Neural Bases of Childhoos Speech Disorders.pdf
20
8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 1/20
-
Upload
patricia-amillos -
Category
Documents
-
view
228 -
download
0
Transcript of Neural Bases of Childhoos Speech Disorders.pdf

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 1/20

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 2/20

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 3/20
F.J. Liégeois, A.T. Morgan / Neuroscience andBiobehavioral Reviews 36 (2012) 439–458 441
sound production, that is, across the domains of articulation,
resonance, vocal quality, prosody and respiration. For instance,dysarthric speech may sound imprecise or ‘slurred’ due to afailure of execution of the lips or tongue, or severely distortedas regards nasal resonance due to velopharyngeal dysfunction.
Various sub-types of dysarthria have been reported to occur in iso-lation or combination depending on the neuroanatomical lesionsite, as early as 1943 (Froeschels, see Duffy and Kent, 2001,for a historical perspective and Duffy, 2005, for an update on
the widely used Mayo classification by Darley et al., 1969). Incontrast, apraxia of speech is a disorder of planning and program-ming , where execution of individual speech sounds is reportedlymostly preserved but coarticulation and sequencing may be
impaired.
1.2.1. Neural correlates of dysarthriaAlthough “not a rare disorder . . . in paediatric neurology” (Van
Mourik et al., 1997b, p. 299), dysarthria in conjunction with neu-roimaging has mainly been reported in the adult population.Consistent with recent functional imaging studies during overtspeech (see Price, 2010, f or a recent review), unilateral damage to
the pyramidal or extrapyramidal system and associated pathways
is sufficientto resultin dysarthria in adults(see reviewin Kent et al.,2001). A recent report (Urban et al., 2006) indicated that extracere-bellarinfarcts to the left hemisphere (irrespective of location) were
notonlymore likelyto resultin dysarthria,but also resulted in moresevere dysarthria than right hemisphere infarctions, especially forarticulation and prosody, in the acute stage (within 72h). Alto-gether, the findings therefore suggesta left hemisphere dominance
for articulatory functions in the mature brain.
1.2.2. Neural correlates of apraxia of speechApraxia of speech is the main symptom noted in adults with
Broca’s aphasia, resulting from infarcts to the left hemisphere and
involving the inferior frontal region, including the posterior part of
Broca’s area (Hilliset al., 2004; Jordanand Hillis, 2006) andthe insu-lar cortex (Dronkers, 1996; Nagao et al., 1999) or adjacent whitematter( Jaffe et al., 2003; seereviews Ackermannand Riecker, 2010;
Ogar et al., 2005). It is also a feature of neurological degenerativediseases (e.g., Josephs et al., 2006), such as corticobasal degenera-tion ( Josephs and Duffy, 2008), where pathology is bilateral. Sincethere is little evidence to suggest that right hemisphere damage
alone is sufficientto resultin apraxia of speech, theliterature there-fore suggests that the planning/programming of speech may alsobe predominantly subserved by left hemisphere networks in themature brain.
Given that conditions such as infarcts and neurodegenera-tive diseases are rare in childhood, motor speech outcomes inchildren and adults with similar aetiologies have not been com-
pared. Despite recent advances in neuroimaging data acquisitionand analysis techniques that allow the detection of functional(e.g., functional MRI, PET) and subtle structural (e.g., voxel-brainmorphometry or VBM, Ashburner and Friston, 2000) brain abnor-malities, no neuroanatomical model of paediatric motor speech
disorders is available. As a result, the question of a left hemisphericdominance for motor speech functions throughout developmentremains unanswered, and the potential for post-lesional functionalreorganization remains difficult to predict in childhood.
In order to address these questions, theaim of thepresent articlewas to systematically review and describe recent evidence report-ing on a link between motor speech disorders (apraxia of speechand dysarthria) and brain abnormalities in children and adoles-
cents (16 years or younger) with developmental, progressive, orchildhood-acquired neurological conditions.
2. Methods
2.1. Search strategy
Articles were searched using the OvidSP interface, which pro-
vides access to the following biomedical and health relateddatabases: AMED; Biotechnology Abstracts; EMBASE; Health andPsychosocial Instruments; HMIC; Maternity and Infant Care; MED-LINE; PsycEXTRA; PsycINFO; PsycCRITIQUES; Social Policy and
Practice.For inclusion purposes, children and adolescents were defined
asaged 16 orunder,although adult cases were included ifpathologyonset was at or before the age of 16. The term brain abnormality
was used here in the broad sense, encompassing overt damage,dysfunction, or morphological abnormality (i.e., detectable usingquantitative MRI analysis methods) to grey or white matter struc-tures. We examined articles published after a seminal review on
acquired childhood dysarthria by Van Mourik et al. (1997b), that is,between January 1997 and January 2010.
2.2. Step 1: search criteria and abstract extraction
Thirty-six search terms were used for neuropathology (includ-ing developmental, progressive and acquired disorders, seeAppendix 1 f or complete list), three search term to encompass
the paediatric population (see Appendix 2), and six search termsdescribing motorspeech disorders (dysarthriaand CAS with all syn-onyms, see Appendix 3). Abstracts fulfilling selection criteria (i.e.,abstracts available, English language, published between January
1997 and January 2010) that included one or more terms fromAppendix 1 AND one or more terms from Appendix 2 AND oneor more terms from Appendix 3, were retrieved.
2.3. Step 2: abstract selection
The 3730 abstracts generated from Step 1 were reviewed inde-pendently by both authors to exclude those that (i) were not data
driven, (ii) did not mention motor speech disorders (see Appendix3 f or included terms),or (iii)included adult-onset conditions.Therewas disagreement on 4% (154), solved by mutual agreement. Themain reasonfor exclusionwas that terms such as “speechdisorder”
or “speech delay” were used generically to refer to impairmentsof language comprehension or production, rather than of motorspeech. Where views were not in accordance, and the content of the abstract did not provideenough information to make an agreed
upon decision,the authors erred on the sideof caution andselectedthe abstract forfurther examination in Step 3 (106abstracts, 2.8%of total). Of the 3730 titles and abstracts identified via the computer-generated search strategy, 260 potentiallyeligible full articles were
retrieved.
2.4. Step 3: article selection
The 260 retrieved articles were reviewed independently by theauthors to exclude thosewithout neuroimaging evidence or explicitmention of a motor speech disorder diagnosis in the full text.Reviews not containing original data were also identified at this
stage and were excluded. All articles containing routine clinical ormore sophisticated CT and MRI scan reports were included, evenwhere only brief mention of neurological status was made such as‘CTreports were normal’. Disagreementswere discussedin onefur-
ther round of review where consensus was reached. Seventy-twoarticles were selected for the present review.

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 4/20
442 F.J. Liégeois, A.T. Morgan / Neuroscience and Biobehavioral Reviews 36 (2012) 439–458
Fig. 2. Proportion of cases with childhood apraxia of speech (A)and childhooddysarthria (B)falling into each neurological condition listed in thepresent review.
3. Results
Only 12 reports of CAS were accompanied by neuroimaginginvestigations. CAS was either associated with epilepsy disor-ders (five reports), metabolic disorders (two reports), syndromicconditions (two reports), idiopathic forms arising from FOXP2 dis-
ruption (tworeports), orwas of unknown origin(one report). Whenexamining the number of cases (Fig. 2A), epilepsy and metabolicdisorders accounted for about 70% of cases (31 individuals) alto-gether.
Neuroimaging correlates of dysarthria were reported in chil-dren with known clinical syndromic entities (16 reports), tumours(mainly of the posterior fossa, ten reports), infarcts (six reports),metabolic disorders (eight reports), traumatic brain injury (seven
reports), degenerative diseases (four reports), epilepsy disorders
(three reports), and other conditions not falling into the abovementioned categories (“miscellaneous”, six reports). The highestproportion of cases with dysarthria (Fig.2B) experienced metabolic
disorders, accounting for about one quarter (74 individuals) of allcases.
4. Discussion
Within the past 13 years, seventy-two articles have reportedon motor speech disorder in the paediatric population togetherwith neuroimaging data. Dysarthria and CAS were reported fornumerous categories of neurological conditions (ten including our
“miscellaneous” category). The human motor speech systemthere-fore appears vulnerable to a wide range of neurological events
arising in the pre- and post-natal period, although motor speechdisorders were rarely the only symptoms for the cases listed in the
present review (i.e., frequent co-morbidities included motor andlanguage impairments). The main findings will be summarized anddiscussed below for each condition.
4.1. Neural bases of childhood apraxia of speech
It is perplexing that withinthe past 13 years,onlytwelvearticles
(reporting on 45 cases, see Table 1) have reported neural findingsassociated with CAS. Around 60% (27 cases)had MRI scans reportedto be radiologically normal. These negative MRI findings suggestthat brain abnormalities may be present at the sub-macroscopic
level, compromising for instance white matter integrity or grey
matter density. They could also indicate that CAS is associated with
brain functional anomalies at the metabolic or neurotransmitter
level.Such evidence for subtle abnormalities in CAS differs strikingly
from the adult cases where apraxia of speech is overwhelminglyreported as being associated with frank lesions to the left hemi-sphere, mainly due to infarcts (see Section 1). This aetiological
difference highlights the fact that neither CAS associated withneural abnormality nor the developmental idiopathic form of thedisorder may be comparable to its adult-acquired counterpart (assuggested by Maassen, 2002).
4.1.1. Genetic disorders (idiopathic form)The scarcity of studies examining the neural basis of CAS is par-
ticularly surprising with regard to the idiopathic form given that,
since the discovery of the FOXP2 gene in 2001 (the only knowngene associated with CAS), a considerable amount of studies haveinvestigated the possible genetic basis for the disorder (Fisher andScharff, 2009;MacDermot et al., 2005;Vernes et al., 2009). In addi-tion, the clinical diagnostic markers of CAS have been extensively
researched during this time period (Shriberg et al., 1997a,b,c).Neuroimaging investigations in the affected members of a
British family (“KE” family), who have a FOXP2 gene mutation(Belton et al., 2003), and other studies on the same individuals not
included in the present review (Watkins et al., 2002; see Vargha-Khadem et al., 2005, for a review) have revealed bilateral greymattermorphological abnormalities in the perisylvian and rolandiccortices, basal ganglia and cerebellum (Fig. 3; see Liégeois et al.,
2003 f or functionalabnormalitiesin overlapping regions). It is note-
worthythat these structuralabnormalities in the affected membersof the KE family were detected with a more sensitive quantitativeimaging analysis technique (voxel-based morphometry, or VBM),
while the routine clinical MRI scans appeared radiologically nor-mal. Normal structural MRI was also reported for the other casewith a genetic abnormality identified in the present review, whosedeletion encompasses FOXP2 (single case study, Lennon et al.,
2007), but no quantitative imaging analysis technique was used. Inthecase of genetic disruption, therarity ofCAS (1–2/1000 accordingto Shriberg et al., 1997a; 3–4% in Delaney and Kent, 2004) makesit difficult to identify large families or homogeneous samples with
the disorder. This is a major hurdle when quantitative MRI meth-ods must be used,as these methods require large samples to detectsubtle differences between the brains of affected and unaffected
individuals.

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 5/20

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 6/20
444 F.J. Liégeois, A.T. Morgan / Neuroscience and Biobehavioral Reviews 36 (2012) 439–458
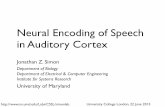
Fig. 3. Schematic illustration of lesions or morphological abnormalities associated with childhood apraxia of speech. Red, bilateral reduced grey matter in cases withFOXP2
gene mutation(VBM analyses, fromBelton et al.,2003). Blue, epilepsydisorders (rolandicepilepsy in Probands1 and2, Roll etal.,2006). Yellow,thin corpus callosumreported
in one case with unknown aetiology(Le Normand et al., 2000) and in onecasewith creatine transporter deficit(Battini et al., 2007). Green,cerebellaratrophyin 7 cases with
galactosemia (Hughes et al., 2009). Other neuroimaging results from the latter article are not illustrated since abnormalities were reported throughout the cerebral whitematter. See Table 1 f or details. (For interpretation of thereferences to color in this figure legend, the readeris referred to theweb version of the article.)
4.1.2. Epilepsy disordersIn children suffering from CAS associated with epilepsy,
including the rolandic form, MRIs were reported normal for
most cases (12/18 cases). In the remainder, bilateral perisylvianhypometabolism or polymicrogyria (Fig. 3) was reported. These
scarce findings suggest that bilateral disruption of the speech plan-ning/programming cortices (possibly the premotor and Broca’s
regions, see Fig. 1) may be at the root of epilepsy-related CAS.This disruption is however difficult to detect using routine clinicalinvestigations as it may involve dysfunction arising from epilep-tic activity, which is not necessarily associated with underlying
structural abnormality. Overall, again only limited neuroimagingevidence is currently available for this sub-group of children withCAS.
4.1.3. Metabolic disorders
A total of 13 individuals with CAS associated with metabolicdisorders were included in the present review, with 12 hav-ing classical galactosaemia. Neuroimaging revealed white matter
anomalies (including delayed or absent myelination) and cerebel-lar atrophy, suggesting that developmental disruption of the whitematter structures may be at the root ofCAS inthose cases. Becauseabnormalities were reported in the corpus callosum, periventric-ular region, as well as in the deep white matter, it is difficult to
establish a causal link between damage to a particular white mat-ter tract and speech symptoms. Furthermore, only a proportion(up to 50%—Nelson et al., 1991) of cases diagnosed with clas-sic galactosaemia present with a diagnosis of “verbal dyspraxia”.
Future studies directly comparing children with and without CASare therefore needed to improve our understanding of the vari-ability in speech outcome for those children. In conclusion, furtherresearch is needed to understand theneural basis of CASin children
with metabolic disorders. Despite the rarity of metabolic disorders
(about 1 per 60,000 births for classic galactosaemia), those studiesmay shed light on brain structures that arecrucial to normalspeechplanning during development.
4.1.4. Syndromes of unknown originThree single-case studiesreported CAS in Floating Harbour syn-
drome, Klinefeler syndrome, and of unknown origin, respectively.MRIs were reported normal in the first two cases, whereas incom-
plete myelination was reported for the third case. The sparseevidence in those cases makes it difficult to establisha link betweenneural disorder and CAS symptoms. As concluded in the cases of metabolic disorders, further neuroimaging data will be necessary
to understand the neural mechanisms that explain the phenotypic
speech variability within each syndromic entity reported here.
4.1.5. InfarctsThe lack of studies reporting on CAS in childhood stroke is note-
worthy given the well-documented association between Broca’s
aphasia and apraxia of speech in adults. Although childhood strokeis rare (2–3 per 100,000 persons-year, Beslow and Jordan, 2010),
the condition has long been recognized, and numerous outcomestudies are now available for language skills (e.g., Raja Beharelle
et al., 2010). Motor speech outcome has not been reported in thosestudies, making it difficult to compare childhood and adult cases,and to assess the consequences of left vs. right hemisphere infarcts.The question of hemispheric specialization for the planning and
programming of speech will be discussed further below.The study of motor speech outcome in children who have expe-
rienced a unilateral hemispheric neurological event should helpclarify whether the adult left hemispheric dominance for speech
planning is also present in childhood. If so, such studies shouldalso help elucidate whether the right hemisphere can compen-sate for these functions after left hemisphere insult. Unfortunately,such evidence is not available, and the fact that within the last
13 years no report of CAS and left hemisphere infarct or tumourhas been reported remains surprising. Our current interpretationis that the intact left and right hemispheres can alone compen-sate for speech planning/programming functions, so that even if
CAS is observed, it is only transient. This interpretation wouldbe consistent with the fact that young people who underwentleft or right hemispherectomy (that is, who have only one func-tioning hemisphere) in childhood do not present with CAS long
term (Liégeois et al., 2010). However, until a large sample of chil-dren post left and right hemisphere infarct is screened for CAS inthe acute stage, the hypothesis of a left hemispheric dominancefor speech planning in childhood can neither be confirmed nor
refuted.
4.1.6. Childhood apraxia of speech: concluding commentsIn summary, it seems that the neural basis for CAS remains
poorly understood, and rarely examined. Several reasons can beproposed. First, the brain structural abnormalities associated withCAS may be too subtle to be detected with clinical MRI sequences,
and quantitative methods are required to reveal morphologicalchanges in the grey and white matter. Another possibility is thatCAS is mainly the result of functional, metabolic or neurotransmis-sion defects, which again can only be detected by methods that
are not always available as part of routine clinical examinations.Thirdly, it should be noted that a general consensus on the diag-nostic features of CAS has been reached only recently (AmericanSpeech-Language-Hearing Association, 2007) and remains under
debate. This diagnostic issue probably makes CAS difficult to iden-
tify in paediatric settings.

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 7/20
Table 2
Neuroimaging findings in childhood dysarthria associated with metabolic disorders.
Article Aetiology Sample size (gender) Age/age range Description of speech
disorder
Neuroim
Pellecchia et al. (2003) Wilson’s disease N = 5 with both dysarthriaand neuroimaging (2
m)/series of 30 (15m)
? (inwholeseries, onset5–30 yrs) “Cerebellar dysarthria” in6 MRI “inrecovery
Alajoki et al. (2004) Salla disease N =15 with
neuroimaging/series of 41
(22 m)
11mthsto 63yrs (mean 24
yrs)
Expressive speech
impairment; “motor
difficulties connected to
dyspraxiaand dysarthria”
4 cannot speak
MRI
Golombet al. (2004) Pelizaeus–Merzbacher
disease
10 with
neuroimaging/series of 11
(10 m)
10 mths to 20 yrs All those who speak:
dysphoniaand dysarthria
MRI
Gootjes et al.(2004) Peroxisome biogenesis
disorder
N = 1 (f) 22 yrs at last investigation Dysarthria diagnosed at
age 5
CT
Muthane et al.(2004) Adult GM1 Gangliosidosis N = 2 (2 m)/series of 3 16 and 17 yrs (onset of
symptoms within 1st
decade)
Case1: at 16, speech
gradually worsened and
wasdifficultto
comprehend
MRI
Case2: lost his ability to
speak bythe age of 15
(anarthria)
Iturriaga et al. (2006) Niemann-Pick C disease N = 27 (?) 4 days to 43 yrs (onset of
symptoms from birth)
Dysarthriab (diagnosis
2–19yrs)
MRI
Fuijkschot et al. (2009) Sjögren–Larsson syndrome N = 13 (8 m)/series of 16 1;9–34;11 yrs Pseudobulbar (10),
hypokinetic (2), or both (1)
dysarthriaSeverity:3 severe, 2
moderate-severe, 5
moderate, 3 mild
MRI
Gupta and Nagarkar (2009) Nijmegen breakage
syndrome
N = 1 (f) 13 yrs Reduced loudness
Articulatory errors:distortion of velars and
dentals, omissions; “not
CAS”
MRI
Abbreviations as in Table 1.a Individual results are not reported in thearticle.b From Table 3, page 3 in original article.

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 8/20

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 9/20

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 10/20
448 F.J. Liégeois, A.T. Morgan / Neuroscience and Biobehavioral Reviews 36 (2012) 439–458
Fig. 4. Schematic illustration of locations of lesions/abnormalities associated with childhood dysarthria for each neurological condition. See Tables 2–8 f or details. (A)
Metabolicdisorders. Red,Wilson’sdisease(Pellecchiaet al.,2003). Blue, gangliosidosis(Muthaneet al.,2004). Yellow, cerebellar atrophyin Niemann-PickC disease(Iturriaga
et al., 2006). Other reports are not illustrated as atrophy and white matter changes are reported throughout the brain. (B) Syndromic conditions: Green, bilateral perisylvian
and opercularsyndromes(overview of findings fromTable 3). Red,suprabulbar palsy (Suresh andDeepa,2004). Blue, cerebellar andvermal atrophyin bothJoubert syndrome
(Andermannet al., 1999) and opsoclonus-myoclonus syndrome (Klein et al., 2007). Yellow, congenital non-progressive cerebellar ataxia (Dudding et al., 2004). (C) Infarcts:
Yellow, middle cerebral artery territory (Agrawal et al., 2007); white, brainstem (Miyakita et al., 1999); Green, cases 4 and 5 from Gout et al. (2005); pink, single case from
Golomb et al., 2002; red, basal ganglia (two left- and three right-sided cases from Rowan et al., 2007). Data from Horton et al. (1997) are only illustrated in the thalami
(blue) as the location of multipleinfarcts within thecerebellum is notspecified. (D)Neurodegenerative and progressivediseases: red, Charcot Marie Tooth disease (Siskind
et al., 2009); blue, PKAN (pantothenate kinase-associated neurodegeneration, Mikati et al., 2009); green, juvenile Huntingdon’s disease (Papapetropoulos et al., 2005). (For
interpretation of thereferences to color in this figure legend, the readeris referred to theweb version of the article.)
Therefore, we cannot rule out that numerous other neurolog-ical conditions exist that are associated with CAS in childhood,but that the diagnostic criteria are so contentious that CAS is
impossible to sensitively diagnose by health professionals not
trained in the specific diagnostic features of the condition (i.e.,not Speechand Language Therapists/Pathologists). Finally, the puz-zling absence of a single report of CAS following childhood stroke,
supratentorial tumour, or unilateral brain injury in the last decade

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 11/20

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 12/20

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 13/20
F.J. Liégeois, A.T. Morgan / Neuroscience andBiobehavioral Reviews 36 (2012) 439–458 451
strongly suggests that unilateral hemispheric lesion/damage is
not sufficient to result in CAS during development (as previouslyhypothesized by Vargha-Khadem et al.,1998; seealsoLiégeois et al.,2008; Morgan et al., 2010a). This hypothesis is corroborated byrecent findings indicating that even complete removal of a cere-
bral hemisphere in childhood does not result in apraxia of speech(Liégeois et al., 2010).
4.2. Neural bases of childhooddysarthria
Neuroimaging evidence in childhood dysarthria was better doc-umented than for CAS, with a total of 60 articles, reporting on 254cases. Given the heterogeneity of aetiologies associated withchild-
hood dysarthria, the possible neural basis for this speech disorderwill be discussed separately for each condition.
4.2.1. Metabolic disorders
Although representing only eight reports (Table 2), childrenwith dysarthria associated with metabolic conditions represent thelargest proportion of cases.As reported forCAS, neuroimagingfind-ings included white matter changes and hypomyelination across
the cerebral hemispheres (including periventricular regions) andthe cerebellum, with little regional specificity. In two conditions,
namely gangliosidosis and Wilson’s diseases, the basalganglia wereaffected bilaterally (Fig. 4A). Overall, dysarthria associated with
metabolic disorders therefore seems to disrupt brain structuresbilaterally, affecting both white matter integrity and basal gangliafunction. The mechanisms underlying such neural dysfunction of the speech systems remain to be explored.
4.2.2. Syndromic conditionsThe majority of articles (16 reports, 46 cases representing
18% of the total) included here reported on long-term childhood
dysarthria in children and adolescents with syndromic conditions(Table 3), withover two thirds (31 cases) presenting with Worster-Drought, bilateral perisylvian, and bilateral operculum syndromes.There is an ongoing debate as to whether these separate syn-
dromes represent a clinical continuum (Clark et al., 2000), but froma neuroimaging perspective they form a cohesive group in thatthey all affect the perisylvian or perirolandic cortices bilaterally(Fig. 4B). Aetiologies include anomalies of cortical development,
such as polymicrogyria or schizencephaly (see Spalice et al., 2009,for a review on migration disorders), and acquired neurologicalinsults, such as encephalopathy or infarct. Youngpeople presentingwith these syndromes most commonly suffer from severe forms
of dysarthria or anarthria (complete lack of speech). Altogether,results from this group suggest that when there is neuroimagingevidence of bilateral structural abnormality within the perisylvianand perirolandic cortices in childhood, motor speech prognosis is
poor, and spontaneous compensation is unlikely.Dysarthria was also reported in syndromes affecting the cere-
bellum, namely Joubert syndrome, congenital non-progressivecerebellar ataxia, and opsoclonus-myoclonus syndrome. In allcases, either agenesis or atrophy/hypoplasia of the cerebellar ver-mis was reported. The role of the cerebellum in speech productionwill be discussed further in a separate section (“posterior fossa
tumours”), but these few reports suggest that the cerebellarvermismay play a crucial role in normal speech execution.
4.2.3. Traumatic brain injury
As predicted, lesions associated with traumatic brain injury inthe series of cases reported here (10% of all cases with dysarthria)were highly heterogeneous (Table 4). Moreover, white and greymatter structures were affected at multiple sites. Cortical regions
affected included the frontal, parietal, and occipital cortices, while
subcortically lesions to the basal ganglia and cerebellum were T
a b l e
6
N
e u r o i m a g i n g fi n d i n g s i n c h i l d h o o d d y s a r t h r i a a s s o c i a t e d w i t h e p i l e p t i c d i s o r d e r s .
A r t i c l e
A e t i o l o g y
S a m p l e s i z e ( g e n d e r )
A g e / a g e r a n g e
D e s c r i p t i o n o f
s p e e c h
d i s o r d e r
N e u r o i m a g i n g
t e c h n i q u e
R e p o r t e d
n e u r o i m a g i n g
a b n o r m a l i t i e s
K r a m e r e t a l . ( 2 0 0 1 )
B C E C T S
N = 4 ( 3 m )
7 ; 6 – 1 5 y r s ( o n s e t o f
s y m p t o m s 4 – 1 0 ; 5 y r s )
I c t a l d y s a r t h r i a
M R I i n 4
N o r m a l i n a l l
P a r k e t a l . ( 2 0 0 5 )
B e n i g n r o l a n d i c
e p i l e p s y
N = 1 1 ( 8 m )
5 – 1 2 y r s ( s z o n s e t 4 – 1 1
y r s )
I n t e r i c a t a l h y p
o k i n e t i c
p a t t e r n o f a r t i c u l a t i o n ;
w o r s e n e d a f t e r C B Z
t r e a t m e n t
M R I
N o r m a l i n a l l
S e r r a e t a l . ( 2 0 0 8 )
C a t a p l e x y i n c h i l d
h o o d
n a r c o l e p s y
N = 3 ( ? ) / s e r i e s o f 2 3
( 1 3 m )
6 – 1 7 y r s ( s z o n s e t 6 – 1 6
y r s )
S l u r r e d s p e e c h
i n 1 3 %
d u r i n g c a t a p l e
c t i c
a t t a c k s
M R I
N o r m a l i n a l l
A
b b r e v i a t i o n s : B C E C T S , B e n i g n C h i l d h o o d E p i l e p s y w i t h C e n t r a l T e m p o r a l S p i k e s ; C B Z , c a r b a m a z e p i n e . O t h e r a b b r e v i a t i o n s a s i n T a b l e 1 .

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 14/20
Table 7
Neuroimaging findings in childhood dysarthria associated with infarcts.
Article Aetiology Sample size (gender) Age/age range Description of speech
disorder
Neuroimaging
technique
Hortonet al.(1997) Brainstem infarct
(basilar artery
occlusion)
N = 1 (m) 9 yrs (infarctat 5 yrs) 2 mthspost: slurred
speech then mutism
for2 mths, then severe
dysarthria
At9 yrs:
moderate-severedysfunction at all
levelsa
CT (2mthspost)
MRI (10days later)
CT (3yrs post)
Miyakita et al.(1999) Brainstem infarct N = 1 (f) 3;7 yrs Mute for 10 days, then
dysarthria
CT
MRI
Golomb et al. (2002) Infarct (possible
arteriopathy)
N =1 (m) 15 yrs Mild dysarthria
Difficulty forming
complex syllables
CT
DW MRI
Gout et al. (2005) Subcortical stroke 3 (?)/series of 9 5;4–10;6 yrs Case 4: mild at +1 mth;
resolved at +3mths
Case5: atday 1:resolved at +48mths
Case6: mutism for 12
days then slurred
speech; not mentioned
at+19 days
MRI
Agrawal et al.(2007) Ischemic infarct N =1 (m) 16 yrs Sudden mild slurring of
speech
CT
Contrast-enhanced
MRI
Rowan et al.(2007) Basal ganglia stroke (10
L, 7 R)
N =5 (1 m)/series of 17
(5m)
6;10–19;11 yrs (infarct
at 1;1–15;0 yrs)
Acute “slurred speech”
in 5 cases
MRI
Abbreviations:IC, internal capsule; MCA, middle cerebralartery; LH cases,left infarct cases;RH cases,right infarct cases; DW, diffusion-weighted; GP, globus pallidus. Othera For detailed reportof speech features seeoriginal article.

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 15/20

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 16/20

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 17/20
F.J. Liégeois, A.T. Morgan / Neuroscience andBiobehavioral Reviews 36 (2012) 439–458 455
reported on patients with left hemisphere infarcts (cortical or sub-
cortical, Fig. 4C). These latter findings raise the question of whethera bias exists in mainly reporting or examining motor speech out-come in children with left hemisphere infarcts. With regard to thelong-term speech outcome, it is noteworthy that only two articles
reported motor speech outcome more than one month post infarct.One case suffered from severe dysarthria four years after multi-ple infarcts caused by basilar artery occlusion (Horton et al., 1997).In contrast, dysarthria had resolved at 3 months and 4 years post
subcortical strokes in the two other cases, respectively (Gout et al.,2005, see Table7 for details).Importantly, in thecase with longtermdysarthria, both thalami were affected.
Regarding hemispheric differences, no cases with right hemi-
sphere basal ganglia strokes were recruited in the study by Goutet al.(2005). The studyby Rowan et al.(2007), which examined lan-guage (not motor speech) outcome after left or right basal gangliastroke, anecdotally reported on “slurred” speech in the acute phase
forfive cases, two with left and three with right hemisphere stroke.Whether these motor speech deficits were also present long-termwas not examined. In conclusion, from the sparse evidence avail-able we may conclude that (i) there is no hemispheric difference
for articulation in childhood, (ii) only transient dysarthria occursafter childhood unilateral stroke, and that (iii) longterm dysarthria
only occurs after bilateral stroke to speech-related neural systems.These claims however will need further substantiation.
4.2.7. Neurodegenerative and progressive diseasesIn adults, neurodegenerative diseases such as Parkinson’s dis-
ease(PD, Pintoetal.,2004), Huntington’s disease (HD, e.g.,Hartelius
et al., 2003) and corticobasal degeneration (e.g., Josephs and Duffy,2008) are closely associated with motor speech disorders. Giventhe natural prevalence of these conditions in the ageing popu-lation, a comparison with childhood-onset equivalents must be
approached with caution. Overall, both HD and PD fall howeverinto the category of basal ganglia dysfunction, and have their owndysarthria classifications aligned with hypokinetic or hyperkineticmotor symptoms, respectively in the model originally proposed by
Darley et al. (1969). In the present review a total of only 7 caseswere reported alongside neuroimaging evidence (Table 8), consis-tent with the rarity of the disorders. Apart from four cases withno reported abnormalities, two cases had bilateral abnormalities
in the basal ganglia (Fig. 4D), namely the caudate nucleus for juve-nile HD, and the globus pallidus and surrounding white matter inpantothenate kinase-associatedneurodegeneration. In the remain-ing case, white matter changes were reported across the brain, in
periventricular and cerebellar white matter, the posterior limb of the internal capsule, and cerebral peduncles (Fig. 4D). Altogether,the limited evidence therefore suggests that bilateral disruption tothebasalganglia circuits may be at theroot of dysarthria in children
with these neurodegenerative diseases, as seen in adults. Furtherinvestigations will be needed however to draw firm conclusions on
the role of the basal ganglia control circuits and their disruption inneurodegenerative conditions that affect children.
4.2.8. Miscellaneous conditionsA significant proportion of cases (17%) with conditions not
falling into the above categories had neuroimaging data alongsidedysarthria diagnosis (Table 9). The majority of cases (38/43, onereport) had the pyramidal form of infantile cerebral palsy. In thisreport, the extent of changes was reported to correlate with the
severity of the disorder, but no information was provided as to thelocation of brain abnormalities (Otapowicz et al., 2007). In one case(Brugnolettiet al.,2009), whitematter abnormalities were detectedwithin the centrum semiovale and frontal lobes bilaterally, to a
greater extent in the left hemisphere. In the remainder of cases,
the cerebellum and brainstem were affected bilaterally. Overall
therefore, these reports indicate bilateral abnormality at different
levels of the speech neural systems.
4.2.9. Dysarthria types in relation to neuroimaging evidenceUse of correct terminology in relation to dysarthria was poor in
the articles reviewed here. Six of the 60 reviewed studies used only
the term ‘slurred’ speech (or other such terms “impaired speecharticulation,” “speech less smooth”) in place of dysarthria itself.Of the 54 studies reporting on dysarthria as such, only 12 (mainlyin the areas of TBI and posterior fossa tumour resection) reported
specific diagnoses of dysarthria sub-types using the Darley et al.(1969) classification. Specific diagnoses were highly mixed bothwithin and across the various populations of interest, as is typicallyseen in use of the scale with adults (Simmons and Mayo, 1997),
partly reflecting the heterogeneity of the underlying neural basesfor the problems. This heterogeneity also reflects a main criticismof the Darley and colleagues’ scale, in that few clear associationscan be made between speech outcome and disruption of underly-
ingneural function,in which case clinicians typicallyreport ‘mixed’dysarthria diagnoses (e.g., ataxic-spastic dysarthria, Simmons andMayo, 1997). These findings, taken together with the lack of CASresultingfrom left hemispherestroke, suggest that it may be timely
for development of a child-specific neuro-anatomical classification
system for motor speech disorders (Van Mourik et al., 1997b; seeMorgan and Liégeois, 2010, f or further discussion on this topic).
4.3. Childhood speechdisorders: a window into the developing
neural systems involved in speech
Neuroimaging correlates of CAS reviewed here are not incon-sistent with the adult model of speech planning (illustrated in
Fig. 1), with dysfunction involving the basal ganglia and the infe-rior frontal cortices. This speech planning network might thereforebe functional early in development. Similarly, neuroimaging cor-relates of childhood dysarthria are not inconsistent with current
neuroanatomical models of adult speech execution (Fig. 1). Indeed,childhood dysarthria was associated with white matter lesions
located along the corticobulbar and corticospinal tracts (coronaradiata, central semiovale, internal capsule, midbrain), and with
grey matter lesions within the perisylvian and peri-rolandic cor-tices, basal ganglia (putamen, caudate nucleus) thalamus, andcerebellum (Fig. 4). It seems therefore that the adult speech execu-tion systemsmay be in place early in development. Altogether, data
from the present review suggest that the neuroanatomical basesfor speech production in adults and children overlap, but that thepotential for functional compensation after unilateral lesion differsbetween the two age groups.
5. Concluding remarks
Thepresent reviewconfirms that the conditionsassociated with
speech disorders differ between adults and children. However cur-rent adult models of the neural basis for speech seem to applyin childhood, whereby the perisylvian and perirolandic cortices,the basal ganglia, and the cerebellum all play a major role in bothspeech execution and planning. Yet one major difference is of crit-
ical note. Where uni-hemispheric damage in the adult populationseems to be sufficient to result in chronic speech disorders, bilat-eral disruption of these systems in childhood seems necessary toresult in the most severe and long-lasting deficits (see also Vargha-
Khadem et al., 1985 f or a similar conclusion regarding languagedevelopment). This suggests that either hemisphere has the poten-tial to subserve speech functions in childhood. Further, in the caseof unilateral lesion/disruption, the evidence for a left hemispheric
dominance for speech functions, including articulation, was sparse.
Additional scientific evidence is therefore needed to improve our

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 18/20
456 F.J. Liégeois, A.T. Morgan / Neuroscience and Biobehavioral Reviews 36 (2012) 439–458
understanding of the neuralbasis of speech disordersduringdevel-
opment.Such evidence would provide a major stepforward for thedevelopment of a clinicoanatomical classification of motor speechdisorders in children and adolescents.
Conflict of interest
The authors reported no conflict of interest.
Acknowledgements
We thank Cristina Mei for her assistance in retrieving andarchiving abstracts and articles. We also thank Dr. Baldeweg andDr. Vogel for their helpful comments on an earlier version of the
manuscript, and Dr. Schulze for her assistance with illustrations.Dr. Morgan is supported by NHMRC Career Development Award607315.
Appendix 1.
Search terms for neuropathology
1. Brain Injuries/ or Brain Diseases, Metabolic/ or Hypoxia, Brain/or Brain Damage, Chronic/ or Brain/ or Hypoxia-Ischemia,Brain/ or Brain Injury, Chronic/ or Brain Hemorrhage, Trau-matic/ or Brain Ischemia/ or Brain Diseases, Metabolic, Inborn/or “Pick Disease of the Brain”/ or Brain Stem Neoplasms/ or
Brain Infarction/ or Brain Stem Hemorrhage, Traumatic/2. Brain Neoplasms/ or Tumor Necrosis Factor-alpha/ or Carcinoid
Tumor/ or tumour.mp. or tumor.mp. or Wilms Tumor/3. infarct.mp. or exp Infarction/
4. Neurology/ or neuropathology.mp. or neurodevelopmen-tal.mp.
5. Developmental Disabilities/ or Nervous System Diseases/ orChildDevelopment Disorders,Pervasive/or developmental dis-
order.mp.
6. Magnetic Resonance Imaging/ or Neocortex/ or Cerebral Cor-tex/ or migration disorder.mp.
7. polymicrogyria.mp. or “Malformations of Cortical Develop-
ment”/8. Infant/ or Tomography, X-Ray Computed/ or Microcephaly/ or
lissencephaly.mp. or Abnormalities, Multiple/ or CobblestoneLissencephaly/ or Lissencephaly/ or Syndrome/
9. pachygiria.mp.10. schizencephaly.mp.11. heterotopia.mp. or Cerebral Ventricles/ or Brain Neoplasms/ or
Periventricular Nodular Heterotopia/
12. cortical dysplasia.mp.13. hemimegalencephaly.mp.14. exp Epilepsy/ or epilepsy.mp.
15. cerebral palsy.mp. or Cerebral Palsy/16. traumatic brain injury.mp.17. Encephalitis/ or Encephalitis.mp.18. Brain Diseases, Metabolic/ or Metabolic Diseases/ or
metabolic.mp. or Brain Diseases, Metabolic, Inborn/
19. galactosaemia.mp. or Galactosaemias/20. Perisylvian syndrome/ or perisylvian.mp.21. moebius.mp. or Mobius Syndrome/22. Bulbar Palsy, Progressive/ or worster-drought.mp.
23. exp Williams Syndrome/ or william.mp. or Child/24. exp Down Syndrome/ or down.mp.25. foix-chavany-marie.mp.26. Brain Diseases/ or Magnetic Resonance Imaging/ or opercular
syndrome.mp. or Speech Disorders/ or Syndrome/ or Epilepsy,Frontal Lobe/
27. sturge-weber.mp.
28. juvenile Parkinson*.mp.29. juvenile Huntington*.mp.30. encephalopathy.mp.31. myotonic dystrophy.mp.
32. muscular dystrophy.mp.33. multiple sclerosis.mp.34. Friedrich ataxia*.mp.35. spinocerebellar ataxia.mp.
36. Niemann Pick.mp.
Appendix 2.
Search terms for paediatric population
37. exp Child/ or Infant/38. exp Pediatrics/ or paediatric.mp.
39. Adolescent/ or exp Adolescent/
Appendix 3.
Search terms for motor speech disorders
40. Speech/ or Speech Therapy/ or Speech Disorders/ or Aphasia/or Dysarthria/
41. Speech Articulation Tests/ or Articulation Disorders/ or Speechintelligibility/
42. verbal dyspraxia.mp.43. Language Disorders/
44. Verbal Behavior Language Development Disorders/45. (oral dyspraxia or speech dyspraxia).mp
References
Ackermann, H., Riecker, A., 2010. The contribution(s) of the insula to speech pro-duction: a reviewof theclinical andfunctional imaging literature. Brain Struct.Funct. 214, 419–433.
Agrawal,A., Joharapurkar, S.R., Gharde, P., 2007. Ischemic stroke in a child mistakenas functional disorder. Clin. Neurol. Neurosurg. 109, 876–879.
Alajoki, L., Varho, T., Posti, K., Aula, P., Korhonen, T., 2004. Neurocognitive profiles inSalla disease. Dev. Med. Child Neurol. 46, 832–837.
Andermann,F., Andermann, E.,Ptito,A., Fontaine, S.,Joubert,M., 1999.Historyof Jou-bert syndrome anda 30-year follow-upof theoriginalproband. J. Child Neurol.14, 565–569.
Anderson, V., Spencer-Smith,M., Leventer,R., Coleman,L., Anderson, P., Williams, J.,et al., 2009. Childhood brain insult: can age at insult help us predict outcome?Brain 132, 45–56.
American Speech-Language-Hearing Association, 2007. Childhood Apraxia of Speech [Technical Report], Available from: www.asha.org/policy (retrieved26.06.10).
Arbelaez, A., Castillo, M., Tennison, M., 2000. MRI in a patient with the Worster-Drought syndrome. Neuroradiology 42, 403–405.
Ashburner,J., Friston,K.J., 2000.Voxel-based morphometry—the methods.Neuroim-age 11, 805–821.
Battini, R.,Chilosi, A., Mei, D., Casarano, M., Alessandrì, G.M., Leuzzi, V., et al., 2007.Mental retardation, verbal dyspraxia in a new patient with de novo creatinetransporter (SLC6A8) mutation. Am. J. Med. Genet. A 143A, 1771–1774.
Belton, E., Salmond, C.H., Watkins, K.E., Vargha-Khadem, F., Gadian, D.G., 2003.Bilateral brain abnormalities associated with dominantly inherited verbal andorofacial dyspraxia. Hum. Brain Mapp. 18, 194–200.
Beslow, L.A., Jordan, L.C., 2010. Pediatric stroke: the importance of cerebral arteri-opathy and vascular malformations. Childs Nerv. Syst. (Epub ahead of print).
Brugnoletti, F., Morris, E.B., Laningham, F.H., Patay, Z., Pauley, J.L., Pui, C-H., et al.,2009. Recurrent intrathecal methotrexate induced neurotoxicity in an adoles-cent with acute lymphoblastic leukemia: serial clinical and radiologic findings.Pediatr. Blood Cancer 5, 293–295.
Cahill, L.M., Murdoch, B.E., Theodoros, D.G., 2002. Perceptual analysis of speechfollowing traumatic brain injury in childhood. Brain Inj. 16, 415–446.
Cao, Z., Lv, J., Ding, Z., Du, H., 2008. Pathological laughter in a patient with Rathkecleft cyst. J. Clin. Neurosci. 15, 1279–1282.
Caspari, S.S., Strand, E.A., Kotagal, S., Bergqvist, C., 2008. Obstructive sleep apnea,seizures, and childhood apraxia of speech. Pediatr. Neurol. 38, 422–425.
Chilosi, A.M., Cipriani,P., Pecini, C.,Brizzolara, D.,Biagi, L., Montanaro,D., Tosetti, M.,Cioni, G.,2008.Acquiredfocal brain lesionsin childhood:effects ondevelopment
and reorganization of language. Brain Lang. 106, 211–225.

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 19/20

8/10/2019 Neural Bases of Childhoos Speech Disorders.pdf
http://slidepdf.com/reader/full/neural-bases-of-childhoos-speech-disorderspdf 20/20