
CRANIAL NERVE LESIONS IN THE EMERGENCY DEPARTMENT BY RAKSHA RAMLAKHAN.

Nerve lesions

Lesion: a structural change in a body part due to injury or disease.
signs and symptoms of a nerve lesion are directly correlated to the function of the nerve
Definitions

Neurapraxia = segmental demyelinationLocal injury may distort/disrupt the myelin sheath locally, resulting in focal demyelination. => temporary conduction block
Sheath is restored locally
Wallerian degeneration Occurs distal to lesion site = loss of conduction Accompanied by corresponding muscle atrophy followed by removal by macrophages and recycling of myelin-
derived material
responses to Injury

Classification of Nerve lesions

Incomplete/completeComplete when all neurons traversing the injured segment are disrupted
Incomplete when not all neurons are disrupted, sparing of distal motor/sensory function
By SEVERITY
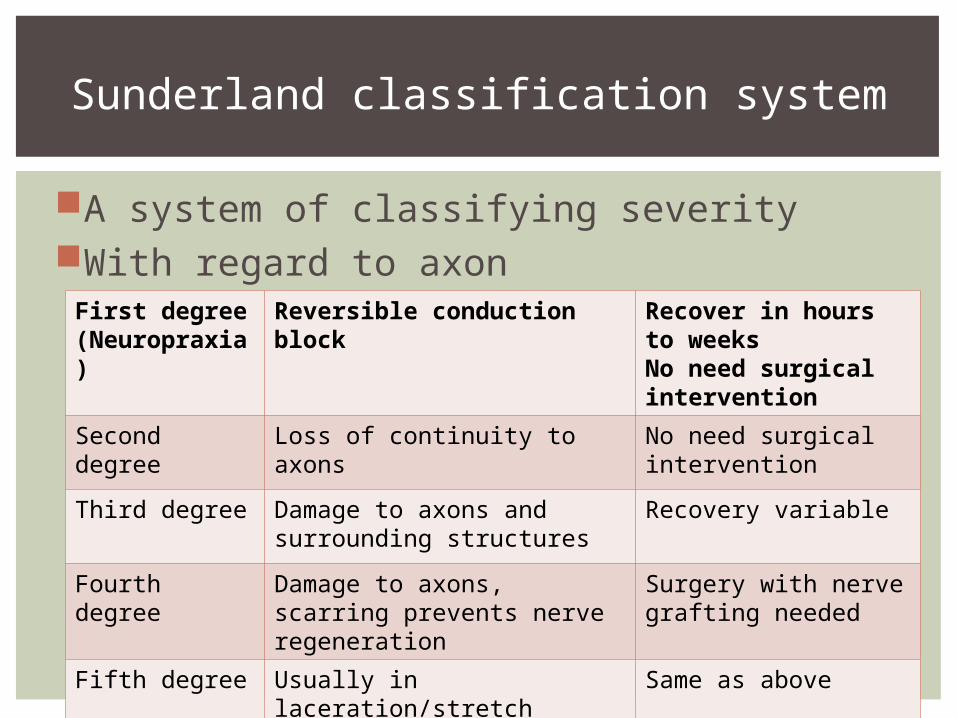
A system of classifying severityWith regard to axon
Sunderland classification system
First degree (Neuropraxia)
Reversible conduction block
Recover in hours to weeksNo need surgical intervention
Second degree Loss of continuity to axons No need surgical intervention
Third degree Damage to axons and surrounding structures
Recovery variable
Fourth degree Damage to axons, scarring prevents nerve regeneration
Surgery with nerve grafting needed
Fifth degree Usually in laceration/stretch injuries: nerve divided into 2
Same as above
NB: some sources include ‘sixth degree’- mixed patterns of injuryAffects management of injury
about the classification

By how they damage nerves:Those which cause anoxic anoxia
CO, cyanideThose which cause demyelination
Lead, trimethyl tin, thalliumThose which damage peripheral neurons
Usually from chronic exposure e.g. Ethanol, organophosphates (e.g. malathion, DDT)
Those which damage cell body of neuron Organic mercury, vinca alkaloids
Those which damage NMJ specifically tetrodoxin (from pufferfish), botulinum toxin (botox),
Those which cause lesions within CNS e.g. Gold thioglucose
For Neurotoxins:

methods and reflex testsDiagnosis

Recall: reflex arcSensory -> interneuron -> motor
Tests help in localisation of nerve lesions(some primitive reflexes are a sign of brain
injury in general)
Reflex tests

Name What you have to do
Positive sign What it means
Orbicularis oris/snout/nasomental
tap finger/tongue depressor on lateral corner of mouth/lips
pursing oflips
exaggerated with lesions affecting supranuclear corticopontine pathways- e.g. multi-infarct dementia, extrapyrimidal diseases e.g. Parkinson)
Suck Gently stroke lips Sucking/swallowing movements
Biting
Mouth opening and head turning to stimulus
Normal in babies, but in adults indicates sv, diffuse brain injury
Wartenberg/’thumb sign’
Forcefully flex 2nd-5th fingers
Flexion of thumb Pyramidal tract lesion
Palmomental (exaggerated/asymmetrical)
Intensely stroke ball of thumb/palm of hand with fingernail
Contraction of ipsilateral chin muscles
If unilateral, contralateral brain lesion;also in diffuse cerebral injury
Pathological Reflexes

Name of reflex What you have to do Positive sign What it meansGrasp stroke palm finger flexion,
graspingNormal in infantsOtherwise, sign of diffuse brain injury
Gegenhalten (paratonia)
Attempted passive stretching of muscle
active and intense contraction of muscle in question – patient involuntarily resist movement
Frontal lobe damage, neurodegenerative conditions
Grasping/groping (magnet phenomenon)
object brought near palm of conscious patient
Hand follows presented object like a magnet
Normal in infantsOtherwise, sign of diffuse brain injury
Mass reflexes of lower limbs
Forceful passive flexion of toes/forefoot (Marie-Foix handgrip)
Retraction of lower limb by flexion at knee and hip
reveals intactness of spinal reflex arc => peripheral nervous sys
reflex tests

Name What you have to do
Positive sign What it means
Babinski reflex Stroke lateral edge of foot from heel to 5th toe
Tonic extension of big toe, other toes remain/splayed
Lesion of pyramidal pathway on corresponding side
Oppenheim reflex Forcefully stroking ant. margin of tibia, proximal -> distal (painful!)
Same as Babinski
Grasping/groping (magnet phenomenon)
object brought near palm of conscious patient
Hand follows presented object like a magnet
Normal in babies, sign of diffuse cerebral injury in adults
Gordon reflex Forcefully stroking/squeezing calf muscles
Same as Babinski
reflex tests

Often used with EMG to differentiate nerve disorder from muscle disorder
Speed of conduction depends on degree of myelination diameter of nerve
Normal: 50-60m/s Slower could indicate problems with
myelinationFalse negative: lower body temperature => slower conduction
Nerve conduction velocity test

Procedure:Two electrode patches placed on skin over the nerve; electrodes attached
One electrode stimulates the nerve with electrical current. The other records the nerve’s
Time taken for electrical impulse to travel betweenprobes is measured.
NCV cont’d

Gold standardfor neuromusculardisorders
Procedure:Needles are inserted through skin into muscleElectrical activity is measured during rest, slight contraction and forceful contraction
Electromyogram (EMG)

To identify nerve defect more specifically Typical sites: radial, sural nerves
Nerve biopsy

Common peripheral nerve lesionsSigns and symptoms

Nerve Probable cause
Sensory loss Motor loss
Sciatic n. ● penetrating wounds,
● fractures of the pelvis
● hip dislocations
● badly-placed intramuscular injections
Below knee except medial side of leg and medial border of foot Tingling suggests nerve is not totally severed
● Weakness extending hip joint and flexing knee joint due to impaired hamstring ability
● Cannot move foot● Cannot bend knee● Foot drop (below)
Lower limbs

Nerve Probable cause
Sensory loss Motor loss
Common peroneal nerve
Commonly injured in fractures of the neck of the fibula.
LOS on skin of leg & foot anteriorly & laterally except the lateral border of the foot (sural nerve) and medial border of the foot (saphenous).
● Damaged to innervation of anterior leg muscles => weakened extension of ankle
● Innervation (superficial peroneal nerve) to lateral leg muscles damaged=>
● weakened flexion of ankle joint; inversion of foot
● Unsupported/unopposed foot exhibits foot drop and inversion (equinovarus) (below)
Lower limbs

Lower limbs
Nerve Probable cause
Sensory loss Motor loss
Femoral n.
Rarely injured unless gunshot/stab wounds
LOS over anterior and medial sides of thigh, along medial border of leg as far as big toe
Unable to flex knee as all quadriceps muscles are paralyzed
Tibial n. Rarely injured; protected by muscles
● LOS on sole of foot● Ulcers can develop
● Posterior muscles of leg paralysed => no plantar flexion
● Foot is dorsiflexed and everted => calcaneovagus (left)

upper limbs nerve lesions (brachial Plexus)

Probable cause Motor loss Sensory loss Observable effect
Axillary n.
Badly adjusted crutch, downward displacemt of humerus in shoulder dislocations, humerus fracture
Paralysis of deltoid/teres minor
Lower deltoid Cannot abduct arm past 15 deg
Radial n.
Axilla lesion: triceps, anconeus, extensor m. of forearm
Post. forearm, lat. dorsum of hand, lat. 3.5 fingers
Cannot extend elbow + wrist joint, fingersWrist drop (below)
Upper limbs
NB: Radial n. lesions are also called ’Saturday night palsy’ because people get drunk and fall asleep with their arms hanging over the backs of chairs. Also ‘Honeymoon palsy’ when one of the newlyweds sleeps on the arm of the other.

Upper limbs
left image: positive Froment’s sign

Upper limbs

Body’s response to injury

Nerves can regrow under favourable environment of the Schwann cells
In contrast, oligodendrites and astrocytes in CNS are generally inhibitory to axonal growth
can nerves recover?

Recovery depends on severity (naturally)
depends on severity
Type of injury Spont? Rate of recovery
Surgery
First degree Full Days- 3 months after injury
None
Second degree Full Regenerates: 1 in/mth
Third degree Partial Neurolysis?
Fourth degree None After surgery, 1 in/mth
Nerve repair, graft, transfer
Fifth degree None

1. Macrophage invasion mitogenic input to Schwann cell remove debris (e.g. axonal fragments)
2. Regenerating axon sprouts within hours3. Axon contacts the Schwann cell basal laminae on
one side and the Schwann cell membrane on the other
Schwann cell basal lamina provides promoters of axonal outgrowth (e.g. laminin, fibronectin)
Schwann cell directs regenerating axon back to its target using endoneurial tube
But can result in neuroma formation4. BUT loss of cell body = irreversible
e.g. polio, motor neurone disease No regeneration is possible
After an injury
Limited because:neurons are postmitotic in the mature CNSneurons are localised to certain sitesglial cells in CNS are inhibitory to axonal outgrowth
Regeneration in CNS

of nerve lesionsTreatment

Surgical NonsurgicalIndications:•Injury/continuity defect in nerve which cannot regain normal function without surgical intervention•Loss of normal neural function which cannot be corrected non-surgically•Distressing subjective symptoms
Indications:•Evident improvement indicating electrical regeneration•Mild, tolerable subjective symptoms
• Effects last longer • Short-term
Categories of treatment

of nerve lesionssurgical Treatment

= joining up of the ends of the nerves using sutures
Best when nerve has been cut sharplyBUT nerve elasticity causes retraction of
segmentscauses tension
can lead to scarring, ischemia
Nerve repair
Requires a donor nerveAverage size 2-5cm
Cable grafts used if greater than 2-3cm->Most common:
Sural n.Great auricular n.
Decided by Ease of harvestingMinimising resulting loss of function
Because once you take out the donor nerve, the dermatomes it innervates will have no sensation etc.
Nerve graft

To consider:Diameter of donor and host nerves
Should match!! But can combine 2 strands => bigger diameter (“cable
graft”)Length of graftNumber of fasciclesCross-sectional shape and area
Nerves can be round or flatPatient preference!
Harvesting donor nerve => loss of sensation, patients might prefer that the loss of sensation be somewhere specific.
When choosing donor nerves

VascularitySchwann cells survive when the graft is revascularised quickly
Time since injuryAvoids problems like Wallerian degeneration, etc.
Extent of injury/length of graft required(for peripheral nerves) Tension on prepared
nerveThe limb must be kept in a relaxed position
What affects recovery

Other tissues can be used to graft nerves too!
Most common: veinsGenerally good results in studiesEasy to find good size match for nerves
BUT:poor resistance to kinking and collapse
Unsuitable for longer grafts
Nerve grafting: alternatives

of nerve lesionsnonsurgical Treatment

= removal of scar tissueWorks best when
nerve is entrapped, not cutnerve is not transected, electrical impulses still can flow
Requires skill and cautionMight damage surrounding, functional nerves
Neurolysis

MedicationLifestyle changes
e.g. for carpal tunnel syndrome, patients can be taught to take frequent breaks during repetitive tasks
NSAIDS relieve pain
Nonsurgical treatment

Transcutaneous nerve stimulation (left)using gating mechanism
Physical therapyRadiofrequency techniques
‘cooking’ the nerve!
Nonsurgical treatment

Regional nerve-blocking procedures using local anestheticsLocal anesthetic at nerveAt neuroma
= mass of nerve fibres and Schwann cells formed after injury
Neurolysis at peripheral nerves Usually for terminal patients Phenol/ethanol injected directly to nerves supplying body
part in pain Effect lasts 6-8 weeks
nonsurgical treatment

Sources and biblio

http://www.instantanatomy.net/arm/nerves/medianwrist.htmlhttp://www.aic.cuhk.edu.hk/web8/peripheral_nerve_lesions.htmhttp://www.ncbi.nlm.nih.gov/pubmed/8832668http://www.rsdsa.org/glial_workshop/glialpdf/James_Campbell/NerveLesionsPain.pdfhttp://emedicine.medscape.com/article/1172408-overviewhttp://www.hopkinsmedicine.org/neurology_neurosurgery/specialty_areas/peripheral_nerve_surgery/conditions/nerve_injury.html
NCV and EMG: http://www.nlm.nih.gov/medlineplus/ency/article/003927.htm - NCVhttp://www.urmc.rochester.edu/encyclopedia/content.aspx?ContentTypeID=92&ContentID=P07657http://www.hopkinsmedicine.org/healthlibrary/test_procedures/neurological/electromyography_emg_92,P07656/ - about EMGhttp://www.neneuro.com/nn_12_use_of_emg.html - Use of EMG in nerve/muscle disord
sources

Cell response to injury:http://faculty.swosu.edu/scott.long/txcl/cnstox.htm - CNS toxinshttp://www.jneuroinflammation.com/content/8/1/109Surgical Management of Pain edited by Kim Burchiel
Treatment of nerve lesions:http://www.medscape.com/viewarticle/423216_6http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1201001/http://surgerydept.wustl.edu/Surgery_M.aspx?id=2936&menu_id=284http://cal.vet.upenn.edu/projects/saortho/chapter_65/65mast.htmhttp://www.painclinic.org/treatment-peripheralnerveblocks.htm - Nerve blockshttp://emedicine.medscape.com/article/1298684-treatment
Clinical:http://www.dartmouth.edu/~dons/index.html
sources

PICTURES:http://images.rheumatology.org/image_dir/album75674/md_99-12-0031.tif.jpghttp://1.bp.blogspot.com/-WhtUSzuIB54/ThhNNr7QF4I/AAAAAAAACu0/6bJ_wG8OLfk/s1600/Radial+nerve-wrist+drop.jpghttp://www.bailey-law.com/docs/acute-nerve-injuries.htmhttp://www.taringa.net/posts/imagenes/15519439/Sabia-usted-que____-_Propio_-_Curiosidades_.html
INTERESTING READINGS:http://ntp.neuroscience.wisc.edu/neuro670/reqreading/RegeneratingTheNervousSystem.pdf
Picture sources


















