Neurointerventional Therapy for Brain Aneurysms and Acute Stroke
59
2014 UPDATE Neurointerventional therapy for brain aneurysms and acute stroke at Abbott Northwestern Hospital Yasha Kadkhodayan, MD Interventional Neuroradiology Abbott Northwestern Hospital Consulting Radiologists Ltd Minneapolis, MN
-
Upload
allina-health -
Category
Health & Medicine
-
view
234 -
download
0
Transcript of Neurointerventional Therapy for Brain Aneurysms and Acute Stroke

2014 UPDATE
Neurointerventional therapy forbrain aneurysms and acute strokeat Abbott Northwestern Hospital
Yasha Kadkhodayan, MD
Interventional Neuroradiology
Abbott Northwestern Hospital
Consulting Radiologists Ltd
Minneapolis, MN

Disclosures
• Consultant for Covidien
• Site investigator for– Penumbra 3D Separator Trial for Acute Ischemic Stroke
– Study of the Penumbra Coil 400 System to Treat Aneurysms (ACE), Sponsor: Penumbra Inc.
– Pivotal Study of the FRED Stent System in the Treatment of Intracranial Aneurysms, Sponsor: Microvention-Terumo Inc.

Interventional Neuroradiology at ANW


International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling
in 2,143 patients with ruptured intracranial aneurysms:a randomised trial
Dr. Andrew Molyneux, International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group
The Lancet, Volume 360, Issue 9342, Pages 1267 -1274, 26 October 2002


ISAT Death at 7 years

ISAT Rebleeding at 7 years


Clipping vs coiling for4,899 unruptured brain aneurysms in USA

Management of a ruptured brain aneurysm
• Securing the aneurysm to prevent re-bleeding
• EVD for hydrocephalus
• ICU care for blood pressure control, vasospasm, salt wasting…
• Endovascular treatment of vasospasm

49 y/o man with confusion, blurry vision,crawling around in North Dakota oil fields

NCCT at St. Joseph’s HospitalDickinson, ND
523 miles
OneCall Transfer Center arrangesconference call between referring
ED physician, neurointerventionalist& neurointensivist at Abbott
Patient air-lifted to Abbott
(612) 863-1000

Upon arrival, stuporous, withdrawing to painful stimuli
EVD placed emergently by neurosurgeon on call

Basilar tip aneurysm
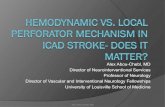
Balloon-assisted coiling

Balloon-assisted coiling

POD #10New right arm drift
Marked increased in left MCA velocity123 256 cm/s

CTA

Balloon angioplasty

Before and after

Transferred from ICU on POD #11
Home to Illinois on POD #17

MRA at 6 months

Endovascular treatment of aneurysms at Abbott Northwestern

6(1%)
30(5%)
86(14%)
86(14%)
89(15%)
76(12%)
49(8%)
52(9%)
33(5%)
27(4%)
21(3%)
21(3%)
13(2%)
24(4%)
0
10
20
30
40
50
60
70
80
90
<2 2 3 4 5 6 7 8 9 10 11 12 13 >13
Nu
mb
er
of
An
eu
rysm
s
Maximum Aneurysm Dimension (mm)Rounded to the closest whole number
Ruptured Cerebral Aneurysms Treated Endovascularly (n=613)
373
Aneurysms
<7mm
(61%)
134
Aneurysms
7-9mm
(22%)
106
Aneurysms
≥10mm
(17%)

Ruptured brain aneurysms at Abbott
• 149 patients treated endovascularly from 1/1/09 to 6/30/13– 97% of ruptured aneurysms treated at Abbott
• 70% women, 30% men
• Mean age: 56 years (20 – 91 years)
• Mean aneurysm size: 7 mm (1.4 – 27 mm)
• Mean distance traveled from presenting ED to Abbott for transfers: 136 miles (7 – 525 miles)

Other interventions performed
• Emergent external ventricular drainage: 54%
• Endovascular vasospasm treatment: 21%
• Decompressive craniectomy: 5%
• Ventriculoperitoneal shunt: 20%

• Mean ICU LOS: 13.8 days (1 – 39 days)
• Mean hospital LOS: 18.6 days (1 – 39 days)
• Discharge disposition– Home: 50%
– Rehabilitation facility: 29%
– Skilled nursing facility: 12%
– Expired: 9%
• 3 patients lost to follow-up (2%)
• Mean time to last follow-up among survivors: 19.5 months (0.8 – 55.1 months)
Disposition

All Patients Hunt-Hess 1-2 Hunt-Hess 3 Hunt-Hess 4 Hunt-Hess 5
146(100%)
61 (42%)
43 (29%)
29 (20%)
13 (9%)
mRS 0-2:103
(71%)56
(92%)28
(65%)14
(48%)5
(38%)
mRS 3:15
(10%)2
(3%)6
(14%)3
(10%)4
(31%)
mRS 4-5:7
(5%)0 2
(5%)4
(14%)1
(8%)
mRS 6:21
(14%)3
(5%)7
(16%)8
(28%)3
(23%)
Clinical outcomes

Acute stroke intervention in 2014
In light of NEJM trials published last year
46 y/o woman with atrial fibrillation on Pradaxa,remarkable recovery from previous left MCA stroke in 2011,now with sudden onset right-sided weakness and aphasia
NIHSS 14

LKW at midnight
OSH 0400 at ANW

CTA, ASPECTS 6-7

Puncture at 0620

Solitaire in place

TICI 2b, 7 hours from LKW

Next day

Clinical follow-up
• NIHSS 2 at 48 hours
• mRS 2 at 30 days
• Minimal right pronator drift, slurs some words
• Going back to work next month

IMS 3
Endovascular Therapy after Intravenous t-PA versus t-PA Alone for Stroke
Joseph P. Broderick, M.D., Yuko Y. Palesch, Ph.D., Andrew M. Demchuk, M.D., Sharon D. Yeatts, Ph.D., Pooja Khatri, M.D., Michael D. Hill, M.D., Edward C. Jauch, M.D., Tudor G. Jovin, M.D., Bernard Yan, M.D., Frank L. Silver, M.D., Rüdiger von Kummer, M.D., Carlos A. Molina, M.D., Bart M. Demaerschalk, M.D., Ronald Budzik, M.D., Wayne M. Clark, M.D., Osama O. Zaidat, M.D., Tim W. Malisch, M.D., Mayank Goyal, M.D., Wouter J. Schonewille, M.D., Mikael Mazighi, M.D., Ph.D., Stefan T. Engelter, M.D., Craig Anderson, M.D., Ph.D., Judith Spilker, R.N., B.S.N., Janice Carrozzella, R.N., B.A., R.T.(R.), Karla J. Ryckborst, R.N., B.N., L. Scott Janis, Ph.D., Renée H. Martin, Ph.D., Lydia D. Foster, M.S., Thomas A. Tomsick, M.D., for the Interventional Management of Stroke (IMS) III Investigators
N Engl J MedVolume 368(10):893-903March 7, 2013

Acute stroke, ages 18 to 82NIHSS ≥10, IV-tPA eligible
Randomized 2 to 1 in favor of intervention
1/3 received onlystandard dose IV-tPA
2/3 receivedIV-tPA
Standard dose
Plus angiography and endovascular treatment
Low dose
IMS 3: Trial design

mRS distribution
mRS 0-2: 42.7% in endovascular armmRS 0-2: 40.2% in IV-tPA alone arm

Safety endpoints

Limitations
• Only 10% of patients were treated with current technology
• Only 1/3 of all patients had confirmed LVO
• Nearly 1/5 of patients in the interventional arm had no treatable occlusion
• Intervention occurred 1 hour after IV-tPA
• TICI 2b or 3 achieved in only 44% of patients with an M1 occlusion, similar or lower rate for other sites
IMS 3 reflects obsolete technology and does not reflect current clinical practice

Demchuk A, IMS III: Comparison of outcomes between IV and IV/IA treatment in baseline CTA confirmed ICA, M1, M2 and
basilar occlusions. Presented at ISC 2013. Honolulu, HI
Outcomes with confirmed occlusion
0-2: 47.2%
0-2: 38.5%
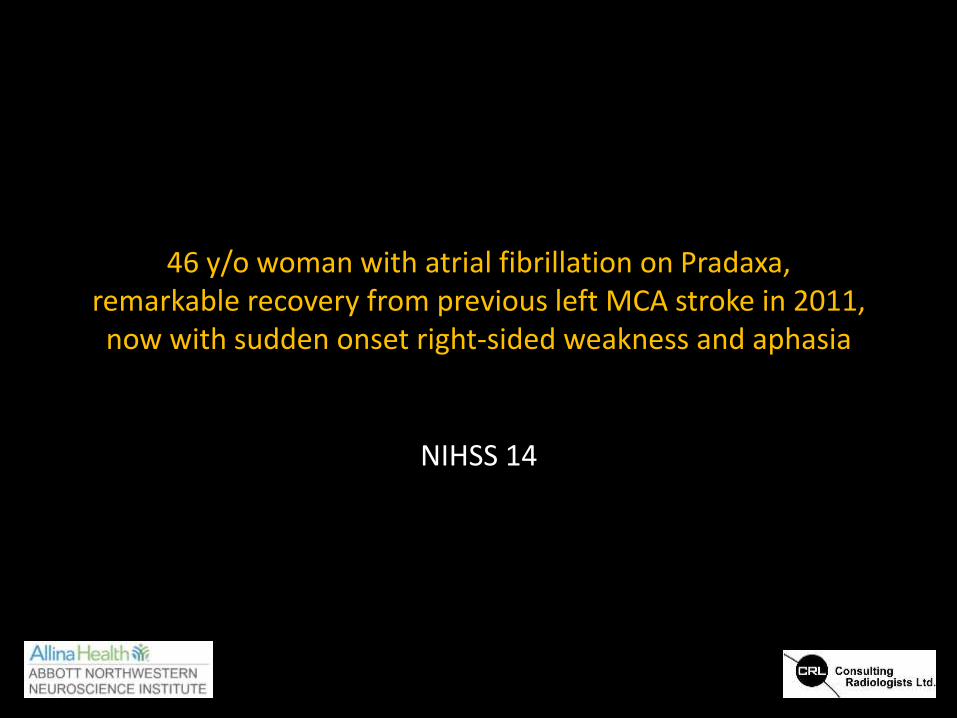
Time is brain
Each 30 minutes = 10% loss!

Optimizing delivery of stroke care
• Comprehensive care requires a complete neurovascular team available 24/7/365– Vascular Neurologist
– Neurointerventionalist
– Neurointensivist
– Neurosurgeon

ANW stroke network
• 33 regional sites
• 15 sites with tele-health
• 15 sites with imaging link
• Mean distance to Abbott
– 76 miles (13 to 150 miles)

Initial focus
• Prompt IV-tPA (≤ 60 min) to ALL eligible patients– 4.5 hrs from LKW
– No intracranial hemorrhage
– Blood glucose ≥ 60 mg/dL
– INR < 1.7 (only required if on anticoagulation)
– No recent surgery or stroke (relative)

ANW door to needle(as of March 2014)
0
10
20
30
40
50
60
70
80
90
100
2010 2011 2012 2013 2014
98
67
5855
47
76
69
53
47
37
MinutesDoor to IV tPA
Mean
Median
N= 31 N= 22 N=37 N=10N=59
American Stroke AssociationBenchmark: < 60 minutes
ANW 2014 Goal: < 40 minutes

Small subset go to angiography suite

Optimizing stroke care
6 hours mRS 0-2: 46%mRS 6: 23%
4.5 hoursmRS 0-2: 67%mRS 6: 17%
Standardizedalgorithm
implemented

– July 1st 2011 to March 31st, 2014
85 mechanical thrombectomies
– 51% women, 49% men
– Mean age: 67 years (33 - 90 years)
– Mean admission NIHSS: 15.4 (3 - 27)
– History of atrial fibrillation: 38%
– Mean distance from presenting ED to Abbott for transfers: 56 miles (13 - 314 miles)
– Successful recanalization (TICI 2b/3): 85%
– Mean time from onset to reperfusion: 5 hours 40 minutes
ANW thrombectomy experience

ANW Mechanical ThrombectomyAnterior Circulation Strokes
Administer IV-tPA when appropriate
NIHSS ≥8 or global aphasia
Contact ANW Stroke Neurologist via OneCallNIR calculates NCCT ASPECTS
ASPECTS ≥5
Not optimal candidate for
thrombectomy, may consider on an individual basis
Age < 70LKW ≤ 6 hrs
No
Yes
Age < 70LKW > 6 hours
or unknown
Age ≥ 70
Transfer for emergent
thrombectomy
Obtain emergent CTA head / neck(on-site if possible)
NIR calculates CTA ASPECTSCTA ASPECTS
≥5
CTA ASPECTS <5

• Discharge disposition– Home: 26%
– Rehabilitation facility: 40%
– Skilled nursing facility: 13%
– Expired/hospice: 21%
Disposition

All patientsTICI 0-2a
(15%)TICI 2b/3
(85%)p-value
mRS 0-2 46% 8% 53% 0.003
mRS 3 11% 15% 10% 0.6
mRS 4-6 43% 77% 37% 0.008
7x
2x
Clinical outcomes

Conclusions
• Requires coordinated team effort
• New devices have led to– Decreased procedure times
– Higher rates of recanalization
– Fewer complications
• Recanalization a requisite but not guarantee of good outcome
• Integrating systems of care and standardizing patient selection to decrease time from onset to recanalization imperative to maximize good outcomes

• Randomized trials
– THERAPY: IA tx + IV-tPA vs IV-tPA alone for acute ischemic stroke
– Penumbra 3D Separator device for acute ischemic stroke
– HEAT: Hydrogel vs bare platinum coils
• MHI-partnered trials
– RECOVER-STROKE: IA stem cell infusion for acute ischemic stroke
• Registries
– ACE: Penumbra coil registry
– GEL-THE-NEC: Hydrogel coil registry
– ASPIRE: Pipeline device registry
– INTREPED: Pipeline device registry
– NAISR: Intracranial stent registry
• Humanitarian use devices
– Neuroform intracranial stent
– Onyx HD-500 liquid embolic
– NeuroFlo perfusion augmentation for cerebral vasospasm
– Wingspan intracranial stent
• Investigational devices
– FRED: Flow-diversion device PMA
– LVIS & LVIS Jr: Intracranial stent PMA
• Investigator-initiated research
– SPASM: Advanced MRI for patients with ruptured brain aneurysms
• funded by the ANW Foundation
NeuroIR clinical trials at ANW

Continuous improvement
• A model that– Values centers of excellence
– Concentrates high volume of tertiary care
– Practices evidence-based medicine
– Monitors outcomes in robust and rigorous manner
– Advances the field through clinical research

Neurointervention
Benjamin Crandall, DO
Josser Delgado, MD
Jill Scholz, CNP
Anna Blem, CNP
Jennifer Fease, BS
Kira Tran, BS
Sandee Verootis
NeurosurgeryGregg Dyste, MDKyle Uittenbogaard, MDRobert Roach, MDHart Garner, MDMahmood Nagib, MDMichael McCue, MD
Vascular Neurology
Mark Young, MD
Ronald Tarrel, DO
Richard Shronts, MD
David Dorn, MD
Adam Todd, MD
Ruth Anderson, CNP
Karen Gozel, CNP
Timothy Hehr, MSN
Holly Carroll, MSN
Neuro Critical Care
Kelley Lockhart, MD
Lisa Kirkland, MD
Roman Melamed, MD
Ramiro Saavedra, MD
Clara Zamorano, MD
Omer Sultan, MD
Alyssa Maizan, CNP
Ken Johnson, CNP
Acknowledgements
Abbott One Call Transfer Center612-863-1000
Interventional Neuroradiology612-863-4808


















