NEWBORN & 6 WEEK CHECK Kavitha Kanakanti Lydia Scott.
56
NEWBORN & 6 WEEK CHECK Kavitha Kanakanti Lydia Scott
-
Upload
margaretmargaret-collins -
Category
Documents
-
view
214 -
download
0
Transcript of NEWBORN & 6 WEEK CHECK Kavitha Kanakanti Lydia Scott.

NEWBORN &6 WEEK CHECK
Kavitha KanakantiLydia Scott

BRIEF HISTORY
• Any concerns?• Birth Hx – normal/C-section/instrumental, ?
breech, birth wt & HC• FHx of DDH, cataracts• Feeding & wt gain• Wet nappy/meconium (newborn)• Development (6 weeks) – vision, hearing,
smile
GENERAL EXAM
• Dysmorphology• Skin colour• Rashes/birth marks• How they handle when you undress
them• Weight

Dysmorphology

Downs Syndrometypical facial features of Down's syndrome: up slanting palpebral fissures, a suggestion of epicanthal folds, and a flat nasal bridge

Jaundice
Investigation indicated if:• Jaundice at <24 hours• Conjugated hyperbilirubinaemia
(direct bili >20mm/l or >10% total bili)• Prolonged jaundice >14 daysNeed Ix according to hospital protocol
Unconjugated hyperbilirubinaemia may require treatment with phototherapy or exchange transfusion depending on gestation/age of baby

Rashes

Erythema toxicumvery common, completely benign. Seen in about half of newborns. Lesions are erythematous macules, within which papules and pustules develop. Trunk most commonly involved. Resolves spontaneously within 10 days.

MiliaMilia are tiny pearly white cysts that are on the surface of the skin mainly on the face..40% of newborn infants develop it.

Birth marks

Mongolian blue spotCaused by a collection of melanocytes scattered through deep dermis. Most frequently located over the sacral area. Found in Afro-Caribbean or Asian infants & less commonly in Caucasians. Usually present at birth, fade during early years.

Strawberry haemangiomaBright red, well demarcated, compressibleWithin few weeks of birth,10%Spontaneous regression 2- 10 yearsLarge-feeding/visual problems/bleedingReassureHigh dose steroids if indicated

Port Wine StainMacular nevus present at birthPale pink to purpleAssociated Sturge Weber 10%-Orbital with intracranial malformation, C/L hemiparesis, seizures,mental retardationPermanent defect of mature capillaries
Cosmetic camouflage/Laser treatment

Capillary haemangioma(at birth)can occur in variety of sizes, locations, and combinations of capillaries & larger vessels. Simplest form is limited in size, superficial and largely capillary –a Capillary Haemangioma or Strawberry mark.

Capillary haemangioma(at 2yrs of age)

Cavernous haemangiomaCavernous haemangiomata are deeper, darker in colour and may be relatively large. Both tend to increase in size for a period & then gradually involute partially or totally. Parents should be re-assured that most lesions will resolve spontaneously by 5-6 years. They do not require routine follow-up.
HEAD/FACE
• HEAD – shape, circumference, fontanelles
• EARS – shape, position• EYES – position, red reflex• MOUTH – cyanosis, tongue, palate,
sucking reflex

Head

Caput Succadaneumcaput can cross over suture lines (since it affects the scalp), it is often predominantly or entirely unilateral. caput -- maximal at birth, with rapid resolution over the next 24 - 48 hours.

CephalhaematomaCephalohematoma is a collection of blood under the periosteum of a skull bone. Because of its location, it is impossible for cephalohematoma to cross suture lines.

Ears

Ear tagA single, small ear tag is an occasional finding on physical examination. It is often inherited as a familial trait.

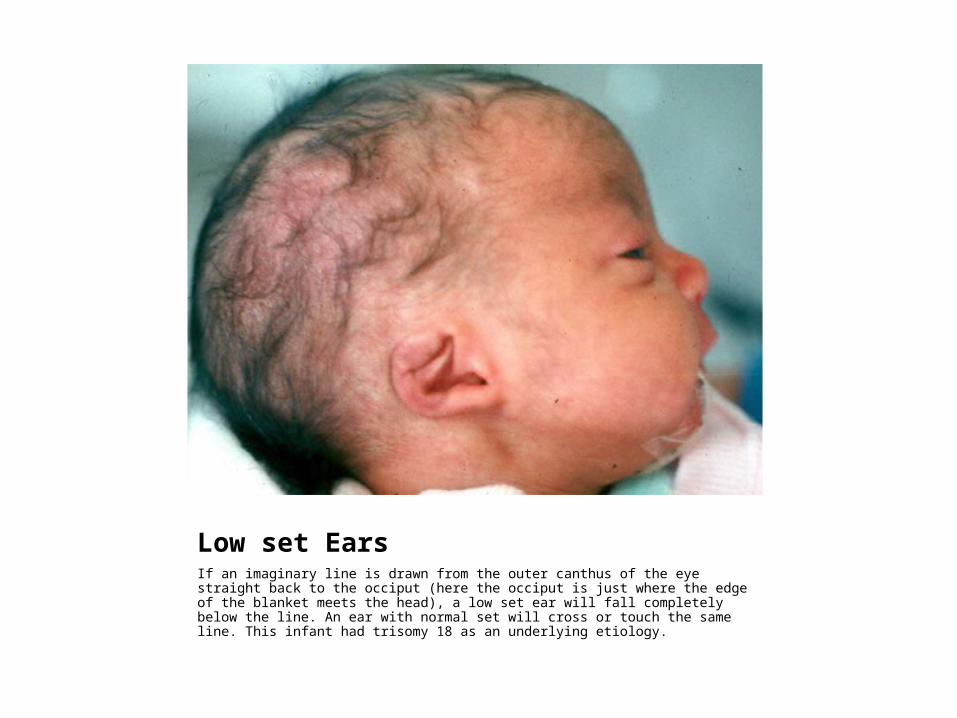
Low set EarsIf an imaginary line is drawn from the outer canthus of the eye straight back to the occiput (here the occiput is just where the edge of the blanket meets the head), a low set ear will fall completely below the line. An ear with normal set will cross or touch the same line. This infant had trisomy 18 as an underlying etiology.
Eyes

CataractsRed reflux cant be seen. Refer paediatric ophthalmologists

Cataracts

Sub Conjunctival haemorrhageSubconjunctival haemorrhage is a frequent finding in normal newborns. It results from the breakage of small vessels during the pressure of delivery.

Gonococcal Conjunctivitisit typically presents in the first few days of life
gonococcal conjunctivitis is an ophthalmologic emergency.
bacteria can erode through an intact cornea, treatment is very aggressive and includes systemic intravenous antibiotics, frequent eye washes, and monitoring in a neonatal intensive care unit.

Mouth

CLEFT PALATEonly the lateral margins of the palate are visible. Because the mouth is wide open to the nasal cavity, the NG tube can be seen passing through the nasopharynx as well as the mouth.

CLEFT LIPThis infant has a normally formed, intact palate, but has a unilateral cleft on the left side of the lip. Feeding can be impaired in infants with cleft lip

NEONATAL TEETHThis infant's tooth is erupted and is clearly visible. When the tooth is mobile, it can easily be removed with a gauze and a twisting motion.

CHEST/ARMS
• LUNGS – resp rate, breath sounds• HEART – heart rate, murmurs• ARMS – inspect, brachial pulses• HANDS – palms, count fingers

Asymptomatic heart murmur
• Ensure asymptomatic & feeding well• Check femoral pulses & pulse oximetry (pre-ductal
and post ductal)
• Middle Grade review prior to discharge
• If baby well then arrange 6 week review with Consultant
• If murmur loud/diastolic then needs middle grade review and scbu admission
• Ask parents to return if symptoms suggestive of cardiac disease- e.g. breathlessness, sweatiness, not completing feeds, failure to gain weight, cyanosis etc.

Hands
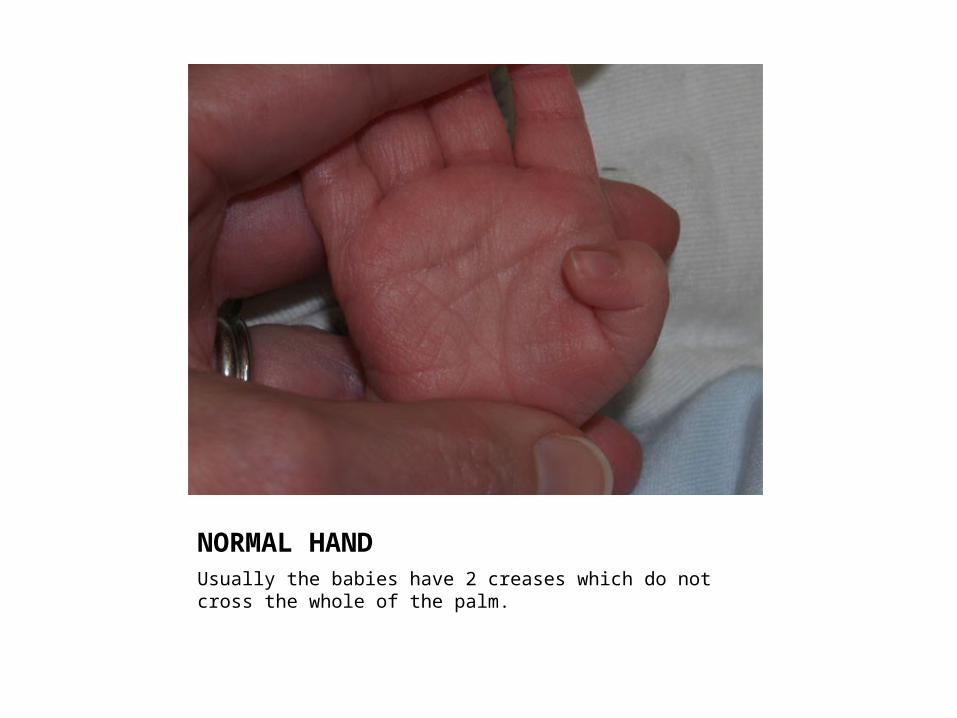
NORMAL HANDUsually the babies have 2 creases which do not cross the whole of the palm.

Transverse CreaseIt is most characteristic feature in Downs syndrome. It is inherited as familial trait in 5%.

PolydactylyIf the extra digit has a bony component referral should be to the hand surgeon, Professor S. Kaye in Leeds.If there is no bony component, referral may be needed to the plastic surgeon, Mr Fu in Bradford.

Oedema of the hand
It IS common in Turner Syndrome. It is associated with other physical findings like short stature, short fourth metacarpal, webbed neck, high palate and nail dysplasia.

ABDOMEN/LEGS
• ABDO – inspect, palpate, check for hernias, femoral pulses
• GENITALS – insect, palpate testes• ANUS – patency• LEGS – inspect length/creases, hips• FEET – position, number of toes

Abdomen
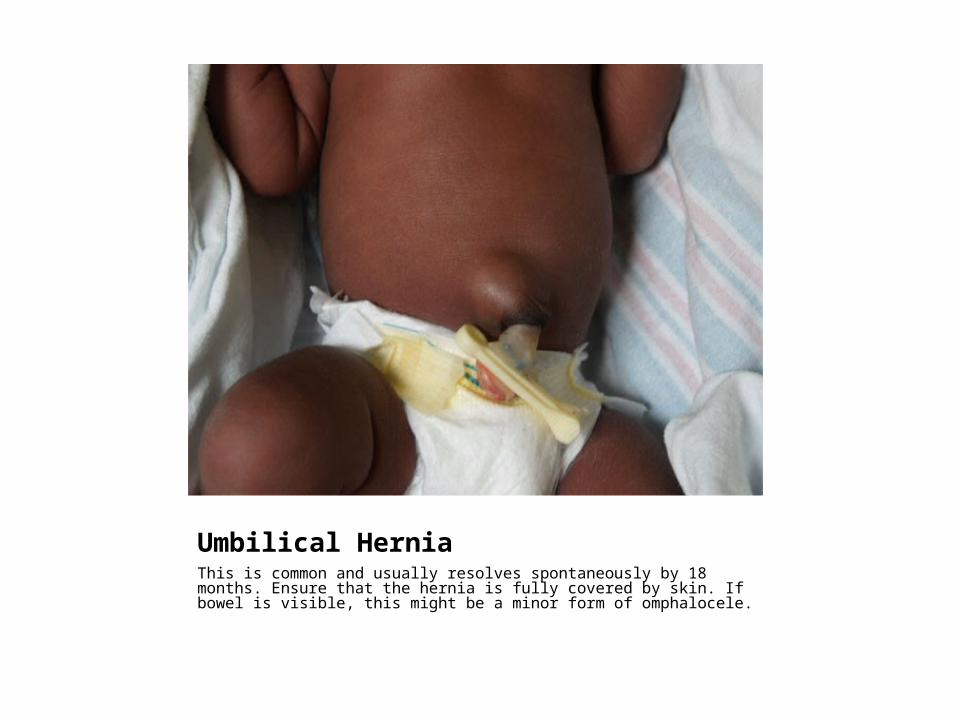
Umbilical HerniaThis is common and usually resolves spontaneously by 18 months. Ensure that the hernia is fully covered by skin. If bowel is visible, this might be a minor form of omphalocele.

Genitals
• Hydrocoele: no treatment, normally resolves spontaneously within few months (if not gone within 1year then refer)
• Hypospadias: urethral opening is in abnormal position; ensure flow of the urine ok; need to refer urology; advise baby shouldn’t be circumcised until seen

Genitals
• Undescended testes: 2% babies; put on discharge letter/red book so GP aware; if not descended by 1 year needs referral
• Ambiguous genitalia: explain genitalia not quite normal & baby will need further exam/Ix before sex rearing can be determined; inform neonatal consultant immediately

Legs

Club Foot

Talipes
• Talipes, particularly equinovarus, is relatively common lower limb abnormality
• Majority are positional with no need for specific treatment (but inform GP)
• Sig. positional talipes need physio referral • Physio can refer to orthopaedics if needed• Fixed talipes (the foot cannot be moved back into
position) need urgent orthopaedic referral and hip scan

Feet

SyndactylyIf there is fusion of the bone referral is to the hand specialist as above .If not the referral is to the plastic surgeon as above.

Downs syndmany infants with Down's syndrome is an increased gap between the great and first toes.

Hips
• Barlow’s test(?dislocatable)• Ortolani’s test(?reducable)
If positive tests then urgent USS If risk factors then USS at 6/52

BACK/TONE
• BACK – inspect for dimples, palpate• TONE – during ventral suspension, head
lag, Moro reflex

Sacral hairIf the base of the dimple can be identified no further action is required. If this cannot be identified or there is a hairy patch or swelling present, a spinal USS needs to be arranged.

Sacral dimple

HEALTH PROMOTION
• Immunisations• Feeding/weaning advice• Reducing risk of SIDS• Smoking• Injury prevention• Dental health

![[IJCT V3I4P9] Authors:Ms. Sivashankari .A, Mrs. Kavitha .S.K](https://static.fdocuments.net/doc/165x107/58a5dd5d1a28abd14d8b55f5/ijct-v3i4p9-authorsms-sivashankari-a-mrs-kavitha-sk.jpg)









![[IJCT V3I4P7] Authors: Mahalakshmi S., Kavitha S](https://static.fdocuments.net/doc/165x107/58f132911a28aba03e8b4611/ijct-v3i4p7-authors-mahalakshmi-s-kavitha-s.jpg)





