
Neuroticism & FMS
13
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/51688339 The Relationship Between the Fear-Avoidance Model of Pain and Personality Traits in Fibromyalgia Patients Article in Journal of Clinical Psychology in Medical Settings · October 2011 DOI: 10.1007/s10880-011-9263-2 · Source: PubMed CITATIONS 25 READS 199 5 authors, including: Ana Isabel Sánchez University of Granada 38 PUBLICATIONS 492 CITATIONS SEE PROFILE Elena Miró University of Granada 57 PUBLICATIONS 708 CITATIONS SEE PROFILE Ana Medina National University of Colombia 3 PUBLICATIONS 82 CITATIONS SEE PROFILE María José Lami University of Granada 9 PUBLICATIONS 46 CITATIONS SEE PROFILE All in-text references underlined in blue are linked to publications on ResearchGate, letting you access and read them immediately. Available from: María José Lami Retrieved on: 13 November 2016
-
Upload
paul-coelho-md -
Category
Healthcare
-
view
48 -
download
0
Transcript of Neuroticism & FMS

Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/51688339
TheRelationshipBetweentheFear-AvoidanceModelofPainandPersonalityTraitsinFibromyalgiaPatients
ArticleinJournalofClinicalPsychologyinMedicalSettings·October2011
DOI:10.1007/s10880-011-9263-2·Source:PubMed
CITATIONS
25
READS
199
5authors,including:
AnaIsabelSánchez
UniversityofGranada
38PUBLICATIONS492CITATIONS
SEEPROFILE
ElenaMiró
UniversityofGranada
57PUBLICATIONS708CITATIONS
SEEPROFILE
AnaMedina
NationalUniversityofColombia
3PUBLICATIONS82CITATIONS
SEEPROFILE
MaríaJoséLami
UniversityofGranada
9PUBLICATIONS46CITATIONS
SEEPROFILE
Allin-textreferencesunderlinedinbluearelinkedtopublicationsonResearchGate,
lettingyouaccessandreadthemimmediately.
Availablefrom:MaríaJoséLami
Retrievedon:13November2016
The Relationship Between the Fear-Avoidance Model of Painand Personality Traits in Fibromyalgia Patients
Marıa Pilar Martınez • Ana Isabel Sanchez •
Elena Miro • Ana Medina • Marıa Jose Lami
� Springer Science+Business Media, LLC 2011
Abstract This study examined the relationship between
several cognitive-affective factors of the fear-avoidance
model of pain, the big five model of personality, and
functional impairment in fibromyalgia (FM). Seventy-four
FM patients completed the NEO Five-Factor Inventory, the
Pain Catastrophizing Scale, the Pain Anxiety Symptoms
Scale-20, the Pain Vigilance and Awareness Question-
naire, and the Impairment and Functioning Inventory.
Results indicated that the cognitive-affective factors of
pain are differentially associated with personality traits.
Neuroticism and conscientiousness were significant pre-
dictors of pain catastrophizing, and neuroticism, openness,
and agreeableness were significant predictors of pain anx-
iety. Personality traits did not contribute significantly to
vigilance to pain. The effect of neuroticism upon pain
anxiety was mediated by pain catastrophizing, and neu-
roticism showed a trend to moderate the relationship
between impairment and pain anxiety. Results support the
fear-avoidance model of pain. Implications of the findings
for the understanding and management of FM are
discussed.
Keywords Fibromyalgia � Pain catastrophizing �Pain anxiety � Vigilance to pain � Neuroticism
Introduction
Fibromyalgia (FM) is a chronic pain syndrome of uncertain
origin that leads to a significant deterioration of patient’s
quality of life. According to the American College of
Rheumatology (ACR; Wolfe et al., 1990), this disease is
characterized by the presence of widespread musculoskel-
etal pain for at least three months in all four quadrants of
the body, as well as pain in digital palpation in at least 11
of the 18 sensitive points of the body. Although FM may
have a very heterogeneous nature, the most important
diagnostic variables are widespread pain, cognitive symp-
toms, unrefreshed sleep, fatigue, and a number of somatic
symptoms (Wolfe et al., 2010). Considerable links between
these variables have been reported (e.g. Miro et al., 2011).
According to epidemiological studies, the prevalence of
FM ranges from 10.2 to 15.7% in visits to rheumatologists
(Neumann & Buskila, 2003), and FM is the third most
common rheumatic disorder after low back pain and
osteoarthritis (Lawrence et al., 2008). Aside from personal
discomfort, FM causes a notable economic burden for the
healthcare system. The annual medical costs for FM
patients ($4065) are significantly higher than those for
control patients not diagnosed with FM ($2766) (Lachaine,
Beauchemin, & Landry, 2010).
Although the etiology of FM is not clearly established,
accumulating evidence suggests that patients with FM have
a dysregulation of the hypothalamic–pituitary–adrenal
(HPA) axis that occurs in response to a chronic stressor and
is associated to impaired immunity (Ross et al., 2010).
Bazzichi et al. (2007) found higher levels of cytokines in
FM patients than in controls, which suggests the presence
of an inflammatory response system (for reviews, see
Bazzichi et al., 2007; Nishikai et al., 2001; Pamuk & Cakir,
2007). In fact, some FM symptoms are reminiscent of
M. P. Martınez (&) � A. I. Sanchez � E. Miro � A. Medina �M. J. Lami
Departamento de Personalidad, Evaluacion y Tratamiento
Psicologico, Universidad de Granada, Facultad de Psicologıa,
Campus Universitario de Cartuja, 18071 Granada, Spain
e-mail: [email protected]
123
J Clin Psychol Med Settings
DOI 10.1007/s10880-011-9263-2
‘‘sickness behavior,’’ a syndrome of pain, fatigue, depres-
sion, and impaired cognition caused by the production of
pro-inflammatory cytokines (Ross et al., 2010).
In addition, there is growing acceptance of the role that
psychological factors play in exacerbation of the symptoms
as well as dysfunctional adjustment. These psychological
factors mainly include coping and appraisal styles and
personality traits. Cognitive appraisal is a dual process. In
primary appraisal, individuals assess the significance of a
particular encounter with the environment for their well-
being; in secondary appraisal, individuals assess whether
they can take action to improve their relationship with the
environment, and which coping strategies (cognitive and
behavioral efforts aimed to manage the demand of the
environment) may be useful for this (Lazarus & Folkman,
1984). Personality traits are distinguishing qualities or
characteristics of individuals, that is, a readiness to think or
act in a similar fashion in response to a variety of different
stimuli or situations (Carver & Scheier, 2000).
Several cognitive-affective factors have contributed to
further understanding of FM. A few examples are helpless-
ness (Nicassio, Schuman, Radojevic, & Weisman, 1999),
hypervigilance to pain (Crombez, Eccleston, Van den
Broeck, Goubert, & Van Houdenhove, 2004), fear of pain
(Turk, Robinson, & Burwinkle, 2004), pain catastrophizing
(Hassett, Cone, Patella, & Sigal, 2000), self-efficacy expec-
tancies (Buckelew, Murray, Hewett, Johnson, & Huyser,
1995), and coping strategies (Garcıa-Campayo, Pascual,
Alda, & Gonzalez-Ramırez, 2007). Strong links between
some of these cognitive-affective factors have been reported
in FM patients (Sanchez, Martınez, Miro, & Medina, 2011).
Moreover, a number of reports have indicated that FM is
related to personality traits such as neuroticism (Malt,
Olafsson, Lund, & Ursin, 2002), alexithymia (Brosschot &
Aarsse, 2001), hypochondriasis and hysteria (Trygg,
Lundberg, Rosenlund, Timpka, & Bjorn, 2002), perfection-
ism (Mcallister, 2000), and harm avoidance (Anderberg,
Forsgren, Ekselius, Marteinsdottir, & Hallman, 1999).
Additionally, recent studies suggest that the clinical person-
ality profile of FM patients is mainly oriented to expressing a
great variety of somatic complaints, health problems, and
physical malfunctioning (Perez-Pareja, Sese, Gonzalez-Ordi,
& Palmer 2010). Despite previous reports, the role of per-
sonality in the abovementioned cognitive and emotional
dimensions of pain has not been sufficiently explored. It
should be noted that the status of some of the psychological
characteristics mentioned has not definitively established.
For example, there is controversy about whether pain catas-
trophizing should be considered as a personality trait or as a
situation-specific response (for a review, see Quartana,
Campbell, & Edwards, 2009; Turner & Aaron, 2001).
The ‘‘fear-avoidance’’ model (Leeuw et al., 2007;
Vlaeyen & Linton, 2000) is an influential theoretical
approach that addresses chronic pain. It considers the
contribution of personality in the cognitive-affective fac-
tors of pain. The model suggests that negative appraisal of
pain and its consequences (pain catastrophizing) is a
potential precursor to pain-related fear and this fear leads
patients to focus their attention on possible somatic signals
of threat (hypervigilance) and to show avoidance/escape
behaviors. All these factors aggravate the pain problem,
leading to disability, gradual deterioration of the muscular
system, and depression. The latter maintain the pain
experience, thereby contributing to a spiral of increasing
fear and avoidance. According to the model, pain catas-
trophizing is influenced by negative affectivity (neuroti-
cism) and threatening illness information. While this model
has scientific support in chronic musculoskeletal pain prob-
lems (e.g. Cook, Brawer, & Vowles, 2006), its explanatory
value in FM patients is unknown.
Various studies have examined the relationship between
personality traits and pain cognitive-affective factors in
non-clinical samples as well as samples with no FM pain.
In an experimental study of pain among college students,
Thorn et al (2004) found that the tendency to describe
oneself as emotionally vulnerable mediated sex differences
in pain catastrophizing. Muris et al. (2007) observed that
pain catastrophizing in young adolescents was explained
by the behavioral inhibition system, reactive temperament
traits (fear), and perceptual sensitivity. In a study of two
experimental pain models with healthy individuals, Lee
(2009) found that neuroticism was positively correlated
with somatosensory amplification, fear of pain, and pain
catastrophizing; the study found that these cognitive-
affective factors were generally more strongly related to
qualitative and quantitative pain measures than personality
indices. In a clinical sample composed of patients with low
back pain, Goubert, Crombez, and Van Damme (2004)
found that neuroticism moderated the relationship between
pain severity and catastrophic thinking about pain; they
also observed that pain catastrophizing and pain-related
fear mediated the relationship between neuroticism and
vigilance to pain. However, other studies have not identi-
fied a link between personality and appraisal of pain. For
example, in patients with chronic pain, Herrero, Ramırez-
Maestre, and Gonzalez (2008) found that personality
profiles (schizoid-compulsive-dependent, antisocial-com-
pulsive, and compulsive) did not differ in the type of
cognitive appraisal of pain (harm, threat, and challenge
appraisal). The discrepancy observed in these studies
points to the need to collect new evidence on the rela-
tionship between chronic pain and personality.
To the best of our knowledge, current study is the first to
explore the links between personality traits and cognitive-
affective factors of pain in FM patients, according to the
fear-avoidance model. Although neuroticism appears to be
J Clin Psychol Med Settings
123

an important factor in the heightened experience of pain,
other personality traits may also play a prominent role. It is
important to take the big five personality model into
account, as it greatly contributes to the understanding of
individual’s physical and emotional well-being. It has been
found that neuroticism and conscientiousness are relevant
to understanding depressive moods (Vearing & Mak,
2007), neuroticism and extraversion have predicted the
severity of bodily anxiety symptoms (Kristensen, Mortensen,
& Mors, 2009), and neuroticism and introversion are linked
to greater pain-related cardiac vagal tone changes (Paine,
Kishor, Worthen, Gregory, & Aziz, 2009). Therefore,
taking into account the fear-avoidance model and previous
findings with other chronic pain conditions, the objectives
of this cross-sectional study in FM patients were the fol-
lowing: (1) analyze the relationships between personality
dimensions and pain catastrophizing, pain anxiety, and
vigilance to pain; (2) determine the contribution of per-
sonality dimensions in these cognitive-affective factors; (3)
explore the mediating role of pain catastrophizing in the
relationship between neuroticism and pain anxiety; and (4)
explore the moderating role of neuroticism in the rela-
tionship between impairment and both pain catastrophizing
and pain anxiety.
Method
Subjects and Procedure
Seventy-four subjects with FM (70 women and four men)
with a mean age of 46.54 years (SD = 8.13, ran-
ge = 24–62 years) recruited from a FM association in
Granada (Spain), participated in this study. All the patients
were diagnosed with FM in a rheumatology clinic
according to the criteria of the American College of
Rheumatology (ACR; Wolfe et al., 1990). The fulfillment
of the following criteria was required: (1) age range from
18 to 65 years; (2) no history of alcoholism or drug
addiction; (3) absence of concomitant major medical con-
ditions (e.g., inflammatory rheumatic diseases, endocrine
disorders), and (4) no presence of major depressive disor-
der with severe symptoms or suicide ideation, or other
major axis I diagnoses of the DSM-IV-TR (APA, 2000).
The patients of the FM association were contacted by
telephone and invited to participate in the study. From a
potential sample of 100 people, 74 participants were
selected as the final clinical group for the study. Of the
sample contacted, 15 patients refused to participate in the
study, four subjects met the criteria of major depressive
disorder with severe symptoms, and seven had comorbidity
with other rheumatic diseases (mainly arthritis). The
remarkable percentage of female patients selected
(70 women vs. 4 men) matches that found in several epi-
demiological studies. For example, the female/male ratio of
patients with FM ranged from 9:1 (Burckhardt, Jones, &
Clark, 1998) to 20:1 (Schneider, 1995). Moreover, a recent
study reported that, in the context of rheumatology, 94% of
patients with FM were women (Branco et al., 2010).
Participants were asked to complete an interview (semi-
structured format) with a duration of approximately one
hour. The interview focused on onset and course of symp-
toms, life history, lifestyle, work, personal relations, the
family and the participant’s attitudes about his/her illness,
and psychological status. After the interview, participants
were given a set of questionnaires to be completed at home.
It was verified that patients had an adequate level of reading
comprehension of the self-report measures. Questionnaires
were delivered in one week at the most. All participants were
informed about the characteristics of the study and informed
consent was obtained. Patients did not receive any incentives
to participate in the study. The study received ethical
approval from the University of Granada ethics committee.
Most of the participants were married (74.3%), had
elementary or secondary education (57.8%), and had an
inactive work situation (59.5%). The mean duration of
the diagnosed disease was 4.11 years (SD = 3.07).
Among participants, 94.6% were receiving current phar-
macological treatment (mainly analgesics, anxiolytics,
anti-inflammatory drugs, skeletal muscle relaxants, and
anti-depressants), and 93.2% of them also received other
treatments (e.g. physical exercise, acupuncture, oxygen
therapy, psychotherapy). At the time of the study, patients
had a stabilized pharmacological pattern and none of them
were receiving structured cognitive-behavioral therapy for
their problem.
Measurements
The Short-Form McGill Pain Questionnaire (SF-MPQ;
Melzack, 1987)
The SF-MPQ assesses pain experience using 15 verbal pain
descriptors, a current pain intensity index, and a visual
analogue scale (VAS) to assess pain intensity during the
previous week, anchored with ‘‘no pain’’ (1) and ‘‘extreme
pain’’ (10). Several studies have reported the reliability and
validity of the Spanish version of the MPQ (e.g. Lazaro
et al., 2001). The internal consistency of the MPQ was .74
(Masedo & Esteve, 2000). The VAS was used in this study.
The Impairment and Functioning Inventory
(IFI; Ramırez-Maestre & Valdivia, 2003)
The 19-item IFI evaluates daily functioning and deterio-
ration of patients with chronic pain in several areas of life.
J Clin Psychol Med Settings
123

The IFI includes two general indices (Functioning and
Impairment) and four specific dimensions (Household
activity, Independent functioning, Social activities, and
Leisure activities). This inventory has adequate reliability
(.76 in functioning and .72 in impairment) and a factor
analysis confirmed its four-factor structure (Ramırez-
Maestre & Valdivia, 2003). The Impairment index was
used in this study.
The Pain Catastrophizing Scale (PCS; Sullivan, Bishop, &
Pivik, 1995)
The PCS assesses the rumination, magnification, and
helplessness associated with pain. It includes 13 items
measured on a 5-point Likert scale ranging from 0 (not at
all) to 4 (all the time). The PCS shows adequate internal
consistency and concurrent and discriminant validity
(Osman et al., 2000). In the present study, the Cronbach
alpha of the Spanish version of the PCS was .93.
The Pain Anxiety Symptoms Scale-20 (PASS-20;
McCracken & Dhingra, 2002)
The PASS-20 assesses the fear, cognitive anxiety, escape/
avoidance behavior, and physiological anxiety associated
with pain. This is a 20-item scale where subjects respond to
a 6-point Likert scale ranging from 0 (never) to 5 (always).
The PASS-20 has good convergent validity and reliability
(Roelofs et al., 2004). In the present study, the Cronbach
alpha of the Spanish version of the PASS-20 was .88.
The Pain Vigilance and Awareness Questionnaire (PVAQ;
McCracken, 1997)
The PVAQ consists of 16 items that evaluate attention to
pain using a 6-point Likert scale ranging from 0 (never) to
5 (always). The PVAQ shows adequate convergent validity
and internal consistency (Roelofs, Peters, McCracken, &
Vlaeyen, 2003). In the present study, the Cronbach alpha of
the Spanish version of the PVAQ was .79.
The NEO Five-Factor Inventory, NEO-FFI
(Costa & McCrae, 1992)
The NEO-FFI is a well validated self-report inventory
that assesses the big five personality factors: neuroticism,
extraversion, openness, agreeableness, and conscientious-
ness. The inventory includes 60 items measured on a
5-point Likert scale ranging from ‘‘strongly disagree’’ to
‘‘strongly agree.’’ The present study used the Spanish
version by TEA Ediciones. In this version the factors
showed an internal consistency between .82 and .90.
Data Analyses
Statistical analyses were performed with SPSS 15.0 soft-
ware for Windows. The moderational and mediational
effects were performed using MedGraph (Jose, 2003) and
ModGraph (Jose, 2008). All the analyses were two-tailed
and probabilities of less than .05 were taken as significance
levels. The statistical power of the analyses was greater
than .80. The minimum required sample size for the study
was 56 subjects, given an alpha level of .05, seven pre-
dictors, an anticipated effect size of .30 (medium), and a
desired statistical power level of .80.
In order to determine the association between the cog-
nitive-affective factors of pain and personality traits,
Pearson’s correlation coefficient was obtained. A multi-
variate regression analysis was performed to explore the
contribution of personality traits to the prediction of cog-
nitive-affective factors.
The mediator effect of pain catastrophizing in the
relationship between neuroticism and pain anxiety was
analyzed using the criteria developed by Baron and Kenny
(1986). The following conditions had to be met to estab-
lish the mediation: (1) variations in neuroticism (inde-
pendent variable, IV) significantly account for variations
in pain anxiety (dependent variable, DV) (path c); (2)
variations in neuroticism (IV) significantly account for
variations in pain catastrophizing (mediator) (path a); (3)
variations in pain catastrophizing (mediator) significantly
account for variations in pain anxiety (DV) (path b); and
(4) the previous relationship between neuroticism and pain
anxiety is no longer significant once pain catastrophizing
(mediator) is controlled (path c’). Several linear regression
analyses were performed to test these conditions. The
Sobel test was used as a post-hoc analysis of the media-
tion effect.
The moderator effect of neuroticism was also analyzed
using the criteria put forward by Baron and Kenny
(1986): in predicting pain catastrophizing or pain anxiety
(DVs), the model considers the impact of the impairment
(VI), the impact of neuroticism (moderator), and the
interaction of both (VI 9 moderator); the moderator
effect is supported if the interaction is significant. Sev-
eral hierarchical regression analyses were conducted to
test this condition. Following the recommendations of
Aiken and West (1991) to eliminate multicollinearity
effects, the variables were centered (scores are put into
deviation score form by subtracting the sample mean
from all individual scores). Later, the interaction term
was formed by multiplying the centered scales. As a
post-hoc analysis of the moderation effects, several
regression lines were plotted for low, medium and high
levels of neuroticism.
J Clin Psychol Med Settings
123
Results
Descriptive Analyses
Descriptive statistics and correlation coefficients for all
measures are shown in Table 1. The mean score in pain
intensity (SF-MPQ) was 7.38. This score is within the
expectations for FM patients and indicates relatively high
levels of pain. The mean score of impairment level (3.76)
in the FM group was very similar to that reported by
patients with musculoskeletal chronic pain (Ramırez-
Maestre, Esteve, & Lopez, 2008). The mean scores of
patients with FM on the PCS, PASS-20, and PVAQ were
slightly to moderately higher than those reported in pre-
vious studies with FM patients (Roelofs et al., 2003, 2004).
Taking into account the Spanish normative data in the
NEO-FFI (Manga, Ramos, & Moran, 2004), the FM group
obtained mean scores corresponding to percentiles 85 in
neuroticism, 15 in extraversion, 30 in openness, 65 in
agreeableness, and 50 in conscientiousness.
Men (n = 4) and women with FM (n = 70) in the
present study did not differ significantly in the following
demographic variables: age (U = 110.00, p = .473), mari-
tal status (v32 = .68, p = .877), educational level (v3
2 =
3.05, p = .383) and work status (v42 = 6.65, p = .155).
No significant differences were found between men and
women (U values between 74.00, p = .107 and 132.50,
p = .894) or age groups (\40.75 years vs. [53.00 years,
groups established considering percentiles 25 and 75) in
the clinical variables analyzed (t35 values between -1.83,
p = .075 and 1.57, p = .125).
Relationship Between Self-Report Variables
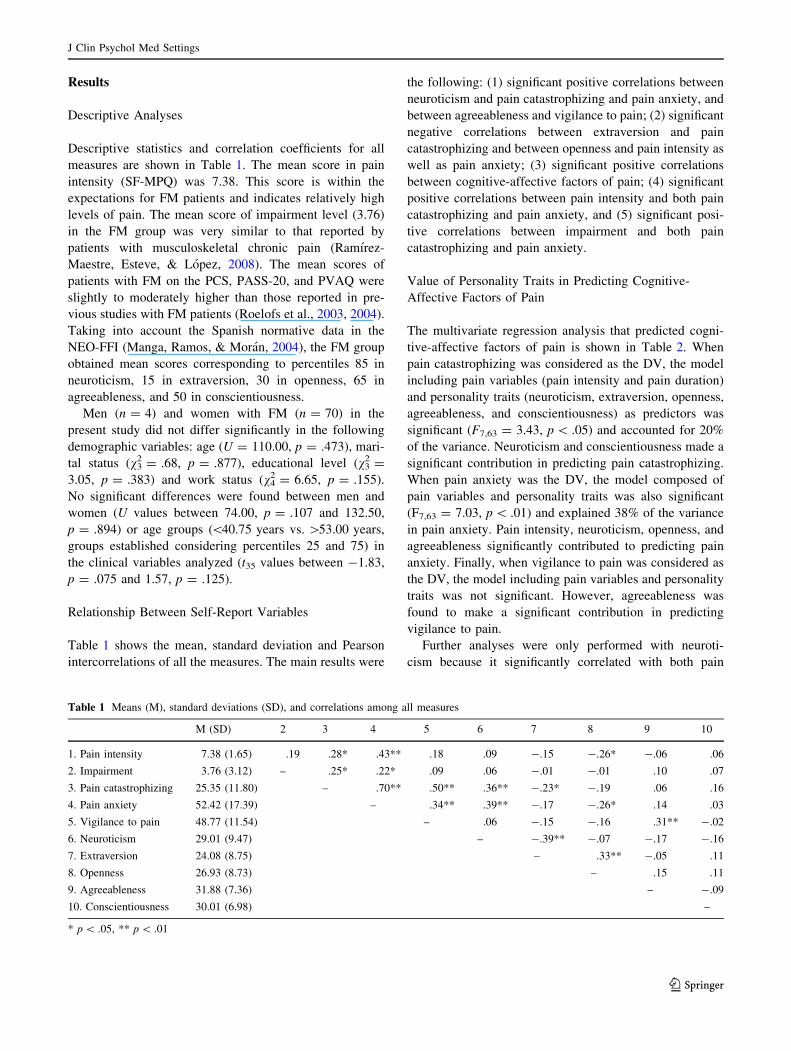
Table 1 shows the mean, standard deviation and Pearson
intercorrelations of all the measures. The main results were
the following: (1) significant positive correlations between
neuroticism and pain catastrophizing and pain anxiety, and
between agreeableness and vigilance to pain; (2) significant
negative correlations between extraversion and pain
catastrophizing and between openness and pain intensity as
well as pain anxiety; (3) significant positive correlations
between cognitive-affective factors of pain; (4) significant
positive correlations between pain intensity and both pain
catastrophizing and pain anxiety, and (5) significant posi-
tive correlations between impairment and both pain
catastrophizing and pain anxiety.
Value of Personality Traits in Predicting Cognitive-
Affective Factors of Pain
The multivariate regression analysis that predicted cogni-
tive-affective factors of pain is shown in Table 2. When
pain catastrophizing was considered as the DV, the model
including pain variables (pain intensity and pain duration)
and personality traits (neuroticism, extraversion, openness,
agreeableness, and conscientiousness) as predictors was
significant (F7,63 = 3.43, p \ .05) and accounted for 20%
of the variance. Neuroticism and conscientiousness made a
significant contribution in predicting pain catastrophizing.
When pain anxiety was the DV, the model composed of
pain variables and personality traits was also significant
(F7,63 = 7.03, p \ .01) and explained 38% of the variance
in pain anxiety. Pain intensity, neuroticism, openness, and
agreeableness significantly contributed to predicting pain
anxiety. Finally, when vigilance to pain was considered as
the DV, the model including pain variables and personality
traits was not significant. However, agreeableness was
found to make a significant contribution in predicting
vigilance to pain.
Further analyses were only performed with neuroti-
cism because it significantly correlated with both pain
Table 1 Means (M), standard deviations (SD), and correlations among all measures
M (SD) 2 3 4 5 6 7 8 9 10
1. Pain intensity 7.38 (1.65) .19 .28* .43** .18 .09 -.15 -.26* -.06 .06
2. Impairment 3.76 (3.12) – .25* .22* .09 .06 -.01 -.01 .10 .07
3. Pain catastrophizing 25.35 (11.80) – .70** .50** .36** -.23* -.19 .06 .16
4. Pain anxiety 52.42 (17.39) – .34** .39** -.17 -.26* .14 .03
5. Vigilance to pain 48.77 (11.54) – .06 -.15 -.16 .31** -.02
6. Neuroticism 29.01 (9.47) – -.39** -.07 -.17 -.16
7. Extraversion 24.08 (8.75) – .33** -.05 .11
8. Openness 26.93 (8.73) – .15 .11
9. Agreeableness 31.88 (7.36) – -.09
10. Conscientiousness 30.01 (6.98) –
* p \ .05, ** p \ .01
J Clin Psychol Med Settings
123

catastrophizing and pain anxiety and obtained the highest B
values in predicting these variables. Taking into account
the significant correlation between pain intensity and pain
catastrophizing (potential mediator), pain intensity was
included as a controlled variable in the mediational
analysis.
Pain Catastrophizing as a Mediator Between
Neuroticism and Pain Anxiety
Several regression analyses were performed to explore the
mediation of pain catastrophizing in the relationship
between neuroticism and pain anxiety, controlling for the
effect of pain intensity. In Analysis 1 (path c), both pain
intensity (b = .39, p \ .001) and neuroticism (b = .36,
p \ .001) were significant predictors and explained 28% of
the variance in pain anxiety (F2,69 = 15.27, p \ .001). In
Analysis 2 (path a) in which pain catastrophizing was
entered as the DV, both IVs were significant (pain inten-
sity, b = .23, p \ .05; and neuroticism, b = .34, p \ .01)
and explained 16% of the variance (F2,70 = 7.98, p \ .05).
In Analysis 3 (path b), pain intensity (b = .27, p \ .001)
and pain catastrophizing (b = .63, p \ .001) were signifi-
cant predictors and explained 56% of the variance in pain
anxiety (F2,70 = 46.92, p \ .001). In Analysis 4 (path c’),
pain anxiety was included as the DV (as in Analysis 1), and
pain intensity and pain catastrophizing were entered as
additional IVs with neuroticism. All of them were signifi-
cant predictors (pain intensity, b = .26, p \ .001; pain
catastrophizing, b = .58, p \ .001; and neuroticism,
b = .18, p \ .05) and explained 57% of the variance
(F3,68 = 32.74, p \ .001). The contribution of neuroticism
to pain anxiety greatly decreased (b from .36 to .18) when
the effect of pain catastrophizing was considered. The
difference between path c and path c’ was significant, as
revealed by the Sobel test (z = 2.86, p \ .01). The ratio
index (computed by dividing the indirect effect by the total
effect; Jose, 2003) indicated that 53% of the influence of
neuroticism on pain anxiety was mediated by pain
catastrophizing.
Neuroticism as a Moderator Between Impairment
and Pain Catastrophizing
To test for neuroticism as a moderator between impairment
and pain catastrophizing, the cross-product terms neuroti-
cism and impairment were entered in a separate block in a
hierarchical regression analysis, following the entry of
Table 2 Multivariate regression analysis predicting pain catastrophizing, pain anxiety, and vigilance to pain
Dependent variable Independent variable B SEB t Adjusted R2 F
Pain catastrophizing Pain intensity 1.14 .80 1.41 .20 3.43*
Pain duration .18 .41 .44
Neuroticism .49 .15 3.29*
Extraversion -.01 .17 -.11
Openness -.24 .16 -1.53
Agreeableness .33 .17 1.84
Conscientiousness .43 .18 2.38*
Pain anxiety Pain intensity 3.72 1.05 3.53** .38 7.03**
Pain duration .86 .53 1.61
Neuroticism .89 .19 4.55**
Extraversion .22 .22 1.01
Openness -.43 .21 -2.04*
Agreeableness .67 .23 2.85*
Conscientiousness .33 .24 1.40
Vigilance to pain Pain intensity .64 .84 .76 .09 2.01
Pain duration .02 .43 .06
Neuroticism .10 .15 .69
Extraversion -.02 .17 -.11
Openness -.25 .16 -1.47
Agreeableness .60 .18 3.23*
Conscientiousness .06 .19 .35
* p \ .05, ** p \ .01
J Clin Psychol Med Settings
123
impairment and neuroticism as first-order terms. Signifi-
cant main effects were found for impairment (b = .24,
p \ .05) and neuroticism (b = .34, p \ .01). Yet, the
interaction impairment 9 neuroticism was not a significant
predictor of pain catastrophizing (b = .08, p = .449).
Neuroticism did not have a significant moderating effect on
the relationship between impairment and pain
catastrophizing.
Neuroticism as a Moderator Between Impairment
and Pain Anxiety
To explore neuroticism as a moderator, we tested whether
the interaction impairment 9 neuroticism was a signifi-
cant predictor of pain anxiety, after controlling the influ-
ence of impairment and neuroticism. Significant main
effects were observed for impairment (b = .23, p \ .05)
and neuroticism (b = .39, p \ .001). An effect close to
statistical significance was observed in the impair-
ment 9 neuroticism interaction (b = .20, p = .06),
revealing that the link between impairment and pain anx-
iety is probably moderated by neuroticism. The overall
model explained 21% of the variance in pain anxiety
(F3,68 = 7.36, p \ .01).
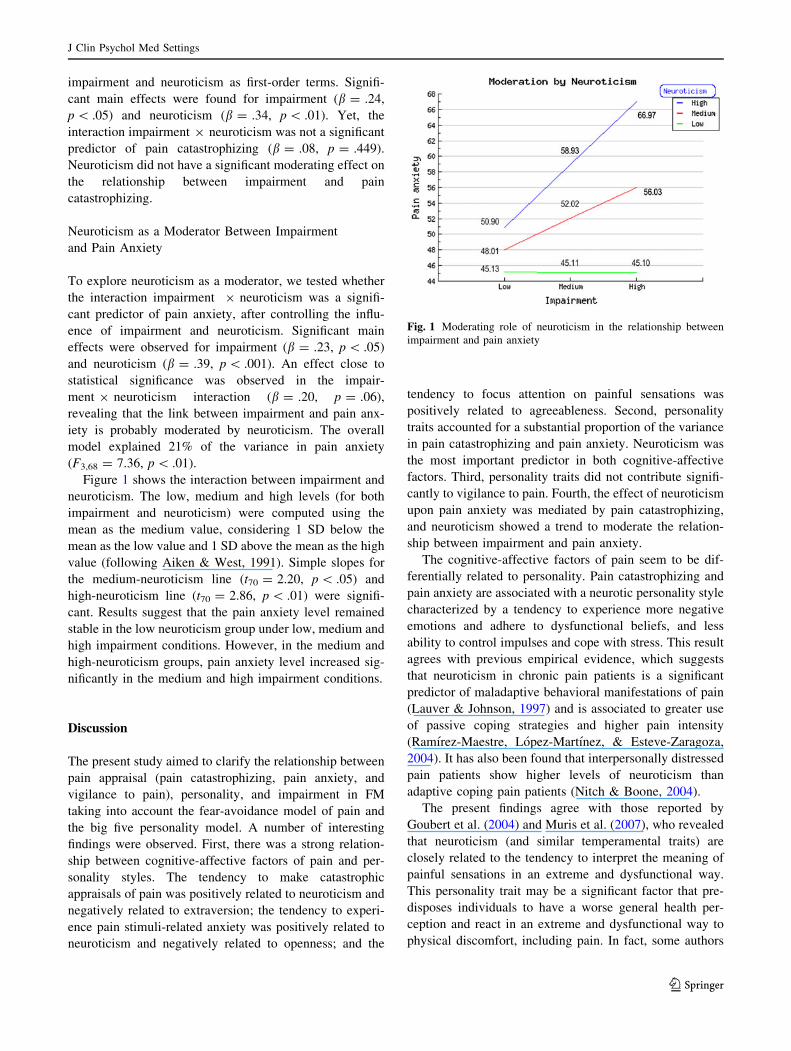
Figure 1 shows the interaction between impairment and
neuroticism. The low, medium and high levels (for both
impairment and neuroticism) were computed using the
mean as the medium value, considering 1 SD below the
mean as the low value and 1 SD above the mean as the high
value (following Aiken & West, 1991). Simple slopes for
the medium-neuroticism line (t70 = 2.20, p \ .05) and
high-neuroticism line (t70 = 2.86, p \ .01) were signifi-
cant. Results suggest that the pain anxiety level remained
stable in the low neuroticism group under low, medium and
high impairment conditions. However, in the medium and
high-neuroticism groups, pain anxiety level increased sig-
nificantly in the medium and high impairment conditions.
Discussion
The present study aimed to clarify the relationship between
pain appraisal (pain catastrophizing, pain anxiety, and
vigilance to pain), personality, and impairment in FM
taking into account the fear-avoidance model of pain and
the big five personality model. A number of interesting
findings were observed. First, there was a strong relation-
ship between cognitive-affective factors of pain and per-
sonality styles. The tendency to make catastrophic
appraisals of pain was positively related to neuroticism and
negatively related to extraversion; the tendency to experi-
ence pain stimuli-related anxiety was positively related to
neuroticism and negatively related to openness; and the
tendency to focus attention on painful sensations was
positively related to agreeableness. Second, personality
traits accounted for a substantial proportion of the variance
in pain catastrophizing and pain anxiety. Neuroticism was
the most important predictor in both cognitive-affective
factors. Third, personality traits did not contribute signifi-
cantly to vigilance to pain. Fourth, the effect of neuroticism
upon pain anxiety was mediated by pain catastrophizing,
and neuroticism showed a trend to moderate the relation-
ship between impairment and pain anxiety.
The cognitive-affective factors of pain seem to be dif-
ferentially related to personality. Pain catastrophizing and
pain anxiety are associated with a neurotic personality style
characterized by a tendency to experience more negative
emotions and adhere to dysfunctional beliefs, and less
ability to control impulses and cope with stress. This result
agrees with previous empirical evidence, which suggests
that neuroticism in chronic pain patients is a significant
predictor of maladaptive behavioral manifestations of pain
(Lauver & Johnson, 1997) and is associated to greater use
of passive coping strategies and higher pain intensity
(Ramırez-Maestre, Lopez-Martınez, & Esteve-Zaragoza,
2004). It has also been found that interpersonally distressed
pain patients show higher levels of neuroticism than
adaptive coping pain patients (Nitch & Boone, 2004).
The present findings agree with those reported by
Goubert et al. (2004) and Muris et al. (2007), who revealed
that neuroticism (and similar temperamental traits) are
closely related to the tendency to interpret the meaning of
painful sensations in an extreme and dysfunctional way.
This personality trait may be a significant factor that pre-
disposes individuals to have a worse general health per-
ception and react in an extreme and dysfunctional way to
physical discomfort, including pain. In fact, some authors
Fig. 1 Moderating role of neuroticism in the relationship between
impairment and pain anxiety
J Clin Psychol Med Settings
123

have argued that neuroticism may not simply reflect over-
reporting of physical complaints but can also be seen as a
potential vulnerability factor to poor health (Johnson,
2003). This trait has also been found to predispose indi-
viduals to psychological distress and not to show positive
emotions, which in turn may lead to medically unexplained
symptoms (De Gucht, Fischler, & Heiser, 2004).
Interestingly, our findings suggest that neuroticism
(negative affectivity) was the greatest contributor to both
pain catastrophizing and pain anxiety. The present study
also found that 53% of the influence of neuroticism on
pain anxiety was mediated by pain catastrophizing. This
finding is consistent with the ‘‘fear-avoidance’’ model of
pain developed by Leeuw et al. (2007). The present results
agree with previous studies that showed that pain catas-
trophizing and pain-related fear mediated the relationship
between neuroticism and vigilance to pain (Goubert et al.,
2004). However, they differ from those reported by
Asghari and Nicholas (2006), who found, in a prospective
study with chronic pain patients, that neuroticism was not
a significant predictor of residualized change in catastro-
phizing over time. The present data also differ from those
reported by Goubert et al. (2004), who observed that
neuroticism predicted vigilance to pain. It should be noted
that the present study did not analyze exactly the same
paths as those reported by Goubert et al., that it did not
use the prospective design by Asghari and Nicholas, and
that none of these studies included FM patients. Addi-
tionally, we observed that neuroticism is probably a sig-
nificant moderator in the relationship between impairment
in daily functioning and anxiety responses associated to
painful stimuli: pain anxiety tends to be more marked at
higher levels of impairment when neuroticism is high.
This result is in line with the study performed by Goubert
et al. (2004), who found that neuroticism moderated
the relationship between pain severity and pain
catastrophizing.
The fact that neuroticism shows a trend to moderate the
relationship between impairment and pain anxiety but not
between impairment and pain catastrophizing may be
explained considering that pain anxiety involves a more
severe stage than pain catastrophizing in the spiral of fear-
avoidance. The PASS-20 assesses a broad construct that
includes alarmist appraisal of pain (like the PCS), but also
avoidance and escape strategies of coping with pain, and
physiological anxiety responses. Therefore, when faced
with the functional limitations associated with his/her dis-
ease, a FM patient with a neurotic personality style may
tend to respond in a maladaptive way at multiple levels
(cognitive, behavioral, or physiological), reflecting a
greater degree of pain anxiety. Further studies are needed
to explain the hierarchical relationship between the cog-
nitive-affective factors associated with pain.
The present findings indicate maladaptive aspects of
neuroticism, which is consistent with the abovementioned
studies and evidence that show that this personality trait is
associated with many psychological and physical problems
(see review by Lahey, 2009). However, neuroticism as a
strategy may have an adaptive value. According to Watson
and Casillas, (2003), extremely low levels of neuroticism
increase individual’s vulnerability to several types of
threat, so neuroticism may play an active and beneficial
role in health-related awareness.
The present research considers pain catastrophizing as
an appraisal process, however, different theoretical con-
ceptualizations of pain catastrophizing have been proposed.
For example, the communal coping model suggests that
catastrophizing represents an interpersonal strategy to cope
with pain (Sullivan et al., 2001). Catastrophizers may
exaggerate pain expression to obtain proximity, assistance
and support from others, thereby heightening pain experi-
ence and making difficult adaptation to pain. According to
this model, solicitous or reinforcing responses from others
may contribute to maintain the exaggerated pain expression
of catastrophizers.
The present study also highlighted the role of other
personality dimensions such as conscientiousness, open-
ness, and agreeableness in pain appraisal. The findings
show that a high level of conscientiousness (characterized
by a tendency to plan, persistence, control, and motivation
in goal-directed behavior) is a significant predictor of pain
catastrophizing. This finding differs from those reported by
Goubert et al. (2004), who found that conscientiousness
was not a significant predictor of pain catastrophizing but
of vigilance to pain. Some studies have shown that the
relationship between this personality trait and health is
influenced by gender differences. For example, conscien-
tious women report more lumps or growths while consci-
entious men report less depression and constipation as
well as better general health perception and more vitality
(Jerram & Coleman, 1999).
Our study revealed that a low level of openness to
experience is closely related to pain-related anxiety and
predicts a significant proportion of variance in this cogni-
tive-affective factor. Individuals with lower levels of
intellectual curiosity, creativity, and open-mindedness to
fantasy, internal feelings, news activities, values, etc., show
a greater tendency to react anxiously to painful stimuli.
This is in line with some reports that suggest high openness
is associated with positive appraisals to health (Jerram &
Coleman, 1999; Nitch & Boone, 2004).
We observed that a high level of agreeableness (char-
acterized by a tendency to be altruistic, cooperative and
helpful towards others) was a significant predictor of pain
anxiety. Similarly, this personality trait was related to
vigilance to pain, explaining a significant proportion of the
J Clin Psychol Med Settings
123

variance. It is necessary to consider that these finding may
be showing the alexithymic trends of FM patients. People
with high levels of agreeableness tend to inhibit commu-
nicating negative emotions to others. Previous studies have
reported that FM subjects scored higher on alexithymia
than healthy controls, even when negative affectivity was
considered as a covariate (Brosschot & Aarsse, 2001) and
difficulty identifying feelings is the dimension of alexi-
thymia most closely associated with FM (Sayar, Gulec, &
Topbas, 2004). This is consistent with the well-known
difficulty of patients with somatoform pain to communicate
their emotions and pain experiences (Cox, Kuch, Parker,
Shulman, & Evans, 1994). It is noteworthy, however, that
findings on agreeableness differ from those obtained in
previous studies (Jerram & Coleman, 1999).
Although several studies have supported the role of
catastrophizing as a cognitive vulnerability-stress factor
related to emotional distress in chronic pain patients (Lee,
Wu, Lee, Cheing, & Chan, 2008), this study suggests that
other more basic personality traits influence the develop-
ment of these dysfunctional cognitive styles that disrupt
mood and adjustment in FM. Personality is probably an
important factor in the pathophysiology of FM. Studies
about the alterations of the autonomic nervous system and
the HPA axis suggest a contribution of these stress-
response systems in vulnerability to FM or in symptom
expression in FM (Dadabhoy, Crofford, Spaeth, Russell, &
Clauw, 2008). Recent research has analyzed the association
between personality traits and the HPA axis, reporting that
high levels of neuroticism were associated with elevated
levels of evening cortisol in subjects under 75 years old
(Gerritsen et al., 2009). In this context, a marked neurotic
style may influence the way individuals cognitively process
pain-related stimuli, reduce their perceived ability to
manage distress, and predispose individuals with limita-
tions in daily functioning to experience pain anxiety. All
this ultimately leads to exacerbation of disease. Much more
research is needed to understand the vulnerability role of
neuroticism and other personality dimensions in FM.
Limitations and Conclusions
The present study has some limitations. All the measures
used were self-reported. Although the VAS of the SF-MPQ
has good sensitivity and specificity, and these values are
considerably similar to those obtained with dolorimetry
(Marques, Assumpcao, Matsutani, Pereira, & Lage, 2008),
in future research, it would be advisable to use a pressure
algometer. The algometer may offer complementary
information to that provided by self-report measures.
Another limitation of our study is the small sample, which
we hope to expand in future studies. This is a preliminary
study within broader research we are currently conducting.
The cross-sectional design did not provide knowledge
about the direction of causality of the relationships
explored. In addition, since only one pain sample was used,
it was not possible to determine whether the findings were
specific to FM or would have also been identified in other
chronic pain problems. Patients in this study came from a
FM association and may have different clinical character-
istics (including perception of pain and ability to manage
it) from those observed in patients of rheumatology ser-
vices. In future research, it would be advisable to replicate
the study using a longitudinal design as well as a sample of
patients with different pain conditions from other medical
contexts.
Lastly, the combination of personality traits may explain
some of the differences observed between studies. It would
be useful for future studies to explore in FM patients with
high-neuroticism whether agreeableness, openness, and
conscientiousness are associated with worse perception of
physical health. It would also be important to study whe-
ther the role of these personality traits is due to some
specific facets of the traits and can be modulated by vari-
ables such as sex, health status, pain intensity, and so on.
Additional studies are needed to clarify the conditions
under which the big five factors influence the experience of
pain.
Our findings have relevant practical implications.
Keeping in mind the heterogeneity of FM patients, it
would be very useful to assess personality traits that
predispose individuals to have a greater risk of experi-
encing pain as threatening and fearful. Early identification
of FM patients with high levels of these traits seems
crucial, given that such patients could greatly benefit from
therapies focused on changing dysfunctional attitudes
toward pain. This is relevant to successfully preventing
disability. Several reviews have reported that cognitive-
behavioral interventions are effective in reducing fear-
avoidance beliefs in chronic pain (Lohnberg, 2007) and
catastrophizing in FM (Glombiewski et al., 2010), how-
ever, it is unknown how personality traits influence the
efficacy of this type of intervention. Considering our
findings, neuroticism might modulate the degree of change
in pain anxiety of FM patients and might therefore be a
useful predictor of treatment outcomes. Future research
analyzing the relationship between personality traits and
the fear-avoidance model in greater depth is needed to
improve our understanding of FM and its clinical
management.
Acknowledgments This study is part of a broader research project
financially supported by the Spanish ministry of science and inno-
vation (research project PSI2009-13765PSIC). The authors wish to
thank AGRAFIM (Association of People Affected with FM in Gra-
nada, Spain) for its cooperation in the study.
J Clin Psychol Med Settings
123

References
Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing andinterpreting interactions. Newbury Park, CA: Sage.
American Psychiatric Association. (2000). Diagnostic and statisticalmanual of mental disorders (4th ed. rev.). Washington, DC: APA
(Spanish translation: Barcelona, Masson, 2002).
Anderberg, U. A., Forsgren, T., Ekselius, L., Marteinsdottir, I., &
Hallman, J. (1999). Personality traits on the basis of the
temperament and character inventory in female fibromyalgia
syndrome patients. Nordic Journal of Psychiatry, 53, 353–359.
Asghari, A., & Nicholas, M. K. (2006). Personality and pain-related
beliefs/coping strategies: A prospective study. Clinical Journalof Pain, 22, 10–18.
Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator
variable distinction in social psychology research: Conceptual,
strategic, and statistical considerations. Journal of Personalityand Social Psychology, 51, 1173–1182.
Bazzichi, L., Rossi, A., Massimetti, G., Giannaccini, G., Giuliano, T.,
De Feo, F., et al. (2007). Cytokine patterns in fibromyalgia and
their correlation with clinical manifestations. Clinical Experi-mental Rheumatology, 25, 225–230.
Branco, J. C., Bannwarth, B., Failde, I., Abello, C. J., Blotman, F.,
Spaeth, M., et al. (2010). Prevalence of fibromyalgia: A survey
in five European countries. Seminars in Arthritis and Rheuma-tism, 39, 448–453.
Brosschot, J. F., & Aarsse, H. R. (2001). Restricted emotional
processing and somatic attributions in fibromyalgia. Interna-tional Journal of Psychiatry and Medicine, 31, 127–146.
Buckelew, S. P., Murray, S. E., Hewett, J. E., Johnson, J., & Huyser,
B. (1995). Self-efficacy, pain and physical activity among
fibromyalgia subjects. Arthritis and Rheumatism, 8, 43–50.
Burckhardt, C. S., Jones, K. D., & Clark, S. R. (1998). Soft tissue
problems associated with rheumatic disease. Lippincott’sPrimary Care Practice, 2, 20–29.
Carver, C. S., & Scheier, M. F. (2000). Perspectives on personality(4th ed.). Needham Heights, MA: Simon & Schuster.
Cook, A. J., Brawer, P. A., & Vowles, K. E. (2006). The fear-
avoidance model of chronic pain: Validation and age analysis
using structural equation modeling. Pain, 121, 195–206.
Costa, P. T., & McCrae, R. R. (1992). NEO-PI-R, Revised NEOPersonality Inventory and NEO Five-Factor Inventory (NEO-
FFI). Psychological Assessment Resources, Inc. Odessa, FL,
(Spanish version: Madrid, TEA Ediciones, 2002).
Cox, B. J., Kuch, K., Parker, J. D., Shulman, I. D., & Evans, R. J.
(1994). Alexithymia in somatoform disorder patients with
chronic pain. Journal of Psychosomatic Research, 38, 523–527.
Crombez, G., Eccleston, C., Van den Broeck, A., Goubert, L., & Van
Houdenhove, B. (2004). Hypervigilance to pain in fibromyalgia:
The mediating role of pain intensity and catastrophic thinking
about pain. Clinical Journal of Pain, 20, 98–102.
Dadabhoy, D., Crofford, L. J., Spaeth, M., Russell, I. J., & Clauw, D.
J. (2008). Biology and therapy of fibromyalgia. Evidence-based
biomarkers for fibromyalgia syndrome. Arthritis Research andTherapy, 10:211. doi:10.1186/ar2443.
De Gucht, V., Fischler, B., & Heiser, W. (2004). Neuroticism,
alexithymia, negative affect, and positive affect as determinants
of medically unexplained symptoms. Personality and IndividualDifferences, 36, 1655–1667.
Garcıa-Campayo, J., Pascual, A., Alda, M., & Gonzalez-Ramırez, M.
T. (2007). Coping with fibromyalgia: Usefulness of the Chronic
Pain Coping Inventory-42. Pain, 132, S68–S76.
Gerritsen, L., Geerlings, M. I., Bremmer, M. A., Beekman, A. T. F.,
Deeg, D. J. H., Penninx, B. W. J. H., et al. (2009). Personal-
ity characteristics and hypothalamic-pituitary-adrenal axis
regulation in older persons. American Journal of GeriatricPsychiatry, 17, 1077–1084.
Glombiewski, J. A., Sawyer, A. T., Gutermann, J., Koenig, K., Rief,
W., & Hofmann, S. G. (2010). Psychological treatments for
fibromyalgia: A meta-analysis. Pain, 151, 280–295.
Goubert, L., Crombez, G., & Van Damme, S. (2004). The role of
neuroticism, pain catastrophizing and pain-related fear in
vigilance to pain: A structural equations approach. Pain, 107,
234–241.
Hassett, A. I., Cone, J., Patella, S. J., & Sigal, L. H. (2000). The role of
catastrophizing in the pain and depression of women with
fibromyalgia syndrome. Arthritis and Rheumatism, 43, 2493–2500.
Herrero, A. M., Ramırez-Maestre, C., & Gonzalez, V. (2008).
Personality, cognitive appraisal and adjustment in chronic pain
patients. Spanish Journal of Psychology, 11, 531–542.
Jerram, K. L., & Coleman, P. G. (1999). The big five personality traits
and reporting of health problems and health behaviour in old age.
British Journal of Health Psychology, 4, 181–192.
Johnson, M. (2003). The vulnerability status of neuroticism: Over-
reporting or genuine complaints? Personality and IndividualDifferences, 35, 877–887.
Jose, P. E. (2003). MedGraph-I: A programme to graphically depictmediation among three variables: The internet version, version2.0. Victoria University of Wellington, Wellington, New Zea-
land. Retrieved from http://www.victoria.ac.nz/staff/paul-jose-
files/medgraph/medgraph.php.
Jose, P. E. (2008). ModGraph-I: A programme to compute cell meansfor the graphical display of moderational analyses: The internetversion, Version 2.0. Victoria University of Wellington, Wel-
lington, New Zealand. Retrieved from: http://www.victoria.ac.
nz/psyc/staff/paul-jose-files/modgraph/modgraph.php.
Kristensen, A. S., Mortensen, E. L., & Mors, O. (2009). The
association between bodily anxiety symptom dimensions and the
scales of the revised NEO Personality Inventory and the
Temperament and Character Inventory. Comprehensive Psychi-atry, 50, 38–47.
Lachaine, J., Beauchemin, C., & Landry, P.-A. (2010). Clinical and
economic characteristics of patients with fibromyalgia syn-
drome. Clinical Journal of Pain, 26, 284–290.
Lahey, B. B. (2009). Public health significance of neuroticism.
American Psychologist, 64, 241–256.
Lauver, S. C., & Johnson, J. L. (1997). The role of neuroticism and
social support in older adults with chronic pain behavior.
Personality and Individual Differences, 23, 165–167.
Lawrence, R. C., Felson, D. T., Helmick, C. G., Arnold, L. M., Choi,
H., Deyo, R. A., et al. (2008). Estimates of the prevalence of
arthritis and other rheumatic conditions in the United States. Part
II. Arthritis and Rheumatism, 58, 26–35.
Lazaro, C., Caseras, X., Whizar-Lugo, V. M., Wenk, R., Baldioceda,
F., Bernal, R., et al. (2001). Psychometric properties of a Spanish
version of the McGill Pain Questionnaire in several Spanish-
speaking countries. Clinical Journal of Pain, 17, 365–374.
Lazarus, R. S., & Folkman, S. (1984). Stress appraisal and coping.New York: Springer.
Lee, J. E. (2009). The psychology of pain: The influence of
personality on experimentally-induced pain perception. Disser-tation Abstracts International: Section B: The Sciences andEngineering, 70, 1348.
Lee, E.-J., Wu, M.-Y., Lee, G. K., Cheing, G., & Chan, F. (2008).
Catastrophizing as a cognitive vulnerability factor related to
depression in workers’ compensation patients with chronic
musculoskeletal pain. Journal of Clinical Psychology in MedicalSettings, 15, 182–192.
Leeuw, M., Goossens, M. E. J. B., Linton, S. J., Crombez, G.,
Boersma, K., & Vlaeyen, J. W. S. (2007). The fear-avoidance
J Clin Psychol Med Settings
123

model of musculoskeletal pain: Current state of scientific
evidence. Journal of Behavioral Medicine, 30, 77–94.
Lohnberg, J. A. (2007). A review of outcome studies on cognitive-
behavioural therapy for reducing fear-avoidance beliefs among
individuals with chronic pain. Journal of Clinical Psychology inMedical Settings, 14, 113–122.
Malt, E. A., Olafsson, S., Lund, A., & Ursin, H. (2002). Factors
explaining variance in perceived pain in women with fibromy-
algia. BMC Musculoskeletal Disorders, 3, 12. doi:10.1186/14
71-2474-3-12.
Manga, D., Ramos, F., & Moran, C. (2004). The Spanish norms of the
NEO five-factor inventory: New data and analyses for its
improvement. International Journal of Psychology and Psycho-logical Therapy, 4, 639–648.
Marques, A. P., Assumpcao, A., Matsutani, L. A., Pereira, C. A. B., &
Lage, L. (2008). Pain in fibromyalgia and discriminative power
of the instruments: Visual analog scale, dolorimetry and the
McGill Pain Questionnaire. Acta Reumatologica Portuguesa, 33,
345–351.
Masedo, A. I., & Esteve, R. (2000). Some empirical evidence
regarding the validity of the Spanish version of the McGill Pain
Questionnaire (MPQ-SV). Pain, 85, 451–456.
Mcallister, M. J. (2000). The unvanquished: Prevalence of moral
masochistic personality characteristics in persons with fibromy-
algia. Dissertation Abstracts International Section B: TheSciences and Engineering, 61, 540.
McCracken, L. M. (1997). ‘Attention’ to pain in persons with chronic
pain: A behavioural approach. Behaviour Therapy, 28, 271–284.
McCracken, L. M., & Dhingra, L. (2002). A short version of the Pain
Anxiety Symptoms Scale (PASS-20): Preliminary development
and validity. Pain Research and Management, 7, 45–50.
Melzack, R. (1987). The short form McGill Pain Questionnaire. Pain,30, 191–197.
Miro, E., Lupianez, J., Hita, E., Martınez, M. P., Sanchez, A. I., &
Buela-Casal, G. (2011). Attentional deficits in fibromyalgia and
its relationships with pain, emotional distress and sleep dys-
function complaints. Psychology and Health, 26, 765–780.
Muris, P., Meesters, C., Van den Hout, A., Wessels, S., Franken, I., &
Rassin, E. (2007). Personality and temperament correlates of
pain catastrophizing in young adolescents. Child Psychiatry andHuman Development, 38, 171–181.
Neumann, L., & Buskila, D. (2003). Epidemiology of fibromyalgia.
Current Pain and Headache Reports, 7, 362–368.
Nicassio, P. M., Schuman, C., Radojevic, V., & Weisman, M. H.
(1999). Helplessness as a mediator of health status in fibromy-
algia. Cognitive, Therapy and Research, 23, 181–196.
Nishikai, M., Tomomatsu, S., Hankins, R. W., Takagi, S., Miyachi,
K., Kosaka, S., et al. (2001). Autoantibodies to a 68/48 kDa
protein in chronic fatigue syndrome and primary fibromyalgia: A
possible marker for hypersomnia and cognitive disorders.
Rheumatology, 40, 806–810.
Nitch, S. R., & Boone, K. B. (2004). Normal personality correlates of
chronic pain subgroups. Journal of Clinical Psychology inMedical Settings, 11, 203–209.
Osman, A., Barrios, F. X., Gutierrez, P. M., Kopper, B. A., Merrifield,
T., & Grittman, L. (2000). The Pain Catastrophizing Scale:
Further psychometric evaluation with adult samples. Journal ofBehavioral Medicine, 23, 351–365.
Paine, P., Kishor, J., Worthen, S. F., Gregory, L. J., & Aziz, Q.
(2009). Exploring relationships for visceral and somatic pain
with autonomic control and personality. Pain, 144, 236–244.
Pamuk, O. N., & Cakir, N. (2007). The frequency of thyroid
antibodies in fibromyalgia patients and their relationship with
symptoms. Clinical Rheumatology, 26, 55–59.
Perez-Pareja, J., Sese, A., Gonzalez-Ordi, H., & Palmer, A. (2010).
Fibromyalgia and chronic pain: Are there discriminating patterns
by using the Minnesota Multiphasic Personality Inventory-2
(MMPI-2)? International Journal of Clinical and HealthPsychology, 10, 41–56.
Quartana, P. J., Campbell, C. M., & Edwards, R. R. (2009). Pain
catastrophizing: A critical review. Expert Review of Neurother-apeutics, 9, 745–758.
Ramırez-Maestre, C., Esteve, R., & Lopez, A. E. (2008). Cognitive
appraisal and coping in chronic pain patients. European Journalof Pain, 12, 749–756.
Ramırez-Maestre, C., Lopez-Martınez, A. E., & Esteve-Zaragoza, R.
(2004). Personality characteristics as differential variables of the
pain experience. Journal of Behavioral Medicine, 27, 147–165.
Ramırez-Maestre, C., & Valdivia, Y. (2003). Evaluacion del funcio-
namiento diario en pacientes con dolor cronico [Evaluation of
daily functioning in patients with chronic pain]. PsicologıaConductual, 11, 283–291.
Roelofs, J., McCracken, L., Peters, M. L., Crombez, G., van
Breukelen, G., & Vlaeyen, J. W. S. (2004). Psychometric
evaluation of the Pain Anxiety Symptoms Scale (PASS) in
chronic pain patients. Journal of Behavioral Medicine, 27,
167–183.
Roelofs, J., Peters, M. L., McCracken, L., & Vlaeyen, J. W. S. (2003).
The Pain Vigilance and Awareness Questionnaire (PVAQ):
Further psychometric evaluation in fibromyalgia and other
chronic pain syndromes. Pain, 101, 299–306.
Ross, R. L., Jones, K. D., Bennett, R. M., Ward, R. L., Druker, B. J.,
& Wood, L. J. (2010). Preliminary evidence of increased pain
and elevated cytokines in fibromyalgia patients with defective
growth hormone response to exercise. Open ImmunologyJournal, 3, 9–18.
Sanchez, A. I., Martınez, M. P., Miro, E., & Medina, A. (2011).
Predictors of the pain perception and self-efficacy for pain
control in patients with fibromyalgia. Spanish Journal ofPsychology, 14, 366–373.
Sayar, K., Gulec, H., & Topbas, M. (2004). Alexithymia and anger in
patients with fibromyalgia. Clinical Rheumatology, 23, 441–448.
Schneider, M. J. (1995). Tender points/fibromyalgia vs. trigger points/
myofascial pain syndrome: A need for clarity in terminology anddifferential diagnosis. Journal of Manipulative and Physiolog-ical Therapeutics, 18, 398–406.
Sullivan, M. J. L., Bishop, S., & Pivik, J. (1995). The Pain
Catastrophizing Scale: Development and validation. Psycholog-ical Assessment, 7, 524–532.
Sullivan, M. J. L., Thorn, B., Haythornthwaite, J. A., Keefe, F.,
Martin, M., Bradley, L. A., et al. (2001). Theoretical perspec-
tives on the relation between catastrophizing and pain. ClinicalJournal of Pain, 17, 52–64.
Thorn, B. E., Clements, K. L., Ward, L. C., Dixon, K. E., Kersh, B.
C., Boothby, J. L., et al. (2004). Personality factors in the
explanation of sex differences in pain catastrophizing and
response to experimental pain. Clinical Journal of Pain, 20,
275–282.
Trygg, T., Lundberg, G., Rosenlund, E., Timpka, T., & Bjorn, G.
(2002). Personality characteristics of women with fibromyalgia
and of women with chronic neck, shoulder, or low back
complaints in terms of Minnesota Multiphasic Personality
Inventory and defense mechanisms technique modified. Journalof Musculoskeletal Pain, 10, 33–55.
Turk, D. C., Robinson, J. P., & Burwinkle, T. (2004). Prevalence of
fear of pain and activity in patients with fibromyalgia syndrome.
Journal of Pain, 5, 483–490.
Turner, J. A., & Aaron, L. A. (2001). Pain-related catastrophizing:
What is it? Clinical Journal of Pain, 17, 65–71.
Vearing, A., & Mak, A. S. (2007). Big five personality and effort-
reward imbalance factors in employee’s depressive symptoms.
Personality and Individual Differences, 43, 1744–1755.
J Clin Psychol Med Settings
123

Vlaeyen, J. W. S., & Linton, S. J. (2000). Fear-avoidance and its
consequences in chronic musculoskeletal pain: A state of the art.
Pain, 85, 317–332.
Watson, D., & Casillas, A. (2003). Neuroticism: Adaptive and
maladaptive features. In E. C. Chang & L. J. Sanna (Eds.),
Virtue, vice, and personality: The complexity of behavior (pp.
145–161). Washington, DC: American Psychological
Association.
Wolfe, F., Clauw, D. J., Fitzcharles, M. A., Goldenberg, D. L., Katz,
R. S., Mease, P., et al. (2010). The American College of
Rheumatology preliminary diagnostic criteria for fibromyalgia
and measurement of symptom severity. Arthritis Care andResearch, 62, 600–610.
Wolfe, F., Smythe, H. A., Yunus, M. B., Bennet, R. M., Bombardier,
C., Goldenberg, D. L., et al. (1990). The American College of
Rheumatology 1990 criteria for the classification of fibromyal-
gia. Report of the Multicenter Criteria Committee. Arthritis andRheumatism, 33, 160–172.
J Clin Psychol Med Settings
123


















