

New Technologies and Health Behavior Change Iowa State University Exercise Psychology Class April...
62
New Technologies and Health Behavior Change Iowa State University Exercise Psychology Class April 18, 2011 Steven N. Blair Arnold School of Public Health University of South
-
Upload
ethan-johnson -
Category
Documents
-
view
213 -
download
0
Transcript of New Technologies and Health Behavior Change Iowa State University Exercise Psychology Class April...

New Technologies and Health Behavior Change
Iowa State UniversityExercise Psychology Class
April 18, 2011
Steven N. Blair
Arnold School of Public Health
University of South Carolina

2008 Physical Activity Guidelines for Americans
At-A-Glance
www.health.gov/PAGuidelines/
U.S. Department of Health and Human Services

WHO PA Recommendation• Released by WHO in December 2010• PA recommendations
– 5-17 yr—60 min MVPA/day, vigorous intensity, including muscle and bone strengthening 3 X week
– 18-64 yr—each week accumulate in bouts of at least 10 min, 150 min moderate intensity, 75 min vigorous intensity, or combination of both; and resistance training 2 X week
– 65 yr & older—same as 18-64 yr, those with poor mobility should also do balance exercises, and take health conditions into account

Improving Physical Activity for All Americans
The US National Physical Activity Plan
A Call to Action
Released May 3, 2010

Background• Release of the 2008 PA Guidelines for
Americans necessitates action to ensure greater ability to comply with those guidelines.
• National Plans in other domains (e.g. smoking cessation, diabetes,
arthritis) have proven successful in the U.S.

Background
• Other nations (e.g. Finland, Australia, U.K.) have developed National PA Plans.
• Until May 3, 2010 there was no U.S. National PA Plan.

What is a Physical Activity Plan?
• A comprehensive set of strategies including policies, practices, and initiatives aimed at increasing physical activity in all segments of the population.
* CDC/WHO Collaborating Center Workshop On Global Advocacy For National Physical Activity Plans Workshop report. January, 2007

•Public Health•Education•Healthcare•Volunteer and Non-Profit Organizations•Transportation, Urban Design, Community Planning •Business and Industry•Parks, Recreation, Fitness, and Sports•Mass Media

National Physical Activity Plan White Papers
• Published in a November 2009 supplement to the Journal of Physical Activity and Health– Published by Human Kinetics (
www.hkusa.com) – Go to journal page, then to the Journal of
Physical Activity and Health, then to the November 2009 supplement
– http://journals.humankinetics.com/jpah-back-issues/jpah-volume-6-supplement-november

Public Health SectorSample Strategy:
• Disseminate tools and resources important to promoting physical activity:
– Burden of disease due to inactivity
– Evidence-based interventions

Public Health SectorPublic Health Sector
Sample Tactic:
• Support and expand the National Society of Physical Activity Practitioners in Public Health resource.

Healthcare Sector
Sample Strategy:
• Make physical activity a patient “vital sign” that all healthcare providers assess and discuss with their patients.

Healthcare Sector
Sample Tactic:
• Track patients’ level of physical activity in electronic medical records/health records (EMRs/EHRs).

Overview• Medical care costs in the U.S are ~17%
of GNP, by far the highest in the world• By traditional public health markers
such as longevity, chronic disease rates, infant mortality, etc; the U.S. ranks far behind many other countries
• Most health problems are the result of unhealthy lifestyles
• We must be more aggressive in integrating lifestyle interventions into medical practice and public health programs

How to Promote Healthful Lifestyles
• Relatively new area of research
• Application of theories, models, & methods from behavioral science
• Social Cognitive Theory, Transtheoretical Model (Motivational Readiness), etc– Helping individuals use cognitive and
behavioral strategies to implement behavioral change

Lessons Learned from Physical Activity Intervention Studies
• Individuals who use cognitive and behavioral strategies are more likely to be active at 24 months than individuals who do not use these strategies
• Approximately 25-30% of initially sedentary persons who participate in Active Living will be meeting consensus public health guidelines for physical activity at 24 months

Behavioral Approaches to Physical Activity Interventions
• Theoretical foundations– Social Learning Theory– Stages of Change Model– Environmental/Ecological Model
• Methods– Problem solving– Self-monitoring– Goal setting– Social support– Cognitive restructuring– Incremental changes– Manipulating the environment

How Do People Change? Cognitive StrategiesHow Do People Change? Cognitive Strategies
Increasing Knowledge Encourage person to read and think about physical activity
Warning of Risks Provide person with message that being inactive is very unhealthy
Caring about Encourage person to recognize Consequences to Others how his/her inactivity affects
his/her family and friends
Comprehending Benefits Help person to think about the personal benefits of being active
Increasing Healthy Help person to become aware of Opportunities societal changes in regard to
physical activity
Marcus. Motivating People to Be Physically Active. Human Kinetics, 2003

How Do People Change? Behavioral StrategiesHow Do People Change? Behavioral Strategies
Substituting Alternatives Encourage person to engage in physical activity when it might be most beneficial, yet is rarely done
Enlisting Social Support Encourage person to find a friend or family member who will provide support for being active
Rewarding Yourself Encourage person to reward and praise self for being active
Committing Yourself Encourage person to make commitment to be active
Reminding Yourself Help person to set up reminders to be active
Marcus. Motivating People to Be Physically Active. Human Kinetics, 2003

32
33
34
35
0 6 12 18 24
Lifestyle Structured
Mean Energy Expenditurek
cal. k
g-1
.d
ay-1
time in months
Project Project ActiveActiveDunn et al. JAMA 1999; 281:327
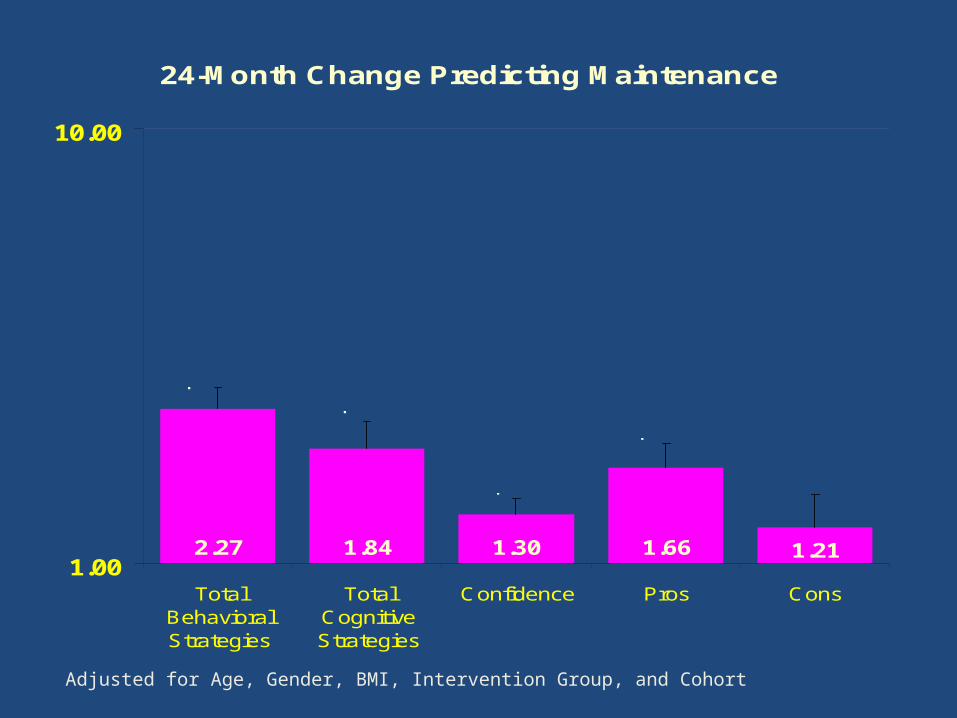
24-Month Change Predicting Maintenance
2.27 1.84 1.30 1.66 1.211.00
10.00
TotalBehavioralStrategies
TotalCognitiveStrategies
Confidence Pros Cons
p=.003p=.03
p=.03
p=.03
p=.42
Od
ds R
ati
o
Adjusted for Age, Gender, BMI, Intervention Group, and Cohort

Change in Behavioral Strategies Over 24-Months Predicts Maintenance
1.68 1.31 1.88 1.44 1.571
10
CommittingYourself
EnlistingSupport
RemindingYourself
SubstitutingAlternatives
RewardingYourself
Od
ds
Ra
tio
s
p=.02
p=.14
p=.001
p=.06
p=.03
Adjusted for Age, Gender, BMI, Intervention Group, and Cohort

Odds Ratios for Maintenance of Physical Activity at 24 Months
2.61
1.72
4.75
0.1
1
10
Family HighPeer High
Family Low PeerHigh
Family HighPeer Low
Family Low PeerLow
p < .001
p = .02
p =.003Referent
Od
ds
Rat
io

The Active Living Every Day (ALED) Program

Active Living Every Day
S Blair takes no personal royalties from the ALED book

ALED Program
Participant Resources
• Active Living Every Day book
• Online study guide– Tracks the ALED book– Stage-based “buddy”– Interactive (quizzes, links, forms)

Active Living Every Day program philosophy
• Moderate physical activity = significant health benefits
• Lifestyle physical activity: an important alternative
• People are more likely to become and stay active when they learn lifestyle skills based on their readiness to change

Flexible delivery options• Weekly in-person group or
individual sessions
• Online or Web-based, with facilitator support
о Hybrid: online participation with periodic group sessions (either in-person, teleconference, or Web conference)

Changes in Physical Functioning in the Active Living Every Day Program (ALED)• The 4-year Active for Life Initiative
– Goal: help participants accumulate at least 30 min MVPA most days of the week
• 877 adults from Southwestern Ohio age ≥50 years, sedentary or underactive (≤2 days/wk and <120 min/wk)
• Measurements at baseline and at 20 weeks– survey assessing BMI, PA, health-related practices, and
psychosocial variables– 4 performance-based physical functioning tests
• Results: Participants significantly increased performance on all four tests regardless of BMI, race/ethnicity, or baseline impairment status
Baruth M et al Int J Behav Med 2010

Improvements in Physical Functioning Impairment Status Among Adults in
ALED Program
Baruth M et al Int J Behav Med 2010
Pre Post
Percentages adjusted for race, age, BMI, and gender
Impaired: ≤25th percentile*Not impaired: >25th percentile*
*based on Rikli and Jones’ Senior Fitness Test Manual normative data
Pre PostPre Post
30-sec Chair Stand
Eight Foot Up & Go
ChairSit-and-Reach
p<0.0001 p<0.0001 p=0.0019

How to Achieve Lifestyle Change
• Counseling by a PhD level behavioral psychologist
• Counseling by B.A. level health educators
• Counseling by mail and telephone
• Counseling by electronic communications

CoEE for Technology Center to Enhance Healthful Lifestyles
University of South Carolina Dr. Steven Blair
Dr. Saundra Glover
Medical University of South Carolina Dr. Carolyn Jenkins
Dr. Lisa Vandemark

Lifestyle Interventions Integrated with Electronic
Health Records—Kaiser Permanente

Within the Visit Navigator, you will now see the “Exercise Vitals” section immediately following the “Vitals” section.
Exercise as a Vital SignKaiser Permanente
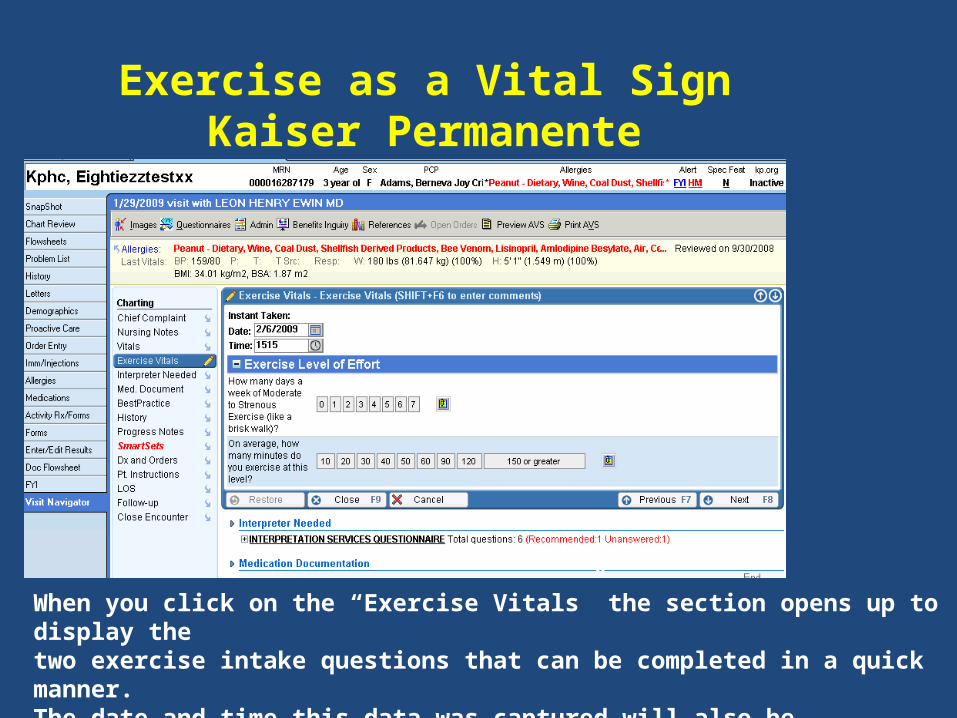
When you click on the “Exercise Vitals” the section opens up to display the two exercise intake questions that can be completed in a quick manner. The date and time this data was captured will also be noted/stored.
Exercise as a Vital SignKaiser Permanente

Telehealth and Weight Change•87 participants (73 women & 14 men)•Mean age 50 years•Treatment groups (Quasi-experimental design)
•Traditional class•Telehealth—interaction with RD via web and email•Control
•No difference in satisfaction between traditional and telehealth•Telehealth more convenient than traditional (p<0.0001)
Kg change at 6 mo
Traditional Telehealth Control
p <0.05
Haugen HA et al. Obes 2007; 15:3067-77

Promoting PA via PDA• 37 healthy, inactive adults, ≥50 years of
age
• 8-week RCT
• PDA intervention (93% had not used PDAs)– Questions about amount and type of PA – Alerted at 2 PM and 9 PM to complete PA
assessment– Gave motivational and behavioral tips
• Controls—standard written materialsKing AC et al. Am J Prev Med 2007; 34:138-42

Promoting PA via PDA
• Intervention participants completed 68% of the 112 PDA entries available
• After adjusting for baseline differences– PDA group reported 310.6 minutes of
moderate to vigorous PA/week– Control group reported 125.5 minutes/week– p=0.048 for group comparison
• 78.6% of PDA group reported enjoying using the device
King AC et al. Am J Prev Med 2007; 34:138-42

Internet-plus-email Intervention for Increasing Physical Activity
• 3-month RCT156 ethnically-diverse adult women (mean age=42.8 y, 65% White)
• Study groups– Tailored website + email messages– Wait-list control
• Intervention group significantly increased walking and total moderate-vigorous physical activity compared with controls
Dunton GF & Robertson TP. Prev Med 2008; 47:605-11

Review of Electronic Computer Interventions to Increase Activity
• Search of PubMed or Web of Science yields <25 studies on electronic interventions for physical activity and <15 of these focus exclusively on activity
• Conclusions– Using the internet can reach large populations– Research is still in infancy but
• Results are promising with beneficial changes in physiological and psychological factors reported
• Appears that response is similar to established interventions
Marcus BH et al. Br J Sports Med Feb 2009

Internet-Based Learning in the Health Professions
• Meta-analysis of 201 studies of interventions for health professionals– 201 studies identified– Internet-based intervention, no interventions, or
non-internet interventions• Conclusions
– Internet-based interventions produced consistent and large positive effects compared with no intervention
– Differences between internet and non-internet (traditional) interventions were heterogeneous and generally small, suggesting comparable effects
Cook DA et al. JAMA 2008; 300:1181-96

Web- and Computer-Based Smoking Cessation
• 22 RCTs of Web- and computer-based smoking cessation programs– 16,050 enrolled in
smoking cessation groups
– 13,499 enrolled in control groups
• Those in smoking cessation groups were significantly more likely to quit smoking—RR 1.44 (95% CI, 1.27-1.64)
• Conclusion—there is sufficient evidence to recommend Web- and computer-based smoking cessation programs for adultsMyung SK et al. Arch Int Med
2009; 169:929

Basic Internet vs Internet plus behavioral e-counseling
• 92 overweight adults ~BMI 33.1(3.8), 12 month RCT, Providence RI, age = 48.5yrs(9.4)
• Randomized to basic internet or internet plus behavioral e-counseling.
• Initial body weight loss was doubled in the e-counseling group
• Intent-to-treat analysis showed the behavioral e-counseling group lost more at 12 months than basic Internet group – Weight: -4.4[6.2] vs -2.0[5.7]kg; P=.04– Waist circumference: -7.2[7.5] vs -4.4[5.7]cm; P=.05
• Internet e-counseling may be a alternative to more burdensome clinic programs
Tate DF. JAMA, 2003; 289(14);1833-1836

Basic Internet vs Internet plus behavioral e-counseling
Tate DF. JAMA, 2003; 289(14);1833-1836

HEALTH Project• Physical activity and diet intervention for
TRICARE enrollees in Indiana, Ohio, Michigan, and Illinois
• Interventions– bookHEALTH– teleHEALTH– eHEALTH
• Weight loss ~5% of baseline weight at 18 months
• Increases in fruit and vegetable intake, physical activity, and quality of life
• Cost recovery 3-6 years

• RCT with 4 arms:
1.) Standard Care group included self-help with a diet and PA manual
2.) GWL health counselor and 14 sessions
3.) GWL + SenseWear™ Armband group
4.) SWA alone
• Follow-up data collection visits occur at month 4 and month 9
LEAN Study Design

Effects across time for weight. Estimates adjust for age, gender, race, education, and wave.
92
94
96
98
100
102
104
Baseline Month 4 Month 9
We
igh
t (K
g)
GWL
GWL+SWA
SWA alone
Standard care

Summary• Unhealthful lifestyles are the major cause
of chronic disease morbidity and mortality
• Lifestyle interventions have demonstrated efficacy and effectiveness in a variety of populations
• Our challenge now is to develop translational interventions, using modern technology, to reach large numbers of individuals at a low cost.

Questions?

Behavior change topics• Identifying and overcoming barriers
• Enlisting social support
• Setting realistic goals
• Coping with lapses
• Rewarding yourself
• Positive self-talk
• Self-monitoring

Active Grandmothering

Attributable Fractions (%) forAll-Cause Deaths
40,842 Men & 12,943 Women, ACLS
02468
1012141618
Low CRF
Obese
Smoker
Hypertension
High Chol
Diabetes
MenWomen
Blair SN. Br J Sports Med 2009;43;1-2

WEB-BASED
COMPUTER-BASED

0
2
4
6
8
10
0 2 4 6 8 10 12 14 16 18 20 22 24
Noon-time jog
Walk to busstop
After-dinner
walk
Energy Expenditure (METS)
Time (hours)
Theoretical Patterns of Physical ActivityOver 24 Hours
Sedentary
Lifestyle Exercise
Leisure-Time Exercise

Center Vision

How to Change Unhealthful Lifestyle Behaviors?

Solutions for the US Health Care Crisis

President Obama—Speech at the National
Academy of Science, April 27, 2009• "The Recovery Act will support the long
overdue step of computerizing America's medical records, to reduce the duplication, waste, and errors that cost billions of dollars and thousands of lives.
But it's important to note: these records also hold the potential of offering patients the chance to be more active participants in prevention and treatment. …we have the opportunity to offer billions and billions of anonymous data points to medical researchers who may find in this information evidence that can help us better understand disease."

Steps to Success• Begins with current behaviors, and how
they compare to public health guidelines
• Encourages small steps
• Builds confidence
• Cognitive behavioral strategies
• Scientifically-tested methods

Computer Tailored Lifestyle Intervention for Diet and Physical Activity
• 310 participants, BMI ≥25.0• Treatment groups
• Computer-based assessment of motivational readiness for change
• Computer-generated 4-5 page individualized report
• Discussed report with physician
• Control group received packet of health education materials
• Outcomes—12-month change in• Physical activity• Body weight
• % reaching 150 MET-min of PA/week at 12 months– Experimental group increased
from 26% to 53% (p <0.001)
– Controls—30% at baseline, 37% (p=0.27)
• No difference in weight at 12-months between groups– 21% of experimental group lost
≥5% of baseline weight compared with 10.6% of controls (p <0.01)
– 32% of experimental group lost ≥2.7 kg at 12-months compared with 19% of controls losing ≥2.7 kg (OR=2.2, p <0.01)
Christian JG et al. Arch Int Med 2008; 168:141-6

Telephone Counseling for Increasing Physical Activity
• 6-month RCT with 298 sedentary adults (mean age=45.9 y), 72% women, 45% white & 45% African-American
• Study groups– Fully automated telephone-linked counseling
(TLC-PA) based on Stages of Motivational Readiness
– TLC-Eat counseling for healthy eating• Results
– 3-mo TLC-PA more likely to meet PA recommendations
– 6-mo, no differences between groups
Pinto BM et al. Am J Prev Med 2002; 23:113-20


















