

3D Multimodal Imaging: When modalities combine you see disease ...

New Modalities for Imaging the Failing Heart: How Do They Help?
Paul J. Kim, MD, FACCAssistant Clinical Professor of MedicineDivision of CardiologyUniversity of California, San Diego
18th Annual San Diego Heart Failure SymposiumJanuary 19-20, 2018

• Grant/Research Support: Astellas Pharma
2
Disclosures

We will review in this session:
1. Cardiac imaging modalities available
2. Choosing the appropriate cardiac imaging modality
3. Nonbiopsy diagnosis of cardiac amyloid
4. Imaging for cardiac sarcoidosis
5. Other advanced cardiac imaging techniques
3
Learning Objectives

• Echocardiogram• Nuclear cardiac imaging• Cardiac MRI• Cardiac CT
4
Non-invasive Cardiac Imaging Modalities

• Essential tool that provides structure, function and assessment of intracardiac hemodynamics.
• No radiation, relatively quick exam with reasonable spatial and excellent temporal resolution.
• Limited acoustic windows (obesity) and myocardial tissue characterization.
• Significant advancements with 3D acquisition and contrast echocardiography.
5
Echocardiogram

6
Echocardiogram

7
Echocardiogram

8
Echocardiogram

9
3D Echocardiogram

10
3D Echocardiogram

• Widespread cardiac imaging modality that provides function (not structure), perfusion, and viability.
• Newer advancements for evaluation of sarcoid and amyloid cardiomyopathies.
• Does not evaluate valvular disease, pericardium or intracardiachemodynamics.
• Patients are exposed to ionizing radiation.
• Shortages in technetium-99m in the late 2000s.
11
Nuclear cardiac imaging

• SPECT/CT
• Perfusion (99mTc-sestamibi, 99mTc-tetrosfosmin, 201Tl)
• Viability (201Tl)
• ATTR amyloid (99mTc-PYP, 99mTc-DPD)
• PET/CT
• Perfusion ([82Rb]-Rubidium, [13N]-Ammonia)
• Viability ([18F]-FDG)
• Sarcoid ([18F]-FDG)
• MUGA
• Function (99mTc-red blood cell)
12
Nuclear cardiac imaging

13
SPECT myocardial perfusion imaging
Heller and Hendel. Handbook of Nuclear Cardiology 2013.

14
PET viability
Heller and Hendel. Handbook of Nuclear Cardiology 2013.

• Advanced cardiac imaging technique with high spatial and temporal resolution.
• No radiation and gadolinium contrast can be used without concern for acute kidney injury.
• Provides high resolution structure, function and myocardial perfusion. Can demonstrate myocardial viability.
• Limited by longer time for acquisition (narrow bore) and arrhythmias at time of exam.
• Excellent for myocardial tissue characterization and pericardial evaluation.
• Cannot estimate intracardiac pressures and does not provide enough spatial resolution to evaluate for coronary artery disease.
15
Cardiac MRI

16
Myocardial infarction with Cardiac MRI

17
Late gadolinium enhancement shows nonviable myocardium

18
Cardiac MRI is excellent for characterization of myocardial mass

19
Late gadolinium enhancement in cardiac sarcoma

• Advanced cardiac imaging technique with high spatial resolution but lower temporal resolution.
• Of all the modalities, provides the highest spatial resolution consistently. Can provide detailed evaluation of coronary anatomy.
• Provides high quality anatomical structure (great for cardiac masses), function.
• Great tool for prognostication (CAC).
• Does not provide evaluation for valvular regurgitation, intracardiachemodynamics and limited myocardial tissue characterization. Patients are exposed to ionizing radiation and iodinated contrast.
• Able to diagnose other causes of chest pain (e.g. pulmonary embolism, aortic dissection).
20
Cardiac CT

21
Coronary CTA

22
Cardiac CT

• Structure
• Cardiac CT• Cardiac MRI
• Echo
• Function – Echo or Cardiac MRI• Myocardial tissue characterization
• Cardiac MRI• PET; Tc 99m pyrophosphate SPECT
• Ischemia
• CMR, FFR-CT, PET, SPECT, stress echocardiogram
• Viability
• Cardiac MRI, PET, Thallium23
Choosing the “right” cardiac imaging

Ischemic
• CCT
• Stress
• Echo
• MRI
• Nuclear
24
Another paradigm for choosing a cardiac imaging test
Non-ischemic
• MRI
• Sarcoid – PET
• Amyloid – 99m Tc PYP
or MRI

• Nuclear imaging with bone seeking tracers shows high sensitivity (91%) and specificity (92%) for ATTR cardiac amyloid1.
• A positive Tc 99m pyrophosphate scan without evidence of an abnormal monoclonal protein can diagnose ATTR cardiac amyloid without the need for biopsy2.
• Cardiac MRI can demonstrate late gadolinium enhancement that can provide early diagnosis and offer prognostic value3.
25
Nonbiopsy diagnosis of Cardiac Amyloid
1. Castano et al. JAMA Cardiol 2016.2. Castano et al. Current Cardiovascular Risk Reports 2017.3. Fontana et al. Circulation 2015.

26
Nonbiopsy diagnosis of Cardiac Amyloid
• HFpEF• LVH (>1.3 cm), biatrial enlargement
and restrictive filling pattern
• Tc 99m pyrophosphate scan• SPEP, UPEP, immunofixation,
kappa & lambda light chains
• Cardiac MRI
Tc 99m PYP + - -
Monoclonal protein
- + -
Cardiac MRI + + +
ATTR AL Other

27
99mTc pyrophosphate imaging for TTR cardiac amyloid
Bokhari et al. J Nucl Cardiol 2016.

28
99mTc pyrophosphate imaging for TTR cardiac amyloid
Castano et al. JAMA Cardiol 2016.

29
MRI in Cardiac Amyloid
Fontana et al. Circulation 2015.
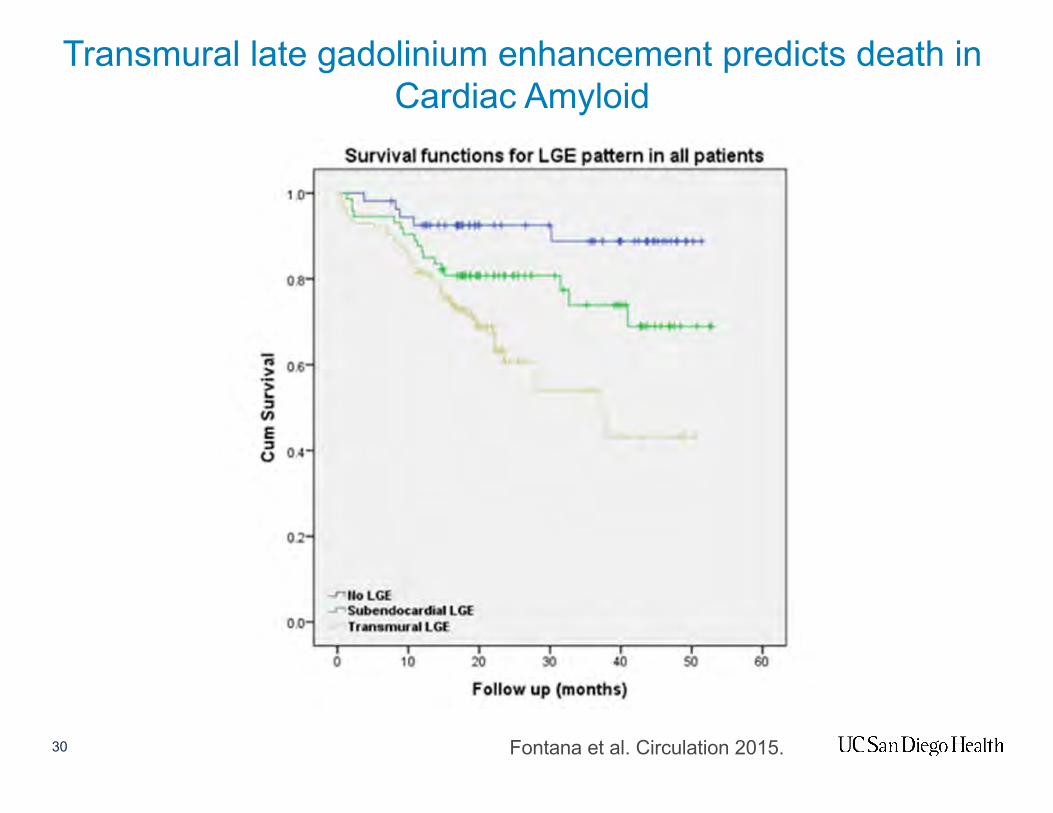
30
Transmural late gadolinium enhancement predicts death in Cardiac Amyloid
Fontana et al. Circulation 2015.

• FDG-PET shows high sensitivity to detect active cardiac sarcoidosis1.
• Following treatment, degree of FDG uptake reduces or resolves with good response to treatment2.
• Cardiac MRI is also a useful diagnostic tool to determine cardiac involvement with excellent sensitivity (>90%)3. However, cardiac MRI has not been demonstrated to follow treatment response.
31
Imaging of Cardiac Sarcoidosis
1. Mc Ardle et al. Circ Cardiovascular Imaging 2013.2. Osborne et al. J Nucl Cardiol Off Publ Am soc Nucl Cardiol 2014.3. Smedema et al. JACC 2005.

32
FDG-PET positive in Cardiac Sarcoidosis

33
Serial PET with treatment of cardiac sarcoid
1. Osborne et al. J Nucl Cardiol Off Publ Am Soc Nucl Cardiol 2014.

34
4D Flow with Cardiac MRI

35
Aortic regurgitant fraction
36
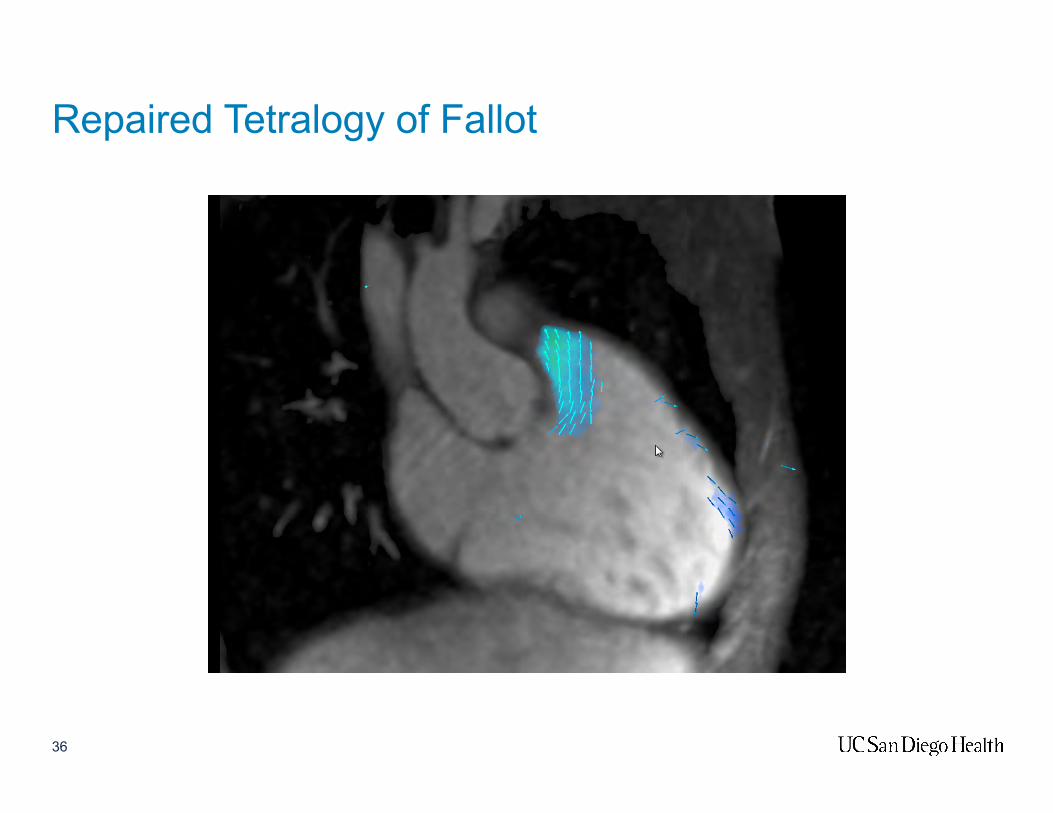
Repaired Tetralogy of Fallot

Repaired Tetralogy of Fallot
Net flow: 4.835 L/minRegurgitant fraction: 48%
Regurgitant volume: 4.433 L/min
Excess volume loading

38
FFR-CT
1. Koo et al. JACC 2011.2. Douglas et al. Eur Heart J 2015.

39
Quantitative Perfusion Cardiac MRI

• Which question are you asking:
• Structure? Echo, Cardiac CT or MRI
• Function? Echo or Cardiac MRI
• Myocardial tissue characterization? Cardiac MRI
• Coronary disease? Cardiac CT
• Viability? Cardiac MRI or PET
• Non-biopsy diagnosis of amyloid can be obtained with:
• Tc 99m PYP scan AND SPEP/UPEP with immunofixation and kappa/lambda ratio.
• For cardiac sarcoid, refer for FDG PET with sarcoid protocol
40
Summary


















