New Drugs Update final - American Pharmacists...
25
10/30/2016 1 New Drugs of 2016 Amy M. Lugo, PharmD, BCPS, BC-ADM, FAPhA Clinical Pharmacy Specialist Director, Managed Care Residency Defense Health Agency Pharmacy Operations Division Formulary Management Branch San Antonio, Texas LCDR Kendra N. Jenkins, USPHS PharmD, BCPS Program Management Officer Immigration and Customs Enforcement (ICE) Enforcement and Removal Operations ICE Health Service Corps Washington, DC CPE Information and Disclosures The American Pharmacist Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. Amy Lugo declares no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria. Kendra Jenkins declares no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria. DoD Disclaimer: The information discussed here represents the views of the presenter, and do not necessarily reflect the views of the Department of Defense (DoD), or the Departments of the Army, Navy, and Air Force. CPE Information • Target Audience: Pharmacists & Technicians • ACPE#: 0202-0000-16-172-L01-P/T • Activity Type: Knowledge-based Learning Objectives – Pharmacist 1. List new therapeutic agents that were approved by the Food and Drug Administration (FDA) in 2016. 2. Describe the mechanism of actions and indications for new therapeutic drugs. 3. Compare and contrast the new therapeutic agents with products available with similar indications. 4. Discuss important patient education and therapeutic monitoring parameters for new therapeutic agents. 5. Summarize the adverse effects and patient safety considerations for new therapeutic agents. Learning Objectives – Technician 1. List new therapeutic agents that were approved by the Food and Drug Administration (FDA) in 2016. 2. Recognize the new therapeutic agents and discuss how they compare with currently available products that have similar indications. 3. State the indication and adverse effects for each new therapeutic drug. Self-Assessment Question 1 1. What is the mechanism of action of ixekizumab? a) IL-2 inhibitor b) BCL-2 inhibitor c) IL-17a receptor antagonist d) Tyrosine kinase inhibitor
Transcript of New Drugs Update final - American Pharmacists...
10/30/2016
1
New Drugs of 2016Amy M. Lugo, PharmD, BCPS, BC-ADM, FAPhA
Clinical Pharmacy Specialist Director, Managed Care Residency
Defense Health AgencyPharmacy Operations DivisionFormulary Management Branch
San Antonio, Texas
LCDR Kendra N. Jenkins, USPHSPharmD, BCPS
Program Management OfficerImmigration and Customs Enforcement (ICE)
Enforcement and Removal OperationsICE Health Service Corps
Washington, DC
CPE Information and Disclosures
The American Pharmacist Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
Amy Lugo declares no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria.
Kendra Jenkins declares no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria.
DoD Disclaimer: The information discussed here represents the views of the presenter, and do not necessarily reflect the views of the Department of Defense (DoD), or the Departments of the Army, Navy, and Air Force.
CPE Information
• Target Audience: Pharmacists & Technicians
• ACPE#: 0202-0000-16-172-L01-P/T
• Activity Type: Knowledge-based
Learning Objectives – Pharmacist
1. List new therapeutic agents that were approved by the Food and Drug Administration (FDA) in 2016.
2. Describe the mechanism of actions and indications for new therapeutic drugs.
3. Compare and contrast the new therapeutic agents with products available with similar indications.
4. Discuss important patient education and therapeutic monitoring parameters for new therapeutic agents.
5. Summarize the adverse effects and patient safety considerations for new therapeutic agents.
Learning Objectives – Technician
1. List new therapeutic agents that were approved by the Food and Drug Administration (FDA) in 2016.
2. Recognize the new therapeutic agents and discuss how they compare with currently available products that have similar indications.
3. State the indication and adverse effects for each new therapeutic drug.
Self-Assessment Question 1
1. What is the mechanism of action of ixekizumab?
a) IL-2 inhibitorb) BCL-2 inhibitorc) IL-17a receptor antagonistd) Tyrosine kinase inhibitor

10/30/2016
2
Self-Assessment Question 2
2. Tumor lysis syndrome is a concern with which drug?
a) lifitegrastb) pimavanserinc) cabozantanibd) venetoclax
Self-Assessment Question 3
3. Which drug : indication pairing is correct?
a) Elbasvir/grazoprevir: cholerab) Glycopyrrolate/formoterol fumarate: COPDc) Lifitegrast: erectile dysfunctiond) Fluciclovine F18: breast cancer
Drug to be Reviewed
• Endocrinology (1)• Dermatology (1 of 2)• Hematology/Oncology (2 of 4)• Neurology/Psychiatry (3)• Gastrointestinal (1)• Infectious Disease (4)• Ophthalmology (1)• Pulmonology (1 of 2)• Nuclear (1 of 2)• Miscellaneous
Endocrinology
Lixisenatide (Adlyxin)
11
Lixisenatide
12
Parameter Drug InformationGeneric LixisenatideBrand AdlyxinManufacturer SanofiFDA Approval Date July 2016
Approval Type NDAType of drug Glucagon-like peptide-1 (GLP-1) receptor agonistFDA Indications To improve glycemic control in type II diabetics
Dosing Initiate at 10 mcg once daily for 14 days; On Day 15, increase dose to 20 mcg once daily
Available preparations
Injection: 50 mcg/mL and 100 mcg/mL in 3 mL in prefilled pen
Lixisenatide (Adlyxin). Product labeling. Sanofi. July 2016.

10/30/2016
3
Lixisenatide Administration & Dosing
• Dosage forms– 50 mcg/mL in 3 mL in green prefilled pen (for 14 pre-set doses; 10
mcg per dose)– 100mcg/mL in 3mL in burgundy prefilled pen (for 14 pre-set doses;
20mcg/dose) • Clear and colorless• Inject into the abdomen, thigh or upper arm; rotate sites• Dose: 10 mcg daily x 14 days then ↑ to 20 mcg daily
13Lixisenatide (Adlyxin). Product labeling. Sanofi. July 2016.
Lixisenatide
14
Parameter Drug Information
Background • Lixisenatide is available in 60 countries world wide as Lyxumia
ADRs • N/V/D, HA, dizziness, and hypoglycemia Contraindications • Hypersensitivity including anaphylaxis
Warnings/Precautions
• Anti-lixisenatide antibodies• Hypersensitivity• Acute pancreatitis• Gastroparesis/slows gastric emptying
Black Box Warning
• None; only Exenatide BID and lixisenatide do NOT have the BBW for medullary thyroid carcinoma (MTC) or multiple endocrine neoplasia syndrome type 2 (MEN2)
Lixisenatide (Adlyxin). Product labeling. Sanofi. July 2016.
GLP-1 RA Adverse Events
DULA ALBI EQW ExBID LIRA LIXI Insulin Glargine
≥5%: N/V/D, Abd
pain, dyspepsia, ↓appetite, &
fatigue
≥10%: URTI, N/D, inj site rxn
≥5%: HA,
N/V/C/D, inj site
pruritus, inj site nodule, dyspepsia
≥5%: hypoglycemia, V/D/C, feeling
jittery, dizziness, HA,
dyspepsia, asthenia
≥5%:HA, N/D,
Ab formation
≥5%: N/V/D,
HA, dizziness
Severe hypogly, HSR,
retinopathy, lipodystrophy,
wt gain, peripheral
edema, allergic rxn, Ab production, CV
safety, Ca
15
ADRDULA
0.75 mg(%)
DULA 1.5 mg
(%)
ALBI(%)
EQW(%)
ExBID(%)
LIRA(%)
LIXI(%)
Insulin Glargine
(%)Nausea 12.4 21.1 11.1 14.4 34.7 20.7 25.0 1.3Diarrhea 6.7 12.6 13.1 10.5 8.6 13.1 8.0 4.0Vomiting 2.3 12.7 4.2 5.8 14.2 10.7 10.0 1.3
Lixisenatide (Adlyxin). Product labeling. Sanofi. July 2016.
Lixisenatide StudiesStudy Duration Background Therapy Detail
GetGoal-Mono 12 weeks N/A Lixisenatide vs placeboGetGoal-P 24 weeks Pioglitazone Lixisenatide vs placebo
GetGoal-Duo1 24 weeks Insulin Glargine Lixisenatide vs placeboGetGoal-L-Asia 24 weeks Basal Insulin +/- SU Lixisenatide vs placebo
Ratner 13 weeks Metformin Lixisenatide daily or BID 5, 10, 20 or 30ug vs placebo
Kapitza 28 days Metformin Lixisenatide vs Liraglutide*GetGoal-Mono
Japan LTS 76 weeks N/A Lixisenatide OL safety study
*GetGoal-L 24 weeks Basal insulin +/- metformin Lixisenatide vs placebo*GetGoal-S 24 weeks Sulfonylurea +/- metformin Lixisenatide vs placebo
*GetGoal-O 24 weeks Basal insulin and/or OAMLixisenatide vs placebo in older T2DM patients
*GetGoal-X 24 weeks Metformin Lixisenatide vs Exenatide BID
*GetGoal-M 24 weeks Metformin Lixisenatide (Morning or Evening) vs placebo*GetGoal-M-Asia 27 weeks Metformin +/- SU Lixisenatide vs placebo
*GetGoal-F1 24 weeks Metformin Lixisenatide vs placebo*GetGoal-Duo2 26 weeks Insulin Glargine +/- metformin Lixisenatide vs Insulin glulisine
Lixisenatide (Adlyxin). Product labeling. Sanofi. July 2016.
Study Wks Treatment ArmsΔ
HbA1c (%)
HbA1c< 7% (%)
Δ FPG(mg/dL)
Baselinewt (kg)
Δ Wt(kg)
Avg #
hypo event
GetGoal-Mono 12
Placebo LIXI 2 stepLIXI 1 step
-0.27-0.77-0.94
26.852.546.5
--16.2-19.8
86.189.086.5
-2-2-2
231
GetGoal-P 24 Pioglitazone
LIXI + Pioglitazone-0.34-0.9
26.452.3
-5.77-20.9
96.792.9
+0.2-0.2
211
GetGoal-Duo 1 24 Glargine
LIXI + glargine-0.4-0.7
3956
9.05.4
86.787.5
+1.2+0.3
2645
GetGoal-L-Asia
24Basal Insulin +/- SU
LIXI + Basal Insulin +/-SU
+0.11-0.77
5.235.6
+4.5-7.6
65.665.9
+0.06-0.38
3766
Kapitza 4 Liraglutide 1.8 + metLIXI 20 + met
-0.51-0.32
--
-23.4-6.13
92.991.2
-2.4-1.6
00
GetGoal-X 24 LIXI 20 + met
Exenatide 10 BID + met-0.79-0.96
48.549.8
-23.4-27.0
94.096.1
-2.8-3.8
825
GetGoal-Duo2 26
LIXI + glargine +/- metInsulin glulisine + glargine +/- met
-0.60-0.75
42.143.8
-40.0-48.5
89.888.8
+0.4+0.45
3649
Lixisenatide Results
Lixisenatide (Adlyxin). Product labeling. Sanofi. July 2016. Met=metformin; LIXI=lixisenatide; SU=sulfonylurea
LixisenatideSummary
• Lixisenatide is the 6th available GLP1RA and the 2nd once daily agent
• Lixisenatide has been compared head to head with liraglutide and exenatide twice daily– There are no clinically significant differences between
agents in terms of glycemic control• Warnings and precautions with lixisenatide are
similar to the rest of the class except there is no increased risk of MTC or MEN2
• As with all GLP1RAs, there is an increased risk of hypoglycemia when combined with a sulfonylurea
• Lixisenatide does not increase or decrease cardiovascular risk (ELIXA trial)
18

10/30/2016
4
LixisenatideSummary
• When adding lixisenatide to background therapy, or when using as monotherapy, A1c may improve ~0.5% to 1%
• When used in combination with metformin, patients may observe weight loss
• Lixisenatide offers no compelling advantages over existing GLP1RAs
19
Dermatology
Ixekizumab (Taltz)
21
Ixekizumab
22
Parameter Drug InformationGeneric IxekizumabBrand TaltzManufacturer Eli Lilly & CompanyApproval Date March 2016Approval Type BLA 351(a)
Type of drug Humanized monoclonal antibody (mAb) against IL-17A; IL-17A receptor antagonist
FDA Indications
Treatment of adults with moderate-severe plaque psoriasis who are candidate for systemic therapy or phototherapy
Dosing SQ administration: 160 mg at Week 0; followed by80mg at Weeks 2, 4, 6, 8, 10 and 12; then 80mg q4 weeks
Available preparations
Auto-injector – 80 mg/mLPrefilled Syringe – 80 mg/mL
Ixekizumab (Taltz). Product labeling. Eli Lilly & Co. March 2016.
Immunobiologics
• Numerous agents approved for plaque psoriasis– Adalimumab (TNF)– Etanercept (TNF)– Certolizumab (TNF)– Golimumab (TNF)– Ustekinumab (IL 12/23)– Apremilast (PDE-4)– Secukinumab (IL-17A)– Ixekizumab (IL-17A)
BackgroundPlaque Psoriasis (PsO)
24
Parameter Rare Disease
Background
• Most prevalent autoimmune condition• 7.5 million Americans (2 to 4% of population)• 20 to 30% will have moderate to severe dz requiring systemic Rx• 10 to 30% patient will develop psoriatic arthritis
Diagnosis & Severity
• Diagnosed by visual inspection; rare skin biopsy• Severity depends on body surface area involved
Mild = < 3%Moderate = 3 to 10%Severe = > 10%
Age of onset • Any age but typically 15 to 25 years of age
Guidelines
• Medical board of the National Psoriasis Foundation (NPF)guideline for moderate - severe psoriasis
− First line systemic agent = MTX, etanercept, adalimumab & ustekinumab (2012)
− Combine biologics with other systemic treatments (2014)
www.psoriasis.org
10/30/2016
5
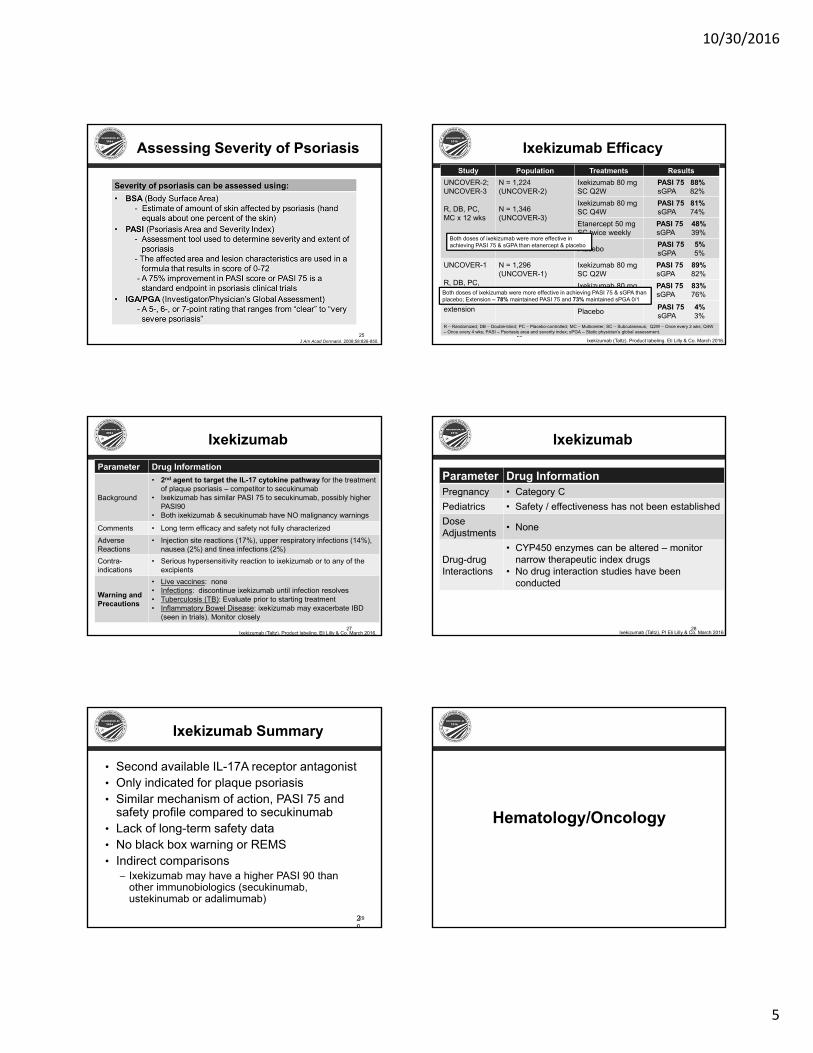
Assessing Severity of Psoriasis
J Am Acad Dermatol. 2008;58:826-850. 25
Ixekizumab Efficacy
26
Study Population Treatments ResultsUNCOVER-2; UNCOVER-3
R, DB, PC, MC x 12 wks
N = 1,224 (UNCOVER-2)
N = 1,346 (UNCOVER-3)
Adults with chronic plaque psoriasis
Ixekizumab 80 mg SC Q2W
PASI 75 88%sGPA 82%
Ixekizumab 80 mg SC Q4W
PASI 75 81%sGPA 74%
Etanercept 50 mg SC twice weekly
PASI 75 48%sGPA 39%
Placebo PASI 75 5%sGPA 5%
UNCOVER-1
R, DB, PC, MC; 12 wks + 48 wk extension
N = 1,296 (UNCOVER-1)
Adults with chronic plaque psoriasis
Ixekizumab 80 mg SC Q2W
PASI 75 89%sGPA 82%
Ixekizumab 80 mg SC Q4W
PASI 75 83%sGPA 76%
Placebo PASI 75 4%sGPA 3%
R – Randomized; DB – Double-blind; PC – Placebo-controlled; MC – Multicenter; SC – Subcutaneous; Q2W – Once every 2 wks; Q4W – Once every 4 wks; PASI – Psoriasis area and severity index; sPGA – Static physician’s global assessment.
Both doses of ixekizumab were more effective in achieving PASI 75 & sGPA than etanercept & placebo
Both doses of ixekizumab were more effective in achieving PASI 75 & sGPA than placebo; Extension – 78% maintained PASI 75 and 73% maintained sPGA 0/1
Ixekizumab (Taltz). Product labeling. Eli Lilly & Co. March 2016.
Ixekizumab
27
Parameter Drug Information
Background
• 2nd agent to target the IL-17 cytokine pathway for the treatment of plaque psoriasis – competitor to secukinumab
• Ixekizumab has similar PASI 75 to secukinumab, possibly higher PASI90
• Both ixekizumab & secukinumab have NO malignancy warnings
Comments • Long term efficacy and safety not fully characterizedAdverse Reactions
• Injection site reactions (17%), upper respiratory infections (14%), nausea (2%) and tinea infections (2%)
Contra-indications
• Serious hypersensitivity reaction to ixekizumab or to any of the excipients
Warning and Precautions
• Live vaccines: none• Infections: discontinue ixekizumab until infection resolves• Tuberculosis (TB): Evaluate prior to starting treatment• Inflammatory Bowel Disease: ixekizumab may exacerbate IBD
(seen in trials). Monitor closely
Ixekizumab (Taltz), Product labeling. Eli Lilly & Co. March 2016.
Ixekizumab
28
Parameter Drug InformationPregnancy • Category CPediatrics • Safety / effectiveness has not been establishedDose Adjustments • None
Drug-drugInteractions
• CYP450 enzymes can be altered – monitor narrow therapeutic index drugs
• No drug interaction studies have been conducted
Ixekizumab (Taltz), PI Eli Lilly & Co. March 2016
29
Ixekizumab Summary
• Second available IL-17A receptor antagonist• Only indicated for plaque psoriasis• Similar mechanism of action, PASI 75 and
safety profile compared to secukinumab• Lack of long-term safety data• No black box warning or REMS• Indirect comparisons
– Ixekizumab may have a higher PASI 90 than other immunobiologics (secukinumab, ustekinumab or adalimumab)
29
Hematology/Oncology
10/30/2016
6
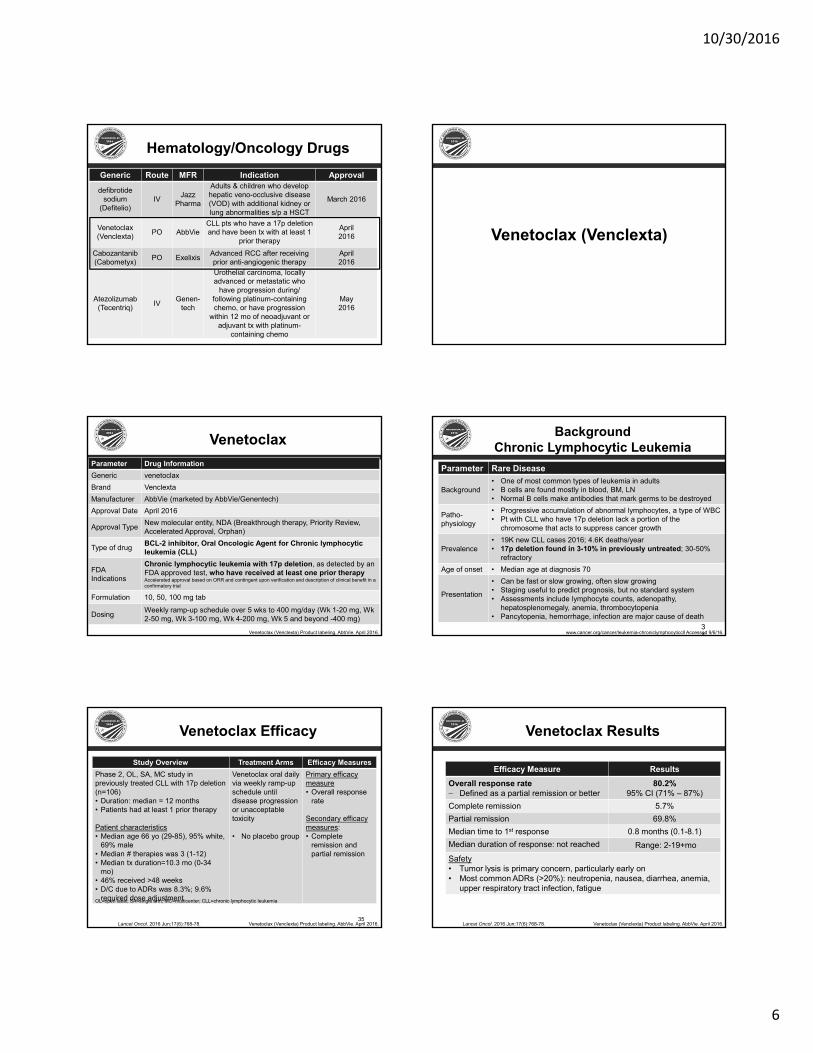
Hematology/Oncology DrugsGeneric Route MFR Indication Approval
defibrotide sodium
(Defitelio)IV Jazz
Pharma
Adults & children who develop hepatic veno-occlusive disease (VOD) with additional kidney or lung abnormalities s/p a HSCT
March 2016
Venetoclax(Venclexta) PO AbbVie
CLL pts who have a 17p deletion and have been tx with at least 1
prior therapy
April2016
Cabozantanib(Cabometyx) PO Exelixis Advanced RCC after receiving
prior anti-angiogenic therapyApril2016
Atezolizumab(Tecentriq) IV Genen-
tech
Urothelial carcinoma, locally advanced or metastatic who
have progression during/ following platinum-containing chemo, or have progression
within 12 mo of neoadjuvant or adjuvant tx with platinum-
containing chemo
May2016
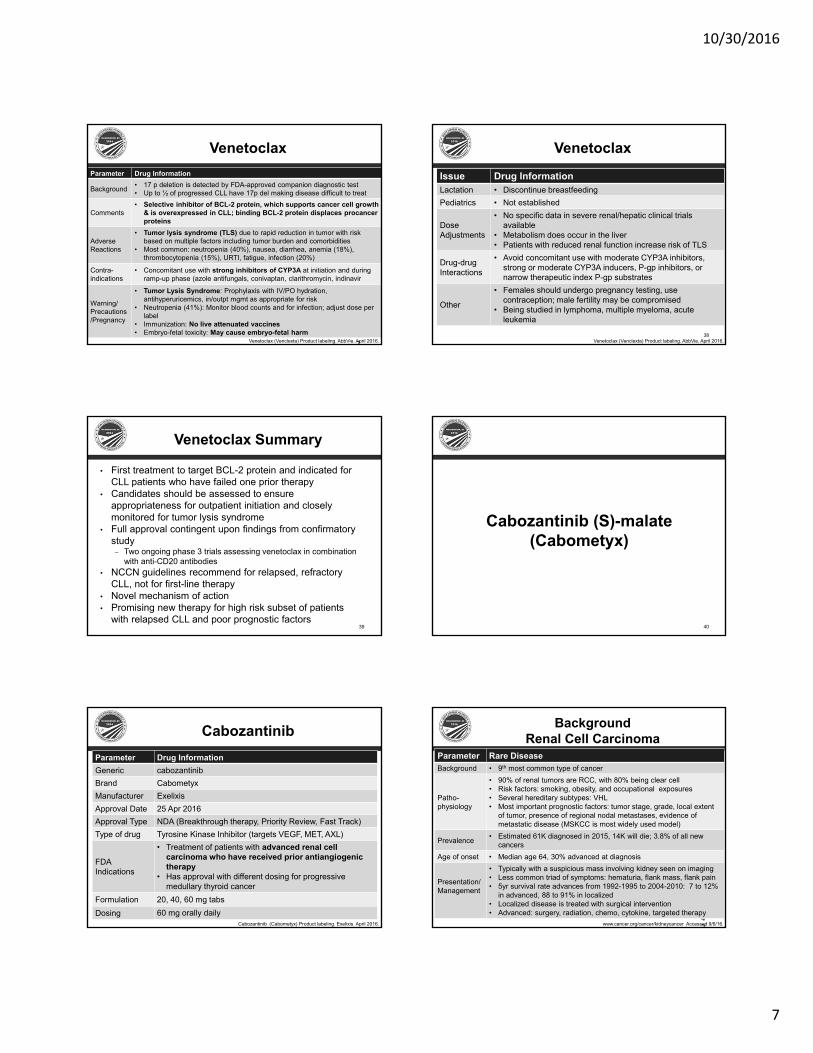
Venetoclax (Venclexta)
VenetoclaxParameter Drug InformationGeneric venetoclaxBrand VenclextaManufacturer AbbVie (marketed by AbbVie/Genentech)Approval Date April 2016
Approval Type New molecular entity, NDA (Breakthrough therapy, Priority Review, Accelerated Approval, Orphan)
Type of drug BCL-2 inhibitor, Oral Oncologic Agent for Chronic lymphocytic leukemia (CLL)
FDA Indications
Chronic lymphocytic leukemia with 17p deletion, as detected by an FDA approved test, who have received at least one prior therapyAccelerated approval based on ORR and contingent upon verification and description of clinical benefit in a confirmatory trial
Formulation 10, 50, 100 mg tab
Dosing Weekly ramp-up schedule over 5 wks to 400 mg/day (Wk 1-20 mg, Wk 2-50 mg, Wk 3-100 mg, Wk 4-200 mg, Wk 5 and beyond -400 mg)
Venetoclax (Venclexta) Product labeling. AbbVie. April 2016. 34
Background Chronic Lymphocytic Leukemia
Parameter Rare Disease
Background• One of most common types of leukemia in adults• B cells are found mostly in blood, BM, LN• Normal B cells make antibodies that mark germs to be destroyed
Patho-physiology
• Progressive accumulation of abnormal lymphocytes, a type of WBC• Pt with CLL who have 17p deletion lack a portion of the
chromosome that acts to suppress cancer growth
Prevalence• 19K new CLL cases 2016; 4.6K deaths/year• 17p deletion found in 3-10% in previously untreated; 30-50%
refractoryAge of onset • Median age at diagnosis 70
Presentation
• Can be fast or slow growing, often slow growing• Staging useful to predict prognosis, but no standard system• Assessments include lymphocyte counts, adenopathy,
hepatosplenomegaly, anemia, thrombocytopenia• Pancytopenia, hemorrhage, infection are major cause of death
www.cancer.org/cancer/leukemia-chroniclymphocyticcll Accessed 9/6/16.
Study Overview Treatment Arms Efficacy MeasuresPhase 2, OL, SA, MC study in previously treated CLL with 17p deletion (n=106)• Duration: median = 12 months• Patients had at least 1 prior therapy
Patient characteristics• Median age 66 yo (29-85), 95% white,
69% male• Median # therapies was 3 (1-12)• Median tx duration=10.3 mo (0-34
mo)• 46% received >48 weeks• D/C due to ADRs was 8.3%; 9.6%
required dose adjustment
Venetoclax oral daily via weekly ramp-up schedule until disease progression or unacceptable toxicity
• No placebo group
Primary efficacy measure• Overall response
rate
Secondary efficacy measures: • Complete
remission and partial remission
35
Venetoclax Efficacy
Lancet Oncol. 2016 Jun;17(6):768-78. Venetoclax (Venclexta) Product labeling. AbbVie. April 2016.
OL=open label; SA=single arm; MC=multicenter; CLL=chronic lymphocytic leukemia
Venetoclax Results
• ResultsEfficacy Measure ResultsOverall response rate− Defined as a partial remission or better
80.2%95% CI (71% – 87%)
Complete remission 5.7%Partial remission 69.8%Median time to 1st response 0.8 months (0.1-8.1)Median duration of response: not reached Range: 2-19+moSafety• Tumor lysis is primary concern, particularly early on• Most common ADRs (>20%): neutropenia, nausea, diarrhea, anemia,
upper respiratory tract infection, fatigue
Lancet Oncol. 2016 Jun;17(6):768-78. Venetoclax (Venclexta) Product labeling. AbbVie. April 2016.
10/30/2016
7
37
VenetoclaxParameter Drug Information
Background • 17 p deletion is detected by FDA-approved companion diagnostic test• Up to ½ of progressed CLL have 17p del making disease difficult to treat
Comments• Selective inhibitor of BCL-2 protein, which supports cancer cell growth
& is overexpressed in CLL; binding BCL-2 protein displaces procancer proteins
Adverse Reactions
• Tumor lysis syndrome (TLS) due to rapid reduction in tumor with risk based on multiple factors including tumor burden and comorbidities
• Most common: neutropenia (40%), nausea, diarrhea, anemia (18%), thrombocytopenia (15%), URTI, fatigue, infection (20%)
Contra-indications
• Concomitant use with strong inhibitors of CYP3A at initiation and during ramp-up phase (azole antifungals, conivaptan, clarithromycin, indinavir
Warning/ Precautions/Pregnancy
• Tumor Lysis Syndrome: Prophylaxis with IV/PO hydration, antihyperuricemics, in/outpt mgmt as appropriate for risk
• Neutropenia (41%): Monitor blood counts and for infection; adjust dose per label
• Immunization: No live attenuated vaccines• Embryo-fetal toxicity: May cause embryo-fetal harm
Venetoclax (Venclexta) Product labeling. AbbVie. April 2016.
Venetoclax
38
Issue Drug InformationLactation • Discontinue breastfeedingPediatrics • Not established
Dose Adjustments
• No specific data in severe renal/hepatic clinical trials available
• Metabolism does occur in the liver• Patients with reduced renal function increase risk of TLS
Drug-drugInteractions
• Avoid concomitant use with moderate CYP3A inhibitors, strong or moderate CYP3A inducers, P-gp inhibitors, or narrow therapeutic index P-gp substrates
Other
• Females should undergo pregnancy testing, use contraception; male fertility may be compromised
• Being studied in lymphoma, multiple myeloma, acute leukemia
Venetoclax (Venclexta) Product labeling. AbbVie. April 2016.
Venetoclax Summary
• First treatment to target BCL-2 protein and indicated for CLL patients who have failed one prior therapy
• Candidates should be assessed to ensure appropriateness for outpatient initiation and closely monitored for tumor lysis syndrome
• Full approval contingent upon findings from confirmatory study
– Two ongoing phase 3 trials assessing venetoclax in combination with anti-CD20 antibodies
• NCCN guidelines recommend for relapsed, refractory CLL, not for first-line therapy
• Novel mechanism of action• Promising new therapy for high risk subset of patients
with relapsed CLL and poor prognostic factors39
Cabozantinib (S)-malate (Cabometyx)
40
CabozantinibParameter Drug InformationGeneric cabozantinibBrand CabometyxManufacturer ExelixisApproval Date 25 Apr 2016Approval Type NDA (Breakthrough therapy, Priority Review, Fast Track)Type of drug Tyrosine Kinase Inhibitor (targets VEGF, MET, AXL)
FDA Indications
• Treatment of patients with advanced renal cell carcinoma who have received prior antiangiogenic therapy
• Has approval with different dosing for progressive medullary thyroid cancer
Formulation 20, 40, 60 mg tabsDosing 60 mg orally daily
Cabozantinib (Cabometyx) Product labeling. Exelixis. April 2016. 42
Background Renal Cell Carcinoma
Parameter Rare DiseaseBackground • 9th most common type of cancer
Patho-physiology
• 90% of renal tumors are RCC, with 80% being clear cell• Risk factors: smoking, obesity, and occupational exposures • Several hereditary subtypes: VHL• Most important prognostic factors: tumor stage, grade, local extent
of tumor, presence of regional nodal metastases, evidence of metastatic disease (MSKCC is most widely used model)
Prevalence • Estimated 61K diagnosed in 2015, 14K will die; 3.8% of all new cancers
Age of onset • Median age 64, 30% advanced at diagnosis
Presentation/Management
• Typically with a suspicious mass involving kidney seen on imaging• Less common triad of symptoms: hematuria, flank mass, flank pain• 5yr survival rate advances from 1992-1995 to 2004-2010: 7 to 12%
in advanced, 88 to 91% in localized• Localized disease is treated with surgical intervention• Advanced: surgery, radiation, chemo, cytokine, targeted therapy
www.cancer.org/cancer/kidneycancer Accessed 9/6/16.
10/30/2016
8
43
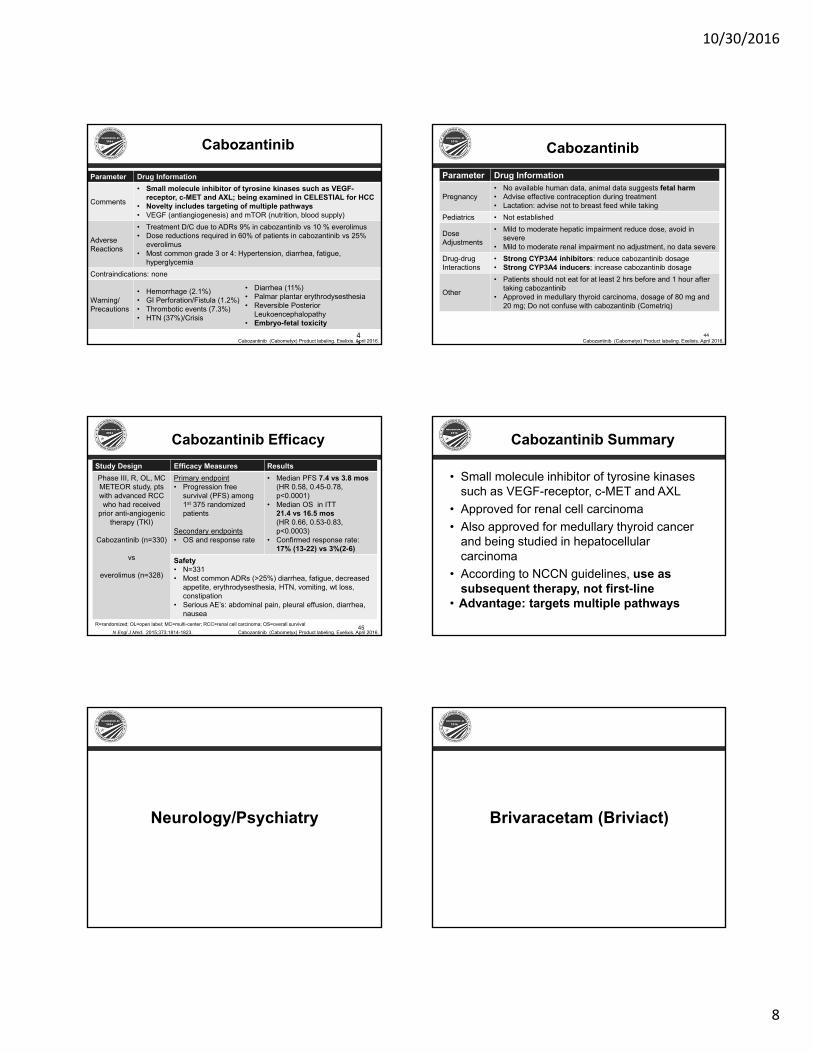
Cabozantinib
Parameter Drug Information
Comments
• Small molecule inhibitor of tyrosine kinases such as VEGF-receptor, c-MET and AXL; being examined in CELESTIAL for HCC
• Novelty includes targeting of multiple pathways • VEGF (antiangiogenesis) and mTOR (nutrition, blood supply)
Adverse Reactions
• Treatment D/C due to ADRs 9% in cabozantinib vs 10 % everolimus• Dose reductions required in 60% of patients in cabozantinib vs 25%
everolimus• Most common grade 3 or 4: Hypertension, diarrhea, fatigue,
hyperglycemiaContraindications: none
Warning/ Precautions
• Hemorrhage (2.1%)• GI Perforation/Fistula (1.2%)• Thrombotic events (7.3%)• HTN (37%)/Crisis
• Diarrhea (11%)• Palmar plantar erythrodysesthesia• Reversible Posterior
Leukoencephalopathy• Embryo-fetal toxicity
Cabozantinib (Cabometyx) Product labeling. Exelixis. April 2016.
Cabozantinib
44
Parameter Drug Information
Pregnancy• No available human data, animal data suggests fetal harm• Advise effective contraception during treatment• Lactation: advise not to breast feed while taking
Pediatrics • Not established
Dose Adjustments
• Mild to moderate hepatic impairment reduce dose, avoid in severe
• Mild to moderate renal impairment no adjustment, no data severeDrug-drugInteractions
• Strong CYP3A4 inhibitors: reduce cabozantinib dosage• Strong CYP3A4 inducers: increase cabozantinib dosage
Other
• Patients should not eat for at least 2 hrs before and 1 hour after taking cabozantinib
• Approved in medullary thyroid carcinoma, dosage of 80 mg and 20 mg; Do not confuse with cabozantinib (Cometriq)
Cabozantinib (Cabometyx) Product labeling. Exelixis. April 2016.
Study Design Efficacy Measures ResultsPhase III, R, OL, MC METEOR study, pts with advanced RCC who had received
prior anti-angiogenic therapy (TKI)
Cabozantinib (n=330)
vs
everolimus (n=328)
Primary endpoint• Progression free
survival (PFS) among 1st 375 randomized patients
Secondary endpoints• OS and response rate
• Median PFS 7.4 vs 3.8 mos (HR 0.58, 0.45-0.78, p<0.0001)
• Median OS in ITT 21.4 vs 16.5 mos (HR 0.66, 0.53-0.83, p<0.0003)
• Confirmed response rate: 17% (13-22) vs 3%(2-6)
Safety• N=331• Most common ADRs (>25%) diarrhea, fatigue, decreased
appetite, erythrodysesthesia, HTN, vomiting, wt loss, constipation
• Serious AE’s: abdominal pain, pleural effusion, diarrhea, nausea
45
Cabozantinib Efficacy
R=randomized; OL=open label; MC=multi-center; RCC=renal cell carcinoma; OS=overall survivalN Engl J Med. 2015;373:1814-1823. Cabozantinib (Cabometyx) Product labeling. Exelixis. April 2016.
Cabozantinib Summary
• Small molecule inhibitor of tyrosine kinases such as VEGF-receptor, c-MET and AXL
• Approved for renal cell carcinoma• Also approved for medullary thyroid cancer
and being studied in hepatocellular carcinoma
• According to NCCN guidelines, use as subsequent therapy, not first-line
• Advantage: targets multiple pathways
Neurology/Psychiatry Brivaracetam (Briviact)

10/30/2016
9
Brivaracetam
49
Parameter Drug InformationGeneric brivaracetamBrand BriviactManufacturer UCB Approval Date February 2016Approval Type New molecular entityType of drug Antiepileptic drug (AED)
FDA Indications Adjunctive therapy in the treatment of partial-onset seizures in patients ≥16 years old
Dosing 50 mg BID and titrate to 100 mg BID
Available preparations
Tablets: 10, 25, 50, 75, and 100 mgOral solution: 10 mg/mLInjection for IV use: 50 mg/5 mL single-dose vial
Briviact (brivaracetam). Product labeling. Smyrna, GA: UCB, Inc.; Feb 2016.
Brivaracetam
50
Parameter Drug Information
Adverse Reactions
Most common (≥5%): somnolence and sedation (16%), dizziness (12%), fatigue (9%), and nausea and vomiting (5%)
Contra-indications
Hypersensitivity to brivaracetam or inactive ingredients (bronchospasm and angioedema have occurred)
BBW or Significant Adverse Effects
• Suicidal behavior and ideation• Neurological adverse reactions• Psychiatric adverse reactions
Briviact (brivaracetam). Product labeling. Smyrna, GA: UCB, Inc.; Feb 2016.
Comparisons
51
Parameter Brivaracetam Levetiracetam
Indication
• Adjunctive therapy in the tx of partial-onsetseizures in pts 16yo and older with epilepsy
• Partial onset seizures in pts ≥ 1 mo of age with epilepsy
• Myoclonic seizures in pts ≥12 yo with juvenile myoclonic epilepsy
• Primary generalized tonic-clonicseizures in patients ≥6 yo with idiopathic generalized epilepsy
Half Life • 9 hours • 7 hours
MOA • High and selective affinity for synaptic vesicle protein 2A (SV2A) in the brain, which may contribute to the anticonvulsant effect
Strengths
Tabs: 10, 25, 50, 75, & 100 mg: Oral solution: 10 mg/mL; Injection for IV use: 50 mg/5 mL single-dose vial
• IR & XR Tabs: 250, 500, 750, 1000 mg• Oral Solution: 100mg/mL• Injection for IV use: 500mg/5mL• Orally disintegrating tablet
Chemical Structure
Briviact (brivaracetam). Product labeling. Smyrna, GA: UCB, Inc.; Feb 2016.
Brivaracetam
52
Parameter Drug InformationPregnancy • Category CPediatrics • Patients < 16yo have not been established
Dose Adjustments
• No adjustment for renal• Adjustments necessary for all stages of
hepatic impairment
Drug-drugInteractions
• Rifampin decreases brivaracetam plasma concentrations by 45% (CYP2C19 induction)
• Co-admin with carbamazepine can ↑exposure of active metabolite of carbamazepine
• Increases concentrations of phenytoinBriviact (brivaracetam). Product labeling. Smyrna, GA: UCB, Inc.; Feb 2016.
Brivaracetam Efficacy
• ScaleStudy Design Treatment Arms Endpoints
Three R, DB, PC, MCstudies; Duration: 12 weeksStudy 1 (n=398); Study 2 (n=396); Study 3 (n=760)
Baseline characteristics: • ≥ 8 partial onset
seizures (POS) at baseline
• Not adequately controlled with 1-2 concomitant AEDs
R (1:1:1:1)3 doses (20mg, 50mg,
100mg)
BrivaracetamBID
vs
Placebo
Primary endpoint:Study 1 and 2: % ↓ in POS frequency over a 7-day period
Study 3: % ↓ in POS frequency over PBO over a 28-day period; ≥50% responder rate
Epilepsia. 2014;55(1):47-56.Epilepsia. 2014;55(1):57-66.
Epilepsia. 2015;56(12):1890-1898.
Brivaracetam Results
• ScaleStudy Endpoint % decrease in POS over placeboBrivaracetam
20mg 50mg 100mg PBO
Study 1 % Dec in POS -6.8%* -6.5% -11.7%* -5mg 20mg 50mg PBO
Study 2 % Dec in POS -0.9% -4.1% -12.8%* 100mg 200mg - PBO
Study 3n=760
% Dec in POS -22.8%* -23.2%*
≥ 50% responder rates 38.9%* 37.8%* 21.6%
POS = partial onset seizures; PBO = placebo*Statistically significant (p < 0.001) compared to placebo
Epilepsia. 2014;55(1):47-56.Epilepsia. 2014;55(1):57-66.
Epilepsia. 2015;56(12):1890-98.

10/30/2016
10
55
Brivaracetam Summary
• Discontinuation rates due to ADRs– 5% (50 mg/day)– 8% (100 mg/day)– 7% (200 mg/day) – 4% (placebo)
• Place in therapy– Similar in structure to levetiracetam– Less titration– Controlled substance (C-V) designation– No compelling advantage over levetiracetam
55Briviact (brivaracetam). Product labeling. UCB, Inc.; February 2016.
Pimavanserin (Nuplazid)
56
Pimavanserin
57
Parameter Drug InformationGeneric Pimavanserin Brand NuplazidManufacturer Acadia Pharmaceuticals Inc.FDA Approval Date April 29, 2016
Approval Type 505(b)Type of drug Atypical antipsychotic
FDA Indications Hallucinations and delusions associated with Parkinson’s disease psychosis (PDP)
Dosing 34 mg (2 tabs) PO daily, without titration, with or without food
Available preparations Oral IR tablets, 17 mg
Nuplazid (pimavanserin). Product labeling. Acadia Pharmaceuticals Inc. April 2016.
Pimavanserin
58
Parameter Drug Information
Background
• FDA agreed in 2013 to approve NDA on 1 positive study; 3 additional studies failed to show benefit
• First AAP approved for psychosis in Parkinson’s disease• 5-HT2A inverse agonist which lacks dopamine receptor
interaction and the associated motor function effects
Comments • QT prolongation; avoid with other QT prolonging agents or risks
Adverse Reactions
• Peripheral edema, confusion, hallucination, abnormal gait, nausea, constipation
Contra-indications • None
Black Box Warning
• Increased risk of death in elderly patients with dementia-related psychosis (class warning)
Nuplazid (pimavanserin). Product labeling. Acadia Pharmaceuticals Inc. April 2016.
Pimavanserin
59
Parameter Drug Information
Pregnancy
• No human data• Animal data showed no teratogenicity, however
decreased rat pup survival and weight at 2x max recommended dose
Pediatrics • Safety and effectiveness have not been established
Dose Adjustments
• No dose adjustments required for mild-moderate renal impairment or geriatric patients
• Not recommended in hepatic impairment or severe renal impairment
Drug-drugInteractions
• Strong CYP3A4 Inhibitors – reduce dose by 50%• Strong CYP3A4 Inducers – monitor for reduced
efficacy
Nuplazid (pimavanserin). Product labeling. Acadia Pharmaceuticals Inc. April 2016.
Psychosis in Parkinson’s Disease (PDP)Current standards of care
• 2006 American Academy of Neurology– Recommend clozapine (Level B), quetiapine
(Level C)– Clozapine requires frequent hematologic
monitoring for potentially fatal agranulocytosis• 2016 systematic review in the Journal of
Geriatric Psychiatry and Neurology– Daily doses of 100 mg quetiapine do not provide
significant symptom relief for PD psychosis– Available quetiapine efficacy studies have many
limitations
60Neurology 2006;66(7):996-1002.
J Geriatr Psychiatry Neurol 2016;pii:0891988716640378.

10/30/2016
11
Pimavanserin Efficacy
61
Study Design Treatment Efficacy Measures
ResultsΔ SAPS-PD
R, DB, MC, OP, PCDuration: 6 weeks, n = 199
Patient characteristics• 40 years or older• PD >1 year• Active psychosis after
PD dx and ≥1 month• SAPS-PD global item
score ≥3 and non-global item >3
R (1:1)
Pimavanserin34mg PO
daily
vs
PBO
PrimarySAPS-PD
SecondaryUPDRSCGI
ExploratorySCOPA-sleepCBS
Pimavanserin= -5.79PBO = -2.73
Difference from PBO = -3.06
95% CI (-4.9, -1.2)
NNT = 11
R=randomized; DB=double-blind; OP=outpatient; PC=placebo-controlled; MC=multi-center; LSM=least-squares mean; PD=Parkinson’s Disease; SAPS-PD=Scale for the Assessment of Positive Symptoms in Parkinson’s Disease; UPDRS=Unified Parkinson’s Disease Rating Scale (UPDRS); CGI=Clinical Global Impression scale; SCOPA=Scales for Outcomes in Parkinson’s Disease; CBS=Caregiver Burden Scale;
FDA Briefing Document. Psychopharmacologic Drugs Advisory Committee. March 2016.
Pimavanserin Safety
• Included data from 2 safety extension trials• OR for serious adverse effects, including death
– 2.4 (95% CI 1.0 to 5.7, p=0.05) for 34 mg vs. placebo
• Deaths considered class effect of antipsychotic use in the elderly dementia population
• Common adverse reactions– Peripheral edema (7% vs. 2% placebo)– Confusional state (6% vs. 3% placebo)– QT prolongation of 10-14 msec found at 68 mg, not
studied at recommended 34 mg dose62
FDA Briefing Document. Psychopharmacologic Drugs Advisory Committee. March 2016.
63
Pimavanserin Summary
• First drug approved for the indication of PDP• Unique mechanism of action• Current recommendations include use of
quetiapine or clozapine first• Very costly compared to generic AAPs• No long-term safety data• Place in therapy currently unclear
63
Daclizumab(Zinbryta)
Daclizumab
65
Parameter Drug InformationGeneric DaclizumabBrand ZinbrytaManufacturer BiogenApproval Date May 27, 2016Approval Type BLA
Type of drug Interleukin-2 (IL-2) inhibitor; Immunosuppressant/monoclonal antibody
FDA Indications Multiple Sclerosis, relapsingDosing 150 milligrams once monthly; self-injectableAvailable preparations
150 mg/mL solution in a single-dose prefilled syringe Limited distribution; REMS
Zinbryta (daclizumab). Product labeling. Biogen, Inc. May 2016.
Daclizumab
66
Parameter Drug Information
Background• Daclizumab was previously marketed as Zenapax for the
prophylaxis of acute organ rejection in patients receiving renal transplants (discontinued in 2009 for commercial reasons)
Pharmaco-kinetics
• Protein binding (>99%) primarily to serum albumin and alpha1-acid glycoprotein
• Metabolism: Hepatic, primarily by CYP3A4 and CYP2D6; major metabolite, DM-3411 (inactive)
Adverse Reactions
Nasopharyngitis, upper respiratory infections, rash, influenza, dermatitis, oropharyngeal pain, bronchitis, eczema, lymphadenopathy, tonsillitis, acne
Serious Adverse Reactions
• Risk of anaphylaxis and angioedema • Increased risk of infections • Increased risk of depression and suicide
Zinbryta (daclizumab). Product labeling. Biogen, Inc. May 2016.

10/30/2016
12
Daclizumab
Zinbryta (daclizumab).FDA Summary review. May 2016.
Parameter Drug Information
Warnings & Precautions
• Autoimmune hepatitis, bilirubin elevation, skin reactions, lymphadenopathy, colitis, hypersensitivity, infections, depression, and suicide
Contra-indications
• Pre-existing hepatic disease or hepatic impairment • History of autoimmune hepatitis or other autoimmune
condition involving the liver • History of hypersensitivity to daclizumab or any other
component of the formulation BBW Or Significant Adverse Effects
• Hepatic injury including autoimmune hepatitis• Other immune-mediated disorders
Comments • Available only through a Risk Evaluation and Mitigation Strategy (REMS) program
Daclizumab Efficacy
• ResultsStudy Design Treatment Arms Primary Endpoints
DECIDE Trial: Phase III, R, DB, AC (301), PC (201), PG, FD; n= 2462Duration: 1-2 years
Patient characteristics• Adults with relapsing MS• 41% had prior disease
modifying therapy• 34% had prior interferon
beta therapy• Baseline MSIS-29= 21.7
1:1
Daclizumab
vs
Interferon beta-1a
PrimaryAnnual relapse rate (ARR)
Secondary• # of new or newly enlarging
T2 hyper-intense lesions• Confirmed disability
progression• Patients that are relapse
free• >7.5-point worsening from
baseline MSIS-29 PIS AC= active controlled; PC= placebo controlled; PG= parallel grouped; DB= double blind; FD= fixed dose; R= random; MS=multiple sclerosis; ARR= annual relapse rate; PIS= physical impact score; MSIS-29= multiple sclerosis impact scale
N Engl J Med. 2015;373:1418-1428.
Daclizumab Results
69
Daclizumab150 mg SC Q4W
(n = 919)
Interferon 30 mcg IM QW
(n = 922)P-Value
Clinical Results
ARR 0.216 0.393
< 0.0001Relative reduction 45% N/A
Proportion relapse free (wk 144) 67% 51%Proportion with 12-week confirmed disability progression 16% 20% 0.16
NNT 7
MRI ResultsMean number of new or newly enlarging T2 hyperintense lesions
4.31 9.44
< 0.0001Relative reduction 54% N/AProportion of patients with clinically meaningful worsening of MSIS-29 score
19% 23%
N Engl J Med. 2015;373:1418-1428.
Daclizumab
Zinbryta (daclizumab).FDA Summary review. May 2016.
Parameter Drug Information
Drug Interactions
• Avoid concomitant use: BCG, natalizumab, pimecrolimus, tacrolimus (topical), tofacitinib, live vaccines
Pregnancy Concerns
• ADEs were observed in some animal reproduction studies
• Use is not recommended for the treatment of MS in pregnant women
Monitoring Parameters
• Serum transaminases, total bilirubin; evaluate for TB and immunization status
Daclizumab Comparisons
Parameter Zinbryta(daclizumab)
Avonex(Interferon
Beta-1a)
Copaxone(glatiramer
acetate)
Betaseron(Interferon
Beta-1b)
Plegridy (Peginterferon
Beta-1a)
Tecfidera(Dimethyl Fumarate)
Dosage form SQ IM SQ SQ SQ Capsule
Dosing Monthly Weekly QD-3XW QOD Q2W BID
Generic No No No No No No
Renal adjustments No No No No No No
Hepaticadjustments
Yes(BBW) No No No No No
ARR 0.46 0.87 0.67 0.67 0.65 0.50
NNT 7 12 17 6 8 6ARR = annual relapse rate (ARR = [% relapse in treatment group]/[% relapse in placebo group]; NNT = number needed to treat 71
Lexicomp.com. Accessed 8/11/16
Daclizumab Summary
• Disease modifying monoclonal antibody• Because of its safety profile, daclizumab should be
reserved for patients who have had an inadequate response to 2 or more MS drugs
• Daclizumab is a costly injectable with a mandatory REMS program due to the risk of severe hepatic injury
• Daclizumab is the only once monthly self-injectable– Indicated for relapsing MS– Data from head to head trials have shown it to be more
effective than interferon beta-1a and placebo in treating MS72

10/30/2016
13
Gastrointestinal Obeticholic acid(Ocaliva)
74
Obeticholic acid
75
Parameter Drug InformationGeneric Obeticholic acid Brand OcalivaManufacturer Intercept Pharmaceuticals, IncApproval Date May 27, 2016Approval Type New molecular entity; NDA 505(b)Type of drug Farnesoid X receptor (FXR) agonist
FDA Indications
Tx of primary biliary cholangitis (PBC) in combination with ursodeoxycholic acid (UDCA) in adults with an inadequate response to UDCA, or as monotherapy in adults unable to tolerate UDCA
Dosing
5mg orally once daily in adults who have not achieved an adequate response to an appropriate dosage of UDCA for at least 1 year or are intolerant to UDCA; dose is titrated based on alk phos and/or Tbili; Max dose: 10mg once daily
Preparations 5mg and 10mg tablets
Ocaliva (Obeticholic acid ). Package insert. Intercept Pharma. May 2016.
Obeticholic acid
76
Parameter Drug InformationDrug Interactions
• Warfarin = potential decreased INR• CYP1A2 substrates with narrow therapeutic index (theophylline)
Adverse Reactions
(≥ 5%): pruritus, fatigue, abdominal pain and discomfort, rash, oropharyngeal pain, dizziness, constipation, arthralgia, thyroid function abnormality, and eczema
Contra-indications • Patients with complete biliary obstruction
Warnings & Precautions
• Liver-Related ADRs: Monitor for elevations in LFTs & development of liver-related ADRs; weigh the potential risk against the benefits of continuing tx. Do not exceed 10 mg qday. Adjust the dose for patients with moderate or severe hepatic impairment. D/C in patients who develop complete biliary obstruction
• Severe Pruritus: addition of bile acid binding resins or antihistamines; reduce dose and/or temporary dose interruption
• Reduction in HDL: Monitor for changes in serum lipid levels during tx
Ocaliva (Obeticholic acid ). Package insert. Intercept Pharma. May 2016.
Clinical TrialNo improvement in survival or disease-related symptoms has been establishedPOISE Trial: R (1:1:1), DB, PC, 12 month trial (n=216) pts with PBC taking UDCA for ≥ 12mo or who could not tolerate UDCABaseline characteristics• ALP ≥1.67x ULN; Tbili between 1 and 2 x ULN• Excluded if other liver disease, MELD score ≥15• Primary endpoint: composite (↓ ALP number and %, ↓Tbili)
77
Obeticholic acid
Ocaliva (obeticholic acid ). Product labeling. Intercept Pharma. May 2016.
Obet acid10mg (n=73)
Obet acidtitration (n=70)
PBO(n=73)
Primary composite endpointResponder rate, (%) [95% CI] 48 [36, 60] 46 [34, 58] 10 [4,19]
Components of Primary endpointALP < 1.67x ULN, n (%) 40 (55) 33 (47) 12 (16)Dec in ALP at least 15%, n (%) 57 (78) 54 (77) 21 (29)Total bili ≤ ULN, n (%) 60 (82) 62 (89) 57 (78) 7
8
Obeticholic acidSummary
• For primary biliary cholangitis (PBC) after UDCA therapy or those who cannot tolerate UDCA
• Not effective for alcoholic liver disease• Not effective for NAFLD or NASH
78
10/30/2016
14
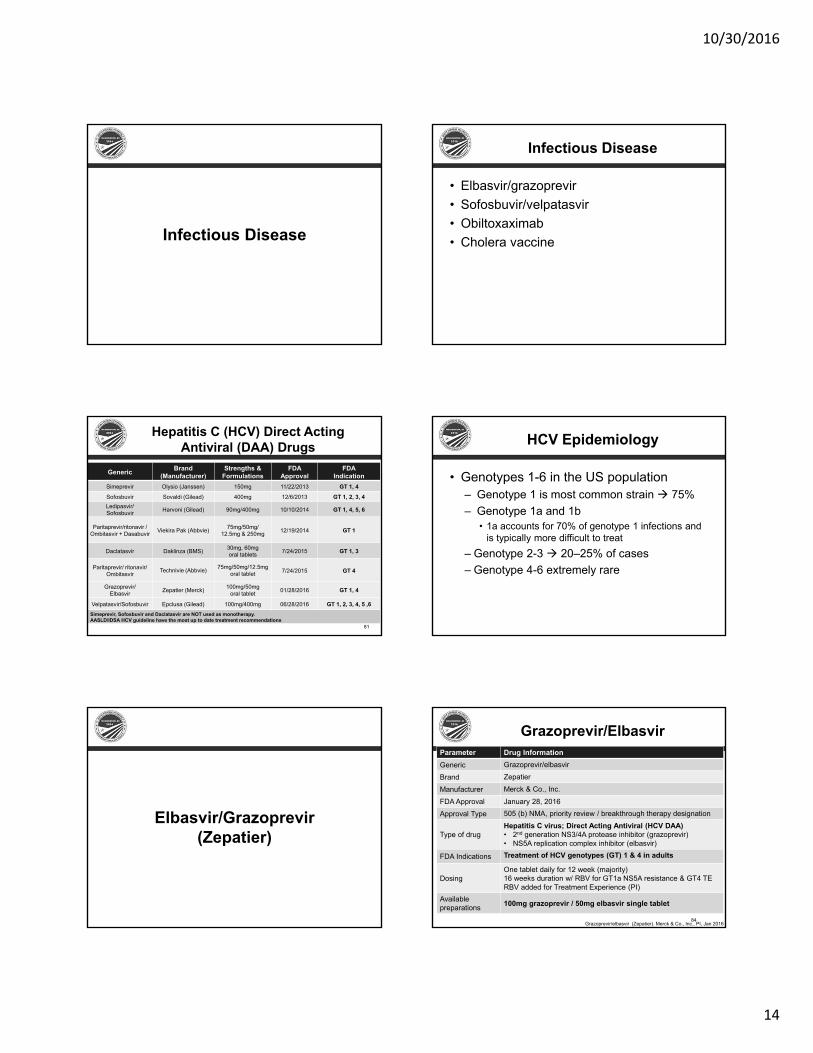
Infectious Disease
Infectious Disease
• Elbasvir/grazoprevir• Sofosbuvir/velpatasvir • Obiltoxaximab• Cholera vaccine
Hepatitis C (HCV) Direct Acting Antiviral (DAA) Drugs
81
Generic Brand (Manufacturer)
Strengths & Formulations
FDA Approval
FDAIndication
Simeprevir Olysio (Janssen) 150mg 11/22/2013 GT 1, 4
Sofosbuvir Sovaldi (Gilead) 400mg 12/6/2013 GT 1, 2, 3, 4Ledipasvir/Sofosbuvir Harvoni (Gilead) 90mg/400mg 10/10/2014 GT 1, 4, 5, 6
Paritaprevir/ritonavir /Ombitasvir + Dasabuvir Viekira Pak (Abbvie) 75mg/50mg/
12.5mg & 250mg 12/19/2014 GT 1
Daclatasvir Daklinza (BMS) 30mg, 60mgoral tablets 7/24/2015 GT 1, 3
Paritaprevir/ ritonavir/Ombitasvir Technivie (Abbvie) 75mg/50mg/12.5mg
oral tablet 7/24/2015 GT 4
Grazoprevir/Elbasvir Zepatier (Merck) 100mg/50mg
oral tablet 01/28/2016 GT 1, 4
Velpatasvir/Sofosbuvir Epclusa (Gilead) 100mg/400mg 06/28/2016 GT 1, 2, 3, 4, 5 ,6Simeprevir, Sofosbuvir and Daclatasvir are NOT used as monotherapy.AASLD/IDSA HCV guideline have the most up to date treatment recommendations
HCV Epidemiology
• Genotypes 1-6 in the US population– Genotype 1 is most common strain 75%– Genotype 1a and 1b
• 1a accounts for 70% of genotype 1 infections and is typically more difficult to treat
– Genotype 2-3 20–25% of cases– Genotype 4-6 extremely rare
Elbasvir/Grazoprevir(Zepatier)
Grazoprevir/Elbasvir
84
Parameter Drug InformationGeneric Grazoprevir/elbasvirBrand ZepatierManufacturer Merck & Co., Inc.FDA Approval January 28, 2016Approval Type 505 (b) NMA, priority review / breakthrough therapy designation
Type of drugHepatitis C virus; Direct Acting Antiviral (HCV DAA)• 2nd generation NS3/4A protease inhibitor (grazoprevir)• NS5A replication complex inhibitor (elbasvir)
FDA Indications Treatment of HCV genotypes (GT) 1 & 4 in adults
DosingOne tablet daily for 12 week (majority) 16 weeks duration w/ RBV for GT1a NS5A resistance & GT4 TERBV added for Treatment Experience (PI)
Availablepreparations 100mg grazoprevir / 50mg elbasvir single tablet
Grazoprevir/elbasvir (Zepatier). Merck & Co., Inc., PI, Jan 2016

10/30/2016
15
Grazoprevir/Elbasvir
85
Parameter Drug Information
Background
• Grazoprevir = 2nd gen protease inhibitor (PI)• Multiple DDI (esp HIV)• Contraindicated in mod-severe liver disease; LFTs testing required
• Elbasvir = NS5A inhibitor • HCV GT1a reduced response w/ NS5A RAVs
• Single daily tablet GT1 & 4 for 12 weeks• Difficult to treat patients – increase duration (16 wks) & + RBV
• Studied in advance kidney dz, & opiate sub. therapy• SVR >90% (comparable to Harvoni or Viekira)
Comments• Niche in severe kidney dz (CKD 4 or 5 on dialysis)• Testing for NS5A resistance in HCV GT1a prior to treatment• Hepatic testing prior and during treatment
Adverse Reactions
• Fatigue, headache and nausea • Anemia and headache in ZEP + RBV for 16 weeks
Warning and Precautions
• ALT elevations: hepatic testing prior to treatment and 8 wks• Risk associated with ribavirin combination treatment
Contra-indications
• Moderate or severe hepatic impairment (Child-Pugh B or C)• OAT1B1/3 inhibitors, strong CYP3A inducers and efavirenz
Grazoprevir/elbasvir (Zepatier). Merck & Co., Inc., PI, Jan 2016
Grazoprevir/Elbasvir
Parameter Drug InformationPregnancy Category BPediatrics Safety and efficacy have not been established
DoseAdjustments
No dose adjustments are required for geriatric patients, or mild hepatic impairment (Child-Pugh A). No dose adjustment for ANY degree of renal impairment including dialysis
Drug-druginteractions
• OATP1B1/3 inhibitors (e.g. atazanavir, darunavir, lopinavir, saquinavir, tipranavir, cyclosporine)
• CYP3A Inducers (e.g. carbamazepine, phenytoin, rifampin, St. John’s Wort) efavirenz
Grazoprevir/elbasvir (Zepatier). Merck & Co., Inc., PI, Jan 2016
87
Study Entry Criteria Study Design Interventions with SVR12 Primary Endpoint
C-EDGE TNN=316
12 weeks
GT 1,4,5,6; TN +cirrhosis
RCT, DB, PC, MC
2:1
GZR/EBRPBO (followed by OL GZR/EBR)
C-EDGE CO-INFECTION
N=21812 weeks
GT 1,4,5,6; TN +cirrhosis HIV co-infxn OL, SA, MC GZR/EBR
C-EDGE TEN=420
12 and 16 weeks
GT 1,4,6; TE (RBV/IFN) + cirrhosis +RBV
RCT, DB, MC
1:1:1:1
12 weeks GZR/EBR GZR/EBR + RBV16 weeks GZR/EBR GZR/EBR + RBV
C-SURFERN=237
12 weeks
GT 1; TN & TE +cirrhosis; Advanced kidney dz (CKD 4 or 5)
RCT, DB, PC, MC
1:1
GZR/EBR pharmacokineticGZR/EBR PBO (followed by OL GZR/EBR)
GT=genotype, RCT= randomized control trial, DB= double blind, PC=placebo controlled, GZR/EBR = grazoprevir/elbasvir,OL=open-label, TN=treatment naiive, TE=treatment experienced, PBO=Placebo
Grazoprevir/Elbasvir Efficacy
Grazoprevir/Elbasvir Results
C-EDGE TN
C-EDGECO-INFXN C-EDGE TE C-
SURFER
GZR/EBR GZR/EBR w/o RBV
w/ RBV
w/o RBV
w/ RBV
GZR/EBR + PK
n 316 218 105 104 105 106 122
Duration (weeks) 12 12 12 12 16 16 12
All pt SVR12 95% 95% 92% 94% 92% 97% 99%*
Cirrhotic 97% 100% 89% 89% 92% 100% 100%
Non-cirrhotic 94% 94% 94% 97% 93% 96% 99%
PK=Pharmacokinetic*Modified full analysis set (FAS) with 2 lost to follow-up
89
• 5th highly potent oral DAA combination regimen for HCV genotype 1
• Ledipasvir/sofosbuvir combo and sofosbuvir alone based regimens are market leaders
• Comparable efficacy and safety to ledipasvir/sofosbuvir, paritaprevir/ritonavir/ombitasvir + dasabuvir
• No other regimen to treat patients with CrCl< 30 mL/min
89
Grazoprevir/Elbasvir Summary
Sofosbuvir/Velpatasvir (Epclusa)

10/30/2016
16
Hepatitis C (HCV) Direct Acting Antiviral (DAA) Drugs
91
Generic Brand (Manufacturer)
Strengths & Formulations
FDA Approval
FDAIndication
Simeprevir Olysio (Janssen) 150mg 11/22/2013 GT 1, 4
Sofosbuvir Sovaldi (Gilead) 400mg 12/6/2013 GT 1, 2, 3, 4Ledipasvir/Sofosbuvir Harvoni (Gilead) 90mg/400mg 10/10/2014 GT 1, 4, 5, 6
Paritaprevir/ritonavir /Ombitasvir + Dasabuvir Viekira Pak (Abbvie) 75mg/50mg/
12.5mg & 250mg 12/19/2014 GT 1
Daclatasvir Daklinza (BMS) 30mg, 60mgoral tablets 7/24/2015 GT 1, 3
Paritaprevir/ ritonavir/Ombitasvir Technivie (Abbvie) 75mg/50mg/12.5mg
oral tablet 7/24/2015 GT 4
Grazoprevir/Elbasvir Zepatier (Merck) 100mg/50mg
oral tablet 01/28/2016 GT 1, 4
Velpatasvir/Sofosbuvir Epclusa (Gilead) 100mg/400mg 06/28/2016 GT 1, 2, 3, 4, 5 ,6Simeprevir, Sofosbuvir and Daclatasvir are NOT used as monotherapy.AASLD/IDSA HCV guideline have the most up to date treatment recommendations
Sofosbuvir/VelpatasvirParameter Drug InformationGeneric Sofosbuvir / velpatasvirBrand EpclusaManufacturer Gilead Sciences, Inc.FDA Approval Date June 28, 2016Approval Type 505 (b) NMA, priority review / breakthrough therapy designation
Type of drug
Hepatitis C virus; Direct Acting Antiviral (HCV DAA)• 2nd generation NS5A replication complex inhibitor
(velpatasvir)• Nucleotide analog inhibitor (sofosbuvir)
FDA Indications Treatment of HCV genotypes (GT) 1 - 6 in adults
DosingOne tablet daily for 12 weekAdd RBV for patients with decompensate cirrhosis (Child-Pugh B & C)
Availablepreparations 100mg velpatasvir / 400 mg sofosbuvir
Sofosbuvir/velpatasvir (Epclusa). Gilead Sciences, Inc., PI, Jun 2016.
Parameter Drug Information
Background
• Velpatasvir = 2nd generation NS5A replication complex inhibitor • Pangenomic and improved resistance profile
• Sofosbuvir = nucleotide analog inhibitor• Does not inhibit host DNA / RNA polymerases• Not recommended in advance kidney dz (CRCL <30 ml/min)
• Single daily tablet for 12 weeks• Add RBV to patients with decompensated cirrhosis
• SVR >90% in all HCV genotypes
Comments
• Pangenomic 12 week regardless of genotypes• GT 1 TE CC, no longer need RBV compared to Harvoni + RBV 12
weeks• GT2 patients, no longer need RBV • GT 3 TN TE NC CC, improves SVR vs SOF + DVC• GT1-4 DC, improved efficacy compared to previous SOF regimen
Efficacy: SVR rate >95% in diverse patient populations including decompensated cirrhosis / negative predictors of responseSafety: Well tolerated with low SAE & discontinuation rates
Sofosbuvir/Velpatasvir Sofosbuvir/VelpatasvirParameter Drug InformationPregnancy Category BPediatrics Safety and efficacy have not been establishedGeriatrics No dosage adjustment
Doseadjustments
• Not recommended for severe renal impairment (eGFR < 30mL/min) or with ESRD
• No dosage adjustment for any hepatic impairment
Drug-druginteractions
Inducers of P-gp and moderate inducers of P450 may reduce Epclusa therapeutic effect.
• PPI, H2 antagonist, anticonvulsants, select HIV anti-retrovirals & rifampin
Sofosbuvir/velpatasvir (Epclusa). Gilead Sciences, Inc., PI, Jun 2016.
Sofosbuvir/Velpatasvir Efficacy
Study Entry Criteria Study Design Interventions with SVR12 Primary Endpoint
ASTRAL 1N=740
12 weeks
GT 1,2 4,5,6; TN, TE + cirrhosis
RCT, DB, PC, MC5:1 (GT5 excluded)
SOF/VEL vs PBO (followed by OL SOF/VEL)
ASTRAL 2N=266
12 weeks
GT 2; TN, TE +cirrhosis
R, OL, MC1:1 SOF/VEL vs SOF + RBV
ASTRAL 3N=552
12 or 24 weeks
GT 3; TN/TE +cirrhosis
R, OL, MC1:1
12 weeks: SOF/VEL24 weeks: SOF + RBV
ASTRAL 4N=267
12 or 24 weeks
GT 1 – 6; TN & TE; Decompensated cirrhosis
R, OL, MC1:1:1
12 weeks: SOF/VEL SOF/VEL + RBV24 weeks: SOF/VEL
ASTRAL 5N=104
12 weeks
GT 1-6; TN & TE+ cirrhosis; HIV co-infections on ART
OL, SA, MC 12 weeks: SOF/VEL
GT=genotype, RCT= randomized control trial, DB= double blind, PC=placebo controlled, SOF/VEL=sofosbuvir/velpatasvir
ASTRAL 1- Feld JJ, et al. N Engl J Med 2015;373(27):2599-607. ASTRAL 2 & 3 – Foster GR et al. N Engl J Med 2015;373(27):2608-17.ASTRAL 4: Curry MP, et al. N Engl J Med 2015;373(27):2618-28
Sofosbuvir/VelpatasvirEfficacy
ASTRAL-4
SOF/VEL12 Weeks
(N=90)
SOF/VEL + RBV
12 Weeks(N=87)
SOF/VEL24 Weeks
(N=90)
SVR12 Rate (95% CI)
83.3%(74.0%, 90.4%)
94.3%(87.1%, 98.1%)
85.6% (76.6%, 92.1%)
ASTRAL-3
SOF/VEL12 Weeks(N=277)
SOF + RBV24 Weeks(N=275)
SVR12 Rate (95% CI)
95% (92%, 97%)
80%(75%, 85%)
ASTRAL-2
SOF/VEL12 Weeks(N=134)
SOF + RBV12 Weeks(N=132)
SVR12 Rate (95% CI)
99.3%(95.9%, 100%)
80%(88.4%, 97.3%)
ASTRAL-1
SOF/VEL12 Weeks(N=624)
PLACEBO(N=116)
SVR12 Rate (95% CI)
99.0%(97.9%, 99.6%) 0%
ASTRAL 1- Feld JJ, et al. N Engl J Med 2015;373(27):2599-607. ASTRAL 2 & 3 – Foster GR et al. N Engl J Med 2015;373(27):2608-17.ASTRAL 4: Curry MP, et al. N Engl J Med 2015;373(27):2618-28.

10/30/2016
17
97
Sofosbuvir/Velpatasvir Summary
• 1st pangenomic DAA available• Well tolerated• Incidence of AEs was similar in subjects with or
without cirrhosis• Most common AEs (>2%) in the trials were
headache, fatigue, and nausea• Low discontinuation and relapse rate• One death in the trials – after subject completed
12 weeks of treatment and died post-treatment day
Obiltoxaximab(Anthim)
Obiltoxaximab
Parameter Drug InformationGeneric ObiltoxaximabBrand AnthimManufacturer Elusys TherapeuticsApproval Date 18 Mar 2016Approval Type BLA 351(a)Type of drug • Monoclonal antibody that binds the PA of B. anthracis
FDA Indications
• Anthrax antitoxin for tx and prevention of inhalational anthrax caused by Bacillus anthracis in children and adults
Formulation • Injection: 600 mg/6 mL (100 mg/mL) in a single-dose vial
Dosing • Dilute the injection in 0.9% Sodium Chloride Injection, USP, before administering as an intravenous infusion
Obiltoxaximab (Anthim). Product labeling. Elusys Therapeutics. March 2016.10
Background Anthrax
Parameter
Background • Category A bioterrorism agent
Pathophysiology
• Bacterial infection caused by B. anthracis• Inhalation of B. anthracis spores causes inhalational
anthrax• Protective antigen (PA) is a component of edema toxin
and lethal toxin• Fatality rate of 45-89%
Presentation/ Management
• Toxins cause hemorrhage, edema, tissue necrosis and death
• Antibacterial drugs are the main treatment • Raxibacumab and Anthrax immune globulin are used
with antibacterial drugs• Must be taken for a prolonged period of time
Anthim (obiltoxaximab).FDA Summary Review. Mar 2016.
10
Obiltoxaximab
Parameter Drug Information
Adverse Reactions
• Headache, pruritus, upper respiratory tract infections, cough, vessel puncture site bruise, infusion site swelling, nasal congestion, infusion site pain, urticaria, and pain in extremity
Contraindications • None
Warning/ Precautions
• Hypersensitivity reactions, including anaphylaxis
obiltoxaximab (Anthim). Product labeling. Elusys Therapeutics. March 2016.102
Obiltoxaximab Efficacy
obiltoxaximab (Anthim). Product labeling. Elusys Therapeutics. March 2016.
StudyOverview Animal Characteristics
Animal Trials
4 studies compared obiltoxaximabvs PBO vs obiltoxaximab+ antibacterial drugs
• Cynomolgus macaque• NZA rabbit• Prophylaxis studies, animals treated prior to the
development of symptoms• Treatment studies, animals administered treatment after
exhibiting symptoms of anthrax• Survival assessed at 28 days post challenge
Primary efficacy measure• Proportion of survival at day 28

10/30/2016
18
103
Obiltoxaximab Results
obiltoxaximab (Anthim). Product labeling. Elusys Therapeutics. March 2016.
Proportion of Survival at Day 281
(#survived/n) p-value2 95% CI3
Placebo ANTHIM 16mg/kg IV
NZW RabbitsStudy 1 0 (0/9) 93% (13/14) 0.0010 (0.59, 1.00)Study 2 0 (0/13) 62% (8/13) 0.0013 (0.29, 0.86)
Cynomolgus Macaques
Study 3 6% (1/16) 47% (7/15) 0.0068 (0.09, 0.68)
Study 44 0 (0/17) 31% (5/16)35% (6/17)
0.00850.0055
(0.08, 0.59)(0.11, 0.62)
IV: intravenous, CI: Confidence Interval1Survival assessed 28 days after spore challenge1p-value is from 1-sided Boschloo Test (with Berger-Boos modification of gamma=0.001) compared to placebo3Exact 95% confidence interval of difference in survival rates4ANTHIM products manufactured at two different facilities were tested in two separate treatment arms
Obiltoxaximab
104
Parameter Drug Information
Pregnancy• No available human data• Only use if clearly needed
Pediatrics • Not established
Dose Adjustments
• Mild to moderate hepatic impairment reduce dose, avoid in severe
• Mild to moderate renal impairment no adjustment, no data severe
Drug-drugInteractions
• Ciprofloxacin, co-administration does not alter pharmacokinetics of ciprofloxacin or obiltoxaximab
cabozantinib(Cabometyx) PI. Exelixis, Apr 2016. .
Obiltoxaximab Summary
• No human studies• Current main treatments are antibacterial
drugs, raxibacumab and Anthrax immune globulin
• Obiltoxaximab proves effective with or without antibacterial drugs
• Provides another treatment option for a fatal infection
Cholera Vaccine, Live, Oral(Vaxchora)
Cholera: Current Treatment
• Mainstay of therapy is hydration
107
Recommendations for the Use of Antibiotics for the Treatment of Cholera. Centers for Disease Control and Prevention. Accessed 29 Aug 2016.
Cholera Vaccine, Live, Oral
108
Parameter Drug Information
Background
• Cholera is caused by toxin producing strains of V. cholerae serogroups O1 and O139
• It is characterized as an acute, painless watery diarrhea which can be voluminous and lead to severe dehydration if adequate rehydration and electrolyte replacement are not initiated promptly
Comments • Pregnancy registry that monitors pregnancy outcomes in pregnant women exposed to Vaxchora
Adverse Reactions
• Tiredness, headache, abdominal pain, nausea/vomiting, lack of appetite, diarrhea
Contraindications • Anaphylaxis to active ingredients of Vaxchora or to a previous dose of any cholera vaccine
Vaxchora (cholera vaccine, live, oral). Product labeling. PaxVax Bermuda Ltd. June 2016.

10/30/2016
19
Cholera Vaccine, Live, Oral
109
Parameter Drug InformationGeneric Cholera Vaccine, Live, OralBrand VaxchoraManufacturer Pax Vax Bermuda Ltd. FDA Approval Date June 10, 2016
FDA Indications Active immunization against disease caused by Vibrio cholerae serogroup O1
Dosing Administered orally a minimum of 10 days before potential exposure to cholera
Available preparations
Suspension for oral administration supplied as a single dose carton containing two packets. Reconstitute: 100 mL water
Vaxchora (cholera vaccine, live, oral). Product labeling. PaxVax Bermuda Ltd. June 2016.
Cholera Vaccine, Live, OralEfficacy
• ResultsStudy Design Treatment Arms Primary Endpoints
R, DB, PC (201), PG, FDDuration: 1 year; N= 197
Patient characteristics• Healthy males and
females, age 18 to 45 years
1:1
PXVX0200 vaccine
vsPBO
Primary• Attack rate: Proportion of
subjects in each treatment arm who experienced moderate or severe diarrhea (cumulative diarrheal purge ≥ 3.0 L) after challenge through 10 days and 3 months post-challenge.
Secondary• Post-challenge disease severity• Tolerability of vaccine prior to
challenge
PC= placebo controlled; PG= parallel grouped; DB= double blind; FD= fixed dose; R= randomized
Cholera Vaccine, Live, Oral (Vaxchora).FDA clinical review. Jun 2016.
Cholera Vaccine, Live, OralResults
Parameter
PXVX0200 10 Day
Challenge N=35, n (%)
PXVX0200 3 Month
Challenge N=35, n (%)
Combined Placebo
Challenges N=66, n (%)
Efficacy - Against Moderate to Severe Diarrhea Vaccine Efficacy (95% CI)
90.3(62.7,
100.00)
79.5(49.9,
100.00)-
Overall SeverityNo qualifying
diarrhea 30 (85.7) 18 (54.5) 5 (7.6)
Mild: < 3 L – L of diarrhea 3 (8.6) 11 (33.3) 22 (33.3)
Cholera Vaccine, Live, Oral (Vaxchora).FDA clinical review. Jun 2016.
Cholera Vaccine, Live, OralResults
Vaccine Efficacy Against Secondary Study Endpoint
Parameter
PXVX0200 10 Day Challenge
N=35n (%)
PXVX0200 3 Month Challenge
N=35 n (%)
Combined Placebo Challenges
N=66n (%)
Attack Rate of Mild or Worse
Diarrhea5 (14.3) 15 (45.5) 61 (92.4)
Vaccine Efficacy (95% CI) Against
Mild or Worse Diarrhea
84.5(67.0, 100.0)
50.8(33.6, 66.8)
Attack Rate of Severe Diarrhea 1 (2.9) 2 (6.1) 28 (42.4)
Vaccine Efficacy (95% CI) Against Severe Diarrhea
93.3(56.2, 100.0)
85.7(46.2, 100.0)
Cholera Vaccine, Live, Oral (Vaxchora).FDA clinical review. Jun 2016.
• Pharmacokinetics– Protein binding (>99%) primarily to serum albumin and alpha1-acid
glycoprotein– Metabolism: Hepatic, primarily by CYP3A4 and CYP2D6; major
metabolite, DM-3411 (inactive)• Contraindications: pre-existing hepatic disease or
impairment, autoimmune diseases, and hypersensitivity• Warnings & Precautions
– Autoimmune hepatitis, bilirubin elevation, skin reactions, lymphadenopathy, colitis, hypersensitivity, infections, depression, and suicide
• Adverse Reactions– Nasopharyngitis, upper respiratory infections, rash, influenza,
dermatitis, oropharyngeal pain, bronchitis, eczema, lymphadenopathy, tonsilitis, acne
Cholera Vaccine, Live, Oral
Vaxchora (cholera vaccine, live, oral). Product labeling. PaxVax Bermuda Ltd. June 2016.
Cholera Vaccine, Live, Oral• Drug Interactions
– Avoid concomitant administration with systemic antibiotics since these agents may be active against the vaccine strain and prevent a sufficient degree of multiplication to occur in order to induce a protective immune response
– Chloroquine, antimalarial– Immunosuppressive therapies, including irradiation, antimetabolites,
alkylating agents, cytotoxic drugs and corticosteroids• Pregnancy Concerns
– Not absorbed systemically following oral administration– Maternal use is not expected to result in fetal exposure to the drug
Vaxchora (cholera vaccine, live, oral). Product labeling. PaxVax Bermuda Ltd. June 2016.

10/30/2016
20
Cholera Vaccine, Live, Oral Summary
• Effectiveness demonstrated based on human challenge data
• Serious adverse events were uncommon• Ongoing studies required to evaluate
efficacy in children ≥ 2 years to < 18 years• First viable option for prevention of cholera
Ophthalmology
Lifitegrast(Xiidra)
117
LifitegrastParameter Drug InformationGeneric lifitegrastBrand XiidraManufacturer ShireFDA Approval July 11, 2016Approval Type New molecular entityType of drug LFA-1 antagonistFDA Indications
Treatment for the signs and symptoms of dry eye disease (DED)
Dosing 1 drop into each eye BID (~12 hours apart) Available preparations
Ophthalmic solution containing lifitegrast 5%(50mg/mL)
Xiidra (lifitegrast). Product labeling. Shire PLC. July 2016.LFA: Lymphocyte Function Associated Antigen-1
Lifitegrast
Parameter Drug Information
Comments
• Discard single use container immediately after use
• Remove contacts before using and do not reinsert for 15 minutes
Adverse Reactions
• Instillation site irritation, dysgeusia and reduced visual acuity
Contra-indications
• None
BBW/Significant ADRs
• None
Xiidra (lifitegrast). Product labeling. Shire PLC. July 2016.
Lifitegrast Efficacy
120
Study Design Treatment Efficacy MeasuresFour studies, R, DB, MC, PA,PC, Duration: 84 days, n = 1181
Patient characteristics• >18 years of age (mean 59 yo)• Baseline CFS (mean 2.1) and
STT (mean 4.8) • Baseline EDS (mean 58) and
ODS (mean 1.9)
R (1:1)
Lifitegrast
vs
PBO
PrimaryAvg Δ from baseline and tx difference in EDS (symptoms)
EDS scale0 = no discomfort100= maximal discomfort
DB=double-blind; MC=multi-center; PA=parallel arm; PC=placebo-controlled; R=randomized; CFS= corneal fluorescein staining; STT= Schirmer tear test; EDS= eye dryness score, ODS= ocular discomfort score
Ophthalmology 2014;121:475-483. Ophthalmology 2015;122:2423-2431.
Xiidra (lifitegrast).FDA Summary review. July 2016.

10/30/2016
21
Lifitegrast Results
Xiidra (lifitegrast).FDA Summary review. July 2016.
Phase 2
Visit Placebo(N=58)
LIF 5.0%(N=58)
Difference(95% CI)
Baseline 51.8 51.5
Day 14 -3.9 -8.9 -5.1 (-13.1, 3.0)
Day 42 -7.9 -17.3 -9.4(-17.0, -1.9)
Day 84 -7.2 -14.4 -7.3 (-16.1, 1.4)
Phase 3: OPUS-2
Visit Placebo(N=360)
LIF 5.0%(N=358)
Difference(95% CI)
Baseline 69.2 69.7
Day 14 -13.1 -19.7 -6.4 (-10.0, -2.8)
Day 42 -18.2 -28.3 -10.0(-13.8, -6.1)
Day 84 -22.8 -35.3 -12.3 (-16.4, -8.3)
Phase 3: OPUS-1
Visit Placebo(N=295)
LIF 5.0%(N=293)
Difference(95% CI)
Baseline 41.6 40.2
Day 14 -7.5 -6.7 0.1 (-3.9, 4.1)
Day 42 -9.1 -12.6 -4.2(-8.5, 0.0)
Day 84 -11.2 -15.2 -4.7 (-8.9, -0.4)
Phase 3: OPUS-3
Visit Placebo(N=356)
LIF 5.0%(N=355)
Difference(95% CI)
Baseline 69.0 68.3
Day 14 -14.9 -22.7 -8.0 (-11.4, -4.5)
Day 42 -23.7 -33.0 -9.6(-13.4, -5.8)
Day 84 -30.5 -37.7 -7.5 (-11.6, -3.5)
Lifitegrast vs Cyclosporine
Parameter Cyclosporine (Restasis)
Lifitegrast(Xiidra)
Frequency of administration Twice daily Twice daily
Dosage forms Ophthalmic emulsion Ophthalmic emulsionStrengths 0.05% 5%
Package Sizes 30 vials, each 0.4 ml60 vials, each 0.4 ml 60 vials, each 0.4 ml
CommentsCan be used
concomitantly with artificial tears
Single use containersRemove contacts before
instillation
Lifitegrast Summary
• Novel mechanism of action• Only agent approved to treat the signs and
symptoms of dry eye disease• Adverse events were minor and limited in
duration• Closest comparator is cyclosporine 0.05%
topical emulsion• Possible faster onset of action than
cyclosporine 0.05%
Pulmonology
Glycopyrrolate/Formoterol fumarate(Bevespi Aerosphere)
125
Glycopyrrolate/Formoterol
126
Parameter Drug InformationGeneric Glycopyrrolate and formoterol fumarateBrand Bevespi AerosphereManufacturer AstraZeneca (Pearl Therapeutics Inc.)FDA Approval April 25, 2016Approval Type NDA – 505(b)(2)Type of drug Inhaled LABA-LAMA combination
FDA Indications Long-term, maintenance treatment of airflow obstruction in COPD
Dosing 2 inhalations BID
Available preparations
• Pressurized metered dose inhaler of 9 mcg glycopyrrolate/4.8 mcg formoterol as inhalation aerosol
• 120 inhalations/canister
Bevespi Aerosphere (glycopyrrolate/formoterol fumarate). Product labeling. AstraZeneca. April 2016.

10/30/2016
22
Glycopyrrolate/Formoterol
127
Parameter Drug Information
Background• First LAMA-LABA combination bronchodilator
therapy for COPD formulated in a pressurized metered-dose inhaler (pMDI)
Comments • Not indicated for use in asthmaAdverse Reactions • UTI and cough
Contraindications • Use in asthma without long-term asthma controller medication
Black Box WarningOr Significant Adverse Effects
• BBW: LABAs can increase risk of asthma-related death
• Paradoxical bronchospasm• Hypokalemia or hyperglycemia• Worsening of narrow-angle glaucoma or urinary
retentionBevespi Aerosphere (glycopyrrolate/formoterol fumarate). Product labeling. AstraZeneca. April 2016.
Parameter Drug Information
ClinicalDevelopment
Program
8 dose-ranging trials (n= 822)Glycopyrrolate: 6 doses, 14-day R, DB, PC, incomplete-block crossover trialFormoterol: 3 doses, single-dose, R, DB, PC, crossover trial2, R, DB, PC, PG lung function trials, 24-weeksBaseline characteristics• 40-80 years old• ≥ 10 pack year smoking history• Post-albuterol FEV1 < 80% predicted, and
FEV1/FVC < 0.7
128
Glycopyrrolate/Formoterol Efficacy
Bevespi Aerosphere (glycopyrrolate/formoterol fumarate). Product labeling. AstraZeneca. April 2016.
129
Glycopyrrolate/Formoterol Results
Bevespi Aerosphere (glycopyrrolate/formoterol fumarate). Product labeling. AstraZeneca. April 2016.
Treatment N
Trough FEV1 (mL) at Week 24Difference from
Placebo LS Mean(95% CI)
Glycopyrrolate 18 mcg BID
(95% CI)
Formoterol Fumarate 9.6 mcg BID LS Mean (95%
CI)Trial 1
Bevespi Aerosphere 429
N=161150 mL
(114, 186)
N=34459 mL
(31, 88)
N=36764 mL
(36, 92)Trial 2
Bevespi Aerosphere 433
N=170103 mL
(67, 140)
N=36754 mL
(25, 83)
N=35056 mL
(27, 85)
Glycopyrrolate/Formoterol Summary
• 4th LAMA/LABA combination• 1st pMDI, others are breath
actuated or Respimat• COPD maintenance therapy• BID drug vs 2 other once daily
drugs• Offers no compelling advantages
130
Nuclear
131
Fluciclovine F 18 (Axumin)
132

10/30/2016
23
Fluciclovine F 18
133
Parameter Drug InformationGeneric Fluciclovine F 18Brand AxuminManufacturer Blue Earth Diagnostics Ltd.FDA Approval May 27, 2016
Approval Type NDA
FDA Indications
Positron emission tomography (PET) imaging in men with suspected prostate cancer recurrence based on elevated blood prostate specific antigen (PSA) levels following prior treatment
Dosing 370 MBq (10 mCi) administered as an intravenous bolus injection
Available preparations
30 mL multiple-dose glass vial containing approximately 26 mL solution
Fluciclovine F 18 (Axumin). Product labeling. Blue Earth Diagnostics Ltd. May 2016.
Fluciclovine F 18
134
Parameter Drug Information
Background• Amino acid transported across cell membranes by
amino acid transporters which are upregulated in prostate cancer cells
Comments • Not for female useAdverse Reactions • Injection site pain, erythema, and dysgeusia
Contraindications • None
Special Instructions
• Patients should avoid significant exercise for at least a day before the PET scan
• Patients should not eat or drink for at least 4 hours before the PET scan
Fluciclovine F 18 (Axumin). Product labeling. Blue Earth Diagnostics Ltd. May 2016.
Fluciclovine F 18 Efficacy/Results
135
Study Study Design Treatment Efficacy Measures Results
Study 1
Patient characteristics• Men with suspected
recurrence of prostate cancer
• N = 99, open label, prospective, single center study
• Fluciclovine F18• 111 Capromab
pendetide
Positive predictive value (PPV)
PPVPSA ≤ 1.7811/15 (73.3%)
PSA >1.78 - ≤ 4.4817/22 (77.3%)
PSA >4.48 - ≤ 9.2521/25 (84%)
PSA > 9.2520/24 (83.3%)
Study 2
Patient characteristics• Men with median
PSA value of 1.44 ng/mL
• N = 50, open label, prospective, single center study
• Fluciclovine F18• C11 choline
Concordance between Axumin and C11 choline scans
Next Slide
J Urol 191: 1446-1453, 2014Clin Nucl Med, 40 (8): 386-391, 2015
Axumin (Fluciclovine F18).FDA Summary review. May 2016.
Fluciclovine F 18 Results
136Clin Nucl Med, 40 (8): 386-391, 2015Axumin (Fluciclovine F18).FDA Summary review. May 2016.
11C-Choline (-) 11C-Choline (+)
18F-Fluciclovine (-) 33 0
18 F-Fluciclovine (+) 6 11
Fluciclovine F 18Summary
• Primary and recurrent prostatic carcinoma is a major public health issue in the US
• In men with recurrent prostate cancer Fluciclovine F18 is useful for the detection of metastases as verified by histopathology and patient follow up
• The standard imaging modalities have limitations
• New diagnostic options are needed
137
Miscellaneous Drugs
138

10/30/2016
24
Morphine Extended-Release
139Morphine Extended-Release (Morphabond ER). Product labeling. IDT, LLC. October 2015.
Parameter Drug InformationGeneric Morphine Extended-ReleaseBrand MorphabondManufacturer Inspirion Delivery Technologies , LLCApproval Date October 2, 2015
FDA Indications
Management of severe pain that requires long-term treatment and for which other options are inadequate
Dosing Administered orally every 12 hoursAvailable preparations 15, 30, 60, 100 mg tablets
Oxycodone Extended-Release
140
Parameter Drug InformationGeneric Oxycodone Extended-ReleaseBrand Xtampza ERManufacturer Collegium Pharmaceutical, Inc.Approval Date April 26, 2016
FDA Indications
Management of severe pain that requires long-term treatment and for which other options are inadequate
Dosing Administered orally every 12 hours with foodAvailable preparations 9, 13.5, 18, 27, 36 mg capsules
Oxycodone Extended-Release (Xtampza). Product labeling. Collegium Pharmaceutical, Inc. May 2016.
Nebivolol/Valsartan
141
Parameter Drug InformationGeneric Nebivolol/valsartanBrand ByvalsonManufacturer Allergan, IncApproval Date June 3, 2016FDA Indications
Treatment of hypertension, to lower blood pressure
Dosing Administered orally once dailyAvailable preparations 5 mg/80 mg tablets
Nebivolol and valsartan (Byvalson). Product labeling. Allergan, Inc. June 2016.
Calcifediol
142
Parameter Drug InformationGeneric CalcifediolBrand RayaldeeManufacturer Opko Ireland GlobalFDA Approval Date June 17, 2016
Approval Type New Formulation, Standard Review Drug
FDA Indications
Treatment of secondary hyperparathyroidism in adults with stage 3 or 4 chronic kidney disease and serum total 25-hydroxyvitamin D levels less than 30 ng/mL
Dosing Administered orally once daily at bedtimeAvailable preparations 30 mcg extended-release capsules
Calcifediol (Rayaldee). Product labeling. OPKO Pharmaceuticals, LLC. March 2016.
Key Points
• For further details regarding formulary decisions, see individual agency websites– www.health.mil/formulary– http://www.ihs.gov/nptc/index.cfm?module=dsp_nptc_resources– http://www.pbm.va.gov/– http://www.bop.gov/resources/pdfs/formulary.pdf– https://online.epocrates.com/ TRICARE formulary
• For more information on specific drugs, see the Drugs at FDA website and individual manufacturer websites– http://www.accessdata.fda.gov/scripts/cder/drugsatfda/
Self-Assessment Question 1
1. What is the mechanism of action of ixekizumab?
a) IL-2 inhibitorb) BCL-2 inhibitorc) IL-17a receptor antagonistd) Tyrosine kinase inhibitor

10/30/2016
25
Self-Assessment Question 2
2. Tumor lysis syndrome is a concern with which drug?
a) lifitegrastb) pimavanserinc) cabozantanibd) venetoclax
Self-Assessment Question 3
3. Which drug : indication pairing is correct?
a) Elbasvir/grazoprevir: cholerab) Glycopyrrolate and formoterol fumarate:
COPDc) Lifitegrast: erectile dysfunctiond) Fluciclovine F18: breast cancer
New Drugs of 2016Amy M. Lugo, PharmD, BCPS, BC-ADM, FAPhA
Clinical Pharmacy Specialist Director, Managed Care Residency
Defense Health AgencyPharmacy Operations DivisionFormulary Management Branch
San Antonio, Texas
LCDR Kendra N. Jenkins, USPHSPharmD, BCPS
Program Management OfficerImmigration and Customs Enforcement (ICE)
Enforcement and Removal OperationsICE Health Service Corps
Washington, DC