Nephrology
23
Morning Report Morning Report Nephrology Team Nephrology Team Sharla Hays, M.D. Sharla Hays, M.D. August 9, 2004 August 9, 2004
description
Transcript of Nephrology

Morning ReportMorning ReportNephrology TeamNephrology Team
Sharla Hays, M.D.Sharla Hays, M.D.
August 9, 2004August 9, 2004

12yo Caucasian female presents to nephrology 12yo Caucasian female presents to nephrology clinic for evaluation secondary to father’s recent clinic for evaluation secondary to father’s recent death from kidney disease and significant family death from kidney disease and significant family history of kidney disease.history of kidney disease.
She is asymptomatic with no signs or symptoms of She is asymptomatic with no signs or symptoms of kidney diseasekidney disease
No hospitalizations, no surgeriesNo hospitalizations, no surgeries NKDANKDA Lives in El Paso with mother and 9 yr old brother, Lives in El Paso with mother and 9 yr old brother,
active in sports, and does well in schoolactive in sports, and does well in school

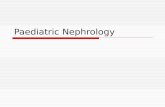
PedigreePedigree
This is our patient

ExamExam VS T36.5 P84 BP 123/57 R 20VS T36.5 P84 BP 123/57 R 20 Wt 69kg (>95%) Ht174.5cm (>95%)Wt 69kg (>95%) Ht174.5cm (>95%) Gen-healthy, NADGen-healthy, NAD HEENT-normal findingsHEENT-normal findings Chest-clear Chest-clear Heart-RRR without murmur, pulses 2+Heart-RRR without murmur, pulses 2+ Abd-+BS, soft, non-tender, non-distended, Abd-+BS, soft, non-tender, non-distended,
no HSM, no mass or kidneys palpableno HSM, no mass or kidneys palpable Ext-no c/c/eExt-no c/c/e

Problem List ?Problem List ? Differential for Hereditary kidney diseases?Differential for Hereditary kidney diseases?
(answers on next slide)(answers on next slide)

Differential for Hereditary Kidney Differential for Hereditary Kidney DiseasesDiseases
Autosomal Dominant Polycystic Kidney DiseaseAutosomal Dominant Polycystic Kidney Disease Autosomal Recessive Polycystic Kidney DiseaseAutosomal Recessive Polycystic Kidney Disease Thin Basement Membrane DiseaseThin Basement Membrane Disease Alport SyndromeAlport Syndrome Juvenile NephronothisisJuvenile Nephronothisis Medullary Cystic DiseaseMedullary Cystic Disease Sickle Cell DiseaseSickle Cell Disease Tubular Disorders (Cystinosis)Tubular Disorders (Cystinosis)

LabsLabs
Hgb/Hct: 13/38, Plt: 330KHgb/Hct: 13/38, Plt: 330K
Na 143, K 4.2, Cl 106, HCO3 25, Ca 9.8Na 143, K 4.2, Cl 106, HCO3 25, Ca 9.8
BUN 18, Cr 0.9BUN 18, Cr 0.9

LabsLabs Renal US-multiple cysts of varying sizes are Renal US-multiple cysts of varying sizes are
identified in both kidneys. In the right kidney identified in both kidneys. In the right kidney cyst measures 2x2 cm, second cyst cyst measures 2x2 cm, second cyst measures 1x1 cm, and a third cyst in the measures 1x1 cm, and a third cyst in the mid pole measures 1.3 cm. The left kidney mid pole measures 1.3 cm. The left kidney also has various cyst. The mid pole there is also has various cyst. The mid pole there is a two small cyst (both <1cm). The third cyst a two small cyst (both <1cm). The third cyst is also <1cm. No evidence of solid mass or is also <1cm. No evidence of solid mass or hydronephrosis.hydronephrosis.

Cystic Diseases of the KidneyCystic Diseases of the Kidney
Autosomal Dominant Polycystic Kidney Autosomal Dominant Polycystic Kidney DiseaseDisease
Autosomal Recessive Polycystic Kidney Autosomal Recessive Polycystic Kidney DiseaseDisease
Multicystic Dysplastic Kidney DiseaseMulticystic Dysplastic Kidney Disease

Autosomal Dominant PolycysticAutosomal Dominant Polycystic Kidney Kidney DiseaseDisease
Characterized by cystic dilation in all parts of Characterized by cystic dilation in all parts of the nephron including Bowman’s spacethe nephron including Bowman’s space
Focal with areas of normal and abnormal Focal with areas of normal and abnormal nephrons interspersednephrons interspersed
Cysts in the liver, pancreas, and other Cysts in the liver, pancreas, and other organs are commonorgans are common
Incidence at birth 1:400-1000, but rarely Incidence at birth 1:400-1000, but rarely identified prenatallyidentified prenatally
PKD1 gene abnormality responsible for 90%PKD1 gene abnormality responsible for 90%

ADPKD continuedADPKD continued
Clinical manifestations usually present in the Clinical manifestations usually present in the fourth decade with chronic flank pain and fourth decade with chronic flank pain and intermittent hematuriaintermittent hematuria– Account for 10-15% of ESRDAccount for 10-15% of ESRD
Familial incidence of childhood presentationFamilial incidence of childhood presentation Affected children can develop renal Affected children can develop renal
symptoms of ADPKD including gross or symptoms of ADPKD including gross or microscopic hematuria, hypertension, cyst microscopic hematuria, hypertension, cyst infection, and renal insufficiencyinfection, and renal insufficiency

ADPKD continuedADPKD continued Diagnosis usually established by USDiagnosis usually established by US
– Reveals diffuse hyperechogenicity, enlarged Reveals diffuse hyperechogenicity, enlarged kidneys, and cysts, usually bilateralkidneys, and cysts, usually bilateral
– Criteria for ADPKD: <30 at least 2 cyst in one Criteria for ADPKD: <30 at least 2 cyst in one kidney, 30-60 at least 2 cyst in each kidney,and kidney, 30-60 at least 2 cyst in each kidney,and >60y at least 4 cyst per kidney>60y at least 4 cyst per kidney
Prenatal US-kidneys may look normal or Prenatal US-kidneys may look normal or appear enlarged and echogenic appear enlarged and echogenic – If either parent has ADPKD the finding of If either parent has ADPKD the finding of
enlarged echogenic kidneys in fetus confirms enlarged echogenic kidneys in fetus confirms prenatal diagnosisprenatal diagnosis

ADPKD continuedADPKD continued
Child presenting in first year of life usually Child presenting in first year of life usually do not progress rapidly to ESRDdo not progress rapidly to ESRD
Most have few or no symptoms and present Most have few or no symptoms and present as adultsas adults
Renal insufficiency usually develops after Renal insufficiency usually develops after age of 30age of 30

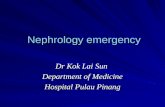
Polycystic kidney Polycystic Kidney

Liver cysts

Autosomal Recessive Polycystic Kidney Autosomal Recessive Polycystic Kidney DiseaseDisease
Also called Infantile Polycystic Kidney Also called Infantile Polycystic Kidney diseasedisease
Nonobstructive dilatation or ectasia of the Nonobstructive dilatation or ectasia of the collecting tubules in the renal medullacollecting tubules in the renal medulla– Results in microcysts of 1-2mmResults in microcysts of 1-2mm
Severity proportional to percentage of Severity proportional to percentage of nephrons affected by cystsnephrons affected by cysts
Hepatic involvement with cysts, fibrosis, and Hepatic involvement with cysts, fibrosis, and portal hypertensionportal hypertension– Also called congenital hepatic fibrosisAlso called congenital hepatic fibrosis

ARPKD continuedARPKD continued
Incidence 1:40,000-50,000Incidence 1:40,000-50,000 Typically presents in infancyTypically presents in infancy Clinical manifestations included Clinical manifestations included
hyponatremia during first weeks of life, hyponatremia during first weeks of life, reduced concentrating ability, decreased reduced concentrating ability, decreased urinary acidification capacity leads to urinary acidification capacity leads to metabolic acidosis, and recurrent pyuriametabolic acidosis, and recurrent pyuria
Hypertension common earlyHypertension common early ESRD usually after 15yr of ageESRD usually after 15yr of age

ARPKD continuedARPKD continued Neonatal presentation with profound Neonatal presentation with profound
respiratory compromise secondary to respiratory compromise secondary to oligohydramniosoligohydramnios
Older Children (4-8y) hepatic disease Older Children (4-8y) hepatic disease predominatespredominates– 23% experience variceal bleeding by 12y23% experience variceal bleeding by 12y
Prenatal US-enlarged kidneys with Prenatal US-enlarged kidneys with increased echogenicityincreased echogenicity
In children, kidney size is typically at least 2 In children, kidney size is typically at least 2 standard deviations greater than normalstandard deviations greater than normal

Multicystic Dysplastic KidneyMulticystic Dysplastic Kidney Severe form in which the kidney consists of Severe form in which the kidney consists of
a group of cysts with some connective a group of cysts with some connective tissue, but no identifiable renal tissuetissue, but no identifiable renal tissue
Defect is an abnormality of ureteral bud Defect is an abnormality of ureteral bud leading to atresia or absence of ureterleading to atresia or absence of ureter
Often associated with antenatal obstruction Often associated with antenatal obstruction of urinary tract due to PUV, prune-belly, or of urinary tract due to PUV, prune-belly, or UPJUPJ
Most unilateral, left kidney affected most Most unilateral, left kidney affected most commonlycommonly

MCDK continuedMCDK continued Incidence 1:3000, boys>girlsIncidence 1:3000, boys>girls Most common cause of abdominal mass in Most common cause of abdominal mass in
newborn periodnewborn period– Palpable flank mass in otherwise healthy infantPalpable flank mass in otherwise healthy infant
Reported in a variety of syndromesReported in a variety of syndromes– Beckwith-Wiedemann, Trisomy 18, VACTERLBeckwith-Wiedemann, Trisomy 18, VACTERL

MCDK continuedMCDK continued
US-kidney grossly enlarged with loss of US-kidney grossly enlarged with loss of reniform shape and ureter is atretic or reniform shape and ureter is atretic or absent and multiple variably size, absent and multiple variably size, noncommunicating cysts separated by little noncommunicating cysts separated by little or no echogenic parenchymaor no echogenic parenchyma
DMSA absence of function in affected DMSA absence of function in affected kidneykidney
VCUG to evaluate for VURVCUG to evaluate for VUR US every 6-12mo until age 5 or involutionUS every 6-12mo until age 5 or involution

MCDK continuedMCDK continued
Role of nephrectomy controversialRole of nephrectomy controversial– Recommended to treat or prevent Recommended to treat or prevent
abdominal/flank pain, UTI, hypertension, or abdominal/flank pain, UTI, hypertension, or renal malignancyrenal malignancy
Lifetime follow up despite involution or Lifetime follow up despite involution or nephrectomy secondary to complicationsnephrectomy secondary to complications– Hypertension, UTI, proteinuria, renal Hypertension, UTI, proteinuria, renal
malignancymalignancy

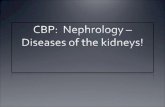
Multicystic Kidney on Ultrasound