Neonatal Jaundice Carrie Phillipi, MD, PhD. Newborn with Jaundice.

ð
NEWBORNTRANSITIONANDNEONATALRESUSCITATION
LIMPOPOINIATIVEFORNEWBORNCARE2017

1

2
TABLEOFCONTENTS
INTRODUCTIONTOTHECOURSEONNEWBORNTRANSITIONANDNEONATALRESUSCITATION 4
COURSEOVERVIEW 4HOWTHECOURSEWORKS 4COURSEDEVELOPERSANDFACILITATORS 4
MODULE1:NEWBORNTRANSITIONANDRESUSCITATION 6
MODULE1:PREPARINGFORTHEBIRTH 9
STEP1:PREPAREANEMERGENCYPLAN 9STEP2:HANDWASHING 9STEP3:PREPARETHEMOTHERANDBIRTHCOMPANIONFORTHEDELIVERY 11STEP4:PREPARETHEAREAFORDELIVERY. 11STEP5:PREPAREFORRESUSCITATIONANDCHECKTHEEMERGENCYEQUIPMENT. 11SELFASSSEMENTQUESTIONS:MODULE1 15
MODULE2:ROUTINECAREATBIRTH 16
DRYTHOROUGHLY 16CHECKIFTHEBABYISCRYING,CHECKBREATHING,KEEPWARM 16CLAMPANDCUTTHECORD. 16ROUTINECAREOFBABIESBORNBYCAESAREANSECTION 17ROUTINECAREOFPRETERMBABIES 17MONITORBABYWITHMOTHERANDINITIATEBREASTFEEDING 18RAPIDLYASSESSTHEBABYIMMEDIATELYAFTERBIRTH 18SELFASSESSMENTQUESTIONS:MODULE2 21
MODULE3:HELPTHEBABYWHOISNOTBREATHINGWELL 22
3.1CLEARTHEAIRWAYANDSTIMULATEBREATHING. 223.2VENTILATEWITHBAGANDMASK 233.3IMPROVEVENTILATIONIFTHEBABYISSTILLNOTBREATHINGWELL 24SELFASSESSMENTQUESTIONS:MODULE3 25
MODULE4.ADVANCEDRESUSCITATION 26
4.1PATHOPHYSIOLOGYOFBIRTHASPHYXIA 264.2ADVANCEDCARE:HEARTRATE 274.3ENDOTRACHEALINTUBATION 304.4UMBILICALVEINCATHETERISATION 334.5WHENTOWITHHOLDORDISCONTINUELIFESUPPORT 344.6POSTRESUSCITATIONCAREOFTHENEONATE 35SELFASSESSMENTQUESTIONSMODULE4 35REFERENCES 37CLINICALPRACTICESESSIONS 39

3

4
INTRODUCTIONTOTHECOURSEONNEWBORNTRANSITIONANDNEONATALRESUSCITATION
COURSEOVERVIEW
Thecourse is fordoctors,midwivesandclinicalassociatesworking indistrictandregionalhospitals inSouthAfrica.Thecoursecoversthe immediatecareofthenewbornduringtransition inthedeliveryroomaswellasallneonatalresuscitation prior to the transfer of both mother and baby to the postnatal or neonatal ward. This course iscomplimentary to theHelpingBabiesBreathe (HBB) course, an iniativeof theAmericanAcademyofPediatricsandpartners.AllmidwivesinSouthAfricaarerequiredtoundergotheHBBcourse.ThiscoursefollowsthesamestepsasHBB and then incorporates advanced resuscitation, resuscitation of the preterm newborn, care of the newborndeliveredbycaesareansectionandtheimmediatepostresuscitationcareofallnewborns.
HOWTHECOURSEWORKS
Thecourseconsistsof4modules,eachfollowedbyanassessment.Eachmoduleincorporatesreading,chartreviews,videosandassessmentquestions.Alistofadditionalreadingmaterialwillbeprovided.
Thecoursecanbedoneinanumberofways.
1. Pre-reading andattendanceataplannedcourse inyourdistrict.Read thismaterialandwatch thevideo’swhichareavailableonthewebsitewww.lincare.co.zabeforeattendingacourseinyourdistrictorprovince.AtthestarttothecoursethefacilitatorwillbegiveyoutheMCQ’stodobeforegoingontotheclinicalskillssessions.
2. Ase-learning.Youcanenrol for thee-learningcourse.Gotothewebsitewww.lincare.co.zaandfollowtheinstructionsonthee-learningtab.Thee-learningishostedbytheUniversityofLimpopoontheBlackboardlearnplatform.YoucandownloadtheBlackboard learnAPPonyoursmartphone.Aspartofthee-learningyouwillbeassignedafacilitator;thiswillusuallybeaPaediatricianorseniorclinicianworkinginyourfacility,district or region. Your facilitator will host a discussion forum with a group of participants, and may setadditionaloptionaltasks.Yourfacilitatorandgroupwilldecideonadatefortheclinicalskillssession.
ParticipantswhoworkinLimpopoandotherparticipatingprovinceswillbeinvitedbytheirfacilitatortoenrolina2–3hourskillssession.
CEUpointswillbeavailableonsuccessfulcompletionoftheon-siteande-learningcourse.
Youarewelcometoreadthismaterialandwatchanddownloadthevideo’s.WewillhowevernotbeabletoprovideyouwithCEUpointsunlessyouenrolonaformalcourse.
COURSEDEVELOPERSANDFACILITATORS
ThecoursedevelopersareDrAnneRobertsonandDrRienkBaarsma.
Dr Anne Robertson is the Provincial Paediatrician in the Limpopo Province, Department of Health and jointlyappointedwiththeUniversityofLimpopo.SheisinvolvedinseveralinitiativestoimprovepaediatricandchildhealthinLimpopoProvinceandSouthAfrica.
DrRienkBaarsmaisaNeonatologistfromtheNetherlands,withextensiveexperienceinclinicalneonatology,generalpaediatrics, teaching and research. He worked in Mankweng Hospital, Limpopo Province from 2012-2015, as aNeonatalogist.
Acknowledgements
5
Thevideo’swereproducedbyDrRienkBaarsmawiththeassistanceofMsLollyMashao(LimpopoProvincialNeonatalcoordinator)andDrGlenroseRikhotso.(PaediatricRegistrar,UniversityofLimpopo)
DrDelinaManzini(Paediatrician)hasassistedwitheditinganddevelopingfurtherassessmentmaterial.
MrAndrewScholtz(Educationaltechnologist)hasadvisedontheeducationmethodologyandhasdevelopedandsetuptheon-lineplatformande-learningcourse.
Coursefacilitators
Youwillbeassignedacoursefacilitatorwithwhomyoucaninteractanddiscuss.YourfacilitatorwillusuallybeaPaediatricianorseniorclinicianinyourfacility,districtorregionalhospital.

6
MODULE1:NEWBORNTRANSITIONANDRESUSCITATION
Thetransitionfromafoetustoanewborn isaphysiologicalprocessthatbegins inthe latterpartofpregnancyandcontinues throughout labour. At around 28weeks gestation, the alveolar cells begin to secrete surfactant on thesurfaceoffluid-filledlungs.Duringlabour,fluidisclearedfromthelungs,andwiththefirstbreathoutsidethewomb,airfillsthepreviouslyfluid-filledlungs.Thetransitionfromfoetaltonewborncirculationoccurswiththecessationofthe placental circulation as the umbilical cord is cut or the placenta is removed. There is a decrease in pulmonaryvascularresistanceandanincreaseinpulmonarybloodflowthatiscausedbytheincreaseinarterialoxygentensionafter the baby starts breathing, thus the gaseous exchange via the placenta ceases and the lungs take over thisfunction. Cortisol and catecholamines prepare the foetus for the birth process and support the multi – organtransitionfromintrauterinetoextrauterinelife.Initiatingbreastfeedingsoonafterbirthformspartofthetransition.
Themajorityofnewbornsdonotencounteranyproblemswiththetransition.Abnormalitiestoadaptationaremorefrequentlyfoundfollowingpretermdelivery;deliverybycaesareansectionordeliveryfollowingfoetaldistress.
Thevastmajorityofbabiesbornattermbreathespontaneouslywithin10–30secondsofbirth.Anestimated5-10%respond to drying and stimulation, airway clearing or positioning to breathe. Only 3 – 6% of all newborns requireassistedventilationwithabagandmasktohelpthembreathe.Lessthan1%ofnewbornsrequirechestcompressionand drugs to assist with transition and establish breathing. We will refer to the need for drugs and chestcompressions as requiring advanced resuscitation. In several large studies, only ~0.1% of newborns required chestcompression and/or drugs as part of resuscitation. These numbers vary in different places in theworld: in a largeSwedish study, less than 1% of babies needed any resuscitation at all, including not requiring bag and maskventilation.TwolargestudiesdoneinGautengprovince,SouthAfrica,showedthat4,7/1000and8,5/1000newbornsneededhelpwithbreathingatCharlotteMaxekehospitalandChrisHaniBaragwanthhospital,respectively.Veryfew0,1% newborns needed cardiac compression and only 0,04% newborns required adrenaline as part of advancedresuscitation.Theprognosisofthosewhodidrequirecardiaccompressionandadrenalinewasgenerallypoor.

7
Figure1.Newbornsrequiringneonatalresuscitation
“Neonatalresuscitation,whenimplementedsystematicallybypersonnelusingstandardguidelinesandcompetency-based training, has the potential to avert 30% of intrapartum-related neonatal deaths per year.” (2) Furthermoreresuscitation may avert 5 – 10% of deaths due to the complications of preterm birth. This is the premise forsimplifying and increasing access to skills based training in neonatal transition and resuscitation for all health careworkers.
ThechartbelowistheactionplansourcedfromtheHelpingBabiesBreathecoursematerial,(6)whichyoumayhavealreadydone.Reviewthestepsinthechart.Thestepsintheactionplanofferasystematicapproachtothecareofthenewborninfant,whichifcorrectlyappliedareeffectivewithinoneminute:THEGOLDENMINUTESM
(References1–8)
85%ofbabiesbreathespontaneouslywithin10-30secondsofbirth
Approximately5-10%ofpalentssimplyrequireslmulalonanddryingatbirthtohelpthembreathe
Approximately3-6%requirebasicresuscitalon(bagandmaskvenllalon)
<<1%requireadvanced
resuscitation<0.1%require
chestcompression<0.05%require

8
Figure2:HelpingBabiesBreatheActionChart(8)

9
MODULE1:PREPARINGFORTHEBIRTH
Planandpreparefortransitionbyfollowingthese5steps.
STEP1:PREPAREANEMERGENCYPLAN
Identifysomeonetohelpwith transition forEVERYbirth.Supportduring transitionatbirthor resuscitationmayberequiredwithanydeliverybut ismorelikely ifthebabyis lessthan35weeksgestation,deliveredbyanemergencycaesarean section or has documented foetal distress. Arrange for a healthworker to assist if normal transition isanticipatedorfortwohealthworkerstoassistifadvancedresuscitationisanticipated.Fourhealthworkersshouldbeavailableatatwindelivery.Reviewtheemergencyplaninyourfacility;includingwhomtocall,howtocommunicate,andhowtotransportthebabyshouldneonatalwardcareortransferberequired.
STEP2:HANDWASHING
Everyonewhoattendsadeliverymustwashhisorherhands.This includesthemother, father,orbirthcompanion.Goodhandwashinghelpstopreventthespreadofinfection.Handsmustbewashedthoroughlywithsoapandcleantepidwater. An alcohol-based cleanermaybeused afterwashing. For thehealthcareworker, thismust bedonebefore checking theemergencyequipment aswell asbeforeandafter caring for amotheror ababy. In addition,sterileglovesmustbewornwhenassistingthenewbornwithtransition.Glovesprotectyoufrominfectionscarriedbybloodandotherbodyfluids.

10
Figure3:HandWashingandcleaningchart(8)

11
STEP3:PREPARETHEMOTHERANDBIRTHCOMPANIONFORTHEDELIVERY
Explaintothemotherandbirthcompanionwhatwillhappen if thebabyhasanormal transition,andwhatwillbedoneshouldthebabyrequiresupportfortransition.Ifyouexpectanormaltransition,explaintothemotherandbirthcompanionthatthebabywillbeplacedskintoskinonthemothersabdomenimmediatelyafterbirth,andkeptskintoskininordertofacilitatetheinitiationofbreastfeeding.
STEP4:PREPARETHEAREAFORDELIVERY.
The area where the baby is to be born must be clean, warm and well lit. Eliminate draughts from fans, airconditioners,openwindowsanddoors.Warmthebirthingroomortheatreto23–25oCandusearadiantwarmertowarmthearea forventilation should thisbe required. If thegestationalageof thebaby is less than28weeks thetemperatureofthedeliveryroomortheatreshouldbe>25oC.Itistheresponsibilityofthepersonpreparingforthedeliverytoensurethattheareaiscomfortableforthebaby.
STEP5:PREPAREFORRESUSCITATIONANDCHECKTHEEMERGENCYEQUIPMENT.
Prepare the resuscitation surface before every delivery. This should be a flat padded surface with an overheadwarmer,goodlightingandatimer.Havingwashedhandsthoroughly,checkthatallequipmentandsuppliesarereadyforuse.Basicequipmentisrequiredateachdeliverysite.Additionalequipmentmaybestoredonamobiletrolleyincleanplasticbagsor inabox,usedonly forthispurpose.Thetablebelowprovidesachecklistofall theequipmentthatisrequired.

12
Table1:NeonatalResuscitationequipment
BasicneonatalResuscitationequipment(ateachbedside)
NeonatalResuscitationstation,trolleyorbox,atleast1per4deliverybedsand1intheatre
General ! Firmpaddedresuscitationsurface! Overheadwarmer! Lightforthearea! Clockwithtimerinseconds! Warmreceivingtowels! Stethoscope! HeadCaps/hats
! Firmpaddedresuscitationsurface! Overheadwarmer! Lightforthearea! Clockwithtimerinseconds! Warmreceivingtowels! Stethoscope! HeadCaps/hats! Pulseoximeterwithneonatalprobe! Transportincubator! Sterilegloves
AirwayManagement
! PortableSuctionDevicelikePenguin
! Suctionapparatus! Suctioncatheters6F! Suctioncatheters8F! Suctioncatheters10F
! OrophayngealairwaysSize0! OrophayngealairwaysSize00! Laryngoscopehandle
! MillerBlade00! MillerBlade0
! Spareworkingbatteries! Spareworkingbulb! ETTintroducer/stylet! SuppliesforfixingETT! McGillforceps(paediatricsize)! ETTuncuffed2.5
! ETTuncuffed3.0! ETTuncuffed3.5
Breathingsupport
! Bagvalvemaskventilator(e.g.LaerdalNeonatalVentilationBag)
! MaskforventilationbagSize0! MaskforventilationbagSize1
! Bagvalvemaskventilator(e.g.Laerdal)! Maskforventilationbag! Size0! Size1! Sourceofoxygenwithflowmeter! Oxygentubing
Circulationsupport
! UmbilicalvenouscatheterSize3.5F! UmbilicalvenouscatheterSize5F! IVcannula24G! Skinprepe.g.Webcol! Tapes/devicestosecureUVC/IVcannula! Syringesandneedles(assortedsizes)! 2X3waytaps! UmbilicalVeinCatheterisationsterilepack
Drugsandfluids
! Adrenaline1:1000! WaterforInjection! (Naloxone)! NormalSaline0,9%! Neonatolyteor10%glucose! 60drops/mindripset! Buretol! Dial-a-flow! 3waytap! Glucoseteststripsandglucometer! VitaminK(Konakion)! Chloramphenicol(Chloromax)eyeointment
Documentation
! Equipmentchecklist! Neonatalexaminationticksheet
13
WatchLINCVideo:EmergencyEquipment.
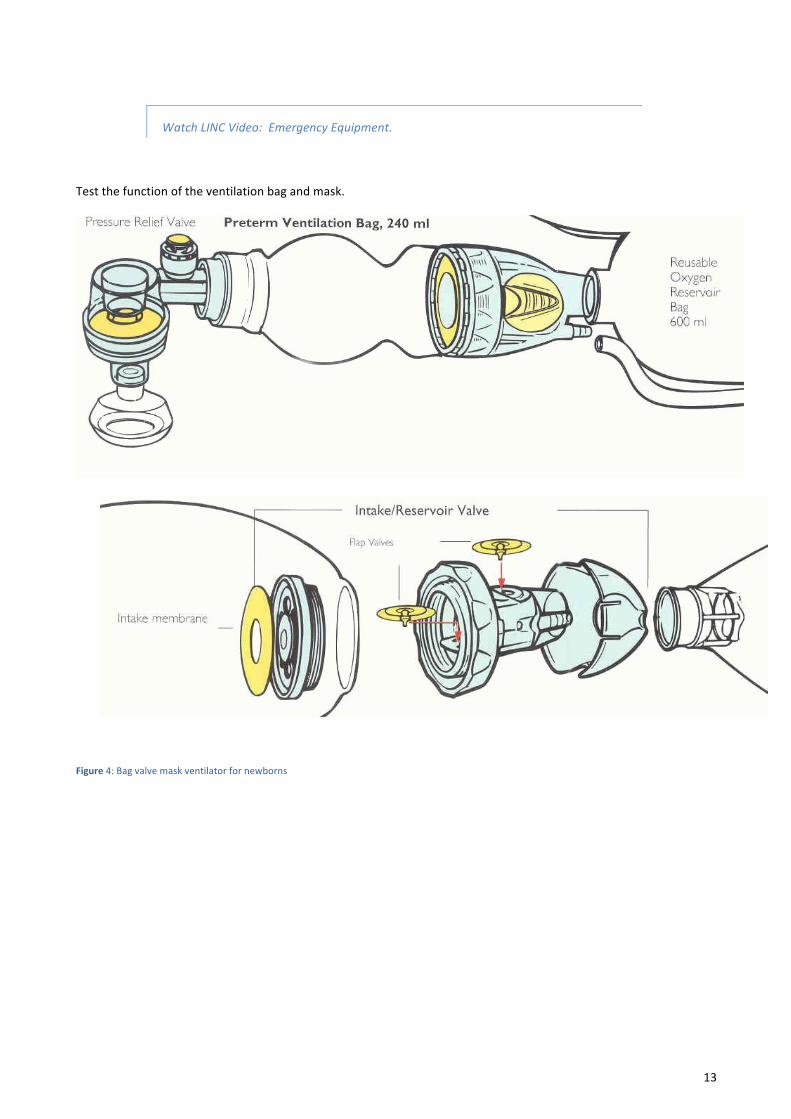
Testthefunctionoftheventilationbagandmask.
Figure4:Bagvalvemaskventilatorfornewborns
14
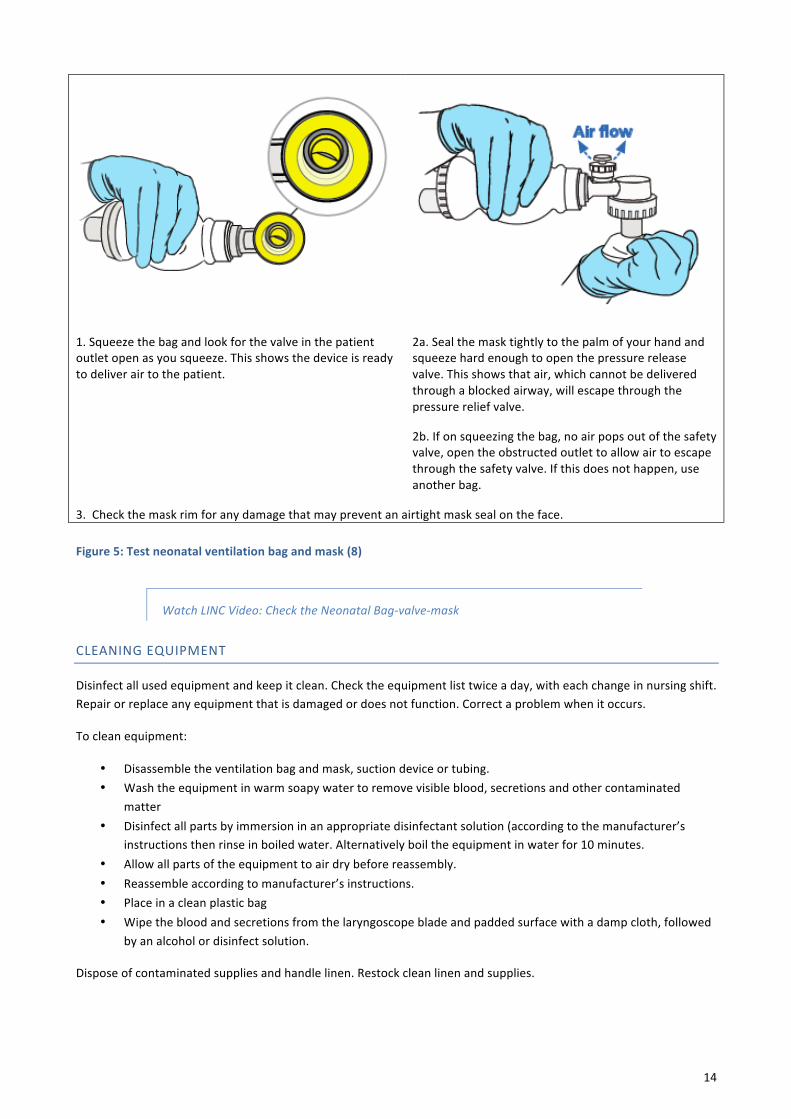
1.Squeezethebagandlookforthevalveinthepatientoutletopenasyousqueeze.Thisshowsthedeviceisreadytodeliverairtothepatient.
2a.Sealthemasktightlytothepalmofyourhandandsqueezehardenoughtoopenthepressurereleasevalve.Thisshowsthatair,whichcannotbedeliveredthroughablockedairway,willescapethroughthepressurereliefvalve.
2b.Ifonsqueezingthebag,noairpopsoutofthesafetyvalve,opentheobstructedoutlettoallowairtoescapethroughthesafetyvalve.Ifthisdoesnothappen,useanotherbag.
3.Checkthemaskrimforanydamagethatmaypreventanairtightmasksealontheface.
Figure5:Testneonatalventilationbagandmask(8)
WatchLINCVideo:ChecktheNeonatalBag-valve-mask
CLEANINGEQUIPMENT
Disinfectallusedequipmentandkeepitclean.Checktheequipmentlisttwiceaday,witheachchangeinnursingshift.Repairorreplaceanyequipmentthatisdamagedordoesnotfunction.Correctaproblemwhenitoccurs.
Tocleanequipment:
• Disassembletheventilationbagandmask,suctiondeviceortubing.• Washtheequipmentinwarmsoapywatertoremovevisibleblood,secretionsandothercontaminated
matter• Disinfectallpartsbyimmersioninanappropriatedisinfectantsolution(accordingtothemanufacturer’s
instructionsthenrinseinboiledwater.Alternativelyboiltheequipmentinwaterfor10minutes.• Allowallpartsoftheequipmenttoairdrybeforereassembly.• Reassembleaccordingtomanufacturer’sinstructions.• Placeinacleanplasticbag• Wipethebloodandsecretionsfromthelaryngoscopebladeandpaddedsurfacewithadampcloth,followed
byanalcoholordisinfectsolution.
Disposeofcontaminatedsuppliesandhandlelinen.Restockcleanlinenandsupplies.

15
SELFASSSEMENTQUESTIONS:MODULE1
Answer the multiple choice or true / false questions below. If you do not get the questions correct, review thematerialbeforeansweringthequestionsagain.Onceyouhavesuccessfullycompletedthequestionsyoumaymovetothenextsection.
1.1 Tickthestatementthatiscorrectregardingneonatalresuscitation.Thereisonly1correctanswer.
☐About3-6%ofbabieswillrequireassistedventilationwithtrachealintubation
☐Mostbabieswillnotneedanyneonatalresuscitationtobreathe(CORRECT)
☐About75%ofbabiesrequirebasicsupportsuchasdryingandstimulation
☐1%ofbabiesrequirecardiaccompressionanddrugsinneonatalresuscitation
1.2Preparationforhelpingababybreathebeforebirthincludesthefollowing:
1 Identifyahelperandgoingthroughtheemergencyplan
2 Checkingtheequipment
3 Washinghands
4 Communicatingwiththemother
Whatisthecorrectsequence?
☐1,2,3,4
☐3,2,1,4
☐1,3,4,2
☐1,4,3,2(CORRECT)
1.3 Neonatal resuscitation, when implemented systematically using standard guidelines and competency based
training
☐Haspotentialtoavert30%ofintrapartumrelateddeaths(CORRECT)
☐Haspotentialtoavert70%ofintrapartumrelateddeaths
☐Haspotentialtodecreasepretermmortalityby30-35%
☐Haspotentialtodecreasepretermmortalitybe50-55%

16
MODULE2:ROUTINECAREATBIRTH
Assoonasthebabyisborn:
DRYTHOROUGHLY
Check the timeofbirthad thendry thebaby thoroughly.Drying thoroughly involvesgently rubbing thebody, legs,armsandheadwithawarmcloth.Dryinghelpskeepthebabywarmandclean,andalsostimulatesbreathing.Blottingor patting does not stimulate breathing. Awet baby can easily become cold, and a cold baby can have difficultybreathing.Dryingalsoremovesblood,bodyfluidsandstoolsofthemother. Removethewetcloth.Placethebabyskin-to-skinonthemother’sabdomen,coverwithadryclothandplaceacaponthehead.
A note about suctioning andmeconium: Babiesdonot require routine suctioningatbirth,evenifthereismeconium.Meconiumintheamnioticfluidmaybeasignoffoetaldistress, especially if there is thick meconium. While these babies may be at risk ofMeconium Aspiration Syndrome (MAS), recent randomised control trials have foundtheretobenoreductioninMASwhenthesebabiesareroutinelysuctionedondeliveryorwithroutineintubationandsuctioningofthevigorousbabywithmeconium.(7)
If at birth the baby has very poor tone and does not breathe, youmay immediatelyvisualise the cords with direct laryngoscopy. If meconium is seen through the cords,intubateandthenapplysuctionandremovetheETtube.Thisprocedureshouldnottakelonger than15seconds,andventilationshouldneverbedelayed if thiscannotbedoneimmediately.
CHECKIFTHEBABYISCRYING,CHECKBREATHING,KEEPWARM
Check if thebaby iscryingandbreathing.Ifthebabyiscrying,thenbyimplication,thebabyisbreathingandhasaheartratethatisusuallyabove100beatsperminute.Inthissituation,itisnotnecessarytophysicallychecktheheartrateimmediately.IfthebabyisNOTcrying;checkingwhetherthebabyisbreathingnormallyisthefirstpriority.Lackofbreathingoranabnormalpatternofbreathingwarrantsimmediateinterventionasdiscussedinmodule3)
Keep babywarm. The babywho is cryingor breathingwell should be placed skin-to-skin, proneon themother’sabdomenwith the baby’s head cranially and turned to the side. This keeps the babywarm andhelps the baby tobreatheandfacilitatesearlyinitiationofbreastfeeding.Keepthebabycoveredwithawarmclothandwiththecaponthehead.
Recheckbreathing.Continuetocheckthebaby’sbreathingwhilethebabyisonthemother’sabdomen.Mostbabieswhocryatbirthcontinuetobreathewell.Somebabieshavealargeamountoffluidintheirmouthandnose.Positionthesebabiesontheir side tohelpdrain the fluid.Thebaby’sneckshouldbe in theneutralposition–not flexedorhyperextendedtofacilitatedrainageofexcessfluidfromthemouthandnoseaswelltofacilitatebreathing.
CLAMPANDCUTTHECORD.
Delayclampingandcuttingofthecordfor1-3minutesinthenewbornwhoisbreathingwell.Delayingcordclampingforatleastoneminuteoruntilthecordstopspulsatingimprovestheironstatusofthebabyfornext3–6months.Inpreterm infants, delayed cord clamping to 3minutes improves blood pressure and results in a lower incidence ofintra-ventricular haemorrhage, periventricular leukomalacia, late onset sepsis and fewer blood transfusions.Randomized control trials found that there was NO correlation between delayed cord clamping and hyper-bilirubinaemia.(10,11,12)

17
Keepthenewbornonthemother’sabdomenorattheleveloftheperineumwhilewaitingtocutthecord.Tocutthecord,placetwoclampsonthecord,withthefirstclampplacedtwofingersawayfromthebaby’sabdomenandthesecondclampthreefingersawayfromthefirstclamp.Usesterilescissorstocutthecordbetweentheclamps.Keepthebabyskintoskinandencouragebreastfeedingandroutinecare.
Watch Global Health Media Video, Routine care in the first hour of birth:https://globalhealthmedia.org/videos/
ROUTINECAREOFBABIESBORNBYCAESAREANSECTION
BabiesbornbyCaesareansectionrequirethesameinitialstepsofcare,butusuallyrequireassistancewithtransitionmorefrequently:
PREPARATION
• Find out why themother is having a Caesarean section, the gestational age and condition of the foetus, anymaternal illness that may affect the baby, and whether steroids were given to the mother in the case of apretermdelivery.
• Prepareforthetransitionandresuscitation.o Identifysomeonetoassistwiththetransition,andanadditionalpersontohelpwithresuscitationo Discussthefollowingwiththesurgeonandanaesthetist
§ Thepossibilityofdelayedcordclampingormilkingthecord§ Ifthebabymaybekeptskintoskinwithmomordadafterbirth§ Timingofinitiationofbreastfeeding
o Preparethetheatre,checkthetheatretemperatureandeliminateanydraughtso Preparetheemergencyandtransportequipmento Speaktothemotherandbirthcompanionaboutwhattoexpect
TRANSITION
• Drythebabythoroughly,placeacapontheheadandkeepwarm• Ifthebabydoesnotneedhelpwithbreathing,andthemother’sconditionallows,clampandcutthecordafter1
–3minutes,otherwiseclampandcutthecordimmediatelyandinitiateresuscitation.• Keepthebabywarm,eitherskin-to-skinwiththemotherorfather,orunderapre-warmedradiantwarmerorin
awarmedtransportincubator.• Monitor thebabytoensurethebaby isbreathingwell,andkeepthetemperatureof thebabybetween36.5oC
and37.5oC.
ROUTINECAREOFPRETERMBABIES
Preparefortheprematurebabyinthesameway,butanticipatethatthebabymayneedassistanceinbreathing,andmayneedextrasupporttomaintainwarmth.
Babieswhoare<32weeksgestationor<1,5kgareatahigherriskofhypothermia.Inordertopreventthiscomplicationofpretermdelivery,thesebabiescanhavetheirbodyplacedinapolyethylenewrappingoropenbagwhilestillwet(beforedrying)andthenbeplacedunderaradiantheater.DONOTcovertheface.Theheadmayhoweverbewrappedinpolyethylene.Monitorthebabyclosely.Ifyouarenotabletocarefullyapplythisprocedureandmonitorthebaby’stemperature,itmaybesafertodrythebabyandthenplaceskintoskinwiththemotherorfathertokeepthebabywarmortoplacethebabyinatransportincubatorpre-warmedto35,5oC.

18
MONITORBABYWITHMOTHERANDINITIATEBREASTFEEDING
Aftercuttingthecord,movethebabyclosertothemothers’breasts,andmonitortoensurethatthebabyisactiveandbreathingwell.
RAPIDLYASSESSTHEBABYIMMEDIATELYAFTERBIRTH
Rapidlyassessthebabyimmediatelyafterbirth.Reviewthechart“B.RapidlyAssessBabyImmediatelyAfterBirth.”SourcedfromtheEssentialNewbornCareChartBook.
Explain to themother and birth companion that you are rapidly assessing that the baby for any serious illness orabnormality,andifnonearefoundthatthebabywillhaveamorethoroughassessmentinthepostnatalward.
Inordertoassessthebaby,ask,listenandfeel
• ChecktheApgarscoreat1and5minutesanddocumentyourfindings.IstheApgar<8at5minutes?
• Observethebreathing:isthereanyfastbreathing,cyanosis,gruntingorchestin-drawing?
• Observethebaby’stoneandmovement:Isthebabyhypoorhypertonicandisthebabyactiveandmovingalllimbswell?
• Isthereamajorabnormality?Istheheadlarge?Ifsomeasuretheheadcircumference?Isit>39cm?
• Whatisthegender?Isthebabyaboyorgirlorareyouunsure?
• Estimatethebaby’sweight,isit<2kg?
• Isthemotherdiabeticordoesthebabyweighmorethan4,5kg?
Inawellbaby,theApgarscorewillbemorethan8at5minutes.Thebabywillalsobebreathingwellwithgoodtone;nomajorabnormalities;withdistinctmaleor femalegenitaliaanda weightof 2-3,9kgandhavebeenborn toanotherwisehealthymother.
Thereafter
• Keepthebabyskintoskinwiththemother.Thisisimportantformanyreasons,includingkeepingthebabywarmandbreathing,supportingbondingandenablingbreastfeedinginthefirsthour.
• Youwillseehowababycancrawltobreastfeedandwillbeabletoprovidesupporttothemothertoenablefeeding.
• Aftertheinitialfeed,weighthebaby,measurethelengthandtheheadcircumference,anddocumentyourfindingsandthecareyouprovide.
• AdministerVitaminK1mgIMandChloramphenicoleyeointmentintobotheyes.
• Checkifthemotherisdiabeticorifthebirthweightis>4.5kg,ifsochecktheglucosehourlyforthefirst6hours and breastfeed hourly or give 3ml/kg of breastmilk or replacement feed every hour for the first 6hours.

19
• Check if themother is HIV positive, if sowhat treatment she is getting and initiate the first dose of ARVprophylaxistothebabyaccordingtothecurrentPMTCTstandardguideline.
• Identifythebabywiththemotherandplacethenametagsonthebaby’sankle.
• Keepthebabywiththemotherandmaintainskintoskincontactwiththemotherifherconditionallowsit,otherwiseplacethebabyinawarmtransportincubatorandmonitorthecondition.
• Ifthemotherandbabyarewelltransferthemotherandbabytothepostnatalward.Babieswhosemothershavehadacaesareansectionbutwhoarewellshouldreceivecarewiththeirmother,andnotbetransferredtotheneonatalunit.
Ifanyoftheabnormalsignsarefound,thebabyrequiresintervention.Checkthebloodglucose,oxygensaturationandfullyassessthebaby.Keepthebabywarmandmanagethebabyforhypoglycaemia,hypoxia,hypothermiaifthisisfound.IfthebabyisnotwellorissmalltransferthebabytotheNeonatalunitinatransportincubator,afterinitiatinganynecessarycareforhypothermia,hypoglycaemiaorhypoxaemia.
Ifthebabyweighs<2kgortheheadcircumferenceismorethan39cm,thebabywillneedcareintheneonatalunit,butthebabycanremainskintoskinwiththemotherifthereisnootherimmediatecarethatisrequired.
AlltheseguidelinesarefoundintheEssentialNewbornCareChartBook.(15)

20
Figure6:RapidlyAssessBabyimmediatelyafterbirth(10)
WatchGlobal HealthMedia Video: Breastfeeding in the first hour for healthworkers:https://globalhealthmedia.org/videos/

21
SELFASSESSMENTQUESTIONS:MODULE2
Answertheassessmentquestionsbeforecontinuingtothenextmodule.Ifyoudonotgetthequestionscorrect,re-reviewthematerialbeforeansweringthequestionsagain.Onceyouhavesuccessfullycompletedthequestionsyoumaymovetothenextsection.
2.1WhenthebabyisdeliveredbyCaeseriansection
☐SuctionallbabiesdeliveredbyCaeseriansection
☐Thecordmustalwaysbecutimmediatelybythesurgeon
☐Thesebabiesrequireadmissiontotheneonatalunit
☐Requirethesameinitialstepsofcare(TRUE)
2.2Babieswhoare<32weeksgestationor<1,5kgareatahigherriskofhypothermia.Whichofthefollowingstatementsiscorrect?
☐Hypothermiacanbepreventedbydryingthebabyandthenwrappingthebabyinpolyethelinewrappingwithoutcoveringtheface.
☐Thedeliveryroomtemperatureshouldbe>25oC.
☐Skintoskincontactdoesnotworkforpretermbabies
☐Suctionallbabiesdeliveredpreterm
ReadthefollowingCasestudyandthenanswerthequestionbelow,
Youareonduty for theatreandare informedaboutanemergencycaeseriansectionforanotherwisewellmother,withfoetaldistress. Youmakeallthenecessarypreparationsandawaitdeliveryofthe infant. Upondelivery,thickmeconiumismixedwiththeliquorandthebabyhasverypoortoneanddoesnotbreathe.Whichofthestatementsbelowiscorrect?
2.3
! Thebabyrequiresvigoroussuctioningthroughthemouthandthenthenoseuntilnomeconiumisvisibleinthemouthorthenose
! Thebabyneedsstimulationtobreatheimmediately! Waitfor1minutetoavoidoverstimulatingthebabyandtoseeifthebabywillbreathespontaneously! Visualizethecordsandsuctiononceforanymeconiumseenbelowthevocalcordswithin20secondsbefore
thebabytakesabreath.(TRUE)

22
MODULE3:HELPTHEBABYWHOISNOTBREATHINGWELL
3.1CLEARTHEAIRWAYANDSTIMULATEBREATHING.
If the baby is not crying or breathing well after drying, help the baby breathe in the first minute. This is a veryimportanttimeandiscalledTheGoldenMinute©byHelpingBabiesBreathe©.
1.CLEARTHEAIRWAY.
Ifafterdrying,thebabyisstillnotcryingorbreathing,positionthebabyonthesideandensurethattheneckisintheneutralpositiontokeeptheairwayopen.Whenthebabyisintheneutralpositionthenosewillbemoreprominentthanboththeforeheadorthechin.Repositionasnecessarytoopentheairway.
If thebabystilldoesnotbreathe,gently suction themouthand then thenosewitha suctiondevice.Themouth issuctioned first to remove secretions closest to the airway. Insert the suction tubing into the side of the mouthadvancingforapproximately3–4cmintothemouth,whilestillvisualisingthetipofthesuctiontubing.Suctioningfortoolongcandamagethemucosaandcausebradycardiaduetovagalstimulation.
2.STIMULATEBREATHING.
Ifaftersuctioningtheairwaythebabyisstillnotbreathing,gentlystimulatethebabyagainbyrubbingthebackfirmly.Donotliftthebabyup,slapthebabyorinjurethebabyinanyway.
IFTHEBABYDOESSTARTBREATHINGAFTERSTIMULATION,CONTINUETOOBSERVETHEBREATHINGTOMAKESURETHATADEQUATEBREATHINGISSUSTAINED.
3.PLANFURTHERCARE
Somebabieswillhave shallow, irregular, slow,noisyorabsentbreathing immediatelyafterbirth.Othersmayhavechestindrawingandgrunting.Thesebabieswillrequirefurthercare.
Thereare3categoriesofbabiestoconsiderandmakeplansforfurthercare.
Ifthebabyisnotbreathingatallorisgasping,youwillneedtobeginventilationwithabag-valve-maskimmediately.Quickly clampand cut theumbilical cordbeforemoving thebaby to the area for resuscitation (clean, flat surfaceunder a radiantwarmer,with good lighting, prepared and checked prior to the birth) to begin BVM ventilation. Adelayinventilationmayresultinapreventabledeathorbraindamage.Inthisscenario,ventilationclearlyhaspriorityoverdelayinclampingoftheumbilicalcordandisdescribedindetailbelow.
Ifthebabyisbreathingbutiscyanosed,breathingtoofast(>60breathsperminute)orgruntingwithchestindrawing,takethebabytotheresuscitationareaandassesswhetherthebabyneedsoxygenandfurthercareornot.Beginbychecking theoxygen saturationof thebaby,using apulseoximeterwithaneonatalprobe, and then checking thesaturationagainsttheageofthebabyinminutes(table2).Ifthesaturationisbelowthetargetrange,oxygenshouldbe adminstrered by face mask or nasal prongs. Generally, if saturation is less than 90%, oxygen should beadministered.
Ifthebabyisprematureorweighslessthan2000gandhasrespiratorydistress,hemayneedearlyinitiationofnasalCPAP,whichisbest,administeredintheneonatalunitassoonaspossible.
All such babies will require referral to the neonatal unit for close monitoring including monitoring of oxygensaturation.Donotforgettospeaktothemotherandthebirthcompanionaboutthebaby’sconditionandtoexplaintheplanforthebaby’sfurthercare.

23
.
Table2:Targetoxygensaturationimmediatelyafterbirth
Timefrombirth Targetoxygensaturations1minute 60–70%2minutes 65–85%3minutes 70–90%4minutes 75–90%5minutes 80–90%10minutes 85–90%
Term>24hrs >96%Preterm>24hrs >90%
3.2VENTILATEWITHBAGANDMASK
Ventilationwithabag-valve-maskdeviceisforbabieswhostillhavenotinitiatedbreathingafterstimulation.Ventilationhelpscarryairintothelungsandinsodoing,initiatethetransitionneededtoallowspontaneousbreathing.Delayinstartingventilationcanresultinseriousinjurytothebrainastheresultoftissueanoxia.Aimtoinitiateventilationwithin60secondsofbirth,orwithinthe“goldenminute℠”.
Ventilationwithbagandmaskisthemostimportantandeffectivewaytohelpthebabywhoisnotbreathingorisgasping.Ventilationopensthelungswithair.
INITIATEVENTILATIONWITHABAG-VALVE-MASKStandbehindthebaby’shead.Thisenablescontroloftheheadpositionandvisualisationofchestmovementwithventilation.Selectthecorrectmask.Themaskshouldcoverthebaby’schin,mouth,andnose,butnottheeyes.Themaskshouldmakeatightsealonthefacesothatairwillenterthebaby’slungsandnotescapesunderthemask.Amaskthatistoolargewillnotsealwellontheface.Airwillescapeunderthemask.Amaskthatistoosmallwillnotcoverboththemouthandnoseandmayblockthenose.Airwillnotenterthelungsfreely.Asageneralguide,atermbabyusuallyrequiresamasksize1andapretermbabyamasksize0.Positiontheheadintheneutralposition(avoidover-extension).Helpkeepthebaby’sairwayopenbypositioningtheheadintotheneutralpositionandsupportingthechin.Positionthemaskontheface.Positiontherimofthemasktorestonthetipofthechin,andthenplacethemaskovermouthandnose.
Formafirmsealbetweenthemaskandthefacewhilesqueezingthebagtoproduceagentlemovementofthechest.Holdthemaskonthefacewiththethumbandindexfingerontopofthemask.Usethemiddlefingertoliftthechinuptowardthemask.Usethe4thand5thfingersalongthejawtoliftitforwardandhelpkeeptheairwayopen.Formatightsealbypressinglightlyonthetopofthemaskandgentlyholdingthechinuptowardthemask.Ifthesealisnottight,youwillnotmoveairintothelungsasyousqueezethebag.Theairwillescapeundertherimofthemask.Donotpushthemaskdownontotheface.Thismaychangetheheadpositionandinterferewithaerationofthelungs.

24
Figure7:Twopointholdoffacemask
Ventilatebysqueezingthebagtoproduceagentlemovementofthechest,asifthebabyweretakinganeasybreath.Makesurethereisnoleakbetweenthemaskandthebaby’sface.Squeezethebagharderifyouneedtodelivermoreairwitheachbreath.Forthefirst5breaths,maintaintheinflationpressurefor2–3seconds.Thiswillaidlungexpansion.Thereafterventilateatarateofabout30-40breathsperminute.Thiscanbeachievedbycountingaloud;“Bag…two…three…Bag…two…three…….”Ifyousqueezethebagasyousay,“Bag,”andreleasewhileyousay,“two…three,”youwillventilateatthecorrectrate.
Ventilatethebabywithroomairandnotoxygen.Theefficacyoftheventilationcanbeseenbyarapidincreaseintheheartrateandobservingchestrisingandsomeabdominalrising.
EVALUATETHEBABYDURINGVENTILATIONBYASKING:ISTHEBABYBREATHINGWELL?
Mostbabiesrequiringventilationatbirthwillrespondwithin30secondsofventilation,andthenbeginbreathingwell.Stopventilationwhenthebabystartstobreathewell.
Otherbabiesrequirecontinuedventilationwithbagandmask.Suchbabiesmayhavegaspingrespirationseenasasingledeepfutilebreathingmovement,followedbyalongpauseorseveraldeep,irregularbreathingmovementsfollowedbyapause.Continueventilationwithbagandmaskinthisscenario.
.
3.3IMPROVEVENTILATIONIFTHEBABYISSTILLNOTBREATHINGWELL
Ifthebabyisnotbreathing,continueventilationandcallforhelp.
Inthemeantime,checkthatventilationbreathsproducemovementofthechestasifthebabywerebreathingnormally.Takestepstoimproveventilationifthechestisnotmoving.
Mouth:- Checkthemouth,thebackofthethroat,andthenoseforsecretions,andclearasnecessary.- Openthebaby’smouthslightlybeforereapplyingthemask.- Reattemptventilation
Head:
- Reapplythemasktothefacetoformabetterseal.- Repositiontheheadwiththeneckintheneutralposition.Inordertoachievethis,onecanplaceacloth
underthebaby’sshoulders.

25
- Reattemptventilation
Consideranalternativeairway-Insertanoralairway,oranasopharyngealtube,orintubate.
Anairleakunderthemaskorincorrectpositionoftheheadisacommonreasonforpoorchestmovement.Ifyoustilldonotseegentlemovementofthechest,trytofindtheproblemandrepeatthenecessarystepstoimproveventilation.Recheckthefunctionoftheventilationbag.Replaceitifanotherbagisavailable.
WatchtheLINCvideo:Bagandmaskventilationavailableonwww.lincare.co.za
WatchtheLINCvideo:Improveventilationavailableonwww.lincare.co.za
SELFASSESSMENTQUESTIONS:MODULE3
3.1 The one most important skill that is required by health workers to help a baby breathe is (choose 1 correctanswer)
☐Correctlyapplynasalprongsforoxygenadministration
☐Intubation
☐Bagandmaskventilation(CORRECT)
☐Cardiaccompression
3.2Toensurethatallbabiesbreathewithin1minuteofbirth(GOLDENMINUTE),whichstepiscorrecttotake?
☐Cuttheumbilicalcordimmediately
☐Ifbabydoesnotcryimmediatelystimulate,positionairwayandcheckbreathing(CORRECT)
☐Ifbabydoesnotbreathecommencebagandmaskventilationby2minutes
☐Administeroxygenviaendotrachealtubeifbabydoesnotbreatheby60seconds
3.3Tosuccessfullybagandmaskventilatethebabydothefollowing,exceptfor
☐Standorsitatthebaby’sheadandselectthecorrectmask
☐Positionthemaskonthebaby’sface,makeafirmsealbetweenthemaskandthefaceandgentlysqueezethebag
☐Ventilatethebabyatabout20breathsperminute(FALSE)
☐Watchthechest/abdomenformovement

26
MODULE4.ADVANCEDRESUSCITATION
Ifthebabyisstillnotbreathingafterbagandmaskventilationandcheckingthatthisiseffective,youwillneedtostartadvancedresuscitation.Advancedresuscitationreferstotheadditionofchestcompressionsanddrugstohelpthebabytorecover.Beforeproceeding,takesometimetoreviewthepathophysiologyonbirthasphyxia.
4.1PATHOPHYSIOLOGYOFBIRTHASPHYXIA
If subjected tohypoxia inutero, the foetuswill start gasping. If thehypoxic insult is sustained, the foetuswill loseconsciousness. The neural centres controlling the breathing efforts ultimately cease to function because of lack ofoxygen.Asaresult,thefoetusthenentersaperiodknownasprimaryapnoea.Theheartrate,whichwasunchangeduptothispoint,nowdecreasestoabouthalfthenormalrateandthemyocardiumrevertstoanaerobicmetabolism.Thecirculationtonon-vitalorgansisreducedinanattempttopreserveperfusionofvitalorgans.Lacticacid,theresultofanaerobicmetabolismofglucoseisproduced,andcausesmetabolicacidosis.
If the insult continues, the primitive basal gangliainitiategaspsatarateofabout12gaspsperminute.If the foetus is still in utero, or if for some otherreasonthesegaspsfailtoaeratethelungs,thegaspsgradually fade away until the foetus enters a periodknownassecondary,or terminal,apnoea.Untilnow,the circulation has been maintained, however, asterminalapnoeaprogresses,therapidlydeterioratingbiochemical milieu begins to impair circulation byhinderingcardiacfunction.Thehearteventuallyfails,in both frequency of contraction and contractility.Without effective intervention, the baby dies. In aterm newborn, the entire process takesapproximately20minutes.
It is important to note that, in the face of asphyxia,the baby is able maintain an effective circulation.From the period of primary apnoea, through thegaspingphase,andevenforawhileaftertheonsetofterminal apnoea, circulation ismaintained. Thus, themosturgentrequirementofanyasphyxiatedbabyatbirth iseffectiveaerationof the lungs.Provided thebaby’s circulation is sufficient, oxygenatedbloodwillbeconveyedfromtheaeratedlungstotheheart.Theheartratewillincreaseandthebrainwillbeperfusedwith oxygenated blood. Following this, the neuralcentresresponsiblefornormalbreathingwill,inmanyinstances, function once again and the baby willrecover.
Figure8:Sequenceofeventsfollowingbirthasphyxia(1)

27
ReviewFigure8.ThisfiguresummarisesthechangesinHR,BP,pHandthepatternofgaspingrespirationattheonsetofasphyxia.Thefigurealsodemonstratestherecoverywiththeinitiationofresuscitation.
Merelyaeratingthelungsissufficientforrecoveryinthevastmajorityofcases.Althoughlungaerationisvital,thereareafewcasesinwhichcardiacfunctionwillhavedeterioratedtosuchanextenttoresultininadequatecirculation.Aninadequatecirculation(identifiedbyaslowheartrateoflessthan60beatsperminute)cannotconveyoxygenatedblood from the aerated lungs to the heart. In this scenario, a brief cycle of chest compressionmay be necessary.Furthermore,inveryfewcaseslungventilationandchestcompressionalonemaynotbesufficient,withtheneedfordrugs to restore the circulation. The outlook in this small group of infants is generally poor. Themanagement ofbabieswhorequirechestcompressionsanddrugsoverandaboveeffectivebagmaskventilationisdiscussedindetailbelow.
WatchtheLINCvideo:Pathophysiologyofperinatalasphyxia.www.lincare.co.za
4.2ADVANCEDCARE:HEARTRATE
Thealgorithmforadvancedresuscitationbeginswithassessmentoftheheartrateinababywhohasbeenventilatedeffectively,butfailstobreathespontaneouslyand/orfailstorestoreheartratetomorethan60beatsperminute.Ifababydoesnotbegintobreathespontaneouslyafter1minuteofeffectiveventilation(withchestmovement),evaluatetheheartratetodecideifventilationaloneissufficient.Askyourselfthequestion:Istheheartratenormalorslow?
Toevaluatetheheartrate,palpateforumbilicalcordpulsationorlistenforaheartbeatwithastethoscope.Palpateorlistenjustlongenoughtorecognizeiftheheartrateisnormalorslow.Iftheheartrateisfasterthanyourown,itismostlikelynormal.Iftheheartrateisslowerthanyourownpulse,thenitisslow.
Intheresuscitationsetting,itisimportanttocommunicateinformationabouttheheartratequickly.Asanaide,feelforapulseintheumbilicalcordorauscultateandthen“tapwhatyoufeel”onahardsurfacetogetabettersenseofthepulserate
WatchtheLINCvideo:Checkthepulserate.www.lincare.co.za
IFTHEHEARTRATEISNORMAL
If theheart rate is normalwhile youprovideeffective ventilation; continue to ventilateuntil thebaby isbreathingspontaneously.Graduallyreducetherateofventilationwhileobservingthebaby’sbreathing.Iftheheartrateremainsnormalasthebabybreathesspontaneouslyandregularly,stopventilation.
Ventilation canbe stoppedwhen thebaby isbreathing spontaneouslyand regularlywhilstmaintaininganormaltheheartrate(morethan100beatsperminute).
Iftheheartrateisnormalandthebabystilldoesnotbreathe,checkwhetherthemotherreceivedpethidineoranyopioids,inthepreceding4hours.Ifpethidineoranyopioidsweregivenandthebabyisnotbreathing,thebabymayneednaloxone (Narcan®). Ababywhohasanormalheart ratebutdoesnotbreatheneedscontinuedventilation.Slowly decrease the rate of ventilation over several minutes to see if there is a return of normal, spontaneous

28
breathing.Ifthebabystilldoesnotbreathe,continueventilationandconsultaspecialistwiththeviewofinsertinganalternativeairway.
Ifthebabyisbreathing,butbecomesbluewheneffectiveBVMventilationisdiscontinuedorifthebabyisbreathingandlookscyanosed,checktheoxygensaturationandifnecessarygivesupplementaloxygen.Supplementaloxygencanbeadministeredthroughaheadbox,nasalprongsorcatheter.
Assessthenewbornsresponsetooxygenbymeasuringthepre-ductalsaturation.Pre-ductalsaturationismeasuredbyputting thepulseoximeterprobeon therighthandof thebaby. Targetoxygensaturations fornewborns fromthetime of birth are presented in table 2. Regardless of gestation, the goal of oxygen administration is an oxygensaturation resembling that of a healthy term newborn. High concentrations of oxygen have been associated withincreasedmortality,anddonotimproverecoveryfromasphyxia;infact,thecontrarymightbetruewithdelayintimeofonsetofspontaneousrespiration.Provideaslittleoxygenaswillbenecessarytokeepthesaturationat90%.Youcan add a venturi (60%, 40%, and 28%) to modify the percentage of oxygen provided. Compare the pre-ductalsaturation with the post-ductal saturation, as a difference in saturation of more than 15% may be indicative ofpersistent pulmonary hypertension of the newborn. Reduce or stop oxygen if the newborns oxygen saturation isabove90%atanypointinthefirst10minutes.
Ifthebabyhasseverechestin-drawing,veryfastbreathing,grunting,orfrequentpausesinbreathing(longerthan15to20seconds)thebabyrequiresnasalCPAPtosupporttheaerationofthelungs.TransferthebabytotheNeonatalunitwherethiscarecanbeinitiated.
Ofnote: If thebabyshowsregularbreathing,andhas lowoxygensaturation,anddoesnot improveonoxygen(i.e.thereisnoincreaseinsaturation),thebabymayhaveacongenitalheartlesionwitharight-to-leftshunt.
Allbabieswhohaverequiredbagandmaskventilationwillrequireclosemonitoringintheneonatalunitafterwards.
Speaktomotherandthebirthcompanionaboutthebabyandtheplanofcare.
ADVANCECARE:SLOWHEARTRATE,CHESTCOMPRESSIONANDDRUGS
Iftheheartrateisslow,makesurethatyouhavetakenallthestepstoimproveventilation.Aslowheartrateisasignof hypoxaemia, which ismost often the result of inadequate ventilation. If the chest is notmovingwell youmayconsideranalternativeairway,orintubation.
Ifventilationseemsadequateandthechestismovingwell,withaslowheartrate,youwillneedtoprovidecirculatorysupport.Startchest compression, to improve thecirculation. Ifyouaregoing toadministerchestcompression it isusuallybesttointubatethebabyfirstandventilateviatheendotrachealtube.
CHESTCOMPRESSION
Circulatory support with chest compressions is only effective if the lungs are successfully inflated. Give chestcompressionsiftheheartrateislessthan60beatsperminute.Forthistobesuccessful,oneneedsaskilledhelper.
Therearetwotechniquesforchestcompression.Firstly,youmayusethe2-fingerorsecondlythe2-thumbmethod.The2-thumbmethodisthemosteffective:gripthechestinbothhandsinsuchawaythatthetwothumbscanpressonthelowerthirdofthesternum,justbelowanimaginarylinejoiningthenipples,withthefingersoverthespineattheback.(Figure9)
Compressthechesttoadepthof1/3theAPdiameterofthechest. Count1,2,3Bag,1,2,3Bag(3compressionstoeachbreath).Asateam,onehealthcareproviderwillcompressthebagtoprovideventilationandtheotherhealthcare providerwill do chest compression. By definition, the leader is the health care providerwho is bagging andshouldthereforebetheoneresponsibleforcounting.

29
Chest compressions move oxygenated blood from the lungs back to the heart. Allow enough time during therelaxationphaseofeachcompressioncycle for theheart to refillwithblood.Ensure that thechest is inflatingwitheachbreath.Continuechestcompressionsforatleastoneminuteandthenevaluateheartrateagain.Ifthereisstillbradycardia,thencontinuechestcompressions,andpreparetoadministeradrenalin.
In less than one per thousand births, effective ventilation and effective chest compression will be insufficient toproduceaneffectivecirculation.Inthisscenario,administeringdrugsmaybehelpful.
Figure9:Chestcompression,a)2-thumbandb)2-fingermethod
IFHEARTRATESTILLSLOW,GIVEADRENALINE
Bradycardiausually followshypoxiadue to inadequateventilationandoxygenationof thebrainstem,with resultingapnoea.Establishingadequateventilationisthemostimportantinterventiontoimproveheartrate.If,however,theheartrateremains lessthan60beatsperminutedespiteadequateventilation,administeringadrenaline isthenextmostimportantsteptoimproveheartrate.
Adrenaline is to be administered if the heart rate is less than 60 beats per minute after oneminute of effectiveventilationwithchestcompression.Adrenalinisbestadministeredviaanumbilicalvenouscatheter.Seethesectionbelowoninsertingofanumbilicalvenouscatheter.Alternativeaccessisviaanendotrachealtube,peripheralvein,orintraosseousline.
Prepareadrenalinbymixing1mlof1 in1000adrenalinewith9mlofSalinetoget1 in10000Adrenalinesolution.Administer 0.01-0.03mg/kg (equates to 0.1-0.3mL/kg of 1 in 10 000 adrenaline).Give as a rapid bolus followedby0.9%SodiumChlorideflushofequalvolume.
Alternatively,ifresuscitatingatermbaby,drawup1mLofAdrenalineandadministeritallintravenously.Ifthebabyis 27–32weeks gestation, thengive0.25ml, if 33–37weeks give0.5ml and if 38–43weeks thengive1mlofadrenalinperCPRcycleof1-2minutesduration.
IfadrenalinistobegiventhroughtheETtube,thedosesofadrenalinemustbe3timeshigherthantheintravenousdoses. Follow administration of ET tube adrenalinwith positive pressure ventilation to ensure that the AdrenalinedoseisventilatedintothelungsandisnotleftintheETTortheadaptor!.
Repeatevery1-2minutes,iftheheartrateremainslessthan60beatsperminute.Seesectionorwhentodiscontinueorwithhold lifesupportbelow. (Andcontinue forhow long?)IfanETTdose isadministeredwith inadequateeffect,giveanIVdoseassoonasvascularaccessisobtained

30
WHENWOULDYOUGIVEAFLUIDBOLUS?
If,inaterminfant,thereissuspectedbloodlossortheinfanthasclinicalsignsofshock(pallor,poorperfusion,weakpulse, increased capillary refill time) and has not responded adequately to other resuscitation measures, thenconsidergivingabolusof fluid.Givean initialbolusof10ml/kgofNormalSaline intravenously. Ifeffective, itmayneedtoberepeatedtomaintainimprovement.Inpretermbabies,volumeexpansionisrarelyneeded,andhasbeenassociatedwithintraventricularandpulmonaryhaemorrhages.
WHENWOULDYOUUSEBICARBONATE
There is insufficient data to recommend the routine use of bicarbonate in the resuscitation of the newborn.Bicarbonate is not recommended during brief Cardio Pulmonary Resuscitation (CPR). It may be considered duringprolonged cardiac arrests unresponsive to other therapy. It should only be given after adequate ventilation andcirculationisestablishedwithCPR.TheuseofbicarbonateshouldbelimitedtocaseswhereanABGhasbeendonetoguidecorrectdosingofbicarbonate.
4.3ENDOTRACHEALINTUBATION
Asdiscussed inthe introductiontothiscourse, bagandmaskventilation isusuallyadequatetoventilatethebaby.However insomecircumstances,ET intubation isunavoidable. Endotracheal intubation is indicatedwhenthebabyneedsadvancedcarewithchestcompressionsandadrenalinorwheneffectiveventilationwithbagandmaskfails.
In summary, a decision to perform endotracheal intubation will depend on the newborn’s gestation, degree ofrespiratorydepression,responsetofacemaskventilation,and,ofcourse,theskillandexperienceoftheresuscitator.
Only clinicians with appropriate training and experience in the procedure should attempt neonatal endotrachealintubation. If successful intubation cannot be achieved within 20 seconds, then continued positive pressureventilation(PPV)viaafacemaskisrecommended.
Ifthereisnohealthcareproviderskilledinintubationpresent,continuepositivepressureventilationviaafacemask,andwaitforaskilledhelper.
INDICATIONS
• Trachealsuctioninginanon-breathingandfloppynewbornexposedtomeconiumstainedliquor*• Unsuccessfulventilationviaa facemask(e.g.heartrateremainsslow,oxygensaturationfallingor failingto
riseorprolongedapnoea)• Administrationofendotrachealmedications(e.g.adrenalineorartificialsurfactant)• Expectedneedforcontinuedorprolongedventilationandchestcompression
WHATISNEEDED
• Straightbladedlaryngoscopewithabrightlightthathasbeencheckedo Millerbladesize00orsize0
• Suctionapparatusthathasbeenchecked• ETtube
o sizes2.5to3,5(see:table1)o Donotusesize2.0tubesorshoulderedtubes.
• McGillforcepswithlubricatingjellyfornaso-trachealintubation• Guidewirefororo-trachealintubation(makesurethattheguidewiredoesnotprotrudeoutsidethetube,as
thismaycausetrachealperforation).

31
• Strappingsforsecuringthetube
POSITIONINGOFTHEBABY
• Placethebabyontheresuscitairewiththeheadtowardsyou.• Ensurethehead is inneutralposition.Flexion,andhyperextensionblockvisualisationofthevocalcords.A
smallclothplacedundertheshoulders,orundertheneck,mayhelpwithadequatepositioning.
TECHNIQUE• Toobtaingoodvisualisation,theoropharynxshouldbegently,albeitadequately,suctioned.• Fornasalintubation,introduceETtube,afterlubrication,intoonenostrilandadvanceittoapositionbeyond
thepalate.• Holdingthelaryngoscopeinyourlefthand,introducethebladeintotherightsideofthemouth,movingthe
tonguetotheleftasthetipofthebladeisadvancedintothevallecula.Thevalleculaisthespacebetweentheepiglottisandthebaseofthetongue
• Gentleverticalpressureofthe laryngoscope,witha littlepressureonthecricoid,willbringthevocalcordsintoview.
• VisualizetheETtubeandgrabitwiththetheMcGillforcepsbeforeadvancingthetubeapproximately1cmbeyondthecordsintothetrachea.
• Verifyequalandbilateralairentrybyauscultatingbothaxillaewhileventilatingwithabagandmask.• SecuretheETtubepositionwiththehelphelpofanotherhealthcareprovider.• Ventilatingwithaventilationbag.
Figure10:NeonatalIntubation

32
ETTTUBESIZE
ETTsizeandinsertionlengtharebasedonthenewborn’sweightandcorrectedgestation.ETTinternaldiametercanbecalculatedusingtheformulaofgestationalageinweeksdividedby10.
ApproximateETTinsertiondepthfromthemiddleoftheupperlipcanbecalculatedusingtheformulaofweightinkg+6cmandfornasotrachealintubation,weightinkg+1cm.
Table3:ETTtubesizeandlength
Weightinkg ETTmarkatupperlip(cm)
ETTinsidediameter(mm)
ETTsuctioncathetersize(F)
<1kg 6.0 2.5 5or61.1–1.9 7.0 3.0 6or82.0–3.0 8.0 3.5 8>3kg 9.0 3.5 8or10
POSITIONVERIFICATIONo ETT insertion depth must always be checked by comparing the markings on the tube with the formula or
tabulatedfindings.o Primarily,correctETTpositionisconfirmedbyeffectiveventilationasdemonstratedby:
o Chestrisewitheachinflationo Heartrateincreasingtoabove100bpmo Improvingoxygenation(oximetryismoreaccuratethanvisualassessment,althoughfalsenegativesmay
occurinnewbornsifthereisveryloworabsentpulmonarybloodflow)
Onlyperformintubationforthepurposeofsuctioningmeconiumfromthetracheainnewbornswithdecreasedmuscletone,immediatelyafterbirthandbeforetheonsetofbreathing or crying. An experienced clinician should be the one to perform theprocedureandeventhen,onlyifalltheequipmentrequiredisimmediatelyavailable.In this scenario, suctioning should only be done once followed by rapidcommencementofresuscitationasrequired
WatchLINCvideo:Endotrachealintubation(www.lincare.co.za)

33
4.4UMBILICALVEINCATHETERISATION
Whenintravenousaccessisrequiredintheemergencysituation,insertionofanumbilicalveincathetercanfacilitaterapidaccess
INDICATIONS
• Duringresuscitationifquickivaccessisindicatedforexamplefor:o Toadministerabolusoffluidsforvolumeexpansiono Toadministeradrenalineo Topreventor,correctseverehypoglycaemia
• Ifivaccessisdifficult• Inpreparationforanexchangetransfusion
WHATYOUWILLNEED
Ideally,asterilepackcontaining
• Size5FGsterilenasogastrictubeorumbilicalveincatheter• Sterileswabs• Sterilescalpelandblade• Umbilicalcordties• Strapping• NormalSalineampoule• 5mlsyringe• Arteryforceps
STERILEUMBILICALVEINCATHETERISATION
• Positiontheinfantunderaradiantwarmerwithgoodlighting• Putonamask,washyourhandsthoroughlyandputonsterilegloves.• Attachthecatheter/nasogastrictubetoasyringecontainingsalineandflushit(alsoeliminateanyfreeair)• Cleantheumbilicalcordareawithspirits• Placeasteriletowelaroundtheumbilicus• Placetheumbilicaltape1cmabovetheabdominalskinandtieloosely• Cutthecord2cmabovetheskin• Identifytheumbilicalvein:thereisoneumbilicalveinandtwoumbilicalarteries,withtheveinsituatedat
thetop(towardsthebaby’shead)andthetwoarteriesbelow.• Insertthetipofthesalinefilledcatheterornasogastrictubeintotheveinandadvancewhileaspiratinguntil
blood return is seen. Inserting the catheter 1-2cm beyond this point is an appropriate position for theemergencyusewithoutradiographicconfirmationofposition.
• Securelystraptheumbilicalcatheterinplace.Rugbypoststrappingworkswell.• Youcanreplacethesyringewithanintravenousgivingsetor3waytapifyouneedtogivemedications
PRECAUTIONS
• Bleedingifthebaseofthecordisnotsecuredtightly• Ensurenot toallowair tobe introduced into thecatheter, this iswhyyou fill thecatheterwithsalineand
leavethesyringeattached.Ifyouseeairinthecatheter,withdrawontheenduntilthereisnoairandreplacesyringe

34
• Don’tgivehypertonicsolutions(e.g.50%glucoseand8%sodabicarbonate)throughthecatheter• Portalveinthrombosismaycomplicateumbilicalveincatheterization• Donotinsertanumbilicalveincatheterifitispossibletoinsertaperipheralveininfusion
Figure11:Umbilicalvenouscatheterisation
4.5WHENTOWITHHOLDORDISCONTINUELIFESUPPORT
The decision towithhold or discontinue life support is not an easy one. The decision largely depends on theavailabilityofresourcesandonyourexpectationofthefunctionalsurvivalofthebabybeingresuscitated,giventheresourcesintheregioninwhichyouwork.Thedecisionisnoteasy,andonemustbeawarethattheparentsmaywanttobeinvolved.Themostseniorhealthworkeravailableshouldassistwiththedecisionmaking. Youmaywanttoconsultthepaediatricianatyourreferralhospital.Thefollowinggeneralguidelinesmayassist:
• If the baby has no heart rate after 10 minutes of ventilation it is appropriate to consider stoppingresuscitation,asdisabilityfreesurvivalisunlikely.
• Whenthepossibilityoffunctionalsurvivalishighlyunlikelysuchaso Extremeprematurityo AbnormalitiessuchasanencephalyorTrisomy13or18
• Ifthereisnobreathingeffortwhatsoeverafter20minutes,oronlygaspingrespirationafter30minutes.
Whenwithholdingorwithdrawingresuscitation,talkrespectfullytothefamilyofthebabyandprovidecomfort.

35
4.6POSTRESUSCITATIONCAREOFTHENEONATE
Ifthebabyhasrequiredbagandmaskventilationoradvancedresuscitation,thebabyneedsfurtherimmediatecareandmonitoringandshouldbeadmittedtotheneonatalunitforobservationandfurthercare.
StabilisethebabypriortotransfertotheNeonatalunit
1. Checkbloodglucose.Ababywhohashadasphyxiaandrequiredresuscitationwillneedmaintenanceglucoseandpossiblyadditionalglucose.Establishaperipheralintravenousline,orputupanumbilicalline.Ifthereishypoglycaemia administer 2ml/kg of 10% glucose IV slowly, and in all babies put up Neonatolyte or 10%glucose iv at 2.5 – 3.0 ml/kg/hr. as maintenance. Monitor the fluid intake with an infusion controller orBuretrolandinlineflowregulatingdevice.
2. Keepwarm.Ensurethatthebaby’stemperatureiskeptinthethermoneutralrange.Ifthebabyisprematureensurethebaby’stemperature isbetween36.5and37.5oC. If thebaby isatermbabywithbirthasphyxiakeep the temperature between 35 and 36 oC. Transfer the baby in a temperature regulated transportincubator.
3. If the baby has respiratory distress (central cyanosis, fast breathing, chest – in-drawing, grunting) and theoxygen saturation is less than 90% give supplemental oxygen by nasal prong or face mask. If the babyrequiresoxygen,provideoxygenevenduringtransfer.
Transfer the baby to theNeonatal Unit,where the babywill have a full assessment and receive further care. TheassessmentandcarearedescribedintheNewbornCareCharts:Managementofthesickandsmallnewborn(MSSN).Ane-learningcourseonMSSNisindevelopment.TheNewbornCareChartsareavailablefromwww.lincare.co.za
SELFASSESSMENTQUESTIONSMODULE4
4.1Oxygenadministration(indicatewhichonestatementiscorrect)
☐Isimportantforallbabieswhodonotinitiatebreathingontheirown
☐Isnotnecessaryforinitialbagandmaskventilation,useroomair(CORRECT)
☐Isgiventoallbabieswithmeconiumaspiration
☐Isnecessaryforallpretermbabies
4.2Ifthebabyhasaslowheartrateandisnotbreathing,dothefollowingexcept
☐Intubateimmediatelyandgiveadrenaline(ALLEXCEPTTHIS)
☐Improveventilationwithbagandmaskventilation
☐Ifventilationadequateinitiatechestcompression
☐Ifheartrateremainsslowdespiteadequateventilationandchestcompressiongiveadrenaline

36
4.4.Discontinuelifesupporttothebabyif(choosetheincorrectstatement)
☐Thebabyhasnoheartrateandnobreathingaftergivingventilationfor10minutes
☐Thereisnobreathingeffortafter20minutes
☐Thereisonlygaspingafter30minutes
☐After45minutesifthebabyis“precious”(INCORRECT)
4.5Aftersuccessfulresuscitationwithbagandmaskventilation,youdecidetoadmitababytoneonatalwardforthefollowingmonitoringand/ortreatment,exceptfor:
☐Oxygensaturation
☐Glucose
☐Temperature
☐Antibiotics

37
REFERENCESANDRECOMMENDEDREADING
1. ErsdalHL,MdumaE,SvensenE,PerlmanJM.Earlyinitiationofbasicresuscitationinterventionsincludingfacemaskventilationmayreducebirthasphyxiarelatedmortalityinlow-incomecountries.Aprospectivedescriptiveobservationalstudy.Resuscitation83(2012)869–873
2. PerlmanJM,RisserR.Cardiopulmonaryresuscitationinthedeliveryroom.Associatedclinicalevents.ArchPediatrAdolescMed1995;149:20-25
3. WallSN,LeeAC,NiermeyerS,etal.Neonatalresuscitationinlowresourcesettings:what,whoandhowtoovercomechallengestoscaleup?IntJGynecolObstet2009;107:47–64
4. LeeACC,CousensS,WallSNetal.Neonatalresuscitationandimmediatenewbornassessmentandstimulationforthepreventionofneonataldeaths:asystematicreview,meta-analysisandDelphiestimationofmortalityeffect.BMCPublicHealth2011,11(Suppl3):S12http://www.biomedcentral.com/1471-2458/11/S3/S12
5. KattwinkelJ.Addressinghighinfantmortalityinthedevelopingworld.AGlimmerofhope.Pediatrics.http//paediatrics.aappublications.org/content/early/2013/01/15/peds2012-3171
6. PadayacheeN,BallotDE.OutcomesofneonatewithperinatalasphyxiaatatertiaryacademichospitalinJohannesburg,SouthAfrica.SAJCH2013,7(3):89–94
7. Bruikman,E.K,IntrapartumAsphyxiaandHypoxicIschaemicEncephalopathyinaPublicHospital:Incidenceandpredictorsofpooroutcome.MMEDThesis,Wits18May2015
8. HelpingBabiesBreathe,ProviderGuide,Secondedition.(2016)AmericanAcademyofPediatrics;http://www.helpingbabiesbreathe.org/.
9. WyllieJ,BruinenbergJ,etal.EuropeanResuscitationCouncilGuidelinesforResuscitation2015.Section7.Resuscitationandsupportoftransitionofbabiesatbirth.Resuscitation2015;95:249–263
10. WyckoffMH,AzizK,EscobedoMBetal.Part13:NeonatalResuscitation:2015AmericanHeartAssociationGuidelinesUpdateforCardiopulmonaryResuscitationandEmergencyCardiovascularCare.Circulation.2015Nov;132(18Suppl2):S543-60

38
11. Delayedumbilicalcordclampingafterbirth.Committeeopinionno684.AmericanCollegeofGynecologists.ObstetGynecol2017;129e5–10
12. Weineretal,Part15:NeonatalResuscitation:2010AmericanHeartAssociationGuidelinesforCardiopulmonaryResuscitationandEmergencyCardiovascularCareM.Circulation.2010;122:S909-S919http://circ.ahajournals.org/content/122/18_suppl_3/S909
13. NewbornLifeSupport,ResuscitationCouncil(UK)2010ResuscitationGuidelines
14. NeonatalResuscitation:2010AmericanHeartAssociationGuidelinesforCardiopulmonaryResuscitationandEmergencyCardiovascularCare.http://pediatrics.aappublications.org/content/early/2010/10/18/peds.2010-2972E.citation
15. EssentialNewbornCare2013.NDOH.LimpopoInitiativeforNewbornCare.www.lincare.co.za
16. SinghalN,LockyerJ,FidlerH,etal.HelpingBabiesBreathe:Globalneonatalresuscitationprogramdevelopmentandformativeeducationalevaluation.Resuscitation2011
17. MsemoG,MassaweA,MnbandoDetal,NewbornMortalityandFreshStillbirthratesinTanzaniaafterHBBtraining.PediatricsDOI:10.1542/peds.2012-1795.
18. Little,GA,KeenanWJ,NiermeyerS,SinghalN,LawnJE.NeonatalnursingandHBB:Aneffectiveinterventiontodecreaseglobalneonatalmortality.Newbornandinfantnursingreviews.June2011VolIIno2.www.nainr.com

39
CLINICALPRACTICESESSIONS
Onceyouhavecompletedthereading,arrangeforafacilitatortotakeyouthroughthefollowingdemonstrationsandskillssessions.Yourfacilitatorwilldemonstrateeachstepandyouwillthenpracticeinpairs,beforedoingthefinal2OSCE’s.Satisfactoryperformancesonalltheskillsstationsarerequired.Preparationforbirth
1. Routinecare2. Stimulateandclearairwayifnotbreathing3. Bagandmaskventilation4. Howtoimproveventilation5. Endotrachealintubation6. Chestcompression7. Administrationofdrugsandfluids8. Umbilicalcatheterinsertion9. OSCE110. OSCE2