Neural Circuitry of Upper Airway Respiratory Plasticity ...
172
Neural Circuitry of Upper Airway Respiratory Plasticity: Identifying the Neural Circuitry Underlying Long-Term Facilitation of Inspiratory Genioglossus Motor Output by Simon Kent Chow Lui A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy Department of Cell and Systems Biology University of Toronto © Copyright by Simon Kent Chow Lui (2019)
Transcript of Neural Circuitry of Upper Airway Respiratory Plasticity ...

Neural Circuitry of Upper Airway Respiratory Plasticity:
Identifying the Neural Circuitry Underlying Long-Term Facilitation of
Inspiratory Genioglossus Motor Output
by
Simon Kent Chow Lui
A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy
Department of Cell and Systems Biology
University of Toronto
© Copyright by Simon Kent Chow Lui (2019)

ii
Abstract
Neural Circuitry of Upper Airway Respiratory Plasticity: Identifying the
Neural Circuitry Underlying Long-Term Facilitation of Inspiratory
Genioglossus Motor Output
Simon Kent Chow Lui
Doctor of Philosophy
Department of Cell and Systems Biology
University of Toronto
2019
The respiratory system is highly adaptive and can change its behaviour to provide protective
responses in face of repeated respiratory challenges. Elucidating the role of how neurons and
neural circuits mediate these responses can open new treatments for those that cannot adapt.
Respiratory long-term facilitation (LTF) is one form of adaptation that can increase genioglossus
motor output, potentially providing a means to mitigate respiratory disorders such as
obstructive sleep apnea. I examined the neural circuitry that underlies this form of respiratory
motor plasticity and I identified: (1) the neural circuit that mediates respiratory LTF of
inspiratory genioglossus motor output, (2) a novel trigger that elicits LTF without directly or
indirectly modulating the respiratory feedback systems, and (3) the neurotransmitter(s) that
are essential to the manifestation of respiratory motor plasticity of genioglossus motor output.
Using tract-tracing, immunohistochemical and pharmacological approaches, I have identified a

iii
tripartite circuit connecting the nucleus tractus solitarius (NTS), the locus coeruleus (LC), and
the hypoglossal motor nuclei (XII) that are individually critical to the elicitation of LTF. I also
employed a series of optogenetic approaches to identify the LC as a trigger that can elicit LTF
following intermittent stimulation of the LC alone. Lastly, I identified noradrenaline, released by
the LC and acting on α1-adrenergic receptors at the hypoglossal motor nuclei, to be the key
neurotransmitter-receptor system that gates the expression of respiratory motor plasticity.
These findings provide direction and novel therapeutic targets to treat respiratory disorders
such as obstructive sleep apnea.

iv
Acknowledgements
Deciding to pursue a doctoral degree was easy, but completing this task was something that I
never could have been capable of without the help of many wonderful people.
The most important and influential person in this journey is undoubtedly my doctoral
supervisor, Dr. John Peever. I consider myself extremely lucky to have found such a truly
patient, kind, and brilliant mentor to take me under his wing. I have never met anyone who is
so dedicated to guiding and molding his students to become the best scientists they can be.
John’s dedication to his students and his brilliant mentorship has allowed me to become not
only a better scientist, but also a better person. The difference he has made in my life is
immeasurable and with everything in my heart, I want to thank you for everything you have
done for me. Thank you. Thank you. Thank you.
In addition to John, I would like to thank the members of my advisory committee, Dr. Melanie
Woodin, Dr. Richard Horner, and Dr. Leslie Buck. Your help and guidance throughout my PhD
career shaped me into a better scientist and a better person. I would like to thank Dr. David
Lovejoy for participating in my final oral examination, and Dr. Deborah Sloboda, from McMaster
University for serving as my external examiner.
I also want to thank many members of the Peever lab. Dr. Jennifer Lapierre has been my friend,
my manager, my mentor, and most importantly, my lab wife. Jenn has helped me through
sickness and in health, and I owe her more than I can say to have succeeded this far. Dr. Jimmy
Fraigne has been a friend and mentor as well. Jimmy has been the one I turn to on more than

v
one occasion to troubleshoot the realm of science. He has been the calm voice of reason when I
needed it and is truly a gift to the Peever lab.
I want to thank the staff of the Department of Cell & Systems Biology, especially Ian Buglass,
Tamar Mamourian, and Peggy Salmon for all their help. I want to thank the staff of the
Bioscience Facility, especially Christine McCaul with all her help throughout the years.
My family and friends have been overwhelmingly supportive throughout my 7 year journey.
Without my parent’s support, my brother Leo’s help, and the love my dearest Kevin Dyal, I
could not have completed this journey. Dr. Stephanie Hughes and Justin Cooke have been my
best friends and often times my statisticians and programmers. Their support has been vital to
my success.
Lastly, I would like to thank Natural Sciences and Engineering Research Council of Canada
(NSERC) for my Ph.D. funding. The work presented in this thesis was supported by grants held
by Dr. John Peever.

vi
Preface
My journey into the scientific community began with a desire to understand what it means to
have a healthy brain. I’ve been told from a young age to wear a helmet to protect my head, to
eat foods that are nutritious for my brain, and to avoid drugs and alcohol because it will harm
my body and my mind. But what defines a healthy brain? A generic definition of health can be
translated to being fit for survival. Therefore, a healthy brain must facilitate the organism’s
survival, and the best way to survive is to adapt. By this definition, neural adaptation or neural
plasticity defines a healthy brain. A brain must be adaptable, plastic, and capable of responding
to acute and persistent stimuli. If the brain cannot adapt, and the organism will likely perish.
The pursuit of science has allowed means to prolong a healthy brain – introduce plasticity
where there was none or augment plasticity when it is insufficient. However, plasticity cannot
occur if the organism cannot breathe. Breathing is critical to survival, and plasticity of breathing
is therefore of utmost importance. Long-term facilitation is a form of plasticity within the
respiratory system. My encounter with this form of plasticity has led me to desire
understanding how it works. I want to know how it works so I can induce it, augment it, deliver
it to those who cannot adapt, and have as many people breathing for as long as possible.

vii
Table of Contents
Abstract ......................................................................................................................................................... ii
Acknowledgements ...................................................................................................................................... iv
Preface ......................................................................................................................................................... vi
Table of Contents ........................................................................................................................................ vii
List of Figures and Tables ............................................................................................................................. xi
List of Abbreviations ...................................................................................................................................xiii
Chapter One – Introduction .......................................................................................................................... 1
Overview ................................................................................................................................................... 1
Neural Circuits ........................................................................................................................................... 5
Neural Circuit Underlying Respiratory Control ......................................................................................... 7
Plasticity .................................................................................................................................................. 10
Respiratory Plasticity .............................................................................................................................. 11
Phrenic LTF .......................................................................................................................................... 13
Hypoglossal LTF ................................................................................................................................... 16
How Noradrenaline Induces Plasticity .................................................................................................... 20
Noradrenaline and Hypoglossal LTF........................................................................................................ 23
Neural Circuits Underlying Hypoglossal LTF ........................................................................................... 25
Experimental Objectives ......................................................................................................................... 27
Chapter Two – Materials and Methods ...................................................................................................... 29
Animals .................................................................................................................................................... 29
Drug and Tracer Preparation .................................................................................................................. 29
Surgical Procedures ................................................................................................................................. 30
Stereotaxic Injection (Virus / Tracer) .................................................................................................. 31
Drug Delivery....................................................................................................................................... 32
Optogenetic Manipulations ................................................................................................................ 32
Electrophysiology Recordings ................................................................................................................. 33
Measurement of ET-CO2 and O2 Saturation ............................................................................................ 34
Experimental Protocol ............................................................................................................................ 34
Objective 1 – To determine the brainstem structures activated alongside apnea-induced hLTF ...... 35

viii
Objective 2 – To determine the anatomical connections between the noradrenergic locus coeruleus
neurons and the hypoglossal motor pool ........................................................................................... 36
Objective 3 – To determine whether the locus coeruleus is a critical component of the neural circuit
mediating apnea-induced hLTF ........................................................................................................... 36
Objective 4 – To determine whether optogenetic manipulation of ChR2-expressing locus coeruleus
neurons alone can elicit hLTF .............................................................................................................. 37
Objective 5 – To determine whether optical silencing of eNpHR-expressing locus coeruleus neurons
prevent apnea-induced hLTF .............................................................................................................. 38
Objective 6 – To determine whether noradrenaline released specifically from the locus coeruleus is
the underlying mechanism that mediates hLTF ................................................................................. 39
Data Analysis ........................................................................................................................................... 40
Histology ................................................................................................................................................. 40
Cell Quantification .................................................................................................................................. 42
Statistical Analysis ................................................................................................................................... 42
Chapter Three – A Tripartite Circuit Mediates Respiratory Motor Plasticity ............................................. 45
Summary ................................................................................................................................................. 45
Introduction ............................................................................................................................................ 45
Locus Coeruleus and its Role in Breathing and Plasticity .................................................................... 47
Projections of Locus Coeruleus Neurons ............................................................................................ 48
Results ..................................................................................................................................................... 48
Repeated Obstructive Apneas Trigger LTF of Inspiratory Genioglossus Muscle Activity ................... 48
Activation of Noradrenergic LC Neurons Correlates with hLTF .......................................................... 50
Activation of Noradrenergic Cells in the LC is Specific to hLTF Responders ....................................... 51
Noradrenergic LC Neurons Have Direct Projections to the Hypoglossal Motor Pool ......................... 55
Bilateral Inactivation of the LC Prevents Apnea-Induced hLTF ........................................................... 57
Discussion................................................................................................................................................ 59
Noradrenergic Cells in the LC are Active During hLTF ........................................................................ 59
Noradrenergic LC Neurons Project to the Hypoglossal Motor Pool ................................................... 61
LC Activation is Independent of Hypoxia or Hypercapnia Associated with Repeated Apneas ........... 61
The LC is a Required Component of the Neural Circuit Underlying Apnea-Induced hLTF .................. 62
Brainstem regions associated with apnea-induced hLTF .................................................................... 63
Methodological Considerations .......................................................................................................... 65
Scientific Importance and Clinical Significance ................................................................................... 67

ix
Chapter Four – Optical LC Stimulation Triggers for LTF of Inspiratory Genioglossus Motor Output ......... 69
Summary ................................................................................................................................................. 69
Introduction ............................................................................................................................................ 69
Triggers of LTF That Act Through the Chemosensory or Broncho-Pulmonary Feedback System ...... 70
Triggers of LTF Independent of the Chemosensory and Broncho-Pulmonary Feedback Systems ..... 70
The LC and its Potential Role in hLTF .................................................................................................. 71
Results ..................................................................................................................................................... 71
LC Cells Equally Infected by Viral Vectors Across All Groups .............................................................. 71
Baseline Genioglossus Motor Activity is Decreased During Optical Inactivation of eNpHR-Expressing
LC Neurons .......................................................................................................................................... 74
LTF of Genioglossus Motor Activity is Elicited After Intermittent Stimulation of ChR2-Expressing LC
Neurons ............................................................................................................................................... 76
Intermittent Light Exposure on Non-ChR2-Expressing mCherry LC Neurons Does Not Trigger hLTF 80
hLTF Expression Requires an Intermittent Pattern of LC Stimulation ................................................ 81
Intermittent LC stimulation elicits hLTF at the same frequency as repeated apneas ........................ 84
hLTF Requires a Minimum Threshold Activation of LC Cells ............................................................... 86
Inactivation of the LC Abolishes Apnea-Induced hLTF ........................................................................ 89
Discussion................................................................................................................................................ 94
LC Provides an Endogenous Noradrenergic Drive to Hypoglossal Motor Neurons ............................ 95
Baseline Genioglossus Motor Activity is Unaffected During Stimulation of ChR2-Expressing LC
Neurons ............................................................................................................................................... 96
Stimulation of ChR2-Expressing LC Neurons Trigger LTF of Inspiratory Genioglossus Motor Output 97
LC is Critical for hLTF ........................................................................................................................... 98
A Minimum Threshold of LC Stimulation is Required for hLTF Expression ......................................... 98
Plasticity Occurs at the Level of the LC and at the Level of the Hypoglossal Motor Neuron ............. 99
Methodological Considerations ........................................................................................................ 100
Scientific Importance and Clinical Significance ................................................................................. 102
Chapter Five - α1-Adrenergic Receptor Binding at the Hypoglossal Motor Pool Is Required for LC-Induced
hLTF ........................................................................................................................................................... 103
Summary ............................................................................................................................................... 103
Introduction .......................................................................................................................................... 103
Results ................................................................................................................................................... 108
Intermittent Stimulation of LC Axons at the Hypoglossal Motor Pool Did Not Trigger hLTF ........... 108

x
Noradrenaline Released from the LC is Critical for hLTF .................................................................. 110
Saline Perfusion into the Hypoglossal Motor Pool Does Not Influence hLTF Expression ................. 112
α1-Adrenergic Receptor Blockade Abolishes hLTF Expression ......................................................... 113
Discussion.............................................................................................................................................. 115
Direct Stimulation of LC Axons Projecting to the Hypoglossal Motor Pool Did Not Elicit hLTF ........ 115
The LC Co-Releases Neurotransmitters That Can Induce Plasticity and/or Modulate Respiratory
Output ............................................................................................................................................... 117
The Same Intracellular Machinery is Involved in Mediating hLTF Expression Across Multiple Triggers
.......................................................................................................................................................... 118
Methodological Considerations ........................................................................................................ 119
Scientific Importance and Clinical Significance ................................................................................. 120
Chapter Six – General Discussion .............................................................................................................. 122
Hypoglossal / Genioglossus LTF is Mechanistically Distinct From Phrenic / Diaphragm LTF ................ 123
The Brainstem Circuit Mediating hLTF: NTS → LC → XII ...................................................................... 126
The Site of Plasticity in the hLTF Tripartite Circuit ................................................................................ 128
Plasticity at the NTS .......................................................................................................................... 128
Plasticity at the LC ............................................................................................................................. 129
Plasticity at the Hypoglossal Motor Neuron ..................................................................................... 131
Summary of Proposed Mechanism Underlying hLTF ............................................................................ 132
Methodological Considerations ............................................................................................................ 134
Significance of Findings ......................................................................................................................... 137
Future Directions .................................................................................................................................. 139
References ............................................................................................................................................ 140

xi
List of Figures and Tables
Figure 1.1. A schematic showing the cyclic sequence of events leading to the development of
obstructive sleep apnea and the events that restore patency in the upper airways ............................... 3
Figure 1.2. Representative trace of integrated phrenic nerve activity before, during and after acute
intermittent hypoxia or no hypoxia in rats, and the subsequent increase in phrenic nerve amplitude
(i.e. pLTF) ................................................................................................................................................... 4
Figure 1.3. A schematic of the respiratory control network ................................................................... 10
Figure 1.4. Working model of acute intermittent hypoxia-induced pLTF............................................... 15
Figure 1.5. Schematic diagram of human tongue and the muscles innervated by the hypoglossal nerve
................................................................................................................................................................ 17
Figure 1.6. LTF of genioglossus motor output induced by intermittent apneas .................................... 20
Figure 1.7. Schematic of the signalling cascade following noradrenaline-binding to α1- or α2-
adrenergic receptors ............................................................................................................................... 23
Figure 1.8. Hypothesized circuit responsible for hypoglossal LTF .......................................................... 27
Figure 2.1. Protocol for the delivery of repeated apneas in Objective 1 ................................................ 35
Figure 2.2. Protocol for clonidine intervention followed by repeated apneas in Objective 3 ............... 37
Figure 2.3. Protocol for intermittent LC stimulation in Objective 4 ....................................................... 38
Figure 2.4. Protocol for continuous LC stimulation in Objective 4 ......................................................... 38
Figure 2.5. Protocol for continuous inhibition of the LC with repeated apneas in Objective 5 ............. 39
Figure 2.6. Protocol for terazosin perfusion with intermittent LC stimulation in Objective 5 ............... 39
Figure 3.1. Repeated obstructive apneas elicit LTF of the genioglossus motor activity ......................... 50
Figure 3.2. LC activation correlates with apnea-induced hLTF ............................................................... 53
Figure 3.3. Levels of anesthesia, expired CO2, O2 saturation and blood pressure do not correlate with
hLTF ......................................................................................................................................................... 54
Figure 3.4. Noradrenergic LC neurons have direct projections to the hypoglossal motor pool ............ 56
Figure 3.5. Inactivation of the LC prevents apnea-induced hLTF............................................................ 58
Figure 3.6. Hypothesized circuitry responsible for hLTF. ........................................................................ 65
Figure 4.1. Increased or decreased c-Fos expression following light-induced manipulation to ChR2- or
eNpHR-expressing LC cells ...................................................................................................................... 73
Figure 4.2. Optical inactivation of LC cells decreased genioglossus motor output ................................ 76
Figure 4.3. Intermittent optical stimulation of the LC elicits LTF of genioglossus motor activity .......... 79

xii
Figure 4.4. Intermittent LC stimulation activates ChR2-expressing LC neurons more than mCherry-
expressing LC cells or continuous LC stimulation ................................................................................... 83
Figure 4.5. Probability of LTF expression was increased following intermittent stimulation of the LC . 85
Figure 4.6. LTF requires a minimum LC stimulation threshold ............................................................... 88
Figure 4.7. Optical inactivation of the LC prevents apnea-induced LTF ................................................. 91
Figure 4.8. LTF did not manifest following LC inactivation ..................................................................... 94
Figure 5.1. Protocol for intermittent LC stimulation with and without terazosin perfusion ................ 107
Figure 5.2. Intermittent stimulation of LC axons did not trigger LTF .................................................... 109
Figure 5.3. LTF is mediated by α1-adrenergic receptor binding of noradrenaline released from the LC
.............................................................................................................................................................. 111
Figure 5.4. Saline perfusion at hypoglossal motor pool does not affect LTF ........................................ 113
Figure 5.5. Probability of LTF was reduced following α1-adrenergic receptor blockade at the
hypoglossal motor pool ........................................................................................................................ 114
Figure 6.1. Hypothesized neural circuit underlying hLTF ...................................................................... 132
Table 3.1. LC is the only noradrenergic cell group implicated in the LTF circuit .................................... 50
Table 6.1. Comparison of mechanisms underlying pLTF vs GG LTF ...................................................... 125

xiii
List of Abbreviations
°C Degree Celcius
< Less than
> Greater than
± Plus or minus
µL Microliter
µM Micromolar
µm Micrometer (micron)
5-HT 5-hydroxytryptamine (i.e., serotonin)
5-HT2A 5-hydroxytryptamine receptor subtype 2A
AIH Acute intermittent hypoxia
AMPA α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid
ANOVA Analysis of variance
AP Anterior posterior
ATP Adenosine triphosphate
Aug-E Augmenting expiratory
BDNF Brain-derived neurotrophic factor
BötC Bötzinger complex
ChR2 Channelrhodopsin2
CIH Chronic intermittent hypoxia
CLO Clonidine
cm Centimeter
CO2 Carbon dioxide
CSN Carotid sinus nerve

xiv
CtB Cholera toxin subunit B
cVRG Caudal ventral respiratory group
DAG Diacylglycerol
Dia Diaphragm
DRG Dorsal respiratory group
Early-I Early-inspiratory
EMG Electromyogram
eNpHR3.0 Halorhodopsin
ERK Extracellular signal-regulated kinases
ET-CO2 End-tidal carbon dioxide
fB Breath frequency
FiCO2 Fraction of inspired carbon dioxide
FiO2 Fraction of inspired oxygen
FW Formula weight
GABA Gamma-aminobutyric acid
GG Genioglossus
Gq/Gi G protein-mediated activation / inhibition
hLTF Hypoglossal / genioglossus long-term facilitation
kHz Kilohertz
Hz Hertz
IP3 Inositol triphosphate
IPSC Inhibitory post-synaptic current
Late-E Late-expiratory
LC Locus coeruleus

xv
LTF Long-term facilitation
LTP Long-term potentiation
MAPK Mitogen-activated protein kinases
Min Minute
mg Milligram
mm Millimeter
mw Milliwatts
N2 Nitrogen
NA Noradrenaline
NMDA N-methyl-D-aspartate
NTS Nucleus tractus solitarius
O2 Oxygen
OLS Ordinary least square
OSA Obstructive sleep apnea
PI3K Phosphoinositol 3-kinase
PKC Protein kinase C
PLC Phospholipase C
pLTF Phrenic / diaphragm long-term facilitation
Post-I Post-inspiratory
preBötC PreBötzinger complex
Pre-I/I Pre-inspiratory/inspiratory
PRG Pontine respiratory group
PSR Pulmonary stretch receptors
Ramp-I Ramping-inspiratory

xvi
REM Rapid Eye Movement
RM Repeated measures
RNA Ribonucleic acid
RTN Retrotrapezoid nucleus
RRG Respiratory rhythm generator
rVRG Rostral ventral respiratory group
SEM Standard error of the mean
SubC Subcoeruleus
TrkB Tropomyosin receptor kinase B
vLTF Ventilatory long-term facilitation
VRG Ventral respiratory group
XII Hypoglossal

1
Chapter One – Introduction
1.1 Overview
Respiration is a natural function that is critical for survival. It involves the intake of oxygen and
expulsion of carbon dioxide and requires the activation of respiratory pump muscles such as the
diaphragm and secondary muscles that include upper airway dilator muscles such as the
genioglossus. The activity of these muscles is controlled by the respiratory network situated
within the brainstem (Fitzgerald, 1995, Smith et al., 2007). Under normal circumstances, there
are peripheral and central chemosensors that detect levels of dissolved gases in the blood and
adjusts respiratory output to maintain homeostatic balance within the body (Duffin, 2005, Kline
and Mendelowitz, 2012, Moreira et al., 2011, Yokhana et al., 2012). For example, peripheral
chemosensors such as the carotid bodies sense O2, CO2/H+, and glucose in arterial blood and
signal the respiratory network to adjust respiratory output accordingly (Mohan and Duffin, 1997,
Nakayama et al., 2003, Peng et al., 2010). Central chemosensors, such as the retrotrapezoid nucleus
(RTN) act by detecting pH/H+ ions in cerebral spinal fluid (Basting et al., 2015, Takakura et al., 2006)
and signal the respiratory network to adjust respiratory output by changing tidal volume and/or
respiratory frequency (Abbott et al., 2013, Abbott et al., 2009, Holloway et al., 2015). However,
during sleep, there is a reduction in muscle tone and a reduced response from the genioglossus
to hypercapnia (Fung and Chase, 2015, Horner et al., 2002). Under abnormal conditions, as
observed in patients with obstructive sleep apnea (OSA), the reduction of upper airway muscle
tone can increase the collapsibility of the upper airways leading to an apnea which causes
hypoxia and hypercapnia. Due to the physical obstruction, hypoxia and hypercapnia will build,
thus homeostatic balance cannot be reached. The reflexive increase in ventilatory effort to
correct the hypoxia and hypercapnia can wake the patient, ending the apnea, only to repeat the
cycle when the patient resumes sleep (Fig. 1.1) (Syed et al., 2013). This is OSA and these
repetitive airway occlusions throughout the night can cause adverse effects such as sleep loss,
day time fatigue, and increase the risk of other adverse health effects such as hypertension,
stroke, or congestive heart failure (Hung et al., 1990, Nieto et al., 2000, Shahar et al., 2001).
Currently, the prevalence of OSA in North America is at 2% in middle-aged women and 4% in

2
middle-aged men (Young et al., 1993, Young et al., 2002). However, the prevalence of OSA
increases further East, with reports showing 4-6% in patients of East-Asian descent (Ip et al.,
2001, Ip et al., 2004), despite having an average lower body-mass index compared to
Caucasians; this difference can be attributed to craniofacial physiology and size of the upper
airways that may influence collapsibility (Lam et al., 2005, Pham et al., 2018). Optimistically,
studies have showed that humans exposed to intermittent episodes of hypoxia can trigger
respiratory motor plasticity (Aboubakr et al., 2001, Harris et al., 2006), which may mitigate the
reduction of upper airway muscle tone during sleep. For example, repeated bouts of hypoxia
can lead to a decrease in upper airway resistance (Aboubakr et al., 2001, Chowdhuri et al.,
2008), which suggests that the respiratory network can use previous experiences or stimuli (i.e.
intermittent hypoxia) to modulate factors that control respiratory output. This type of motor
plasticity is known as long-term facilitation (LTF) (Fig. 1.2) and may serve to improve effective
lung ventilation (Harris et al., 2006).

3
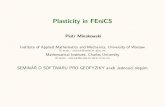
Figure. 1.1. A schematic showing the cyclic sequence of events leading to the development of obstructive sleep apnea and the events that restore patency in the upper airways. Sleep onset is accompanied by a reduction in muscle tone, pharyngeal dilator muscle reflex, as well as increase the hypercapnia recruitment threshold for genioglossus (GG) muscle activity. This can lead to an increase in the propensity for upper airway collapse, effectively producing an obstructive apnea. The resultant increase in hypoxia and hypercapnia reflexively triggers an increase in ventilatory effort and eventual arousal from sleep to restore upper airway patency to correct hypoxia and hypercapnia. This cycle repeats, leading to the disorder known as obstructive sleep apnea (OSA). Long-term facilitation (LTF) may mitigate the reduction in upper airway muscle tone (Adapted from Mateika and Syed, 2013).
My work addresses the neural circuits and mechanisms underlying a form of plasticity that
augments respiratory motor output. Over the last three decades, it has been established that
repeated modulation of chemosensory feedback (e.g. intermittent episodes of hypoxia) can
trigger respiratory motor plasticity (Devinney et al., 2015, Dodig et al., 2012), and the
neurochemical mechanism that facilitates this process is hypothesized to be serotonin released
from the medullary raphe to act on the respiratory control network (Bocchiaro and Feldman,

4
2004, Dodig et al., 2012, McGuire et al., 2004). My work addresses a novel form of respiratory
motor plasticity that is independent of hypoxia but is instead triggered by repeated apneas or
repeated stimulation of the locus coeruleus (LC). This form of respiratory motor plasticity is
mediated by the noradrenergic system and I will provide evidence demonstrating noradrenaline
released from the LC to be the critical component mediating LTF of inspiratory genioglossus
motor output. I will also introduce a novel neural circuit that I hypothesize outlines the critical
brainstem structures required for respiratory motor plasticity to occur. The goal of this thesis is
to determine the mechanisms and circuits that mediate LTF to provide a better understanding
of LTF. Since this is a form of neural plasticity that naturally exists in humans and other animals
(Cao et al., 1992, Chowdhuri et al., 2008, Tadjalli et al., 2010, Terada et al., 2008, Turner and
Mitchell, 1997), elucidating the neural circuits and mechanisms that mediate LTF may help
provide new therapeutic targets to treat OSA and mitigate symptoms in some respiratory
disorders.
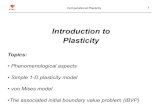
Figure 1.2 Representative trace of integrated phrenic nerve activity before, during and after acute intermittent hypoxia or no hypoxia in rats, and the subsequent increase in phrenic nerve amplitude (i.e. pLTF). Dotted line indicates baseline amplitude. Gray represents increases from baseline. (Adapted from Devinney et al., 2015).
To this end, I will first review the known neural networks underlying respiratory control
followed by an overview of plasticity within the respiratory control network. Next, I will focus
on studies that demonstrate that noradrenaline plays a significant role in LTF, then outline the
gaps in knowledge that this thesis focused on. I will then identify the main objectives of this

5
thesis, and in the subsequent chapters, I describe the experiments I performed to elucidate the
role of noradrenergic neurons in the LC in respiratory motor plasticity.
1.2 Neural circuits
A fundamental concept of neuroscience is that the ability of the brain to produce complex
behaviours, such as motor control, arises from a network of interconnected neurons (Getting,
1989). A network can be simplified into an anatomical and functional organization. An
anatomical organization refers to the afferent and efferent projections, and the synaptic
connectivity between neurons within the network (Getting, 1989). This can be expanded to
include the number of connections between interconnected neurons and the density of
dendritic spines at each connection (Lendvai et al., 2000, Segal, 2005). The anatomical
organization defines the structural limits of the network and identifies which neurons are
communicating with each other. It does not provide information regarding the function of
these neurons and the behaviour that it generates. The functional organization refers to how
the network processes information and generates an output pattern to produce a behaviour.
The ability for a network to produce a behaviour depends on the state of the network at the
time it is activated. Specifically, it depends on factors at the network level (i.e. which neurons
are being activated), at the synapse (i.e. amount of neurotransmitter release and receptors
expressed), and at the cellular level (i.e. the intrinsic excitability of the post-synaptic cell and its
firing properties). These factors can be modulated and the anatomical network can be
reconfigured to produce various behaviours. For example, in rats with T5 spinal cord
transection, elevated levels of nerve growth factor (NGF), a neurotrophin that supports survival
and differentiation of neurons, was observed (Lujan et al., 2010). This correlated with an
increase in innervation and arborization of sympathetic preganglionic neurons, suggesting
neurons can undergo plasticity and initiate the process for making new connections. The most
intuitive modulator is activity (i.e. activity-dependent plasticity) (Cline, 1993, Hawkins et al.,
1993).

6
Traditionally, activity-dependent changes to a neural circuit were first described in Hebbian
synaptic plasticity, where activity between pre- and post- synaptic neurons led to an increase in
synaptic strength between the connected neurons (Hebb, 1949). This later led to the famous
quote “cells that fire together wire together” (Shatz, 1992), which suggests that activity guides
the formation of a neural circuit. Although activity is not the sole contributor to the formation
of neuronal connections (Goodman and Shatz, 1993), activity is nonetheless a potent stimulus
that modulates the strength of neuronal connections. Through repeated use or activation, the
connection is strengthened and the circuit is reinforced. However, these neural circuits are
subject to modulation (e.g. through repeated use or disuse), and modulation of a neural circuit
is what allows for adaptation to match ongoing needs. In other words, activity reinforces the
anatomical organization of a neural circuit, and the functional organization can undergo
plasticity to match it.
The mechanism that mediates anatomical reorganization and functional plasticity is
hypothesized to be attributed (but not limited) to the neurotrophin brain-derived neurotrophic
factor (BDNF), and its receptor tropomyosin kinase receptor B (TrkB), also known as tyrosine
kinase B (Schaser et al., 2012, Schjetnan and Escobar, 2012, Wilkerson and Mitchell, 2009). The
production and release of BDNF is regulated by activity (Isackson et al., 1991, Wetmore et al.,
1994, Zafra et al., 1991); however BDNF itself can also regulate activity (Rutherford et al., 1998).
For example, a decrease in TrkB receptor activation reduced pyramidal neuron firing rates,
while an increase in BDNF levels increase the activity of interneurons (Rutherford et al., 1998).
This suggests that manipulations to BDNF levels changes both the activity of cortical neural
circuits and how they interact. Another example where a neural circuit can be modulated by
BDNF is the circuit that mediates respiratory motor plasticity (Baker-Herman et al., 2004,
Wilkerson and Mitchell, 2009). Respiratory motor output is constantly changing to match its
environment. For example, respiratory output changes during phonation, exercise, or eating
(Dobbins and Feldman, 1995, Fregosi and Fuller, 1997, Tangel et al., 1995). Characterizing the
neural circuitry underlying respiratory control can help us understand how this circuit can

7
exhibit plasticity. In this thesis, I will discuss the neural circuit that underlies a respiratory motor
behaviour and the circuit that underlies upper airway respiratory motor plasticity.
1.3 Neural circuit underlying respiratory control
To understand the neural circuit underlying respiratory motor plasticity, it is necessary to
understand the circuit that controls respiratory output. This is important because the metric for
respiratory plasticity varies across studies. For example, respiratory plasticity can be measured
as an increase in respiratory nerve activity (e.g. hypoglossal or phrenic nerve activity) (Blitz and
Ramirez, 2002, Bocchiaro and Feldman, 2004, Neverova et al., 2007, Schwartz et al., 2012), an
increase in respiratory muscle activity (Cao and Ling, 2010, Ryan and Nolan, 2009, Tadjalli et al.,
2010), a decrease in the resistance of airflow in upper airways (Chowdhuri et al., 2008, Wirth et
al., 2013), or a change in tidal volume or breath frequency (Edge and O'Halloran, 2015, Gerst et
al., 2011, Griffin et al., 2012). Respiratory plasticity could, therefore, be occurring at the level of
the motor neuron or within the respiratory network that control breathing. To understand how
respiratory plasticity could interact with the respiratory network, it is necessary to define the
structures that control breathing.
Respiratory output involves the coordinated contraction of thoracic respiratory muscles (e.g.
diaphragm) and muscles of the upper airways (e.g. the genioglossus). The contraction of these
muscles is controlled by the structures situated within the brainstem (Fitzgerald, 1995, Molkov
et al., 2017, Smith et al., 2007). Historically, the region of the brainstem that control breathing
was found when sections were “extracted” from rabbits until breathing stopped (Legallois,
1813). Over the next century and a half, it was found that respiratory premotor neurons within
the medulla are predominantly found bilaterally in two distinct columns of cells termed the
dorsal respiratory group (DRG) and the ventral respiratory group (VRG) (Duffin, 2004, Feldman
et al., 1985). Respiratory premotor neurons have also been identified in the pons, termed the
pontine respiratory group (PRG) (Duffin, 2004). These respiratory groups coordinate with each
other to generate a continuous breathing rhythm (Fig. 1.3) (Duffin, 2004, Smith et al., 2007).

8
The VRG can be divided into the rostral and caudal regions within the medulla. The caudal VRG
primarily contains expiratory premotor neurons that provide the drive onto respiratory muscles
to contract during expiration (Feldman et al., 1985, Shen and Duffin, 2002). The rostral VRG
(rVRG) can be further subdivided into the rVRG, the Bötzinger complex (BötC) and pre-
Bötzinger complex (preBötC). Neurons in the rVRG are premotor inspiratory neurons with
augmenting activity pattern (ramp-inspiratory neuron) that shape phrenic motor output (Smith
et al., 2007). BötC neurons are primarily inhibitory and project to the VRG and spinal motor
neurons where they are hypothesized to play a critical role in forming the phases of breathing
by acting to initiate expiration by inhibiting premotor and motor neurons (Jiang and Lipski,
1990, Merrill and Fedorko, 1984). The neurons in the preBötC are considered to be the critical
structure for respiratory rhythm as they are both necessary and sufficient for its generation
(Bacak et al., 2016, Gray et al., 1999, Guyenet and Wang, 2001, Johnson et al., 2001, Koshiya
and Smith, 1999, Tan et al., 2008). When preBötC neurons are isolated in vitro, preBötC
neurons continue to fire in a coordinated pattern demonstrating pacemaker-like properties (Del
Negro et al., 2002). Studies in vivo have shown ablation of preBötC neurons produces ataxic
breathing (Tan et al., 2008). This led to the theory that the preBötC is the source of rhythm
generation with neurons showing pre-inspiratory and early-inspiration patterns of activity
(Guyenet and Wang, 2001). However, because animals with the preBötC ablated could still
breathe, in addition to studies showing retrotrapezoid nucleus (RTN) neurons activated prior to
preBötC neurons in an inspiratory pattern (Mellen et al., 2003, Onimaru and Homma, 2003),
other sources may contribute or control the generation of breathing rhythm. The current
hypothesis is that there exist two respiratory rhythm generators; the preBötC generates
inspiratory rhythm and the RTN generates active expiratory rhythm (Janczewski and Feldman,
2006).
The DRG is situated dorsal to the VRG and contains neurons whose activity increases
progressively during inspiration (de Castro et al., 1994). The DRG is involved in sensory afferent
processing and contains the nucleus tractus solitarius (NTS) (de Castro et al., 1994, Ezure and

9
Tanaka, 2000), which is responsible for integration and transmission of signals received from
arterial baroreceptors (i.e. receptors that sense pressure changes in the arterial wall)
(Andresen, 1994), pulmonary stretch receptors (i.e. receptors that detect the physical
distension of the lungs) (Bonham and McCrimmon, 1990), and chemoreceptors (i.e. receptors
that detect changes in the blood such as pH and dissolved CO2 and O2) (Mifflin, 1992). The cells
in this region are critical to the respiratory reflex to terminate inspiration upon sufficient lung
inflation, known as the Hering-Breuer reflex, as inactivation or silencing of cells in this region
abolishes the reflex (Torontali, 2012, Widdicombe, 2001). The NTS is also the first structure to
receive chemoreceptor signals (Mifflin, 1992), acting as a gateway to integrate chemosensory
information (Andresen, 1994, Dampney, 1994).
The PRG is situated in the lateral pons and contains the parabrachial and Kolliker-Fuse nuclei.
The PRG controls the transition from inspiration to expiration and expiration to inspiration as
stimulation of this region switched the phase from inspiration to expiration (Cohen, 1971,
Okazaki et al., 2002). The PRG may also be involved in prolonging inspiration as lesioning these
two nuclei or blockade of neuronal activity extended inspiratory duration (Berger et al., 1978,
Caille et al., 1981). This region may, therefore, act to control inspiratory activity, likely through
its connections with medullary respiratory groups (Duffin, 2004).
The respiratory network coordinates respiratory activity to generate a continuous breathing
rhythm. The network provides continuous adjustments to respiratory output to compensate for
changes or perturbations in the environment that alter breathing rhythm, such as changes in
arousal state, health status associated with disease, posture and phonation (Feldman et al.,
2003). The respiratory network reflexively responds to these perturbations but the respiratory
network can also adapt and exhibit plasticity.

10
Figure 1.3. A schematic of the respiratory control network. Pulmonary stretch receptors (PSRs) provide mechanical feedback to pump cells in the nucleus tractus solitarius (NTS). Excitatory pump cells P(e) activate post-inspiratory (post-I) neurons in the Bötzinger complex (BötC) to inhibit pre-inspiratory/inspiratory neurons (pre-I/I) in the pre-Bötzinger complex (pre-BötC). The inihibition of these neurons decrease ramp-inspiratory neuron (ramp-I) activity in the rostral ventral respiratory group (rVRG) and disfacilitate phrenic nerve (PN) activity and diaphragm muscle contraction. PSRs also provide feedback to inhibitory pump cells P(i) to inhibit early-inspiratory neurons (early-I) in the pre-BötC, which in turn inhibit ramp-I neurons in the rVRG, disfacilitating PN and diaphragm activity. The retrotrapezoid nucleus (RTN) receives chemical feedback to provide a tonic drive onto late expiratory (late-E) neurons within the RTN, which act to activate expiratory neurons in the caudal VRG (cVRG) to activate the abdominal nerve (AbN) and abdominal muscles. The RTN also provides tonic drive onto augmenting-expiratory neurons (aug-E) in the BötC, which inhibit early-I neurons in the preBötC to inhibit inspiration via ramp-I neurons. (Adapted from Molkov et al. 2017).
1.4 Plasticity
Before discussing respiratory plasticity, it is necessary to first establish neuroplasticity in
general. The term “plasticity” originated in 1906 by Italian psychiatrist, Ernesto Lugaro, which
was translated from Italian into English in 1909 (Berlucchi, 2002). In both Italian and English, the
index states “psychic plasticity; plasticity of the neurons; plasticity of the neurofibrils”, and in
later text discusses compensation following brain lesions. Lugaro proposed that prenatal

11
organization of the nervous system can continue throughout life in order to adapt anatomical-
functional connections between neurons (Berlucchi, 2002). The concept that learning and
memory involved changes in the connections between neurons was proposed by Cajal in 1911
(Cajal, 1911), but it was not until 1949 when Donald Hebb refined the concept into a model to
illustrate that synaptic strength could be augmented through repeated use. He postulated that
synaptic modifications occur as a consequence of coincidence between pre- and post- synaptic
activity (Hebb, 1949). It was in 1966-1973 that LTP was discovered and created the basis or
model that underlie learning and memory and launched the field of LTP (Bliss and Lomo, 1973,
Lomo, 1966). Over time, the term “plasticity” has broadened to include various short and long-
term changes, as well as changes occurring in the cell, the synapse, or at the molecular level.
For example, GAP43 is a protein associated with plasticity as it has been linked to the formation
of new synapses (Benowitz and Routtenberg, 1997, Collingridge et al., 1983, Strittmatter et al.,
1992). At the level of the cell, parvalbumin basket cells have been suggested to regulate
plasticity (Karunakaran et al., 2016, Mendez and Bacci, 2011).
Other types of plasticity are also included, such as long-term depression (LTD) induced by
prolonged periods of low-frequency stimulation, opposed to short, high-frequency bursts
required for LTP (Dunwiddie and Lynch, 1978, Kemp et al., 2000, Lee et al., 1998). In this thesis,
I will discuss a type of plasticity within the respiratory control network known as long-term
facilitation (LTF), where repeated respiratory stimuli (e.g. intermittent hypoxia) can induce a
prolonged increase in respiratory nerve or muscle output, such as the phrenic nerve and
diaphragm muscle, respectively.
1.5 Respiratory plasticity
The ability to undergo plasticity and adjust respiratory output is a fundamental characteristic of
the respiratory system. Plasticity within the respiratory system was first noticed when Millhorn
and colleagues (Millhorn et al., 1980a), where they showed that intermittent electrical
stimulation of the carotid sinus nerve (CSN) triggered a prolonged (50-90 minutes) increase in

12
phrenic nerve activity in an anaesthetized cat preparation. At the time, this prolonged increase
in phrenic nerve activity was termed “afterdischarge”, presumably referring to the persistent
discharge in phrenic nerve activity after the stimulus. This was later termed “long-lasting
facilitation” in their subsequent findings (Millhorn et al., 1980b).
Since then, long-lasting facilitation, now referred to as long-term facilitation (LTF), has been
identified in multiple mammals including cats, dogs, goats, rats, mice, and humans (Cao et al.,
1992, Chowdhuri et al., 2008, Griffin et al., 2012, Harris et al., 2006, Hickner et al., 2014,
Millhorn et al., 1980b, Song and Poon, 2017, Tadjalli et al., 2010, Terada et al., 2008, Turner and
Mitchell, 1997), suggesting this form of plasticity is conserved across mammals. It is important
to note that the trigger for respiratory plasticity varied in each animal model. To date, multiple
triggers to induce respiratory motor plasticity have been discovered. The most commonly used
trigger to elicit LTF mimics the original CSN stimulation by delivering 3 episodes of hypoxia (10%
O2), each lasting 5-minutes in duration separated by 5-minutes of normoxic breathing (Bach
and Mitchell, 1996, Fuller et al., 2000, Kinkead et al., 2001). Other triggers for LTF include
variations in the number and/or duration of hypoxic episodes (Cao et al., 1992, Turner and
Mitchell, 1997), repeated loss or suppression of vagus activity (Tadjalli et al., 2010, Zhang et al.,
2003), repeated application of serotonin (Bocchiaro and Feldman, 2004) or noradrenaline
(Neverova et al., 2007) in vitro, or episodic loss of respiratory activity such as that experienced
in neural apneas (Baertsch and Baker-Herman, 2013, Mahamed et al., 2011). The consistent
theme in all triggers is the requirement for an intermittent stimulus (Baker et al., 2001, Baker
and Mitchell, 2000), similar to triggers in forms of plasticity observed in other systems (i.e. LTP)
(Bliss and Lomo, 1973, Huang and Kandel, 1997)
Changes or variations to the intervention can alter aspects of how respiratory motor plasticity
will manifest. For example, the time course of the plasticity (i.e. short-term lasting seconds vs
long-term persisting for hours) can differ depending on the stimulus. Continuous CSN
stimulation triggers short-term facilitation (>3 minutes) post-stimulation (Wagner and Eldridge,
1990) whereas repeated CSN stimulation elicits LTF that persists for more than 60 minutes

13
(Baker and Mitchell, 2000, Olson et al., 2001). Variations to the trigger can also affect the
direction of respiratory motor plasticity (i.e. facilitation or depression). For example, instead of
using repeated bouts of hypoxia, it was demonstrated that 3 episodes of hyperoxic hypercapnia
(i.e., 50% O2, 10% CO2), each 5 minutes in duration separated by 5 minutes of hyperoxic
normocapnia, elicited long-term depression of phrenic nerve activity (Bach and Mitchell, 1998).
The differing results suggest that the respiratory system naturally adapts under various
environmental conditions and exhibits distinct forms of plasticity in response. This thesis will
focus only on one form of respiratory motor plasticity: long-term (>60 minutes) facilitation of
inspiratory genioglossus motor output.
1.5.1 Phrenic LTF
To understand the neural circuit and mechanisms that underlie LTF, it is necessary to first
understand what is known about LTF. To date, the majority of LTF studies focus on phrenic
nerve activity and/or the diaphragm muscle that it innervates. LTF of the phrenic nerve (pLTF)
or diaphragm muscle increases the strength of diaphragm muscle contractions, increasing
airflow into the lungs and therefore ventilation. The mechanisms that underlie pLTF is a
serotonin-dependent mechanism (Fuller et al., 2001, Millhorn et al., 1980b). Systemic delivery
of the serotonergic antagonist, ketaserin, prevents CSN-stimulated induced facilitation of
phrenic nerve activity, but was unaffected by dopaminergic or noradrenergic antagonists,
suggesting serotonin plays a critical role in mediating LTF. The importance of serotonin was
further supported when pLTF was elicited following repeated bouts of hypoxia (3 episodes of
hypoxia at 11% FIO2, each 5 minutes in duration separated by 5 minutes of hyperoxia at 50%
FIO2), and subsequently abolished by systemic pre-treatment with 5-HT2A antagonist (Fuller et
al., 2001) or 5-HT2B antagonist, methysergide (Bach and Mitchell, 1996). This suggests that
intermittent 5-HT2 receptor activation is critical for hypoxia-induced pLTF.
The circuits that cause serotonin release to initiate pLTF have been well elucidated. LTF was
first demonstrated in an anaesthetized cat preparation that stimulation of the raphe obscurus

14
can trigger pLTF (Millhorn, 1986). Specifically, continuous stimulation of the raphe obscurus
triggered pLTF manifesting an increase in tidal volume and breath frequency. This approach
used a continuous stimulus which differed from the intermittent triggers used to induce LTP or
LTF. However, the role of the raphe obscurus was supported when it was demonstrated that
hypoxia activates chemosensory brainstem nuclei that include the ventral medulla which
encompass the medullary raphe (Teppema et al., 1997). In addition, the medullary raphe also
has direct projections to the hypoglossal and phrenic motor nuclei (Dobbins and Feldman,
1994), making the medullary raphe anatomically and functionally positioned to mediate
hypoxia-induced LTF. Most importantly, it was demonstrated that pLTF expression correlated
with an increase in raphe obscurus neuron firing (Morris et al., 2001), again reinforcing the
hypothesis that the raphe to be the source of serotonin mediating pLTF. An increase in activity
was also observed in the inspiratory-augmenting neurons of the rVRG (Morris et al., 2001),
suggesting plasticity within the respiratory network also contribute to pLTF.
In addition to this, pLTF requires new protein synthesis following an intermittent hypoxia
intervention (Baker-Herman et al., 2004, Baker-Herman and Mitchell, 2002, Satriotomo et al.,
2012). Earlier, I mentioned that the production and release of BDNF is regulated by activity
(Isackson et al., 1991, Wetmore et al., 1994, Zafra et al., 1991); BDNF also plays an important
role in mediating plasticity and in this case, pLTF. For example, BDNF activates TrkB receptors
which initiate a signaling cascade through the mitogen-activated protein kinase (MAPK) and
phosphoinositide 3-kinase (PI3K) pathways (Gottschalk et al., 1999). BDNF-induced activation of
MAPK can lead to phosphorylation of synapsin I, which primes synaptic vesicles for release on
the pre and/or post synaptic cell (Valente et al., 2012), allowing for immediate (<15 minutes)
changes at the synapse. Alternatively, BDNF modulates plasticity via BDNF-induced protein
synthesis as LTP was blocked when protein synthesis was inhibited (Scharf et al., 2002).
In the context of LTF, increased levels of BDNF synthesis was observed in the region containing
the phrenic motor pool following intermittent hypoxia and in proportion to the magnitude of
pLTF (Baker-Herman et al., 2004). The importance of BDNF was further supported when

15
blockade of BDNF with interfering RNA or blockade of its receptor (TrkB) prevented hypoxia-
induced pLTF (Baker-Herman et al., 2004). The involvement of BDNF led to further
investigations into the intracellular cascades following TrkB receptor binding, where it can
either initiate a downstream signalling to AKT (i.e. protein kinase B) or extracellular signal-
regulated kinases (ERK), which is also referred to as MAPK. It was determined that pLTF could
be prevented following ERK inhibition but not AKT inhibition (Hoffman et al., 2012), suggesting
that pLTF requires BDNF-TrkB receptor binding to initiate the ERK signalling pathway. How ERK
activation subsequently mediates pLTF is not known, but may involve MAPK-mediated
phosphorylation of synapse I mentioned earlier (see Figure 1.4).
Figure 1.4. Working model of acute intermittent hypoxia-induced pLTF. Acute intermittent hypoxia (AIH) induces release of serotonin from the medullary raphe to activate 5HT2 receptors on phrenic motor neurons, increasing protein kinase C-θ (PKCθ) activity and initiating new BDNF synthesis. TrkB activation by BDNF is necessary for pLTF, and that the relevant TrkB (red) is localized within phrenic motor neurons. Subsequent ERK/MAP kinase activation is hypothesized to facilitate descending respiratory drive through unknown mechanisms that enhance glutamate-mediated excitation. (Adapted from Dale et al. 2017).

16
1.5.2 Hypoglossal LTF
LTF of respiratory motor output occurs in muscles other than the diaphragm. The other most
studied form of LTF is hypoglossal LTF (hLTF), which innervates the genioglossus, hyoglossus
and styloglossus muscles. The genioglossus is of particular importance as it is the largest muscle
in the upper airway that acts to maintain upper airway patency (Sauerland and Mitchell, 1970).
This is particularly important during sleep where there is a reduction in upper airway muscle
tone, which can result in the narrowing of the upper airways and increase the propensity for
upper airway collapse and obstruct the airways (Horner, 1996). This obstruction causes an
apnea which results in a decrease in blood oxygen saturation (hypoxia) and carbon dioxide
buildup (hypercapnia), leading to a reflexive response to increase ventilatory effort (Blanco et
al., 1984, Duffin, 1990, Hirakawa et al., 1997). This eventually leads to arousal to restore muscle
tone and upper airway patency to correct the hypoxia and hypercapnia, only to repeat the cycle
when the patient resumes sleep (Fig. 1.1), as seen in patients with OSA. LTF of the hypoglossal
or genioglossus muscle activity may, therefore, be important in mitigating the reduction in
upper airway muscle tone during sleep. For example, during non-rapid eye movement sleep in
humans, repeated episodes of hypoxia triggered an increase in ventilatory output (vLTF)
(Shkoukani et al., 2002), a decrease in upper airway resistance (Aboubakr et al., 2001,
Chowdhuri et al., 2008, Shkoukani et al., 2002) or an increase in genioglossus muscle activity
(Chowdhuri et al., 2008). In awake humans, intermittent hypoxia triggered LTF of genioglossus
muscle activity and vLTF (Harris et al., 2006). Together, it suggests that hLTF increases the
strength of genioglossus muscle contractions, which can reduce upper airway resistance and
facilitate airflow into the lungs during inspiration. As such, understanding the neural circuits
that underlie plasticity of hypoglossal motor neuron activity could provide an increase in
genioglossus muscle tone that may mitigate the reduction in airway muscle tone and aid
patients with OSA.

17
Figure 1.5. Schematic diagram of human tongue and the muscles innervated by the hypoglossal nerve. The hypoglossal nerve innervates the medial genioglossus (M. Geniogloggus), the largest muscle of the tongue involved in inspiration. The hypoglossal nerve also innervates the medial styloglossus (M. Styloglossus) and medial hyoglossus (M. Hyoglossus), which are involved with swallowing. The vectors represented by solid lines show the direction of the tongue movement produced by contraction of the respective muscle. The dashed vectors are estimates based on anatomical attachment of the tongue muscle fibres (Adapted from Fregosi and Fuller 1997).
The circuit and mechanisms underlying hLTF have not been established. To date, triggers of
hLTF include repeated bouts of hypoxia (Fuller, 2005, Harris et al., 2006), but also hypoxia-
independent stimuli. For example, repeated modulation of vagal feedback by intermittently
cooling the vagus nerve elicits LTF of genioglossus motor output (Tadjalli et al., 2010).
Alternatively, studies using an in vitro preparation of brainstem slices showed repeated
application of serotonergic 5-HT2- (Bocchiaro and Feldman, 2004) or noradrenergic α1-
(Neverova et al., 2007) receptor agonists can induce hLTF. Moreover, hLTF can be elicited by

18
repeated optical stimulation of the A5 or A7 noradrenergic cell groups (Song and Poon, 2017).
Unique to these findings is that the triggers used elicited LTF solely in the hypoglossal /
genioglossus, with no long-term effects on diaphragm activity. Even triggers that induce mild
hypoxia, such as repeated obstructive apneas, can also trigger LTF of genioglossus activity
without long-term effects on diaphragm activity in anaesthetized rats (Ryan and Nolan, 2009,
Song and Poon, 2017, Tadjalli et al., 2010). This suggests that the trigger mechanism underlying
hLTF differs from pLTF as it either operates at different sensitivities or can be elicited with a
hypoxia-independent trigger.
The neural mechanism separating hLTF and pLTF may be due to a difference in the
neurotransmitter released. LTF of the phrenic nerve / diaphragm muscle is serotonin-
dependent (Bach and Mitchell, 1996, Fuller et al., 2001), whereas LTF of the hypoglossal nerve /
genioglossus muscle is noradrenaline-dependent (Huxtable et al., 2014, Tadjalli et al., 2010).
Although hLTF can be elicited by 5HT application under in vitro conditions (Bocchiaro and
Feldman, 2004), it is possible that hLTF was elicited due to the similar mechanisms between 5-
HT receptor activation and noradrenergic receptor activation. Both 5-HT2 and α1-adrenergic
receptors are Gq protein-coupled receptors and their activation have similar intracellular
cascades such as activation of inosotol 1,4,5-triphosphate (IP3) and protein kinase C (PKC). In
fact, α1-adrenergic receptor activation at the phrenic motor pool can be used to elicit pLTF, but
systemic blockade of α1-adrenergic receptors does not prevent hypoxia-induced pLTF (Huxtable
et al., 2014). In comparison, systemic 5-HT2A receptor blockade prevented apnea-induced hLTF
(Huxtable et al., 2014, Tadjalli, 2012), but blockade of 5-HT2A receptors at the level of the
hypoglossal motor pool did not prevent apnea-induced hLTF (Tadjalli et al., 2010). Although
there may be some degree of cross-talk between the noradrenergic and serotonergic
neurotransmitters systems in mediating LTF, there is a clear distinction between the
neurotransmitter mechanisms that are essential for the elicitation of pLTF versus hLTF. Direct
stimulation of noradrenergic cell groups that project to the hypoglossal motor pool (i.e. A5 or
A7) alone can also trigger hLTF (Song and Poon, 2017), further supporting the concept that
noradrenaline is the key neurotransmitter mediating hLTF (Fig. 1.6). This separation from pLTF

19
is further emphasized by the fact that there is little to no noradrenergic input from the
brainstem to phrenic motor neurons (Dobbins and Feldman, 1994). However, this does not
nullify the role of serotonin on hypoglossal motor neurons nor noradrenaline on phrenic motor
neurons; both modulate motor neuron activity, respectively.
The source of noradrenaline involved in hLTF has not been fully elucidated, although the source
of serotonin acting on phrenic motor neurons to elicit pLTF has been suggested to originate
from the medullary raphe (Bach and Mitchell, 1996, Fuller et al., 2001, Millhorn, 1986). The
sources of noradrenaline acting on hypoglossal motor neurons have been suggested to arise
from the A1 (18.5% of the noradrenergic input to hypoglossal motor neurons arise from the
A1), A5 (43.5%), A6 or LC (1.7%), A7 (15.0%), and the subcoeruleus (21.0%) (Fig. 1.6) (Aldes et
al., 1992, Rukhadze and Kubin, 2007). The release of noradrenaline, presumably from these cell
groups, provide the tonic noradrenergic drive on hypoglossal motor activity as blockade of α1-
adrenergic receptors at the level of the hypoglossal motor pool reduce the amplitude of
inspiratory genioglossus motor activity (Chan et al., 2006). The LC is of particular interest as it
considered the largest source of noradrenaline in the brain (Moore, 1979). Although the LC was
reported to provide only 1.7% of the noradrenergic input to the hypoglossal motor pool
(Rukhadze and Kubin, 2007), the LC is dorsal to the subcoeruleus and together is referred to as
the “dorsal noradrenergic bundle” (Stanton and Sarvey, 1985). Studies of plasticity have shown
noradrenaline to play a critical role in the manifestation of LTP. Specifically, ablation of the
dorsal noradrenergic bundle prevented LTP in the dentate gyrus following intermittent
stimulation (Stanton and Sarvey, 1985). This further supports the concept that noradrenaline is
a neuromodulator that can promote or induce plasticity.

20
Figure 1.6. LTF of genioglossus motor output induced by intermittent apneas. (A) Example trace showing repeated obstructive apneas lasting 10–15 seconds in a urethane-anesthetized, vagi-intact, and mechanically ventilated rat eliciting a reflexive increase in the amplitude of integrated genioglossus motor activity (∫GG EMG) during each apnea (denoted by dots above the ∫GG EMG recording). Following 10 apneas, a sustained facilitation of ∫GG EMG amplitude was observed above baseline denoted by dashed red line, evidence of long-term facilitation (LTF). Integrated diaphragm motor activity (∫Dia EMG) was unaffected. (B) Brain map showing the approximate location of the A1, A5, locus coeruleus (LC), A7, nucleus tractus solitaris (NTS) and hypoglossal motor pool (XII), highlighting afferents and efferents (red arrows) to the hypoglossal and LC. Insert provides expanded view of the brainstem nuclei and noradrenergic structures potentially involved in mediating hLTF (Adapted from Song and Poon 2017).
1.6 How noradrenaline induces plasticity
LTF has been considered to be a serotonin-dependent form of plasticity due to numerous
studies showing pLTF to require serotonin. However, unlike pLTF, noradrenaline is required for
LTF of the upper airways (Huxtable et al., 2014, Tadjalli et al., 2010). This distinction is
supported anatomically as noradrenergic cells innervate the hypoglossal motor pool (Aldes et

21
al., 1992, Rukhadze and Kubin, 2007) but few if any project to the phrenic motor pool (Dobbins
and Feldman, 1994). Since α1-adrenergic receptor activation is necessary for apnea-induced
hLTF (Tadjalli et al., 2010), it is necessary to understand how noradrenaline can induce
plasticity.
Noradrenaline can mediate three types of plasticity: developmental (which will not be
addressed in this thesis), intrinsic (modulating the excitability of a neuron), or synaptic
(modulating activity at the level of the synapse). Noradrenaline mediates these changes via
ligand-binding to two primary receptor subtypes: α and β. Within hypoglossal motor neurons
only α receptors are expressed, specifically excitatory α1-adrenergic receptor and inhibitory α2-
adrenergic receptors (Volgin et al., 2003, Volgin et al., 2001). This thesis will only focus on α
receptor binding on hypoglossal motor neurons.
Noradrenergic α receptors are primarily divided into two classes: α1 and α2. α1-adrenergic
receptor activation can induce plasticity synaptically or intrinsically on the post-synaptic neuron
(Jones et al., 1985). Changes at the synapse are induced when noradrenaline acts on α1-
adrenergic receptors. For example, noradrenaline potentiates the excitatory actions of
glutamate on motor neurons (Katakura and Chandler, 1990, Kiehn et al., 1999). The mechanism
underlying this potentiation is hypothesized to involve Gq protein-mediated activation of
phospholipase C β (PLC β) (Jiao et al., 2002). This in turn can generate the second messengers
inositol-(1,4,5)-trisphosphate (IP3) and diacyl-glycerol (DAG). IP3 causes the release of
intracellular Ca2+, which together with DAG activates protein kinase C (PKC) (Zhong and
Minneman, 1999). The activation of PKC causes AMPA receptor phosphorylation and is the
hypothesized mechanism that potentiates glutamate-evoked cell firing (Feldman et al., 2005,
Neverova et al., 2007). The activation of DAG and subsequently PKC can also increase protein
synthesis of BDNF (Juric et al., 2008), which in turn can lead to the insertion of new ion
channels at the synapse (Itami et al., 2003) (Fig. 1.7).

22
Intrinsic changes to the post-synaptic cell also occur following α1-adrenergic receptor
activation. Activation of α1-adrenergic receptors inhibit TASK-1 potassium leak channel to
increase motor neuron excitability (Talley et al., 2000), and in hypoglossal motor neurons, α1-
adrenergic receptor stimulation can increase motor neuron excitability by increasing the input
resistance. This may be mediated by a reduction in a resting potassium current and activation
of a barium-insensitive inward current (Parkis et al., 1995). Together with changes at the
synapse, these mechanisms may increase the excitability of the post-synaptic cell (Fig. 1.7).
α2-adrenergic receptors are located on both pre- and post- synaptic sites and can modulate cell
activity at either site intrinsically (Aoki et al., 1994). Binding of α2-adrenergic receptor initiates a
Gi/o protein-mediated signalling cascade that can hyperpolarize the cell through the opening of
inwardly rectifying potassium channels (Surprenant and North, 1988), the activation ATP-
dependent potassium channels (Zhao et al., 2008), or through the inhibition of voltage-sensitive
calcium channels by (DeBock et al., 2003). These mechanisms all contribute to the reduction of
neurotransmitter release following α2-adrenergic receptors activation (Fig. 1.7).

23
Figure 1.7. Schematic of the signalling cascade following noradrenaline-binding to α1- or α 2- adrenergic receptors. Binding of noradrenaline (NA) to α1-adrenergic receptors (top) can depolarize the cell membrane by triggering the G protein-mediated activation (Gq) to inhibit TASK-1 potassium leak channels, as well as activate barium-insensitive inward currents. Activation of the Gq pathway also triggers the activation of phospholipase C β (PLC β). This activates diacylglycerol (DAG) and produces inositol triphosphate (IP3) which causes release of calcium from intracellular stores. Both contribute to the activation of protein kinase C (PKC) which can phosphorylate AMPA-receptor subunits to potentiate glutamate-evoked action potentials. PKC activation can also increase the synthesis of brain-derived neurotrophic factors (BDNF), which bind to TrkB receptors where it in turn can lead to the insertion of new ion channels. Binding of NA to α2-adrenergic receptor (bottom) activates the G protein-mediated inhibition (Gi/o) to increase potassium conductance via ATP-dependent potassium channels, as well as inwardly rectifying potassium channels. Initiation of the Gi/o signalling cascade also suppresses voltage-activated calcium channels. (Modified from Marzo et al.2009).
1.7 Noradrenaline and hypoglossal LTF
To understand how noradrenaline acts on hypoglossal motor neurons to induce plasticity, it is
necessary to understand the physiology of hypoglossal motor neurons themselves. The
hypoglossal nuclei are bilateral structures situated along the midline in the caudal brainstem

24
directly below the fourth ventricle and central canal. In rats, the hypoglossal nuclei extend
approximately 2 mm rostral-caudal and send descending axons to form the twelfth (XII) cranial
nerve. Currently, there are two known distinct types of neurons within the hypoglossal motor
pool: the motor neurons which drive contraction of respiratory muscles such as the
genioglossus, and the interneurons that modulate its activity, likely via inhibitory inputs (Boone
and Aldes, 1984, Peever et al., 2002). Estimations have placed 95% of the population to be
motor neurons and 5% to be interneurons (Sawczuk and Mosier, 2001). The activity of these
neurons control the dilation of upper airways muscles during inspiration in eupneic breathing,
as well as under an anaesthetized, tracheostomized, spontaneously breathing condition
(Fregosi and Fuller, 1997). The inspiratory drive on hypoglossal motor neurons is glutamatergic,
originating from the lateral tegmental field (Peever et al., 2002) and the rhythm generator (i.e.
preBötC) (Li et al., 2003), and act primarily through AMPA and NMDA receptors, both of which
are expressed on hypoglossal motor neurons (G.D. et al., 1993). Noradrenergic input onto the
hypoglossal motor neurons likely act through α1-adrenergic receptors as they are the most
highly expressed (Rukhadze et al., 2010, Volgin et al., 2001).
In the context of respiratory motor plasticity, direct evidence demonstrating noradrenaline to
be critical in LTF of hypoglossal/genioglossus activity have been observed in vitro and in vivo.
Repeated application of phenylephrine to brainstem slices elicits LTF of the hypoglossal nerve
(Neverova et al., 2007). Specifically, they found that episodic, not continuous activation of α1-
adrenergic receptors must act through protein kinase C to elicit a prolonged increase in
hypoglossal nerve activity. Alternatively, in an in vivo approach, repeated apneas delivered to
an anaesthetized, spontaneously breathing rat model can induce LTF of genioglossus motor
output but was completely abolished upon α1-adrenergic receptor blockade at the level of the
hypoglossal motor pool (Tadjalli et al., 2010). Taken together, it suggests that noradrenaline can
induce hLTF. However, neither study provides any insight into how noradrenaline may be
mediating hLTF.

25
Noradrenaline may be mediating hLTF through α1-adrenergic receptor activation. Hypoglossal
motor neurons primarily express α1-adrenergic receptors (Rukhadze et al., 2010, Volgin et al.,
2001) and α1-adrenergic receptor activation can induce plasticity in other systems (Mouradian
et al., 1991). Furthermore, in direct context of respiratory plasticity, α1-adrenergic receptors
increase expression at the hypoglossal motor pool following chronic intermittent hypoxia,
increasing the endogenous excitatory drive onto hypoglossal motor neurons (Rukhadze et al.,
2010, Stettner et al., 2012). Direct application of phenylephrine induces LTF in vitro by
potentiating AMPA-mediated currents on hypoglossal motor neurons (Feldman et al., 2005).
This suggests that noradrenaline-induced plasticity may be occurring via changes on the
synapse at the level of the hypoglossal motor neuron through AMPAR-mediated changes.
However, it is also possible that the intrinsic excitability of the hypoglossal motor neuron is
mediating hLTF. For example, input resistance was increased on hypoglossal motor neurons
following application of noradrenaline (Parkis et al., 1995), requiring less current to induce
repetitive firing. This mechanism is hypothesized to act through reduction in Ba-sensitive
potassium channels and activating Ba-insensitive inward current carried by sodium ions. hLTF
could, therefore, be a result of noradrenaline inducing both intrinsic and synaptic plasticity at
the level of the hypoglossal motor pool.
1.8 Neural circuit underlying hypoglossal LTF
To date, the neural circuit underlying hypoglossal LTF has not been elucidated. The known
neural circuit involves the NTS (Torontali, 2012) and the activation of α1-adrenergic receptors
on hypoglossal motor neurons (Tadjalli et al., 2010). The hypoglossal motor neuron must in turn
trigger muscle contraction of the genioglossus muscle. The hypoglossal motor pool is,
therefore, a fundamental part of the hLTF circuit. The source of noradrenaline however,
remains unknown. Endogenous noradrenergic drive play a defined role in facilitating motor
output from hypoglossal motor neurons during wakefulness, sleep and during anaesthesia
(Chan et al., 2006). The source of noradrenaline could arise from one or more noradrenergic
cell groups that project to it. For example, the source of noradrenaline that mediates hLTF may

26
originate from the A5 and/or A7 (Song and Poon, 2017). Specifically, intermittent apneas
increase c-Fos expression at the A5 and A7, and intermittent optical stimulation of these
regions triggered an increase in inspiratory genioglossus motor output persisting for 20 mins. In
addition, carbachol-induced “REM sleep” decreased A5 and A7 activity which correlated with a
decrease in hypoglossal nerve activity (Fenik et al., 2002, Fenik et al., 2008), suggesting the A5
and A7 may be positioned to provide the noradrenergic drive onto hypoglossal motor neurons
to trigger hLTF. However, the A5 may not act on hypoglossal motor neurons as the cells that
exhibited a reduction in activity did not project to hypoglossal motor nucleus as determined by
antidromic mapping (Fenik et al., 2002).
Alternatively, the LC also has direct projections to the hypoglossal motor pool and can
modulate respiratory activity (Aldes et al., 1992, Cedarbaum and Aghajanian, 1978, Hakuno et
al., 2004, Rukhadze and Kubin, 2007). For example, an increase in inspired CO2 increases LC
activity, suggesting the LC to be involved in chemoreception (Coates et al., 1993, Gargaglioni et
al., 2010, Haxhiu et al., 1996, Oyamada et al., 1999, Teppema et al., 1997). In fact, lesioning of
the LC decreases the hypercapnic ventilatory response (Biancardi et al., 2008, Li and Nattie,
2006), and prevents noradrenaline-induced increases in respiratory activity (Hilaire et al., 2004,
Oyamada et al., 1999). This suggests that the LC is capable of modulating respiratory output.
This was further supported when a reduction in LC activity correlated with REM sleep, and REM
sleep correlated with a reduction in upper airway muscle tone (Aston-Jones and Bloom, 1981,
Nitz and Siegel, 1997), suggesting LC activity may be involved in the reduction of muscle tone
during REM sleep. This connection was again supported when it was shown that LC inactivation
with tetrodotoxin reduced hypoglossal nerve firing rate in an isolated brainstem-spinal cord
preparation, and electrical stimulation of the LC under the same preparation increased the
firing rate (Hakuno et al., 2004). Together, it suggests that the LC may contribute to the
reduction of upper airway muscle tone during REM sleep. Although this correlation does not
directly implicate the LC, markers for cell injury in LC neurons following prolonged exposure to
intermittent hypoxia has been observed (Zhu et al., 2007), suggesting hypoxia experienced by
OSA patients may have added comorbidities that may circumvent the LC’s role in facilitating

27
upper airway motor plasticity. Taken together, this suggests that the LC has the potential to
induce or promote respiratory motor plasticity.
Aside from the noradrenergic input required for hLTF, which could originate from the A5, A7, or
LC, there is evidence to suggest other structures are involved in the neural circuit mediating
hLTF. The triggers to induce hLTF (e.g. repeated bouts of hypoxia, repeated apneas, or repeated
modulation to vagal feedback) activate the chemosensory feedback (by hypoxia or apneas)
and/or the broncho-pulmonary feedback (by apneas or vagal modulation) systems. The latter is
of particular importance since the vagal afferents that deliver broncho-pulmonary feedback
have been shown to terminate in the NTS (Kalia and Sullivan, 1982), and pharmacological
inactivation of NTS cells prevented the expression of hLTF following repeated apneas (Torontali,
2012). In addition, LTF of genioglossus motor output can be triggered by repeated modulation
to vagal feedback alone (Tadjalli et al., 2010). Together, this suggests that the NTS is a critical
component of the hLTF circuit, providing a basic layout of the hypothesized neural circuit
underlying hLTF (Fig. 1.8).
Figure 1.8. Hypothesized circuit responsible for hypoglossal LTF. Repeated obstructive apneas modulate vagal afferent activity, which terminates in the nucleus tractus solitarius (NTS). Cells in the NTS send projections to and activate noradrenergic cell group(s), which in turn extend axons directly to the hypoglossal (XII) motor pool to modulate hypoglossal (and therefore genioglossus) activity, effectively triggering hypoglossal long-term facilitation (hLTF). I hypothesize that this is the neural circuit underlying LTF of inspiratory genioglossus motor output.

28
1.9 Experimental objectives
The above evidence supports the working hypothesis that noradrenaline, the NTS, and the
hypoglossal motor pool are all critically important for the manifestation of hLTF. However, what
remains unknown is the source of noradrenaline, the circuit that mediates hLTF, and how these
structures work together within this proposed circuit. The goal of this thesis is to, therefore,
determine the neural circuit and mechanism underlying LTF of inspiratory genioglossus motor
output. I propose that the current hypothesized circuit involves recurrent apneas acting
through vagal afferents terminating in the NTS, which in turn activates noradrenergic
structure(s) to episodically release noradrenaline onto hypoglossal motor neurons to induce
plasticity. I will test this hypothesis in the following research objectives:
Objective 1 (Chapter 3): To determine the brainstem structures activated by apnea-induced
hLTF.
Objective 2 (Chapter 3): To determine anatomical connections between the noradrenergic
neurons of the locus coeruleus and the hypoglossal motor pool.
Objective 3 (Chapter 3): To determine if the locus coeruleus is a critical component of the
neural circuit mediating apnea-induced hLTF.
Objective 4 (Chapter 4): To determine whether optogenetic manipulation of channelrhodopsin
(ChR2) -expressing locus coeruleus neurons alone can elicit hLTF.
Objective 5 (Chapter 4): To determine whether optical silencing of halorhodopsin (eNpHR) -
expressing locus coeruleus neurons prevent apnea-induced hLTF.
Objective 6 (Chapter 5): To determine whether noradrenaline released specifically from the
locus coeruleus is the underlying mechanism that mediates hLTF.

29
Chapter Two – Materials and Methods
2.1 Animals
Experiments were performed on anaesthetized, spontaneously breathing adult male Sprague-
Dawley rats. A total of 107 rats, 447 ± 58 g, aged 8-12 weeks, were included in this study. Rats
were shipped from Charles River Laboratories (Wilmington, MA) and housed at the University
of Toronto Cell and Systems Biology Animal Bioscience Facility. Rats were housed in pairs with
unlimited access to food and water in room temperature on a 12:12 hour light-dark cycle.
Animals were given minimum 1 week to acclimatize to housing conditions upon arrival before
any experimental procedures were performed. All experimental procedures in this study were
performed in accordance with both the Canadian Council on Animal Care and University of
Toronto Animal Care Committee.
2.2 Drug and tracer preparation
All drugs were made on the day of experiments; drugs were dissolved in lactated Ringer’s then
filtered (0.2 μm nylon; Thermo Fisher Scientific). Clonidine (clonidine hydrochloride; 266.55 FW;
Sigma-Aldrich), an α-2 noradrenergic auto-receptor agonist, was delivered through a 28-gauge
stainless steel cannula via microinjection of 200 nL over 2 minutes at 4.8 µg/mL. This
concentration has been shown to be effective at reducing cortical noradrenaline levels by more
than 60% (Sakamoto et al., 2013), which is sufficient at affecting LC-dependent behaviours
(Mair et al., 2005). Terazosin (terazosin hydrochloride; 423.80 FW; Sigma-Aldrich), an α1
noradrenergic receptor antagonist, was delivered through reverse-microdialysis at 1 μM
perfusing at 2 μL per min at the LC. This concentration was also chosen as it was used
previously in the lab to show efficacy at preventing apnea-induced hLTF (Tadjalli et al., 2010)
without affecting baseline genioglossus activity (Tadjalli, 2012).
Cholera toxin B (CtB) is a neuroanatomical tracer that is taken up at the site of injection and
retrogradely labels cells that project to the target site. Here, CtB was used to determine the
projections to the hypoglossal motor pool. CtB was chosen because it is currently available

30
conjugated with Alexa Fluor 488, which is a fluorescent tag that has shown to be bright and
more photostable than other fluorescent dyes conjugated to other neuroanatomical tracers
(Panuchuk-Voloshina et al., 1999). CtB was reconstituted in sterile phosphate buffered saline
the day of use (Conte et al., 2009).
In contrast, an adeno-associated viral vector (AAV-hSyn-ChR2(H134R)-mCherry) was used to
trace anterograde projections from the LC to the hypoglossal motor pool to verify CtB results.
Although an AAV viral vector is not inherently an anterograde tracer, it provides clear
visualizations of axonal projections (Hunanyan et al., 2013, Muzerelle et al., 2016).
2.3 Surgical procedures
Animal were weighed before each surgery. Anaesthesia was introduced by placing rats into an
induction chamber with 3.5% isoflurane in a 50/50 oxygen nitrogen mix and maintained via a
nose cone at 3% isoflurane. In all experiments, rectal temperature was monitored and
maintained at 37.5 ± 0.5°C via a servo-controlled heating pad (09585; FHC, Bowdoinham, ME,
or TC-1000; CWE Inc.) throughout surgeries and experimental recordings. After complete
absence of corneal and foot-withdrawal reflexes, a tracheostomy was performed where a
midline ventral incision was made to expose the trachea and a custom-made silicone T-tube
cannula was inserted just below the larynx. Anaesthesia was maintained through the T-tube for
the remainder of the experiments at 2-2.5% isoflurane set to a flow rate of 1 L per min. To
prevent the accumulation of mucosal secretions that may occlude the tracheal T-tube, a
subcutaneous injection of atropine sulfate (0.4 mg/kg) was administered. Airway obstructions
were introduced by occluding the custom T-tube cannula with hemostats. The jugular vein was
cannulated for administration of fluids (lactated Ringer’s solution) at a rate of 1.5 ml per hour.
Lactated ringer’s solution was administered by a way of pump driver (Hive Syringe Pump
Controller, MD-1020, BASi). To record upper airway respiratory motor activity, two needle
electrodes (F-E2; Grass Technologies) were inserted into the genioglossus muscle, with one
electrode on either side of the muscle. To record diaphragm EMG activity, a 1-2 cm midline

31
abdominal incision was made and a custom-made bipolar electrode was fastened onto the
fascia of the right diaphragm. All incisions were closed with 9mm wound clips (Becton
Dickinson) to prevent tissue desiccation.
2.3.1. Stereotaxic injection (virus / tracer)
In some experiments, stereotaxic surgery was performed on animals to introduce an adeno-
associated virus (AAV) or a neuronal retrograde tracer into the locus coeruleus (LC) or
hypoglossal motor pool. Animals were placed in a stereotaxic setup (David Kopf Instruments)
with their heads secured with ear bars and a snout clamp. Animals were draped and had their
eyes covered with an ophthalmic ointment to prevent drying. All stainless surgical instruments
are autoclaved prior to surgery. When performing multiple surgeries, tools are sterilized
between surgeries with a dry bead sterilizer for minimum 15 seconds, 1 minute for items larger
than forceps/scissors. A 1:16 dilution of Accel is used as a surface disinfectant. A 2 cm midline
incision was made onto the skin on the dorsal surface of skull. Hydrogen peroxide and saline
was used to remove overlying connective tissue and to expose bregma and lambda. To level the
skull, a digital reader (David Kopf Instruments) was used to ensure ±0.01 mm accuracy between
bregma and lambda. Burr holes were drilled (TX Series, Foredom Electric Co.) at the surface of
the skull to expose the dura, bilaterally above the LC at coordinates (relative to bregma) 10.0
mm posterior, 1.4 mm lateral, 7.5 mm ventral, or unilaterally above the hypoglossal motor pool
(AP 14.5 mm, ML 0.2 mm, DV 9.0 mm). Coordinates were guided by the stereotaxic brain atlas
by Paxinos and Watson (1998). The dura was then punctured using a 25-gauge sterile
hypodermic needle. Bleeding caused by puncturing the dura ceased after applying pressure
with a sterile cotton swab on the burr hole. A stainless steel 28-gauge cannula connected to a
digital microinjection syringe pump (Pump 11 Elite; Harvard Apparatus) was then lowered to
the target region to deliver 600 nL of either AAV5-hsyn-ChR2(H134R)-mCherry (4.1x10^12
vg/mL), AAV5-hsyn-eNpHR3.0-mCherry (6.7x10^12 vg/mL), or AAV5-hsyn-mCherry (3.4x10^12
vg/mL), purchased from the University of North Carolina Vectorcore. For retrograde tracing,
200 nL of CtB was injected into the hypoglossal motor pool. After microinjection, the incision

32
was sutured and post-operative care was given. Animals injected with a viral vector given for 3-
4 weeks for recovery and to allow for gene expression before experiments began. Animals
injected with CtB were killed after 10 days with an overdose of isoflurane and perfused with 4%
paraformaldehyde.
2.3.2 Drug delivery
In some experiments, a drug was delivered to the LC or hypoglossal motor pool through
microinjection or perfusion through reverse microdialysis. To do this, animals were surgically
instrumented for stereotaxic injections (See section 2.3.1). Microinjection was performed using
a stainless steel 28-gauge cannulas connected to a 1 mL gastight syringe (MD00500 Gastight
Syringes, BASi) with FEP Teflon tubing (inner diameter of 0.12 mm; Eicom). The cannula was
lowered into the LC to deliver the drug or vehicle solution at a rate of 0.1 μL per min.
Alternatively, reverse microdialysis was performed using a microdialysis probe (6000 Da cut-off
membrane: 1 mm long × 250 μm wide; CMA) connected to a 1 mL gastight syringe (MD00500
Gastight Syringes, BASi) with FEP Teflon tubing (inner diameter of 0.12 mm; Eicom). The probe
was lowered into the hypoglossal motor pool to perfuse Terazosin (1 µM) at a rate of 2 µL per
min for 20 minutes prior to any intervention. In both cases, drug delivery was controlled via a
syringe pump driver and controller (Hive Syringe Pump Controllers, MD-1020, BASi) and
cannula placements was verified by post-mortem histology.
2.3.3 Optogenetic manipulations
Optogenetic manipulations involved the use of optic fibres to deliver light to targeted brain
regions expressing ChR2 or eNpHR, such as millisecond control of neuronal activity could be
manipulated. In some experiments, optogenetic stimulation or inhibition was performed using
473 nm wavelength laser system (LRS-0473, Laserglow) or a 532 nm wavelength laser system
(LRS-0532, Laserglow), respectively. Each laser system was connected to a mono fiberoptic
patchcord (MFP-200/230/900-0.37-2m-FC-ZF1.25(F), Doric Lenses), which was connected to a
custom made optic implant that consisted of an optic fibre (200 nm diameter, ThorLabs). Only

33
optic implants that provided a circular light path with no visible light diffractions were accepted
for experimental use. Custom optic implants were made by connecting optic fibre to a ceramic
ferrule (MM-FER2007C-2300, Precision Fibre Products) using epoxy. The length of the optic
implant was measured to reach 7.5 mm ventral to bregma such that the optic probe tip would
presumably be at the top of the target site (i.e., locus coeruleus). Optic probe tip would be
inserted past the target site by approximately 0.1-0.2 mm to verify probe tip location in post-
mortem histology then retracted. Only light output that was greater than 25 mW and less than
50 mW measured at the optic fibre tip using a power meter (PM100A, ThorLabs) were used for
experiments. This power output is higher compared to recent reports on optical LC stimulation
in mice which used 20 mW (Carter et al., 2010) or 10-12 mW (Wang et al., 2014). At 25-50 mW,
there is potential for heat-induced cell damage (Qian and Gu, 2005), heat-induced cell firing
(Reig et al., 2010, Stujenske et al., 2015), and photodilation of blood vessels (Rungta et al.,
2017). Despite these potential side effects, I chose this power output to ensure sufficient ChR2
activation. The amount of heat produced is dependent on the size of the optic fibre, the
duration of light-exposure, and the wavelength of light (Gysbrechts et al., 2016, Stujenske et al.,
2015). To reduce potential side effects caused by heat production, I used a 200 µm optic fibre
to deliver light in 5 ms pulses at 5 Hz for 15 seconds, which has been reported to produce a
0.005ᵒC increase in temperature (Anikeeva et al., 2011). This value is within the range of the
natural fluctuations observed in the awake rat brain (Shirey et al., 2015). Unfortunately, the
effects of light in naïve mice on cerebral blood flow has been reported to occur at levels as low
as 1 mW (Rungta et al., 2017) and was, therefore, not avoided in these experiments. For
optogenetic stimulation and inhibition protocols, see sections 2.6.4 and 2.6.5.
2.4 Electrophysiology recordings
Genioglossus and diaphragm EMG signals were amplified between 500-2000 Hz using a Super-Z
High Impedance Head Stage (cat# 10-02010, CWE Inc.) and a BMA-400 AC/DC Bioamplifier
(cat#09-03010, CWE Inc.). Signals were filtered with a bandpass between 1-3000 Hz for EMG
signals sampled at 1000 Hz. End tidal CO2 and temperature measurements were sampled at

34
40Hz (Spike2 software, 1401 Interface; CED) and digitized (1 kHz; Micro1401; Cambridge
Electronic Design). Integrated respiratory EMG activities were quantified using Spike2 software
(Cambridge Electronic Design). All signals were stored on a computer for offline analysis.
2.5 Measurement of ET-CO2 and O2 saturation
End-tidal CO2 (ET-CO2) was monitored in real-time using a calibrated fast response CO2 analyzer
(Model 17630; VacuMed or MicroCapster Endtidal CO2 analyzer, CWE Inc.) connected to the
tracheal T-tube. End-tidal CO2 monitor was calibrated using carbagen (5% CO2 in 95% O2) before
every experiment. Arterial O2 saturation was measured using a pulse oximeter designed for
rodents, connected to the hind-paw of the animal (MouseOx Pulse Oximeter; STARR Life
Sciences Corp.) WINDAQ Waveform Browser software (Dataq Instruments) was used to digitize
and analyze O2 saturation signals, which were then recorded using Spike2 software. Both
variables were analyzed and quantified offline using Spike2 software.
2.6 Experimental protocol
After each experimental paradigm’s surgical intervention, animals were left to stabilize for 60
minutes to establish a baseline activity for the genioglossus and diaphragm EMG amplitude, ET-
CO2, and O2 saturation. After a stable baseline is established, specific experimental protocols
were executed (e.g. repeated obstructive apneas). After each intervention, physiological
variables were recorded for an additional 60-90 minutes. Control experiments underwent an
identical procedure with vehicle solutions or control viral vectors. Furthermore, an absence of
an intervention was included as well to control for time-dependent fluctuations in variables
measured.

35
2.6.1 Objective 1 – To determine the brainstem structures activated alongside apnea-induced
hLTF
To reaffirm that repeated obstructive apneas can trigger long-term facilitation of genioglossus
motor activity (hLTF), genioglossus and diaphragm EMG activity was recorded from
anaesthetized, spontaneously breathing rats (n=14). After a baseline was established, a
repeated apnea protocol was performed (Fig. 2.1). This included 10 apneas, each 15-seconds in
duration separated by 1-minute recovery. Apneas were triggered during end-expiration in order
to mimic the obstruction pattern experienced in OSA patients (Sanders and Moore, 1983,
Sanders et al., 1985). Following repeated apneas, genioglossus and diaphragm EMG, ET-CO2 and
O2 saturation was recorded over 60-90 minutes. Time matched control group of animals
without exposure to repeated apneas (n=10) were used to account for the effects of the
anaesthetic and surgical intervention over the duration of the recording period. At the end of
the recording period, the animal was killed by isoflurane overdose and transcardial perfusion.
All animals perfused were used for analysis.
Figure 2.1. Protocol for the delivery of repeated apneas in Objective 1.
To determine whether brainstem structures (noradrenergic or otherwise) were activated by
apnea-induced hLTF, rats were divided into 3 groups: rats that exhibited apnea-induced hLTF
(n=5), non-responders (i.e., rats that did not exhibit hLTF following the repeated apnea
protocol) (n=5), and time matched controls (i.e., without apneas) (n=5). All brains were
sectioned and stained for c-Fos, a neuronal marker for cell activation (Haxhiu et al., 1996,
Kaliszewska et al., 2012, Lim and Veasey, 2010, Teppema et al., 1997), and tyrosine hydroxylase
expression to identify noradrenergic neurons.

36
2.6.2 Objective 2 – To determine the anatomical connection between the noradrenergic locus
coeruleus neurons and the hypoglossal motor pool
Previous studies investigating the anatomical connection between the LC and the hypoglossal
motor pool initially reported that cells in the LC (noradrenergic or otherwise) do not project to
the hypoglossal motor pool (Aldes, 1990, Aldes et al., 1992, Aston-Jones et al., 1970, Fritschy
and Grzanna, 1990, Levitt and Moore, 1979). However, more recent studies suggest
approximately 1.7% of LC neurons project to the region of the hypoglossal motor pool
(Rukhadze and Kubin, 2007). Furthermore, a decrease in LC activity was observed during REM
sleep (Aston-Jones and Bloom, 1981), and a decrease in genioglossus activity was also observed
during REM sleep [23]. Taken together, I hypothesize that LC activity contributes to
genioglossus activity, and that there is an anatomical connection between the LC and
hypoglossal motor pool. To determine whether LC neurons have direct axonal projections to
the hypoglossal motor pool, rats (n=6) were unilaterally injected with a retrograde tracer, CtB,
into the hypoglossal motor pool. A control injection (n=7) was performed by injecting CtB
ventral to the hypoglossal motor pool. Ten days were given for CtB to retrogradely label cells
before the animal was killed by isoflurane overdose and transcardial perfusion. Tissue was then
stained for tyrosine hydroxylase (TH) to determine whether noradrenergic cells of the LC are
colocalized with CtB. Cells were counted manually using an upright fluorescent microscope
(AxioImager Z1; Zeiss). To further verify the anatomical connection between the LC and the
hypoglossal motor nucleus, an AAV was injected into the LC and allowed to express over 3-4
weeks post injections. The brains were later imaged to determine the presence of axonal
projections at the level of the hypoglossal motor.
2.6.3 Objective 3 – To determine whether the locus coeruleus is a critical component of the
neural circuit mediating apnea-induced hLTF
To determine whether the LC is critical for the manifestation of hLTF following a repeated
apnea protocol, I bilaterally inactivated the LC to prevent apnea-induced hLTF. Rats (n=14) were
injected with 200 nL of clonidine (4.8 µg/mL) (Mair et al., 2005, Sakamoto et al., 2013) or

37
vehicle solution (i.e., lactated Ringer’s) into the LC at 0.1 µL/min over 2 minutes, followed by
repeated obstructive apnea protocol (Fig. 2.2). Genioglossus and diaphragm EMG, ET-CO2 and
O2 saturation was recorded over 60 minutes prior to clonidine application or vehicle solution to
establish a baseline. After administration of clonidine, another 30 minutes was recorded for a
second baseline under the influence of clonidine before performing repeated apneas, and
subsequently recorded for another 60-90 minutes before the animal was killed by isoflurane
overdose and transcardial perfusion.
Figure 2.2. Protocol for clonidine intervention followed by repeated apneas in Objective 3.
2.6.4 Objective 4 – To determine whether optogenetic manipulation of ChR2-expressing locus
coeruleus neurons alone can elicit hLTF
To determine whether intermittent optical stimulation of the LC can trigger hLTF in lieu of
repeated apneas, rats (n=26) were infected with either AAV5-hSyn-ChR2(H134R)-mCherry or
AAV5-hSyn-mCherry. After a minimum of 3 weeks for viral expression, optic implants were
inserted bilaterally into the LC and I again recorded genioglossus and diaphragm EMG, ET-CO2
and O2 saturation over 60 minutes to establish a baseline. Unfortunately, the firing rates of LC
neurons have never been recorded during or after repeated apneas and thus, the frequency in
which LC neurons fire during apneas is not known. However, studies that have recorded LC
activity has reported that the LC fires at 0.5 Hz under anaesthesia (Seager et al., 2004, Vazey
and Aston-Jones, 2014), 1-2 Hz tonically (Aston-Jones and Bloom, 1981, Dremencov et al.,
2007), and up to 5 Hz when activated (Kogan et al., 1992). Therefore, I chose to repeatedly
stimulate LC neurons with 473 nm light at 5 Hz for 15 seconds separated by 1 minute of no
stimulation, repeated 10 times (Fig. 2.3). This intervention mimics the repeated apnea protocol

38
in Objective 1. Following this intervention, recordings continued for another 60-90 minutes
before the animal was killed by isoflurane overdose and transcardial perfusion. Three controls
were included: an off-target control (n=6) to determine the effect of stimulation outside the LC,
a continuous stimulation control (n=5) to determine the requirement for the intermittent
nature of the stimulus (Fig. 2.4), and a viral vector control (n=6) that is absent the light-sensitive
ion channel, channelrhodopsin2 (Chr2), to determine whether viral infection alone influenced
the manifestation of hLTF.
Figure 2.3. Protocol for intermittent LC stimulation in Objective 4.
Figure 2.4. Protocol for continuous LC stimulation in Objective 4.
2.6.5 Objective 5 – To determine whether optical silencing of eNpHR-expressing locus
coeruleus neurons prevent apnea-induced hLTF
To determine whether optical inactivation of the LC prevents apnea-induced hLTF, rats (n=22)
were infected with either AAV5-hSyn-eNpHR3.0-mCherry or AAV5-hSyn-mCherry. After a
minimum of 3 weeks for viral expression, optic implants were inserted bilaterally into the LC
and I again recorded genioglossus and diaphragm EMG, ET-CO2 and O2 saturation over 60
minutes to establish a baseline. LC neurons were then exposed to 532 nm light continuously
while simultaneously delivering obstructive apneas for 15 seconds separated by 1 minute
recovery, repeated 10 times (Fig. 2.5). Following the intervention, recordings continued for

39
another 60-90 minutes before the animal was killed by isoflurane overdose and transcardial
perfusion. A viral vector absent the light-sensitive ion channel, halorhodopsin (eNpHR), was
used to determine whether viral infection itself influenced the manifestation of hLTF.
Figure 2.5. Protocol for continuous inhibition of the LC with repeated apneas in Objective 5.
2.6.6 Objective 6 – To determine whether noradrenaline released specifically from the locus
coeruleus is the underlying mechanism that mediates hLTF
To determine whether hLTF elicited by intermittent LC stimulation is truly mediated by
noradrenaline, rats (n=9) were infected with AAV5-hSyn-ChR2(H134R)-mCherry. After a
minimum of 3 weeks for viral expression, optic implants were inserted bilaterally into the LC
and I again recorded genioglossus and diaphragm EMG, ET-CO2 and O2 saturation over 60
minutes to establish a baseline. I then perfused 1 µM Terazosin over 20 minutes at rate of 0.1
μL/min (Tadjalli, 2012) to antagonize α1-adrenergic receptors at the level of the hypoglossal
motor pool using reverse microdialysis. LC neurons were then repeatedly stimulated with 473
nm light at 5 Hz for 15 seconds separated by 1 minute of no stimulation, repeated 10 times (Fig.
2.6). Following the intervention, recordings continued for another 60-90 minutes before the
animal was killed by isoflurane overdose and transcardial perfusion.
Figure 2.6. Protocol for Terazosin perfusion with intermittent LC stimulation in Objective 5.

40
2.7 Data analysis
Peak integrated inspiratory genioglossus and diaphragm EMG amplitudes as well as respiratory
frequency were quantified on a breath-by-breath basis in 60 second intervals during all
experiments. Inspiratory amplitude and respiratory frequency were expressed as a percent
change from baseline ± standard error of the mean (SEM). Baseline values for inspiratory
amplitude and respiratory frequency were acquired during the 240 seconds prior to each
experimental intervention. Data were quantified and expressed before (i.e., baseline) and at 15,
30, 45 and 60 minutes after experimental interventions. Equivalent time points were quantified
and expressed in experiments serving as controls without particular interventions. Animals
were determined to exhibit hLTF if they met two specific criteria: (1) genioglossus inspiratory
amplitude was two standard deviations above baseline levels 60-min after recurrent apneas;
and, (2) summated genioglossus inspiratory amplitude averaged over 60-min was two standard
deviations above baseline levels. If an animal failed either criterion, they were considered not
to exhibit hLTF and were placed in a separate group henceforth known as “non-responders”.
This allowed for a clear separation between animals that exhibited hLTF and non-responders.
Although setting a standard to exclude non-responders is traditionally used in the field of LTP
research (Abraham et al., 1993, Watanabe et al., 2002), this selection approach can skew
statistical comparisons that only compare hLTF-expressing animals. To address this, further
analysis appropriately included one or both groups for statistical comparisons (see section
2.10). Arterial O2 saturation and end-tidal CO2 values were also expressed as a percentage
change from baseline ± SEM and presented at 15, 30, 45 and 60 minutes after each
experimental intervention or at equivalent time points in control experiments. Each presented
data point was an average over 60 seconds.
2.8 Histology
Immunohistochemical staining was performed on all rats to verify (1) probe tract locations, (2)
cell activity as determined by c-Fos expression, and (3) cell phenotype as determined by
tyrosine hydroxylase staining to identify noradrenergic neurons. At the end of each experiment,

41
rats were overdosed with isoflurane (5%) until ventilation ceased, followed by transcardial
perfusion with 4% paraformaldehyde (in 0.1M phosphate buffer). Brains were extracted and
stored in 4% paraformaldehyde overnight, followed by a cryoprotection step by submerging
brains into 30% sucrose in 0.1M PB solution over several days until brains were saturated.
Brains were then immersed in Tissue-Tek OCT Compound (Electron Microscope Sciences) and
frozen on dry ice. Frozen brains were then sliced in a cryostat (CM3050 S, Leica Microsystems)
at 40 μm coronal sections. To determine whether noradrenergic cells were activated alongside
apnea-induced hLTF, immunohistochemistry was used to identify colocalized expression of c-
Fos and tyrosine hydroxylase. Primary antibody rabbit anti-c-Fos (1:5000 dilution, cat# 26209,
lot# 113018B, Immunostar) was used in conjunction with mouse anti-TH (1:1000 dilution, cat#
22941, lot# 907001, Immunostar). After 48 hours of incubation at 4°C, biotinylated secondary
antibodies, biotinylated goat anti-rabbit IgG (1:800 dilution, cat# BA-1000, lot# Z0619, Vector
Laboratories) and biotinylated goat anti-mouse IgG (1:600 dilution, cat# BA-9200, lot# W2206,
Vector Laboratories) were used. To visualize, an avidin biotin complex (ABC) kit (VECTASTAIN
Elite ABC HRP Kit, PK-6100, Vector Laboratories) used in conjunction with a 3,3’-
diaminobenzidine (DAB) peroxidase kit (DAB Kit, VECTSK4100, Vector Laboratories) to oxidize
DAB, providing a brown-black colour in the nuclei of c-Fos positive cells, and NovaRed (NovaRed
Kit, VECTSK4800, Vector Laboratories) was used to provide a contrasting red colour to identify
noradrenergic cells. Stained tissue was then imaged using Cellsens Slide Scanner (Olympus,
FSX100) under bright field at 4x magnification. The location of lesion tracts were plotted on
standardized brain maps (Paxinos and Watson, 1998). In experiments where virally infected LC
neurons expressed mCherry, tissue was incubated in primary rabbit anti-mCherry (1:500
dilution, cat# NBP2-25157, lot# 12016, Novus Biologicals) and secondary goat anti-rabbit Cy3
antibodies (1:500, cat# 111-167-003, lot#78034, Jackson ImmunoResearch). To identify
noradrenergic cells under fluorescence, tissue was incubated again in primary mouse anti-TH
with fluorescent secondary goat anti-mouse Alexa Fluor 488 (1:500, cat# 111-167-003, lot#
130258, Jackson ImmunoResearch). Tissue was then counterstained with DAPI. Sections were
imaged with the upright fluorescent (AxioImager Z1; Zeiss), confocal microscope (AxioObserver

42
Z1; Zeiss), or under bright-field through a slide scanner (FSX-100 Inverted Microscope,
Olympus).
2.9 Cell quantification
In initial studies, sections were first non-quantitatively analyzed to identify regions with notable
changes in c-Fos expression. A cell was considered c-Fos+ if a cell expressed a black nucleus and
excluded cells that expressed nuclei that were light/medium brown (which may or may not be
c-Fos+). This level of stringency ensured that we only identified c-Fos+ cells and thereby
excluded the possibility of identifying false positive cells. Noradrenergic cells were identified by
a red-brown colour in the whole cell obtained with NovaRed staining. Noradrenergic regions
and areas with unambiguous c-Fos expression were then manually counted with observers
blinded to the treatment. An automatic counting process was not possible for the LC due to the
irregular shape of LC neurons relative to standard automatic cell counting parameters available.
Regions of interest were identified using the rat brain atlas (Paxinos and Watson, 1998) and
counted using ImageJ. Three images representative of slices across the rostral/caudal axis were
taken for each region per animal, and this sampling strategy is based on a recent study that
showed that the distribution of LC projections had no specific organization across
anterior/posterior or medial/lateral axes (Schwarz et al., 2015). Each image was 0.5 x 0.5 mm
and encompassed the structure of interest. In later studies, fluorescent staining was used to
identify mCherry and tyrosine hydroxylase (TH) positive cells. In these studies, cells were
manually counted for each image with the experimenter blinded to the treatment.
2.10 Statistical analysis
The specific statistical tests used for each experiment are stated within the results section. All
datasets passed normality. In all groups, values were compared as percent change from
baseline. Comparisons for each respiratory variable within a treatment across time (e.g.,
repeated apneas on genioglossus amplitude at baseline, 15, 30, 45, and 60 minute time points)
were made using a one-way repeated measure analysis of variance (one-way RM ANOVA) and

43
post hoc comparisons were performed using the Dunnett test. Comparisons between
treatments for each respiratory variable were made using a two-way RM ANOVA with post hoc
Bonferroni test to infer statistical significance. One caveat with this approach is the exclusion of
animals that do not exhibit hLTF when comparing genioglossus amplitude between groups. To
determine whether an intervention influenced hLTF expression, a chi-square comparison was
performed to determine whether my intervention was significantly correlated with hLTF
expression. A chi-square test can help determine whether my observed values fit within an
expected distribution. In other words, the chi-square tests the null hypothesis that the variables
are independent. The test compares the observed data to a model that expects that the
variables are independent. Where the observed data do not fit provides the likelihood that the
variables are dependent. In addition to this, I also performed a Firth logistic regression to
measure the relationship between one or more independent variable that determines an
outcome. In other words, a Firth logistic regression allows me to determine whether my
predictors (e.g. an intervention such as repeated apneas) influenced my dependent outcome
(i.e., hLTF expression). This differs from a chi-square test because a chi-square test is not a
modelling technique. By providing the probability of hLTF expression based on my predictors
(i.e., intervention such as repeated apneas), a logistic regression can model whether my
intervention can predict an outcome. In both calculations (chi-square test and Firth logistic
regression), I included all animals (i.e., hLTF-expressing animals and non-responders) to
determine whether an intervention influenced the probability of hLTF expression. Lastly,
comparisons of respiratory muscle activity between all groups were also made using an
ordinary least square (OLS) linear regression. An OLS allowed me to identify whether my
intervention had a statistically significant effect compared to controls and determine the
strength and direction of the effect. This approach allowed me to compare the muscle activity
of all animals (i.e., hLTF-expressing animals and non-responders), in all treatment groups (i.e.,
intervention and controls), at a specific time point to infer statistical significance. Cell counts
between groups were compared using a one-way ANOVA and post hoc comparisons were
performed using the Bonferroni test, or a student t-test where applicable. All statistical

44
analyses used GraphPad Prism (Prism v5.0, GraphPad), STATA (v5.10 and R Studio (v3.4.3). Data
are presented as a mean + standard error of the mean.

45
Chapter Three – A Tripartite Circuit Mediates Respiratory Motor Plasticity
(Data in Chapter 3 is published; Lui, S. et al., 2018. The data generated by the co-authors were
not included in this thesis. Only data generated by myself is presented in Chapter 3).
3.1 Summary
The respiratory network takes in various stimuli and adjusts respiratory output accordingly. The
respiratory network can make long-term adjustments to its output by undergoing plasticity. For
example, following repeated obstructive apneas the respiratory network can augment
respiratory motor output and strengthen genioglossus muscle contractions for a prolonged
period, implicating it to have potential in mitigating obstructive sleep apnea. This form of
plasticity is known as hypoglossal (XII) long-term facilitation (hLTF). The neural circuit
underlying hLTF is unknown but was suggested to require activation of the nucleus tractus
solitaris (NTS) and required the activation of α1-adrenergic receptors on hypoglossal motor
neurons. Here I propose the locus coeruleus (LC) to be the source of noradrenaline acting on
α1-adrenergic receptors to mediate hLTF. First, I elicited hLTF with repeated apneas to identify
which cell groups were activated alongside hLTF. Next, I identified the LC to be the only
noradrenergic cell group to display an increase in neural activity following hLTF, then traced its
axonal projections from the LC to the hypoglossal motor pool. Lastly, I show that inactivation of
the LC prevented apnea-induced hLTF. Taken together, I have identified a three-part circuit
within the brainstem (NTS → LC → XII) that underlies respiratory motor plasticity.
3.2 Introduction
Understanding motor neuron physiology is important because respiratory motor neurons are
critical in triggering effective breathing movements. Respiratory motor neurons (e.g.,
hypoglossal) are sensitive to and modulated by repeated perturbations in central respiratory
drive. For example, intermittent episodes of hypoxia or airway obstruction induce a form of
respiratory motor plasticity known as long-term facilitation (LTF) (Hickner et al., 2014, Hoffman

46
et al., 2012, Ryan and Nolan, 2009, Song and Poon, 2017, Tadjalli et al., 2010). LTF results in a
long-lasting increase in inspiratory motor outflow to inspiratory muscles (e.g., genioglossus),
which may function to facilitate ventilation. Previously, it was demonstrated that repeated
airway obstructions trigger LTF of hypoglossal motor outflow (i.e., apnea-induced hLTF) and
that this form of respiratory plasticity is mediated by a noradrenergic mechanism (Tadjalli et al.,
2010). Specifically, the blockade of α1-noradrenergic receptors at the level of hypoglossal
motor pool prevented hLTF, suggesting that noradrenaline release likely underlies hLTF (Tadjalli
et al., 2010). Here, I reaffirm that repeated apneas can consistently trigger hLTF and
investigated the brainstem regions that were activated during apnea-induced hLTF.
Currently, the source(s) of the noradrenaline that drives respiratory motor plasticity remains
unidentified. What is known is that the hypoglossal motor pool receives noradrenergic input
from several noradrenergic cell groups within the brainstem including the A1, A5, A6 (i.e. LC),
A7, and subcoeruleus (Aldes et al., 1992, Rukhadze and Kubin, 2007), with the proportions of
noradrenergic input to the hypoglossal motor pool being 18.5%, 43.5%, 1.7%, 15.0%, and
21.0%, respectively (Rukhadze and Kubin, 2007). The A5 and A7 are of particular interest as
they have been previously shown to mediate a form of hLTF (Song and Poon, 2017). Specifically,
an increase in c-Fos expression was observed at the A5 and A7 following apnea-induced hLTF,
and intermittent optical stimulation of these regions triggered a transient increase in
inspiratory genioglossus motor output persisting for up to 20 minutes (Song and Poon, 2017).
This suggests that the A5 and A7 are likely candidates in mediating hLTF. Alternatively, although
the A1 and subcoeruleus has not been directly shown to mediate respiratory motor plasticity,
studies of the A1 have suggested that it is involved in mediating structural plasticity on
oxytocinergic neurons (Michaloudi et al., 1997), and its inactivation can reduce phrenic burst
activity (Hilaire, 2006, Zanella et al., 2006). Studies of the subcoeruleus’s role in plasticity were
often integrated with the LC, making the role of the subcoeruleus difficult to isolate (Stanton
and Sarvey, 1985). However, some studies have suggested the subcoeruleus to be involved in
learning and memory (Siwek et al., 2014), suggesting the subcoeruleus is involved in mediating
some forms of plasticity. In the context of respiration, the subcoeruleus responds to hypoxia

47
(Berquin et al., 2000, Bodineau and Larnicol, 2001, Joubert et al., 2016, Teppema et al., 1997).
This suggests that the A1 and the subcoeruleus may also be involved in the neural circuit
mediating hLTF. Lastly, the LC has been intensively studied and well established to be involved
in both breathing and plasticity.
3.2.1 Locus coeruleus and its role in breathing and plasticity
The locus coeruleus is the largest source of noradrenaline within the central nervous system
(Moore, 1979), with diffuse projections throughout the entire neuroaxis (Schwarz et al., 2015).
The LC has shown very little topographical organization within itself, suggesting cells across the
neuroaxis within the LC have equal probability to project rostrally or caudally (Schwarz et al.,
2015). The most prominent role of the LC in the context of breathing has been as a central
chemoreceptor. Many studies have shown that an increase in inspired CO2 correlates with an
increase in LC activity, determined by an increase in c-Fos expression in the LC (Coates et al.,
1993, Gargaglioni et al., 2010, Haxhiu et al., 1996, Oyamada et al., 1999, Teppema et al., 1997).
In fact, lesioning of the LC decreased the hypercapnic ventilatory response (Biancardi et al.,
2008, Li and Nattie, 2006). The LC also has direct effects on hypoglossal nerve activity because
LC inactivation with tetrodotoxin reduced hypoglossal nerve firing rate in an isolated brainstem-
spinal cord preparation, and electrical stimulation of the LC under the same preparation
increased the firing rate (Hakuno et al., 2004).
In the context of plasticity, the LC has long been considered to be a mediator for plasticity, such
as LTP (Jedrzejewska-Szmek et al., 2017, Stanton and Sarvey, 1985). The ablation of
noradrenergic LC neurons prevents the manifestation of some forms of plasticity (Stanton and
Sarvey, 1985), suggesting that the LC is capable of promoting or inducing plasticity. However,
the role of the LC in mediating respiratory motor plasticity was not as readily studied. Studies
have linked a decreased in locus coeruleus activity during REM sleep (Aston-Jones and Bloom,
1981), and REM sleep with a decrease in upper airway muscle tone (Nitz and Siegel, 1997).
Together, it may suggest that a reduction in LC activity may be involved in the reduction of

48
upper airway muscle tone during REM sleep. This is supported by data showing LC inactivation
with tetrodotoxin reduced hypoglossal nerve firing, while electrical LC stimulation increased
hypoglossal firing rates (Hakuno et al., 2004). Considering the LC is involved in influencing
hypoglossal nerve activity and plasticity in other systems, this places the LC in a prime position
to mediate noradrenaline-dependent respiratory plasticity.
3.2.2 Projections of locus coeruleus neurons
Earlier I mention that the hypoglossal motor pool receives dense noradrenergic input from the
A1, A5, LC, A7 and subcoeruleus. However, despite the dense noradrenergic innervations to the
hypoglossal motor pool, previous studies have claimed that the LC does not project to the
hypoglossal motor pool (Aldes, 1990, Aldes et al., 1992, Aston-Jones et al., 1970, Fritschy and
Grzanna, 1990, Levitt and Moore, 1979), or at most, provide 1.7% of the total noradrenergic
input at the hypoglossal motor pool (Rukhadze and Kubin, 2007). Here, I provide evidence
showing a higher proportion of LC neurons possess a direct anatomical connection between the
LC and the hypoglossal motor pool using a retrograde tracer, cholera toxin B (CtB).
3.3 Results
3.3.1 Repeated obstructive apneas trigger LTF of inspiratory genioglossus muscle activity
First, I wanted to reaffirm that repeated obstructive apneas can trigger LTF of inspiratory
genioglossus motor output. I found that recurrent airway occlusions (10, 15-s apneas each
separated by 1-min) triggered a robust and sustained increase in inspiratory genioglossus
muscle activity that peaked at 96 ± 17% above baseline levels by 60 min min (2-way RM
ANOVA, F=11.22, p<0.0001; Fig. 3.1A,B,C). Apneas, which were confirmed by a total loss of
expired CO2 and a drop in O2 saturation (Fig. 3.1D,E), only amplified the magnitude of
inspiratory genioglossus activity; they had no long-term effect on respiratory frequency or
diaphragm inspiratory activity (2-way RM ANOVA, F=2.113, p=0.0880 and F=2.433, p=0.0557,
breath frequency and inspiratory diaphragm amplitude, respectively; Fig. 3.1F,G). LTF of

49
inspiratory genioglossus amplitude was not attributable to changes in end-tidal CO2 nor
changes to O2 saturation as both variables remained consistent between groups over the 60-
min recording period (2-way RM ANOVA, F=0.4221, p=0.7921 and F=1.043, p=0.4160, for end-
tidal-CO2 and O2 saturation, respectively; Figure 3.1H,I).
It is important to note that within the group of animals given repeated apneas, 35% did not
exhibit hLTF and were labelled as non-responders. The lack of hLTF in these animals were not a
result of incomplete apneas, which were again confirmed by a total loss of expired CO2 and a
drop in O2 saturation (Fig. 3.1D,E). Non-responders are further discussed in section 3.3.3.
To demonstrate that respiratory activity remained stable throughout the recording period,
genioglossus and diaphragm activity were recorded in a control group of rats that experienced
no recurrent apneas. I found that genioglossus amplitude, breath frequency, end-tidal CO2 and
O2 saturation remained stabled during the 60 minute time-window (RM ANOVA, genioglossus:
F=1.33, p=0.2757; breath frequency: F=1.988, p=0.1148; ET-CO2: F=1.485, p=0.2272; O2
saturation: F=1.546, p=0.2776; Figure 3.1), indicating that genioglossus activity does not change
over the 60 minute recording period and that LTF of genioglossus muscle activity is attributable
to recurrent apneas per se. A decrease in diaphragm amplitude over time was observed (RM
ANOVA, F=4.996, p=0.0026), but was in line with animals given recurrent apneas (RM ANOVA,
F=6.408, p=0.0007). Taken together, this reaffirms that repeated apneas can successfully trigger
apnea-induced LTF of inspiratory genioglossus muscle activity.

50
Figure 3.1. Repeated obstructive apneas elicit LTF of the genioglossus motor activity. (A) Integrated inspiratory genioglossus motor output (∫GG EMG) recorded from an anaesthetized spontaneously breathing rat, depicting baseline genioglossus amplitude and the subsequent increase in EMG amplitude following repeated apneas (i.e., hLTF). (B) High-temporal resolution EMG traces showing genioglossus (top) and diaphragm (bottom) activity at baseline, 15, 30, 45, and 60 min after repeated apneas. (C) Group data showing inspiratory genioglossus activity time matched control (i.e. no apneas; black bars) and intermittent apnea groups (white bars) at 15, 30, 45, and 60 min. Dotted line represents baseline activity. Intermittent apneas induced an increase in inspiratory genioglossus amplitude peaking at 96 ± 17%. A raw trace showing end-tidal CO2 (D) and arterial O2 saturation (E) before, during, and after an apnea (left), and group data (right) showing undetectable end-tidal CO2 levels during apnea indicating complete occlusion, and arterial O2 saturation levels reduced by 20 ± 4% following an apnea. Although intermittent apneas triggered a robust increase in inspiratory genioglossus activity (i.e., hLTF), this same intervention had no significant effect on either (F) inspiratory diaphragm (∫Dia EMG) amplitude or breath frequency. (H) Both end-tidal CO2 and (I) O2 saturation levels remained constant across the 60 min recording period. Data is presented as mean + SEM.*Denotes a significant difference (p < 0.05) from baseline.
3.3.2 Activation of noradrenergic LC neurons correlates with hLTF
To determine the source of noradrenaline mediating apnea-induced hLTF, I investigated the
activity of all noradrenergic cell groups with known projections to the hypoglossal motor pool

51
following apnea-induced hLTF. I did this by quantifying c-Fos expression within noradrenergic
cell groups (i.e., A1, A2, A5, A6 [LC], and A7) following induction of hLTF and compared
expression levels with a control group (i.e., animals not exposed to recurrent airway
occlusions). Specifically, noradrenergic cells that were c-Fos positive were counted in each
region. Compared to the time control group, I found that apnea-induced hLTF increased c-Fos
expression in the LC by 176 ± 7% (unpaired t-test, t(51) = 3.334, p = 0.0016; Figure 3.2); however,
I found no evidence for changes in c-Fos expression in the other noradrenergic cells groups (i.e.,
A1, A2, A5 and A7; Table 3.1), suggesting that apnea-induced hLTF only activates noradrenergic
cells in the LC.
3.3.3 Activation of noradrenergic cells in the LC is specific to hLTF responders
While the preceding experiments suggest that hLTF activates LC cells, LC activity is also
increased by hypoxic, hypercapnia and airway occlusion (Berquin et al., 2000, Haxhiu et al.,
2001, Haxhiu et al., 1996, Teppema et al., 1997), which makes it difficult to link the observed
increases in LC activity with hLTF induction. Therefore, I wanted to determine if increased LC
activity is attributable to hLTF per se, so I examined LC c-Fos expression levels in which

52
recurrent apneas triggered hLTF and compared them with cases in which recurrent apneas did
not trigger hLTF (i.e. non-responders) (Figure 3.2A). I was able to make such comparisons
because hLTF does not always occur following repeated apneas. Specifically, I found that
recurrent apneas only triggered hLTF 65% of the time (i.e., 35% of the time repeated apneas did
not induce hLTF), and this rate of plasticity induction is in line with classic long-term
potentiation (LTP) studies which report that LTP only occurs 50 to 90% of the time (i.e. LTP does
not occur 10 to 50% of the time) (Abraham et al., 1993, Watanabe et al., 2002). Nonetheless, I
first wanted to ensure that the lack of hLTF expression in the non-responder group was not
influenced by changes in anaesthesia depth. Therefore, in addition to corneal and toe pinch
reflexes used throughout the experiment, I quantified the percentage of inhaled isoflurane at
the beginning and end of each experiment and recorded respiratory frequency as an index of
anaesthesia depth in the hLTF and No hLTF groups. In both cases, animals were induced at 3.5%
isoflurane and reduced after tracheostomy to maintain anaesthesia. Maintenance varied
between animals but averaged around 2.5% isoflurane (Fig. 3.3A). Similarly, no difference in
breath frequency at 60-min post apneas and presumably anaesthesia depth was observed
(unpaired t-test, t(12)=0.3227, p=0.7525) (Fig. 3.3B). Next, I compared end-tidal CO2 and oxygen
saturation levels between groups to ensure blood gases were not confounding factors in hLTF
expression. Neither ET-CO2 nor oxygen saturation levels were significantly different between
groups (2-way RM ANOVA, responders vs non-responders, ET-CO2: F = 0.7049, p=0.5933. O2
saturation: F = 0.5439, p=0.7054) (Fig. 3.3C,D). I also compared mean arterial blood pressure
between groups and found no observable difference between animals that developed hLTF and
those that did not (Fig. 3.3E). Limited numbers of non-responders with blood pressure
recordings prevented a statistical comparison. I then compared c-Fos expression between
animals that exhibited apnea-induced hLTF and those that did not (non-responders). Compared
to non-responders, we found that apnea-induced hLTF increased c-Fos expression in the LC by
186 ± 7% (apnea-induced hLTF vs non-responders: unpaired t-test, t(56) = 2.103, p=0.0399; Fig.
3.2B,C). This observation suggests that activation of noradrenergic cells in the LC is hLTF-
dependent and is not associated with the hypoxia and hypercapnia associated with apneic
stimuli.

53
Figure 3.2. LC activation correlates with apnea-induced hLTF. (A) Group data showing inspiratory genioglossus amplitude after recurrent apneas in responders (i.e., apnea-induced hLTF; n = 9, white bars) and non-responders (i.e. apnea without hLTF; n = 5, grey bars) at 15, 30, 45, and 60 min. Dotted line represents percent baseline activity. Intermittent apneas produced hLTF with inspiratory genioglossus amplitude peaking at 96 ± 17% but non-responders did not exhibit hLTF following the repeated apnea intervention. (B) Group data showing LC activity in the no apnea (time control, n = 5, black bar), apneas without hLTF (“non-responders”, n = 5), and apnea-induced hLTF (n = 5) groups. Animals that exhibited hLTF had LC activity increased by 176 ± 7%. This increase is correlated with hLTF and not the apneas themselves as an identical intervention but absent hLTF did not display an increase in double-labelled cells. In fact, animals exhibiting hLTF had LC activity increase by 186 ± 7% compared to animals given an identical protocol but did not exhibit hLTF. No difference was observed between the time control and non-responder group. (C) An example of LC activity represented by c-Fos expression in the time control, non-responders, and apnea-induced hLTF groups. c-Fos expression was identified by cell nuclei stained black with DAB and tyrosine hydroxylase (TH) expression was identified by red-brown NOVA-Red stain to phenotype noradrenergic cells. Magnified examples of LC neurons (black arrows) that are c-Fos negative, TH-positive (time control and non-responders) and LC neurons that are double-positive (last panel). Data is presented as mean + SEM. *Denotes a significant difference (p < 0.05).

54
Figure 3.3. Levels of anesthesia, expired CO2, O2 saturation and blood pressure do not correlate with hLTF. (A) A comparison of the percentage of isoflurane used to maintain anesthesia in animals that exhibited hLTF after repeated apneas (i.e., “apnea-induced hLTF”; n = 9, white diamonds) and animals that did not exhibit hLTF after apneas (i.e., “non-responders”; n = 5, black diamonds). (B) Breath frequency of each animal expressed as a percent change from baseline did not differ between animals exhibiting apnea-induced hLTF and non-responders. No difference was observed in levels of anaesthesia, ET-CO2, oxygen saturation, and mean arterial blood pressure (ABP) in the apnea-induced hLTF and non-responder groups (A–E) suggest these factors are unlikely contributors to the lack of hLTF in the non-responder group. Dotted line represents percent baseline. Data is presented as mean + SEM.

55
3.3.4 Noradrenergic LC neurons have direct projections to the hypoglossal motor pool
Having shown that noradrenergic LC cell activity is associated with apnea-induced hLTF, my
next goal was to verify that these cells project to and synapse on neurons within the
hypoglossal motor pool. Available anatomical tracing data has shown minimal to no projections
between the LC the hypoglossal motor pool (Aldes et al., 1992, Fritschy and Grzanna, 1990,
Rukhadze and Kubin, 2007). By injecting CtB conjugated with AlexaFluor-488 into the
hypoglossal motor pool, I aimed to determine if noradrenergic cells (i.e., TH+ noradrenergic
cells) project to the hypoglossal motor pool. Following CtB injection into the hypoglossal motor
pool, I quantified the total number of TH positive, CtB positive, and double-labelled cells and
found that CtB injection within the hypoglossal motor pool labeled 71 ± 9% of noradrenergic
neurons in the LC (Figure 3.4A-C,G-J). However, I found that injections that were 0.2-0.8 mm
ventral to the hypoglossal motor pool did not result in CtB labeling of noradrenergic LC cells
(Figure 3.4D-F), demonstrating that noradrenergic LC cell labeling is selective to CtB injections
in the hypoglossal motor pool. This suggests that the CtB labeling observed arose from a direct
projection from the LC to the hypoglossal motor pool.
To further demonstrate that LC cells project to hypoglossal motor neurons, I also injected an
adeno-associated virus (AAV) carrying reporter protein mCherry to trace LC axonal projections
to the hypoglossal motor pool. Specifically, when AAV5-hSyn-ChR2(H134R)-mCherry was
injected into the LC, I found clear evidence of mCherry labelled axon terminals at the level of
the hypoglossal motor pool (Figure 3.4K). Together, these results indicate that noradrenergic LC
cells project to the hypoglossal motor pool, presumably on hypoglossal motor neurons.

56

57
Figure 3.4. Noradrenergic LC neurons have direct projections to the hypoglossal motor pool. A histological example of the LC 10 days after injection of cholera toxin B (CtB) conjugated with AlexaFluor-488 into the hypoglossal motor pool (n=6). (A) Cells double-labelled for cholera toxin B (CtB, green) (B) and tyrosine hydroxylase (TH, red) (C) can be observed, identifying noradrenergic LC neurons that project to the hypoglossal motor pool. Blue hue in overlay represents DAPI staining. CtB injected ventral to the hypoglossal motor pool (n=7) did not double-label cells in the LC (D) as no CtB positive cells were observed (E), but TH positive cells are still present (F). Magnified images of cells positive for CtB (H), TH (I), DAPI (J), or triple-labelled cells (G). Triple-labelled neurons are indicated by the white arrows, suggesting noradrenergic cells in the LC directly project to the hypoglossal motor pool. To verify this connection, AAV5-hsyn-ChR2(H134R)-mCherry injected into the LC showed visible axon terminals at the level of the hypoglossal motor pool (K). Differences in hue in the images above are attributed to different filters used on different microscopes. CC, central canal.
3.3.5 Bilateral inactivation of the LC prevented apnea-induced hLTF
Having demonstrated that noradrenergic LC cells were activated during hLTF and that they
project to the hypoglossal motor pool, my next step was to determine if noradrenergic LC cells
mediate LTF of genioglossus muscle activity. To do this, I pharmacologically inactivated LC cells
by focally injecting clonidine into the left and right LC nuclei. However, before this I wanted to
verify that bolus fluid injections alone did not influence the expression of apnea-induced hLTF.
Therefore, I injected an equal volume of vehicle (Ringer’s) into the left and right LC nuclei 30
min before recurrent airway occlusions. I found that vehicle injections had no effect on
expression of apnea-induced hLTF (RM ANOVA, F=6.476, p=0.0008) with inspiratory
genioglossus activity increasing up to 40 ± 3% above baseline levels (Fig. 3.5D). However,
compared to vehicle injections, I found that inactivating noradrenergic LC cells with bilateral
clonidine microinjection prevented apnea-induced hLTF (RM ANOVA, F=0.5975, p=0.6686; Fig.
3.5C,D), with inspiratory genioglossus activity remaining with baseline levels during the 60 min
period following injection. This observation suggests that noradrenergic LC cells are required
for driving the expression of apnea-induced hLTF. Post-mortem histology was used to confirm
that injections were located within the left and right LC nuclei (Fig. 3.5A).
To ensure that clonidine applied to the LC did not suppress baseline genioglossus activity we
compared baseline genioglossus activity before and after clonidine application, and found no
significant effect of clonidine on genioglossus activity (unpaired t-test, t(10) = 0.5490, p=0.5950;

58
Fig. 3.5B). This suggests that the absence of hLTF after clonidine treatment does not stem from
suppressed genioglossus activity.

59
Figure 3.5. Inactivation of the LC prevented apnea-induced hLTF. (A) Probe tract locations in the LC following bilateral microinjection of clonidine. Green circles represent clonidine-treated animals and blue circles represent vehicle controls. (B) Group data showing inspiratory genioglossus (GG) activity before (BL) is not significantly different after clonidine application at the LC (BL w/CLO). (C) A representative EMG traces of integrated inspiratory genioglossus (GG) activity after LC inactivation at baseline, 15, 30, 45, and 60 min after repeated apneas. (D) Group data showing inspiratory genioglossus activity in the vehicle-treated (n=6, white bars) and clonidine-treated (n=8, black bars) animals at 15, 30, 45, and 60 min following repeated apneas. Dotted line represents average baseline activity. Intermittent apneas induced a peak of 40 ± 13% increase in inspiratory genioglossus amplitude (i.e., hLTF) in vehicle-treated animals, but in the presence of clonidine, LC cells were inactivated effectively abolishing apnea-induced hLTF. Data are presented as mean ± SEM. * denotes a significant difference (p<0.05).
3.5 Discussion
This study is scientifically important because it contributes to our understanding of circuit and
transmitter mechanisms underlying respiratory motor plasticity. Here, I identified a tripartite
circuit that underlies apnea-induced LTF of genioglossus motor activity. It has already been
shown that hLTF requires noradrenaline (Tadjalli, 2012), the activation of NTS neurons
(Torontali, 2012), and the activation of α1-adrenergic receptors on hypoglossal motor neurons
(Tadjalli et al., 2010). Here, I reaffirm that repeated apneas can elicit hLTF, which has allowed
me to further investigate the brainstem regions that may be involved in mediating hLTF. Using
c-Fos expression as an index of cell activity, I found that noradrenergic cells in the LC were
activated during apnea-induced hLTF, suggesting that they could be the neural substrate that
triggers noradrenaline release onto hypoglossal motor neurons. I then show that hypoglossal
motor neurons receive noradrenergic inputs from the LC, indicating that hLTF could be
triggered by noradrenaline released from the LC onto hypoglossal motor neurons. Lastly, I
inactivated the LC and found repeated apneas could no longer elicit hLTF. These results suggest
that a tripartite circuit in the brainstem (i.e., NTS ➔ LC ➔ XII) is responsible for triggering
apnea-induced LTF of genioglossus motor output.
3.5.1 Noradrenergic cells in the LC are active during hLTF
Hypoglossal motor neurons receive noradrenergic inputs from several different cells groups,
including the A1, A5, A7, LC, and subcoeruleus (Aldes et al., 1992, Rukhadze and Kubin, 2007),
indicating that hLTF could be triggered by noradrenaline onto hypoglossal motor neurons from

60
one or more of these noradrenergic nuclei. Using c-Fos expression as an index of noradrenergic
activity, I found that noradrenergic cells in the LC were activated by apnea-induced hLTF,
suggesting that they could be the neural substrate that triggers noradrenaline release onto
hypoglossal motor neurons.
However, unlike a previous report (Song and Poon, 2017), I found no evidence to indicate that
noradrenergic cells in either the A5 or A7 nuclei were activated following hLTF induction.
Methodological differences are the likely reason for the differences between our observations.
Here, I probed c-Fos expression levels 90 min after hLTF induction, whereas, Song and Poon
examined expression levels 20 min after hLTF induction. I quantified c-Fos expression 90 min
following hLTF induction because c-Fos levels are maximal 60-90 min following stimulus-
induced neuronal activation (Bullitt, 1990, Morgan et al., 1987). My choice to identify c-Fos
protein expression matched the time frame for hLTF persisting for >60 minutes post
intervention. This is in contrast to other biomarkers for neuronal activation such as ERK/pERK
(expression window within 2-10 minutes) (Gao and Ji, 2009), Arc (expression window within 5-
30 minutes from activation) (Guzowski et al., 1999), or Zif268 (expression window within 15-60
minutes from activation) (Guzowski et al., 1999). As such, it may be possible my protocol
captured the brain regions required to sustain hLTF, while the A5 and A7 cell groups may be
involved in the trigger. Differences between my results and those of Song and Poon could also
stem from the use of different anaesthetics, which are known to influence c-Fos expression
(Dragunow et al., 1990, Roda et al., 2004). Alternatively, it may be possible that the initial
increase in noradrenaline release at the hypoglossal motor pool recruited the A5 and A7, but
persistent hLTF (i.e. hLTF persisting for more than 20 minutes) requires the LC. This synergy
between noradrenergic cell groups was observed before. For example, neonatal rats receive
stronger inhibitory inputs from the A5 on the respiratory rhythm generator (RRG), while the
RRG is simultaneously being modulated by excitatory noradrenergic input from the LC in
adulthood (Dobbins and Feldman, 1994, Viemari et al., 2004a, Viemari et al., 2004b).

61
3.5.2 Noradrenergic LC neurons project to the hypoglossal motor pool
Current literature reported limited to no anatomical connections between the LC neurons and
the hypoglossal motor neurons (Aldes, 1990, Aldes et al., 1992, Aston-Jones et al., 1970,
Fritschy and Grzanna, 1990, Levitt and Moore, 1979, Rukhadze and Kubin, 2007). At most, it
was reported that only 1.7% of the noradrenergic input to the hypoglossal motor pool
originates from the LC (Rukhadze and Kubin, 2007). However, I suspected that the percent of
noradrenergic LC neurons to be larger than previous reports as LC activity correlates with
genioglossus activity (Aston-Jones and Bloom, 1981, Chan et al., 2006, Hakuno et al., 2004). It
may be possible that previous tracing studies missed aspects of the hypoglossal motor pool that
may be innervated by the LC. I found that the CtB injected into the hypoglossal motor pool
labelled 71% ± 9.23% of neurons in the LC. These values were higher than previously reported
so to ensure accuracy of these findings, I injected CtB ventral or rostral to the hypoglossal
motor pool to act as off-target controls. When CtB was injected ventral to the hypoglossal
motor pool, I found no double-labelled LC neurons (Fig. 3.4). To further support the premise
that the LC has direct projections to the hypoglossal motor pool, LC neurons were infected with
a virus carrying a fluorescent reporter protein, mCherry. In these animals, 44% of noradrenergic
LC neurons were infected and axon terminals could easily be visualized at the level of the
hypoglossal motor pool. This is in direct contradiction with anterograde tracing studies that
claim the LC does not project to brainstem motor pools (Fritschy and Grzanna, 1990). However,
their approach with PHA-L was limited by time. PHA-L was reported to provide limited
expression in anterogradely labelled cells following 2-4 weeks post injections, with no labelled
cells by 9 weeks (Kott et al., 1991). Fritschy and Grzanna claimed no direct projections from the
LC to brainstem motor pools, but sacrificed the animal at the 2-3 week mark, suggesting the LC
to hypoglossal connections may have been missed with this approach.
3.5.3 LC activation is independent of hypoxia or hypercapnia associated with repeated apneas
My results indicate that noradrenergic LC cell activity is associated with hLTF expression, but
because LC cells are responsive to obstructive apnea, hypercapnia and hypoxia (Berquin et al.,

62
2000, Haxhiu et al., 1996, Teppema et al., 1997), it is possible that changes in LC activity
following recurrent apneas could result for apneic and/or hypercapnia/hypoxic stimuli rather
than hLTF itself. To indirectly test this possibility, I examined c-Fos in cases where recurrent
apneas did not elicit LTF of inspiratory genioglossus activity (i.e., 5 of 14 cases). I found no
evidence for increased c-Fos expression in LC cells when recurrent apneas did not trigger hLTF,
which contrasts with the robust increase in c-Fos expression when recurrent apneas triggered
hLTF (Fig. 3.2B,C). This is important because the increased activity in the LC was strictly limited
to animals that exhibited hLTF suggesting that activation of noradrenergic LC cells is not caused
by chemical stimuli associated with repeated apneas; instead, LC activation is linked to hLTF
induction per se. I interpret these findings to indicate that increased LC activity is the causal
mechanism that triggers LTF of genioglossus activity because: (1) noradrenergic cells are only
active when hLTF is triggered by apneas (i.e., increased c-Fos in animals that exhibit hLTF; Fig.
3.2B,C); (2) that noradrenergic LC neurons project to hypoglossal motor neurons (Fig. 3.4); and,
(3) inactivation of LC cells during apneas prevented hLTF (Fig. 3.5). Based on these pieces of
evidence and the fact that apneas act through vagal afferents and NTS neurons, which in turn
project to LC neurons (Lopes et al., 2016, Tadjalli et al., 2010), I claim that recurrent apneas
activate LC neurons to trigger apnea-induced hLTF. As presented and interpreted, my data are
consistent with previously published studies showing that increases in c-Fos expression can be
used to identify cells associated with inducing other forms of plasticity, such as granule cells
and their role in mediating long-term potentiation (LTP) in the cerebellum (Gandolfi et al.,
2017), or parvalbumin basket cells and their role in regulating plasticity (Karunakaran et al.,
2016).
3.5.4 The LC is a required component of the neural circuit underlying apnea-induced hLTF
Apnea-induced hLTF is is mediated by a noradrenergic-dependent mechanism (Lui et al., 2018,
Tadjalli et al., 2010). However, the source of noradrenaline responsible for mediating hLTF
remained, until now, unidentified. Here, I provide evidence indicating that LC cells are the likely
source of noradrenaline release onto hypoglossal motor neurons that ultimately underlies LTF

63
of inspiratory genioglossus activity. First, I provide correlative evidence showing that LC cells
are recruited during hLTF (Fig. 3.2B,C). I also show that noradrenergic LC cells project to and
innervate hypoglossal motor neurons (Fig. 3.4), confirming previous reports that LC neurons
innervate hypoglossal motor neurons (Rukhadze and Kubin, 2007). Taken together, these
observations suggest that recurrent obstructive apneas activate LC cells, which in turn release
noradrenaline onto hypoglossal motor neurons thereby triggering hLTF. Most importantly, I
showed that pharmacologically inactivating LC cells prevented the expression of apnea-induced
hLTF. This observation provides support for the causal link between apnea-induced LC
activation and its contribution to triggering LTF of inspiratory genioglossus activity. LC neurons
are anatomically and functionally poised to mediate hLTF and are, therefore, likely the source
of noradrenaline acting on hypoglossal motor neurons.
Although focal inactivation of the LC blocked hLTF expression, it did not suppress genioglossus
activity as LC inactivation did not reduce baseline inspiratory genioglossus activity, suggesting
that LC cells release negligible amounts of noradrenaline onto hypoglossal motor neurons
during anaesthetized conditions. Because previous studies show that inspiratory hypoglossal
motor outflow is facilitated by an endogenous noradrenergic drive during both natural
behaviors and anaesthesia, it is likely that other noradrenergic nuclei (e.g., A5 and/or A7 cell
groups) provide this drive (Fenik et al., 2008, Song and Poon, 2017).
3.5.5 Brainstem regions associated with apnea-induced hLTF
To date, most studies have examined the molecular pathways that trigger respiratory hLTF
within motor neurons (Devinney et al., 2015, Huxtable et al., 2014, Kinkead et al., 2001,
Neverova et al., 2007, Song and Poon, 2017), but my current study is important because it
identifies an intact circuit underlying apnea-induced respiratory motor plasticity. I propose that
hLTF is mediated by a tripartite circuit (NTS → LC → XII) and I base this on 5 lines of evidence:
1) apnea-induced hLTF is noradrenaline-dependent (Tadjalli, 2012); 2) inactivation of the NTS
prevents apnea-induced hLTF (Torontali, 2012); 3) noradrenergic LC cells were only active when

64
hLTF is triggered by apneas (i.e., increased c-Fos in animals that exhibit hLTF; Fig. 3.2); 4)
noradrenergic LC neurons project to hypoglossal motor neurons (Fig. 3.4); and, 5) inactivation
of LC cells during apneas prevented hLTF (Fig. 3.5D). Based on these results I propose that
recurrent obstructive apneas – similar to those experienced in obstructive sleep apnea –
modulate vagal feedback, which activates NTS cells. These cells in turn manipulate LC cells
(Aston-Jones et al., 1970, Lopes et al., 2016, Rukhadze and Kubin, 2007), which episodically
releases noradrenaline onto hypoglossal motor neurons thereby triggering motor neuron
plasticity and hence LTF of inspiratory genioglossus motor activity (Fig. 3.6).

65
Figure 3.6. Hypothesized circuitry responsible for hLTF. (A) Brain map showing the potential sources of noradrenaline mediating hLTF (red arrows). The locus coeruleus (LC) was activated alongside hLTF and the hypothesized circuit is outlined in purple (inset) and expanded in (B). Repeated obstructive apneas modulate vagal afferent activity, which terminates in the nucleus tractus solitarius (NTS). Cells in the NTS send excitatory projections to the noradrenergic cells of the locus coeruleus (LC), which in turn extend axons directly to the hypoglossal (XII) motor pool to modulate hypoglossal (and therefore genioglossus) activity, effectively triggering hypoglossal long-term facilitation (hLTF). I hypothesize that this is the neural circuit underlying LTF of inspiratory genioglossus motor output.
3.5.6 Methodological considerations
The c-Fos protein, though useful in identifying neural networks (Lu et al., 2006), undoubtedly
has limitations. The most notable is the inability to detect cells that have been inactivated or
inhibited (Chan and Sawchenko, 1994). This is important because hypercapnia can
hyperpolarize neurons (Ritucci et al., 1997); my intervention introduced a low hypercapnic load
but it is possible for some cell groups to have been hyperpolarized or inactivated. These

66
neurons would not have been visualized by my approach. Furthermore, not all activated
neurons express c-Fos. For example, hypercapnic load increases respiratory output without
changing c-Fos expression in phrenic or hypoglossal motor neurons (Haxhiu et al., 1996). It is
therefore possible for our proposed neural circuit to exclude regions that also facilitate the
elicitation of apnea-induced hLTF. For example, the A5 and A7 are noradrenergic structures
with known reciprocal connections to the LC, as well as direct connections to the hypoglossal
motor pool (Aldes et al., 1992, Byrum, 1987, Rukhadze and Kubin, 2007). It may therefore be
possible the involvement of these structures, as well as others, were not captured by my
approach but may still play a role in mediating hLTF. Nonetheless, my results suggest the LC to
be involved in apnea-induced hLTF.
Other methodological considerations include my choice in clonidine. In this study, I chose
clonidine due to its specificity to agonizing α2-adrenergic receptors. Other candidate drugs such
as yohimbine, simultaneously activates α1-adrenergic receptors and 5HT receptors, both of
which are present on LC neurons (Nakamura et al., 1988, Szabo et al., 2000). In addition, I chose
a dose that was found effective at decreasing overall noradrenaline levels in the brain to 30% of
baseline levels (Mair et al., 2005, Sakamoto et al., 2013), while maintaining a small enough
volume to confidently deliver the drug to a confined region. Nonetheless, perfusion of CLO can
spread beyond the targeted region of interest. It is possible that regions outside the LC were
affected, which could have influenced the manifestation of hLTF. For example, the Kolliker-Fuse
is a respiratory group that is rostral to the LC and may have been influenced by CLO perfusion,
thereby affecting the manifestation of apnea-induced hLTF. As such, it is critical that future
steps manipulate the LC with more precision, such as that of an optogenetic approach.
One caveat to this study is that LC inhibition can increase blood pressure by ~10 mmHg
(Bhaskaran and Freed, 1988), potentially influencing the absence of hLTF observed. However,
hLTF can still be generated even when blood pressure is elevated by 10–15 mmHg (Tadjalli,
2012), suggesting that increased blood pressure does not prevent apnea-induced hLTF
expression. My results are therefore physiologically important because they suggest that the

67
absence of hLTF following LC inactivation is not due to blood pressure changes but is due to
reduced noradrenergic drive to hypoglossal motor neurons.
Lastly, the largest caveat in this study is the comparison of clonidine-treated animals to hLTF-
expressing animals following repeated obstructive apneas. The field of LTF has always selected
animals that express LTF and intentionally separated them from non-responders. However, in
the study using focal inactivation of LC cells with clonidine, all animals were included in
statistical comparisons. This is problematic as I had reported that 35% of animals do not exhibit
hLTF following repeated apneas, which implies that the same percentage of animals would not
have exhibited hLTF regardless of the clonidine intervention. One potential solution would be
to identify animals that presumably would exhibit hLTF. For example, I showed that hLTF was
correlated with increased c-Fos expression at the LC, indicative of LC activation. It may be
possible to only include animals that show high c-Fos expression in the LC in the clonidine-
treated group. Unfortunately, my intervention involved focal inactivation of LC cells and, thus,
the increase in c-Fos expression observed in the LC of hLTF-expressing animals cannot be used
as a marker to distinguish responders from non-responders. In the next chapter, I introduce an
alternative statistical approach to address this issue.
3.5.7 Scientific importance and clinical significance
LTF is a form of neural plasticity that directly affects respiratory output. Apnea-induced hLTF is
unique in that its effects are localized to the upper airway (genioglossus), can be triggered in
vivo, uses a physiologically relevant trigger (repeated obstructive apneas), and occurs naturally.
hLTF is a form of respiratory plasticity that requires a trigger, where the plasticity itself occurs
on its own. Understanding the neural circuit underlying this plasticity is therefore critical to
opening a vast number of pharmacological approaches to augmenting genioglossus activity.
This is particularly relevant during sleep where muscle tone is decreased, potentially leading to
obstructive sleep apneas in humans (OSA) (Aboubakr et al., 2001, Fung and Chase, 2015,
Horner, 2008). These patients either do not exhibit hLTF, or their manifestation of hLTF is

68
insufficient at overcoming the apnea. In fact, LC cells are largely inactive during sleep (Aston-
Jones and Bloom, 1981, Fung et al., 1991, Szymusiak and McGinty, 2008), suggesting that the
circuits required for hLTF are dysfunctional during sleep. OSA has also been linked to a loss of
LC cells (Lim and Veasey, 2010), further supporting our findings that the LC is vital in providing
the noradrenergic drive onto hypoglossal motor neurons to mediate hLTF. Although respiratory
LTF was identified in humans, its potential role in mitigating reduced genioglossus muscle tone
in OSA remains to be determined. A recent study demonstrated LTF in humans could not be
elicited using a chemical trigger (hypercapnic/hypoxia) (Deacon et al., 2017). My results are
particularly important in this context because I have defined the potential neural circuitry that
mediates hLTF, providing novel therapeutic targets that could elicit hLTF. Here I show that hLTF
depends on noradrenergic LC cell activity, independent of hypercapnia/hypoxia, suggesting this
mechanism could be targeted to treat OSA.

69
Chapter Four – Optical LC Stimulation Triggers LTF of Inspiratory Genioglossus Motor Output
4.1 Summary
Respiratory long-term facilitation of genioglossus motor output (hLTF) is a form of respiratory
motor plasticity that can be elicited by repeated apneas or repeated bouts of hypoxia. Here, I
demonstrate that hLTF can be triggered in the absence of repeated apneas or hypoxia by
intermittently stimulating locus coeruleus (LC) neurons. In cells expressing channelrhodopsin2
(ChR2), I show that repeated optical stimulation of the LC in the same pattern as repeated
obstructive apneas can elicit hLTF. I also show that the LC is critical for hLTF as optical
inactivation of LC cells expressing halorhodopsin (eNpHR) prevented apnea-induced hLTF.
These results implicate the LC as being a critical component mediating hLTF. I then go on to use
c-Fos expression as an indicator of cell activity and found evidence to suggest that a minimum
stimulation threshold is required to elicit hLTF. I, therefore, propose that hLTF requires the
activation of the LC to release noradrenaline onto hypoglossal motor neurons to trigger hLTF.
4.2 Introduction
Respiratory LTF of inspiratory genioglossus motor output can be elicited by intermittent bouts
of hypoxia (Baker and Mitchell, 2000, Chowdhuri et al., 2015, Dale et al., 2017). However, it has
shown that LTF of hypoglossal/genioglossus activity can be elicited solely through the broncho-
pulmonary feedback system, such as through intermittent cooling of vagal afferents (Tadjalli et
al., 2010). More recently, hLTF was elicited transiently for 20 minutes while bypassing both the
broncho-pulmonary and chemosensory feedback altogether by directly stimulating the A5 or A7
noradrenergic cell group (Song and Poon, 2017). Here, I demonstrate that hLTF can be elicited
in the absence of repeated apneas or repeated bouts of hypoxia by using intermittent optical
stimulation of the LC, eliciting hLTF that persists for 60 min post intervention.

70
4.2.1 Triggers of LTF that act through the chemosensory or broncho-pulmonary feedback
system
To understand the mechanism underlying the trigger for hLTF, it is necessary to distinguish the
various factors that induce it. As mentioned earlier, the most common trigger involves
intermittent bouts of hypoxia to elicit LTF. This approach, 3 bouts of hypoxia (i.e., FiO2 10%)
separated by 5 minutes of normoxic breathing, is the most robust at eliciting phrenic LTF (pLTF)
(Dale et al., 2017, Devinney et al., 2015, Dodig et al., 2012) but is less consistent at eliciting
hypoglossal/genioglossus LTF (hLTF) (Baker-Herman and Strey, 2011, Janssen and Fregosi,
2000), though still possible (Fuller, 2005, Harris et al., 2006). This contrasts triggers used for
hLTF; repeated apneas or intermittent vagal cooling can elicit LTF of genioglossus muscle
activity but do not trigger pLTF (Tadjalli et al., 2010). This suggests that pLTF largely interacts
with the chemosensory feedback system whereas hLTF interacts with both chemosensory and
broncho-pulmonary feedback systems. Here I demonstrate a trigger that does not interact with
either feedback systems to trigger LTF of inspiratory genioglossus motor activity.
4.2.2 Triggers of LTF independent of the chemosensory and broncho-pulmonary feedback
systems
To date, only one study has shown a trigger that does not interact with the respiratory
feedback systems in an in vivo model (Song and Poon, 2017). Song and Poon (2017)
demonstrated a form of hypoglossal/genioglossus LTF persisting for 20 minutes following
intermittent optical stimulation of the A5 or A7 noradrenergic cell group in anaesthetized,
spontaneously breathing rats. Although the duration of hLTF persisted for 20 minutes, differing
from the most commonly reported form of LTF that lasts 60 minutes, this was the first
demonstration of hLTF that was elicited in the absence of chemosensory or broncho-pulmonary
feedback in vivo. Here I demonstrate that prolonged hLTF persisting for 60 minutes can be
triggered by intermittent optical stimulation of the LC.

71
4.2.3 The LC and its potential role in hLTF
In Chapter 3, I showed that c-Fos expression is associated with apnea-induced hLTF expression,
suggesting that apnea-induced hLTF may be induced by activation of noradrenergic LC cells,
which release noradrenaline onto hypoglossal motor neurons. I also demonstrated that the LC
is critical for the manifestation of hLTF as its inactivation prevented apnea-induced hLTF. The
role of the LC in mediating hLTF has not been tested directly, therefore my next goal was to
determine whether activation of noradrenergic LC cells alone can trigger hLTF. Specifically, LC
neurons expressing ChR2 via infection with a viral vector (AAV5-hSyn-ChR2(H134R)-mCherry)
were activated using intermittent light pulses.
It is important to note that the activity of LC cells before, during, or after hLTF expression has
not been reported. As a result, it is not possible to mimic the exact pattern of LC activity using
light. However, LC cells have been reported to be maximally active at 5 Hz (Kogan et al., 1992).
Therefore, I aimed to optically stimulate ChR2-expressing LC cells at 5 Hz. In addition, since
repeated apneas can trigger hLTF, I aimed to optically stimulate the LC in the same pattern as
repeated obstructive apneas (i.e., 10 episodes of stimulation, each 15 seconds in duration
separated by 1 minute).
4.3 Results
4.3.1 LC cells equally infected by viral vectors across all groups
Before investigating whether optical manipulation of LC neurons influences hLTF, I first wanted
to determine whether there was an equal viral infection rate in animals that received the empty
viral vector (AAV5-hSyn-mCherry), or the viral vector containing stimulating opsin (AAV5-hSyn-
ChR2(H134R)-mCherry) or inhibitory opsin (AAV5-hSyn-eNpHR3.0-mCherry). This is important
as it addresses the quality of the viral vectors used across all treatment groups. To determine
whether LC neurons were equally infected, I quantified the total number of cells expressing the

72
mCherry reporter protein in the LC across all groups. Specifically, all mCherry positive cells were
manually counted for each experimental group with the experimenter blinded to the treatment
(see Chapter 2, section 2.9 for additional details). My cell counts revealed no difference in
mCherry expression across all groups (1-way ANOVA, F=1.153, p=0.3333 Figure 4.1A,B),
suggesting viral infection rates were equal for all animals used in this study.
Next, I aimed to determine the percentage of virally infected noradrenergic neurons. The viral
vector used here non-specifically targets all cells, but my goal is to determine whether
noradrenergic LC neurons mediate hLTF. Therefore, I quantified the number of virally infected
(i.e., mCherry expressing) cells co-expressing tyrosine hydroxylase and found that
approximately 61 ± 14% of noradrenergic LC cells were infected.
Lastly, I aimed to verify that virally infected cells expressing ChR2 or eNpHR were functional
(i.e., responded to light exposure). To determine whether the virally-expressed ion channel,
ChR2, was functional within LC neurons, I optically stimulated LC neurons (432nm, 40mW, 15s
at 5 Hz separated by 1 minute of no stimulation repeated 10 times) and found c-Fos expression
in LC cells to be increased by 49 ± 13% compared to animals absent ChR2 (unpaired t-test, LC
Stim. vs Non-ChR2-expressing mCherry, t(7)=4.326, p=0.0035, Fig. 4.1C,D), suggesting light
exposure on LC neurons did increase LC activity. To determine whether the virally-expressed
ion channel, eNpHR, was functional within LC neurons, I optically inhibited LC neurons
expressing (532nm, 40mW, continuously) while simultaneously attempted to activate LC cells
using apnea-induced hLTF (15s apneas separated by 1 minute repeated 10 times). Following
this intervention, I found fewer c-Fos positive neurons in the LC of animals with the LC
inactivated compared to the LC of animals absent the inhibitory opsin and exhibiting hLTF
(unpaired t-test, LC inactivation + apneas vs Non-eNpHR-expressing mCherry + apneas,
t(8)=4.305, p=0.0026, Fig. 4.1E), suggesting light exposure on LC neurons inhibited their activity.

73

74
Figure 4.1. Increased or decreased c-Fos expression following light-induced manipulation to ChR2- or eNpHR-expressing LC cells. Following microinjection of a viral construct AAV5-hSyn-ChR2(H134R)-mCherry (n=13), AAV5-hSyn-eNpHR3.0-mCherry (n=6), or AAV5-hSyn-mCherry (n=6), expression of mCherry, tyrosine hydroxylase (TH), and c-Fos was quantified with experimenters blinded to the treatment. All infected animals expressed an equal number of mCherry positive cells (A,B). (C) Histological example showing LC neurons that are mCherry positive (red) to identify virally infected cells, TH positive (green) to identify noradrenergic cells, the overlay (third panel), and c-Fos (black) to identified activated cells. Visualization of c-Fos was under bright field and therefore could not be overlaid with fluorescent images in earlier panels. White arrows point to infected noradrenergic cells that were activated (i.e., c-Fos positive). Yellow arrow points to infected noradrenergic cell that was considered c-Fos negative (i.e., not activated). (D) Cells infected with the excitatory opsin, ChR2 (n=6, blue), displayed a significant increase in c-Fos expression following intermittent light stimulation compared to animals absent any opsin (non-ChR2-expressing mCherry, n=3, white). Approximate location of c-Fos positive cells in the LC (dotted outline) are shown on the right for animals absent any opsin (non-ChR2-expressing mCherry) and animals expressing ChR2. (E) Cells infected with the inhibitory opsin, eNpHR (n=6, green), displayed a significant decrease in c-Fos expression following light exposure and repeated obstructive apneas compared to animals absent any opsin (non-eNpHR-expressing mCherry + Apneas, n=4, white) but received light exposure and repeated apneas. Approximate location of c-Fos positive cells are shown on the right for animals absent any opsin (non-eNpHR-expressing mCherry) and animals expressing eNpHR following repeated apneas. *denotes significance (p<0.05) between groups. Data presented as mean + SEM.
4.3.2. Baseline genioglossus motor activity is decreased during optical inactivation of eNpHR-
expressing LC neurons
My next goal was to determine if LC stimulation or inhibition affected respiratory output.
Therefore, to address this, I quantified respiratory output directly after optical manipulation of
LC cells. I hypothesized that hypoglossal motor neurons would increase in activity following LC
stimulation because hypoglossal motor neurons had been previously demonstrated to increase
in activity following application of phenylephrine or norepineprine (Chan et al., 2006, Neverova
et al., 2007, Parkis et al., 1995). However, when LC neurons were exposed to intermittent light
stimulation, I found no change in genioglossus amplitude, or any other respiratory variable
measured (paired t-test, genioglossus: t(8)=0.8608, p=0.4144, diaphragm: t(3)=1.511, p=0.2279,
respiratory frequency: t(3)=1.965, p=0.1442, O2 saturation: t(3)=0.1060, p=0.9223, end-tidal CO2:
t(2)=0.3183, p=0.7804. Fig. 4.2A,B,E). The lack of increase in genioglossus output during LC
stimulation may be due to insufficient noradrenaline release to augment genioglossus motor
output. Similarly, no change in genioglossus output was observed in a study that optically
stimulated noradrenergic groups (A5 and A7), which has greater noradrenergic innervations to

75
the hypoglossal motor pool (Song and Poon, 2017). In contrast, when eNpHR-expressing LC
neurons were inactivated with a continuous pulse of light, I found genioglossus amplitude
decreased by 19 ± 7% (paired t-test, t(8)=2.506, p=0.0366, Fig. 4.2C,D), but no change was
observed in any other respiratory variable measured (paired t-test, diaphragm: t(3)=0.5763,
p=0.6048, respiratory frequency: t(3)=1.708, p=0.1862, O2 saturation: t(3)=0.2496, p=0.8190,
end-tidal CO2: t(3)=0.3068, p=0.3068. Fig. 4.2E). The decrease in genioglossus motor output
following optical inhibition of eNpHR-expressing LC neurons suggest that LC neurons provide an
endogenous noradrenergic drive to hypoglossal motor neurons.

76

77
Figure 4.2. Genioglossus motor output was decreased during optical LC inactivation. (A) A raw trace of integrated genioglossus amplitude (∫GG EMG) recorded from an anaesthetized spontaneously breathing rat, before (baseline) and during LC stimulation (dotted blue line). Bottom panel depicts a higher temporal resolution of genioglossus amplitude during the switch from light off to light on. (B) Group data (n=11) comparing genioglossus amplitude at baseline (black bar) and during intermittent LC stimulation (blue bar), where no significant difference was observed. (C) A raw trace showing genioglossus activity before (baseline) and during LC inactivation (green line). Bottom panel shows higher temporal resolution genioglossus activity before and after the laser was turned on and the subsequent decrease in genioglossus amplitude. (D) In the group data (n=9), baseline genioglossus amplitude (black bar) was significantly decreased following LC inactivation (green bar) by 19 ± 7% from baseline. (E) In both groups (LC activation or inactivation), integrated diaphragm amplitude, respiratory frequency, oxygen saturation levels and end-tidal CO2 levels were unaffected. Data presented as mean + SEM. *denotes significance (p<0.05) between groups.
4.3.3 LTF of genioglossus motor output is elicited after intermittent stimulation of ChR2-
expressing LC neurons
My next goal was to investigate whether intermittent stimulation of LC neurons could trigger
hLTF. I hypothesized that the activation of the LC would cause intermittent release of
noradrenaline onto hypoglossal motor neurons to trigger hLTF. To test this hypothesis, I
modelled a stimulation protocol that is similar to repeated obstructive apneas by optically
stimulating LC neurons in the same pattern (i.e., stimulation at 5 Hz for 15 seconds separated
by 1 minute of no stimulation, repeated 10 times). Following this optical stimulation protocol, I
found that repeated optical stimulation of ChR2-expressing LC neurons increased genioglossus
amplitude by 41 ± 10% at 60 min post-stimulation (1-way RM ANOVA, F=3.629, p=0.0167, Fig.
4.3A-C), suggesting intermittent LC stimulation can trigger hLTF.
The viral vector used was non-specific and therefore infected all neurons. As a result, the
location of the optic probe tip is critically important in determining whether the LC is truly being
stimulated. To address the non-specific nature of the viral vector used, I stimulated cells 0.2-0.4
mm lateral to the LC in an identical fashion (Fig. 4.3G). I found that repeated stimulation of cells
outside the LC had no effect on genioglossus activity (1-way RM ANOVA, F=3.898, p=0.8289,
Figure 4.3C), or any effect on other respiratory variables measured (2-way RM ANOVA,
diaphragm: F=0.5053, p=0.7320, respiratory frequency: F=1.329, p=0.2726, O2 saturation:

78
F=0.5756, p=0.6820, Figure 4.3D-F). This suggests that the manifestation of hLTF was due to the
stimulation of LC cells, and not the cells surrounding the LC.

79

80
Figure 4.3. LTF of genioglossus motor activity is elicited after intermittent optical stimulation of LC neurons. (A) Integrated inspiratory genioglossus motor output (∫GG EMG) recorded from an anaesthetized spontaneously breathing rat, depicting baseline genioglossus amplitude and the subsequent increase in EMG amplitude after intermittent LC stimulation (i.e., hLTF). (B) High-temporal resolution EMG traces showing genioglossus activity at baseline, 15, 30, 45, and 60 min after intermittent LC stimulation. (C) Group data showing an increase in inspiratory genioglossus activity following intermittent LC stimulation (n=8, blue bars) compared to animals given the same intervention but outside of the LC nuclei (i.e., Off-Target Stimulation, n=6, black bars) at 15, 30, 45, and 60 min. Dotted line represents percent baseline activity. Intermittent LC stimulation induced an increase in inspiratory genioglossus amplitude of 41 ± 10% at 60 minutes. In both groups, inspiratory diaphragm amplitude (∫Dia EMG), respiratory frequency, and oxygen saturation levels were unaffected over time (D-F). (G) Optic probe tract locations for animals that received on-target LC stimulation (blue circles), or off-target stimulation (grey circles). Dotted outline represents the LC. Each shade represents an individual animal. Data is presented as mean + SEM. * denotes a significant difference (p<0.05) from baseline.
4.3.4 Intermittent light exposure on non-ChR2-expressing mCherry LC neurons does not
trigger hLTF
Recent reports have suggested that light exposure in naïve mice (i.e., mice absent any opsin)
can cause heat-induced cell damage (Qian and Gu, 2005), heat-induced cell firing (Reig et al.,
2010, Stujenske et al., 2015), and photodilation of blood vessels (Rungta et al., 2017). To
control for the potential adverse effects caused by light exposure, I performed an identical
stimulation protocol in animals infected with a control viral vector (i.e., AAV5-hSyn-mCherry).
This viral vector is identical to the viral vector used in the treatment group but absent the light-
sensitive ion channel, ChR2. Repeated light exposure should, therefore, have no effect on LC
cells and thus should not trigger hLTF.
Here, I demonstrated that optical exposure of non-ChR2-expressing mCherry LC neurons did
not affect respiratory activity throughout the recording period and that light exposure had no
effect on genioglossus activity throughout the 60-minute time period (1-way RM ANOVA, Non-
ChR2-expressing mCherry, F=0.7763, p=0.5535, Fig. 4.4 C,D). Furthermore, no changes were
observed in any other respiratory variables measured (2-way RM ANOVA, Int. LC Stim. vs Non-
ChR2-expressing mCherry, diaphragm amplitude: F=0.2242, p=0.9233, respiratory frequency:
F=0.8425, p=0.5058, O2 saturation: F=0.5823, p=0.6772. Fig. 4.4E-G). These data indicate that

81
light per se is not responsible for hLTF and as demonstrated in section 4.3.3, hLTF is induced by
intermittent activation of LC neurons themselves.
4.3.5 hLTF expression requires an intermittent pattern of LC stimulation
Previous studies have demonstrated that an intermittent stimulus is required to elicit plasticity
(Baker and Mitchell, 2000, Bliss and Lomo, 1973). In the context of LTF, repeated episodes of
hypoxia were required whereas a single continuous episode of hypoxia did not elicit pLTF
(Baker and Mitchell, 2000). This was again demonstrated when intermittent cooling of vagal
afferents triggered hLTF, but a single cooling episode of equal duration did not trigger hLTF
(Tadjalli, 2012). I wanted to determine whether the intermittent nature of optical stimulation
was required to trigger hLTF. Here, I show that continuous light exposure encompassing the
duration of the optical stimulation protocol did not trigger hLTF. To do this, I continuously
stimulated ChR2-expressing LC cells for the duration equal to the total time taken for the
intermittent optical stimulation protocol (i.e., 5 Hz for 12.5 minutes continuously). With
continuous LC stimulation, I found that genioglossus activity decreased to 70 ± 19% of baseline
levels following initial exposure to light (paired t-test, genioglossus at baseline vs during
continuous stimulation: t(4)=3.418, p=0.0268. Fig. 4.4A) but had returned to baseline levels by
the 15-minute time point, where it remained consistent for the rest of the recording period (1-
way RM ANOVA, F=0.4031, p=0.8037. Fig. 4.4C,D). Following continuous LC stimulation, I again
did not observe any change over time in other respiratory variables measured (2-way RM
ANOVA, Int. LC Stim. vs Cont. Stim., Diaphragm: F=0.5053, p=0.7320, respiratory frequency:
F=0.0381, p=0.9971, O2 saturation: F=1.077, p=0.3806. Fig. 4.4E-G), suggesting continuous LC
stimulation had minimal effect on respiratory output.
The decrease in GG activity following continuous LC stimulation may be due to insufficient
noradrenaline release. A previous study has shown that intermittent electrical stimulation of
the LC caused more release of noradrenaline than continuous stimulation (Florin-Lechner et al.,

82
1996). Since no increase in genioglossus activity was observed following intermittent LC
stimulation, as demonstrated in section 4.3.2., it is not surprising that no increase in
genioglossus activity was observed when the LC was stimulated continuously. The decrease in
GG motor output may suggest that continuous stimulation caused auto-inhibition of LC cells or
potentially induced depolarization block following prolonged LC stimulation (Adams and Foote,
1988). This is supported by histological c-Fos expression in the LC following continuous LC
stimulation. Specifically, continuous LC stimulation had fewer activated cells (i.e., c-Fos positive
cells) than intermittent LC stimulation (unpaired t-test, Int. LC Stim. vs Continuous LC Stim.,
t(8)=5.163, p=0.0009. Fig. 4.4B), suggesting LC cells were less activated following continuous
stimulation.

83

84
Figure 4.4. Intermittent LC stimulation activates ChR2-expressing LC neurons more than non-ChR2-expressing mCherry LC neurons or continuous LC stimulation. (A) Group data showing integrated genioglossus activity (∫GG EMG) decreased following continuous light exposure (purple bars, n=5), but had no effect in animals with no opsins (i.e., non-ChR2-expressing mCherry, white bars, n=6) relative to percent baseline (black bars). (B) Group data showing more c-Fos positive cells in ChR2-expressing animals that received intermittent LC stimulation (blue bars, n=6) and exhibited hLTF compared to non-ChR2-expressing mCherry (white bars, n=3) or animals given continuous LC stimulation (purple bars, n=4). (C) Representative EMG traces of integrated inspiratory genioglossus activity recorded from an anesthetized spontaneously breathing rat after intermittent light pulses in an animal with no opsin (i.e., non-ChR2-expressing mCherry, top trace) or continuous light exposure in ChR2-expressing LC cells (i.e., Continuous LC Stimulation, bottom trace). (D) Group data showing no change in inspiratory genioglossus activity in non-ChR2-expressing mCherry and continuous LC stimulation groups at 15, 30, 45, and 60 min compared to ChR2-expressing animals that received intermittent LC stimulation. Dotted line represents percent baseline activity. In all groups, diaphragm amplitude (∫Dia EMG), respiratory frequency, and oxygen saturation (E-G) were unaffected over time. Data is presented as mean + SEM. * denotes a significant difference (p<0.05) from baseline.
4.3.6 Intermittent LC stimulation elicits hLTF at the same frequency as repeated apneas
It is important to note that hLTF does not always manifest following repeated apneas or
repeated LC stimulation. In studies of long-term potentiation, intermittent stimulation triggered
plasticity 50-90% of the time (Abraham et al., 1993, Watanabe et al., 2002). In the field of LTF,
animals that expressed LTF were intentionally separated from non-responders but the percent
of animals that did not exhibit LTF was never reported. In Chapter 3, 35% of the animals did not
exhibit hLTF following repeated obstructive apneas. Here, I found that intermittent LC
stimulation triggered hLTF 73% of the time (i.e., 27% of animals did not exhibit hLTF following
intermittent LC stimulation). However, in animals where no intervention was performed (i.e.,
time control, non-ChR2-expressing mCherry and off-target groups), hLTF spontaneously
occurred in 25% of animals. To determine whether intermittent LC stimulation had an influence
on hLTF expression, and that it was not a result of random chance, I performed a chi-square
test to determine whether my observed probability fit within an expected distribution.
Intermittent LC stimulation significantly correlated with hLTF expression (chi-square test, Int. LC
Stimulation vs controls, chi2=10.8107, p<0.001), suggesting it was not due to random chance.
To further emphasize that intermittent LC stimulation increases the probability of hLTF
expression, I also performed a Firth logistic regression to determine whether LC stimulation can

85
predict the probability of hLTF expression. This differs from a chi-square test because a Firth
logistic regression provides a model to predict the likelihood of an outcome following an
intervention, whereas a chi-square test measures the strength of the relationship, akin to a
correlation. Specifically, using a Firth logistic regression, I found that hLTF was more likely to
manifest than controls (Firth logistic regression, Int. LC stimulation vs controls, p=0.004. Fig.
4.5). This shows that hLTF expression following intermittent LC stimulation is not due to
random chance but can be triggered through LC stimulation.
Figure 4.5. Probability of hLTF expression was increased following intermittent stimulation of the LC. Following intermittent LC stimulation (n=8, blue), hLTF expression was more likely to manifest compared to other groups, which include animals given intermittent stimulation with no opsin (i.e., non-ChR2-expressing mCherry, n=6, orange), given continuous LC stimulation (n=4, purple), or given intermittent stimulation outside of the LC (i.e., off-target stimulation, n=6, black). Each line represents an animal that received one of the interventions. Intermittent LC stimulation is significantly more likely to augment genioglossus motor output above baseline levels at 60 minutes post-intervention.

86
Lastly, I compared the frequency of hLTF expression following repeated apneas to the
frequency of hLTF expression following intermittent LC stimulation to determine whether
intermittent LC stimulation had a higher probability of eliciting hLTF than repeated apneas. I
hypothesized that direct modulation of the source of noradrenaline in the proposed hLTF
pathway would increase the probability for hLTF expression compared to repeated apneas.
Using a chi-square test, I found that the occurrence of hLTF was not different whether the
trigger was repeated apneas or intermittent LC stimulation (chi-square test, Repeated Apneas
vs Int. LC Stim., chi2=0.2017, p=0.653). When I compared the same groups with a Firth logistic
regression analysis, I again found no difference in the probability of hLTF expression between
either trigger (Firth logistic regression, Repeated Apneas vs Int. LC Stim., p=0.654). These results
support my finding that intermittent LC stimulation increases the probability for hLTF
expression and it elicit hLTF in an equally consistent manner as the repeated apnea trigger.
4.3.7 hLTF requires a minimum threshold activation of LC cells
Following LC stimulation, 27% of animals did not exhibit hLTF. My next goal was to examine
why hLTF was not expressed in these animals. One possibility could be due to fewer infected
noradrenergic LC neurons. Therefore, I quantified the total number of double-labelled mCherry
and tyrosine hydroxylase (TH) positive cells in animals that did and did not exhibit hLTF
following LC stimulation. What I found was that the number of cells expressing both mCherry
and TH were not significantly different between animals that exhibited hLTF and those that did
not (unpaired t-test, ChR2 hLTF vs ChR2 No hLTF, t(7)=1.086, p=0.3134. Fig. 4.6A). This suggests
that the number of infected noradrenergic LC cells was not the reason for a lack of hLTF
observed following intermittent LC stimulation in these animals.
Next, I aimed to determine whether the animals that did not exhibit hLTF was a result of
insufficient LC stimulation. Although there were similar levels of mCherry and TH expression,
this may not reflect the same level of LC activity during light exposure. I, therefore, examined

87
the c-Fos expression in noradrenergic LC cells of animals that exhibited hLTF and those that did
not. What I found was that there were a greater number of double-labelled c-Fos and TH
positive cells in animals that exhibited hLTF compared to animals that did not (unpaired t-test,
ChR2 hLTF vs ChR2 No hLTF, t(7)=2.499, p=0.0411. Fig. 4.6B), suggesting the lack of hLTF in these
animals may be a result of insufficient LC stimulation. This is supported by my results in Chapter
3 that showed higher c-Fos expression in animals that exhibited hLTF compared to animals that
did not following repeated apneas (Lui et al., 2018). In addition, this is further supported by
studies that showed noradrenergic LC neurons naturally fire synchronously when sufficiently
stimulated (Aston-Jones and Bloom, 1981, Christie et al., 1989, Ishimatsu and Williams, 1996). It
may therefore be possible that insufficient LC stimulation did not meet the threshold required
to trigger a synchronous response in LC activity and therefore did not elicit hLTF.

88
Figure 4.6. Hypoglossal LTF requires a minimum LC stimulation threshold. (A) Group data showing equal amounts of mCherry and tyrosine hydroxylase (TH) expression in animals that expressed hLTF (Int. LC Stim. (hLTF), n=6, blue bar) compared to animals that did not express hLTF (Int. LC Stim. (No hLTF), n=3, grey bars). (B) Group data showing animals that exhibited hLTF had c-Fos expression increased by 43 ± 11% in noradrenergic cells compared to animals that did not express hLTF. (C) An example of LC activity represented by c-Fos expression (black nuclei) in animals given intermittent LC stimulation and exhibiting hLTF (left) or intermittent LC stimulation but did not exhibit hLTF (right). Dotted outline identifies the LC. Data is presented as mean + SEM. * denotes a significant difference (p<0.05).

89
4.3.8 Inactivation of the LC abolishes apnea-induced hLTF
Lastly, I aimed to determine whether the LC is critical for apnea-induced hLTF. In Chapter 3, I
demonstrated that pharmacological inactivation of the LC with clonidine prevented apnea-
induced hLTF. However, pharmacological approaches have limitations including the spread of
the drug and the timing of the drug’s effect persisting after initial application. For example,
application of clonidine could inhibit nearby cells such as the subCoeruleus (subC), which may
provide a tonic drive on hypoglossal motor neurons (Chan et al., 2006); the unintended
inactivation of the subC by clonidine may persist after the intervention. An inhibitory
optogenetic approach could mitigate these issues. In addition, it may also be possible that
repeated stimulation of the LC activates the hLTF circuit without the LC being directly involved
in the circuit itself. To determine if the LC is part of the hLTF circuit, I optically silenced LC
activity during repeated obstructive apneas. Specifically, LC neurons expressing halorhodopsin
(eNpHR) via infection with a viral vector (AAV5-hSyn-eNpHR3.0-mCherry) were inhibited using a
continuous light source. Since repeated apneas can trigger hLTF, I aimed to optically inhibit
eNpHR-expressing LC cells during this trigger. If the LC is indeed mediating hLTF, then I
hypothesized that optical inactivation of the LC would prevent apnea-induced hLTF.
Similar to my results using pharmacological inactivation of the LC, optical inactivation of
eNpHR-expressing LC neurons prevented apnea-induced hLTF. In fact, a significant decrease in
genioglossus motor output at 60 minutes was observed (1-way RM ANOVA, F=4.874, p=0.0041,
Figure 4.7A,B) but other respiratory variables were unaffected (2-way RM ANOVA, LC
Inactivation + apneas vs non-eNpHR-expressing mCherry + apneas, diaphragm amplitude:
F=1.128, p=0.3535, respiratory frequency: F=0.4403, p=0.7789, O2 saturation: F=1.032,
p=0.3998, end-tidal CO2: F=1.552, p=0.2023. Fig. 4.6C-F). These findings support my results
from Chapter 3 demonstrating that LC activity is critical for apnea-induced hLTF.
To ensure that light itself did not influence hLTF expression, or that virally infected cells did not
compromise LC function, I used a control viral vector that is absent the inhibitory opsin (i.e.,

90
AAV5-hSyn-mCherry). In these animals, I performed the same intervention exposing the LC to
continuous beam of green light while simultaneously delivering repeated apneas. I hypothesize
that LC cells would not be inhibited due to the absence of the light-sensitive inhibitory opsin
(eNpHR) and repeated apneas should therefore elicit hLTF. Congruent with earlier uses of the
control viral vector, repeated apneas were able to elicit hLTF with genioglossus amplitude
reaching 120 ± 8% above baseline (1-way RM ANOVA, F=2.771, p=0.0466, Figure 4.7A,B). This
suggests that LC inactivation prevents apnea-induced hLTF and the LC is a critical component of
the neural circuit underlying apnea-induced hLTF.

91

92
Figure 4.7. Optical inactivation of the LC prevents apnea-induced hypoglossal LTF. (A) Representative EMG traces of integrated inspiratory genioglossus activity (∫GG EMG) recorded from an anaesthetized, spontaneously breathing rat after LC inactivation (top) or non-eNpHR-expressing mCherry control (bottom) at baseline, 15, 30, 45, and 60 min following repeated apneas. (B) Group data showing inspiratory GG activity in animals that did not express the inhibitory opsin (non-eNpHR-expressing mCherry, n=6, white bars) increased by 120 ± 8% following repeated apneas (i.e., hLTF). However, when the LC was inactivated (eNpHR, n=9, green bars), repeated apneas produced a decrease in GG amplitude over time. In both groups, diaphragm activity, respiratory frequency, oxygen saturation, and end-tidal CO2 levels (C-F) were unaffected over time. Dotted line represents percent baseline. Data are presented as mean + SEM. * denotes a significant difference (p<0.05).
Although the above findings suggest LC inactivation prevents apnea-induced hLTF, there is one
caveat in the statistical analysis that requires additional examination. Specifically, the analysis
above compares animals that exhibited apnea-induced hLTF to animals that did not exhibit hLTF
following LC inactivation. However, as mention in section 4.3.6, about 27% of animals do not
exhibit hLTF following intermittent LC stimulation, and about 35% of animals do not exhibit
hLTF following repeated obstructive apneas. This may skew my earlier statistical analysis
because it implies that the 35% of animals would not have exhibited hLTF regardless of my
intervention at the LC.
There is no precedent on how to address this caveat as previous LTF studies follow the same
statistical analysis applied above (Bach and Mitchell, 1996, Baker-Herman and Mitchell, 2002,
Dale et al., 2017, Fuller et al., 2001, McGuire et al., 2005). Here, I introduce a statistical
approach that addresses this problem by including all animals (i.e., animals that exhibit hLTF
and non-responders) in the statistical analysis. In addition to the chi-square test and Firth
logistic regression that provides insight into whether my intervention prevented apnea-induced
hLTF (i.e., not due to random chance), I also perform an ordinary least squares linear regression
(OLS). This differs from the chi-square test and Firth logistic regression in that it uses the
measured genioglossus EMG values across all groups and includes all animals (responders and
non-responders). A chi-square test and Firth logistic regression are useful when determining
whether a categorical outcome variable (i.e., did hLTF occur, yes or no). An OLS analysis is more

93
stringent in that measured genioglossus EMG values are taken into account to determine
whether the intervention affected genioglossus amplitude at the 60-minute time point.
Following a chi-square test, I found that LC inactivation significantly correlated with an absence
of hLTF expression (chi-square test, LC Inactivation + Apneas vs non-eNpHR-expressing mCherry
+ Apneas, chi2=9.6923, p=0.002). Similarly, upon performing a Firth logistic regression analysis,
I found a significant difference in the probability of hLTF expression when the LC is inactivated
(Firth logistic regression, LC inactivation + Apneas vs non-eNpHR-expressing mCherry + Apneas,
p=0.022. Fig. 4.8). Lastly, upon performing OLS analysis, I found that LC inactivation prevented
apnea-induced hLTF (OLS, LC inactivation + apneas vs non-eNpHR-expressing mCherry + apneas,
R2=0.3629, F(19)=10.82, β=-0.40125, p=0.004). Taken together, this suggests that the LC is critical
for apnea-induced hLTF.

94
Figure 4.8. hLTF did not manifest following LC inactivation. Following LC inactivation (eNpHR, n=9, green), repeated apneas did not elicit hLTF. This is in contrast to the results observed in animals that were given the same intervention but had no opsin (non-eNpHR-expressing mCherry, n=6, blue), where repeated apneas continued to elicit hLTF in 65% of animals. Repeated apneas had a significantly greater probability at inducing an increase in genioglossus motor output above baseline at 60 minutes than when the LC was inactivated and hLTF never occurred.
4.4 Discussion
Long-term facilitation of inspiratory genioglossus motor output can be elicited by various
triggers. Here I presented a novel trigger that can elicit hLTF without interacting with the
chemosensory or broncho-pulmonary feedback systems. By intermittently stimulating LC
neurons in the same pattern as repeated apneas, I was able to increase inspiratory genioglossus
motor output for 60 minutes post-intervention, with no effects on other respiratory variables
measured (i.e. diaphragm amplitude, respiratory frequency, and blood oxygen saturation).
Furthermore, I showed that hLTF was not elicited when LC neurons were optically inactivated.

95
These findings suggest that the LC is essential for hLTF as manipulation of the LC alone can
trigger hLTF and inactivation of LC prevents apnea-induced hLTF.
4.4.1 LC provides an endogenous noradrenergic drive to hypoglossal motor neurons
Genioglossus motor output is under noradrenergic state-dependent modulation (Chan et al.,
2006). Here I provide evidence demonstrating the presence of an endogenous noradrenergic
drive arising from the LC onto hypoglossal motor neurons. In chapter three, I showed that the
hypoglossal motor pool was directly innervated by noradrenergic LC neurons. I also showed
that pharmacological inactivation of the LC had no effect on baseline genioglossus activity
(Chapter 3), which would suggest that the LC does not provide a tonic drive to hypoglossal
motor neurons. However, it is possible that my pharmacological approach did not adequately
inhibit LC neurons. The concentration of clonidine used was shown to be effective at reducing
cortical noradrenaline levels by approximately 72% (Sakamoto et al., 2013). The LC is the sole
contributor of noradrenaline to the cortex; the remaining active noradrenergic LC neurons may
therefore have been sufficient at providing the tonic drive necessary to maintain genioglossus
motor output at baseline levels, but insufficient at mediating hLTF. By using an optogenetic
approach, I could inactivate cells using light to penetrate cells within a small cone (Gradinaru et
al., 2010, Yizhar et al., 2011) possibly inhibiting more cells than with a pharmacological
approach. Following LC inactivation, basal genioglossus amplitude decreased by 19 ± 7% of
baseline, suggesting the presence of an endogenous noradrenergic drive arising from the LC
that acts on hypoglossal motor neurons. Despite reports of limited innervation (Aldes et al.,
1992, Rukhadze and Kubin, 2007), these findings suggest that a portion of the tonic
noradrenergic drive at the hypoglossal motor pool stems from the LC. My findings also showed
that continuous LC stimulation did not increase genioglossus muscle activity nor trigger hLTF. In
fact, a decrease in genioglossus amplitude was observed upon continuous LC stimulation,
suggesting a decrease in LC activity with prolonged excitation. The reason for the decrease in
genioglossus motor output observed here is not known, but was likely due to auto-inhibition or

96
depolarization block where excessive activation of LC cells can lead to a decrease in LC activity
(Adams and Foote, 1988).
4.4.2. Baseline genioglossus motor activity is unaffected during stimulation of ChR2-
expressing LC neurons
We observed genioglossus motor output at baseline and found that during intermittent light
stimulation of ChR2-expressing LC neurons, genioglossus motor output did not change. Similar
results were observed in other studies showing baseline genioglossus activity to remain
unchanged during optical stimulation of ChR2-expressing neurons in the A5 or A7 noradrenergic
cell groups (Song and Poon, 2017). This suggests that the immediate effect of intermittent
optical stimulation of noradrenergic cell groups likely does not release enough noradrenaline to
directly augment genioglossus motor output, but instead may be changing the pattern of LC
activity and thereby noradrenaline release.
In addition, studies that showed an increase in genioglossus or hypoglossal activity following
application of noradrenaline or phenylephrine use concentrations that are at minimum, 1000
fold higher than endogenous noradrenaline levels. For example, microdialysis in the rat
prefrontal cortex show that electrical LC stimulation increases noradrenaline levels to
approximately 0.0006 µM (Florin-Lechner et al., 1996), but studies that directly applied
noradrenaline or phenylephrine to hypoglossal motor neurons had concentrations ranging from
10 µM (Neverova et al., 2007), 50 µM (Parkis et al., 1995), or 1000 µM (Chan et al., 2006,
Schwarz et al., 2014). The concentrations of noradrenaline at the hypoglossal motor pool during
LC stimulation (intermittent or continuous) may therefore be too low to induce an immediate
response in genioglossus amplitude.

97
4.4.3 Stimulation of ChR2-expressing LC neurons trigger LTF of inspiratory genioglossus motor
output
In Chapter 3, I showed an increase in c-Fos expression at the LC correlated with apnea-induced
hLTF. Here, I showed that intermittent stimulation of the LC in the same pattern as repeated
apneas elicits hLTF. My controls support this claim as intermittent light pulses did not elicit hLTF
when absent the excitatory opsin ChR2. More importantly, I also showed that intermittent
stimulation lateral to the LC does not trigger hLTF. These findings suggest that stimulation of
the LC itself is required for hLTF, although it may be possible that stimulation of cells in the LC
that are not noradrenergic in nature may have contributed to hLTF. These studies used a non-
specific viral vector to target cells in the region of the LC in non-transgenic rats. It would be
ideal to repeat these studies using either a viral vector specific to LC neurons, or a cre-
dependent viral vector in TH-cre rats (i.e. transgenic rats expressing cre in tyrosine hydroxylase
positive cells). These approaches would allow me to determine the role of the noradrenergic LC
neurons in the manifestation of hLTF. However, this will be addressed in my next chapter
(Chapter 5).
Previously, it was shown that repeated application of noradrenaline on hypoglossal motor
neurons in vitro can potentiate their response to excitatory inputs (Neverova et al., 2007). My
stimulation protocol forced intermittent release of noradrenaline from the LC onto the
hypoglossal motor pool, thereby triggering hLTF. This intervention could, therefore, not be
reflective of what happens during the natural trigger (i.e., repeated apneas), but simply an
observation of an already known phenomenon (i.e., that repeated exposure to noradrenaline
can trigger hLTF). However, a recent study has shown in vivo that repeated exposure of
noradrenaline from non-LC sources does not trigger sustainable hLTF (Song and Poon, 2017).
Specifically, repeated optical stimulation of hypoglossal-projecting noradrenergic cell groups
(A5 and A7) increases genioglossus motor output transiently, persisting for approximately 20
minutes. Here, I show that the same intervention targeting LC neurons triggers hLTF that

98
persists for a minimum of 60 minutes, suggesting that repeated stimulation of the LC in
particular elicits hLTF that is reflective of the plasticity observed with repeated apneas.
4.4.4 LC is critical for hLTF
My hypothesis was that optically inactivating the LC would prevent apnea-induced hLTF. My
results directly supported this hypothesis as apnea-induced hLTF was abolished when the LC
was inactivated. This suggests that LC activity is critical for hLTF expression triggered by
repeated apneas and is therefore a required component of the hLTF circuit. Experiments in
control (non-ChR2-expressing mCherry) animals supported these results, as repeated apneas in
the presence of continuous light exposure continued to trigger hLTF. Taken together, it suggests
that the repeated apnea trigger halts at the inactivated LC within the hLTF circuit, preventing
the intermittent release of noradrenaline onto hypoglossal motor neurons to elicit hLTF.
4.4.5 A minimum threshold of LC stimulation is required for hLTF expression
Here, I demonstrated that repeated stimulation of the LC triggered respiratory plasticity of
inspiratory genioglossus motor output. However, some animals did not exhibit hLTF following
intermittent LC stimulation. These animals may have had a different response to the fixed
stimulus delivered (i.e. 10 periods of LC stimulation at 5 Hz for 15 seconds, separated by 1
minute) as it does not account for the variability between each animal. Despite receiving the
same intervention, some animals may not have received the same level of stimulation. This is
supported in my results as c-Fos expression in the LC was lower in animals that did not exhibit
hLTF compared to animals that exhibited hLTF. Considering LC neurons have been suggested to
fire synchronously (Aston-Jones and Bloom, 1981, Christie et al., 1989, Ishimatsu and Williams,
1996), it may be possible that an insufficient number of cells were stimulated to trigger
plasticity. This implies that a minimum threshold of LC stimulation is required to trigger
synchronous firing in order for hLTF to manifest.

99
4.4.6 Plasticity occurs at the level of the LC and at the level of the hypoglossal motor neuron
A previous study showed terazosin perfused onto hypoglossal motor neurons after repeated
apneas can reverse signs of hLTF (Tadjalli, 2012), suggesting on-going activation of α1-
adrenergic receptor signalling at the hypoglossal motor pool is necessary to maintain hLTF. An
alternative interpretation of my histological results may support this finding. c-Fos expression is
maximally active between 30-90 minutes. My results showed an increase in c-Fos expression at
the LC following intermittent LC stimulation (i.e., 90 minutes from the trigger) is indicative of LC
cells being activated by light. However, the increase in c-Fos expression could reflect hLTF
expression from the 60-minute time point (i.e., 30 minutes after maximal hLTF expression),
potentially representing an increase in LC activity persisting after the trigger. It may be possible
that repeated LC stimulation has altered the firing pattern of LC neurons (i.e., the LC has
undergone plasticity).
The implication above contrasts what is known regarding phrenic LTF, which has shown
plasticity to occur at the level of the motor neuron (Dale et al., 2017, Devinney et al., 2015,
Hoffman et al., 2012, Satriotomo et al., 2012). However, plasticity could also be happening at
the hypoglossal motor neuron by changing its intrinsic plasticity. I base this on two lines of
evidence: (1) the binding of neuromodulators such as noradrenaline can initiate a signalling
cascade that acts through TrkB receptors to trigger plasticity (Andero et al., 2014, Baker-
Herman et al., 2004, Minichiello et al., 2002, Wilkerson and Mitchell, 2009, Yoshii and
Constantine-Paton, 2010). When TrkB receptors are antagonized at the level of the hypoglossal
motor neuron, repeated apneas did not elicit hLTF (Tadjalli, 2012), suggesting noradrenaline-
induced changes within the hypoglossal motor neuron following repeated apneas could be
mediating plasticity. (2), TrkB receptor activation alone induced hLTF (Tadjalli, 2012), suggesting
hLTF expression may initiate and/or require activation of the TrkB signalling pathway.
The above data has led me to postulate that plasticity may be happening at two fronts:
plasticity at the LC alters its firing pattern to provide on-going release of noradrenaline onto

100
hypoglossal motor neurons, and the hypoglossal motor neuron itself undergoes plasticity
following noradrenaline-mediated activation of the TrkB signalling cascade to induce plasticity
at the level of the hypoglossal motor neuron.
4.4.7 Methodological considerations
As with any approach, there were limitations to my methodology. First and foremost, during LC
inhibition, it may be possible for LC neurons to fired spontaneously due to the inhibitory post-
synaptic current (IPSC) reversal potential (Mahn et al., 2016). Although this may have occurred
during my intervention, the use of halorhodopsin (eNpHR3.0) is arguably the most effective at
maintaining prolonged inhibition compared the other inhibitory opsins such as archaerhodopsin
which has been shown to increase spontaneous neurotransmitter release (Mahn et al., 2016).
In addition, my histology showed fewer c-Fos positive cells in the LC following LC inactivation,
which suggest that LC neurons were largely inactivated during my intervention.
Another limitation involves potential drawbacks with the use of optogenetics. For example, the
use of light is accompanied by heat produced at the tip of the optic fibre (Han, 2012, Stujenske
et al., 2015, Tye and Deisseroth, 2012), which can lead to heat-induced cell damage (Qian and
Gu, 2005), heat-induced cell firing (Reig et al., 2010, Stujenske et al., 2015), and photodilation
of blood vessels (Rungta et al., 2017). The amount of heat produced depends on the power
output, the distance from the optic fibre tip, and duration of light exposure. The power output
used in my experiments (25-50 mW) was greater than in recent reports on optical LC
stimulation in mice which used 20 mW (Carter et al., 2010) or 10-12 mW (Wang et al., 2014). To
reduce heat production, I used a 200 µm optic fibre to deliver light in 5 ms pulses at 5 Hz for 15
seconds, which has been reported to produce a 0.005ᵒC increase in temperature (Gysbrechts et
al., 2016).

101
The next limitation involves the use of c-Fos as a marker for cell activity. As stated in chapter
three, c-Fos does not provide insight into cells that have been inactivated or inhibited (Chan
and Sawchenko, 1994). Furthermore, not all activated neurons express c-Fos. As a result, my
claims on LC activity following LC stimulation or inhibition may not truly reflect the real-time
activities of the cell before, during, or after hLTF induction. It can only provide a snapshot of
what may be occurring at the LC during my intervention. In addition, noradrenaline levels were
not measured in these studies following stimulation or inhibition of LC cells. Going forward, it
would be ideal to record the firing pattern of LC cells before, during, and after hLTF induction,
as well as direct measurements of noradrenaline levels at the hypoglossal motor pool to
determine how LC neurons contribute to hLTF expression.
In chapter three, I discussed how LC manipulation also affects blood pressure. In this chapter, I
showed that intermittent LC stimulation had no effect on diaphragm amplitude, respiratory
frequency, oxygen saturation, or end-tidal CO2, but did not measure other variables such as
blood pressure and heart rate. LC stimulation can decrease blood pressure and heart rate
(Hakuno et al., 2004, Sved and Felsten, 1987). It may therefore be possible that repeated
modulation of these factors contributed to the manifestation of hLTF.
Lastly, one concerning limitation is in the exclusion of non-responders for statistical analyses. In
the field of LTF, animals that do not exhibit LTF are not reported and excluded in the statistical
comparisons. By omitting these animals, there is a degree of sampling bias by selecting for
responders. In this chapter, I discussed the use of several statistical analyses to address this
concern. My solution is to use a chi-square test, Firth logistic regression, and an OLS to include
all animals, responders and non-responders, to objectively determine whether hLTF was
expressed. I believe is the start to addressing this concern and I encourage future studies to
report how non-responders are dealt with statistically.

102
4.4.8 Scientific importance and clinical significance
My results provide evidence that the LC contributes to the tonic noradrenergic drive onto
hypoglossal motor neurons and there by genioglossus motor output. Furthermore, I show that
LC stimulation alone can increase genioglossus motor output. This is significant as a reduction in
LC activity correlated with rapid-eye movement (REM) sleep, and REM sleep correlated with a
reduction in upper airway muscle tone (Aston-Jones and Bloom, 1981, Nitz and Siegel, 1997),
suggesting LC activity may be involved in the reduction of muscle tone during REM sleep. My
results provide evidence that manipulation of LC activity could potentially aid in maintaining
upper airway muscle tone during sleep. By mitigating the reduction in muscle tone observed
during sleep, it may reduce the number of apneic events in obstructive sleep apnea patients.
Lastly, I propose two sites at which plasticity of genioglossus motor output can be manipulated:
at the LC and at the hypoglossal motor pool as both are required to mediate hLTF. The
identification of these regions could provide a new therapeutic target to induce plasticity and
treat OSA.

103
Chapter Five - α1-Adrenergic Receptor Binding at the Hypoglossal Motor Pool is Required for
LC-Induced Hypoglossal LTF
5.1 Summary
My previous chapters have provided evidence that the locus coeruleus (LC) is critical for and
can drive hypoglossal long-term facilitation (hLTF) expression. It is reasonable to hypothesize
that the LC releases noradrenaline onto hypoglossal motor neurons to trigger hLTF. However,
the LC co-releases multiple neurotransmitters (e.g., glutamate) that may influence the
manifestation of hLTF. To determine whether noradrenaline released onto the hypoglossal
motor pool, specifically from the LC, is the critical neurotransmitter for the manifestation of
hLTF, I employed two approaches. First, I used intermittent stimulation of LC axons at the level
of the hypoglossal motor pool to determine whether stimulation of this connection can trigger
hLTF. I then elicited hLTF with intermittent stimulation of the LC while simultaneously blocking
α1-receptors at the hypoglossal motor pool. Here, I demonstrated that stimulation of LC axons
could not trigger hLTF, but hLTF elicited by intermittent LC stimulation was abolished following
α1-receptor blockade at the hypoglossal motor pool. This suggests that LC-induced hLTF
requires α1-adrenergic receptor activation on hypoglossal motor neurons, and that the source
of noradrenaline acting on α1 receptors may originate from the LC.
5.2 Introduction
My findings to this point have identified the LC as being a critical component of the circuit
underlying hLTF. The first aim of this chapter was to determine whether hLTF was mediated by
a direct LC to hypoglossal connection. In chapter 3, I showed that LC neurons send projections
to the hypoglossal motor pool, creating the neural circuit (NTS→LC→XII) that I hypothesize
underlies hLTF. The first aim in this chapter was therefore to determine if stimulation of LC
axons at the level of the hypoglossal motor pool can elicit hLTF. My hypothesis is that
intermittent stimulation of LC axons would cause episodic release of noradrenaline onto
hypoglossal motor neurons to trigger hLTF. This would address whether LC-induced hLTF is
acting through a direct connection between LC neurons and hypoglossal motor neurons.

104
To test this hypothesis, I recorded respiratory activity in anaesthetized, spontaneously
breathing, male Sprague-Dawley rats expressing channelrhodopsin2 (ChR2) in the region of the
LC. At four weeks post-injection (AAV5-hSyn-ChR2(H134R)-mCherry) into the LC region, I
stimulated the axon fibres originating from the region of the LC at the level of the hypoglossal
motor pool. I stimulated ChR2-expressing LC axons in same fashion as my previous studies (i.e.,
15 second pulses at 5 Hz, separated by 1 minute no stimulation, repeated 10 times, Fig. 5.1A). I
recorded genioglossus and diaphragm activity, as well as respiratory frequency and oxygen
saturation for 60-90 minutes post stimulation.
The second aim of this chapter was to determine whether the LC is the source of noradrenaline
mediating hLTF. In chapter 4, I demonstrated that intermittent stimulation of the LC alone can
elicit hLTF that persists for 60 minutes, suggesting intermittent noradrenaline released from a
specific source (i.e., the LC) is driving hLTF. Direct application of noradrenaline onto hypoglossal
motor neurons in vitro has been shown to trigger hLTF (Feldman et al., 2005, Neverova et al.,
2007), and that blockade of α1-receptors at the hypoglossal motor pool prevents apnea-
induced hLTF (Tadjalli et al., 2010), suggesting that noradrenaline acting on α1-receptors is
required for hLTF to manifest. However, when similar experiments were performed in vivo,
intermittent noradrenaline release induced by stimulation of noradrenergic cell group A5 or A7
elicited a transient form of hLTF, persisting for 10-20 minutes (Song and Poon, 2017). This
suggests that another mechanism may be involved in mediating hLTF that persists for more
than 20 minutes.
Several studies have shown LC neurons to co-release multiple neurotransmitters including
glutamate (Fung et al., 1994, Trudeau, 2004), neuropeptide Y (Everitt et al., 1984, Holets et al.,
1988, Tsuda et al., 1989), galanin (Holets et al., 1988, Tsuda et al., 1989), enkephalin (Van
Bockstaele et al., 2000), and dopamine (Devoto and Flore, 2006, Kempadoo et al., 2016, Smith
and Greene, 2012). This suggests that other neurotransmitters may be involved following hLTF
induced by intermittent LC stimulation. In fact, the neurotransmitters co-released by the LC can

105
modulate respiratory output and/or plasticity (Bocchiaro and Feldman, 2004, Feldman et al.,
2005, Kempadoo et al., 2016, Ling et al., 2001, McGuire et al., 2005, Rukhadze et al., 2010,
Sharifullina et al., 2004, Steenland et al., 2006, Tadjalli et al., 2010). For example, the LC co-
releases glutamate which can act on NMDA receptors found on hypoglossal motor neurons to
augment respiratory output (Steenland et al., 2006). In fact, phrenic LTF was abolished upon
NMDA receptor blockade at the level of this motor pool (McGuire et al., 2005). Similarly, LTF of
hypoglossal nerve activity elicited in vitro was abolished upon metabotropic glutamate receptor
blockade (Feldman et al., 2005, Sharifullina et al., 2004). This suggests that hLTF elicited by
intermittent LC stimulation may have been influenced or dependent on the co-release of
glutamate acting on NMDA and/or metabotropic glutamate receptors on the hypoglossal motor
neuron to induce post-synaptic changes.
In the field of LTF research, it was well demonstrated that multiple neurotransmitters can
influence the manifestation of LTF, and the trigger dictates which neurotransmitter is released.
For example, LTF of phrenic/diaphragm activity was induced by repeated application of
adrenaline (Huxtable et al., 2014) but is dependent on serotonin when elicited by an
intermittent hypoxia trigger (Fuller et al., 2001, Kinkead et al., 2001, Ling et al., 2001, Niebert et
al., 2011). Similarly, repeated activation of 5-HT2 can elicit hLTF in vitro (Bocchiaro and
Feldman, 2004, Feldman et al., 2005) but serotonin is not critical for hLTF elicited by a repeated
apnea trigger (Tadjalli et al., 2010). This overlap is likely due to similar intracellular mechanisms
following 5HT or α1-adrenergic receptor binding. Both receptor subtypes are Gq protein-
coupled metabotropic receptors whose signalling cascade involve inositol 1,4,5-triphosphate
(IP3) and protein kinase C (PKC) (Hannon and Hoyer, 2008).
To determine whether hLTF is induced by noradrenaline released from the LC, I elicited hLTF
using intermittent stimulation of LC cells expressing channelrhodopsin2 (ChR2) while
simultaneously blocking α1-adrenergic receptors at the level of the hypoglossal motor pool
with 1 µM Terazosin, an α1-adrenergic receptor antagonist (Fig. 5.1B). This concentration is
found effective at preventing apnea-induced hLTF without reducing basal genioglossus activity

106
(Tadjalli, 2012). If hLTF requires noradrenaline released from the LC, then intermittent LC
stimulation should no longer elicit hLTF. Alternatively, if hLTF is critically-dependent by other
neurotransmitters co-released from the LC, then blockade of α1-adrenergic receptors at the
level of the hypoglossal motor pool should have no effect on the manifestation of hLTF
triggered by LC stimulation.
Together, these experiments would show that the projections arising from the region of the LC
are directly acting on hypoglossal motor neurons to trigger noradrenaline release to elicit hLTF,
providing a functional and anatomical circuit underlying hLTF.

107
Figure 5.1 – Protocols for intermittent LC stimulation with and without terazosin perfusion. (A) Protocol for recording genioglossus (GG) activity in an anaesthetized, spontaneously breathing rat at baseline, followed by intermittent stimulation of LC axons at the hypoglossal motor pool (XII) with 10 light pulses at 5 Hz for 15 seconds (black bars), separated by 1 minute no stimulation, and subsequent recording for an additional 90 minutes. (B) Protocol for recording genioglossus activity followed by intermittent LC stimulation with simultaneous perfusion of saline at the hypoglossal motor pool, switch to terazosin (1 µM, dotted line), and washout with saline for the remainder of the experiment. (C) Protocol for recording genioglossus activity followed by saline perfusion at the hypoglossal motor pool with simultaneous repeated obstructive apneas (10 apneas for 15 seconds separated by 1-minute recovery) and subsequent 90-minute recording.

108
5.3 Results
5.3.1 Intermittent stimulation of LC axons at the hypoglossal motor pool did not trigger hLTF
In chapter four, I showed that intermittent stimulation of the LC triggered hLTF, presumably
through the release of noradrenaline from the LC onto hypoglossal motor neurons.
Furthermore, my own findings, in addition to another study (Rukhadze and Kubin, 2007), report
the existence of an anatomical connection between LC neurons and the hypoglossal motor
pool. Based on these findings, I hypothesized that intermittent optical stimulation of ChR2-
expressing LC axons at the hypoglossal motor pool would induce repeated release of
noradrenaline onto hypoglossal motor neurons and trigger hLTF of inspiratory genioglossus
motor activity. I found that repeated stimulation of LC axons did not change genioglossus motor
activity over time (1-way RM-ANOVA, F=0.2538, p=0.9031, Fig. 5.2). This could imply that LC-
induced hLTF is not mediated by a direct connection (i.e., LC cells do not directly act on
hypoglossal motor neurons to trigger hLTF). Alternatively, it could also imply that axon terminal
stimulation did not cause sufficient release of noradrenaline onto hypoglossal motor neurons to
trigger hLTF.
Measurements of diaphragm amplitude and oxygen saturation showed a minor decrease
compared to baseline (1-way RM ANOVA, diaphragm amplitude: F=6.816, p=0.0021. O2
saturation: F=3.709, p=0.0255 Fig. 5.2C,E), but this change was within the range of other
experimental groups as no change can be observed when compared to animals given
intermittent LC stimulation (2-way RM ANOVA, Int. Stim of LC axons vs Int. LC Stim, Diaphragm
amplitude: F=0.08737, p=0.9859. O2 saturation: F=2.199, p=0.0864). Respiratory frequency was
unaffected following intermittent stimulation of LC axons (1-way RM ANOVA, F=0.3989,
p=0.8066. Fig. 5.2D). Taken together, it suggests that intermittent stimulation of LC axons could
not elicit hLTF, and did not influence other respiratory variables.

109
Figure 5.2. Intermittent stimulation of LC axons did not trigger hLTF. (A) Histological example of the LC expressing tyrosine hydroxylase (TH, green), channelrhodopsin2 (mCherry, red), and the overlay. Last panel depicts the presence of non-ChR2-expressing mCherry positive axons at the hypoglossal motor pool, and optic probe tract location. CC, central canal. (B) Group data (n=5) showing integrated genioglossus amplitude (∫GG EMG) following intermittent stimulation of LC axons at the level of the hypoglossal motor pool. No change in genioglossus amplitude was observed across all time points. A significant decrease in Integrated diaphragm amplitude (∫Dia EMG) was observed at 30, 45, and 60 minutes, and in oxygen saturation at 60 minutes (C,E). Respiratory frequency was unaffected (D). Data presented as mean + SEM. *denotes significance (p<0.05) between groups.

110
5.3.2 Noradrenaline released from the LC is critical for hLTF
Although intermittent stimulation of LC axons did not trigger hLTF suggesting it is not a direct
connection, my next step indirectly readdresses this connection by directly stimulating LC
neurons while simultaneously blocking its downstream effects. Specifically, I performed
repeated optical stimulation of ChR2-expressing LC cells (5 Hz for 15 seconds separated by 1
minute recovery, repeated 10 times) while perfusing 1 µM terazosin, an α1-adrenergic receptor
antagonist, at the hypoglossal motor pool (Fig. 5.1B). When α1-adrenergic receptors on the
hypoglossal motor pool are blocked, intermittent LC stimulation could not trigger hLTF. In fact,
a significant decrease in genioglossus motor output was observed (1-way RM ANOVA, F=3.737,
p=0.0166, Fig. 5.3). The absence of hLTF suggests that the release of noradrenaline from the LC
acts on α1-adrenergic receptors at the hypoglossal motor pool for hLTF to manifest.
This finding supports earlier studies that show α1-adrenergic receptors at the hypoglossal
motor pool prevented apnea-induced hLTF (Tadjalli et al., 2010), suggesting α1-adrenergic
receptor activation is a critical step in initiating the mechanism underlying hLTF of inspiratory
genioglossus motor output.
To ensure the α1-adrenergic receptor blockade did not influence other respiratory variables, I
quantified diaphragm amplitude, respiratory frequency, and oxygen saturation. Intermittent LC
stimulation with α1-adrenergic receptor blockade did not significantly influence these
respiratory variables over time (2-way RM ANOVA, Intermittent LC stimulation vs Intermittent
LC stimulation + Terazosin: diaphragm: F=0.0888, p=0.9856; respiratory frequency: F=0.4509,
p=0.7712; oxygen saturation: F=1.967, p=0.1133, Fig. 5.3E-G), suggesting neither intermittent
LC stimulation nor the dose of terazosin used had any impact on respiratory output.
A minor increase end-tidal CO2 was observed at the 45 and 60 minute time points (1-way RM
ANOVA, F=3.707, p=0.0152, Fig. 5.3H), however this increase was not physiologically relevant as
ET-CO2 at 60 minutes was at 5.25 ± 0.28% and was not accompanied by changes in respiratory
frequency or diaphragm amplitude.

111

112
Figure 5.3. hLTF is mediated by α1-adrenergic receptor binding of noradrenaline released from the LC. (A) Raw trace recorded from an anaesthetized, spontaneously breathing rat depicting spike in genioglossus motor activity following successful targeting of the hypoglossal motor pool with microdialysis probe. (B) A representative EMG trace of integrated inspiratory genioglossus (GG) activity following intermittent LC stimulation with simultaneous α1-adrenergic receptor blockade at the level of the hypoglossal motor pool at 15, 30, 45, and 60 min. (C) Probe tract locations in the LC (dotted outline, left panels) and in the hypoglossal motor pool (dotted outline, right panels) following LC stimulation and terazosin perfusion. Matching shade of pink/purple represents probe locations in the LC and hypoglossal motor pool within each animal. (D) Group data showing inspiratory genioglossus activity of animals perfused with the α1-adrenergic blocker (n=8, black bars) could not exhibit hLTF following intermittent LC stimulation. Diaphragm activity, respiratory frequency, and oxygen saturation was unaffected compared to animals that received the same intervention absent terazosin (n=8, E-G). A significant but physiologically irrelevant increase was observed in end-tidal CO2 levels at 45 and 60 min (H). Dotted line represents percent baseline activity. Data are presented as mean + SEM. * denotes a significant difference (p<0.05).
5.3.3 Saline perfusion into the hypoglossal motor pool does not influence hLTF expression
Perfusion of α1-adrenergic receptor antagonist, terazosin, prevents both apnea-induced and
LC-induced hLTF of inspiratory genioglossus motor output. However, it is important to ensure
that the absence of hLTF observed is a result of α1-adrenergic receptor blockade thereby
preventing LC-induced hLTF, and not a result of damage caused by probe insertion into the
hypoglossal motor pool. However, experiments that show saline perfusion into the hypoglossal
motor pool do not affect hLTF expression has already been performed in earlier experiments
(chapter 3), as well as in past studies (Tadjalli, 2012, Tadjalli et al., 2010). As such, I deliberately
did not perform experiments with repeated stimulation of LC neurons while perfusing saline
into the hypoglossal motor pool. However, to provide a direct comparison showing LC-induced
hLTF with and without α1-adrenergic receptor blockade, here I show genioglossus amplitude
following perfusion of saline or terazosin after exposure to an hLTF trigger (i.e., repeated
apneas or repeated LC stimulation). When saline was perfused at the hypoglossal motor pool,
the manifestation of hLTF was uninterrupted compared to when α1-adrenergic receptors were
blocked (2-way RM-ANOVA, Int. LC Stim + Teraz vs Saline perfusion at hypoglossal, F=9.653,
p<0.0001. Fig. 5.4A). In both groups, diaphragm amplitude and respiratory frequency were
unaffected (2-way ANOVA, Int. LC Stim + Teraz vs Saline, Diaphragm amplitude: F=0.7625,
p=0.5549. Respiratory frequency: F=1.901, p=0.1243. Fig. 5.4B,C). This reinforces that saline
perfusion into the hypoglossal motor pool does not negatively influence the expression of hLTF
following a trigger.

113
Figure 5.4. Saline perfusion at hypoglossal motor pool does not affect hLTF. (A) Group data showing apnea-induced hLTF of integrated genioglossus activity (∫GG EMG) was unaffected following saline perfusion into the hypoglossal motor pool (n=6, white bars) compared to terazosin perfused animals following intermittent LC stimulation (n=8, black bars). In both groups, integrated diaphragm activity (∫Dia EMG) and respiratory frequency (B,C) were unaffected. Dotted line represents percent baseline activity. Data are presented as mean + SEM. * denotes a significant difference (p<0.05).
5.3.4 α1-Adrenergic receptor blockade abolishes hLTF expression
As discussed in chapter 4, this statistical analysis used in these experiments compares animals
that exhibited hLTF following intermittent LC stimulation to animals that did not exhibit hLTF
following terazosin perfusion. However, approximately 27% of animals do not exhibit hLTF
following intermittent LC stimulation and the exclusion of these animals may skew the
statistical analysis used. Here, I use a chi-square test, a Firth logistic regression, and an ordinary
least square linear regression (OLS) to statistically analyze whether my intervention influenced
the probability of hLTF expression. These statistical approaches remove the confound of
excluding non-responders by including all animals (i.e., animals that exhibit hLTF and non-
responders) in my analysis.

114
Following a chi-square test, I found that terazosin perfusion prevented LC-induced hLTF and this
result was significantly correlated with my intervention (chi-square test, Int. LC Stim. vs Int. LC
Stim. + Teraz, chi2=10.05, p=0.002). Similarly, upon performing a Firth logistic regression, I
found a significant difference in the probability of hLTF expression when terazosin is perfused
at the hypoglossal motor pool compared to intermittent stimulation alone (Firth logistic
regression, Int. LC Stim. vs Int. LC Stim. + Teraz, p=0.019. Fig. 5.5). Lastly, upon performing an
OLS analysis, I showed that terazosin perfusion at the hypoglossal motor pool prevented LC-
induced hLTF and that it was not due to random chance (OLS, Int. LC Stim. vs Int. LC Stim. +
Teraz, R2=0.3272, F(32)=7.782, β=0.9541, p=0.002). Taken together, all three statistical analyses
support the same finding, suggesting that the LC-induced hLTF is mediated through
noradrenergic mechanism with noradrenaline release from the LC onto α1-adrenergic receptors
on the hypoglossal motor neurons.
Figure 5.5. Probability of hLTF was reduced following α1-adrenergic receptor blockade at the hypoglossal motor pool. Following intermittent LC stimulation (n=8, blue), hLTF expression was observed in 73% of all attempts. However, intermittent LC stimulation could not elicit hLTF when α1-adrenergic receptors were blocked at the hypoglossal motor pool (pink). Each line represents an animal that received one of the interventions. α1-adrenergic receptor binding is required for hLTF expression.

115
5.4 Discussion
The first aim of this chapter was to determine whether the LC directly influences hypoglossal
motor neuron activity to trigger hLTF. Since the LC was reported to be the largest source of
noradrenaline in the brain (Moore, 1979) and its stimulation elicits hLTF (chapter 4),
noradrenaline is presumably the critical neurotransmitter mediating hLTF. However, since the
LC has diverse projections to other noradrenergic brainstem structures that innervate
hypoglossal motor neurons such as the A5 and subcoeruleus (Byrum, 1987, Sakai et al., 1977), it
became necessary to determine whether hLTF elicited by intermittent LC stimulation was
mediated by a direct connection. Here I show that intermittent stimulation of ChR2-expressing
LC axons at the hypoglossal motor pool did not elicit hLTF.
The second aim of this chapter was to determine whether noradrenaline released from the LC
is the underlying mechanism mediating hLTF. The LC was reported to co-release multiple
neurotransmitters. Here I show that noradrenaline acting on α1-adrenergic receptors is
required for hLTF expression, suggesting noradrenaline is the critical neurotransmitter
mediating hLTF.
5.4.1 Direct stimulation of LC axons projecting to the hypoglossal motor pool did not elicit
hLTF
In Chapter 3, I provided evidence to show that the LC has direct noradrenergic projections to
the hypoglossal neurons, with clearly visible axon terminals at the hypoglossal motor pool. In
this chapter, I aimed to stimulate these axon terminals in an attempt to elicit hLTF. However,
upon intermittent stimulation of LC axons expressing ChR2, hLTF was not expressed. Although
these experiments were performed in a small group of animals (n=5), this finding suggests that
hLTF may not be mediated by a direct connection originating from the region of the LC to the
hypoglossal motor pool, but could be mediated by the LC to another noradrenergic structure
such as the A5 or subcoeruleus (SubC) (Byrum, 1987, Sakai et al., 1977). If hLTF is mediated by
an indirect connection stemming from the LC, I theorize it would act through these

116
noradrenergic structures to activate α1-adrenergic receptors on the hypoglossal motor neurons
to elicit hLTF. It may therefore be possible for LC-induced hLTF to be mediated through an
indirect pathway (i.e., LC → A5/SubC → XII).
Alternatively, the absence of hLTF observed following stimulation of LC axons could be a failure
in the technique. Prior to my findings in chapter 3, the LC was reported to possess 1.7% of the
noradrenergic input to the hypoglossal motor pool. The limited noradrenergic input from the LC
may result in insufficient stimulation of LC axons and therefore insufficient noradrenaline
release to induce hLTF.
In chapter 4, I provide evidence that a minimum threshold of LC stimulation is required to
trigger hLTF. LC neurons have been reported to fire synchronously upon stimulation (Aston-
Jones, 1981, Ishimatsu and Williams, 1996), and any stimulation below the threshold may not
trigger a synchronous response. Stimulation of LC axons may have been insufficient at
triggering a synchronous response in LC cells. Furthermore, the synchronicity of LC firing was
hypothesized to be mediated by gap junctions (Travagli et al., 1995) and axon stimulation may
not trigger a synchronous response that may only be achievable through stimulation at the cell
body.
Lastly, the absence of hLTF observed could be due to the use of a non-specific viral vector. The
axons observed at the level of the hypoglossal motor pool may not be noradrenergic. As such,
stimulation of these axons may be causing the release of neurotransmitters that do not elicit
hLTF. Further experiments would be required to verify the phenotype of these axon terminals.
Due to the difficulties associated with axon stimulation listed above, I decided to focus on the
mechanism underlying hLTF and determine whether noradrenaline released from the LC is the
critical neurotransmitter mediating hLTF.

117
5.4.2 The LC co-releases neurotransmitters that can induce plasticity and/or modulate
respiratory output
The LC was reported to co-release multiple neurotransmitters including glutamate (Fung et al.,
1994, Trudeau, 2004), galanin (Holets et al., 1988, Tsuda et al., 1989), neuropeptide y (Everitt et
al., 1984, Holets et al., 1988, Tsuda et al., 1989), enkephalin (Van Bockstaele et al., 2000), and
dopamine (Devoto and Flore, 2006, Kempadoo et al., 2016, Smith and Greene, 2012). These
neurotransmitters can induce plasticity and/or influence respiratory activity. The most studied
co-released neurotransmitter is glutamate, which can act on NMDA receptors found on
hypoglossal motor neurons to augment respiratory output (Steenland et al., 2006). In the
context of LTF, NMDA receptor blockade abolished hypoxia-induced phrenic LTF (McGuire et
al., 2005). Similarly, LTF of hypoglossal nerve activity was abolished upon metabotropic
glutamate receptor blockade (Feldman et al., 2005, Sharifullina et al., 2004). Together, this
suggests that glutamate may play an important role in mediating hLTF. The mechanism
mediating hLTF was hypothesized to involved post-synaptic changes to AMPA receptor function
(Feldman et al., 2005, Wang et al., 2005) or AMPA receptor recruitment (Itami et al., 2003). In
this study, I showed that noradrenaline is the critical neurotransmitter required for hLTF
expression; co-released glutamate acting on AMPA receptors may still be involved.
Other neurotransmitters co-released by LC neurons include galanin which can attenuate the
chemosensory reflex by reducing phrenic nerve activity during hypoxia (Abbott and Pilowsky,
2009). Galanin can inhibit other forms of plasticity such as long-term potentiation (Coumis and
Davies, 2002), presumably through the inhibition of the CREB signalling cascade (Badie-Mahdavi
et al., 2005). Neuropeptide Y is another co-released neurotransmitter that can reduce
respiratory rate and tidal volume when applied to the nucleus tractus solitarius (NTS) (Barraco
et al., 1990) as well as reduce presynaptic glutamate release (Furtinger et al., 2001), suggesting
neuropeptide Y may interact with the tripartite circuit (NTS → LC → XII) hypothesized to be
mediating respiratory motor plasticity. Enkephalin has also been shown to depress the activity
of respiratory neurons in the NTS (Sessle and Henry, 1985), and potentially plays a crucial role
in regulating the efficiency of neurotransmission at the synapse by disinhibiting nearby

118
GABAergic transmission (Morris and Johnston, 1995), although this interaction requires further
investigation. Lastly, dopamine can be co-released by activating LC neurons. Electrical
stimulation of the LC has increased dopamine levels in the prefrontal cortex in a frequency-
dependent manner (Choi et al., 2015), and optical stimulation of the LC increases dopamine
levels in the dorsal hippocampus (Kempadoo et al., 2016). In the context of respiration,
dopamine can modulate the chemosensory response (Hedner et al., 1982, Hsiao et al., 1989),
and dopamine receptor agonists can increase the hypercapnic ventilatory response (Lalley,
2008). In the context of plasticity, dopamine promotes structural changes at the synapse
(Yagishita et al., 2014). Neuromodulators such as noradrenaline and dopamine can initiate
rapid activation of neurotrophic downstream signalling (Natarajan and Berk, 2006), which in
turn can enhance synaptic signalling by acting on phospholipase C (PLC) or protein kinase
pathways (Blum and Konnerth, 2005). However, there is little evidence to suggest dopamine is
playing an active role in hLTF. Instead, noradrenaline is the critical neurotransmitter required
for hLTF expression.
5.4.3 The same intracellular machinery is involved in mediating hLTF expression across
multiple triggers
Upon intermittent stimulation of LC neurons while simultaneously blocking α1-adrenergic
receptors at the hypoglossal motor pool, hLTF could not be elicited. This supports previous
findings that show hLTF elicited by repeated apneas was abolished upon α1-adrenergic
receptor blockade at the hypoglossal motor pool (Tadjalli et al., 2010). In fact, hLTF elicited by
repeated episodes of hypoxia was also abolished upon systemic α1-receptor blockade
(Neverova et al., 2007). Taken together, this suggests that noradrenaline, and specifically α1-
adrenergic receptor activation, is critical for hLTF regardless of the trigger (i.e., repeated
apneas, repeated episodes of hypoxia, or repeated LC stimulation).
In my results, I showed that the probability of hLTF was greatly reduced upon LC inactivation or
α1-adrenergic receptor blockade. This suggests that the trigger (repeated apneas or optical LC
stimulation) must act through the LC which in turn intermittently releases noradrenaline to

119
bind α1-adrenergic receptors at the hypoglossal motor pool to initiate hLTF. This is important
because it suggests that the same intracellular machinery is involved in mediating hLTF
regardless of trigger. These findings could also provide direction for pharmaceutical companies
to direct their focus towards activating α1-adrenergic machinery to trigger hLTF.
5.4.4 Methodological Considerations
One consideration in these experiments was discussed in earlier chapters which identified the
viral vector used in these studies to be non-specific to noradrenergic cells but instead infected
all neurons. As such, it is possible that stimulation of cells in the LC that are non-noradrenergic
in nature may have contributed to hLTF. However, the findings in this chapter still identify
noradrenaline to be the key player in mediating hLTF. It does not however imply that other
neurotransmitters co-released are uninvolved as my approach does not address the role of
other cells and neurotransmitters and their effects on hLTF. For example, astrocytes produce
and release L-lactate which can trigger noradrenaline release from the LC (Tang et al., 2014). It
could, therefore, be possible for intermittent stimulation to cause astrocytic release of L-lactate
to induce and/or enhance noradrenaline release from the LC. Nonetheless, noradrenaline
acting on α1-adrenergic receptors on hypoglossal motor neurons is critical to the manifestation
of hLTF.
Another consideration includes my approach which involved the perfusion of 1 µM terazosin
into the hypoglossal motor pool via reverse microdialysis. It is possible that terazosin perfusion
affected α1-adrenergic receptors found on NTS neurons (Zhang and Mifflin, 2007), and that this
interaction influenced the expression of hLTF. However, α1-adrenergic receptors on NTS
neurons are not tonically active (Zhang and Mifflin, 2007) and its antagonism should therefore
have no influence on hLTF expression.
Following terazosin perfusion, intermittent stimulation of ChR2-expressing LC cells induced a
decrease in genioglossus amplitude. This was initially surprising considering the dose of
terazosin (1 µM) delivered through reverse-microdialysis was used previously without affecting

120
baseline genioglossus motor output (Tadjalli, 2012). The decrease in genioglossus amplitude
observed may be attributed to the effects of the co-released neurotransmitter galanin. Galanin
co-released from LC terminals has been shown to be inhibitory, reducing LC firing rate and
inducing hyperpolarization presumably via an increase in K+ conductance (Xu et al., 2005). Its
release is also dependent on the depletion of noradrenaline following high phasic bursting of LC
neurons (Consolo et al., 1994, Weinshenker and Holmes, 2016). The decrease in genioglossus
amplitude observed may therefore be a result of decreased LC activity caused by galanin, but
further studies are needed to verify this interaction.
Alternatively, the decrease in genioglossus amplitude could also be due to the intended release
of noradrenaline from the LC. Hypoglossal motor neurons have been reported to express both
α1 and α2 adrenergic receptors (Volgin et al., 2001). Although α1-adrenergic receptor
activation has been reported to produce excitatory effects on the post-synaptic cell, α2-
adrenergic receptor activation is traditionally considered to inhibit activity (DeBock et al., 2003).
In fact, activation of α2-adrenergic receptors with hypercapnia can cause long-term depression
of hypoglossal motor activity (Bach and Mitchell, 1996). Here, I block α1-adrenergic receptor
activation but continue to stimulate LC cells. It may, therefore, be possible that noradrenaline
could not bind to α1-adrenergic receptors on the hypoglossal motor neuron and bound instead
to open α2-adrenergic receptors causing the decrease in genioglossus amplitude observed.
Further studies would be required to confirm this interaction.
5.4.5 Scientific importance and clinical significance
Sleep onset is accompanied by a reduction in upper airway muscle tone and a sudden decrease
in LC activity (Aston-Jones and Bloom, 1981, Chan et al., 2006, Fenik et al., 2013, Fung and
Chase, 2015), which may suggest that noradrenaline released specifically from the LC is
involved in maintaining upper airway muscle tone during sleep. The results of this chapter
provide more definitive evidence that α1-adrenergic receptor activation, presumably by
noradrenaline released from the LC, to be the key required drive hLTF expression. The

121
involvement of the LC is important because forced noradrenaline release from other
noradrenergic cell groups such as the A5 and A7 only augments inspiratory genioglossus motor
output for 20 minutes (Song and Poon, 2017). It is possible that persistent release of
noradrenaline from the LC is required to sustain hLTF for longer durations, implying that
plasticity at the LC is necessary for persistent hLTF.
The fact that α1-adrenergic receptors activation is consistently involved in gate-keeping hLTF
expression regardless of the trigger suggests that direct manipulation of α1 receptor
intracellular machinery could be the next steps towards a pharmaceutical treatment to induce
LTF of genioglossus motor output. These findings could provide a direction for pharmaceutical
companies to focus towards a treatment for respiratory disorders such as obstructive sleep
apnea.

122
Chapter Six – General Discussion
Prior to the experiments discussed in this thesis, the mechanism and circuit underlying
hypoglossal/genioglossus long-term facilitation (hLTF) were not clearly elucidated. What was
known included the requirement for an intermittent stimulus (Tadjalli, 2012), activation of α1-
adrenergic receptors on the hypoglossal motor pool (Tadjalli et al., 2010), and activation of the
nucleus tractus solitarius (NTS) (Torontali, 2012), the primary terminate site for vagal afferents.
However, (1) the source of noradrenaline was unknown, (2) the complete neural circuit
underlying hLTF was unknown, and (3) the site of plasticity was unknown.
Over the last 6 years, I have addressed all three unknowns. I have identified the source of
noradrenaline to be the LC as it is the only noradrenergic structure to increase in c-Fos
expression, and presumably increase activity, following apnea-induced hLTF (chapter 3). I have
also shown that the LC has direct projections to the hypoglossal motor pool (chapter 3),
suggesting a neural circuit (NTS → LC → XII) may underlie hLTF. I also showed that intermittent
stimulation of the LC alone can trigger hLTF (chapter 4), while inactivation of the LC reduced the
probability for hLTF to manifest (chapter 3 and 4). In addition, intermittent stimulation of the LC
while blocking α1-adrenergic receptors at the hypoglossal motor pool prevented hLTF (chapter
5), suggesting the LC releases noradrenaline onto hypoglossal motor neurons to drive hLTF.
Furthermore, I showed a greater increase in c-Fos expression in the LC of animals that exhibited
hLTF compared to animals that did not, suggesting an increase in LC activity (i.e., plasticity at
the LC) is what drives hLTF (chapter 4). Taken together, my data has added to the field of
respiratory motor plasticity research by identifying the neural circuit that mediates hLTF (i.e.,
NTS → LC → XII), in addition to identifying a new trigger for hLTF that bypasses respiratory
feedback by directly stimulating the LC. Lastly, this research provides further evidence to
support the role of noradrenaline in mediating plasticity of the upper airways as hLTF requires
sustained noradrenaline release from the LC onto α1-adrenergic receptors on the hypoglossal
motor pool. In this section, I discuss the significance of my experimental findings, the
methodological considerations, and the future directions of LTF research.

123
6.1. Hypoglossal / genioglossus LTF is mechanistically distinct from phrenic LTF
The field of LTF research has largely been focused on the diaphragm or phrenic nerve (pLTF).
However, LTF can occur in other respiratory muscles such as the genioglossus. Although the
duration of LTF (and thereby its definition) varies across studies, ranging from 20 minutes
(Harris et al., 2006, Song and Poon, 2017) to the standard experimental duration of 60 minutes
(i.e., the standard for pLTF), I chose to abide by the time frame of 60 minutes to define hLTF to
provide a better comparison to the most commonly studied form of LTF. The goal of my PhD is
to elucidate the mechanisms and neural circuit underlying hLTF. By choosing the 60-minute
time frame, it allowed for comparisons with pLTF, which comes with a rich foundation of
research, providing insight into what could be happening at the level of the neuron during LTF
of genioglossus muscle activity.
The triggers and mechanisms underlying pLTF have been extensively studied, with current
evidence identifying the most common trigger to be repeated bouts of hypoxia (Bach and
Mitchell, 1996, Baker and Mitchell, 2000, Bocchiaro and Feldman, 2004, Fuller et al., 2001). The
mechanism which underlies hypoxia-induced pLTF is hypothesized to be serotonin (5HT)
dependent, correlating an increase in phrenic nerve activity with an increase serotonergic
raphe firing rates in cats (Morris et al., 2001). This led to studies in rats showing hypoxia-
induced pLTF required the binding of serotonin to 5HT2 receptors at the level of the phrenic
motor pool (Bocchiaro and Feldman, 2004, Fuller et al., 2001, Kinkead et al., 2001, McGuire et
al., 2004), and that inhibition of caudal raphe neurons prevented hypoxia-induced pLTF (Dodig
et al., 2012, Valic et al., 2010), suggesting caudal raphe neurons are the source of serotonin
mediating pLTF. The intracellular cascade at the phrenic motor neuron has also been
investigated, identifying the requirement of TrkB receptor activation (Dale et al., 2017), as well
as identifying ERK/MAPK activation at the level of the motor neuron that ultimately determine
drives and maintains pLTF (Hoffman et al., 2012, Wilkerson and Mitchell, 2009).
By direct comparison, the triggers and mechanisms underlying hLTF have been less extensively
studied. Current evidence show various triggers for hLTF, including repeated apneas (Lui et al.,

124
2018, Song and Poon, 2017, Tadjalli et al., 2010), repeated modulation of vagal afferents
(Tadjalli et al., 2010), or repeated stimulation of the LC (chapter 4). The mechanism which
underlies hLTF is hypothesized to be noradrenaline-dependent, correlating an increase in
genioglossus motor activity with an increase in c-Fos expression in LC neurons (Lui et al., 2018).
In addition, studies have shown apnea-induced hLTF required the binding of noradrenaline to
α1-adrenergic receptors at the level of the hypoglossal motor pool (Tadjalli et al., 2010; chapter
five), and that inhibition of LC neurons prevented apnea-induced hLTF (chapter 3 and 4),
suggesting LC neurons are the source of noradrenaline mediating hLTF. The intracellular
cascade at the hypoglossal motor neuron has also been investigated, identifying the
requirement of TrkB receptor activation (Tadjalli, 2012). Taken together, this suggests that the
mechanism underlying hLTF was investigated in the same manner as pLTF but was found to be
mechanistically distinct from each other (i.e., serotonin vs. noradrenaline) (Table 6.1).

125
Table 6.1. Comparison of mechanisms underlying pLTF vs hLTF
Animal Model
Intervention Used Primary Finding Reference
Ph
ren
ic /
Dia
ph
ragm
LTF
Rats Repeated bouts of hypoxia
Hypoxia-induced pLTF occurs in rats and requires serotonin
(Bach and Mitchell, 1996)
Cats Repeated bouts of hypoxia
Hypoxia-induced pLTF correlates with an increase in serotonergic raphe neurons firing
(Morris et al., 2001)
Rats Repeated bouts of hypoxia + 5HT2 receptor antagonism
Hypoxia-induced pLTF requires serotonin binding to 5HT2 receptors
(Fuller et al., 2001, McGuire et al., 2004)
Rats Repeated bouts of hypoxia + inhibition of caudal raphe
Hypoxia-induced pLTF requires activation of caudal raphe neurons
(Dodig et al., 2012, Valic et al., 2010)
Rats Repeated bouts of hypoxia + TrkB receptor blockade at phrenic motor pool
Hypoxia-induced pLTF requires TrkB receptor activation at the phrenic motor pool
(Dale et al., 2017)
Rats Repeated bouts of hypoxia + ERK/MAPK antagonism
Hypoxia-induced pLTF requires ERK/MAPK activation at the phrenic motor pool
(Hoffman et al., 2012, Wilkerson and Mitchell, 2009)
Hyp
ogl
oss
al /
Gen
iogl
oss
us
LTF
Rats Repeated apneas Apnea-induced hLTF occurs in rats and requires noradrenaline
(Tadjalli et al., 2010)
Rats Repeated apneas Apnea-induced hLTF correlates with an increase in c-Fos expression in LC neurons
(Lui et al., 2018)
Rats Repeated apneas + α1-receptor blockade at hypoglossal
Apnea-induced hLTF requires noradrenaline binding to α1-receptor at hypoglossal motor pool
(Tadjalli et al., 2010)
Rats Repeated apneas + LC inactivation
Apnea-induced hLTF requires activation of LC neurons
Chapter 3 Chapter 4
Rats Intermittent LC stimulation
LC stimulation triggers hLTF Chapter 4
Rats Intermittent LC stimulation + α1-receptor blockade at hypoglossal
LC-induced hLTF requires α1-receptor activation at hypoglossal
Chapter 5
Rats Repeated apneas + TrkB receptor blockade at hypoglossal
Apnea-induced hLTF requires TrkB activation at the hypoglossal motor pool
(Tadjalli, 2012)
Rats TrkB agonist at hypoglossal
hLTF can be induced by activating TrkB signalling alone
(Tadjalli, 2012)

126
6.2. The brainstem circuit mediating hLTF: NTS → LC → XII
Prior to the current experiments outlined in this thesis, the hypothesized neural circuit
underlying hLTF was not clearly elucidated. hLTF could be elicited by modulation of vagal
afferents alone by repeatedly cooling the vagus nerve to inhibit vagal neurotransmission
(Tadjalli et al., 2010). This suggested that vagal neurotransmission (or the absence of it) is
required for hLTF expression, and was further supported when apnea-induced hLTF was
prevented by vagotomy or continuous cooling of vagal afferents (Tadjalli et al., 2010). Since the
nucleus tractus solitarius (NTS) is the primary termination site for vagal afferents, these
experiments suggested that the NTS is critical for apnea-induced hLTF (Tadjalli et al., 2010). This
was supported when the inactivation of NTS neurons also prevented apnea-induced hLTF (Lui,
S., et al. 2018), solidifying the NTS as a critical component of the hLTF circuit.
In chapter 3, I showed that apnea-induced hLTF correlated with an increase in c-Fos expression
in LC neurons. In fact, it was the only noradrenergic brainstem region to display a greater
increase in c-Fos expression compared to animals without intervention (i.e., repeated apneas),
and animals exposed to the intervention but were absent hLTF. The latter is important as it
suggests that the increase in c-Fos expression in LC cells is not attributed to the hypoxia or
hypercapnia associated with repeated obstructive apneas. Instead, it suggested that the LC is
the source of noradrenaline mediating hLTF. The LC also receives direct projections from the
NTS (Lopes et al., 2016, van Bockstaele et al., 1999). These experiments were followed by a
tracing study to determine whether the LC has direct projections to the hypoglossal motor pool.
Current literature claims that LC neurons have limited, if any, direct innervations to hypoglossal
motor neurons (Aldes, 1990, Fritschy and Grzanna, 1990, Levitt and Moore, 1979, Rukhadze
and Kubin, 2007), suggesting the link between an increase in LC activity and LTF of genioglossus
motor output may, therefore, not be a direct interaction. However, contrary to published
studies, a large proportion of LC neurons were found to project to the hypoglossal motor pool,
setting LC neurons to be anatomically positioned to drive hypoglossal motor activity. To verify
that the LC provides a functional role in mediating hLTF, ChR2-expressing LC cells were
stimulated in the same pattern as the repeated apnea protocol and was found to trigger hLTF of

127
genioglossus motor output. These results are important because it identifies a novel trigger of
respiratory motor plasticity; it suggests that respiratory motor plasticity of genioglossus muscle
activity can be elicited without directly manipulating respiratory activity. In addition, LC
neurons were pharmacologically inactivated, whereupon its inactivation prevented apnea-
induced hLTF. To account for the limitations of a pharmacological approach and to increase
precision, this study was repeated using optical inactivation of the LC and yielded identical
results (chapter 4).
Furthermore, I verified that LC manipulation (i.e., stimulation or inhibition) influenced the
probability for hLTF to manifest compared to controls. This is important as few studies to date
in the field of LTF have reported the percentage of responders and non-responders following an
intervention. Repeated bouts of hypoxia can be effective at eliciting pLTF, but some studies
have reported no pLTF following repeated bouts of hypoxia (Chowdhuri et al., 2015, Janssen
and Fregosi, 2000, McGuire et al., 2002). However, the exact percentage of responders was not
reported. This suggests that LTF, although not directly reported, does not always occur
following an intervention. Here, I showed that repeated apneas consistently elicit hLTF in 65%
of animals exposed to the intervention, while intermittent LC stimulation elicit hLTF in 73% of
animals, both of which are comparable to the probability of plasticity occurring in other
systems, such as long-term potentiation in hippocampal neurons (Abraham and Huggett, 1997,
Karunakaran et al., 2016, Watanabe et al., 2002). Taken together, this suggests that the LC is a
critical component of the hLTF circuit, and its manipulation influences hLTF expression.
Lastly, it is unsurprising that the hypoglossal motor pool is involved in mediating hLTF to drive
genioglossus activity, completing the tripartite circuit (NTS → LC → XII) that mediates hLTF.

128
6.3 The site of plasticity in the hLTF tripartite circuit
Within the neural circuit mediating hLTF, there remains the question of where plasticity is
occurring. This question can be addressed by investigating the wealth of data within the
histology. Specifically, using c-Fos as an indicator for cell activity, it is possible to deduce where
plasticity may be occurring. The neural circuit (i.e., NTS → LC → XII) identifies the NTS as the
first structure critical to apnea-induced hLTF with direct projections to the LC (Lopes et al.,
2016, van Bockstaele et al., 1999). The LC is the second critical structure in the hLTF circuit and
was shown to not only possess direct projections to the hypoglossal motor pool but is critical in
apnea-induced hLTF and its stimulation can trigger hLTF. Plasticity could therefore potentially
be occurring at one or more structures within the neural circuit.
6.3.1 Plasticity at the NTS
Plasticity in the NTS has been observed before (Kline, 2008, Yamamoto et al., 2015). For
example, in hypertensive rats, NTS neurons displayed an increase in AMPA receptors and
expression of larger dendritic spines (Aicher et al., 2003, Chan et al., 2000, Saha et al., 2004). In
the context of respiration and LTF, chronic intermittent hypoxia attenuated glutamate-induced
inhibition of phrenic nerve activity (Costa-Silva et al., 2011), and acute intermittent optical
stimulation of NTS neurons triggered pLTF (Yamamoto et al., 2015). This suggests that the NTS
alone is capable of inducing LTF of phrenic/diaphragm activity. It may, therefore, be possible
that since the LC projects to the NTS (Lopes et al., 2016), intermittent LC stimulation resulted in
NTS stimulation, thereby eliciting hLTF through plasticity induced within NTS neurons. This
outcome may be unlikely since pLTF was not observed in my results, but it nonetheless suggests
that NTS neurons are capable of inducing hLTF, and a subset of NTS neurons may, therefore, be
undergoing plasticity to induce hLTF. In addition to these studies, hLTF requires NTS activity
(Torontali, 2012), and the NTS has projections to the hypoglossal motor pool (Rukhadze and
Kubin, 2007), suggesting the potential for direct modulation of hypoglossal motor neuron
activity. Although my results do not support this possibility (i.e., no increase in c-Fos activity
was observed in the NTS), c-Fos is not definitive and only provides an index of cell activity. This

129
approach naturally has limitations and cannot account for all cell activation (or inactivation)
that may have occurred. Some neurons do not express c-Fos and may not have been detected
(Teppema et al., 1997). The NTS could, therefore, be a potential site of plasticity in the hLTF
circuit.
6.3.2 Plasticity at the LC
The LC is a stronger candidate to be the site of plasticity. Majority of the studies on pLTF has
suggested that plasticity is occurring at the level of the phrenic motor neuron. Serotonin and
noradrenaline are neuromodulators that can alter the synaptic efficacy and intrinsic membrane
properties of the post-synaptic neuron. However, it is possible that the site of plasticity
mediating LTF of inspiratory genioglossus motor output is not at the hypoglossal motor neuron.
Although this differs from pLTF where plastic changes have been reported at the level of the
motor neuron (Baker-Herman et al., 2004, Dale et al., 2017, Hoffman et al., 2012, Wilkerson
and Mitchell, 2009), some experimental evidence suggest plasticity could be occurring
elsewhere. Specifically, pLTF observed in cats reported an increase in serotonergic raphe firing
rates during pLTF (Morris 2001), suggesting serotonergic raphe neurons altered their firing
pattern after repeated bouts of hypoxia (i.e., serotonergic raphe neurons exhibited plasticity).
In the context of hLTF, blockade of α1-adrenergic receptors after repeated apneas prevented
hLTF (Tadjalli, 2012). The lack of hLTF observed upon α1-receptor antagonism after hLTF
induction suggests that plasticity may not have occurred at the level of the hypoglossal motor
neuron but is responding to an increased and persistent release of noradrenaline. Plasticity is
therefore likely upstream of the hypoglossal motor pool, occurring potentially at the LC.
In this thesis, I provided evidence showing an increase in c-Fos expression (and presumably LC
activity) correlated with my intervention. For example, I showed an increase in c-Fos expression
in the LC following intermittent LC stimulation and fewer c-Fos positive cells following LC
inactivation. However, c-Fos expression represents a time window of cell activation that range
from 30 to 90 minutes. Therefore, the c-Fos expression could reflect cell activity at the 90-

130
minute time point when it was reported to be maximally activated (Bullitt, 1990, Morgan et al.,
1987), or the c-Fos expression could reflect activity at the 30-minute time window. At 30
minutes, the c-Fos profile observed would not reflect the intervention but instead reflect LC
activity during hLTF expression at the 60-minute time point. The possibility that the c-Fos
profile observed is reflective of hLTF (i.e., the 60-minute time point) was supported when I
compared c-Fos profiles in animals that exhibited hLTF to non-responders. Animals that
exhibited hLTF had more c-Fos positive cells than non-responders which could be reflective of
persistent LC firing, indicating a prolonged change in LC firing pattern (i.e., the LC has
undergone plasticity), and implicating the LC as the site of plasticity.
LC neurons also fire synchronously when activated (Christie et al., 1989, Ishimatsu and Williams,
1996a) and release more noradrenaline following repeated stimulation compared to
continuous stimulation (Florin-Lechner et al., 1996), suggesting the LC is capable of increasing
the activity to release more noradrenaline. This too, was reflected in the histology as the
percentage or proportion of c-Fos positive cells was greater than the total number of non-
ChR2-expressing mCherry positive cells, suggesting that LC activation likely recruited uninfected
cells during LC stimulation (i.e., synchronous firing). This is further supported by the fact that
stimulation of any part of the LC (i.e., rostral, medial, or caudal) can still trigger hLTF. Taken
together, the LC is likely a site for plasticity to occur within the hLTF circuit.
Further evidence that suggests plasticity to be occurring at the LC involves a recent study that
showed a persistent form of hLTF lasting 60 minutes could not be elicited following stimulation
of non-LC noradrenergic cell groups (i.e., A5 and A7) (Song and Poon, 2017). This implies that
noradrenaline release caused by in vivo stimulation of non-LC noradrenergic cell groups is
insufficient at triggering a persistent form of hLTF. Plasticity may, therefore, be occurring at the
LC itself to deliver persistent release of noradrenaline. Over the last several decades, studies
showed that the LC can alter its firing patterns and adapt under context-specific conditions,
suggesting that the LC itself readily undergoes plastic changes to its firing pattern (Aston-Jones
and Bloom, 1981, Fazlali et al., 2016, Rajkowski et al., 2004, Vankov et al., 1995), further placing

131
the LC as the likely site of plasticity in mediating hLTF. However, it is important to note that this
does not mean hypoglossal motor neurons did not undergo plastic changes as well. It is possible
that the LC mediates plasticity on two fronts - (1) the LC itself undergoes plastic changes to
modulate noradrenaline release to the target site, and (2) the LC modulates the activity of the
post-synaptic neurons via adrenergic receptor binding.
6.3.3 Plasticity at the hypoglossal motor neuron
Although the LC itself can undergo plasticity, the LC can also mediate plasticity via α- or β-
adrenergic receptor binding on the post-synaptic cell. In my introduction, I discussed how
noradrenaline binding can induce plastic changes to the post-synaptic motor neuron. Briefly,
the binding of α1-adrenergic receptors triggers a signalling cascade that initiates potentiation of
motor neuron firing by activating diacyl-glycerol (DAG) to activate protein kinase C (PKC). PKC is
hypothesized to cause AMPA receptor phosphorylation and is the hypothesized mechanism
that potentiates glutamate-evoked cell firing (Feldman et al., 2005, Neverova et al., 2007). The
activation of DAG and subsequently PKC can also increase protein synthesis of BDNF (Juric et
al., 2008), which in turn can lead to the insertion of new ion channels at the synapse (Itami et
al., 2003). Studies have shown that α1-adrenergic receptor activation on hypoglossal motor
neurons alone can trigger hLTF (Neverova et al., 2007). This suggests that noradrenaline
released from the LC could be initiating synaptic changes onto hypoglossal motor neurons, and
these changes could be the mechanism underlying hLTF.
Several studies also showed that the hypoglossal motor neuron can indeed undergo plasticity
and exhibit long-term changes on motor neuron membrane properties. For example, chronic
intermittent hypoxia spanning three months can increase α1-adrenergic receptor expression
and decrease 5HT-2A receptor expression at the hypoglossal motor pool (Rukhadze et al.,
2010). This suggests the hypoglossal motor neuron can adapt by changing receptor expression
at the synapse.

132
Desipramine, a noradrenaline reuptake inhibitor, was recently shown to abolish the reduction
in genioglossus activity associated with the transition from wakefulness to non-rapid eye
moment (NREM) sleep (Taranto-Montemurro et al., 2016), suggesting the increased action on
α1-receptors presumably on hypoglossal motor neurons can augment genioglossus muscle
tone. In addition, the activation of α1-adrenergic receptors could cause brain-derived
neurotrophic factor (BDNF) to bind to TrkB receptors at the hypoglossal motor neuron, thereby
inducing hLTF. Activation of TrkB receptors can initiate kinase cascades leading to enhanced
synaptic efficacy or insertion of new ion channels to the pre- or post- synaptic membrane (Itami
et al., 2003, Juric et al., 2008). This was supported in studies that investigated the mechanisms
underlying pLTF where it was found to require novel protein synthesis via BDNF for pLTF to
manifest (Baker-Herman et al., 2004, Baker-Herman and Mitchell, 2002). In addition, activation
of TrkB receptors on or near phrenic motor neurons can elicit pLTF (Golder et al., 2008). Similar
mechanisms are observed in hLTF. Specifically, TrkB receptor blockade at the hypoglossal motor
pool prevented apnea-induced hLTF while TrkB receptor activation alone at the hypoglossal
could elicit hLTF (Tadjalli, 2012). By altering the activity of TrkB receptors at the level of the
hypoglossal motor pool, it was possible to alter genioglossus motor output, suggesting hLTF to
be mediated by a TrkB-receptor mechanism within the hypoglossal motor pool.
6.4 Summary of proposed mechanism underlying hLTF
My working hypothesis stemmed from apnea-induced hLTF. The trigger (repeated apneas)
elicited hLTF via repeated modulation of vagus-mediated broncho-pulmonary feedback (Tadjalli
et al., 2010), indicating an obstruction of airflow. This signal (or lack thereof) is propagated via
vagal afferents to terminate at the NTS, the first critical structure in my hypothesized hLTF
neural circuit (Fig. 6.1). The NTS in turns send direct excitatory projections to the LC. I
hypothesize that this connection is glutamatergic based on 4 lines of evidence: (1) there is an
increase in LC activity following apnea-induced hLTF, suggesting an excitatory neurotransmitter
is involved, (2) recordings from LC neurons that receive NTS innervations showed an increase in
the firing rates of LC neurons during hypercapnia (Lopes et al., 2016), and (3) LC-projecting NTS

133
neurons were shown using electron microscopy to possess structures that implicate they are
glutamatergic axon terminals (van Bockstaele et al., 1999), and (4) plasticity at the NTS has
been reported to involve glutamatergic signalling (Bonham et al., 2006, Kline, 2008). Together,
these data suggest that the NTS → LC connection is likely a glutamatergic connection. The
patterned activation of LC neurons by the NTS causes a recruitment of additional LC neurons to
release noradrenaline onto hypoglossal motor neurons (Christie et al., 1989, Ishimatsu and
Williams, 1996b). The LC then undergoes plastic changes by increasing its activity for persistent
noradrenaline release. Noradrenaline binds to α1-adrenergic receptors on hypoglossal motor
neurons to induce hLTF, potentially via increased excitability to the post-synaptic cell caused by
reduce potassium currents and AMPA channel insertion. The increased excitability of
hypoglossal motor neurons allows for increased genioglossus motor output (i.e., hLTF). I
thereby hypothesize that plasticity is occurring at two fronts: (1) increased noradrenaline
release from altered LC activity, and (2) increased excitability of hypoglossal motor neurons
through post-synaptic changes.

134
Figure 6.1. Hypothesized neural circuit underlying hLTF. (A) Brain map showing the potential sources of noradrenaline mediating hLTF. The locus coeruleus (LC) was shown to be the critical structure mediating hLTF and the hypothesized circuit is outlined in purple (inset) and expanded in (B). (B) Repeated obstructive apneas modulate vagal afferent activity, which terminates in the nucleus tractus solitarius (NTS). Cells in the NTS send glutamatergic (Glu) projections to activate locus coeruleus neurons to release noradrenaline (NA) directly onto the α1-adrenergic receptors on hypoglossal (XII) motor neurons to modulate hypoglossal (and therefore genioglossus) activity, effectively triggering hLTF. Intermittent stimulation of the locus coeruleus directly can also induce noradrenaline release onto hypoglossal motor neurons to trigger hLTF. I hypothesize that this is the neural circuit and mechanism underlying LTF of inspiratory genioglossus motor output.
6.5 Methodological considerations
Throughout this thesis, I chose 60 minutes to define hLTF in healthy animals. There are many
limitations with this approach as OSA patients experience apneas throughout the night (i.e.,

135
longer than 60 minutes). In addition, my approach investigated a neural circuit prior to chronic
exposure to hypoxia and hypercapnia and thus may be less physiological relevant in OSA
patients. It may therefore be possible that these findings are less applicable in a clinical setting.
However, hLTF can be observed in OSA patients (Aboubakr et al., 2001, Younes et al., 2014),
suggesting that the capability for hLTF is present but may be compromised or insufficient at
mitigating the obstructions. In addition, studies using chronic intermittent hypoxia over a
course of 3 months showed changes in α1-adrenergic and 5-HT2A receptor expression on rat
hypoglossal motor neurons (Rukhadze et al., 2010), suggesting long-term plasticity may be
involved to help mitigate symptoms. My approach provides insight into an existing neural
circuit but cannot address the possible long-term changes that may have greater impact on
how hLTF manifests in a clinical setting.
Another consideration in these studies is the fact that all experiments conducted used
genioglossus EMG amplitude as my metric to define hLTF. Although the genioglossus muscle is
a major airway dilator muscle, other muscles contribute to airway patency (Fuller et al., 1999).
Without direct measurements on airway resistance or airflow, I can only postulate the potential
benefits of hLTF. However, hLTF is noradrenaline-dependent and ventilatory LTF was observed
mice absent serotonin in the central nervous system (Hickner et al., 2014). This suggests that
ventilatory LTF may be mediated by noradrenaline-dependent hLTF. In addition, measurements
of upper airway resistance and airflow are performed human studies using similar triggers (i.e.,
repeated bouts of hypoxia) where hLTF was observed (Aboubakr et al., 2001, Chowdhuri et al.,
2008, Griffin et al., 2012, Harris et al., 2006, Shkoukani et al., 2002), and likely involved an
increase in genioglossus muscle tone (Harris et al., 2006).
Other considerations include my approach to blood gas measurements. I did not measure blood
gases in my experiments. Instead, end-tidal CO2 measurements were recorded in animals as a
percent and no real units (e.g. mmHg) are available. In my experiments, ET-CO2 levels peaked at
6% at the end of the repeated apnea intervention which can be approximated to 46 mmHg
(Carroll, 1999). Ideally, direct measurements of arterial CO2 levels would have been more

136
accurate as changes within a few mmHg can have a significant influence on the expression of
hLTF and diaphragm activity. Similarly, measurements of blood oxygen saturation were also
performed non-invasively using pulse oximetry to monitor arterial oxygenation levels. Although
a significant reduction in oxygen saturation was observed during apneas, actual arterial partial
pressures of oxygen were not measured. hLTF induced by intermittent hypoxia typically lowers
oxygen saturation to a partial pressure of 35-45 mmHg (Dale et al., 2017, Devinney et al., 2015,
Fuller et al., 2000). My approach using repeated apneas does not allow a direct comparison to
these studies.
One large limitation in this thesis involves the statistical analyses used to compare animals that
exhibited apnea-induced hLTF to animals that did not exhibit hLTF following LC inactivation.
Excluding animals that did not exhibit hLTF in one group may skew my statistical analyses
because it implies that 27-35% of animals would not have exhibited hLTF regardless of my
intervention. However, by simply comparing the number of animals that did and did not
express hLTF, it is very unlikely that the non-responders (i.e., 27-35% of animals) were
repeatedly observed in my LC inactivation or hypoglossal α1-receptor blockade studies. In
animals that were given repeated apneas, out of 14 animals, 9 animals expressed hLTF, 5 did
not (i.e., 65% of animals exhibited hLTF). In animals given intermittent light stimulation, 8
expressed hLTF, 3 did not (i.e., 73% of animals exhibited hLTF). In animals that got no
stimulation, 1 expressed hLTF, 4 did not (i.e., 25% of animals exhibit hLTF without intervention).
In animals that received LC inactivation, all 9 animals did not express hLTF. Similarly, in animals
with hypoglossal α1-receptors blocked, all 8 animals did not express hLTF. By simply comparing
n-values, I would expect to observe hLTF in 25% (natural variation) to 73% (stimulation) of
animals following an intervention. When the LC was inactivated or hypoglossal α1-receptors
blocked, I did not get hLTF in any of the 17 animals tested. Therefore, the probability that 17
animals were coincidentally all non-responders is unlikely, suggesting LC activation and
hypoglossal α1-receptor activation is likely necessary for hLTF expression. Nonetheless, I
continue to address this concern using different statistical approaches.

137
Current LTF studies have not set a precedent on how to address non-responders, but instead
continue to follow statistical analysis traditionally used (i.e., a one-way ANOVA or a two-way
ANOVA). The statistical approach that I introduced here addresses this problem by including all
animals (i.e., animals that exhibit hLTF and non-responders) in my statistical analysis. The chi-
square test and the Firth logistic regression provide insight into whether my intervention
prevented apnea-induced hLTF (i.e., not due to random chance), and showed that the
expression of hLTF following my intervention was in fact not due to random chance. In addition,
the ordinary least squares linear regression (OLS) can determine the strength and direction of
my intervention on the outcome and found that my intervention significantly influenced the
outcome of hLTF expression. These statistical solutions may not be the best approach but
provides what I believe is the start to addressing this caveat.
Lastly, the interpretation of my histology results allowed me to provide insight into where I
hypothesize plasticity is occurring within the hLTF circuit (NTS → LC → XII). However, these
interpretations were based on c-Fos results which is (1) correlative, and (2) inherently biased
towards cells that express c-Fos (i.e., the approach ignores cells that do not express c-Fos). My
interpretations could therefore undervalue the contribution of other cell groups that may be
involved with hLTF and plasticity. Ideally, this would be addressed using cell recordings from the
hypothesized structures in the hLTF circuit.
6.6 Significance of findings
I have shown that repeated apneas are a trigger that can elicit a naturally occurring form of
plasticity that can augment respiratory motor output. hLTF is naturally protective when faced
with repeated respiratory challenges. My findings have added to the field of respiratory motor
plasticity research by identifying the neural circuit that mediates hLTF (i.e., NTS → LC → XII).
This circuit underlies a naturally protective form of respiratory motor plasticity, which can help
identify new therapeutic targets to mitigate some respiratory disorders such as obstructive
sleep apnea (OSA).

138
OSA is defined by a reduction in upper airway muscle tone during sleep can lead to obstructions
in the upper airways causing apneas. Wakefulness caused by a reflexive increase in ventilatory
effort from apnea-induced hypoxia and hypercapnia ends the apnea, only to repeat when the
patient resumes sleep. LTF of genioglossus motor output, which humans exhibit (Aboubakr et
al., 2001, Chowdhuri et al., 2008, Griffin et al., 2012, Harris et al., 2006, Schwartz et al., 2012,
Shkoukani et al., 2002), could potentially increase upper airway muscle tone, mitigating the
reduction that occurs during sleep, which may aid OSA patients.
In this thesis, I identified a novel trigger to elicit this form of plasticity. The LC is critical to hLTF
and stimulation of this structure alone can elicit hLTF. To date, LTF has focused largely on
changes to phrenic motor neuron activity. The identification of the LC as a trigger not only
allows for targeted therapeutic treatments, but also provides insight to the possible interaction
with current pharmaceutical treatments that have shown to be promising for treating OSA. For
example, clinical studies have shown desipramine, a noradrenaline reuptake inhibitor, to
prevent the natural reduction in genioglossus muscle tone during transition from wakefulness
to NREM sleep (Taranto-Montemurro et al., 2016). It may therefore be possible for a
noradrenaline reuptake inhibitor to elevate noradrenaline levels to maintain upper airway
muscle tone during sleep.
My findings have also contributed to the identification of potential sites where plasticity could
be occurring. It may be possible to trigger hLTF by inducing plasticity within the hLTF circuit. For
example, by increasing α1-adrenergic receptor expression at the hypoglossal motor pool
through chronic exposure to hypoxia (Rukhadze et al., 2010), it may be possible to increase
genioglossus motor output thereby mitigating the apnea. Taken together, these findings
provide a foundation to guide future studies into therapeutic directions to treat OSA.

139
6.7 Future directions
Currently, I have shown that the LC is a critical structure in mediating hLTF. However, the
activity of the LC prior to hLTF induction and its activity following hLTF induction have not been
recorded. In this thesis, I show an increase in c-Fos expression and presumably LC activity. The
next step would be to use cell recording to quantify LC activity before, during, and after hLTF
induction. Furthermore, cell recordings taken from tripartite circuit could help determine the
site(s) of plasticity. By identifying the role each site plays, it may be possible to target structures
upstream of the motor pool to induce hLTF.
In addition, other neurotransmitters and neuromodulators require further investigation to
elucidate their role in hLTF. Although I have shown that the LC mediates hLTF via noradrenaline
binding to α1-adrenergic receptors on hypoglossal motor neurons, these findings do not
address the role of co-released neurotransmitters and modulators that may facilitate this
process. For example, serotonin is not required for apnea-induced hLTF (Tadjalli et al., 2010)
but still possess a large influence on hypoglossal motor neuron activity (Sood et al., 2005).
These neurotransmitters and neuromodulators require further investigation to decipher a more
comprehensive view of the mechanisms underlying hLTF.
It is my hope that LTF research will continue to grow in the field of respiratory plasticity such
that better treatments can be provided for respiratory disorders, and greater knowledge can be
achieved for plasticity research.

140
References
Abbott SB, Coates MB, Stornetta RL, Guyenet PG (2013) Optogenetic stimulation of c1 and retrotrapezoid nucleus neurons causes sleep state-dependent cardiorespiratory stimulation and arousal in rats. Hypertension 61:835-841.
Abbott SB, Pilowsky PM (2009) Galanin microinjection into rostral ventrolateral medulla of the rat is hypotensive and attenuates sympathetic chemoreflex. American journal of physiology Regulatory, integrative and comparative physiology 296:R1019-R1026.
Abbott SB, Stornetta RL, Fortuna MG, Depuy SD, West GH, Harris TE, Guyenet PG (2009) Photostimulation of retrotrapezoid nucleus phox2b-expressing neurons in vivo produces long-lasting activation of breathing in rats. The Journal of neuroscience : the official journal of the Society for Neuroscience 29:5806-5819.
Aboubakr SE, Taylor A, Ford R, Siddiqi S, Badr MS (2001) Long-term facilitation in obstructive sleep apnea patients during NREM sleep. J Appl Physiol (1985) 91:2751-2757.
Abraham WC, Huggett A (1997) Induction and reversal of long-term potentiation by repeated high-frequency stimulation in rat hippocampal slices. Hippocampus 7:137-145.
Abraham WC, Mason SE, Demmer J, Williams JM, Richardson CL, Tate WP, Lawlor PA, Dragunow M (1993) Correlations between immediate early gene induction and the persistence of long-term potentiation. Neuroscience 56:717-727.
Adams LM, Foote SL (1988) Effects of locally infused pharmacological agents on spontaneous and sensory-evoked activity of locus coeruleus neurons. Brain Research Bulletin 21:395-400.
Aicher SA, Sharma S, Mitchell JL (2003) Structural changes in AMPA-receptive neurons in the nucleus of the solitary tract of spontaneously hypertensive rats. Hypertension 41:1246-1252.
Aldes LD (1990) Topographically organized projections from the nucleus subceruleus to the hypoglossal nucleus in the rat: a light and electron microscopic study with complementary axonal transport techniques. The Journal of comparative neurology 302:643-656.
Aldes LD, Chapman ME, Chronister RB, Haycock JW (1992) Sources of noradrenergic afferents to the hypoglossal nucleus in the rat. Brain Res Bull 29:931-942.
Andero R, Choi DC, Ressler KJ (2014) BDNF-TrkB receptor regulation of distributed adult neural plasticity, memory formation, and psychiatric disorders. Progress in molecular biology and translational science 122:169-192.
Andresen MC (1994) Nucleus tractus solitarius - gateway to neural circulatory control. Annu Rev Physiol 56:93-116.
Anikeeva P, Andalman AS, Witten I, Warden M, Goshen I, Grosenick L, Gunaydin LA, Frank LM, Deisseroth K (2011) Optetrode: a multichannel readout for optogenetic control in freely moving mice. Nature neuroscience 15:163-170.
Aoki C, Go C, Venkatesan C, Kurose H (1994) Perikaryal and synaptic localization of a a2A-adrenergic receptor-like immunoreactivity. Brain research 650:181-204.
Aston-Jones G, Bloom FE (1981) Activity of norepinephrine-containing locus coeruleus neurons in behaving rats anticipates fluctuations in the sleep-waking cycle. The Journal of neuroscience : the official journal of the Society for Neuroscience 1:876-886.
Aston-Jones G, Bloom, F.E. (1981) Activity of norepinephrine-containing locus coeruleus neurons in behaving rats anticipates fluctuationsin the sleep-wake cycle. Neuroscience 1:876-886.
Aston-Jones G, Ennis M, Pieribone VA, Nickell WT, Shipley MT (1970) The brain nucleus locus coeruleus: restricted afferent control of a broad efferent network. Science 234:734-737.
Bacak BJ, Kim T, Smith JC, Rubin JE, Rybak IA (2016) Mixed-mode oscillations and population bursting in the pre-Bӧtzinger complex. pp 1-58 eLife.

141
Bach KB, Mitchell GS (1996) Hypoxia-induced long-term facilitation of respiratory activity is serotonin dependent. Respiration physiology 104:251-260.
Bach KB, Mitchell GS (1998) Hypercapnia-induced long-term depression of respiratory activity requires alpha(2)-adrenergic receptors. Journal of Applied Physiology 84:2099-2105.
Badie-Mahdavi H, Lu X, Behrens MM, Bartfai T (2005) Role of galanin receptor 1 and galanin receptor 2 activation in synaptic plasticity associated with 3',5'-cyclic AMP response element-binding protein phosphorylation in the dentate gyrus: studies with a galanin receptor 2 agonist and galanin receptor 1 knockout mice. Neuroscience 133:591-604.
Baertsch NA, Baker-Herman TL (2013) Inactivity-induced phrenic and hypoglossal motor facilitation are differentially expressed following intermittent vs. sustained neural apnea. J Appl Physiol (1985) 114:1388-1395.
Baker-Herman TL, Fuller DD, Bavis RW, Zabka AG, Golder FJ, Doperalski NJ, Johnson RA, Watters JJ, Mitchell GS (2004) BDNF is necessary and sufficient for spinal respiratory plasticity following intermittent hypoxia. Nature neuroscience 7:48-55.
Baker-Herman TL, Mitchell GS (2002) Phrenic long-term facilitation requires spinal serotonin receptor activation and protein synthesis. The Journal of neuroscience : the official journal of the Society for Neuroscience 22:6239-6246.
Baker-Herman TL, Strey KA (2011) Similarities and differences in mechanisms of phrenic and hypoglossal motor facilitation. Respiratory physiology & neurobiology 179:48-56.
Baker TL, Fuller DD, Zabka AG, Mitchell GS (2001) Respiratory plasticity: differential actions of continuous and episodic hypoxia and hypercapnia. Respiration physiology 129:25-35.
Baker TL, Mitchell GS (2000) Episodic but not continuous hypoxia elicits long-term facilitation of phrenic motor output in rats. The Journal of physiology 529.1:215-219.
Barraco RA, Ergene E, Dunbar JC, El-Ridi MR (1990) Cardiorespiratory Response Patterns Elicited by Microinjections of Neuropeptide Y in the Nucleus Tractus Solitarius. Brain Research Bulletin 24:465-485.
Basting TM, Burke PG, Kanbar R, Viar KE, Stornetta DS, Stornetta RL, Guyenet PG (2015) Hypoxia silences retrotrapezoid nucleus respiratory chemoreceptors via alkalosis. The Journal of neuroscience : the official journal of the Society for Neuroscience 35:527-543.
Benowitz LI, Routtenberg A (1997) GAP-43: an intrinsic determinant of neuronal development and plasticity. TINS 20:84-91.
Berger AJ, Herbert DA, Mitchell RA (1978) Properties of apneusis produced by reversible cold block of the rostral pons. Respiration physiology 33:323-337.
Berlucchi G (2002) The origin of the term plasticity in the neurosciences: Ernesto Lugaro and chemical synaptic transmission. Journal of the history of the neurosciences 11:305-309.
Berquin P, Bodineau L, Gros F, Larnicol N (2000) Brainstem and hypothalamic areas involved in respiratory chemoreflexes: a Fos study in adult rats. Brain research 857:30-40.
Bhaskaran D, Freed CR (1988) Changes in Neurotransmitter Turnover in Locus Coeruleus Produced by Changes in Arterial Blood Pressure. Brain Research Bulletin 21:191-199.
Biancardi V, Bicego KC, Almeida MC, Gargaglioni LH (2008) Locus coeruleus noradrenergic neurons and CO2 drive to breathing. Pflugers Archiv : European journal of physiology 455:1119-1128.
Blanco CE, Dawes GS, Hanson MA, McCooke HB (1984) The response to hypoxia of arterial chemoreceptors in fetal sheep and new-born lambs. The Journal of physiology 351:25-37.
Bliss TVP, Lomo T (1973) Long-lasting potentiation of synaptic transmission in the denrate area of the anaesthetized rabbit following stimulation of the perforant path. The Journal of physiology 232:331-356.
Blitz DM, Ramirez JM (2002) Long-term modulation of respiratory network activity following anoxia in vitro. Journal of neurophysiology 87:2964-2971.

142
Blum R, Konnerth A (2005) Neurotrophin-Mediated Rapid Signaling in the Central Nervous System: Mechanisms and Functions. Physiology 20:70-78.
Bocchiaro CM, Feldman JL (2004) Synaptic activity-independent persistent plasticity in endogenously active mammalian motoneurons. Proceedings of the National Academy of Sciences of the United States of America 101:4292-4295.
Bodineau L, Larnicol N (2001) Brainstem and hypothalamic areas activated by tissue hypoxia: Fos-like immunoreactivity induced by carbon monoxide inhalation in the rat. Neuroscience 108:643-653.
Bonham AC, Chen CY, Sekizawa S, Joad JP (2006) Plasticity in the nucleus tractus solitarius and its influence on lung and airway reflexes. J Appl Physiol (1985) 101:322-327.
Bonham AC, McCrimmon DR (1990) Neurones in a discrete region of the nucleus tractus solitarius are required for the Breuer-Hering reflex in rat. The Journal of physiology 427:261-280.
Boone TB, Aldes LD (1984) The ultrastructure of two distinct neuron populations in the hypoglossal nucleus of the rat. Exp Brain Res 54:321-326.
Bullitt E (1990) Expression of c-Fos-like protein as a marker for neuronal activity following noxious stimulation in the rat. The Journal of comparative neurology 296:517-530.
Byrum CEG, P.G. (1987) Afferent and Efferent Connections of the A5 Noradrenergic Cell Group in the Rat. The Journal of comparative neurology 261:529-542.
Caille D, Vibert JF, Hugelin A (1981) Apneusis and apnea after parabrachial or Kolliker-Fuse n. lesion; influence of wakefulness. Respiration physiology 45:79-95.
Cajal SR (1911) Histologie du Systeme Nerveux de l’Homme et des Vertebres,. New York: Oxford University Press.
Cao Y, Ling L (2010) Urethane inhibits genioglossal long-term facilitation in un-paralyzed anesthetized rats. Neuroscience letters 477:124-128.
Cao Y, Zwillich CW, Berthon-Jones M, Sullivan CE (1992) Increased normoxic ventilation induced by repetitive hypoxia in conscious dogs. J Appl Physiol 73:2083-2088.
Carroll P (1999) Respiratory monitoring. RN 62:68-72. Carter ME, Yizhar O, Chikahisa S, Nguyen H, Adamantidis A, Nishino S, Deisseroth K, de Lecea L (2010)
Tuning arousal with optogenetic modulation of locus coeruleus neurons. Nature neuroscience 13:1526-1533.
Cedarbaum JM, Aghajanian GK (1978) Afferent projections to the rat locus coeruleus as determined by a retrograde tracing technique. The Journal of comparative neurology 178:1-16.
Chan E, Steenland HW, Liu H, Horner RL (2006) Endogenous excitatory drive modulating respiratory muscle activity across sleep-wake states. American journal of respiratory and critical care medicine 174:1264-1273.
Chan RKW, Peto CA, Sawchenko PE (2000) Fine Structure and Plasticity of Barosensitive Neurons in the Nucleus of Solitary Tract. The Journal of comparative neurology 422:338-351.
Chan RKW, Sawchenko PE (1994) Spatially and Temporally Differentiated Patterns of c-fos Expression in Brainstem Catecholaminergic Cell Groups Induced by Cardiovascular Challenges in the Rat. The Journal of comparative neurology 348:433-460.
Choi SJ, Panhelainen A, Schmitz Y, Larsen KE, Kanter E, Wu M, Sulzer D, Mosharov EV (2015) Changes in neuronal dopamine homeostasis following 1-methyl-4-phenylpyridinium (MPP+) exposure. The Journal of biological chemistry 290:6799-6809.
Chowdhuri S, Pierchala L, Aboubakr SE, Shkoukani M, Badr MS (2008) Long-term facilitation of genioglossus activity is present in normal humans during NREM sleep. Respiratory physiology & neurobiology 160:65-75.
Chowdhuri S, Pranathiageswaran S, Franco-Elizondo R, Jayakar A, Hosni A, Nair A, Badr MS (2015) Effect of age on long-term facilitation and chemosensitivity during NREM sleep. J Appl Physiol (1985) 119:1088-1096.

143
Christie MJ, Williams JT, North RA (1989) Electrical Coupling Synchronizes Subthreshold Coeruleus Neurons in vitro from Neonatal Rats. Neuroscience 9:3584-3589.
Cline HT (1993) Adivity-dependent plasticity in the visual systems of frogs and fish. TINS 14:104-111. Coates EL, Li A, Nattie EE (1993) Widespread sites of brain stem ventilatory chemoreceptors. J Appl
Physiol (1985) 75:5-14. Cohen MI (1971) Switching of the respiratory phases and evoked phrenic responses produced by rostral
pontine electrical stimulation. The Journal of physiology 217:133-158. Collingridge GL, Kehl SJ, McLennan H (1983) Excitatory amino acids in synaptic transmission in the
schaefer colateral-commissural pathway of the rat hippocampus. The Journal of physiology 334:33-46.
Consolo S, Baldi G, Russi G, Civenni G, Bartfai T, Vezzani A (1994) Impulse flow dependency of galanin release in vivo in the rat ventral hippocampus. Proceedings of the National Academy of Sciences of the United States of America 91:8047-8051.
Conte WL, Kamishina H, Reep RL (2009) Multiple neuroanatomical tract-tracing using fluorescent Alexa Fluor conjugates of cholera toxin subunit B in rats. Nature protocols 4:1157-1166.
Costa-Silva JH, Zoccal DB, Machado BH (2011) Chronic intermittent hypoxia alters glutamatergic control of sympathetic and respiratory activities in the commissural NTS of rats. American journal of physiology Regulatory, integrative and comparative physiology 302:R785-793.
Coumis U, Davies CH (2002) The effects of galanin on long-term synaptic plasticity in the CA1 area of rodent hippocampus. Neuroscience 112:173-182.
Dale EA, Fields DP, Devinney MJ, Mitchell GS (2017) Phrenic motor neuron TrkB expression is necessary for acute intermittent hypoxia-induced phrenic long-term facilitation. Experimental neurology 287:130-136.
Dampney RAL (1994) Functional Organization of Central Pathways Regulating the Cardiovascular System. Physiological reviews 74:323-364.
de Castro D, Lipski J, Kanjhan R (1994) Electrophysiological study of dorsal respiratory neurons in the medulla oblongata of the rat. Brain research 639:49-56.
Deacon NL, McEvoy DR, Stadler DL, Catcheside PG (2017) Intermittent hypercapnic hypoxia during sleep does not induce ventilatory long term facilitation in healthy males. J Appl Physiol 1-31.
DeBock F, Kurz J, Azad SC, Parsons CG, Hapfelmeier G, Zieglgänsberger W, Rammes G (2003) α2-Adrenoreceptor activation inhibits LTP and LTD in the basolateral amygdala: involvement of Gi/o-protein-mediated modulation of Ca2+-channels and inwardly rectifying K+-channels in LTD. European Journal of Neuroscience 17:1411-1424.
Del Negro CA, Morgado-Valle C, Feldman JL (2002) Respiratory rhythm: an emergent network property? Neuron 34:821-830.
Devinney MJ, Fields DP, Huxtable AG, Peterson TJ, Dale EA, Mitchell GS (2015) Phrenic long-term facilitation requires PKCtheta activity within phrenic motor neurons. The Journal of neuroscience : the official journal of the Society for Neuroscience 35:8107-8117.
Devoto P, Flore G (2006) On the Origin of Cortical Dopamine: Is it a Co-Transmitter in Noradrenergic Neurons? Current neuropharmacology 4:115-125.
Dobbins EG, Feldman JL (1994) Brainstem network controlling descending drive to phrenic motoneurons in rat. The Journal of comparative neurology 347:64-86.
Dobbins EG, Feldman JL (1995) Differential Innervation of Protruder and Retractor Muscles of the Tongue in Rat. The Journal of comparative neurology 376-394.
Dodig PI, Pecotic R, Valic M, Dogas Z (2012) Acute intermittent hypoxia induces phrenic long-term facilitation which is modulated by 5-HT1A receptor in the caudal raphe region of the rat. Journal of sleep research 21:195-203.

144
Dragunow M, Faull RLM, Jansen KLR (1990) MK-801, an antagonist of NMDA receptors, inhibits injury-induced c-Fos protein accumulation in rat brain. Neuroscience letters 109.
Dremencov E, El Mansari M, Blier P (2007) Distinct electrophysiological effects of paliperidone and risperidone on the firing activity of rat serotonin and norepinephrine neurons. Psychopharmacology (Berl) 194:63-72.
Duffin J (1990) The chemoreflex control of breathing and its measurement. Canadian Journal of Anaesthesia 37:933-942.
Duffin J (2004) Functional organization of respiratory neurones: a brief review of current questions and speculations. Experimental physiology 89:517-529.
Duffin J (2005) Role of acid-base balance in the chemoreflex control of breathing. J Appl Physiol (1985) 99:2255-2265.
Dunwiddie T, Lynch G (1978) Long-term potentiation and depression of synaptic responses in the rat hippocampus: localization and frequency dependency. The Journal of physiology 276:353-367.
Edge D, O'Halloran KD (2015) Chronic Intermittent Hypoxia Blunts the Expression of Ventilatory Long Term Facilitation in Sleeping Rats. Adv Exp Med Biol 860:335-342.
Everitt BJ, Hokfelt T, Terenius L, Tatemoto K, Mutt V, Goldstein M (1984) Differential co-existence of neuropeptide y (NPY)-like immunoreactivity with catecholamines in the central nervous system of the rat. Neuroscience 11:443-462.
Ezure K, Tanaka I (2000) Identification of deflation-sensitive inspiratory neurons in the dorsal respiratory group of the rat. Brain research 883:22-30.
Fazlali Z, Ranjbar-Slamloo Y, Adibi M, Arabzadeh E (2016) Correlation between Cortical State and Locus Coeruleus Activity: Implications for Sensory Coding in Rat Barrel Cortex. Frontiers in neural circuits 10:14.
Feldman JL, Loewy AD, Speck DF (1985) Projections from the Ventral Respiratory Group to Phrenic and Intercostal Motoneurons in Cat: An Autoradiographic Study. Neuroscience 5:1993-2000.
Feldman JL, Mitchell GS, Nattie EE (2003) Breathing: rhythmicity, plasticity, chemosensitivity. Annual review of neuroscience 26:239-266.
Feldman JL, Neverova NV, Saywell SA (2005) Modulation of hypoglossal motoneuron excitability by intracellular signal transduction cascades. Respiratory physiology & neurobiology 147:131-143.
Fenik V, Marchenko V, P. J, Davies RO, Kubin L (2002) A5 cells are silenced when REM sleep-like signs are elicited by pontine carbachol. J Appl Physiol 93:1448-1456.
Fenik VB, Fung SJ, Lim V, Chase MH (2013) Quantitative analysis of the excitability of hypoglossal motoneurons during natural sleep in the rat. Journal of neuroscience methods 212:56-63.
Fenik VB, Rukhadze I, Kubin L (2008) Inhibition of pontine noradrenergic A7 cells reduces hypoglossal nerve activity in rats. Neuroscience 157:473-482.
Fitzgerald R (1995) Lung Biology in Health and Disease: A History of Breathing Physiology. In: The Regulation of Breathing (Proctor, D. F., ed), pp 303-333 New York: Marcel Dekker Inc.
Florin-Lechner SM, Druhan JP, Aston-Jones G, Valentino RJ (1996) Enhanced norepinephrine release in prefrontal cortex with burst stimulation of the locus coeruleus. Brain research 742:89-97.
Fregosi RF, Fuller DD (1997) Respiratory-related control of extrinsic tongue muscle activity. Respiration physiology 110:295-306.
Fritschy J, Grzanna R (1990) Distribution of locus coeruleus axons within the rat brainstem demonstrated by phaseolus vulgaris leucoagglutinin anterograde tracing in combination with dopamine-b-hydroxylase immunofluorescence. The Journal of comparative neurology 293:616-631.
Fuller DD (2005) Episodic hypoxia induces long-term facilitation of neural drive to tongue protrudor and retractor muscles. J Appl Physiol (1985) 98:1761-1767.
Fuller DD, Bach KB, Baker TL, Kinkead R, Mitchell GS (2000) Long term facilitation of phrenic motor output. Respiration physiology 121:135-146.

145
Fuller DD, Williams JS, P.L. J, Fregosi RF (1999) Effect of co-activation of tongue protrudor and retractor muscles on tongue movements and pharyngeal airflow mechanics in the rat. The Journal of physiology 519.2:601-613.
Fuller DD, Zabka AG, Baker TL, Mitchell GS (2001) Phrenic long-term facilitation requires 5-HT receptor activation during but not following episodic hypoxia. J Appl Physiol (1985) 90:2001-2006; discussion 2000.
Fung SJ, Chase MH (2015) Postsynaptic inhibition of hypoglossal motoneurons produces atonia of the genioglossal muscle during rapid eye movement sleep. Sleep 38:139-146.
Fung SJ, Manzoni D, Chan JY, Pompeiano O, Barnes CD (1991) Locus coeruleus control of spinal motor output. Progress in brain research 88:395-409.
Fung SJ, Reddy VK, Liu RH, Wang Z, Barnes CD (1994) Existence of glutamate in noradrenergic locus coeruleus neurons of rodents. Brain Research Bulletin 35:505-512.
Furtinger S, Pirker S, Czech T, Baumgartner C, Ransmayr G, Sperk G (2001) Plasticity of Y1 and Y2 Receptors and Neuropeptide Y Fibers in Patients with Temporal Lobe Epilepsy. Neuroscience 21:5804-5812.
G.D. F, Smith JC, Feldman JL (1993) Generation and Transmission of Respiratory Oscillations in Medullary Slices: Role of Excitatory Amino Acids. Journal of neurophysiology 70:1497-1515.
Gandolfi D, Cerri S, Mapelli J, Polimeni M, Tritto S, Fuzzati-Armentero MT, Bigiani A, Blandini F, Mapelli L, D'Angelo E (2017) Activation of the CREB/c-Fos Pathway during Long-Term Synaptic Plasticity in the Cerebellum Granular Layer. Frontiers in cellular neuroscience 11:184.
Gao WJ, Ji RR (2009) c-Fos or pERK, which is a better marker for neuronal activation and central sensitization after noxious stimulation and tissue injury? The Open Pain Journal 2:11-17.
Gargaglioni LH, Hartzler LK, Putnam RW (2010) The locus coeruleus and central chemosensitivity. Respiratory physiology & neurobiology 173:264-273.
Gerst DG, 3rd, Yokhana SS, Carney LM, Lee DS, Badr MS, Qureshi T, Anthouard MN, Mateika JH (2011) The hypoxic ventilatory response and ventilatory long-term facilitation are altered by time of day and repeated daily exposure to intermittent hypoxia. J Appl Physiol (1985) 110:15-28.
Getting PA (1989) Emerging principles governing the operation of neural networks. Ann Rev Neurosci 12:185-204.
Golder FJ, Ranganathan L, Satriotomo I, Hoffman M, Lovett-Barr MR, Watters JJ, Baker-Herman TL, Mitchell GS (2008) Spinal adenosine A2a receptor activation elicits long-lasting phrenic motor facilitation. The Journal of neuroscience : the official journal of the Society for Neuroscience 28:2033-2042.
Goodman CS, Shatz CJ (1993) Developmental Mechanisms that Generate Precise Patterns of Neuronal Connectivity. Neuron 10:77-98.
Gottschalk WA, Jiang H, Tartaglia N, Feng L, Figurov A, Lu B (1999) Signalling mechanisms mediating BDNF modulation of synaptic plasticity in the hippocampus. Learning and Memory 6:243-256.
Gradinaru V, Zhang F, Ramakrishnan C, Mattis J, Prakash R, Diester I, Goshen I, Thompson KR, Deisseroth K (2010) Molecular and cellular approaches for diversifying and extending optogenetics. Cell 141:154-165.
Gray PA, Rekling JC, Bocchiaro CM, Feldman JL (1999) Modulation of Respiratory Frequency by Peptidergic Input to Rhythmogenic Neurons in the PreBo¬tzinger Complex. Science 286:1566-1568.
Griffin HS, Pugh K, Kumar P, Balanos GM (2012) Long-term facilitation of ventilation following acute continuous hypoxia in awake humans during sustained hypercapnia. The Journal of physiology 590:5151-5165.
Guyenet PG, Wang H (2001) Pre-Bo¨tzinger Neurons With Preinspiratory Discharges “In Vivo” Express NK1 Receptors in the Rat. American Physiological Society 86:438-446.

146
Guzowski JF, McNaughton BL, Barnes CA, Worley PF (1999) Environment-specific expression of the immediate-early gene Arc in hippocampal neuronal ensembles. Nature neuroscience 2:1120-1124.
Gysbrechts B, Wang L, Trong NN, Cabral H, Navratilova Z, Battaglia F, Saeys W, Bartic C (2016) Light distribution and thermal effects in the rat brain under optogenetic stimulation. Journal of biophotonics 9:576-585.
Hakuno H, Oyamada Y, Murai M, Ito Y, Yamaguchi K (2004) Effects of inactivation and stimulation of locus coeruleus on respiratory activity of neonatal rat. Respiratory physiology & neurobiology 140:9-18.
Han X (2012) Optogenetics in the nonhuman primate. Progress in brain research 196:215-233. Hannon J, Hoyer D (2008) Molecular biology of 5-HT receptors. Behavioural brain research 195:198-213. Harris DP, Balasubramaniam A, Badr MS, Mateika JH (2006) Long-term facilitation of ventilation and
genioglossus muscle activity is evident in the presence of elevated levels of carbon dioxide in awake humans. American journal of physiology Regulatory, integrative and comparative physiology 291:R1111-1119.
Hawkins RD, Kandel ER, Siegalbaum SA (1993) Learning to modulate transmitter release: Themes and Variations in Synaptic Plasticity. Ann Rev Neurosci 16:625-665.
Haxhiu MA, Tolentino-Silva F, Pete G, Kc P, Mack SO (2001) Monoaminergic neurons, chemosensation and arousal. Respiration physiology 129:191-209.
Haxhiu MA, Yung K, Erokwu B, Cherniack NS (1996) CO2-induced c-fos expression in the CNS catecholaminergic neurons. Respiration physiology 105:35-45.
Hebb DO (1949) Organization of Behavior: A Neuropsychological Theory: Psychology Press. Hedner J, Hedner T, Jonason J, Lundberg D (1982) Evidence for a dopamine interaction with the central
respiratory control system in the rat. Eur J Pharmacol 81:603-615. Hickner S, Hussain N, Angoa-Perez M, Francescutti DM, Kuhn DM, Mateika JH (2014) Ventilatory long-
term facilitation is evident after initial and repeated exposure to intermittent hypoxia in mice genetically depleted of brain serotonin. J Appl Physiol 116:240-250.
Hilaire G (2006) Endogenous noradrenaline affects the maturation and function of the respiratory network: possible implication for SIDS. Autonomic neuroscience : basic & clinical 126-127:320-331.
Hilaire G, Viemari JC, Coulon P, Simonneau M, Bevengut M (2004) Modulation of the respiratory rhythm generator by the pontine noradrenergic A5 and A6 groups in rodents. Respiratory physiology & neurobiology 143:187-197.
Hirakawa H, Nakamura T, Hayashida Y (1997) Effect of carbon dioxide on autonomic cardiovascular responses to systemic hypoxia in conscious rats. The American journal of physiology 273:R747-754.
Hoffman MS, Nichols NL, Macfarlane PM, Mitchell GS (2012) Phrenic long-term facilitation after acute intermittent hypoxia requires spinal ERK activation but not TrkB synthesis. J Appl Physiol (1985) 113:1184-1193.
Holets VR, Hokfelt T, Rokaeus A, Terenius L, Goldstein M (1988) Locus coeruleus neurons in the rat containing neuropeptide y, tyrosine hydroxylase or galanin and their efferent projections to the spinal cord, cerebral cortex and hypothalamus. Neuroscience 24:893-906.
Holloway BB, Viar KE, Stornetta RL, Guyenet PG (2015) The retrotrapezoid nucleus stimulates breathing by releasing glutamate in adult conscious mice. The European journal of neuroscience 42:2271-2282.
Horner RL (1996) Motor Control of the Pharyngeal Musculature and Implications for the Pathogenesis of Obstructive Sleep Apnea. Sleep 19:827-853.
Horner RL (2008) Pathophysiology of obstructive sleep apnea. J Cardiopulm Rehabil Prev 28:289-298.

147
Horner RL, Liu X, Gill H, Nolan P, Liu H, Sood S (2002) Selected Contribution: Effects of sleep-wake state on genioglossus vs. diaphragm muscle responses to CO2 in rats. J Appl Physiol 92:878-887.
Hsiao C, Lahiri S, Mokashi A (1989) Peripheral and central dopamine receptors in respiratory control. Respiration physiology 76:327-336.
Huang YY, Kandel ER (1997) Recruitment of Long-lasting and Protein Kinase A-dependent Long-term Potentiation in the CA I Region of Hippocampus Requires Repeated Tetanization. Learning and Memory 1:74-82.
Hunanyan AS, Petrosyan HA, Alessi V, Arvanian VL (2013) Combination of chondroitinase ABC and AAV-NT3 promotes neural plasticity at descending spinal pathways after thoracic contusion in rats. Journal of neurophysiology 110:1782-1792.
Hung J, Whitford EG, Parsons RW, Hillman DR (1990) Association of sleep apnoea with myocardial infarction in men. The Lancet 336:261-264.
Huxtable AG, MacFarlane PM, Vinit S, Nichols NL, Dale EA, Mitchell GS (2014) Adrenergic a1-receptor activation is sufficient, but not necessary for phrenic long-term facilitation. J Appl Physiol 116:1345-1352.
Ip MSM, Lam B, Lauder IJ, Tsang KWT, Chung KF, Mok YW, Lam WK (2001) A Community Study of Sleep-Disordered Breathing in Middle-aged Chinese Men in Hong Kong. CHEST Journal 119:62-69.
Ip MSM, Lam B, Tang LCH, Lauder IJ, Ip TY, Lam WK (2004) A Community Study of Sleep- Disordered Breathing in Middle-Aged Chinese Women in Hong Kong. CHEST Journal 125:127-134.
Isackson PJ, Huntsman MM, Murray KD, Gall CM (1991) BDNF mRNA Expression Is Increased in Adult Rat Forebrain after Limbic Seizures: Temporal Patterns of Induction Distinct from NGF. Neuron 6:937-948.
Ishimatsu M, Williams JT (1996a) Synchronous Activity in Locus Coeruleus Results from Dendritic Interactions in Pericoerulear Regions. Neuroscience 16:5196-5204.
Ishimatsu M, Williams JT (1996b) Synchronous activity in locus coeruleus results from dendritic interactions in pericoerulear regions. The Journal of neuroscience : the official journal of the Society for Neuroscience 16:5196-5204.
Itami C, Kimura F, Kohno T, Matsuoka M, Ichikawa M, Tsumoto T, Nakamura S (2003) Brain-derived neurotrophic factor-dependent unmasking of "silent" synapses in the developing mouse barrel cortex. Proceedings of the National Academy of Sciences of the United States of America 100:13069-13074.
Janczewski WA, Feldman JL (2006) Distinct rhythm generators for inspiration and expiration in the juvenile rat. The Journal of physiology 570:407-420.
Janssen PL, Fregosi RF (2000) No evidence for long-term facilitation after episodic hypoxia in spontaneously breathing, anesthetized rats. J Appl Physiol (1985) 89:1345-1351.
Jedrzejewska-Szmek J, Luczak V, Abel T, Blackwell KT (2017) beta-adrenergic signaling broadly contributes to LTP induction. PLoS computational biology 13:e1005657.
Jiang C, Lipski J (1990) Extensive monosynaptic inhibition of ventral respiratory group neurons by augmenting neurons in the B6tzinger complex in the cat. Exp Brain Res 81:639-648.
Jiao XX, Gonzalez-Cabrera PJ, Xiao L, Bradley ME, Abel PW, Jeffries WB (2002) Tonic Inhibitory Role for cAMP in a1a-Adrenergic Receptor Coupling to Extracellular Signal-Regulated Kinases 1/2. The Journal of pharmacology and experimental therapeutics 303:247-256.
Johnson SM, Koshiya N, Smith JC (2001) Isolation of the Kernel for Respiratory Rhythm Generation in a Novel Preparation: The Pre-Bo¨tzinger Complex “Island”. Rapid Communication 1772-1776.
Jones LS, Gauger LL, Davis JN (1985) Anatomy of Brain Alpha1-Adrenergic Receptors: In Vitro Autoradiography With [125I]-Heat. The Journal of comparative neurology 231:190-208.
Joubert F, Loiseau C, Perrin-Terrin AS, Cayetanot F, Frugiere A, Voituron N, Bodineau L (2016) Key Brainstem Structures Activated during Hypoxic Exposure in One-day-old Mice Highlight

148
Characteristics for Modeling Breathing Network in Premature Infants. Frontiers in physiology 7:609.
Juric DM, Loncar D, Carman-Krzan M (2008) Noradrenergic stimulation of BDNF synthesis in astrocytes: mediation via alpha1- and beta1/beta2-adrenergic receptors. Neurochemistry international 52:297-306.
Kalia M, Sullivan JM (1982) Brainstem Projections of Sensory and Motor Components of the Vagus Nerve in the Rat. The Journal of comparative neurology 211:248-264.
Kaliszewska A, Bijata M, Kaczmarek L, Kossut M (2012) Experience-dependent plasticity of the barrel cortex in mice observed with 2-DG brain mapping and c-Fos: effects of MMP-9 KO. Cereb Cortex 22:2160-2170.
Karunakaran S, Chowdhury A, Donato F, Quairiaux C, Michel CM, Caroni P (2016) PV plasticity sustained through D1/5 dopamine signaling required for long-term memory consolidation. Nature neuroscience 19:454-464.
Katakura N, Chandler SH (1990) An iontophoretic analysis of the pharmacologic mechanisms responsible for trigeminal motorneuronal discharge during masticatory-like activity in the guinea pig. Journal of neurophysiology 63:356-369.
Kemp N, McQueen J, Faulkes S, Bashir ZI (2000) Different forms of LTD in the CA1 region of the hippocampus: role of age and stimulus protocol. The European journal of neuroscience 12:360-366.
Kempadoo KA, Mosharov EV, Choi SJ, Sulzer D, Kandel ER (2016) Dopamine release from the locus coeruleus to the dorsal hippocampus promotes spatial learning and memory. Proceedings of the National Academy of Sciences of the United States of America 113:14835-14840.
Kiehn O, Sillar KT, Kjaerulff O, McDearmid JR (1999) Effects of noradrenaline on locomotor rhythm-generating networks in the isolated neonatal rat spinal cord. The Journal of physiology 82:741-746.
Kinkead R, Bach KB, Johnson SM, Hodgeman BA, Mitchell GS (2001) Plasticity in respiratory motor control: intermittent hypoxia and hypercapnia activate opposing serotonergic and noradrenergic modulatory systems. Comparative biochemistry and physiology Part A, Molecular & integrative physiology 130:207-218.
Kline DD (2008) Plasticity in glutamatergic NTS neurotransmission. Respiratory physiology & neurobiology 164:105-111.
Kline DD, Mendelowitz D (2012) Intermittent Hypoxia Alters the Function of Cardiovascular Neurons and Reflex Pathways in the Brainstem. pp 71-83.
Kogan JH, Nestler EJ, Aghajanian GK (1992) Elevated basal firing rates and enhanced responses to 8-Br-cAMP in locus coeruleus neurons in brain slices from opiate-dependent rats. Eur J Pharmacol 211:47-53.
Koshiya N, Smith JC (1999) Neuronal pacemaker for breathing visualized in vitro. Nature 400:360-363. Kott JN, Westrum LE, Bhatia AM (1991) Is phaseotus vulgaris leucoagglutinin (PHA-L) a useful marker for
labeling neural grafts? Journal of Neural Transplatation and Plasticity 2:249-253. Lalley PM (2008) Opioidergic and dopaminergic modulation of respiration. Respiratory physiology &
neurobiology 164:160-167. Lam B, Ip MS, Tench E, Ryan CF (2005) Craniofacial profile in Asian and white subjects with obstructive
sleep apnoea. Thorax 60:504-510. Lee HK, Kameyama K, Huganir RL, Bear MF (1998) NMDA Induces Long-Term Synaptic Depression and
Dephosphorylation of the GluR1 Subunit of AMPA Receptors in Hippocampus. Neuron 21:1151-1162.
Legallois M (1813) Experiments on the principle of life. Philadelphia: Thomas.

149
Lendvai B, Stern EA, Chen B, Svoboda K (2000) Experience-dependent plasticity of dendritic spines in the developing rat barrel cortex in vivo. Nature 404:876-881.
Levitt P, Moore RY (1979) Origin and organization of brainstem catecholamine innervation in the rat. The Journal of comparative neurology 186:505-528.
Li A, Nattie E (2006) Catecholamine neurones in rats modulate sleep, breathing, central chemoreception and breathing variability. The Journal of physiology 570:385-396.
Li YM, Shen L, Peever JH, Duffin J (2003) Connections between respiratory neurones in the neonatal rat transverse medullary slice studied with cross-correlation. The Journal of physiology 549:327-332.
Lim DC, Veasey SC (2010) Neural injury in sleep apnea. Current neurology and neuroscience reports 10:47-52.
Ling L, Fuller DD, Bach KB, Kinkead R, Olson Jr. BE, Mitchell GS (2001) Chronic Intermittent Hypoxia Elicits Serotonin-Dependent Plasticity in the Central Neural Control of Breathing. Neuroscience 21:5381-5388.
Lomo T (1966) Frequency potentiation of excitatory synaptic activity in the dentate area of the hippocampal formation. Acta Physiol Scand 68:128.
Lopes LT, Patrone LG, Li KY, Imber AN, Graham CD, Gargaglioni LH, Putnam RW (2016) Anatomical and functional connections between the locus coeruleus and the nucleus tractus solitarius in neonatal rats. Neuroscience 324:446-468.
Lu J, Sherman D, Devor M, Saper CB (2006) A putative flip-flop switch for control of REM sleep. Nature 441:589-594.
Lui S, Torontali Z, Tadjalli A, Peever J (2018) Brainstem Nuclei Associated with Mediating Apnea-Induced Respiratory Motor Plasticity. Scientific reports 8.
Lujan HL, Palani G, DiCarlo SE (2010) Structural neuroplasticity following T5 spinal cord transection: increased cardiac sympathetic innervation density and SPN arborization. American journal of physiology Regulatory, integrative and comparative physiology 299:R985-R995.
Mahamed S, Strey KA, Mitchell GS, Baker-Herman TL (2011) Reduced respiratory neural activity elicits phrenic motor facilitation. Respiratory physiology & neurobiology 175:303-309.
Mahn M, Prigge M, Ron S, Levy R, Yizhar O (2016) Biophysical constraints of optogenetic inhibition at presynaptic terminals. Nature neuroscience 19:554-556.
Mair RD, Zhang Y, Bailey KR, Toupin MM, Mair RG (2005) Effects of clonidine in the locus coeruleus on prefrontal- and hippocampal-dependent measures of attention and memory in the rat. Psychopharmacology (Berl) 181:280-288.
McGuire M, Zhang Y, White DP, Ling L (2002) Effect of hypoxic episode number and severity on ventilatory long-term facilitation in awake rats. J Appl Physiol (1985) 93:2155-2161.
McGuire M, Zhang Y, White DP, Ling L (2004) Serotonin receptor subtypes required for ventilatory long-term facilitation and its enhancement after chronic intermittent hypoxia in awake rats. American journal of physiology Regulatory, integrative and comparative physiology 286:R334-341.
McGuire M, Zhang Y, White DP, Ling L (2005) Phrenic long-term facilitation requires NMDA receptors in the phrenic motonucleus in rats. The Journal of physiology 567:599-611.
Mellen N, Janczewski WA, Bocchiaro CM, Feldman JL (2003) Opioid-Induced Quantal Slowing Reveals Dual Networks for Respiratory Rhythm Generation. Neuron 37:821-826.
Mendez P, Bacci A (2011) Assortment of GABAergic plasticity in the cortical interneuron melting pot. Neural plasticity 2011:976856.
Merrill EG, Fedorko L (1984) Monosynaptic inhibition of phrenic motoneurons: a long descending projection from Botzinger neurons. Neuroscience 4:2350-2353.

150
Michaloudi HC, el Majdoubi M, Poulain DA, Papadopoulos GC, Theodosis DT (1997) The noradrenergic innervation of identified hypothalamic magnocellular somata and its contribution to lactation-induced synaptic plasticity. Journal of neuroendocrinology 9:17-23.
Mifflin SW (1992) Arterial chemoreceptor input to nucleus tractus solitarius. American journal of physiology Regulatory, integrative and comparative physiology 263:R368-375.
Millhorn DE (1986) Stimulation of raphe (obscurus) nucleus causes long-term potentation of phrenic nerve activity in cat. The Journal of physiology 381:169-179.
Millhorn DE, Eldridge FL, Waldrop TG (1980a) Prolonged stimulation of respiration by a new central neural mechanism. Respiration physiology 41:81-103.
Millhorn DE, Eldridge FL, Waldrop TG (1980b) Prolonged stimulation of respiration by endogenous central serotonin. Respiration physiology 42:171-188.
Minichiello L, Calella AM, Medina DL, Bonhoeffer T, Klein R, Korte M (2002) Mechanism of TrkB-mediated hippocampal long-term potentiation. Neuron 36:121-137.
Mohan R, Duffin J (1997) The effect of hypoxia on the ventilatory response to carbon dioxide in man. Respiration physiology 108:101-115.
Molkov YI, Rubin JE, Rybak IA, Smith JC (2017) Computational models of the neural control of breathing. Wiley interdisciplinary reviews Systems biology and medicine 9.
Moore RY (1979) Central catecholamine neuron systems: anatomy and physiology of the norepinephrine and epinephrine systems. Ann Rev Neurosci 2:113-168.
Moreira TS, Takakura AC, Damasceno RS, Falquetto B, Totola LT, Sobrinho CR, Ragioto DT, Zolezi FP (2011) Central chemoreceptors and neural mechanisms of cardiorespiratory control. Brazilian journal of medical and biological research = Revista brasileira de pesquisas medicas e biologicas / Sociedade Brasileira de Biofisica [et al] 44:883-889.
Morgan JI, Cohen DR, Hempstead JL, Curran T (1987) Mapping patterns of c-fos expression in the central nervous system after seizure. Science 237:192-198.
Morris BJ, Johnston HM (1995) A role for hippocampal opioids in long-term functional plasticity. TINS 18:350-355.
Morris KF, Shannon R, Lindsey BG (2001) Changes in cat medullary neurone firing rates and synchrony following induction of respiratory long-term facilitation. The Journal of physiology 532:483-497.
Mouradian RD, Sessler FM, Waterhouse BD (1991) Noradrenergic potentiation of excitatory transmitter action in cerebrocortical slices: evidence for mediation by an alpha 1 receptor-linked second messenger pathway. Brain research 546:83-95.
Muzerelle A, Scotto-Lomassese S, Bernard JF, Soiza-Reilly M, Gaspar P (2016) Conditional anterograde tracing reveals distinct targeting of individual serotonin cell groups (B5-B9) to the forebrain and brainstem. Brain structure & function 221:535-561.
Nakamura S, Sakaguchi T, Kimura F, Aoki F (1988) The role of alpha1-adrenoceptor-mediated collateral excitation in the regulation of the electrical activity of locus coeruleus neurons. Neuroscience 27:921-929.
Nakayama H, Smith CA, Rodman JR, Skatrud JB, Dempsey JA (2003) Carotid body denervation eliminates apnea in response to transient hypocapnia. J Appl Physiol (1985) 94:155-164.
Natarajan K, Berk BC (2006) Crosstalk Coregulation Mechanisms of G Protein-Coupled Receptors and Receptor Tyrosine Kinases. Methods in Molecular Biology 332:51-77.
Neverova NV, Saywell SA, Nashold LJ, Mitchell GS, Feldman JL (2007) Episodic stimulation of alpha1-adrenoreceptors induces protein kinase C-dependent persistent changes in motoneuronal excitability. The Journal of neuroscience : the official journal of the Society for Neuroscience 27:4435-4442.

151
Niebert M, Vogelgesang S, Koch UR, Bischoff AM, Kron M, Bock N, Manzke T (2011) Expression and function of serotonin 2A and 2B receptors in the mammalian respiratory network. PloS one 6:e21395.
Nieto FJ, Young TB, Lind BK, Shahar E, Samet JM, Redline S, D'Agostino RB, Lebowitz MD, Pickering TG (2000) Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study. JAMA : the journal of the American Medical Association 284:1829-1836.
Nitz D, Siegel J (1997) GABA release in the locus coeruleus as a function of sleep/wake state. Neuroscience 78:795-801.
Okazaki M, Takeda R, Yamazaki H, Haji A (2002) Synaptic mechanisms of inspiratory off-switching evoked by pontine pneumotaxic stimulation in cats. Neuroscience Research 44:101-110.
Olson EB, Jr., Bohne CJ, Dwinell MR, Podolsky A, Vidruk EH, Fuller DD, Powell FL, Mitchel GS (2001) Ventilatory long-term facilitation in unanesthetized rats. J Appl Physiol (1985) 91:709-716.
Onimaru H, Homma I (2003) A Novel Functional Neuron Group for Respiratory Rhythm Generation in the Ventral Medulla. Neuroscience 23:1478-1486.
Oyamada Y, Andrzejewski M, Muckenhoff K, Scheid P, Ballantyne D (1999) Locus coeruleus neurones in vitro: pH-sensitive oscillations of membrane potential in an electrically coupled network. Respiration physiology 118:131-147.
Panuchuk-Voloshina N, Haugland RP, Bishop-Stewart J, Bhalgat MK, Millard PJ, Mao F, Leung WY, Haugland RP (1999) Alexa Dyes, a Series of New Fluorescent Dyes that Yield Exceptionally Bright, Photostable Conjugates. Journal of Histochemistry and Cytochemistry 47:1179-1188.
Parkis MA, Bayliss DA, Berger AJ (1995) Actions of norepinephrine on rat hypoglossal motoneurons. Journal of neurophysiology 74:1911-1919.
Paxinos G, Watson C (1998) The rat brain: in stereotaxic coordinates. San Diego, California: Academic Press, Inc.
Peever JH, Shen L, Duffin J (2002) Respiratory pre-motor control of hypoglossal motorneurons in the rat. Neuroscience 110:711-722.
Peng YJ, Nanduri J, Raghuraman G, Souvannakitti D, Gadalla MM, Kumar GK, Snyder SH, Prabhakar NR (2010) H2S mediates O2 sensing in the carotid body. Proceedings of the National Academy of Sciences of the United States of America 107:10719-10724.
Pham J, Young A, Kuo YT, O’Driscoll DM (2018) Polysomnographic comparison between Chinese and Caucasian patients with obstructive sleep apnea. Sleep and Biological Rhythms 16:223-230.
Qian Z, Gu Y (2005) In vivo measurement of absorption coefficient (ua) in rat brain and statistic analysis. Chinese Optic Letters 3.
Rajkowski J, Majczynski H, Clayton E, AstonJones G (2004) Activation of monkey locus coeruleus neurons varies with difficulty and performance in a target detection task. Journal of neurophysiology 92:361-371.
Reig R, Mattia M, Compte A, Belmonte C, Sanchez-Vives MV (2010) Temperature modulation of slow and fast cortical rhythms. Journal of neurophysiology 103:1253-1261.
Ritucci NA, Dean JB, Putnam RW (1997) Intracellular pH response to hypercapnia in neurons from chemosensitive areas of the medulla. Rapid Communication R433-R441.
Roda F, Pio J, Bianchi AL, Gestreau C (2004) Effects of anesthetics on hypoglossal nerve discharge and c-Fos expression in brainstem hypoglossal premotor neurons. The Journal of comparative neurology 468:571-586.
Rukhadze I, Fenik VB, Benincasa KE, Price A, Kubin L (2010) Chronic intermittent hypoxia alters density of aminergic terminals and receptors in the hypoglossal motor nucleus. American journal of respiratory and critical care medicine 182:1321-1329.

152
Rukhadze I, Kubin L (2007) Differential pontomedullary catecholaminergic projections to hypoglossal motor nucleus and viscerosensory nucleus of the solitary tract. Journal of chemical neuroanatomy 33:23-33.
Rungta RL, Osmanski BF, Boido D, Tanter M, Charpak S (2017) Light controls cerebral blood flow in naive animals. Nature communications 8:14191.
Rutherford LC, Nelson SB, Turrigiano GG (1998) BDNF Has Opposite Effects on the Quantal Amplitude of Pyramidal Neuron and Interneuron Excitatory Synapses. Neuron 21:521-530.
Ryan S, Nolan P (2009) Episodic hypoxia induces long-term facilitation of upper airway muscle activity in spontaneously breathing anaesthetized rats. The Journal of physiology 587:3329-3342.
Saha S, Spary EJ, Maqbool A, Asipu A, Corbett EK, Batten TF (2004) Increased expression of AMPA receptor subunits in the nucleus of the solitary tract in the spontaneously hypertensive rat. Brain research Molecular brain research 121:37-49.
Sakai K, Touret M, Salvert D, Leger L, Jouvet M (1977) Afferent Projections to the Cat Locus Coeruleus as Visualized by the Horseradish Peroxidase Technique. Brain research 119:21-41.
Sakamoto H, Fukuda S, Minakawa Y, Sawamura S (2013) Clonidine induces sedation through acting on the perifornical area and the locus coeruleus in rats. J Neurosurg Anesthesiol 25:399-407.
Sanders M, Moore S (1983) Inspiratory and expiratory partitioning of airway resistance during sleep in patients with sleep apnea. Am Rev Respir Dis 127:554-558.
Sanders M, Rogers R, Pennock B (1985) Prolonged expiratory phase in sleep apnea. A unifying hypothesis. Am Rev Respir Dis 131:401-408.
Satriotomo I, Dale EA, Dahlberg JM, Mitchell GS (2012) Repetitive acute intermittent hypoxia increases expression of proteins associated with plasticity in the phrenic motor nucleus. Experimental neurology 237:103-115.
Sauerland EK, Mitchell SP (1970) Electromyographic activity of the human genioglossus muscle in response to respiration and to positional changes of the head. Bulletin of the Los Angeles neurological societies 2:69-73.
Sawczuk A, Mosier KM (2001) Neural control of tongue movement with respect to respiration and swallowing. Crit Rev Oral Biol Med 12:18-37.
Scharf MT, Woo NH, Lattal M, Young JZ, Nguyen PV, Abel T (2002) Protein synthesis is required for the enhancement of long-term potentation and long-term memory by spaced training. Journal of neurophysiology 87:2770-2777.
Schaser AJ, Stang K, Connor NP, Behan M (2012) The effect of age and tongue exercise on BDNF and TrkB in the hypoglossal nucleus of rats. Behavioural brain research 226:235-241.
Schjetnan AG, Escobar ML (2012) In vivo BDNF modulation of hippocampal mossy fiber plasticity induced by high frequency stimulation. Hippocampus 22:1-8.
Schwartz AR, Barnes M, Hillman D, Malhotra A, Kezirian E, Smith PL, Hoegh T, Parrish D, Eastwood PR (2012) Acute upper airway responses to hypoglossal nerve stimulation during sleep in obstructive sleep apnea. American journal of respiratory and critical care medicine 185:420-426.
Schwarz LA, Miyamichi K, Gao XJ, Beier KT, Weissbourd B, DeLoach KE, Ren J, Ibanes S, Malenka RC, Kremer EJ, Luo L (2015) Viral-genetic tracing of the input-output organization of a central noradrenaline circuit. Nature 524:88-92.
Schwarz PB, Mir S, Peever JH (2014) Noradrenergic modulation of masseter muscle activity during natural rapid eye movement sleep requires glutamatergic signalling at the trigeminal motor nucleus. The Journal of physiology 592:3597-3609.
Seager MA, Huff KD, Barth VN, Phebus LA, Rasmussen K (2004) Fluoxetine administration potentiates the effect of olanzapine on locus coeruleus neuronal activity. Biological psychiatry 55:1103-1109.
Segal M (2005) Dendritic spines and long-term plasticity. Nature reviews Neuroscience 6:277-284.

153
Sessle BJ, Henry JL (1985) Effects of Enkephalin and 5-Hydroxytryptamine on Solitary Tract Neurones Involved in Respiration and Respiratory Reflexes. Brain research 327:221-230.
Shahar E, Whitney CW, Redline S, Lee ET, Newman AB, Nieto FJ, O'connor GT, Boland LL, Schwarz JE, Samet JM (2001) Sleep-disordered breathing and cardiovascular disease. American journal of respiratory and critical care medicine 163:19-25.
Sharifullina E, Ostroumov K, Nistri A (2004) Activation of group I metabotropic glutamate receptors enhances efficacy of glutamatergic inputs to neonatal rat hypoglossal motoneurons in vitro. The European journal of neuroscience 20:1245-1254.
Shatz CJ (1992) The Developin Brain. Scientific American 267:60-67. Shen L, Duffin J (2002) Caudal expiratory neurones in the rat. Pflugers Archiv : European journal of
physiology 444:405-410. Shirey MJ, Smith JB, Kudlik DE, Huo BX, Greene SE, Drew PJ (2015) Brief anesthesia, but not voluntary
locomotion, significantly alters cortical temperature. Journal of neurophysiology 114:309-322. Shkoukani M, Babcock MA, Badr MS (2002) Effect of episodic hypoxia on upper airway mechanics in
humans during NREM sleep. J Appl Physiol (1985) 92:2565-2570. Siwek DF, Knapp CM, Kaur G, Datta S (2014) Dorsal subcoeruleus nucleus (SubCD) involvement in
context-associated fear memory consolidation. Exp Brain Res 232:1535-1545. Smith CC, Greene RW (2012) CNS dopamine transmission mediated by noradrenergic innervation. The
Journal of neuroscience : the official journal of the Society for Neuroscience 32:6072-6080. Smith JC, Abdala AP, Koizumi H, Rybak IA, Paton JF (2007) Spatial and functional architecture of the
mammalian brain stem respiratory network: a hierarchy of three oscillatory mechanisms. Journal of neurophysiology 98:3370-3387.
Song G, Poon CS (2017) α2-adrenergic blockade rescues hypoglossal motor defense against obstructive sleep apnea. JCI insight 2:1-16.
Sood S, Morrison JL, Liu H, Horner RL (2005) Role of endogenous serotonin in modulating genioglossus muscle activity in awake and sleeping rats. American journal of respiratory and critical care medicine 172:1338-1347.
Stanton PK, Sarvey JM (1985) Depletion of Norepinephrine, But Not Serotonin, Reduces Long-term Potentiation in the Dentate Gyrus of Rat Hippocampal Slices. Neuroscience 5:2169-2176.
Steenland HW, Liu H, Sood S, Liu X, Horner RL (2006) Respiratory activation of the genioglossus muscle involves both non-NMDA and NMDA glutamate receptors at the hypoglossal motor nucleus in vivo. Neuroscience 138:1407-1424.
Stettner GM, Fenik VB, Kubin L (2012) Effect of chronic intermittent hypoxia on noradrenergic activation of hypoglossal motoneurons. J Appl Physiol (1985) 112:305-312.
Strittmatter SM, Vartanian T, Fishman MC (1992) GAP-43 as a Plasticity Protein in Neuronal Form and Repair. Journal of neurobiology 23:507-520.
Stujenske JM, Spellman T, Gordon JA (2015) Modeling the Spatiotemporal Dynamics of Light and Heat Propagation for In Vivo Optogenetics. Cell reports 12:525-534.
Surprenant A, North RA (1988) Mechanism of synaptic inhibition by noradrenaline acting at a2-adrenoceptors. Proc R Soc Lond B 234.
Sved AF, Felsten G (1987) Stimulation of the locus coeruleus decreases arterial pressure. Brain research 414:119-132.
Syed Z, Lin HS, Mateika JH (2013) The impact of arousal state, sex, and sleep apnea on the magnitude of progressive augmentation and ventilatory long-term facilitation. J Appl Physiol (1985) 114:52-65.
Szabo ST, de Montigny C, Blier P (2000) Progressive attenuation of the firing activity of locus coeruleus noradrenergic neurons by sustained administration of selective serotonin reuptake inhibitors. Int J Neuropsychopharmacol 3:1-11.

154
Szymusiak R, McGinty D (2008) Hypothalamic regulation of sleep and arousal. Annals of the New York Academy of Sciences 1129:275-286.
Tadjalli A (2012) Plasticity of Vagal Origin: Identification and characterization of a novel form of neural plasticity in respiratory motor control. In: Cell and Systems Biology, vol. PhD, pp 1-242: University of Toronto.
Tadjalli A, Duffin J, Peever J (2010) Identification of a novel form of noradrenergic-dependent respiratory motor plasticity triggered by vagal feedback. The Journal of neuroscience : the official journal of the Society for Neuroscience 30:16886-16895.
Takakura AC, Moreira TS, Colombari E, West GH, Stornetta RL, Guyenet PG (2006) Peripheral chemoreceptor inputs to retrotrapezoid nucleus (RTN) CO2-sensitive neurons in rats. The Journal of physiology 572:503-523.
Talley EM, Lei Q, Sirois JE, Bayliss DA (2000) TASK-1, a two-pore domain K+ channel, is modulated by multiple neurotransmitters in motoneurons. Neuron 25:399-410.
Tan W, Janczewski WA, Yang P, Shao XM, Callaway EM, Feldman JL (2008) Silencing preBotzinger complex somatostatin-expressing neurons induces persistent apnea in awake rat. Nature neuroscience 11:538-540.
Tang F, Lane S, Korsak A, Paton JF, Gourine AV, Kasparov S, Teschemacher AG (2014) Lactate-mediated glia-neuronal signalling in the mammalian brain. Nature communications 5:3284.
Tangel DJ, Mezzanotte WS, White DP (1995) Respiratory-related control of palatoglossus and levator palatini muscle activity. J Appl Physiol (1985) 78:680-688.
Taranto-Montemurro L, Edwards BA, Sands SA, Marques M, Eckert DJ, White DP, Wellman A (2016) Desipramine Increases Genioglossus Activity and Reduces Upper Airway Collapsibility during Non-REM Sleep in Healthy Subjects. American journal of respiratory and critical care medicine 194:878-885.
Teppema LJ, Veening JG, Kranenburg A, Dahan A, Berkenbosch A, Olievier C (1997) Expression of c-fos in the rat brainstem after exposure to hypoxia and to normoxic and hyperoxic hypercapnia. The Journal of comparative neurology 388:169-190.
Terada J, Nakamura A, Zhang W, Yanagisawa M, Kuriyama T, Fukuda Y, Kuwaki T (2008) Ventilatory long-term facilitation in mice can be observed during both sleep and wake periods and depends on orexin. J Appl Physiol (1985) 104:499-507.
Torontali Z (2012) The Nucleus of the Solitary Tract is Necessary for Apnea-Induced Respiratory Plasticity. In: Cell and Systems Biology, vol. M.Sc, pp 1-89: University of Toronto.
Travagli RA, Dunwiddie T, Williams JT (1995) Opioid inhibition in locus coeruleus. Journal of neurophysiology 74:518-528.
Trudeau LE (2004) Glutamate co-transmission as an emerging concept in monoamine neuron function. Journal of psychiatry & neuroscience : JPN 29:296-310.
Tsuda K, Yokoo H, Goldstein M (1989) Neuropeptide Y and Galanin in Norepinephrine Release in Hypothalamic Slices. Hypertension 14:81-86.
Turner DL, Mitchell GS (1997) Long-term facilitation of ventilation following repeated hypoxic episodes in awake goats. The Journal of physiology 499.2:543-550.
Tye KM, Deisseroth K (2012) Optogenetic investigation of neural circuits underlying brain disease in animal models. Nature reviews Neuroscience 13:251-266.
Valente P, Casagrande S, Nieus T, Verstegen AM, Valtorta F, Benfenati F, Baldelli P (2012) Site-specific synapsin I phosphorylation participates in the expression of post-tetanic potentiation and its enhancement by BDNF. The Journal of neuroscience : the official journal of the Society for Neuroscience 32:5868-5879.
Valic M, Pecotic R, Pavlinac I, Valic Z, Peros K, Dogas Z (2010) Microinjection of methysergide into the raphe nucleus attenuated phrenic long-term facilitation in rats. Exp Brain Res 202:583-589.

155
van Bockstaele EJ, Peoples J, Telegan P (1999) Efferent Projections of the Nucleus of the Solitary Tract to Peri-Locus Coeruleus Dendrites in Rat Brain: Evidence for a Monosynaptic Pathway. The Journal of comparative neurology 412:410-428.
Van Bockstaele EJ, Saunders A, Commons KG, Liu XB, Peoples J (2000) Evidence for coexistence of enkephalin and glutamate in axon terminals and cellular sites for functional interactions of their receptors in the rat locus coeruleus. The Journal of comparative neurology 417:103-114.
Vankov A, Herve-Minivielle A, Sara SJ (1995) Response to novelty and its rapid habituation in locus coeruleus neurons of the freely exploring rat. The European journal of neuroscience 7:1180-1187.
Vazey EM, Aston-Jones G (2014) Designer receptor manipulations reveal a role of the locus coeruleus noradrenergic system in isoflurane general anesthesia. Proceedings of the National Academy of Sciences of the United States of America 111:3859-3864.
Viemari JC, Bevengut M, Burnet H, Coulon P, Pequignot JM, Tiveron MC, Hilaire G (2004a) Phox2a gene, A6 neurons, and noradrenaline are essential for development of normal respiratory rhythm in mice. The Journal of neuroscience : the official journal of the Society for Neuroscience 24:928-937.
Viemari JC, Bevengut M, Coulon P, Hilaire G (2004b) Nasal Trigeminal Inputs Release the A5 Inhibition Received by the Respiratory Rhythm Generator of the Mouse Neonate. Journal of neurophysiology 91:746-758.
Volgin DV, Fay R, Kubin L (2003) Postnatal development of serotonin 1B, 2A and 2C receptors in brainstem motoneurons. The European journal of neuroscience 17:1179-1188.
Volgin DV, Mackiewicz M, Kubin L (2001) a1B receptors are the main postsynaptic mediators of adrenergic excitation in brainstem motoneurons, a single-cell RT-PCR study. Journal of chemical neuroanatomy 22:157-166.
Wagner PG, Eldridge FL (1990) Development of short-term potentiation of respiration. Respiration physiology 82:129-140.
Wang JQ, Arora A, Yang L, Parelkar NK, Zhang G, Liu X, Choe ES, Mao L (2005) Phosphorylation of AMPA Receptors. Molecular Neurobiology 32:237-249.
Wang X, Pinol RA, Byrne P, Mendelowitz D (2014) Optogenetic stimulation of locus ceruleus neurons augments inhibitory transmission to parasympathetic cardiac vagal neurons via activation of brainstem alpha1 and beta1 receptors. The Journal of neuroscience : the official journal of the Society for Neuroscience 34:6182-6189.
Watanabe S, Hoffman DA, Migliore M, Johnston D (2002) Dendritic K+ channels contribute to spike-timing dependent long-term potentiation in hippocampal pyramidal neurons. Proceedings of the National Academy of Sciences of the United States of America 99:8366-8371.
Weinshenker D, Holmes PV (2016) Regulation of neurological and neuropsychiatric phenotypes by locus coeruleus-derived galanin. Brain research 1641:320-337.
Wetmore C, Olson L, Bean AJ (1994) Regulation of Brain-derived Neurotrophic Factor (BDNF) Expression and Release from Hippocampal Neurons Is Mediated by Non-NMDA Type Glutamate Receptors. Neuroscience 14:1688-1700.
Widdicombe J (2001) Airway receptors. Respiration physiology 125:3-15. Wilkerson JE, Mitchell GS (2009) Daily intermittent hypoxia augments spinal BDNF levels, ERK
phosphorylation and respiratory long-term facilitation. Experimental neurology 217:116-123. Wirth KJ, Steinmeyer K, Ruetten H (2013) Sensitization of upper airway mechanoreceptors as a new
pharmacologic principle to treat obstructive sleep apnea: investigations with AVE0118 in anesthetized pigs. Sleep 36:699-708.
Xu ZQ, Zheng K, Hokfelt T (2005) Electrophysiological studies on galanin effects in brain--progress during the last six years. Neuropeptides 39:269-275.

156
Yamamoto K, Lalley P, Mifflin S (2015) Acute intermittent optogenetic stimulation of nucleus tractus solitarius neurons induces sympathetic long-term facilitation. American journal of physiology Regulatory, integrative and comparative physiology 308:R266-275.
Yizhar O, Fenno LE, Davidson TJ, Mogri M, Deisseroth K (2011) Optogenetics in neural systems. Neuron 71:9-34.
Yokhana SS, Gerst DG, 3rd, Lee DS, Badr MS, Qureshi T, Mateika JH (2012) Impact of repeated daily exposure to intermittent hypoxia and mild sustained hypercapnia on apnea severity. J Appl Physiol (1985) 112:367-377.
Yoshii A, Constantine-Paton M (2010) Postsynaptic BDNF-TrkB signaling in synapse maturation, plasticity, and disease. Developmental neurobiology 70:304-322.
Younes M, Loewen A, Ostrowski M, Hanly P (2014) Short-term potentiation in the control of pharyngeal muscles in obstructive apnea patients. Sleep 37:1833-1849.
Young T, Palta M, Dempsey JA, Skatrud JB, Weber S, Badr MS (1993) The occurence of sleep-disordered breathing among middle-aged adults. The New England Journal of Medicine 328:1230-1235.
Young T, Peppard PE, Gottlieb DJ (2002) Epidemiology of Obstructive Sleep Apnea. American journal of respiratory and critical care medicine 165:1217-1239.
Zafra F, Castren E, Thoenen H, Lindholm D (1991) Interplay between glutamate and y-aminobutyric acid transmitter systems in the physiological regulation of brain-derived neurotrophic factor and nerve growth factor synthesis in hippocampal neurons. Proceedings of the National Academy of Sciences of the United States of America 88:10037-10041.
Zanella S, Roux JC, Viemari JC, Hilaire G (2006) Possible modulation of the mouse respiratory rhythm generator by A1/C1 neurones. Respiratory physiology & neurobiology 153:126-138.
Zhang W, Mifflin SW (2007) Modulation of synaptic transmission to second-order peripheral chemoreceptor neurons in caudal nucleus tractus solitarius by alpha1-adrenoreceptors. The Journal of pharmacology and experimental therapeutics 320:670-677.
Zhang Y, McGuire M, White DP, Ling L (2003) Episodic phrenic-inhibitory vagus nerve stimulation paradoxically induces phrenic long-term facilitation in rats. The Journal of physiology 551:981-991.
Zhao Y, Fang Q, Straub SG, Sharp GW (2008) Both G i and G o heterotrimeric G proteins are required to exert the full effect of norepinephrine on the beta-cell K ATP channel. The Journal of biological chemistry 283:5306-5316.
Zhong H, Minneman KP (1999) a1-Adrenoceptor subtypes. European Journal of Pharmacology 375:261-276.
Zhu Y, Fenik P, Zhan G, Mazza E, Kelz M, Aston-Jones G, Veasey SC (2007) Selective loss of catecholaminergic wake active neurons in a murine sleep apnea model. The Journal of neuroscience : the official journal of the Society for Neuroscience 27:10060-10071.