
New parameters for the gait analysis in the orthopaedic private practice
1
250 Gait & Posture 1994; 2: No 4 physically real to the patient. The other evaluation methods might include cinematography, motion analy- sis, and radiographic data on alignment and contain- ment, and residual limb/socket force analysis. All of these are valuable evaluation methods but most of them are not practical since they need time and skills. In pedography the examination of a patient requires minutes. Sometimes trying to give satisfactory answers to patient’s requirements means that their rehabilitation times may lengthen. (Normal average time of below knee 10 days, above knee 21 days.) Rehabilitation time is maintained until symmetric footprints are obtained in pedography. During the time spent in getting symmetric footprints, the patient’s subjective criteria were parallel and 2 days earlier than the ending of conventional reha- bilitation times (average 8 days for below knee and 19 days for above knee). Symmetry of gait patterns in pedography will assist in revealing the optimal length of rehabilitation time, and also will help to get more quantitative measurements during the alignment of prostheses. On the importance of monitoring walking speed in pressure distribution measurements S Hautmann, D Rosenbaum, M Gold, L Claes Abteilung Unfallchirurgische Forschung & Biomechanik, Universitat Ulm, Germany Introduction Kinetic and kinematic parameters are used in gait analysis to evaluate pathological or post-traumatic foot function. Usually, the data are compared to those of normal healthy subjects in order to determine the degree of the functional deficit. However, patients may exhibit different gait dynamics that impede direct comparisons. One of the potentially influential factors is walking speed. This project was designed (1) to deter- mine the impact of walking speed on plantar pressure patterns, (2) to investigate whether possible differences can be explained by kinematic parameters, and (3) to compare the effects in subjects with different arch types. Methods In 30 healthy subjects (26.7 years of age) plantar pressure distribution patterns were measured with the EMED-SF2 platform at slow, normal, and fast walking speeds (0.8, 1.2, 1.7 m .s-l).. The data for * eversion/inversion and plantar flexia dorsiflexion during walking were obtained with a Penny & Giles electrogoniometer. Podograms of the subjects feet were used to determine an arch type index (arch width divided by foot length w/o toes) and attribute them to a normal, low or high arch group (each group n = 10). Results There was a significant (P < 0.05) increase in plantar peak pressure with increasing walking speed under the heel, first and second metatarsal, and the hallux for all subjects. The fifth metatarsal showed a significant decrease of plantar pressure with increasing walking speed. The midfoot showed a decrease of pressure with increasing walking speed which was not significant. Eversion and plantarflexion increased significantly with increasing walking speed for all subjects. The three arch types did not react differently to changes in walking speed. Peak pressures at three walking speeds Conclusions Increasing walking speed shows a medial shift of plantar peak pressure from the lateral to the medial forefoot. This can possibly be explained by a more pronounced eversiompronation motion. The arch type appears to have only little impact on these findings. The presented data clearly indicate that gait dynamics (i.e. walking speed) have to be monitored and taken into account when patient and normal data are being compared. New Parameters for the Gait Analysis in the Orthopaedic Private Practice Dr med. Christian Wyss, Baaden The Orthopaedic diagnostic should not be guided by the so-called normal or pathological signs. This way of thinking is too simple and does not do justice to the individuality and complexity of gait problems in the orthopaedic Ipractice. We often find patients with the same clinical symptoms (for example shin splints) but with quite different aetiologies. For this reason the thinking in the orthopaedic practice should be more teleological and -functional than statical like the pure research. Illustrative examples show that this way of gait analysis opens a new dimension for gait analysis in the orthopaedic private practice. Additionally we present new parameters (roll of schedules, a special diagram of gait lines and ‘risk factors’ with diabetic ulcerations). We will also discuss the applications and limits of these new parameters.
Transcript of New parameters for the gait analysis in the orthopaedic private practice
250 Gait & Posture 1994; 2: No 4
physically real to the patient. The other evaluation methods might include cinematography, motion analy- sis, and radiographic data on alignment and contain- ment, and residual limb/socket force analysis. All of these are valuable evaluation methods but most of them are not practical since they need time and skills. In pedography the examination of a patient requires minutes.
Sometimes trying to give satisfactory answers to patient’s requirements means that their rehabilitation times may lengthen. (Normal average time of below knee 10 days, above knee 21 days.) Rehabilitation time is maintained until symmetric footprints are obtained in pedography. During the time spent in getting symmetric footprints, the patient’s subjective criteria were parallel and 2 days earlier than the ending of conventional reha- bilitation times (average 8 days for below knee and 19 days for above knee). Symmetry of gait patterns in pedography will assist in revealing the optimal length of rehabilitation time, and also will help to get more quantitative measurements during the alignment of prostheses.
On the importance of monitoring walking speed in pressure distribution measurements S Hautmann, D Rosenbaum, M Gold, L Claes Abteilung Unfallchirurgische Forschung & Biomechanik, Universitat Ulm, Germany
Introduction
Kinetic and kinematic parameters are used in gait analysis to evaluate pathological or post-traumatic foot function. Usually, the data are compared to those of normal healthy subjects in order to determine the degree of the functional deficit. However, patients may exhibit different gait dynamics that impede direct comparisons. One of the potentially influential factors is walking speed. This project was designed (1) to deter- mine the impact of walking speed on plantar pressure patterns, (2) to investigate whether possible differences can be explained by kinematic parameters, and (3) to compare the effects in subjects with different arch types.
Methods
In 30 healthy subjects (26.7 years of age) plantar pressure distribution patterns were measured with the EMED-SF2 platform at slow, normal, and fast walking speeds (0.8, 1.2, 1.7 m .s-l).. The data for * eversion/inversion and plantar flexia dorsiflexion during walking were obtained with a Penny & Giles electrogoniometer. Podograms of the subjects feet were used to determine an arch type index (arch width divided by foot length w/o toes) and attribute them to a normal, low or high arch group (each group n = 10).
Results
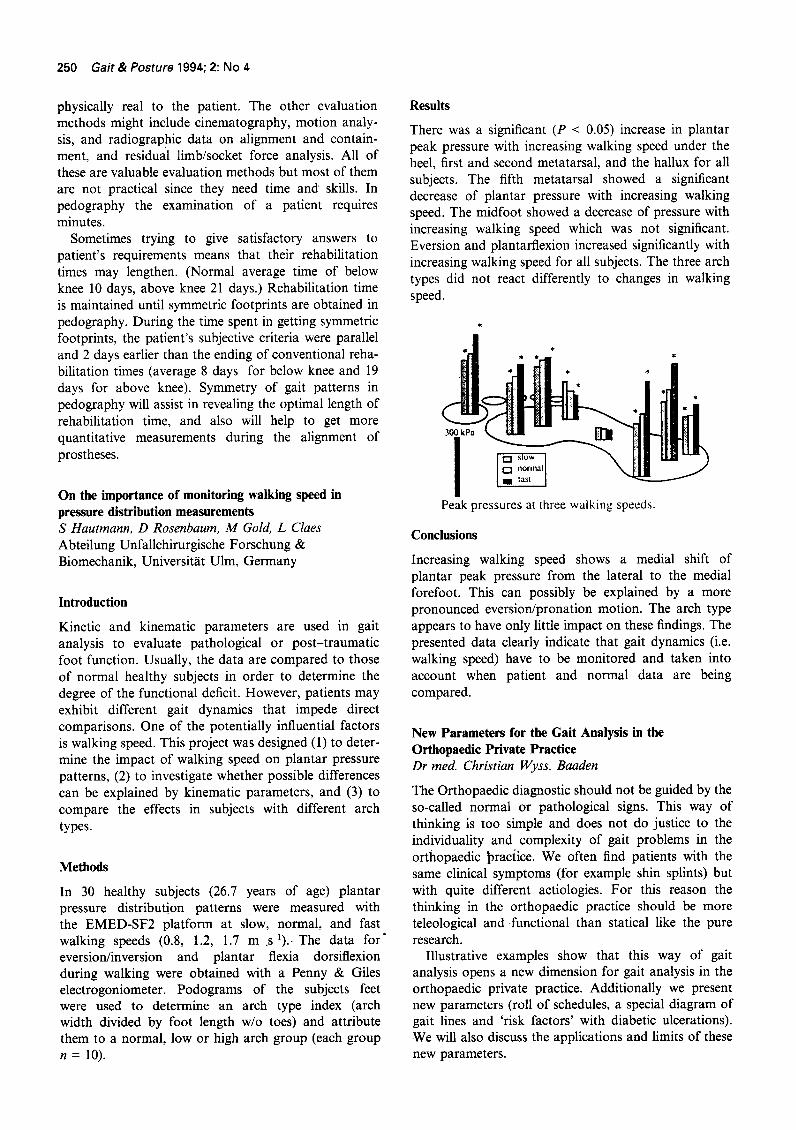
There was a significant (P < 0.05) increase in plantar peak pressure with increasing walking speed under the heel, first and second metatarsal, and the hallux for all subjects. The fifth metatarsal showed a significant decrease of plantar pressure with increasing walking speed. The midfoot showed a decrease of pressure with increasing walking speed which was not significant. Eversion and plantarflexion increased significantly with increasing walking speed for all subjects. The three arch types did not react differently to changes in walking speed.
Peak pressures at three walking speeds
Conclusions
Increasing walking speed shows a medial shift of plantar peak pressure from the lateral to the medial forefoot. This can possibly be explained by a more pronounced eversiompronation motion. The arch type appears to have only little impact on these findings. The presented data clearly indicate that gait dynamics (i.e. walking speed) have to be monitored and taken into account when patient and normal data are being compared.
New Parameters for the Gait Analysis in the Orthopaedic Private Practice Dr med. Christian Wyss, Baaden
The Orthopaedic diagnostic should not be guided by the so-called normal or pathological signs. This way of thinking is too simple and does not do justice to the individuality and complexity of gait problems in the orthopaedic Ipractice. We often find patients with the same clinical symptoms (for example shin splints) but with quite different aetiologies. For this reason the thinking in the orthopaedic practice should be more teleological and -functional than statical like the pure research.
Illustrative examples show that this way of gait analysis opens a new dimension for gait analysis in the orthopaedic private practice. Additionally we present new parameters (roll of schedules, a special diagram of gait lines and ‘risk factors’ with diabetic ulcerations). We will also discuss the applications and limits of these new parameters.





![Variability of Gait Parameters in Different Daily Situations2010/01/04 · 28 VOLUME 14, No. 1, 2010 development of marker-free gait analysis system MAFRAN [1, 2] trying to increase](https://static.fdocuments.net/doc/165x107/60d47512ea143a358576814c/variability-of-gait-parameters-in-different-daily-situations-20100104-28-volume.jpg)












