Neuroimmune Axes of the Blood–Brain Barriers and Blood–Brain...
37
1521-0081/70/2/278–314$35.00 https://doi.org/10.1124/pr.117.014647 PHARMACOLOGICAL REVIEWS Pharmacol Rev 70:278–314, April 2018 Copyright © 2018 by The Author(s) This is an open access article distributed under the CC BY-NC Attribution 4.0 International license. ASSOCIATE EDITOR: ROBERT DANTZER Neuroimmune Axes of the Blood–Brain Barriers and Blood–Brain Interfaces: Bases for Physiological Regulation, Disease States, and Pharmacological Interventions Michelle A. Erickson and William A. Banks Geriatric Research and Education and Clinical Center, Veterans Affairs Puget Sound Health Care System, Seattle, Washington; and Division of Gerontology and Geriatric Medicine, Department of Medicine, University of Washington, Seattle, Washington Abstract..................................................................................... 279 I. Introduction ................................................................................. 280 A. The Blood–Brain Barrier and Immune Privilege ......................................... 280 B. Working Definitions of Brain Barriers and Interfaces .................................... 280 C. Historical Work: Defining the Brain Barriers ............................................ 280 II. Features and Functions of the Blood–Brain Barrier and Blood–Brain Interface ............... 281 A. Specialized Features That Confer Barrier Functions ..................................... 281 1. Tight Junctions ...................................................................... 281 2. Reduced Macropinocytosis ............................................................ 282 3. Efflux Transporters .................................................................. 282 4. Metabolic Enzymes .................................................................. 282 B. Specialized Features That Confer Interface Functions .................................... 282 1. Transcellular Diffusion ............................................................... 282 2. Blood–Brain Barrier Transport via Solute Carriers ................................... 283 3. Blood–Brain Barrier Transport via Receptor-Mediated Transcytosis ................... 283 4. Blood–Brain Barrier Transport via Adsorptive Transcytosis ........................... 283 C. From Brain Barriers to Brain Interfaces: Components of the Neurovascular Unit ......... 284 1. Endothelial Cells..................................................................... 284 2. Brain Pericytes ...................................................................... 284 3. Astrocytes ........................................................................... 285 4. Neurons ............................................................................. 286 5. Microglia and Perivascular Macrophages ............................................. 286 6. Mast Cells ........................................................................... 286 7. Extracellular Matrix ................................................................. 286 8. Glycocalyx ........................................................................... 287 D. Arms of the Blood–Brain Barrier and Their Neuroimmune Functions..................... 287 1. The Vascular Blood–Brain Barrier ................................................... 287 2. The Blood–Cerebrospinal Fluid Barrier ............................................... 287 3. Tanycytic/Ependymal Barriers of Circumventricular Organs .......................... 288 III. The Neuroimmune Axes ..................................................................... 289 A. Axis 1: Blood–Brain Barrier Disruption .................................................. 289 1. Disruption of Paracellular Tight Junctions............................................ 290 2. Transcytotic Vesicular Pathways ..................................................... 290 3. Endothelial Cell Damage and Hemorrhage ........................................... 291 B. Axis 2: Modulation of Barrier and Interface Functions by Immune Substances ............ 291 Address correspondence to: Dr. William A. Banks, Veterans Affairs Puget Sound Health Care System, Room 810A/Building 1, 1660 S. Columbian Way, Seattle, WA 98108. E-mail: [email protected] This work was supported by the Department of Veterans Affairs and the National Institutes of Health National Institute on Aging [Grant R01 AG046619]. https://doi.org/10.1124/pr.117.014647. 278 by guest on October 30, 2020 Downloaded from
Transcript of Neuroimmune Axes of the Blood–Brain Barriers and Blood–Brain...
-
1521-0081/70/2/278–314$35.00 https://doi.org/10.1124/pr.117.014647PHARMACOLOGICAL REVIEWS Pharmacol Rev 70:278–314, April 2018Copyright © 2018 by The Author(s)This is an open access article distributed under the CC BY-NC Attribution 4.0 International license.
ASSOCIATE EDITOR: ROBERT DANTZER
Neuroimmune Axes of the Blood–Brain Barriers andBlood–Brain Interfaces: Bases for PhysiologicalRegulation, Disease States, and Pharmacological
InterventionsMichelle A. Erickson and William A. Banks
Geriatric Research and Education and Clinical Center, Veterans Affairs Puget Sound Health Care System, Seattle, Washington; andDivision of Gerontology and Geriatric Medicine, Department of Medicine, University of Washington, Seattle, Washington
Abstract. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 279I. Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 280
A. The Blood–Brain Barrier and Immune Privilege . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 280B. Working Definitions of Brain Barriers and Interfaces . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 280C. Historical Work: Defining the Brain Barriers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 280
II. Features and Functions of the Blood–Brain Barrier and Blood–Brain Interface . . . . . . . . . . . . . . . 281A. Specialized Features That Confer Barrier Functions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 281
1. Tight Junctions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2812. Reduced Macropinocytosis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2823. Efflux Transporters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2824. Metabolic Enzymes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 282
B. Specialized Features That Confer Interface Functions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2821. Transcellular Diffusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2822. Blood–Brain Barrier Transport via Solute Carriers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2833. Blood–Brain Barrier Transport via Receptor-Mediated Transcytosis . . . . . . . . . . . . . . . . . . . 2834. Blood–Brain Barrier Transport via Adsorptive Transcytosis . . . . . . . . . . . . . . . . . . . . . . . . . . . 283
C. From Brain Barriers to Brain Interfaces: Components of the Neurovascular Unit . . . . . . . . . 2841. Endothelial Cells. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2842. Brain Pericytes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2843. Astrocytes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2854. Neurons . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2865. Microglia and Perivascular Macrophages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2866. Mast Cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2867. Extracellular Matrix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2868. Glycocalyx . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 287
D. Arms of the Blood–Brain Barrier and Their Neuroimmune Functions. . . . . . . . . . . . . . . . . . . . . 2871. The Vascular Blood–Brain Barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2872. The Blood–Cerebrospinal Fluid Barrier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2873. Tanycytic/Ependymal Barriers of Circumventricular Organs . . . . . . . . . . . . . . . . . . . . . . . . . . 288
III. The Neuroimmune Axes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 289A. Axis 1: Blood–Brain Barrier Disruption . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 289
1. Disruption of Paracellular Tight Junctions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2902. Transcytotic Vesicular Pathways . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2903. Endothelial Cell Damage and Hemorrhage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 291
B. Axis 2: Modulation of Barrier and Interface Functions by Immune Substances. . . . . . . . . . . . 291
Address correspondence to: Dr. William A. Banks, Veterans Affairs Puget Sound Health Care System, Room 810A/Building 1, 1660 S.Columbian Way, Seattle, WA 98108. E-mail: [email protected]
This work was supported by the Department of Veterans Affairs and the National Institutes of Health National Institute on Aging [GrantR01 AG046619].
https://doi.org/10.1124/pr.117.014647.
278
by guest on October 30, 2020
Dow
nloaded from
https://doi.org/10.1124/pr.117.014647http://creativecommons.org/licenses/byc/4.0/mailto:[email protected]://doi.org/10.1124/pr.117.014647
-
C. Axis 3: Transport, Penetration, and Uptake of Neuroimmune-Related Substances. . . . . . . . . 292D. Axis 4: Immune Cell Trafficking between Blood and Brain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 294E. Axis 5: Immune Secretions of the Barrier Cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 296
IV. Physiologic Conditions, Disease States, and Pharmacologic Agents . . . . . . . . . . . . . . . . . . . . . . . . . . . 297A. Sickness Behavior . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 297B. Perinatal Brain Ischemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 297C. Multiple Sclerosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 298D. Human Immunodeficiency Virus-1 Penetration of the Blood–Brain Barrier and
Consequences of Human Immunodeficiency Virus-1 Infection on Blood–Brain BarrierFunction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 299
E. Amyloid b Peptide and Alzheimer Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 300F. Neuromyelitis Optica . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 301G. Euthyroid Sick Syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 301H. Chemobrain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 301I. Inflammation, ATP-Binding Cassette Transporters, and Central Nervous System Drug
Delivery. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 302J. Emergence of Progressive Multifocal Leukoencephalopathy Associated with Therapies
That Inhibit T-Cell Immune Surveillance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 303K. IL-1ra, Febrile Infection-Related Epilepsy Syndrome, and Neonatal-Onset Multisys-
tem Inflammatory Disease. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 303L. Immunomodulatory Therapies and Stroke . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304M. Methamphetamine and Blood–Brain Barrier Alterations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304N. Cerebral Cavernous Malformations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304O. Antibody-Associated Autoimmune Encephalitis Syndromes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304
V. Conclusions and Future Directions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 305Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 306References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 306
Abstract——Central nervous system (CNS) barriers pre-dominantly mediate the immune-privileged status of thebrain, and are also important regulators of neuroimmunecommunication. It is increasingly appreciated thatcommunication between the brain and immune systemcontributes to physiologic processes, adaptive responses,and disease states. In this review, we discuss the highlyspecialized features of brain barriers that regulateneuroimmune communication in health and disease. Insection I, we discuss the concept of immune privilege,provideworkingdefinitionsofbrainbarriers, andoutlinethehistoricalwork that contributed to theunderstandingofCNS barrier functions. In section II, we discuss the uniqueanatomic, cellular, and molecular characteristics of the
vascular blood–brain barrier (BBB), blood–cerebrospinalfluid barrier, and tanycytic barriers that confer theirfunctions as neuroimmune interfaces. In section III, weconsider BBB-mediated neuroimmune functions andinteractions categorized as five neuroimmune axes:disruption, responses to immune stimuli, uptake andtransport of immunoactive substances, immune celltrafficking, and secretions of immunoactive substances.In section IV, we discuss neuroimmune functions ofCNS barriers in physiologic and disease states, as wellas pharmacological interventions for CNS diseases.Throughout this review, we highlight many recent advancesthat have contributed to the modern understanding ofCNS barriers and their interface functions.
ABBREVIATIONS: Ab, amyloid b; ABC, ATP-binding cassette; AD, Alzheimer disease; AJ, adherens junction; ART, anti-retroviral therapy; BALT,bronchus-associated lymphoid tissue; BBB, blood–brain barrier; BCRP, breast cancer resistance protein; BCSFB, blood–CSF barrier; BEC, brainendothelial cell; BUI, brain uptake index; CCL, C-C motif chemokine ligand; CICD, chemotherapy-induced cognitive dysfunction; CMB, cerebralmicrobleed; CNS, central nervous system; COX, cyclooxygenase; CP, choroid plexus; CPE, choroid plexus epithelium; CSF, cerebrospinal fluid; CVO,circumventricular organ; DHA, docosahexaenoic acid; DOX, doxorubicin; EAE, experimental autoimmune encephalomyelitis; ECM, extracellular matrix;FIRES, febrile infection-related epilepsy syndrome; GRP78, glucose-regulated protein 78; HAART, highly active antiretroviral therapy; HAND, HIV-associated neurologic disorder; HIV, human immunodeficiency virus; HIVE, HIV encephalitis; IDT, indicator diffusion technique; IFN, interferon; IL,interleukin; IL-1R1, type 1 IL-1 receptor; ISF, interstitial fluid; JAM, junctional adhesionmolecule; LPC, lysophosphatidylcholine; LPS, lipopolysaccharide;LRP, low-density lipoprotein receptor-related protein; LTP, long-term potentiation; ME, median eminence; MFSD2A, major facilitator superfamilydomain-containing 2A; MMP, matrix metalloproteinase; MRP, multidrug resistance protein; MS, multiple sclerosis; NF-kB, nuclear factor kB; NLR,nucleotide-binding oligomerization domain-like receptor; NMO, neuromyelitis optica; NNRTI, non-NRTI; NOD, nucleotide-binding oligomerizationdomain; NRTI, nucleoside reverse transcriptase inhibitor; NVU, neurovascular unit; OVLT, organum vasculosum of the lamina terminalis; PDGF-B,platelet-derived growth factor subunit B; PDGFRb, platelet-derived growth factor receptor b; Pgp, P-glycoprotein; Plvap, plasmalemma vesicle-associatedprotein; PML, progressive multifocal leukoencephalopathy; RAGE, receptor for advanced glycation endproducts; RMT, receptor-mediated transcytosis; T3,triiodothyronine; TEER, transendothelial electrical resistance; TGF, transforming growth factor; TJ, tight junction; TNF, tumor necrosis factor; TSH,thyroid-stimulating hormone; VCAM, vascular cell adhesion molecule; VEGF, vascular endothelial growth factor; ZO, zonula occulins.
BBB and Neuroimmune Axes 279
-
I. Introduction
A. The Blood–Brain Barrier and Immune Privilege
The central nervous system (CNS) has traditionallybeen viewed as an immune-privileged area in that it isprotected against the immune events of the periphery.This immune privilege was once considered absolutewith its violation only occurring in disease states,resulting in dire consequences for the CNS. Currentappreciation is that the immune privilege is real, butrelative. Both past and current thinking ascribes thisimmune privilege to the BBB. By its ability to prevent(past thinking) or to control and modulate (currentthinking) the impact of peripheral immune events onthe CNS, the BBB acts to protect the brain fromperipheral immune events. However, whereas thebarrier aspects of the BBB induce immune privilege, it isalso the BBB that makes such protection relative. TheBBBmakes immune privilege relative by possessing waysin which it controls the interplay of CNS and peripheralimmune events. Such interplay relies on the transfer ofimmune elements (substances or cells) between the CNSand blood; such a transfer can be termed a neuroimmuneaxis. Five neuroimmune axes can be currently identifiedthat involve the BBB and a sixth that does not but ismediated by afferent and efferent nerve activities (Goehleret al., 1999; Romeo et al., 2001; Kelley et al., 2003; Kenneyand Ganta, 2014; Kanashiro et al., 2016). The fivepathways involving the BBB are as follows: 1) BBBdisruption; 2)modulation of barrier and interface functions(other than BBB integrity) by immune substances; 3)transport, penetration, and uptake of neuroimmune-related substances; 4) immune cell trafficking betweenblood and brain; and 5) immune secretions of the barriercells. Most likely, these axes work together rather thanindependently, and it is one of the great promises of thefield, as well as one of its greatest challenges, that it willelucidate the mechanisms of neuroimmune integrationthat underlie such diverse phenomena as sleep, responsesto sepsis, mindfulness, and depression. Below, we considereach of the five axes involving the BBB.This review will first consider the concepts, compo-
nents, functions, and interactions that form the basis ofthe BBB field that are germane to neuroimmunology,then discuss how the BBBdefines and participates in thefive known neuroimmune axes, and finally discuss howthe BBB in general and how these axes in particular areinvolved in CNS diseases, drug delivery, and therapy.
B. Working Definitions of Brain Barriersand Interfaces
BBB is a term that refers to one function of a highlyspecialized cellular interface between the blood and theCNS parenchyma. The barrier function of this interfaceprevents unregulated diffusion of circulating sub-stances into the brain, which is critical for maintaininga CNS milieu that supports neuronal function and
survival. Generally, the BBB refers to the vascularbarrier where capillary endothelial cells are the in-terface between the blood and brain parenchyma.Specialized vascular CNS barriers that have distinctfeatures from brain parenchymal vessels include theblood–retinal barrier, the blood–nerve barrier, theblood–labyrinth barriers, and the blood–spinal cordbarrier (Neuwelt et al., 2008). Other cellular barriers/interfaces such as the choroid plexus epithelial cells ofthe blood–cerebrospinal fluid (CSF) barrier (BCSFB)and tanycytes that are located along the ventricularboundaries of circumventricular organs (CVOs) may beconsidered arms of the BBB as well because they alsoprevent unregulated leakage of blood components intothe CSF and adjacent brain interstitial fluid (ISF)(Ghersi-Egea et al., 1996). Furthermore, these inter-faces have many nonbarrier functions that are essentialin supporting CNS homeostasis. The nonbarrier func-tions include regulating the transport of circulatingsubstances into the brain, removing potentially harmfulsubstances from the brain, secreting molecules thatsignal to cells in the brain parenchyma, and respondingto stimuli that arise within both the brain and bloodcompartments. In the remainder of this section, we willprovide an overview of the historical work that definedthe barrier functions of brain interfaces, discussaspects of their barrier and interface functions thatcontribute to CNS homeostasis, and relate eachblood–brain interface to one another with regard totheir unique structures and functions in neuroim-mune communication.
C. Historical Work: Defining the Brain Barriers
Evidence in support of a BBB dates back to workspublished in the late 19th/early 20th century. At thetime, the field of medicinal chemistry was in its infancy,and Paul Ehrlich, who would later make many seminalcontributions to the field (Bosch and Rosich, 2008), wasinvestigating the selectivity of dyes for different cellsand tissues. As part of this work, Ehrlich (1885) notedthat certain water-soluble dyes that were parenterallyinjected into animals stained peripheral tissues and thechoroid plexus, but did not stain the brain or spinal cordparenchyma. Ehrlich (1906) posited that the reducedCNS staining was due to a low affinity of the dyes forCNS tissue. However, other groups who were investi-gating bile acids (Biedl and Kraus, 1898) and sodiumferrocyanide (Lewandowski, 1900) found that the toxic-ities of these substances were much more potent whenintroduced directly into the cerebrospinal fluid versussystemically. Both groups interpreted their findings tomean that brain capillaries had unique properties thatblocked the transfer of certain molecules from blood tobrain. Goldmann (1909, 1913) later conducted criticalexperiments showing that Ehrlich’s trypan blue dye,which did not bind CNS tissue when injected parenter-ally, did stain CNS tissue when injected into the CSF.
280 Erickson and Banks
-
This finding demonstrated that exclusion of trypan bluefrom the CNS was not due to reduced binding affinity toCNS tissue, which had been suggested by Ehrlich(1906). However, Goldmann (1913) supposed in thiswork that the choroid plexus was the predominantbarrier site of the CNS, supplying nutrients to theCNS in a fashion analogous to the placenta. The termBBB (barrière hémato-encéphalique) was first used in apublication by Stern andGautier (1921); althoughmanyattribute the first use of this term (Blut-Hirnschranke)to Lewandowski, this term was not used in his originalpublication (Saunders et al., 2014).Following these early studies, controversy sur-
rounded the true nature of the BBB. Early ultrastruc-tural studies of the brain using electron microscopyused methods of tissue preservation that led to thebelief that the CNS had essentially no extracellularspace (Bradbury, 2000). Therefore, some adopted thebelief that the limited CNS penetration of aqueoussolutes was due to tightly packed neuronal and glialmembranes and a lack of aqueous medium for diffusion(Davson and Spaziani, 1959; Bradbury, 2000). However,it was then demonstrated that extracellular markersinjected in ventricular CSF did penetrate the brain andspinal cord, and therefore, CNS tissue contained extra-cellular fluid permissive to solute diffusion (Davson andSegal, 1969). Based on these findings, it was positedthat a BBB to such solutes injected in blood must exist(Davson et al., 1961). Later that decade, Vanharreveldet al. (1965) showed that the brain extracellular spacecould be visualized by electron microscopy when mod-ified techniques were used for tissue preservation. Thisreport was followed by the eminent findings of Reeseand Karnovsky (1967), who used electron microscopy toexplore the subcellular features of brain capillaries.They found that the brain’s limited uptake of peroxi-dase, which had been shown previously (Straus, 1958),could be attributed to two specialized features of thebrain endothelium: uniquely impermeant tight junc-tions (TJs) that were present at contacts betweencapillary membranes, and markedly reduced endothe-lial vesicles (Reese and Karnovsky, 1967). In a laterstudy, Brightman and Reese (1969) explored the distri-bution of peroxidase injected into CSF of mice, chickens,and goldfish to determine which cell types of the CNSexpressed peroxidase-impermeant TJs. Although per-oxidase did diffuse through gap junctions that werepresent at contacts of astrocytic endfeet, it did notpermeate the junctions between brain endothelial cells(BECs) or choroid plexus ependymal cells. This workhighlighted that TJs were a unique feature of BECs, aswell as epithelial cells of the choroid plexus thatconferred barrier properties (Brightman and Reese,1969). The tight barriers of the brain vasculature werefurther exemplified by Crone and Olesen (1982) and byButt et al. (1990), who showed that brain vessels haveexceptionally low ion permeabilities due to very high
transendothelial electrical resistance (TEER), averagingover 1000 V/cm2 in frog and mammalian pial vessels. Aspial vessels lack astrocytes, TEER is estimated to bemuch higher in brain parenchymal vessels that areensheathed by astrocyte endfeet, which contribute tothe BBB phenotype (Abbott et al., 2006). By determiningthe CNS permeability/surface area coefficients for K, Na,and Cl in vivo, Smith and Rapoport (1986) estimatedTEER of the parenchymal vessels to be approximately8000 V/cm2, which compares to that of a cell membrane.
II. Features and Functions of the Blood–BrainBarrier and Blood–Brain Interface
A. Specialized Features That ConferBarrier Functions
Barrier functions are largely thought of as thoserelated to the exclusion of blood-borne substances fromthe brain. Such exclusion is critical to the CNS being animmune-privileged tissue. The specialized features thatunderlie those functions include TJs, mechanisms thatlimit macropinocytosis, efflux mechanisms, and enzy-matic activities.
1. Tight Junctions. TJs are macromolecular com-plexes that prevent the paracellular diffusion of solutesacross brain barriers. They communicate with adherensjunctions (AJs), which are another junctional complexthat contributes to the tightness of the barrier (Wolburgand Lippoldt, 2002). AJs are located at the basalmembrane and are comprised of cadherins, whichassociate with each other in the extracellular space,and catenins, which link the cadherins to the cytoskel-eton (Huber et al., 2001). TJ proteins at the vascularBBB include occludin, claudins, junctional adhesionmolecules (JAMs), zonula occludens (ZO), and cytoplas-mic accessory proteins such as cingulin (Hawkins andDavis, 2005). Occludins, claudins, and JAMs aremembrane-spanning proteins that heterotypically in-teract in the intercellular space between adjacentcapillary membranes. ZOs and cingulin are adaptorproteins that link TJ membrane proteins to the cyto-skeleton and contribute to junction stability (Abbottet al., 2010). TJ stability is regulated by calcium,phosphorylation, cyclic AMP, and G proteins (Huberet al., 2001), and decreases in TJ expression as well asTJ mislocalization and post-translational modificationscan cause increases in paracellular permeability ofsolutes across the BBB (Deli et al., 2005). Importantly,TJs are not only a diffusion barrier for transcellularpassage of circulating substances into the CNS, but alsofor the lateral diffusion of membrane proteins (Abbottet al., 2010). Therefore, TJs also contribute to themembrane polarity of BECs. Later in this review, wewill compare TJ organization in the different arms ofthe BBB as well as the contributions of TJs to theneuroimmune axes of the BBB.
BBB and Neuroimmune Axes 281
-
2. Reduced Macropinocytosis. Reese and Karnovsky(1967) were the first to note that BECs had relativelylow numbers of vesicles compared with endothelial cellsin the periphery. In contrast, epithelial cells of thechoroid plexus do have vesicles that largely reside attheir apical membranes (Johanson et al., 2011). Recentwork has begun to identify the molecular mechanismsthat suppress brain endothelial pinocytic vesicle forma-tion. In a study that aimed to characterize gestationaldevelopment of the BBB, Ben-Zvi et al. (2014) foundthat the BBB tightening that occurred around E15.5 inmice was associated with upregulation of major facili-tator superfamily domain-containing 2A (MFSD2A) inBECs. In the same study, it was shown that MFSD2Aknockout mice had a leaky BBB, although the morphol-ogy of the brain vasculature and TJs did not appear tobe affected. Instead, MFSD2A knockout mice had in-creased luminal, abluminal, and cytoplasmic vesicles intheir BECs, which facilitated the fluid-phase uptake ofsolutes such as peroxidase and dextrans, which areusually excluded from the CNS. In a parallel study, itwas realized thatMFSD2A knockoutmice had cognitiveand behavioral symptoms that resembled omega-3fatty-acid deficiency (Nguyen et al., 2014). Using alipidomics approach, this group revealed that docosa-hexaenoic acid (DHA), an omega-3 fatty acid that isimportant for CNS development and cognition, wasreduced in the CNS of mice lacking MFSD2A. Theyfurther demonstrated that MFSD2A was a transporterfor lysophosphatidylcholine (LPC)-DHA, as well asLPC-oleate and LPC-palmitate at slightly lower capac-ities (Nguyen et al., 2014). Andreone et al. (2017) thenshowed that the DHA-transporting function ofMFSD2A also facilitated DHA enrichment of BECmembranes, which inhibited caveolin-1–induced forma-tion of vesicles. In mice lacking MFSD2A, caveolin-1knockout inhibited the increased formation of brainendothelial vesicles as well as leakage of the BBB(Andreone et al., 2017). Therefore, BECs acquire aspecialized lipid composition during embryonic devel-opment that inhibits caveolae-mediated fluid-phasetranscytosis.3. Efflux Transporters. Efflux transporters at brain
barriers facilitate the passage of substances in thebrain-to-blood or CSF-to-blood direction. A subset ofefflux transporters, namely members of the ATP-binding cassette (ABC) protein family, confers barrierfunctions by limiting the brain uptake of endogenousmacromolecules and xenobiotics. ABC transporter sub-types, their localization, and functions in the CNS havebeen extensively reviewed elsewhere (Hartz and Bauer,2011). Some of the most studied ABC transporters atthe BBB include P-glycoprotein (Pgp/ABCB1), multi-drug resistance protein (MRPs/ABCC), and breastcancer resistance protein (BCRP/ABCG2) (Qosa et al.,2015). ABC transporters have a broad substrate spec-trum, including some phospholipids, sphingolipids,
aldosterone, and amyloid b (Ab) for Pgp; glutathione,glutathione-conjugated leukotrienes and prostaglandins,and glucoronidation and sulfation products for MRP-1;and bile acids and estrones for BCRP (Qosa et al., 2015).ABC transporters also efflux a broad range of xenobioticsubstrates, including opioids, antibiotics, antiretroviraldrugs, chemotherapeutics, and others (Qosa et al., 2015).The expression and function of efflux transporters at theBBB are dynamically regulated, for example, at thetranscriptional level by nuclear receptors (Chan et al.,2013), and at post-translational levels by vascular endo-thelial growth factor (VEGF) (Hawkins et al., 2010).Aspects of ABC transporter modulation regardingimmune-regulated functions are discussed in greaterdetail later in this review.
4. Metabolic Enzymes. The BBB is also an enzy-matic barrier, and expresses phase I and phase IIenzymes that contribute to the metabolism and elimi-nation of biomolecules and drugs from the body. BECscontain monoamine oxidase and catechol-O-methyltransferase, which metabolize adrenaline, nor-adrenaline, and dopamine, as well as 4-aminobutyrateaminotransferase, which metabolizes GABA (Lasbenneset al., 1983; Spatz et al., 1986). Therefore, enzymaticbarriers inhibit the transport of many neurotransmit-ters in the blood-to-brain and brain-to-blood directions.Furthermore, the toxicity of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine when systemically administered isinversely associated with monoamine oxidase expres-sion in BECs (Kalaria et al., 1987; Riachi and Harik,1988). The cytochrome P450 enzyme CYP1B1 isexpressed in human BECs (Dauchy et al., 2008;Shawahna et al., 2011), and its expression can beregulated by environmental toxicants such as2,3,7,8-tetrachlorodibenzo-p-dioxin through the arylhydrocarbon receptor (Jacob et al., 2015). GlutathioneS-transferases are also expressed in human braincapillaries (Shawahna et al., 2011).
B. Specialized Features That ConferInterface Functions
Brain barriers do much more than divide the CNSfrom the peripheral circulation. They are also critical inCNS homeostasis, nutrition, and brain–body communi-cation. These features are essential to the existence ofsome of the neuroimmune axes. Features that aid inthese functions include transcellular diffusion andtransport via solute carriers, receptor-mediated trans-cytosis, and adsorptive endocytosis.
1. Transcellular Diffusion. Early work by Davsondemonstrated that lipid solubility and size determinedpartitioning of substances from blood into CSF andbrain tissue (Davson, 1955; Davson and Smith, 1957). Itis now appreciated that small, lipophilic molecules cancross the BBB by passive transmembrane diffusion.Passive transmembrane diffusion is a nonsaturablemechanism by which most drugs that can enter the
282 Erickson and Banks
-
CNSdo so. The degree to which lipid-soluble compoundsmay cross the BBB is often determined by theirpartitioning into aqueous versus nonpolar medium,such as water and octanol (Oldendorf, 1974; Levin,1980). However, as substances that passively diffuseacross the BBB must traverse the luminal membrane,cytosol, and then the abluminal membrane prior toreaching the CNS, there is a limit to the lipophilicity of asubstance that favors diffusion across the BBB versussequestration within the cell membrane (Banks, 2016).Transcellular diffusion of substances across the BBB isalso affected when the test substance is an effluxtransporter substrate. In this case, CNS uptake is muchlower than what would be predicted based on size andlipophilicity.2. Blood–Brain Barrier Transport via Solute
Carriers. Solute carrier proteins are integral mem-brane proteins that permit the directional or facilitateddiffusion of aqueous molecules across cell membranes.The initial studies that identified carrier-mediatedtransporters at the BBB investigated nutritional sub-strates of the brain. D-glucose was the first substancedemonstrated to have a saturable transport system(Crone, 1965). In this study, Crone used an indicatordiffusion technique (IDT) to quantify first-pass uptakeof glucose by the brain. The IDT involves coinjecting aradioactive test substance and a capillary-impermeanttracer (e.g., Evan’s blue albumin), which estimates thedilution of the injected substance in blood. The sub-stances are injected into the carotid artery, and thenvenous blood from the superior sagittal sinus is imme-diately sampled to determine the percent loss of injectedsubstance. Crone used the IDT to assess the brainuptake of D-glucose during hypo- and hyperglycemicstates, and found that CNS uptake of the glucose tracerwas highest when blood glucose was low, and lowestwhen blood glucose was high, indicating that glucoseused a saturable transport system (Crone, 1965). Sub-sequently, Oldendorf (1971) used a different techniqueto assess the brain uptake of glucose and amino acids.The method, called the brain uptake index (BUI), iscarried out by coinjecting a highly brain-penetrantradioactive standard along with a radioactive test sub-stance into the carotid artery, and then immediatelyremoving and counting brain tissue for uptake of thetest substance with reference to the standard. The BUIis therefore also a first-pass measurement of brainuptake. In support of the findings by Crone (1965),Oldendorf’s BUI method also demonstrated saturabletransport of glucose, as well as amino acids. Impor-tantly, Oldendorf (1971) also conducted cross-inhibitionstudies and found that amino acids with similar chem-ical properties often used a common transporter. It isnow understood that there are three broad classes ofamino acid transporters with many subtypes in eachclass (Hawkins et al., 2006; Abbott et al., 2010). Glucosetransport across the BBB is mediated by GLUT1 (Dick
et al., 1984; Pardridge et al., 1990; Boado and Par-dridge, 1994), andGLUT1 expression is considered to bea hallmark of BBB endothelial cells (Cornford et al.,1993, 1994), as its expression is absent from endothelialcells within brain regions that lack an endothelial BBB(Rahner-Welsch et al., 1995). In addition to glucose andamino acids, solute carriers transport nucleosides, ions,prostaglandins, and many other small polar molecules(Bito et al., 1976; Abbott et al., 2010). Therefore, onefunction of solute carriers is to provide the brain withthe essential circulating substrates for energy genera-tion, protein and nucleic acid synthesis, and mainte-nance of pH and electrolytes. At the choroid plexusepithelium, solute carriers are necessary for the pro-duction of CSF from plasma ultrafiltrate (Johansonet al., 2011). Solute carrier proteins may be present onthe luminal and/or abluminal membrane of brainendothelial and epithelial barrier cells, and the di-rectionality of their transport may be in the blood-to-brain or brain-to-blood direction, depending on theirorientation within the membrane (Abbott et al., 2010).
3. Blood–Brain Barrier Transport via Receptor-Mediated Transcytosis. Another mechanism of trans-port across the BBB is receptor-mediated transcytosis(RMT), which is thought to be the predominant mode oftransport of larger macromolecules such as peptidesand proteins across the BBB (Bickel et al., 2001). RMTis energy dependent, saturable, and depends on vesic-ular pathways. RMT may be in the blood-to-braindirection, or brain-to-blood direction. For ligands tocompletely cross the BBB via RMT, they must first bindtheir transporter at either the luminal or abluminalendothelial membrane. Second, they must be internal-ized in a vesicle, which may be clathrin or cavaeolaedependent (Georgieva et al., 2014). Third, they must berouted from the luminal to abluminal membrane orvice versa, which may involve subcellular traffickingthrough organelles such as endosomes, or the Golgi(Bickel et al., 2001). Furthermore, ligands must escapevesicular routing to and degradation by the lysosome.Ligands may become dissociated from their receptorsduring subcellular routing, due to the slightly acidic pHof the endosome (Bickel et al., 2001). Fourth, the ligandmust be exocytosed to the opposite side of the mem-brane and released into brain interstitial fluid (Bickelet al., 2001). This final step also requires the dissocia-tion of the ligand from its transporter. RMT at the BBBcan be regulated at the level of transporter expression,localization, and conformation, as well as by concentra-tions of other molecules that might compete with theligand for transport, or that may sequester the ligandfrom interacting with its transporter at the BBB.
4. Blood–Brain Barrier Transport via AdsorptiveTranscytosis. Adsorptive endocytosis is a receptor-independent mode of vesicular transport across theBBB and involves interactions of cationic proteinresidues with the anionic glycocalyx, which lines the
BBB and Neuroimmune Axes 283
-
lumial surface of endothelial cells, or membrane glyco-proteins (Broadwell et al., 1988; Villegas and Broad-well, 1993). Conferring a positive charge to proteins thattypically do not cross the BBB, such as albumin (Griffinand Giffels, 1982; Kumagai et al., 1987), enhances theiruptake by BECs by adsorptive mechanisms. Adsorptiveendocytosis may be saturable (Kumagai et al., 1987),but may also be induced by compounds such as wheatgerm agglutinin and the human immunodeficiencyvirus (HIV) coat proteins TAT and gp120 (Mann andFrankel, 1991; Banks et al., 1998a). Adsorptive endo-cytosis increases in vitro following lipopolysaccharide(LPS) or cytokine treatment (Schenk and de Vries,2016).
C. From Brain Barriers to Brain Interfaces:Components of the Neurovascular Unit
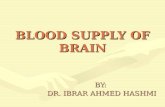
Brain barriers are uniquely poised to communicatesignals between the CNS and peripheral compart-ments. Communication is not only achieved throughtransporters, but also frommolecules that are producedand secreted by cells of the brain interfaces. Thesesecreted substances can engage autocrine targets,and/or signal to other cells of the neurovascular unit(NVU), and distal cells in the brain and periphery. BBBsecretions may be constitutive or inducible, and are alsopolarized in that they may be released into either bloodor brain compartments (Banks, 2016). Finally, cells ofthe BBB respond to signals that arise from the CNS orblood compartments, which may stimulate alterationsin their barrier, transport, and secretory functions(Verma et al., 2006; Krasnow et al., 2017). How theseinterface functions contribute to the neuroimmunomo-dulatory activities of brain barriers will be discussed insection II of this review. First, we consider the individ-ual components and their functions (Fig. 1).1. Endothelial Cells. In addition to their barrier,
transport, and interface functions, BECs contribute tothe specialized phenotypes of other cells of the NVU.Endothelial cells induce astrocyte differentiation invitro via leukemia-inhibitory factor production (Miet al., 2001). They influence the localization of the waterchannel aquaporin 4 on the plasma membrane ofastrocyte endfeet and stimulate the upregulation ofantioxidant enzymes within astrocytes (Abbott, 2002).Endothelial cells secrete factors such as transforminggrowth factor (TGF)-b and platelet-derived growthfactor subunit B (PDGF-B) and signal through Tie2and sphingosine-1 phosphate, which maintain pericytefunctions (Armulik et al., 2005). Neuroimmune func-tions of BECs are discussed extensively in latersections.2. Brain Pericytes. Pericytes have important func-
tions in the development and maintenance of thevascular BBB. Of the cells of the NVU, pericytes arethe most closely apposed to capillary endothelial cells;they share a basement membrane and make direct
contact with BECs via peg and socket as well as gapjunctions (Dore-Duffy and Cleary, 2011). Brain peri-cytes are derived from the mesoderm and neuroecto-derm (Winkler et al., 2011) and undergo proliferativeexpansion and recruitment to the developing neuro-vasculature during embryonic development and theearly postnatal period (Daneman et al., 2010). Pericyteattachment to BECs during embryonic developmentfacilitates BBB tightening by downregulating genesthat are associated with pinocytic vesicle formationand immune cell recruitment (Daneman et al., 2010;Ben-Zvi et al., 2014). PDGF-B produced by braincapillaries signals to platelet-derived growth factorreceptor b (PDGFRb) on brain pericytes and regulatespericyte proliferation, attachment to endothelial cells,and survival. The absence of PDGF-B or PDGFRb islethal in mice (Leveen et al., 1994; Kaminski et al.,2001), whereas mice with partial PDGF-B or PDGFRbdeficiency survive into adulthood, but have reductionsin capillary-associated pericytes (Armulik et al., 2010;Bell et al., 2010; Daneman et al., 2010). Pericytedeficiency induced by a PDGF-B mutation results inleakage of intravascular markers of different sizes intothe CNS, indicative of BBB disruption. Astrocyteassociations with capillaries were also altered in thismodel; however, TJ protein expression and localizationwere relatively unaffected (Armulik et al., 2010). Micelacking one copy of PDGFRb have an age-dependentloss in pericytes of about 20% by 1 month of age, and60% by 14–16months (Bell et al., 2010). BBB disruptionis evident by 1 month and worsens with age. In thismodel, synaptic deficits and impaired learning and
Fig. 1. The neurovascular unit. The BBB is in contact and communicateswith other cells of the CNS as well as circulating immune cells andperipheral tissues through the endocrine-like secretions of the latter.Differences occur in NVU function regionally as well as among theanatomic areas in which barrier cells are located. As an example of thelatter, immune cell trafficking occurs largely at the postcapillary venule.Endothelial cells, astrocyes, pericytes, neurons, and macrophages/micro-glia, as well as the extracellular matrix and glycocalyx are part of theNVU. There is renewed interest in mast cell functions, and the cellulisincompertus represents cell types yet to be discovered that participate inthe NVU. Not drawn to scale.
284 Erickson and Banks
-
memory are evident by 6–8 months, but precede neuro-inflammation, which does not significantly increaseuntil 14–16 months of age. Pericytes are also importantfor the induction of the BBB phenotype in vitro, aspericyte coculture with BECs increases the integrity ofthe barrier (Nakagawa et al., 2007).Pericytes also have dynamic functions in the NVU.
Pericytes are multipotent stem cells that can differen-tiate into cells of neural lineage (Dore-Duffy et al.,2006). Theymay also adopt a contractile phenotype thatcontributes to the regulation of cerebral blood flow (Hallet al., 2014). Pericytes contribute to the neuroimmuneresponse and are potent modulators of BBB functiondue to their proximity to endothelial cells. Pericytessecrete cytokines and chemokines constitutively inculture and upregulate cytokine and nitric oxide pro-duction in response to LPS (Fabry et al., 1993; Kovacet al., 2011). They present antigen in response tointerferon (IFN)-g, which may contribute to T-cellactivation (Balabanov et al., 1999). They also enhancethe transcytosis of HIV-1 free virus and neutrophilsacross in vitro BEC monolayers in the presence of animmune stimulus (Dohgu and Banks, 2013; Pieperet al., 2013). In response to injuries that are associatedwith neuroinflammation such as hypoxia (Gonul et al.,2002) and traumatic brain injury (Dore-Duffy et al.,2000), pericytes dissociate from the brain vasculatureand migrate away from the vessels within 1–2 hoursfollowing the insult (Dore-Duffy et al., 2000; Gonulet al., 2002). In contrast, a systemic inflammatory insultsuch as intraperitoneal LPS results in pericyte de-tachment from thebasal lamina between6and24hours,which coincides with reactive microgliosis and BBBdisruption (Nishioku et al., 2009). Pericytes that leavethe basement membrane and enter brain parenchymahave been reported to adopt a phenotype similar to thatof infiltrating macrophages (Guillemin and Brew,2004). In summary, pericytes may contribute to theneuroimmune response as follows: 1) causing a leakyBBB, either by secreting endothelial-disrupting factors,or by physical disassociation; 2) facilitating the trans-port of immune cells and pathogens into the brain; and3) propagating neuroinflammation by stimulating bothresident and recruited immune cells.3. Astrocytes. Astrocytes are the most abundant
brain cell type and regulate a number of physiologicprocesses in the CNS that include neurotransmission,synaptic plasticity, functional hyperemia, and convec-tive flow of brain interstitial fluid (Sofroniew andVinters, 2010). Astrocytes are also integral in theinduction and maintenance of the mature BBB pheno-type (Abbott et al., 2006). Their endfeet surround braincapillaries, arterioles, and venules. At capillaries, theastrocytic endfeet are located on the CNS side of thebasement membrane that ensheaths the endothelialcells and pericytes (Abbott et al., 2006). These endfeetare in close proximity to the endothelial cells (Thal,
2009) and therefore positioned for crosstalk that pro-motes the phenotypic specialization of both cell types.The contribution of astrocytes to BBB formation duringembryonic development is thought to be negligible inrodents, as astrocytes appear immediately after birthand do not begin to ensheath brain vessels until the firstpostnatal week (Daneman et al., 2010). In contrast,radial glia, which are precursors for neurons andastrocytes, do form endfeet around capillaries in fetalbaboons and humans (Bass et al., 1992; Bertossi et al.,1999). Therefore, theremay be species differences in thecontribution of astrocytes or their precursors to theembryonic BBB. Astrocytes do contribute to BBBfunctions during postnatal development and through-out adulthood. In vitro, astrocytes strengthen thebarrier properties of BECs and also enhance expressionof BBB transporters, such as Pgp and Glut1, andenzymes of the metabolic barrier (Abbott et al., 2006).The close proximity of astrocytes and endothelial cellsat capillaries likely favors BBB tightening, as in vitrostudies have demonstrated that in vitro BEC barriersare tightest when astrocytic processes contact theendothelial monolayer (Abbott, 2002). However, se-creted factors from astrocytes also contribute to theBBB phenotype. BECs likewise contribute to the orga-nization of aquaporin 4 and potassium channels onastrocytic endfeet (Abbott, 2002), which regulate waterand ion exchange in the CNS (Stokum et al., 2015).Therefore, communication between endothelial cellsand astrocytes is important for both the barrier andinterface functions of BECs.
Astrocytes are immune-active cells and were the firstcell type in the CNS shown to express class II majorhistocompatibility complex upon IFN-g stimulationin vitro (Wong et al., 1984). More recent work hasreviewed aspects of astrocyte responses to systemicinflammation; additionally, CNS injury in the contextof novel subsets of reactive astrocytes and their func-tions are beginning to be characterized (Liddelow andBarres, 2017). In response to systemic inflammatoryinsults such as sepsis, astrocytes upregulate their pro-duction of proinflammatory cytokines and chemokines,as well as VEGF (Bellaver et al., 2017). Inflammatorylesions and interleukin (IL)-1b can induce astrocyteproduction of VEGF-A and thymidine phosphorylase,which downregulate TJ protein expression in BECs(Chapouly et al., 2015). Astrocytes also upregulatecytokines and chemokines in response to proinflamma-tory stimuli and in disease states (Dong andBenveniste,2001; Norden et al., 2016). Astrocytic inflammatoryresponses are differently regulated in comparison withthose of microglia; for example, astrogliosis followinginduction of systemic inflammation is inhibited byindomethacin, whereas microgliosis is not (Bankset al., 2015). Furthermore, in response to a systemicinflammatory insult, astrocytes adopt a delayed proin-flammatory phenotype in comparison with that of
BBB and Neuroimmune Axes 285
-
microglia (Norden et al., 2016). Astrocytes may alsofunction in the resolution of neuroinflammation, as theycan downregulate microglial activation by secretingTGF-b (Vincent et al., 1997).4. Neurons. The brain is extensively vascularized—
the mean distance of a neuronal cell body to a capillaryis approximately 15 mm in mice (Tsai et al., 2009) and30 mM in nonhuman primates (Mabuchi et al., 2005).Therefore, each neuron receives and can regulate itsown blood supply from an adjacent capillary. Neuronsregulate their blood supply through communicationwith astrocytes, which facilitate dilation of arteriolesin response to neuronal glutamate release (Zonta et al.,2003). Some studies suggest that capillary pericytescontribute to functional hyperemia; however, the rela-tive contribution of pericytes versus mural cells ofarterioles to neurovascular coupling has been disputed(Fernandez-Klett et al., 2010; Winkler et al., 2011;Fernandez-Klett and Priller, 2015). Neuronal activityalso contributes to the NVU architecture by promotingneurovascular density and branching during adulthood(Lacoste et al., 2014), but, during neonatal develop-ment, excessive sensorimotor stimulation and repeti-tive neural activation result in reduced microvasculardensity (Whiteus et al., 2014).Neurons exhibit pleiotropic responses to inflamma-
tory stimuli. Cytokines such as tumor necrosis factor(TNF)-a, via its interaction with astrocytes, and frac-talkine, which is expressed by neurons and activates themicroglia fractalkine receptor, can both stimulate syn-aptic activity (Prieto and Cotman, 2017). Furthermore,cytokines such as IL-1b, IL-6, and IL-18 are upregu-lated in the brain following long-term potentiation(LTP) induction in awake rats (del Rey et al., 2013).IL-1b at physiologic concentrations promotes LTP, butat higher concentrations can inhibit LTP and impairlearning and memory (Ross et al., 2003; Prieto et al.,2015). This function of IL-1b may be potentiated withaging (Prieto et al., 2015). TNF-a is not required forlearning andmemory, but its overexpression by glia canimpair memory and synaptic plasticity (Donzis andTronson, 2014).5. Microglia and Perivascular Macrophages.
Microglia are resident macrophages of the CNS andrapidly respond to CNS insults. Their lineage is uniquefrom recruited brain macrophages, in that microgliaderive from the yolk sac during development, whereasrecruited brain macrophages derive from bone marrow(Alliot et al., 1999). During development, microgliaassociate with the brain vasculature and contribute toangiogenesis (Arnold and Betsholtz, 2013). In adultbrains, microglia remain closely associated with theneurovasculature. Their production of proinflammatorymediators such as cytokines, chemokines, nitric oxide,prostaglandins, matrix proteases, and reactive oxygenspecies can have profound effects on cells of the NVUand BBB integrity (da Fonseca et al., 2014). There are
also populations of brainmacrophages that reside in theperivascular space and are thought to derive from bonemarrow (Hickey and Kimura, 1988), although morerecent works suggest that their recruitment to the brainunder physiologic conditions is rare (Prinz et al., 2011).The perivascular macrophages are thought to protectthe brain during infection (Polfliet et al., 2001) andprevent deposition of protein aggregates such as Abpeptide within the perivascular space (Lai andMcLaurin, 2012). However, perivascular macrophagesmay also contribute to neurovascular pathologies asso-ciated with increases in Ab peptide levels in the brain(Park et al., 2017). An important protective function ofmicroglia is their ability to rapidly migrate to sites ofbrain injury and alter their morphology to form aspecialized phagocytic network that prevents diffusionof harmful substances into the brain parenchyma (Rothet al., 2014). Microglia also contribute to the resolutionof inflammation in the brain after injury (Cherry et al.,2014).
6. Mast Cells. Mast cells are granulocytes thatoriginate from bone marrow and circulate as precursorcells. Upon recruitment to tissues, mast cells completetheir differentiation according to their local environ-ment (Silver and Curley, 2013). Mast cells can berecruited to the CNS (Silverman et al., 2000; Nautiyalet al., 2011), where they reside in perivascular spaces ofsome brain regions, as well as in the choroid plexus andmeninges (Silver and Curley, 2013). Mast cells areimportant mediators of peripheral IgE-mediated aller-gic responses; however, they also have emerging func-tions in the CNS. Granules of mast cells containbioactive mediators that include histamine, serotonin,serine proteases, and heparin. Mast cells can alsosynthesize prostaglandins, cytokines, growth factorssuch as nerve growth factor, reactive oxygen species,and substance P in response to stimuli (Silver andCurley, 2013). Therefore, mast cells likely play impor-tant roles in regulating neurotransmission as well asBBB function. Induction of mast cell degranulationcauses BBB disruption that is localized to brain regionsenriched in mast cells, such as the medial habenula indoves (Zhuang et al., 1996). Mast cells are thought tocontribute to CNS dysfunction in conditions such asstress (Theoharides et al., 1995), postoperative cogni-tive dysfunction (Zhang et al., 2016), and rodent modelsof multiple sclerosis (Costanza et al., 2012). However,mast cells may also regulate physiologic aspects ofbehavior, as mice that lack functional mast cells in theCNS display increased anxiety-like behaviors (Nautiyalet al., 2008). Mast cells are also a predominant source ofbrain histamine (Goldschmidt et al., 1985). Serotoninderived from mast cells has been implicated in pro-moting hippocampal neurogenesis and learning andmemory (Nautiyal et al., 2012).
7. Extracellular Matrix. Within the NVU, basementmembranes composed of extracellular matrix (ECM)
286 Erickson and Banks
-
are present between endothelial cells and pericytes,and also along the astrocytic endfeet (McConnellet al., 2017). Microvascular basement membranes arecomposed of laminins, collagen IV, fibronectin, glycos-aminoglycans including hyaluronan, chondroitinsulfate-rich proteoglycans, and glycoproteins that con-tribute to the resiliency of the microvasculature (delZoppo and Mabuchi, 2003; Lennon and Singleton, 2011;Reed et al., 2017). The ECM functions as a cellularscaffold that is generated during development, andendothelial adhesion to the matrix is mediated byintegrins (del Zoppo and Mabuchi, 2003). Integrins areunique receptors that can respond to and relay bothintracellular and extracellular signals (Shen et al.,2012). Blocking the function of b1 integrin in BECsreduces the expression of the TJ protein claudin 5 andcauses BBB disruption (Osada et al., 2011). The ECM isalso a barrier to leukocyte and erythrocyte entry intobrain parenchyma during inflammation and hemor-rhage (del Zoppo and Mabuchi, 2003; del Zoppo, 2009).Components of the ECM can be degraded by matrixmetalloproteinases (MMPs), which contribute to BBBdisruption and leukocyte trafficking during neuroin-flammation (Rosenberg, 2002). MMPs and their modu-latory effects on the BBB have recently been reviewedelsewhere (Rempe et al., 2016). Hyaluronan and itsfragments bind to Toll-like receptors, influencing theneuroimmune environment (Jiang et al., 2011).8. Glycocalyx. The glycocalyx lines the luminal
surface of endothelial cells, including those of the brain.It is a gel-like layer estimated to be approximately 5 mmthick, and is predominantly composed of heparin sulfateproteoglycan, chondroitin sulfate, hyaluronan, and gly-coproteins (Kolá�rová et al., 2014). The glycocalyx beginsto form during brain neovascularization during earlyembryonic development and matures postnatally(Vorbrodt et al., 1990). The glycocalyx has importantbarrier functions in preventing direct exposure ofplasma components to the endothelial luminal mem-brane surface (Vorbrodt, 1989), and it also functions as amechanosensor and relays signals of sheer stress to theendothelium (Tarbell, 2010). Degradation of the glyco-calyx occurs during inflammation, which is associatedwith increased passage of solutes across the endothelialbarrier, and increased leukocyte adhesion to the endo-thelium (Kolá�rová et al., 2014; Varatharaj and Galea,2017).
D. Arms of the Blood–Brain Barrier and TheirNeuroimmune Functions
The barriers formed by the components above and theresulting mechanisms by which they form neuroim-mune axes can be categorized into three main arms: thevascular BBB, the choroid plexus, and the tanycyticbarrier. The unique cellular and anatomic features ofthese barriers with reference to their neuroimmunefunctions are discussed below.
1. The Vascular Blood–Brain Barrier. The vascularBBB is a broadly applied term that most often refers tothe capillaries within the brain parenchyma. However,vascular BBBs extend to pre-and postcapillary arteri-oles and venules, respectively (Bechmann et al., 2007).Vascular BBBs are also present in the spinal cord,retina, nerves, and the inner ear, and the structural andfunctional organization of these has been reviewedelsewhere (Choi and Kim, 2008). Brain capillariesexhibit functional heterogeneity within different ana-tomic locations, as certain brain regions are morevulnerable to disruption during neuroinflammation(Banks et al., 2015), and transport rates of immunoac-tive substrates also vary depending on brain region(Moinuddin et al., 2000; Banks et al., 2001c; Ericksonet al., 2014). Therefore, the heterogeneity of the vascu-lar BBB imparts some anatomic specificity to theneuroimmune response.
In brain capillaries, the perivascular space betweenthe endothelial/pericyte basement membrane andastrocytic endfeet is small (Thal, 2009). The minimaldistance between capillary endothelial cells and thebrain parenchyma makes them ideally positioned forsecreting or transporting molecules into the CNS(Bechmann et al., 2007). In contrast, precapillaryarterioles and postcapillary venules have a laminamedia, and the basement membranes of this layer andastrocytic endfeet form a perivascular space (Thal,2009). The brain CSF/ISF flows along this perivascularspace, which facilitates the clearance of solutes from thebrain parenchyma (Iliff et al., 2012). A subset of brainmacrophages also resides in perivascular spaces(Bechmann et al., 2007), and these macrophages arepositioned to respond to antigens and endogenousimmune signals that are carried by the perivascularbulk flow of CSF, as well as those that are transportedor secreted by the endothelium. Transmigration ofleukocytes across the vascular BBB occurs at postcapil-lary venules (Owens et al., 2008). Some leukocytes thatcross the BBB reside in the perivascular space, whereasothers completely transmigrate across the glia limitansand enter brain parenchyma (Bechmann et al., 2007).
BECs actively respond to immune stimuli and are anactive interface in neuroimmune communication.Mech-anisms by which BECs contribute to neuroimmune axeswill be discussed in section II of this review.
2. The Blood–Cerebrospinal Fluid Barrier.Epithelial cells of the choroid plexus are the primarycellular components that predominantly comprise theblood–CSF barrier/interface. Tanycytes (see below) andthe arachnoid membrane also interface with the CSF,but are structurally and anatomically distinct from thechoroid plexus epithelium (CPE). The choroid plexus isa specialized structure within all four brain ventricles.Choroid plexuses extend from the ependymal lining ofthe ventricles, and consist of a single layer of cuboidalepithelial cells that reside on a basement membrane.
BBB and Neuroimmune Axes 287
-
CPE cells have microvilli and cilia on their apicalsurface, which contacts the CSF (Damkier et al.,2013). These apical projections provide a large surfacearea for secretory activity, and also have functions inregulating and sensing pH, osmolarity, and ion balancein CSF (Damkier et al., 2013). The basal and lateralmembranes of CPE cells are relatively flat, except atlateral membrane contacts near the basal end thatassume a folded labyrinth structure that is thought tocontribute to a paracellular diffusion barrier (Damkieret al., 2013). A plexus of leaky blood vessels is located onthe basal side of the CPE cells. This vascular plexus isdevoid of astrocytes, and secretions of proteins such asVEGF from the basal side of CPE cells may contribute tothe fenestrated vascular phenotype (Esser et al., 1998).Leakage of blood components into the CSF is preventedby the presence of TJs that are present in closeproximity to the apical surface of CPE cells (Johansonet al., 2011). TJ proteins expressed by CPE cells includeclaudins 1, 2, and 11. CPE TJs are thought to be moreleaky than those of the vascular BBB, and this has beenattributed to the presence of claudin-2, which can formdiffusive channels within the junction (Amasheh et al.,2009; Rosenthal et al., 2010; Johanson et al., 2011).However, the BCSFB is still relatively impermeable assmall molecules such as ascorbic acid and ions requiresolute carriers for their passage into CSF (Johansonet al., 2011).The choroid plexus is themajor site of CSF production
in the brain. Humans produce about 500–600 ml CSFper day, with approximately 80% of CSF being producedby the choroid plexus and the remainder derived frombrain ISF (Damkier et al., 2013), as there is no barrierthat prevents mixing of brain ISF with brain CSF in theadult (Ghersi-Egea et al., 1996). The CSF provides anutritive and homeostatic milieu for the brain andcirculates through the ventricular, subarachnoid, andparavascular spaces in the CNS, as well as throughbrain tissue, where it mixes with the brain ISF (Hladkyand Barrand, 2014). This flow pathway contributes tothe homeostatic milieu of the ISF and also acts as a sinkthat prevents the localized buildup of solutes in theparenchyma (Oldendorf and Davson, 1967; Johansonet al., 2011). CSF exits the brain via arachnoid granu-lations into venous sinuses and in spinal nerves, as wellas via perineural spaces that penetrate the cribriformplate (Hladky and Barrand, 2014). CSF turns over inthe human brain approximately three times per day(Damkier et al., 2013), which is governed by CSFproduction, convective forces that facilitate bulk flow,intracranial pressure, and patency of resorption sites(Pollay, 2010). CPE cells express a variety of iontransporters, solute carriers, and water channels thatcontribute to CSF production by enabling passage ofwater and solutes from the plasma ultrafiltrate acrossthe epithelium and into the ventricular space (Damkieret al., 2013). CPE cells also express efflux transporters
that inhibit the buildup of potentially harmful sub-stances in CSF. These include ABC transporters such asMRP-1 (Gazzin et al., 2008) and Pgp (Pascale et al.,2011), as well as monoamine transporters such asSLC29A4, which facilitates histamine efflux from CSFinto blood (Usui et al., 2016), and the organic cationtransporter 3, which clears creatinine from CSF(Tachikawa et al., 2008). CPE cells also express recep-tors that have been implicated in transcytosis, includ-ing low-density lipoprotein receptor-related protein-1(LRP-1), -2, (LRP-2/megalin), and the receptor foradvanced glycation endproducts (RAGE) (Zlokovicet al., 1996; Fujiyoshi et al., 2011; Pascale et al., 2011).
The choroid plexus is an immune-active tissue. It is asite of leukocyte trafficking and immune surveillance(Baruch and Schwartz, 2013; Schwartz and Baruch,2014), and CPE cells upregulate their expression ofproinflammatory cytokines, c-fos, cell adhesion mole-cules, and major histocompatibility complex antigensfollowing systemic inflammatory stimuli (Vallieres andRivest, 1997; Endo et al., 1998; Wolburg et al., 1999;Engelhardt et al., 2001; Marques and Sousa, 2015).Structural changes in CPE cells, such as swelling of theapical microvilli, increases in numbers of dark, electrondense epithelial cells, and altered mitochondria, occurduring inflammation (Engelhardt et al., 2001). Inflam-mation also impairs CSF turnover (Erickson et al.,2012b), which influences the clearance of solutes fromthe CNS.
The arachnoid epithelium comprises another compo-nent of the BCSFB. Arachnoid epithelial cells expressTJ proteins such as claudin 11 (Brochner et al., 2015)and form a size-selective diffusion barrier in vitro (Lamet al., 2012). Arachnoid epithelial cells also express highlevels of the efflux transporters Pgp and BCRP at theirapical membranes (Yasuda et al., 2013), which areexposed to plasma ultrafiltrate from the leaky vesselsof the dura matter. Therefore, the activity of thesetransporters would prevent the transport of substancesfrom blood into CSF in the subarachnoid space. BCRPexpression was also noted at the basal membrane ofarachnoid epithelial cells, suggesting that a secondfunction of BCRP is to facilitate the transport ofsubstances into CSF (Yasuda et al., 2013).
3. Tanycytic/Ependymal Barriers of Circumventric-ular Organs. The CVOs of the brain are importantinterfaces for humoral communication with the CNS.Within CVOs, the brain capillaries are leaky, lack TJproteins, and are usually fenestrated, allowing forcommunication of circulating molecules with residentneurons and glia. The CVOs are generally classified asthose having sensory functions, which are the subforn-ical organ, organum vasculosum of the lamina termi-nalis (OVLT), and area postrema, and those havingsecretory functions, which include the neurohypophy-sis, median eminence (ME), and pineal gland (Miyata,2015). The subcomissural organ is also considered a
288 Erickson and Banks
-
CVO, but its capillaries are not leaky and express TJproteins (Petrov et al., 1994; Langlet et al., 2013);however, they lack GLUT1, which is typically expressedin BBB capillaries (Rahner-Welsch et al., 1995). Thechoroid plexus (CP) is also sometimes considered aCVO, but has specialized properties in that the CPhas an epithelial barrier and is located within the brainventricles (Miyata, 2015). Neuronal and glial popula-tions within sensory CVOs can detect and respond tochanges in circulating components such as electrolytes,glucose, cytokines, and hormones. In the sensory CVOs,neuronal cell bodies and dendrites are exposed to blood-derived exudates from leaky capillaries, but projecttheir axons outside of the CVOs to brain regionsprotected by a BBB (Rodriguez et al., 2010). In contrast,secretory CVOs receive axonal projections from neuro-nal cell bodies that are located outside of the CVO.These axons release peptides into the bloodstream thatcan signal to distal organs and elicit physiologic re-sponses such as changes in blood pressure (Mimee et al.,2013). Thus, the CVOs facilitate bidirectional commu-nication between the brain and periphery and regulatevital physiologic functions that include fluid balance,metabolism, reproduction, and immune responses(Ferguson, 2014).Although serum components can freely diffuse into
and within CVOs, tanycytic barriers prevent theirdiffusion into CSF and adjacent regions of the brain.Tanycytes are specialized ependymal cells that differ-entiate from radial glial cells beginning in the last fewdays of prenatal development and continue to maturepostnatally (Edwards et al., 1990). Tanycytes aremorphologically distinct from cuboidal ependymal cellsthat line the ventricles in that they lack cilia, andinstead have long, unipolar projections that are proxi-mal to the fenestrated CVO capillaries (Rodriguez et al.,2010). Tanycyte structure and functions have been bestcharacterized in the ME (Mullier et al., 2010; Rodriguezet al., 2010), although their barrier functions appear tobe similar in other CVOs (Langlet et al., 2013). Fourtypes of ME tanycytes have been described, whichinclude a1, a2, b1, and b2. Barrier properties areascribed to the b1 and b2 tanycytes, which are locatedat the lateral extensions and floor of the infundibularrecess, respectively (Rodriguez et al., 2010). The basalprocesses of b1 tanycytes form bundles with axons thatdefine the boundary of the arcuate nucleus, which hasan intact BBB, and the ME (Rodriguez et al., 2010). TJsand AJs are present between contacts of adjacenttanycyte processes as well as the axons they surround,and the anatomic location of these b1 projectionsdefines the diffusion barrier of i.v. injected substancessuch as Evan’s blue dye between the ME and arcuatenucleus (Rodriguez et al., 2010). In contrast, the b2tanycytes express TJ proteins, including ZO-1, occludin,claudin-1, and claudin-5 (Mullier et al., 2010), at theirapical contacts between cell bodies lining the ventricle
(Rodriguez et al., 2010). These junctions form a barrierthat prevents diffusion of blood components into theCSF, and similar TJ organization of tanycytic blood–CSF barriers has been characterized in the subfornicalorgan, OVLT, and area postrema (Langlet et al., 2013).Tanycytes of the ME also have important interfacefunctions. They are thought to participate in the regu-lation of hypothalamic pathways that control energybalance through glucose sensing and leptin transportinto CSF (Balland et al., 2014; Elizondo-Vega et al.,2015).
The sensory CVOs are important interfaces for neuro-immune communication. Neuroimmune functions ofCVOs were first demonstrated by the pioneering workof Blatteis et al. (1983) in the 1980s, in context of thefebrile response, which was diminished by OVLTablation. It was later shown that cells within CVOsrapidly upregulate proinflammatory cytokines follow-ing systemic application of LPS, whereas the brainparenchymal inflammatory response occurs as a secondwave (Quan et al., 1998). The localized inflammation inCVOs may disrupt the tanycytic blood–CSF barrier, asincreased paracellular permeability between junctionsof tanycytes lining the third ventricle has been observedin response to LPS (Liu et al., 1996).
III. The Neuroimmune Axes
A. Axis 1: Blood–Brain Barrier Disruption
Strictly speaking, disruption is usually considered apathologic condition. However, there is a perceptionthat, even under physiologic conditions, barrier func-tion may slightly vary. As such, a role for neuroinflam-mation in the physiologic regulation of barrier tightnessmay emerge, and so this section is presented as aneuroimmune axis. Furthermore, the term “disruption”as it pertains to brain barriers is often not clearlydefined. In the strictest sense, disruption refers to lossof barrier function resulting from loss of TJ function,reinstitution of macropinocytosis or fenestrae, ordevelopment of cannulae/vesiculo-tubular structures(Lossinsky and Shivers, 2004), thus allowing leakageof normally restricted substances, such as serum pro-teins, across barrier cells. But it is often used muchmore loosely to describe an alteration in endothelial orepithelial function permitting leukocyte entry intobrain parenchyma, loss of Pgp function, or dysfunctionsresulting in some form of enhanced passage. Notably,the latter are distinct but possibly interrelated molec-ular processes. In this work, we will use “disruption” inits strictest sense and explore inflammatory influenceson immune cell trafficking and Pgp function in separatesections.
The experimental determination of BBB disruptionand the subsequent leakage under various neuroin-flammatory states are often accomplished bymeasuringthe CNS entry of serum proteins or i.v. injected tracer,
BBB and Neuroimmune Axes 289
-
as well as assessment of TJ protein expression(Saunders et al., 2015). In living humans, the CSF/se-rum albumin ratio is also a common indicator used toinfer BBB leakage, and technical aspects of this ap-proach and others that have been used to detect BBBdisruption in humans are critically appraised elsewhere(Erickson and Banks, 2013). BBB leakage is observed indiverse pathologic states in which distinct modes ofBBB disruption may be apparent. In this study, wedescribe three mechanisms by which inflammatoryconditions may contribute to a leaky BBB (Fig. 2).1. Disruption of Paracellular Tight Junctions.
BBB leakage between endothelial cell contacts canoccur when TJ proteins decrease in expression, misloc-alize, or are posttranslationally modified (Luissintet al., 2012). In many instances, inflammatory media-tors can modulate TJ proteins and induce paracellularBBB leakage. For example, an injection into brainparenchyma of IL-1b results in the loss of occludinand ZO-1 expression at endothelial cells, which coin-cides with paracellular leakage of an intravasculartracer and neutrophil recruitment to vessels whereTJs are absent (Bolton et al., 1998). TGF-b1, whichplays classic roles in the resolution of inflammation,also increases tyrosine phosphorylation of VE-cadherinand claudin-5 and downregulates claudin-5 expression(Shen et al., 2011; McMillin et al., 2015). The chemokineC-C motif chemokine ligand (CCL) 2, which attractsmonocytes, causes loss of TJ protein expression, as wellas TJ protein redistribution that is mediated by cav-eolae (Stamatovic et al., 2005, 2006, 2009). Enzymaticdegradation of TJ proteins at the BBB can also occur inresponse to neuroinflammatory insults. MMP inhibi-tion or knockout prevents the degradation of TJs andBBB disruption in the acute phase following brainischemia-reperfusion injury (Asahi et al., 2001; Yanget al., 2007). Protective factors have also been identified
that preserve TJ protein expression at the brainendothelium. These include IL-25, netrin-1, andannexin A1, which are expressed by BECs, and sonichedgehog, which is secreted by astrocytes (Sonobe et al.,2009; Alvarez et al., 2011; Cristante et al., 2013;Podjaski et al., 2015). IL-1b can decrease sonic hedge-hog expression (Wang et al., 2014b). Other inflamma-tory mediators of increased paracellular BBBpermeability include bradykinin, histamine, serotonin,arachidonic acid, and ATP (Abbott, 2000). Clearly, TJsmay become dysfunctional under a number of differentproinflammatory states. However, other routes of BBBdysfunction that result in leakiness also occur in re-sponse to inflammation and are discussed below.
2. Transcytotic Vesicular Pathways. Ultrastruc-tural studies of the BBB dating as far back as the1970s have revealed that damaged BECs can formpatent vesicular channels that permit the passage oflarge molecular tracers such as horseradish peroxidaseinto the CNS (Lossinsky and Shivers, 2004). Suchvesicular structures have been described in cerebraledema, traumatic brain injury, and sepsis (Castejon,1980, 1998; Esen et al., 2012). In some instances, theformation of transcellular channels occurs in the ab-sence or independently of ultrastructural changes inTJs (Lossinsky and Shivers, 2004; Esen et al., 2012;Goncalves et al., 2017). Despite the potential contribu-tion of vesicles and transendothelial channels to BBBleakage, the molecular underpinnings of their forma-tion remain relatively understudied. One protein that isubiquitously expressed in peripheral endothelial cells isplasmalemma vesicle-associated protein (Plvap), whichis sometimes referred to as MECA-32. Plvap associateswith endothelial fenestrae and contributes to fenestraeformation in peripheral vessels (Herrnberger et al.,2012a,b). Plvap is suppressed in brain endothelium(Hallmann et al., 1995), but is upregulated in diseases
Fig. 2. Axes 1 and 3: disruption, transport, and penetration. Major influx mechanisms are transcellular diffusion and saturable transport. Influx iscountered by efflux (transcellular diffusion, saturable transport, reabsorption of CSF) and enzymatic activity at the BBB. Disruption can be by way oftranscellular/transcytotic or paracellular mechanisms. Endothelial damage and hemorrhage are not depicted. The extracellular pathways arerelatively inefficient routes of CNS uptake vs. saturable transport and used by substances that include albumin, immunoglobulins, erythropoietin, andsoluble receptors.
290 Erickson and Banks
-
that are associated with BBB disruption, such asAlzheimer disease (AD) or multiple sclerosis (MS)(Engelhardt et al., 1994; Yu et al., 2012). Furthermore,Mfsd2a (described above in Features and Functions ofthe Blood–Brain Barrier and Blood-Brain Interface) isdownregulated in a mouse model of intracerebralhemorrhage that, in part, mediates BBB disruption(Yang et al., 2017). Therefore, formation of endothelialfenestrations may be an important contributor to BBBleakage in some disease states.3. Endothelial Cell Damage and Hemorrhage.
Cerebral microbleeds (CMB) are associated with neuro-vascular insults such as ischemia-reperfusion injury,intracranial hemorrhage, cerebrovascular diseases, andfollowing traumatic brain injury (Kleinig, 2013). CMBsare also observed in sepsis patients (Correa et al., 2012),and systemic inflammation is higher in patients withCMBs (Miwa et al., 2011). CMBs are visualized ashemodesmerin deposits, which are iron-rich breakdownproducts of hemoglobin (Kleinig, 2013). Recent workusing animal models of subchronic systemic inflamma-tion and ischemia-reperfusion injury has demonstratedthat BBB disruption and neuroinflammation can beassociated with subsequent development of microbleeds(Krueger et al., 2015; Sumbria et al., 2016). In C57BL6/Jmice treated with three repeated doses of LPS, CMBsbecame evident 2 days after the final injection andpersisted by day 7. Furthermore, CMBs significantlycorrelated with markers of neuroinflammation follow-ing LPS treatment (Sumbria et al., 2016). In a rodentischemic-reperfusion injury model, it was observed thatleakage of albumin within the ischemic area occurs inthe absence of changes in TJ or AJ protein-stainingpatterns (Krueger et al., 2015). However, structuralalterations to the endothelial surface were evident andindicated regions where the endothelium was damagedor absent; these damaged endothelial cells colocalizedwith albumin extravasation. Ultrastructural analysisrevealed that, at early stages of damage, endothelial celledema occurs without apparent extravasation of in-travascular tracer. Influx of tracer into the brainparenchyma only became apparent after complete lossof endothelial cell integrity, and influx of red blood cellsinto the CNS occurred following basement membranedegradation (Krueger et al., 2015). Neutrophil-derivedproteases such as MMP9 and elastase have been shownto contribute to the breakdown of the ECM and de-struction of the endothelium in ischemia-reperfusioninjury (Gidday et al., 2005; Stowe et al., 2009; Ikegameet al., 2010; Turner and Sharp, 2016). Intracerebralinjection of neutrophil elastase causes endothelialswelling and focal necrosis of blood vessels, as well asfocal hemorrhages and leukocyte cuffing of the vessels(Armao et al., 1997).The existence of these three modes of BBB disruption
necessitates a careful interpretation of TJ proteinexpression data. The absence of apparent changes in
TJ proteins does not necessarily mean that the BBB isintact, as leakage may occur via vesicles, transcellularchannels, or damaged endothelial cell membranes.Conversely, a decrease in TJ protein expression mayreflect BBB damage that is more severe than para-cellular leakage, such as endothelial cell degenerationwhere the whole cell is lost in addition to the TJ. Theworks that have highlighted these varied modes of BBBdisruption also suggest that different therapeutic ap-proaches to protect the BBB may need to be consideredbased on which mode of BBB leakage predominates.
B. Axis 2: Modulation of Barrier and InterfaceFunctions by Immune Substances
The BBB has many functions other than that offorming a barrier between the peripheral circulationand the CNS. It broadly serves other roles, includingthat of regulating the homeostatic environment of theCNS, supplying the nutritional needs of the CNS, andbeing the center point in the humoral-based communi-cations between the CNS and peripheral tissues. One ofthe main ways in which the BBB fulfills these functionsis through the possession of various transport systems.These transporters have in common that they are self-saturable. As described above, transporters can bevariously classified as energy requiring (active trans-port) or not energy requiring (facilitated diffusion).Active transport can be unidirectional, transporting asubstance against its concentration gradient, whereasfacilitated diffusion is bidirectional with net transportbeing in the direction of higher to lower concentration.As a rough guide, substances that are the major ligandfor a blood-to-brain (influx) transporter can enter thebrain at rates that are 10–100 times faster than if theywere to depend on nonsaturable mechanisms, andsubstances transported out of the CNS (efflux trans-porters) accumulate at rates 1/10 or so lower thanwouldbe expected from their transcellular diffusion. Severalimportant transporters are modulated by neuroinflam-mation and neuroimmune substances (Fig. 3). Pgp is amajor efflux transporter for small, lipid-soluble mole-cules. It resides in the luminal membrane of BECs andthe ependymal cells forming the choroid plexus. Asdiscussed above, its ligands represent a diverse group ofsubstances and include protease inhibitors, opiates(endogenous and exogenous; peptides and small mole-cules), anti-epileptics, cyclosporins, glucocorticoids, al-dosterone, dexamethasone, and calcium channelblockers (Begley, 2004). Its activity explains why cer-tain substances do not accumulate in the brain insufficient quantities to produce an effect on the CNS.As such, it can be viewed either as protecting the brainfrom xenobiotics, including drugs, that would otherwiseproduce significant CNS side effects or as a majorobstacle to the development of CNS therapeutics. Pgpfunction is modulated by inflammation with the maineffect in vivo being a downregulation of its transport
BBB and Neuroimmune Axes 291
-
function. Details of immune regulation of Pgp functionare detailed later in section IV of this review.Influx transport can also be affected by inflammation.
The Na-K-Cl cotransporter at the BEC, important incerebral ionic homeostasis, is modulated by IL-6 se-creted from astrocytes (Sun et al., 1997). Insulin istransported across the BBB and acts in the brain,having effects on cognition and feeding (Banks et al.,2012b). CSF/serum ratios of insulin are reduced in AD,and delivery of insulin to the brain of AD patients canimprove cognitive functions (Craft et al., 1998, 1999,2012). LPS acts indirectly through a nitric oxide–dependent pathway to increase BBB transport of in-sulin (Xaio et al., 2001).Some of the many and diverse effects of LPS on
barrier functions are directly mediated by the presenceof Toll-like receptors on barrier cells. The expression byBECs of at least some of these receptors are themselvesregulated by oxidative stress and TNF-a (Nagyosziet al., 2010). The bacterial cell wall components LPSand muramyl dipeptide also regulate the BEC expres-sion of nucleotide-binding oligomerization domain(NOD) and NOD-like receptors (NLRs), intracellularsensors of pathogen and damage/danger-associatedmolecules (Nagyoszi et al., 2010). Expression of NLRsand of NODs, the domain of NLRs that binds glycopep-tides such as N-acetylglucosamine, is upregulated aswell by inflammatory cytokines, including IFN-g, TNF-a, and IL-1b (Nagy}oszi et al., 2015).The response of the brain barriers to neuroimmune
stimuli can be modulated, reversed, or blocked by anumber of agents as well. BECs express cannabinoidtype 2 receptors. Agonists of these receptors prevented32 of 33 genes from being upregulated by TNF-a anddiminished TNF-induced BBB disruption and macro-phagemigration (Persidsky et al., 2015). Prostaglandins,
as evidenced by the effects of treatment with indometh-acin, can block, enhance, or have no effect on the actionsof LPS on BBB functions (Guillot and Audus, 1990;Minami et al., 1998; Xaio et al., 2001).
C. Axis 3: Transport, Penetration, and Uptake ofNeuroimmune-Related Substances
Blood-to-brain entry has been assessed for someneuroimmune substances. Several cytokines have beenshown to cross the BBB by way of saturable transportsystems and antibodies and soluble receptors can enterthe brain by way of the extracellular pathways.
Many cytokines are transported across the BBB inthe blood-to-brain direction (Fig. 2). Such transportintermingles the peripheral pool of the cytokine withits CNS pool. The transport systems for cytokines aresaturable and are selective, perhaps even specific, for acytokine or family of cytokines. For example, the trans-port of TNF-a is self inhibited, but not inhibited by IL-6nor by any of the IL-1s (Gutierrez et al., 1993; Bankset al., 1994). The IL-1s (IL-1a, IL-1b, IL-1 receptorantagonist) both self inhibit as well as inhibit eachother’s transport, but have not been found to inhibit thetransport of any other cytokine (Banks et al., 1991).Therefore, the IL-1 family either shares a single trans-porter or a family of closely related transporters.Epidermal growth factor crosses the BBB using atransporter shared with TGF-a (Pan and Kastin,1999). CCL2 (monocyte chemoattractant protein 1)transport is not shared with CCL3 (macrophage-inhibitory protein 1-a) (Ge et al., 2008). Other cytokinesformally demonstrated to be transported across theBBB include ciliary neurotrophic factor and TGF-b2(Pan et al., 1999; McLennan et al., 2005), but TGF-b1 isnot transported across the intact BBB (Kastin et al.,2003). To date, only IL-2 and CCL11 have been found to
Fig. 3. Axis 2: modulation of barrier/interface function. Immunoactive (IA) substances work through four main pathways to alter BBB functions. (A) IAsubstances act on a peripheral cell that then releases a substance that acts on the barrier. Example: LPS acts on a peripheral cell inducing it to releasenitric oxide, and the nitric oxide then acts on BECS to alter insulin transport. (B) IA acts on the BEC to induce an alteration mediated throughintracellular machinery. Example: TNF alteration of Pgp function, which is mediated through a pathway involving nitric oxide and endothelin-1. (C) IAacts directly at a BEC receptor or transporter. Example: IL-1ra blocks BBB transport of IL-1b. (D) IA acts on barrier cell receptor/transporter (i)inducing barrier cell secretion that acts in autocrine fashion to affect barrier function (example: LPS induces BEC to secrete IL-6 and granulocyte-macrophage colony-stimulating factor, which mediates LPS-induced increase in HIV-1 passage across the BBB) or (ii) to induce barrier cell tocommunicate with another CNS cell whose release modifies barrier cell activity (example: presence of pericyte enhances LPS-induced increase in HIV-1passage across the BBB).
292 Erickson and Banks
-
have a saturable component to their brain-to-bloodefflux phase (Banks et al., 2004b; Erickson et al.,2014), although others can enter the circulation withCSF reabsorption (Chen et al., 1997; Chen and Reichlin,1998). It has also been suggested that the duffy antigenchemokine receptor on brain endothelial cells contrib-utes to brain efflux of CCL2 and CCL5 following aneuroinflammatory stimulus (Minten et al., 2014).Little is known about the cellular biology of cytokine
transport across the BBB or what circulating factorsmay affect such transport. Cytokine-induced neutrophilchemoattractant 1 enters the brain by a nonsaturablemechanism, presumably that of transcellular diffusion(Pan and Kastin, 2001a). At a mol. wt. of 7800 Da, thiswould be the largest known substance to use thispathway, which essentially involves the molecule firstpartitioning into the lipids of the barrier cell membraneand eventually back into the aqueous environment ofbrain interstitial fluid or CSF. Erythropoietin entersthe CNS by the nonsaturable process of the extracellu-lar pathways, although it is unclear the degree to whichthis underlies its many neuroprotective effects (Brineset al., 2000; Banks et al., 2004a). In general, theextracellular pathways account for little of the uptakefor cytokines that use a saturable transporter to crossthe BBB (Plotkin et al., 1996). For most endogenousbiologics studied to date, the protein responsible fortransport is not the same as that used by the cell forreceptor functions (Pan and Kastin, 1999), althoughthere seem to be more exceptions to this rule forcytokines than for other biologics (Pan and Kastin,2002; Pan et al., 2006a; Ge et al., 2008). CCL2 transportis caveolae dependent (Ge et al., 2008); IL-2 blood-to-brain transport is inhibited, in addition to other mech-anisms, by protein binding (Banks et al., 2004b); andCCL11 (eotaxin-1) binds to cellular components in bloodthat slows its early-phase entry (Erickson et al., 2014).Most