parenteral antipsychotics are given, especially when higher doses are used. Staff should be sufficiently well trained to interpret ECG traces (including calculation of QT/QTc interval). If an ECG shows any cause for concern then a physician must be asked for advice on patient management. NOTE: An ECG is essential if IM antipsychotics are used in adolescents.
Management of problems occurring during Rapid Tranquillisation
Problem Remedial Measures
Acute Dystonia (including oculogyric crises)
Give procyclidine 5 - 10mg Orally or IM
Reduced respiratory rate <10/minute or oxygen saturation <92%
Give oxygen; ensure patient is not lying face down. Give flumazenil if benzodiazepine induced. If induced by any other agent the patient will require mechanical ventilation.
Irregular or slow pulse <50 beats/min
Refer to specialist medical care immediately.
Fall in blood pressure > 30mmHg drop in systolic BP on standing or diastolic BP <50mmHg
Lie patient flat, raise legs if possible. Monitor closely and seek further medical advice if necessary.
Increased temperature Withhold antipsychotics –risk of NMS or perhaps arrhythmias. Monitor closely, cool the patient, and check muscle creatinine kinase. Refer to specialist medical care if continued or other signs of NMS present e.g. sweating, hypertension or fluctuating BP, tachycardia, incontinence (retention or obstruction), muscular rigidity (may be confined to head and neck), confusion, agitation or loss of consciousness. See Appendix D for further information on NMS.
FOR GUIDELINES ON THE USE OF IV FLUMAZENIL SEE APPENDIX 5
TRANSFER PATIENT TO EMERGENCY DEPARTMENT
Rapid Tranquilisation Guidelines Version 3_0 Page 22 of 24
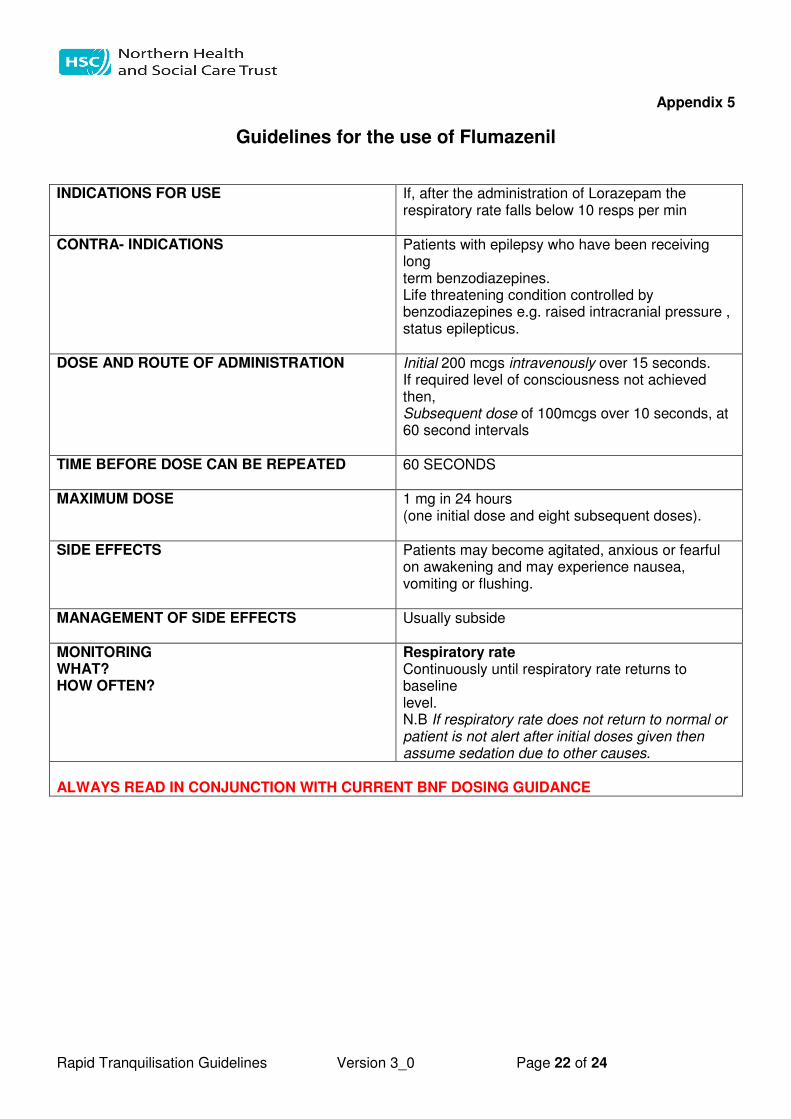
Appendix 5
Guidelines for the use of Flumazenil INDICATIONS FOR USE If, after the administration of Lorazepam the
respiratory rate falls below 10 resps per min
CONTRA- INDICATIONS Patients with epilepsy who have been receiving long term benzodiazepines. Life threatening condition controlled by benzodiazepines e.g. raised intracranial pressure , status epilepticus.
DOSE AND ROUTE OF ADMINISTRATION Initial 200 mcgs intravenously over 15 seconds. If required level of consciousness not achieved then, Subsequent dose of 100mcgs over 10 seconds, at 60 second intervals
TIME BEFORE DOSE CAN BE REPEATED 60 SECONDS
MAXIMUM DOSE 1 mg in 24 hours (one initial dose and eight subsequent doses).
SIDE EFFECTS Patients may become agitated, anxious or fearful on awakening and may experience nausea, vomiting or flushing.
MANAGEMENT OF SIDE EFFECTS Usually subside
MONITORING WHAT? HOW OFTEN?
Respiratory rate Continuously until respiratory rate returns to baseline level. N.B If respiratory rate does not return to normal or patient is not alert after initial doses given then assume sedation due to other causes.
ALWAYS READ IN CONJUNCTION WITH CURRENT BNF DOSING GUIDANCE
Rapid Tranquilisation Guidelines Version 3_0 Page 23 of 24
Appendix 6
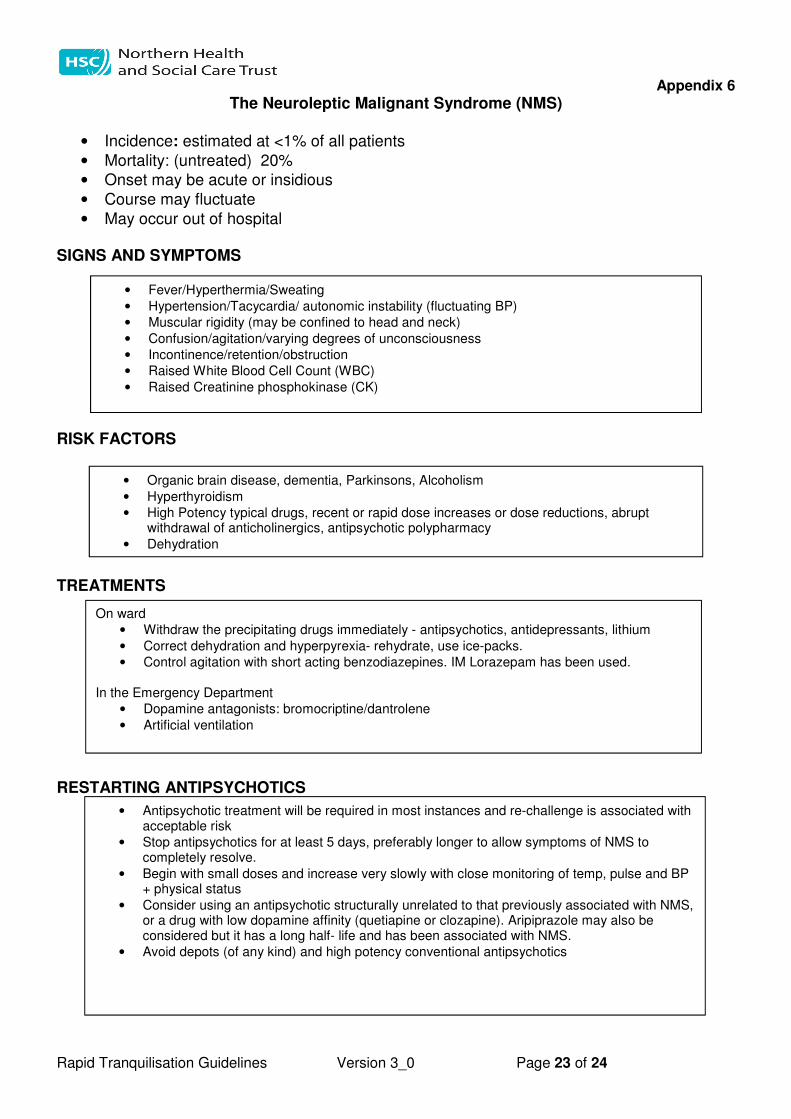
The Neuroleptic Malignant Syndrome (NMS)
• Incidence: estimated at <1% of all patients
• Mortality: (untreated) 20%
• Onset may be acute or insidious
• Course may fluctuate
• May occur out of hospital
SIGNS AND SYMPTOMS RISK FACTORS TREATMENTS RESTARTING ANTIPSYCHOTICS
• Fever/Hyperthermia/Sweating
• Hypertension/Tacycardia/ autonomic instability (fluctuating BP)
• Muscular rigidity (may be confined to head and neck)
• Confusion/agitation/varying degrees of unconsciousness
• Incontinence/retention/obstruction
• Raised White Blood Cell Count (WBC)
• Raised Creatinine phosphokinase (CK)
• Organic brain disease, dementia, Parkinsons, Alcoholism
• Hyperthyroidism
• High Potency typical drugs, recent or rapid dose increases or dose reductions, abrupt withdrawal of anticholinergics, antipsychotic polypharmacy
• Dehydration
On ward
• Withdraw the precipitating drugs immediately - antipsychotics, antidepressants, lithium
• Correct dehydration and hyperpyrexia- rehydrate, use ice-packs.
• Control agitation with short acting benzodiazepines. IM Lorazepam has been used. In the Emergency Department
• Dopamine antagonists: bromocriptine/dantrolene
• Artificial ventilation
• Antipsychotic treatment will be required in most instances and re-challenge is associated with acceptable risk
• Stop antipsychotics for at least 5 days, preferably longer to allow symptoms of NMS to completely resolve.
• Begin with small doses and increase very slowly with close monitoring of temp, pulse and BP + physical status
• Consider using an antipsychotic structurally unrelated to that previously associated with NMS, or a drug with low dopamine affinity (quetiapine or clozapine). Aripiprazole may also be considered but it has a long half- life and has been associated with NMS.
• Avoid depots (of any kind) and high potency conventional antipsychotics
Rapid Tranquilisation Guidelines Version 3_0 Page 24 of 25
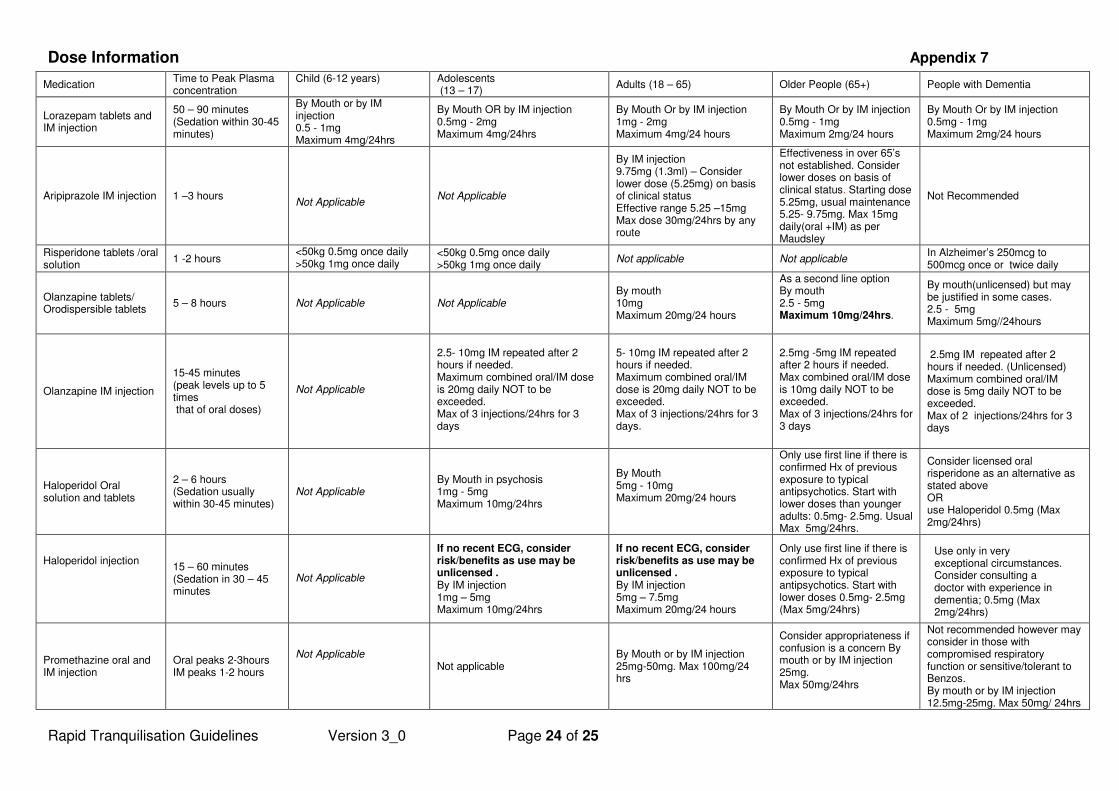
Dose Information Appendix 7
Medication Time to Peak Plasma concentration
Child (6-12 years) Adolescents (13 – 17)
Adults (18 – 65) Older People (65+) People with Dementia
Lorazepam tablets and IM injection
50 – 90 minutes (Sedation within 30-45 minutes)
By Mouth or by IM injection 0.5 - 1mg Maximum 4mg/24hrs
By Mouth OR by IM injection 0.5mg - 2mg Maximum 4mg/24hrs
By Mouth Or by IM injection 1mg - 2mg Maximum 4mg/24 hours
By Mouth Or by IM injection 0.5mg - 1mg Maximum 2mg/24 hours
By Mouth Or by IM injection 0.5mg - 1mg Maximum 2mg/24 hours
Aripiprazole IM injection 1 –3 hours
Not Applicable
Not Applicable
By IM injection 9.75mg (1.3ml) – Consider lower dose (5.25mg) on basis of clinical status Effective range 5.25 –15mg Max dose 30mg/24hrs by any route
Effectiveness in over 65’s not established. Consider lower doses on basis of clinical status. Starting dose 5.25mg, usual maintenance 5.25- 9.75mg. Max 15mg daily(oral +IM) as per Maudsley
Not Recommended
Risperidone tablets /oral solution
1 -2 hours <50kg 0.5mg once daily >50kg 1mg once daily
<50kg 0.5mg once daily >50kg 1mg once daily
Not applicable Not applicable In Alzheimer’s 250mcg to 500mcg once or twice daily
Olanzapine tablets/ Orodispersible tablets
5 – 8 hours
Not Applicable Not Applicable
By mouth 10mg Maximum 20mg/24 hours
As a second line option By mouth 2.5 - 5mg Maximum 10mg/24hrs.
By mouth(unlicensed) but may be justified in some cases. 2.5 - 5mg Maximum 5mg//24hours
Olanzapine IM injection
15-45 minutes (peak levels up to 5 times that of oral doses)
Not Applicable
2.5- 10mg IM repeated after 2 hours if needed. Maximum combined oral/IM dose is 20mg daily NOT to be exceeded. Max of 3 injections/24hrs for 3 days
5- 10mg IM repeated after 2 hours if needed. Maximum combined oral/IM dose is 20mg daily NOT to be exceeded. Max of 3 injections/24hrs for 3 days.
2.5mg -5mg IM repeated after 2 hours if needed. Max combined oral/IM dose is 10mg daily NOT to be exceeded. Max of 3 injections/24hrs for 3 days
2.5mg IM repeated after 2 hours if needed. (Unlicensed) Maximum combined oral/IM dose is 5mg daily NOT to be exceeded. Max of 2 injections/24hrs for 3 days
Haloperidol Oral solution and tablets
2 – 6 hours (Sedation usually within 30-45 minutes)
Not Applicable
By Mouth in psychosis 1mg - 5mg Maximum 10mg/24hrs
By Mouth 5mg - 10mg Maximum 20mg/24 hours
Only use first line if there is confirmed Hx of previous exposure to typical antipsychotics. Start with lower doses than younger adults: 0.5mg- 2.5mg. Usual Max 5mg/24hrs.
Consider licensed oral risperidone as an alternative as stated above OR use Haloperidol 0.5mg (Max 2mg/24hrs)
Haloperidol injection
15 – 60 minutes (Sedation in 30 – 45 minutes
Not Applicable
If no recent ECG, consider risk/benefits as use may be unlicensed . By IM injection 1mg – 5mg Maximum 10mg/24hrs
If no recent ECG, consider risk/benefits as use may be unlicensed . By IM injection 5mg – 7.5mg Maximum 20mg/24 hours
Only use first line if there is confirmed Hx of previous exposure to typical antipsychotics. Start with lower doses 0.5mg- 2.5mg (Max 5mg/24hrs)
Use only in very exceptional circumstances. Consider consulting a doctor with experience in dementia; 0.5mg (Max 2mg/24hrs)
Promethazine oral and IM injection
Oral peaks 2-3hours IM peaks 1-2 hours
Not Applicable
Not applicable By Mouth or by IM injection 25mg-50mg. Max 100mg/24 hrs
Consider appropriateness if confusion is a concern By mouth or by IM injection 25mg. Max 50mg/24hrs
Not recommended however may consider in those with compromised respiratory function or sensitive/tolerant to Benzos. By mouth or by IM injection 12.5mg-25mg. Max 50mg/ 24hrs
Rapid Tranquilisation Guidelines Version 3_0 Page 25 of 25
Appendix 8
Medication notes:
• Remember, 0.5mg Lorazepam is equivalent to 5mg Diazepam
• The repeated use of a benzodiazepine may result in tolerance to the effect and this will probably become evident
by 7 to 10 days.
• Haloperidol 5mg IM is equivalent to approximately 8mg orally
• IM Benzodiazepines (Lorazepam) should not be given until at least one hour after IM olanzapine (severe
bradycardia and a couple of deaths associated with giving these two medications together)
• If the patient has received parenteral benzodiazepine, IM olanzapine administration should only be considered
after careful evaluation of clinical status, and the patient should be closely monitored for excessive sedation and
cardiorespiratory depression.
• Olanzapine injection is not licensed for use beyond 3 days
• There is probably an increased risk of cerebro-vascular events in older patients with all antipsychotics
• Risperidone is the only licensed antipsychotic drug for the treatment of aggression in Alzheimer’s dementia.
• Haloperidol is licensed for treatment of agitation and restlessness in the elderly. SPC recommends a pre-
treatment ECG.
• Olanzapine is licensed for treatment of agitation and disturbed behaviour in schizophrenia or mania.
• Orodispersible tablets no advantage in speed of onset but are harder to spit out or conceal
• Avoid antipsychotics if: known cardiac problems, abnormal ECG parameters, on concomitant meds which may
prolong QTc, diagnosis of Lewy Body Dementia or Parkinson’s disease.