Neuropsychiatric Symptoms Clinical Decision Education ...
42
Neuropsychiatric Symptoms Clinical Decision Education Series: The Treatment and Management of Neuropsychiatric Symptoms in Skilled Nursing Centers Elizabeth J. Santos, MD, MPH, DFAPA, DFAAGP Associate Professor of Psychiatry, Neurology & Medicine Clinical Chief, Division of Geriatric Mental Health & Memory Care University of Rochester School of Medicine & Dentistry Kaylee Mehlman, PharmD, RPh, BCGP, FASCP Clinical Consultant Pharmacist Geramed Senior Care Consulting Moderator: Chad Worz, PharmD, BCGP Chief Executive Officer, ASCP
Transcript of Neuropsychiatric Symptoms Clinical Decision Education ...

Neuropsychiatric Symptoms Clinical Decision Education Series:The Treatment and Management of Neuropsychiatric Symptoms in
Skilled Nursing Centers
Elizabeth J. Santos, MD, MPH, DFAPA, DFAAGP
Associate Professor of Psychiatry, Neurology & Medicine
Clinical Chief, Division of Geriatric Mental Health & Memory Care
University of Rochester School of Medicine & Dentistry
Kaylee Mehlman, PharmD, RPh, BCGP, FASCP
Clinical Consultant Pharmacist
Geramed Senior Care Consulting
Moderator: Chad Worz, PharmD, BCGP
Chief Executive Officer, ASCP

Thank you!
Series Sponsor Session Partner

Meet The Speaker
Elizabeth J. Santos, MD, MPH is an Associate Professor of Psychiatry, Neurology and Medicine at the University of Rochester School of Medicine and Dentistry. Dr. Santos is the Clinical Chief of the Division of Geriatric Mental Health & Memory Care. She does nursing home consultation and is the Director or Medical Director of a number of programs including the UR Geriatric Telepsychiatry, UR Memory Care, Older Adult Services, and Project ECHO – GeMH OMH.

Meet The Speaker
Kaylee (Adams) Mehlman is a Board-Certified Geriatric Pharmacist and Fellow of ASCP with experience in Long Term Care since 2009 and an ASCP member since 2012. Currently, she is an Independent Consultant Pharmacist and owner of Geramed Senior Care Consulting and Corporate Clinical Consultant for Psych360 in Northeast Ohio.

Disclosures
• No financial relationships
• No conflicts of interest
• No promotion of commercial products or services

Follow Up: Helpful MDS Sections for CPh
• Section N:• Psychotropics received in the last 7 days
• Antipsychotic (AP) GDR history and physician documentation of CI
• Section V:• Delirium
• Cognitive loss dementia (BIMS)
• Psychosocial well-being – activities, person centered care
• Mood state (PHQ9)
• Behavioral symptoms
• Pain

Limitations of MDS Data
• BIMS (Brief interview for Mental Status) is a “snapshot” • SLUMS, MoCA, MMSE more accurate for cognitive impairment
• It has to be documented for it have happened• Ex: behaviors not charted because viewed as “baseline behavior”
Current Models
• Primary driven GDR intervals (rare) with Pharmacist oversight
• Pharmacist driven GDR intervals – addressed by Primary (no Psych involvement)
• Pharmacist driven GDR intervals – addressed by Psych• CPh to then ensure documentation of CI appropriate
• Pharmacist and Psych GDR collaboration via remote monitoring
• Pharmacist and Psych GDR collaboration as part of IDT
• Psych driven GDR intervals with Pharmacist oversight

Challenges with Current Models when No Psych
• Having primary providers address GDR recommendations – period
• If providers are not forthcoming with CI rationale, the burden can fall on the CPh and nursing staff• Do not assume the documentation in the EHR “speaks for itself”
• Psychotropics often used to target behaviors versus psychiatric conditions

Using Existing Documentation for GDR Rationale
Use to bolster documentation for – or – against GDR within recommendations. Examples:
• Newly prescribed AP?• Evaluate delirium assessments (section C)
• Ensure diagnosis is part of cumulative list (section I)
• Check for documentation of hallucinations/delusions (section E)
• Depression• Use PHQ9 score
This same documentation can be used to monitor effectiveness of psychotropic
medications

Pain and Non-pharm
• Assess pain management regardless of cognitive function• Ensure proper pain scales are used for cognitively impaired patients
• Some patients may be resistant to admit pain
• Just one aspect of considering the patient “as a whole” when treating psychiatric conditions• Always work with the interdisciplinary team for non-pharm interventions and
care planning
Other Ways to Approach Management
of Neuropsychiatric Symptomsin Skilled Nursing Facilities

Disclosures
I have no relevant financial relationships to disclose.
Salary support from the University of Rochester, NYS OMH, NIJ and HRSA.
Thanks to the UR Telepsychiatry Team for slides I have adapted.
Special thanks to:
Drs. Adam Simning & Michael Hasselberg
Senior Health Project Coordinator Mrs. Lara Press-Ellingham

Workforce Shortage▪ Only 1,596 physicians are currently
certified in geriatric psychiatry
▪ One for every 11,372 older Americans
▪ By 2030 that total is predicted to rise to only 1,659, which would then be only
one for every 20,195 older Americans (ADGAP, 2007b).
▪ Half of fellowship positions go unfilled nationwide
▪ General psychiatry is a partial solution
▪ 71% feel very prepared to dx and
treat delirium
▪ 56% to diagnose and treat
dementia.
Source: Retooling for an Aging America: Building the Health Care Workforce http://www.nap.edu/catalog/12089.htm

Overuse of Psychotropics

624 Nursing Homes
• 30% of new admissions are
among persons with mental
illness
• 50% of all residents have
cognitive impairment
• Three-fold increased risk of
hospitalization
Grabowski, et. al., 2009.; Becker, et. al., 2009; The Long Term Care Community Coalition, 2014; NYSDOH, 2017
Growing Need

• Telementoring: Project ECHO® in Geriatric Mental Health (GeMH)
• Telepsychiatry
• Psychiatric Nurse Engagement Specialist
University of Rochester Solution
Multi-level Service Approach

19
Telementoring
ECHO® HUB
University of RochesterTeam of Specialists
ECHO® SPOKE
Community-basedFront-line Clinicians
PATIENT REACH
“One to Many”

20
How Project ECHO® Works▪ Use Technology (multipoint
videoconferencing and Internet)
▪ Disease Management Model focused on reducing variation in processes of care and sharing “best practices”
▪ Case based learning through three main routes:
1. Learning Loops
2. Knowledge Networks3. Content Knowledge
Arora (2013); Supported by N.M. Dept. of Health, Agency for Health Research and Quality HIT Grant 1 UC1 HS015135-04, New Mexico Legislature, and the Robert Wood Johnson Foundation.

21
Knowledge Networks

Project ECHO® GeMH for LTC

Project ECHO® GeMHGeriatric Mental Health (GEMH -LTC) in Long Term Care (12/3/2015–11/30/2019)
• 163 TeleECHO™ clinics • 5,643 total attendees
• 1756 CME credits awarded
Office of Mental Health (GEMH -OMH) (6/27/2017 – 11/30/2019)
• 55 TeleECHO™ clinics
• 2,589 total attendees
• 603 CME credits awarded

Triaging Through Project ECHO®
• Serves as a mechanism to identify residents that
might need immediate behavioral health treatment
• Used to allocate need for higher level of care
o Telepsychiatry
o Psychiatric nurse engagement specialist
o Emergency room / hospitalization
• Educates nursing homes on how to prioritize certain
patient case presentations by level of risk severity

TelepsychiatrySkilled Nursing Facilities
Staffed by:
• Geriatric Psychiatrists
• Psychiatric Nurse Practitioners
• Geropsychologists
Service is available:
Monday – Friday
830am – 5:00pm
Excluding University Holidays

Psychiatric Nurse Engagement Specialist• Provide on-site visits for training and support to nursing home treatment
teams
oCare plan development for patients with challenging behaviors
oDevelop crisis management/intervention training
oParticipate in unit rounds and case reviews
• Assists in implementing a behavior management interdisciplinary team approach to care, including medication reconciliation and reduction
• Develops Crisis Intervention Strategies
• Helps treatment team identifying appropriate case referrals for Project ECHO® GeMH and Telepsychiatry

Model Implementation in Finger Lakes Region
May 9, 2017 through October 23, 2020
38 Skilled Nursing Facilities engaged
4,925 Telepsychiatry Consults Completed
• Reasons for referralo 38% Behavior
o 31% Medication
676 Nurse Engagement visits (onsite and virtual)
• 2,228 Behavioral Care Plans created and/or reviewed
• 1,037 Residents on antipsychotics reviewed
• 269 Residents scoring 10+ on the PHQ9 reviewed
• 65 on-site Telepsych consult supports provided

28
April 3, 2019 through December 5, 2019
22 Skilled Nursing Facilities engaged
(up to 38 more to be added)
291 Telepsychiatry Referrals
•Reasons for referral:
o38% Behavior
o34% Medication
Model Expansion with OMH

SNFs Served Across NYS

TELEPSYCHIATRY CONSULTS
0
500
1000
1500
2000
2500
3000
2017 2018 2019 2020 2021
291
1115
1362
2687
544
Total
As of 3/10/2021


Common Hospital Psychiatric Consult
85 yo male admitted with failure to thrive keeps getting out of bed, yelling, and resisting care.
• What did we often do as general psychiatrists? Start quetiapine or low-dose risperidone.
• This is a problem though because, once this patient is stabilized, SNFs may be reluctant to accept him.

Why the antipsychotic pushback in SNFs?
• Star ratings
• Small effect sizes with significant safety concerns (cerebrovascular events, metabolic effects, extrapyramidal symptoms, death)
• None FDA approved for dementia with behaviors
• Only three non-penalized uses of antipsychotics in NHs: Schizophrenia/Schizoaffective Disorders, Tourette Syndrome, Huntington’s Disease
** This has resulted in dementia residents being newly diagnosed with schizophrenia. **

• 15% of all NH long-stay residents receive antipsychotics
• Antipsychotics prescribing varies considerably across NHs – even by psych consultant groups (26.4% vs 12.2%)!
• Older adults admitted to NHs heavily utilizing antipsychotics have increased mortality
• NH behavioral health services in short supply – NH providers not trained to use antipsychotics.
Why the antipsychotic pushback in SNFs?

UR Medication Management ApproachTelepsychiatry Nurse
Engagement Specialist
This is rare – only 2-3x in 18 months (e.g.,
ECT, refusing medications and
medical conditions worsened)
Use antipsychotics for psychosis.


0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
12/31/16 3/31/17 6/30/17 9/30/2017 12/31/2017 3/31/18 06/30/18 09/30/18 12/30/18 03/31/19 6/30/2019
Antipsychotic Use in the SNFs (12/2016 to 6/2019)
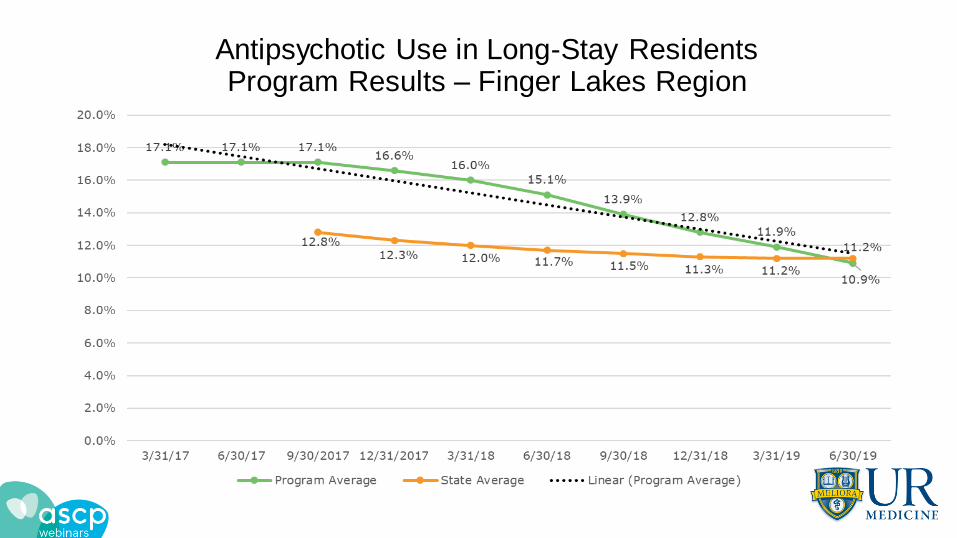
Antipsychotic Use in Long-Stay ResidentsProgram Results – Finger Lakes Region

One SNFs Success Story!Antipsychotic Use in Long-Stay Residents

Recognition of Our Work

Roundtable Discussion