
Neurotransmission and drug action in the central nervous system Neuroleptics Anton Kohút.
37
Neurotransmission and drug action in the central nervous system Neuroleptics Anton Kohút
-
Upload
peregrine-cox -
Category
Documents
-
view
223 -
download
3
Transcript of Neurotransmission and drug action in the central nervous system Neuroleptics Anton Kohút.

Neurotransmission and drug action in the central nervous system
Neuroleptics Anton Kohút

18451845 FREUD FREUD cocaine cocaine from 1933from 1933 iinsulin and electric shocks nsulin and electric shocks 19431943 Hoffmann Hoffmann LSDLSD19491949 lithium treatment of lithium treatment of psychosispsychosis19521952 chlorpromazinechlorpromazine19541954 meprobamatmeprobamat19571957 benzodiazepinebenzodiazepine - - chlordiazepoxidechlordiazepoxide19581958 iproniazid iproniazid (inhibítor MAO)(inhibítor MAO) imipraminimipramin (tricyclic antidepressive (tricyclic antidepressive
drug)drug)

Actions of drugs in CNS
Nonspecific Anesthetic gases and
vapors, The aliphatic alcohols, Some hypnotic-
sedative drugs.
Specific Act on specific
receptors in CNS

Neurotransmiters in CNS
Inhibitory:GABA
Excitatory:NMDA (glutamate)
Fast (ligand gated ion channels) – NMDA, GABA
Slow (G-protein coupled receptors

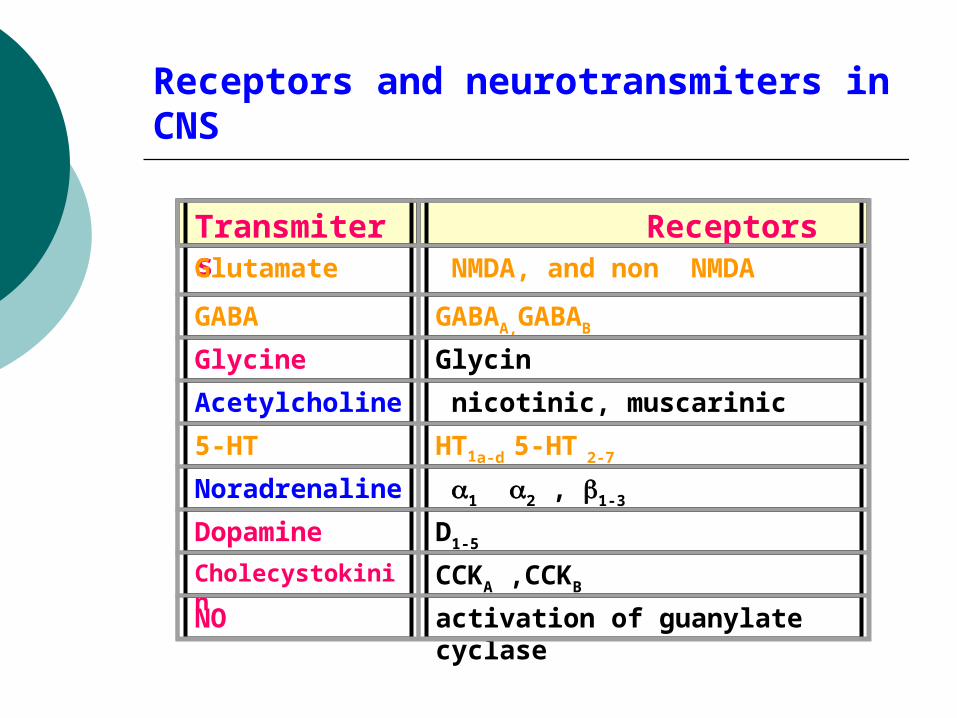
Receptors and neurotransmiters in CNS
Transmiters
ReceptorsGlutamate NMDA, and non NMDA
GABA GABAA,GABAB
Glycine Glycin
Acetylcholine nicotinic, muscarinic
5-HT HT1a-d 5-HT 2-7
Noradrenaline
1 2 , 1-3
Dopamine D1-5
Cholecystokinin
CCKA ,CCKB
NO activation of guanylate cyclase
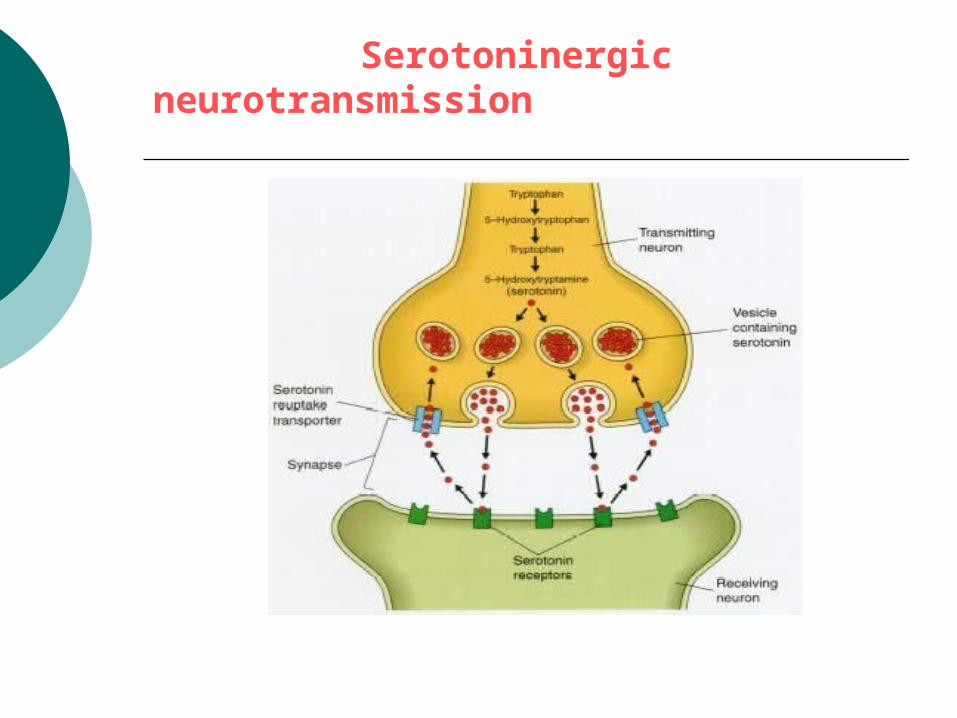
Serotoninergic neurotransmission

5HT-R Action Agonist Antagonist
1A, B neuronal inhibition, behavioural effects: sleep, feeding, anxiety, thermoregul.
Buspirone, Sertindole
Ergotamine Metiotepine
1D vasoconstriction Sumatriptan Ergotamine Metiotepine
2A neuronal excitation(increase in the number in suicides)
LSD KetanserineCyproheptadineNefazodone
3 neuronal excitation, vomiting, anxiety
-Metyl-5-HT
OndanzetroneGranizetroneTropizetrone
7 not known LSD KetanserineCyproheptadine
5-HT-R classification and function in CNS

Biogenic monoamine hypothesis

Dopamine and Parkinsonism

Subunits of GABA receptor

GABA receptor – inhibitory

Excitotoxicity has been implicated as a pathophysiologic mechanism in many diseases, including neurodegenerative syndromes, stroke and trauma, hyperalgesia, and epilepsy.
Although the clinical applications of interrupting excitoxicity remain limited, it is hoped that better understanding of glutamate-induced excitotoxicity will lead to the development of new approaches to treatment of these diseases.




Classification of drugs influencing CNS
1. Neuroleptic drugs (D receptors) antipsychotic drugs, antischizophrenic drugs Increase of dopaminergic activity in the brain
is the cause of schizoprenia,
2. Antidepressive drugs – antidepressans (NA, 5-HT)
Depression and bipolar disorders are pervasive mood altering ilnesses affecting energy, sleep, appetite, libido and the ability to function.
Depression is due to a decrease of noradrenaline and serotonine,
Mania is due to oposite changes,

3. Anxiolytic and sedative - hypnotic drugs (GABA)
Unpleasant state of tension, apprehension, or uneasiness. Disorders involving anxiety are the most common mental disturbances.
The role of GABA receptors, Agonists of GABA receptors –
benzodiazepines a effecive in the treatment of anxiety.
4. Psychomimetics -psychomotor stimulants (NA, D)
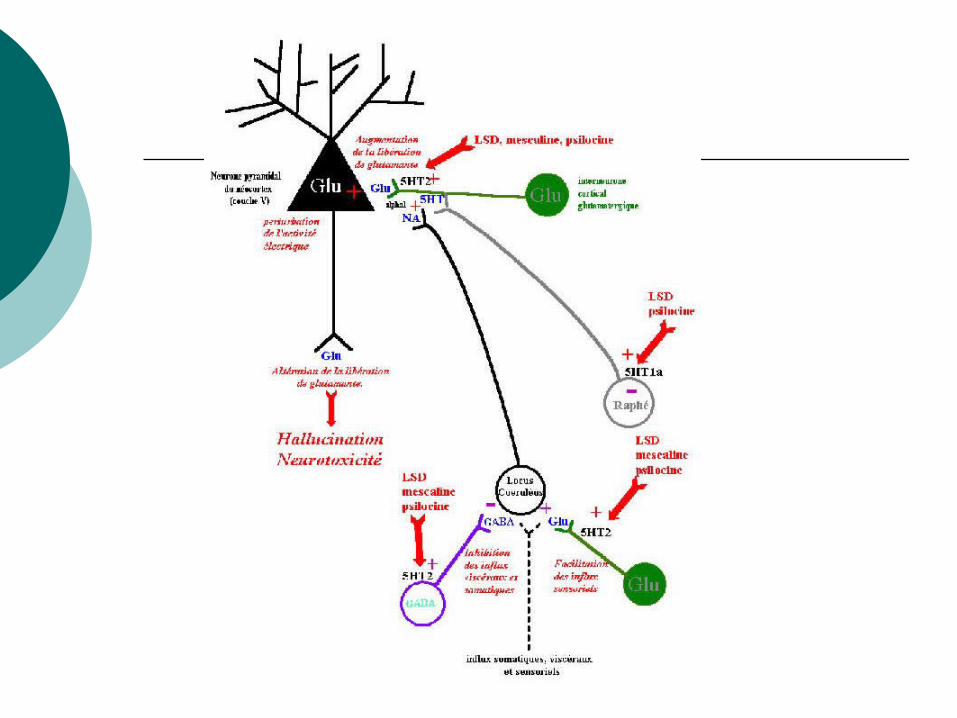
5. Psychotomimetic drugs – halucinogenes (5-HT)
6. Antiepileptics, antiparkinsonics -used to treat Parkinsonism and epilepsy (GABA, NMDA)

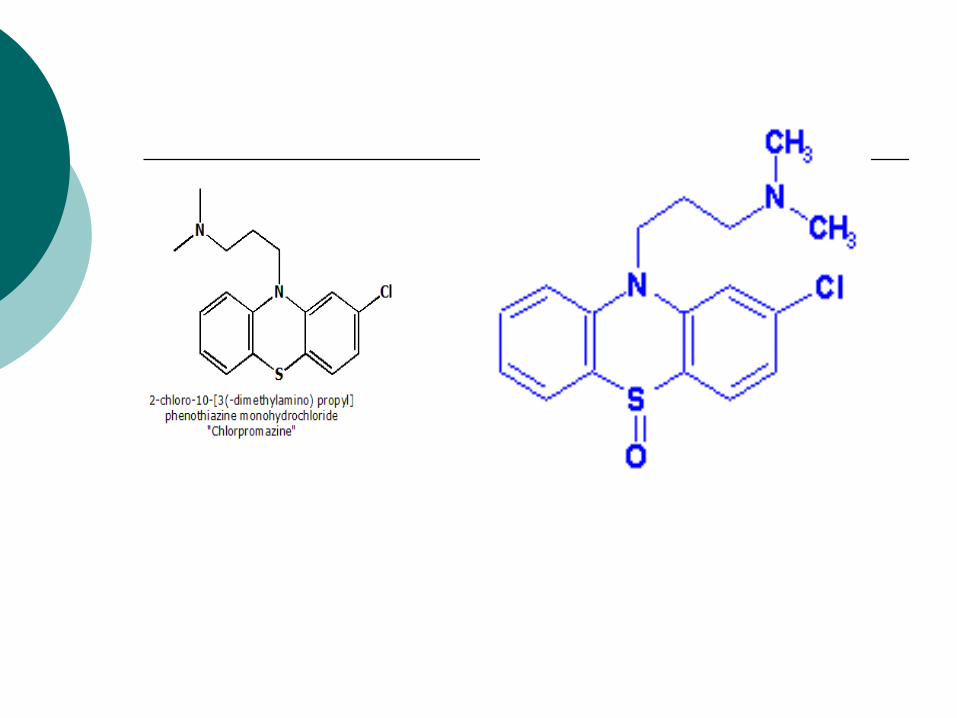
Neuroleptics (antipsychotics) Chlorpromazine

The spliting of the mind




Antipsychotic drugs - neuroleptics
- are the best treatment now available. They do not cure schizophrenia but they have greatly improved the outlook for individual patients.
reduce the psychotic symptoms of schizophrenia, such as hallucinations and delusions, and usually allow the patient to function more effectively and appropriately.
patients vary a great deal in the amount of drug needed to reduce symptoms without producing troublesome side effects.

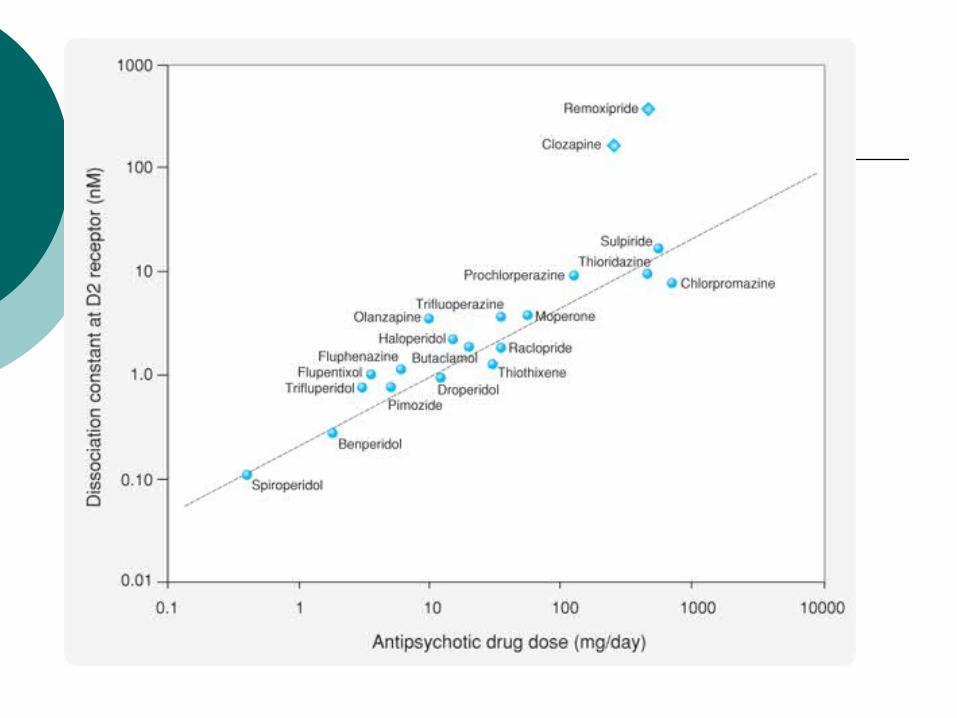
Dopaminergic bases of schisophrenia and mechanism of action of neuroleptics
Schizophrenia in man is associated with dopaminergic hyperactivity (D2).
- number of D2 receptors increase twoo-fold in schizophrenic patients
- amphetamine, which release dopamine in brain, can produce in man syndrome similar as the symptoms of schizophrenia
- all the neuroleptic drugs block dopamine receptor (brain, periphery)
- there are at least twoo types of receptor: D1 and D2
- clinical efficacy correlates closely with relative ability to block D2 receptors

Classification of neuroleptics
I. Typical neuroleptics Phenothiazines 1. with aliphatic ring: chlorpromazine, levopromazine2. with piperidine ring: thioridazine3. with piperazine ring: prochlorperazine, perhenazine (5-
10 x more active as CHPR, antiemetic action), trifluoperazine, flufenazín Thioxantines: chlorprothixen,flupentixol, Butyrophenones: haloperidol, droperidol,
II. atypical neuroleptics Dibenzodiazepines- : clozapine, olanzepine, quetapine,
ziprasidone, and risperidone - block D1, 4 a 5-HT2 ??? –

Site of chlorpromazine action

Actions of chlorpromazineantipsychotic actions:- reduction of hallucinations, - reduction of spontaneous physical
movement- they do not depress intelectual function of the patient- antipsychotic effect usually take several veeks to occur
extrapyramidal effects: parkinsonian symptoms, diskynesiaantiemetic effects: block of D2 receptors of the chemoreceptor
triger zone of the medulla
antimuscarinic effects:- atropine like effect
blockade of alfa-adrenoreceptor: orthostatic hypotension
hypothermia: neuroleptics alter temperature-regulating mechanisms (poikilothermia)
endocrine effect: - increase in prolactin release
Atypical neuroleptics
have a relatively low affinity for D2 receptor
are more effective than typical antipsychotics at treating the “negative” symptoms of schizophrenia,
some atypical antipsychotics also act as antagonists at 5-HT2 and D4 receptors

Therapeutic uses and side effects
Therapeutic uses treatment of
schizophrenia: prevention of severe
nausea and vomiting other: - neuroleptanalgesia
(droperidol)
- chronic pain (+ opioids)
Side effects parkinsonian effects: CNS depresion: drowsiness occurrs during
the firs twoo weeks of therapy
antimuscarinic effects endocrinne
depression of the hypothalamus > galactorhea, infertility, impotence




















